Diagnostics for Patient Safety and Quality of Care
|
|
|
- Ferdinand Tyler Logan
- 5 years ago
- Views:
Transcription
1 Session L17 The presenters have nothing to disclose Diagnostics for Patient Safety and Quality of Care Carol Haraden Kate Jones Pat O Connor Orlando, FL December 09, 2012
2
3 Objectives P3 Describe the current diagnostic approach of their organization Discuss the use of the data gained from diagnostic tools to prevent, detect, and mitigate harm to patients Appraise the usefulness of the presented diagnostic tools to improve the safety and quality of their organization over time
4 Agenda 4 Introduction to learning lab 1:00-1:05 Diagnostics introduction 1:05-1:10 Mortality Diagnostic1:10-1:45 GTT- 1:45-2:45 Break 2:45-3:00 Waste tool- 3:00-3:45 Using What is Learned from the Tools 3:45-4:25 Wrap up 4:25-4:30
5 5 What data do you have about how people are harmed and why they die? So what do you do with all this information?
6 Once we have information 6 Organization of information, display, prioritization and plan of action.
7 7 GTT Clinical data Mortality review Waste tool Concurrent review Risk management information
8 8 Mortality review Waste tool GTT deaths HARM Risk Management information Concurrent review What are important and recurrent issues? High volume and high impact with success.
9 How can we learn about our system performance?
10 Diagnostic Journey People die and are harmed unnecessarily every day in our hospitals. In order for us to understand this, we need a diagnostic journey that moves out of a model for judgment and into a model for learning.
11 11 Mortality Diagnostic
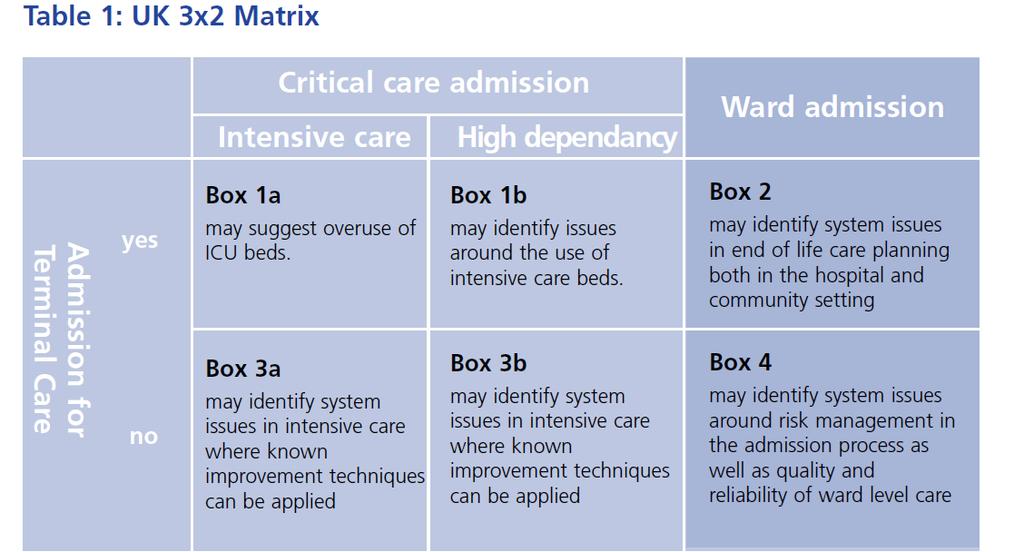
12 The Mortality Diagnostic 2x2 Matrix Review most recent 50 consecutive deaths. Place them into a two by two matrix based on: - Was the patient admitted for palliative care? - Was the patient admitted to the ICU? Focus your work initially on boxes that have at least 20% of your mortality.
13 Diagnostic The 2 x 2 Matrix Admitted to the ICU? Yes No Admitted for Palliative Care Only? Yes No Box #1 Box #2 Box #3 Box #4
14 The Mortality Diagnostic - Failure to Recognize, Plan, Communicate Analyze deaths in box 3 and 4 for evidence of failure to: recognize, communicate, plan. This will help you understand the local environment.
15 Recognize, Communicate, Plan Failure to Recognize: Any situation in which a patient has died and there was evidence that an intervention could have been made anytime prior to the patient s death Failure to Plan, such as: diagnosis, treatment, or calling a rescue team. Failure to Communicate: Patient to staff, clinician to clinician, inadequate documentation, inadequate supervisor, leadership (no quarterback for the team), etc.
16 The Mortality Diagnostic - The Impact of Care Evaluate ALL deaths in box 3 and box 4 to assess the estimated impact of our care on mortality *As you review the deaths in box 3 & 4, ask yourself the questions honestly (focusing on learning, not judgment): Was perfect care rendered? If perfect care wasn t rendered, could the outcome of death have been prevented if the care had been better?
17 The Mortality Diagnostic - Evidence of Adverse Events Analyze deaths in box 3 and 4 for evidence of adverse events using the Global Trigger Tool. This will give some further direction to local problems.
18 US 2X2 Table Aggregate 64 Hospitals ICU Admission Comfort Care 86/3175 3% (0-14%) Non Comfort Care 1161/ % (10-72%) No ICU Admission 402/ % (0-40%) 1526/ % (18-76%)
19 Unknown unknowns There are known knowns. These are things we know that we know. There are known unknowns. That is to say, there are things that we know we don't know. But there are also unknown unknowns. There are things we don't know we don't know. Donald Rumsfeld

20 Knowing what might go wrong...

21 Reduces the chance of error

22

23
24
25 Reliability First review (all deaths) 6/53 identified by 1 st Assessor 5/53 confirmed by 2 nd Assessor Second review (unexpected deaths) 9/37 identified by 1 st Assessor 9/37 confirmed by 2 nd Assessor
26 Mortality Review May cases (from Jan 2011) 14/53 excluded (death anticipated) 8/14 from Nursing Homes 37/39 death unexpected VTE prophylaxis prescription rate Time to first Consultant review Time to first dose antibiotic (if sepsis) Data collection form revised further
27 Case Study hrs 84 year old was admitted with diarrhoea and vomiting hypoglycaemic. treated with IV fluids and oral glucose. Arterial blood gases were checked and showed a partially compensated metabolic acidosis with base excess -11. No explanation was documented Blood results showed acute kidney injury grade 2. The blood gas results handwritten in the notes and a serum lactate 9.0 but no comment was made as to the significance. The drug chart confirms that no antibiotics were prescribed hours after arrival at hospital the patient suffered a fatal cardiac arrest. A discussion with the family was documented which states they were happy for a death certificate to be issued and she was not referred for a Post Mortem. The cause of death on the death certificate was pulmonary thromboembolism.
28 Case Study 1: Key points This case represents a failure to recognise severe metabolic acidosis due to lactate representing hypoperfusion most likely due to septic shock. Early aggressive fluid resuscitation and IV antibiotics are essential treatments
29 Case Study 2 An 84 year old man with previous pulmonary thromboembolism was admitted by his GP with acute breathlessness and chest pain, suspected further PTE. On arrival his observations were stable, SEWS = 0. The working diagnosis was?acs,?pte. His first ECG was performed after 2.5 hours and there were no diagnostic changes. 4 hours after arrival he was given Aspirin, Clopidogrel and Fondaparinux. At that time he was noted to appear unwell and routine observations were repeated for first time since admission SEWS now = 7. Medical staff reviewed now noted to be severely hypoxic, given stat dose Dalteparin and commenced CPAP although patient rapdily deteriorated with ventricular arrhythmias and fatal cardiac arrest.
30 Case Study 2: Key points When the GP letter suggests pulmonary embolism the diagnosis should be given strong consideration and if in doubt treated. A 4 hour delay between initial observations is too long in an emergency admission, even if the initial observations are normal. In addition a 2.5 hour delay in performing an ECG in suspected ACS is unacceptable.
31 Case Study 3 An 87 year old lady blind and lived at home, semi-independent with support from relatives developed a sore wrist and was prescribed a regular NSAID by her GP Two days later (a Public Holiday) her pain remained uncontrolled and oramorph was prescribed. The next day she was admitted to hospital with severe acute kidney injury, serum creatinine 422, potassium 6.6, and noted to be receiving Ibuprofen 400 mg tds and also on Lisinopril 5 mg daily. The AKI recovered with rehydration and stopping nephrotoxic drugs and she appeared to be making reasonable progress until she had a sudden acute deterioration on day 7 with dyspnoea and hypoxia and died within 24 hours. The presumptive diagnosis was a pulmonary embolus. Review of the drug chart showed that DVT prophylaxis had not been prescribed although there was no reason stated in the medical notes.
32 Case Study 3: Key points NSAIDs are a high risk prescription in the elderly and co-prescription with angiotensin-blocking drugs can cause severe acute kidney injury. All medical admissions are at risk of venous thromboembolism and should be prescribed DVT prophylaxis unless there is a contra-indication.
33 Local use Understand and track our own mortality rate Develop local specialty team reviews of cases of concern Recruit more Second Assessors Develop comparison indicators Address recording, coding and data quality issues Use established service meetings to share Case Studies and highlight themes.
34 Reporting Monthly reporting to from ward to Board trustees Ensure transparency of methodology Develop appropriate presentation, publication and practical dissemination of results Meet needs of different audiences in relation to interpretation, use and context ( public, Board, Chief Executive,C suite, Healthcare Professionals
35 35 Global Trigger Tool
36 Why use trigger tools Traditional reporting of errors, incidents or events does not reliably occur Voluntary methods underestimate events Trigger tool does not rely on technology Establishes baseline of adverse events for hospital
37 Global Trigger Tool Review chart for triggers that are sensitive and specific for harm Find a trigger- was there harm? Not all triggers mean there was harm!
38 Global Trigger Tool Modules Cares (General) Critical Care Medication Surgery L&D ED
39 Definition of Harm Unintended physical injury resulting from or contributed by medical care that requires additional monitoring, treatment or hospitalisation or results in death
40 Category of Harm E Temporary harm, intervention required F Temporary harm, initial or prolonged hospitalization G Permanent patient harm H Life sustaining intervention required I Contributing to Death
41 C1 C2 C3 C4 C5 C6 C7 C8 C9 C10 C11 C12 C13 C14 C15 Cares Module Triggers Transfusion or use of blood products Any Code or arrest Dialysis Positive blood culture X-Ray or Doppler studies for emboli Abrupt drop of greater than 25% in Hg or Hemtocrit Patient fall Decubiti Readmission within 30 days Restraint use Infection of any kind In hospital Stroke Transfer to higher level of care Any procedure complication Other

42 20 notes selected by medical records

43 20 minutes per case by one reviewer

44 Steps in review process LOOK FOR TRIGGERS Coding summary Discharge summary Lab results Radiology reports Procedure notes Nursing/multidisciplinary notes
45 STOP! STOP Ask yourself: Ask yourself Would I want it to happen to me? Would I want it to happen to me? An adverse event is an event that results in harm from the patient s point of view
46 Endoscopy Example of a trigger: Transfer to higher level of care Post procedure somnolent and hypotensive (BP 80) transferred to ICU Placed on Bi-Pap Received standard Demerol and Versed for procedure Given Romazicon; stayed in unit 12 hours.
47 Global Trigger Tool Examples Readmit within 30 days with recurrence of abscess right hip. Readmit next day w/ileus s/p exp lap for tumor. Stopped lasix-acute renal failure. Readmitted in 30 days for wound revision due to incisional seroma. Volume Depletion with altered mental status caused by Lasix -resulted in hospital admission. ARF due to nephrotoxicity due to combination of ACE and NSAIDS taken at home. Ischemic colitis had rt hemicolectomy. Unresponsive, coded. Decreased loc & sats on Morphine PCA. Rec'd Narcan.
48 Consecutive Adverse Events 1-Iatrogenic pneumothorax 2-Sternal wound infection 3-Thrombophlebitis 4-Post Surgical bleed 5-ICU delirium 6-Nosocomial pneumonia 7-Theophyline toxiciy/arrythmia 8-GI bleed 9-Iatrogenic pneumothorax 10-ICU delirium 11-Fluid overload 12-Oversedation 13-Urinary obstruction 14-ICU delirium 15-Rash 16-Aspiration pneumonia 17-Nausea 18-Pulmonary embolus 19-Nosocomial pneumonia 20-Sternal wound dehiscence 21-Dialysis induced hypotension 22-Severe hypotension with NTG 23-Renal failure post surgery 24-ICU delirium 25-Sternal wound infection
49 Cost Analysis Variable Favorable/(Unfav) Charge Net Revenue Direct NOI Pt. # Impact Impact Impact Cost Impact Impact entire stay $57,484 $15,525 $16,700 ($1,175) extra hospital days $3,428 $0 $1,170 ($1,170) extra ICU days $10,422 $0 $2,650 ($2,650) extra ICU days $7,930 $0 $2,500 ($2,500) Total ICU costs $1,502 $0 $865 ($865) Total Hospital Costs $21,500 $3,958 $6,430 ($2,472) extra ICU days $6,592 $0 $2,695 ($2,695) Indwelling Cath, 8 vent hours, 1 critical care day $8,768 $0 $3,245 ($3,245) extra ICU days $9,180 $0 $2,345 ($2,345) days ICU care $13,756 $0 $4,485 ($4,485) No additional cost n/a n/a n/a n/a extra ICU days $19,341 $0 $7,150 ($7,150) extra ICU days $19,032 $0 $3,730 ($3,730) 2 extra ICU days and return to OR $16,436 $0 $5,125 ($5,125) extra ICU days $15,090 $0 $4,408 ($4,408) no additional cost n/a n/a n/a n/a extra ICU days $4,086 $0 $1,619 ($1,619)

50
51 Trigger Tool Drill Down 51 When you find harm reoccurring and you want to understand it more deeply, Pull an enriched sample of patients: from the population of patients who may have a condition predisposing them to a particular harm: diabetics: hyperglycemia; patients with atrial fibrillation: anti-coagulation Using codes to find patients with particular harm like pressure ulcers and falls Other?
52 Look at the enriched sample 52 What can you learn about: - the real occurrence rate? - the clinical care processes underlying the harm - particular characteristics of the patients that suffer that harm?


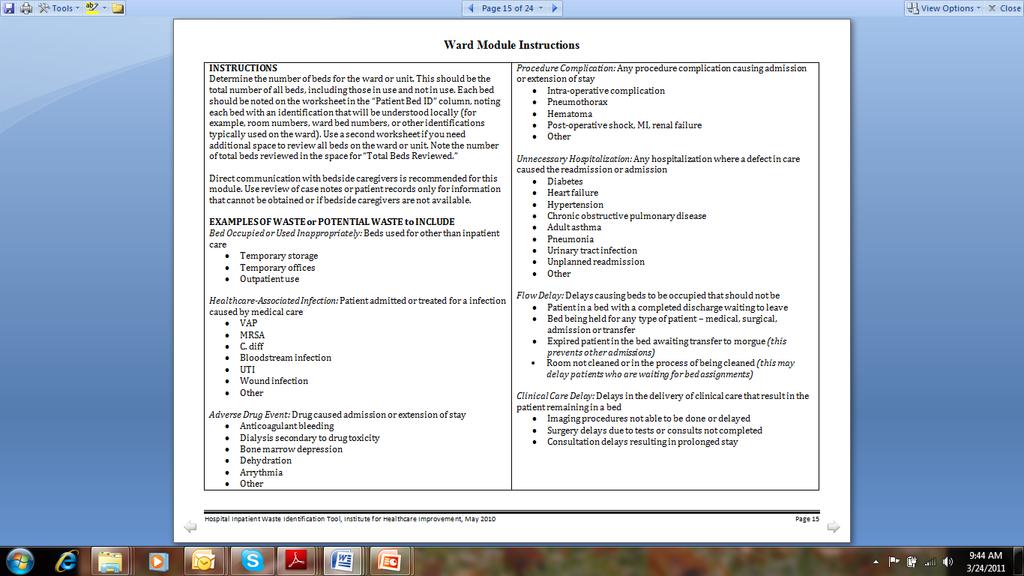
53 Waste Identification Tool
54 Design Elements Identifies waste from perspective of the shop floor Engages front line staff Use of the Tool is simple Provides an infrastructure for continuous and deliberate waste identification and reduction sensitive to the political and economic environment
55 Modules Ward waste related to bed utilization Patient Care - unnecessary patient care Diagnosis unnecessary diagnostic tests and procedures Treatment treatments given that are not supported by scientific evidence and therefore may be unnecessary (protocols, pathways, guidelines) Patient waste from the patient s perspective
56 Key Questions Ward module Hospital bed use related to flow represents a huge opportunity for wasted beds. Patient in a bed with a completed discharge waiting to go. Bed being held for a patient (medical or surgical) Bed being held for any kind of admission or transfer
57 Ward Module continues Imaging procedures not able to be done or delayed Surgery delayed due to blood tests not done Consultation not done within your institutions period of time

58
59
60 Waste Identification Tool Worksheet Ward Module Clinical Waste Unit ICU) Reviewers Date Wed, April 10 Bed ID Waste Waste Waste Streams Yes No Nosocomial Infection Adverse Drug Event Procedure Complication Unnecessary Hospitalization Flow Delay Clinical Care Delay Comments T-1 X Awaiting PICC IR T-2 X X Lap chole comp T-4 X X Futility EOL,family T-5 X X T-7 X X No Plan T-8 X X No drip on floor. Pt walking around ICU T-9 X T-10 X X No (insulin) drip on floor B-S X X No OR til Fri B-T X X X Card. Consult, no family meeting, EOL B-O X X Pt fell, No OR til Fri B-S X C-M X X End of Life (EOL) C-A X C-J X X Trach Collar trial not done V-R x X Awaiting trach & G-Tube V-A X X X Inf & EOL futility V-A X X X Pneumothorax, & EOL futility V-P X X X Graft inf. & hematoma Total # of wasted beds the numerator 16 Total # beds reviewed the denominator 19 % waste 84%
61 Operational Waste Examples Bed is empty, but no demand Bed empty for reasons such as equipment failure/bathroom not working/no hot water Patient in a private room for medical purposes and the other bed or beds are not able to be used (ex: isolation room with 2 beds in one room, but no one occupying the other bed) Room is dirty and waiting to be cleaned Patient rooms used as storerooms or offices Patients in bed for outpatient services such as administration of chemo or blood
62 I Day, 6 Units (10 mins each Unit) Medical floor Unit 1 24 patients -4 waste criteria Unit 2 21 patients -5waste criteria Unit 1 24 patients -2 waste criteria Unit 1 22 patients -5 waste criteria Unit 1 24 patients -3 waste criteria Unit 1 24 patients -2 waste criteria Opportunity for efficiencies 21! Lost hours organisational/patient waiting/delays 312Hrs
63 Patient Module Interview 54 year old male with recent hip replacement: EKG done the day of surgery when had been done in internists office two days before surgery. Sequential compression devices which kept falling off and did not ever seem to work. Physical therapy continued walking patient even after he was walking on his own without difficulty. Portion sizes for meals continued to be large even though he requested smaller portions at least three times.
64 Customizing the Waste Tool Customization for any setting as long as: Front-line approach is used. Evaluation is qualitative (responding yes or no to whether waste is present at the time of review). Waste types are clearly identified and defined.
65 Example of a Customization A large health care system customized Tool for use in its office practices. Waste types tested include: room contains non-functioning equipment room used inappropriately patient in room but MD is not in clinic patient in room dilating patient in room waiting for diagnostic testing patient in room longer because initial paperwork is incomplete
66 Using What is Learned From the Tools
67 After you use the tools Tools can be used to help us understand where we are with system level outcomes We need to then measure and improve the processes related to the harms and problems (waste) we are finding
68 A Story
69 The journey. What are our problems seen from the diagnostics? How would we prioritise these? How reliable are we? What are the issues? How do they relate to our strategic plan? How do we deploy the work in a way that we meet our most important aims?
70 The journey. What are our problems as seen from the diagnostics? How would we prioritise these? How reliable are we? What are the issues? How do they relate to our strategic plan? How do we deploy the work in a way that we meet our most important aims?
71 The journey. What are our problems seen from the diagnostics? How would we prioritise these? How reliable are we? What are the issues? How do they relate to our strategic plan? How do we deploy the work in a way that we meet our most important aims?
72 Tools 1. Pareto 2.? 3.?
73 The journey. What are our problems seen from the diagnostics? How would we prioritise these? How reliable are we? What are the issues? How do they relate to our strategic plan? How do we deploy the work in a way that we meet our most important aims?
74 What do we mean by process reliability? Chaos; failure in more than 20% of opportunities 80-90% reliability the process fails less than one in ten times 95% reliability - five in 100 times the process fails. 99% reliability - one in 100 times the process fails well designed system with low variation and co-operative relationships
75 A quick diagnosis of reliability? Less than 80% process reliability Five frontline users can not easily articulate the process 80-90% reliability less than1 in 10 times the process fails. 95% reliability - 1 in 20 times the process fails Five frontline users can easily articulate the process 99% reliability - 1 in 100 times the process fails, a well designed system with low variation and cooperative relationships
76 The journey. What are our problems seen from the diagnostics? How would we prioritise these? How reliable are we? What are the issues? How do they relate to our strategic plan? How do we deploy the work in a way that we meet our most important aims?
77 Making the links Large System Aims Meso-System Projects
78 The journey. What are our problems seen from the diagnostics? How would we prioritise these? How reliable are we? What are the issues? How do they relate to our strategic plan? How do we deploy the work in a way that we meet our most important aims?
79 The Intuitive Structure Large System Tier 1 Meso- System Meso- System Meso- System Tier 2 Project Project Project Project Project Project Project Tier 3 Project
80 Example: System Medication Safety SYSTEM Medication Safety Tier 1: Big Dot Hospitals Rehab Offices Tier 2: Portfolio Med. reconciliation Standardized dosing Self med Family Capacity Correct list Patient capability Drug availability Tier 3: Projects
81 Example: Hospital Medication Safety Hospital Medication Safety Tier 1: Big Dot Med Surg Medication process Pharm Tier 2: Portfolio Med. reconciliation IV pumps Prescribing Administration Admix Standardized dosing Tier 3: Projects Drug Availability
82 So what next? What do we think we need to improve in order to improve our outcomes? Where is the greatest opportunity? What process do we need to make more reliable?
83 Patient Observation Chart Audit Audit Guidelines: Collect a sample of observation charts for patients on the ward and answer the questions on the checklist. Sample size: Frequency: Scoring and individual chart: If all items are answered 'YES' then the chart receives a score '1'. If any item is answered 'NO' then the chart receives a score '0'. Calculating the overall audit score: Sum the individual chart scores. Convert to a percentage: Sum of chart scores Number of charts audited x 100 Chart Answer YES or NO only 1 Standard Has the chart got an addressograph or full name and hospital number? 2 Is the page numbered at the top of the chart? 3 Have doctors requested frequency of Observations? 4 Does the chart indicate the frequency of observation? 5 Is the temperature recorded correctly and as requested? 6 Is the BP recorded correctly and as requested? 7 Is the pulse recorded correctly and as requested? 8 Are respirations recorded correctly and as requested? x 9 Are O2 SATs recorded correctly and as requested? 10 Has the patient triggered in TPR or BP? 11 If yes, has the appropriate action been taken? 12 Was action taken within 1 hour? 13 Has pain assessment been documented? 14 Is urinalysis recorded? 15 Is bowel action recorded? CHART SCORE 0 1 Ward: Date: AUDIT SCORE Audit carried out by:
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
Diagnostics for Patient Safety and Quality of Care
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD Vice President Institute for Healthcare Improvement Cindy Hupke, BSN, MBA Director Institute for Healthcare Improvement Objectives
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD Vice President Institute for Healthcare Improvement Cindy Hupke, BSN, MBA Director Institute for Healthcare Improvement Objectives
Introductions. Welcome to the APAC Global Trigger Tool Session. Dr Carol Haraden IHI Gillian Robb CMDHB. Carol Haraden.
 Welcome to the APAC Global Trigger Tool Session Dr Carol Haraden IHI Gillian Robb CMDHB Carol Haraden Introductions Gillian Robb Outline for this session Introduction to the Global Trigger Tool What is
Welcome to the APAC Global Trigger Tool Session Dr Carol Haraden IHI Gillian Robb CMDHB Carol Haraden Introductions Gillian Robb Outline for this session Introduction to the Global Trigger Tool What is
Practical Tools in Patient Safety Tools Carol Haraden Amelia Brooks Jennifer Lenoci-Edwards
 Session Code These presenters have nothing to disclose Practical Tools in Patient Safety Tools Carol Haraden Amelia Brooks Jennifer Lenoci-Edwards December 5 th 8:30 4:00 #IHIFORUM Introduction 2 Morning
Session Code These presenters have nothing to disclose Practical Tools in Patient Safety Tools Carol Haraden Amelia Brooks Jennifer Lenoci-Edwards December 5 th 8:30 4:00 #IHIFORUM Introduction 2 Morning
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Measuring Medication Harm: Advantages of Using a Trigger Tool. Frank Federico Executive Director
 Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
NHS TAYSIDE MORTALITY REVIEW PROGRAMME
 NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
Sepsis The Silent Killer in the NHS
 Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
OPERATIONAL POLICY DOCUMENT FOR THE DIALYSIS UNIT WARD 20 UNIVERSITY HOSPITAL AINTREE
 OPERATIONAL POLICY DOCUMENT FOR THE DIALYSIS UNIT WARD 20 UNIVERSITY HOSPITAL AINTREE CHRISTINE JONES RENAL SPECIALIST NURSE JANUARY 2005 UNIVERSITY HOSPITAL AINTREE OPERATIONAL POLICY DIALYSIS UNIT WARD
OPERATIONAL POLICY DOCUMENT FOR THE DIALYSIS UNIT WARD 20 UNIVERSITY HOSPITAL AINTREE CHRISTINE JONES RENAL SPECIALIST NURSE JANUARY 2005 UNIVERSITY HOSPITAL AINTREE OPERATIONAL POLICY DIALYSIS UNIT WARD
Commissioning for Quality & Innovation (CQUIN)
") Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
EarlySense InSight. Integrating Acute and Community Care
 EarlySense InSight Integrating Acute and Community Care Helps Comply with CQC Standards Timely Discharge from Hospital Reduces Bed Blocking Reduces Agency Staffing Costs Provides Early Warnings of Deterioration
EarlySense InSight Integrating Acute and Community Care Helps Comply with CQC Standards Timely Discharge from Hospital Reduces Bed Blocking Reduces Agency Staffing Costs Provides Early Warnings of Deterioration
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance?
 Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Sample. A guide to development of a hospital blood transfusion Policy at the hospital level. Effective from April Hospital Transfusion Committee
 Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
Sample A guide to development of a hospital blood transfusion Policy at the hospital level Name of Policy Blood Transfusion Policy Effective from April 2009 Approved by Hospital Transfusion Committee A
National Patient Safety Goals & Quality Measures CY 2017
 National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
Innovation. Successful Outpatient Management of Kidney Stone Disease. Provider HealthEast Care System
 Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm
 Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
National Provider Call: Hospital Value-Based Purchasing
 National Provider Call: Hospital Value-Based Purchasing Fiscal Year 2015 Overview for Beneficiaries, Providers, and Stakeholders Centers for Medicare & Medicaid Services 1 March 14, 2013 Medicare Learning
National Provider Call: Hospital Value-Based Purchasing Fiscal Year 2015 Overview for Beneficiaries, Providers, and Stakeholders Centers for Medicare & Medicaid Services 1 March 14, 2013 Medicare Learning
GAMUT QI Collaborative Consensus Quality Metrics (v. 05/16/2016)
") 1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU)
") Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Quality Care Amongst Clinical Commotion: Daily Challenges in the Care Environment
 Quality Care Amongst Clinical Commotion: Daily Challenges in the Care Environment presented by Sherry Kwater, MSM,BSN,RN Chief Nursing Officer Penn State Hershey Medical Center Objectives 1. Understand
Quality Care Amongst Clinical Commotion: Daily Challenges in the Care Environment presented by Sherry Kwater, MSM,BSN,RN Chief Nursing Officer Penn State Hershey Medical Center Objectives 1. Understand
Effective Tools to Prevent and Manage Adverse Events
 Effective Tools to Prevent and Manage Adverse Events Based on Office of Inspector General Adverse Events Report Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com Objectives Upon completion
Effective Tools to Prevent and Manage Adverse Events Based on Office of Inspector General Adverse Events Report Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com Objectives Upon completion
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair
 or Atrial Septal Defect (ASD) Repair") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
National Hospital Inpatient Quality Reporting Measures Specifications Manual
 National Hospital Inpatient Quality Reporting Measures Specifications Manual Release Notes Version: 4.4a Release Notes Completed: October 21, 2014 Guidelines for Using Release Notes Release Notes 4.4a
National Hospital Inpatient Quality Reporting Measures Specifications Manual Release Notes Version: 4.4a Release Notes Completed: October 21, 2014 Guidelines for Using Release Notes Release Notes 4.4a
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Iowa Healthcare Collaborative - HEN 2.0 Measures
 Iowa Healthcare Collaborative - HEN 2.0 Measures Yellow Pink Purple Green Blue Legend Readmissions and Care Transitions Healthcare-associated Infections Hospital Acquired Conditions Safety Across the Board
Iowa Healthcare Collaborative - HEN 2.0 Measures Yellow Pink Purple Green Blue Legend Readmissions and Care Transitions Healthcare-associated Infections Hospital Acquired Conditions Safety Across the Board
Broad expectations of PRINT
 Congratulations on passing your finals! Now you ve got those out of the way, you can turn your attention to developing skills as interns rather than preparing for examinations. So, welcome to your PRINT
Congratulations on passing your finals! Now you ve got those out of the way, you can turn your attention to developing skills as interns rather than preparing for examinations. So, welcome to your PRINT
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
Additional Considerations for SQRMS 2018 Measure Recommendations
 Additional Considerations for SQRMS 2018 Measure Recommendations HCAHPS The Hospital Consumer Assessments of Healthcare Providers and Systems (HCAHPS) is a requirement of MBQIP for CAHs and therefore a
Additional Considerations for SQRMS 2018 Measure Recommendations HCAHPS The Hospital Consumer Assessments of Healthcare Providers and Systems (HCAHPS) is a requirement of MBQIP for CAHs and therefore a
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
UW MEDICINE PATIENT EDUCATION. Angiography: Kidney Exam. How to prepare and what to expect. What is angiography? DRAFT. Why do I need this exam?
 UW MEDICINE PATIENT EDUCATION Angiography: Kidney Exam How to prepare and what to expect This handout explains how to prepare and what to expect when having a kidney exam using angiography. What is angiography?
UW MEDICINE PATIENT EDUCATION Angiography: Kidney Exam How to prepare and what to expect This handout explains how to prepare and what to expect when having a kidney exam using angiography. What is angiography?
Coroner's Corner - Inquest into the death of Gwendoline Mead
 Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
General information. Hospital type : Acute Care Hospitals. Provides emergency services : Yes. electronically between visits : Yes
 General information 80 JESSE HILL, JR DRIVE SE ATLANTA, GA 30303 (404) 616 45 Overall rating : 1 out of 5 stars Learn more about the overall ratings General information Hospital type : Acute Care Hospitals
General information 80 JESSE HILL, JR DRIVE SE ATLANTA, GA 30303 (404) 616 45 Overall rating : 1 out of 5 stars Learn more about the overall ratings General information Hospital type : Acute Care Hospitals
Objectives. Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004
 Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
This is a high level overview report to update the Board on the Acute Adult Safety Programme consisting of the following sections:
 Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Adverse Events in Hospitals: How Many and Why Not Reported. Fran Griffin Senior Manager Clinical Programs, BD
 Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Kupu Taurangi Hauora o Aotearoa
 Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
PATIENT ASSESSMENT POLICY Page 1 of 7
 Page 1 of 7 Policy applies to: All staff and allied health professionals involved in patient care delivery at Mercy Hospital including Manaaki. Related Standards: Health & Disability Services (core) Standards
Page 1 of 7 Policy applies to: All staff and allied health professionals involved in patient care delivery at Mercy Hospital including Manaaki. Related Standards: Health & Disability Services (core) Standards
Basic Skills for CAH Quality Managers
 Basic Skills for CAH Quality Managers MARCH 20, 2014 THE BASICS OF DATA MANAGEMENT Data Management Systems COLLECTION AGGREGATION ASSESSMENT REPORTING 1 Some Data Management Terminology Objective data
Basic Skills for CAH Quality Managers MARCH 20, 2014 THE BASICS OF DATA MANAGEMENT Data Management Systems COLLECTION AGGREGATION ASSESSMENT REPORTING 1 Some Data Management Terminology Objective data
Principles In developing these recommendations the Consensus Panel first established the following principles for anesthesia outcomes capture:
 Outcomes of Anesthesia: Core Measures The following Core Measures are the consensus recommendations of the Anesthesia Quality Institute (AQI) and the Multicenter Perioperative Outcomes Group (MPOG). They
Outcomes of Anesthesia: Core Measures The following Core Measures are the consensus recommendations of the Anesthesia Quality Institute (AQI) and the Multicenter Perioperative Outcomes Group (MPOG). They
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
OPAT CELLULITIS PATHWAY
 OPAT CELLULITIS PATHWAY ANY exclusion criteria for OPAT Sepsis syndrome Active drug/alcohol abuse Active underlying orthopaedic condition Craniofacial cellulitis Failure to improve with > 48hrs IV Rx YES
OPAT CELLULITIS PATHWAY ANY exclusion criteria for OPAT Sepsis syndrome Active drug/alcohol abuse Active underlying orthopaedic condition Craniofacial cellulitis Failure to improve with > 48hrs IV Rx YES
SCORING METHODOLOGY APRIL 2014
 SCORING METHODOLOGY APRIL 2014 HOSPITAL SAFETY SCORE Contents What is the Hospital Safety Score?... 4 Who is The Leapfrog Group?... 4 Eligible and Excluded Hospitals... 4 Scoring Methodology... 5 Measures...
SCORING METHODOLOGY APRIL 2014 HOSPITAL SAFETY SCORE Contents What is the Hospital Safety Score?... 4 Who is The Leapfrog Group?... 4 Eligible and Excluded Hospitals... 4 Scoring Methodology... 5 Measures...
2 Midnight Case Examples and Documentation Tips. Ralph Wuebker, MD Executive Health Resources, Inc. All rights reserved.
 2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
In a common ICU situation like this, there are two main questions we have to answer daily:
 MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
The School Of Nursing And Midwifery. CLINICAL SKILLS PASSPORT
 The School Of Nursing And Midwifery. BMedSci Nursing (Adult) CLINICAL SKILLS PASSPORT Student Details NAME: COHORT: I understand that this booklet may be reviewed by my mentor, the programme leader, my
The School Of Nursing And Midwifery. BMedSci Nursing (Adult) CLINICAL SKILLS PASSPORT Student Details NAME: COHORT: I understand that this booklet may be reviewed by my mentor, the programme leader, my
Consumers Union/Safe Patient Project Page 1 of 7
 Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
NHS HIGHLAND. Significant Event Report
 ` NHS HIGHLAND Significant Event Report Report to - Quality & Patient Safety Raigmore Management Team of Findings from Significant Event Review Meeting QPS040 26/10/2011 1.0 Outline of Significant Event
` NHS HIGHLAND Significant Event Report Report to - Quality & Patient Safety Raigmore Management Team of Findings from Significant Event Review Meeting QPS040 26/10/2011 1.0 Outline of Significant Event
1. Recommended Nurse Sensitive Outcome: Adult inpatients who reported how often their pain was controlled.
 Testimony of Judith Shindul-Rothschild, Ph.D., RNPC Associate Professor William F. Connell School of Nursing, Boston College ICU Nurse Staffing Regulations October 29, 2014 Good morning members of the
Testimony of Judith Shindul-Rothschild, Ph.D., RNPC Associate Professor William F. Connell School of Nursing, Boston College ICU Nurse Staffing Regulations October 29, 2014 Good morning members of the
Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model
 Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model June 2017 Requested by: House Report 114-139, page 280, which accompanies H.R. 2685, the Department of Defense
Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model June 2017 Requested by: House Report 114-139, page 280, which accompanies H.R. 2685, the Department of Defense
Hospital Inpatient Quality Reporting (IQR) Program Measures (Calendar Year 2012 Discharges - Revised)
 Program Measures (Calendar Year 2012 Discharges - Revised)") The purpose of this document is to provide a reference guide on submission and Hospital details for Quality Improvement Organizations (QIOs) and hospitals for the Hospital Inpatient Quality Reporting (IQR)
The purpose of this document is to provide a reference guide on submission and Hospital details for Quality Improvement Organizations (QIOs) and hospitals for the Hospital Inpatient Quality Reporting (IQR)
PQRS Success in 2015:
 PQRS Success in 2015: The Effects of Applicability Validation (MAV) on s Selection for Hospitalists Why is Applicability Validation (MAV) important? CMS requires all eligible professionals (EPs) successfully
PQRS Success in 2015: The Effects of Applicability Validation (MAV) on s Selection for Hospitalists Why is Applicability Validation (MAV) important? CMS requires all eligible professionals (EPs) successfully
Value-based incentive payment percentage 3
 Report Run Date: 07/12/2013 Hospital Value-Based Purchasing Value-Based Percentage Payment Summary Report Page 1 of 5 Percentage Summary Report Data as of 1 : 07/08/2013 Total Score Facility State National
Report Run Date: 07/12/2013 Hospital Value-Based Purchasing Value-Based Percentage Payment Summary Report Page 1 of 5 Percentage Summary Report Data as of 1 : 07/08/2013 Total Score Facility State National
Are you at risk of blood clots?
 Are you at risk of blood clots? DVT (deep vein thrombosis) & PE (pulmonary embolism) Information for patients in hospital or going home from hospital Are you at risk of blood clots? (DVT & PE) This leaflet
Are you at risk of blood clots? DVT (deep vein thrombosis) & PE (pulmonary embolism) Information for patients in hospital or going home from hospital Are you at risk of blood clots? (DVT & PE) This leaflet
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
SCIP. Surgical Care Improvement Project. Making Surgeries Safer. By: Roshini Mathew, RN
 SCIP Surgical Care Improvement Project Making Surgeries Safer By: Roshini Mathew, RN Importance Hospitals could prevent 13,000 patient deaths and 271,000 surgical complications each year 4 measures are
SCIP Surgical Care Improvement Project Making Surgeries Safer By: Roshini Mathew, RN Importance Hospitals could prevent 13,000 patient deaths and 271,000 surgical complications each year 4 measures are
CARE OF THE PATIENT REQUIRING CONTINUOUS FLOLAN INFUSION GUIDELINE
 Page Number: 1 of 5 TITLE: CARE OF THE PATIENT REQUIRING CONTINUOUS FLOLAN INFUSION GUIDELINE PURPOSE: To provide guidelines for the nursing care of the patient with a Flolan infusion delivered thru continuous
Page Number: 1 of 5 TITLE: CARE OF THE PATIENT REQUIRING CONTINUOUS FLOLAN INFUSION GUIDELINE PURPOSE: To provide guidelines for the nursing care of the patient with a Flolan infusion delivered thru continuous
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.
 Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.") Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
Medicare Value Based Purchasing August 14, 2012
 Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
CME Disclosure. HCAHPS- Hardwiring Your Hospital for Pay-for-Performance Success. Accreditation Statement. Designation of Credit.
 CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
1. CRITICAL CARE. Preamble. Adult and Pediatric Critical Care
 1. CRITICAL CARE Complete understanding of the following paragraphs is essential to appropriate billing of the critical care fees. Members of the team billing the Critical Care Payment Schedule can not
1. CRITICAL CARE Complete understanding of the following paragraphs is essential to appropriate billing of the critical care fees. Members of the team billing the Critical Care Payment Schedule can not
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
QUALITY REPORT. Part A Patient Experience
 QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
KEY TO INITIALS OF ALL STAFF COMPLETING THIS ICP Print name Designation Initials Signature date
 Forename Surname Unit number Address (including Postcode) NHS Lothian Arrived in.unit for procedure Date: & time: GP Address Religion Ethnic Origin Tel. number Next of Kin: /address Tel. number(s):home
Forename Surname Unit number Address (including Postcode) NHS Lothian Arrived in.unit for procedure Date: & time: GP Address Religion Ethnic Origin Tel. number Next of Kin: /address Tel. number(s):home
@ncepod #tracheostomy
 @ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
@ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
Working together to improve health care quality, outcomes, and affordability in Washington State. Coronary Artery Bypass Graft Surgical Bundle
 Working together to improve health care quality, outcomes, and affordability in Washington State. Coronary Artery Bypass Graft Surgical Bundle TBD 2015 The intent of the Coronary Artery Bypass Graft Surgical
Working together to improve health care quality, outcomes, and affordability in Washington State. Coronary Artery Bypass Graft Surgical Bundle TBD 2015 The intent of the Coronary Artery Bypass Graft Surgical
How to conduct second line assessments. Barry Beiles-Clinical Director VASM
 How to conduct second line assessments Barry Beiles-Clinical Director VASM ASM receives notification of death Surgical case form sent to surgeon for completion by paper or Fellows Interface Completed paper
How to conduct second line assessments Barry Beiles-Clinical Director VASM ASM receives notification of death Surgical case form sent to surgeon for completion by paper or Fellows Interface Completed paper
Auckland District Health Board Summary 1 July 2011 to 30 June 2012 Serious and Sentinel Events
 DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
DHB SSE Report 0 Auckland District Health Board Summary July 0 to 30 June 0 Serious and Sentinel Events There were 60 serious and sentinel events reported by ADHB in the July 0 to June 0 year. Events identified
THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING. Australasian Rehabilitation Nurses Association June 26 th 2015
 THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING Australasian Rehabilitation Nurses Association June 26 th 2015 Conflict of Interest and affiliations No conflicts of interest regarding this topic. Current
THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING Australasian Rehabilitation Nurses Association June 26 th 2015 Conflict of Interest and affiliations No conflicts of interest regarding this topic. Current
Laparoscopic partial nephrectomy
 Laparoscopic partial nephrectomy This leaflet is written to give you information and answer questions you may have about your surgery. If you have any further questions, please speak to your doctor or
Laparoscopic partial nephrectomy This leaflet is written to give you information and answer questions you may have about your surgery. If you have any further questions, please speak to your doctor or
Patient information. Breast Reconstruction TRAM Breast Services Directorate PIF 102 V5
 Patient information Breast Reconstruction TRAM Breast Services Directorate PIF 102 V5 Your consultant has recommended that you have a TRAM flap to reconstruct your breast. TRAM stands for Transverse Rectus
Patient information Breast Reconstruction TRAM Breast Services Directorate PIF 102 V5 Your consultant has recommended that you have a TRAM flap to reconstruct your breast. TRAM stands for Transverse Rectus
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16
 Schemes for 2015/16") Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule
 HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
Quality Provisions in the EPM Final Rule. Matt Baker Scott Wetzel
 Quality Provisions in the EPM Final Rule Matt Baker Scott Wetzel Overview Quality Scoring Overview Quality Metrics in AMI and CABG EPMs Quality Metrics in SHFFT EPMs COTH Performance in these programs
Quality Provisions in the EPM Final Rule Matt Baker Scott Wetzel Overview Quality Scoring Overview Quality Metrics in AMI and CABG EPMs Quality Metrics in SHFFT EPMs COTH Performance in these programs
Why try to reduce hospitalizations? How many are avoidable?
 Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry
 TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry DEPARTMENT: PERSONNEL: Telemetry Telemetry Personnel EFFECTIVE DATE: 6/86 REVISED: 02/00, 4/10, 12/14 Admission Procedure: 1. The admitting
TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry DEPARTMENT: PERSONNEL: Telemetry Telemetry Personnel EFFECTIVE DATE: 6/86 REVISED: 02/00, 4/10, 12/14 Admission Procedure: 1. The admitting
April Clinical Governance Corporate Report Narrative
 April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
Quality Improvement in the ICU: A Way Forward
 Quality Improvement in the ICU: A Way Forward Ognjen Gajic M.D. Mayo Clinic Rochester MN, USA Multidisciplinary Epidemiology and Translational Research in Intensive Care, Emergency and Perioperative Medicine
Quality Improvement in the ICU: A Way Forward Ognjen Gajic M.D. Mayo Clinic Rochester MN, USA Multidisciplinary Epidemiology and Translational Research in Intensive Care, Emergency and Perioperative Medicine
LAPAROSCOPIC SIMPLE REMOVAL OF THE KIDNEY
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
The Primary Care Trigger Tool: Practical Guidance
 The Primary Care Trigger Tool: Practical Guidance Reviewing clinical records to detect and reduce patient safety incidents Index Content Page Introduction 2 What is a Trigger Tool Review? 2 What types
The Primary Care Trigger Tool: Practical Guidance Reviewing clinical records to detect and reduce patient safety incidents Index Content Page Introduction 2 What is a Trigger Tool Review? 2 What types
UPMC ST. MARGARET CONTINUING EDUCATION PROGRAMS (Classroom and/or Electronic) PROFESSIONAL STANDARDS OF PRACTICE AND PERFORMANCE
 PROFESSIONAL STANDARDS OF PRACTICE AND PERFORMANCE") TOTAL 2010-2013 3761 First Three Minutes 07/09/2010 3 NIHSS - Stroke Scale 08/05/2010 2 CLABS Review 08/05/2010 08/24/2010 08/30/2010 09/07/2010 64 SMH Journal Club: "Conscious Sedation" 09/01/2010 19
TOTAL 2010-2013 3761 First Three Minutes 07/09/2010 3 NIHSS - Stroke Scale 08/05/2010 2 CLABS Review 08/05/2010 08/24/2010 08/30/2010 09/07/2010 64 SMH Journal Club: "Conscious Sedation" 09/01/2010 19