Do No Harm: Evidence Based Prevention Strategies to Reduce Readmission
|
|
|
- Ross McDowell
- 5 years ago
- Views:
Transcription


1 Do No Harm: Evidence Based Prevention Strategies to Reduce Readmission Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING kvollman@comcast.net Northville Michigan ADVANCING NURSING LLC 2016


2 Disclosures for Kathleen Vollman Consultant-Michigan Hospital Association Keystone Center Consultant/Faculty for CUSP for MVP AHRQ funded national study Subject matter expert CAUTI, CLABSI, HAPU, Sepsis, Safety culture Consultant and speaker bureau for Sage Products LLC Consultant and speaker bureau for Hill-Rom Inc Consultant and speaker bureau for Eloquest Healthcare
3 Session Objectives Describe the forces within the health care environment that are driving the need to resuscitate the basics Outline a screening process for early recognition of septic resident and initial management Define key evidence based care practice that reduces pneumonia and CAUTI s Understanding the fundamentals of Antimicrobial Stewardship and resources available for implementation of a AMS program
4
5 The Requirements for Long-Term Care (LTC) Facilities Must Meet in Order to Participate in the Medicare or Medicaid Programs Person-Centered Care Quality Development of a QI system-quality assurance and quality improvement Facility Assessment Competency-Based Approach Alignment with HHS priorities Comprehensive Review and Modernization Implementation of Legislation Education/Outreach/NPC/Downloads/Compliant-LTC-PP-for-MLN-National- Provider-Call.pdf
6 Align with Current HHS Initiatives Reducing unnecessary hospital readmissions In NQF# 2510: assesses the risk standardize rate of all cause, unplanned inpatient hospital readmissions for Medicare fee-for-service SNF patients within 30 days of discharge from a prior proximal hospitalization A prior proximal hospitalization is defined as an admission to an inpatient prospective payment system hospital, critical access hospital or psychiatric hospital Reducing the incidences of healthcare acquired infections Improving behavioral healthcare Safeguarding nursing home residents from the use of unnecessary psychotropic (antipsychotic) medications. Education/Outreach/NPC/Downloads/Compliant-LTC-PP-for- MLN-National-Provider-Call.pdf
7 Hospitalization by Age: US Levant S, Chari K, DeFrances CJ. Hospitalizations for patients aged 85 and over in the United States, NCHS data brief, no 182. Hyattsville, MD: National Center for Health Statistics
8 8
9 Common Causes of Hospitalization Adults aged 85 and over: U.S. Levant S, Chari K, DeFrances CJ. Hospitalizations for patients aged 85 and over in the United States, NCHS data brief, no 182. Hyattsville, MD: National Center for Health Statistics
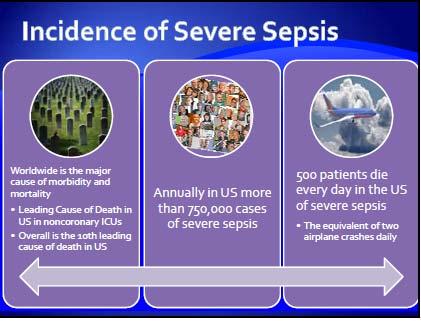
10 Mortality and Cost Sepsis is a leading cause of death and the most expensive disease in U.S. hospitals Mortality increased 26% in patients and 38% in those 85 years of age. 10
11 Discharge Disposition After Sepsis Septicemia or sepsis Other diagnoses Disposition Percent Routine Transfer to other short-term 6 3 care facility Transfer to long-term care institution Died during the 17 2 hospitalization Other or not stated 8 6 Total Difference is statistically significant at the 0.05 level. SOURCE: CDC/NCHS, National Hospital Discharge Survey,
12 Total All-Cause, 30 day Readmissions and Aggregate Cost by Payer

13 Chang DW; Tseng CH; Shapiro MF. Critical Care Medicine. 43(10): , 2015 Oct. 13 3
14 Michigan 2014 SNF Readmission Statistics Selected Diagnosis Codes for All Cause Readmissions Congestive Heart Failure (CHF) 28.57% Acute Myocardial Infarction (AMI) 24.77% Chronic Obstructive Lung Disease (COPD) 26.76% Dialysis/End Stage Renal Disease 38.27% Pneumonia 21.7% Sepsis 26.42% All-Cause Readmission Within 30 Days of Index Discharge from State of Michigan Acute Care Facilities by Selected Population Segments, State of Michigan Medicare Fee- For-Service (FFS) Beneficiaries [Q1, Q4, 2014 ] MPRO July 2015


15 Readmission Rates Among D/C Location 07/ /2015

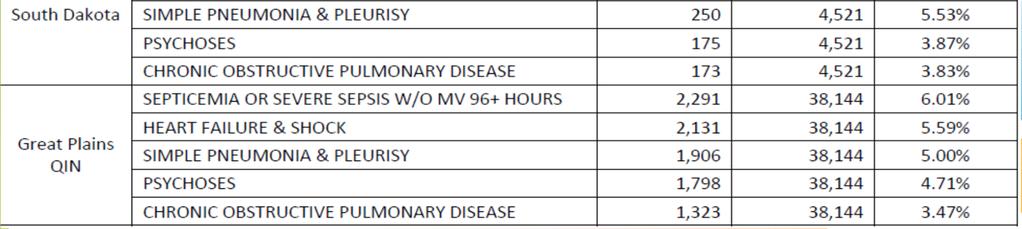
16 South Dakota Readmissions
17 Screen for Sepsis and Create and Early Management Program
18
 Crit Care Med.")
19 Sepsis Impact on the Elderly Age itself independent risk factor for death More likely admitted to ICU Highest mortality in the old elderly (85+) Prolonged hospitalization Post Sepsis Impact Contributes to Cognitive decline Contributes to Physical long term disabilities (walking, ADLs, and IADLs) Crit Care Med Jan;34(1):15-21

20 Sepsis Recognition Challenges Febrile response not present in 47% of elderly Temperature >101 generally indicates severe infection Delirium occurs in 50% Common symptoms: altered mental status, delirium, of older adults with sepsis weakness, anorexia, malaise, falls, and urinary incontinence Dementia can make obtaining a history challenging Positioning for tests due to osteoarthritis presents challenges Girard et al Insights into severe sepsis in older patients: from epidemiology to evidence-based management. Clin Infect Dis 2005; 40:
21 Severe Sepsis: Defining a Disease Continuum Infection SIRS Sepsis Severe Sepsis Adult Criteria A clinical response arising from a nonspecific insult, including 2 of the following: Temperature: > 38 C or < 36 C Heart Rate: > 90 beats/min Respirations: > 20/min WBC count: > 12,000/mm 3, or < 4,000/mm 3, or > 10% immature neutrophils SIRS = Systemic Inflammatory Response Syndrome Bone et al. Chest. 1992;101: SIRS with a presumed or confirmed infectious process Sepsis with 1 sign of organ dysfunction, hypoperfusion or hypotension. Examples: Cardiovascular (refractory hypotension) Renal Respiratory Hepatic Hematologic CNS Unexplained metabolic acidosis Shock
22 Definitions Infection Sepsis: infection plus 2 or more SIRS Severe Sepsis: infection plus 2 or more SIRS plus new organ dysfunction Septic Shock: severe sepsis with a lactic acid greater than or equal to 4mmol/L OR continued hypotension (systolic BP<90 or 40mmHg decrease from their baseline) after initial fluid bolus (30ml/kg)
23 CORNERSTONES OF MULTIDISCIPLINARY MANAGEMENT OF SEVERE SEPSIS Prevention Screening and Early Identification Early Intervention: Source control, Blood cultures and broad spectrum antibiotics Initial Resuscitation Bundle Septic Shock Bundle at the hospital
24 SEP-1 SEP-1 TO BE COMPLETED WITHIN 3 HOURS OF TIME OF PRESENTATION : 1. Measure lactate level 2. Obtain blood cultures prior to administration of antibiotics 3. Administer broad spectrum antibiotics 4. Administer 30ml/kg crystalloid for hypotension or lactate 4mmol/L time of presentation is defined as the time of earliest chart annotation consistent with all elements severe sepsis or septic shock ascertained through chart review.
25 SEP-1 SEP-1 TO BE COMPLETED WITHIN 6 HOURS OF TIME OF PRESENTATION: 5. Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation) to maintain a mean arterial pressure (MAP) 65mmHg 6. In the event of persistent hypotension after initial fluid administration (MAP < 65 mm Hg) or if initial lactate was 4 mmol/l, re-assess volume status and tissue perfusion and document findings according to table Re-measure lactate if initial lactate elevated.

26 Screening When do you screen? Upon admission, daily, with condition change or stop and watch alert First step: Does the patient have a known or suspected infection?
?")
27 Screening Second Step: Does the patient have signs of systemic inflammatory response syndrome (SIRS)?


28 Screening Third Step: Does the patient have any new organ dysfunction in an organ system distant from site of infection?


29 Screening If screens positive for severe sepsis, then follow the SBAR at bottom of tool
30 ACT FAST! Early Detection of SEPSIS requires fast action STOP AND WATCH (INTERACT) S Seems different than usual T Talks or communicates less O Overall needs more help P Pain- new or worsening; Participated less in activities A Ate less N No bowel movement in 3 days; or diarrhea D Drank less W Weight change A Agitated or nervous more than usual T Tired, weak, confused, or drowsy C Change in skin color or condition H Help with walking, transferring, and toileting more than usual
31
32 The Importance of Early Detection Efforts to just treat recognized sepsis alone is not enough. A critical aspect of mortality reduction has been pushing practitioners to identify sepsis early. It may well be that earlier recognition accounts for much of the signal in mortality reduction and partially explains sharply increasing incidence. Without recognition that the clock is ticking, there is simply no incentive to recognize a challenging diagnosis early. Levy MM, Dellinger RP, Townsend SR,et al. Crit Care Med Feb;38(2): Gaieski 13 DF, Edwards JM, Kallan MJ, et al. Crit Care Med Feb 25
33 Early Recognition and Management of Sepsis Overview of Training Program Example Monthly one hour face to face meetings Jan to June Monthly site specific coaching calls, starting in February to provide individualized support Provide training and educational materials Defined process and outcome measures to evaluate success of the program
34 Roles and Responsibilities Each facility must have a team identified to do this work Should include: medical director, DON, infection prevention nurse at a minimum Team work through action plan provided in specified timeframe Implement screening process Implement early management of sepsis process Educate staff on screening and management processes Collect defined process and outcome data
35 Sepsis Early Identification Action Plan Step Who? When? Status 1. Get team together to create early identification process 2. Develop screening tool/process 3.Get medical staff support for screening and early intervention 4. Develop and implement educational plan for sepsis and screening 5. Develop patient & family education process and tools 6. Develop an infection prevention education plan for PNA, UTI, and CLABSI, 7. Evaluate screening: define outcome and process metrics
36 Pneumonia Statistics Leading cause of death due to infectious disease in the USA, sixth leading cause of death overall >65, leading cause for NH. >900, 000 CAP cases in population over 65. Mortality rate in USA about 5%. Estimated HCAP per 1000 NH residents. 1st or 2 nd most common infection in NH (13-48%) Mortality rate 13-41% if NH resident. Medicare paid 17.4 billion in 2004 for readmissions (about 17%).
37 STATISTICS. Out of 12 million fee-for-service Medicare beneficiaries: 20% readmitted within 30 days 34% readmitted within 90 days 54% readmitted within one year 68.9% discharged with medical condition died within a year 53% discharged with surgical condition died within one year.

38 Preventing Infection Pneumonia
39 PNEUMONIA Infection of one or both lungs, lobar, segmental, or bronchial More than 30 different causes Can be serious, even fatal, especially for very young/very old. Pneumococcal vaccine, influenza vaccine, and ACE inhibitors may have protective effect.
40 Epidemiological & Risk Factor Categories for Institutional Pneumonia Residents >75 years old at 6x higher risk 33 out of 1000 nursing home residents require hospitalization for pneumonia per year vs out of 1000 elderly living in the community per year Leading cause of death in nursing home residents Annual cost of nursing home acquired pneumonia exceeds $8 billion dollars Factors that increase bacterial burden or colonization Factors that increase risk of aspiration Terpenning M. et al. JAGS 2002;50: Murder RR. Am J Med 1998;105:
41 The Older Adult At Risk Cognitively impaired Diminished swallow and cough reflex Functionally dependent Dry mouth Aspiration Multiple medications High rate tooth decay Behavioral problems during oral hygiene Lack of immunization Research Dissemination Core. Iowa City (IA): University of Iowa Gerontological Nursing Interventions Research Center; 2002 Nov. 48 p. Marik PE. et al. Chest; 2003; 124:
42 Significant Independent Predictors of Aspiration Pneumonia Dependant for feeding Dependant for oral care Number of decayed teeth Tube feeding Multiple medical diagnoses Number of medications Dry mouth Smoking Langmore SE. et al. Dysphagia 1998;13:69-81
43 Pathogenesis Prevention Germs in Mouth Dental plaque provides microhabitat Bacteria replicate 5X/24 hrs Aspirated into Lungs Most common route 50% of healthy adults micro-aspirate in sleep Weak Defenses Poor cough Immunosuppressed Multiple co-morbidities

44 Formation of Biofilm Over 13 Hours Loesche, W. 2012
45 Pathogenesis Prevention Germs in Mouth Dental plaque provides microhabitat Bacteria replicate 5X/24 hrs Aspirated into Lungs Most common route 50% of healthy adults micro-aspirate in sleep Weak Defenses Poor cough Immunosuppressed Multiple co-morbidities




46 Pathogenesis Prevention Germs in Mouth Comprehensive oral care Oral care protocol that includes all patients Aspirated into Lungs Swallow screens Tube feeding protocols Head of bed elevated Weak Defenses Lung expansion/mobilize Adequate nutrition Serum glucose target range Immunization
47 Risk Factor Categories for Health Care Acquired Pneumonia Factors that increase bacterial burden or colonization Factors that increase risk of aspiration
48 Why NV-HAP? HAP 1st most common HAI in U.S. Increased morbidity 50% are not discharged back home Increased mortality 18%-29% Extended LOS 4-9 days Increased Cost $28K to $109K 2x likely for readmission <30 day Understudied, under-addressed Focus has been on the other HAP VAP Surveillance not required.yet Kollef, M.H. et.al. (2005). Chest. 128, ATS, (2005). AmJ Respir Crit Care Med. 171, Lynch (2001) Chest. 119, 373S-384S. Pennsylvania Dept of Public Health (2010)
49


50 Oropharyngeal Colonization Methodology: 49 elderly nursing home residents admitted to the hospital Examined baseline dental plaque scores & microorganism within dental plaque Used pulse field gel electrophoresis to compare chromosomal DNA Results: 14/49 adults developed pneumonia 10 of 14 pneumonias, the causative organism was identical via DNA analysis El-Solh AA. Chest. 2004;126:
51 Practices in Oral Care Culture cup, ½ H2O2, ½ sterile H2O little bit of mouthwash Lemon glycerin swabs Toothette with water &/or mouthwash No oral care That s not the way we do it here!!!
52 Lemon & Glycerin Swabs Harmful Hastens drying of mucosa by depleting the saliva reserve caused by over-stimulation of salivary glands by lemon juice Citric acid has no moisturizing capabilities Irritates oral mucosa & decalcifies teeth Glycerin is a trihydric alcohol that absorbs water causing drying Foss-Durant Am et al. Clin Nurs Res. 1997;6(1): Krishnasamy M. Eur J Cancer Care. 1995;4(4): Regnard C et al. Br Med J. 1997;315(7114): Van Drimmelen JR et al. Nurs Res 1969;18:
53 Oral Care Reduces Pneumonia In Nursing Homes Methodology 11 nursing homes in Japan over 2 year period 417 enrolled / 366 residents analyzed (death from other causes) 184 received oral care program/182 did not Tooth brushing after each meal (teeth or dentures) & 1x weekly review by dentist/or hygienist Results No Oral Oral Care p value Febrile 29% 15% p<.01 Pneumonia 19% 11% p<.05 Death 16% 7% p<.01 MMSE Increase p<.05 Yoneyama et al. JAGS. 2002;50:
54 Impact of Oral Care on HAP Kaneoka A, et al Infect. Control Hosp. Epidemiol, 2015;36(8):
55 Oral Care Reduces Pneumonia In Nursing Homes Residents Oral care improves swallowing and cough reflex sensitivities Watando A. et al. Chest, 2004; 126: )
56 BRUSH & SWAB 77% more clean proximal sites with brushing 44% more clean crevice sites with brushing Benefit of brushing is directly correlated with technique Foam swabs could not remove plaque from sheltered areas on or between teeth Pearson LS. et. al. J of Adv Nursing. 2002;39(5): Toothbrush; grade D, Swabs; unresolved, Use of flexible suction catheter post oral cleansing; Grade D (Berry AM et al. AJCC, 2007;16: )
57 Brushing Removes Plaque Methodology: 34 volunteers. Double-blind crossover study. Examine the amount and % of plaque removed with a single brushing with 3 solutions (Sodium Bicarb, Crest, Cologate). Results: Significantly higher % of plaque removed with one minute brush using Sodium Bicarb. Mankodi et al. J Clin Dent. 1998; 9(3):57-60
58 Proposed Oral Care Plan Independent Dependent on Oral Care Weekly assessment Encouragement to perform tooth brushing /denture cleaning minimum x2 daily Ability to expectorate Assist with brushing teeth/clearing out debris & /or cleaning dentures using with CPC after each meal/night & moisturize following cleaning Unable to expectorate Brush teeth (dentures) /clear debris using suction toothbrush am & pm with CPC followed by moisturizing Assist oral cleansing (dentures)/clear debris after lunch & dinner using a suction swab with CPC followed by moisturizing denture cleaning

59 Oral Care Protocol

60 Your Role in Preventing Pneumonia Proper hand hygiene Comprehensive Oral Care Prevention of Aspiration Swallow screens Proper positioning during eating/feeding and sleep Immunizations Mobility/ Lung expansion Adequate nutrition
61 PNA Prevention Action Plan Step Who? When? Status 1. Assess current infection prevention practices for PNA. 2. Identify gaps in application of PNA prevention practices and develop plan to implement strategies to close gaps 3. Develop an infection prevention education plan for PNA. 4. Audit PNA prevention practices 5. Submit facility acquired PNA rates to portal
62 Current State Assessment related to PNA Prevention Practices Prevention Practices Current Policy in Place Audit 5 patients to see if compliant with policy Proper hand hygiene Comprehensive Oral Care Prevention of Aspiration Swallow screens Proper positioning during eating/feeding and sleep Mobility/ Lung expansion (up at least 1/day) Adequate nutrition (consumed >50% of diet)

63
64 The Why Urinary tract infection (UTI) are one of the most common hospitalacquired infections Along with other device associated infections (CLABSI and VAP) account for 25% of all hospital acquired infections 70-80% of UTIs are due to urinary catheters 12-16% of inpatients are catheterized Leads to increased morbidity and costs ($896) Medicare no longer reimburses U.S. hospitals for the additional costs of certain infections CLA-BSI & CAUTI are 65% of the clinical conditions for VBP CAUTI prevention is part of the 2012 National Patient Safety Goal Magill et al NEJM 2014; APIC Guide to Prevention of CAUTI, 2014; Lo et al SHEA/IDSA Practice Recommendations Inf Control and Hosp Epid 2014 Zimlichman E, et al. JAMA Intern, 2013;17:373:
65 Partnership for Patients CAUTI Venous thromboembolism Pressure ulcers Immobility Urinary Catheter Harm Increased Length of Stay Patient discomfort Falls Trauma Adverse drug events Isn t this a patient safety issue, not just CAUTI?
66 Pathogenesis of CAUTI Source: colonic or perineal flora on hands of personnel Microbes enter the bladder via extraluminal {around the external surface} (proportion = 2/3) or intraluminal {inside the catheter} (1/3) Daily risk of bacteriuria with catheterization is 3% to 10%; by day 30 = 100% APIC Guide to Preventing CAUT

67 Disrupting the Lifecycle of the Urinary Catheter 1. Preventing Unnecessary and Improper Placement 1 4. Preventing Catheter Replacement Maintaining Awareness & Proper Care of Catheters 3 3. Prompting Catheter Removal (Meddings. Clin Infect Dis 2011)
68 CDC, SHEA, IDSA and NHS: Indications for Placement Perioperative use for selected surgical procedures Urine output in critically ill patients Management of acute urinary retention and urinary obstruction Assistance in pressure ulcer healing for incontinent patients At a patient request to improve comfort(shea) or for comfort during end of life care (CDC) How-to Guide: Prevent Catheter-Associated Urinary Tract Infections. Cambridge, MA: Institute for Healthcare Improvement; (Available at Lo E, et al. Infect Contr & Hosp Epidemiol. 2014;35(5):
69 Core Recommendations Insert catheters only for appropriate indications (1B) Leave catheters in only as long as needed (1B) Ensure that only properly trained persons insert and maintain catheters (1B) Insert catheters using aseptic technique and sterile equipment (acute care settings) (1C) Consider use of alternatives (II) Maintain a close drainage system (1B) Secure the system (1B) Maintain unobstructed urine flow (1B) Key the collecting bag below the level of the bladder at all times (1B) Lo E, et al. Infect Contr & Hosp Epidemiol. 2014;35(5):
70 Simplified Insertion Checklist for Urinary Catheter 70
71 Core Recommendations Insert catheters only for appropriate indications (1B) Leave catheters in only as long as needed (1B) Ensure that only properly trained persons insert and maintain catheters (1B) Insert catheters using aseptic technique and sterile equipment ( acute care settings) (1C) Consider use of alternatives (II) Maintain a close drainage system (1B) Secure the system (1B) Maintain unobstructed urine flow (1B) Key the collecting bag below the level of the bladder at all times (1B)

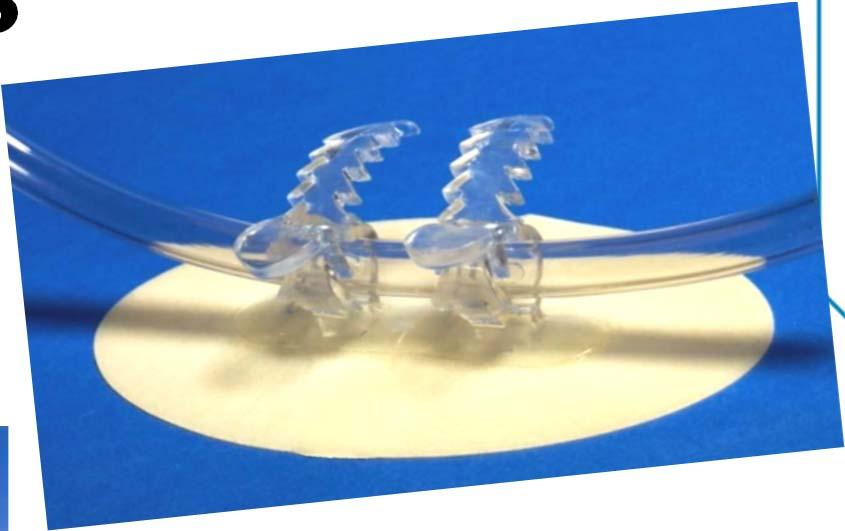
72 Challenges with Current Appropriate Alternatives: External Male Catheters 1 out of every 200 men is born with what s medically known as micro-penis





73 Buried Penis

74 Condom Catheter
75 Common Problems Most common problems are: Skin irritation and maceration Difficult to keep the condom from falling off/retraction of the penis or decrease size Ischemia and penile obstruction/tightness Adherence: requires to secure on the shaft & adhesive mechanisms are challenging Reference: Newman, DK. Managing and Treating Urinary Incontinence. Health Professions Pr. 2002


76 Before & After QI Project 60 day comparison Use of a novel EMC device vs. indwelling catheter Inclusion criteria: No restraints No BPH No neurogenic bladder Cooperative Hospitalize 2 wks or greater Monitored wear time and evaluated the skin Average Wear Time = 24hrs Fitzwater M, IP Kindred Albuquerque, 2015
77 Core Recommendations Insert catheters only for appropriate indications (1B) Leave catheters in only as long as needed (1B) Ensure that only properly trained persons insert and maintain catheters (1B) Insert catheters using aseptic technique and sterile equipment ( acute care settings) (1C) Consider use of alternatives (II) Maintain a close drainage system (1B) Secure the system (1B) Maintain unobstructed urine flow (1B) Key the collecting bag below the level of the bladder at all times (1B)




78 Securement Devices
79 Core Recommendations Insert catheters only for appropriate indications (1B) Leave catheters in only as long as needed (1B) Ensure that only properly trained persons insert and maintain catheters (1B) Insert catheters using aseptic technique and sterile equipment ( acute care settings) (1C) Consider use of alternatives (II) Maintain a close drainage system (1B) Secure the system (1B) Maintain unobstructed urine flow (1B) Key the collecting bag below the level of the bladder at all times (1B)
80 Cleansing of Patients with Indwelling Catheter Indwelling catheter care should occur with the daily bath (basinless bathing)*, as a separate procedure using clean technique There is no evidence to support 2x a day indwelling catheter care If a large liquid stool occurs, bathe the patient with basin less bathing Use separate cloths to clean front to back in the perineal area and 6 inches of the catheter** Apply barrier cloth to area of skin requiring protection **Universal ICU Decolonization: An Enhanced Protocol. (Prepared by The REDUCE MRSA Trial Working Group, under contract HHSA i). AHRQ Publication No EF. Rockville, MD: Agency for Healthcare Research and Quality; September *Sage recommends following hospital policy
81 Additional Recommendations: SHEA Compendium Update 2014 Replace the catheter and the collecting system using aseptic technique when breaks in aseptic technique, disconnection, or leakage occur (quality of evidence: III). For examination of fresh urine, collect a small sample by aspirating urine from the needleless sampling port with a sterile syringe/cannula adaptor after cleansing the port with disinfectant (quality of evidence: III). Unresolved Antiseptic or sterile saline foe meatal cleaning before insertion Lo E, et al. Infect Contr & Hosp Epidemiol. 2014;35(5):

82


83 Cost-Benefit Ratio CA-UTI vs. IAD & Pressure Ulcer


84 IAD Assessment Tool Junkin J, Selek JL. J WOCN 2007;34(3):
85 Preventing UTIs (no indwelling catheter) Ensure adequate fluid intake Urine should be light and clear Adequate toileting Bladder should be emptied every 2-3 hours Cleaning: front to back Manage incontinence with appropriate toileting and products
86 Strategies to not over treat asymptomatic bacteriuria.
87 Guidelines for Antibiotic Use The guidelines are based on evidence. Researchers developed guidelines for a few key infections, including a UTI. Other researchers independently used these guidelines, tested them, and found that they were effective in reducing the number of antibiotics used. 87

88 ABC for Diagnosing UTI

89 ABC for Diagnosing UTI
90 UTI SBAR UTI SBAR form: Is intended to guide communication regarding the potential need for antibiotic use between nursing staff and prescribing clinicians in long-term care facilities, such as nursing homes. Is based on the Situation, Background, Assessment, and Recommendation form of communication, or SBAR. Is based on clinical practice guidelines.
91 SBAR Tool Design S Situation: A concise statement of the problem (what is going on now). B Background: Pertinent and brief information related to the situation (what has happened). A Assessment: Analysis and consideration of options (what you found/think is going on). R Recommendation: Request/recommend action (what you want done).
92 Suspected UTI SBAR

93 Suspected UTI SBAR
94 Current State Assessment related to UTI/CAUTI Prevention Practices Prevention Practices Current Policy in Place Audit 5 patients to see if compliant with policy Proper hand hygiene Without indwelling catheter: Adequate fluid so urine is light and clear Appropriate toileting (empty bladder every 2-3 hours) With indwelling catheter: Aseptic technique followed during insertion Daily catheter care Catheter secured Closed system No dependent loops Catheter Bag not on floor

95 Prevention Bundles Work Chahoud J, et al. Heart & Lung, 2015;44: Navoa-Ng JA, et al. J of Infection and Public Health 2013;6:
96
97 RESOURCES New Jersey Sepsis Learning-Action Collaborative Surviving Sepsis Campaign Centers for Disease Control and Prevention Sepsis Centers for Disease Control and Prevention - Nursing Homes and Assisted Living Resources Minnesota Hospital Association Seeing Sepsis Long Term Care Resources and-septic-shock American Hospital Association s Health Research and Educational Trust Sepsis Resources EVIDENCE-BASED LITERATURE RESOURCES Goodwin, A.J., Rice, D. A., Simpson, K. N. & Ford, D. W. Frequency, cost, and risk factors of readmissions among severe sepsis survivors. Critical Care Medicine. No. 43, Issue 4. (April 2015): Otego, A. et al. Hospital-based acute care use in survivors of septic shock. Critical Care Medicine. No. 43, Issue 4. (April 2015):
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Clinical Intervention Overview: Objectives
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
The Power of the Pyramid:
 The Power of the Pyramid: A Proven Sepsis Implementation Program for Saving Lives SepsisSolutionsInternational 2011 Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist, Educator, Consultant
The Power of the Pyramid: A Proven Sepsis Implementation Program for Saving Lives SepsisSolutionsInternational 2011 Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist, Educator, Consultant
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
CAUTI reduction at Mayo Clinic
 CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
CAUTI reduction at Mayo Clinic Priya Sampathkumar, MD, FIDSA, FSHEA Associate Professor of Medicine, Division of Infectious Diseases, Mayo Clinic, Rochester Jean (Wentink) Barth, MPH, RN, CIC Director,
Interventional Patient Hygiene: Impacting Patient Outcomes by Implementing Evidence Based Nursing Care Interventions
 Interventional Patient Hygiene: Impacting Patient Outcomes by Implementing Evidence Based Nursing Care Interventions Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator /
Interventional Patient Hygiene: Impacting Patient Outcomes by Implementing Evidence Based Nursing Care Interventions Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator /
The Next Big Adventure: Prevention of Hospital Acquired Non-Ventilator Pneumonia
 The Next Big Adventure: Prevention of Hospital Acquired Non-Ventilator Pneumonia Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING kvollman@comcast.net
The Next Big Adventure: Prevention of Hospital Acquired Non-Ventilator Pneumonia Kathleen M. Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist / Educator / Consultant ADVANCING NURSING kvollman@comcast.net
HOSPITAL ACQUIRED COMPLICATIONS. Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program
 HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
Stopping Sepsis in Virginia Hospitals and Nursing Homes. Hospital Webinar #6 - Tuesday, December 19, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
From Defeating CAUTI to Preventing Urinary Catheter Harm
 From Defeating CAUTI to Preventing Urinary Catheter Harm Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University Senior Medical Director, Center of Excellence for Antimicrobial Stewardship
From Defeating CAUTI to Preventing Urinary Catheter Harm Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University Senior Medical Director, Center of Excellence for Antimicrobial Stewardship
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers
 Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
ICU - Sepsis, CAUTI and CLABSI Less May Be Better. HRET HIIN ICU Virtual Event April 11, 2017
 ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
When is it really a UTI?
 When is it really a UTI? Adrienne Mims, MD, MPH, FAAFP, AGSF VP, Chief Medical Officer Adrienne.Mims@AlliantQuality.org 2/19/2016 1 Disclosure This educational activity does not have commercial support
When is it really a UTI? Adrienne Mims, MD, MPH, FAAFP, AGSF VP, Chief Medical Officer Adrienne.Mims@AlliantQuality.org 2/19/2016 1 Disclosure This educational activity does not have commercial support
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
RELIAFIT MALE URINARY DEVICE. Case Study
 RELIAFIT MALE URINARY DEVICE Case Study Quality Improvement Initiative Successful in Achieving CAUTI Reduction Mary Fitzwater, RN INTRODUCTION Catheter-associated urinary tract infections (CAUTI) negatively
RELIAFIT MALE URINARY DEVICE Case Study Quality Improvement Initiative Successful in Achieving CAUTI Reduction Mary Fitzwater, RN INTRODUCTION Catheter-associated urinary tract infections (CAUTI) negatively
Early Management Bundle, Severe Sepsis/Septic Shock
 Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Hospital Acquired Conditions. Tracy Blair MSN, RN
 Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT
 04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
04/24/13 1 SKILLED NURSING FACILITY HOSPITAL COLLABORATION: ANTIOCH & LONE TREE CONVALESCENT Phylene Sunga, NHA Wednesday, April 24, 2013 Change is NOW and NOT Tomorrow "If I am interested in change I
Current Status: Active PolicyStat ID: Guideline: Sepsis Identification And Management in Adults GUIDELINE: COPY
 Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Running head: EBN & CAUTIS 1
 Running head: EBN & CAUTIS 1 Evidence-Based Nursing & Reducing Catheter-Associated Urinary Tract Infections Dana L Knoll Ferris State University EBN & CAUTIS 2 Evidence-Based Nursing & Reducing Catheter-Associated
Running head: EBN & CAUTIS 1 Evidence-Based Nursing & Reducing Catheter-Associated Urinary Tract Infections Dana L Knoll Ferris State University EBN & CAUTIS 2 Evidence-Based Nursing & Reducing Catheter-Associated
2/20/2017. Are You Addressing the New #1 Patient Harm in Your Hospital? Pneumonia NOT Related to a Ventilator
 Barbara Quinn, RN, ANCS-BC Sutter Medical Center, Sacramento, CA Are You Addressing the New #1 Patient Harm in Your Hospital? Pneumonia NOT Related to a Ventilator The story of May and how we began this
Barbara Quinn, RN, ANCS-BC Sutter Medical Center, Sacramento, CA Are You Addressing the New #1 Patient Harm in Your Hospital? Pneumonia NOT Related to a Ventilator The story of May and how we began this
Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation
 Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation Christine Aceves, MSN, RN, CEN, CNL Sepsis Program Manager, Stanford Health Care Santa Clara County Sepsis Collaborative
Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation Christine Aceves, MSN, RN, CEN, CNL Sepsis Program Manager, Stanford Health Care Santa Clara County Sepsis Collaborative
Sepsis/Septic Shock Pre-Hospital Care
 Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Indwelling Urinary Catheters: A One- Point Restraint?
 Broadcast live from... Outline The Technical & Socio-Adaptive Aspects of Preventing -Associated Urinary Tract Infection Sanjay Saint, MD, MPH George Dock Professor of Internal Medicine Ann Arbor VAMC &
Broadcast live from... Outline The Technical & Socio-Adaptive Aspects of Preventing -Associated Urinary Tract Infection Sanjay Saint, MD, MPH George Dock Professor of Internal Medicine Ann Arbor VAMC &
Antimicrobial Stewardship in Continuing Care. Nursing Home Acquired Pneumonia Clinical Checklist
 Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Medicare Value Based Purchasing August 14, 2012
 Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures. Today s Presenters
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures National Content Webinar Series October 15, 2015 Today s Presenters Barbara
AHRQ Safety Program for Long-term Care: HAIs/CAUTI The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures National Content Webinar Series October 15, 2015 Today s Presenters Barbara
Eliminating Catheter-Associated Urinary Tract Infections: Implementing a Quality Improvement Project
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Healthcare-Associated Infections
 Healthcare-Associated Infections A healthcare crisis requiring European leadership Healthcare-associated infections (HAIs - also referred to as nosocomial infections) are defined as an infection occurring
Healthcare-Associated Infections A healthcare crisis requiring European leadership Healthcare-associated infections (HAIs - also referred to as nosocomial infections) are defined as an infection occurring
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
The Urine Dipstick: A Quick Way To Over-Treat! Ann McFeeters, RN Infection Control Practitioner September 26, 2012
 The Urine Dipstick: A Quick Way To Over-Treat! Ann McFeeters, RN Infection Control Practitioner September 26, 2012 Objectives Discuss what is a Urinary Tract Infection (UTI) Reflect on current practices
The Urine Dipstick: A Quick Way To Over-Treat! Ann McFeeters, RN Infection Control Practitioner September 26, 2012 Objectives Discuss what is a Urinary Tract Infection (UTI) Reflect on current practices
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents. Payment Model
 Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
Understand. Learning Objectives Module 1. Surviving Sepsis Campaign Sepsis e learn Module 1. Situation & Background. Sepsis e Learn: Module 1
 Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
BEHAVIORAL HEALTH & LTC. Mary Ann Kellar, RN, MA, CHES, IC March 2011
 BEHAVIORAL HEALTH & LTC Mary Ann Kellar, RN, MA, CHES, IC March 2011 CDC Isolation Guidelines-adapting to special environments MDRO s CMS-F 441 C.difficile Norovirus Federal (CMS), State & Joint Commission
BEHAVIORAL HEALTH & LTC Mary Ann Kellar, RN, MA, CHES, IC March 2011 CDC Isolation Guidelines-adapting to special environments MDRO s CMS-F 441 C.difficile Norovirus Federal (CMS), State & Joint Commission
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Evidence Based Practices to Prevent HAIs/CAUTI and Improve Resident Safety
 AHRQ Safety Program for Long term Care: HAIs/CAUTI Evidence Based Practices to Prevent HAIs/CAUTI and Improve Resident Safety Objectives Upon completion of this module, participants will be able to: Describe
AHRQ Safety Program for Long term Care: HAIs/CAUTI Evidence Based Practices to Prevent HAIs/CAUTI and Improve Resident Safety Objectives Upon completion of this module, participants will be able to: Describe
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU)
") Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals
 Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis
 Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success
 Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success May 15, 2013 Sharon Bradley, RN, CIC Senior Infection Prevention Analyst Pennsylvania Patient Safety Authority
Bridging the Gap Between Research and Practice in Long- Term Care An Innovative Model for Success May 15, 2013 Sharon Bradley, RN, CIC Senior Infection Prevention Analyst Pennsylvania Patient Safety Authority
Chasing Zero Infections Webinar: Reducing Sepsis September 15, 2017
 Chasing Zero Infections Webinar: Reducing Sepsis September 15, 2017 Agenda Welcome & HIIN Update Sally Forsberg, RNC-OB, BSN, MBA, NEA-BC, CPHQ, Clinical Performance Improvement Advisor, FHA Reducing Sepsis
Chasing Zero Infections Webinar: Reducing Sepsis September 15, 2017 Agenda Welcome & HIIN Update Sally Forsberg, RNC-OB, BSN, MBA, NEA-BC, CPHQ, Clinical Performance Improvement Advisor, FHA Reducing Sepsis
Kansas Heart and Stroke Collaborative
 Sepsis in the Long Term Care Facility Aligning with Requirements of Participation Dr. Bob Moser, MD F.A.A.F.P Executive Director, Kansas Heart & Stroke Collaborative University of Kansas Health System
Sepsis in the Long Term Care Facility Aligning with Requirements of Participation Dr. Bob Moser, MD F.A.A.F.P Executive Director, Kansas Heart & Stroke Collaborative University of Kansas Health System
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Lightning Overview: Infection Control
 Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
RCFE ADMINISTRATOR INITIAL CERTIFICATION PROGRAM
 RCFE ADMINISTRATOR INITIAL CERTIFICATION PROGRAM Day 5 DAY 5 1) Physical Needs Monitoring residents for changes in condition Health-related services Allowable, restricted, and prohibited conditions Diabetes
RCFE ADMINISTRATOR INITIAL CERTIFICATION PROGRAM Day 5 DAY 5 1) Physical Needs Monitoring residents for changes in condition Health-related services Allowable, restricted, and prohibited conditions Diabetes
Presenters. Tiffany Osborn, MD, MPH. Laura Evans, MD MSc. Arjun Venkatesh, MD, MBA, MHS
 Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Right Sizing Healthcare-Associated Infection Prevention Measures for Critical Access Hospitals. Bonnie M. Barnard, MPH, CIC
 Right Sizing Healthcare-Associated Infection Prevention Measures for Critical Access Hospitals Bonnie M. Barnard, MPH, CIC Objectives Describe the features of critical access hospitals (CAHs) Describe
Right Sizing Healthcare-Associated Infection Prevention Measures for Critical Access Hospitals Bonnie M. Barnard, MPH, CIC Objectives Describe the features of critical access hospitals (CAHs) Describe
The 5 W s of the CMS Core Quality Process and Outcome Measures
 The 5 W s of the CMS Core Quality Process and Outcome Measures Understanding the process and the expectations Developed by Kathy Wonderly RN,BSPA, CPHQ Performance Improvement Coordinator Developed : September
The 5 W s of the CMS Core Quality Process and Outcome Measures Understanding the process and the expectations Developed by Kathy Wonderly RN,BSPA, CPHQ Performance Improvement Coordinator Developed : September
19th Annual. Challenges. in Critical Care
 19th Annual Challenges in Critical Care A Multidisciplinary Approach Friday August 22, 2014 The Hotel Hershey 100 Hotel Road Hershey, Pennsylvania 17033 A continuing education service of Penn State College
19th Annual Challenges in Critical Care A Multidisciplinary Approach Friday August 22, 2014 The Hotel Hershey 100 Hotel Road Hershey, Pennsylvania 17033 A continuing education service of Penn State College
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
BUGS BE GONE: Reducing HAIs and Streamlining Care!
 BUGS BE GONE: Reducing HAIs and Streamlining Care! SUSAN WHITNEY, RN, PCCN, MM, BME FLORIDA HOSPITAL ORLANDO, FL SUWHIT@AOL.COM LEARNING OUTCOMES 1. Describe HAI s and the impact disposable ECG leads have
BUGS BE GONE: Reducing HAIs and Streamlining Care! SUSAN WHITNEY, RN, PCCN, MM, BME FLORIDA HOSPITAL ORLANDO, FL SUWHIT@AOL.COM LEARNING OUTCOMES 1. Describe HAI s and the impact disposable ECG leads have
Engaging Residents and Families in HAIs/CAUTI Prevention. Presenters
 AHRQ Safety Program for Long term Care: Engaging Residents and Families in Prevention National Content Webinar Series for Core Team January 21, 2016 Presenters Kathy Bradley, Family Member CEO and Executive
AHRQ Safety Program for Long term Care: Engaging Residents and Families in Prevention National Content Webinar Series for Core Team January 21, 2016 Presenters Kathy Bradley, Family Member CEO and Executive
A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals
 A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals Joshua Dunn, Pharm.D. Anne Teichman, Pharm.D. School of Pharmacy University of Charleston Charleston WV Corresponding author:
A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals Joshua Dunn, Pharm.D. Anne Teichman, Pharm.D. School of Pharmacy University of Charleston Charleston WV Corresponding author:
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management
 SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
Is It Really a UTI? Do You Know It When You See It?
 Is It Really a UTI? Do You Know It When You See It? Today s Objectives 1. Define Symptomatic UTI versus Asymptomatic Bacteriuria 2. Review RAI MDS Coding Manual Definition of UTI 3. Analyze UTI as a Quality
Is It Really a UTI? Do You Know It When You See It? Today s Objectives 1. Define Symptomatic UTI versus Asymptomatic Bacteriuria 2. Review RAI MDS Coding Manual Definition of UTI 3. Analyze UTI as a Quality
APPLICATION FORM. Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes. Director of Quality
 APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
For audio, join by telephone at , participant code #
 For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
HIMSS Davies Enterprise Application --- COVER PAGE ---
 HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
Antibiotic Use and Resistance in Nursing Homes
 Antibiotic Use and Resistance in Nursing Homes GHINWA DUMYATI, MD PROFESSOR OF MEDICINE CENTER FOR COMMUNITY HEALTH UNIVERSITY OF ROCHESTER MEDICAL CENTER FEBRUARY 8, 2017 Nicolle LE, et al. Antimicrobial
Antibiotic Use and Resistance in Nursing Homes GHINWA DUMYATI, MD PROFESSOR OF MEDICINE CENTER FOR COMMUNITY HEALTH UNIVERSITY OF ROCHESTER MEDICAL CENTER FEBRUARY 8, 2017 Nicolle LE, et al. Antimicrobial
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT
, PREVENTION AND TREATMENT") COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Treatments POLICY NUMBER: 420 Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT 1.
COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Treatments POLICY NUMBER: 420 Effective Date: August 31, 2006 SUBJECT: PRESSURE SORE (DECUBITUS ULCER), PREVENTION AND TREATMENT 1.
Advanced Measurement for Improvement Prework
 Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
Infection Prevention, Control & Immunizations
 Infection Control: This facility task must be used to investigate compliance at F880, F881, and F883. For the purpose of this task, staff includes employees, consultants, contractors, volunteers, and others
Infection Control: This facility task must be used to investigate compliance at F880, F881, and F883. For the purpose of this task, staff includes employees, consultants, contractors, volunteers, and others
Critical Thinking Steps
 CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
Quality Improvement in the ICU: A Way Forward
 Quality Improvement in the ICU: A Way Forward Ognjen Gajic M.D. Mayo Clinic Rochester MN, USA Multidisciplinary Epidemiology and Translational Research in Intensive Care, Emergency and Perioperative Medicine
Quality Improvement in the ICU: A Way Forward Ognjen Gajic M.D. Mayo Clinic Rochester MN, USA Multidisciplinary Epidemiology and Translational Research in Intensive Care, Emergency and Perioperative Medicine
Sepsis The Silent Killer in the NHS
 Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care. Dial in # 855/ Reference conference ID#
 MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care Dial in # 855/427-9512 Reference conference ID# 61200088 Implementing a Hospital Wide Sepsis Program: Strategies and Challenges
MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care Dial in # 855/427-9512 Reference conference ID# 61200088 Implementing a Hospital Wide Sepsis Program: Strategies and Challenges
Stop Sepsis: Evidence Based Strategies to Decrease Mortality Across the Continuum
 Stop Sepsis: Evidence Based Strategies to Decrease Mortality Across the Continuum Angela Craig APN, MS, CCNS Clinical Nurse Specialist Critical Care Cookeville Regional Medical Center Cookeville, TN acragi@crmchealth.org
Stop Sepsis: Evidence Based Strategies to Decrease Mortality Across the Continuum Angela Craig APN, MS, CCNS Clinical Nurse Specialist Critical Care Cookeville Regional Medical Center Cookeville, TN acragi@crmchealth.org
DEVELOPMENT OF AN INFECTION CONTROL PROGRAM FOR LONG-TERM CARE FACILITIES. Evelyn Cook, RN, CIC Associate Director
 DEVELOPMENT OF AN INFECTION CONTROL PROGRAM FOR LONG-TERM CARE FACILITIES Evelyn Cook, RN, CIC Associate Director Understanding Long-Term Care Varying terms and degrees of inclusiveness Difficult to have
DEVELOPMENT OF AN INFECTION CONTROL PROGRAM FOR LONG-TERM CARE FACILITIES Evelyn Cook, RN, CIC Associate Director Understanding Long-Term Care Varying terms and degrees of inclusiveness Difficult to have
Goals today 6/14/2011. Disclosures, 2004-May Sepsis A Medical Emergency. Jim O Brien, MD, MSc So what is sepsis anyway?
 Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
CMS and NHSN: What s New for Infection Preventionists in 2013
 CMS and NHSN: What s New for Infection Preventionists in 2013 Joan Hebden RN, MS, CIC Clinical Program Manager Sentri7 Wolters Kluwer Health - Clinical Solutions Objectives Define the current status of
CMS and NHSN: What s New for Infection Preventionists in 2013 Joan Hebden RN, MS, CIC Clinical Program Manager Sentri7 Wolters Kluwer Health - Clinical Solutions Objectives Define the current status of
Initial Pool Process: Resident Interview
 Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
June 24, Dear Ms. Tavenner:
 1275 K Street, NW, Suite 1000 Washington, DC 20005-4006 Phone: 202/789-1890 Fax: 202/789-1899 apicinfo@apic.org www.apic.org June 24, 2013 Ms. Marilyn Tavenner Administrator Centers for Medicare & Medicaid
1275 K Street, NW, Suite 1000 Washington, DC 20005-4006 Phone: 202/789-1890 Fax: 202/789-1899 apicinfo@apic.org www.apic.org June 24, 2013 Ms. Marilyn Tavenner Administrator Centers for Medicare & Medicaid
Objectives 2/23/2011. Crossing Paths Intersection of Risk Adjustment and Coding
 Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
August 28, Dear Ms. Tavenner:
 August 28, 2013 Ms. Marilyn Tavenner Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services Room 445-G Hubert H. Humphrey Building 200 Independence Avenue,
August 28, 2013 Ms. Marilyn Tavenner Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services Room 445-G Hubert H. Humphrey Building 200 Independence Avenue,
August 1, 2012 (202) CMS makes changes to improve quality of care during hospital inpatient stays
 CMS makes changes to improve quality of care during hospital inpatient stays") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
WHY IMPLEMENT CENTRAL LINE INSERTION BUNDLES
 WHY IMPLEMENT CENTRAL LINE INSERTION BUNDLES WHY IMPLEMENT A CENTRAL LINE BUNDLE? Hospital-acquired infections (HAIs) are the fourth largest killer in America. The death toll from HAIs is estimated at
WHY IMPLEMENT CENTRAL LINE INSERTION BUNDLES WHY IMPLEMENT A CENTRAL LINE BUNDLE? Hospital-acquired infections (HAIs) are the fourth largest killer in America. The death toll from HAIs is estimated at
APIC Questions with Answers. NHSN FAQ Webinar. Wednesday, September 9, :00-3:00 PM EST
 APIC Questions with Answers NHSN FAQ Webinar Wednesday, September 9, 2015 2:00-3:00 PM EST General Questions We are an acute general hospital - psych, do we need to be reporting anything to NSHN? Yes,
APIC Questions with Answers NHSN FAQ Webinar Wednesday, September 9, 2015 2:00-3:00 PM EST General Questions We are an acute general hospital - psych, do we need to be reporting anything to NSHN? Yes,
Charting the Future: Implications and Insights for Informatics. Dana Alexander RN MSN MBA FHIMSS FAAN
 Charting the Future: Implications and Insights for Informatics Dana Alexander RN MSN MBA FHIMSS FAAN Conflict of Interest Disclosure Dana Alexander RN Has no real or apparent conflicts of interest to report.
Charting the Future: Implications and Insights for Informatics Dana Alexander RN MSN MBA FHIMSS FAAN Conflict of Interest Disclosure Dana Alexander RN Has no real or apparent conflicts of interest to report.
Care Coordination What Matters
 Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Care Coordination What Matters Researchers, Improvers, Providers, Patients and Caregivers Jane Brock, MD, MSPH Telligen 2 A little background how did we get here? Transitional care/care coordination A
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum. May 2015 avalere.com
 Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
2014 Partnership in Prevention Award. November 21, :00-1:00PM EST. Introduction
 2014 Partnership in Prevention Award November 21, 2014 12:00-1:00PM EST Introduction Don Wright, MD, MPH Deputy Assistant Secretary for Health (Disease Prevention and Health Promotion) U.S. Department
2014 Partnership in Prevention Award November 21, 2014 12:00-1:00PM EST Introduction Don Wright, MD, MPH Deputy Assistant Secretary for Health (Disease Prevention and Health Promotion) U.S. Department
Hospitals Face Challenges Implementing Evidence-Based Practices
 United States Government Accountability Office Report to Congressional Requesters February 2016 PATIENT SAFETY Hospitals Face Challenges Implementing Evidence-Based Practices GAO-16-308 February 2016 PATIENT
United States Government Accountability Office Report to Congressional Requesters February 2016 PATIENT SAFETY Hospitals Face Challenges Implementing Evidence-Based Practices GAO-16-308 February 2016 PATIENT
Joint Commission NPSG 7: 2011 Update and 2012 Preview
 Joint Commission NPSG 7: 2011 Update and 2012 Preview Pharmacy OneSource Webinar June 1, 2011 Louise M. Kuhny, RN, MPH, MBA, CIC The Joint Commission Objectives Upon completion of this program, participants
Joint Commission NPSG 7: 2011 Update and 2012 Preview Pharmacy OneSource Webinar June 1, 2011 Louise M. Kuhny, RN, MPH, MBA, CIC The Joint Commission Objectives Upon completion of this program, participants
Commissioning for Quality & Innovation (CQUIN)
") Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance
 Open Call Series #1 Surveillance") Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance Diane Dohm MT, IP, CIC, CPHQ MetaStar February 6, 2018 IPC Open calls: Bi-weekly Series Surveillance What data should
Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance Diane Dohm MT, IP, CIC, CPHQ MetaStar February 6, 2018 IPC Open calls: Bi-weekly Series Surveillance What data should
Worth a Thousand Words: Telling a Story with Data
 A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
Goal Elements of Performance APIC Comments APIC Recommendations
 Association for Professionals in Infection Control and Epidemiology, Inc. Comments on the Joint Commission s Proposed 2012 National Patient Safety Goals The Joint Commission Practice Guidance Team Accreditation
Association for Professionals in Infection Control and Epidemiology, Inc. Comments on the Joint Commission s Proposed 2012 National Patient Safety Goals The Joint Commission Practice Guidance Team Accreditation
August 22, Dear Sir or Madam:
 August 22, 2012 Office of Disease Prevention and Health Promotion 1101 Wootton Parkway Suite LL100 Rockville, MD 20852 Attention: Draft Phase 3 Long-Term Care Facilities Module Dear Sir or Madam: The Society
August 22, 2012 Office of Disease Prevention and Health Promotion 1101 Wootton Parkway Suite LL100 Rockville, MD 20852 Attention: Draft Phase 3 Long-Term Care Facilities Module Dear Sir or Madam: The Society
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers
 Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to