Governing Body Meeting - Agenda
|
|
|
- Randall Sullivan
- 6 years ago
- Views:
Transcription
1 MEETING HELD IN PUBLIC GP/GB/ Governing Body Meeting - Agenda, The Lantern Centre, Vicarage Lane, Fulwood PR2 8DY 2.00pm 4.00pm 1. Welcome and introductions Apologies for absence Mr P Richardson Information 2. Declarations of interest Mr P Richardson Information 3. Minutes of Governing Body meeting 25 April 2013 Agenda NHS Greater Preston CCG Governing Body Meeting Mr P Richardson Review GP/GB/ Matters Arising Mr P Richardson Information GP/GB/ Standing Items 5. Chair s Update Mr P Richardson Information Verbal 6. Chief Officer s Update Mrs J Ledward Information GP/GB/ Items for decision 7. Financial Performance Report May 2013 Mr I Crossley Approval GP/GB/ Performance Management Report June 2013 Mr I Crossley Approval GP/GB/ Assurance Framework 2013/14 Mr M Barker Approval GP/GB/ Memorandum of Understanding Provision of Commissioning Support by NHS Blackpool CCG Mr M Barker Approval GP/GB/ Developing Specialist Dementia Services Mrs J Ledward Approval GP/GB/ Use of the Seal Mr M Barker Approval GP/GB/ Never Events Update Mr A Stedman Approval GP/GB/
2 MEETING HELD IN PUBLIC 14. Questions from the Public Mr P Richardson Discussion Items for assurance 15. Quality Improvement Committee Minutes Mr D Noblett Information GP/GB/ Delivery and Finance Committee Minutes Mr I Crossley Information GP/GB/ Network of Lancashire CCGs Minutes Mrs J Ledward Information GP/GB/ Any Other Business 18. Any Other Business 19. Date, Time and Venue of next meeting 25 July 2013, 2.00pm, The Lantern Centre, Vicarage Road, Fulwood, Preston PR2 8DY Agenda NHS Greater Preston CCG Governing Body Meeting
3 GP/GB/ Governing Body Meeting - Minutes 25 April 2013, The Gujerat Hindu Centre, South Meadow Lane, Preston PR1 8JN at 2.00pm Present In attendance Mrs Anne Bowen Governing Body Nurse Dr Steve Cairns Secondary Care Doctor Mr Iain Crossley Chief Finance and Contracting Officer Dr Brigid Finlay Clinical Lead Mr Sam Jones Lay Member Audit and Finance Mrs Jan Ledward Chief Officer Mr David Noblett Lay Member Patient and Public Involvement Mr Paul Richardson Lay Member Governance and Vice Chair Mr Mike Barker Head of Constitution and Governance Mrs Louise Giles Head of GP and Stakeholder Engagement Dr Anthony Sudell Consultant in Public Health Medicine Mrs Anne Whittle Governing Body Secretary Members of the Public No members of the public were present GPGB/13/04/01 Welcome, Introductions and Apologies for Absence Mr Richardson welcomed everyone to the first official meeting in public of NHS Greater Preston Clinical Commissioning Group (CCG) since becoming a statutory organisation. Apologies for absence were received from Dr Ann Bowman Chair and Clinical Lead, Dr Manjit Jandu Clinical Lead, Dr Sandeep Prakash and Mr Alan Stedman, Head of Quality, Strategy and Outcomes. GPGB/13/04/02 GPGB/13/04/03 GPGB/13/04/04 Declarations of Interest There were no declarations of interest made within the meaning of Section 8 of the Group s Constitution. Minutes of the CCG Governing Body meeting held on 21 March 2013 The minutes of the previous meeting held on 21 March 2013 were agreed as an accurate record, subject to the following corrections: That the meeting started at 2.00pm and not 12.30pm, and that Item 13/13/10 Planning Framework (i) Delivery Plan first line should read Greater Preston and not Chorley and South Ribble. Matters Arising from the minutes of the previous meeting 13/01/06 Chief Officer Update it was noted that there has been Minutes NHS Greater Preston CCG Governing Body Meeting Page 1 of 5
4 national delay in progressing GP IT services. Mr Crossley reported that NHS England is progressing this work. 13/03/05 Chair s Update Mr Jones requested an update regarding the capacity of the Commissioning Support Unit (CSU). Mr Crossley advised that the CSU is now at 80-85% capacity. It was advised that the Network of Lancashire CCGs would be discussing this matter at its meeting on 25 April Mr Barker advised members that the CCG now has an understanding of the gaps and risks involved with the CSU and as a consequence would increase its capacity also. 13/03/06 - Chief Officer s Update In response to a request for an update on the outcome of the dementia consultation, Mrs Ledward referred members to a letter received from the CSU. This explained the process which had been followed in arriving at the outcome, which is to have one facility across Lancashire with significant investment to support the service through District Nursing and support teams. The site for the facility is subject to further discussion. Mr Noblett expressed concern that investment in the new site must not result in detracting funds from dementia support services. Mrs Giles reported that significant investment is already in place to allow programmes of work for the development of dementia services. A copy of the letter from the CSU regarding the outcome of the dementia services public consultation was circulated under Any Other Business to members for information. GPGB/13/04/05 GPGB/13/04/06 Chair s Update Mr Richardson referred the Governing Body to the Chief Officer s report in respect of the CCG s progress and key priorities. Chief Officer s Report Mrs Ledward presented a report on CCG progress since the last Governing Body meeting. The key issues identified to members were as follows: The CCG is 25 days old and business is running smoothly with no major issues resulting from the transition. There are several areas of conflict of interest which the CCG will be able to address now that further national guidance has been issued. The Audit Committee will consider these issues. Mrs Ledward advised members for information of the interest from the media on managing conflicts of interest. An invitation from the Chairs of NHS Greater Preston and NHS Chorley and South Ribble CCGs to board to board meetings has been warmly received from Lancashire Teaching Hospitals NHS Foundation Trust (LTH) and Lancashire Care NHS Foundation Trust (LCFT) and a date has been offered by LTH of 12 June Members were encouraged to attend these meetings. It was noted Minutes NHS Greater Preston CCG Governing Body Meeting Page 2 of 5
5 that Lancashire County Council (LCC) has yet to respond. In relation to seasonal pressures, Mrs Ledward advised members that this is a national issue which cannot be addressed locally, although the CCG will do what it can and any suggestions were welcome. This has been a particularly testing time for CCGs during establishment. Members discussed the whole system review which is to be conducted, and in response to a suggestion that there is enough expertise in the system to undertake this work, Mrs Ledward replied that previous organisations have carried individual utilisation management reviews which often resulted in the same issues/outcomes, and that a whole system review, carried out by former Department of Health colleagues on behalf of the National Commissioning Board (NCB) looking at the patient pathways and experience will help Lancashire CCGs to understand a whole range of issues and what can be done collectively to avoid the same situation next year. Mrs Giles highlighted the importance of nurses input and suggested that this will be more easily achieved for nurses through an external review. Guidance has been received in relation to the quality premium, which will be paid on the basis of achieving targets and outcomes at 5 per head of population. Mrs Ledward explained how this will effectively be an expansion of targets already in place for the CCG. Mrs Ledward recommended the guidance for members to read. Discussion included NHS England s direction to CCGs on primary care commissioning and the future role of GPs and contracted hours, particularly in respect of providing urgent care for the local population on a 24/7 basis. Resolved: That the Governing Body noted the update provided by the Chief Officer. GPGB/13/04/07 Delivery Plan Mrs Ledward presented an updated draft of the Delivery Plan for NHS Greater Preston CCG and reported that the organisation is ready to implement much of the plan. Mrs Ledward welcomed any final comments on the plan before circulating to stakeholders and publishing on the website. The plan will also act as a starting point for the prospectus which will be published in May. Comments and corrections were put forward, to which members agreed in order to reach a final position on the Delivery Plan. Resolved That the Governing Body approved the final version of the Delivery Plan , subject to the amendments agreed by members. GPGB/13/04/08 Financial Position April 2013 Mr Crossley presented for approval the financial update and risk Minutes NHS Greater Preston CCG Governing Body Meeting Page 3 of 5
6 assessment for NHS Greater Preston CCG as at April Mr Crossley highlighted key issues and areas of note regarding the update, to which members provided the following comments: That the CCG s budget is based on planned investments and savings, with ledger systems in place and that the first financial report since becoming a statutory organisation will be available to the Governing Body in May An issue in relation to national allocations which do not match organisational contracts has resulted in Lancashire CCGs not being in a position to sign contracts with providers. Lancashire CCGs are writing to the Local Area Team (LAT) to ask for their assistance in resolving this matter as this is the biggest risk to the organisation. Discussion included how members would wish to understand at what point the 4.8 million savings will become part of that risk. Mr Crossley explained various activities in respect of savings and that a whole system of review has started for CCGs to understand how these savings will be delivered. Resolved That the Governing Body noted the financial update and risk assessment for NHS Greater Preston CCG. GPGB/13/04/09 Performance Report April 2013 Mr Crossley presented a report on progress against the key targets in the Delivery Plan. The report set the scene for performance and quality monitoring of the targets as set out in the Delivery Plan for the coming year. Key issues were highlighted in the report and debated by members, including: A suggestion was received to look at building into the report the quality premium targets and to use a traffic light approach. Consider what has moved from the LAT/CSU, and what is required to provide assurance and improve health services for the local population. To differentiate between national and local priorities and explain what indicators are in place. Members would like to see a month by month progress update in terms of the quality aspect in order to identify any trends. It was noted that the organisation is data rich, and is in a good position to look at how best to use the intelligence received. A combination of indicators was suggested to reflect what the CCG is being measured against from a membership perspective and in terms of members of the public. Members felt strongly that, post Francis, the CCG needs to maintain a keen awareness of patient experience. Future reports could incorporate the Family and Friends test. It was suggested that perhaps GPs could take part in the Family and Minutes NHS Greater Preston CCG Governing Body Meeting Page 4 of 5
7 Friends test, as many patients see their GP after discharge from hospital. It was also suggested that GP services could be included in the Family and Friends test. Future reports should pick up key areas of concern and identify any trends in areas of risk, as well as performance against the risks already identified in the CCG s Risk Register. It was also suggested that seeing the Risk Register populated will inform Governing Body members of what they need to know. Mr Richardson explained that stakeholders views, including those around key risks and financial liability, could be built into performance reports to provide increased assurance to the Governing Body. Mr Barker suggested that the forthcoming Board to Board meetings with major providers might be able to action some aspects of this report and the comments received. Mr Richardson asked that the key issues be refined as per the comments received, to allow more focus and targeted discussion around key issues In future. Resolved That the Governing Body noted the contents of the report and provided comments upon the style and format as above. GPGB/13/04/10 GPGB/13/04/11 Questions from the Public No members of the public were present and no questions had been submitted in advance. Quality Improvement Committee Minutes Mr Noblett presented for information the minutes of the joint Quality Improvement Committee meeting held on 13 March 2013, and emphasised the need to ensure that information received from providers correlated with the CCG s own intelligence Resolved That the Governing Body noted the minutes of the joint Quality Improvement Committee meeting. GPGB/13/04/12 Any Other Business Mrs Ledward circulated for information a copy of a letter from Lancashire CSU which explained the outcome of the recent public consultation on dementia services in Lancashire. Date and time of next meeting: 27 June, 2.00pm Venue the Lantern Centre, Vicarage Lane, Fulwood PR2 8DY Signed as an accurate record. Minutes NHS Greater Preston CCG Governing Body Meeting Date... Page 5 of 5
8 GP/GB/ Matters Arising There are no matters arising from the minutes of previous Governing Body meetings. Matters Arising NHS Greater Preston CCG Governing Body Meeting
9 GP/GB/ Part 1 Part 2 Report Title Written by Presented by Purpose of the paper Governing Body Meeting Chief Officer s Report Jan Ledward, Chief Officer Jan Ledward, Chief Officer This paper provides an update on the CCG s progress from the Chief Officer since the last Governing Body meeting. Key issues Heatwave Plan Constitutional Changes Procedures for changes to constitutions Patient Health Budgets (PHB) NHS Property Services Ltd NHS Procurement, Patient Choice and Competitor (No. 2) Regulations 2013 consultation Responsibilities within Community Safety Partnerships Feedback from Board to Boards and Team to teams Lancashire CCG network Urgent and Emergency care review Commissioning Support Recommendations Actions required by Governing Body Members The Governing Body is asked to approve the Constitutional change outlined note the content of the report Chief Officer s Report NHS Greater Preston CCG Governing Body Meeting
10 Chief Officer s Report 1. Introduction 1.1 Since the CCG s last governing body meeting NHS England has announced the intention of Sir David Nicholson, Chief Executive, to retire in March Sir David has a career in the NHS of over 35 years, in many aspects of the service and has led the NHS through the transition. 1.2 NHS England also announced the designation of 15 new Academic Health Science Networks (AHSNs). They are an opportunity to pull together the adoption and spread of innovation with clinical research and trials, informatics, education and health care delivery. Our local AHSN is North West Coast and covers Lancashire, Cumbria and Merseyside. 2. Heatwave Plan 2.1 The Heatwave Plan for England 2013 is a Public Health plan to protect health and reduce harm from severe heat and heatwaves. The Plan has been published every year since 2004, following the devastating pan-european heatwave of It is intended to ensure that mechanisms are in place to identify vulnerable individuals and mitigate the effect of heat or a heatwave to reduce excess mortality and morbidity. 2.2 CCGs have a key role in this, in close liaison with NHS England area teams, to ensure that all providers of NHS funded care take appropriate action as required and that agreed systems are in place to ensure the cascade of alerts to providers. 2.3 The following documents are available on the Public Health England (PHE) website: the Heatwave Plan for England 2013 Making the Case, a companion document giving further information on a range of topics related to the Heatwave Plan three information pamphlets containing action cards based on the plan for easy use by organisations, staff and the public the joint letter from NHS England, Public Health England (PHE) and the Department of Health 2.4 Public Health England (PHE) has also recently published a new website that shows the variation in early death rates. The data is at Lancashire level and shows the number of premature deaths from each of England s four biggest killers cancer, heart disease and stroke, lung and liver disease. It allows easy access to comparative data of an area against that for similar populations, income and levels of health. The Lancashire data is attached at appendix A for information. Chief Officer s Report NHS Greater Preston CCG Governing Body Meeting Page 2 of 7
11 3. Constitutional Changes 3.1 Approval of Severance Payments and wording in constitutions on whistle blowing 3.2 In a letter from Sir David Nicholson, NHS England Chief Executive, to Clinical Leads on 2 May he set out the process for CCGs to follow in respect of severance payments and in particular gagging clauses and what if anything is contained in CCGs constitutions. He has requested that CCGs make explicit, in a governing body meeting, formal adoption and inclusion of the following statement in the CCGs constitution: The CCG recognises and confirms that nothing in or referred to in our constitution (including in relation to the issue of any press release or other public statement or disclosure) will prevent or inhibit the making of any protected disclosure (as defined in the Employment Rights Act 1998) by any member of the CCG, any member of the governing body, any member of any of our committees or sub committees or any employee or any of our members, nor will it affect the rights of any workers (as defined under the Act) under that Act. 3.3 The CCG values openness and transparency in all it does, it is vital that members of the Governing Body, staff and our membership feel they are protected and can raise concerns in an environment that is safe and supportive. 3.4 We also have a duty to assure ourselves that our providers of NHS services have appropriate arrangements in place to support staff to raise concerns and arrangements covering severance payments and compromise agreements. Letters have been sent to all our providers requesting information in respect of these arrangements and processes. 4. Procedures for changes to constitutions 4.1 NHS England has recently published guidance that sets out the procedures to be followed by CCGs and NHS England when a CCG wishes to apply to make changes to its constitution, to dissolve or if two or more CCGs want to merge. 4.2 Submissions are required to be made to the relevant regional director of operations and delivery by 1 June or 1 November each year for changes to constitutions June 1 for mergers to come into effect the following April; and Applications for CCG dissolutions will be considered at any time of the year. 4.3 An additional paragraph has been added to our constitution as requested by NHS England as above:- This change has been incorporated with immediate effect. Chief Officer s Report NHS Greater Preston CCG Governing Body Meeting Page 3 of 7
12 5. Patient Health Budgets (PHB) 5.1 A key objective for commissioners of healthcare is to become dramatically better at involving patients; empowering them to manage and make decisions about their own care and treatment. Patients are increasingly involved in their own personal care planning, becoming central to the decisions made about their care. Patient Health Budgets (PHB) will give them the opportunity to manage funds and say how they are used. 5.2 Following a successful pilot programme, from April 2014 people eligible for NHS continuing healthcare (including parents of children) across England will have the right to ask for a PHB. Others with long term health, physical or mental health conditions or disabilities may also benefit. The latest national personal budgets found that early adopter sites are getting very good results. 5.3 A programme of support is available to the CCG that builds on best practice and other information developed during the pilot programme and learning from early adopter sites. 5.4 The programme is asking all CCGs (and other NHS organisations responsible for delivery of PHBs) to take part in the programme. It includes: support to carry out a local self-assessment using markers of progress; the chance to take part in an accelerated development programme; taking part in the next national personal budgets survey; access to the personal health budgets toolkit and FAQ; access to a learning network. 5.5 The CCG is required to register for the support programme by 30 June 2013 so the delivery team can support the CCG over the coming months. 6. NHS Property Services Ltd 6.1 From April 2013 property portfolios previously managed by primary care trusts (PCTs), transferred to NHS Property Services Ltd (NHS PS) and Community Health Partnerships Ltd (CHP). The arrangements for funding the cost of these properties were agreed between NHS England, Department of Health (DH), NHS PS and CHP. 6.2 Information about these changes was initially set out in a letter dated 18 April 2013 from the Department of Health to Accountable Officers of CCGs and others and covered such topics as changes to occupiers of buildings; under-recovered costs and the future direction of travel. 6.3 More recently, CCGs and NHS England commissioners in Area Teams were sent schedules informing them of the amounts they will need to pay to NHS PS and CHP for property costs that are not recovered from occupiers. To help understand the Chief Officer s Report NHS Greater Preston CCG Governing Body Meeting Page 4 of 7
13 basis of the charges contained in the schedules a letter was issued by the Department of Health on 15 May 2013 to accompany the schedules. 6.4 The CCG is working through the implications and consequences of the new information and will advise the governing body in due course. 7. NHS Procurement, Patient Choice and Competitor (No. 2) Regulations 2013 consultation 7.1 As part of its new role as sector regulator for health, Monitor has launched a consultation on the guidance it intends to publish: on how to comply with the NHS (Procurement, Patient Choice and Competition) Regulations 2013 and with the requirements for patient choice in the NHS England and CCGs. The guidance is available on the Monitor website at about the general approach that it proposes to take in using its enforcement powers under these regulations. This can also be found on the same website; a series of case studies which consider how the regulations might apply to a number of hypothetical situations. 7.2 Commissioners are being asked to comment on the guidance by 15 July Responsibilities within Community Safety Partnerships 8.1 Commissioners recognise the link between health inequalities and offending behaviour that by improving outcomes reoffending can be reduced. Along with Police, local authorities, fire and probation services, PCTs previously had a statutory duty to play into community safety, law and order as part of a Community Safety Partnership. This responsibility has passed to CCGs. We are in the process of understanding the local scenario in respect of all partnerships to understand our roles and responsibilities and who the most appropriate person is to represent the CCG. 9. Primary Care Trust and Strategic Health Authority Transfer Schemes 9.1 The Staff and Property Transfer Schemes are a legal instrument made by the Secretary of State in exercise of the powers conferred by sections 300(1) and (2) to (3), (4) and (6) of, and Schedule 22 to, the Health and Social Care Act The schemes transferred the property, rights and liabilities of PCTs and SHAs (other than rights or liabilities under or in connection with contracts of employment) to transferees ( Receivers ) as permitted by section 300(2) of, and Schedule 22 to, the Health and Social Care Act Each Property Transfer Scheme was signed by a member of the Senior Civil Service by authority of the Secretary of State for Health and came into effect on 1 April 2013 and was formally received by the CCG on 6 June The Audit Committee will oversee the formal process of receiver Assurance and Due Diligence to satisfy the Governing Body that they: Chief Officer s Report NHS Greater Preston CCG Governing Body Meeting Page 5 of 7
14 have received the appropriate assets to deliver the functions for which they have statutory responsibility; and have not received assets or liabilities associated with functions outside their statutory responsibility. 10. Feedback from first set of Board to Board and team to team meetings 10.1 Lancashire Teaching Hospitals NHS Foundation Trust - The Governing Bodies from Chorley and South Ribble & Greater Preston CCGs met with the board of Lancashire Teaching Hospital NHS Foundation Trust on 12 June, The purpose of the meeting was to develop relationships and agree a collaborative approach to the development and improvement of health care services for the population. The meeting was very positive and both organisations agreed that meetings would be arranged quarterly throughout the year and that a set of principles for the development of a strategy for health care provision for the future be developed Adult Social Care Team - Senior managers from the Adult Social Care Team from Lancashire County Council (LCC) met with senior manages of the CCG to discuss how our respective teams would work together and progress with delivering the Long Term Conditions work programme. This was a very productive meeting with LCC agreeing to develop a scoping document identifying opportunities for further joint work areas and integration Board to Boards with Lancashire County Council and Lancashire Care NHS Foundation trust are being arranged, as are team to team meetings with senior managers. 11. Lancashire CCG Network 11.1 Progress continues to be made agreeing the governance arrangements for the collaborative work programme to support the CCG network. An away day is taking place in June to discuss the development of a clinical strategy for Lancashire and working relationships with NHS England Area Team Lancashire. An update on this will be provided to a future meeting. 12. Urgent and Emergency Care Review 12.1 Views are being sought by NHS England on a review of urgent and emergency care. In January the national Medical Director, Professor Sir Bruce Keogh, announced a review into the way the NHS responds to and receives emergency patients. The review was a priority for NHS England in its planning guidance Everyone Counts The aim of the review is to develop a national framework to help CCGs ensure highquality, consistent standards of care across the country. A steering group has been established which has developed an evidence base for change and emerging principles. The evidence base identified:- Chief Officer s Report NHS Greater Preston CCG Governing Body Meeting Page 6 of 7
15 more and more people are using the urgent and emergency care system; overall fragmentation of the system means many patients may not be able to access the most appropriate urgent or emergency care service to meet their needs; there is significant variation in patient experience across urgent and emergency care; demographic change in the population means that more and more patients need support managing long term conditions; emergency admissions are rising and there is a variation in outcomes for these patients Using the evidence, four emerging principles have been drafted which outline the case for change for a system that: provides consistently high quality and safe care, across all seven days of the week; is simple and guides good choices by patients and clinicians; provides the right care in the right place, by those with the right skills, the first time; is efficient in the delivery of care and services There are no agreed solutions at this stage, but the emerging principles have been presented to stimulate a debate and help shape a future urgent and emergency care system. Comments are being sought in order to develop a national framework for commissioning urgent and emergency care. The engagement period will take place between 17 June and 11 August A questionnaire has been developed to obtain views. The CCG will consider the documents in more detail and will submit a questionnaire based on our collective views. The joint management executive will oversee this process Locally we are conducting a collaborative review of the urgent care system and how it has performed over the last winter period. This is due to be concluded and a report produced by September Details of the outcome of this review will be brought to the governing body in due course. 13. Commissioning Support Service 13.1 Senior managers from the CCG and the CSU met to consider the results of the first full month of the business processes and to review the continued development of the back office support functions going forward. The meeting considered the successes to date and identified a number of improvements which can be implemented over the next business cycle; particularly around business intelligence and the provision of financial information to support the Governing Bodies. 14. Recommendations 14.1 The Governing Body is asked to: approve the constitutional change outlined; note the content of the report. Chief Officer s Report NHS Greater Preston CCG Governing Body Meeting Page 7 of 7
16 Report on the Longer Lives Programme launched by Public Health England on 11 th June 2013 Contact for further information: Dr. Sakthi Karunanithi, Public Health, Adult and Community Services, Executive Summary 1. Longer Lives is a programme launched by Public Health England to publish the data on premature mortality (under 75). It highlights premature mortality across every local authority in England, giving people important information to help them improve their community s health. This is the first time Lancashire County Council (LCC) has been benchmarked against a peer group of authorities with similar deprivation levels. Data can be accessed via longerlives.phe.org.uk. 2. Data analysis of premature deaths between shows that Lancashire is: a. 103rd out of 150 LAs for overall premature deaths (where 1st is best and 150th is worst) b. 95th for premature deaths from Cancer c. 100th for premature deaths from heart disease and stroke d. 106th for premature deaths from lung disease e. 104th for premature deaths from liver disease 3. LCC's own analysis shows that premature mortality rates have declined significantly since the last two decades. However, there are considerable inequalities within Lancashire in relation to premature mortality. There is approximately a twofold difference in age standardized premature death rates between Preston (highest) and South Ribble (lowest). The gaps in circulatory and respiratory premature deaths show narrowing whereas in liver disease it is widening. 4. Most of the premature deaths can be prevented by addressing the key risk factors including smoking, poor diet, physical inactivity, alcohol misuse, high blood pressure, high blood pressure and diabetes. As well as behavioural and physiological risk factors, there are a number of other conditions associated with premature deaths. These include low income, fuel poverty, social isolation and lack of control and job security in the workplace. 5. LCC's new key responsibilities to reduce premature mortality since April 2013 include commissioning of NHS Health Checks, Smoking Cessation Services, Substance misuse services (including alcohol), and promoting healthy living e.g. healthy diet and promoting physical activity, as well as working with the NHS, District Councils and the third sector in addressing the determinants of premature mortality. Other contributions that the council can make in addressing the root causes of early deaths include developing the economy, increasing educational attainment, providing social support to vulnerable groups, promoting active travel and 20 mph speed limits, tackling illicit tobacco and alcohol and improving
17 access to the natural environment. The move of public health into LCC has provided us with opportunities to reinvigorate these actions across the whole system. 6. We will continue to learn from the best performing areas and implement relevant actions in Lancashire. Background and Advice On 3 rd June, PHE released Longer Lives, its first major product, embargoed until the 11 th June. This aims to support Living Well for Longer the Secretary of State s call for action on premature mortality. Longer Lives presents mortality data which have previously been available in the public domain for example through the National Clinical and Health Outcomes Database (though not for LCC, only its constituent districts, including trend data) and the PH Outcomes dataset (where it is labelled provisional). Premature mortality is considered to be deaths under the age of 75. Living Longer considers deaths from the four main causes that contribute most to deaths under 75. These big killers include cardiovascular disease (heart disease and stroke), cancer, respiratory disease and liver disease. These account for almost ¾ of the total number of premature deaths. For each of these diseases, a standardised <75 death rate was calculated, as well as a standardised rate for the four diseases combined. (Standardisation was for age and adjusts for possible differences in age structure in each authority.) These were calculated for each of the 152 (with very occasional exclusions) upper tier local authorities. Deprivation scores (IMLD, 2010) were used to aggregate the authorities into 10 groups with 15 authorities in each. Group 1 was the least deprived and Group 10 the most. LCC was placed in Group 6 (described as Average ) on the basis of deprivation score. (see Appendix A for the authorities making up this group.) There were a total of 12,302 premature deaths in Lancashire in the period Lancashire was ranked 103 rd of 150 authorities for overall premature mortality with the best, Wokingham and the worst Manchester. It is also featured on the opening page of the site as one having the worst mortality rate authority in one of the less deprived groups Lancashire s ranking for the each of the main causes of premature mortality is shown below (Table 1) (The Unitary Authorities rankings for overall premature mortality were Blackburn with Darwen, 143/159 Las and Blackpool 149/150) Lancashire is close to the bottom 3 rd for all premature mortality and also for each o the constituent disease areas.
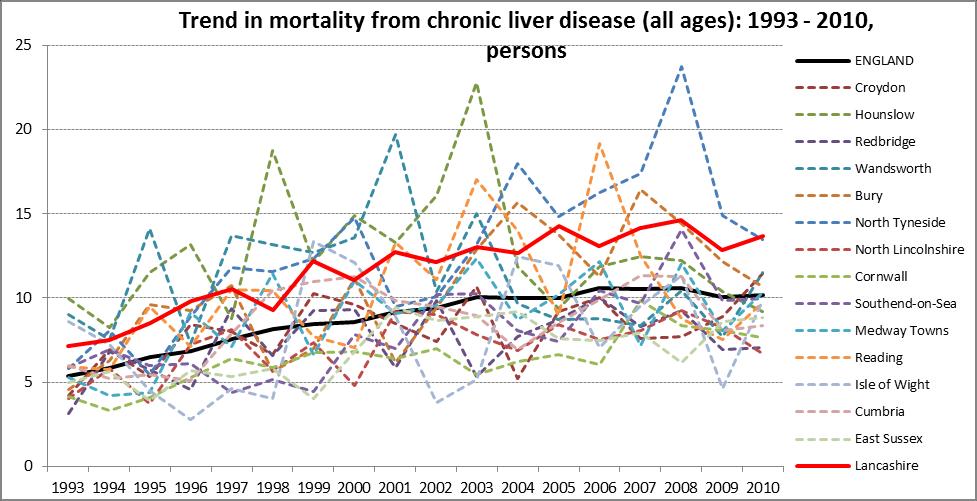
18 Table 1. Comparison between Premature Mortality in Lancashire vs All other Upper Tier LAs Rate/100,000 Rank out of all authorities considered (1 is best) Overall premature mortality /150 Cancer /150 Cardiovascular disease /150 Respiratory disease /149 Liver disease /149 Table 2 shows How Lancashire is ranked in its matched group. Table 2. Comparison between Premature Mortality in Lancashire vs Group 6 Upper Tier LAs Rate/100,000 Rank out of all authorities considered (1 is best, 15 worst) Overall premature mortality /15 Cancer /15 Cardiovascular disease 72 14/15 Respiratory disease 29 13/15 Liver disease 18 14/15 Compared to the 14 other local authorities in its deprivation group (6) Lancashire performs poorly. For overall premature mortality it is ranked 15 th (of 15), with the best in the group being Redbridge. For each of the other disease areas, Lancashire is 2nd (Cardiovascular and Liver disease), 3rd (Respiratory disease) or 4 th (Cancer) worst. Our further analysis shows that for the last 17 years when data are available the overall falling trend in premature mortality in Lancashire is similar to the rest of the peer group and to England as a whole. Lancashire however experienced higher premature mortality rates historically and the gap compared to National figures reduced in the case of circulatory and respiratory diseases premature mortality only. See graphs in Appendix B. In case of premature death caused by liver diseases are on the rise both nationally, in the peer group and in Lancashire. The bad news is that the increase, from an already higher base, was more intense in Lancashire compared to National and peer trends.
19 There are considerable inequalities within Lancashire in relation to premature mortality. Overall there is an approximately twofold difference in age standardized premature death rates between Preston (highest) and South Ribble (lowest). The gap in circulatory and respiratory premature death show narrowing whereas in liver diseases it is widening. See graphs in Appendix C. Discussion While these data have been available for a while, this is the first time Lancashire level mortality data have been compared either against all authorities or against some form of peer group of authorities. As Public Health has only recently moved to the LCC, the poor performance is likely to generate interest and discussion, both within the council and in the media. The position of Lancashire compared with a matched deprivation group is particularly poor. This is notable as the report notes the strong relationship between deprivation and premature mortality deprivation accounts for almost 80% of the national variation. However, Lancashire may differ from this peer group in other ways for instance it has at least twice the population as the other authorities and is at least 4-5 times bigger than most. It does show great variation both in deprivation and mortality, which may or may not be reflected in peers. For example the premature mortality rates for Lancashire in 2010 ranged from per 100,000 (Preston) to 58 per 100,00 (South Ribble). LCC is very familiar with using appropriate peer groups for comparative purposes and it should be possible to explore other groups, perhaps more appropriate groups for mortality comparisons. Not all premature mortality can be avoided. Nationally ONS suggest that about 60% of overall premature mortality could be avoided. This proportion includes those deaths that could be avoided through the application of good quality medical care (Amenable Mortality) or through the public health actions in the broadest sense (Preventable Mortality). Some deaths would fall into both categories). The risk factors associated with the premature mortality related to the diseases considered in the report are well known and include smoking, Alcohol, poor diet/low levels of physical activity, obesity. Improving the detection/treatment of conditions such as hypertension finding the missing thousands in GP registers - and improved management of people with existing disease can also contribute to reducing the amenable mortality. (Many of these actions were identified for the previous "spearhead" PCTs by the National Support Team for Health Inequalities). Though delivering services will have an effect, the key actions are likely to be those that focus on the wider determinants of health and reduce the need for interventions by creating environments which support healthy living and wellbeing. (i.e. focus on "healthy place".) Public Health's move to LCC provides the new opportunities to influence the promotion of healthy policies, integrated lifestyle services and working with NHS colleagues to improve detection and treatment of pre-existing conditions. The Health and Wellbeing Board could provide an overall focus for an integrated approach to mortality prevention that includes primary and secondary health care, local authority and other third sector partners. It is worth pointing out that considerable progress has already been made on this agenda. For example premature mortality rates for cardiovascular disease show substantial decreases across all
20 Lancashire districts. For example, Burney has fallen from per 100,000 in 2000 to 99.5 in 2010; Ribble Valley from to 69.2 over the same period. Some summary points Looking at the last 17 years for which we have data, historically Lancashire had higher premature mortality rates. These rates have fallen but the gap with the rest of the country has only narrowed for circulatory and respiratory disease There are considerable inequalities within Lancashire in relation to premature mortality. Overall there is an approximately twofold difference in age standardized premature death rates between Preston (highest) and South Ribble (lowest). For Liver disease, the gap between Lancashire districts is widening, while the gaps for circulatory and respiratory premature death are narrowing. Premature deaths from Liver disease are increasing as they are the rest of the country and in our peer group. It is important to note that deaths are rising from an already high level more rapidly than nationally or in our peers. To improve our respective position and improve the health experience of our residents, there is a need for coordinated action at scale across Lancashire to improve faster. Key Actions being pursued by the PH department 1. There is a need to apply a system-wide approach to activity for improvement including actions on the wider determinants of health, primary and secondary health care and specific public health interventions to tackle risk factors, in partnership with the NHS, Districts, third sector and other directorates within LCC. 2. With advice from LCC colleagues, we should explore options for other, perhaps more appropriate, peer groups of authorities for comparative purposes. More importantly, we should be learning from some of the best performing areas to identify opportunities for improvement. 3. Consider setting up a premature mortality dashboard for districts across Lancashire County Council area to monitor, and facilitate, improvement. Also, provide updates on the JSNA. 4. Explore opportunities to further improve the quality of public health services in Lancashire. 5. Work with the matrix area leads as the most appropriate senior PH experts to plan and lead delivery for improvement in each premature mortality area 6. Explore further collaboration with the Unitary authorities via the Directors of Public Health group, possibly with input from the Public Health Collaborative
21 Appendix A. Upper Tier authorities in Group 6 Alphabetical listing Bury Cornwall Croydon Cumbria CC East Sussex CC Hounslow Isle of Wight Lancashire CC Medway North Lincolnshire North Tyneside Reading Redbridge Southend-on-Sea Wandsworth Appendix B Time trends of premature mortality within the proposed peer group.
22
23
24 Appendix C Time trends in premature mortality in districts within Lancashire County Council area
25
26
27 GP/GB/ Part 1 Part 2 Report Title Written by Presented by Purpose of the paper Governing Body meeting Financial Performance Report Matt Gaunt, Head of Finance Iain Crossley, Chief Finance & Contracting Officer The Financial Performance Report sets out the financial position for the CCG as at May 2013 and provides an update to the Governing Body on progress against the proposed CCG Assurance Framework financial measures. Key issues The Governing Body is statutorily responsible for ensuring the CCG expenditure does not exceed the budget allocated from NHS England for 2013/14 and for ensuring expenditure on administrative running costs is below the specified allowance. A risk concerning the impact of resource allocation issues relating to specialist services remains unresolved and as a consequence the CCG has an 8.6m shortfall in allocations to meet the expected CCG financial commitments and deliver a balanced plan. The CCG is on target to deliver underlying recurrent surplus provided the funding shortfall is resolved for the CCG either through a correction in allocation or an implementation of additional cost savings. Actions required by Governing Body Members The Governing Body is asked to note the content of the Financial Performance Report Financial Performance Report NHS Greater Preston CCG Governing Body Meeting
28 Financial Performance Report: Greater Preston CCG May This paper reports on the 2013/14 financial position for NHS Greater Preston CCG as at the end of May CCG Assurance Framework - Financial Measures NHS England has set out interim arrangements for CCG assurance. The definitive assurance framework will be published later this year and some measures, for Financial Management, have yet to be determined. Where this is the case, the report reflects expected performance measures. 2.1 Financial Performance Indicator Year to date Full year forecast Underlying recurrent surplus 2.0% RAG Rating Surplus position 555k surplus 3,167k surplus Management of 2% NR funds within Nil 4,848k agreed processes QIPP savings delivery 756k 4,780k Activity trends main provider growth 100% of 100% of plan plan Running costs 592k 5,015k Clear identification of risks against financial delivery and mitigations 2.2 Financial Management Indicator Internal and External audit opinions This month RAG Rating Balance sheet: Better Payment Practice Code 98.8% Financial Performance Report Greater Preston Governing Body Meeting Page 1 of 8
29 2.3 Commentary: A risk position was flagged at the last Governing Body meeting which highlighted the impact of resource allocation issues relating to specialist services. A resolution proposed by the Cheshire, Warrington and Wirral Area Team has failed to meet the shortfall and as a consequence the CCG has flagged to the Lancashire Area Team an 8.6m shortfall in allocations to meet the expected CCG financial commitments and deliver a balanced plan. To achieve a balanced full year position the CCG has assumed that either there will be an allocation adjustment resolving the issue or additional savings will be generated to meet the shortfall. As this remains unresolved both QIPP delivery and the underlying recurrent surplus is rated Amber/Green. 3. k Revenue Resource Limit Budget to date Actual to date Variance to date Fav/(Adv) Annual Forecast Annual Forecast Variance 41,067 41, , Commentary: The revenue resource limit includes anticipated reduction in resource due to the proposed specialist services commissioning adjustment of 2,555k. 4. k Commissioning Expenditure Budget to date Actual to date Variance to date Fav/(Adv) Annual Forecast Annual Forecast Variance 39,564 39, , Commentary: Commissioning expenditure in the period is in line with budget; with a slight underspend on free nursing care. Provider activity information is available for April only and indicates that activity for LTH FT is in line with expected levels; therefore costs are expected to be in line with contract. Financial Performance Report NHS Greater Preston CCG Governing Body Meeting Page 2 of 8
30 Commissioning expenditure is set out in detail in appendix k Running Costs Budget to date Actual to date Variance to date Annual Forecast Annual Forecast Variance , Commentary: Running costs are underspent in the period to date as a result of vacancies within the structure. Running costs are set out in detail in appendix Financial Risk and Uncertainties The financial risks identified are: Allocation errors Acute activity over-performance Acute tariff deflation not delivered QIPP cost saving delivery There is limited activity information available for any update on the risks associated with Acute activity and tariff or associated QIPP. Allocation errors have not been resolved and remain the principle financial issue for the CCG. There are two approaches to mitigate risk: 1. The Lancashire and Cheshire, Warrington and Wirral Area Teams have agreed a piece work to investigate the extent of the allocation issue across Lancashire for 2 trusts; Lancashire Teaching Hospitals and Blackpool Teaching Hospitals. KPMG have been asked to carry out the work and this will be concluded in June. The scope of the work will be to identify any contracts or allocations where there is a material disagreement and recommend resolution. There is a commitment to correct material allocation issues from NHS England. 2. Resolution is uncertain therefore to achieve a balanced plan the CCG has developed an additional savings plan to meet the 4.8m shortfall. An options paper will be presented to the Governing Body which sets out how the additional savings could be met. Financial Performance Report NHS Greater Preston CCG Governing Body Meeting Page 3 of 8
31 There are other areas of uncertainty which may have a financial impact: Contract status The CCG has not yet signed contracts with its providers. The providers continue to be paid on expected contract values pending conclusion of the specialised commissioning allocations review. NHS Property Services the CCG will be recharged occupancy costs for the premises it operates from and any under-recovery of costs for the properties that NHS Property services operate on its behalf. Funding for these costs was include within the CCG allocation however indicative costs received from NHS Property Services in May suggest the CCG is underfunded by 0.1m. A Lancashire wide review of Property services charging is underway across Lancashire. The Integrated Single Financial Environment (ISFE) the new finance system has not so far provided the expected visibility of financial performance. The CCG Finance teams across Lancashire and the Lancashire CSU are working together to resolve reporting limitations. 7. Balance Sheet The Transfer Scheme from the DH Legacy Team was received in June and will be taken to the Audit Committee in July. The legacy transition arrangements in discharging the remaining liabilities of the PCT have not been confirmed. Funding arrangements for successor organisations have been proposed to meet short term liabilities should they be required. Matt Gaunt Head of Finance June 2013 Financial Performance Report NHS Greater Preston CCG Governing Body Meeting Page 4 of 8
32 Greater Preston CCG APPENDIX 1.1 Summary Budget to Date 000 Expenditure to Date 000 Variance to Date 000 Annual Budget 000 Annual Forecast 000 Annual Forecast Variance 000 Summary Income & Expenditure Revenue Resource Limit Confirmed 41,205 41, , ,416 0 Anticipated (138) (138) 0 (826) (826) 0 Total Revenue Resource Limit 41,067 41, , ,590 0 Expenditure Commissioning 39,564 39, , ,320 0 Corporate (0) 2,240 2,240 0 Reserves ,848 4,848 0 Healthcare Sub Total 39,932 39, , ,408 0 Running Costs ,015 5,015 0 Total Expenditure 40,540 40, , ,423 0 Surplus/(Defiicit) ,167 3,167 0 Financial Performance Report NHS Greater Preston CCG Governing Body Meeting Page 5 of 8
33 Greater Preston CCG APPENDIX 1.2 Healthcare Commissioning Report Budget to Date 000 Expenditure to Date 000 Variance to Date 000 Annual Budget 000 Annual Forecast 000 Annual Forecast Variance 000 Acute services NHS contracts -(includes Ambulance services) 20,543 20, , ,256 0 Other provider contracts (non-nhs, incl. VS) 1,404 1, ,423 8,423 0 NHS Contract Exclusions / cost per case ,556 1,556 0 NCAs Other (6,599) (6,599) 0 Sub-total Acute services 22,780 22, , ,271 0 Mental Health Services NHS contracts Other provider contracts (non-nhs, incl. VS) 3,650 3, ,903 21,903 0 NHS Contract Exclusions / cost per case NCAs 1,339 1,339 (0) 8,033 8,033 0 Other Sub-total MH services 5,152 5,152 (0) 30,910 30,910 0 Community Health Services NHS contracts 3,062 3, ,374 18,374 0 Other provider contracts (non-nhs, incl. VS) ,229 2,229 0 NHS Contract Exclusions / cost per case NCAs Other Sub-total Community services 3,438 3, ,629 20,629 0 Total Healthcare Contracts 31,370 31,370 (0) 178, ,810 0 Continuing Care services Continuing Care Services 1,418 1, ,507 8,507 0 Free Nursing Care ,301 1,301 0 Sub-total Continuing Care services 1,635 1, ,808 9,808 0 Primary Care services Prescribing 5,398 5, ,387 32,387 0 Enhanced services Out of Hours ,968 1,968 0 Commissioning Other Sub-total Primary Care services 6,014 6, ,082 36,082 0 Other Programme services Patient Transport Services ,266 1,266 0 Other non acute - NHS Other non acute - other non NHS providers ,890 4,890 0 Sub-total Other Programme services ,620 6,620 0 Total - Commissioning services 39,564 39, , ,320 0 Financial Performance Report NHS Greater Preston CCG Governing Body Meeting Page 6 of 8
34 Greater Preston CCG APPENDIX 1.3 Non HC Commissioning Budget to Date 000 Expenditure to Date 000 Variance to Date 000 Annual Budget 000 Annual Forecast 000 Annual Forecast Variance 000 Other Corporate Costs (Non-Running Costs) CSU Re-charge (0) 1,893 1,893 0 NHS Property Services re-charge Other 7 7 (0) Sub Total - Corporate costs (0) 2,240 2,240 0 Plan requirements & reserves 2% Headroom (Subject to BC Approval) ,848 4,848 0 Reserves Sub-total - Reserves ,848 4,848 0 Commissioning Corporate Reserves ,399 1,399 0 CSU Re-charge ,739 1,739 0 Running Costs Other Running Costs Reserve ,246 1,246 0 Sub Total - Running costs ,015 5,015 0 Total ,103 12,103 0 Financial Performance Report NHS Greater Preston CCG Governing Body Meeting Page 7 of 8
35 Greater Preston CCG APPENDIX 2 Healthcare Contract Report Budget to Date 000 Actual to Date 000 Variance to Date 000 Annual Budget 000 Annual Forecast 000 Annual Forecast Variance 000 Acute Services Main Provider: Lancashire Teaching Hospitals NHSFT 17,669 17, , ,016 0 Other Lancashire Providers: Blackpool Teaching Hospitals NHSFT ,375 4,375 0 East Lancashire Hospitals NHST ,298 1,298 0 University Hospitals of Morecambe Bay NHSFT Commissioning ,663 5,663 0 Sub Total - Lancashire Providers 19,653 19, , ,919 0 Greater Manchester Providers: Wrightington Wigan & Leigh NHSFT ,065 1,065 0 University Hospitals of Central Manchester NH ,198 1,198 0 Other Greater Manchester Providers Sub-total - Greater Manchester Providers ,831 2,831 0 Merseyside Providers: Liverpool Heart & Chest Hospital NHST ,003 1,003 0 Walton Centre NHSFT Other Merseyside Providers Sub Total - Merseyside Providers ,476 2,476 0 Independent Sector Contracts Ramsey 1,367 1, ,204 8,204 0 Sub Total - Independent Sector Contracts 1,367 1, ,204 8,204 0 Total Acute Contracts 21,910 21, , ,459 0 Mental Health Service Lancashire Care NHSFT 3,218 3, ,310 19,310 0 Calderstones Partnership NHSFT Other Mental Health Providers Total Mental Health Contracts 3,381 3, ,284 20,284 0 Community Health Contracts Lancashire Care NHSFT 2,893 2, ,356 17,356 0 Blackpool Fylde & Wyre Hospitals NHSFT Other Community Providers Total Mental Health Contracts 3,062 3, ,374 18,374 0 Financial Performance Report NHS Greater Preston CCG Governing Body Meeting Page 8 of 8
36 GP/GB/ Part 1 Part 2 Performance Management Report NHS Greater Preston CCG Governing Body Meeting Governing Body Meeting Report Title: Performance Management Report June 2013 Written by : Presented by: Purpose of the paper: Alison Hewitt, Head of health Economics / Senior Finance Lead Iain Crossley, Chief Finance and Contracting Officer The aim of the Performance Report is to provide the Governing Body with the information required to gain assurance that the aims and objectives set out in the Integrated Commissioning Plan and the annual Delivery Plan are being achieved and to identify those areas where current plans may need to be amended to improve delivery. Key issues Performance is summarised as a Balanced Scorecard which sets out progress on all of the key indicators. These form the basis for the CCG Assurance Framework and the Quality Premium assessment. The information is presented as a briefing book; it is planned to develop both the content and style as further information becomes available. The report details performance against the Constitution, Quality and Outcomes indicators and progress towards the achievement of the Delivery Plan 2013/14. The majority of the data relates to only the first month of the year to the end of April 2013, although this has been updated where possible for the key indicators. At present there is no reliable data available on the performance of the health economy in terms of primary care referrals, outpatient or hospital activity. Areas for Improvement Indicator A&E performance against the 4 hour wait target is below the threshold at Lancashire Teaching Hospitals Referral to Treatment Times are below expectations at Lancashire Teaching Hospitals Cancer waiting times are under pressure at Lancashire Teaching Hospitals C-Difficile healthcare acquired infection rates are high (6 actual v 4 expected) Actions required by Governing Body Members The Governing Body is asked to note the content of this report. Action A plan has been developed to improve performance and this has been considered by the Joint Executive Team A plan has been developed to improve performance and this has been considered by the Joint Executive Team A plan has been developed to improve performance and this has been considered by the Joint Executive Team This is being reviewed by the Quality Improvement Committee

37 Performance Management Report June Introduction 1.1. This paper is the first Performance Report prepared for the CCG and comprises performance data for the first month of the operating year, April 2013, supplemented where possible with month 2 data The Performance Report has been compiled from two primary external information sources; the integrated business report compiled by the Commissioning Support Unit and the NHS England Regional Brief. This has been supplemented from a number of other sources of data and intelligence gathered and prepared by the CCG Additional performance data acquired via NHS England covers performance to 2 June which equates to a month 2 position on many of the key sensitive indicators such as A&E waiting times and Referral to Treatment times The Commissioning Support Unit has had considerable operational difficulties in compiling performance data for April, predominantly due to National data issues. It is anticipated both the timeliness and quality of the performance management information CSU can be improved in the coming months. 2. Plan on a Page Performance Management Report NHS Greater Preston CCG Governing Body Meeting

38 2.1. The CCG Plan on a Page summarises the delivery framework the CCG is working within, and the key performance indicators which are being used to assess delivery The outcomes are detailed on the right of the schematic and as data becomes available, will be reported monthly on the Balanced Scorecard. The Scorecard has been developed by NHS England and is the prime performance tool to support ongoing CCG performance discussions. 3. Quality Premium Indicators 3.1. The quality premium is intended to reward the CCG for improvements in the quality of the services it commissions and for associated improvements in health outcomes and reducing inequalities. There are 4 national and 3 local measures which the CCG must deliver to earn portions of the quality premium. However, there are three overall quality measures which pre-qualify the CCG to receive the premium. In summary these are: management of the CCG resources within its financial allocation no serious quality failures in the year achievement of constitutional rights of patients in relation to: (a) maximum 18-week waits from referral to treatment, (b) maximum four-hour waits in A&E departments, Performance Management Report NHS Greater Preston CCG Governing Body Meeting Page 3 of 7
39 (c) maximum 62-day waits from urgent GP referral to first definitive treatment for cancer, and (d) maximum 8-minute responses for Category A red 1 ambulance calls 3.2. As at the end of May, the main acute services provider, Lancashire Teaching Hospitals FT are not meeting the A&E 4 hour waiting time threshold and the 18 week RTT threshold could also potentially be missed. Cancer waiting times are also under pressure, with deteriorating results in consecutive months C-difficile occurrences in April are on plan (6 actual versus 4 plans). 4. Summary Performance the Balanced Scorecard 4.1. Constitutional indicators have been rated as amber at CCG level. This means performance is not optimal, but overall no measures are red at CCG level. However, significantly at provider level, Lancashire Teaching Hospitals FT has missed the 4 hour A&E target in April (and May) and there is 1 breach of the 52 week complete pathway target On amber alert are two constitutional measures; RTT for admitted patients are falling slightly short of the 90% target, and the 6 week waiting time for diagnostic tests has been breached at 2.3% (1% target) Quality performance overall has been rated as amber. Whilst many of the indicators are on target, the relative weighting of Never events and SIs is driving this rating. There is a possibility of a Never event being recorded in May, whilst 7 new SIs have been recorded in April. The data from Friends and Family tests is not yet available The CCG s outcomes overall have been rated as amber, with more than one indicator significantly off track. However, these indicators are longer term and span 2009 to Two of the threshold key indicators MRSA and C-difficile, are both green and in line with plan; although the C-difficile performance requires careful observation Of the three CCG local priorities, which have been chosen as key improvement areas for this year, one measure is significantly off track while two are progressing: dementia diagnosis projects are underway, with some actions implemented. Liaison with Lancashire Teaching Hospitals FT commences in July and further LES activity is in development. there is no project underway to specifically focus on Under 19s Admissions, although other projects will positively impact on this target. Further work needs to be undertaken on this priority. direct access to cardiology diagnostics has been recently implemented and is progressing in line with expectations. Performance Management Report NHS Greater Preston CCG Governing Body Meeting Page 4 of 7
40 5. Performance against the Operating Plan 2013/ In April 2013, the CCG approved a portfolio of projects as part of the Annual Delivery Plan 2013/14. All these projects have now been reviewed, categorised and analysed to ensure the CCG has an appropriate portfolio of activity to support its aims and outcomes for this year. The projects have been categorised into manageable groups (programmes) of work Projects have also been aligned within the emerging collaborative structure. The initial programme categories have been set as: Collaborative working, Elective care, Primary Care, Urgent care. CCG Projects - Domain Alignment Overview Project Collaborative Working Bariatric Surgey Chronic Fatigue Reconfiguration of Mental Health Beds Elective Care Dermatology Diabetes - Shift to Primary Care Diagnostics ENT Tier 2 Gynaecology GpwSI Integrated Referral Gateway Neurology / Headache Pathway - GPwSI Orthopaedic Review Physiotherapy Service Review Podiatry Service Review Long Term conditions Long Term Conditions (Integrated Teams) Primary Care Anti-Coagulant Service GP - IT Help Direct Pain Management (Online Programme) Phlebotomy Review RAIDR Urgent Care Alcohol Liaison Dementia DVT Pathway End of Life Frequent Callers IAPT Review of Urgent Care Services including OOH U19's Admissions for Asthma, Diabetes and Epilepsy QUALITY PREMIUIM NHS Constution Quality, Innovation Domain Alignment National Measures Local Measures Local Priorities Rights & Pledges Productivity, Prevention Phase Dom 1 Dom 2 Dom 3 Dom 4 Dom 5 NM1 NM2 NM3 NM4 NM5 NM6 NM7 LP1 LP2 LP3 CRP1 CRP2 CRP3 CRP4 Q I P P KEY: Phases: Scoping Dom 1 Domains Preventing people dying prematurely National Measures NM1 Reducing PYLL from amen' mortality (12.5%) Local Priorities LP1 LTC NHS Constitution CRP1 Referral to treatment times Pilot Dom 2 Enhancing Quality of Life for people - NM2 Reducing avoidable Emerg' Admis' (25%) LP2 Admis' Avoid' maximum - 18 Weeks Contract/procur'mt Long Term Conditions NM3 Improving patient exp' of Hospital (12.5%) LP3 Diagnostics CRP2 A & E Waits - Max 4hrs Full implementation Dom 3 Helping people recover from episodes NM4 Preventing healthcare assoc Infect' (12.5%) CRP3 Cancer waits - Max 62 days Review point of ill health or following injury NM5 U 19's Admissions (12.5%) from referral to 1st treat' Evaluation Dom 4 Ensuring people have a positive NM6 Dementia (12.5%) CRP4 Max 8mins response for Cat' Dom 5 experience of care NM7 Cardiology Diagnostics (12.5%) A Red 1 Ambulance Calls Treating & caring for people in a safe environment, protecting from harm 5.3. The above mapping exercise has been undertaken to ensure that the programmes of work: Covers all domains of the outcomes framework, Performance Management Report NHS Greater Preston CCG Governing Body Meeting Page 5 of 7
41 5.4. This shows: Supports delivery of the Constitution, Drives achievement of the Quality Premium, and Focuses on the agreed National and Local Priorities. The CCG has programmes of work across all key priorities and targets, The current phase of delivery (from scoping to evaluation) of each project A small number of the projects underway this year will deliver the majority of the Operating Plan the 80 / 20 rule. These projects are high value / high risk / high benefit in nature. The CCG has classified these projects as major projects for performance monitoring and will focus on their delivery even more closely than the smaller, less risky or impactful projects. 6. Major Projects Project ADMISSIONS AVOIDANCE Orthopaedic Service Review Physiotherapy Service Review Podiatry Service Review Integrated Referral Gateway Reconfiguration of Mental Health Beds Review of Urgent Care Services Inc. OOH DIAGNOSTICS Cardiology Direct Access LONG TERM CONDITIONS Integrated Teams Performance Management Report NHS Greater Preston CCG Governing Body Meeting Update Review is now complete. Feedback to both CCGs, implementation to be determined by Joint Executive Committee. Full evaluation of the project is now complete, awaiting further direction from the Clinical Leads and consideration of Procurement options. Service Model to be agreed and consideration of Procurement options underway. Project roll out has been delayed. Anticipate implementation for end of July Business Case has now been developed for triage for procedures of Low Clinical Value. Project led by Blackburn with Darwen CCG; no delivery issues Whole Systems Urgent Care review underway Project implemented in June for access to 24 hours tape and echo. Annual work programme agreed to look at all specialities for direct access over a 12 month period. For Urgent requests, telephone line to be introduced and all referrals to be triaged. Pilot has commenced in Leyland and Ashton but slow start. Virtual Team will work with both sites to identify high risk patients, and determine solutions on best processes and pathways to support admission avoidance. Pilot will inform Page 6 of 7
42 Dementia Medicines Management future Integration model / structure. Project implemented. A Dementia Liaison is to be established in LTHFT by July. Dementia LES in the process of development. New lead has been appointed to oversee the project for Chorley & South Ribble and Greater Preston CCG s. Awaiting update on prescribing data, milestones and agreed processes The Programme Office team will support the Operations and Delivery team to ensure corrective activity is defined and implemented as necessary to ensure the best possible chance of achieving the outcomes within this year. 7. Actions Required by the Governing Body 7.1. The Governing Body is asked to note the content of this report. Performance Management Report NHS Greater Preston CCG Governing Body Meeting Page 7 of 7

43 Performance Report Governing Body June 2013
44 NHS CONSTITUTION OUTCOMES QUALITY Organisation: LTH LCFT GP CCG Organisation: LTH LCFT Organisation: GP CCG QP QP OVERALL Apr-13 Apr-13 Apr-13 OVERALL No data No data OVERALL Apr-13 Urgent care ACUTE TRUST A&E 4 hour Apr-13 Apr-13 n/a Regulators * * Red 1 Cat A8 Amb n/a n/a Apr-13 NWAS CQC Enforcement Apr-13 Apr-13 * Red 2 Cat A8 Amb n/a n/a Apr-13 NWAS Monitor Quality All Reds (<19mins) n/a n/a Apr-13 NWAS compliance Apr-13 Apr-13 Mixed Sex breach Apr-13 Apr-13 Apr-13 NHSTDA Quality risk n/a n/a Cancelled Ops No data n/a No data Years of life lost Clinical effectiveness Unplanned Planned care SHMI outlier n/a hospitalisation RTT Adm 90% Apr-13 n/a Apr-13 HSMR outlier n/a Ambulatory care RTT non Adm 95% Apr-13 Apr-13 Apr Asthma & diabetes * RTT Incomp 92% Apr-13 Apr-13 Apr-13 Patient experience * CCG BALANCED SCORECARD Monthly Review GREATER PRESTON CCG NHS CONSTITUTION QUALITY OUTCOMES Compared to the England average at present wk breaches Apr-13 n/a Apr-13 F&Family concern No data No data EM admissions 6 week diagnostic Apr-13 n/a Apr-13 Mixed sex > 0 Apr-13 Apr-13 Acute not normally requiring admission week cancer Q4 12/13 n/a Q4 12/13 PCT Safety Children with LRTI week breast Q4 12/13 n/a Q4 12/13 PCT MRSA >0 Apr-13 Apr-13 <> 30 days of discharge day cancer Q4 12/13 n/a Q4 12/13 PCT Cdiff > trajectory Apr-13 Apr day surgery Q4 12/13 n/a Q4 12/13 PCT Unclosed SUIs Apr-13 Apr Positive experience 31 day drug Q4 12/13 n/a Q4 12/13 PCT Never events in Q May-13 May-13 * Friends & Family test No data 31 day radioth. Q4 12/13 n/a Q4 12/13 PCT day cancer May-13 n/a Q4 12/13 PCT CCG 5. Safe environment 62 day screening Q4 12/13 n/a Q4 12/13 PCT Authorisation - MRSA Apr day cons upg Q4 12/13 n/a Q4 12/13 PCT clinical governance Mar-13 Mar-13 C Diff Apr-13 Mental Health CPA 7 days n/a Apr-13 Q4 12/13 PCT Local priorities Dementia Diagnosis Apr-13 * QP * * Impacts on quality premium payment * Indicator RAG ratings -available separately Overall domain RAG rating no indicators rated red no indicators rated red but future concerns 1 indicator rated red 2+ indicators red Indicator RAG ratings -national criteria yes/no white denotes within range Overall domain RAG rating All No responses 1+ Yes responses but mitigating plan in place for patient risk 1+ Yes responses but NO mitigating plan/doesn t address patient risk Enforcement action by CQC, Monitor or TDA. CCG not engaged in action planning * Combined measure * 1. Preventing people from dying 2. Quality of life for LTC 3. Helping people to recover Under 19 Yrs Admissions Apr-13 Diagnostics: Cardiology Apr IAPT Quality premium (QP) * national measure, * local measure Apr-13 Indicator RAG ratings -not clear, in the interim England comparison used Overall domain RAG rating All KPIs on track for Quality Premium Not all KPIs on track for Quality Premium 1+ KPI statistically significantly off track All KPIs statistically significantly off track

45 A&E Performance During the week ending 02/06/13 the North region met the 95% national standard of patients waiting less than 4 hours in A&E with performance overall at 96.8%. Performance for Q1 to date is currently above the national standard at 95.1%. Lancashire Teaching Hospital 92.07%
46 A&E Performance to April 2013 A&E 4 Hour Target Lancashire Teaching Hospitals Trust Period There are national pressures relating to this indicator. LTHFT have informed the CCG that they have informed their Board and actions are being developed to reduce waiting times in the Accident and Emergency Department. Target YTD CSR CCG Performance April % 83.31% Trend Analysis April 2012 April 2013

47 18 Weeks Referral To Treatment Provider (provisional April 2013 data) Lancashire Teaching Hospitals FT Adm 95% 90% Adm 95% Non In- 85.7% Adm 88.1% 95.5% 92.6% comp 92%
 Lancashire Care FT Non Adm 95% In- 98.5% 99.")
48 18 Weeks Referral To Treatment Provider (provisional April 2013 data) Lancashire Care FT Non Adm 95% In- 98.5% 99.8% comp 92%
49 18 Weeks Referral To Treatment - April 2013 Period Referral to Treatment (Adjusted Admitted) Percentage of patients seen within 18 weeks Referral to Treatment (RTT) for adjusted admitted pathways (Commissioner) Month 1 is indicating underperformance at 88.1 % with the overall target for achievement being 90%. Trauma & Orthopaedics has failed at 83% which is indicating red, however there is underperformance in General Surgery achieving 87% which has the greatest variance in terms if actual activity with 18 cases not achieving 18 weeks. This will be investigated with LTH and placed on the contractual issue log for discussion at the next contract meeting. Target YTD GP CCG Performance April % 88.1% Trend Analysis April 2012 March 2013
50 52 Week Breaches to April 2013 Number of incomplete pathways waiting >52 weeks The number of patients waiting at period end for incomplete pathways >52 weeks. Period This indicator has been reported as red throughout the last financial year. In March 2012 there were 23 patients waiting beyond 52 weeks. This has improved to a position of 1 patient in February and March and April Target YTD CSR CCG Performance April Trend Analysis April 2012 March 2013
51 Cancer 62 day RTT to 02/06/13 62 day wait for treatment Percentage of patients seen within 62 days from date of urgent referral to first definitive treatment Period April 2013 May 2013 Target >85% GP CCG Performance 83.6% 77.8% This indicator was reported as not meeting the target in April and May 2013, by Lancashire Teaching Hospitals NHS Foundation Trust (LTHFT) as part of their briefing to the Elective Care Board. The predicted outturn for Q is that performance may deteriorate further with possibly as few as 63.5% of patients receiving treatment within the 62 day window. Trend Analysis April 2012 March 2013
52 Diagnostic Waits to April 2013 CB_B4: RTT The % of patients waiting 6 weeks or more for a diagnostic test- breach of target is 1% Period This indicator was reported as not meeting the target in April and May 2012 and then again in March and April There were 83 breaches of the 6 week diagnostic standard. In April 77 breaches in Cystoscopy, 4 breaches in Urodynamic and 2 breaches in Colonoscopy. Lancashire Teaching Hospitals NHS Foundation Trust (LTHFT) has subcontracted Spire Healthcare and Ramsay Healthcare to support the improvement of this indicator. Target GP CCG Performance April 2013 <1% 4.1% Trend Analysis April 2012 April 2013
53 Healthcare Aquired Infection HCAI to April 2013 Regional Comparators Published commissioner data for April 2013 shows that the North Region had 32 cases of MRSA, this is 3 cases less than the same period in For acute providers in the North Region provisional MRSA data indicates that there were 10 cases in April 2013 compared to 17 in April Published commissioner data for April 2013 shows that the North Region had 386 cases of C-difficile which is 53 cases above the plan of 333 cases. For acute providers in the North Region provisional C-difficile data indicates there were 166 cases in April 2013 which is 42% of the quarter one plan of 392 cases. Greater Preston CCG MRSA 0 Actual C-difficile 6 Actual 4 Plan


54 Prevention and Safety to April 2013 Lancashire Teaching Hospitals FT Mortality analysis for the period 2011/12 HSMR is which is within the expected range SHMI is which is within the expected range Deaths after surgery is which is within the expected range Deaths in low-risk conditions is 0.7 which is within the expected range There have been 0 recorded never events in April 2013 in Lancashire Teaching Hospitals NHS Foundation Trust. There have been 0 recorded never events in April 2013 in Lancashire Care NHS Foundation Trust. There have been 0 recorded never events in April 2013 in Ramsay Healthcare. We are aware of 2 possible cases which may be recorded as never events in the near future (or SI events)
55 Prevention and Safety to April 2013 Care Quality Commission (CQC) Lancashire Teaching Hospitals NHS Foundation Trust is compliant with all of the 16 CQC Essential Standards. Serious Incidents (SI) As at the end of April 2013, there were 52 Serious Incidents open in the footprint of Chorley & South Ribble CCG and Greater Preston. 7 Serious Incidents were reported in April Reporting Trust No of open SIs Lancashire Teaching NHS Foundation Trust 13 Lancashire Care Foundation Trust - Community 13 Lancashire Care Foundation Trust - Mental Health 26
56 GP/GB/ Part 1 Part 2 Governing Body Meeting 26 June 2013 Report Title Assurance Framework 2013/14 Written by Presented by Purpose of the paper Lisa Stott, Corporate Affairs and Governance Manager Mike Barker, Head of Corporate Services This paper is presented to the Governing Body to provide an overview of the strategic risks which may threaten the achievement of the Clinical Commissioning Group s strategic objectives. Key issues All NHS organisations are required to develop and maintain an Assurance Framework in accordance with government regulations applied to the NHS. The CCG has developed this Governing Body Assurance Framework for 2013/14 in alignment with its operating plan for the financial year. It includes the principles of an assurance framework drawn from NHSLA guidance and serves as an integral part of the CCG s internal controls systems and processes. The Assurance Framework is presented at Annex A as a high level dashboard of the top 10 risks currently identified, and at Appendix A in more detail. Actions required by Governing Body Members The Governing Body is asked to: agree the initial BAF for 2013/14; support the further development of action plans to mitigate risks where they are not currently captured; note the positive assurances currently detailed and that the Audit Committee will maintain oversight of the detailed risk management strategy and assessment challenge process on its behalf. Assurance Framework 2013/14 NHS Greater Preston CCG Governing Body Meeting
57 Assurance Framework 2013/ Purpose of the paper 1.1 This paper is presented to the Governing Body to provide an overview of the strategic risks which may threaten the achievement of the Clinical Commissioning Group s strategic objectives. 2.0 Background 2.1 All NHS organisations are required to develop and maintain an Assurance Framework in accordance with government regulations applied to the NHS. 2.2 The Assurance Framework allows the Governing Body to consider the risks that may hamper the CCG from delivering its statutory duties and functions. 2.3 The CCG has developed this Governing Body Assurance Framework for 2013/14 in alignment with its operating plan for the financial year. It includes the principles of an assurance framework drawn from NHSLA guidance and serves as an integral part of the CCG s internal controls systems and processes. 2.4 The operating plan identifies eight key strategic priorities that form the principles of the CCG s assurance framework. The description of the risk identified is based on each team s business and delivery priorities that support the eight key priorities. 3.0 Principles of Assurance 3.1 The principles of assurance are set out in the NHS guidance document Building the Assurance Framework: A Practical Guide for NHS Boards. 3.2 The CCG is required to have a framework for assurance that provides a simple but comprehensive system for effective and focused management. It also provides a structure for the evidence required for completion of the Annual Governance Statement. 3.3 For the Governing Body to determine the level of assurance it is receiving, it needs to assess the following: Full assurance: there are sufficient, relevant and positive assurances to confirm the effectiveness of controls and objectives are met Gaps in control: there is a clear conclusion, based on sufficient and relevant work, that one or more of the key controls on which the organisation is relying, is not effective. Gaps in assurance: there is a lack of assurance, either positive or negative, about the effectiveness of one or more of the controls. This may be due to Assurance Framework 2013/14 NHS Greater Preston CCG Governing Body Meeting Page 1of 4
58 lack of relevant reviews or concerns about the scope or depths of the reviews that have taken place. 4.0 Developing the Assurance Framework 4.1 The Assurance Framework is presented at Annex A (below) as a high level dashboard of the top 10 risks currently identified, and at Appendix A in more detail. 4.2 It has been developed through consultation with the Senior Management Team around the following Strategic objectives: i. To Improve Health Outcomes ii. To maximise value from our financial resources iii. To focus on interventions that will make a major difference iv. To build successful partnerships which promote system working and integrated service delivery v. To hold providers of commissioned services to account for the quality of services delivered vi. To effectively engage patients and the public in decision making vii. To ensure continuous improvements in primary care services viii. To be an effective, efficient, innovative, clinically-led CCG 4.3 A member of the Senior Management Team was identified for each Strategic Objective and asked to identify and assess any associated obstacles or issues that were risks to the successful delivery of their risk. 4.4 The level of risk was assessed in relation to: Gross Risk: the level of risk if no arrangements are in place to control, manage or mitigate. Net Risk: the level of risk given existing controls, e.g. policies. Target Risk: representative of the risk appetite and where the risk should move with further mitigating actions. 4.5 Further work is required to ensure each risk is challenged, the appropriate controls are in place, the assurances are sought and validated, and actions to mitigate completed in a timely manner. 4.6 Additionally, the risks to delivery of the CCG s Strategic business will be expanded further to include the operational objectives of each business area and work programme to ensure these are appropriately captured and monitored. 5.0 Assurance Framework A Summary Assessment 5.1 The Assurance Framework demonstrates to the Governing Body that there is a range of controls and assurance in place to support the achievement of the CCG s Strategic Operating Plan. Assurance Framework 2013/14 NHS Greater Preston CCG Governing Body Meeting Page 2of 4
59 5.2 Twenty two strategic risks have been identified across six of the eight strategic objectives outlined at point 4.2 above. 5.3 Risks associated with two of the objectives are currently being worked up, and are not included within this first submission. 5.4 Ten risks have been assessed as presenting a high level (current risk score of 15 or above) of risk to the delivery of the CCG s objectives. Actions to mitigate these risks will be agreed and progressed accordingly, where they are not already in place. The target level of risk for these objectives is depicted on the Assurance Framework summary dashboard. 5.5 A further seven risks have a medium (current risk score between 9 and 12) risk rating. Action plans will be developed to ensure the risks remain on track to achieve their target position. 5.6 All remaining risks are currently assessment as presenting low levels of risk, with the exception of one risk which is still undergoing assessment. 5.7 All risks within the framework have identified controls and assurances. Further work will be completed to validate their effectiveness. 6.0 Recommendations 6.1 The Governing Body is asked to: Agree the initial BAF for 2013/14 Support the further development of action plans to mitigate risks where they are not currently captured Note the positive assurances currently detailed and that the Audit Committee will maintain oversight of the detailed risk management strategy and assessment challenge process on its behalf. Lisa Stott Corporate Affairs and Governance Manager June 2013 Assurance Framework 2013/14 NHS Greater Preston CCG Governing Body Meeting Page 3of 4

60 Annex A Assurance Framework 2013/14 NHS Greater Preston CCG Governing Body Meeting Page 4of 4
61 Appendix A Board Assurance Framework Objective 1 To Improve Health Outcomes Alan Stedman Objective 2 To maximise value from our financial resources Iain Crossley Objective 3 To focus on interventions that will make a major difference Louise Giles Objective 4 Objective 5 To build successful partnerships which promote system working and intergrated service delivery To hold providers of commissioned services to account for the quality of services delivered Jan Ledward Louise Giles Iain Crossley Alan Stedman Objective 6 To effectively engage patients and the public in decision making Mike Barker Objective 7 To ensure continuous improvements in primary care services Louise Giles Objective 8 To be an effective, efficient, innovative clinically-led CCG All Assurance Framework 2013/14 Appendix A NHS Greater Preston CCG Governing Body meeting Page 1 of 1
62 CSR/GB/ Part 1 Part 2 Governing Body Meeting 26 June 2013 Report Title: Written by : Presented by: Memorandum of Understanding Provision of Commissioning Support by Blackpool CCG to the North West CCGs Anne Whittle, Governing Body Secretary Mike Barker, Head of Corporate Services Purpose of the paper: The paper outlines how Blackpool CCG Ambulance Commissioning Team (BCCGACT), formerly NHS Blackpool PCT, will provide commissioning support to the North West CCGs from 1 April 2013 with regards to: Key issues North West Ambulance Service Paramedic Emergency Service (PES) North West Ambulance Service & Arriva Patient Transport Services (PTS) NHS Direct NHS 111 Service The structure of BCCGACT has now been agreed with CCG Chief Officers on principles of how ambulance and 111 commissioning will be undertaken collaboratively on behalf of the CCGs in the North West. The agreement has been signed off on behalf of CCGs by their nominated representative at the Strategic Partnership Board on 4 March The details of the roles and responsibilities will be incorporated into each of the contracts and co-ordinated on behalf of CCGs by NHS Blackpool CCG. The emphasis will be on a localised approach to focus on the key areas that collective CCGs think will have the biggest impact on reducing demand requiring ambulance attendance and conveyance. The governance process map in appendix 1 identifies how the links at a regional and CCG footprint level could work in practice. The configuration of the local governance element remains for local determination. The support is provided under a three-year service level agreement. This will be updated and formalised following the publication of the new contract transition governance arrangements by the Department of Health prior to 1 April Actions required by Governing Body Members The Governing Body is asked to approve the attached Memorandum of Understanding and the Chief Officer to confirm the agreement with NHS Blackpool CCG. Memorandum of Understanding - Provision of Commissioning Support by Blackpool CCG to the North West CCGs NHS Greater Preston CCG Governing Body Meeting

63 Memorandum of Understanding-Provision of Commissioning Support by Blackpool CCG to the North West CCGs Background Ambulance Commissioning is not designated as either a Commissioning Board or Specialist Commissioning function and is clearly a CCG responsibility. However it is widely acknowledged that Ambulance Commissioning mirrors many of the key tasks and role associated with Specialist Commissioning, from complex relationship management where expert knowledge of the services, contractual requirements and relationship management is essential in holding the Provider to account and instigating reform. Consequently CCG s throughout the North West have agreed to retain the current centralised team at Blackpool CCG to provide this function/service as well as the contract management of 111. Within a collaborative Lead Commissioning framework there needs to be an appropriate level of leadership, ownership of issues and accountability for delivery delegated to health economies/areas and CCG s in the governance process. There is a clear recognition of the principle that one size does not fit all even within a regionally coordinated framework. There needs to be clear accountability with local flexibility to deliver change both centrally and locally. Summary The paper outlines how Blackpool CCG Ambulance Commissioning Team (BCCGACT) formally NHS Blackpool PCT will provide commissioning support to the North West CCGs from the 1 st April 2013 with regards to: North West Ambulance Service Paramedic Emergency Service (PES) North West Ambulance Service & Arriva - Patient Transport Services (PTS) NHS Direct NHS 111 service The structure has now been agreed with CCG Chief Officers on principles of how ambulance and 111 commissioning will be undertaken collaboratively on behalf of the CCGs in the North West. The agreement has been signed off on behalf of CCGs by their nominated representative at the Strategic Partnership Board on the 4 th March. The details of roles and responsibilities will be incorporated into each of the contracts coordinated on behalf of CCGs by NHS Blackpool CCG. The emphasis will be on a localised approach to focus on the key areas that Collective CCGs think will have the biggest impact on reducing demand requiring ambulance attendance and conveyance. The governance process map in Appendix 1 identifies how the links at a regional and CCG footprint level could work in practice. The configuration of the local governance element remains for local determination. The support is provided under a three year service level agreement. This will be updated and formalised following the publication of the new contract transition governance arrangements by the Department of Health prior to the 1st April As previously shared and agreed by CCGs the costs of the team split by CCG are included in Appendix 2. 1
Governing Body Meeting - Agenda
 MEETING HELD IN PUBLIC Governing Body Meeting - Agenda GP/GB/20130425 25 April 2013, Gujerat Centre, South Meadow Lane, Preston PR1 8JN 2.00pm - 3.30pm 1. Welcome and introductions Apologies for absence
MEETING HELD IN PUBLIC Governing Body Meeting - Agenda GP/GB/20130425 25 April 2013, Gujerat Centre, South Meadow Lane, Preston PR1 8JN 2.00pm - 3.30pm 1. Welcome and introductions Apologies for absence
Governing Body Meeting - Agenda
 MEETING HELD IN PUBLIC CSR/GB/20130424 Governing Body Meeting - Agenda 24 April 2013, Fox Lane Cricket Club, Leyland PR25 1HB 12.30pm 2.30pm 1. Welcome and introductions Apologies for absence Dr G Bangi
MEETING HELD IN PUBLIC CSR/GB/20130424 Governing Body Meeting - Agenda 24 April 2013, Fox Lane Cricket Club, Leyland PR25 1HB 12.30pm 2.30pm 1. Welcome and introductions Apologies for absence Dr G Bangi
MEMORANDUM OF UNDERSTANDING
 MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Our mission. Our values. Our aims. Our strategic objectives
 Our mission To ensure that the health services we manage for the people of Trafford are provided at the right place and at the right time, and that services are safe, of a high quality and are value for
Our mission To ensure that the health services we manage for the people of Trafford are provided at the right place and at the right time, and that services are safe, of a high quality and are value for
Commissioning for Value insight pack
 Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
Commissioning for Value insight pack NHS England Gateway ref: 00525 Contents Introduction: the call to action The approach Where to look using indicative data Phase 2 & 3 Why act what benefits do the population
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST EXECUTIVE REPORT - CURRENT ISSUES
 Agenda item A4(i) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST EXECUTIVE REPORT - CURRENT ISSUES 1. Executive Team Particular attention is drawn to: i) Half year trading positions with actions
Agenda item A4(i) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST EXECUTIVE REPORT - CURRENT ISSUES 1. Executive Team Particular attention is drawn to: i) Half year trading positions with actions
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aneurin Bevan Health Board. Living Well, Living Longer: Inverse Care Law Programme
 Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
SUPPORT FOR VULNERABLE GP PRACTICES: PILOT PROGRAMME
 Publications Gateway Reference 04476 For the attention of: NHS England Directors of Commissioning Operations Clinical Leaders and Accountable Officers, NHS Clinical Commissioning Groups Copy: NHS England
Publications Gateway Reference 04476 For the attention of: NHS England Directors of Commissioning Operations Clinical Leaders and Accountable Officers, NHS Clinical Commissioning Groups Copy: NHS England
A healthier Lancashire and South Cumbria
 A healthier Lancashire and South Cumbria Improving health and care for local people Published May 2017 Bay Health & Care Partners Pennine Lancashire Fylde Coast West Lancashire Central Lancashire Healthier
A healthier Lancashire and South Cumbria Improving health and care for local people Published May 2017 Bay Health & Care Partners Pennine Lancashire Fylde Coast West Lancashire Central Lancashire Healthier
DRAFT CONTINUING HEALTHCARE (CHC) CHOICE & EQUITY POLICY. Version 2
 CHOICE & EQUITY POLICY. Version 2") DRAFT CONTINUING HEALTHCARE (CHC) CHOICE & EQUITY POLICY Version 2 1 Subject and version number of document: Continuing Healthcare (CHC) and Funded Nursing Care (FNC) Choice and Equity Policy Serial number:
DRAFT CONTINUING HEALTHCARE (CHC) CHOICE & EQUITY POLICY Version 2 1 Subject and version number of document: Continuing Healthcare (CHC) and Funded Nursing Care (FNC) Choice and Equity Policy Serial number:
Telford and Wrekin Clinical Commissioning Group. Prospectus 2013/2014
 Telford and Wrekin Clinical Commissioning Group Prospectus 2013/2014 Who we are Telford and Wrekin Clinical Commissioning Group (CCG) is responsible for healthcare in the Telford and Wrekin area. We Plan
Telford and Wrekin Clinical Commissioning Group Prospectus 2013/2014 Who we are Telford and Wrekin Clinical Commissioning Group (CCG) is responsible for healthcare in the Telford and Wrekin area. We Plan
5. Does this paper provide evidence of assurance against the Governing Body Assurance Framework?
 Item Number: 6.3 Governing Body Meeting: 4 February 2016 Report Sponsor Anthony Fitzgerald Director of Strategy and Delivery Report Author Anthony Fitzgerald Director of Strategy and Delivery 1. Title
Item Number: 6.3 Governing Body Meeting: 4 February 2016 Report Sponsor Anthony Fitzgerald Director of Strategy and Delivery Report Author Anthony Fitzgerald Director of Strategy and Delivery 1. Title
NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION
 NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: [78] NHS England Effective Date: 1 December 2015 April 2017 CONTENTS Part Description Page Foreword 1 1 Introduction and Commencement
NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: [78] NHS England Effective Date: 1 December 2015 April 2017 CONTENTS Part Description Page Foreword 1 1 Introduction and Commencement
Policy reference Policy product type LGiU essential policy briefing Published date 08/12/2010. This covers England.
 1 of 7 23/03/2012 15:23 Healthy Lives, Healthy People: Public Health White Paper Policy reference 201000810 Policy product type LGiU essential policy briefing Published date 08/12/2010 Author Janet Sillett
1 of 7 23/03/2012 15:23 Healthy Lives, Healthy People: Public Health White Paper Policy reference 201000810 Policy product type LGiU essential policy briefing Published date 08/12/2010 Author Janet Sillett
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Sustainability and transformation plan (STP)
") Sustainability and transformation plan (STP) David Bowen-Cassie, Harrow CCG Alex Dewsnap, London Borough of Harrow Sanjay Dighe, Lay Member, Harrow CCG About Harrow A population of more than 239,000 people
Sustainability and transformation plan (STP) David Bowen-Cassie, Harrow CCG Alex Dewsnap, London Borough of Harrow Sanjay Dighe, Lay Member, Harrow CCG About Harrow A population of more than 239,000 people
North West COPD Report Nov 2011
 North West COPD Report Nov 2011 Working together to improve respiratory care in the North West 1 Contents Introduction foreword by NW Respiratory Leads... 3 4 reasons why COPD is important in the North
North West COPD Report Nov 2011 Working together to improve respiratory care in the North West 1 Contents Introduction foreword by NW Respiratory Leads... 3 4 reasons why COPD is important in the North
CONTINUING HEALTHCARE (CHC) CHOICE & EQUITY POLICY
 CHOICE & EQUITY POLICY") CONTINUING HEALTHCARE (CHC) CHOICE & EQUITY POLICY Ref: Version: Supersedes: Author (inc Job Title): Ratified by: (Name of responsible Committee) Date ratified: To be completed by Corporate Team To be
CONTINUING HEALTHCARE (CHC) CHOICE & EQUITY POLICY Ref: Version: Supersedes: Author (inc Job Title): Ratified by: (Name of responsible Committee) Date ratified: To be completed by Corporate Team To be
Vale of York Clinical Commissioning Group Governing Body Public Health Services. 2 February Summary
 Vale of York Clinical Commissioning Group Governing Body Public Health Services 2 February 2017 Summary 1. The purpose of this report is to provide the Vale of York Clinical Commissioning Group (CCG) with
Vale of York Clinical Commissioning Group Governing Body Public Health Services 2 February 2017 Summary 1. The purpose of this report is to provide the Vale of York Clinical Commissioning Group (CCG) with
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
Quality Strategy. CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July Head of Clinical Quality & Patient Safety
 Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Lincolnshire JSNA: Chronic Obstructive Pulmonary Disease (COPD)
") Disease (COPD) What do we know? Summary is a long-term condition, which is affecting increasing numbers of people. There is a wide range of interventions to address COPD, from prevention to the ongoing
Disease (COPD) What do we know? Summary is a long-term condition, which is affecting increasing numbers of people. There is a wide range of interventions to address COPD, from prevention to the ongoing
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
Making an impact on the public's health and wellbeing in England: Emerging Approaches and Lessons
 Making an impact on the public's health and wellbeing in England: Emerging Approaches and Lessons Professor Kevin Fenton Snr. Advisor, Health and Wellbeing Public Health England Director of Health and
Making an impact on the public's health and wellbeing in England: Emerging Approaches and Lessons Professor Kevin Fenton Snr. Advisor, Health and Wellbeing Public Health England Director of Health and
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: 3. Key Messages: The paper discussed by the Governing Body on 17 th November 2016 was included as an agenda item for discussion
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: 3. Key Messages: The paper discussed by the Governing Body on 17 th November 2016 was included as an agenda item for discussion
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
STP: Latest position. Developing and delivering the Humber, Coast and Vale Sustainability and Transformation Plan. July 2016
 STP: Latest position Developing and delivering the Humber, Coast and Vale Sustainability and Transformation Plan July 2016 Who s involved? NHS Commissioners East Riding of Yorkshire CCG Hull CCG North
STP: Latest position Developing and delivering the Humber, Coast and Vale Sustainability and Transformation Plan July 2016 Who s involved? NHS Commissioners East Riding of Yorkshire CCG Hull CCG North
Quarterly Reporting Template - Guidance
 Quarterly Reporting Template - Guidance Notes for Completion The data collection template requires the Health & Wellbeing Board to track through the high level metrics and deliverables from the Health
Quarterly Reporting Template - Guidance Notes for Completion The data collection template requires the Health & Wellbeing Board to track through the high level metrics and deliverables from the Health
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
REPORT TO CROYDON CLINICAL COMMISSIONING GROUP GOVERNING BODY Meeting in Public. 30 October 2012
 REPORT TO CROYDON CLINICAL COMMISSIONING GROUP GOVERNING BODY Meeting in Public 30 October 2012 Title: CROYDON CCG AND CROYDON PUBLIC HEALTH MEMORANDUM OF UNDERSTANDING Lead Director Report Author Contact
REPORT TO CROYDON CLINICAL COMMISSIONING GROUP GOVERNING BODY Meeting in Public 30 October 2012 Title: CROYDON CCG AND CROYDON PUBLIC HEALTH MEMORANDUM OF UNDERSTANDING Lead Director Report Author Contact
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Kingston Clinical Commissioning Group Report Summary
 Kingston Clinical Commissioning Group Report Summary Meeting Title Governing Body in public Date 9 th January 2018 Report Title Minutes of the 34 th Meeting held on 7 th November 2017 Agenda Item 3 Attachment
Kingston Clinical Commissioning Group Report Summary Meeting Title Governing Body in public Date 9 th January 2018 Report Title Minutes of the 34 th Meeting held on 7 th November 2017 Agenda Item 3 Attachment
NHS England (Wessex) Clinical Senate and Strategic Networks. Accountability and Governance Arrangements
 Clinical Senate and Strategic Networks. Accountability and Governance Arrangements") NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
Figure 1: Domains of the Three Adult Outcomes Frameworks
 Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
TRAINING PROSPECTUS WARRINGTON BOROUGH COUNCIL
 TRAINING PROSPECTUS WARRINGTON BOROUGH COUNCIL 1. INTRODUCTION The Town Hall Golden Gates Why Warrington? It is said that Warrington is where the north begins when travelling up the M6 or on the west coast
TRAINING PROSPECTUS WARRINGTON BOROUGH COUNCIL 1. INTRODUCTION The Town Hall Golden Gates Why Warrington? It is said that Warrington is where the north begins when travelling up the M6 or on the west coast
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
CVS Rochdale Policy Briefing
 CVS Rochdale Policy Briefing Healthy Lives, Healthy People: The Public Health White Paper Introduction People in England are healthier and living longer than ever before. However health inequalities in
CVS Rochdale Policy Briefing Healthy Lives, Healthy People: The Public Health White Paper Introduction People in England are healthier and living longer than ever before. However health inequalities in
Agenda Item No. 9. Key Information
 Key Information Name of footprint and no: Sussex and East Surrey (33) Region: NHSE South Nominated lead of the footprint including organisation/function: Michael Wilson, Chief Executive, Surrey and Sussex
Key Information Name of footprint and no: Sussex and East Surrey (33) Region: NHSE South Nominated lead of the footprint including organisation/function: Michael Wilson, Chief Executive, Surrey and Sussex
GOVERNING BODY MEETING 30 July 2014 Agenda Item 2.2
 GOVERNING BODY MEETING 30 July 2014 Report Title Purpose of report Personal Health Budgets This report provides an overview of the use of Personal Health Budgets (PHBs) within NHS Eastern Cheshire Clinical
GOVERNING BODY MEETING 30 July 2014 Report Title Purpose of report Personal Health Budgets This report provides an overview of the use of Personal Health Budgets (PHBs) within NHS Eastern Cheshire Clinical
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Wolverhampton Public Health Effective Commissioning Strategy
 Date: 24 September 2014 ATTACHED: Wolverhampton Public Health Effective Commissioning Strategy 2014-2019 Executive summary. Wolverhampton Public Health Effective Commissioning Strategy 2014-2019 Executive
Date: 24 September 2014 ATTACHED: Wolverhampton Public Health Effective Commissioning Strategy 2014-2019 Executive summary. Wolverhampton Public Health Effective Commissioning Strategy 2014-2019 Executive
Reducing Variation in Primary Care Strategy
 Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Quality Framework Supplemental
 Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
MEMORANDUM OF UNDERSTANDING THE PROVISION OF PUBLIC HEALTH ADVICE TO NHS COMMISSIONING IN ROTHERHAM
 MEMORANDUM OF UNDERSTANDING THE PROVISION OF PUBLIC HEALTH ADVICE TO NHS COMMISSIONING IN ROTHERHAM 1. Parties to the agreement: Rotherham Metropolitan Borough Council ( the Council ) NHS Rotherham Clinical
MEMORANDUM OF UNDERSTANDING THE PROVISION OF PUBLIC HEALTH ADVICE TO NHS COMMISSIONING IN ROTHERHAM 1. Parties to the agreement: Rotherham Metropolitan Borough Council ( the Council ) NHS Rotherham Clinical
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
Delegated Commissioning Updated following latest NHS England Guidance
 Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
EMPLOYEE HEALTH AND WELLBEING STRATEGY
 EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
A Quick Guide to Health Terminology
 A Quick Guide to Health Terminology August 2011 Health Terminology This quick guide provides an a-z of common health terminology. Asset-Based Working - a form of working whereby assets within communities
A Quick Guide to Health Terminology August 2011 Health Terminology This quick guide provides an a-z of common health terminology. Asset-Based Working - a form of working whereby assets within communities
Central Lancashire Local Delivery Plan 2016/ /21
 Central Lancashire Local Delivery Plan 2016/17 2020/21 1 Contents 1. Introduction and context 2. Our priorities 3. The health and wellbeing gap 4. The care and quality gap 5. Financial challenges, gap
Central Lancashire Local Delivery Plan 2016/17 2020/21 1 Contents 1. Introduction and context 2. Our priorities 3. The health and wellbeing gap 4. The care and quality gap 5. Financial challenges, gap
CLINICAL COMMISSIONING GROUP RESPONSIBILITIES TO ENSURE ROBUST SAFEGUARDING AND LOOKED AFTER CHILDREN ARRANGEMENTS
 MEETING DATE: 14 March 2013 AGENDA ITEM NUMBER: Item 8.6 AUTHOR: JOB TITLE: DEPARTMENT: Sarah Glossop Designated Nurse Safeguarding Children NHS North Lincolnshire Clinical Commissioning Group REPORT TO
MEETING DATE: 14 March 2013 AGENDA ITEM NUMBER: Item 8.6 AUTHOR: JOB TITLE: DEPARTMENT: Sarah Glossop Designated Nurse Safeguarding Children NHS North Lincolnshire Clinical Commissioning Group REPORT TO
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Worcestershire Public Health Directorate. Business plan 2011/12
 Worcestershire Public Health Directorate Business plan Public Health website: www.worcestershire.nhs.uk/publichealth 1 Worcestershire Public Health Directorate Business Plan Vision 1. The Public Health
Worcestershire Public Health Directorate Business plan Public Health website: www.worcestershire.nhs.uk/publichealth 1 Worcestershire Public Health Directorate Business Plan Vision 1. The Public Health
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
The Urgent Care Conundrum The importance of Information and Technology
 The Urgent Care Conundrum The importance of Information and Technology Mark Newton MSc Head of Service Urgent Care NWAS NHS Trust Consultant Paramedic Informatics: So what s it all about? Deals with the
The Urgent Care Conundrum The importance of Information and Technology Mark Newton MSc Head of Service Urgent Care NWAS NHS Trust Consultant Paramedic Informatics: So what s it all about? Deals with the
Policy: P15 Physical Healthcare Policy
 Policy: P15 Physical Healthcare Policy Version: P15/04 Ratified by: Trust Management Team Date ratified: 15 th April 2015 Title of originator/author: Director of Primary Care Title of responsible Director
Policy: P15 Physical Healthcare Policy Version: P15/04 Ratified by: Trust Management Team Date ratified: 15 th April 2015 Title of originator/author: Director of Primary Care Title of responsible Director
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Chief Executive Officer s Business Report 3. Key Messages: This report provides an overview of important clinical commissioning
QUALITY STRATEGY
 QUALITY STRATEGY 2012-2016 SPONSOR: Sue Hardy Director of Nursing Signature: AUTHORS: Sue Hardy Director of Nursing Denise Flowers Associate Director Clinical Effectiveness APPROVED BY: Southend University
QUALITY STRATEGY 2012-2016 SPONSOR: Sue Hardy Director of Nursing Signature: AUTHORS: Sue Hardy Director of Nursing Denise Flowers Associate Director Clinical Effectiveness APPROVED BY: Southend University
Whittington Health Quality Strategy
 Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
NHS Rotherham. The Board is recommended to note the proposal to adopt the NHS EDS and to approve the development and implementation of the EDS
 NHS Rotherham Management Executive 31 May 2011 NHS Rotherham Board 6 June 2011 Equality Delivery System This report has been informed by a briefing note from the SHA Contact Details: Lead Director: Sarah
NHS Rotherham Management Executive 31 May 2011 NHS Rotherham Board 6 June 2011 Equality Delivery System This report has been informed by a briefing note from the SHA Contact Details: Lead Director: Sarah
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
Position statement: GP practices in the West End of Newcastle (paper 2)
") Position statement: GP practices in the West End of Newcastle (paper 2) This statement has been provided to the Board to give an overview of the changes to GP provision in the inner west of Newcastle.
Position statement: GP practices in the West End of Newcastle (paper 2) This statement has been provided to the Board to give an overview of the changes to GP provision in the inner west of Newcastle.
DARLINGTON CLINICAL COMMISSIONING GROUP
 DARLINGTON CLINICAL COMMISSIONING GROUP CLEAR AND CREDIBLE PLAN 2012 2017 Working together to improve the health and well-being of Darlington May 2012 Darlington Clinical Commissioning Group Clear and
DARLINGTON CLINICAL COMMISSIONING GROUP CLEAR AND CREDIBLE PLAN 2012 2017 Working together to improve the health and well-being of Darlington May 2012 Darlington Clinical Commissioning Group Clear and
NHS Herts Valleys Clinical Commissioning Group Board Meeting November 5 th 2015
 NHS Herts Valleys Clinical Commissioning Group Board Meeting November 5 th 2015 Title Locality Committee Reports Q2 2015/16 Agenda Item: 13 Purpose (tick one only) Responsible Director(s) and Job Title
NHS Herts Valleys Clinical Commissioning Group Board Meeting November 5 th 2015 Title Locality Committee Reports Q2 2015/16 Agenda Item: 13 Purpose (tick one only) Responsible Director(s) and Job Title
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
The prevention and self care workshop 16 th September Dr. Jenny Harries Regional Director PHE South Regional Office
 The prevention and self care workshop 16 th September 2016 Dr. Jenny Harries Regional Director PHE South Regional Office Jenny.harries@phe.gov.uk The health and wellbeing gap If the nation fails to get
The prevention and self care workshop 16 th September 2016 Dr. Jenny Harries Regional Director PHE South Regional Office Jenny.harries@phe.gov.uk The health and wellbeing gap If the nation fails to get
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION THE BUDGET NUMBERS
 BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
PUBLIC HEALTH IN HALTON. Eileen O Meara Director of Public Health & Public Protection
 PUBLIC HEALTH IN HALTON Eileen O Meara Director of Public Health & Public Protection Aim of Presentation What we do. How we do it. What are the service outputs. What are the outcomes. How can we help.
PUBLIC HEALTH IN HALTON Eileen O Meara Director of Public Health & Public Protection Aim of Presentation What we do. How we do it. What are the service outputs. What are the outcomes. How can we help.
Equality and Health Inequalities Strategy
 Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Outcomes benchmarking support packs: CCG level
 Outcomes benchmarking support packs: CCG level NHS South Devon and Torbay CCG Produced with input from: Public Health England Forward and Introduction Local decision making is at the heart of the NHS,
Outcomes benchmarking support packs: CCG level NHS South Devon and Torbay CCG Produced with input from: Public Health England Forward and Introduction Local decision making is at the heart of the NHS,
UKMi Conference 2011 Structural Changes in the NHS Vic Standing Pharmaceutical Adviser NHS NW. Healthier Horizons
 UKMi Conference 2011 Structural Changes in the NHS Vic Standing Pharmaceutical Adviser NHS NW Healthier Horizons 1988 Secretary of State For Health Department of Health Special Health Authorities (8) NHS
UKMi Conference 2011 Structural Changes in the NHS Vic Standing Pharmaceutical Adviser NHS NW Healthier Horizons 1988 Secretary of State For Health Department of Health Special Health Authorities (8) NHS
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
17. Updates on Progress from Last Year s JSNA
 17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
Item No. 9. Meeting Date Wednesday 6 th December Glasgow City Integration Joint Board Finance and Audit Committee
 Item No. 9 Meeting Date Wednesday 6 th December 2017 Glasgow City Integration Joint Board Finance and Audit Committee Report By: Contact: Sharon Wearing, Chief Officer, Finance and Resources Allison Eccles,
Item No. 9 Meeting Date Wednesday 6 th December 2017 Glasgow City Integration Joint Board Finance and Audit Committee Report By: Contact: Sharon Wearing, Chief Officer, Finance and Resources Allison Eccles,
Expression of Interest for the Co-commissioning of Primary Care Services STATEMENT FROM OUR CHAIRMAN AND CHIEF ACCOUNTABLE OFFICER
 Brierley Hill Health and Social Care Centre Venture Way Brierley Hill West Midlands DY5 1RU Tel: 01384 321763 Fax: 01384 322414 20 June 2014 Dudley Clinical Commissioning Group Expression of Interest for
Brierley Hill Health and Social Care Centre Venture Way Brierley Hill West Midlands DY5 1RU Tel: 01384 321763 Fax: 01384 322414 20 June 2014 Dudley Clinical Commissioning Group Expression of Interest for
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
Enclosures Appendix 1: Annual Director of Public Health Report 2015 Rachel Wells Consultant in Public Health
 Title Health and Wellbeing Board 21 January 2016 The Five Ways to Mental Wellbeing in Barnet: The Annual Report of the Director of Public Health (2015) Report of Director of Public Health Wards All Status
Title Health and Wellbeing Board 21 January 2016 The Five Ways to Mental Wellbeing in Barnet: The Annual Report of the Director of Public Health (2015) Report of Director of Public Health Wards All Status
Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years
 Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years Introduction 1. Islington CCG funds a range of health services for children
Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years Introduction 1. Islington CCG funds a range of health services for children
NHS Right Care expanding the approach in the context of delivering the Five Year Forward View
 NHS Right Care expanding the approach in the context of delivering the Five Year Forward View Background 1. NHS Right Care originated as part of the QIPP programme within the Department of Health in 2009.
NHS Right Care expanding the approach in the context of delivering the Five Year Forward View Background 1. NHS Right Care originated as part of the QIPP programme within the Department of Health in 2009.
Cheshire & Merseyside Sustainability and Transformation Plan. People and Services Fit for the Future
 Cheshire & Merseyside Sustainability and Transformation Plan People and Services Fit for the Future 2 The Challenge for the NHS As a nation we are fortunate to have a National Health Service that is free
Cheshire & Merseyside Sustainability and Transformation Plan People and Services Fit for the Future 2 The Challenge for the NHS As a nation we are fortunate to have a National Health Service that is free
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Clinical Commissioning Strategy
 What we want to do Clinical Commissioning Strategy 2013-2016 Document Information Document location : This document is only valid on the day it was printed. Authorship: This document has been prepared
What we want to do Clinical Commissioning Strategy 2013-2016 Document Information Document location : This document is only valid on the day it was printed. Authorship: This document has been prepared