Get Ready for Phase 1 of the New Requirements of Participation
|
|
|
- Damian Neal
- 5 years ago
- Views:
Transcription

1 PADONA Convention March 30, 2017 Get Ready for Phase 1 of the New Requirements of Participation Paula G. Sanders, Esquire
2 New Requirements of Participation (RoPs) Published October 4, 2016 (81 Fed. Reg ) Available at 10/04 First comprehensive update since 1991 CMS estimated cost per SNF Year 1: ~ $62,900 Subsequent years: ~$55, Fed. Reg
3 CMS: Themes Of The RoPs Person-centered care Quality Facility assessment, competency-based approach Comprehensive review & modernization Implementation of legislative requirements 3
4 Survey Implementation Phase 1: effective November 28, 2016 Same survey process New RoPs merged into existing F-tags (March 8, a-961c-3c9f83717bd8/SOM_Appendix_PP_3_8_17.pdf) Phase 2: effective November 28, 2017 New Appendix PP (State Operations Manual, SOM) with all new F-tags New survey process combines traditional & Quality Indicator Survey (QIS) 4
5 Multi-Phase Implementation Of RoPs Phase 1: November 28, 2016 Phase 2: 1 year following the effective date of the final rule (Nov. 28, 2017) Phase 3: 3 years following the effective date of the final rule (November 28, 2019) 5



6 6
7 7
8 New Definitions abuse adverse event exploitation misappropriation of resident property neglect person-centered care resident representative sexual abuse mistreatment 8
9 Phase 1: Highlights Resident rights/facility responsibilities combined and expanded Drug regimen review process more detailed Must have discharge planning process & plan for all residents Person-centered care plan More extensive resident assessment process Must include CNA and dietary worker PASARR incorporated into assessment, care plan and discharge plan 9
10 Phase 1: Highlights New behavioral health services ( ) Pre-dispute Binding Arbitration Agreements prohibited but AHCA sued and this rule is currently enjoined
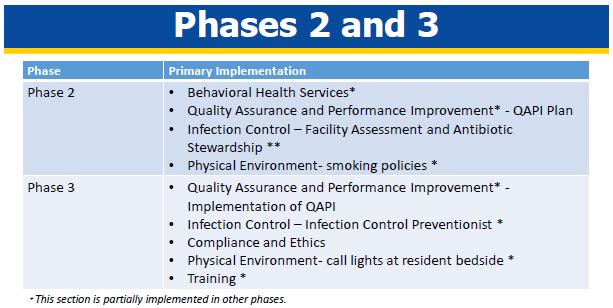
11 Phases 2 And 3: Highlights Quality assurance and performance improvement (QAPI) Added compliance and ethics section Greater monitoring and documentation related to appropriateness of meds Psychotropic & antibiotic stewardship Requires Infection Control Program & Infection Preventionist 11
12 Phases 2 And 3: Highlights Added a staff competency requirement to determine nursing staffing levels Based on a facility assessment, which includes but is not limited to the number of residents, resident acuity, range of diagnoses, and the content of individual care plans Require facility provide behavioral health care and services training (for patients with trauma)
13 483.5 Definitions Person-centered care focus on resident as locus of control and support resident in making own choices and having control over daily lives Resident representative individual chosen by resident to act on behalf of resident; person authorized by State or Federal law Review PA Act 169 Right to access medical, social or other personal information of the resident 13
14 483.10(b)(1-4) Changes in Resident Representative Representative has the right to exercise the resident s rights to the extent those rights are properly delegated to them Resident retains those rights not delegated, including the right to revoke a delegation Must treat Representative decisions as decisions of the Resident BUT not beyond what is required by court or delegated by Resident Must report concerns that Representative not acting in best interests of Resident. 14
15 Resident Rights Includes facility responsibilities Resident must receive information in language that he or she can understand about various topics, including medical condition Consider also Section 1557 of Affordable Care Act (ACA): Facility must have policies and procedures (P&Ps) re: visitation rights of resident, including any clinically necessary or reasonable restriction or limitation or safety restriction or limitation when consistent with the regulations 15
16 Resident Rights Facility acts as fiduciary if resident deposits personal funds Reasonable access to electronic communication Advance directives (b)(8) Accommodate needs of LGBT residents and same sex spouses Facility must have a grievance policy and a Grievance Official Must also have a grievance officer under Section 1557 of the ACA 16
17 Resident Grievance Rights Right to voice grievances without discrimination or reprisal and without fear of discrimination or reprisal Includes care and treatment which has been furnished as well as that which has not been furnished Behavior of staff and of other residents Other concerns regarding their stay 17
18 Resident Grievance Rights SNF Duties Make prompt efforts to resolve grievances Provide residents with information on how to file a grievance or complaint Establish a grievance policy to ensure the prompt resolution of all grievances Must give copy of grievance policy to resident upon request 18
19 Grievance Policy Address Resident Rights Notifying resident individually or through postings in prominent locations throughout facility of right to file grievances orally (meaning spoken) or in writing Right to file grievances anonymously Contact information of the grievance official with whom a grievance can be filed Name, business address (mailing and ) and business phone number 19
20 Grievance Policy Address Resident Rights Reasonable expected time frame for completing review of grievance Right to obtain a written decision regarding his or her grievance Contact information of independent entities with whom grievances may be filed 20
21 Grievance Policy Grievance Official Identify a Grievance Official and responsibilities Overseeing the grievance process Receiving and tracking grievances through to their conclusion Leading any necessary investigations Maintaining confidentiality of all information associated with grievances Issuing written grievance decisions to resident Coordinating with state and federal agencies as necessary in light of specific allegations 21
22 Grievance Policy Decisions All written grievance decisions must include: Date the grievance was received Summary statement of the grievance Steps taken to investigate the grievance Summary of pertinent findings or conclusions Statement whether grievance was confirmed or not confirmed Any corrective action taken or to be taken Date the written decision was issued 22
23 Grievance Policy Corrective Action Taking appropriate corrective action in accordance with State law if the alleged violation of the residents rights is confirmed by the facility or if an outside entity having jurisdiction, such as the State Survey Agency, Quality Improvement Organization, or local law enforcement agency confirms a violation of any of these residents rights within its area of responsibility 23
24 Grievance Policy Log Must maintain evidence demonstrating the results of all grievances for a period of no less than 3 years from the issuance of the grievance decision Consider whether to combine RoP Grievance Log with OCR Grievances 24
25 Freedom From Abuse, Neglect, And Exploitation Review P&Ps for consistency with new definitions and requirements Prohibits hiring anyone with a disciplinary action in effect against professional license by a state licensure body as result of a finding of abuse, neglect, exploitation, mistreatment of residents or misappropriation of resident property Impact of Pennsylvania s Protective Services Laws (OAPSA, APSA, CPSL)? 25
26 (c)(1) Freedom From Abuse, Neglect, and Exploitation Note change in reporting timing: In response to allegations of abuse, neglect, exploitation, or mistreatment, the facility must Ensure that all alleged violations involving abuse, neglect, exploitation or mistreatment, including injuries of unknown source and misappropriation of resident property, are reported immediately, but not later than 2 hours after the allegation is made, if the events that cause the allegation involve abuse or result in serious bodily injury, or not later than 24 hours if the events that cause the allegation do not involve abuse and do not result in serious bodily injury, to the administrator of the facility and to other officials (including to the State Survey Agency and adult protective services where state law provides for jurisdiction in longterm care facilities) in accordance with State law through established procedures.
27 Admission, Transfer, And Discharge Rights Heightened emphasis on discharge planning Phase 2 implementation Transfer/Discharge Documentation Establish and implement (or review/revise) admission policy Requires orientation of resident for transfer or discharge to ensure safe and orderly transfer or discharge Review/revise/create written policy on permitting residents to return after hospitalization or therapeutic leave Include specific provisions outlined in regulation 27
28 48-Hour Baseline Care Plan New requirement - Phase 2 Initial set of instructions to facilitate smooth transition of care and to provide effective, person-centered care starting at admission
29 48-Hour Baseline Care Plan Minimum of 6 key elements: Initial goals based on admission orders; All physician orders, including medications and administration schedule; Dietary orders; Therapy services; Social services; and PASARR recommendations, if PASARR completed. Could be replaced by the comprehensive care plan if done within 48 hours of admission.
30 Comprehensive Person - Centered Care Planning Specific information must be included in comprehensive care plan Plan must be developed within 7 days after completion of the comprehensive assessment Requires IDT preparing plan to include Nurse aide with responsibility for the resident Member of food and nutrition services staff If participation of resident and representative in development of plan not practicable, explanation must be in resident s medical record 30
31 Comprehensive Person - Centered Care Planning: Discharge Planning Must focus on discharge goals and residents must be active partners in the planning and transition process Regular re-evaluation and modification of plan Specifies what must be included in the plan and considerations that must be taken in development of the plan 31
32 Discharge Planning Process #1 Required steps Create an IDT which includes the resident Evaluate the resident s discharge potential, goals, and needs Document results of discharge plan Create a discharge plan Update discharge plan Share discharge plan with the resident
33 Discharge Planning Process #1 Prepare resident & their representative for discharge Notify Ombudsman of all discharges and transfers Document reason for discharge or transfer Provide required information to receiving provider Complete a discharge summary
34 Information Accompanying Resident at Discharge or Transfer Ensure specified information is copied and available to go with resident: Contact information of practitioner responsible for care Resident representative information Advance Directive information Special instructions or precautions
35 Information Accompanying Resident at Discharge or Transfer Ensure specified information is copied and available to go with resident: (con t.) Most recent comprehensive care plan goals Resident s discharge summary Other documents as needed Resident s consent to share information Develop checklist to ensure all required information is sent
36 Discharge Summary Template: Phase 1 Requirement Recapitulation of stay (diagnoses, pertinent lab tests and results, course of illness, treatments, therapy) Final summary of resident s status (specified items from comprehensive resident assessment, including needs, strengths, goals, preferences) Medication reconciliation Post-discharge plan of care (where individual will reside, arrangements for follow-up care, consent to share discharge summary) Other elements as determined by facility
37 Quality of Care Quality of care is a fundamental principle that applies to all treatment and care provided to facility residents. Based on the comprehensive assessment of a resident, the facility must ensure that residents receive treatment and care in accordance with professional standards of practice, the comprehensive person centered care plan, and the resident's choices, including but not limited to the following :* Vision & Hearing; Skin Integrity; Mobility; Incontinence; Assisted Nutrition & Hydration; Respiratory Care; * Emphasis supplied Prostheses; Pain Management; Dialysis; Trauma Informed Care; Bed Rails 37
38 Quality of Care Includes care issues that were previously included at F-tag 309 Entire RoP implemented in Phase 1 except trauma-centered care (Phase 3) Very specific requirements on addressing certain conditions Based on the comprehensive assessment of a resident 38
39 Physician Services No requirement for credentialing No requirement for physician visit prior to transfer Allows delegation for writing dietary orders Allows delegation for writing therapy orders Tip: review all physician agreements to require compliance with new pharmacy provisions, as well as Stark Law and Anti-Kickback Statute 39
40 Nursing Services Must have sufficient nursing staff with appropriate competencies and skills sets to assure resident safety and attain maintain highest practicable physical, mental, and psychosocial well-being of each resident Determined by resident assessments Residents individual plans of care Number & acuity & diagnoses of residents Other nursing personnel includes nurse aides 40
41 Behavioral Health Services Based on comprehensive assessment, resident with mental disorder or psychosocial adjustment difficulty receives appropriate treatment and services to correct the problem or attain highest practicable mental and psychosocial well-being Resident with dementia receives treatment & services 41
42 Behavioral Health Services If assessment does not reveal mental or psychosocial adjustment difficulties, no pattern of decreased social interaction and/or increased withdrawn, angry, or depressive behaviors unless clinical condition demonstrates development of such a pattern was unavoidable Must provide medically-related social services for highest practicable well-being Sufficient, competent staff
43 Pharmacy Services Psychotropic drug: any drug that affects brain activities associated with mental processes and behavior; includes but not limited to: Anti-psychotic Anti-depressant Anti-anxiety Hypnotic Drug regimen review & reporting Pharmacist must report irregularities to attending physician, medical director and DON and reports must be acted upon 43
44 Laboratory, Radiology, and Other Diagnostic Services Facility must promptly notify the ordering physician, PA, NP, or clinical nurse specialist of lab results that fall outside of clinical reference ranges in accordance with facility policies and procedures for notification of a practitioner or per the ordering physician s orders Physician extenders can order radiology and other diagnostic services and must be promptly notified of results falling outside of clinical reference ranges in accordance with facility policies and procedures 44
45 Dental Services Note new requirements for replacement of lost dentures within 3 days Phase 2 implementation 45
46 Food & Nutrition Services Sufficient and competent staff New education requirements for dietitian and food service manager Must make reasonable efforts to address religious, cultural and ethnic needs Policy for use and storage of foods brought to residents by family and visitors 46
47 Resident/Facility Assessment (Nursing Services) - The facility must have sufficient nursing staff with the appropriate competencies and skills sets to provide nursing and related services to assure resident safety and attain or maintain the highest practicable physical, mental, and psychosocial well-being of each resident, as determined by resident assessments and individual plans of care and considering the number, acuity and diagnoses of the facility s resident population in accordance with the facility assessment required at (e).
48 Resident/Facility Assessment (e) Facility assessment. The facility must conduct and document a facility wide assessment to determine what resources are necessary to care for its residents competently during both day to- day operations and emergencies. The facility must review and update that assessment, as necessary, and at least annually. The facility must also review and update this assessment whenever there is, or the facility plans for, any change that would require a substantial modification to any part of this assessment. The facility assessment must address or include: [resident population, facility resources, and a facility and community based risk assessment, utilizing an all hazards approach.
49 Administration Facility assessment implemented in Phase 2 but should start reviewing now Requires full time social worker for >120 beds Incorporates recent regulations (facility closure, hospice, payroll based journal) 49
50 Quality Assurance and Performance Improvement QA&A committee all provisions except the inclusion of the infection prevention control officer in Phase 1 State may not require disclosure of the records of the committee except related to requirements of the committee (e.g., who is on committee; that committee meets as required; etc.) Good faith attempts by the committee to identify and correct quality deficiencies will not be used as a basis for sanctions Most QAPI requirements in Phase 2 50
51 Infection Control Infection prevention and control program Written standards, policies, and procedures for the program including specified topics Consider relation to current Infection Control Plan already required by Pennsylvania [community representative] Annual review of the infection prevention and control program and update as necessary Antibiotic stewardship Phase 2 Infection Control Preventionist- Phase 3 Flu & pneumonia vaccines 51
52 Compliance & Ethics Program Written standards for compliance and clear reporting path for suspected violations of compliance and ethics Designate a compliance and ethics contact Identify a high level person to oversee the program Sufficient resources and authority to oversee compliance Regulations have conflicting implementation dates CMS is aware and will be issuing clarification Not a Phase 1 issue 52
53 Compliance & Ethics Program Effective communication of compliance standards to all staff Audit and monitoring system Publicize a reporting system Annual review of program and its efficacy Consistent enforcement through appropriate disciplinary action Mandatory annual training on compliance & ethics Designate Compliance liaisons in each facility (>5)
54 Physical Environment After Nov. 28, 2016, for any facility newly certified or approved for construction/major renovation Each resident room must have its own bathroom with at least a commode and sink Two residents to room Smoking policies Phase 2 Resident call next to bed Phase 3 54
55 Training Requirements Training program for all new and existing staff, individuals providing services under a contractual arrangement and volunteers, consistent with their expected role Abuse, neglect and exploitation In-service training for nurse aides Must include dementia management training and resident abuse prevention training If providing care for individuals with cognitive impairment, training on care of the cognitively impaired 55


56 Increased Enforcement a Reality Marked increase in citations and sanctions Marked increase in CMS & DOH civil money penalties 56
57 Federal Civil Penalties Inflation Adjustment Act Improvements Act of 2015 Intended to improve effectiveness of CMPs and maintain deterrent effect of CMPs Requires annual adjustment of CMPs using October Consumer Price Index for all Urban Consumers (CPI-U) First increase was in 2016; most recent increase effective February 3, 2017 (82 Fed. Reg. 9174, 2/3/2017)
58 Federal Civil Penalties Inflation Adjustment Act Improvements Act of 2015 Secretary of covered agency may provide lesser CMP by less than the new formula through a rulemaking only if: Secretary finds that increasing penalty by required amount will have a negative economic impact or that the social costs outweigh the benefits and Director of the Office of Management and Budget (OMB) concurs with this analysis 58
59 Impact of Inflation Adjustment Act CMS CMPs for surveys have increased astronomically Pre-August 2016 August 1, 2016 Cat.2 Per Day $50 -$3,000 $103 - $6,188 Cat. 2 Per Instance $1,000 - $10,000 Cat. 3 Per Day $3,050 - $10,000 Cat. 3 Per Instance $1,000 - $10,000 $2,063 $20,628 $6,291 - $20,628 $2,063 $20,628 February 3, 2017 $105 $6,289 $2,097 - $20,965 $6,394 - $20,955 $2,097 - $20,965
60 Federal Scope and Severity Grid I Immediate Jeopardy To Resident Health Or Safety Actual Harm That Is Not Immediate Jeopardy Isolated Pattern PoC J Required: Cat. 3 Optional: Cat. 1 Optional: Cat. 2 PoC G Required: Cat. 2 Optional: Cat. 1 PoC K Required: Cat. 3 Optional: Cat. 1 Optional: Cat. 2 PoC H Required: Cat. 2 Optional: Cat. 1 Widespread PoC L Required: Cat. 3 Optional: Cat. 1 Optional: Cat. 2 PoC I Required: Cat. 2 Optional: Cat. 1 Optional: Temporary Mgmt No Actual Harm With Potential For More Than Minimal Harm That Is Not Immediate Jeopardy PoC D Required: Cat. 1 Optional: Cat. 2 PoC E Required: Cat. 1 Optional: Cat. 2 PoC F Required: Cat. 2 Optional: Cat. 1 No Actual Harm With Potential For Minimal Harm Substandard Quality of Care (F ; F ; F ) No PoC No remedies Commitment to Correct Not on CMS-2567 A PoC B No remedies PoC C No remedies Out of Compliance Substantial Compliance 60
61 Federal Remedies Categories Category 1 (Cat.1) Category 2 (Cat.2) Category 3 (Cat.3) Directed Plan of Correction; State Monitor; and/or Directed In-Service Training Note: If CMP >$10,4830 or SQC, automatic loss of Nurse Aide Training Competency Evaluation Program (NATCEP) Denial of Payment for New Admissions; Denial of Payment for All Individuals imposed by CMS; Termination; Temp. Mgmt and/or Civil Money Penalties: Old: $50 - $3,000/day $1,000 - $10,000/ instance New: * $105 - $6,289/day $2,097 - $20,628/ instance Temp. Mgmt.; Termination; Civil money penalties Old: 3,050-$10,000/day $1,000 - $10,000/ instance New:* $6,394 - $20,965/day $2,097 - $20,965/ instance * Updated effective Feb. 3,
62 Areas of Potential Substandard Quality Of Care Major Expansion Resident Rights Resident Rights Exercise of Rights Respect and Dignity Self-Determination Safe Environment F Tags F F F
63 Pennsylvania Nursing Care Facility Sanctions P1 & CP P2 & CP P1 Only P2 Only P3 Only P4 Only BAN CP Only Amount Imposed $62, $176, $401, Jan $284,250.00

64 DOH CP Guideline 64

65 Immediate Jeopardy Citations
66 State IDR v. IIDR Tags Disputed Deleted Revised Upheld Withdrawn 2013 IDR 69 19% (13) 7% (5) 72% (50) IIDR % (1) 86% (12) 7% (1) 2014 IDR 60 15% (9) 20% (12) 63% (38) 2% (1) 2014 IIDR 24 25% (6) 0 75% (18) IDR % (33) 11% (15) 63% (82) 1% (1) 2015 IIDR 30 20% (6) 10% (3) 70% (21) 0 Jan-Oct IDR % (47) 11% (18) 60% (104) 2% (3) Jan-Oct IIDR 42 17% (7) 7% (3) 69% (29) 7% (3)
67 New CMS CMP Analytic Tool New approach to federal per day (PD) Civil Money Penalties (CMPs) Begin CMP on 1 st day noncompliance is documented, even if that date precedes the first day of the current survey Unless facility can demonstrate that it corrected the noncompliance prior to the current survey (past noncompliance) CMS Survey & Certification Memo, Civil Money Penalty (CMP) Analytic Tool and Submission of CMP Tool Cases, S&C: NH (Dec. 19, 2014) 67
68 Starting the PD CMP Calculate the start date for the proposed CMP with the first supportable date of noncompliance, as determined by the evidence documented by surveyors in the statement of deficiencies (CMS form 2567) Surveyors instructed to determine the earliest date for which supportable evidence shows that the non-compliant practice began 68
69 Ambiguity About Start of Deficient Practice CMS analysts will contact state agency if start date is ambiguous or not clearly identified and supportable, to see if start date can be determined CMS analysts required to document their discussions and conclusion with the state agency 69
70 If Start Date Not Determinable If start date cannot be determined, then PD CMP would start on 1 st day during the survey on which the survey team identified the noncompliant practice If the team cannot document the first day of noncompliance, then the CMP should start on the day the noncompliance was observed and documented at the time of the current survey 70
71 CMS: Past Noncompliance Reduce a CMP by 50% if: (i) self-reported noncompliance to CMS or State before it was otherwise identified by or reported to CMS or State; and (ii) correction of the self-reported noncompliance occurred within 15 days of the incident. 42 C.F.R
72 Get Credit for Correcting Past Noncompliance Treat any incident that results in reporting to DOH as you would if it was on your 2567 Develop corrective action and document monitoring and auditing for ongoing compliance Give evidence to surveyors at the time of the survey that a monitoring plan was implemented and maintained to assure continued compliance.
73 Survey Strategy Reevaluate how you approach survey Surveyors may reject any documents not provided at time of survey Where are your critical documents What do your medical records look like How up to date is your filing Review 2567 carefully and prepare IDRs for any factual inaccuracies 73
74 Questions Paula G. Sanders, Esquire Principal & Co-Chair, Health Care Practice Group Post & Schell, PC
Get Ready for Phase 1 of the New Requirements of Participation
 Pennsylvania Health Care Association November 7, 2016 Get Ready for Phase 1 of the New Requirements of Participation Paula G. Sanders, Esquire Post & Schell, P.C. Gail Weidman Dawn Murr-Davidson Pennsylvania
Pennsylvania Health Care Association November 7, 2016 Get Ready for Phase 1 of the New Requirements of Participation Paula G. Sanders, Esquire Post & Schell, P.C. Gail Weidman Dawn Murr-Davidson Pennsylvania
The New Survey Process What To Expect Paula G. Sanders, Esq.
 PHCA Webinar February 14, 2018 The New Survey Process What To Expect Paula G. Sanders, Esq. DEPARTMENT OF HEALTH ENFORCEMENT TRENDS How to Read State Tags DOH CMPs Per Year 2014-2017 2014 $79,250.00 2015
PHCA Webinar February 14, 2018 The New Survey Process What To Expect Paula G. Sanders, Esq. DEPARTMENT OF HEALTH ENFORCEMENT TRENDS How to Read State Tags DOH CMPs Per Year 2014-2017 2014 $79,250.00 2015
CMS and DOH Enforcement Activities and Proactive Strategies
 PACAH 2017 Spring Conference April 27, 2017 CMS and DOH Enforcement Activities and Proactive Strategies Paula G. Sanders, Esquire CMS Requirements of Participation (RoPs) Published October 4, 2016 (81
PACAH 2017 Spring Conference April 27, 2017 CMS and DOH Enforcement Activities and Proactive Strategies Paula G. Sanders, Esquire CMS Requirements of Participation (RoPs) Published October 4, 2016 (81
The Updated CMS Nursing Facility Regulations
 The Updated CMS Nursing Facility Regulations NHELP Conference December 5, 2016 Lori Smetanka, Consumer Voice Toby Edelman, Center for Medicare Advocacy Objectives Understand the important changes made
The Updated CMS Nursing Facility Regulations NHELP Conference December 5, 2016 Lori Smetanka, Consumer Voice Toby Edelman, Center for Medicare Advocacy Objectives Understand the important changes made
Find Your Purpose with the Phase 2 Regulations!
 Find Your Purpose with the Phase 2 Regulations! The New MegaRule! MONTANA HOSPITAL ASSOCIATION OVERVIEW OF PHASE 2 REQUIREMENTS WWW.PATHWAYHEALTH.COM Objectives Understand the new and revised final rule
Find Your Purpose with the Phase 2 Regulations! The New MegaRule! MONTANA HOSPITAL ASSOCIATION OVERVIEW OF PHASE 2 REQUIREMENTS WWW.PATHWAYHEALTH.COM Objectives Understand the new and revised final rule
Federal Requirements of Participation for Nursing Homes Summary of Key Changes in the Final Rule Issued September 2016 Phase 2
 Federal Requirements of Participation for Nursing Homes Summary of Key Changes in the Final Rule Issued September 2016 Phase 2 On September 28, 2016, the Centers for Medicare & Medicaid Services (CMS)
Federal Requirements of Participation for Nursing Homes Summary of Key Changes in the Final Rule Issued September 2016 Phase 2 On September 28, 2016, the Centers for Medicare & Medicaid Services (CMS)
Final Rule to Reform the Requirements for Long-Term Care Facilities
 Final Rule to Reform the Requirements for Long-Term Care Facilities Karen Tritz Division of Nursing Homes Director Clinical Standards Group Long-Term Care Team Survey & Certification Group Division of
Final Rule to Reform the Requirements for Long-Term Care Facilities Karen Tritz Division of Nursing Homes Director Clinical Standards Group Long-Term Care Team Survey & Certification Group Division of
An Overview of the new LTCF Requirements of Participation: Are You Ready?
 An Overview of the new LTCF Requirements of Participation: Are You Ready? David Gifford MD MPH Sr VP for Quality & Regulatory Affairs Feb 9 th 2017 3:15 pm 4:45 pm Boise ID CMS Changes to SNF Regs New
An Overview of the new LTCF Requirements of Participation: Are You Ready? David Gifford MD MPH Sr VP for Quality & Regulatory Affairs Feb 9 th 2017 3:15 pm 4:45 pm Boise ID CMS Changes to SNF Regs New
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care
 Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
The RoPs are here! Do you know what s changing?
 The RoPs are here! Do you know what s changing? Mary Madison, RN, RAC-CT, CDP Clinical Consultant, LTC/Senior Care Briggs Healthcare March 7, 2017 2 What we ll cover today CMS goals behind the updated
The RoPs are here! Do you know what s changing? Mary Madison, RN, RAC-CT, CDP Clinical Consultant, LTC/Senior Care Briggs Healthcare March 7, 2017 2 What we ll cover today CMS goals behind the updated
PACAH 2018 SPRING CONFERENCE April 26, 2018
 PACAH 2018 SPRING CONFERENCE April 26, 2018 Presented by Tanya Daniels Harris, Esq. 2018 LATSHA DAVIS & McKENNA, P.C. 2 OVERVIEW OF RECENT SURVEY AND ENFORCEMENT ISSUES Performance Audit of DOH Regulation
PACAH 2018 SPRING CONFERENCE April 26, 2018 Presented by Tanya Daniels Harris, Esq. 2018 LATSHA DAVIS & McKENNA, P.C. 2 OVERVIEW OF RECENT SURVEY AND ENFORCEMENT ISSUES Performance Audit of DOH Regulation
4/3/2018. Nursing Facility Changes to Conditions of Participation (& Enforcement): What You Need to Know. Revisions to State Operations Manual
: What You Need to Know. Revisions to State Operations Manual") DAVIS, BROWN, KOEHN, SHORS & ROBERTS, 1P.C. Nursing Facility Changes to Conditions of Participation (& Enforcement): What You Need to Know Lynn Böes and Ken Watkins 2 Revisions to State Operations Manual
DAVIS, BROWN, KOEHN, SHORS & ROBERTS, 1P.C. Nursing Facility Changes to Conditions of Participation (& Enforcement): What You Need to Know Lynn Böes and Ken Watkins 2 Revisions to State Operations Manual
3/27/2017. SNF Requirements for Participation. Objectives. New Rules to Live By RoP Changes for 2017 and Beyond Sunday, April 2, :30 5:30pm
 Disclosure of Commercial Interest Commercial Interest Employed by a consulting organization Name of Employer Pathway Health, Inc. Title Director of Quality and Government Services Description Pathway Health
Disclosure of Commercial Interest Commercial Interest Employed by a consulting organization Name of Employer Pathway Health, Inc. Title Director of Quality and Government Services Description Pathway Health
CMS Final Rule: The Good, the Bad and the Ugly. Live Webinar Wednesday, February 8, :00 p.m. ET
 CMS Final Rule: The Good, the Bad and the Ugly Live Webinar Wednesday, February 8, 2017 1:00 p.m. ET Q+A Submit a question below the slides Resources List To the right of the slides. Download presentation
CMS Final Rule: The Good, the Bad and the Ugly Live Webinar Wednesday, February 8, 2017 1:00 p.m. ET Q+A Submit a question below the slides Resources List To the right of the slides. Download presentation
Phase 2: 4/24/2017. Implementation Phases. Objectives. Phase 1: November 28, Phase 3: November 28, 2019
 NEW Requirements for Participation for Skilled Nursing Facilities The Elements of Compliance for Phase 2 April 28, 2017 1:30pm 2:45pm Objectives Identify the new and revised regulations in the Final Rule
NEW Requirements for Participation for Skilled Nursing Facilities The Elements of Compliance for Phase 2 April 28, 2017 1:30pm 2:45pm Objectives Identify the new and revised regulations in the Final Rule
Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities Proposed Rule
 Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities Proposed Rule Summary of Major Provisions Summary adapted from Proposed Rule (with AHCA Comments) July 14, 2015 Updates
Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities Proposed Rule Summary of Major Provisions Summary adapted from Proposed Rule (with AHCA Comments) July 14, 2015 Updates
Reviewing regulatory requirements for top ten federal Nursing Home Tags issued in Minnesota. Eva Loch, MDH Nursing Evaluator
 Reviewing regulatory requirements for top ten federal Nursing Home Tags issued in Minnesota. Eva Loch, MDH Nursing Evaluator F282- Comprehensive Care Plans Regulatory language (SOM): 483.21(b)(3) Comprehensive
Reviewing regulatory requirements for top ten federal Nursing Home Tags issued in Minnesota. Eva Loch, MDH Nursing Evaluator F282- Comprehensive Care Plans Regulatory language (SOM): 483.21(b)(3) Comprehensive
Managing employees include: Organizational structures include: Note:
 Nursing Home Transparency Provisions in the Patient Protection and Affordable Care Act Compiled by NCCNHR: The National Consumer Voice for Quality Long-Term Care, April 2010 Part I Improving Transparency
Nursing Home Transparency Provisions in the Patient Protection and Affordable Care Act Compiled by NCCNHR: The National Consumer Voice for Quality Long-Term Care, April 2010 Part I Improving Transparency
CMS REVISED RULES OF PARTICIPATION
 CMS REVISED RULES OF PARTICIPATION Webinar #3 December 1, 2016 Rebecca J. Bartle, RN, MSN, HFA Hoosier Owners and Providers for the Elderly Ref: S&C 17-07-NH (11/9/16) Centers for Medicare and Medicaid
CMS REVISED RULES OF PARTICIPATION Webinar #3 December 1, 2016 Rebecca J. Bartle, RN, MSN, HFA Hoosier Owners and Providers for the Elderly Ref: S&C 17-07-NH (11/9/16) Centers for Medicare and Medicaid
CMS Requirements of Participation
 CMS Requirements of Participation Goals Reflect substantial changes in theory, service delivery and improvements Address requirements of Affordable Care Act Align with current HHS quality initiatives Reduce
CMS Requirements of Participation Goals Reflect substantial changes in theory, service delivery and improvements Address requirements of Affordable Care Act Align with current HHS quality initiatives Reduce
Writing a Plan of Correction
 Writing a Plan of Correction for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: 3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607 800.275.6252 www.polaris-group.com Writing
Writing a Plan of Correction for clients of: www.teamtsi.com 800.765.8998 Content developed and presented by: 3030 N. Rocky Point Drive, Suite 240 Tampa, FL 33607 800.275.6252 www.polaris-group.com Writing
Center for Clinical Standards and Quality/Survey & Certification Group
 DRAFT DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2 21 16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
DRAFT DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2 21 16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
The Changing Role of Physicians in LTCF
 The Changing Role of Physicians in LTCF David Gifford MD MPH Boise ID Feb 9 th, 2017 CMS Changes to SNF Regs New rule makes extensive changes to SNF Requirements of Participation (RoP) Last major update
The Changing Role of Physicians in LTCF David Gifford MD MPH Boise ID Feb 9 th, 2017 CMS Changes to SNF Regs New rule makes extensive changes to SNF Requirements of Participation (RoP) Last major update
Caring in the Carolinas 11/5/2016
 The Mega Rule: Reform of Requirements for Long- Term Care Facilities Robert Smith, Pharm D, BCPS, CGP, FASCP Director of Clinical Services Neil Medical Group Disclosures I have no conflicts of interest
The Mega Rule: Reform of Requirements for Long- Term Care Facilities Robert Smith, Pharm D, BCPS, CGP, FASCP Director of Clinical Services Neil Medical Group Disclosures I have no conflicts of interest
CMS PROPOSED REVISIONS OF THE NURSING HOME REGULATIONS
 We are almost done here for the day! CMS PROPOSED REVISIONS OF THE NURSING HOME REGULATIONS SNF Regulatory Day September 17, 2015 CMS s Major Initiatives Reduce unnecessary readmissions Reduce Healthcare
We are almost done here for the day! CMS PROPOSED REVISIONS OF THE NURSING HOME REGULATIONS SNF Regulatory Day September 17, 2015 CMS s Major Initiatives Reduce unnecessary readmissions Reduce Healthcare
Overview of New Federal Nursing Facility Regulations * What s happened? When are the new regs effective?
 Overview of New Federal Nursing Facility Regulations * Alison Hirschel (Grand Blanc) Director & Managing Attorney, Michigan Elder Justice Initiative Salli Pung (Rochester Hills) State Long Term Care Ombudsman
Overview of New Federal Nursing Facility Regulations * Alison Hirschel (Grand Blanc) Director & Managing Attorney, Michigan Elder Justice Initiative Salli Pung (Rochester Hills) State Long Term Care Ombudsman
CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW
 CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-242-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-242-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
(a) Licensure. A facility must be licensed under applicable State and local law.
 Licensure. A facility must be licensed under applicable State and local law.") 42 C.F.R. 483.705. Administration. A facility must be administered in a manner that enables it to use its resources effectively and efficiently to attain or maintain the highest practicable physical, mental,
42 C.F.R. 483.705. Administration. A facility must be administered in a manner that enables it to use its resources effectively and efficiently to attain or maintain the highest practicable physical, mental,
Tag Description Page. F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125. F622 Transfer & Discharge 155
 Tag Description Page F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125 F622 Transfer & Discharge 155 F626 Permitting Residents to Return to Facility 170 F656 Comprehensive Care Plans
Tag Description Page F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125 F622 Transfer & Discharge 155 F626 Permitting Residents to Return to Facility 170 F656 Comprehensive Care Plans
Prepublication Requirements
 Prepublication Requirements Standards Revisions for Swing Bed Final Rule in Critical Access Hospitals The Joint Commission has approved the following revisions for prepublication. While revised requirements
Prepublication Requirements Standards Revisions for Swing Bed Final Rule in Critical Access Hospitals The Joint Commission has approved the following revisions for prepublication. While revised requirements
Health Care Reform (Affordable Care Act) Leadership Summit April 26, 2010 Cindy Graunke
 Leadership Summit April 26, 2010 Cindy Graunke") Health Care Reform (Affordable Care Act) Leadership Summit April 26, 2010 Cindy Graunke 2 Contents Transparency Disclosure of Ownership Nursing Home Compare Reporting of Staffing Notice of Facility Closure
Health Care Reform (Affordable Care Act) Leadership Summit April 26, 2010 Cindy Graunke 2 Contents Transparency Disclosure of Ownership Nursing Home Compare Reporting of Staffing Notice of Facility Closure
Transfer and Discharge Issues 4/6/2017. How the Mega Rule Affects (and Will Affect) What You Do Every Day
 What You Do Every Day") How the Mega Rule Affects (and Will Affect) What You Do Every Day Rick E. Harris Of Counsel Starnes Davis Florie LLP Birmingham, AL October 27, 2016 What We Are Going to Discuss 1. 2. Admission Issues
How the Mega Rule Affects (and Will Affect) What You Do Every Day Rick E. Harris Of Counsel Starnes Davis Florie LLP Birmingham, AL October 27, 2016 What We Are Going to Discuss 1. 2. Admission Issues
Grievances and Resident/Family Councils
 A Closer Look at the Revised Nursing Facility Regulations Grievances and Resident/Family Councils Executive Summary Residents have the right to file grievances and the facility must work to resolve those
A Closer Look at the Revised Nursing Facility Regulations Grievances and Resident/Family Councils Executive Summary Residents have the right to file grievances and the facility must work to resolve those
Highlights of the New LTCSP and Regulations
 Highlights of the New LTCSP and Regulations New York State Department of Health Division of Nursing Homes and ICF/IID Surveillance November 15, 2017 November 15, 2017 2 Resources https://www.cms.gov/medicare/provider-enrollment-andcertification/guidanceforlawsandregulations/nursinghomes.html
Highlights of the New LTCSP and Regulations New York State Department of Health Division of Nursing Homes and ICF/IID Surveillance November 15, 2017 November 15, 2017 2 Resources https://www.cms.gov/medicare/provider-enrollment-andcertification/guidanceforlawsandregulations/nursinghomes.html
Subpart C Conditions of Participation PATIENT CARE Condition of participation: Patient's rights Condition of participation: Initial
 Subpart C Conditions of Participation PATIENT CARE 418.52 Condition of participation: Patient's rights. 418.54 Condition of participation: Initial and comprehensive assessment of the patient. 418.56 Condition
Subpart C Conditions of Participation PATIENT CARE 418.52 Condition of participation: Patient's rights. 418.54 Condition of participation: Initial and comprehensive assessment of the patient. 418.56 Condition
CMS Mega Rule: Implications for Pharmacists and Pharmacies
 CMS Mega Rule: Implications for Pharmacists and Pharmacies Curt Wood, RPh, BCGP, FASCP Disclosure and Conflict of Interest Curt Wood declares no conflicts of interest, real or apparent, and no financial
CMS Mega Rule: Implications for Pharmacists and Pharmacies Curt Wood, RPh, BCGP, FASCP Disclosure and Conflict of Interest Curt Wood declares no conflicts of interest, real or apparent, and no financial
Pub State Operations Provider Certification Transmittal- ADVANCE COPY
 CMS Manual System Pub. 100-07 State Operations Provider Certification Transmittal- AVANCE COPY epartment of Health & Human Services (HHS) Centers for Medicare & Medicaid Services (CMS) ate: XXXX SUBJECT:
CMS Manual System Pub. 100-07 State Operations Provider Certification Transmittal- AVANCE COPY epartment of Health & Human Services (HHS) Centers for Medicare & Medicaid Services (CMS) ate: XXXX SUBJECT:
Minnesota Hospice Bill of Rights PER MINNESOTA STATUTES, SECTION 144A.751
 Combined Minnesota & Federal Hospice Bill of Rights Minnesota Hospice Bill of Rights PER MINNESOTA STATUTES, SECTION 144A.751 The language in BOLD print represents additional consumer rights under federal
Combined Minnesota & Federal Hospice Bill of Rights Minnesota Hospice Bill of Rights PER MINNESOTA STATUTES, SECTION 144A.751 The language in BOLD print represents additional consumer rights under federal
Goodbye Grace Period. What will be expected from your Facility Assessment in the Coming Year. Ellen Kuebrich Chief Strategy Officer, Providigm
 Goodbye Grace Period What will be expected from your Facility Assessment in the Coming Year Ellen Kuebrich Chief Strategy Officer, Providigm Final Rule Final Rule Effective Date These regulations are effective
Goodbye Grace Period What will be expected from your Facility Assessment in the Coming Year Ellen Kuebrich Chief Strategy Officer, Providigm Final Rule Final Rule Effective Date These regulations are effective
G-TAGS A RE T HEY THE N EW IJ S?
 G-TAGS A RE T HEY THE N EW IJ S? LIBBY YOUSE, LNHA LONG TERM CARE LEADERSHIP COACH QIPMO SINCLAIR SCHOOL OF NURSING UNIVERSITY OF MISSOURI WHY TAKE A LOOK AT G TAGS November of 2016 brought in Phase I
G-TAGS A RE T HEY THE N EW IJ S? LIBBY YOUSE, LNHA LONG TERM CARE LEADERSHIP COACH QIPMO SINCLAIR SCHOOL OF NURSING UNIVERSITY OF MISSOURI WHY TAKE A LOOK AT G TAGS November of 2016 brought in Phase I
The Impact on Compliance
 Highlights of the CMS Final Rule: The Impact on Compliance 21 st Annual Compliance Institute March 27, 2017 Presenters: Kris D Ann Maples and Lyn Bentley Kris D Ann Maples, Esq. 19 years in Healthcare
Highlights of the CMS Final Rule: The Impact on Compliance 21 st Annual Compliance Institute March 27, 2017 Presenters: Kris D Ann Maples and Lyn Bentley Kris D Ann Maples, Esq. 19 years in Healthcare
NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017
 NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017 Disclaimer: The information contained in this presentation is representative of the current information provided
NEW LONG TERM CARE SURVEY PROCESS PHASE 2 REQUIREMENTS OF PARTICIPATION AUGUST 23, 2017 Disclaimer: The information contained in this presentation is representative of the current information provided
Rules of Participation, Phase 1 Review
 1 Rules of Participation, Phase 1 Review A Foundation check to launch Phase 2 from Presented by: Anabelle Locsin, RN, Ed.D., RAC-CT, LNC Quality Improvement Consultant PROGRAM OVERVIEW 2 This program was
1 Rules of Participation, Phase 1 Review A Foundation check to launch Phase 2 from Presented by: Anabelle Locsin, RN, Ed.D., RAC-CT, LNC Quality Improvement Consultant PROGRAM OVERVIEW 2 This program was
The CMS State Operations Manual Overview and Changes
 The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
Neglect Critical Element Pathway
 Use this pathway for concerns in structures or processes that have led to resident outcome such as unrelieved pain, avoidable pressure injuries, poor grooming, avoidable dehydration, lack of continence
Use this pathway for concerns in structures or processes that have led to resident outcome such as unrelieved pain, avoidable pressure injuries, poor grooming, avoidable dehydration, lack of continence
Annual Quality Improvement Report: The Nursing Home Survey Process REPORT TO THE MINNESOTA LEGISLATURE FOR FEDERAL FISCAL YEAR 2014
 Annual Quality Improvement Report: The Nursing Home Survey Process REPORT TO THE MINNESOTA LEGISLATURE FOR FEDERAL FISCAL YEAR 2014 HEALTH REGULATION DIVISION Annual Quality Improvement Report: The Nursing
Annual Quality Improvement Report: The Nursing Home Survey Process REPORT TO THE MINNESOTA LEGISLATURE FOR FEDERAL FISCAL YEAR 2014 HEALTH REGULATION DIVISION Annual Quality Improvement Report: The Nursing
3/6/2017. CMS nursing home requirements have not been comprehensively updated since 1991 despite significant changes in the industry.
 Debra Brown, PharmD Pharmaceutical Consultant II Specialist Licensing and Certification QCHF/CAHF Spring Legislative Conference March 2017 1 Describe impact of 2016 CMS Final Rule on SNF pharmacy services
Debra Brown, PharmD Pharmaceutical Consultant II Specialist Licensing and Certification QCHF/CAHF Spring Legislative Conference March 2017 1 Describe impact of 2016 CMS Final Rule on SNF pharmacy services
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care
 Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
WhWwhaht. SNF CMS, RoP, Survey, and Regulatory Update October /25/2017. The New and Improved Survey Process
 303 Cleveland Avenue SE Suite 206 Tumwater, WA 98501 Tel 800 562 6170 www.whca.org SNF CMS, RoP, Survey, and Regulatory Update October 2017 Elena Madrid Director of Regulatory Affairs The New and Improved
303 Cleveland Avenue SE Suite 206 Tumwater, WA 98501 Tel 800 562 6170 www.whca.org SNF CMS, RoP, Survey, and Regulatory Update October 2017 Elena Madrid Director of Regulatory Affairs The New and Improved
IMPORTANT NOTICE PLEASE READ CAREFULLY SENT VIA FEDEX AND INTERNET (Receipt of this notice is presumed to be May 7, 2018 date notice ed)
") Department of Health & Human Services Centers for Medicare & Medicaid Services 61 Forsyth Street, SW, Suite 4T20 Atlanta, Georgia 30303-8909 ` Refer to: 34-5529.NOTC.G.05.07.18.docx IMPORTANT NOTICE PLEASE
Department of Health & Human Services Centers for Medicare & Medicaid Services 61 Forsyth Street, SW, Suite 4T20 Atlanta, Georgia 30303-8909 ` Refer to: 34-5529.NOTC.G.05.07.18.docx IMPORTANT NOTICE PLEASE
9/8/2017. Making the Connection: Linking the Facility Assessment and QAPI Plan. Cindy Mason VP Provider Services. Final Rule. Providigm, LLC,
 Making the Connection: Linking the Facility Assessment and QAPI Plan Cindy Mason VP Provider Services Final Rule Providigm, LLC, 2017 1 Final Rule Effective Date These regulations are effective as of November
Making the Connection: Linking the Facility Assessment and QAPI Plan Cindy Mason VP Provider Services Final Rule Providigm, LLC, 2017 1 Final Rule Effective Date These regulations are effective as of November
What to Expect on Your Next Survey
 What to Expect on Your Next Survey Linda M. Elizaitis RN, BS, RAC-CT President CMS Compliance Group, Inc. E. lmelizaitis@cmscg.net T. 631.692.4422 cmscompliancegroup.com @lindaelizaitis @cmscompliance
What to Expect on Your Next Survey Linda M. Elizaitis RN, BS, RAC-CT President CMS Compliance Group, Inc. E. lmelizaitis@cmscg.net T. 631.692.4422 cmscompliancegroup.com @lindaelizaitis @cmscompliance
Informal Dispute Resolution and Independent Informal Dispute Resolution Key Elements and Updates
 Informal Dispute Resolution and Independent Informal Dispute Resolution Key Elements and Updates Charlene Kawchak-Belitsky, R.N., BSN, NHA Senior manager, IDR/IIDR, MPRO Presented to LeadingAge Michigan
Informal Dispute Resolution and Independent Informal Dispute Resolution Key Elements and Updates Charlene Kawchak-Belitsky, R.N., BSN, NHA Senior manager, IDR/IIDR, MPRO Presented to LeadingAge Michigan
Center for Medicare and Medicaid Services (CMS) REQUIREMENTS OF PARTICIPATION Final Rule for Nursing Homes September LeadingAge Provider Summary
 REQUIREMENTS OF PARTICIPATION Final Rule for Nursing Homes September LeadingAge Provider Summary") Center for Medicare and Medicaid Services (CMS) REQUIREMENTS OF PARTICIPATION Final Rule for Nursing Homes September 2016 LeadingAge Provider Summary Background: The new Requirements of Participation for
Center for Medicare and Medicaid Services (CMS) REQUIREMENTS OF PARTICIPATION Final Rule for Nursing Homes September 2016 LeadingAge Provider Summary Background: The new Requirements of Participation for
Hospice Care in the Nursing Home: The New Interpretive Guidelines for NF Surveyors
 Hospice Care in the Nursing Home: The New Interpretive Guidelines for NF Surveyors Subscriber Webinar The Plan 1. Brief Look: The Hospice Nursing Home Partnership 2. Brief Look: The Nursing Home Survey
Hospice Care in the Nursing Home: The New Interpretive Guidelines for NF Surveyors Subscriber Webinar The Plan 1. Brief Look: The Hospice Nursing Home Partnership 2. Brief Look: The Nursing Home Survey
HOME HEALTH CARE PROPOSED CONDITIONS OF PARTICIPATION
 HOME HEALTH CARE PROPOSED CONDITIONS OF PARTICIPATION Mary Carr, BSN,MPH V.P. for Regulatory Affairs National Association for Home Care & Hospice October 19, 2014 Proposed rule HH COPS Federal Register
HOME HEALTH CARE PROPOSED CONDITIONS OF PARTICIPATION Mary Carr, BSN,MPH V.P. for Regulatory Affairs National Association for Home Care & Hospice October 19, 2014 Proposed rule HH COPS Federal Register
THE BIG PICTURE. The Impact of Survey In THE SURVEY & ENFORCEMENT SESSION: WHAT HAS CHANGED? OHCA Annual Convention/April 29, 2015
 THE SURVEY & ENFORCEMENT SESSION: WHAT HAS CHANGED? OHCA Annual Convention/April 29, 2015 Carol Rolf Christopher M. Tost Rolf Goffman Martin Lang LLP THE BIG PICTURE The Impact of Survey In 2015 Reputation
THE SURVEY & ENFORCEMENT SESSION: WHAT HAS CHANGED? OHCA Annual Convention/April 29, 2015 Carol Rolf Christopher M. Tost Rolf Goffman Martin Lang LLP THE BIG PICTURE The Impact of Survey In 2015 Reputation
IMPORTANT NOTICE PLEASE READ CAREFULLY SENT VIA FEDEX AND INTERNET
 Department of Health & Human Services Centers for Medicare & Medicaid Services 61 Forsyth Street, SW, Suite 4T20 Atlanta, Georgia 30303-8909 Refer to: 5213.abIJ.06.27.18. docx ` June 27, 2018 IMPORTANT
Department of Health & Human Services Centers for Medicare & Medicaid Services 61 Forsyth Street, SW, Suite 4T20 Atlanta, Georgia 30303-8909 Refer to: 5213.abIJ.06.27.18. docx ` June 27, 2018 IMPORTANT
DEFINITIONS (c)(1) Discharge Planning : Home Health Agency (HHA) : Inpatient Rehabilitation Facility (IRF) : Local Contact Agency :
(1) Discharge Planning : Home Health Agency (HHA) : Inpatient Rehabilitation Facility (IRF) : Local Contact Agency :") F660 483.21(c)(1) Discharge Planning Process The facility must develop and implement an effective discharge planning process that focuses on the resident s discharge goals, the preparation of residents
F660 483.21(c)(1) Discharge Planning Process The facility must develop and implement an effective discharge planning process that focuses on the resident s discharge goals, the preparation of residents
CMS-3819-F Condition of participation: Reporting OASIS information. (a) Standard: Encoding and transmitting OASIS data. An HHA must encode
 Standard: Encoding and transmitting OASIS data. An HHA must encode") CMS-3819-F 319 OASIS information to the public. 484.45 Condition of participation: Reporting OASIS information. HHAs must electronically report all OASIS data collected in accordance with 484.55. (a) Standard:
CMS-3819-F 319 OASIS information to the public. 484.45 Condition of participation: Reporting OASIS information. HHAs must electronically report all OASIS data collected in accordance with 484.55. (a) Standard:
New Strategies for Managing Medicare Risk
 New Strategies for Managing Medicare Risk John Sheridan, MHSA, FACHE President, ehealth Data Solutions Keith Knapp, PhD, CFACHCA CEO, Christian Care Communities 1001. Survey and Certification Phase II
New Strategies for Managing Medicare Risk John Sheridan, MHSA, FACHE President, ehealth Data Solutions Keith Knapp, PhD, CFACHCA CEO, Christian Care Communities 1001. Survey and Certification Phase II
#212 How to Submit a Successful Informal Dispute Resolution (IDR)
") #212 How to Submit a Successful Informal Dispute Resolution (IDR) Wisconsin Health Care Association April 12, 2018 3:30pm to 4:30pm By: Leah Killian Smith, BA, NHA, RHIA, HSE Director of Quality & Government
#212 How to Submit a Successful Informal Dispute Resolution (IDR) Wisconsin Health Care Association April 12, 2018 3:30pm to 4:30pm By: Leah Killian Smith, BA, NHA, RHIA, HSE Director of Quality & Government
LeadingAge Maryland Update April 24, Office of Health Care Quality Protecting the health and safety of Marylanders
 LeadingAge Maryland Update April 24, 2017 Office of Health Care Quality Protecting the health and safety of Marylanders Today s Presentation Overview of OHCQ Nursing Homes Assisted Living Programs IDR
LeadingAge Maryland Update April 24, 2017 Office of Health Care Quality Protecting the health and safety of Marylanders Today s Presentation Overview of OHCQ Nursing Homes Assisted Living Programs IDR
New CMS Survey Initiatives Require Immediate Attention
 PHCA Webinar March 17, 2015 New CMS Survey Initiatives Require Immediate Attention Paula G. Sanders, Esquire Chair, Health Care Practice Post & Schell, PC Survey Overview Receive statement of deficiencies
PHCA Webinar March 17, 2015 New CMS Survey Initiatives Require Immediate Attention Paula G. Sanders, Esquire Chair, Health Care Practice Post & Schell, PC Survey Overview Receive statement of deficiencies
National Overview of CMS RoP & Quality. Holly Harmon, RN, MBA, LNHA, FACHCA May 3, 2018
 National Overview of CMS RoP & Quality Holly Harmon, RN, MBA, LNHA, FACHCA May 3, 2018 It s a Time of Change.. Reform of Requirements of Participation (RoP) - 3-Phase Implementation Phase 1: Upon the effective
National Overview of CMS RoP & Quality Holly Harmon, RN, MBA, LNHA, FACHCA May 3, 2018 It s a Time of Change.. Reform of Requirements of Participation (RoP) - 3-Phase Implementation Phase 1: Upon the effective
Federal Bill of Rights
 Federal Bill of Rights FOR RESIDENTS IN MEDICARE/MEDICAID CERTIFIED SKILLED NURSING FACILITIES OR NURSING FACILITIES All residents in long-term care facilities have rights guaranteed to them under Federal
Federal Bill of Rights FOR RESIDENTS IN MEDICARE/MEDICAID CERTIFIED SKILLED NURSING FACILITIES OR NURSING FACILITIES All residents in long-term care facilities have rights guaranteed to them under Federal
Center for Medicaid, CHIP, and Survey & Certification/Survey & Certification Group
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop 02 02 38 Baltimore, Maryland 21244 1850 Center for Medicaid, CHIP, and Survey & Certification/Survey
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop 02 02 38 Baltimore, Maryland 21244 1850 Center for Medicaid, CHIP, and Survey & Certification/Survey
Rights in Residential Settings
 WISCONSIN COALITION FOR ADVOCACY Rights in Residential Settings Jeffrey Spitzer-Resnick, Attorney Catharine Krieps, Litigation Specialist Wisconsin Coalition for Advocacy Introduction Nursing homes are
WISCONSIN COALITION FOR ADVOCACY Rights in Residential Settings Jeffrey Spitzer-Resnick, Attorney Catharine Krieps, Litigation Specialist Wisconsin Coalition for Advocacy Introduction Nursing homes are
ADULT LONG-TERM CARE SERVICES
 ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
PATIENT BILL OF RIGHTS & NOTICE OF PRIVACY PRACTICES
 Helping People Perform Their Best PRIVACY, RIGHTS AND RESPONSIBILITIES NOTICE PATIENT BILL OF RIGHTS & NOTICE OF PRIVACY PRACTICES Request Additional Information or to Report a Problem If you have questions
Helping People Perform Their Best PRIVACY, RIGHTS AND RESPONSIBILITIES NOTICE PATIENT BILL OF RIGHTS & NOTICE OF PRIVACY PRACTICES Request Additional Information or to Report a Problem If you have questions
8/27/2015. Background Overview Overarching Themes & Highlights of the Proposed Rule Areas of Concern Submitting Comments Resources Questions
 OHCA WEBINAR CMS PROPOSED REQUIREMENTS FOR PARTICIPATION AUGUST 27, 2015 Carol Rolf, Senior Partner, Rolf Goffman Martin Lang LLP Mandy Smith, Regulatory Director, OHCA WHAT WE WILL COVER Background Overview
OHCA WEBINAR CMS PROPOSED REQUIREMENTS FOR PARTICIPATION AUGUST 27, 2015 Carol Rolf, Senior Partner, Rolf Goffman Martin Lang LLP Mandy Smith, Regulatory Director, OHCA WHAT WE WILL COVER Background Overview
Complaint Investigations of Minnesota Health Care Facilities
 Complaint Investigations of Minnesota Health Care Facilities Report to the Minnesota Legislature explaining the investigative process and summarizing investigations from July 1, 2004 to June 30, 2007 and
Complaint Investigations of Minnesota Health Care Facilities Report to the Minnesota Legislature explaining the investigative process and summarizing investigations from July 1, 2004 to June 30, 2007 and
DIA COMPLIANCE OVERVIEW FOR HOME HEALTH AGENCIES
 DIA COMPLIANCE OVERVIEW FOR HOME HEALTH AGENCIES Mary Spracklin RN, M.S.N Rosemary Kirlin RN, M.S.N September 30, 2014 ROLE OF THE STATE AGENCY (SA) The Centers for Medicare and Medicaid Services (CMS)
DIA COMPLIANCE OVERVIEW FOR HOME HEALTH AGENCIES Mary Spracklin RN, M.S.N Rosemary Kirlin RN, M.S.N September 30, 2014 ROLE OF THE STATE AGENCY (SA) The Centers for Medicare and Medicaid Services (CMS)
CMHC Conditions of Participation
 CMHC Conditions of Participation Mary Rossi-Coajou Center for Clinical Standards and Quality/Clinical Standards Group The Centers for Medicare and Medicare Services March 4,2014 Key Themes The CMHC NPRM
CMHC Conditions of Participation Mary Rossi-Coajou Center for Clinical Standards and Quality/Clinical Standards Group The Centers for Medicare and Medicare Services March 4,2014 Key Themes The CMHC NPRM
WHAT TO EXPECT IF YOUR FACILITY RECEIVES A G LEVEL OR ABOVE DEFICIENCY
 WHAT TO EXPECT IF YOUR FACILITY RECEIVES A G LEVEL OR ABOVE DEFICIENCY Presented to: Massachusetts Senior Care Association October 27, 2017 Today s Presenters 2 Robert Griffin, Esq. Managing Partner Anthony
WHAT TO EXPECT IF YOUR FACILITY RECEIVES A G LEVEL OR ABOVE DEFICIENCY Presented to: Massachusetts Senior Care Association October 27, 2017 Today s Presenters 2 Robert Griffin, Esq. Managing Partner Anthony
Requirements of Participation - Phase 1 Admission Updates Guide
 - Phase 1 Guide This Requirements of Participation Guide provides a brief informational overview of the revisions to the Nursing Home Requirements of Participation (RoPs) that may apply to a SNF s admission
- Phase 1 Guide This Requirements of Participation Guide provides a brief informational overview of the revisions to the Nursing Home Requirements of Participation (RoPs) that may apply to a SNF s admission
Lou Anne Page, HFE NE II
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: Z6PT PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: Z6PT PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
Pharmacy Services. Division of Nursing Homes
 Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Based on the comprehensive assessment of a resident, the facility must ensure that:
 7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
SEP Memorandum Report: "Trends in Nursing Home Deficiencies and Complaints," OEI
 DEPARTMENT OF HEALTH &. HUMAN SERVICES Office of Inspector General SEP 18 2008 Washington, D.C. 20201 TO: FROM: Kerry Weems Acting Administrator Centers for Medicare & Medicaid Services Daniel R. Levinson~
DEPARTMENT OF HEALTH &. HUMAN SERVICES Office of Inspector General SEP 18 2008 Washington, D.C. 20201 TO: FROM: Kerry Weems Acting Administrator Centers for Medicare & Medicaid Services Daniel R. Levinson~
Behavioral Health Services. Division of Nursing Homes
 Behavioral Health Services Division of Nursing Homes 483.40 Behavioral Health Services Overview F740 Introduction to Behavioral Health Services F741 Sufficient and Competent Staff F742 Treatment/Services
Behavioral Health Services Division of Nursing Homes 483.40 Behavioral Health Services Overview F740 Introduction to Behavioral Health Services F741 Sufficient and Competent Staff F742 Treatment/Services
Medication Related Changes Phase 1&2
 Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Survey Protocol for Long Term Care Facilities
 Attachment B Survey Protocol for Long Term Care Facilities The provision of home dialysis treatments in a Long Term Care (LTC) facility place an increased burden on the LTC facility staff and may place
Attachment B Survey Protocol for Long Term Care Facilities The provision of home dialysis treatments in a Long Term Care (LTC) facility place an increased burden on the LTC facility staff and may place
DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 73
 DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 73 NURSING FACILITIES/MEDICAID - REMEDIES 411-073-0000 Purpose The purpose of
DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 73 NURSING FACILITIES/MEDICAID - REMEDIES 411-073-0000 Purpose The purpose of
Abuse, Neglect, and Exploitation. Division of Nursing Homes
 Abuse, Neglect, and Exploitation Division of Nursing Homes Overview of 42 CFR 483.12 F600 Abuse and Neglect F602 -Misappropriation of Resident Property and Exploitation F603 Involuntary Seclusion F604
Abuse, Neglect, and Exploitation Division of Nursing Homes Overview of 42 CFR 483.12 F600 Abuse and Neglect F602 -Misappropriation of Resident Property and Exploitation F603 Involuntary Seclusion F604
New Long Term Care Survey Process
 New Long Term Care Survey Process Disclaimer The information provided within these slides are current as of May 15,2017. It provides information related to the CMS' intent to implement the survey process
New Long Term Care Survey Process Disclaimer The information provided within these slides are current as of May 15,2017. It provides information related to the CMS' intent to implement the survey process
HOSPICE CONTRACTING CHECKLIST FOR INPATIENT SERVICES, RESPITE CARE AND VENDOR AGREEMENTS
 HOSPICE CONTRACTING CHECKLIST FOR INPATIENT SERVICES, RESPITE CARE AND VENDOR AGREEMENTS The following checklist can be used to verify that the regulatory requirements are addressed in hospice contracts
HOSPICE CONTRACTING CHECKLIST FOR INPATIENT SERVICES, RESPITE CARE AND VENDOR AGREEMENTS The following checklist can be used to verify that the regulatory requirements are addressed in hospice contracts
Quality Performance: The Central Focus of Home Health Care Policy
 Quality Performance: The Central Focus of Home Health Care Policy Wisconsin Association for Home Health Care June 9, 2016 William A. Dombi National Association for Home Care & Hospice HOME HEALTH CARE
Quality Performance: The Central Focus of Home Health Care Policy Wisconsin Association for Home Health Care June 9, 2016 William A. Dombi National Association for Home Care & Hospice HOME HEALTH CARE
CMS Final Rule Pharmacy Services Update: What You Need to Know!
 CMS Final Rule Pharmacy Services Update: What You Need to Know! Presented by: Dr. William C. Hallett, Pharm.D., MBA, CGP, C-MTM Guardian Consulting Services, Inc. (855) 675-6235 whallett@guardianconsulting.com
CMS Final Rule Pharmacy Services Update: What You Need to Know! Presented by: Dr. William C. Hallett, Pharm.D., MBA, CGP, C-MTM Guardian Consulting Services, Inc. (855) 675-6235 whallett@guardianconsulting.com
Conditions of Participation for Hospice Programs
 Conditions of Participation for Hospice Programs Code of Federal Regulations --- Title 42, Volume 2, Parts 400 to 429 TITLE 42 PUBLIC HEALTH CHAPTER IV CENTERS FOR MEDICARE AND MEDICAID SERVICES DEPARTMENT
Conditions of Participation for Hospice Programs Code of Federal Regulations --- Title 42, Volume 2, Parts 400 to 429 TITLE 42 PUBLIC HEALTH CHAPTER IV CENTERS FOR MEDICARE AND MEDICAID SERVICES DEPARTMENT
Home Health Agency Updated Conditions of Participation. Thursday, December 7, :00 4:00 PM EST
 Home Health Agency Updated Conditions of Participation Thursday, December 7, 2017 2:00 4:00 PM EST Home Health Agency (HHA) Training Session Presented by: Peggye Wilkerson Director, Division of Continuing
Home Health Agency Updated Conditions of Participation Thursday, December 7, 2017 2:00 4:00 PM EST Home Health Agency (HHA) Training Session Presented by: Peggye Wilkerson Director, Division of Continuing
Annual Quality Improvement Report on the Nursing Home Survey Process
 Commissioner s Office 625 Robert St. N., Suite 500 P.O. Box 64975 St. Paul, MN 55164-0975 (651) 201-5000 Annual Quality Improvement Report on the Nursing Home Survey Process Minnesota Department of Health
Commissioner s Office 625 Robert St. N., Suite 500 P.O. Box 64975 St. Paul, MN 55164-0975 (651) 201-5000 Annual Quality Improvement Report on the Nursing Home Survey Process Minnesota Department of Health
ADMISSION CONSENTS. 1. Yes No Automobile Medical or No Fault insurance due to an accident?
 Patient Name: I.D. Number: Section A: Identifying Proper Payor ADMISSION CONSENTS Are services provided to you by Hospice reimbursements through health insurance other than Medicare due to one of the following
Patient Name: I.D. Number: Section A: Identifying Proper Payor ADMISSION CONSENTS Are services provided to you by Hospice reimbursements through health insurance other than Medicare due to one of the following
HOW WE GOT HERE 1935: Social Security Act Private nursing homes
 1 LeadingAge Oklahoma Annual Conference March 8, 2017 CMS Revised Pharmacy Regulations: Lessons Learned from Phase 1, Guidance for Phase 2 William M. Vaughan RN, BSN Vice President, Education and Clinical
1 LeadingAge Oklahoma Annual Conference March 8, 2017 CMS Revised Pharmacy Regulations: Lessons Learned from Phase 1, Guidance for Phase 2 William M. Vaughan RN, BSN Vice President, Education and Clinical
This presentation will be updated as new information becomes available.
 New Long Term Care Survey Process Disclaimer The information provided within these slides are current as of May 15,2017. It provides information related to the CMS' intent to implement the survey process
New Long Term Care Survey Process Disclaimer The information provided within these slides are current as of May 15,2017. It provides information related to the CMS' intent to implement the survey process
Division of Quality Assurance. Updates
 Updates Otis L. Woods, MBA, Administrator Nursing Home Update CMS Updates DQA Updates Survey Statistics AGENDA CMS Update Partnership to Improve Dementia Care in Nursing Homes Antipsychotic use MDS Staffing
Updates Otis L. Woods, MBA, Administrator Nursing Home Update CMS Updates DQA Updates Survey Statistics AGENDA CMS Update Partnership to Improve Dementia Care in Nursing Homes Antipsychotic use MDS Staffing
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2011
 2011") CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2011 What Hospitals Need to Know About Grievances Speaker Sue Dill Calloway RN, Esq. CPHRM AD, BA, BSN, MSN, JD President Patient Safety and Education 5447
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2011 What Hospitals Need to Know About Grievances Speaker Sue Dill Calloway RN, Esq. CPHRM AD, BA, BSN, MSN, JD President Patient Safety and Education 5447
MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL. PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID: 00695
 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: D9GP PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES MEDICARE/MEDICAID CERTIFICATION AND TRANSMITTAL ID: D9GP PART I - TO BE COMPLETED BY THE STATE SURVEY AGENCY Facility ID:
Assisted Living Facility Resource Manual
 Assisted Living Facility Resource Manual August 2015 Assisted Living Facility Resource Manual August 2015 Table of Contents Survey Process... 1 ALF Resident Centered Survey Process... 1 LNS & ECC Monitoring...
Assisted Living Facility Resource Manual August 2015 Assisted Living Facility Resource Manual August 2015 Table of Contents Survey Process... 1 ALF Resident Centered Survey Process... 1 LNS & ECC Monitoring...
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to