The New Survey Process for the NAC. Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC
|
|
|
- Lorraine Conley
- 5 years ago
- Views:
Transcription
1 The New Survey Process for the NAC Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC
2 Faculty Disclosure I have no financial relationships to disclose I have no conflicts of interests to disclose I will not promote any commercial products or services 2
3 Requirements for Successful Completion 1.0 contact hour will be awarded for this continuing nursing education activity Criteria for successful completion includes attendance for at least 80% of the entire event. Partial credit may not be awarded Approval of this continuing education activity does not imply endorsement by AANAC or ANCC (American Nurses Credential Center) of any commercial products or services American Association of Post-Acute Care Nursing (AAPACN)* is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center s Commission on Accreditation. *AAPACN d/b/a American Association of Nurse Assessment Coordination 3
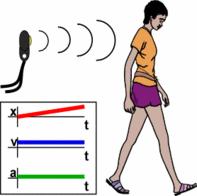
4 Objectives State how the MDS will be used to develop the survey sample off-site Explain how motion sensors can have the effect of restraining a resident State the timeline for Baseline Care Plans Describe how the new 2017 Section N MDS items tie to the new regulations and the survey process 4
5 Phase 2 of New SNF Regulations Implement by November 28, 2017 Providers must be in compliance with Phase 2 regulations All States will use new computer based survey process for LTC surveys All training on new survey process needs to be completed before go live date 5
6 Phase 2: November 28, 2017 Implementation Date Phase 1: November 28, 2016 (Implemented) Phase 2: November 28, 2017 Phase 3: November 28, 2019 Type of Change Nursing Home Requirements for Participation F Tag numbering Interpretive Guidance (IG) Implement new survey process Requirements need more time to implement Details of Change New Regulatory Language uploaded to the Automated Survey Processing Environment (ASPEN) under current F Tags New F Tags Updated IG Begin surveying with the new survey process Requirements that need more time to implement 6
7 Phase 2 of LTC Regulations 1 Phase 2 includes, but is not limited to: Comprehensive Person-Centered Care Planning: Baseline Care Plans Pharmacy Services: psychotropic medications; drug regimen review and reporting Dental Services: replacing lost dentures Administration: Facility Assessment tied to sufficient and competent staff requirements 7
8 Phase 2 of LTC Regulations 2 Continued Phase 2 includes: Behavioral Health Services Quality Assurance and Performance Improvements: QAPI Plan Only Infection Control and Antibiotic Stewardship Physical Environment: smoking policies 8
9 Phase 2 of LTC Regulations 3 Continued Phase 2 includes, but is not limited to: Resident Rights and Facility Responsibilities: Required Contact Information Freedom from Abuse, Neglect, and Exploitation: 1150B Admission, Transfer, and Discharge Rights: Transfer/Discharge Documentation 9

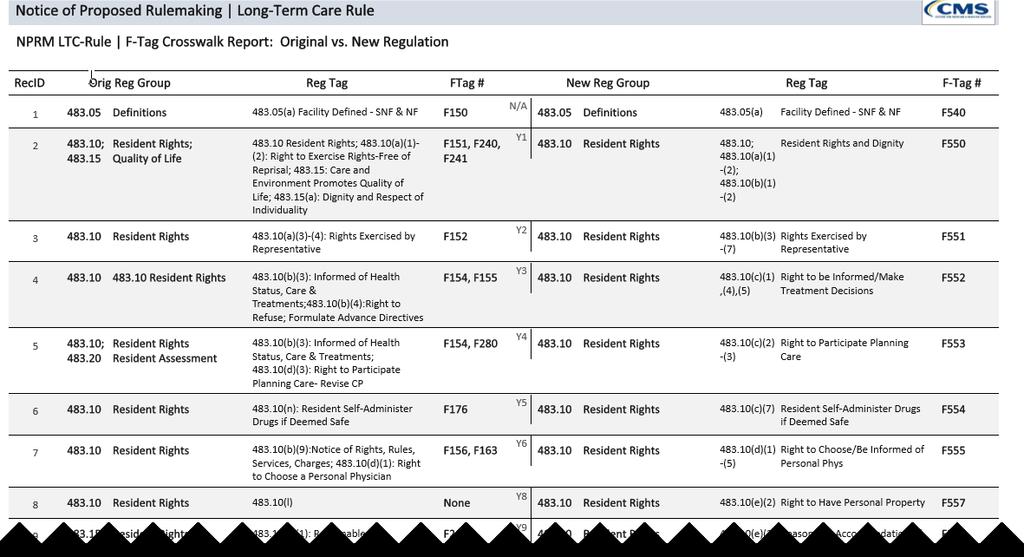
10 Survey F-Tags Renumbered 10


11 F-Tag Renumbering The image above is the F Tag Crosswalk showing: The original regulatory grouping and the new associated grouping The original regulation number and the new associated regulation number The original F Tag and the associated new F Tag lowest tag number will be
12 F-Tag Renumbering 12
13 Why is CMS Changing the Survey Process? Two different survey processes existed to review for the Requirements of Participation (Traditional and QIS) Surveyors identified opportunities to improve the efficiency and effectiveness of both survey processes The two processes appeared to identify slightly different quality of care/quality of life issues CMS set out to build on the best of both the Traditional and QIS processes to establish a single nationwide survey process 13
14 Goals for the New Survey Process Same survey for entire country Strengths from Traditional and QIS Traditional survey strength surveyor Could ask residents questions QIS survey strength computer based Process and pathways as investigative tools New innovative approaches Effective and efficient Resident-centered resident-specific concerns identified through observation and interviews are emphasized Balance between structure and surveyor autonomy 14

15 New Survey Process Each survey team member uses a tablet or laptop PC throughout the survey process to record findings that are synthesized and organized by new software Automation 15
16 New Survey Process Sample Selection Sample size is determined by the facility census 70% of the total sample is MDS pre-selected residents and 30% of the total sample is surveyor-selected residents. Surveyors finalize the sample based on observations, interviews, and a limited record review Maximum sample size is 35 residents 16
17 Off-Site Preparation Each surveyor team member independently reviews the CASPER 3 report and other facility history information Review offsite selected residents (70% chosen by their MDS data) and their indicators and the facility rates. (NAC Alert: Run the Resident Roster report in the CASPER system at least monthly. This report lists residents who are present in the facility according to the MDS assessments transmitted to QIES ASAP). 17
18 Information Needed on Entrance Completed new matrix (shown in later slide) Facility census number Alphabetical list of residents List of residents who smoke and designated smoking times (NAC Alert: Be sure that a care plan has been developed and updated for each resident who smokes). Updated information related to Medicare Beneficiary and Denial Notices 18
19 The Other 30% of the Sample The team will select 30% of the residents onsite, including vulnerable residents who are dependent on staff, new admissions within the last 30 days, complaints or facility-reported incidents or FRIs which would cover any alleged violation involving mistreatment, neglect, abuse, injuries of unknown origin, and misappropriation of property and any resident who has a significant concern but does not fall into any of the sub-groups. 19
20 Sample Size The sample size is based on the facility census Generally, the sample size is about 20% of the facility census In some cases, the sample size is slightly higher than the numbers included in the Traditional sample size grid but lower than the sample size for QIS One example is the cap for facilities with a census at or above 175 residents The cap for the Traditional is set at 30 and the cap for QIS is set at 40. The New LTC Survey Process has a cap of 35 residents for larger facilities 20
21 Surveyor Assignments Unit and mandatory facility task assignments Dining Infection Control (Antibiotic stewardship) Skilled Nursing Facility (SNF) Beneficiary Protection Notification Review Resident Council Meeting 21

22 Facility Entrance Skilled Nursing Facility 22
")
23 Updated Facility Matrix (Draft) 23
24 Day One of Survey The first day of the survey, or about eight hours, depending on when the team enters, is spent conducting observations, interviews, and a limited record review for the residents in the initial pool The survey team will be out on the units observing the residents in their assigned areas. They will focus on the 70% sample and will add additional names from their observation of vulnerable residents and new admissions 24
25 Resident Interviews by Surveyors Surveyors will screen every resident Suggested questions, but not a specific surveyor script Must cover all care areas Includes: Rights, QOL, QOC Interviews will take about 20 minutes each Investigate further or decide there was no issue (For example, if the resident says they had an issue with their roommate, but the facility addressed the concern to their satisfaction, surveyors would not need to investigate further; conversely, they would want to investigate a concern if the resident says they have lost weight recently because of their loose dentures unaddressed by the facility). 25
26 Surveyor Observations Cover all care areas and probes Conduct rounds Complete formal observations (e.g., wounds or incontinence care) Investigate further or no issue identified (Surveyors may complete formal observations for wounds or incontinence care if the situation presents itself or is necessary. For example, if a resident has not been assisted to the bathroom for a long period of time or is covered in bed). 26
27 Family/Representative Interviews for 3 Non-interviewable Residents Non-interviewable residents (goal is to complete at least 3 representative/family interviews) Surveyors will interview representatives who are familiar with the resident s care Complete at least three during initial pool process or early enough to follow up on concerns Sampled residents if possible Investigate further or no issue 27
28 Limited Record Reviews Surveyors will conduct limited record review after interviews and observations are completed prior to sample selection All initial pool residents: advance directives and confirm specific information If interview not conducted: review certain care areas in record Confirm insulin, anticoagulant, and antipsychotic with a diagnosis of Alzheimer s or dementia, and PASARR (Pre-Admission Screening and Resident Review)[e.g., has appropriate diagnosis but is not receiving PASARR Level II services] 28

29 October 1, 2017 RAI Manual Updates Section N 29

30 October 1, 2017 MDS Update 30

31 October 1, 2017 Update 31
32 MDS Focus Ensure Section N entries are correct for psychotropic, anticoagulant, and antibiotic medications Remember, medications are coded in Section N according to their pharmacological classification, not how they are used/ordered For example, Trazadone is an antidepressant medication that is often ordered to help a resident to sleep. Code it as an antidepressant on the MDS Are the care plans up-to-date? 32
33 Section I Diagnoses Surveyors will be looking for residents with dementia who are also on an antipsychotic medication, insulin or anticoagulants. Is your Section I coding correct? Did the physician write the diagnosis within the last 60 days? Is the diagnosis active in the last 7 days? 33
34 PASARR Are there residents who have diagnoses of mental illness when dementia is not primary or an intellectual or developmental disability in the facility who are not identified as a Level II in the PASSAR process? If the resident does have a Level II PASSAR determination, are the PASSAR recommendations included in the resident s care plan? 34

35 Restraints 35
36 Regulation (a)(2) Ensure that the resident is free from physical or chemical restraints imposed for purposes of discipline or convenience and that are not required to treat the resident s medical symptoms. When the use of restraints is indicated, the facility must use the least restrictive alternative for the least amount of time and document ongoing reevaluation of the need for restraints. 36
37 Intent The intent of this requirement is for each resident to attain and maintain his/her highest practicable wellbeing in an environment that: Prohibits the use of physical restraints for discipline or convenience; Prohibits the use of physical restraints to unnecessarily inhibit a resident s freedom of movement or activity; and Limits physical restraint use to circumstances in which the resident has medical symptoms that may warrant the use of restraints. When a physical restraint is used, the facility must: Use the least restrictive restraint for the least amount of time; and Provide ongoing re-evaluation of the need for the physical restraint. 37
38 Definitions Convenience is defined as the result of any action that has the effect of altering a resident s behavior such that the resident requires a lesser amount of effort or care, and is not in the resident s best interest Discipline is defined as any action taken by the facility for the purpose of punishing or penalizing residents Freedom of movement means any change in place or position for the body or any part of the body that the person is physically able to control Manual method means to hold or limit a resident s voluntary movement by using body contact as a method of physical restraint Medical symptom is defined as an indication or characteristic of a physical or psychological condition Position change alarms are alerting devices intended to monitor a resident s movement. The devices emit an audible signal when the resident moves in certain ways 38

39 October 1, 2017 MDS Items 39
40 Definition of Physical Restraint Physical restraint is defined as any manual method, physical or mechanical device, equipment, or material that meets all of the following criteria: Is attached or adjacent to the resident s body; Cannot be removed easily by the resident; and Restricts the resident s freedom of movement or normal access to his/her body Removes easily means that the manual method, physical or mechanical device, equipment, or material, can be removed intentionally by the resident in the same manner as it was applied by the staff 40
41 Examples of Facility Practices that Meet the Definition of Restraint Use 1 Using bed rails that keep a resident from voluntarily getting out of bed; Placing a chair or bed close enough to a wall that the resident is prevented from rising out of the chair or voluntarily getting out of bed; Placing a resident on a concave mattress so that the resident cannot independently get out of bed; Tucking in a sheet tightly so that the resident cannot get out of bed, or fastening fabric or clothing so that a resident s freedom of movement is restricted; Placing a resident in a chair, such as a beanbag or recliner, that prevents a resident from rising independently; 41
42 Examples of Facility Practices that Meet the Definition of Restraint Use 2 Using devices in conjunction with a chair, such as trays, tables, cushions, bars or belts, that the resident cannot remove and prevents the resident from rising; Applying leg or arm restraints, hand mitts, soft ties or vests that the resident cannot remove; Holding down a resident in response to a behavioral symptom or during the provision of care if the resident is resistive or refusing the care; Placing a resident in an enclosed framed wheeled walker, in which the resident cannot open the front gate or if the device has been altered to prevent the resident from exiting the device; and Using a position change alarm to monitor resident movement, and the resident is afraid to move to avoid setting off the alarm 42
43 Determination of the Use of Position Change Alarms as Restraints 1 Position change alarms are any physical or electronic device that monitors resident movement and alerts the staff when movement is detected. Types of position change alarms include chair and bed sensor pads, bedside alarmed mats, alarms clipped to a resident s clothing, seatbelt alarms, and infrared beam motion detectors. Position change alarms do not include alarms intended to monitor for unsafe wandering such as door or elevator alarms. 43
44 Determination of the Use of Position Change Alarms as Restraints 2 While position change alarms may be implemented to monitor a resident s movements, for some residents, the use of position change alarms that are audible to the resident(s) may have the unintended consequence of inhibiting freedom of movement. For example, a resident may be afraid to move to avoid setting off the alarm and creating noise that is a nuisance to the resident(s) and staff, or is embarrassing to the resident. For this resident, a position change alarm may have the potential effect of a physical restraint. 44
45 Potential Negative Outcomes from Position Change Alarms Examples of negative potential or actual outcomes which may result from the use of position change alarms as a physical restraint, include: Loss of dignity; Decreased mobility; Bowel and bladder incontinence; Sleep disturbances due to the sound of the alarm or because the resident is afraid to move in bed thereby setting off the alarm; and Confusion, fear, agitation, anxiety, or irritation in response to the sound of the alarm as residents may mistake the alarm as a warning or as something they need to get away from 45


46 Surveyors Will Observe 1 st Meal Dining surveyors to observe first full meal after their entrance Cover all dining rooms and room trays Observe enough to adequately identify concerns If feasible, observe initial pool residents with weight loss If concerns identified, observe another meal 46
47 Unnecessary Medication Survey software system selects 5 residents for full medication review. Selection process considers all psychotropic meds, insulin, anticoagulants, opioids, diuretics and antibiotics, as well as adverse consequences, such as falls, weight loss and sedation There are exclusions; for example, a resident would be excluded if they had a diagnosis of Huntington s or Schizophrenia and was receiving an antipsychotic Residents selected for full medication review include insulin, an anticoagulant, and an antipsychotic with Alzheimer s or dementia, if available Based on observation, interview, record review, and MDS Broad range of high-risk medications and adverse consequences Residents may or may not be in sample 47
 Continuous observations, if required. Is the care plan being followed?")
48 Surveyor Investigations Surveyors will conduct investigations for all concerns that warrant further investigation for sampled residents (pressure ulcers, incontinence, etc.) Continuous observations, if required. Is the care plan being followed? Interview representative, if appropriate, when concerns are identified 48
49 Closed Record Reviews Completed during the investigation portion of survey Unexpected death (not on hospice), hospitalization (went to the hospital and did not return in last 90 days), and community discharge in last 90 days System selected or discharged resident Use Appendix PP and Critical Elements Pathways 49
50 Infection Control Throughout survey, all surveyors should observe for infection control Assigned surveyor coordinates a review of influenza and pneumococcal vaccinations for at least 5 residents Assigned surveyor reviews infection prevention and control, and antibiotic stewardship program One resident who is on transmission-based precautions will be reviewed The assigned surveyor will also complete a review of the infection prevention and control and antibiotic stewardship program 50
51 Transmission-based Precautions Coding O0100M Code O0100M only when all of the following conditions are met: The resident has active infection with highly transmissible or epidemiologically significant pathogens that have been acquired by physical contact or airborne or droplet transmission Precautions are over and above Standard Precautions. That is, transmission-based precautions (contact, droplet, and/or airborne) must be in effect The resident is in a room alone because of active infection and cannot have a roommate. That means the resident must be in the room alone and not cohorted with a roommate regardless of whether the roommate has a similar active infection that requires isolation The resident must remain in his/her room. This requires that all services be brought to the resident (e.g., rehabilitation, activities, dining, etc.) 51

52 Criteria Would Not Apply 1. Urinary Tract Infections, 2. Encapsulated Pneumonia 3. Wound Infections 4. S/P MRSA with no active symptoms 5. S/P C-diff with no active symptoms 52
53 SNF Beneficiary Protection Notification Review A new pathway has been developed List of residents (home and in-facility) Randomly select three residents (Facility must report residents who had been discharged from Medicare A during the surveyors entrance conference) Facility completes new worksheet Review worksheet and notices 53

54 Kitchen Observations In addition to the brief kitchen observation upon entrance, conduct full kitchen investigation Follow Appendix PP and Facility Task Pathway to complete kitchen investigation 54


55 Med Carts and Medication Storage Rooms will be Examined Medication Storage Observe half of medication storage rooms and half of medication carts If issues, expand medication room/cart 55
56 Sufficient and Competent Staff Is a mandatory task, refer to revised Facility Task Pathway Sufficient and competent staff Throughout the survey, consider if staffing concerns can be linked to quality of life (QOL) and quality of care (QOC) concerns 56


57 Person-Centered Care Heart of the RAI Process Survey Focus 57
58 Person-Centered Care Person-centered care means the facility focuses on the resident as the center of control, and supports each resident in making his or her own choices Person-centered care includes making an effort to understand what each resident is communicating, verbally and nonverbally, identifying what is important to each resident with regard to daily routines and preferred activities, and having an understanding of the resident s life before coming to reside in the nursing home 58
59 F Comprehensive Person-Centered Care Planning Baseline Care Plan Comprehensive Care Plan 59
60 Baseline Care Plan (a)(1) The facility must develop and implement a baseline care plan for each resident that includes the instructions needed to provide effective and person-centered care of the resident that meet professional standards of quality care. The baseline care plan must: (i) Be developed within 48 hours of a resident s admission (ii) Include the minimum healthcare information necessary to properly care for a resident including, but not limited to: (A) Initial goals based on admission orders (B) Physician orders (C) Dietary orders (D) Therapy services (E) Social services (F) PASARR recommendation, if applicable 60
61 Baseline Care Plan The baseline care plan must include the minimum healthcare information necessary to properly care for each resident immediately upon their admission, which would address resident-specific health and safety concerns to prevent decline or injury, such as elopement or fall risk, and would identify needs for supervision, behavioral interventions, and assistance with activities of daily living, as necessary 61
62 Content of Baseline CP The baseline care plan must reflect the resident s stated goals and objectives, and include interventions that address his/her current needs. It must be based on the admission orders, information about the resident available from the transferring provider, and discussion with the resident and resident representative, if applicable Because the baseline care plan documents the interim approaches for meeting the resident s immediate needs, professional standards of quality care would dictate that it must also reflect changes to approaches, as necessary, resulting from significant changes in condition or needs, occurring prior to development of the comprehensive care plan Facility staff must implement the interventions to assist the resident to achieve care plan goals and objectives 62
63 Intent Completion and implementation of the baseline care plan within 48 hours of a resident s admission is intended to promote continuity of care and communication among nursing home staff, increase resident safety, and safeguard against adverse events that are most likely to occur right after admission; and to ensure the resident and representative, if applicable, are informed of the initial plan for delivery of care and services by receiving a written summary of the baseline care plan. 63
64 Guidance to Surveyors Nursing homes are required to develop a baseline care plan within the first 48 hours of admission which provides instructions for the provision of effective and person-centered care to each resident. This means that the baseline care plan should strike a balance between conditions and risks affecting the resident s health and safety, and what is important to him or her, within the limitations of the baseline care plan timeframe. 64
65 Baseline Care Plan Summary (a)(3) The facility must provide the resident and the representative, if applicable with a written summary of the baseline care plan by completion of the comprehensive care plan. The summary must be in a language and conveyed in a manner the resident and/or representative can understand. Summary must include: o Initial goals for the resident; o A list of current medications and dietary instructions, and o Services and treatments to be administered by the facility and personnel acting on behalf of the facility; The format and location of the summary is at the facility s discretion, however, the medical record must contain evidence that summary was given to the resident and resident representative, if applicable. Facility may choose to provide a copy of the baseline care plan itself as the summary, if it meets all of the summary requirements 65
66 What Might the Summary Look Like? Summaries have become common at discharge from the hospital, or after visits to an Urgent Care or physician s office Must be in plain language not medical terminology 66
67 Preparation Talk to your facility s software vendor. Are they planning to develop a template to pull the physician orders, diet orders and medications into a summary format? Build a simple template: Physician s orders Medications: list of and what to watch for Treatments Resident goals 67
68 Involve the Resident/Representative Ask the resident about their goals for their care What is their discharge plan? What is important to them while receiving care during this stay? What would they like us to know about them? 68
69 Care Plan vs. Summary The actual baseline care plan (due with 48 hours) may be in a format other than a summary format The resident should be given a summary or the actual baseline care plan if the actual care plan is in a format that is easily understandable to the resident/representative 69
70 F657 Comprehensive Care Plans (b) Comprehensive Care Plans (b)(2) A comprehensive care plan must be (i) Developed within 7 days after completion of the comprehensive assessment (ii) Prepared by an IDT, that includes but is not limited to: A. The attending physician B. A registered nurse with responsibility for the resident C. A nurse aide with responsibility for the resident D. A member of food and nutrition services staff E. To the extent practicable, the participation of the resident and the resident's representative(s). An explanation must be included in a resident s medical record if the participation of the resident and their resident representative is determined not practicable for the development of the resident s care plan F. Other appropriate staff or professionals in disciplines as determined by the resident's needs or as requested by the resident (iii) Reviewed and revised by the interdisciplinary team after each assessment, including both the comprehensive and quarterly review assessments 70
71 Interdisciplinary Interdisciplinary means that professional disciplines, as appropriate, will work together to provide the greatest benefit to the resident. It does not mean that every goal must have an interdisciplinary approach. The mechanics of how the interdisciplinary team (IDT) meets its responsibilities in developing an interdisciplinary care plan (e.g., a face-to-face meeting, teleconference, written communication) is at the discretion of the facility. In instances where an IDT member participates in care plan development, review or revision via written communication, the written communication in the medical record must reflect involvement of the resident and resident representative, if applicable, and other members of the IDT, as appropriate. 71

72 Resident s Rights in Care Planning Each resident has the right to participate in choosing treatment options and must be given the opportunity to participate in the development, review and revision of his/her care plan. Residents also have the right to refuse treatment. 72
73 Notices of Care Plan Conferences The facility must provide the resident and resident representative, if applicable with advance notice of care planning conferences to enable resident/resident representative participation. Resident and resident representative participation in care planning can be accomplished in many forms such as holding care planning conferences at a time the resident representative is available to participate, holding conference calls or video conferencing. 73
74 Documentation When Resident Not Capable Facilities are expected to facilitate the residents and if applicable, the resident representatives participation in the care planning process. There are limited circumstances in which the inclusion of the resident and/or resident representative may not be practicable (or feasible). An example may be the case of a severely cognitively impaired resident who is unable to understand or participate in care plan development, and the resident s representative does not respond to facility attempts to make contact. If the facility determines that the inclusion of the resident and/or resident representative is not practicable, documentation of the reasons, including the steps the facility took to include the resident and/or resident representative, must be included in the medical record. 74
75 Surveyor Probes Related to Care Plans Was a comprehensive plan of care developed within seven days of completion of the resident s comprehensive assessment? Is there evidence of participation in the care planning process by required IDT members? Ask required members of the IDT how they participate in the development, review and revision of care plans. Based on the resident s goals and needs, were other appropriate staff or professionals expertise utilized to develop a plan to improve the resident s functional abilities? Ask the resident and resident representative, if applicable if he or she actively participates in the care planning process? If not, what have been the barriers to participation? Ask the resident and if applicable, the resident representative if he or she has requested the participation of additional individuals care planning process. If so, was the request respected? 75
76 Successfully Completing the RAI Process Will Lead to: Resident-Centered Care Better resident outcomes Happier residents, families and staff. (When the residents participate in care planning and know that their voices have been heard, the residents are happier. When residents are happy, families are happy. When residents and families are happy, the staff is happy.) 76


77 You and Your Work are Very Important! 77


78 Questions? 78
NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017
 NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017 Disclaimer: The information contained in this presentation is representative of the current information provided
NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017 Disclaimer: The information contained in this presentation is representative of the current information provided
This presentation will be updated as new information becomes available.
 New Long Term Care Survey Process 1 Disclaimer The information provided within these slides are current as of May 15,2017. It provides information related to the CMS' intent to implement the survey process
New Long Term Care Survey Process 1 Disclaimer The information provided within these slides are current as of May 15,2017. It provides information related to the CMS' intent to implement the survey process
This presentation will be updated as new information becomes available.
 New Long Term Care Survey Process Disclaimer The information provided within these slides are current as of May 15,2017. It provides information related to the CMS' intent to implement the survey process
New Long Term Care Survey Process Disclaimer The information provided within these slides are current as of May 15,2017. It provides information related to the CMS' intent to implement the survey process
New Long Term Care Survey Process
 New Long Term Care Survey Process Disclaimer The information provided within these slides are current as of May 15,2017. It provides information related to the CMS' intent to implement the survey process
New Long Term Care Survey Process Disclaimer The information provided within these slides are current as of May 15,2017. It provides information related to the CMS' intent to implement the survey process
BLENDED SURVEY PROCESS
 BLENDED SURVEY PROCESS UPDATE OF LESSONS LEARNED UNDER THE NEW SURVEY PROCESS KATHY CREEGAN-TEDESCHI DIRECTOR LTC VDH APRIL PAYNE, LNHA VP OF QUALITY IMPROVEMENT & DIRECTOR OF VCAL VHCA-VCAL NEW LONG TERM
BLENDED SURVEY PROCESS UPDATE OF LESSONS LEARNED UNDER THE NEW SURVEY PROCESS KATHY CREEGAN-TEDESCHI DIRECTOR LTC VDH APRIL PAYNE, LNHA VP OF QUALITY IMPROVEMENT & DIRECTOR OF VCAL VHCA-VCAL NEW LONG TERM
CMS RAI MANUAL ERRATA DOCUMENT
 CMS RAI MANUAL ERRATA DOCUMENT SECTION I UTI S In Chapter 3, page I-9, under Coding Tips in I: Active Diagnoses in the Last 7 Days, a third bullet has been added: If the diagnosis of UTI was made prior
CMS RAI MANUAL ERRATA DOCUMENT SECTION I UTI S In Chapter 3, page I-9, under Coding Tips in I: Active Diagnoses in the Last 7 Days, a third bullet has been added: If the diagnosis of UTI was made prior
The New Survey Process What To Expect Paula G. Sanders, Esq.
 PHCA Webinar February 14, 2018 The New Survey Process What To Expect Paula G. Sanders, Esq. DEPARTMENT OF HEALTH ENFORCEMENT TRENDS How to Read State Tags DOH CMPs Per Year 2014-2017 2014 $79,250.00 2015
PHCA Webinar February 14, 2018 The New Survey Process What To Expect Paula G. Sanders, Esq. DEPARTMENT OF HEALTH ENFORCEMENT TRENDS How to Read State Tags DOH CMPs Per Year 2014-2017 2014 $79,250.00 2015
Final Rule to Reform the Requirements for Long-Term Care Facilities
 Final Rule to Reform the Requirements for Long-Term Care Facilities Karen Tritz Division of Nursing Homes Director Clinical Standards Group Long-Term Care Team Survey & Certification Group Division of
Final Rule to Reform the Requirements for Long-Term Care Facilities Karen Tritz Division of Nursing Homes Director Clinical Standards Group Long-Term Care Team Survey & Certification Group Division of
SECTION P: RESTRAINTS
 SECTION P: RESTRAINTS Intent: The intent of this section is to record the frequency over the 7-day look-back period that the resident was restrained by any of the listed devices at any time during the
SECTION P: RESTRAINTS Intent: The intent of this section is to record the frequency over the 7-day look-back period that the resident was restrained by any of the listed devices at any time during the
Highlights of the New LTCSP and Regulations
 Highlights of the New LTCSP and Regulations New York State Department of Health Division of Nursing Homes and ICF/IID Surveillance November 15, 2017 November 15, 2017 2 Resources https://www.cms.gov/medicare/provider-enrollment-andcertification/guidanceforlawsandregulations/nursinghomes.html
Highlights of the New LTCSP and Regulations New York State Department of Health Division of Nursing Homes and ICF/IID Surveillance November 15, 2017 November 15, 2017 2 Resources https://www.cms.gov/medicare/provider-enrollment-andcertification/guidanceforlawsandregulations/nursinghomes.html
Federal Requirements of Participation for Nursing Homes Summary of Key Changes in the Final Rule Issued September 2016 Phase 2
 Federal Requirements of Participation for Nursing Homes Summary of Key Changes in the Final Rule Issued September 2016 Phase 2 On September 28, 2016, the Centers for Medicare & Medicaid Services (CMS)
Federal Requirements of Participation for Nursing Homes Summary of Key Changes in the Final Rule Issued September 2016 Phase 2 On September 28, 2016, the Centers for Medicare & Medicaid Services (CMS)
Frequently Asked Questions Related to Long Term Care Regulations, Survey Process, and Training
 Related to Long Term Care Regulations, Survey Process, and Training Updated 01/12/2018 Table of Contents A. 483.10 Resident Rights... 1 B. 483.12 Freedom from Abuse, Neglect, and Exploitation... 1 Reporting
Related to Long Term Care Regulations, Survey Process, and Training Updated 01/12/2018 Table of Contents A. 483.10 Resident Rights... 1 B. 483.12 Freedom from Abuse, Neglect, and Exploitation... 1 Reporting
Resident Rights in Nursing Facilities
 Your Guide to Resident Rights in Nursing Facilities 1-800-499-0229 1 Table of Contents The Ombudsman Advocate...3 You Take Your Rights with You...4 Federal Regulations Protect You...5 Medical Assessment
Your Guide to Resident Rights in Nursing Facilities 1-800-499-0229 1 Table of Contents The Ombudsman Advocate...3 You Take Your Rights with You...4 Federal Regulations Protect You...5 Medical Assessment
Overview of the New Long-Term Care Survey Process FOR LONG-TERM CARE (LTC) PROVIDERS
 PROVIDERS") Overview of the New Long-Term Care Survey Process FOR LONG-TERM CARE (LTC) PROVIDERS Navigation To Start the training, please press Function + F5 To advance through each slide use the icon located at the
Overview of the New Long-Term Care Survey Process FOR LONG-TERM CARE (LTC) PROVIDERS Navigation To Start the training, please press Function + F5 To advance through each slide use the icon located at the
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care
 Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
MDS Essentials. MDS Essentials: Content. Faculty Disclosures 5/22/2017. Educational Activity Completion
 MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
What to Expect on Your Next Survey
 What to Expect on Your Next Survey Linda M. Elizaitis RN, BS, RAC-CT President CMS Compliance Group, Inc. E. lmelizaitis@cmscg.net T. 631.692.4422 cmscompliancegroup.com @lindaelizaitis @cmscompliance
What to Expect on Your Next Survey Linda M. Elizaitis RN, BS, RAC-CT President CMS Compliance Group, Inc. E. lmelizaitis@cmscg.net T. 631.692.4422 cmscompliancegroup.com @lindaelizaitis @cmscompliance
WhWwhaht. SNF CMS, RoP, Survey, and Regulatory Update October /25/2017. The New and Improved Survey Process
 303 Cleveland Avenue SE Suite 206 Tumwater, WA 98501 Tel 800 562 6170 www.whca.org SNF CMS, RoP, Survey, and Regulatory Update October 2017 Elena Madrid Director of Regulatory Affairs The New and Improved
303 Cleveland Avenue SE Suite 206 Tumwater, WA 98501 Tel 800 562 6170 www.whca.org SNF CMS, RoP, Survey, and Regulatory Update October 2017 Elena Madrid Director of Regulatory Affairs The New and Improved
The RoPs are here! Do you know what s changing?
 The RoPs are here! Do you know what s changing? Mary Madison, RN, RAC-CT, CDP Clinical Consultant, LTC/Senior Care Briggs Healthcare March 7, 2017 2 What we ll cover today CMS goals behind the updated
The RoPs are here! Do you know what s changing? Mary Madison, RN, RAC-CT, CDP Clinical Consultant, LTC/Senior Care Briggs Healthcare March 7, 2017 2 What we ll cover today CMS goals behind the updated
Center for Clinical Standards and Quality/Survey & Certification Group
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
Prepublication Requirements
 Prepublication Requirements Standards Revisions for Swing Bed Final Rule in Critical Access Hospitals The Joint Commission has approved the following revisions for prepublication. While revised requirements
Prepublication Requirements Standards Revisions for Swing Bed Final Rule in Critical Access Hospitals The Joint Commission has approved the following revisions for prepublication. While revised requirements
Get Ready for Phase 1 of the New Requirements of Participation
 Pennsylvania Health Care Association November 7, 2016 Get Ready for Phase 1 of the New Requirements of Participation Paula G. Sanders, Esquire Post & Schell, P.C. Gail Weidman Dawn Murr-Davidson Pennsylvania
Pennsylvania Health Care Association November 7, 2016 Get Ready for Phase 1 of the New Requirements of Participation Paula G. Sanders, Esquire Post & Schell, P.C. Gail Weidman Dawn Murr-Davidson Pennsylvania
2/28/2018. Marilyn Mines RN, BC, RAC CT
 Illinois Council on Long Term Care HealthCare Council of Illinois The New Long Term Care Survey Process March 1, 2018 marcumllp.com Marilyn Mines RN, BC, RAC CT Marcum LLP Nine Parkway North Deerfield,
Illinois Council on Long Term Care HealthCare Council of Illinois The New Long Term Care Survey Process March 1, 2018 marcumllp.com Marilyn Mines RN, BC, RAC CT Marcum LLP Nine Parkway North Deerfield,
The QIS was designed to achieve several objectives:
 CMS Quality Indicator Survey, ASE-Q The Quality Indicator Survey CMS is implementing the Quality Indicator Survey (QIS) which is a computer assisted long term care survey process used by selected State
CMS Quality Indicator Survey, ASE-Q The Quality Indicator Survey CMS is implementing the Quality Indicator Survey (QIS) which is a computer assisted long term care survey process used by selected State
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
The Updated CMS Nursing Facility Regulations
 The Updated CMS Nursing Facility Regulations NHELP Conference December 5, 2016 Lori Smetanka, Consumer Voice Toby Edelman, Center for Medicare Advocacy Objectives Understand the important changes made
The Updated CMS Nursing Facility Regulations NHELP Conference December 5, 2016 Lori Smetanka, Consumer Voice Toby Edelman, Center for Medicare Advocacy Objectives Understand the important changes made
Hospice and End of Life Care and Services Critical Element Pathway
 Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
PACAH 2018 SPRING CONFERENCE April 26, 2018
 PACAH 2018 SPRING CONFERENCE April 26, 2018 Presented by Tanya Daniels Harris, Esq. 2018 LATSHA DAVIS & McKENNA, P.C. 2 OVERVIEW OF RECENT SURVEY AND ENFORCEMENT ISSUES Performance Audit of DOH Regulation
PACAH 2018 SPRING CONFERENCE April 26, 2018 Presented by Tanya Daniels Harris, Esq. 2018 LATSHA DAVIS & McKENNA, P.C. 2 OVERVIEW OF RECENT SURVEY AND ENFORCEMENT ISSUES Performance Audit of DOH Regulation
Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities Proposed Rule
 Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities Proposed Rule Summary of Major Provisions Summary adapted from Proposed Rule (with AHCA Comments) July 14, 2015 Updates
Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities Proposed Rule Summary of Major Provisions Summary adapted from Proposed Rule (with AHCA Comments) July 14, 2015 Updates
Rules of Participation, Phase 1 Review
 1 Rules of Participation, Phase 1 Review A Foundation check to launch Phase 2 from Presented by: Anabelle Locsin, RN, Ed.D., RAC-CT, LNC Quality Improvement Consultant PROGRAM OVERVIEW 2 This program was
1 Rules of Participation, Phase 1 Review A Foundation check to launch Phase 2 from Presented by: Anabelle Locsin, RN, Ed.D., RAC-CT, LNC Quality Improvement Consultant PROGRAM OVERVIEW 2 This program was
RALF Behavior Management Rules IDAPA
 RALF Behavior Management Rules IDAPA 16.03.22 DEFINITIONS: 010.10. Assessment. The conclusion reached using uniform criteria which identifies resident strengths, weaknesses, risks and needs, to include
RALF Behavior Management Rules IDAPA 16.03.22 DEFINITIONS: 010.10. Assessment. The conclusion reached using uniform criteria which identifies resident strengths, weaknesses, risks and needs, to include
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT
 A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
CMS Updates RAI User s Manual
 CMS Updates RAI User s Manual By Rena R. Shephard, MHA, RN, RAC MT, C NE AANAC Executive Editor The Centers for Medicare & Medicaid Services (CMS) June 2 posted revisions to the Long Term Care Facility
CMS Updates RAI User s Manual By Rena R. Shephard, MHA, RN, RAC MT, C NE AANAC Executive Editor The Centers for Medicare & Medicaid Services (CMS) June 2 posted revisions to the Long Term Care Facility
Phase 2: 4/24/2017. Implementation Phases. Objectives. Phase 1: November 28, Phase 3: November 28, 2019
 NEW Requirements for Participation for Skilled Nursing Facilities The Elements of Compliance for Phase 2 April 28, 2017 1:30pm 2:45pm Objectives Identify the new and revised regulations in the Final Rule
NEW Requirements for Participation for Skilled Nursing Facilities The Elements of Compliance for Phase 2 April 28, 2017 1:30pm 2:45pm Objectives Identify the new and revised regulations in the Final Rule
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT
 Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
Pharmacy Services. Division of Nursing Homes
 Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Initial Pool Process: Resident Interview
 Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW
 CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-242-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-242-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
Hospice Care in the Nursing Home: The New Interpretive Guidelines for NF Surveyors
 Hospice Care in the Nursing Home: The New Interpretive Guidelines for NF Surveyors Subscriber Webinar The Plan 1. Brief Look: The Hospice Nursing Home Partnership 2. Brief Look: The Nursing Home Survey
Hospice Care in the Nursing Home: The New Interpretive Guidelines for NF Surveyors Subscriber Webinar The Plan 1. Brief Look: The Hospice Nursing Home Partnership 2. Brief Look: The Nursing Home Survey
Objectives. The New Long Term Care Survey Process 9/5/2018 THE NEW SURVEY PROCESS- LESSONS LEARNED
 Objectives THE NEW SURVEY PROCESS- LESSONS LEARNED Presenter: Shelly Maffia, MSN, MBA, RN, NHA, QCP Director of Regulatory Services Identify significant differences between old and new survey process Describe
Objectives THE NEW SURVEY PROCESS- LESSONS LEARNED Presenter: Shelly Maffia, MSN, MBA, RN, NHA, QCP Director of Regulatory Services Identify significant differences between old and new survey process Describe
Find Your Purpose with the Phase 2 Regulations!
 Find Your Purpose with the Phase 2 Regulations! The New MegaRule! MONTANA HOSPITAL ASSOCIATION OVERVIEW OF PHASE 2 REQUIREMENTS WWW.PATHWAYHEALTH.COM Objectives Understand the new and revised final rule
Find Your Purpose with the Phase 2 Regulations! The New MegaRule! MONTANA HOSPITAL ASSOCIATION OVERVIEW OF PHASE 2 REQUIREMENTS WWW.PATHWAYHEALTH.COM Objectives Understand the new and revised final rule
Observations for all areas: What type of supervision is provided to the resident and by whom? How are care-planned interventions implemented?
 Use this pathway for a resident who requires supervision and/or assistive devices to prevent accidents and to ensure the environment is free from accident hazards as is possible. Review the Following in
Use this pathway for a resident who requires supervision and/or assistive devices to prevent accidents and to ensure the environment is free from accident hazards as is possible. Review the Following in
CMS PROPOSED REVISIONS OF THE NURSING HOME REGULATIONS
 We are almost done here for the day! CMS PROPOSED REVISIONS OF THE NURSING HOME REGULATIONS SNF Regulatory Day September 17, 2015 CMS s Major Initiatives Reduce unnecessary readmissions Reduce Healthcare
We are almost done here for the day! CMS PROPOSED REVISIONS OF THE NURSING HOME REGULATIONS SNF Regulatory Day September 17, 2015 CMS s Major Initiatives Reduce unnecessary readmissions Reduce Healthcare
AANAC Education Advancement. MDS Essentials: An Introduction. Learning Objectives 3/22/2017. Education Advancement
 AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
MDS 3.0: What Leadership Needs to Know
 MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
Survey Protocol for Long Term Care Facilities
 Attachment B Survey Protocol for Long Term Care Facilities The provision of home dialysis treatments in a Long Term Care (LTC) facility place an increased burden on the LTC facility staff and may place
Attachment B Survey Protocol for Long Term Care Facilities The provision of home dialysis treatments in a Long Term Care (LTC) facility place an increased burden on the LTC facility staff and may place
Requirements for Successful Completion
 Faculty Disclosure I have no financial relationships to disclose I have no conflicts of interests to disclose I will not promote any commercial products or services 2 Requirements for Successful Completion
Faculty Disclosure I have no financial relationships to disclose I have no conflicts of interests to disclose I will not promote any commercial products or services 2 Requirements for Successful Completion
Session #8. The Key to Preventing Immediate Jeopardies. Speaker: Janine Lehman 4/17/2013 KBN:
 2013 KAHCF Spring Education Conference Session #8 The Key to Preventing Immediate Jeopardies Speaker: Janine Lehman 4/17/2013 KBN: 5-0002-707-041-1217 The Key to Preventing Immediate Jeopardies Janine
2013 KAHCF Spring Education Conference Session #8 The Key to Preventing Immediate Jeopardies Speaker: Janine Lehman 4/17/2013 KBN: 5-0002-707-041-1217 The Key to Preventing Immediate Jeopardies Janine
We use many of them. The devices are part of our restraint policy. See below
 Do you utilize body pillow, beveled mattresses, moxi mattresses, rolled blankets, swim noodles for positioning or bed demarcation? Do you have a comprehensive device assessment? If so, would you please
Do you utilize body pillow, beveled mattresses, moxi mattresses, rolled blankets, swim noodles for positioning or bed demarcation? Do you have a comprehensive device assessment? If so, would you please
Reviewing regulatory requirements for top ten federal Nursing Home Tags issued in Minnesota. Eva Loch, MDH Nursing Evaluator
 Reviewing regulatory requirements for top ten federal Nursing Home Tags issued in Minnesota. Eva Loch, MDH Nursing Evaluator F282- Comprehensive Care Plans Regulatory language (SOM): 483.21(b)(3) Comprehensive
Reviewing regulatory requirements for top ten federal Nursing Home Tags issued in Minnesota. Eva Loch, MDH Nursing Evaluator F282- Comprehensive Care Plans Regulatory language (SOM): 483.21(b)(3) Comprehensive
CMS Mega Rule: Implications for Pharmacists and Pharmacies
 CMS Mega Rule: Implications for Pharmacists and Pharmacies Curt Wood, RPh, BCGP, FASCP Disclosure and Conflict of Interest Curt Wood declares no conflicts of interest, real or apparent, and no financial
CMS Mega Rule: Implications for Pharmacists and Pharmacies Curt Wood, RPh, BCGP, FASCP Disclosure and Conflict of Interest Curt Wood declares no conflicts of interest, real or apparent, and no financial
3/27/2017. SNF Requirements for Participation. Objectives. New Rules to Live By RoP Changes for 2017 and Beyond Sunday, April 2, :30 5:30pm
 Disclosure of Commercial Interest Commercial Interest Employed by a consulting organization Name of Employer Pathway Health, Inc. Title Director of Quality and Government Services Description Pathway Health
Disclosure of Commercial Interest Commercial Interest Employed by a consulting organization Name of Employer Pathway Health, Inc. Title Director of Quality and Government Services Description Pathway Health
National Regulatory Overview. Lyn Bentley, Vice President Quality & Regulatory Affairs September 19, 2018
 National Regulatory Overview Lyn Bentley, Vice President Quality & Regulatory Affairs September 19, 2018 Topics The new survey process obe prepared Frequently cited tags onation oregion VII onebraska Compliance
National Regulatory Overview Lyn Bentley, Vice President Quality & Regulatory Affairs September 19, 2018 Topics The new survey process obe prepared Frequently cited tags onation oregion VII onebraska Compliance
Medication Related Changes Phase 1&2
 Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
CMS REVISED RULES OF PARTICIPATION
 CMS REVISED RULES OF PARTICIPATION Webinar #3 December 1, 2016 Rebecca J. Bartle, RN, MSN, HFA Hoosier Owners and Providers for the Elderly Ref: S&C 17-07-NH (11/9/16) Centers for Medicare and Medicaid
CMS REVISED RULES OF PARTICIPATION Webinar #3 December 1, 2016 Rebecca J. Bartle, RN, MSN, HFA Hoosier Owners and Providers for the Elderly Ref: S&C 17-07-NH (11/9/16) Centers for Medicare and Medicaid
An Overview of the new LTCF Requirements of Participation: Are You Ready?
 An Overview of the new LTCF Requirements of Participation: Are You Ready? David Gifford MD MPH Sr VP for Quality & Regulatory Affairs Feb 9 th 2017 3:15 pm 4:45 pm Boise ID CMS Changes to SNF Regs New
An Overview of the new LTCF Requirements of Participation: Are You Ready? David Gifford MD MPH Sr VP for Quality & Regulatory Affairs Feb 9 th 2017 3:15 pm 4:45 pm Boise ID CMS Changes to SNF Regs New
Agenda: Noon Overview of the regulatory sections affected by the Reform of RoP in Phase 2
 Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
New Strategies for Managing Medicare Risk
 New Strategies for Managing Medicare Risk John Sheridan, MHSA, FACHE President, ehealth Data Solutions Keith Knapp, PhD, CFACHCA CEO, Christian Care Communities 1001. Survey and Certification Phase II
New Strategies for Managing Medicare Risk John Sheridan, MHSA, FACHE President, ehealth Data Solutions Keith Knapp, PhD, CFACHCA CEO, Christian Care Communities 1001. Survey and Certification Phase II
BASELINE & P ERSON- CENTERED C ARE P LANS
 BASELINE & P ERSON- CENTERED C ARE P LANS INTENT Promote continuity of care Communication among nursing home staff Increase resident safety Safeguard against adverse events that are most likely to occur
BASELINE & P ERSON- CENTERED C ARE P LANS INTENT Promote continuity of care Communication among nursing home staff Increase resident safety Safeguard against adverse events that are most likely to occur
The Changing Role of Physicians in LTCF
 The Changing Role of Physicians in LTCF David Gifford MD MPH Boise ID Feb 9 th, 2017 CMS Changes to SNF Regs New rule makes extensive changes to SNF Requirements of Participation (RoP) Last major update
The Changing Role of Physicians in LTCF David Gifford MD MPH Boise ID Feb 9 th, 2017 CMS Changes to SNF Regs New rule makes extensive changes to SNF Requirements of Participation (RoP) Last major update
Facility Name/CCN: Survey Date: Preceptor Name: Surveyor Name: New Surveyor Observational Survey Guidelines Long-Term Care
 Directions: This document is intended to be used as a list of reminders for a preceptor when preparing a new surveyor for a survey, while on a survey, or serving as a preceptor. Place a check mark in the
Directions: This document is intended to be used as a list of reminders for a preceptor when preparing a new surveyor for a survey, while on a survey, or serving as a preceptor. Place a check mark in the
Caring in the Carolinas 11/5/2016
 The Mega Rule: Reform of Requirements for Long- Term Care Facilities Robert Smith, Pharm D, BCPS, CGP, FASCP Director of Clinical Services Neil Medical Group Disclosures I have no conflicts of interest
The Mega Rule: Reform of Requirements for Long- Term Care Facilities Robert Smith, Pharm D, BCPS, CGP, FASCP Director of Clinical Services Neil Medical Group Disclosures I have no conflicts of interest
Get Ready for Phase 1 of the New Requirements of Participation
 PADONA Convention March 30, 2017 Get Ready for Phase 1 of the New Requirements of Participation Paula G. Sanders, Esquire New Requirements of Participation (RoPs) Published October 4, 2016 (81 Fed. Reg.
PADONA Convention March 30, 2017 Get Ready for Phase 1 of the New Requirements of Participation Paula G. Sanders, Esquire New Requirements of Participation (RoPs) Published October 4, 2016 (81 Fed. Reg.
4/3/2018. Nursing Facility Changes to Conditions of Participation (& Enforcement): What You Need to Know. Revisions to State Operations Manual
: What You Need to Know. Revisions to State Operations Manual") DAVIS, BROWN, KOEHN, SHORS & ROBERTS, 1P.C. Nursing Facility Changes to Conditions of Participation (& Enforcement): What You Need to Know Lynn Böes and Ken Watkins 2 Revisions to State Operations Manual
DAVIS, BROWN, KOEHN, SHORS & ROBERTS, 1P.C. Nursing Facility Changes to Conditions of Participation (& Enforcement): What You Need to Know Lynn Böes and Ken Watkins 2 Revisions to State Operations Manual
11/23/2011. Proactive vs. Reactive Relationship
 Overview Focus on Resident Voice Assessment Schedule EOT OMRA and New Resumption Items New PPS Assessment: COT OMRA CMS Clarifications Coding New Quality Measures Draft MDS and Care Planning as Risk Management
Overview Focus on Resident Voice Assessment Schedule EOT OMRA and New Resumption Items New PPS Assessment: COT OMRA CMS Clarifications Coding New Quality Measures Draft MDS and Care Planning as Risk Management
Nursing Assistant
 Western Technical College 30543300 Nursing Assistant Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 The course prepares individuals for employment
Western Technical College 30543300 Nursing Assistant Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 The course prepares individuals for employment
Goodbye Grace Period. What will be expected from your Facility Assessment in the Coming Year. Ellen Kuebrich Chief Strategy Officer, Providigm
 Goodbye Grace Period What will be expected from your Facility Assessment in the Coming Year Ellen Kuebrich Chief Strategy Officer, Providigm Final Rule Final Rule Effective Date These regulations are effective
Goodbye Grace Period What will be expected from your Facility Assessment in the Coming Year Ellen Kuebrich Chief Strategy Officer, Providigm Final Rule Final Rule Effective Date These regulations are effective
3/6/2017. CMS nursing home requirements have not been comprehensively updated since 1991 despite significant changes in the industry.
 Debra Brown, PharmD Pharmaceutical Consultant II Specialist Licensing and Certification QCHF/CAHF Spring Legislative Conference March 2017 1 Describe impact of 2016 CMS Final Rule on SNF pharmacy services
Debra Brown, PharmD Pharmaceutical Consultant II Specialist Licensing and Certification QCHF/CAHF Spring Legislative Conference March 2017 1 Describe impact of 2016 CMS Final Rule on SNF pharmacy services
A SYSTEMS APPROACH TO SURVEY PREPARATION
 4/15/2015 A SYSTEMS APPROACH TO SURVEY PREPARATION Laying a Strong Foundation Demi Haffenreffer, RN MBA Email: demi@consultdemi.net Phone: 1-800-7336590 Survey Preparation Overall Year round systems and
4/15/2015 A SYSTEMS APPROACH TO SURVEY PREPARATION Laying a Strong Foundation Demi Haffenreffer, RN MBA Email: demi@consultdemi.net Phone: 1-800-7336590 Survey Preparation Overall Year round systems and
Upcoming Seminars for the Illinois Health Care Association and the Illinois Council on Long Term Care
 February 8, 2011 Number 47 Upcoming Seminars for the Illinois Health Care Association and the Illinois Council on Long Term Care Seminars included in this issue: MDS 3.0 RAC-CT Certification and Recertification
February 8, 2011 Number 47 Upcoming Seminars for the Illinois Health Care Association and the Illinois Council on Long Term Care Seminars included in this issue: MDS 3.0 RAC-CT Certification and Recertification
5/1/2017 THE BEST DEFENSE IS A GOOD OFFENSE OBJECTIVES. Preparing for a Home Health Medicare Recertification Survey
 THE BEST DEFENSE IS A GOOD OFFENSE Preparing for a Home Health Medicare Recertification Survey OBJECTIVES To gain an understanding how the Medicare Conditions of Participation (CoPs), the individual G-tags,
THE BEST DEFENSE IS A GOOD OFFENSE Preparing for a Home Health Medicare Recertification Survey OBJECTIVES To gain an understanding how the Medicare Conditions of Participation (CoPs), the individual G-tags,
Leveraging Your Facility s 5 Star Analysis to Improve Quality
 Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
MDS 3.0/RUG IV Distance Learning Series January - May 2016
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 ROUTE TO: _Administrator; _MDS Coordinator; _Director of Nursing; _Director of Accounting; _Director of Social Services; _Director of Activities;
MDS 3.0/RUG IV Distance Learning Series January - May 2016 ROUTE TO: _Administrator; _MDS Coordinator; _Director of Nursing; _Director of Accounting; _Director of Social Services; _Director of Activities;
Georgia. Phone. Agency Georgia Department of Community Health, Healthcare Facility Regulation Division (404)
") Georgia Agency Georgia Department of Community Health, Healthcare Facility Regulation Division (404) 657-5850 Contact Elaine Wright (404) 657-5856 E-mail ehwright@dch.ga.gov Phone Web Site http://dch.georgia.gov/healthcare-facility-regulation-0
Georgia Agency Georgia Department of Community Health, Healthcare Facility Regulation Division (404) 657-5850 Contact Elaine Wright (404) 657-5856 E-mail ehwright@dch.ga.gov Phone Web Site http://dch.georgia.gov/healthcare-facility-regulation-0
Countdown to MDS Section GG: Collaboration Between Nursing and Therapy
 Countdown to MDS Section GG: Collaboration Between Nursing and Therapy Presented in Collaboration with NASL: Joanne M. Wisely, MA CCC/SLP, VP Legislative Advocacy Genesis Rehab Services/Respiratory Health
Countdown to MDS Section GG: Collaboration Between Nursing and Therapy Presented in Collaboration with NASL: Joanne M. Wisely, MA CCC/SLP, VP Legislative Advocacy Genesis Rehab Services/Respiratory Health
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
The QIS Survey Process: How to Prepare
 The QIS Survey Process: How to Prepare Faculty: Diane Atchinson, RN- BC, MSN, ANP DPA Associates, Inc Kansas City, MO 800-245-0372 E mail: diane@dpaassociates.com Access the QIS manual KDOA web site License
The QIS Survey Process: How to Prepare Faculty: Diane Atchinson, RN- BC, MSN, ANP DPA Associates, Inc Kansas City, MO 800-245-0372 E mail: diane@dpaassociates.com Access the QIS manual KDOA web site License
F-TAG 675 QUALITY OF LIFE
 F-TAG 675 QUALITY OF LIFE Quality of life is a fundamental principle that applies to all care and services provided to facility residents. Each resident must receive and the facility must provide the necessary
F-TAG 675 QUALITY OF LIFE Quality of life is a fundamental principle that applies to all care and services provided to facility residents. Each resident must receive and the facility must provide the necessary
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care
 Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
North Carolina. Phone. Agency (919) Department of Health and Human Services, Division of Health Service Regulation
 Department of Health and Human Services, Division of Health Service Regulation") North Carolina Agency Department of Health and Human Services, Division of Health Service Regulation (919) 855-3765 Contact Doug Barrick (919) 855-3778 E-mail doug.barrick@dhhs.nc.gov Phone Web Site http://ncdhhs.gov/dhsr/acls
North Carolina Agency Department of Health and Human Services, Division of Health Service Regulation (919) 855-3765 Contact Doug Barrick (919) 855-3778 E-mail doug.barrick@dhhs.nc.gov Phone Web Site http://ncdhhs.gov/dhsr/acls
2014 AANAC 9_30_ AANA C AANA
 2013 2014 AANAC AANAC 9_30_14 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT Requirements for Successful Completion 1 Contact hour will be awarded for this continuing
2013 2014 AANAC AANAC 9_30_14 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT Requirements for Successful Completion 1 Contact hour will be awarded for this continuing
(a) Licensure. A facility must be licensed under applicable State and local law.
 Licensure. A facility must be licensed under applicable State and local law.") 42 C.F.R. 483.705. Administration. A facility must be administered in a manner that enables it to use its resources effectively and efficiently to attain or maintain the highest practicable physical, mental,
42 C.F.R. 483.705. Administration. A facility must be administered in a manner that enables it to use its resources effectively and efficiently to attain or maintain the highest practicable physical, mental,
New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert-
 New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert- Rodney Farley, CHC Terry Raser, RN, RAC-CT, C-NE LW Consulting, Inc. LW Consulting, Inc. 5925 Stevenson Ave, Suite G 5925 Stevenson Ave,
New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert- Rodney Farley, CHC Terry Raser, RN, RAC-CT, C-NE LW Consulting, Inc. LW Consulting, Inc. 5925 Stevenson Ave, Suite G 5925 Stevenson Ave,
Summary of RCF rule changes
 Summary of RCF rule changes Please find below details of some of the changes made for the five year review for the sections of the administrative code that apply to Residential Care Facilities. 3701-17-50
Summary of RCF rule changes Please find below details of some of the changes made for the five year review for the sections of the administrative code that apply to Residential Care Facilities. 3701-17-50
Tag Description Page. F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125. F622 Transfer & Discharge 155
 Tag Description Page F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125 F622 Transfer & Discharge 155 F626 Permitting Residents to Return to Facility 170 F656 Comprehensive Care Plans
Tag Description Page F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125 F622 Transfer & Discharge 155 F626 Permitting Residents to Return to Facility 170 F656 Comprehensive Care Plans
ADULT LONG-TERM CARE SERVICES
 ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
BED RAIL SAFETY 9/15/2015. A Clinical Process Guideline. Background. Federal Nursing Home Reform Act
 BED RAIL SAFETY A Clinical Process Guideline Laura Funsch, RN, BSN, MS Director of Regulatory Strategy, LeadingAge Michigan Background Safety hazards related to bed rail use have been realized since 1990.
BED RAIL SAFETY A Clinical Process Guideline Laura Funsch, RN, BSN, MS Director of Regulatory Strategy, LeadingAge Michigan Background Safety hazards related to bed rail use have been realized since 1990.
Iowa. Phone. Web Site. https://dia-hfd.iowa.gov/dia_hfd/home.do. Licensure Term
 Iowa Phone Agency Department of Inspections and Appeals, Health Facilities Division (515) 281-6325 Contact Linda Kellen (515) 281-7624 E-mail Linda.Kellen@dia.iowa.gov. Web Site https://dia-hfd.iowa.gov/dia_hfd/home.do
Iowa Phone Agency Department of Inspections and Appeals, Health Facilities Division (515) 281-6325 Contact Linda Kellen (515) 281-7624 E-mail Linda.Kellen@dia.iowa.gov. Web Site https://dia-hfd.iowa.gov/dia_hfd/home.do
CMS Final Rule: The Good, the Bad and the Ugly. Live Webinar Wednesday, February 8, :00 p.m. ET
 CMS Final Rule: The Good, the Bad and the Ugly Live Webinar Wednesday, February 8, 2017 1:00 p.m. ET Q+A Submit a question below the slides Resources List To the right of the slides. Download presentation
CMS Final Rule: The Good, the Bad and the Ugly Live Webinar Wednesday, February 8, 2017 1:00 p.m. ET Q+A Submit a question below the slides Resources List To the right of the slides. Download presentation
Neglect Critical Element Pathway
 Use this pathway for concerns in structures or processes that have led to resident outcome such as unrelieved pain, avoidable pressure injuries, poor grooming, avoidable dehydration, lack of continence
Use this pathway for concerns in structures or processes that have led to resident outcome such as unrelieved pain, avoidable pressure injuries, poor grooming, avoidable dehydration, lack of continence
9/17/2015. Bed Rail Safety A Clinical Process Guideline. Background. Federal Nursing Home Reform Act
 Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
Bed Rail Safety A Clinical Process Guideline. Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy
 Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
FORM CMS (2/2013)
") Facility Name: Facility ID: Date: Surveyor Name: The purpose of the observation of the meal service is to determine whether this service takes into account: Resident choice/preferences for food items and
Facility Name: Facility ID: Date: Surveyor Name: The purpose of the observation of the meal service is to determine whether this service takes into account: Resident choice/preferences for food items and
c) Facilities substantially in compliance with the requirements of this Subpart will receive written recognition from the Department.
 Facilities substantially in compliance with the requirements of this Subpart will receive written recognition from the Department.") TITLE 77: PUBLIC HEALTH CHAPTER I: DEPARTMENT OF PUBLIC HEALTH SUBCHAPTER c: LONG-TERM CARE FACILITIES PART 300 SKILLED NURSING AND INTERMEDIATE CARE FACILITIES CODE SECTION 300.7000 APPLICABILITY Section
TITLE 77: PUBLIC HEALTH CHAPTER I: DEPARTMENT OF PUBLIC HEALTH SUBCHAPTER c: LONG-TERM CARE FACILITIES PART 300 SKILLED NURSING AND INTERMEDIATE CARE FACILITIES CODE SECTION 300.7000 APPLICABILITY Section
CMS s RAI Version 3.0 Manual October 2016
 Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
US Health Health Policy
 Memorandum US Health Health Policy Date January 22, 2015 To From Subject CMS Abt Associates MDS 3.0 Focused Survey Pilot Results Executive Summary This memo describes the results of the MDS 3.0 Focused
Memorandum US Health Health Policy Date January 22, 2015 To From Subject CMS Abt Associates MDS 3.0 Focused Survey Pilot Results Executive Summary This memo describes the results of the MDS 3.0 Focused
RELEVANT STATE STANDARDS OF CARE AND SERVICES AND PROCESSES TO ENSURE STANDARDS ARE MET 1
 Appendix D RELEVANT STATE STANDARDS OF CARE AND SERVICES AND PROCESSES TO ENSURE STANDARDS ARE MET 1 I. STATE STANDARDS OF CARE AND SERVICES Excerpts From RSA 171-A 171-A:1 Purpose and Policy. The purpose
Appendix D RELEVANT STATE STANDARDS OF CARE AND SERVICES AND PROCESSES TO ENSURE STANDARDS ARE MET 1 I. STATE STANDARDS OF CARE AND SERVICES Excerpts From RSA 171-A 171-A:1 Purpose and Policy. The purpose
DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES CHAPTER 411
 DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 57 INDORSEMENT OF ALZHEIMER'S CARE UNITS 411-057-0000 Statement of Purpose (1)
DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 57 INDORSEMENT OF ALZHEIMER'S CARE UNITS 411-057-0000 Statement of Purpose (1)
National Overview of CMS RoP & Quality. Holly Harmon, RN, MBA, LNHA, FACHCA May 3, 2018
 National Overview of CMS RoP & Quality Holly Harmon, RN, MBA, LNHA, FACHCA May 3, 2018 It s a Time of Change.. Reform of Requirements of Participation (RoP) - 3-Phase Implementation Phase 1: Upon the effective
National Overview of CMS RoP & Quality Holly Harmon, RN, MBA, LNHA, FACHCA May 3, 2018 It s a Time of Change.. Reform of Requirements of Participation (RoP) - 3-Phase Implementation Phase 1: Upon the effective