MDS 3.0: What Leadership Needs to Know
|
|
|
- Duane Barker
- 5 years ago
- Views:
Transcription

1 MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN
2 History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted by Congress in the Omnibus Budget Reconciliation Act of 1987 (OBRA 87). These were the most sweeping reforms to nursing homes regulation since the onset of the federal payment for nursing home care with the passage of Medicare and Medicaid programs in the mid 1960 s.
3 History of the MDS and RAI Process (Continued) In 1983 Congress asked the National Academy of Science and Institute of Medicine to examine nursing home quality and report on how to improve nursing home regulations. After two and a half years of study one of the central recommendations was the development of a uniform comprehensive resident assessment system.
4 History of the MDS and RAI Process (Continued) The development of the RAI involved the work of 18 clinical work groups. The MDS was scheduled for launch in October 1990 and was fully implemented by spring of Development of MDS 2.0 started in early 1993.
5 History of the MDS and RAI Process (Continued) MDS 2.0 launched in October A major overhaul of the MDS 2.0 manual was published in December Quarterly updates as indicated.
6 PPS Balanced Budget Act (BBA) of 1997 included implementation of a Medicare Prospective Payment System (PPS) for skilled nursing facilities. The PPS system replaced the retrospective costbased system for skilled nursing homes under Part A. The final rule was published May 12, 1998.
7 Why MDS 3.0? Response to changes in nursing home care. Change in resident characteristics. Advances in resident assessment methods. Provider and consumer concerns about the performance of MDS 2.0.
8 MDS 3.0 Development CMS contracted with RAND Corp. and Harvard University to draft the revisions and nationally test MDS 3.0. The major goals of MDS 3.0: Increase the relevance of items. Improve accuracy and validity of the tool. Increase user satisfaction. Increase residents voices by increasing resident interviews.
9 MDS 3.0 Development (Continued) In 2005, CMS initiated a national nursing home staff time measurement (STM) study, named the Staff Time and Resource Intensity Verification (STRIVE) Project. This was the first nationwide time study since Based on this analysis CMS developed the RUG-IV classification system incorporated into MDS 3.0.
10 Resource Utilization Groups (RUGs) Over half the state Medicaid programs use the MDS for case mix payment. With MDS 3.0 state agencies have the option to continue the use of RUG-III or adopt RUG-IV. CMS has provided alternate RUG-IV versions with 47, 57 and 66 groups. States that currently use the RUG-III system can continue to utilize the 34, 44, or 53 groups.
11 RUG-IV The RUG-IV classification system has eight major classification categories: 1. Rehabilitation plus extensive services 2. Rehabilitation 3. Extensive services 4. Special care high 5. Special care low 6. Clinically complex 7. Behavioral symptoms and cognitive performance problems 8. Reduced physical function
12 RUG-IV (Continued) RUG-IV categories are further categorized: All categories (with the exception of extensive services) categorized by intensity of the resident s ADLs. Special care high and low and clinically complex categories categorized by the presence of depression. Behavioral symptoms and cognitive performance problems and reduced physical function categorized by the provision of restorative nursing services.
13 Components of MDS 3.0 SECTION BY SECTION
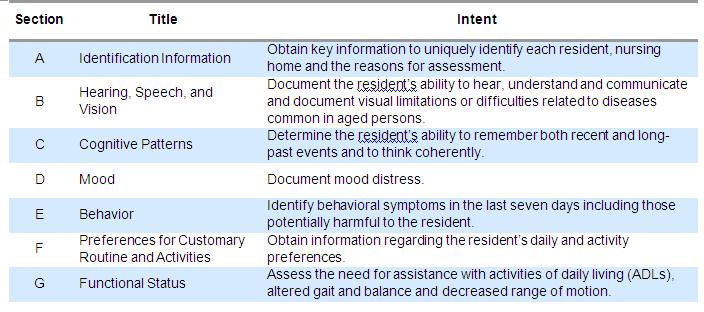
14
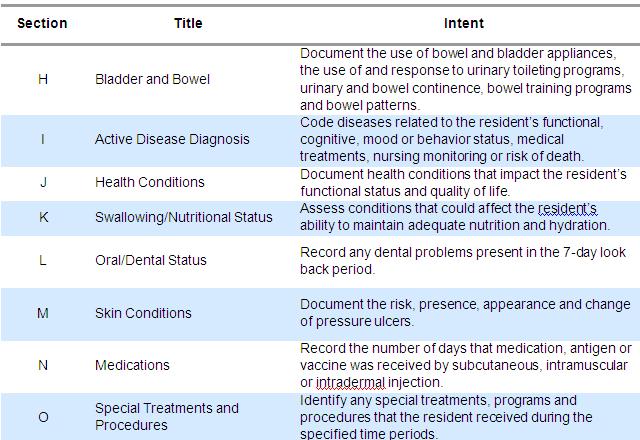
15
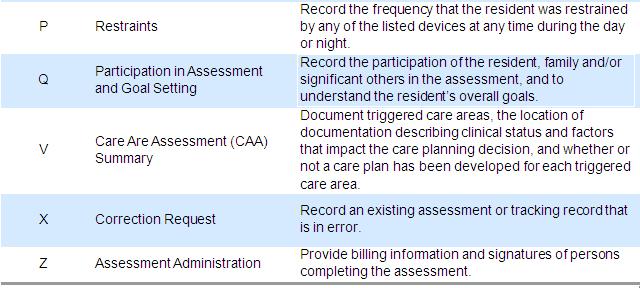
16
17 The MDS 3.0 Manual Intent. The reasons for including this set of assessment items in the MDS. Item display. In order to facilitate accurate resident assessment using the MDS, each assessment section is accompanied by screen shots which display the item from the MDS 3.0 item set.
18 The MDS 3.0 Manual1 Item Rationale. The purpose of assessing this aspect of a resident s clinical or functional status. Health-related Quality of Life. How the condition, impairment, improvement or decline being assessed can affect a resident s quality of life, along with the importance of staff understanding the relationship of the clinical or functional issue to quality of life.
19 The MDS 3.0 Manual2 Planning for Care. How assessment of the condition, impairment, improvement or decline being assessed can contribute to appropriate care planning. Steps for Assessment. Sources of information and methods for determining the correct response for coding each MDS item. Coding Instructions. The proper method of recording each response, with explanations of individual response categories.
20 The MDS 3.0 Manual3 Coding Tips and Special Populations. Clarifications, issues of note and conditions to be considered when coding individual MDS items. Examples. Case examples of appropriate coding for most, if not all, MDS sections/items.
21 Major Changes to MDS 3.0
22 Interviews One of the major changes in the MDS 3.0 is the number of resident interviews. Each section that requires an interview, will be indicated by a symbol (a small black box with an ear in it). MDS 3.0 allows for a staff assessment if the resident is unable to complete the interview.
23 Time Frames Throughout the MDS 3.0 the look-back period is 7 days UNLESS otherwise stated. Interviews should be completed as close to the assessment reference date as possible to gather the most complete and accurate information.
24 Section C Screening question to determine if a resident interview should be attempted: Brief Interview for Mental Status (BIMS) If an interview is not possible, a staff assessment of the resident s mental status is conducted. Other assessments: Delirium Acute onset of mental change
25 Section D Assessment for resident interview PHQ-9 (Patient Health questionnaire) If an interview is not possible, a staff assessment of the resident s mood is conducted.
26 Section F Interview for daily preferences and activity preferences. Make every effort to complete this interview with the resident, but you may complete the interview with a family member or significant other. Complete the staff assessment of daily activities preferences if unable to complete interview with resident, family or significant other.
27 Section G G0110 is very similar to section G1 in MDS 2.0. Major differences include the addition of code 7 (activity occurred 2 or fewer times). Instructions for a rule of 3. (see flow diagram) Change in definition of independent and total dependence.
28 Section G Includes balance during transitions and walking. Functional limitations. Mobility devices. Functional rehabilitation.
29 Section I Much more comprehensive list of active diagnoses. The term active diagnosis requires two parts: A documented diagnosis in the past 60 days. Once you have this then you need to determine if the diagnosis is active Active diagnoses are those that have a direct relationship to the resident s functional status, cognitive status, mood or behavior, medical treatments, nursing monitoring or risk of death during the look-back period.
30 Section J New pain interview including a pain intensity scale Other health conditions including assessment for dyspnea. Fall history Prior to admission Falls since admission Number of falls since admission and type of injury
31 Section M This section is completely re-structured. Pressure Ulcers (PUs): Is the resident at risk for PU? Does resident have an unhealed PU? Current number of unhealed PU s per stage. Dimensions of unhealed stage 3 or 4 ulcer or eschar.
32 Section M (Continued) Worsening of PU since prior assessment Healed pressure ulcer Present upon admission Number of venous and arterial ulcers Other ulcers, wounds and skin problems Skin and ulcer treatments
33 Section O Look back is different: 14 days for special treatments and programs. Two assessments for each question: While NOT a resident While a resident
34 Section O (Continued) Influenza and pneumococcal vaccine Therapies (7 day look back) Individual Minutes (no units or rounding) Concurrent Minutes (with one other resident) Group Minutes Definitions differ for Medicare A and Medicare B Days (the number of days therapy was administered for at least 15 minutes) Therapy start date Therapy end date (enter dashes if the therapy is still in progress. No coding changes to restorative nursing programs
35 Section P MDS 3.0 created a section specifically for physical restraints. Evaluations of two areas: In Bed Bed rails, trunk restraint, limb restraint, other Used in chair or out of bed Trunk restraint, limb restraint, chair prevents rising, other When coding a restraint you must evaluate the effect of the device on the resident.
36 Section Q Components include: Participation in assessment Resident s overall expectation Discharge plan Return to the community (must be asked on each assessment unless it is determined that a discharge to the community is not feasible). Referral
37 Section V 20 Care Area Assessment (CAA) replace the RAPs from MDS 2.0. Each CAA is comprised of: Introduction A list of items and responses from the MDS that are considered triggers for the issue or condition (CAT) A list of resources that nursing homes can use in performing the assessment/review of the particular issue or condition
38 CAAs in MDS 3.0 Delirium Cognitive loss/dementia Visual function Communication ADL functional/rehabilitation potential Pain (new) Urinary Incontinence and Indwelling Catheter Return to the community (new) Psychosocial well-being Mood State Behavioral Symptoms Activities Falls Nutritional Status Feeding Tubes Dehydration/fluid maintenance Dental Care Pressure ulcer Psychotropic drug use Physical restraints
39 CAAs in MDS 3.0 CAAs are required for comprehensive assessments. not required for Medicare assessments. Use the CAA process to guide your assessment and then chart your thinking. Nursing homes should assess the resident in the area triggered using current, evidence-based or expert endorsed research and clinical practice guidelines/resources.
40 CAAs in MDS 3.0 (Continued) CMS has provided a set of CAA tools in Appendix C of the manual. These forms are a resource and are NOT mandated.
41 Section X and Section Z Section X applies only when submitting a correction request. Section Z Medicare Part A billing Medicare non therapy Part A billing State Medicaid billing (if required) Alternate state Medicaid billing (if required) Insurance billing
42 How Does a NH Prepare for MDS 3.0? Become familiar with all the new forms and the coding methodology. Plan on going to a comprehensive education program that reviews the comprehensive full MDS 3.0 item-by item. Purchase or download the MDS 3.0 manual when available. READ (and re-read) the manual!
43 How Does a NH Prepare for MDS 3.0? Talk to your software vendor. Determine which departments will complete sections. Make sure all members of the team who are going to complete the MDS 3.0 get educated Educate residents. Practice prior to October 1 st. The entire interdisciplinary team should be included. Determine systems to be instituted after October 1 st.
44 Operational Changes to Consider with MDS 3.0 The number of interviews that need to be completed: Who will completed them, how will they be divided? How will staff get training to complete the interviews? How will staff manage their time/tasks to complete the interviews?
45 Operational Changes to Consider with MDS 3.02 Discharge assessments: Need to be completed for all residents who are out of the facility for greater than 24 hours (even if not admitted to the hospital) Exceptions for those on therapeutic leaves. This assessment includes all of the interview sections. On paper this form is 27 pages.
46 Operational Changes to Consider with MDS 3.03 How will the MDS get completed in your facility? Paper with a data entry person? Directly into the computer? Many skip patterns in this tool, this may be the easier method. If direct entry, do you have enough computers that are networked to allow direct entry into the MDS.
47 Operational Changes to Consider with MDS 3.04 Time for all staff to complete the MDS: How many admissions do you have per month? How many discharges or residents out of the facility for greater than 24 hours per month? How many residents are covered under Medicare per month? How many comprehensive assessments per month?
48 Operational Changes to Consider with MDS 3.05 When completing the Care Area Assessments, what tools will you use? How can you integrate these tools into assessments to eliminate duplication of work? Does your facility have many non-english speaking residents? If so, how are you going to meet the needs of these residents so interviews can be completed and the residents voice can be heard?
49 Questions
50 Contact Information Ann M. Spenard Qualidigm
Critical Thinking Steps
 CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
CMS s RAI Version 3.0 Manual October 2016
 Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
AANAC Education Advancement. MDS Essentials: An Introduction. Learning Objectives 3/22/2017. Education Advancement
 AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
Wilhide Consulting, Inc. (c) 1
 1") Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Required by the Omnibus Reconciliation Act of 1987 Correction OBRA Scheduling January 2017 NC
Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Required by the Omnibus Reconciliation Act of 1987 Correction OBRA Scheduling January 2017 NC
3/12/2015. Session Objectives. RAI User s Manual. Polling Question
 Session Objectives MDS 3.0 Coding Challenges: Questions, Answers, and Explanations Jen Pettis, BS, RN, WCC Associate March 19, 2015 Upon completion of the program, the participate will: Describe the four
Session Objectives MDS 3.0 Coding Challenges: Questions, Answers, and Explanations Jen Pettis, BS, RN, WCC Associate March 19, 2015 Upon completion of the program, the participate will: Describe the four
MDS Essentials. MDS Essentials: Content. Faculty Disclosures 5/22/2017. Educational Activity Completion
 MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
New Strategies for Managing Medicare Risk
 New Strategies for Managing Medicare Risk John Sheridan, MHSA, FACHE President, ehealth Data Solutions Keith Knapp, PhD, CFACHCA CEO, Christian Care Communities 1001. Survey and Certification Phase II
New Strategies for Managing Medicare Risk John Sheridan, MHSA, FACHE President, ehealth Data Solutions Keith Knapp, PhD, CFACHCA CEO, Christian Care Communities 1001. Survey and Certification Phase II
MDS FOR THE ADMINISTRATOR: WHAT YOU NEED TO KNOW
 MDS FOR THE ADMINISTRATOR: WHAT YOU NEED TO KNOW LIBBY YOUSE, LNHA Long Term Care Leadership Coach OBJECTIVES Understanding factors why MDS s are so important in your home Identify the effects it places
MDS FOR THE ADMINISTRATOR: WHAT YOU NEED TO KNOW LIBBY YOUSE, LNHA Long Term Care Leadership Coach OBJECTIVES Understanding factors why MDS s are so important in your home Identify the effects it places
OASIS-B1 and OASIS-C Items Unchanged, Items Modified, Items Dropped, and New Items Added.
 Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
MDS 3.0/RUG IV Distance Learning Series January-June 2014
 MDS 3.0/RUG IV Distance Learning Series January-June 2014 ROUTE TO: Administrator; MDS Coordinator; Director of Nursing; Director of Social Services; Director of Activities; Director of Rehabilitation
MDS 3.0/RUG IV Distance Learning Series January-June 2014 ROUTE TO: Administrator; MDS Coordinator; Director of Nursing; Director of Social Services; Director of Activities; Director of Rehabilitation
11/23/2011. Proactive vs. Reactive Relationship
 Overview Focus on Resident Voice Assessment Schedule EOT OMRA and New Resumption Items New PPS Assessment: COT OMRA CMS Clarifications Coding New Quality Measures Draft MDS and Care Planning as Risk Management
Overview Focus on Resident Voice Assessment Schedule EOT OMRA and New Resumption Items New PPS Assessment: COT OMRA CMS Clarifications Coding New Quality Measures Draft MDS and Care Planning as Risk Management
MDS Training for Social Services Directors
 MDS Training for Social Services Directors Kathy Sanders RN, RAC-CT, DNSCT Sanders Consulting 630 N. 3 rd St. Tecumseh, NE 68450 Hm: (402) 335-2736 Cell: (402) 921-0250 kathy@mdshelp.com Disclaimer The
MDS Training for Social Services Directors Kathy Sanders RN, RAC-CT, DNSCT Sanders Consulting 630 N. 3 rd St. Tecumseh, NE 68450 Hm: (402) 335-2736 Cell: (402) 921-0250 kathy@mdshelp.com Disclaimer The
Carol Maher, RN-BC, RAC-CT. Long-Term Care MDS Coordinator s Field Guide
 Carol Maher, RN-BC, RAC-CT Long-Term Care MDS Coordinator s Field Guide Long-Term Care MDS Coordinator s Field Guide Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC Long-Term Care MDS Coordinator s Field Guide
Carol Maher, RN-BC, RAC-CT Long-Term Care MDS Coordinator s Field Guide Long-Term Care MDS Coordinator s Field Guide Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC Long-Term Care MDS Coordinator s Field Guide
CMS Updates RAI User s Manual
 CMS Updates RAI User s Manual By Rena R. Shephard, MHA, RN, RAC MT, C NE AANAC Executive Editor The Centers for Medicare & Medicaid Services (CMS) June 2 posted revisions to the Long Term Care Facility
CMS Updates RAI User s Manual By Rena R. Shephard, MHA, RN, RAC MT, C NE AANAC Executive Editor The Centers for Medicare & Medicaid Services (CMS) June 2 posted revisions to the Long Term Care Facility
MDS 3.0/RUG IV Distance Learning Series January - May 2016
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 ROUTE TO: _Administrator; _MDS Coordinator; _Director of Nursing; _Director of Accounting; _Director of Social Services; _Director of Activities;
MDS 3.0/RUG IV Distance Learning Series January - May 2016 ROUTE TO: _Administrator; _MDS Coordinator; _Director of Nursing; _Director of Accounting; _Director of Social Services; _Director of Activities;
Restorative Nursing: The NHA s Role and Organizational Outcomes
 Restorative Nursing: The NHA s Role and Organizational Outcomes SUE LAGRANGE, RN, BSN, NHA, CDONA, CIMT DIRECTOR OF EDUCATION PATHWAY HEALTH 1 Objectives Upon completion of this program, attendees should
Restorative Nursing: The NHA s Role and Organizational Outcomes SUE LAGRANGE, RN, BSN, NHA, CDONA, CIMT DIRECTOR OF EDUCATION PATHWAY HEALTH 1 Objectives Upon completion of this program, attendees should
Medicaid RAC Audit Results
 Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Attachment C: Itemized List of OASIS Data Elements
 Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
State and federal regulations supersede any information provided in this toolkit.
 DPA Associates, Inc Toolkit author: Diane Atchinson, RN-BC, MSN, ANP, RAC-CT President, DPA Associates, Inc, Kansas City, MO E mail: diane@dpaassociates.com Clinical editor: Kathy Newman, MSW, LSCW, Consultant
DPA Associates, Inc Toolkit author: Diane Atchinson, RN-BC, MSN, ANP, RAC-CT President, DPA Associates, Inc, Kansas City, MO E mail: diane@dpaassociates.com Clinical editor: Kathy Newman, MSW, LSCW, Consultant
All Medicare Advantage Organizations (MAOs), PACE Organizations, Cost Plans, and certain Demonstrations
, PACE Organizations, Cost Plans, and certain Demonstrations") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
6/29/2015. Focused Survey for MDS Assessment. Objectives: Review the results of the MDS pilot study.
 Focused Survey for MDS Assessment Idaho Health Care Association July 21, 1015 1:45 P.M. 3:15 P.M. Louann Lawson, BA, RN, RAC-CT AHIMA Approved ICD-10-CM/PCS Trainer Nurse Consultant, Clinical Reimbursement
Focused Survey for MDS Assessment Idaho Health Care Association July 21, 1015 1:45 P.M. 3:15 P.M. Louann Lawson, BA, RN, RAC-CT AHIMA Approved ICD-10-CM/PCS Trainer Nurse Consultant, Clinical Reimbursement
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES
 COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT
 Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
Attachment A - Comparison of OASIS-C (Current Version) to OASIS-C1 (Proposed Data Collection)
 to OASIS-C1 (Proposed Data Collection)") Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
A Tool for Maximizing Quality in Your Organization
 OASIS C: A Tool for Maximizing Quality in Your Organization Debbie Costello RN BSN MSM Director of Quality & Safety Caritas Home Care Session Outline Events leading to change in OASIS C Progress in home
OASIS C: A Tool for Maximizing Quality in Your Organization Debbie Costello RN BSN MSM Director of Quality & Safety Caritas Home Care Session Outline Events leading to change in OASIS C Progress in home
Reporter. MDS 3.0: A More Objective Resident Assessment Tool for Nursing Home Use 2010 ISSUE
 FALL MIM Reporter The Review of Medical Information Management for Litigation Published as an educational service to the Corporate, Insurance and Defense Legal Community by Litigation Management, Inc.
FALL MIM Reporter The Review of Medical Information Management for Litigation Published as an educational service to the Corporate, Insurance and Defense Legal Community by Litigation Management, Inc.
All Medicare Advantage Organizations (MAOs), PACE Organizations, Cost Plans, and certain Demonstrations
, PACE Organizations, Cost Plans, and certain Demonstrations") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE MEDICARE PLAN PAYMENT GROUP TO: FROM: SUBJECT:
Executive Summary. This Project
 Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Executive Summary The Health Care Financing Administration (HCFA) has had a long-term commitment to work towards implementation of a per-episode prospective payment approach for Medicare home health services,
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Improving Nursing Home Compare for Consumers. Five-Star Quality Rating System
 Improving Nursing Home Compare for Consumers Five-Star Quality Rating System Improving Nursing Home Compare Major Revision to Nursing Home Compare Mid-December Improved Navigation - Similar to Hospital
Improving Nursing Home Compare for Consumers Five-Star Quality Rating System Improving Nursing Home Compare Major Revision to Nursing Home Compare Mid-December Improved Navigation - Similar to Hospital
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling. Speaker: Thomas Martin November 2014
 Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
Using Structured Post Acute Assessment Data as the Raw Material for Predictive Modeling Speaker: Thomas Martin November 2014 1 Learning Objectives SNF s place in continuum of care Large variance across
Building A Successful MDS Program
 Building A Successful MDS Program Nadine Olness RN, RAC-CT MN State RAI Coordinator March 12, 2018 Objectives Acquire essential knowledge about what is required in order for MDS coordinators to be successful.
Building A Successful MDS Program Nadine Olness RN, RAC-CT MN State RAI Coordinator March 12, 2018 Objectives Acquire essential knowledge about what is required in order for MDS coordinators to be successful.
RAI Panel Q&As August-September 2008
 RAI Panel Q&As August-September 2008 Assessment Questions Question I understand that if a facility misses an assessment and discovers it shortly thereafter, they should do an assessment with a current
RAI Panel Q&As August-September 2008 Assessment Questions Question I understand that if a facility misses an assessment and discovers it shortly thereafter, they should do an assessment with a current
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1)
") CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
CMS Proposed SNF Payment System -- Resident Classification System: Version I (RCS-1) Ohio Health Care Association Mike Cheek, Senior Vice President, Reimbursement Policy October 3, 2017 Background 1 FY18
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model
 and the MDS: A Total Evolution of the SNF Payment Model") Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
Patient Driven Payment Model (PDPM) and the MDS: A Total Evolution of the SNF Payment Model By Devin Kassi, PT, DPT, and Melissa Keiter, RN, RAC-CT, DNS-CT, DON Centers for Medicare & Medicaid Services
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS
 CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit Omnibus Budget Reconciliation Act required (OBRA) MDS records for all residents in Medicare- or Medicaid-certified
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit Omnibus Budget Reconciliation Act required (OBRA) MDS records for all residents in Medicare- or Medicaid-certified
A Closer Look at the Revised Nursing Facility Regulations. Quality of Care
 A Closer Look at the Revised Nursing Facility Regulations Quality of Care Executive Summary The substantive requirements for quality of care are retained in the revised regulations, and the Centers for
A Closer Look at the Revised Nursing Facility Regulations Quality of Care Executive Summary The substantive requirements for quality of care are retained in the revised regulations, and the Centers for
MDS 101 CHAPTER 3 Ingrid Serio Rena R. Shephard
 MDS 101 An Introduction to the RAI Process CHAPTER 3 CAAs, CATs, and Care Planning Ingrid Serio RN, BSN, MPP Rena R. Shephard MHA, RN, RAC -MT, C-NE MDS 101: An Introduction to the RAI Process iii Table
MDS 101 An Introduction to the RAI Process CHAPTER 3 CAAs, CATs, and Care Planning Ingrid Serio RN, BSN, MPP Rena R. Shephard MHA, RN, RAC -MT, C-NE MDS 101: An Introduction to the RAI Process iii Table
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES
 UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated May 2017 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF CONTENTS
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated May 2017 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF CONTENTS
DATA ACCURACY A KEY FACTOR FOR SUCCESSFUL OPERATIONS
 Disclosure of Commercial Interests List the Name of Your Employer: -Executive Director -The Alliance Training Center -Providing Solutions in Health Care If consultant for organizations, only list the names
Disclosure of Commercial Interests List the Name of Your Employer: -Executive Director -The Alliance Training Center -Providing Solutions in Health Care If consultant for organizations, only list the names
CY 2018 Home Health PPS Proposed Rule
 CY 2018 Home Health PPS Proposed Rule Rochelle Archuleta & Caitlin Gillooley AHA Policy August 24, 2017 CY 2018 Proposed Rule Published in July 28 Federal Register Net Reduction: 0.4%, -$80m Same for facility-based
CY 2018 Home Health PPS Proposed Rule Rochelle Archuleta & Caitlin Gillooley AHA Policy August 24, 2017 CY 2018 Proposed Rule Published in July 28 Federal Register Net Reduction: 0.4%, -$80m Same for facility-based
Hospice and End of Life Care and Services Critical Element Pathway
 Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Session #: R14. Robin L. Hillier. Agenda 4/9/2014. Simply Quality Measures. (330) RLH Consulting.
 RLH Consulting.") Session #: R14 Simply Quality Measures Robin L. Hillier robin@rlh-consulting.com (330) 807-2850 RLH Consulting Agenda Quality Measures How are they calculated How to read the reports How to use the reports
Session #: R14 Simply Quality Measures Robin L. Hillier robin@rlh-consulting.com (330) 807-2850 RLH Consulting Agenda Quality Measures How are they calculated How to read the reports How to use the reports
DEFINITIONS (c)(1) Discharge Planning : Home Health Agency (HHA) : Inpatient Rehabilitation Facility (IRF) : Local Contact Agency :
(1) Discharge Planning : Home Health Agency (HHA) : Inpatient Rehabilitation Facility (IRF) : Local Contact Agency :") F660 483.21(c)(1) Discharge Planning Process The facility must develop and implement an effective discharge planning process that focuses on the resident s discharge goals, the preparation of residents
F660 483.21(c)(1) Discharge Planning Process The facility must develop and implement an effective discharge planning process that focuses on the resident s discharge goals, the preparation of residents
Changes to the RAI manual effective October 1, 2013
 Changes to the RAI manual effective October 1, 2013 CMS released on Friday, September 27 an updated version of the RAI manual that became effective October 1, 2013. The manual is found here> http://www.cms.gov/medicare/quality-initiatives-patient-assessment-
Changes to the RAI manual effective October 1, 2013 CMS released on Friday, September 27 an updated version of the RAI manual that became effective October 1, 2013. The manual is found here> http://www.cms.gov/medicare/quality-initiatives-patient-assessment-
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES
 UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated February 2018 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated February 2018 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF
SECTION P: RESTRAINTS
 SECTION P: RESTRAINTS Intent: The intent of this section is to record the frequency over the 7-day look-back period that the resident was restrained by any of the listed devices at any time during the
SECTION P: RESTRAINTS Intent: The intent of this section is to record the frequency over the 7-day look-back period that the resident was restrained by any of the listed devices at any time during the
Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC. Month Day Year / / Month Day Year
 / / UHHC. Month Day Year / / Month Day Year") Transfer (M0010) CMS Certification Number: 367549 (M0014) Branch State: OH (M0016) Branch ID Number: N/A Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC (M0020) Patient
Transfer (M0010) CMS Certification Number: 367549 (M0014) Branch State: OH (M0016) Branch ID Number: N/A Patient Identifiers: Facial Recognition Patient Address DOB (month/day year) / / UHHC (M0020) Patient
5DAY = 1 AND
 July 2008 Revision Table CH. Sect. Pg. July 2008 Revision NA Title Page NA Change the revised date to July 2008 CH 2 2.2 2-11 Revise as follows: Delete the second sentence of the second paragraph, The
July 2008 Revision Table CH. Sect. Pg. July 2008 Revision NA Title Page NA Change the revised date to July 2008 CH 2 2.2 2-11 Revise as follows: Delete the second sentence of the second paragraph, The
CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS)
") CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS) 6.1 Background The Balanced Budget Act of 1997 included the implementation of a Medicare Prospective Payment System (PPS)
CHAPTER 6: MEDICARE SKILLED NURSING FACILITY PROSPECTIVE PAYMENT SYSTEM (SNF PPS) 6.1 Background The Balanced Budget Act of 1997 included the implementation of a Medicare Prospective Payment System (PPS)
Leveraging Your Facility s 5 Star Analysis to Improve Quality
 Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
US Health Health Policy
 Memorandum US Health Health Policy Date January 22, 2015 To From Subject CMS Abt Associates MDS 3.0 Focused Survey Pilot Results Executive Summary This memo describes the results of the MDS 3.0 Focused
Memorandum US Health Health Policy Date January 22, 2015 To From Subject CMS Abt Associates MDS 3.0 Focused Survey Pilot Results Executive Summary This memo describes the results of the MDS 3.0 Focused
Transitioning to the New IRF-PAI
 Transitioning to the New IRF-PAI 2014. FIM, UDS-PROi, UDSMR, and the UDSMR logo are trademarks of, a division of UB Foundation Activities, Inc. Agenda August 2014 final rule summary Discuss IRF PPS changes
Transitioning to the New IRF-PAI 2014. FIM, UDS-PROi, UDSMR, and the UDSMR logo are trademarks of, a division of UB Foundation Activities, Inc. Agenda August 2014 final rule summary Discuss IRF PPS changes
Care Planning: The Road Map for Individualized Resident Care
 Care Planning: The Road Map for Individualized Resident Care Kathy Sanders RN, RAC-CT, DNS-CT Sanders Consulting kathy@mdshelp.com 1 Disclaimer The Care Planning: Care Planning: The Road Map for Individualized
Care Planning: The Road Map for Individualized Resident Care Kathy Sanders RN, RAC-CT, DNS-CT Sanders Consulting kathy@mdshelp.com 1 Disclaimer The Care Planning: Care Planning: The Road Map for Individualized
SNF proposed rule revisions to case-mix methodology
 SNF proposed rule revisions to case-mix methodology Comments due: August 25, 2017 CMS intent to propose case-mix refinements in the FY 2019 SNF PPS proposed rule Summary of changes Goals of the change:
SNF proposed rule revisions to case-mix methodology Comments due: August 25, 2017 CMS intent to propose case-mix refinements in the FY 2019 SNF PPS proposed rule Summary of changes Goals of the change:
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide
 Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide April 2018 April 2018 Revisions Beginning with the April 2018 update of the Nursing Home Compare website and the Five-Star
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide April 2018 April 2018 Revisions Beginning with the April 2018 update of the Nursing Home Compare website and the Five-Star
CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS. Category 4A - General OASIS forms questions.
 Q1. [Q&A RETIRED 09/09; Outdated] CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q2. When integrating the OASIS data items into an HHA's assessment system, can
Q1. [Q&A RETIRED 09/09; Outdated] CATEGORY 4 - OASIS DATA SET: FORMS and ITEMS Category 4A - General OASIS forms questions. Q2. When integrating the OASIS data items into an HHA's assessment system, can
10/14/2014 COMMON MDS CODING ERRORS OVERVIEW OF SS/ACT SECTIONS SECTION B
 COMMON MDS CODING ERRORS K AT H Y Y O S T E N, L C S W, P I P OVERVIEW OF SS/ACT SECTIONS Section B Vision, Speech, Hearing Section C Cognitive Patterns Section D Mood Section E Behaviors Section F Preferences
COMMON MDS CODING ERRORS K AT H Y Y O S T E N, L C S W, P I P OVERVIEW OF SS/ACT SECTIONS Section B Vision, Speech, Hearing Section C Cognitive Patterns Section D Mood Section E Behaviors Section F Preferences
The Shift is ON! Goodbye PPS, Hello RCS
 The Shift is ON! Goodbye PPS, Hello RCS Presented By Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Maureen McCarthy, RN, BS, RAC-MT, QCP-MT Maureen is the President of Celtic Consulting, LLC and
The Shift is ON! Goodbye PPS, Hello RCS Presented By Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Maureen McCarthy, RN, BS, RAC-MT, QCP-MT Maureen is the President of Celtic Consulting, LLC and
Goodbye PPS: Hello RCS!
 Disclosure of Commercial Interests I consult for the following organizations: Celtic Consulting LLC President, CEO Celtic Consulting is a Long-Term Care advisory firm, focused on providing one-on-one oversight
Disclosure of Commercial Interests I consult for the following organizations: Celtic Consulting LLC President, CEO Celtic Consulting is a Long-Term Care advisory firm, focused on providing one-on-one oversight
Outcome Based Case Conference
 Outcome Based Case Conference Are You On the Train or On the Tracks? Michelle Funk, RN BS, COS C 15 years RN 13 years Home Health Clinician Case Manager Program Coordinator Supervisor QA Coordinator Special
Outcome Based Case Conference Are You On the Train or On the Tracks? Michelle Funk, RN BS, COS C 15 years RN 13 years Home Health Clinician Case Manager Program Coordinator Supervisor QA Coordinator Special
OASIS-C Home Health Outcome Measures
 OASIS-C Home Measures 1 End Result Grooming groom self. (M1800) Grooming 2 End Result Grooming same in ability to groom self. (M1800) Grooming 3 End Result Upper Body Dressing dress upper body. (M1810)
OASIS-C Home Measures 1 End Result Grooming groom self. (M1800) Grooming 2 End Result Grooming same in ability to groom self. (M1800) Grooming 3 End Result Upper Body Dressing dress upper body. (M1810)
Department of Veterans Affairs VHA DIRECTIVE Veterans Health Administration Washington, DC December 7, 2005
 Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Final Rule Summary. Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017
 Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Final Rule Summary Medicare Skilled Nursing Facility Prospective Payment System Fiscal Year 2017 August 2016 Table of Contents Overview and Resources... 2 Skilled Nursing Facility (SNF) Payment Rates...
Agenda: Noon Overview of the regulatory sections affected by the Reform of RoP in Phase 2
 Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
2. D Mood E Behavior F Preferences for Customary Routine and Activities G Functional Status H Bladder and Bowel
 Newslet ter Title R A I C o o r d i n a t or 1-7 1 7-7 8 7-1 8 1 6 q a - m d s @ s t a t e. p a. u s RAI Spotlight MDS 3.0 Training R AI C o o r d i n a t o r 1-7 1 7-7 8 7-1 8 1 6 q a -m ds @ state.p
Newslet ter Title R A I C o o r d i n a t or 1-7 1 7-7 8 7-1 8 1 6 q a - m d s @ s t a t e. p a. u s RAI Spotlight MDS 3.0 Training R AI C o o r d i n a t o r 1-7 1 7-7 8 7-1 8 1 6 q a -m ds @ state.p
Chapter Two. Preadmission Screening and Annual Resident Review (PASARR)
") Preadmission Screening and Annual Resident Review (PASARR) Introduction The information in this chapter addresses Preadmission Screening and Annual Resident Review (PASARR) requirements for applicants
Preadmission Screening and Annual Resident Review (PASARR) Introduction The information in this chapter addresses Preadmission Screening and Annual Resident Review (PASARR) requirements for applicants
Quality Measures and the Five-Star Rating
 Quality Measures and the Five-Star Rating Pennsylvania Health Care Association Presented by Reinsel Kuntz Lesher LLP Senior Living Services Consulting October 23, 2014 Disclaimer The information contained
Quality Measures and the Five-Star Rating Pennsylvania Health Care Association Presented by Reinsel Kuntz Lesher LLP Senior Living Services Consulting October 23, 2014 Disclaimer The information contained
Quality Indicators: FY 2015 July 8, Kristen Smith, MHA, PT
 Quality Indicators: FY 2015 July 8, 2014 Kristen Smith, MHA, PT Objectives Review upcoming IRF-PAI changes effective October 1, 2014 Discuss the new quality reporting items as part of the Medicare Quality
Quality Indicators: FY 2015 July 8, 2014 Kristen Smith, MHA, PT Objectives Review upcoming IRF-PAI changes effective October 1, 2014 Discuss the new quality reporting items as part of the Medicare Quality
2014 AANAC 9_30_ AANA C AANA
 2013 2014 AANAC AANAC 9_30_14 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT Requirements for Successful Completion 1 Contact hour will be awarded for this continuing
2013 2014 AANAC AANAC 9_30_14 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT Requirements for Successful Completion 1 Contact hour will be awarded for this continuing
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
CNA OnSite Series Overview: Understanding Restorative Care Part 1 - Introduction to Restorative Care
 Series Overview: Understanding Restorative Care Part 1 - Introduction to Restorative Care Administering the Program Read the Guide View the Video Review the Suggested Questions Complete Post-Test Answer
Series Overview: Understanding Restorative Care Part 1 - Introduction to Restorative Care Administering the Program Read the Guide View the Video Review the Suggested Questions Complete Post-Test Answer
Stage 2 General Critical Element Pathway Facility Name: Facility ID: Date: Surveyor Name:
 Facility Name: Facility ID: Date: Surveyor Name: Resident Name: Resident ID: Initial Admission Date: Care Area(s): Interviewable: Yes No Resident Room: Use Use this General Investigative Protocol to investigate
Facility Name: Facility ID: Date: Surveyor Name: Resident Name: Resident ID: Initial Admission Date: Care Area(s): Interviewable: Yes No Resident Room: Use Use this General Investigative Protocol to investigate
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT
 A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
A Nurse Leader s guide to a successful Restorative Nursing Program PRESENTER: AMY FRANKLIN RN, DNS MT, QCP MT, RAC MT Requirements for Successful Completion 1. 2.0 contact hours will be awarded for this
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS
 CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit MDS records for all residents in Medicare- or Medicaidcertified beds regardless of the pay source. Skilled
CHAPTER 5: SUBMISSION AND CORRECTION OF THE MDS ASSESSMENTS Nursing homes are required to submit MDS records for all residents in Medicare- or Medicaidcertified beds regardless of the pay source. Skilled
Quality Measures (QM) & Five Star Rating System. Objectives 4/18/2016 MDS CODING FOR QUALITY MEASURES
 & Five Star Rating System. Objectives 4/18/2016 MDS CODING FOR QUALITY MEASURES") Quality Measures (QM) & Five Star Rating System Carol Hill MSN, RN, RAC-CT, DNS-CT, RAC-MT, QCP Objectives At the conclusion of this educational offering the participant will be able to: Identify MDS items
Quality Measures (QM) & Five Star Rating System Carol Hill MSN, RN, RAC-CT, DNS-CT, RAC-MT, QCP Objectives At the conclusion of this educational offering the participant will be able to: Identify MDS items
Successful Restorative Program When Therapy and Nursing Collaborate
 Successful Restorative Program When Therapy and Nursing Collaborate AdvantageCare Rehabilitation / Advantage Home Health Services Kathy Kemmerer, NAC, RAC-CT 3.0, CPRA CMI Specialist & Medicare Reimbursement
Successful Restorative Program When Therapy and Nursing Collaborate AdvantageCare Rehabilitation / Advantage Home Health Services Kathy Kemmerer, NAC, RAC-CT 3.0, CPRA CMI Specialist & Medicare Reimbursement
Quality Measures Are My Friends
 s Are My Friends Advantage Home Health Services AdvantageCare Rehabilitation Kathy Kemmerer, NAC, RAC-CT 3.0, CPRA Nurse Consultant / CMI Specialist & Medicare Reimbursement Specialist Dave Lishinsky,
s Are My Friends Advantage Home Health Services AdvantageCare Rehabilitation Kathy Kemmerer, NAC, RAC-CT 3.0, CPRA Nurse Consultant / CMI Specialist & Medicare Reimbursement Specialist Dave Lishinsky,
THE LEADERS GUIDE TO MDS 3.0 IMPLEMENTATION. Update on RUGs IV: The Problem. Update on RUGs IV: The Best Solution. Update on RUGs IV: The Default
 THE LEADERS GUIDE TO MDS 3.0 IMPLEMENTATION June District Meetings, 2010 Update on RUGs IV: The Problem Current RUG-III based on MDS 2.0 RUG-IV based on MDS 3.0 Congress postponed most of RUG IV for 1
THE LEADERS GUIDE TO MDS 3.0 IMPLEMENTATION June District Meetings, 2010 Update on RUGs IV: The Problem Current RUG-III based on MDS 2.0 RUG-IV based on MDS 3.0 Congress postponed most of RUG IV for 1
MDS Inaccuracy: Forecast for Failure!
 MDS Inaccuracy: Forecast for Failure! PRESENTED FOR KHCA BY: BECKY LABARGE, RN, RAC-CT, RAC-MT MDS Inaccuracy: Forecast for Failure! OBJECTIVES: oreview RAI Manual updates for FY2016 ouncover common MDS
MDS Inaccuracy: Forecast for Failure! PRESENTED FOR KHCA BY: BECKY LABARGE, RN, RAC-CT, RAC-MT MDS Inaccuracy: Forecast for Failure! OBJECTIVES: oreview RAI Manual updates for FY2016 ouncover common MDS
Adjusting to change FALL 2010 SUCCESSFUL REHAB MANAGEMENT IN LONG-TERM CARE. Guide to. A Guide. MDS 3.0 arrived. Are YOU prepared?
 SUCCESSFUL REHAB MANAGEMENT IN LONG-TERM CARE FALL 2010 Adjusting to change MDS 3.0 has has arrived. arrived. Are YOU YOU prepared? A Guide Guide to to MDS 3.0 3.0 and and RUG-IV for for therapy service
SUCCESSFUL REHAB MANAGEMENT IN LONG-TERM CARE FALL 2010 Adjusting to change MDS 3.0 has has arrived. arrived. Are YOU YOU prepared? A Guide Guide to to MDS 3.0 3.0 and and RUG-IV for for therapy service
HH Compare. IMPACT Act. Measure HHVBP
 Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
Measure HH Compare Star Rating Improvement in Bathing X X X Improvement in Bed Transferring X X X Improvement in Ambulation/Locomotion X X X Improvement in Management of Oral Medications X X Improvement
An Initial Review of the CY Medicare Home Health Rule. CY2018 Proposed Medicare Home Health Rate Rule and Much More
 An Initial Review of the CY 2018 2019 Medicare Home Health Rule Mary K. Carr William A. Dombi NAHC CY2018 Proposed Medicare Home Health Rate Rule and Much More Published July 25, 2017 https://www.cms.gov/medicare/medicare
An Initial Review of the CY 2018 2019 Medicare Home Health Rule Mary K. Carr William A. Dombi NAHC CY2018 Proposed Medicare Home Health Rate Rule and Much More Published July 25, 2017 https://www.cms.gov/medicare/medicare
11/18/2013 MDS 3.0 RAI MANUAL CHAPTER 1 RAI MANUAL CHAPTER 1 1.8, 1-16, 1-17, I-18
 MDS 3.0 CHANGES EFFECTIVE 10-1-2013 RAI MANUAL CHAPTER 1 1.8, 1-16, 1-17, I-18 Support Agency Contractors to assist in accomplishment of a CMS function. To assist another Federal or SA.for purposes of
MDS 3.0 CHANGES EFFECTIVE 10-1-2013 RAI MANUAL CHAPTER 1 1.8, 1-16, 1-17, I-18 Support Agency Contractors to assist in accomplishment of a CMS function. To assist another Federal or SA.for purposes of
The RoPs are here! Do you know what s changing?
 The RoPs are here! Do you know what s changing? Mary Madison, RN, RAC-CT, CDP Clinical Consultant, LTC/Senior Care Briggs Healthcare March 7, 2017 2 What we ll cover today CMS goals behind the updated
The RoPs are here! Do you know what s changing? Mary Madison, RN, RAC-CT, CDP Clinical Consultant, LTC/Senior Care Briggs Healthcare March 7, 2017 2 What we ll cover today CMS goals behind the updated
Objectives 9/18/2018. Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018
 Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018") Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018 Mission: The trusted voice for aging. Objectives List the five(5) case mix components
Patient Driven Payment Model(PDPM) Janine Finck Boyle, MBA/HCA, LNHA Vice President of Regulatory Affairs Fall 2018 Mission: The trusted voice for aging. Objectives List the five(5) case mix components
LTCH Lay of the Land: Reporting the LTCH CARE Data Set. July 30, 2012
 LTCH Lay of the Land: Reporting the LTCH CARE Data Set July 30, 2012 Purpose LTCH Quality Reporting Program, specifically the LTCH CARE Data Set CMS guidance, training & transmission Dates & Deadlines
LTCH Lay of the Land: Reporting the LTCH CARE Data Set July 30, 2012 Purpose LTCH Quality Reporting Program, specifically the LTCH CARE Data Set CMS guidance, training & transmission Dates & Deadlines
FH16 - Developed by Polaris Group Page 1 of 140
 FH16 - Developed by Polaris Group www.polaris-group.com Page 1 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page 2 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page
FH16 - Developed by Polaris Group www.polaris-group.com Page 1 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page 2 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page
Sneak Peak: MDS 3.0 Changes & New QRP s. Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma
 Sneak Peak: MDS 3.0 Changes & New QRP s Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma Disclaimer These materials, including any medical literature
Sneak Peak: MDS 3.0 Changes & New QRP s Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma Disclaimer These materials, including any medical literature
NURSING FACILITY ASSESSMENTS
 Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
Behavioral Health Services ( )
") Behavioral Health Services ( 483.40) Presenter: Sabine Dettlinger-Metropoulos Summary New Section CMS became aware of concerns that behavioral health services Were either not always being addressed or
Behavioral Health Services ( 483.40) Presenter: Sabine Dettlinger-Metropoulos Summary New Section CMS became aware of concerns that behavioral health services Were either not always being addressed or
New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert-
 New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert- Rodney Farley, CHC Terry Raser, RN, RAC-CT, C-NE LW Consulting, Inc. LW Consulting, Inc. 5925 Stevenson Ave, Suite G 5925 Stevenson Ave,
New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert- Rodney Farley, CHC Terry Raser, RN, RAC-CT, C-NE LW Consulting, Inc. LW Consulting, Inc. 5925 Stevenson Ave, Suite G 5925 Stevenson Ave,
OASIS QUALITY IMPROVEMENT REPORTS
 6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide
 Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide July 2016 Note: In July 2016, the Centers for Medicare & Medicaid Services (CMS) is making several changes to the
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide July 2016 Note: In July 2016, the Centers for Medicare & Medicaid Services (CMS) is making several changes to the
Based on the comprehensive assessment of a resident, the facility must ensure that:
 7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
Center for Clinical Standards and Quality/Survey & Certification Group
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey