Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education Consulting
|
|
|
- Helen Richards
- 5 years ago
- Views:
Transcription


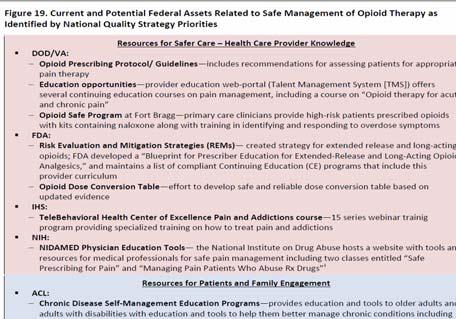
1 The Bloody Truth About IV Medication and Blood Transfusion Compliance Thursday, August 7 th, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education Consulting Board Member Emergency Medicine Patient Safety Foundation sdill1@columbus.rr.com Phone Questions Welcomed, No Questions 2 Learning Objectives 1. Discuss the CMS-issued memo on infection control breaches that will have to be reported to the state agency. 2. Review CMS requirements for ensuring nurses are competent when giving IV medications or blood transfusions. 3. Explain CMS policies and requirements on blood transfusions including staff training expectations. 4. Explain new and revised standards, regulations, and laws put forth by CMS, TJC and the federal government. 5. Evaluate compliance requirements and penalties. 3 1
2 The Conditions of Participation (CoPs) Regulations first published in 1986 and many changes since Manual updated June 6, 2014 and 471 pages New section on IV and blood transfusions is effective on this date and also published in March 14, 2014 advanced memo First regulations are published in the Federal Register then CMS publishes the Interpretive Guidelines and some have survey procedures 2 Hospitals should check this website once a month for changes Location of CMS Hospital CoP Manuals CMS Hospital CoP Manuals new address 5 CMS Hospital CoP Manual nloads/som107_appendixtoc.pdf 6 2


3 CMS Survey and Certification Website ationgeninfo/pmsr/list.asp# TopOfPage 7 8 IV Medication and Blood CMS issues an advanced 32 page memo on March 14, 2014 CMS updates manual and makes it final on June 6, 2014 and issues final transmittal Addresses medication administration, safe opioid use, IV medications and blood transfusion Must have a P&P Must train staff Must document process Questions to hospitalscg@cms.hhs.gov 9 3


4 CMS Memo Med & Safe Opioid Use 10 Final Transmittal Issued June 6, ations-and- Guidance/Guidance/ Transmittals/Downlo ads/r116soma.pdf 11 IV Medication & Transfusions CMS has pharmacy standards that impact nursing practice Pharmacy section at tag CMS wanted to make it clear that medication administration under nursing are only some of the ones that impact the overall medication process CMS states that the pharmacy standards and QAPI CoPs also impact medication administration, IV, blood administration and that nursing should be aware of this 12 4
5 IV Medication & Transfusions This memo updates the CMS guidance for IV medications and blood transfusions CMS also said the purpose of the memo was to reflect the need for patient risk assessment and appropriate monitoring during and after medication administration Particularly for post-operative patients receiving IV opioid medications, in order to prevent adverse events So this is all about medication administration, safe opioid use, IV medications and transfusion CMS discusses the HHS National Action Plan for 13 ADR Prevention National Action Plan for ADR Prevention ADEs are an estimated one-third of all hospital adverse events ADEs account for over 3.5 million physician office visits and one million ED visits and 125,000 hospitalizations Looks at 3 common high alert and priority ADRs: anticoagulants, diabetes agents, and opioids Hospitals can expect an increase focus in the future of these 3 areas by CMS Draft plan and final one expected summer


6 Opioids Section

7 CDC Website on Rx Overdoses 19 National Action Plan for ADR Prevention Hospital ADEs prolong the length of stay from 1.7 to 4.6 days HHS selected anticoagulants, diabetic medication, and opioid finding they are the most common medication errors CMS and HHS said also clinically significant, preventable, measureable, and there fore highpriority targets of the Action Plan Hospitals should review this action plan and consider these areas in their efforts to reduce medication errors and ADEs 20 IV Medication & Transfusions CMS states the medication process is a shared responsibility of the hospital nursing staff This includes using a comprehensive system and compliance with the pharmacy standards and patient safety requirements under the QAPI section The QAPI section was rewritten March 21, 2014 Remember the CMS QAPI worksheet Patient risk assessment and appropriate monitoring of patient response to medications, especially opioids, can reduce medication errors 21 7

8 Medication Safety & IV Opioids CMS said updating their requirements to in order to better align with current acceptable standards of practice Every year there are many fatalities with the use of IV opioid medications in hospitals Opioid-induced respiratory depression deaths might be prevented with appropriate risk assessment and frequent monitoring of respiratory rate, oxygen, and sedation level Also PCA is a form of self administration Added additional guidance or blue box advisories 22 CMS QAPI Work Sheet ADE & Medical Errors Enrollment-and- Certification/SurveyCertificationGenInf o/policy-and-memos-to-states-and- Regions.html 23 QAPI Questions Surveyor Will Ask Is there evidence of training or communication to convey expectations for patient safety related to reporting medication errors including near misses? Is there evidence that the hospital has adopted policies supporting a non-punitive approach to staff reporting of medical errors (including near misses/close calls), adverse events, and situations they consider unsafe? On every unit can staff describe what is meant by medical errors including medication errors, near misses and adverse events? 24 8
9 QAPI Questions Surveyor Will Ask Does the QAPI program identify and track medication administration errors, adverse drug reactions, and drug related incompatibilities? Is there a QAPI program process for staff to report blood transfusion reactions, and reviews of reported blood transfusion reactions to identify medical errors (including near misses/close calls) and/or adverse events? Can the hospital provide evidence that medical errors, near misses, and adverse events are identified in staff reports or incident reports? 25 Follow National Standards of Care Standard: Medications must be prepared and administered with acceptable national standards of practice and mentions five organizations (405) National Coordinating Council for Medication Error Reporting and Prevention Institute for Healthcare Improvement U.S Pharmacopeia Institute for Safe Medication Practices Infusion Nurses Society CDC at Also according to the TJC MM chapter, manufacturer s directions and hospital policy 26 Timing of Medication Administration Tag 405 What are acceptable standards of care? National organizations that are recognized in the field issue written statements and policies that direct patient care The hospital s P&Ps must be consistent with SOC Standards of care can be set by state pharmacy boards and national organizations like the ones mentioned by CMS Others include: ASHP (American Society of Healthcare System Pharmacist), American Nurses Association (ANA), American Pharmacy Association (APA), APIC, etc. 27 9



10 ISMP Institute for Safe Medication Practices 28 Infusion Nurses Society INS 29 Free Publication Business Case IV Teams _The_Business_Case_Paper.pdf 30 10



11 National Coordinating Council Institute for Healthcare Improvement IHI


12 USP U.S. Pharmacopeial 34 Centers for Disease Control & Prevention CDC 35 CDC IV Guidelines Every hospital should have the 2011 CDC Guidelines for the Prevention of Intravascular Catheter Related Infections How to prep the skin for the peripheral IV How to secure the needle How long to change the dressing How long do you change the IV tubing? 36 12

13 ines/bsi-guidelines-2011.pdf Blood Transfusions and IVs & 2014 Standard: Blood transfusions and IV medications must be administered with state law and MS P&P This section has been changed four times over the past several years CMS previously issued a memo on May 13, 2011 Amended June 7, 2013 under new regulations issued July 12, 2012 Updated in manual issued June 6, 2014 Use to require special training for this and there was a long list of things that nurses had to be trained on 39 13

14 40 Blood Transfusions and IVs 409 CMS eliminated the regulations mandating training for non-physicians who administer IV medication and blood and blood products CMS says because this training is already standard practice However, when the June 2013 interpretive guidelines were issued CMS said you must still be competent in those areas So basically hospitals will want to train in these areas Must follow your P&P and state scope of practice 41 Blood and IV Medication Training Must still follow state law requirements In some states an LPN can not hang blood Or the LPN can not push certain IV medications in some states Must show they are competent Must still have approved Medical Staff Policies and Procedures in place Staff must follow these which have most of the things that were previously required 42 14
15 Blood and IV Medication Training CMS mentions that many of the medications given IV are included in the high risk or high alert medication category High alerts are those that if a mistake happens the patient is more likely to be injured or die CMS references several other areas in the CoP on high alert medications Including that patients need be monitored when receiving high alert medications like opioids which is discussed later TJC has section on high alert medication in MM High Risk Medications Need P&P on high alert medications such as dosing limits, administration guidelines, packaging, labeling and storage to reduce medication errors (490) Could be pediatric, geriatric or patients with renal or hepatic impairment Need to have a system to minimize adverse drug events There are several lists of high alert medications and may want to make sure list is posted in medication rooms even though hospital does not select all of them in their policy 44 High Risk Medications High risk medications may include (continued): Such as checklists, dose limits, pre-printed orders, special packaging, special labeling, double-checks and written guidelines Examples of high-risk drugs may include investigational drugs, controlled medications, medications not on the approved FDA list, medications with a narrow therapeutic range, psychotherapeutic medications and lookalike/sound-alike medications and those new to the market or new to the hospital 45 15
16 Policy on High Alert Medications Have a policy on high alert meds, Common ones include Digoxin IV, Heparin, adrenergic agonists, concentrated electrolytes and chemo have highest risk of injury (ISMP) Insulin, Warfarin, Opiates and Narcotics, injectible KCL, Heparin, Fentanyl patches, and NaCl over 0.9% were most commonly ones involved in error CMS amends CoPs and is focusing on safe use of opioids as a high risk medication 46 Policy on High Alert Medications If insulin have vials in different bins or sections of box Use tall man lettering such as NovaLog and NovaLIN High alert may include; Epidural infusions, Fentanyl, Heparin over 1000 units, insulin, Lidocaine with Epi vials, neuromuscular blockers, PCA, TPN, moderate sedation, anesthetic agents (propofol), and adrenergic agonists (phenylephrine)


17 High Alert How to Guide IHI Blood Transfusions and IVs 2014 Hospital P&P for blood and IV medication must be based on state law and MS P&P and must address the following: (all new section) Vascular access route such as central line, peripheral or implanted port and what medications can be given IV and via what type of access devices Basic safety practices for medication administration Tracing line and tubes prior to administration to be sure proper route Verify proper programming of infusion devices 51 17

18 Why Trace the Lines? CMS issues survey memo March 8, 2013 regarding why they want nurses to trace the lines when getting out of report or before injecting medication into an IV line This has been a patient safety issues for many years Staff can connect two things together that do not belong together because the ends match It has been the subject of many reports including a sentinel event alert from TJC 52 Luer Misconnections Memo A study found the Pa Patient Safety Authority found that it occurred once a month in their state and if you extrapolate that to the nation it could be 50 a month For example, a patient had the blood pressure cuff connected to the IV and died of an air embolism Nurse accidentally hangs a medication in the epidural line instead of the IV resulting in the patient s death Luer connections easily link many medical components, accessories and delivery devices 53 Luer Misconnections Memo 54 18



19 PA Patient Safety Authority Article 55 June 2010 Pa Patient Safety Authority 56 ISMP Tubing Misconnections


20 FDA July 9, 2010 Enteral Feeding 58 TJC Sentinel Event Alert #36 www,jointcommission.org l_event_alert_issue_36_tubing_misco nnections a_persistent_and_potentially_deadly_ occurrence/ 59 New Standards Prevent Tubing Misconnections New and unique international standards being developed in 2014 for connectors for gas and liquid delivery systems To make it impossible to connect unrelated systems Includes new connectors for enteral, respiratory, limb cuff inflation neuraxial, and intravascular systems Phase in period for product development, market release and implementation guided by the FDA and national organizations and state legislatures FAQ on small bore connector initiative 60 20


21 Blood Transfusions and IVs 2014 Patient Monitoring Nursing staff must understand each medication and its monitoring requirement Monitor for the effects of the medication since IV medications have a more rapid effect Monitoring to include assessment of risk factors that would influence type and frequency of monitoring Such as patient with renal failure on Vancomycin and dose is based on lab test 63 21

22 Blood Transfusions and IVs 2014 P&P expected to address Monitoring for fluid and electrolyte balance Monitor patients on high alert meds including opioids and evaluate for over-sedation and respiratory depression Tag 405 discusses the assessment and monitoring of patients on opioids Needs to address assessment of patients with risk factors that would influence the type and frequency of monitoring 64 Get Fluid & Electrolyte Balance Updates 65 Assessment & Monitoring of Patients 2014 Patients on medications needed to be carefully monitored (Tag 405) May need clinical and lab data to evaluate medication Monitor respiratory status, pulse ox BP, end tidal CO2 with patients on opioids Evaluate clinical signs such as confusion, agitation, unsteady gait, itching etc. Know high risk medications policy and safe practices Know risk factors for ADE such as patient has liver or kidney failure, history of sleep apnea, obesity, smoking, drug-drug interaction and first time medication use 66 22


23 Assessment & Monitoring of Patients ADE, such as anaphylaxis or opioid-induced respiratory depression may require timely and appropriate (405) Post-medication monitoring in case of a high alert medication may include regular assessment of VS, pulse ox, and sedation levels of post surgery patient on PCA Such as Richmond agitation sedation scale (RASS) or the Pasero Opioid-Induced sedation scale (POSS), Inova Sedation Scale (ISS), Ramsey scale, Aldrete Scoring system 67 Pasero Opioid induced Sedation Scale POSS asero-opioid-induced-sedation-scaleposs.pdf 68 Richmond Agitation Sedation Scale RASS

24 Comparison of Sedation Scales Medscape ewarticle/708387_3 70 Blood Transfusions and IVs 2014 Risk factors for patients receiving opioids include Snoring or history of sleep apnea No recent opioid use or first-time use of IV opioids Increased opioid dose requirement or opioid habituation Longer length of time receiving general anesthesia during surgery Receiving other sedating drugs, such as benzodiazepines, antihistamines, sedatives, or other CNS depressants Preexisting pulmonary or cardiac disease Thoracic or other surgical incisions that may impair breathing 71 Blood Transfusions and IVs Hospital P&P is expected to address: Monitoring for fluid and electrolyte balance Policy must address monitoring and treatment for fluid and electrolyte imbalances that may occur with blood transfusions and IV medications Monitoring patients for high alert medications including IV opioids Policy must include the list the hospital selected as their high risk medications Must include how to monitor for them such as 2 nurses check insulin or use bar coding and how often monitoring of patient on IV insulin and how often glucose checks 72 24

25 Insulin Drip Monitoring Protocol 73 Blood Transfusions and IVs Expected to address monitoring for oversedation and respiratory depression for safe opioid use Can erroneous assume patient is asleep when they are having progressive symptoms of respiratory compromise Factors that put patients at high risk include snoring, history of sleep apnea, first time use of IV opioids, increased opioid dose, longer length of time receiving general anesthesia, pulmonary or cardiac disease or thoracic or surgical incisions 74 Assess and Monitor Patients 2014 Need to assess and monitor the effects of the medications To allow for early identification of adverse effects Some may need to use clinical and lab data to evaluate efficacy of medication therapy For opioids may need to monitor respiratory status, Vitals signs such BP, O2 sat, pain level, sedation scale, and carbon dioxide levels Evaluate symptoms such as confusion, agitation, unsteady gait, pruritus, somnolence etc. Be aware of high alert medications as discussed 75 25
, pain")

26 Blood Transfusions and IVs P&P must include who can conduct the assessments The frequency and duration of the assessments Under what circumstances practitioners prescribing IV opioids are allowed to establish protocols that differ from hospital P&P Assessment includes VS (TPR and BP), pain level, respiratory status, sedation level and ETCO2 Also mentions APSF(Anesthesia Patient Safety Foundation) monitoring of opioids including ETCO2 76 APSF Website Mentioned by CMS 77 Whitepaper and Workshop Dangers Opioids



27 79 ISMP Use a Standard Sedation Scale
28 Safe Opioid Use & Safe Medication Use Patients at great risk for adverse events include age, liver or kidney failure, history of sleep apnea, history of smoking, drug-drug interaction, first time medication use and weight Obesity could increase apnea and smaller patients could more sensitive to dose levels of medications Risk factors need to be considered in determining how often to monitor and what type of monitoring Must communicate important information in hand-offs such as change of shift 82 Safe Opioid Use & Safe Medication Use ADR, such as opioid-induced respiratory depression require timely intervention as per established hospital protocols Must also report to physician or LIP immediately High alert medications would want to check VS, O2 sat, (ETCO2), and sedation levels to prevent respiratory depression and arrest Staff are expected to include patient s reports of his experience of the medication s effects Educate the patient and family about notifying staff if difficulty breathing 83 Safe Opioid Use & Safe Medication Use Hospital policy is expected to address the manner and frequency of monitoring Hospital P&P is expected to include information to be communicated at shift change It is important to document order, medication record, lab reports, vital signs etc. Document after actual administration of medication and no documentation in advance Surveyor will make sure staff is knowledgeable about intervention protocol if ADE occurs 84 28



29 Anesthesia Patient Safety Foundation ASA Standards and Guidelines

30 Blood Transfusions 2014 HHS says there were 13,785,000 units of whole blood and red blood cells were transfused in the US in 2011 Collection, testing, preparation, and storage of blood and blood components are regulated by the FDA However, CMS standards govern administration of blood and blood products Transfusion errors can be fatal Has a number of things that must be in P&Ps 88 Blood Transfusions 2014 Confirm correct patient Verify correct blood product Standard calls for two qualified persons, one who is administering the transfusion TJC NPSG allows one person hanging blood if use bar coding Document monitoring P&P include how frequent you monitor the patient and do vital signs How to identify and treat and report any adverse transfusion reaction
31 Blood Transfusions 2014 Staff must be competent in venipuncture Competent in using vascular access devices Trained in early detection and intervention for opioid over-sedation Must document competency So make sure nursing education is aware and staff trained in orientation periodically Make sure staff educated on P&P 91 Survey Procedure 2014 Interview nursing staff on different units who administer IV medications and blood transfusions. Are staff knowledgeable with respect to: Venipuncture techniques Safe medication administration practices, including general practices applying to all types of medications and practices concerning IV tubing and infusion pumps Maintaining fluid and electrolyte balance Patient assessment for risk related to IV medications and appropriate monitoring Early detection and intervention 92 Survey Procedure 2014 Will look to see if any blood transfusions To review staff files for evidence of competency in administering IV medication and blood products Surveyor encouraged to watch staff hang blood or observe IV medication given Were safe injection practices followed Was appropriate access for IV medication Are patients monitored for adverse reactions Were transfused patients correctly identified and correct blood administered? 93 31

32 Incident Reports A Standard: There must be procedure for reporting transfusion reactions, adverse drug reactions (ADRs) and errors in administration of drugs This was effective December 12, 2013 See tag 508 which was amended in the pharmacy section which affects nursing Important for staff to be versed in the blood and blood products policy and the symptoms of a transfusion reaction Transfusion Reactions, ADEs, Drug Errors Establish a procedure in the case of ADEs and drug errors when nurses administer drugs or transfusions Refers back to tag 508 regarding reporting these into the PI system Often done on an incident report and document in chart and document physician or LIP notified Transfusion reactions can be serious and life threatening Discussed the symptoms of a transfusion reaction: chills, hives, back pain, bloody urine, dizziness, fever, flank pain, skin flushing, kidney failure, anemia, shock, respiratory failure or death 96 32
33 Transfusion Reactions Transfusion reactions can occur during or after a blood transfusion Patient s immune system recognized the foreign blood product and attempts to destroy the infused cells Incompatible blood products are typically the cause of the transfusion reaction Symptoms may include back pain, bloody urine, hives, chills, fainting, dizziness, fever, flank pain, and skin flushing. More serious complications may include acute kidney failure, anemia, respiratory distress, shock and even death. 97 Transfusion Reactions Must have P&P to ensure transfusion reactions are reported Must be reported immediately to practitioner Must be documented in the chart Must be reported to the QAPI program Surveyor is suppose to look at the hospital P&P and internal reports of transfusion reactions Will ask to see any incident reports 98 Survey procedure Request policy for reporting of transfusion reactions They may review the incident reports or other documentation through QAPI program Surveyor is told to interview the nursing staff responsible for administering blood to be sure they are familiar with and complying with the policies Surveyor instructed to ask for transfusion related incident reports and determine if reported to the PI program and to the practitioner responsible for the patient s care 99 33



34 So What s in Your Policy? 100 So What s In Your Policy?

35 103 es/bt/bt_summary.html


36 106 AABB Transfusion Medicine od%20cell%20transfusion%3a%20a%20clinical%20pr actice%20guideline%20from%20the%20aabb&fd_jou rnalid=90&searchsourcetype=
.")
37 109 This presentation is intended solely to provide general information and does not constitute legal advice. Attendance at the presentation or later review of these printed materials does not create an attorney-client relationship with the presenter(s). You should not take any action based upon any information in this presentation without first consulting legal counsel familiar with your particular circumstances. 110 The End Questions???? Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President Patient Safety and Healthcare Education 5447 Fawnbrook Lane Dublin, Ohio (no question, call)
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) Medication Administration, Safe Opioid Use, IV and Blood Administration
 Medication Administration, Safe Opioid Use, IV and Blood Administration") CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2017 Medication Administration, Safe Opioid Use, IV and Blood Administration Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2017 Medication Administration, Safe Opioid Use, IV and Blood Administration Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) Medication Administration, Safe Opioid Use, IV and Blood Administration
 Medication Administration, Safe Opioid Use, IV and Blood Administration") CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2018 Medication Administration, Safe Opioid Use, IV and Blood Administration Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2018 Medication Administration, Safe Opioid Use, IV and Blood Administration Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President
CMS Hospital Discharge Planning Standards 101. Friday, March 21st, 2014
 CMS Hospital Discharge Planning Standards 101 Friday, March 21st, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education Consulting Board Member
CMS Hospital Discharge Planning Standards 101 Friday, March 21st, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education Consulting Board Member
CMS Requirements on Order Sets, Protocols, Preprinted and Standing Orders. Friday, December 5 th, 2014
 CMS Requirements on Order Sets, Protocols, Preprinted and Standing Orders Friday, December 5 th, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and
CMS Requirements on Order Sets, Protocols, Preprinted and Standing Orders Friday, December 5 th, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and
Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use
 Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use Our vision is to create a culture where patients and those who care for them are
Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use Our vision is to create a culture where patients and those who care for them are
Clarifying the Confusing CMS Hospital Surgery, PACU, and Anesthesia Standards. Thursday, August 28 th, 2014
 Clarifying the Confusing CMS Hospital Surgery, PACU, and Anesthesia Standards Thursday, August 28 th, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety
Clarifying the Confusing CMS Hospital Surgery, PACU, and Anesthesia Standards Thursday, August 28 th, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety
CMS Requirements on Order Sets, Protocols, Preprinted and Standing Orders. Wednesday, February 12 th, 2014
 CMS Requirements on Order Sets, Protocols, Preprinted and Standing Orders Wednesday, February 12 th, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety
CMS Requirements on Order Sets, Protocols, Preprinted and Standing Orders Wednesday, February 12 th, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety
Policies and Procedures. Title:
 Policies and Procedures Title: PATIENT CONTROLLED ANALGESIA (PCA) LPN Additional Competency: Patient Controlled Analgesia with an Established Plan of Care RN Entry-Level Competency Authorization: [X] Former
Policies and Procedures Title: PATIENT CONTROLLED ANALGESIA (PCA) LPN Additional Competency: Patient Controlled Analgesia with an Established Plan of Care RN Entry-Level Competency Authorization: [X] Former
Ensuring Compliance with CMS Operating Room, Anesthesia and PACU Standards
 Ensuring Compliance with CMS Operating Room, Anesthesia and PACU Standards November 4, 2013 The information provided in AHC Media Webinars does not, and is not intended to constitute medical or legal advice.
Ensuring Compliance with CMS Operating Room, Anesthesia and PACU Standards November 4, 2013 The information provided in AHC Media Webinars does not, and is not intended to constitute medical or legal advice.
Contact Hours (CME version ONLY) Suggested Target Audience. all clinical and allied patient care staff. all clinical and allied patient care staff
 Suggested Target Audience. all clinical and allied patient care staff. all clinical and allied patient care staff") 1 Addressing Behaviors That Undermine a Culture of Safety PA CE CME FL 8/31/2016 2 2 7 3 43 1.0 1.0 1.0 all staff Sentinel Event Alert, Issue 40: Behaviors that undermine a culture of safety 2 Adverse
1 Addressing Behaviors That Undermine a Culture of Safety PA CE CME FL 8/31/2016 2 2 7 3 43 1.0 1.0 1.0 all staff Sentinel Event Alert, Issue 40: Behaviors that undermine a culture of safety 2 Adverse
Top Risk Management Issues Impacting Patient Safety. Tuesday, June 17 th, 2014
 Top Risk Management Issues Impacting Patient Safety Tuesday, June 17 th, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education Consulting
Top Risk Management Issues Impacting Patient Safety Tuesday, June 17 th, 2014 Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education Consulting
The Joint Commission Medication Management Update for 2010
 Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
Learning Objectives The Joint Commission Medication Management Update for 2010 U.S. Army Medical Command Fort Sam Houston, TX Describe most recent changes in The Joint Commission (TJC) Accreditation Program
Surgery, PACU and Anesthesia Standards: CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) TELNET 2904 May 6, :30 am EDT
 TELNET 2904 May 6, :30 am EDT") Surgery, PACU and Anesthesia Standards: CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2014 TELNET 2904 May 6, 2014 10-11:30 am EDT Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD
Surgery, PACU and Anesthesia Standards: CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2014 TELNET 2904 May 6, 2014 10-11:30 am EDT Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD
201 KAR 20:490. Licensed practical nurse intravenous therapy scope of practice.
 201 KAR 20:490. Licensed practical nurse intravenous therapy scope of practice. RELATES TO: KRS 314.011(10)(a), (c) STATUTORY AUTHORITY: KRS 314.011(10)(c), 314.131(1), 314.011(10)(c) NECESSITY, FUNCTION,
201 KAR 20:490. Licensed practical nurse intravenous therapy scope of practice. RELATES TO: KRS 314.011(10)(a), (c) STATUTORY AUTHORITY: KRS 314.011(10)(c), 314.131(1), 314.011(10)(c) NECESSITY, FUNCTION,
(10+ years since IOM)
") Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Encouraging pharmacy involvement in pharmacovigilance; an international perspective.
 Encouraging pharmacy involvement in pharmacovigilance; an international perspective. Michael R. Cohen, RPh, MS, ScD (hon) DPS (hon) Chairperson, International Medication Safety Network and President, Institute
Encouraging pharmacy involvement in pharmacovigilance; an international perspective. Michael R. Cohen, RPh, MS, ScD (hon) DPS (hon) Chairperson, International Medication Safety Network and President, Institute
60 Tips to Reduce Medications Errors
 60 Tips to Reduce Medications Errors Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education 5447 Fawnbrook Lane Dublin, Ohio 43017 614 791-1468
60 Tips to Reduce Medications Errors Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education 5447 Fawnbrook Lane Dublin, Ohio 43017 614 791-1468
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2011
 2011") CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2011 What Hospitals Need to Know About Grievances Speaker Sue Dill Calloway RN, Esq. CPHRM AD, BA, BSN, MSN, JD President Patient Safety and Education 5447
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2011 What Hospitals Need to Know About Grievances Speaker Sue Dill Calloway RN, Esq. CPHRM AD, BA, BSN, MSN, JD President Patient Safety and Education 5447
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
Saving Lives In the Medical Surgical Unit and Establishing a Successful Capnography Monitoring Program For Patients Receiving Opioid Medications
 Saving Lives In the Medical Surgical Unit and Establishing a Successful Capnography Monitoring Program For Patients Receiving Opioid Medications March 14, 2016 AAMI Foundation Vision: To drive the safe
Saving Lives In the Medical Surgical Unit and Establishing a Successful Capnography Monitoring Program For Patients Receiving Opioid Medications March 14, 2016 AAMI Foundation Vision: To drive the safe
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV TREPROSTINIL (REMODULIN ) Job Title of Reviewer: Director, Pharmacy POLICY
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV TREPROSTINIL (REMODULIN ) Job Title of Reviewer: Director, Pharmacy POLICY
Infusion Therapy Learning Exercise: Infusion Documentation
 Infusion Therapy Learning Exercise: Infusion Documentation INFUSION OF DOCUMENT IN DOCUMENT PERIPHERAL PICC LINE BLOOD TRANSFUSION SPINAL EPIDURAL CLPNA Infusion Therapy: Infusion Documentation Exercise
Infusion Therapy Learning Exercise: Infusion Documentation INFUSION OF DOCUMENT IN DOCUMENT PERIPHERAL PICC LINE BLOOD TRANSFUSION SPINAL EPIDURAL CLPNA Infusion Therapy: Infusion Documentation Exercise
Clarifying the Increased CMS UR Standards. Friday, May 9 th, 2014
 Clarifying the Increased CMS UR Standards Friday, May 9 th, 2014 Speaker Sue Dill Calloway RN, Esq AD, BA, BSN, MSN, JD CPHRM President of Patient Safety and Health Care Consulting Board Member Emergency
Clarifying the Increased CMS UR Standards Friday, May 9 th, 2014 Speaker Sue Dill Calloway RN, Esq AD, BA, BSN, MSN, JD CPHRM President of Patient Safety and Health Care Consulting Board Member Emergency
Small-bore Connectors New Standards and Designs May 31, :15 4:30 pm
 Small-bore Connectors New Standards and Designs May 31, 2014 3:15 4:30 pm Speakers & Panelists Scott Colburn - MS, BSN, RN Director of the Standards Program at the FDA s Center for Devices and Radiological
Small-bore Connectors New Standards and Designs May 31, 2014 3:15 4:30 pm Speakers & Panelists Scott Colburn - MS, BSN, RN Director of the Standards Program at the FDA s Center for Devices and Radiological
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
9/8/2014. I have no conflicts of interest to disclose. Conflict of Interest Disclosure. Carrie Brunson: Except
 ENSURING OPIOID SAFETY: DO OUR NURSES POSSESS THE KNOWLEDGE Click to add subtitle TO RESCUE PATIENTS? Carrie Brunson MSN, APRN-BC, ACNS-BC Clinical Nurse Specialist Acute Pain Service September 2014 ASPMN
ENSURING OPIOID SAFETY: DO OUR NURSES POSSESS THE KNOWLEDGE Click to add subtitle TO RESCUE PATIENTS? Carrie Brunson MSN, APRN-BC, ACNS-BC Clinical Nurse Specialist Acute Pain Service September 2014 ASPMN
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN
 Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Opioid Sedation Comparison Study
 Opioid Sedation Comparison Study Barbara U. Ochampaugh, RN, BSN, CPAN Level IV; Sandra Lowery, RN, CPAN Level III; Deborah J. Marra, RN, BS, CPAN Level III; and Nancy Salerno RN, MSN Respiratory depression
Opioid Sedation Comparison Study Barbara U. Ochampaugh, RN, BSN, CPAN Level IV; Sandra Lowery, RN, CPAN Level III; Deborah J. Marra, RN, BS, CPAN Level III; and Nancy Salerno RN, MSN Respiratory depression
Medication Safety & Electrolyte Administration. Objectives. High Alert Medications. *Med Safety Electrolyte Administration
 Medication Safety & Electrolyte Administration Jennifer Doughty, PharmD PGY2 Pharmacy Resident Emergency Medicine Stormont Vail Health, Topeka, KS Objectives Define and identify high alert medications
Medication Safety & Electrolyte Administration Jennifer Doughty, PharmD PGY2 Pharmacy Resident Emergency Medicine Stormont Vail Health, Topeka, KS Objectives Define and identify high alert medications
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
WYOMING STATE BOARD OF NURSING ADVISORY OPINION INTRAVENOUS THERAPY BY LICENSED PRACTICAL NURSES
 WYOMING STATE BOARD OF NURSING ADVISORY OPINION INTRAVENOUS THERAPY BY LICENSED PRACTICAL NURSES Advisory Opinion Number: 03-123 Board Meeting Date: April 28-May 1, 2003 January 7-10, 2008 February 18,
WYOMING STATE BOARD OF NURSING ADVISORY OPINION INTRAVENOUS THERAPY BY LICENSED PRACTICAL NURSES Advisory Opinion Number: 03-123 Board Meeting Date: April 28-May 1, 2003 January 7-10, 2008 February 18,
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS)
") PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
Sedation/Analgesia by Non-Anesthesiologists. THE UNIVERSITY OF TOLEDO Approving Officer:
 Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare. Friday October 14, 2016
 Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare Friday October 14, 2016 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National
Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare Friday October 14, 2016 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National
PHARMACY SERVICES/MEDICATION USE
 25.01. 10 Drug Reactions & Administration Errors & Incompatibilities. Drug administration errors, adverse drug reactions and incompatibilities must be immediately reported to the attending physician and
25.01. 10 Drug Reactions & Administration Errors & Incompatibilities. Drug administration errors, adverse drug reactions and incompatibilities must be immediately reported to the attending physician and
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool
 Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Within the Scope of Practice/Role of APRN RN _ X_LPN CNA ADVISORY OPINION LPN IV CERTIFIED (IV-C) COURSE REQUIREMENTS
 COURSE REQUIREMENTS") Wyoming State Board of Nursing 130 Hobbs Avenue, Suite B Cheyenne, WY 82002 Phone (307) 777-7601 Fax (307) 777-3519 E-Mail: wsbn-info-licensing@wyo.gov Home Page: https://nursing-online.state.wy.us/ OPINION:
Wyoming State Board of Nursing 130 Hobbs Avenue, Suite B Cheyenne, WY 82002 Phone (307) 777-7601 Fax (307) 777-3519 E-Mail: wsbn-info-licensing@wyo.gov Home Page: https://nursing-online.state.wy.us/ OPINION:
Objectives. Demographics: Type and Services 1/22/2014. ICAHN Aggregate Results. ISMP Medication Safety Self Assessment for Hospitals
 ICAHN Aggregate Results ISMP Medication Safety Self Assessment for Hospitals Matthew Fricker, RPH, MS, FASHP Rebecca Lamis, PharmD, FISMP January 23, 2014 1 Objectives Report the demographic characteristics
ICAHN Aggregate Results ISMP Medication Safety Self Assessment for Hospitals Matthew Fricker, RPH, MS, FASHP Rebecca Lamis, PharmD, FISMP January 23, 2014 1 Objectives Report the demographic characteristics
InformRx. Transition from Hospital to the LTC Facility: Preventing Medication Errors to Reduce Risk of Hospital Readmission
 CLINICAL & REGULATORY NEWS BY PHARMERICA NOV/DEC 2016 Transition from Hospital to the LTC Facility: Preventing Medication Errors to Reduce Risk of Hospital Readmission Transition from the hospital to the
CLINICAL & REGULATORY NEWS BY PHARMERICA NOV/DEC 2016 Transition from Hospital to the LTC Facility: Preventing Medication Errors to Reduce Risk of Hospital Readmission Transition from the hospital to the
The Joint Commission Medication Management Update for 2010
 The Joint Commission Medication Management Update for 2010 U.S. Army Manager, Army Patient Safety Program U.S. Army Medical Command Fort Sam Houston, TX CPE Information and Professional Resources & Business
The Joint Commission Medication Management Update for 2010 U.S. Army Manager, Army Patient Safety Program U.S. Army Medical Command Fort Sam Houston, TX CPE Information and Professional Resources & Business
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV EPOPROSTENOL (FLOLAN, VELETRI ) POLICY #: EFFECTIVE DATE: REVISED DATE: POLICY
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV EPOPROSTENOL (FLOLAN, VELETRI ) POLICY #: EFFECTIVE DATE: REVISED DATE: POLICY
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL
 CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
Interpretation of The Joint Commission Standards Related to Pain Management. Agenda. The Joint Commission Mission 9/6/2012
 Interpretation of The Joint Commission Standards Related to Pain Management ASPMN 22 nd National Conference Baltimore, MD September 13, 2012 Pat Adamski, RN, MS, MBA, FACHE Director, Standards Interpretation
Interpretation of The Joint Commission Standards Related to Pain Management ASPMN 22 nd National Conference Baltimore, MD September 13, 2012 Pat Adamski, RN, MS, MBA, FACHE Director, Standards Interpretation
Pharmacy Services. Division of Nursing Homes
 Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
If viewing a printed copy of this policy, please note it could be expired. Got to to view current policies.
 If viewing a printed copy of this policy, please note it could be expired. Got to www.fairview.org/fhipolicies to view current policies. Department Policy Entity: Fairview Pharmacy Services Department:
If viewing a printed copy of this policy, please note it could be expired. Got to www.fairview.org/fhipolicies to view current policies. Department Policy Entity: Fairview Pharmacy Services Department:
CONSENT FOR SURGERY OR SPECIAL PROCEDURES
 Admission Date THE VALLEY HOSPITAL CONSENT FOR SURGERY OR SPECIAL PROCEDURES - Colonoscopy 1. Authorization. I hereby authorize Dr. (" my Doctor") and any such assistants or designees as may be selected
Admission Date THE VALLEY HOSPITAL CONSENT FOR SURGERY OR SPECIAL PROCEDURES - Colonoscopy 1. Authorization. I hereby authorize Dr. (" my Doctor") and any such assistants or designees as may be selected
A Game Plan to Surviving a Joint Commission Survey. May Adra, BS Pharm, PharmD, BCPS
 A Game Plan to Surviving a Joint Commission Survey May Adra, BS Pharm, PharmD, BCPS Objectives Describe key components of a Joint Commission accreditation visit Identify changes to medication management
A Game Plan to Surviving a Joint Commission Survey May Adra, BS Pharm, PharmD, BCPS Objectives Describe key components of a Joint Commission accreditation visit Identify changes to medication management
WHAT are medication errors?
 Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Storage, Labeling, Controlled Medications Instructor s Guide CFR (b)(2)(3)(d)(e) F431
(2)(3)(d)(e) F431") Centers for Medicare & Medicaid Services (CMS) Storage, Labeling, Controlled Medications Instructor s Guide CFR 483.60(b)(2)(3)(d)(e) F431 2006 Prepared by: American Institutes for Research 1000 Thomas
Centers for Medicare & Medicaid Services (CMS) Storage, Labeling, Controlled Medications Instructor s Guide CFR 483.60(b)(2)(3)(d)(e) F431 2006 Prepared by: American Institutes for Research 1000 Thomas
Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003
 Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003 Susan M. Proulx, Pharm.D. President, Med-E.R.R.S. Subsidiary of ISMP (www.med-errs.com) Mission of ISMP Translate errors into education
Managing Pharmaceuticals to Reduce Medication Errors August 26, 2003 Susan M. Proulx, Pharm.D. President, Med-E.R.R.S. Subsidiary of ISMP (www.med-errs.com) Mission of ISMP Translate errors into education
PROCEDURAL SEDATION AND ANALGESIA: HOSPITAL-WIDE POLICY
 CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
CRAIG HOSPITAL POLICY/PROCEDURE
 CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
UW MEDICINE PATIENT EDUCATION. Angiography: Percutaneous or Transjugular Liver Biopsy. How to prepare and what to expect. What is a liver biopsy?
 UW MEDICINE PATIENT EDUCATION Angiography: Percutaneous or Transjugular Liver Biopsy How to prepare and what to expect This handout explains how to prepare and what to expect when having a percutaneous
UW MEDICINE PATIENT EDUCATION Angiography: Percutaneous or Transjugular Liver Biopsy How to prepare and what to expect This handout explains how to prepare and what to expect when having a percutaneous
Nurse Orientation. Medication Management
 Nurse Orientation Medication Management Objectives Discuss basic principles/rights of medication administration, according to your site policy Describe principles of patient/family education related to
Nurse Orientation Medication Management Objectives Discuss basic principles/rights of medication administration, according to your site policy Describe principles of patient/family education related to
Beth Israel Deaconess Medical Center Perioperative Services Manual. Guidelines for Perioperative Handoffs from OR to receiving units.
 Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Beth Israel Deaconess Medical Center Perioperative Services Manual Title: Guidelines for Perioperative Handoffs from OR to receiving units. Policy #: PSM 100-102A Purpose: This guideline provides a standard
Accreditation Program: Long Term Care
 ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
REVISED: 7/03, 03/05, 04/08, 3/10, 11/11, 09/13, 3/14,1/15, 4/16
 TITLE/DESCRIPTION: DEPARTMENT: PERSONNEL: BLOOD PRODUCT ADMINISTRATION CLINICAL LABORATORY ALL HOSPITAL EMPLOYEES EFFECTIVE DATE: 10/95 REVISED: 7/03, 03/05, 04/08, 3/10, 11/11, 09/13, 3/14,1/15, 4/16
TITLE/DESCRIPTION: DEPARTMENT: PERSONNEL: BLOOD PRODUCT ADMINISTRATION CLINICAL LABORATORY ALL HOSPITAL EMPLOYEES EFFECTIVE DATE: 10/95 REVISED: 7/03, 03/05, 04/08, 3/10, 11/11, 09/13, 3/14,1/15, 4/16
TELNET COURSE T2861 PART 1 (WEBINAR) TELNET COURSE T2864 PART 2 (WEBINAR) TELNET COURSE T2866 PART 3 (WEBINAR) DATE: SEPTEMBER 26, 2013
 TELNET COURSE T2864 PART 2 (WEBINAR) TELNET COURSE T2866 PART 3 (WEBINAR) DATE: SEPTEMBER 26, 2013") CMS Conditions of Participation (CoPs) for Critical Access Hospitals (CAHS): Ensuring Compliance This is a 3-part series; each program can be taken independent of the others. TELNET COURSE T2861 PART 1
CMS Conditions of Participation (CoPs) for Critical Access Hospitals (CAHS): Ensuring Compliance This is a 3-part series; each program can be taken independent of the others. TELNET COURSE T2861 PART 1
Monitoring Medication Storage & Administration
 Monitoring Medication Storage & Administration Objectives Review F-Tags pertaining to medication management Discuss proper medication storage and administration Understand medication cart and medication
Monitoring Medication Storage & Administration Objectives Review F-Tags pertaining to medication management Discuss proper medication storage and administration Understand medication cart and medication
Update on Pharmacy Issues in Long Term Care Lisa Nichols RPh, CGP
 Update on Pharmacy Issues in Long Term Care Lisa Nichols RPh, CGP 1.Review What a Consultant Pharmacist Does and the Role of Pharmacy for Long Term Care Facilities 2.Identify Key Components of a Medication
Update on Pharmacy Issues in Long Term Care Lisa Nichols RPh, CGP 1.Review What a Consultant Pharmacist Does and the Role of Pharmacy for Long Term Care Facilities 2.Identify Key Components of a Medication
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
U: Medication Administration
 U: Medication Administration Alberta Licensed Practical Nurses Competency Profile 199 Competency: U-1 Pharmacology and Principles of Administration of Medications U-1-1 U-1-2 U-1-3 U-1-4 Demonstrate knowledge
U: Medication Administration Alberta Licensed Practical Nurses Competency Profile 199 Competency: U-1 Pharmacology and Principles of Administration of Medications U-1-1 U-1-2 U-1-3 U-1-4 Demonstrate knowledge
N ATIONAL Q UALITY F ORUM. Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT
 N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
Medication Safety Way Beyond the 5 Rights
 Safety Way Beyond the 5 Rights JoAnne Phillips, MSN, RN, CCRN, CCNS, CPPS The University of Pennsylvania Health System Philadelphia, PA Current State. Of Chaos Prescriptions 12 per /person / year 4 BILLION
Safety Way Beyond the 5 Rights JoAnne Phillips, MSN, RN, CCRN, CCNS, CPPS The University of Pennsylvania Health System Philadelphia, PA Current State. Of Chaos Prescriptions 12 per /person / year 4 BILLION
PATIENT CARE MANUAL PROCEDURE
 PATIENT CARE MANUAL PROCEDURE NUMBER III-130 PAGE 1 OF 5 APPROVED BY: CATEGORY: Vice President and Senior Operating Officer, Rural Health Services & Professional Practice Lead Medication Administration
PATIENT CARE MANUAL PROCEDURE NUMBER III-130 PAGE 1 OF 5 APPROVED BY: CATEGORY: Vice President and Senior Operating Officer, Rural Health Services & Professional Practice Lead Medication Administration
UW MEDICINE PATIENT EDUCATION. How to prepare and what to expect DRAFT. What is an IVC filter?
 UW MEDICINE PATIENT EDUCATION Angiography: Inferior Vena Cava (IVC) Filter How to prepare and what to expect This handout explains what an inferior vena cava filter is and what to expect when you have
UW MEDICINE PATIENT EDUCATION Angiography: Inferior Vena Cava (IVC) Filter How to prepare and what to expect This handout explains what an inferior vena cava filter is and what to expect when you have
MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER
 KINGSTON GENERAL HOSPITAL MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER LEARNING GUIDE FOR REGISTERED NURSES AND REGISTERED PRACTICAL NURSES Prepared by: Nursing Education Date: 2001 November Revised:
KINGSTON GENERAL HOSPITAL MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER LEARNING GUIDE FOR REGISTERED NURSES AND REGISTERED PRACTICAL NURSES Prepared by: Nursing Education Date: 2001 November Revised:
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses
 Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses March 2018 College of Licensed Practical Nurses of Nova Scotia http://clpnns.ca Starlite Gallery, 302-7071 Bayers Road,
Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses March 2018 College of Licensed Practical Nurses of Nova Scotia http://clpnns.ca Starlite Gallery, 302-7071 Bayers Road,
University of Mississippi Medical Center University of Mississippi Health Care. Pharmacy and Therapeutics Committee Medication Use Evaluation
 University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
The CMS State Operations Manual Overview and Changes
 The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
Using Clinical Data Categories with the Pyxis MedStation
 Using Clinical Data Categories with the Pyxis MedStation system Using Clinical Data Categories Clinical Data Categories (CDCs) are a Pyxis MedStation system software tool that will allow facilities the
Using Clinical Data Categories with the Pyxis MedStation system Using Clinical Data Categories Clinical Data Categories (CDCs) are a Pyxis MedStation system software tool that will allow facilities the
To prevent harm to patients from adverse medication events involving high-alert medications.
 TITLE MANAGEMENT OF HIGH-ALERT MEDICATIONS DOCUMENT # PS-46-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Management of High-alert Medications Policy APPROVAL LEVEL Alberta Health Services Executive
TITLE MANAGEMENT OF HIGH-ALERT MEDICATIONS DOCUMENT # PS-46-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Management of High-alert Medications Policy APPROVAL LEVEL Alberta Health Services Executive
High Alert Medications: Reducing Patient Harm
 High Alert Medications: Reducing Patient Harm Building a Bridge to Better Health Coalition Brian D. Esters, PharmD, CPPS Assistant Professor of Pharmacy Practice Tennessee Pharmacist Coalition Vision Reduce
High Alert Medications: Reducing Patient Harm Building a Bridge to Better Health Coalition Brian D. Esters, PharmD, CPPS Assistant Professor of Pharmacy Practice Tennessee Pharmacist Coalition Vision Reduce
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) Speaker. You Don t Want One of These 4/26/2017. What Hospitals Need to Know About Grievances
 Speaker. You Don t Want One of These 4/26/2017. What Hospitals Need to Know About Grievances") CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2017 What Hospitals Need to Know About Grievances Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2017 What Hospitals Need to Know About Grievances Speaker Sue Dill Calloway RN, Esq. CPHRM, CCMSCP AD, BA, BSN, MSN, JD President of Patient Safety and Education
Wyoming STATE BOARD OF NURSING
 David D. Freudenthal Governor Wyoming STATE BOARD OF NURSING Mary Kay Goetter, PhD, RNC, NEA-BC Executive Director 1810 Pioneer Avenue Cheyenne, Wyoming 82002 Phone: 307-777-7601 FAX: 307-777-3519 http://nursing.state.wy.us
David D. Freudenthal Governor Wyoming STATE BOARD OF NURSING Mary Kay Goetter, PhD, RNC, NEA-BC Executive Director 1810 Pioneer Avenue Cheyenne, Wyoming 82002 Phone: 307-777-7601 FAX: 307-777-3519 http://nursing.state.wy.us
ACCOUNT NO. MED. REC. NO. NAME BIRTHDATE. Patient Identification ALL ORDERS MUST BE MARKED IN INK WITH A CHECKMARK ( ) TO BE ACTIVE.
 TO BE ACTIVE.") PO7071 *PO7071* Page 1 of 4 ALL MUST BE MARKED IN INK WITH A CHECKMARK ( ) TO BE ACTIVE. Weight: kg Height: cm Allergies: Treatment Start Date: Date(s) of Transfusion(s): Current Labs: WBC: Hgb/Hct: Platelets:
PO7071 *PO7071* Page 1 of 4 ALL MUST BE MARKED IN INK WITH A CHECKMARK ( ) TO BE ACTIVE. Weight: kg Height: cm Allergies: Treatment Start Date: Date(s) of Transfusion(s): Current Labs: WBC: Hgb/Hct: Platelets:
Department Policy. Code: D: MM Entity: Fairview Pharmacy Services. Department: Fairview Home Infusion. Manual: Policy and Procedure Manual
 Department Policy Code: D: MM-5615 Entity: Fairview Pharmacy Services Department: Fairview Home Infusion Manual: Policy and Procedure Manual Category: Home Infusion Subject: Chemotherapy Purpose: Ensure
Department Policy Code: D: MM-5615 Entity: Fairview Pharmacy Services Department: Fairview Home Infusion Manual: Policy and Procedure Manual Category: Home Infusion Subject: Chemotherapy Purpose: Ensure
Reviewed 8/31/2013. Susan Parrish MSN RN
 Reviewed 8/31/2013 Susan Parrish MSN RN After completion of this self study packet, the nurse should be able to: Identify the required components of the physician's order for blood transfusion products.
Reviewed 8/31/2013 Susan Parrish MSN RN After completion of this self study packet, the nurse should be able to: Identify the required components of the physician's order for blood transfusion products.
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Session 2 Improving Narcotics and Opiate Management
 Session 2 Improving Narcotics and Opiate Management Frank Federico, RPh, IHI Executive Director Steve Meisel, Pharm.D., IHI Faculty January 31,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH,
Session 2 Improving Narcotics and Opiate Management Frank Federico, RPh, IHI Executive Director Steve Meisel, Pharm.D., IHI Faculty January 31,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH,
Financial Disclosure. Learning Objectives: Preventing and Responding to Sentinel Events in Surgery 10/13/2015
 Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Medication Related Changes Phase 1&2
 Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Safe Medication Practices
 Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610 X 6 STANDARDS OF NURSING PRACTICE TABLE OF CONTENTS
 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610 X 6 STANDARDS OF NURSING PRACTICE TABLE OF CONTENTS 610 X 6.01 610 X 6.02 610 X 6.03 610 X 6.04 610 X 6.05 610 X 6.06 610 X 6.07 610 X 6.08 610
ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610 X 6 STANDARDS OF NURSING PRACTICE TABLE OF CONTENTS 610 X 6.01 610 X 6.02 610 X 6.03 610 X 6.04 610 X 6.05 610 X 6.06 610 X 6.07 610 X 6.08 610
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Required Organizational Practices Resources for 2016
 Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
HealthStream Ambulatory Regulatory Course Descriptions
 This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
Raise your game: The UP Campaign. Bruce Spurlock, M.D. Cynosure Health
 Raise your game: The UP Campaign Bruce Spurlock, M.D. Cynosure Health 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Can we streamline & simplify making it easier for front-line staff and still improve safety? 16
Raise your game: The UP Campaign Bruce Spurlock, M.D. Cynosure Health 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Can we streamline & simplify making it easier for front-line staff and still improve safety? 16
Bar Code Medication Administration and MAR Resource Manual
 Bar Code Medication Administration and MAR Resource Manual Creating Orders Creating an Order in CareMobile (Ad Hoc Order Entry)...2 Creating an Order for med that is already ordered with a different dose/frequency....4
Bar Code Medication Administration and MAR Resource Manual Creating Orders Creating an Order in CareMobile (Ad Hoc Order Entry)...2 Creating an Order for med that is already ordered with a different dose/frequency....4
Admission Record IVF/Gynae
 Admission Record IVF/Gynae Surgeon: Operation : of Admission: Please state your full name and date of birth - correct Nurse Checklist Yes No Please tell me your full address - correct Consent form signed,
Admission Record IVF/Gynae Surgeon: Operation : of Admission: Please state your full name and date of birth - correct Nurse Checklist Yes No Please tell me your full address - correct Consent form signed,
VERMONT2008 Patient Safety, Surveillance, and Improvement System
 VERMONT2008 Patient Safety, Surveillance, and Improvement System Report to the Legislature on Act 215 (2006), 18 V.S.A. 1913(e) 108 Cherry Street, PO Box 70 Burlington, VT 05402 1.802.863.7341 healthvermont.gov
VERMONT2008 Patient Safety, Surveillance, and Improvement System Report to the Legislature on Act 215 (2006), 18 V.S.A. 1913(e) 108 Cherry Street, PO Box 70 Burlington, VT 05402 1.802.863.7341 healthvermont.gov
3/9/2010. Objectives. Pharmacist Role in Medication Safety and Regulatory Compliance
 Pharmacist Role in Medication Safety and Regulatory Compliance Janet Greiwe Vice President, Systems Management Cleveland County Health System Objectives By the end of this presentation, you should be able
Pharmacist Role in Medication Safety and Regulatory Compliance Janet Greiwe Vice President, Systems Management Cleveland County Health System Objectives By the end of this presentation, you should be able
DRAFT. WORKING DRAFT Nursing associate skills annexe. Part of the draft standards of proficiency for nursing associates. Page 1
 WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
GENERAL ADMINISTRATIVE POLICY: ADVERSE EVENT REPORTING TO CALIFORNIA DEPARTMENT OF PUBLIC HEALTH (CDPH)
") GENERAL ADMINISTRATIVE POLICY: ADVERSE EVENT REPORTING TO CALIFORNIA DEPARTMENT OF PUBLIC HEALTH (CDPH) Effective Date: 02/12 Page No. 1 of 7 I. PURPOSE To comply with mandated reporting requirements of
GENERAL ADMINISTRATIVE POLICY: ADVERSE EVENT REPORTING TO CALIFORNIA DEPARTMENT OF PUBLIC HEALTH (CDPH) Effective Date: 02/12 Page No. 1 of 7 I. PURPOSE To comply with mandated reporting requirements of
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
WYOMING STATE BOARD OF NURSING ADVISORY OPINION
 WYOMING STATE BOARD OF NURSING ADVISORY OPINION INTRAVENOUS THERAPY BY LICENSED PRACTICAL NURSES Advisory Opinion Number: 03-123 Board Meeting Date: April 28-May 1, 2003 January 7-10, 2008 Introduction:
WYOMING STATE BOARD OF NURSING ADVISORY OPINION INTRAVENOUS THERAPY BY LICENSED PRACTICAL NURSES Advisory Opinion Number: 03-123 Board Meeting Date: April 28-May 1, 2003 January 7-10, 2008 Introduction: