ISOLATION PRECAUTIONS AND MANAGEMENT OF MULTIDRUG-RESISTANT ORGANISMS (MDROS) IN LONG-TERM CARE FACILITIES. Evelyn Cook, RN, CIC Associate Director
|
|
|
- Shana Allison
- 6 years ago
- Views:
Transcription


1 ISOLATION PRECAUTIONS AND MANAGEMENT OF MULTIDRUG-RESISTANT ORGANISMS (MDROS) IN LONG-TERM CARE FACILITIES Evelyn Cook, RN, CIC Associate Director
2 OBJECTIVES Review Isolation Precautions Review how Multi-drug Resistant Organisms (MDROs) emerge Review the management of MDROs

3 ISOLATION PRECAUTIONS
4 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings Jane D. Siegel, MD; Emily Rhinehart, RN MPH CIC; Marguerite Jackson, PhD; Linda Chiarello, RN MS; the Healthcare Infection Control Practices Advisory Committee
5 KEY CONCEPTS Risk of transmission of infectious agents occurs in all settings Infections are transmitted from patient-to-patient via HCPs hands or medical equipment/devices Isolation precautions are only part of a comprehensive IP program Unidentified patients who are colonized or infected represent risk to other patients
6 Administrative support FUNDAMENTAL ELEMENTS Adequate Infection Prevention staffing Good communication with clinical microbiology lab and environmental services A comprehensive educational program for HCPs, patients, and visitors Infrastructure support for surveillance, outbreak tracking, and data management
7 STANDARD PRECAUTIONS
8 Component Hand Hygiene Personal Protective Equipment (PPE) Gloves Gown Mask, eye protection Recommendation After touching blood, body fluids, secretions, excretions, contaminated items; immediately after removing gloves; between patient contacts. For touching blood, body fluids, secretions, excretions, contaminated items; for touching mucous membranes and non-intact skin During procedures and patient-care activities when contact of clothing/exposed skin with blood/body fluids, secretions, and excretions is anticipated During procedures and patient-care activities likely to generate splashes or sprays of blood, body fluids, secretions, especially suctioning, endotracheal intubation
9 THE GOLDEN RULES FOR HAND HYGIENE Hand hygiene must be performed exactly where you are delivering health care to patients (at the point-of-care) During health care delivery, there are 5 indications when it is essential that you perform hand hygiene To clean your hands, you should prefer handrubbing with an alcohol-based formulation, if available. Why? Because it makes hand hygiene possible right at the point-of-care, it is faster, more effective, and better tolerated. You should wash your hands with soap and water when visibly soiled, after care of resident with diarrhea, before and after eating or handling food, and after using the bathroom You must perform hand hygiene using the appropriate technique and time duration
10 Component Soiled equipment Environmental Control Laundry Needles and sharps Patient Resuscitation Recommendation Handle in a manner that prevents transfer of microorganisms to others and to the environment; wear gloves if visibly contaminated; perform hand hygiene Develop procedures for routine care, cleaning, and disinfection of environmental surfaces, especially frequently touched surfaces in patient-care areas Handle in a manner that prevents transfer of microorganisms to others and to the environment Do not recap, bend, break, or hand-manipulate used needles; if recapping is required, use a one-handed scoop technique only; use safety features when available; place used sharps in puncture-resistant container Use mouthpiece, resuscitation bag, other ventilation devices to prevent contact with mouth and oral secretions
11 Component Patient placement Respiratory hygiene/cough etiquette (source containment of infectious respiratory secretions in symptomatic patients, beginning at initial point of encounter) Recommendation Prioritize for single-patient room if patient is at increased risk of transmission, is likely to contaminate the environment, does not maintain appropriate hygiene, or is at increased risk of acquiring infection or developing adverse outcome following infection. Instruct symptomatic persons to cover mouth/nose when sneezing/coughing; use tissues and dispose in no-touch receptacle; observe hand hygiene after soiling of hands with respiratory secretions; wear surgical mask if tolerated or maintain spatial separation, >3 feet if possible.
12 RESPIRATORY HYGIENE/COUGH ETIQUETTE
13 RESPIRATORY HYGIENE/COUGH ETIQUETTE
14 Component Safe Injection Practices Special Lumbar Procedures Recommendation Apply to the use of needles, cannulas that replace needles, and, where applicable intravenous delivery systems Use aseptic technique Needles, cannulae and syringes are sterile, singleuse items Use single-dose vials for parenteral medications whenever possible Do not administer medications form single-dose vials or ampules to multiple patients Do not keep multidose vials in the immediate patient treatment area Do not use bags or bottles of IV solution as a common source of supply for multiple patients Wear a surgical mask when placing a catheter or injecting material into the spinal canal or subdural space
15 TRANSMISSION BASED PRECAUTIONS
16 Standard Precautions Transmission Based Precautions Isolation Precautions

17 Contact Droplet Direct Indirect Airborne Modes of Transmission Combination (contact + Airborne)
18 CRITERIA FOR ASSIGNING TRANSMISSION-BASED PRECAUTIONS Category is assigned if there was strong evidence for person-to-person transmission Category assignment reflects predominant mode(s) of transmission If no evidence of person-to-person transmission via major routes, use Standard Precautions Low risk for person-to-person transmission and no evidence of health-care associated transmission, use Standard Precautions

19 Private room or Cohort Gown and gloves prior to entry Hand hygiene Dedicate equipment Disinfect shared Limit patient equipment movement

20 C. difficile and Norovirus
21 CONDITIONS OR DISEASES REQUIRING CONTACT PRECAUTIONS Disease/Condition Anitbiotic Resistant Bacteria MRSA, VRE, ESBL-E.coli, etc. Duration of Isolation Until symptoms resolve Clostridium difficile (C. diff) hours after symptoms resolve Norovirus 48 hours after symptoms resolve Scabies and Lice 24 hours after treatment started Viral Conjunctivitis (pink eye) Until symptoms resolve
22 RESIDENT REQUIREMENTS CONTACT PRECAUTIONS Stay in Room, unless allowed to participate in activities Wash hands frequently Leaving Room Before and after activities Before and after eating After using bathroom Do not share personal items (razors, towel, etc.) with other residents

23 Surgical mask prior to entry No special ventilation Private room or Cohort Hand hygiene Residents use mask outside of room
24 CONDITIONS OR DISEASES REQUIRING DROPLET PRECAUTIONS Disease/Condition Seasonal Influenza Pandemic influenza Duration of Isolation Review the CDC seasonal guidance: for Droplet Precautions should be implemented for residents with suspected or confirmed influenza for 7 days after illness onset or until 24 hours after the resolution of fever and respiratory symptoms, whichever is longer, while a resident is in a health care facility. Droplet precautions for 5 days from onset of symptoms Meningococcal Diseases: meningitis, pneumonia MRSA pneumonia Strep Throat Rhinovirus (cold) For 24 hours after treatment has started For duration of illness (also use Contact Precautions) For 24 hours after treatment has started For duration of illness
25 RESIDENT REQUIREMENTS DROPLET PRECAUTIONS Stay in Room, unless necessary for therapy or treatment Wear a surgical mask when being transported outside of room. Wash hands frequently Leaving Room Before and after activities Before and after eating After using bathroom Observe Respiratory Hygiene/Cough Etiquette

26 Private room only Room requires Negative airflow pressure Doors must remain closed Everyone must wear an N- 95 respirator Limit the movement and transport of the Resident Hand hygiene before and after
27 TUBERCULOSIS Facility does not have a dedicated negative pressure room: Transfer resident to a facility capable of managing and evaluating resident Facility does have negative pressure room: Follow Airborne Precautions
28 CHICKENPOX AND SHINGLES Disease/Condition Chickenpox (varicella) Type and Duration of Isolation Airborne and Contact until lesions are dry and crusted Shingles (Herpes zoster. Varicella zoster) Localize in patient with intact immune system with lesions that can be contained/covered Disseminated disease in any patient Standard Precautions Airborne and Contact precautions for duration of illness Localized disease in immunocompromised patient until disseminated infection ruled out Airborne and Contact precautions for duration of illness Non-immune healthcare personnel should not care for residents with Chickenpox or Shingles
29 SYNDROMIC AND EMPIRIC APPLICATION OF TRANSMISSION-BASED PRECAUTIONS Diagnosis requires lab confirmation Culture-based lab test require 2 or more days Precautions should be implemented while awaiting results Based on clinical presentation and likely pathogen Reduces transmission opportunities
30 Clinical Syndrome or Condition Potential Pathogens Empiric Precautions (always includes Standard Precautions Diarrhea Acute diarrhea with infectious cause is incontinent or diapered patient Enteric Pathogens Contact Precautions Rash or Exanthems, generalized, unknown etiology Petechial/Ecchmotic w/ fever Neisseria meningitides Droplet Precautions for 1 st 24hrs of antimicrobial therapy Vesicular Respiratory Infections Cough/fever/upper lobe infiltrate Skin or Wound Infection Abscess or draining wound that cannot be covered Varicella-zoster, herpes simplex, vaccinia viruses Tb, Respiratory Viruses, S. pneumoniae, S. aureus Staphylococcus aureus, group A streptococcus Airborne plus Contact precautions Airborne Precautions plus contact Contact Precautions Add Droplet for the first 24 hours of antimicrobial therapy if group A strep disease suspected
31 DISCONTINUING TRANSMISSION-BASED PRECAUTIONS Remain in effect for limited period of time (i.e. while the risk for transmission persist or for the duration of illness) Disease specific recommendations in Appendix A of guideline Type and duration of precautions
32 COMMUNICATING PRECAUTIONS

33 You must post the sign on the door.
34 Room Airborne Droplet Contact Airborne Infectious Isolation (AII) room preferred; private room; door closed Private Room Preferred; door may remain open Private room preferred: Either disposable single-use or dedicated use of patient care equipment to one resident Hand Hygiene Standard Precautions Standard Precautions Standard Precautions Gloves Standard Precautions Standard Precautions Wear gloves upon entry and discard before leaving Gown Standard Precautions Standard Precautions Wear gown upon entry and discard before leaving Mask N-95 respirator or PAPR prior to entry Surgical mask upon entry Standard Precautions Eye Protection Standard Precautions Standard Precautions Standard Precautions
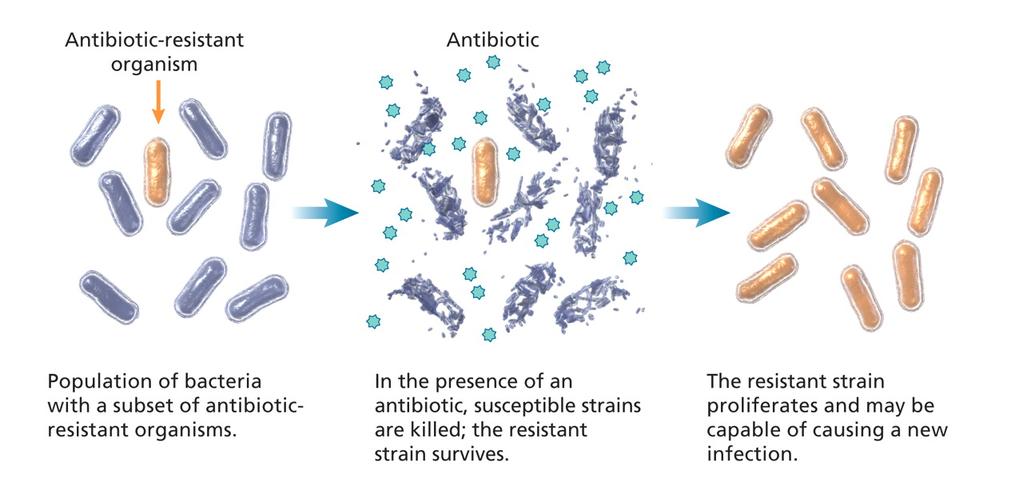
35 MANAGEMENT OF MULTI-DRUG RESISTANT ORGANISMS 2006

36 GROWING COMPLEXITY IN THE NH RESIDENT POPULATION Increased post-acute care population Growing medical complexity Increased exposure to devices, wounds, and antibiotics High prevalence of multidrug-resistant organisms
37 MDROS: EPIDEMIOLOGICALLY IMPORTANT PATHOGENS Any infectious agent that have one or more of the following characteristics 1. Propensity for transmission within facilities 2. Antimicrobial resistance implications 3. Associated with serious disease; increased morbidity and mortality 4. A newly discovered or re-emerging pathogen
38 MORE ON EPIDEMIOLOGICALLY IMPORTANT PATHOGENS Some really bad pathogens are not multi-drug resistant Norovirus Group A strep C. difficile Similar strategies used to control MDROs used to control pathogens other than MDROs
39 ABC S OF MDROS Bacteria Abbreviation Antibiotic Resistance Staphylococcus aureus MRSA Methicillin-resistant Enterococcus VRE Vancomycin-resistant (faecalis/faecium) Enterobacteraceae CRE Carbapenem-resistant (E. coli/klebsiella, etc) (KPC) Pseudomonas/ Acinetobacter MDR Many drug classes
40 MDRO DEVELOPMENT HEALTHCARE SETTINGS Antibiotic pressure Device utilization
41 ANTIBIOTIC PRESSURE

42 HOW RESISTANCE DEVELOPS IN BIOFILMS Bacteria with biofilms grow differently than free floating bacteria Antibiotics cannot penetrate the biofilm Bacteria within a biofilm talk to each other and share traits that allow some to become resistant


43 MDROS SPREAD IN HEALTHCARE SETTINGS Resident to resident transmission via healthcare provider s hands Environmental/equipment contamination
44 BACTERIAL CONTAMINATION OF HANDS PRIOR TO HAND HYGIENE IN A LTCF Gram negative were the most common bacteria cultured from hands Most Gram negative bacteria live in the bowels or colonize the urine!! Mody L, et al. Infect Control Hosp Epi. 2003; 24:165-71
45 Stiefel U, et al. ICHE 2011;32: ENVIRONMENT-TO-HAND-TO-PATIENT 40% 45% Pathogens can be transferred from healthcare surfaces to HCP hands without direct patient contact

46 RESERVOIR OF MDROS X marks the location where VRE was isolated in the room Image from Abstract: The risk of hand and glove contamination after contact with a VRE + patient environment. Hayden M, ICAAC, 2001, Chicago, Il.
47 SURVIVAL OF PATHOGENS ON SURFACES Pathogen Survival MRSA 7 days 7 months VRE 5 days 4 months Acinetobacter 3 days -5 months C. difficile (spores) 5 months Norovirus days Kramer A, et al (2006). BMC Infect Dis; 6:130

48 THOROUGHNESS OF CLEANING Mean = 32% Carling P, et al. APIC, 2012
49 INCREASED RISK FROM PRIOR OCCUPANT Otter J, et al. Infect Control Hosp Epidemiol. 2011; 32:
50 KEY MDRO PREVENTION STRATEGIES Assessing hand hygiene practices Quickly reporting MDRO lab results Implementing Contact Precautions Recognizing previously colonized residents Strategically place residents based on MDRO risk factors Careful device utilization Antibiotic stewardship Inter-facility communication
51 ASSESSING HAND HYGIENE Hand hygiene is one of the most effective measures to reduce HAIs and avoid preventable deaths Hand hygiene intervention should include: Easy access to soap and water/alcohol-based hand rubs Observation of practice particularly before and after contact with residents or their immediate environment Provide feedback on the spot feedback is preferred when failure is observed
52 REPORTING AND RECOGNITION OF MDRO LAB RESULTS Facilities should have a protocol for rapidly reporting positive MDRO lab results to clinicians Facilitates quick initiation of interventions Consider empiric precautions while awaiting lab results Contact precautions for resident with diarrhea
53 CONTACT PRECAUTIONS - YES, NO, OR MAYBE 54 y/o male transferred to your facility for short-term rehab following a total hip replacement Had a positive MRSA nasal swab pre-operatively no signs of active infection on admission Transferred with urinary catheter in place Do you place him on Contact Precautions?

54 CDC SAYS HICPAC, Management of MDROs in healthcare settings, 2006

55 Hand Hygiene Before/after PPE use During resident care Gown and Glove for direct resident care Don prior to room entry Remove prior to exit Dedicated non-essential items for resident care Decrease transmission BP cuffs, Stethoscopes, etc Private room or cohort resident if possible
56 DIFFICULTIES WITH CONTACT PRECAUTIONS Lack of private rooms and limited ability to move residents Determining the duration of Contact Precautions Unable to restrict resident mobility and socialization/therapy for long periods Unlikely to document clearance of carriage Large population of residents with unrecognized MDRO carriage
57 RECOGNIZING PRIOR COLONIZATION Residents can be colonized with MDROs for months Identifying previously colonized or infected residents allows for timely interventions Knowledge allows for planning the safest care For every known MDRO carrier, there are probably 3 others we don t know
58 RESIDENT PLACEMENT MDRO When single patient rooms are available assign priority for these rooms to individuals with known or suspected MDRO colonization or infection When not available, cohort patients with the same MDRO in the same room When cohorting (patients with the same MDRO) is not possible, place MDRO patients in rooms with ones who are at low risk for acquisition of MDROs and associated adverse outcomes from infection and are likely to have short length of stay CDC: Management of MDROs in Healthcare Settings, 2006
59 PLACEMENT OF RESIDENTS BASED ON RISK FACTORS Avoid placing 2 high-risk residents together Safer to cohort low-risk and high-risk residents Don t change stable room assignments based on culture results unless it poses new risk Long-term Roommates have already shared organisms in the past (even if you just learned about it)
60 HIGH-RISK RESIDENTS CONTACT PRECAUTIONS DURING DIRECT CARE High-risk exposures for MDRO transmission if known carrier and high-risk for acquisition if non-carrier Presence of wounds (fresh/new, multiple, increased stage/size, active drainage) Indwelling devices (IV lines, urinary catheters, tracheostomy, PEG tubes) Incontinence Current antibiotic use Dementia
61 RESIDENT CHARACTERISTICS TO CONSIDER THE 5 C S Cognitive function (understands directions) Cooperative (willing and able to follow directions) Continent (of urine or stool) Contained (secretions, excretions, or wounds) Cleanliness (capacity for personal hygiene) Kellar M. APIC Infection Connection. Fall 2010 ed.
62 WHEN TO USE CONTACT PRECAUTIONS AND RESTRICTED MOVEMENT Active symptoms of a contagious infection Nausea/vomiting New or worsening diarrhea New or worsening respiratory symptoms New, undiagnosed fever Precautions and restrictions are time limited Infection is ruled out and/or symptoms resolve
63 WHEN TO DISCONTINUE CONTACT PRECAUTIONS Resume Standard Precautions once high-risk exposures or active symptoms have discontinued Communication to care-givers and clear documentation of rationale is key
64 CASE 1 88 y/o old man recently returns to your facility following hospitalization for dehydration and UTI. Urine culture grew MRSA Resident is ambulatory and continent of urine Resident is alert, oriented and cooperative
65 DOES HE REQUIRE CONTACT PRECAUTIONS? Yes No
66 CASE 2 78 y/o woman admitted to your facility s/p 1 week stay in hospital and 1 week stay in rehab s/p broken hip repair. While in rehab she was noted to have purulent drainage from incision Culture was positive for MDR-Acinetobacter baumanii After transfer to your facility the resident is noted to be constantly removing the dressing and touching her incision Resident is disoriented and unable to follow instructions Drainage has increased and resident has a temperature of 101(F)
67 DOES THIS RESIDENT REQUIRE CONTACT PRECAUTIONS? Yes No
68 CASE 3 87 y/o man recently transferred to LTC following prolonged ICU stay Hospital course was complicated by C. difficile infection Resident is continuing to have 4-8 episodes of diarrhea daily and is incontinent Resident is complaining of sever abdominal cramps and now has a temperature of (F).
69 WHAT PRECAUTIONS ARE INDICATED? Standard Contact Enteric Contact Airborne
70 ONCE DIARRHEA RESOLVES, DO YOU NEED TO CULTURE THE STOOL AGAIN? Yes, we have to test to see if infection is resolved No, testing is not indicated in residents who have formed stool and are doing well clinically
71 PRACTICAL TIPS Maintain ongoing database of residents with history of MDRO carriage (known colonization or infection) Incorporate risk factors for MDRO carriage and acquisition into care planning Have protocols for implementing and discontinuing Contact Precautions Assess staff knowledge of MDRO transmission and steps for prevention HAND HYGIENE, HAND HYGIENE, HAND HYGIENE!!

72 THANKS!!! Evelyn Cook
Lightning Overview: Infection Control
 Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
Infection Prevention and Control and Isolation Authored by: Infection Prevention and Control Department
 Infection Prevention and Control and Isolation 2015 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention and Control and Isolation 2015 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases
 Infection Prevention Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases to yourself, family members,
Infection Prevention Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases to yourself, family members,
Infection Prevention and Control in Ambulatory Care Settings: Minimum Expectations for Safe Care
 Infection Prevention and Control in Ambulatory Care Settings: Minimum Expectations for Safe Care Melissa Schaefer, MD Division of Healthcare Quality Promotion Centers for Disease Control and Prevention
Infection Prevention and Control in Ambulatory Care Settings: Minimum Expectations for Safe Care Melissa Schaefer, MD Division of Healthcare Quality Promotion Centers for Disease Control and Prevention
Objectives. IPC Open calls - bi-weekly series. Introduction to Infection Prevention & Control (IPC) Open Call Series
 Open Call Series") Introduction to Infection Prevention & Control (IPC) Open Call Series #4 Transmission Precautions Isolate the Organism and Not the Resident Diane Dohm MT, IP, CIC, CPHQ MetaStar Anne Haddad, MPH MPRO March
Introduction to Infection Prevention & Control (IPC) Open Call Series #4 Transmission Precautions Isolate the Organism and Not the Resident Diane Dohm MT, IP, CIC, CPHQ MetaStar Anne Haddad, MPH MPRO March
Self-Instructional Packet (SIP)
") Self-Instructional Packet (SIP) Advanced Infection Prevention and Control Training Module 4 Transmission Based Precautions February 11, 2013 Page 1 Learning Objectives Module One Introduction to Infection
Self-Instructional Packet (SIP) Advanced Infection Prevention and Control Training Module 4 Transmission Based Precautions February 11, 2013 Page 1 Learning Objectives Module One Introduction to Infection
NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL
 NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL Infection Control Rev. 3/2018 Hand Hygiene Standard Precautions TOPICS Transmission-Based Precautions Personal Protective Equipment (PPE) Multiple
NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL Infection Control Rev. 3/2018 Hand Hygiene Standard Precautions TOPICS Transmission-Based Precautions Personal Protective Equipment (PPE) Multiple
ISOLATION PRECAUTIONS INTRODUCTION. Standard Precautions are used for all patient care situations, but they
 ISOLATION PRECAUTIONS INTRODUCTION Standard Precautions are used for all patient care situations, but they may not always be sufficient. If a patient is known or suspected to be infected with certain pathogens
ISOLATION PRECAUTIONS INTRODUCTION Standard Precautions are used for all patient care situations, but they may not always be sufficient. If a patient is known or suspected to be infected with certain pathogens
ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 CONTACT PRECAUTIONS... 4 DROPLET PRECAUTIONS... 6 ISOLATION PROCEDURES... 7
 ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 BARRIERS INDICATED IN STANDARD PRECAUTIONS... 2 PERSONAL PROTECTIVE EQUIPMENT... 3 CONTACT PRECAUTIONS... 4 RESIDENT PLACEMENT... 4 RESIDENT TRANSPORT...
ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 BARRIERS INDICATED IN STANDARD PRECAUTIONS... 2 PERSONAL PROTECTIVE EQUIPMENT... 3 CONTACT PRECAUTIONS... 4 RESIDENT PLACEMENT... 4 RESIDENT TRANSPORT...
INFECTION C ONTROL CONTROL CONTROL EDUCATION PROGRAM
 INFECTION CONTROL EDUCATION PROGRAM Isolation Precautions Isolating the disease not the patient The Purpose is To protect compromised patient from environment To prevent the spread of communicable diseases.
INFECTION CONTROL EDUCATION PROGRAM Isolation Precautions Isolating the disease not the patient The Purpose is To protect compromised patient from environment To prevent the spread of communicable diseases.
Emergency Department Isolation Precautions
 Carolinas HealthCare System Department of Infection Prevention I. SCOPE Emergency Department Isolation Precautions This policy applies to all Carolinas HealthCare System Emergency Department (ED) locations
Carolinas HealthCare System Department of Infection Prevention I. SCOPE Emergency Department Isolation Precautions This policy applies to all Carolinas HealthCare System Emergency Department (ED) locations
Infection Prevention and Control Annual Education Authored by: Infection Prevention and Control Department
 Infection Prevention and Control Annual Education 2013 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention and Control Annual Education 2013 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
THE INFECTION CONTROL STAFF
 INFECTION CONTROL THE INFECTION CONTROL STAFF INTEGRIS BAPTIST V. Ramgopal, M.D., Hospital Epidemiologist Gwen Harington, RN, BSN, CIC, Infection Control Specialist Kathy Knecht, RN, Surveillance Coordinator
INFECTION CONTROL THE INFECTION CONTROL STAFF INTEGRIS BAPTIST V. Ramgopal, M.D., Hospital Epidemiologist Gwen Harington, RN, BSN, CIC, Infection Control Specialist Kathy Knecht, RN, Surveillance Coordinator
Infection Prevention and Control for Phlebotomy
 Page 1 of 10 POLICY STATEMENT: It is Sunnybrook s Policy to prevent the spread of infection within the health care institution from patient to patient, patient to staff, staff to patient by: a) providing
Page 1 of 10 POLICY STATEMENT: It is Sunnybrook s Policy to prevent the spread of infection within the health care institution from patient to patient, patient to staff, staff to patient by: a) providing
Department of Infection Control and Hospital Epidemiology. New Employee Orientation
 Department of Infection Control and Hospital Epidemiology New Employee Orientation Infection Control Contact Information Office 350 Parnassus Ave, Suite 510 Main Office Phone: 353-4343 Practitioner On-Call:
Department of Infection Control and Hospital Epidemiology New Employee Orientation Infection Control Contact Information Office 350 Parnassus Ave, Suite 510 Main Office Phone: 353-4343 Practitioner On-Call:
Infection Control Prevention Strategies. For Clinical Personnel
 Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
TRANSMISSION-BASED PRECAUTIONS
 TRANSMISSION-BASED PRECAUTIONS PRECAUTIONS Standard Precautions infection prevention practices used with all patients regardless of suspected or confirmed diagnosis. Based on the principle that all blood,
TRANSMISSION-BASED PRECAUTIONS PRECAUTIONS Standard Precautions infection prevention practices used with all patients regardless of suspected or confirmed diagnosis. Based on the principle that all blood,
2014 Annual Continuing Education Module. Contents
 This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Content Experts: Infection Prevention Target Audience: All Teammates
This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Content Experts: Infection Prevention Target Audience: All Teammates
Standard Precautions (SP) & Transmission-Based Isolation Policies
 & Transmission-Based Isolation Policies") SJMHS Infection Control Policy Standard Precautions (SP) & Transmission-Based Isolation Policies Control of Communicable Disease Section Number 3 Policy Number 1.1 Effective Date: 11/63 Revised Date: 9/96,
SJMHS Infection Control Policy Standard Precautions (SP) & Transmission-Based Isolation Policies Control of Communicable Disease Section Number 3 Policy Number 1.1 Effective Date: 11/63 Revised Date: 9/96,
PRECAUTIONS IN INFECTION CONTROL
 PRECAUTIONS IN INFECTION CONTROL Standard precautions Transmission-based precautions Contact precautions Airborne precautions Droplet precautions 1 2/25/2015 WHO HAVE TO PROTECT IN HOSPITALS? Patients
PRECAUTIONS IN INFECTION CONTROL Standard precautions Transmission-based precautions Contact precautions Airborne precautions Droplet precautions 1 2/25/2015 WHO HAVE TO PROTECT IN HOSPITALS? Patients
Infection Control Prevention Strategies. For Clinical Personnel
 Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
SECTION: PATIENT RELATED INFECTION CONTROL NUMBER: 2.1 TRANSMISSION BASED PRECAUTIONS
 University of Connecticut Health Center Page 1 of 8 SECTION: PATIENT RELATED INFECTION CONTROL NUMBER: 2.1 TRANSMISSION BASED PRECAUTIONS PURPOSE: Transmission-Based s are designed for patients documented
University of Connecticut Health Center Page 1 of 8 SECTION: PATIENT RELATED INFECTION CONTROL NUMBER: 2.1 TRANSMISSION BASED PRECAUTIONS PURPOSE: Transmission-Based s are designed for patients documented
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals
 Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Personal Hygiene & Protective Equipment. NEO111 M. Jorgenson, RN BSN
 Personal Hygiene & Protective Equipment NEO111 M. Jorgenson, RN BSN Hand Hygiene the single most effective way to help prevent the spread of infections agents. (CDC, 2002.) Consistency & Compliancy 50%
Personal Hygiene & Protective Equipment NEO111 M. Jorgenson, RN BSN Hand Hygiene the single most effective way to help prevent the spread of infections agents. (CDC, 2002.) Consistency & Compliancy 50%
Isolation Categories of Transmission-Based Precautions
 Isolation Categories of Transmission-Based Highlights Policy Statement Standard shall be used when caring for residents at all times regardless of their suspected or confirmed infection status. Transmission-Based
Isolation Categories of Transmission-Based Highlights Policy Statement Standard shall be used when caring for residents at all times regardless of their suspected or confirmed infection status. Transmission-Based
Routine Practices. Infection Prevention and Control
 Routine Practices Infection Prevention and Control Routine Practices Elements of Routine Practices: Risk assessment + hand hygiene + personal protective equipment Environmental controls (patient placement,
Routine Practices Infection Prevention and Control Routine Practices Elements of Routine Practices: Risk assessment + hand hygiene + personal protective equipment Environmental controls (patient placement,
CPNE CLINICAL PERFORMANCE IN NURSING EXAMINATION
 22nd edition CPNE CLINICAL PERFORMANCE IN NURSING EXAMINATION Infection Control Module No part of this publication may be reproduced or distributed in any form or by any means, or stored in a database
22nd edition CPNE CLINICAL PERFORMANCE IN NURSING EXAMINATION Infection Control Module No part of this publication may be reproduced or distributed in any form or by any means, or stored in a database
STOP CONTACT PRECAUTIONS. Staff: Families and visitors: Please report to staff before entering. Required: - Gown & Gloves. Bed #
 CONTACT PRECAUTIONS Clean hs Clean hs with A) h foam/gel or B) soap water HOUSEER will - Gown & Gloves Point-of-Care Risk When there is a risk of splash or spray, wear face eye. For more information, refer
CONTACT PRECAUTIONS Clean hs Clean hs with A) h foam/gel or B) soap water HOUSEER will - Gown & Gloves Point-of-Care Risk When there is a risk of splash or spray, wear face eye. For more information, refer
Principles of Infection Prevention and Control
 Principles of Infection Prevention and Control Liz Van Horne Manager, Core Competencies Senior Infection Prevention & Control Professional OAHPP Outbreak Management Workshop September 15, 2010 Objectives
Principles of Infection Prevention and Control Liz Van Horne Manager, Core Competencies Senior Infection Prevention & Control Professional OAHPP Outbreak Management Workshop September 15, 2010 Objectives
INFECTION CONTROL POLICY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT
 Of, INFECTION CONTROL POLICY DEPARTMENT OF RADIOLOGY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT GENERAL The Department of Radiology adheres to the Duke Infection Control policies and the DUMC Exposure Control
Of, INFECTION CONTROL POLICY DEPARTMENT OF RADIOLOGY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT GENERAL The Department of Radiology adheres to the Duke Infection Control policies and the DUMC Exposure Control
POLICIES & PROCEDURES. Number: Authorization: SHR Regional Infection Control Committee
 POLICIES & PROCEDURES Number: 30-40 Title: Signage Authorization: SHR Regional Infection Control Committee Source: Infection Prevention & Control Date Initiated: June 5, 2001 Date Reaffirmed: March, 2007
POLICIES & PROCEDURES Number: 30-40 Title: Signage Authorization: SHR Regional Infection Control Committee Source: Infection Prevention & Control Date Initiated: June 5, 2001 Date Reaffirmed: March, 2007
BEHAVIORAL HEALTH & LTC. Mary Ann Kellar, RN, MA, CHES, IC March 2011
 BEHAVIORAL HEALTH & LTC Mary Ann Kellar, RN, MA, CHES, IC March 2011 CDC Isolation Guidelines-adapting to special environments MDRO s CMS-F 441 C.difficile Norovirus Federal (CMS), State & Joint Commission
BEHAVIORAL HEALTH & LTC Mary Ann Kellar, RN, MA, CHES, IC March 2011 CDC Isolation Guidelines-adapting to special environments MDRO s CMS-F 441 C.difficile Norovirus Federal (CMS), State & Joint Commission
Infection Prevention, Control & Immunizations
 Infection Control: This facility task must be used to investigate compliance at F880, F881, and F883. For the purpose of this task, staff includes employees, consultants, contractors, volunteers, and others
Infection Control: This facility task must be used to investigate compliance at F880, F881, and F883. For the purpose of this task, staff includes employees, consultants, contractors, volunteers, and others
Infection Prevention and Control Annual Education 2010
 Infection Prevention and Control Annual Education 2010 Authored by: Cathy Clark, RN MPH CIC Mary Whitaker, RN CIC Bola Ogundimu, RN MPH Marie Commiskey, RN CCRN CIC Modified for affiliated schools students
Infection Prevention and Control Annual Education 2010 Authored by: Cathy Clark, RN MPH CIC Mary Whitaker, RN CIC Bola Ogundimu, RN MPH Marie Commiskey, RN CCRN CIC Modified for affiliated schools students
Infection Prevention and Control
 Infection Prevention and Control Infection Prevention and Control Program IPAC program consists of three healthcare professionals IPAC department is located on the 9 th floor and is available Monday to
Infection Prevention and Control Infection Prevention and Control Program IPAC program consists of three healthcare professionals IPAC department is located on the 9 th floor and is available Monday to
DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE)
") DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE) Course Health Science Unit VII Infection Control Essential Question What must health care workers do to protect themselves and others
DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE) Course Health Science Unit VII Infection Control Essential Question What must health care workers do to protect themselves and others
Infection Control and Prevention On-site Review Tool Hospitals
 Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
STANDARD PRECAUTIONS POLICY Page 1 of 8 Reviewed: May 2017
 Page 1 of 8 Policy Applies to: All Mercy Staff, Credentialed Specialists, Allied Health Professionals, students, patients, visitors and contractors will be supported to meet policy requirements Related
Page 1 of 8 Policy Applies to: All Mercy Staff, Credentialed Specialists, Allied Health Professionals, students, patients, visitors and contractors will be supported to meet policy requirements Related
Single room with negative pressure ventilation in relation to surrounding areas
 7. Airborne/Contact Precautions 7.1 Introduction Airborne/Contact Precautions are required for patients diagnosed with, or suspected of having an infectious microorganism transmitted by the airborne and
7. Airborne/Contact Precautions 7.1 Introduction Airborne/Contact Precautions are required for patients diagnosed with, or suspected of having an infectious microorganism transmitted by the airborne and
Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 3 Strategies to prevent
 Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 3 Strategies to prevent Nimalie D. Stone, MD,MS Division of Healthcare Quality Promotion National
Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 3 Strategies to prevent Nimalie D. Stone, MD,MS Division of Healthcare Quality Promotion National
PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards. Infection Prevention and Control: Personal Protective Equipment
 PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards : Personal Protective Equipment PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards 2016 PERSONAL PROTECTIVE EQUIPMENT Personal protective
PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards : Personal Protective Equipment PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards 2016 PERSONAL PROTECTIVE EQUIPMENT Personal protective
Approval Signature: Date of Approval: December 6, 2007 Review Date:
 Personal Care Home/Long Term Care Facility Infection Prevention and Control Program Operational Directive Management of Methicillin-Resistant Staphylococcus Aureus (MRSA) Approval Signature: Supercedes:
Personal Care Home/Long Term Care Facility Infection Prevention and Control Program Operational Directive Management of Methicillin-Resistant Staphylococcus Aureus (MRSA) Approval Signature: Supercedes:
INFECTION CONTROL ORIENTATION TRAINING 2009
 INFECTION CONTROL ORIENTATION TRAINING 2009 STANDARD PRECAUTIONS BASICALLY. If it s WET and NOT YOURS, don t get any on you!! PPE And Safety Devices Are Provided!! Use them correctly to protect yourself!!
INFECTION CONTROL ORIENTATION TRAINING 2009 STANDARD PRECAUTIONS BASICALLY. If it s WET and NOT YOURS, don t get any on you!! PPE And Safety Devices Are Provided!! Use them correctly to protect yourself!!
Safe Care Is in YOUR HANDS
 Safe Care Is in YOUR HANDS 1 in25 patients has a Healthcare-Associated Infection Would you like to be part of prevention? It s EASY and we can start TODAY! STOP the spread of germs! Hand Hygiene Before
Safe Care Is in YOUR HANDS 1 in25 patients has a Healthcare-Associated Infection Would you like to be part of prevention? It s EASY and we can start TODAY! STOP the spread of germs! Hand Hygiene Before
Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings
 in Healthcare Settings") Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings : Program Goal Improve personnel safety in the healthcare environment through appropriate use of PPE. :
Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings : Program Goal Improve personnel safety in the healthcare environment through appropriate use of PPE. :
Vancomycin-Resistant Enterococcus (VRE)
") Approved by: Vancomycin-Resistant Enterococcus (VRE) Vice President & Chief Medical Officer Corporate Policy & Procedures Manual VI-40 Date Approved July 14, 2016 August 12, 2016 Next Review (3 years from
Approved by: Vancomycin-Resistant Enterococcus (VRE) Vice President & Chief Medical Officer Corporate Policy & Procedures Manual VI-40 Date Approved July 14, 2016 August 12, 2016 Next Review (3 years from
INFECTION CONTROL ORIENTATION TRAINING 2006
 INFECTION CONTROL ORIENTATION TRAINING 2006 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
INFECTION CONTROL ORIENTATION TRAINING 2006 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
Infection Prevention Isolation Precautions Toolkit
 Infection Prevention Isolation Precautions Toolkit The toolkit provides: Link(s) to revised Isolation Policy on The Point Link to ICON training video and key changes to policy (NEW) Quick Review Chart
Infection Prevention Isolation Precautions Toolkit The toolkit provides: Link(s) to revised Isolation Policy on The Point Link to ICON training video and key changes to policy (NEW) Quick Review Chart
Infection Control and Prevention On-site Review Tool Hospitals
 Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
DEPARTMENTAL POLICY. Northwestern Memorial Hospital
 Northwestern Memorial Hospital DEPARTMENTAL POLICY Subject: INFECTION CONTROL AND PREVENTION Title: ISOLATION PRECAUTIONS 1 of 8 Revision of: 04/2004 Policy # Effective Date: 01/2007 I. PURPOSE: Appropriate
Northwestern Memorial Hospital DEPARTMENTAL POLICY Subject: INFECTION CONTROL AND PREVENTION Title: ISOLATION PRECAUTIONS 1 of 8 Revision of: 04/2004 Policy # Effective Date: 01/2007 I. PURPOSE: Appropriate
Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home
 Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home Nimalie D. Stone, MD,MS Ambulatory and Long-term Care Team Division of Healthcare Quality Promotion
Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home Nimalie D. Stone, MD,MS Ambulatory and Long-term Care Team Division of Healthcare Quality Promotion
1/28/2014. Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home. Thank you to AANAC
 Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home Nimalie D. Stone, MD,MS Ambulatory and Long-term Care Team Division of Healthcare Quality Promotion
Take Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home Nimalie D. Stone, MD,MS Ambulatory and Long-term Care Team Division of Healthcare Quality Promotion
Fall HOLLY ALEXANDER Academic Coordinator of Clinical Education MS157
 Fall 2010 HOLLY ALEXANDER Academic Coordinator of Clinical Education 609-570-3478 AlexandH@mccc.edu MS157 To reduce infection & prevent disease transmission Nosocomial Infection: an infection acquired
Fall 2010 HOLLY ALEXANDER Academic Coordinator of Clinical Education 609-570-3478 AlexandH@mccc.edu MS157 To reduce infection & prevent disease transmission Nosocomial Infection: an infection acquired
Name of Assessor Unit Date. Element Yes No Action Needed
 Figure 10.5 Checklist: Contact Precautions Name of Assessor Unit Date Element Yes No Action Needed CONTACT PRECAUTIONS GENERAL Contact Precautions are used for patients with known or suspected infections
Figure 10.5 Checklist: Contact Precautions Name of Assessor Unit Date Element Yes No Action Needed CONTACT PRECAUTIONS GENERAL Contact Precautions are used for patients with known or suspected infections
Welcome to the Cooper Infection Prevention Team
 Welcome to the Cooper Infection Prevention Team We Need YOU on the Team Healthcare Associated Infections Increase Morbidity & Mortality (Pain, Suffering and Death) CDC estimates that each year about 2
Welcome to the Cooper Infection Prevention Team We Need YOU on the Team Healthcare Associated Infections Increase Morbidity & Mortality (Pain, Suffering and Death) CDC estimates that each year about 2
Part III: Precautions to Prevent Transmission of Infectious Agents There
 Part III: Precautions to Prevent Transmission of Infectious Agents There are two tiers of HICPAC/CDC precautions to prevent transmission of infectious agents, Standard Precautions and Transmission-Based
Part III: Precautions to Prevent Transmission of Infectious Agents There are two tiers of HICPAC/CDC precautions to prevent transmission of infectious agents, Standard Precautions and Transmission-Based
IC CONTACT and CONTACT PLUS PRECAUTIONS REV. JULY 2017
 IC.04.03 CONTACT and CONTACT PLUS PRECAUTIONS REV. JULY 2017 Standard In addition to Routine Practices, Contact Precautions or Contact Plus Precautions will be used for patients known or suspected to have
IC.04.03 CONTACT and CONTACT PLUS PRECAUTIONS REV. JULY 2017 Standard In addition to Routine Practices, Contact Precautions or Contact Plus Precautions will be used for patients known or suspected to have
Standard Precautions & Managing High risk cases. Tuminah Binti Jantan (SRN)
") Standard Precautions & Managing High risk cases Tuminah Binti Jantan (SRN) Outline 1. Infection risk 2. Infection control in dental practice 3. Standard precautions 4. The element of SP (sharps injury)
Standard Precautions & Managing High risk cases Tuminah Binti Jantan (SRN) Outline 1. Infection risk 2. Infection control in dental practice 3. Standard precautions 4. The element of SP (sharps injury)
& ADDITIONAL PRECAUTIONS:
 INFECTION CONTROL GUIDELINES: STANDARD PRECAUTIONS & ADDITIONAL PRECAUTIONS: LESSON PLAN Lesson overview Time: One hour This lesson covers the guidelines developed by the U.S. Centers for Disease Control
INFECTION CONTROL GUIDELINES: STANDARD PRECAUTIONS & ADDITIONAL PRECAUTIONS: LESSON PLAN Lesson overview Time: One hour This lesson covers the guidelines developed by the U.S. Centers for Disease Control
ACG GI Practice Toolbox. Developing an Infection Control Plan for Your Office
 ACG GI Practice Toolbox Developing an Infection Control Plan for Your Office AUTHOR: Louis J. Wilson, MD, FACG, Wichita Falls Gastroenterology Associates, Wichita Falls, Texas INTRODUCTION: Preventing
ACG GI Practice Toolbox Developing an Infection Control Plan for Your Office AUTHOR: Louis J. Wilson, MD, FACG, Wichita Falls Gastroenterology Associates, Wichita Falls, Texas INTRODUCTION: Preventing
A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page
 Page 1 A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page IH0400: Contact Precautions EFFECTIVE DATE: September
Page 1 A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page IH0400: Contact Precautions EFFECTIVE DATE: September
Everyone Involved in providing healthcare should adhere to the principals of infection control.
 Infection Control Introduction The prevention and control of infection is an integral part of the role of all health care personnel. Healthcare Associated Infections (HCAIs) affect an estimated one in
Infection Control Introduction The prevention and control of infection is an integral part of the role of all health care personnel. Healthcare Associated Infections (HCAIs) affect an estimated one in
Infection Prevention & Exposure Control Online Orientation. Kimberly Koerner RN, BSN Associate Health Nurse
 Infection Prevention & Exposure Control Online Orientation Kimberly Koerner RN, BSN Associate Health Nurse Created in 2015 Reviewed/Edited Jan 2017 Hand Hygiene Adherence to hand hygiene guidelines among
Infection Prevention & Exposure Control Online Orientation Kimberly Koerner RN, BSN Associate Health Nurse Created in 2015 Reviewed/Edited Jan 2017 Hand Hygiene Adherence to hand hygiene guidelines among
Investigating Clostridium difficile Infections
 CALIFORNIA DEPARTMENT OF PUBLIC HEALTH Investigating Clostridium difficile Infections Erin P. Garcia, MPH, CPH Healthcare-Associated Infections (HAI) Program Center for Health Care Quality California Department
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH Investigating Clostridium difficile Infections Erin P. Garcia, MPH, CPH Healthcare-Associated Infections (HAI) Program Center for Health Care Quality California Department
INFECTION CONTROL ORIENTATION TRAINING 2006
 INFECTION CONTROL ORIENTATION TRAINING 2006 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
INFECTION CONTROL ORIENTATION TRAINING 2006 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
Developed in response to: Best Practice Infection Prevention and Control
 Transfer of patients within MEHT Clinical Guideline Developed in response to: Best Practice Infection Prevention and Control Version Number 1.0 Issuing Directorate Corporate Governance Approved by Clinical
Transfer of patients within MEHT Clinical Guideline Developed in response to: Best Practice Infection Prevention and Control Version Number 1.0 Issuing Directorate Corporate Governance Approved by Clinical
Replaces: 08/11/16. Formulated: 1/2000 TRANSMISSION-BASED PRECAUTIONS
 CMHC INFECTION CONTROL Effective : 08/10/17 Page 1 of 4 POLICY: TDCJ and any medical contractors will implement Transmission-Based Precautions as needed to interrupt the transmission of potentially contagious
CMHC INFECTION CONTROL Effective : 08/10/17 Page 1 of 4 POLICY: TDCJ and any medical contractors will implement Transmission-Based Precautions as needed to interrupt the transmission of potentially contagious
The Role of Isolation and Contact Precautions in the Elimination of Transmission of MRSA
 The Role of Isolation and Contact Precautions in the Elimination of Transmission of MRSA Marcia Patrick, RN, MSN, CIC Infection Control Director MultiCare Health System Tacoma, WA APIC/BD MRSA Presentation
The Role of Isolation and Contact Precautions in the Elimination of Transmission of MRSA Marcia Patrick, RN, MSN, CIC Infection Control Director MultiCare Health System Tacoma, WA APIC/BD MRSA Presentation
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION
 NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
Erlanger Infection Control Program. Resident Resident Orientation and. and
 Erlanger Infection Control Program Resident Resident Orientation Orientation and and Bloodborne Bloodborne Pathogen Pathogen Review Review 2008-2009 2009 1 Outline 1. Healthcare associated infections 2.
Erlanger Infection Control Program Resident Resident Orientation Orientation and and Bloodborne Bloodborne Pathogen Pathogen Review Review 2008-2009 2009 1 Outline 1. Healthcare associated infections 2.
8. Droplet/Contact Precautions. 8.1 Introduction
 8. Droplet/Contact Precautions 8.1 Introduction Droplet/Contact Precautions are required for patients diagnosed with, or suspected of having infectious microorganisms transmitted by the droplet route and
8. Droplet/Contact Precautions 8.1 Introduction Droplet/Contact Precautions are required for patients diagnosed with, or suspected of having infectious microorganisms transmitted by the droplet route and
Objectives. Hot Topics in Infection Prevention and Control in Post Acute Care Settings. NADONA Infection Prevention and Control Webinar Series
 Hot Topics in Infection Prevention and Control in Post Acute Care Settings J. Hudson Garrett Jr., PhD, MSN, MPH, FNP BC, PLNC, CDONA, VA BC, FACDONA PRESENTS Hot Topics in Infection Prevention and Control
Hot Topics in Infection Prevention and Control in Post Acute Care Settings J. Hudson Garrett Jr., PhD, MSN, MPH, FNP BC, PLNC, CDONA, VA BC, FACDONA PRESENTS Hot Topics in Infection Prevention and Control
Carbapenemase Producing Enterobacteriaceae (CPE) Prevention and Management Toolkit for Inpatient Areas
 Prevention and Management Toolkit for Inpatient Areas") Carbapenemase Producing Enterobacteriaceae (CPE) Prevention and Management Toolkit for Inpatient Areas This toolkit includes examples advice leaflets and forms which may be helpful for use by teams or
Carbapenemase Producing Enterobacteriaceae (CPE) Prevention and Management Toolkit for Inpatient Areas This toolkit includes examples advice leaflets and forms which may be helpful for use by teams or
Infection Control Policy and Procedure Manual. Post-Anesthesia Care Unit (Recovery Room) Page 1 of 6
 Page 1 of 6") (Recovery Room) Page 1 of 6 Purpose: The purpose of this policy is to establish infection prevention guidelines to prevent or minimize transmission of infections in the. Policy: All personnel will adhere
(Recovery Room) Page 1 of 6 Purpose: The purpose of this policy is to establish infection prevention guidelines to prevent or minimize transmission of infections in the. Policy: All personnel will adhere
INTERIM INFECTION PREVENTION AND CONTROL GUIDELINES NOVEL A/H1N1 INFLUENZA
 EXECUTIVE SUMMARY: INTERIM INFECTION PREVENTION AND CONTROL GUIDELINES NOVEL A/H1N1 INFLUENZA This Infection Prevention and Control Guideline is intended for health care workers in the management of suspect
EXECUTIVE SUMMARY: INTERIM INFECTION PREVENTION AND CONTROL GUIDELINES NOVEL A/H1N1 INFLUENZA This Infection Prevention and Control Guideline is intended for health care workers in the management of suspect
Enterobacteriaceae. Preventing the Spread of Carbapenemresistant. in LTCFs. Nimalie D. Sto ne, MD, MS CDC Division of Healthcare Quality Promotion
 Preventing the Spread of Carbapenemresistant Enterobacteriaceae in LTCFs Nimalie D. Sto ne, MD, MS CDC Division of Healthcare Quality Promotion March 29, 2016 Preventing the Spread of Carbapenemresistant
Preventing the Spread of Carbapenemresistant Enterobacteriaceae in LTCFs Nimalie D. Sto ne, MD, MS CDC Division of Healthcare Quality Promotion March 29, 2016 Preventing the Spread of Carbapenemresistant
Infection Control in Healthcare. Facilities
 Infection Control in Healthcare Basic Principles Facilities Hand Hygiene / Respiratory Etiquette Exclusion of ill staff and visitors Standard and droplet precautions Facility-specific measures Hospitals
Infection Control in Healthcare Basic Principles Facilities Hand Hygiene / Respiratory Etiquette Exclusion of ill staff and visitors Standard and droplet precautions Facility-specific measures Hospitals
08/09/ elements required for Infection to occur. Chain of Infection. Evolution of Standard & Transmission Based Precautions
 Helen Murphy, Infection Prevention & Control Nurse Manager, Health Protection Surveillance Centre HPSC/RCPI 2017 Safe Patient Care Course Chain of Infection Evolution of Standard & Transmission Based Precautions
Helen Murphy, Infection Prevention & Control Nurse Manager, Health Protection Surveillance Centre HPSC/RCPI 2017 Safe Patient Care Course Chain of Infection Evolution of Standard & Transmission Based Precautions
Guidelines for the Management of C. difficile Infections in. Healthcare Settings. Saskatchewan Infection Prevention and Control Program November 2015
 Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
Standard Precautions
 Standard Precautions Speciality: Infection Control 1. Indications 1.1 Background Standard Precautions This definition broadens the coverage of the previously known Universal Precautions by recognizing
Standard Precautions Speciality: Infection Control 1. Indications 1.1 Background Standard Precautions This definition broadens the coverage of the previously known Universal Precautions by recognizing
Cystic Fibrosis Foundation Recommendations
 Hospital Epidemiology and Infection Control Department Presenters: Sandra Kistler, RN, PHN, MSN, ICP Cystic Fibrosis Foundation Recommendations Contact Precautions for ALL patients with Cystic Fibrosis
Hospital Epidemiology and Infection Control Department Presenters: Sandra Kistler, RN, PHN, MSN, ICP Cystic Fibrosis Foundation Recommendations Contact Precautions for ALL patients with Cystic Fibrosis
Clinical Research in Antibiotic Resistance
 Clinical Research in Antibiotic Resistance Mary-Claire Roghmann, MD, MS Professor of Epidemiology and Public Health and Medicine Assocaite Hospital Epidemiologist, Staff Physician and Research Health Scientist
Clinical Research in Antibiotic Resistance Mary-Claire Roghmann, MD, MS Professor of Epidemiology and Public Health and Medicine Assocaite Hospital Epidemiologist, Staff Physician and Research Health Scientist
NA REVIEWED/REVISED: DATE TO BE REVIEWED: 01/31/2016 EMERGENCY MEDICAL SERVICES
 POLICY NO: 545 DATE ISSUED: 10/14/2014 DATE NA REVIEWED/REVISED: DATE TO BE REVIEWED: 01/31/2016 EMERGENCY MEDICAL SERVICES Purpose: The purpose of this policy is to state the minimum standards for infection
POLICY NO: 545 DATE ISSUED: 10/14/2014 DATE NA REVIEWED/REVISED: DATE TO BE REVIEWED: 01/31/2016 EMERGENCY MEDICAL SERVICES Purpose: The purpose of this policy is to state the minimum standards for infection
ASSESSMENT ACTIVITY ANSWER PACK
 ASSESSMENT ACTIVITY ANSWER PACK 1 Assessment Activity 1: What is Source Isolation?.. Briefly summarise why some patients require Source Isolation Care. Some patients infected or colonised with certain
ASSESSMENT ACTIVITY ANSWER PACK 1 Assessment Activity 1: What is Source Isolation?.. Briefly summarise why some patients require Source Isolation Care. Some patients infected or colonised with certain
Newborn Nursery/Neonatal Intensive Care Unit
 Newborn Nursery/Neonatal Intensive Care Unit Ref:(a) The Association for Professionals in Infection Control and Epidemiology, Principles and Practice, 1996. (b) Hospital Epidemiology and Infection Control,
Newborn Nursery/Neonatal Intensive Care Unit Ref:(a) The Association for Professionals in Infection Control and Epidemiology, Principles and Practice, 1996. (b) Hospital Epidemiology and Infection Control,
INFECTION CONTROL ORIENTATION TRAINING 2004
 INFECTION CONTROL ORIENTATION TRAINING 2004 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
INFECTION CONTROL ORIENTATION TRAINING 2004 INFECTION CONTROL OSHA BLOODBORNE PATHOGEN STANDARD STANDARD PRECAUTIONS RISK OF EXPOSURE TO CONTAMINATED MATERIALS USE OF PROTECTIVE EQUIPMENT FOLLOW-UP OF
INFECTION PREVENTION, BLOODBORNE PATHOGENS AND SAFETY: STUDENT ORIENTATION
 1 ORIENTATION MODULE #1: INFECTION PREVENTION, BLOODBORNE PATHOGENS AND SAFETY: STUDENT ORIENTATION For Clinical Students and Instructors FVHCA Member Clinical Sites Revised September 26, 2013 Used with
1 ORIENTATION MODULE #1: INFECTION PREVENTION, BLOODBORNE PATHOGENS AND SAFETY: STUDENT ORIENTATION For Clinical Students and Instructors FVHCA Member Clinical Sites Revised September 26, 2013 Used with
Assessment and Educational Tools. Marilyn Weinmaster RN BScN CIC CHICA-SASKPIC September 20,2013
 Assessment and Educational Tools Marilyn Weinmaster RN BScN CIC CHICA-SASKPIC September 20,2013 Present Context Describe Assessment and Educational Tools Demonstrate Point of Care Risk Assessment Introduce
Assessment and Educational Tools Marilyn Weinmaster RN BScN CIC CHICA-SASKPIC September 20,2013 Present Context Describe Assessment and Educational Tools Demonstrate Point of Care Risk Assessment Introduce
a. Goggles b. Gowns c. Gloves d. Masks
 Scrub In A patient is isolated because of an undetermined respiratory condition. Which PPEs will healthcare professionals need before caring for the patient? a. Goggles b. Gowns c. Gloves d. Masks A patient
Scrub In A patient is isolated because of an undetermined respiratory condition. Which PPEs will healthcare professionals need before caring for the patient? a. Goggles b. Gowns c. Gloves d. Masks A patient
Antibiotic Use and Resistance in Nursing Homes
 Antibiotic Use and Resistance in Nursing Homes GHINWA DUMYATI, MD PROFESSOR OF MEDICINE CENTER FOR COMMUNITY HEALTH UNIVERSITY OF ROCHESTER MEDICAL CENTER FEBRUARY 8, 2017 Nicolle LE, et al. Antimicrobial
Antibiotic Use and Resistance in Nursing Homes GHINWA DUMYATI, MD PROFESSOR OF MEDICINE CENTER FOR COMMUNITY HEALTH UNIVERSITY OF ROCHESTER MEDICAL CENTER FEBRUARY 8, 2017 Nicolle LE, et al. Antimicrobial
Infection Prevention Checklist Section I: Policies and Practices I.1 Administrative Measures
 Infection Prevention Checklist Section I: Policies and Practices I.1 Administrative Measures Facility name:... Completed by:... Date:... A. Written infection prevention policies and procedures specific
Infection Prevention Checklist Section I: Policies and Practices I.1 Administrative Measures Facility name:... Completed by:... Date:... A. Written infection prevention policies and procedures specific
Background of Initiative
 Outline 2 Background of Initiative 3 Development of Recommendations 4 5 6 Development and Recommendations 7 Routine Practices Based on the premise that: All patients are potentially infectious (even if
Outline 2 Background of Initiative 3 Development of Recommendations 4 5 6 Development and Recommendations 7 Routine Practices Based on the premise that: All patients are potentially infectious (even if
Infection Prevention & Control Orientation for Housestaff Welcome to Shands at UF!
 Infection Prevention & Control Orientation for Housestaff 2011 Welcome to Shands at UF! Hot Topics: Prevention Initiatives National Patient Safety Goal 07: Prevent Healthcare Associated Infections Prevent
Infection Prevention & Control Orientation for Housestaff 2011 Welcome to Shands at UF! Hot Topics: Prevention Initiatives National Patient Safety Goal 07: Prevent Healthcare Associated Infections Prevent
A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page
 Page 1 A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page IH0200: Airborne Precautions EFFECTIVE DATE:
Page 1 A PRINTED copy of this guideline may not be the most recent version. The OFFICIAL version is located on IHNET at the Policies & Procedures Home Page IH0200: Airborne Precautions EFFECTIVE DATE:
Infection Control Manual. Table of Contents
 This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance
 Open Call Series #1 Surveillance") Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance Diane Dohm MT, IP, CIC, CPHQ MetaStar February 6, 2018 IPC Open calls: Bi-weekly Series Surveillance What data should
Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance Diane Dohm MT, IP, CIC, CPHQ MetaStar February 6, 2018 IPC Open calls: Bi-weekly Series Surveillance What data should
Policy - Infection Control, Safety and Personal Security
 Policy - Infection Control, Safety and Personal Security Origin Date: October 28, 2013 Last Evaluated: April 2018 Responsible Party: Program Director Minimum Review Frequency: Annually Approving Body:
Policy - Infection Control, Safety and Personal Security Origin Date: October 28, 2013 Last Evaluated: April 2018 Responsible Party: Program Director Minimum Review Frequency: Annually Approving Body:
NYC DOHMH Guidance Document for Development of Protocols for Management of Patients Presenting to Hospital Emergency Departments and Clinics with
 NYC DOHMH Guidance Document for Development of Protocols for Management of Patients Presenting to Hospital Emergency Departments and Clinics with Potentially Communicable Diseases of Public Health Concern
NYC DOHMH Guidance Document for Development of Protocols for Management of Patients Presenting to Hospital Emergency Departments and Clinics with Potentially Communicable Diseases of Public Health Concern
Direct cause of 5,000 deaths per year
 HOSPITAL ACQUIRED (NOSOCOMIAL) INFECTION Policies MRSA Policy Meningitis Policy Blood and body fluid Exposure Policy Disinfection Policy Glove Policy Tuberculosis Policy Isolation Policy DEFINITION: ANY
HOSPITAL ACQUIRED (NOSOCOMIAL) INFECTION Policies MRSA Policy Meningitis Policy Blood and body fluid Exposure Policy Disinfection Policy Glove Policy Tuberculosis Policy Isolation Policy DEFINITION: ANY
Clostridium difficile Infection (CDI)
") Approved by: Clostridium difficile Infection (CDI) Vice President and Chief Medical Officer Corporate Policy & Procedures Manual VI-8 Date Approved August 22, 2016 September 16, 2016 Next Review (3 years
Approved by: Clostridium difficile Infection (CDI) Vice President and Chief Medical Officer Corporate Policy & Procedures Manual VI-8 Date Approved August 22, 2016 September 16, 2016 Next Review (3 years