Nebraska Rural Health Association RHC Group
|
|
|
- Dwayne Foster
- 6 years ago
- Views:
Transcription
1 Presented on Behalf of Nebraska Rural Health Association RHC Group By Janet Lytton, Director of Reimbursement Rural Health Development September
2 RHC Billing Regulations CMS RHC Internet Only Claims Manual Guidance/Manuals/Downloads/clm104c09.pdf 2
3 Medicare Benefit Policy Manual Ch 13 RHC and FQHC Services Rev 201 issued 12/12/14, effective 1/1/15 Guidance/Guidance/Manuals/Downloads/bp102c 13.pdf CMS clarification of stand-alone preventive services Service-Payment/FQHCPPS/Downloads/RHC- Preventive-Services.pdf 3
4 An RHC is a certification from CMS that allows physician practices to qualify for cost-based reimbursement from Medicare and Medicaid; Any service provided in a physician s clinic can be performed in an RHC 4,100 RHCs across the country out of 230,187 physician practices (1.7%) Who are the RHCs in your State? Network-MLN/MLNProducts/Downloads/ rhclistbyprovidername.pdf 4
5 Patient Deductible = $147 per year IRHC Rate = $80.44/visit PBRHC PPS Hospital Rate = $80.44/visit PBRHC <50 bed hospitals = No limit 5
6 Physician services NP, PA & CNM services Services & Supplies incident to provider service Diabetes self-management training services and medical nutrition therapy services for diabetic patients provided by registered dietitians or nutritional professionals not separately billable for RHCs but indirectly paid Visiting nurse services in non HHA area Clinical psychologist & clinical social worker CP & CSW supplies & services incident to CMS Manual Ch 13 Sec 50 6
7 Hospital patient services Lab tests (except venipuncture is part of Visit) Part D Drugs & Self administrable drugs DME Ambulance services Technical components of diagnostic tests i.e. xrays & EKG, Holter Monitoring Technical components of screening services i.e. screening paps/pelvic, PSA Prosthetic devices Braces CMS Pub Ch 13, Sec 60 &
8 Nurse service w/o face-to-face visit or incident to visit I.e. allergy injection, hormone injection, dressing change, venipuncture Provider MUST be in clinic to have incident to CMS Manual Chapter 13 Section Telephone services CMS Manual Chapter 13 Section 100 & 120 Prescription services CMS Manual Chapter 13 Section 100 & 120 8
9 Multiple Visits Same Day, Payable if Patient has second visit for additional DX A medical visit and a mental health visit same day (2 visits) IPPE and Medical Visit and Mental Health Visit (3 visits) AWV and a Mental Health Visit (2 visits) Clinic visit and Hospital admit is per your MAC Generally allows based on medically necessary Patient must have face-to-face contact in hospital CMS Pub Ch 13, Sec
10 Face-to-Face with the Provider Physician, PA, NP, CNM Clinical Social Worker or Clinical Psychologist Medically necessary Does it require the skills of a Provider? Payer Class All payer classes are counted in the total visit count Place of Service Clinic, Home, NH, SNF/SW B, Scene of Accident Level of Service All levels apply, to include procedures To include all services incident to 10
11 Significant, separately identifiable E/M service by same provider on the same day of a procedure or other service. Append to E/M code, I.e (in system only) Use Modifier 25 when one of the following criteria is met: Visit for a problem unrelated to the procedure Visit for a new problem or a problem that has changed significantly and requires re-evaluation before performing the procedure. Visit for the same problem in different sites; one treated surgically and one treated medically. 11
12 Visit for a problem unrelated to the procedure or service Preventive Care Visit = patient seen for annual physical E/M service = Patient also c/o leg pain, swelling and hot spot. Evaluated for phlebitis Supporting Documentation E/M documentation identifiably distinct from procedure documentation Must meet ALL requirements for E/M visit along with documentation of procedure. 12
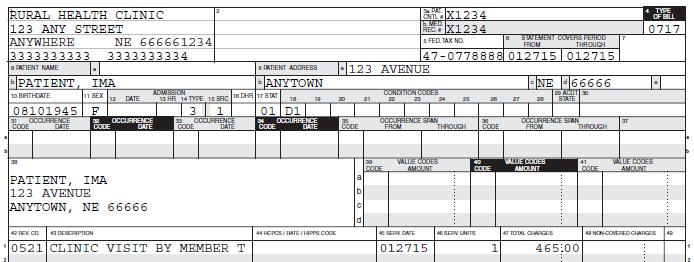
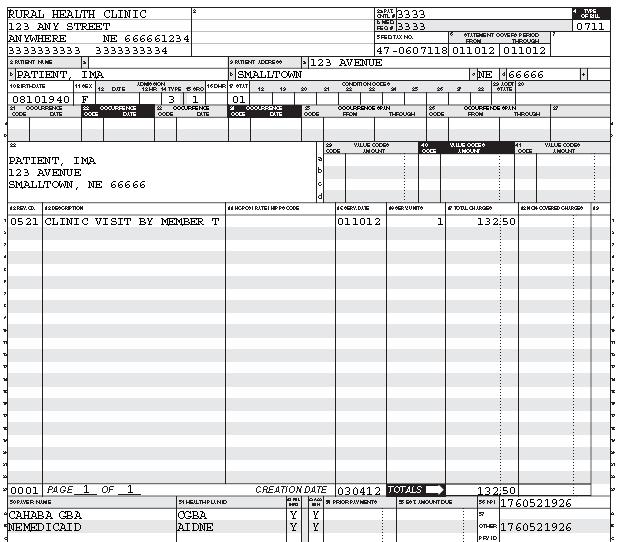
13 UB 04 form or 837i electronic format Bill Type 711 Revenue Codes (NO CPT CODES ON CLAIM) Exception when billing preventive services Sent to Fiscal Intermediary Claims for all RHC visits Office, Skilled Nursing Home, Swing Bed, Nursing Home, Home, Scene of an accident Actual charges billed 13
14 Office visit in clinic Home visit Visit to a Part A SNF or SW patient Only prof service as labs, drugs, x-ray TC, EKG tracing gets billed to the SNF. Visit to a Pt in a SNF, NF, ICF MR, AL Patient not on a Part A SNF Stay Visiting Nurse Service in a HHA shortage Visit at other site, I.e. scene of accident Telehealth site fee Mental Health Services All drugs & supplies, are bundled with the visit code charges in the Revenue Codes shown above 14
15 RHC office visit services Excludes all labs, x-ray TC & EKG Tracing, any TC Includes venipuncture effective 1/1/14 Billed to the FI, UB04 Form or electronic Paid on the clinic s all inclusive rate All Medicare coverage rules apply Reasonable & necessary Allowed preventive is covered, I.e. pap, PSA 15
16 All labs, x-ray TC, EKG tracing, any technical components (venipuncture is part of the office visit bundled service) All hospital services (IP, OP, ER, OBS) Billed to MAC, HCFA 1500 Form Paid on the Medicare Pt B fee schedule 16
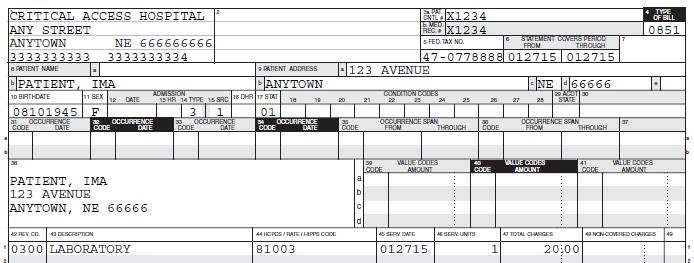
17 All hospital services (IP, OP, ER, OBS)* Billed to WPS MAC, HCFA 1500 Form Paid on the Medicare existing fee schedule * The only exception is if the CAH is Method II reimbursement; then the OP, ER & OBS professional component is part of the hospital s claim. 17
18 ALL Laboratory performed in the RHC, including 6 basic tests (venipuncture is part of the office visit bundled service) Billed using 141 bill type for PPS Hospitals MLN SE1412, December 27, 2013 CAH 851 bill type For any facility owned by CAH or CAH employee performing Technical Component X-ray EKG Holter Monitor All TC s Billed using 131 bill type for PPS Hosp All TC s Billed using 851 bill type for CAH Paid on the Medicare Pt B Fee Schedule 18
19 CAH Method II Hospital bills for both the professional and technical component when performed in the hospital setting: X-ray EKG Holter Monitor ER OP/OBS/ASC Must have separate line item for the prof service Paid on the Medicare Pt B Fee Schedule + 15% 19
20 Must have RHC and nonrhc number Ailments are RHC services Preventive services are nonrhc services IRHCs receive 100% of their Medicaid PPS rate PB of <50 bed hosp receive 100% of their actual charges PB of >50 bed hosp receive 100% of MCD PPS rate Must send in a copy of your Medicare CR annually as is a Federal Requirement With PPS payments there are no cost report settlements either to or from the RHC 20
21 Each Managed Care Payer (MCP) can require either/both UB04 or 1500 Arbor Health United HealthCare Coventry Of which all questions presented in the Spring to all MCPs were not answered All Services for the Managed Care patients are sent to the MCP nothing sent to DHHS MCP can determine how to bill and how to pay claims MCPs are given RHCs facility specific payment rates to assure MCP is paying the most current rate RHC Medicaid year is 7/1 through 6/30 each year 21
22 RHC services = bundled services UB04 Lab, X-ray TC and EKG tracings are billed on the nonrhc provider # X-ray PC and EKG interp is part of visit and bundled on the RHC Provider # All preventive, IP, OP, ER, OBS are nonrhc services, billed with nonrhc Provider # OB is global with exception of first visit If only visits, then nonrhc# and list visit dates All surgeries at the hospital have 2 wk global 22
23 RHC services = bundled services UB04 Lab, X-ray TC, EKG tracing billed with Hosp OP # Professional components are part of the visit All preventive, IP, OP, ER, OBS are nonrhc services, billed with the nonrhc # OB is global with exception of first visit If only OB visits, bill nonrhc# and list visit dates All surgeries at the hospital have 2 wk global 23
24 Incident to services without a face-to-face visit are billed on the nonrhc # i.e. injection only Must have both the administration CPT code and the NDC of the drug administered If VFC is used, only the administration CPT is paid on the nonrhc # NO V-codes as primary nonrhc services paid using the fee schedule and not your RHC rates 24
25 Billed as in fee-for-service clinic No changes in reimbursement Must not discount charges no cash discounts at time of service payment no professional discounts given All discounts given should be based on finances of patients i.e. sliding fee scales can be developed to as high as 400% of poverty guidelines per Federal Regulations 25
26 Two types of plans PFFS Private Fee for Service Send Claims on UB04 with Medicare Rate letter Regional/PPO Plans Must provide service to the entire region per CMS Send Claims on UB04; you negotiate payment When patients switch to MA, they are on your Private section of your visit counts *You may want to keep them separate as they will count as Medicare patients if you need to figure the % of Medicare utilization. 26
27 Injections with an Office Visit Charge All CPT codes in system Bundle all charges and submit claim to RHC MCR If it is a Pt D drug, it must be sent to Pt D plan or Patient Injections only nurse service Charge in system Either DO NOT bill (write off) as there is no f-t-f visit OR can be bundled with a visit within 30 days pre or post nursing service and submitted with that f-t-f visit If injectable is a Part D drug it MUST not be a part of the RHC claim as it is only billable to the patient or to Part D 27
28 Injectable/Vaccine as a Part D drug 1/1/08 The injectable/vaccine is payable only through Pt D If injectable/vaccine is obtained at the clinic level, then the patient is to pay for the injectable/vaccine and the administration privately and then they have to submit that claim to their Part D company to be reimbursed for the services. Clinics can link to: and bill the Pt D drug and get payment to include administration of the drug and let you know the copay amount. 28
29 Injections: Pt D Drugs, i.e. Gardasil, Zostavax, Varivax, Tetanus (as immunization update), DTAP Medicare: Pt D drugs require billing to Pt D or the Patient can pay for these services and send to their Pt D plan and be reimbursed OR submit claim to a company such as MyTransactRX Medicaid: If patient is eligible and has an ailment visit, bill with the visit as an RHC visit; if no ailment visit bill on the nonrhc number on the 1500 form Private/Commercial: Bill as did in FFS clinic For Medicare, these drugs are not to be on your RHC claim as they are not a Part B benefit for the patient 29
30 All coded with the accurate CPT code Don t forget to charge the venepuncture in OV effective 1/1/14 is part of the office bundled services IRHCs All Labs, to include the required basic 6 tests, are payable through Medicare Part B; NE Medicaid labs are billed on the nonrhc prov # PBRHCs All labs, to include the required basic 6 tests, both Medicare & Medicaid are payable through the Hospital OP provider #, either 851 (CAH) or 141 type of bill (TOB) for other hospitals 30
31 All coded with the accurate CPT code for each the technical component and the professional component if provider interprets Chest x-ray = TC Two views frontal & lateral; x-ray interpretation Interpretation is billed with the office visit and included in the total charges that are submitted to Medicare Rural Health Technical Component is billed to Medicare Pt B or for PBRHC, billed using the hospital OP provider # NE Medicaid follows Medicare guidelines Medicare reg on prof component billing: CMS Internet-Only Manual, Publication , Ch 13, Sec
32 Coded using the tracing only for the TC & the interpretation only if provider interprets. EKG Tracing only = EKG Interpretation and report = Interp is billed with the office visit and included in the total charges that are submitted to Medicare Rural Health Tracing only is billed to Medicare Pt B or for PBRHC, billed using the hospital OP provider number NE Medicaid follows Medicare guidelines w/cpts 32
33 Direct supervision by provider required Must be in clinic, not in same room being in the hosp when attached to clinic is NOT incident to Part of provider s services previously ordered integral, though incidental covered as part of an otherwise billable encounter I.e. dressing change, injection, suture removal, blood pressure monitoring Medicare & NE Medicaid services should be billed under the provider that performed the service 33
34 Can be combined on claim with a visit within 30- days pre or post incident to service for plan of treatment NEVER considered a separate visit List only the date of the visit as date of service Charges should reflect all services bundled When added, the added reimb is the 20% copay Adjustments OK 717 Type of Bill; CC=D1; remarks changes in charges Otherwise, the costs are shown on your cost report and claimed indirectly CMS , Ch 13, Sec 110; Sec 130; Sec


35 TOB 717 Claim must be in finalized status Adjustment will appear as a debit or credit on future remittance advice Encourage submitting electronically exceptions denied charges & claims rejected as MSP Do not send another 711 claim as will error as a duplicate Examples of Adjustments: Revenue code changes, Service unit decrease or increase, Total charges changed, Primary payer incorrect 35
36 36
37 Medicare: Bill OV and EKG interp (if provider does the interp) to RHC Medicare on UB 04 (one line item, no CPT codes); Bill EKG tracing to MCR Pt B for IRHCs & PBRHCs bill with 131 or 851 TOB with Hosp OP # on UB04 Bill lab for IRHC to MCR Pt B & PBRHC bill with 141 or 851 TOB with Hosp OP # on UB04 Medicaid: Follows Medicare guidelines w/cpt Private/Commercial: Bill as in FFS clinic 37
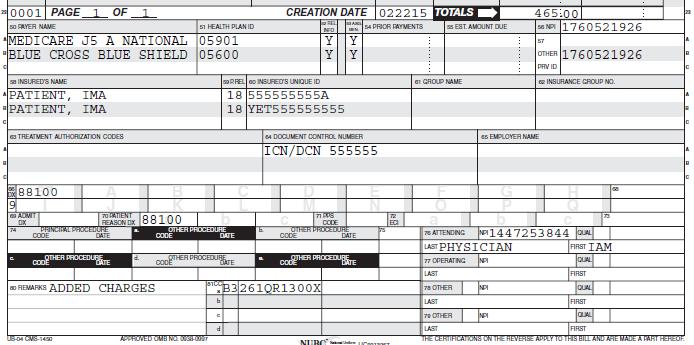
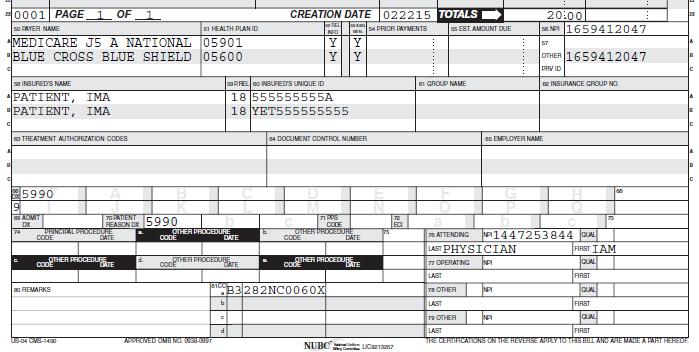
38 I.e. Lesion removal, joint injection, or wound closure, AND E & M code Medicare: Charge the OV level w/-25, the procedure codes, any med used bill all collapsed into the 521 rev code (no CPTs on claim) Medicaid: Charge the OV level w/-25, the procedure codes, any med used on UB, bill all collapsed into the 521 rev code (with E & M CPT on claim) Private/Commercial: Bill as in FFS clinic 38
39 39
40 Medicare: Cahaba & WPS (depends on medical necessity) but generally, if for same ailment, are not allowing both services to be billed; thus bill the Admit (services must take place in the hospital) Medicaid: Bill the hospital admit and not the clinic visit. Private/Commercial: Bill the hospital admit For all payers make sure you are accumulating all services to set the level of admit. 40
41 No global charges for Medicare in the RHC Each visit in the clinic is a billable visit if it wasn t your provider that did procedure, verify they billed with the -54 modifier Code the surgical procedure with -54 (surgical procedure only) and bill to Part B Bill the pre and post visits as RHC visits as it is the RHC facility billing the services, not a specific provider NE Medicaid has a 2 week global for procedures in the hospital setting 41
42 Medicare: Visits would be medically reasonable and necessary and billed as an RHC visit with 711 TOB and 521 revenue code. Delivery only would be billed as a hospital nonrhc service; each post partum visit is a billable visit Medicaid: NE pays global for OB services unless provider transfers for delivery, then bill number of visits with dates 42
43 Clinical Psychologist (PhD) Doctoral level of education Clinical Social Worker (CSW) Masters level with at least 2 years experience Use 900 revenue code to bill therapeutic behavioral health The first visit to determine services by a physician/pa/np is an RHC visit, then behavioral health services apply Reimbursement in 2014> is 80/20 43
44 Allowed Medicare Preventive Services are billed through the Rural Health Clinic on the UB04 Technical Components, labs, EKG tracing are billed on the nonrhc side, either through the Hospital OP provider number (PBRHC) or to MCR Pt B (IRHC) use correct G-codes Each preventive service MUST be on a separate line on the UB with the G-code CMS Pub Ch 13, Sec
45 45
46 46
47 47
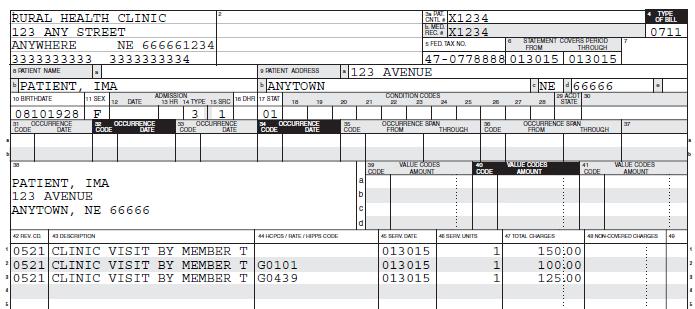
48 48
49 49
50 50
51 Preventive Services Quick Reference Guide: _QuickReferenceChart_1.pdf IPPE Quick Reference Guide: MLN/MLNProducts/downloads/MPS_QRI_IPPE001a.pdf Annual Wellness Visit Quick Reference Guide: work- MLN/MLNProducts/downloads/AWV_Chart_ICN pdf More Preventive Service info: /Downloads/clm104c09.pdf /Downloads/clm104c18.pdf /Downloads/bp102c13.pdf 51
52 Keep a log of injections, or have your computer track Medicare paid on your Medicare Cost Report Flu payable once per season; pneumo initial must be at least 11 months before second of different vaccine (eff 1/1/15) Medicaid is paid only if in your State benefits at time of service Keep track of vaccine and supply costs (invoices) Determine average nursing hours per week Determine average provider hours per week Generally allow 10 minutes per injection on Cost Report, but do a time study NO Medicare Advantage on log LOGS MUST BE LEGIBLE 52
53 Suggest inputting into system with the G0008-flu administration, and G0009-pneumo administration Create a report that will list Medicare flu and pneumo injections Patient Name Date of Service Patient Medicare number Log is sent with your RHC Cost Report for payment through your cost report. NEVER send a claim for a Medicare flu or pneumo injection to either Medicare Rural Health or Pt B 53
54 Medicare: Does not pay for physicals, except for the Introduction to Medicare Physical. If the visit is only for a physical and not for the ailments, then bill the patient. Effective 1/1/11, Medicare will pay for an annual wellness visit per year; This IS NOT a physical Medicaid: Covered for kids and billed on the nonrhc Medicaid provider number Private/Commercial: Bill as in FFS clinic 54
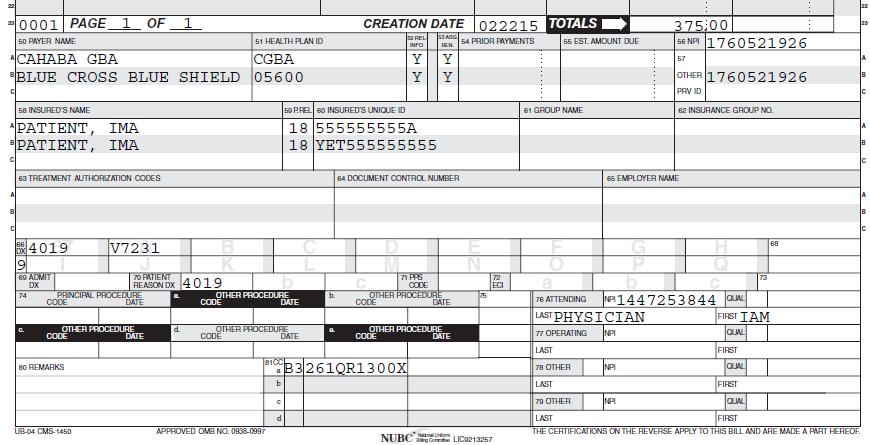
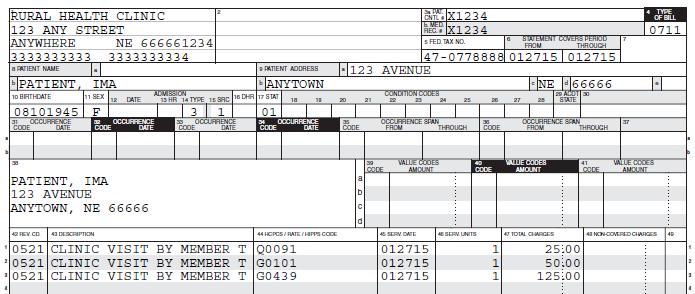
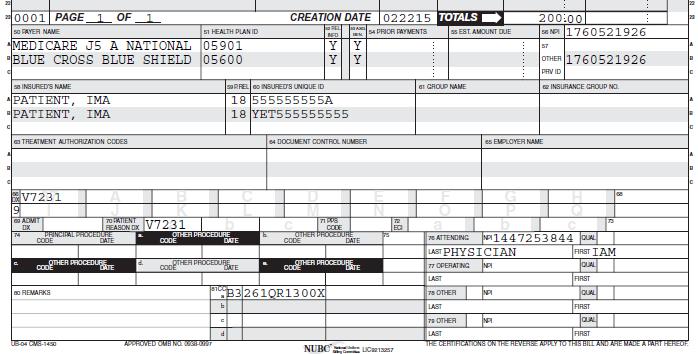
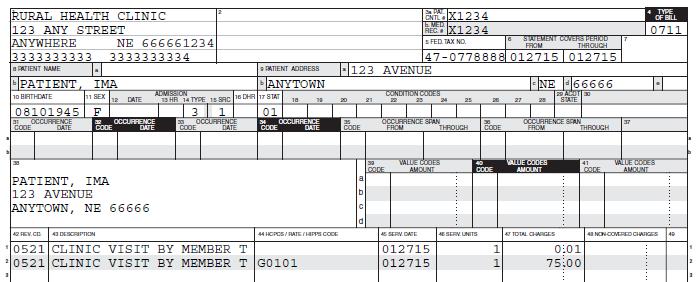
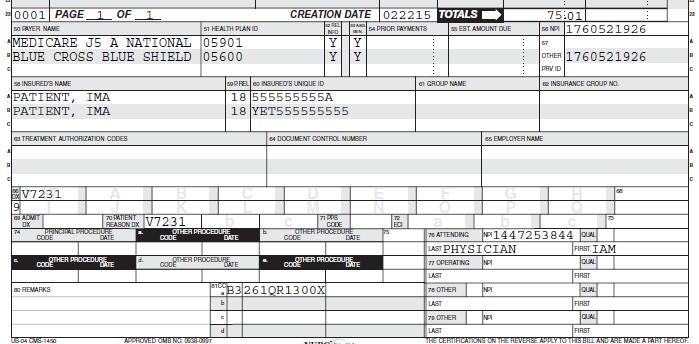
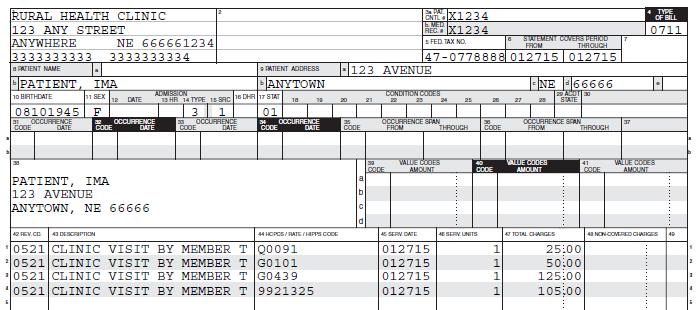
55 How does a RHC bill for a "Well Woman Exam"? Medicare does not have a "Well Woman Exam" as a covered preventive service. Each component of the "Well Woman Exam" would have to be looked at and billed separately. For instance, the Annual Wellness Visit is covered yearly and billed with either G0438 for the initial exam (covered once in a lifetime) or G0439 if it is a subsequent visit (covered annually). Both Screening Pap Tests and Screening Pelvic Examinations are covered every 24 months for low risk women and billed with Q0091 and G0101 respectively. Each of these tests, if the beneficiary is eligible, would be billed on a separate 052x revenue code line. For more information on Medicare's Preventive Services, please see the Medicare Preventive Services Quick Reference Chart 55
56 If a patient comes in for a preventive exam which is not a covered exam, who do we bill? Since it is not a covered service, you will bill the beneficiary. (This includes DOT physical) For any preventive service that has a frequency limitation, it is encouraged to get an ABN just in case the service is done at the incorrect timing, if no ABN, the clinic cannot charge if Medicare does not pay. As of 9/1/12 the UB claim is allowed to have the GA modifier along with the HCPCS code with the Occurrence Code of 32 with the date the ABN was signed. 56
57 57
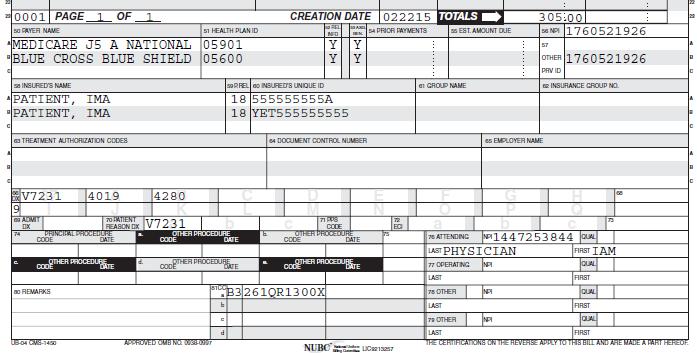
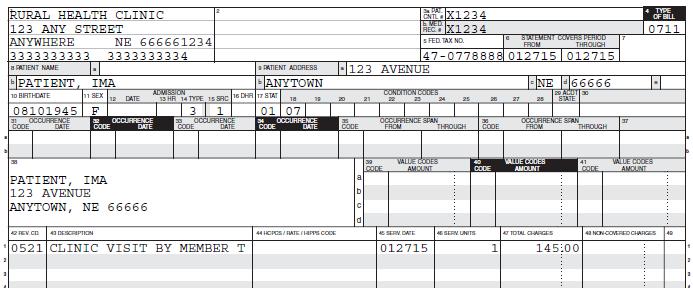
58 58
59 59
60 60
61 61
62 For NF/SNF/SW Bed visits Code/Bill Rev Code for Skilled patient; 525 Rev Code for NH patient NE Medicaid only, NH req d visits on the nonrhc# 62
63 When seen for the hospice condition Is not payable to the clinic and must be coordinated with the Hospice Entity Any TC is billed to the Hospice Co, if required Coordinate all cares with the Hospice Company When seen for a condition other than the reason for being on hospice Bill the MAC/FI as an RHC visit, RC 52X Use Condition Code 07 Use diagnosis for ailment not the hospice DX Medicare Benefits Policy Manual 13, Sec
64 64
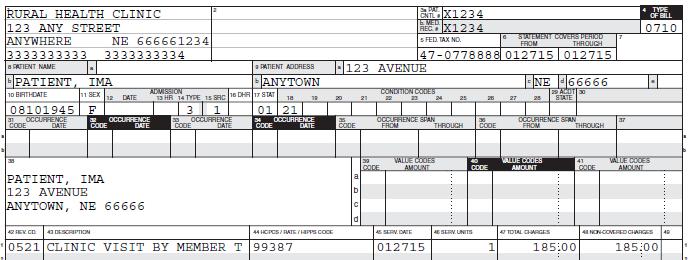
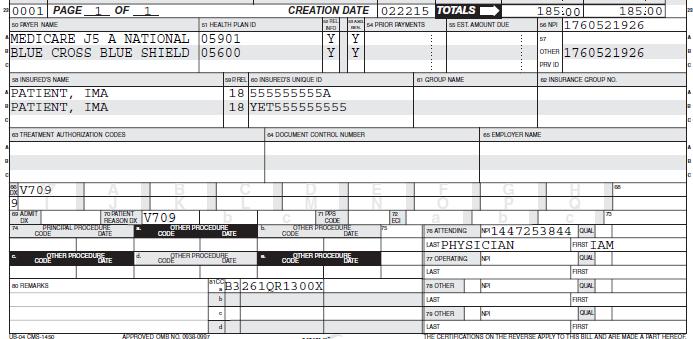
65 How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual, Publication , Chapter 1,Adobe Portable Document Format Section This section of the manual states, "... all of a bundled service must be billed as noncovered, or none of it. Therefore, as long as part of a bundled service is certain to be covered or medically necessary, billing the entire bundled service as covered is appropriate." 65
66 66
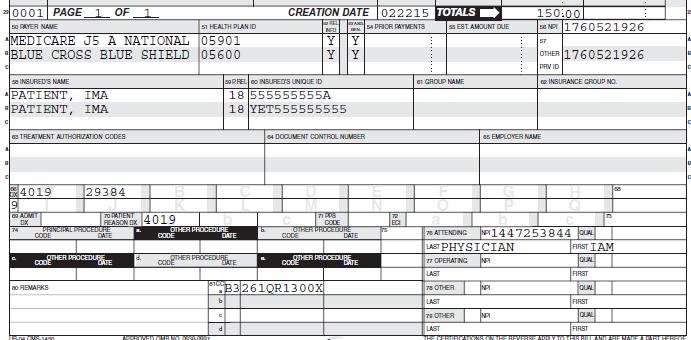
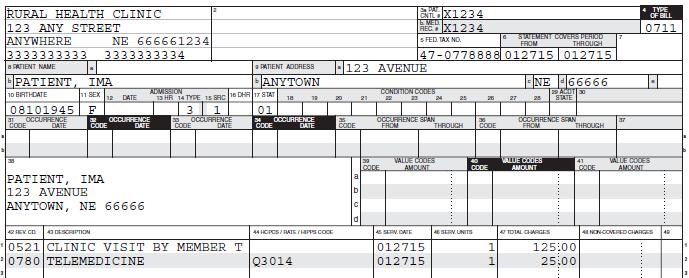
67 Bill to RHC FI Revenue Code 780 Does not require a Face-to-Face visit same day Q3014 code is paid separately from allinclusive rate at the Medicare Phys Fee Schedule Bill for transmission fee REQUIRED to put the Q code on the claim RHCs are not allowed to be the provider 67
68 68
69 30-day transitional period after discharge from inpatient hospital and next 29 days Face-to-face visit within 14 days of discharge moderate medical decision complexity high medical decision complexity Only 1 health care professional may report TCM Report once per beneficiary during TCM Date of service used is the face-to-face DOS TCM cannot be billed during a global period Documentation required: Date of discharge Date of interactive contact with bene and/or caregiver Date of face-to-face visit Complexity of Medical Decision making MLN ICN
70 At this time, this is nonreimbursable in the RHC Will be reimbursed to RHCs per MPFS beginning 1/1/16 Physicians, NPs, PAs, CNMs, CNSs Provider must bill IPPE, AWV or comp E & M prior Must use Electronic Health Record Must get consent from patient for this service At least 20 minutes of clinical staff time per calendar month to include: Multiple (2 or more) chronic conditions to last at least 12 mo or until death Significant risk of death, acute exacerbation/decompensation, or functional decline Comprehensive care plan established, implemented, revised, or monitored Examples: Alzheimers; arthritis; asthma; atrial fibrillation; autism spectrum disorders; cancer; COPD; depression; diabetes; heart failure; hypertension; ischemic heart disease; osteoporosis MLN ICN
71 RHCs will be required to bill by line item, i.e office E & M, meds used, office procedure, each preventive service each a separate line with the CPT code listed instructions yet to be determined Chronic Care Management Services to be billable in the RHC; paid at the MPFS; billed on the UB either with another service or as only service on the claim PQRS will not apply to RHCs for either the RHC or the nonrhc services. PBRHC issue to be determined. 71
72 Because RHCs are not paid based on the Medicare Physician Fee Schedule, they are not included in the erx or PQRS program. PQRS is based on Tax ID. Currently, the PBRHCs with the hospital Tax ID, are not showing up as exempt. NARHC is in conference with CMS on how to fix this issue. Thus, there are no penalties for any services of an RHC, to include any nonrhc services. PBRHCs are encouraged to capture all PQRS data until CMS has a fix in their system. 72
73 All practices that accept Medicare & Medicaid dollars are required to have a Corporate Compliance Policy Hosp/Clinic Corporate Compliance Policy HIPAA Policies in place Do we have consents signed? Are we getting ABNs (Advanced Beneficiary Notices) when appropriate (must be CMS-R /11) Keep copy of ABN Are we asking the MSP (Medicare Secondary Payer) questions? Is our billing appropriate for the documentation in the chart? 73
74 ickreferencechart_1.pdf (interactive preventive service web tool) Network-MLN/MLNProducts/downloads/MPS_QRI_IPPE001a.pdf Network-MLN/MLNProducts/downloads/ /AWV_Chart_ICN pdf /downloads/som107ap_g_rhc.pdf (CMS State Operations Manual) Make sure you are a part of your MAC listserve for updated info! 74
75 (NeRHA) (National Association of RHCs) Manuals/ Downloads/bp102c13.pdf (new RHC/FQHC Regulations 1/15) Downloads/clm104c09.pdf (RHC CMS Claims Manual) Rural Health Development Website & my
76 Any? s 76
How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21.
 How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual,
How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual,
RHC Billing RHC and nonrhc Services Janet Lytton, Director of Reimbursement Rural Health Development
 RHC Billing RHC and nonrhc Services Janet Lytton, Director of Reimbursement Rural Health Development 308-647-6455 janet.lytton@rhdconsult.com SEPTEMBER 18, 2014 1 Understand the billing of the various
RHC Billing RHC and nonrhc Services Janet Lytton, Director of Reimbursement Rural Health Development 308-647-6455 janet.lytton@rhdconsult.com SEPTEMBER 18, 2014 1 Understand the billing of the various
CMS , Ch 13, Sec
 Direct supervision by a provider is required Must be in clinic, not in same room being in the hospital when attached to clinic is NOT incident to Part of provider s services previously ordered integral,
Direct supervision by a provider is required Must be in clinic, not in same room being in the hospital when attached to clinic is NOT incident to Part of provider s services previously ordered integral,
Slide 1. Slide 2. Slide 3. Overview of RHC Regulations. RHC Billing Requirements. RHC Billing How To s. RHC Key Internet sites
 Slide 1 By Janet Lytton, Director of Reimbursement Rural Health Development janet.lytton@rhdconsult.com September 2017 1 Slide 2 Overview of RHC Regulations RHC Billing Requirements RHC Billing How To
Slide 1 By Janet Lytton, Director of Reimbursement Rural Health Development janet.lytton@rhdconsult.com September 2017 1 Slide 2 Overview of RHC Regulations RHC Billing Requirements RHC Billing How To
Provider-Based RHC Billing June 8, 2018
 Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
RHC Billing for Provider-Based RHCs. Charles A. James, Jr. President and CEO North American Healthcare Management Services
 RHC Billing for Provider-Based RHCs Charles A. James, Jr. President and CEO North American Healthcare Management Services Presentation Objectives Provider-Based Requirements Provider-based Enrollment Issues
RHC Billing for Provider-Based RHCs Charles A. James, Jr. President and CEO North American Healthcare Management Services Presentation Objectives Provider-Based Requirements Provider-based Enrollment Issues
Complete RHC Medicare Billing
 Complete RHC Medicare Billing 1 RHC Basics 2 What is a Rural Health Clinic? This CMS publication is an excellent resource as an overview of the RHC Program. Program Basics Certification Process Qualified
Complete RHC Medicare Billing 1 RHC Basics 2 What is a Rural Health Clinic? This CMS publication is an excellent resource as an overview of the RHC Program. Program Basics Certification Process Qualified
RHC Basics and Beginning Billing 03/19/2018. Dedicated to improving access to quality healthcare in rural communities
 RHC Basics and Beginning Billing 03/19/2018 Dedicated to improving access to quality healthcare in rural communities RHC Services An RHC Encounter is defined as a medicallynecessary, face-to face (one-on-one)
RHC Basics and Beginning Billing 03/19/2018 Dedicated to improving access to quality healthcare in rural communities RHC Services An RHC Encounter is defined as a medicallynecessary, face-to face (one-on-one)
Independent RHC Billing Introduction Session 3 Spring, 2018
 Independent RHC Billing Introduction Session 3 Spring, 2018 Contact Information Mark Lynn, CPA (Inactive) RHC Consultant Healthcare Business Specialists Suite 214, 502 Shadow Parkway Chattanooga, Tennessee
Independent RHC Billing Introduction Session 3 Spring, 2018 Contact Information Mark Lynn, CPA (Inactive) RHC Consultant Healthcare Business Specialists Suite 214, 502 Shadow Parkway Chattanooga, Tennessee
Rural Health Clinic Billing
 Critical Access Hospital and Rural Health Clinic Billing September 12, 2017 1 Rural Health Clinic Overview Rural Health Clinic Services Preventive Services in the RHC Non-RHC Services/Non-Covered Services
Critical Access Hospital and Rural Health Clinic Billing September 12, 2017 1 Rural Health Clinic Overview Rural Health Clinic Services Preventive Services in the RHC Non-RHC Services/Non-Covered Services
Rural Health Clinic Overview
 TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
NARHC Spring Institute
 NARHC Spring Institute Tuesday, March 15, 2016 San Antonio Conference Breakouts Your choice Regency Ballroom E Mac Discussion: Novitas Kim Robinson Live Oak Mac Discussion: Noridian Tana Williams You are
NARHC Spring Institute Tuesday, March 15, 2016 San Antonio Conference Breakouts Your choice Regency Ballroom E Mac Discussion: Novitas Kim Robinson Live Oak Mac Discussion: Noridian Tana Williams You are
Medicare Preventive Services
 Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
RURAL HEALTH REIMBURSEMENT OPPORTUNITIES & UB-04 BILLING CHANGES FOR 2016
 WEBINAR FOLLOW-UP QUESTIONS Thank you for attending our webinar on March 9, 2016. In follow-up to that webinar, we have compiled the following summary of all attendee questions and answers received. Pertinent
WEBINAR FOLLOW-UP QUESTIONS Thank you for attending our webinar on March 9, 2016. In follow-up to that webinar, we have compiled the following summary of all attendee questions and answers received. Pertinent
WHY SHOULD A CHC/FQHC CARE?
 Suzanne Niemi, CPA, CMPE, CCE Alaska Primary Care Association April 2017 Medicare Part A & Part B MACRA / MIPS Chronic Care Management Billing WHY SHOULD A CHC/FQHC CARE? 2 DEFINITIONS FQHC Federally Qualified
Suzanne Niemi, CPA, CMPE, CCE Alaska Primary Care Association April 2017 Medicare Part A & Part B MACRA / MIPS Chronic Care Management Billing WHY SHOULD A CHC/FQHC CARE? 2 DEFINITIONS FQHC Federally Qualified
MLN Matters Number: MM6740 Revised Related Change Request (CR) #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010
 #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010") News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
5/1/2017. Medicare Coverage Guidelines for DSMT and MNT Telehealth. Telehealth Defined
 Medicare Coverage Guidelines for DSMT and MNT Telehealth Mary Ann Hodorowicz, RDN, MBA, CDE Certified Endocrinology Coder Mary Ann Hodorowicz Consulting, LLC 4-30-17 MEDICARE DSMT - MNT TELEHEALH KEY TOPICS
Medicare Coverage Guidelines for DSMT and MNT Telehealth Mary Ann Hodorowicz, RDN, MBA, CDE Certified Endocrinology Coder Mary Ann Hodorowicz Consulting, LLC 4-30-17 MEDICARE DSMT - MNT TELEHEALH KEY TOPICS
RHC Billing - Introduction Fall, 2017
 RHC Billing - Introduction www.ruralhealthclinic.com Fall, 2017 Contact Information Mark Lynn, CPA (Inactive) RHC Consultant Healthcare Business Specialists Suite 214, 502 Shadow Parkway Chattanooga, Tennessee
RHC Billing - Introduction www.ruralhealthclinic.com Fall, 2017 Contact Information Mark Lynn, CPA (Inactive) RHC Consultant Healthcare Business Specialists Suite 214, 502 Shadow Parkway Chattanooga, Tennessee
Deleted Codes. Agenda 1/31/ E/M Codes Deleted Codes New Codes Changed Codes
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
SNF Consolidated Billing Exclusions/Inclusions
 SNF Consolidated Billing Exclusions/Inclusions Under SNF consolidated billing rules, certain Part B services provided to SNF residents are to be billed directly by the SNF. The facility would bill the
SNF Consolidated Billing Exclusions/Inclusions Under SNF consolidated billing rules, certain Part B services provided to SNF residents are to be billed directly by the SNF. The facility would bill the
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
REVISION DATE: FEBRUARY
 Mary Ann Hodorowicz, MBA, RDN CDE, CEC, Owner, Mary Ann Hodorowicz Consulting LLC, Palos Heights, IL Coverage: In-Person Payable Places of Services Excluded Places for Part B Payment Excluded Places: 0
Mary Ann Hodorowicz, MBA, RDN CDE, CEC, Owner, Mary Ann Hodorowicz Consulting LLC, Palos Heights, IL Coverage: In-Person Payable Places of Services Excluded Places for Part B Payment Excluded Places: 0
Using Education Codes Effectively and Legally in Clinical Sleep Education
 SOUTHERN SLEEP SOCIETY 39 TH ANNUAL MEETING SOUTHERN SLEEP SOCIETY TECHNOLOGIST COURSE - 2017 Using Education Codes Effectively and Legally in Clinical Sleep Education Jayme R. Matchinski March 23, 2017
SOUTHERN SLEEP SOCIETY 39 TH ANNUAL MEETING SOUTHERN SLEEP SOCIETY TECHNOLOGIST COURSE - 2017 Using Education Codes Effectively and Legally in Clinical Sleep Education Jayme R. Matchinski March 23, 2017
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid s MLN Matters Number: MM9269 Revised Related CR Release : January 26, 2016 Related Transmittal #: R1596OTN Change Request (CR) #:
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid s MLN Matters Number: MM9269 Revised Related CR Release : January 26, 2016 Related Transmittal #: R1596OTN Change Request (CR) #:
Initial Preventive Physical Examination (IPPE) Presented by Provider Outreach and Education (POE) December 2016
 Presented by Provider Outreach and Education (POE) December 2016") Initial Preventive Physical Examination (IPPE) Presented by Provider Outreach and Education (POE) December 2016 DISCLAIMER This information release is the property of Noridian Healthcare Solutions, LLC
Initial Preventive Physical Examination (IPPE) Presented by Provider Outreach and Education (POE) December 2016 DISCLAIMER This information release is the property of Noridian Healthcare Solutions, LLC
Medi-Pak Advantage: Reimbursement Methodology
 Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
Blue Cross provides administrative claims services only. Your employer or plan sponsor is financially responsible for claims.
 HOPE COLLEGE - HOURLY ORANGE 007013084/0011/0012/0013/0014/0015/0016/0017 Simply Blue PPO HSA ASC Effective Date: On or after July 2018 Benefits-at-a-glance This is intended as an easy-to-read summary
HOPE COLLEGE - HOURLY ORANGE 007013084/0011/0012/0013/0014/0015/0016/0017 Simply Blue PPO HSA ASC Effective Date: On or after July 2018 Benefits-at-a-glance This is intended as an easy-to-read summary
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011
 PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
Chronic Care Management Services. Presented by Noridian Part B Medicare Provider Outreach and Education April 2015
 Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
Chronic Care Management Services Presented by Noridian Part B Medicare Provider Outreach and Education April 2015 Continuing Education Unit (CEU) When registering, add all additional attendees First and
RURAL HEALTH CLINICS
 RURAL HEALTH CLINICS Joan Hall, RN, President Nevada Rural Hospital Partners & Steve Boline, CPA, Regional CFO Nevada Rural Hospital Partners Legislative Committee on Health Care EXHIBIT G May 7, 2014
RURAL HEALTH CLINICS Joan Hall, RN, President Nevada Rural Hospital Partners & Steve Boline, CPA, Regional CFO Nevada Rural Hospital Partners Legislative Committee on Health Care EXHIBIT G May 7, 2014
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:
 Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:") Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Transitional Care Management We provide these services a-la-carte...
 Transitional Care Management We provide these services a-la-carte... Initial Patient Outreach* This must be done within 2 days of the patient s discharge from the hospital. During this call patient s medications
Transitional Care Management We provide these services a-la-carte... Initial Patient Outreach* This must be done within 2 days of the patient s discharge from the hospital. During this call patient s medications
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z
 A B C D E F G H I J K L M N O P Q R S T U V W X Y Z A Additional Development Request (ADR) Accessing ADR Information via FISS DDE... July 7, 2011, p. 10 Reason Code 56900... September 2011, p. 19 Tips
A B C D E F G H I J K L M N O P Q R S T U V W X Y Z A Additional Development Request (ADR) Accessing ADR Information via FISS DDE... July 7, 2011, p. 10 Reason Code 56900... September 2011, p. 19 Tips
All but Part A Deductible. Medicare Part A Deductible. Nothing. Inpatient Hospital All but Part A Medicare Part A Nothing.
 Summary of Signature 65 Benefits Signature 65 is a Medicare-complimentary benefit program that fills in the coverage gaps and cost sharing of the traditional Medicare program (Medicare Part A and ). In
Summary of Signature 65 Benefits Signature 65 is a Medicare-complimentary benefit program that fills in the coverage gaps and cost sharing of the traditional Medicare program (Medicare Part A and ). In
Cotiviti Approved Issues List as of February 26, 2018
 Cotiviti Approved Issues List as of February 26, 2018 All physician/npp specialties 32 Ambulance Providers 34 Ambulatory Surgery Center (ASC), Outpatient Hospital 38 Inpatient Hospital 40 Inpatient Hospital,
Cotiviti Approved Issues List as of February 26, 2018 All physician/npp specialties 32 Ambulance Providers 34 Ambulatory Surgery Center (ASC), Outpatient Hospital 38 Inpatient Hospital 40 Inpatient Hospital,
SUMMARY OF BENEFITS 2009
 HEALTH NET VIOLET OPTION 1, HEALTH NET VIOLET OPTION 2, HEALTH NET SAGE, AND HEALTH NET AQUA SUMMARY OF BENEFITS 2009 Southern Oregon Douglas, Jackson, and Josephine Counties, Oregon Benefits effective
HEALTH NET VIOLET OPTION 1, HEALTH NET VIOLET OPTION 2, HEALTH NET SAGE, AND HEALTH NET AQUA SUMMARY OF BENEFITS 2009 Southern Oregon Douglas, Jackson, and Josephine Counties, Oregon Benefits effective
Healthy Indiana Plan Reimbursement Manual
 H P M a n a g e d C a r e U n i t I N D I A N A H E A L T H C O V E R A G E P R O G R A M S Attention: This manual has not been archived, because the associated provider reference module is not yet complete.
H P M a n a g e d C a r e U n i t I N D I A N A H E A L T H C O V E R A G E P R O G R A M S Attention: This manual has not been archived, because the associated provider reference module is not yet complete.
Coding and Billing for Lifestyle Medicine
 Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Telemedicine and Telehealth Services
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Telemedicine and Telehealth Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 8 P U B L I S H E D : J A N U A R Y 1
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Telemedicine and Telehealth Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 8 P U B L I S H E D : J A N U A R Y 1
Telemedicine and Reimbursement
 Telemedicine and Reimbursement Presented for : March 14 th 2018 About Acevedo Consulting Incorporated Acevedo Consulting Incorporated prides itself on not providing cookie-cutter programs, but a quality
Telemedicine and Reimbursement Presented for : March 14 th 2018 About Acevedo Consulting Incorporated Acevedo Consulting Incorporated prides itself on not providing cookie-cutter programs, but a quality
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice
 Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Reporting Preventive Services & Problem-Oriented E & M in RHCs
 Reporting Preventive Services & Problem-Oriented E & M in RHCs John Burns, CPMA, CEMC, CPC, CPC-I Vice President, Audit and Compliance Services John.Burns@RuralHealthCoding.com Your Faculty John F. Burns,
Reporting Preventive Services & Problem-Oriented E & M in RHCs John Burns, CPMA, CEMC, CPC, CPC-I Vice President, Audit and Compliance Services John.Burns@RuralHealthCoding.com Your Faculty John F. Burns,
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
CHRONIC CARE MANAGEMENT. A Guide to Medicare s New Move Toward Patient-Centric Care
 CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
The federal guidelines governing the certification of. were published in the Federal Register on July 14, 1978.
 RHC 101: Rules, Regulations and Rumors March 25, 2010 Rules The federal guidelines governing the certification of Rural Health Clinics (RHCs) were published in the Federal Register on July 14, 1978. Proposed
RHC 101: Rules, Regulations and Rumors March 25, 2010 Rules The federal guidelines governing the certification of Rural Health Clinics (RHCs) were published in the Federal Register on July 14, 1978. Proposed
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM. November 20, 2015
 THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
America s Voice for Community Health Care
 America s Voice for Community Health Care The National Association of Community Health Centers (NACHC) represents Community and Migrant Health Centers, as well as Health Care for the Homeless and Public
America s Voice for Community Health Care The National Association of Community Health Centers (NACHC) represents Community and Migrant Health Centers, as well as Health Care for the Homeless and Public
Telehealth 101. Telehealth Summit May 24, 2018
 Telehealth 101 Telehealth Summit May 24, 2018 Tim Bickel Telehealth Director, University of Louisville Deborah Burton, Telehealth Program Manager, KentuckyOne Health, Lexington; Chair, Kentucky Teleheath
Telehealth 101 Telehealth Summit May 24, 2018 Tim Bickel Telehealth Director, University of Louisville Deborah Burton, Telehealth Program Manager, KentuckyOne Health, Lexington; Chair, Kentucky Teleheath
TELEMEDICINE POLICY. Policy Number: ADMINISTRATIVE T0 Effective Date: January 1, 2018
 TELEMEDICINE POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: ADMINISTRATIVE 114.28 T0 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 APPLICABLE LINES
TELEMEDICINE POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: ADMINISTRATIVE 114.28 T0 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 APPLICABLE LINES
Alabama Rural Health Conference 03/25/2010
 1 This resource is not a legal document. This presentation was prepared as a tool to assist our providers. This presentation was current at the time it was created. Although every reasonable effort has
1 This resource is not a legal document. This presentation was prepared as a tool to assist our providers. This presentation was current at the time it was created. Although every reasonable effort has
Super Blue Plus 2000 WVHTC High Option-B (Non-Grandfathered) $200 Deductible
 $200 Deductible") BENEFIT HIGHLIGHTS 1 Super Blue Plus 2000 WVHTC High Option-B (Non-Grandfathered) $200 Group Effective Date December 1, 2017 Benefit Period (used for and Coinsurance limits) January 1 through December
BENEFIT HIGHLIGHTS 1 Super Blue Plus 2000 WVHTC High Option-B (Non-Grandfathered) $200 Group Effective Date December 1, 2017 Benefit Period (used for and Coinsurance limits) January 1 through December
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Care Plan Oversight Services and Physician Services for Certification
 Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
Clinic Specific Coding and Reporting Changes for 2017
 January 2017 Jean C. Russell, MS, RHIT jrussell@epochhealth.com 518-369-4986 Richard Cooley, BS, CCS, rcooley@epochhealth.com 518-430-1144 Matthew H. Lawney, MSPT, MBA, CHC mlawney@epochhealth.com 845-642-6462
January 2017 Jean C. Russell, MS, RHIT jrussell@epochhealth.com 518-369-4986 Richard Cooley, BS, CCS, rcooley@epochhealth.com 518-430-1144 Matthew H. Lawney, MSPT, MBA, CHC mlawney@epochhealth.com 845-642-6462
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
Coding Guidance for HIV Clinical Practices: Care Management Services
 Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
Summary of benefits Health Net. seniority plus green. Benefits effective January 1, 2009 H0562 Medicare Advantage HMO
 2009 Health Net Summary of benefits Los Angeles, Orange, Riverside and San Bernardino counties s effective January 1, 2009 H0562 Medicare Advantage HMO Material ID H0562-09-0041 CMS Approval 9/08 Section
2009 Health Net Summary of benefits Los Angeles, Orange, Riverside and San Bernardino counties s effective January 1, 2009 H0562 Medicare Advantage HMO Material ID H0562-09-0041 CMS Approval 9/08 Section
Payment Methodology. Acute Care Hospital - Inpatient Services
 Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
Grid Medi-Pak Advantage generally reimburses deemed providers the amount they would have received under Original Medicare for Medicare covered services, minus any amounts paid directly by Original Medicare
Compliance Issues under Medicare Prospective Payment for Nursing Facilities. Presented by: Patricia J. Boyer NHA, RN BDO / Heritage Healthcare Group
 Compliance Issues under Medicare Prospective Payment for Nursing Facilities Presented by: Patricia J. Boyer NHA, RN BDO / Heritage Healthcare Group Anyplace where there is no PPS Risk Areas Physician Certification
Compliance Issues under Medicare Prospective Payment for Nursing Facilities Presented by: Patricia J. Boyer NHA, RN BDO / Heritage Healthcare Group Anyplace where there is no PPS Risk Areas Physician Certification
Incident to Billing. Incident-To. Charla Prillaman, CPC, CPCO, CPMA, CPC-I,CCC, CEMC, CHCO Breakout B4, Friday, 9/7/12
 Incident to Billing Incident-To SING REVENUES IN THE BUSINESS OFFICE Charla Prillaman, CPC, CPCO, CPMA, CPC-I,CCC, CEMC, CHCO Breakout B4, Friday, 9/7/12 Today s Objectives Increase understanding of the
Incident to Billing Incident-To SING REVENUES IN THE BUSINESS OFFICE Charla Prillaman, CPC, CPCO, CPMA, CPC-I,CCC, CEMC, CHCO Breakout B4, Friday, 9/7/12 Today s Objectives Increase understanding of the
MEDICARE CARE1ST DUAL PLUS PLAN SUMMARY OF BENEFITS.
 ine 1-800-544-0088 www.care1st.com CARE1ST DUAL PLUS PLAN SUMMARY OF BENEFITS MEDICARE 2009 COUNTIES: LOS ANGELES - ORANGE - SAN BERNARDINO - SAN DIEGO H5928_09_004_SNP_SB 10/2008 Section I Introduction
ine 1-800-544-0088 www.care1st.com CARE1ST DUAL PLUS PLAN SUMMARY OF BENEFITS MEDICARE 2009 COUNTIES: LOS ANGELES - ORANGE - SAN BERNARDINO - SAN DIEGO H5928_09_004_SNP_SB 10/2008 Section I Introduction
UNIVERSITY OF MICHIGAN BZK Effective Date: 01/01/2018
 UNIVERSITY OF MICHIGAN 68712000 0070051870000-06BZK Effective Date: 01/01/2018 This is intended as an easy-to-read summary and provides only a general overview of your benefits. It is not a contract. Additional
UNIVERSITY OF MICHIGAN 68712000 0070051870000-06BZK Effective Date: 01/01/2018 This is intended as an easy-to-read summary and provides only a general overview of your benefits. It is not a contract. Additional
Modifier -25 Significant, Separately Identifiable E/M Service
 Manual: Policy Title: Reimbursement Policy Modifier -25 Significant, Separately Identifiable E/M Service Section: Modifiers Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM028 Last Updated:
Manual: Policy Title: Reimbursement Policy Modifier -25 Significant, Separately Identifiable E/M Service Section: Modifiers Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM028 Last Updated:
RURAL HEALTH CLINIC BASICS GLEN BEUSSINK NATIONAL ASSOCIATION OF RURAL HEALTH CLINIC INDIANAPOLIS FALL INSTITUTE 2017
 RURAL HEALTH CLINIC BASICS GLEN BEUSSINK NATIONAL ASSOCIATION OF RURAL HEALTH CLINIC INDIANAPOLIS FALL INSTITUTE 2017 AGENDA Overview RHC Rules Brainstorming Objectives & Questions and Answers Best Practices
RURAL HEALTH CLINIC BASICS GLEN BEUSSINK NATIONAL ASSOCIATION OF RURAL HEALTH CLINIC INDIANAPOLIS FALL INSTITUTE 2017 AGENDA Overview RHC Rules Brainstorming Objectives & Questions and Answers Best Practices
Summary of Benefits Advantra Freedom PEBTF
 Advantra Freedom is a Medicare Advantage Private Fee-For-Service (PFFS) Plan. This Summary of Benefits tells you some features of our Plan. It doesn't list every service that we cover or list every limitation
Advantra Freedom is a Medicare Advantage Private Fee-For-Service (PFFS) Plan. This Summary of Benefits tells you some features of our Plan. It doesn't list every service that we cover or list every limitation
04/03/2015. Quality Matters: How to Succeed with PQRS in A Short History of PQRS. Participate Or Else..
 Quality Matters: How to Succeed with PQRS in 2015 Jeanne Chamberlin, MA, FACMPE Director, MSOC Health A Short History of PQRS 2007: 3 measures on 80% 2% Bonus 2012: 3 measures on 50% / 80% 0.5% Bonus Performance
Quality Matters: How to Succeed with PQRS in 2015 Jeanne Chamberlin, MA, FACMPE Director, MSOC Health A Short History of PQRS 2007: 3 measures on 80% 2% Bonus 2012: 3 measures on 50% / 80% 0.5% Bonus Performance
CLASSIC BLUE SECURE/BLUE CROSS BLUE SHIELD COMPLEMENTARY Monroe County Benefit Summary/Comparison (Over 65 Retirees)
") WHO IS COVERED Enrollment Requirement Members must be enrolled in both Medicare Parts A and B Members must be enrolled in both Medicare Parts A and B Type of Tier Single only Single only Dependent/Student
WHO IS COVERED Enrollment Requirement Members must be enrolled in both Medicare Parts A and B Members must be enrolled in both Medicare Parts A and B Type of Tier Single only Single only Dependent/Student
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Rural Health Clinic/ Federally Qualified Health Center
 Fee-for-Service Provider Manual Rural Health Clinic/ Federally Qualified Health Center Updated 08.2013 PART II RURAL HEALTH CLINIC AND FEDERALLY QUALIFIED HEALTH CENTER FEE-FOR-SERVICE PROVIDER MANUAL
Fee-for-Service Provider Manual Rural Health Clinic/ Federally Qualified Health Center Updated 08.2013 PART II RURAL HEALTH CLINIC AND FEDERALLY QUALIFIED HEALTH CENTER FEE-FOR-SERVICE PROVIDER MANUAL
Specific Payment Codes for the Federally Qualified Health Center (FQHC) PPS
 PPS") Specific Payment Codes for the Federally Qualified Health Center (FQHC) PPS In accordance with Section 1834(o)(1)(A) and 1834(o)(2)(C) of the Social Security Act, we established specific payment codes
Specific Payment Codes for the Federally Qualified Health Center (FQHC) PPS In accordance with Section 1834(o)(1)(A) and 1834(o)(2)(C) of the Social Security Act, we established specific payment codes
Cotiviti Approved Issues List as of April 27, 2017
 Cotiviti Approved Issues List as of April 27, 2017 Ambulatory Surgery Center (ASC); Outpatient Hospital 23 Inpatient Hospital 25 Inpatient Hospital; Inpatient Psychiatric Facility 27 Inpatient; Outpatient;
Cotiviti Approved Issues List as of April 27, 2017 Ambulatory Surgery Center (ASC); Outpatient Hospital 23 Inpatient Hospital 25 Inpatient Hospital; Inpatient Psychiatric Facility 27 Inpatient; Outpatient;
BCBSM provides administrative claims services only. Your employer or plan sponsor is financially responsible for claims.
 Michigan Catholic Conference Group Number: 71755 Package Code(s): 010 Section Code(s): 1000, 2000 PPO - PPO1, Hearing, Vision ( Exam only) Effective Date: 01/01/2018 Benefits-at-a-glance This is intended
Michigan Catholic Conference Group Number: 71755 Package Code(s): 010 Section Code(s): 1000, 2000 PPO - PPO1, Hearing, Vision ( Exam only) Effective Date: 01/01/2018 Benefits-at-a-glance This is intended
Telehealth and Telemedicine Policy
 Telehealth and Telemedicine Policy Policy Number Annual Approval Date 7/11/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Telehealth and Telemedicine Policy Policy Number Annual Approval Date 7/11/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Summary of Benefits for SmartValue Classic (PFFS)
") Summary of Benefits for SmartValue Classic (PFFS) Available in Select Counties in Nevada A health plan with a Medicare contract. Rocky Mountain Hospital and Medical Service, Inc. has contracted with the
Summary of Benefits for SmartValue Classic (PFFS) Available in Select Counties in Nevada A health plan with a Medicare contract. Rocky Mountain Hospital and Medical Service, Inc. has contracted with the
Hospital Refresher Workshop. Presented by The Department of Social Services & HP Enterprise Services
 Hospital Refresher Workshop Presented by The Department of Social Services & HP Enterprise Services 1 Training Topics Provider Bulletins Outpatient Claim Billing Changes Explanation of Benefit Codes Web
Hospital Refresher Workshop Presented by The Department of Social Services & HP Enterprise Services 1 Training Topics Provider Bulletins Outpatient Claim Billing Changes Explanation of Benefit Codes Web
99 - No response error No Medical records were received.
 1 May 2017 HCPCS Code Type Error Error Identified by CERT Anesthesia Services 00140 MISSING: 1) Signature attestation statement or signature log for the illegibly signed Pre-Anesthesia evaluation and illegibly
1 May 2017 HCPCS Code Type Error Error Identified by CERT Anesthesia Services 00140 MISSING: 1) Signature attestation statement or signature log for the illegibly signed Pre-Anesthesia evaluation and illegibly
More than a Century of Legal Experience
 Advanced Beneficiary Notice (ABN) and Hospital Issued Notice of Non Coverage(HINN): To Issue, or Not to Issue an ABN or HINN July 30, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience
Advanced Beneficiary Notice (ABN) and Hospital Issued Notice of Non Coverage(HINN): To Issue, or Not to Issue an ABN or HINN July 30, 2013 Presented by: Jennifer McManis More than a Century of Legal Experience
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
TIPS FROM OUR CONSULTANT By: Joy Newby, LPN, CPC, PCS Newby Consulting
 TIPS FROM OUR CONSULTANT By: Joy Newby, LPN, CPC, PCS Newby Consulting CONFUSED ABOUT MEDICARE PREVENTATIVE VISITS? SO ARE YOUR PATIENTS! Congress legislated coverage for two preventive visits for Medicare
TIPS FROM OUR CONSULTANT By: Joy Newby, LPN, CPC, PCS Newby Consulting CONFUSED ABOUT MEDICARE PREVENTATIVE VISITS? SO ARE YOUR PATIENTS! Congress legislated coverage for two preventive visits for Medicare
MEDICAL POLICY No R2 TELEMEDICINE
 Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Chapter 9 Section 1. Ambulatory Surgical Center (ASC) Reimbursement
 Reimbursement") Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Core Services Provided in Federally Clinical Coverage Policy No: 1D-4 Qualified Health Centers and Amended Date: October 1, 2015 Rural Health Clinics
 Qualified Health Centers and Amended Date: October 1, 2015 Rural Health Clinics Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Federally Qualified Health Centers... 1
Qualified Health Centers and Amended Date: October 1, 2015 Rural Health Clinics Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Federally Qualified Health Centers... 1
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications
 Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications Complete and correct coding of claims will become more important, and will have an effect on claim payment. The
Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications Complete and correct coding of claims will become more important, and will have an effect on claim payment. The
HealthPartners Freedom Plan (Cost) 2011 Medical Summary of Benefits Wisconsin
 2011 Medical Summary of Benefits Wisconsin") HealthPartners Freedom Plan 2011 Medical Summary of Benefits Wisconsin HealthPartners Wisconsin Freedom Plan I HealthPartners Wisconsin Freedom Plan II 420421 (10/10) H2462_SB WI_151 CMS Approved 10/5/10
HealthPartners Freedom Plan 2011 Medical Summary of Benefits Wisconsin HealthPartners Wisconsin Freedom Plan I HealthPartners Wisconsin Freedom Plan II 420421 (10/10) H2462_SB WI_151 CMS Approved 10/5/10
Tips for Completing the UB04 (CMS-1450) Claim Form
 Claim Form") Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
The New Medicare PPS For FQHCS. Norma Mendilian, CPA Director of Healthcare Consulting and Reimbursement
 The New Medicare PPS For FQHCS Norma Mendilian, CPA Director of Healthcare Consulting and Reimbursement 508.450.6572 nmendilian@aafcpa.com Health Centers Medicare Program While the Medicare program constitutes
The New Medicare PPS For FQHCS Norma Mendilian, CPA Director of Healthcare Consulting and Reimbursement 508.450.6572 nmendilian@aafcpa.com Health Centers Medicare Program While the Medicare program constitutes
The MITRE Corporation Plan
 Benefit Type Plan Year Type Calendar Year Annual Medical Out of (for certain services) Employee Employee + 1 Family Annual Prescription Drug Out of Employee Employee + 1 Family Copayments: One copay per
Benefit Type Plan Year Type Calendar Year Annual Medical Out of (for certain services) Employee Employee + 1 Family Annual Prescription Drug Out of Employee Employee + 1 Family Copayments: One copay per
9/21/2017. Telemedicine vs. Telehealth. Telemedicine vs. Telehealth. Telemedicine vs. Telehealth. Time is Money. Disruptive Technology
 Telemedicine vs. Telehealth Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients health status. Telemedicine The Virtual Experience
Telemedicine vs. Telehealth Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients health status. Telemedicine The Virtual Experience
Global Surgery Fact Sheet
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Global Surgery Fact Sheet Definition of a Global Surgical Package This fact sheet is designed to provide education on the
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Global Surgery Fact Sheet Definition of a Global Surgical Package This fact sheet is designed to provide education on the
MLN Matters Number: MM6699 Related Change Request (CR) #: 6699
 #: 6699") News Flash Medicare will cover immunizations for H1N1 influenza also called the "swine flu." There will be no coinsurance or copayment applied to this benefit, and beneficiaries will not have to meet their
News Flash Medicare will cover immunizations for H1N1 influenza also called the "swine flu." There will be no coinsurance or copayment applied to this benefit, and beneficiaries will not have to meet their
Provider-Based: What Is It?
 Compliance Risks for Provider-Based and Other Hospital-Based Provider Services 2015 HCCA Compliance Institute Presented by Regan E. Tankersley, Esq. Hall, Render, Killian, Heath & Lyman, P.C. Paul W. Kim,
Compliance Risks for Provider-Based and Other Hospital-Based Provider Services 2015 HCCA Compliance Institute Presented by Regan E. Tankersley, Esq. Hall, Render, Killian, Heath & Lyman, P.C. Paul W. Kim,
MEDICAL POLICY No R1 TELEMEDICINE
 Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Reimbursement for Anticoagulation Services
 Journal of Thrombosis and Thrombolysis 12(1), 73 79, 2001. # 2002 Kluwer Academic Publishers, Manufactured in The Netherlands. Reimbursement for Anticoagulation Services Paul W. Radensky McDermott, Will
Journal of Thrombosis and Thrombolysis 12(1), 73 79, 2001. # 2002 Kluwer Academic Publishers, Manufactured in The Netherlands. Reimbursement for Anticoagulation Services Paul W. Radensky McDermott, Will
NCD for Routine Costs in Clinical Trials (310.1)
") NCD for Routine Costs in Clinical Trials (310.1) Publication Number 100-3 Manual Section Number 310.1 Version Number 2 Effective Date of this Version 7/9/2007 Implementation Date 10/9/2007 Benefit Category
NCD for Routine Costs in Clinical Trials (310.1) Publication Number 100-3 Manual Section Number 310.1 Version Number 2 Effective Date of this Version 7/9/2007 Implementation Date 10/9/2007 Benefit Category