M1: Flipping Healthcare: Operationalizing What Matters Most
|
|
|
- Betty Berry
- 6 years ago
- Views:
Transcription
 Dayna Jornsay-Hester Organizational Development Consultant University of")
1 Orlando, Florida No Disclosures M1: Flipping Healthcare: Operationalizing What Matters Most IHI Summit March 20 22, 2016 Presenters Ana Tuya Fulton Director of Geriatric Medicine & Butler Chief of Medicine Care New England Health System Anthony DiGioia Medical Director University of Pittsburgh Medical Center (UPMC) Dayna Jornsay-Hester Organizational Development Consultant University of Pittsburgh Medical Center (UPMC) Kate DeBartolo National Field Manager Institute for Healthcare Improvement Kate Lally Director of Palliative care Care New England Health System Michelle Giarrusso Director of Patient and Family Centered Care University Of Pittsburgh Sarah Clayton Accountable Care Outcomes Specialist PFCC Innovation Center 1
2 Session Objectives Describe how different practices operationalize "what matters" and use the results to redesign care delivery Identify a replicable approach to integrating what matters as well as what s the matter into their clinical encounters Develop skills to engage with patients in what matters most and in advance care planning Today s Plan 4 12:00 PM 12:15 PM Introduction and Overview 12:15 PM 1:45 PM Care New England 1:45 PM 2:00 PM Break 2:00 PM 2:40 PM Care New England 2:40 PM 4:00 PM UPMC 4:00 PM 4:15 PM Break 4:15 PM 5:10 PM UPMC 5:10 PM 5:30 PM Combined Panel 2




3 Framing 5 Five considerations for operationalizing What Matters? Use your own words What works for your setting? How to Ask What Matters Geraldine Marsh, NHS GG&C and Healthcare Improvement Scotland Design Council, England Jennifer Rodgers, Yorkhill, NHS Scotland Cincinnati Children s Home Care Services What should I know about you that may not be on your medical chart? What does a good day look like to you? (end-of-life) What do you want to be doing six months from today that you re not able to do now? (procedure) Is there anything you re worried or concerned about? (discharge) What will success look like to you? (surgery) 3
4 Framing 7 Five considerations for operationalizing What Matters? Use your own words What works for your setting? Engage clinicians Power of small tests of change Framing 8 Five considerations for operationalizing What Matters? Use your own words What works for your setting? Engage clinicians Power of small tests of change Consider reliability (Always Events) 4
5 Framing 9 Five considerations for operationalizing What Matters? Use your own words What works for your setting? Engage clinicians Power of small tests of change Consider reliability (Always Events) Learn for the organization Framing 10 Five considerations for operationalizing What Matters? Use your own words What works for your setting? Engage clinicians Power of small tests of change Consider reliability (Always Events) Learn for the organization Be thoughtful about scale 5

6 11 Change Areas Asking What Matters Documenting What Matters Physician asks at primary care visit Pen and paper PA asks during vital signs Standardized form Pre-visit planning?????? Whiteboard EHR??? Sharing What Physician Form in Care team?????? Matters head record meeting Updating What N/A N/A Pre-visit?????? Matters planning Learning System N/A Team Meeting Champion Database??? Flipping Healthcare: Operationalizing What Matters Most Kate M. Lally MD, FACP Ana Tuya Fulton, MD, FACP 6
7 Goals for today 12:15-12:45- CNE model overview 12:45-1:45 Group exercise & Case 1:45-2:00 BREAK 2:00-2:40 Didactics Conversations Documentation Billing Disclosures Ana Tuya Fulton & Kate Lally are faculty on and receive funding from Rhode Island Geriatrics Workforce Enhancement Program (#U1QHP28737 from the US Health Resources and Services Administration) Kate Lally serves as a Faculty member for IHI for Conversation Ready 7
8 Acknowledgements Thanks to Dr. LaugeSokol-Hessner, Kelly McCutcheon Adams, and Kate DeBartolo Much of this material developed for the IHI Stat Call Series End of life Conversations: Preparing your Team for Success and CMS reimbursement Thanks to Dr. Joan Teno Welcome and Prework 16 8

9 Setting the stage Advance Care Planning: A Definition a structured dialogue with the ultimate goal that clinical care is shaped by a patient s preferences when the patient is unable to participate in decision making Teno& Lynn


10 Advance Care Planning Tool box Advance Directives are just one of the many tools in the box Limitations of Advance Directives Legal language Hypothetical & limited Don t evolve with the patient and their condition over time We will never have one perfect one size fits all form 10

11 Goals to strive for Series of conversations that evolve over time in an ongoing relationship with a provider Tailored, adapted communication styles to reach many patients with different needs Timing of discussions based on changes in condition or prognosis A treatment plan is the outcome clear wishes, goals of care, and contingency plans known ACP as a routine part of care with health care provider It applies to everyone John is a 26 year old man with no medical history coming in for his annual routine physical. His provider addresses advance care planning by asking In the event that you become incapacitated or unable to speak for yourself do you have someone who you d designate as your decision maker? Alda is an 89 year old widow with multiple medical issues included advanced heart and lung disease. Her doctor asks her about her wishes. She expresses a desire to not feel short of breath, and to avoid extraordinary measures of support. A care plan is completed to provide ongoing palliative care, and to prevent hospitalization. 11
: 8,063 employees 963 licensed beds Four hospitals Our own VNA homecare agency Dedicated hospice program and palliative programs >30% of 13,000")
12 Who are we at Care New England? Care New England by the numbers (fiscal year 2014): 8,063 employees 963 licensed beds Four hospitals Our own VNA homecare agency Dedicated hospice program and palliative programs >30% of 13,000 inpatient admissions/year are >65 Integra ACO Where we started July 2008 Butler hospital geriatric unit geriatrics co-management August 2012 Started an inpatient palliative care program Had a very small hospice One MD four days a week Hospice liaison RN June 2014 Added inpatient geriatric medicine consult service 1 community hospital, 1 MD two days per week 12
13 What our needs were Sick, complex, older patients Palliative care consults experienced explosive growth About 70% were for goals of care Have more conversations with limited resources Conversation Nurse Model: Conversation Nurse Palliative care = Team based Conversation nurse role developed & nurtured Direct ordering physician to conversation nurse communication/collaboration Education about role and team based care Now broad acceptance Growth three positions for conversation nurses (or SW) 13
14 How did we expand Expanded to inpatient palliative care consults at all four hospitals ( MDs, NPs, Conversation RN and MSW) Developed home based palliative care program Developed Palliative care outpatient clinics Boots on the ground approach to primary care offices Education Physician education Resident Simulation Palliative care and geriatrics rotation Nursing education and in-services Lunch and Learns at each operating unit Public awareness campaign Move The Conversation into the home 14

15 15
16 Mr. L 85 yowith Prostate CA, CHF referred to VNA by PCP for urinary catheter management Seen monthly by VNA and 4-6x a year by PCP for 6 years At Age 91 admitted to ICU on ventilator with pneumonia Family discussion in ICU, He wouldn t have wanted this Put on hospice, died 2 days later What Mattered to Mr. L? 6years of monthly visits by RN. Multiple visits with PCP and various specialists Pt well known to our institutions No one ever asked what mattered? 16
17 What We Heard from Staff Feel it isn t their job to ask Not comfortable having conversations about what matters Did not know where to document Did not know what to document How to Change the Culture Document what you hear when you ask What Matters to You Examples I want to die at home I want to see my sister before I die I want my children to make amends with each other I want to continue all treatment until it is clear that I cannot communicate with my family 17
18 VNA of CNE Conversation training with nurses on Palliative care teams Case Conferencing to identify patients with serious illness Conversation nurses who can go into the home and have ongoing conversations Moving into the office Hartford grant Pts seen by inpatient PC are often transitioned to home based services No great way of communicating those wishes Sending Conversation RNs into the community for ongoing goals of care Ongoing communication with PCP Goals of improving transitions/reducing readmissions in Palliative care population 18
19 Integra ACO Multidisciplinary team providing care to high risk patients Weekly meeting with PC and Geriatrics Focus on advance care planning Focus on conversation skills training Conversation Nurse as NCM She is assigned patients most in need of a conversation Moving into the office HRSA grant Meet with primary care team in their office Patient identification process trigger the conversations Who are the high risk patients Education on advance directives/molst Education about community resources NP available to do home visits for patients with highest need (Seen as extension of PCP office) Symptom management Goals of care Goal of providing more of a team to the practices Process development to track the conversations from site to site 19

20 What have we done? Added an extra layer of support to practices Conversations can be with non-physician team members Some patients respond better to non-physician providers Continuum of conversations hospital to home primary care office Group exercise The Conversation 20
21 Am I taking away hope? Does this patient trust me? Relationship and Emotions Do I trust this person? Does she recognize how this will affect my life? Let s talk about your illness Content What are my options? Provid er Patient Mrs. Smith Well Ms. Smith is 68 year-old woman with hypertension, hyperlipidemia, and history of smoking. She was recently diagnosed with emphysema/copd. She s coming in for a routine follow-up for her hypertension with her daughter. You wonder Does she need a conversation? At this stage, what s the purpose? How do I begin? How do I document and bill for this? 21
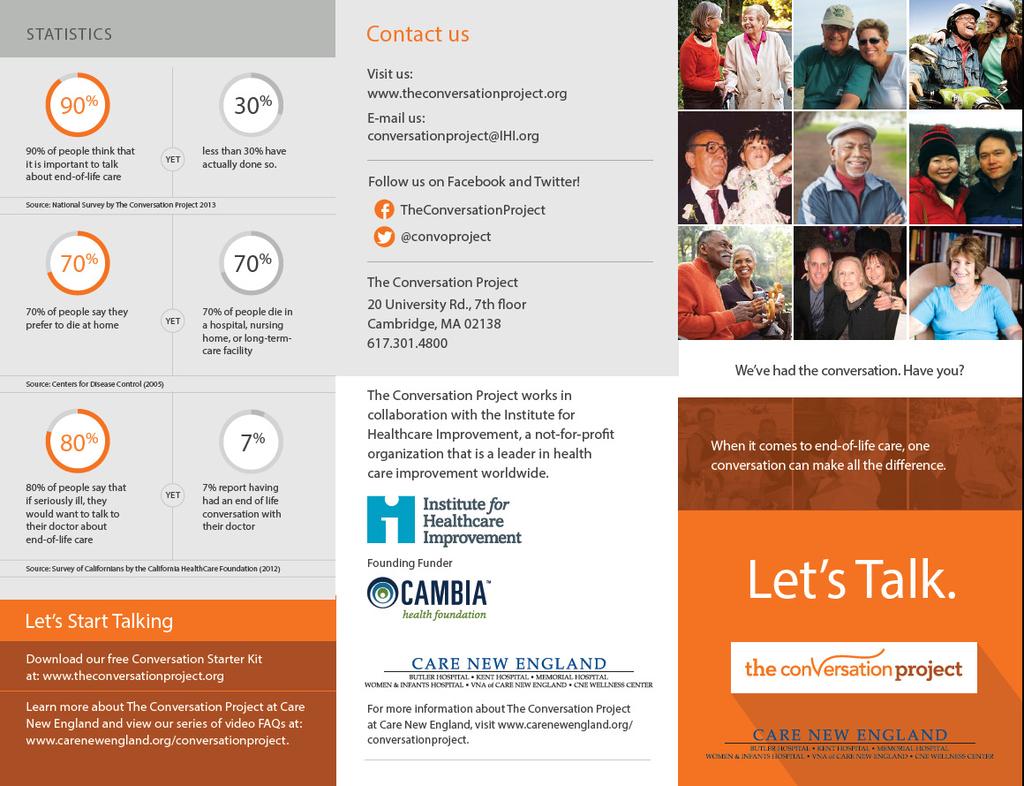
22 Background and goals 90% of people want to talk about their end-of-life care preferences <30% have actually done so with loved ones <10% have done so with their doctor Conversation goals when there is no serious illness Build trusting and respectful relationships Learn about the patient as a person Establish a surrogate decision maker Promote patient-surrogate-family conversations National Survey by The Conversation Project 2013 Survey of Californians by the California HealthCare Foundation 2012 Triggers for the conversation: the 5 D s Death in the family Moment of reflection Divorce Previously selected surrogate may no longer be valid Decade People and preferences change with time Decline would you be surprised if this patient became seriously ill or died? Diagnosis of serious illness Difficult decisions may be ahead 22
23 Starting the conversation Key is to normalize the conversation Try starting it after family history Can you tell me about the supports in your life? Who should speak for you if you cannot speak for yourself? Have you ever thought about your end-of-life wishes? or about the kind of care you d want if you got really sick someday? The conversation (continued) If they already have an advance directive (AD) May I see it? What does it say? If they do not have an AD Can I offer you some tools to start thinking about it? Conversation Project Starter Kit State durable power of attorney form Regardless of AD It is important that your surrogate know what your wishes are A lot can happen beyond what is written in your AD The Conversation can be more powerful than the paper Would it be ok if we talk about this at your next visit? Consider delegating follow up to another member of your team 23
24 Mrs. Smith Advanced Illness Since that visit, Ms. Smith did well for a few years, and then at age 71 developed a COPD exacerbation, which turned into a pneumonia with significant shortness of breath. She was admitted to the hospital and required an ICU stay for BiPAP. There was a disagreement between her children about what her wishes were. You wonder At this stage, what s the purpose of the conversation? How can I begin the conversation, document, and bill for it? Prognosis: recognizing serious illness Who has a serious illness or condition? eprognosis.ucsf.edu Clinical criteria Surprise question It s not just risk of death Incapacity, difficult treatment decisions, anticipated emergencies Identifying risk ahead of time gives us an opportunity to mitigate it Early conversations are an important form of practice for the future Who are your seriously ill patients? Have they engaged in the advance care planning process? Population health management systems triggering the conversation 24
25 Prognosis: recognizing serious illness Has the patient had more than two unplanned hospital admissions in the last twelve months? Yes No Does this patient have Advanced long term condition Yes No New diagnosis of a serious illness Yes No Both Yes No Does the PCP believe that by controlling the symptoms and adding support, we will keep this patient out of the hospital? Yes No Does the patient have multiple chronic conditions resulting in: Functional impairment Yes No Decrease ability to self feed Yes No Inability to walk independently. Yes No Need for more personal care at home Yes No Ambulance trip in the last six months? Yes No Difficult to Control Symptoms Yes No Non-Healing Wound Yes No Recurrent Infections Yes No Three or More Falls Yes No Nine of More Unique Medications Yes No Progressive weight loss Yes No Would you be surprised if this patient were alive in one year? Yes No If the 2 out of three answers are positive for questions 1-3 and there is at least 1 positive in question 4 the patient should be referred and evaluated to the advanced illness management team. Why have another Conversation? Conversation goals when there is a serious illness Continue to build trusting, respectful relationships Continue to learn more about the patient as a person Ensure a good understanding of diagnosis, prognosis, and treatment options Anticipate emergencies and make a plan when appropriate Promote patient-surrogate-family conversations 25
26 Starting the Conversation Talk about what matters most Can you tell me your understanding of what happened in the hospital? What was that like for you? How are you doing now? If surrogate decision making was needed, how was that? Identify the values that guided decision making, i.e. what mattered most Goals, hopes Fears, worries Tradeoffs Try using an RN or MSW to get at what matters most Ensure >50 % of time dedicated to patient, family talking* * Back et al, Compassionate silence in the patient-clinician encounter: a contemplative approach, J PalliatMed 2009 Suggested Language Align around hope, ask for permission We re all hoping things go well, but as you ve experienced, that doesn t always happen. Would it be ok to talk about a plan in case things don t go the way we d like? Ask if anyone else needs to be present Are the right family members/friends here? Explain potential emergencies, reflect on experiences I am worried that you might get sick again and that they might consider putting you on the breathing machine again Align around respect If you get sick again, it s important to me that we re certain we re respecting your wishes. Your family wasn t sure what your wishes were. Give them the gift of knowing what you want. 26
27 Handling difficult situations Patient/family is reluctant to talk about the serious illness Family disagree with patient s choices 53 Handling difficult situations Patient/family is reluctant to talk about the serious illness Ask why? How much information do you like to know about your medical problems? If you only want to know the basics, who can I talk with about the details? Hope for the best, but plan for the worst Ask permission to talk with their surrogate, loved ones, or another support system (e.g. clergy) and include them in the next conversation Family disagree with patient s choices Ask why? Try to understand what they see when they look at the patient Always focus on the patient try to get the patient to express their choices in front of the family and normalize their experience Build and strengthen relationships you may need to draw on them later 27
28 Mrs. Smith Approaching EOL Ms. Smith did well for a few years after your last conversation. She had a couple admissions for less severe COPD exacerbations. She was eventually placed on home oxygen, and then about 2 months ago her illness seemed to progress. She was no longer able to walk around the block as she had been able to, and now can only go to and from the bathroom before getting so short of breath that she has to stop and rest. A hospital social worker during her most recent admission, introduced her to the How to talk with your doctor kit. She read this and decided to come in to see you again. She s now 75 years old and starts the visit by telling you how tired she is. You and she talk more, and it becomes clear that she doesn t want to have to go back to the hospital if it isn t necessary. She really prefers to stay at home. Her daughter is with her again today. Consider your goals You wonder At this stage, what s the purpose of the conversation? How can I begin the conversation? How can I introduce palliative care, and help the patient make a transition to hospice when the time is right for her? How do I document and bill for the conversation? Conversation goals when there is an advanced serious illness Rely on the trusting, respectful relationships that were built Keep the focus on the patient as a person Ensure a good understanding of diagnosis, prognosis, and treatment options before introducing hospice Continue to hope for the best, but prepare for when things don t go well 28
29 Suggested Language You have been in and out of the hospital quite a bit, how has that been? How do you feel about your quality of life? Given everything that has happened, what are you hoping for? Unfortunately, we don t have any more treatments to help your lungs get better. It seems to me what matters most to you is to stay out of the hospital, control your symptoms at home and make the most of each day, and I think hospice is the best way of doing that. Would it be ok if I had one of the hospice nurses come to your home and speak with you about what they can offer? Handling Difficult Situations I still want everything done when curative treatments would be harmful and offer no benefit I want hospice but my family doesn t agree 29
30 Handling difficult situations I still want everything done when curative treatments would be harmful and offer no benefit Return to understanding, ask 1 st, don t tell 1 st Can you help me understand what everything means to you? Work from the foundation of trust and respect that you built Return to what matters most and reflect on prior experiences Make a recommendation consider Temel et al.* I want hospice but my family doesn't agree Hold a family meeting, begin by asking everyone s understanding Then make what matters most to the patient the focus Ask a palliative care specialist or hospice agency for help *Temel et al., Early palliative care for patients with metastatic non-small cell lung cancer. N Engl J Med 2010 Documenting the conversation Who was in the room What was discussed Understanding of illness Spiritual factors Reflections on family/personal losses Why making the decision they are making. Was advance directive offered/filled out Time spent (including start and end time) Follow up 30

31 Logistics & real world implementation System factors Will the documentation be easily available in the future? Is the documentation such that the next provider will know where to begin the next conversation? Do you have a way of managing different versions of the same information? What if a patient changes their surrogate? Will it be clear to the next provider who the right surrogate is? Which of your patients don t yet have a surrogate? Do you have a way of identifying your highest risk patients, identifying gaps, and tracking progress? How reliable are your processes? 31
, by the physician or other qualified health professional; first 30 minutes, face-to-face with the patient, family member(s) and/or surrogate) 99498 each additional 30 minutes")
32 Billing New Codes New advance care planning billing codes Advance care planning including the explanation and discussion of advance directives such as standard forms (with completion of such forms, when performed), by the physician or other qualified health professional; first 30 minutes, face-to-face with the patient, family member(s) and/or surrogate) each additional 30 minutes Note: we are sharing our best understanding of these codes at this time, please be sure to work with your local billing compliance expert 32
33 Billing If billing for medical management If based on medical decision making bill as you normally would Then also bill based on time for advance care planning conversation If based on time do not double count time If not billing for medical management Use if you exceed 15 minutes Use if you exceed 45 minutes Use if you exceed 75 minutes Incident to rules apply in the outpatient setting Billing provider performs an initial service, a non-billing team member (e.g. RN, SW) helps deliver part of the service, with ongoing direct supervision and involvement of the billing provider 65 Summary of billing guidance Recognize the many (non-billing) barriers to these conversations Time Skill (and comfort level) Competing priorities Consider the business case for the new codes Can you use them to carve out more time for encounters? How might non-billing providers fit in? Incident to rules in the outpatient setting Many unknowns CMS will be learning from how they are used Work with your local billing compliance expert(s) 66 33

34 Conclusions Make advance care planning a routinepart of annual visits to health care provider for everyone Educate all providers on the tools they need, and give them the comfort level to have these difficult conversations Anyone on the team can start this conversation Make a living treatment plan that evolves over time and reflects changes in patient s goals and condition Utilize the billing codes and system resources to communicate wishes across the silos Resources 34
35 Our Conversation Nurse Orientation Shadow multiple members of the team for one month See what we do the same and what we do differently Think about things like body language, non-verbal communication, appropriate use of touch Review The Conversation Project starter kit Practice conversations with a team member observing Until ready to undergo formal evaluation Attend weekly team meetings where we all give feedback on how to do better ( All Teach, All Learn ) Undergo formal evaluation Assessment tools CONVERSATION EVALUATION TOOL Task: 1. Re-affirm the patient s goals for future care 2. Discuss CPR/DNR orders Check all skills satisfactorily completed. Basic Interviewing Skills Introduction nurse introduced him/herself Comfort nurse put patient at comfort, ensured privacy Nurse assumed a comfortable interpersonal communication distance Nurse made appropriate eye contact Nurse s posture was open (was leaning forward, didn t cross arms over chest, etc.) Used language that was clear and understandable; no medical jargon Nurse was attentive to comments nodding head, used verbal cues ( yes, hmm, I see ) Nurse gave me opportunity to ask questions Nurse answered questions in a straightforward manner Nurse suggested a follow-up plan Appeared empathic (indicate by body posture, tone of voice, facial expressions and choice of words, that they care about the patient and have some sense of understanding of the impact of the bad news) Copyright 2003, The Medical College of Wisconsin, Inc. Palliative Care Programs 35
36 Assessment tools Assess the understanding of diagnosis and prognosis How are things going? What is your understanding of what has happened? What have the doctors told you about your condition? Tell me more Can you explain what you mean? Can you tell me what you are worried about? You said you were worried about going home. Tell me more Nurse clearly articulated the current status of the disease Explained why the illness is advanced Reviewed treatments that have been tried Explained the probable course of the advanced illness Clarified the treatment options as focus changed from cure to comfort and quality of remaining life Goal: Therapeutic communication Nurse asked patient to articulate personal goals: What matters most? Summary Goal Setting/DNR Skills Nurse asked patient to articulate personal goals Nurse discussed the use of CPR within the context of the disease, and prognosis Nurse made a clear recommendation regarding CPR/no-CPR Summary Copyright 2003, The Medical College of Wisconsin, Inc. Palliative Care Programs Tools for teaching and training about conversation skills Download the app on itunes for 2.99 ihi.org/conversationproject TheConversationProject.org 36


37 Member based organization with membership fee Fantastic resources for all aspects of palliative care CME/CEU courses Pain management Communication skills Palliative care across settings Getting leadership support Gives you sample patient statements and asks for your response $2.99 app for the iphone Can review before a difficult conversation or debrief after Can choose to focus on specific skills Detailed advice If unsure what patient is feeling ask- What is going through your mind? Notice and respond to emotion A moment of silence helps Allows you to watch an expert 37
38 IHI Open School The IHI Open School brings you essential training and tools in an online, educational community to help you and your team deliver excellent, safe care. When you engage with the Open School courses and Chapters, you join more than 250,000 learners from universities, organizations, and health systems around the world in building core skills in improvement, safety, and leadership. There is a free course available that is related to today s topic: ihi.org/conversationproject Great mix of video and text Free CME/CEU! You must be a registered IHI.org user. Focus on why this is so important Focus on engaging with your own family The Conversation Project starter kit TheConversationProject.org 38




39 39
Advance Care Planning Communication Guide: Overview
 Advance Care Planning Communication Guide: Overview The INTERACT Advance Care Planning Communication Guide is designed to assist health professionals who work in Nursing Facilities to initiate and carry
Advance Care Planning Communication Guide: Overview The INTERACT Advance Care Planning Communication Guide is designed to assist health professionals who work in Nursing Facilities to initiate and carry
When and How to Introduce Palliative Care
 When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
When and How to Introduce Palliative Care Phil Rodgers, MD FAAHPM Associate Professor, Departments of Family Medicine and Internal Medicine Associate Director for Clinical Services, Adult Palliative Medicine
POLST Cue Card. If you die a natural death, would you want us to try CPR? If yes Requires Full Treatment in Section B. (Ask about Ventilator Trial)
") POLST Cue Card It s important to talk about your health and your wishes for medical care if you got really sick. We talk about this with everyone with serious illness. Your doctor will review what we talk
POLST Cue Card It s important to talk about your health and your wishes for medical care if you got really sick. We talk about this with everyone with serious illness. Your doctor will review what we talk
The POLST Conversation POLST Script
 The POLST Conversation POLST Script The POLST Script provides detailed information in order to develop comfort and competence when facilitating a POLST conversation. The POLST conversation utilizes realistic
The POLST Conversation POLST Script The POLST Script provides detailed information in order to develop comfort and competence when facilitating a POLST conversation. The POLST conversation utilizes realistic
Becoming a Conversation Ready Organization
 May 23, 2017 Today s presenters have nothing to disclose Becoming a Conversation Ready Organization Session 1: The Conversation Project Kate DeBartolo Kelly McCutcheon Adams Senior Project Manager Angela
May 23, 2017 Today s presenters have nothing to disclose Becoming a Conversation Ready Organization Session 1: The Conversation Project Kate DeBartolo Kelly McCutcheon Adams Senior Project Manager Angela
POLST Discussions Doing it Better. Clinical Update in Geriatric Medicine. Judith S. Black, MD, MHA. POLST Overview. Faculty Disclosure PART I
 Faculty Disclosure POLST Discussions Doing it Better Clinical Update in Geriatric Medicine Dr. Black discloses that she is employed by Allegheny Health Network and is an executive committee member of the
Faculty Disclosure POLST Discussions Doing it Better Clinical Update in Geriatric Medicine Dr. Black discloses that she is employed by Allegheny Health Network and is an executive committee member of the
ADVANCE CARE PLANNING: WHY, HOW, AND IMPACT ON THE TRIPLE AIM
 ADVANCE CARE PLANNING: WHY, HOW, AND IMPACT ON THE TRIPLE AIM John Fox MD, MHA AVP Medical Affairs, Priority Health MCM Board Member Carol Robinson DNP, MS, BSN, RN, CHPN Community Coordinator, MCM OBJECTIVES
ADVANCE CARE PLANNING: WHY, HOW, AND IMPACT ON THE TRIPLE AIM John Fox MD, MHA AVP Medical Affairs, Priority Health MCM Board Member Carol Robinson DNP, MS, BSN, RN, CHPN Community Coordinator, MCM OBJECTIVES
Advance Care Planning Conversations and Goals of Care Discussions: Understanding the Difference
 March 16, 2017 Advance Care Planning Conversations and Goals of Care Discussions: Understanding the Difference Jeff Myers MD, MSEd, CCFP(PC) Nadia Incardona MD, MHSc, CCFP(EM) WHY this is timely JAMA,
March 16, 2017 Advance Care Planning Conversations and Goals of Care Discussions: Understanding the Difference Jeff Myers MD, MSEd, CCFP(PC) Nadia Incardona MD, MHSc, CCFP(EM) WHY this is timely JAMA,
Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care
 Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care July 24, 2012 Presented by: Cindy Campbell RN, BSN Associate Director, Operational Consulting Fazzi Associates
Having the End of Life Conversation: Practical Concepts for Advocacy Within the Continuum of Care July 24, 2012 Presented by: Cindy Campbell RN, BSN Associate Director, Operational Consulting Fazzi Associates
Station Name: Mrs. Smith. Issue: Transitioning to comfort measures only (CMO)
") Station Name: Mrs. Smith Issue: Transitioning to comfort measures only (CMO) Presenting Situation: The physician will meet with Mrs. Smith s children to update them on her condition and determine the future
Station Name: Mrs. Smith Issue: Transitioning to comfort measures only (CMO) Presenting Situation: The physician will meet with Mrs. Smith s children to update them on her condition and determine the future
Supportive Care Consultation
 WVUH Ethics Committee & Ethics Consultation Supportive Care Consultation Carl Grey, MD Outline/ Objectives Provide an example of ethics consultation Recognize the most common reasons for ethics consultation
WVUH Ethics Committee & Ethics Consultation Supportive Care Consultation Carl Grey, MD Outline/ Objectives Provide an example of ethics consultation Recognize the most common reasons for ethics consultation
Advance Directive. A step-by-step guide to help you make shared health care decisions for the future. California edition
 Advance Directive A step-by-step guide to help you make shared health care decisions for the future California edition Advance Directive Instructions for Patients TALK TO YOUR LOVED ONES This is important.
Advance Directive A step-by-step guide to help you make shared health care decisions for the future California edition Advance Directive Instructions for Patients TALK TO YOUR LOVED ONES This is important.
ILLINOIS Advance Directive Planning for Important Health Care Decisions
 ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
IPMG Professional Development Workshop Medicaid Waiver and Hospice Partnerships August 19, 2016
 8/19/2016 IPMG Professional Development Workshop Medicaid Waiver and Hospice Partnerships August 19, 2016 Susan Campbell, Community Liaison Crystal Godfrey, RN, BSN, Director of Clinical Services Premier
8/19/2016 IPMG Professional Development Workshop Medicaid Waiver and Hospice Partnerships August 19, 2016 Susan Campbell, Community Liaison Crystal Godfrey, RN, BSN, Director of Clinical Services Premier
Quality of Life Conversation On Advance Care Planning
 Quality of Life Conversation On Advance Care Planning Information Packet Page 1 About the Integrated Healthcare Association The nonprofit Integrated Healthcare Association (IHA) convenes diverse stakeholders,
Quality of Life Conversation On Advance Care Planning Information Packet Page 1 About the Integrated Healthcare Association The nonprofit Integrated Healthcare Association (IHA) convenes diverse stakeholders,
Becoming a Conversation Ready Organization
 June 20, 2017 These presenters have nothing to disclose Becoming a Conversation Ready Organization Session 3 Steward: Achieving the reliability of allergy information Lauge Sokol-Hessner, MD Kelly McCutcheon
June 20, 2017 These presenters have nothing to disclose Becoming a Conversation Ready Organization Session 3 Steward: Achieving the reliability of allergy information Lauge Sokol-Hessner, MD Kelly McCutcheon
9: Advance care planning and advance decisions
 9: Advance care planning and advance decisions This section explains how advance care planning and Advance Decisions to Refuse Treatment (ADRT) can support your future care. The following information is
9: Advance care planning and advance decisions This section explains how advance care planning and Advance Decisions to Refuse Treatment (ADRT) can support your future care. The following information is
CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada.
 CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada. For more information about advance care planning, please visit
CHPCA appreciates and thanks our funding partner GlaxoSmithKline for their unrestricted funding support for Advance Care Planning in Canada. For more information about advance care planning, please visit
Advance Care Planning: Goals of Care - Calgary Zone
 Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
MY VOICE (STANDARD FORM)
") MY VOICE (STANDARD FORM) a workbook and personal directive for advance care planning WHAT IS ADVANCE CARE PLANNING? Advance care planning is a process for you to: think about what is important to you when
MY VOICE (STANDARD FORM) a workbook and personal directive for advance care planning WHAT IS ADVANCE CARE PLANNING? Advance care planning is a process for you to: think about what is important to you when
PENNSYLVANIA Advance Directive Planning for Important Health Care Decisions
 PENNSYLVANIA Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
PENNSYLVANIA Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
Wow ADVANCE CARE PLANNING The continued Frontier. Kathryn Borgenicht, M.D. Linda Bierbach, CNP
 Wow ADVANCE CARE PLANNING The continued Frontier Kathryn Borgenicht, M.D. Linda Bierbach, CNP Objectives what we want to accomplish Describe the history of advance care planning Discuss what patients/families
Wow ADVANCE CARE PLANNING The continued Frontier Kathryn Borgenicht, M.D. Linda Bierbach, CNP Objectives what we want to accomplish Describe the history of advance care planning Discuss what patients/families
Independent investigation into the death of Mr Stephen Keogh a prisoner at HMP Manchester on 24 April 2016
 Independent investigation into the death of Mr Stephen Keogh a prisoner at HMP Manchester on 24 April 2016 Crown copyright 2015 This publication is licensed under the terms of the Open Government Licence
Independent investigation into the death of Mr Stephen Keogh a prisoner at HMP Manchester on 24 April 2016 Crown copyright 2015 This publication is licensed under the terms of the Open Government Licence
peace of mind. Advance care planning document and instructions are enclosed for:
 ACP Honoring Choices Booklet_Self Cover 16 PAGES 2-COLOR 01.12.17.qxd_Layout 1 2017-01-12 11:09 Page 3 I choose peace of mind. Take time to plan ahead now so future health care challenges don t create
ACP Honoring Choices Booklet_Self Cover 16 PAGES 2-COLOR 01.12.17.qxd_Layout 1 2017-01-12 11:09 Page 3 I choose peace of mind. Take time to plan ahead now so future health care challenges don t create
Last Name: First Name: Advance Directive including Power of Attorney for Health Care
 Patient Medical Record Number: Or Label Advance Directive including Power of Attorney for Health Care Overview This legal document meets the requirements for Wisconsin.* It lets you Name another person
Patient Medical Record Number: Or Label Advance Directive including Power of Attorney for Health Care Overview This legal document meets the requirements for Wisconsin.* It lets you Name another person
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces.
 End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
End of Life Terminology The definitions below applies within the province of Ontario, terms may be used or defined differently in other provinces. Terms Definitions End of Life Care To assist persons who
Your Guide to Advance Directives
 Starting Points: Your Guide to Advance Directives Values Statements Healthcare Directives Durable Power of Attorney for Healthcare 1 2 Advances in medicine are helping people to live longer than ever before.
Starting Points: Your Guide to Advance Directives Values Statements Healthcare Directives Durable Power of Attorney for Healthcare 1 2 Advances in medicine are helping people to live longer than ever before.
Information for Staff. Guidelines for Communicating Bad News with Patients and their Families
 Information for Staff Guidelines for Communicating Bad News with Patients and their Families March 2006 COMMUNICATING BAD NEWS WITH PATIENTS AND THEIR FAMILIES INTRODUCTION As health care professionals
Information for Staff Guidelines for Communicating Bad News with Patients and their Families March 2006 COMMUNICATING BAD NEWS WITH PATIENTS AND THEIR FAMILIES INTRODUCTION As health care professionals
Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee
 Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee What is Advance Care Planning (ACP)? Understanding/clarifying
Cynthia Ann LaSala, MS, RN Nursing Practice Specialist Phillips 20 Medicine Advisor, Patient Care Services Ethics in Clinical Practice Committee What is Advance Care Planning (ACP)? Understanding/clarifying
Advance Health Care Planning: Making Your Wishes Known. MC rev0813
 Advance Health Care Planning: Making Your Wishes Known MC2107-14rev0813 What s Inside Why Health Care Planning Is Important... 2 What You Can Do... 4 Work through the advance health care planning process...
Advance Health Care Planning: Making Your Wishes Known MC2107-14rev0813 What s Inside Why Health Care Planning Is Important... 2 What You Can Do... 4 Work through the advance health care planning process...
HealthStream Regulatory Script
 HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
munsonhealthcare.org/acp
 Advance Care Planning Workbook Making Your Medical Wishes Known Advance Care Planning Workbook 1 munsonhealthcare.org/acp Making Your Medical Wishes Known At any age, a medical crisis could leave someone
Advance Care Planning Workbook Making Your Medical Wishes Known Advance Care Planning Workbook 1 munsonhealthcare.org/acp Making Your Medical Wishes Known At any age, a medical crisis could leave someone
Dear Family Caregiver, Yes, you.
 Dear Family Caregiver, Yes, you. If you re wondering whether the term caregiver applies to you, it probably does. A caregiver is anyone who helps an aging, ill, or disabled family member or friend manage
Dear Family Caregiver, Yes, you. If you re wondering whether the term caregiver applies to you, it probably does. A caregiver is anyone who helps an aging, ill, or disabled family member or friend manage
LIFE CARE planning. Advance Health Care Directive. my values, my choices, my care OREGON. kp.org/lifecareplan
 Advance Health Care Directive OREGON LIFE CARE planning kp.org/lifecareplan 60418810_NW All plans offered and underwritten by Kaiser Foundation Health Plan of the Northwest. 500 NE Multnomah St., Suite
Advance Health Care Directive OREGON LIFE CARE planning kp.org/lifecareplan 60418810_NW All plans offered and underwritten by Kaiser Foundation Health Plan of the Northwest. 500 NE Multnomah St., Suite
Last Name: First Name: Advance Directive. including Power of Attorney for Health Care
 Overview Patient Medical Record Number: Or Label Advance Directive including Power of Attorney for Health Care This legal document meets the requirements for Wisconsin.* It lets you Name another person
Overview Patient Medical Record Number: Or Label Advance Directive including Power of Attorney for Health Care This legal document meets the requirements for Wisconsin.* It lets you Name another person
Making Your Wishes Known With the Help of the Five Wishes Document
 Making Your Wishes Known With the Help of the Five Wishes Document Lora Rhodes, MSW, LSW Oncology Social Worker Department of Medical Oncology LBBC: Annual Conference for Women living with Metastatic Breast
Making Your Wishes Known With the Help of the Five Wishes Document Lora Rhodes, MSW, LSW Oncology Social Worker Department of Medical Oncology LBBC: Annual Conference for Women living with Metastatic Breast
Health Care Directive
 MINNESOTA PATIENT EDUCATION Health Care Directive Making Your Health Care Choices Known My Health Care Directive My health care directive was created to guide my health care agent and family, friends or
MINNESOTA PATIENT EDUCATION Health Care Directive Making Your Health Care Choices Known My Health Care Directive My health care directive was created to guide my health care agent and family, friends or
Living Wills and Other Advance Directives
 UW MEDICINE PATIENT EDUCATION Living Wills and Other Advance Directives Writing down your choices for health care for times when you cannot speak for yourself This handout gives basic information about
UW MEDICINE PATIENT EDUCATION Living Wills and Other Advance Directives Writing down your choices for health care for times when you cannot speak for yourself This handout gives basic information about
Your life and your choices: plan ahead
 Your life and your choices: plan ahead About this booklet About this booklet This booklet is about some of the ways you can plan ahead and make choices about your future care if you live in Northern Ireland.
Your life and your choices: plan ahead About this booklet About this booklet This booklet is about some of the ways you can plan ahead and make choices about your future care if you live in Northern Ireland.
Convening Difficult Conversations
 Convening Difficult Conversations October 27, 2017 Presenter-Lores Vlaminck, MA, BSN, RN, CHPN Grandmother of 10 wonderful grandkids! Nurse Consultant for: Hospice Palliative Care Assisted Living Home
Convening Difficult Conversations October 27, 2017 Presenter-Lores Vlaminck, MA, BSN, RN, CHPN Grandmother of 10 wonderful grandkids! Nurse Consultant for: Hospice Palliative Care Assisted Living Home
Deciding About. Health Care A GUIDE FOR PATIENTS AND FAMILIES. New York State Department of Health
 Deciding About Health Care A GUIDE FOR PATIENTS AND FAMILIES New York State Department of Health 2 Introduction Who should read this guide? This guide is for New York State patients and for those who will
Deciding About Health Care A GUIDE FOR PATIENTS AND FAMILIES New York State Department of Health 2 Introduction Who should read this guide? This guide is for New York State patients and for those who will
For more information and additional resources go to Name:
 Durable Power of Attorney for Health Care & Health Care Directive Documents are legally valid in Alaska, California, Idaho, Montana, and Washington. What is advance care planning? Advance care planning
Durable Power of Attorney for Health Care & Health Care Directive Documents are legally valid in Alaska, California, Idaho, Montana, and Washington. What is advance care planning? Advance care planning
TO HELP EASE DECISION MAKING IN THE FUTURE ADVANCE CARE PLANNING TOOLKIT
 TO HELP EASE DECISION MAKING IN THE FUTURE ADVANCE CARE PLANNING TOOLKIT Advance Care Planning Toolkit Your health care decisions are important. Providing Patient Centered Care is the guiding principle
TO HELP EASE DECISION MAKING IN THE FUTURE ADVANCE CARE PLANNING TOOLKIT Advance Care Planning Toolkit Your health care decisions are important. Providing Patient Centered Care is the guiding principle
An individual may have one type of advance directive or may have both. They may also be combined in a single document.
 Advance Directives History In 1991, the Patient Self-Determination Act became a federal law. The act was signed into law to help ensure that patients preferences about medical treatment would be followed
Advance Directives History In 1991, the Patient Self-Determination Act became a federal law. The act was signed into law to help ensure that patients preferences about medical treatment would be followed
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Revised 2/27/17. POLST For General Providers
 Revised 2/27/17 POLST For General Providers Permission to Use This slide presentation may be used without permission. To promote consistency across the state, the slides may not be altered. You may freely
Revised 2/27/17 POLST For General Providers Permission to Use This slide presentation may be used without permission. To promote consistency across the state, the slides may not be altered. You may freely
Module 1 Program Description
 Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Cancer and Advance Care Planning. Tips for Oncology Professionals
 Cancer and Advance Care Planning Tips for Oncology Professionals Each year, more than 74,000 Canadians die with cancer. When To Have the Discussion...5 Questions to Ask...6 Steps in Initiating and Having
Cancer and Advance Care Planning Tips for Oncology Professionals Each year, more than 74,000 Canadians die with cancer. When To Have the Discussion...5 Questions to Ask...6 Steps in Initiating and Having
Objectives. Integrating Palliative Care Principles into Critical Care Nursing
 1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
1 Integrating Palliative Care Principles into Critical Care Nursing It s the Caring, Compassionate, Holistic, Patient and Family Centered, Better Communication, Keeping my patient comfortable amidst the
S A M P L E. About CPR. Hard Choices. Logo A GUIDE FOR PATIENTS AND FAMILIES
 Hard Choices About CPR A GUIDE FOR PATIENTS AND FAMILIES Logo 2016 by Quality of Life Publishing Co. Hard Choices About CPR: A Guide for Patients and Families adapted with permission from: Dunn, Hank.
Hard Choices About CPR A GUIDE FOR PATIENTS AND FAMILIES Logo 2016 by Quality of Life Publishing Co. Hard Choices About CPR: A Guide for Patients and Families adapted with permission from: Dunn, Hank.
End of Life PSP Module. Case Study: Mr. James Lee
 Case Study: Mr. James Lee Mr. James Lee is a 74 yr old retired electrician. He is married to Mary with two children in their 30 s. They have been in Canada for 35 years and are fluent in English and Cantonese.
Case Study: Mr. James Lee Mr. James Lee is a 74 yr old retired electrician. He is married to Mary with two children in their 30 s. They have been in Canada for 35 years and are fluent in English and Cantonese.
Advance Directives The Patient s Right To Decide CH Oct. 2013
 Advance Directives The Patient s Right To Decide CH80850040 Oct. 2013 Advance Directives Your Right To Make Health Care Decisions Under The Law In Tennessee Tennessee and federal law give every competent
Advance Directives The Patient s Right To Decide CH80850040 Oct. 2013 Advance Directives Your Right To Make Health Care Decisions Under The Law In Tennessee Tennessee and federal law give every competent
My Voice - My Choice
 My Voice - My Choice My Advance Directive Table of Contents Introduction... 2 Words You Need to Know... 3 Legal Document... 4 Helpful Information about your Advance Directive... 10 What makes your life
My Voice - My Choice My Advance Directive Table of Contents Introduction... 2 Words You Need to Know... 3 Legal Document... 4 Helpful Information about your Advance Directive... 10 What makes your life
Responding to Patients and Families that Want Everything Done
 Responding to Patients and Families that Want Everything Done Steven Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative
Responding to Patients and Families that Want Everything Done Steven Pantilat, MD Professor of Clinical Medicine Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care Director, Palliative
Advance Care Planning Information
 Advance Care Planning Information Booklet Planning in Advance for Future Healthcare Choices www.yourhealthyourchoice.org Life Choices Imagine You are in an intensive care unit of a hospital. Without warning,
Advance Care Planning Information Booklet Planning in Advance for Future Healthcare Choices www.yourhealthyourchoice.org Life Choices Imagine You are in an intensive care unit of a hospital. Without warning,
Appendix: Assessments from Coping with Cancer
 Appendix: Assessments from Coping with Cancer Primary Independent Variable of Interest (assessed at baseline with medical chart review and confirmed with clinician) 1. What treatments is the patient currently
Appendix: Assessments from Coping with Cancer Primary Independent Variable of Interest (assessed at baseline with medical chart review and confirmed with clinician) 1. What treatments is the patient currently
ALABAMA Advance Directive Planning for Important Health Care Decisions
 ALABAMA Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CARING CONNECTIONS Caring Connections,
ALABAMA Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CARING CONNECTIONS Caring Connections,
Federal Policy Agenda / 2016 & Beyond
 Federal Policy Agenda / 2016 & Beyond Compassion & Choices is the leading national nonprofit organization dedicated to improving care and expanding choice for people with advanced illness, and nearing
Federal Policy Agenda / 2016 & Beyond Compassion & Choices is the leading national nonprofit organization dedicated to improving care and expanding choice for people with advanced illness, and nearing
GEORGIA Advance Directive Planning for Important Health Care Decisions
 GEORGIA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Organization
GEORGIA Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Organization
Facing Serious Illness: Make Your Wishes Known to your Health Care Professional
 Facing Serious Illness: Make Your Wishes Known to your Health Care Professional Your Guide to the Oregon POLST Program Physician Orders for Life-Sustaining Treatment Revised: February 19, 2015 This material
Facing Serious Illness: Make Your Wishes Known to your Health Care Professional Your Guide to the Oregon POLST Program Physician Orders for Life-Sustaining Treatment Revised: February 19, 2015 This material
Advance Care Planning and Goals of Care
 Advance Care Planning and Goals of Care A Guide For Patients with A Serious Illness and Their Families Nova Scotia Edition www.nshpca.ca Receiving a diagnosis of a serious illness can be life altering.
Advance Care Planning and Goals of Care A Guide For Patients with A Serious Illness and Their Families Nova Scotia Edition www.nshpca.ca Receiving a diagnosis of a serious illness can be life altering.
Hospice Care For Dementia and Alzheimers Patients
 Hospice Care For Dementia and Alzheimers Patients Facing the end of life (as it has been known), is a very individual experience. The physical ailments are also experienced uniquely, even though the conditions
Hospice Care For Dementia and Alzheimers Patients Facing the end of life (as it has been known), is a very individual experience. The physical ailments are also experienced uniquely, even though the conditions
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Advanced Care Planning and Advanced Directives: Our Roles March 27, 2017
 Advanced Care Planning and Advanced Directives: Our Roles March 27, 2017 2017 NPSS Asheville, NC Overview History of Advanced Directives Importance of Advanced Care Planning for Quality care Our Role in
Advanced Care Planning and Advanced Directives: Our Roles March 27, 2017 2017 NPSS Asheville, NC Overview History of Advanced Directives Importance of Advanced Care Planning for Quality care Our Role in
Building a Person-Centered ADVANCE CARE Planning Program. Barbara J. Smith, LBSW, MS, CHC, NHA Carolyn Stramecki, MHSA, CPHQ
 Building a Person-Centered ADVANCE CARE Planning Program Barbara J. Smith, LBSW, MS, CHC, NHA Carolyn Stramecki, MHSA, CPHQ Objectives Describe components of an advance directive document required to meet
Building a Person-Centered ADVANCE CARE Planning Program Barbara J. Smith, LBSW, MS, CHC, NHA Carolyn Stramecki, MHSA, CPHQ Objectives Describe components of an advance directive document required to meet
Advance Directive for Health Care
 Advance Directive for Health Care respecting your right to: Choose Your Healthcare Agent Choose the Authority Given to Your Healthcare Agent Choose Your Preferences Related to Treatment & Care Printed
Advance Directive for Health Care respecting your right to: Choose Your Healthcare Agent Choose the Authority Given to Your Healthcare Agent Choose Your Preferences Related to Treatment & Care Printed
Advance Care Planning Workbook Ontario Edition
 Advance Care Planning Workbook Ontario Edition Speak Up Ontario c/o Hospice Palliative Care Ontario, 2 Carlton Street, Suite 808, Toronto, Ontario M5B 1J3 Who will speak for you? Start the conversation.
Advance Care Planning Workbook Ontario Edition Speak Up Ontario c/o Hospice Palliative Care Ontario, 2 Carlton Street, Suite 808, Toronto, Ontario M5B 1J3 Who will speak for you? Start the conversation.
Health Care Directive
 Health Care Directive Overview Adults with decision-making capacity have the right to make choices about their health care. No treatments may be given to someone who does not want them. The attached Durable
Health Care Directive Overview Adults with decision-making capacity have the right to make choices about their health care. No treatments may be given to someone who does not want them. The attached Durable
Advance Care Planning (and more)
") Advance Care Planning (and more) Tessa & Josie Karl Steinberg, MD, CMD,HMDC @karlsteinberg, karlsteinberg@mail.com WWW.COALITIONCCC.ORG Advance Care Planning ACP is a process that unfolds over a life span
Advance Care Planning (and more) Tessa & Josie Karl Steinberg, MD, CMD,HMDC @karlsteinberg, karlsteinberg@mail.com WWW.COALITIONCCC.ORG Advance Care Planning ACP is a process that unfolds over a life span
Toolbox Talks. Access
 Access The detail of what the Healthcare Charter says in relation to what service users can expect and what they can do to help in relation to this theme is outlined overleaf. 1. How do you ensure that
Access The detail of what the Healthcare Charter says in relation to what service users can expect and what they can do to help in relation to this theme is outlined overleaf. 1. How do you ensure that
Analytics in Action. Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY
 Analytics in Action Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY Imagine an 82-year-old gentleman walks in to your emergency department. He presents with a productive cough and
Analytics in Action Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY Imagine an 82-year-old gentleman walks in to your emergency department. He presents with a productive cough and
LIFE CARE planning. eadvance Health Care Directive. kp.org/lifecareplan. my values, my choices, my care
 eadvance Health Care Directive LIFE CARE planning my values, my choices, my care kp.org/lifecareplan 60262511_14_LifeCarePlanningBookletUPDATE.indd 1 Introduction This Advance Health Care Directive allows
eadvance Health Care Directive LIFE CARE planning my values, my choices, my care kp.org/lifecareplan 60262511_14_LifeCarePlanningBookletUPDATE.indd 1 Introduction This Advance Health Care Directive allows
MY ADVANCE DIRECTIVE
 VERSION 09/28/17 MY ADVANCE DIRECTIVE INTRODUCTION This document expresses my preferences about my medical care if I cannot communicate my wishes or make my own health care decisions. I want my family,
VERSION 09/28/17 MY ADVANCE DIRECTIVE INTRODUCTION This document expresses my preferences about my medical care if I cannot communicate my wishes or make my own health care decisions. I want my family,
Vignette Overviews To Be Used in Conjunction with Various ELNEC Modules
 Vignette Overviews To Be Used in Conjunction with Various ELNEC Modules These vignettes have been developed to assist you in teaching various communication skills for participants attending an ELNEC course.
Vignette Overviews To Be Used in Conjunction with Various ELNEC Modules These vignettes have been developed to assist you in teaching various communication skills for participants attending an ELNEC course.
ALLINA HOME & COMMUNITY SERVICES ALLINA HEALTH. Advance Care Planning. Discussion guide. Discussion Guide. Advance care planning
 ALLINA HOME & COMMUNITY SERVICES ALLINA HEALTH Advance Care Planning Discussion guide Discussion Guide Advance care planning Advance care planning Any of us could think of a time when we might be too sick
ALLINA HOME & COMMUNITY SERVICES ALLINA HEALTH Advance Care Planning Discussion guide Discussion Guide Advance care planning Advance care planning Any of us could think of a time when we might be too sick
Planning in Advance for Future Health Care Choices Advance Care Planning Information & Guide
 Honoring Choices Virginia Planning in Advance for Future Health Care Choices Advance Care Planning Information & Guide Honoring Choices Virginia Imagine You are in an intensive care unit of a hospital.
Honoring Choices Virginia Planning in Advance for Future Health Care Choices Advance Care Planning Information & Guide Honoring Choices Virginia Imagine You are in an intensive care unit of a hospital.
E-Learning Module B: Introduction to Hospice Palliative Care
 E-Learning Module B: Introduction to Hospice Palliative Care This Module requires the learner to have read Chapter 2 of the Fundamentals Program Guide and the other required readings associated with the
E-Learning Module B: Introduction to Hospice Palliative Care This Module requires the learner to have read Chapter 2 of the Fundamentals Program Guide and the other required readings associated with the
Hospice 101. Janet Montgomery, BSN, MBA Chief Marketing Officer, Hospice of Cincinnati
 Hospice 101 Janet Montgomery, BSN, MBA Chief Marketing Officer, Hospice of Cincinnati Hospice of Cincinnati Hospice of Cincinnati creates the best possible and most meaningful EOL experience for all who
Hospice 101 Janet Montgomery, BSN, MBA Chief Marketing Officer, Hospice of Cincinnati Hospice of Cincinnati Hospice of Cincinnati creates the best possible and most meaningful EOL experience for all who
YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE
 YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE Communicating Your Health Care Choices In 1990, Congress passed the Patient Self-Determination Introduction Act. It requires
YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE YOUR RIGHT TO DECIDE Communicating Your Health Care Choices In 1990, Congress passed the Patient Self-Determination Introduction Act. It requires
MY CHOICES. Information on: Advance Care Directive Living Will POLST Orders
 MY CHOICES Information on: Advance Care Directive Living Will POLST Orders My Choices Adults have the right to accept or refuse medical care. As long as you can make health care decisions for yourself,
MY CHOICES Information on: Advance Care Directive Living Will POLST Orders My Choices Adults have the right to accept or refuse medical care. As long as you can make health care decisions for yourself,
NoCVA Preventing Avoidable Readmissions. Moving Beyond the Basics March 27, 2014
 NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
POLST: What s New and How Can We Do Better? Pam Hiransomboon-Vogel, DNP, FNP-BC, ACHPN
 POLST: What s New and How Can We Do Better? Pam Hiransomboon-Vogel, DNP, FNP-BC, ACHPN The OHSU Center for Ethics in Health Care and POLST Program, have no relevant financial relationships to disclose
POLST: What s New and How Can We Do Better? Pam Hiransomboon-Vogel, DNP, FNP-BC, ACHPN The OHSU Center for Ethics in Health Care and POLST Program, have no relevant financial relationships to disclose
10/3/2016 PALLIATIVE CARE WHAT IS THE DEFINITION OF PALLIATIVE CARE DEFINITION. What, Who, Where and When
 PALLIATIVE CARE What, Who, Where and When Mary Grant, RN, MS ANP Connections Nurse Practitioner Palliative Care Program Oregon Region WHAT IS THE DEFINITION OF PALLIATIVE CARE DEFINITION The Center for
PALLIATIVE CARE What, Who, Where and When Mary Grant, RN, MS ANP Connections Nurse Practitioner Palliative Care Program Oregon Region WHAT IS THE DEFINITION OF PALLIATIVE CARE DEFINITION The Center for
Health Care Directive
 Health Care Directive Overview Adults with decision-making capacity have the right to make choices about their health care. No treatments may be given to someone who does not want them. The attached Durable
Health Care Directive Overview Adults with decision-making capacity have the right to make choices about their health care. No treatments may be given to someone who does not want them. The attached Durable
YOUR CARE, YOUR CHOICES. Advance Care Planning Conversation Guide
 YOUR CARE, YOUR CHOICES Advance Care Planning Conversation Guide Table of Contents What is Advance Care Planning?... 1 Our Stories... 2-4 What is an Advance Health Care Directive?....5 What is a Health
YOUR CARE, YOUR CHOICES Advance Care Planning Conversation Guide Table of Contents What is Advance Care Planning?... 1 Our Stories... 2-4 What is an Advance Health Care Directive?....5 What is a Health
National Patient Experience Survey Mater Misericordiae University Hospital.
 National Patient Experience Survey 2017 Mater Misericordiae University Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017,
National Patient Experience Survey 2017 Mater Misericordiae University Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017,
Thank you for your interest in completing an Advance Directive.
 Advance Directives Thank you for your interest in completing an Advance Directive. Writing an Advance Directive is an opportunity to direct your future health needs in advance of an illness or crisis.
Advance Directives Thank you for your interest in completing an Advance Directive. Writing an Advance Directive is an opportunity to direct your future health needs in advance of an illness or crisis.
MARYLAND Advance Directive Planning for Important Healthcare Decisions
 MARYLAND Advance Directive Planning for Important Healthcare Decisions Caring Info 1731 King St, Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Info, a program of the National Organization
MARYLAND Advance Directive Planning for Important Healthcare Decisions Caring Info 1731 King St, Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Info, a program of the National Organization
MISSOURI Advance Directive Planning for Important Healthcare Decisions
 MISSOURI Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of
MISSOURI Advance Directive Planning for Important Healthcare Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program of
Hospice Residences Rev. May 28, 2014 R-4. Dame Cicely Saunders (1976) Founder of modern hospice movement. Design:
 Founder of modern hospice movement. Design:") Hospice Residences w w w. f r a s e r h e a l t h. c a in Fraser Health Dame Cicely Saunders (1976) Founder of modern hospice movement 280119 Rev. May 28, 2014 R-4 Design: www.kochink.com You matter because
Hospice Residences w w w. f r a s e r h e a l t h. c a in Fraser Health Dame Cicely Saunders (1976) Founder of modern hospice movement 280119 Rev. May 28, 2014 R-4 Design: www.kochink.com You matter because
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Advance Health Care Directive. LIFE CARE planning. my values, my choices, my care. kp.org/lifecareplan
 Advance Health Care Directive LIFE CARE planning my values, my choices, my care kp.org/lifecareplan Name of provider: Introduction This Advance Health Care Directive allows you to share your values, your
Advance Health Care Directive LIFE CARE planning my values, my choices, my care kp.org/lifecareplan Name of provider: Introduction This Advance Health Care Directive allows you to share your values, your
2. Unlicensed assistive personnel: any personnel to whom nursing tasks are delegated and who work in settings with structured nursing organizations.
 XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
National Patient Experience Survey South Tipperary General Hospital.
 National Patient Experience Survey 2017 South Tipperary General Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to
National Patient Experience Survey 2017 South Tipperary General Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Leadership in Palliative Care: Strategies for APNs
 Leadership in Palliative Care: Strategies for APNs April 20, 2018 Lyn Ceronsky DNP, GNP, CHPCA, FPCN lcerons1@fairview.org System Director, Palliative Care Director, Fairview Palliative Care Leadership
Leadership in Palliative Care: Strategies for APNs April 20, 2018 Lyn Ceronsky DNP, GNP, CHPCA, FPCN lcerons1@fairview.org System Director, Palliative Care Director, Fairview Palliative Care Leadership
Moral Conversations with ICU Patients and Families
 Moral Conversations with ICU Patients and Families Barb Supanich,RSM, MD,FAAHPM Medical Director, Palliative Care and Senior Services Holy Cross Hospital March 11, 2010 Learner Objectives Describe three
Moral Conversations with ICU Patients and Families Barb Supanich,RSM, MD,FAAHPM Medical Director, Palliative Care and Senior Services Holy Cross Hospital March 11, 2010 Learner Objectives Describe three
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
WISCONSIN Advance Directive Planning for Important Health Care Decisions
 WISCONSIN Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program
WISCONSIN Advance Directive Planning for Important Health Care Decisions Caring Connections 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 Caring Connections, a program