Clinic-Based Retention in Care: Description, Outcomes, and Lessons Learned Jenna Donovan, MPH Byrd Quinlivan, MD Aimee Wilkin, MD Amy Heine, NP
|
|
|
- Patricia Sibyl Casey
- 6 years ago
- Views:
Transcription

1 Clinic-Based Retention in Care: Description, Outcomes, and Lessons Learned Jenna Donovan, MPH Byrd Quinlivan, MD Aimee Wilkin, MD Amy Heine, NP
2 Disclosures Jenna Donovan has no financial interest to disclose. Byrd Quinlivan has no financial interest to disclose. Aimee Wilkin receives research funding from Gilead, Janssen and Pfizer but that does not affect this presentation. Amy Heine has no financial interest to disclose. Grant Support: This project is supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under Systems Linkages for Access to Care Initiative (H97HA22695) and support did not include non-governmental sources. This information, content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, the US Government, or the NCDHHS. This continuing education activity is managed and accredited by Professional Education Services Group in cooperation with HSRA and LRG. PESG, HSRA, LRG and all accrediting organization do not support or endorse any product or service mentioned in this activity. PESG, HRSA, and LRG staff has no financial interest to disclose.
3 NC-LINK Research & Implementation Team NCDPH -AIDS Care Program Duke Region 4: Central Carolina Region 7: Southeastern Region J. Clymore V. Mobley C. Jones M.B. Cox J. Donovan L. Sampson K. Sullivan H. Parnell M. Berger R. Jensen D. Safley S. Willis J. Hatcher J. Hopkins M. Yates D. Rodriguez S. Curry C. Stokes S. Griffin C. Long UNC- CH Region 3: Wake Forest Region 5: Dogwood Healthcare Region 10: East Carolina B. Quinlivan A. Sena-Soberano H. Swygard C. Gay A. Heine E. Klein T. Coleman A. LeViere A. Wilkin J. Keller J. Switzer S. Smith A. Cawthorne B. Fields Y. Early K. Daniels D. Campbell N. Fadul L. Todd A. Boyer B. White
4 Learning Objectives 1. The learner will understand how Out-of-Care lists can be generated and worked in various clinic settings 2. The learner with be able to describe key findings of this intervention, both qualitative and quantitative, and how they can be used to inform future implementation of similar protocols 3. The learner will be able to assess the needs and capacity of their own clinic to develop retention efforts.
5 Obtaining CME/CE Credit If you would like to receive continuing education credit for this activity, please visit:
6 Setting: HIV in North Carolina
7 North Carolina HIV/AIDS Epidemiology 28,101: estimated total number of persons living with HIV at the end of ,347: reported new diagnoses of HIV infection in per 100,000: three-year average HIV diagnosis rate ( ) 31.0 per 100,000: three-year average HIV diagnosis rate in Mecklenburg County (Charlotte)- county with the highest rate in the state African Americans accounted for 64% of all new HIV cases in 2013
8 NC HIV Care Structure NC receives HRSA Ryan White Part B funds through the NC Department of Health and Human Services, Division of Public Health Part B funds are distributed among 10 HIV Ryan White HIV care regions covering 95 of NC s 100 counties Remaining 5 counties are in the HRSA Part A TGA area, funded through the Mecklenburg County Health Department (in Charlotte)
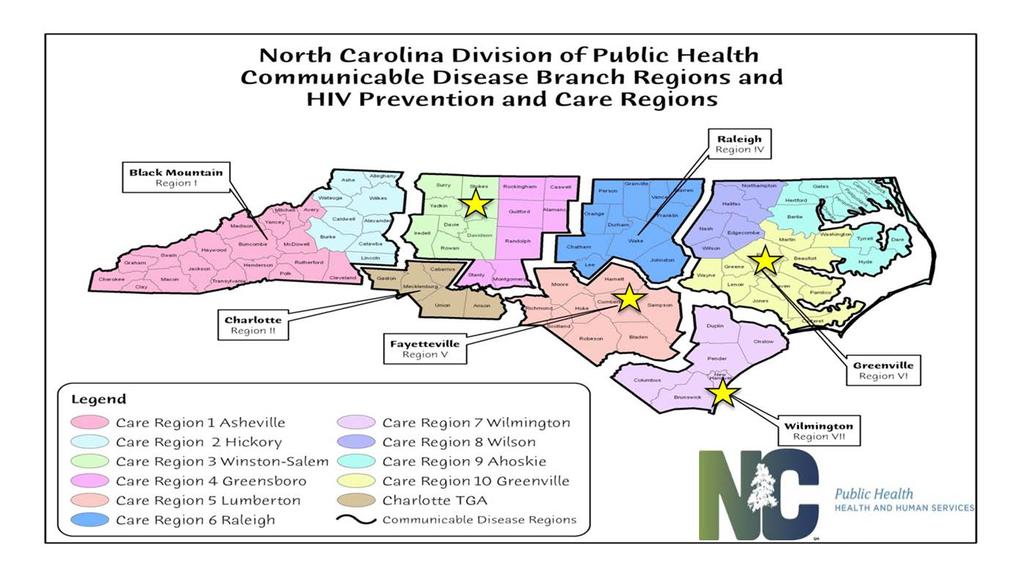
9
10 Challenges in NC HIV Care: Prior to NC-LINK NC HIV Prevention (6) and Care Regions (10) within the state were not aligned Large geographic distances with limited fieldwork capacity for linkage and retention staff within regions/clinics Efforts to re-engage clients being conducted at state level were challenging when conducted by DIS (punitive role) Need for a more supportive role for working with clients and more training Lack of streamlined processes for clinics/regional networks of care to collaborate with others across the state to locate clients or document efforts (i.e. could lead to duplicative work)
11 NC LINK Overview
12 What is NC-LINK? Four-year HRSA Special Projects of National Significance (SPNS) demonstration project NC one of six states to receive funding Follows the goals of the National HIV/AIDS Strategy Purpose: Increase the number of people living with HIV/AIDS engaged in consistent care by creating a system of linkages along the HIV Continuum of Care in NC Funded through the Communicable Disease Branch at the North Carolina Division of Public Health Partnership between Duke University, University of North Carolina- Chapel Hill and intervention sites around the state Key strategies: alternative HIV testing and retention and reengagement efforts for quality and consistent HIV care
13 Overview of Final NC-LINK Interventions Clinic-based HIV Testing Offers an individual who accompanies an HIV-positive patient to a clinic appointment the opportunity to receive free and confidential rapid HIV testing at the clinic Retention Protocol Implemented at the clinic and regional levels to re-engage patients who have not had an HIV care appointment in a designated time period (usually 6-9 months) State Bridge Counseling Linkage and Re-engagement Program at NCDHHS, Communicable Diseases Branch to ensure rapid linkage to care for people who have been newly-diagnosed with HIV and to re-engage PLWH who have been out of care 12 months
14 NC-LINK Pilot Phase ( ) Learning Collaborative Model Formal Collaborative Structure Conference calls monthly with pilot sites Stakeholder meetings, at six months Presentations by test site staff PDSA cycles Availability of team for technical assistance 4 clinic, 2 statewide interventions tested 4 interventions selected for expansion: HIV Partner Testing, SBC Linkage, Retention Protocol, SBC Reengagement
15 NC-LINK Expansion Phase ( ) Expanded the interventions deemed successful during the pilot phase to additional sites throughout North Carolina: HIV Partner Testing 2 Regional Networks of Care Retention Protocol 4 Regional Networks of Care State Bridge Counselors Each Prevention Region has at least 1 SBC with an additional 3 Special Population SBCs provided through CAPUS funding
16 Focus: Clinic-Based Retention Protocol
17 Retention Protocol Overview Focuses on improving the capacity of regional and clinic based retention staff to retain HIV+ individuals in care and to engage those who are lost-to-care back into consistent HIV care Piloted at large academic medical center with approximately 2,000 HIV patients Determined best processes for looking for clients as well as methods for retention staff to document their efforts Decided to utilize CAREWare - required software for Part B providers in NC Allowed for electronic referrals between providers that share the same client in different institutions/agencies. Currently have 4 Part B Regional Networks of Care (with a total of 13 agencies) participating in the Retention Protocol
18 Step by Step Process of NC-LINK Retention Protocol On the first day of the month, clinic runs a list of out-of-care clients (those who have not had a medical care visit in 6-9 months or more) Data manager runs the out-of-care list through clinic EMR or CAREWare (CW) List is checked to remove clients who are not truly out-of-care due to special circumstances or who have upcoming appointments Clinic/community-based retention staff receive list from clinic via an electronic CW referral Retention staff work on locating client for roughly 30 days Work conducted from clinic/agency - not generally done via fieldwork
19 Examples of Local Efforts to Locate Clients Check EMR/local CAREWare for any contact since the last medical visit Call all of patient s phone numbers in the chart as well and any old numbers (3 phone calls on 3 separate days) Conduct internet search of local jails, state prisons, federal prison system Check the Social Security Death Index and Google search for potential obituaries and other information about the patient (i.e. pipl.com) Check the state Medicaid Provider Portal to see if they have been in care elsewhere, accessed EDs or had an inpatient stay, and if there is different contact info in the record Call last pharmacy and see if any other refills have occurred since last medical visit and get any contact info available/info on other prescribing providers Call any home health agency/dialysis center/other provider that can be identified to obtain current contact info or get a message through to the patient Send out a generic letter to last known address encouraging patient to get in touch if no phone calls have been successful
20 Step by Step Process of Retention Protocol (cont.) After 30-day time period of locating, retention staff document efforts and provide outcomes via CAREWare Clinic closes out clients who have been located or a definitive outcome has been determined. Outcomes documented include: Re-engaged in care at referring provider Re-engaged in care with new provider Deceased Re-located Incarcerated Located, not re-engaged in care to-date Unknown-not located Unknown, not located clients and Located, not re-engaged in care todate clients referred to State Bridge Counselor for state-level followup/field work
21 CAREWare Demonstration

22 On or near the first day of the month, the clinic ran an Out-of-Care report to list all patients who have not had a medical care visit in 6 months or more.

23 From the list generated by the out-of-care report, an outgoing internal referral to clinic retention staff was entered at the clinic for each client being referred for clinic-based retention services.
24 Outgoing referrals were displayed on the main menu screen of the clinic s domain.

25 After the referrals were made, the incoming referrals were displayed on the main menu screen when the retention staff logged in to CAREWare.

26 Both outgoing and incoming referrals in CAREWare were monitored and tracked. Reports to do so were created by going to the main menu in CAREWare, clicking reports then selecting Referrals


27 Either Outgoing/External or Incoming and then Select All were selected, followed by clicking Run Report.

28 A Referrals report showed all incoming or outgoing referrals and their current status (pending or completed) but could be customized to show specific status only or results within specific date spans, etc. The Received Date on the report is the completion date, or the date the client referral was resolved/closed by clinic retention staff or the State Bridge Counselor (if additional referral was necessary).



29 Demographics tab: As retention staff worked on patient referrals, they updated demographic information on each patient in the appropriate fields. Any additional contact phone numbers were entered in the common notes field.
30 A custom NC-LINK tab was created to track the time and activities retention staff used to attempt to locate and re-engage out-of-care patient referrals.
 Navigator type (role of retention staff member) # of min for other pt-related activities NOT w/ pt (number of minutes spent working on activities on")
31 After locating the client, every time the retention staff worked on a client record, a Bridge Counselor Service was entered in CAREWare (potentially multiple entries on a single day), entering: BC Provided by (name of retention staff member) Navigator type (role of retention staff member) # of min for other pt-related activities NOT w/ pt (number of minutes spent working on activities on behalf of the client, but not with the client) Type of contact (referred to a contact with the client, if there was one that day) If in person, where? (referred to the location of the in-person contact with the client) Total contact minutes (referred to the TOTAL number of minutes spent in direct contact with the client. Click on all checkboxes that reflect barriers that were addressed and/or services that were provided during that encounter with the client.
32 At the end of the month, the retention staff closed the records in their CAREWare domain for which clinic based retention activities were completed by: 1) Making sure that all data fields were completed on the NC-LINK tab.

33 2) Entering a Bridge Counseling Service Outcome service on the Service tab in CAREWare for each client that was referred to them for Bridge Counseling that month and completing all custom service fields.

34 3) Still on the Service tab, changing the Enrl Status to the most appropriate choice: Referred or Discharged, Incarcerated, or Relocated. The date the work was completed for the client record was entered in the Case Closed: field. The Vital Status was changed if the client is found to be deceased and the Deceased Date was entered, if known.
35 Referral for Additional Follow-up Clients with a regional bridge counseling outcome of Located, not reengaged in care to-date or Unknown-not located were referred to the appropriate State Bridge Counselor (SBC) by the clinic retention staff or data manager via CAREWare using the electronic referral functionality. When the SBC located the client or exhausted all resources looking for the client, the SBC closed the record in CAREWare. Those clients with an SBC outcome status of deceased, relocated, incarcerated, re-engaged in care with new provider, unknown-not located, or located, not re-engaged in care to date, were closed in the clinic domain of CAREWare. These closed client records could be re-opened if the client returned to the clinic for care.
36 Lessons Learned
37 First Steps Before Implementing Retention Protocol A cleaned patient database (e.g. EMR, CAREWare, etc.) that will be used to run regular out-of-care lists First out-of-care lists that were run were very long ( patients for larger clinics) that had to be carefully combed through to ensure patients were truly out-of-care and not deceased, relocated, actually in care, etc. Time-consuming process to go through the list, but important to start with an accurate list Need staff members and time for them to clean the database- hard for busy and overburdened clinic staff, but important for data accuracy Once lists are cleaned up, monthly lists are much smaller and easier to manage Clear and agreed-upon definition for an out-of-care patient (e.g. no HIV medical visit in 6 months, 9 months, 12 months?) Delineated roles and responsibilities for staff members involved with the protocol (e.g. data managers, bridge counselors, medical providers, etc)
38 Important Ingredients to a Successful Retention Protocol Run out-of-care lists regularly so they do not increase in size and become harder to manage Helpful to run monthly at the same time (e.g. 1 st of the month, 5 th of the month) so it becomes a routine part of work Leadership buy-in and encouragement is important Help prioritize bridge counseling efforts as important for busy staff Buy-in from the IT group to get data from EMR is critical Training is key for managing data, referrals and bridge counseling efforts Staff turnover is always an issue Need dedicated staff time and space to successfully conduct bridge counseling activities and document these efforts Helpful to have a specific person to do bridge counseling and a data entry/data manager for managing list/handling referrals Strong working relationships within HIV care network and collaborations with outside agencies for bridge counseling efforts is critical (e.g. other clinics, local ASOs, health departments, etc.)
39 Lessons Learned: New Data Entry Process of running out-of-care list and sending electronic referrals for clinic-based retention work did not change Streamlined the data entry process for activities and time to locate and re-engage the patient. No longer have a separate NC-LINK tab and the data entry screen captures the information below: What month the referral was received Min spent attempting to locate the patient now in categories 1-15 min min >60 min Total minutes spent on case after locating patient None/Not applicable 1-15 min min >60 min Did you provide any services to this patient? Yes or No If services were provided, check all that apply: Transportation Medical- provided info or scheduled apt Financial Insurance/benefits
40 Lessons Learned: New Data Entry (cont.) Also modified the possible outcomes of the retention staff activity Deceased Found to be deceased Re-located out of state Found to be living out of state Re-located to new region in NC Found to now be living in a new region, but still within North Carolina Incarcerated Found to be incarcerated Re-engaged in care at referring provider Successfully returned to clinic Re-engaged in care with new provider within region Known to be attending care at a different provider but within the same region. Located in region, not re-engaged in care Patient was found, but did not return to the clinic, or any that you know of, for care. Should be referred to SBC Unknown- not located Could not locate client, should be referred to SBC Patients with outcomes of Unknown- not located and Located in region, not re-engaged in care are still referred to the SBC for additional follow-up.

41 The new data entry is captured by recording a Bridge Counseling Service Outcome entry on the Service tab in CAREWare.
42 Important Ingredients to a Successful Retention Protocol (cont d) Need to decide time-frame for when to stop looking for out-ofcare patients Difficult because you don t want to give up on looking for patients, but also need to be able to keep the list moving forward and recognize limited staff time and resources A patient no-show/cancellation policy also helps identify patients at-risk for becoming out-of-care. Developing a policy of calling and rescheduling patients who missed their appointment helped keep clients from falling out of care and helped decrease the size of the out-of-care list
43 Interactive Checklist: Implementing the Intervention in your own clinic Small Group Activity
44 NC-LINK Retention Protocol Checklist Out of Care: An active patient who has not had a medical visit in months or more Action Run a report in CAREWare or in the provider s electronic medical record software on the of each month (or closest business day to the 1 st ) of all patients with Active status with no medical visit in months or more. Clean the list (e.g. remove individuals with upcoming appts, already on another list, special cases, etc.) Job Title of Person Responsible Name, if Available Necessary Time (% FTE) Place referrals for bridge counseling services (if using CAREWare can put referrals into CAREWare using the electronic referral functionality) Conduct bridge counseling activities Resolve all current referrals by completing the case closure process. Review all client records that have been closed by retention staff. Ensure enrollment status are updated as appropriate and refer Located, not re-engaged in care to date or Unknown-not located records to reengagement staff (State Bridge Counselors SBC) Once the re-engagement activities are finalized, review the outcomes of all the client cases and ensure enrollment statuses are updated as appropriate
45 Retention Protocol Checklist - Larger Agency ~2,000 patients Out of Care Definition: An active patient who has not had a medical visit in 9 months or more Action Run a report in CAREWare by the 1 st of each month of all patients with Active status with no medical visit in 9 months or more. Job Title of Person Responsible Data Manager Necessary Time to Complete Task ~5 minutes Clean the list (for upcoming appts in next 2 months). Document results on Excel spreadsheet. Data Manager ½ day per month Place referrals for bridge counseling services into CAREWare using the electronic referral functionality Data Manager ½ hour per day Conduct bridge counseling activities Patient Navigators 40-50% 1 FTE combined Resolve all current referrals by completing the case closure process. Data Manager ½ hour per day Review all client records (if utilizing external retention staff) and finalize outcomes. Refer Located, not re-engaged in care to date or Unknown-not located to SBC Once the SBC finalizes counseling activities, review the outcomes of all the client cases completed by the SBC and ensure enrollment statuses are updated as appropriate per the SBCs findings. Data Manager Data Manager ½ hour per day ½ hour per day
46 Retention Protocol Checklist - Smaller Agency ~200 patients Out of Care Definition: An active patient who has not had a medical visit in 6 months or more Action Run a report in CAREWare by the 1 st of each month of all patients with Active status with no medical visit in 9 months or more. Job Title of Person Responsible Data Quality Analyst Necessary Time to Complete Task 5-10 mins per month Clean the list (for upcoming appts in next 2 months). Document results on Excel spreadsheet. Data Quality Analyst 30 mins per month Place referrals for bridge counseling services into CAREWare using the electronic referral functionality Data Quality Analyst 1 day per week Conduct bridge counseling activities Patient Navigators 1 day per week Resolve all current referrals by completing the case closure process. Bridge Counselor ½ hour per day Review all client records (if utilizing external retention staff) and finalize outcomes. Refer Located, not re-engaged in care to date or Unknown-not located to SBC Once the SBC finalizes counseling activities, review the outcomes of all the client cases completed by the SBC and ensure enrollment statuses are updated as appropriate per the SBCs findings. Bridge Counselor Bridge Counselor (included in 1 day per week) (included in 1 day per week)
47 Discuss Activity and Q&A with Local Staff John Switzer Data Manager Emily Andrews Patient Navigator Share experiences and answer audience questions
48 Data Manager Q&A What are some common issues that come up with running the list? What are some of the common technical or programmatic issues with referrals? What do you do for folks who have been on the list for more than one month?
49 Patient Navigator Q&A What is your process after receiving a referral? is there a strategy for the order in the list? What seems to be your most useful retention strategy? What about search strategy? Can you share some information about the amount of time/effort spent looking for patients
50 Outcomes of the NC LINK Retention Intervention
51 Retention Intervention Outcome among PLWH who were identified as Out-of-Care Not Found Ineligible Found - Maintained Region Found - Relocated


52 Characteristics of Eligible Out-of-Care PLWH (Not found = 329; Found = 712)
53 HIV Care Outcomes: Care Initiated 100% Care Initiated 80% 60% 40% 20% 0% 90 days 180 days 365 days
54 HIV Care Outcomes: HAB Measure Meets Retention in Care HAB Measure: 2 care markers > 90 days apart No, 319 Yes, 393
55 HIV Care Outcomes: VL Suppression 100% VL Suppression Achieved 80% 60% 40% 20% 0% 90 Days 180 Days 365 Days


56 Outcomes Based on Prior Viral Load Suppression

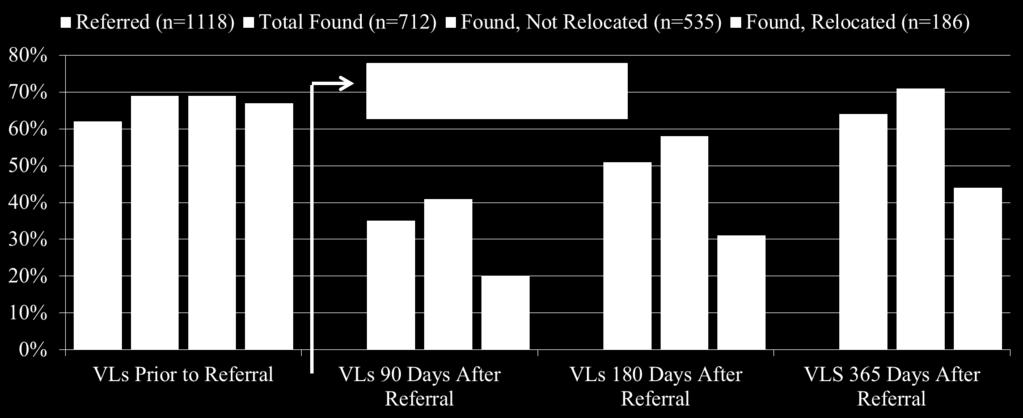
57 12 Month VL Suppression by Retention Outcome
58 Questions?
Transnational Practices and Engagement in Care: Lessons from NYC Rikers Island
 Transnational Practices and Engagement in Care: Lessons from NYC Rikers Island Janet Wiersema, MPH 1,2 Jacqueline Cruzado-Quinones 1 Paul Teixeira, DrPH, MA 3 Alison O. Jordan, LCSW, CPPB 1 1 NYC Health
Transnational Practices and Engagement in Care: Lessons from NYC Rikers Island Janet Wiersema, MPH 1,2 Jacqueline Cruzado-Quinones 1 Paul Teixeira, DrPH, MA 3 Alison O. Jordan, LCSW, CPPB 1 1 NYC Health
Indianapolis Transitional Grant Area Quality Management Plan (Revised)
") Indianapolis Transitional Grant Area Quality Management Plan 2017 2018 (Revised) Serving 10 counties: Boone, Brown, Hamilton, Hancock, Hendricks, Johnson, Marion, Morgan, Putnam and Shelby 1 TABLE OF CONTENTS
Indianapolis Transitional Grant Area Quality Management Plan 2017 2018 (Revised) Serving 10 counties: Boone, Brown, Hamilton, Hancock, Hendricks, Johnson, Marion, Morgan, Putnam and Shelby 1 TABLE OF CONTENTS
SPNS Video Conferencing Intervention in LA State Prisons
 SPNS Video Conferencing Intervention in LA State Prisons Karissa M. Page, MPH Louisiana Department of Health Office of Public Health, STD/HIV Program Disclosures Presenter, Karissa M. Page, has no financial
SPNS Video Conferencing Intervention in LA State Prisons Karissa M. Page, MPH Louisiana Department of Health Office of Public Health, STD/HIV Program Disclosures Presenter, Karissa M. Page, has no financial
2016 NATIONAL RYAN WHITE CONFERENCE ON HIV CARE & TREATMENT
 Innovative Special Project of National Significance (SPNS): Fusing Part A, B, C, & D Data for MyCareContinuum Dashboard and Empowering Consumers with an Award-Winning Low-Health- Literacy Patient Portal
Innovative Special Project of National Significance (SPNS): Fusing Part A, B, C, & D Data for MyCareContinuum Dashboard and Empowering Consumers with an Award-Winning Low-Health- Literacy Patient Portal
!!!! CARE COORDINATION IMPLEMENTATION MANUAL !!!! VIRGINIA DEPARTMENT OF HEALTH SPECIAL PROJECTS OF NATIONAL SIGNIFICANCE
 IMPLEMENTATION MANUAL VIRGINIA DEPARTMENT OF HEALTH SPECIAL PROJECTS OF NATIONAL SIGNIFICANCE SYSTEMS LINKAGES AND ACCESS TO CARE INITIATIVE OCTOBER 2015 Table of Contents Background: System Linkages and
IMPLEMENTATION MANUAL VIRGINIA DEPARTMENT OF HEALTH SPECIAL PROJECTS OF NATIONAL SIGNIFICANCE SYSTEMS LINKAGES AND ACCESS TO CARE INITIATIVE OCTOBER 2015 Table of Contents Background: System Linkages and
Working together to improve HIV/AIDS services in Nevada and the Las Vegas TGA
 Ryan White Part A, B, C, D, F and Prevention Cross Part Collaborative Clinical Plan State of Nevada and the Las Vegas TGA Grant Year 2014-2015 Working together to improve HIV/AIDS services in Nevada and
Ryan White Part A, B, C, D, F and Prevention Cross Part Collaborative Clinical Plan State of Nevada and the Las Vegas TGA Grant Year 2014-2015 Working together to improve HIV/AIDS services in Nevada and
Using Multilingual, Audio-Assisted Web & Mobile Evidence-Based Needs Assessments to Plan, Fund and Actuate Care Services
 Using Multilingual, Audio-Assisted Web & Mobile Evidence-Based Needs Assessments to Plan, Fund and Actuate Care Services Michael McNeill, Health Care Analyst/Administrative Services Coordinator, Wake County
Using Multilingual, Audio-Assisted Web & Mobile Evidence-Based Needs Assessments to Plan, Fund and Actuate Care Services Michael McNeill, Health Care Analyst/Administrative Services Coordinator, Wake County
Ryan White Part A. Quality Management
 Quality Management Central Intake and Eligibility Determination (CIED) 2014 Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal
Quality Management Central Intake and Eligibility Determination (CIED) 2014 Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal
HAB/NQC HIV Cross-Part Care Continuum Collaborative (H4C) Frequently Asked Questions
 Frequently Asked Questions") HAB/NQC HIV Cross-Part Care Continuum Collaborative (H4C) Frequently Asked Questions A) General 1) What is the H4C Collaborative? H4C is an initiative undertaken by the HRSA HIV/AIDS Bureau (HAB) and the
HAB/NQC HIV Cross-Part Care Continuum Collaborative (H4C) Frequently Asked Questions A) General 1) What is the H4C Collaborative? H4C is an initiative undertaken by the HRSA HIV/AIDS Bureau (HAB) and the
Integrating Health Care & Public Health to Improve HIV Early Detection and Control
 Integrating Health Care & Public Health to Improve HIV Early Detection and Control Research In Progress Webinar Thursday, April 20, 2017 1:00-2:00pm ET/ 10:00-11:00am PT Funded by the Robert Wood Johnson
Integrating Health Care & Public Health to Improve HIV Early Detection and Control Research In Progress Webinar Thursday, April 20, 2017 1:00-2:00pm ET/ 10:00-11:00am PT Funded by the Robert Wood Johnson
Quality Management Program
 Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
Improving the Quality and Effectiveness of Medical Case Management HRSA HIV/AIDS Bureau All Grantee Meeting Session 241, November 27, 2012
 Improving the Quality and Effectiveness of Medical Case Management HRSA HIV/AIDS Bureau All Grantee Meeting Session 241, November 27, 2012 Julia Hidalgo, ScD, MSW, MPH Positive Outcomes, Inc. & George
Improving the Quality and Effectiveness of Medical Case Management HRSA HIV/AIDS Bureau All Grantee Meeting Session 241, November 27, 2012 Julia Hidalgo, ScD, MSW, MPH Positive Outcomes, Inc. & George
Ryan White Part A. Quality Management
 Quality Management Medical Case Management 2014 Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal Ryan White CARE Act Part
Quality Management Medical Case Management 2014 Broward County/Fort Lauderdale Eligible Metropolitan Area (EMA) The creation of this public document is fully funded by a federal Ryan White CARE Act Part
Medical Case Management
 Definition: services (including treatment adherence) is the provision of a range of consumer-centered consumer activities focused on improving health outcomes in support of the HIV Care Continuum. Consumer
Definition: services (including treatment adherence) is the provision of a range of consumer-centered consumer activities focused on improving health outcomes in support of the HIV Care Continuum. Consumer
45 CFR 75 Uniform Administrative Requirements, Cost Principles, and Audit Requirements for Health and Human Services Awards
 45 CFR 75 Uniform Administrative Requirements, Cost Principles, and Audit Requirements for Health and Human Services Awards Frances Hodge Public Health Analyst, Southern Services Branch Division of Metropolitan
45 CFR 75 Uniform Administrative Requirements, Cost Principles, and Audit Requirements for Health and Human Services Awards Frances Hodge Public Health Analyst, Southern Services Branch Division of Metropolitan
Ryan White HIV/AIDS Part C Capacity Development Program Pre-Application Technical Assistance Conference Call HRSA January 26, 2017
 Ryan White HIV/AIDS Part C Capacity Development Program Pre-Application Technical Assistance Conference Call HRSA-17-042 January 26, 2017 Department of Health and Human Services Health Resources and Services
Ryan White HIV/AIDS Part C Capacity Development Program Pre-Application Technical Assistance Conference Call HRSA-17-042 January 26, 2017 Department of Health and Human Services Health Resources and Services
The Navigation Program: An Innovative Method for Finding and Re- Engaging Lost HIV Clinic Patients
 The Navigation Program: An Innovative Method for Finding and Re- Engaging Lost HIV Clinic Patients Rhodri Dierst-Davies, MPH Saloniki James, MA Amy Rock Wohl, MPH, PhD Division of HIV and STD Programs
The Navigation Program: An Innovative Method for Finding and Re- Engaging Lost HIV Clinic Patients Rhodri Dierst-Davies, MPH Saloniki James, MA Amy Rock Wohl, MPH, PhD Division of HIV and STD Programs
Integrating Health Care and Public Health to Improve HIV Early Detection and Control Wednesday, January 13, 2016, 12:00 1:00pm ET
 PHSSR Research in Progress Webinar Series Speaker Biographies Integrating Health Care and Public Health to Improve HIV Early Detection and Control Wednesday, January 13, 2016, 12:00 1:00pm ET Presenters
PHSSR Research in Progress Webinar Series Speaker Biographies Integrating Health Care and Public Health to Improve HIV Early Detection and Control Wednesday, January 13, 2016, 12:00 1:00pm ET Presenters
Ryan White HIV/AIDS Treatment Extension Act
 Ryan White HIV/AIDS Treatment Extension Act Administrative Overview Ryan White Part A June 13, 2011 Harold J. Phillips Chief, Northeastern Central Services Branch Department of Health and Human Services
Ryan White HIV/AIDS Treatment Extension Act Administrative Overview Ryan White Part A June 13, 2011 Harold J. Phillips Chief, Northeastern Central Services Branch Department of Health and Human Services
Transforming Overwhelming into Possible: Innovative Models by HIV Pharmacies #6757
 Transforming Overwhelming into Possible: Innovative Models by HIV Pharmacies #6757 Hila Berl, MA, Vice President, EGM Consulting, LLC Catherine Knochel, Business Manager, Walgreens Specialty Pharmacy Alton
Transforming Overwhelming into Possible: Innovative Models by HIV Pharmacies #6757 Hila Berl, MA, Vice President, EGM Consulting, LLC Catherine Knochel, Business Manager, Walgreens Specialty Pharmacy Alton
o Recipients must coordinate these testing services with other HIV prevention and testing programs to avoid duplication of efforts.
 E. GENERAL SERVICE DEFINITIONS & SERVICE DELIVERY The following section provides specific service definitions, service delivery and any special reporting requirements for each of the services funded in
E. GENERAL SERVICE DEFINITIONS & SERVICE DELIVERY The following section provides specific service definitions, service delivery and any special reporting requirements for each of the services funded in
MANAGED CARE READINESS
 MANAGED CARE READINESS A SELF-ASSESSMENT TOOL FOR HIV SUPPORT SERVICE AGENCIES U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES HEALTH RESOURCES & SERVICES ADMINISTRATION HIV/AIDS BUREAU MANAGED CARE READINESS
MANAGED CARE READINESS A SELF-ASSESSMENT TOOL FOR HIV SUPPORT SERVICE AGENCIES U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES HEALTH RESOURCES & SERVICES ADMINISTRATION HIV/AIDS BUREAU MANAGED CARE READINESS
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
2011 Quality Management Plan Wake Forest University Baptist Medical Center Infectious Diseases Specialty Clinic Ryan White Program
 011 Quality Management Plan Wake Forest University Baptist Medical Center Infectious Diseases Specialty Clinic Ryan White Program I. Wake Forest University Baptist Medical Center Mission: Wake Forest University
011 Quality Management Plan Wake Forest University Baptist Medical Center Infectious Diseases Specialty Clinic Ryan White Program I. Wake Forest University Baptist Medical Center Mission: Wake Forest University
Ryan White Part A FY 2017 Housing RFP RFP Conference. Frequently Asked Questions (FAQ) Published November 23 rd, 2016
 Published November 23 rd, 2016") Ryan White Part A FY 2017 Housing RFP RFP Conference Frequently Asked Questions (FAQ) Published November 23 rd, 2016 Questions related to the Section I: Narrative, Instruction, and Attachments Do we need
Ryan White Part A FY 2017 Housing RFP RFP Conference Frequently Asked Questions (FAQ) Published November 23 rd, 2016 Questions related to the Section I: Narrative, Instruction, and Attachments Do we need
DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea
 DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea DISCLOSURES COMPLETING THIS ACTIVITY Successful completion of this continuing education activity
DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea DISCLOSURES COMPLETING THIS ACTIVITY Successful completion of this continuing education activity
Check Hep B Patient Navigation Program
 Check Hep B Patient Navigation Program Nirah Johnson, LCSW Director, Capacity Building & Program Implementation Viral Hepatitis Program New York City Department of Health Hepatitis B in NYC Estimated 100,000
Check Hep B Patient Navigation Program Nirah Johnson, LCSW Director, Capacity Building & Program Implementation Viral Hepatitis Program New York City Department of Health Hepatitis B in NYC Estimated 100,000
Building a Successful Linkage to Continuum of Care Program for Latinos. Pedro Coronado
 Building a Successful Linkage to Continuum of Care Program for Latinos Pedro Coronado Director of Linkage to Continuum of Care Valley AIDS Council-Westbrook Clinic Disclosures Presenter(s) has no financial
Building a Successful Linkage to Continuum of Care Program for Latinos Pedro Coronado Director of Linkage to Continuum of Care Valley AIDS Council-Westbrook Clinic Disclosures Presenter(s) has no financial
MEDICAL CASE MANAGEMENT QI NETWORK March 5, 2013 at 9:30 a.m. Ryan White Part A Program Office 115 S. Andrews Ave., Ft. Lauderdale, FL 33301
 Broward Regional Health Planning Council, Inc. Inc. 200 200 Oakwood Lane, Suite 100 100 Hollywood, Florida 33020 T: T: (954) 561-9681 F: F: (954) 561-9685 MEDICAL CASE MANAGEMENT QI NETWORK March 5, 2013
Broward Regional Health Planning Council, Inc. Inc. 200 200 Oakwood Lane, Suite 100 100 Hollywood, Florida 33020 T: T: (954) 561-9681 F: F: (954) 561-9685 MEDICAL CASE MANAGEMENT QI NETWORK March 5, 2013
Baltimore-Towson EMA Part A Quality Management (QM) Plan I. Introduction
 Plan I. Introduction") Baltimore-Towson EMA Part A Quality Management (QM) Plan 2009-2011 I. Introduction The Baltimore City Health Department (BCHD) is designated the Ryan White Part A Grantee and manages the Clinical Quality
Baltimore-Towson EMA Part A Quality Management (QM) Plan 2009-2011 I. Introduction The Baltimore City Health Department (BCHD) is designated the Ryan White Part A Grantee and manages the Clinical Quality
Exhibit A GENERAL INFORMATION
 GENERAL INFORMATION A. Eligibility 1. What are the criteria for eligibility? Eligibility falls under Rule 64D-4 Florida Administrative Code. Criteria for core eligibility is Proof of HIV, Proof of Living
GENERAL INFORMATION A. Eligibility 1. What are the criteria for eligibility? Eligibility falls under Rule 64D-4 Florida Administrative Code. Criteria for core eligibility is Proof of HIV, Proof of Living
CMS-0044-P; Proposed Rule: Medicare and Medicaid Programs; Electronic Health Record Incentive Program Stage 2
 May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
HIV SERVICES ACUITY TOOL PILOT IMPLEMENTATION MEETING. October 16, 2014
 HIV SERVICES ACUITY TOOL PILOT IMPLEMENTATION MEETING MDPH Office of HIV/AIDS & BPHC HIV/AIDS Ser vices Division October 16, 2014 1 AGENDA Background: How did we get here? Introducing the tool Components
HIV SERVICES ACUITY TOOL PILOT IMPLEMENTATION MEETING MDPH Office of HIV/AIDS & BPHC HIV/AIDS Ser vices Division October 16, 2014 1 AGENDA Background: How did we get here? Introducing the tool Components
Ryan White HIV/AIDS Program Part D Women, Infants, Children, and Youth (WICY) Grants Supplemental Funding
 Grants Supplemental Funding") Ryan White HIV/AIDS Program Part D Women, Infants, Children, and Youth (WICY) Grants Supplemental Funding Pre-Application Technical Assistance Conference Call HRSA-18-044 December 19, 2017 Department of
Ryan White HIV/AIDS Program Part D Women, Infants, Children, and Youth (WICY) Grants Supplemental Funding Pre-Application Technical Assistance Conference Call HRSA-18-044 December 19, 2017 Department of
MENTAL HEALTH / SUBSTANCE ABUSE QI NETWORK April 19, 2013 at 2:00 p.m. Ryan White Part A Program Office 115 S. Andrews Ave., Ft. Lauderdale, FL 33301
 Broward Regional Health Planning Council, Inc. Inc. 200 200 Oakwood Lane, Suite 100 100 Hollywood, Florida 33020 T: T: (954) 561-9681 F: F: (954) 561-9685 MENTAL HEALTH / SUBSTANCE ABUSE QI NETWORK April
Broward Regional Health Planning Council, Inc. Inc. 200 200 Oakwood Lane, Suite 100 100 Hollywood, Florida 33020 T: T: (954) 561-9681 F: F: (954) 561-9685 MENTAL HEALTH / SUBSTANCE ABUSE QI NETWORK April
Cleveland TGA Service Standard of Care
 SERVICE CATEGORY DEFINITION Services: is the provision of nonemergency transportation services that enables an eligible client to access or be retained in core medical and support services. Medical transportation
SERVICE CATEGORY DEFINITION Services: is the provision of nonemergency transportation services that enables an eligible client to access or be retained in core medical and support services. Medical transportation
One Program, Multiple Funding Streams: How to Manage Funding, Resources, and Eligibility
 One Program, Multiple Funding Streams: How to Manage Funding, Resources, and Eligibility AMY DOWNS, MSW RYAN WHITE PART B PROGRAM COORDINATOR JANA COLLINS, MS RYAN WHITE PART C/D PROGRAM COORDINATOR BLUEGRASS
One Program, Multiple Funding Streams: How to Manage Funding, Resources, and Eligibility AMY DOWNS, MSW RYAN WHITE PART B PROGRAM COORDINATOR JANA COLLINS, MS RYAN WHITE PART C/D PROGRAM COORDINATOR BLUEGRASS
Dear Prospective Presenter:
 Dear Prospective Presenter: Page 1 The 2017 South Carolina HIV, STD and Viral Hepatitis Conference Thriving Together for Tomorrow Columbia Metropolitan Convention Center, Columbia, SC October 25-26, 2017
Dear Prospective Presenter: Page 1 The 2017 South Carolina HIV, STD and Viral Hepatitis Conference Thriving Together for Tomorrow Columbia Metropolitan Convention Center, Columbia, SC October 25-26, 2017
New York Presbyterian s HIV Care Cascade: Methodology & Next Steps. Pete Gordon, MD Sam Merrick, MD
 New York Presbyterian s HIV Care Cascade: Methodology & Next Steps Pete Gordon, MD Sam Merrick, MD 1 Cascade Reporting Requirements Open versus Active caseloads - Open: any services at NYP - Active: any
New York Presbyterian s HIV Care Cascade: Methodology & Next Steps Pete Gordon, MD Sam Merrick, MD 1 Cascade Reporting Requirements Open versus Active caseloads - Open: any services at NYP - Active: any
Ryan White Eligibility Determination and Recertification: Improving Efficiency
 Ryan White Eligibility Determination and Recertification: Improving Efficiency Amanda Bowes and Steve Bailey NASTAD OBJECTIVES Review Ryan White eligibility and recertification requirements Share state
Ryan White Eligibility Determination and Recertification: Improving Efficiency Amanda Bowes and Steve Bailey NASTAD OBJECTIVES Review Ryan White eligibility and recertification requirements Share state
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014
 INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
DHRPC Key Informant Interviews for Evaluation and Assessment Committee Brooke Bender, MPH August 3, 2010 Didi Fahey, PhD May 10, 2010
 DHRPC Key Informant Interviews for Evaluation and Assessment Committee Brooke Bender, MPH August 3, 2010 Didi Fahey, PhD May 10, 2010 Key Informant interviews were established to inform the DHRPC of details
DHRPC Key Informant Interviews for Evaluation and Assessment Committee Brooke Bender, MPH August 3, 2010 Didi Fahey, PhD May 10, 2010 Key Informant interviews were established to inform the DHRPC of details
MEDICAL SPECIALISTS OF THE PALM BEACHES, INC. Chronic Care Management (CCM) Program Training Manual
 Program Training Manual") MEDICAL SPECIALISTS OF THE PALM BEACHES, INC. Chronic Care Management (CCM) Program Training Manual September 2017 Table of Contents CCM PROGRAM OVERVIEW... 4 3 STEPS TO BEGIN CCM:... 5 Identify the Patient...
MEDICAL SPECIALISTS OF THE PALM BEACHES, INC. Chronic Care Management (CCM) Program Training Manual September 2017 Table of Contents CCM PROGRAM OVERVIEW... 4 3 STEPS TO BEGIN CCM:... 5 Identify the Patient...
Discussion of Care Integration Best Practices & Challenges
 Discussion of Care Integration Best Practices & Challenges Alicia Downes, LMSW Snr Program Manager-AIDS United Peter Coronado, Jr-Valley AIDS Council Director of Linkage to Continuum of Care South Central
Discussion of Care Integration Best Practices & Challenges Alicia Downes, LMSW Snr Program Manager-AIDS United Peter Coronado, Jr-Valley AIDS Council Director of Linkage to Continuum of Care South Central
340B Drug Program Summary
 Summary Congress created section 340B of the Public Health Service Act in 1992 to allow eligible health care providers known as Covered Entities to stretch scarce Federal resources, reaching more patients
Summary Congress created section 340B of the Public Health Service Act in 1992 to allow eligible health care providers known as Covered Entities to stretch scarce Federal resources, reaching more patients
Improving Access To Care: Using Community Health Workers to Improve Linkage and Retention in HIV Care
 Improving Access To Care: Using Community Health Workers to Improve Linkage and Retention in HIV Care Pre-Application Technical Assistance Webinar Funding Opportunity Announcement HRSA-16-185 June 9, 2016
Improving Access To Care: Using Community Health Workers to Improve Linkage and Retention in HIV Care Pre-Application Technical Assistance Webinar Funding Opportunity Announcement HRSA-16-185 June 9, 2016
Establishing an HIV/AIDS Pharmacy Practice in an Underserved Inner City Environment Facilitators and Barriers
 Establishing an HIV/AIDS Pharmacy Practice in an Underserved Inner City Environment Facilitators and Barriers Madeline Feinberg, Pharm.D Chase Brexton Health Services Baltimore Inner Harbor Overview of
Establishing an HIV/AIDS Pharmacy Practice in an Underserved Inner City Environment Facilitators and Barriers Madeline Feinberg, Pharm.D Chase Brexton Health Services Baltimore Inner Harbor Overview of
AIDS INSTITUTE NEW YORK PRESBYTERIAN DSRIP AND PRACTICE TRANSFORMATION INITIATIVE
 AIDS INSTITUTE NEW YORK PRESBYTERIAN DSRIP AND PRACTICE TRANSFORMATION INITIATIVE 1 Road map What is DSRIP (Delivery System Reform Incentive Payments) Integrating the mission of DSRIP & End the Epidemic
AIDS INSTITUTE NEW YORK PRESBYTERIAN DSRIP AND PRACTICE TRANSFORMATION INITIATIVE 1 Road map What is DSRIP (Delivery System Reform Incentive Payments) Integrating the mission of DSRIP & End the Epidemic
Critical Time Intervention (CTI) (State-Funded)
 (State-Funded)") Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
Critical Time (CTI) (State-Funded) Service Definition and Required Components Critical Time (CTI) is an intensive 9 month case management model designed to assist adults age 18 years and older with mental
Data Submission and Web-Reporting. for the Maryland Hospital Hand Hygiene Collaborative
 Data Submission and Web-Reporting for the Maryland Hospital Hand Hygiene Collaborative Institutional Setup for the Database--Part I Database developed and supported by Johns Hopkins Medicine. A representative
Data Submission and Web-Reporting for the Maryland Hospital Hand Hygiene Collaborative Institutional Setup for the Database--Part I Database developed and supported by Johns Hopkins Medicine. A representative
POLICY & PROCEDURE DEFINITIONS: Referral Status
 POLICY & PROCEDURE TITLE: Referral Policy and Procedure Scope/Purpose: To provide specialized services to patients to obtain accurate diagnoses and for improved patient satisfaction Division/Department:
POLICY & PROCEDURE TITLE: Referral Policy and Procedure Scope/Purpose: To provide specialized services to patients to obtain accurate diagnoses and for improved patient satisfaction Division/Department:
Table 1: Limited Access Summary of Capabilities
 What is the Practice Fusion Limited Access EHR product? The Practice Fusion Limited Access EHR product will be provided to current Practice Fusion customers who have not purchased an EHR subscription plan
What is the Practice Fusion Limited Access EHR product? The Practice Fusion Limited Access EHR product will be provided to current Practice Fusion customers who have not purchased an EHR subscription plan
Checklists for screening for active tuberculosis in high-risk groups
 Checklists for screening for active tuberculosis in high-risk groups General screening program considerations The following are aspects of design and implementation that should be considered before planning
Checklists for screening for active tuberculosis in high-risk groups General screening program considerations The following are aspects of design and implementation that should be considered before planning
Introduction. Jail Transition: Challenges and Opportunities. National Institute
 Urban Institute National Institute Of Corrections The Transition from Jail to Community (TJC) Initiative August 2008 Introduction Roughly nine million individuals cycle through the nations jails each year,
Urban Institute National Institute Of Corrections The Transition from Jail to Community (TJC) Initiative August 2008 Introduction Roughly nine million individuals cycle through the nations jails each year,
Accessing HEALTHeLINK
 Accessing HEALTHeLINK HEALTHeLINK can be accessed through the at www.wnyhealthecommunity.com or www.wnylink.com or you will be redirected from your saved link. Enter your and to open
Accessing HEALTHeLINK HEALTHeLINK can be accessed through the at www.wnyhealthecommunity.com or www.wnylink.com or you will be redirected from your saved link. Enter your and to open
Rx Office Hours: IMPORTANT
 Rx Office Hours: IMPORTANT To ensure a high quality audio experience for all, please: Dial in using your phone (NOT your computer.) Enter your personal Attendee ID (located at the bottom of the box with
Rx Office Hours: IMPORTANT To ensure a high quality audio experience for all, please: Dial in using your phone (NOT your computer.) Enter your personal Attendee ID (located at the bottom of the box with
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE)
") MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.0 October 10, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility, functionality,
MEDICARE CCLF ANALYTICS: MEDICARE ANALYTICS DATA ENGINE (MADE) Frequently Asked Questions 1.0 October 10, 2017 hmetrix hmetrix This document contains frequently asked questions regarding the utility, functionality,
HIV/AIDS SURVEILLANCE HIV STATE FUNDS SEXUALLY TRANSMITTED DISEASES COMMUNICABLE DISEASE EXPANSION BUDGET
 APRIL 2014 HIV CLUSTER: 93.940 93.944 93.977 State Project/Program: HIV PREVENTION ACTIVITIES HEALTH DEPARTMENT BASED HIV/AIDS SURVEILLANCE PREVENTIVE HEALTH SERVICES STD CONTROL GRANTS HIV STATE FUNDS
APRIL 2014 HIV CLUSTER: 93.940 93.944 93.977 State Project/Program: HIV PREVENTION ACTIVITIES HEALTH DEPARTMENT BASED HIV/AIDS SURVEILLANCE PREVENTIVE HEALTH SERVICES STD CONTROL GRANTS HIV STATE FUNDS
Social Determinants of Health: Creating a Multi-Agency Coordinated Care Hub for Homeless Adults
 Social Determinants of Health: Creating a Multi-Agency Coordinated Care for Homeless Adults Boston Health Care for the Homeless Program Green River BHCHP Mission Since 1985, our mission has remained the
Social Determinants of Health: Creating a Multi-Agency Coordinated Care for Homeless Adults Boston Health Care for the Homeless Program Green River BHCHP Mission Since 1985, our mission has remained the
LGBT Health Readiness. Assessments in Health Centers: Key Findings
 LGBT Health Readiness This project was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under cooperative agreement number
LGBT Health Readiness This project was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under cooperative agreement number
Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11
 Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11 Janice Magno, MPA, Project Manager, NYC REACH Liraiza Diaz, Clinical Quality Specialist, NYC REACH IHI Summit 2014, Washington DC
Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11 Janice Magno, MPA, Project Manager, NYC REACH Liraiza Diaz, Clinical Quality Specialist, NYC REACH IHI Summit 2014, Washington DC
Comments on Illinois s Behavioral Health Transformation 1115 Demonstration Waiver
 Comments on Illinois s Behavioral Health Transformation 1115 Demonstration Waiver Contact: Daniel M.O. Frey, Director of Government Relations, (312) 334-0927 or dfrey@aidschicago.org Administrator Andy
Comments on Illinois s Behavioral Health Transformation 1115 Demonstration Waiver Contact: Daniel M.O. Frey, Director of Government Relations, (312) 334-0927 or dfrey@aidschicago.org Administrator Andy
Identify obstacles, and understand the aspects of the revenue cycle that you should be focusing on at your organization
 Case Study: Revenue Cycle Optimization Learning Objectives Identify obstacles, and understand the aspects of the revenue cycle that you should be focusing on at your organization Describe the steps that
Case Study: Revenue Cycle Optimization Learning Objectives Identify obstacles, and understand the aspects of the revenue cycle that you should be focusing on at your organization Describe the steps that
Using Community Health Workers to Improve Linkage and Retention in HIV Care: A National Project and Evaluation
 Using Community Health Workers to Improve Linkage and Retention in HIV Care: A National Project and Evaluation APHA 2017 Annual Meeting Allyson Baughman November 6, 2017 PRESENTER DISCLOSURES Allyson Baughman
Using Community Health Workers to Improve Linkage and Retention in HIV Care: A National Project and Evaluation APHA 2017 Annual Meeting Allyson Baughman November 6, 2017 PRESENTER DISCLOSURES Allyson Baughman
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Electronic Prescribing (erx): The Pros and Cons. Richard Kalish, MD, MPH Medical Director Boston HealthNet August 13, 2009
: The Pros and Cons. Richard Kalish, MD, MPH Medical Director Boston HealthNet August 13, 2009") Electronic Prescribing (erx): The Pros and Cons Richard Kalish, MD, MPH Medical Director Boston HealthNet August 13, 2009 Established in 1995 Boston HealthNet Partnership between Boston Medical Center,
Electronic Prescribing (erx): The Pros and Cons Richard Kalish, MD, MPH Medical Director Boston HealthNet August 13, 2009 Established in 1995 Boston HealthNet Partnership between Boston Medical Center,
Ryan White HIV/AIDS Program Part C HIV Early Intervention Services Program: New Geographic Service Areas
 Ryan White HIV/AIDS Program Part C HIV Early Intervention Services Program: New Geographic Service Areas Pre-Application Technical Assistance Conference Call HRSA-18-092 November 7, 2017 CAPT Mahyar Mofidi,
Ryan White HIV/AIDS Program Part C HIV Early Intervention Services Program: New Geographic Service Areas Pre-Application Technical Assistance Conference Call HRSA-18-092 November 7, 2017 CAPT Mahyar Mofidi,
Meaningful Use Hello Health v7 Guide for Eligible Professionals. Stage 2
 Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 2 Table of Contents Introduction 3 Meaningful Use 3 Terminology 4 Computerized Provider Order Entry (CPOE) for Medication, Laboratory
Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 2 Table of Contents Introduction 3 Meaningful Use 3 Terminology 4 Computerized Provider Order Entry (CPOE) for Medication, Laboratory
Ryan White All Grantee Meeting ENROLLMENT & ELIGIBILITY: HOW TO MANAGE THE PATIENT SLIDING FEE SCALE AND CAP ON CHARGES. Jana D.
 Ryan White All Grantee Meeting ENROLLMENT & ELIGIBILITY: HOW TO MANAGE THE PATIENT SLIDING FEE SCALE AND CAP ON CHARGES Jana D. Collins, MS The Bluegrass Care Clinic ICE BREAKER Presentation Outline Ryan
Ryan White All Grantee Meeting ENROLLMENT & ELIGIBILITY: HOW TO MANAGE THE PATIENT SLIDING FEE SCALE AND CAP ON CHARGES Jana D. Collins, MS The Bluegrass Care Clinic ICE BREAKER Presentation Outline Ryan
CORE COMPETENCIES INDEX
 CORE COMPETENCIES INDEX An Examination of Health Department Efforts to End the Epidemic CHAIR S CHALLENGE READY TO END THE AND VIRAL HEPATITIS EPIDEMICS C O N T E N T I. FOREWORD II. OVERVIEW OF THE ASSESSMENT
CORE COMPETENCIES INDEX An Examination of Health Department Efforts to End the Epidemic CHAIR S CHALLENGE READY TO END THE AND VIRAL HEPATITIS EPIDEMICS C O N T E N T I. FOREWORD II. OVERVIEW OF THE ASSESSMENT
St. Louis Regional HIV Health Services Planning Council
 St. Louis Regional HIV Health Services Planning Council Overview for Prevention and Care Subcommittee Presented by: Montara Renee November, MPA Program Coordinator, PC Support February 2, 2015 Overview
St. Louis Regional HIV Health Services Planning Council Overview for Prevention and Care Subcommittee Presented by: Montara Renee November, MPA Program Coordinator, PC Support February 2, 2015 Overview
Meaningful Use Hello Health v7 Guide for Eligible Professionals. Stage 1
 Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 1 Table of Contents Introduction 3 Meaningful Use 3 Terminology 5 Computerized Provider Order Entry (CPOE) for Medication Orders [Core]
Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 1 Table of Contents Introduction 3 Meaningful Use 3 Terminology 5 Computerized Provider Order Entry (CPOE) for Medication Orders [Core]
MODULE ELEVEN. Getting Credit for the Work You Do: Entering Units of Service
 MODULE ELEVE Getting Credit for the Work ou Do: Entering Units of Service 1 2 Policy In order to effectively evaluate and remain competitive for funding, all service providers and medical case managers
MODULE ELEVE Getting Credit for the Work ou Do: Entering Units of Service 1 2 Policy In order to effectively evaluate and remain competitive for funding, all service providers and medical case managers
Office of Clinical Research. CTMS Reference Guide Patient Entry & Visit Tracking
 Se Office of Clinical Research CTMS Reference Guide Patient Entry & Visit Tracking Table of Contents Logging into CTMS... 3 Search and Recruitment / Quick Search... 4 How to Configure Quick Search Fields...
Se Office of Clinical Research CTMS Reference Guide Patient Entry & Visit Tracking Table of Contents Logging into CTMS... 3 Search and Recruitment / Quick Search... 4 How to Configure Quick Search Fields...
EQuIPNational Survey Planning Tool NSQHSS and EQuIP Actions 4.
 Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Risk-Quality-Safety Management Reporting and the Healthcare SafetyZone Portal
 Risk-Quality-Safety Management Reporting and the Healthcare SafetyZone Portal Heather Annolino, RN, MBA, CPHRM Director, Risk-Quality-Safety Consulting Services Clarity Group, Inc. 04/22/15 1 04/22/15
Risk-Quality-Safety Management Reporting and the Healthcare SafetyZone Portal Heather Annolino, RN, MBA, CPHRM Director, Risk-Quality-Safety Consulting Services Clarity Group, Inc. 04/22/15 1 04/22/15
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 PURPOSE Section 1905 (a) (A) of the Social Security Act does not specify or imply that Medicaid eligibility is precluded for those individuals who are inmates of a public institution. Accordingly
PAGE 1 of 7 PURPOSE Section 1905 (a) (A) of the Social Security Act does not specify or imply that Medicaid eligibility is precluded for those individuals who are inmates of a public institution. Accordingly
Ryan White Services Division Infectious Disease Bureau. Client Services Provider Manual FY Ryan White HIV/AIDS Treatment Extension Act Part A
 Ryan White Services Division Infectious Disease Bureau Client Services Provider Manual FY 2017 Ryan White HIV/AIDS Treatment Extension Act Part A Ryan White HIV/AIDS Treatment Extension Act Part A Boston
Ryan White Services Division Infectious Disease Bureau Client Services Provider Manual FY 2017 Ryan White HIV/AIDS Treatment Extension Act Part A Ryan White HIV/AIDS Treatment Extension Act Part A Boston
Meaningful Use Stage 2
 Meaningful Use Stage 2 Presented by: Deb Anderson, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
Meaningful Use Stage 2 Presented by: Deb Anderson, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
N U R S E C O N S U L T AN T Schematic Code 14102
 N U R S E C O N S U L T AN T Schematic Code 14102 I. DESCRIPTION OF WORK Positions in this banded class provide consultative work to a variety of audiences, including public health, utilization review
N U R S E C O N S U L T AN T Schematic Code 14102 I. DESCRIPTION OF WORK Positions in this banded class provide consultative work to a variety of audiences, including public health, utilization review
What Is Required for a Clinical Quality Management Program? Help! August 29, 2017
 What Is Required for a Clinical Quality Management Program? Help! August 29, 2017 Tracy Matthews Deputy Director, Division of Policy and Data Marlene Matosky Chief Clinical and Quality Branch HIV/AIDS
What Is Required for a Clinical Quality Management Program? Help! August 29, 2017 Tracy Matthews Deputy Director, Division of Policy and Data Marlene Matosky Chief Clinical and Quality Branch HIV/AIDS
PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage
 PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage Please note that this document is intended to supplement the information available on the CMS website for Meaningful Use for
PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage Please note that this document is intended to supplement the information available on the CMS website for Meaningful Use for
TEXAS DEPARTMENT OF CRIMINAL JUSTICE
 TEXAS DEPARTMENT OF CRIMINAL JUSTICE TEXAS CORRECTIONAL OFFICE ON OFFENDERS WITH MEDICAL OR MENTAL IMPAIRMENTS (TCOOMMI) NUMBER: DATE: September 1, 2017 (rev. 7) PROGRAM GUIDELINES AND PROCESSES PAGE:
TEXAS DEPARTMENT OF CRIMINAL JUSTICE TEXAS CORRECTIONAL OFFICE ON OFFENDERS WITH MEDICAL OR MENTAL IMPAIRMENTS (TCOOMMI) NUMBER: DATE: September 1, 2017 (rev. 7) PROGRAM GUIDELINES AND PROCESSES PAGE:
Monitoring the Progress of North Carolina Graduates Entering Primary Care Careers November 2005
 Monitoring the Progress of North Carolina Graduates Entering Primary Care Careers November 2005 Submitted by the University of North Carolina Board of Governors in response to General Statute 143-613 as
Monitoring the Progress of North Carolina Graduates Entering Primary Care Careers November 2005 Submitted by the University of North Carolina Board of Governors in response to General Statute 143-613 as
CME Application Guide
 CME Application Guide Purpose of the CME Application Guide The purpose of this CME Application Guide is to facilitate the development and implementation of Continuing Medical Education (CME) activities
CME Application Guide Purpose of the CME Application Guide The purpose of this CME Application Guide is to facilitate the development and implementation of Continuing Medical Education (CME) activities
GRANTEE CONTRACT MANAGEMENT SYSTEM
 GRANTEE CONTRACT MANAGEMENT SYSTEM Background In 2013, HRSA s HIV/AIDS Bureau (HAB) presented plans to streamline data collection and reduce reporting burden. HAB detailed a plan to reduce reported data
GRANTEE CONTRACT MANAGEMENT SYSTEM Background In 2013, HRSA s HIV/AIDS Bureau (HAB) presented plans to streamline data collection and reduce reporting burden. HAB detailed a plan to reduce reported data
HIV-SPECIFIC QUALITY METRICS FOR MANAGED CARE
 Data Decisions Delivery Directing Comprehensive TA: From Systems to Sustainability ADVANCING HIV PREVENTION THROUGH HEALTH DEPARTMENTS HIV-SPECIFIC QUALITY METRICS FOR MANAGED CARE HIV PREVENTION EDUCATIONAL
Data Decisions Delivery Directing Comprehensive TA: From Systems to Sustainability ADVANCING HIV PREVENTION THROUGH HEALTH DEPARTMENTS HIV-SPECIFIC QUALITY METRICS FOR MANAGED CARE HIV PREVENTION EDUCATIONAL
Essential Characteristics of an Electronic Prescription Writer*
 Essential Characteristics of an Electronic Prescription Writer* Robert Keet, MD, FACP Healthcare practitioners have a professional mandate to prescribe the most appropriate and disease-specific medication
Essential Characteristics of an Electronic Prescription Writer* Robert Keet, MD, FACP Healthcare practitioners have a professional mandate to prescribe the most appropriate and disease-specific medication
2016 Embedded and Rapid Response Care Management
 2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction
 Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
HIV HEALTH & HUMAN SERVICES PLANNING COUNCIL OF NEW YORK Mental Health Service Directive - Tri-County Approved by the HIV Planning Council 3/31/16
 Goals: 1) Provide treatment and counseling services to individuals living with HIV and mental illness, with or without cooccurring substance use disorders, that aim to improve quality of life and mental
Goals: 1) Provide treatment and counseling services to individuals living with HIV and mental illness, with or without cooccurring substance use disorders, that aim to improve quality of life and mental
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Achieving Operational Excellence with an EHR a CIO s Perspective
 Achieving Operational Excellence with an EHR a CIO s Perspective Phyllis Schuck, SPHR CIO of Pinehurst Surgical HIT Session 6.02 Thursday, March 29, 2007 Pinehurst Surgical Organization Overview Founded
Achieving Operational Excellence with an EHR a CIO s Perspective Phyllis Schuck, SPHR CIO of Pinehurst Surgical HIT Session 6.02 Thursday, March 29, 2007 Pinehurst Surgical Organization Overview Founded
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition
 What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
Low-Income Health Program (LIHP) Evaluation Proposal
 Evaluation Proposal") Low-Income Health Program (LIHP) Evaluation Proposal UCLA Center for Health Policy Research & The California Medicaid Research Institute Background In November of 2010, California s Bridge to Reform 1115
Low-Income Health Program (LIHP) Evaluation Proposal UCLA Center for Health Policy Research & The California Medicaid Research Institute Background In November of 2010, California s Bridge to Reform 1115
CMS-3310-P & CMS-3311-FC,
 Andrew M. Slavitt Acting Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Ave., S.W., Room 445-G Washington, DC 20201 Re: CMS-3310-P & CMS-3311-FC, Medicare
Andrew M. Slavitt Acting Administrator Centers for Medicare & Medicaid Services Hubert H. Humphrey Building 200 Independence Ave., S.W., Room 445-G Washington, DC 20201 Re: CMS-3310-P & CMS-3311-FC, Medicare
The Transition from Jail to Community (TJC) Initiative
 Initiative") The Transition from Jail to Community (TJC) Initiative January 2014 Introduction Roughly nine million individuals cycle through the nation s jails each year, yet relatively little attention has been given
The Transition from Jail to Community (TJC) Initiative January 2014 Introduction Roughly nine million individuals cycle through the nation s jails each year, yet relatively little attention has been given
Critical Access Hospital Quality
 Critical Access Hospital Quality Current Performance and the Development of Relevant Measures Ira Moscovice, PhD Mayo Professor & Head Division of Health Policy & Management School of Public Health, University
Critical Access Hospital Quality Current Performance and the Development of Relevant Measures Ira Moscovice, PhD Mayo Professor & Head Division of Health Policy & Management School of Public Health, University
Michigan Department of Community Health Part D Program QM Plan January 2008 Page 1 of 6
 Page 1 of 6 The Michigan Department of Community Health Ryan White Treatment Modernization Act Part D Program Quality Management Plan January 2008 I. Quality Mission: The Michigan Department of Community
Page 1 of 6 The Michigan Department of Community Health Ryan White Treatment Modernization Act Part D Program Quality Management Plan January 2008 I. Quality Mission: The Michigan Department of Community