2017 Optional State Supplementation (OSS) Program
|
|
|
- Magnus Watts
- 6 years ago
- Views:
Transcription
 Program SCDHHS Community and")

1 2017 Optional State Supplementation (OSS) Program SCDHHS Community and Facility Services PO Box Main 1 Street Columbia, SC
2 SCDHHS Department Roles & Contact Numbers Resident s Medicaid Status Eligibility Approve or Deny OSS application Initiate CRCF-01 form and Cost of Living Adjustment (COLA) forms Provide answers for eligibility questions OSS or OSCAP Polices OSS Program Staff Develop policies Daily operations of budget, training, rates OSCAP contracts Update facility information Provider Enrollment/Provider Service Center Update address, telephone numbers, etc. Direct Deposit Change of Ownership option 4 Billing/payment information Medicaid Claims Control System (MCCS) TAD questions Edit Codes questions Billings/payment questions Register for training option 3 2
3 Nurses Consultants Vacant Counties: Lancaster, Marlboro, Chesterfield, Horry, Florence, Darlington, Dillon, Marion Jai-Netta Montgomery, RN (803) Counties: Aiken, Lexington, Richland, Fairfield, Chester, York, Edgefield Sandra Jones, RN (803) Counties: Williamsburg, Georgetown, Berkeley, Dorchester, Colleton, Jasper, Hampton, Allendale, Barnwell, Charleston, Beaufort Charlena Hunter, RN (803) Counties: Bamberg, Orangeburg, Calhoun, Clarendon, Sumter, Lee, Kershaw Darlene Newton, RN (864) Counties: Oconee, Pickens, Greenville, Anderson, Abbeville, McCormick Quantina Williams, RN (864) Counties: Spartanburg, Cherokee, Union, Laurens, Newberry, Greenwood, Saluda 3
4 Program Contact Information Terrell McMorris, MSW OSS Program Coordinator Office: (803) Candice Smith-Byrd, CPC Quality Assurance Manager Office: (803) Alexis Martin, MBA, CPM OSS Program Manager Office: (803)
/Social Security Administration (SSA)].")
5 WHAT IS OPTIONAL STATE SUPPLEMENTATION (OSS)? OSS is an entitlement program that is a state supplement to a person s Security Income [Supplemental Security Income (SSI)/Social Security Administration (SSA)]. The South Carolina Department of Health and Human Services (SCDHHS) pays the difference between the OSS rate and the Social Security payment. The purpose of this program is to provide reimbursement to enrolled CRCFs (also known as Assisted Living Facilities) that provide room and board and a degree of personal care for eligible consumers. OSS is NOT a Medicaid program; it is funded at 100% state funding. 5
6 OSS Program Facilities must accept the OSS entitlement amount as payment in full. Facilities may not charge a resident or a resident s family for any difference over and above the OSS entitlement amount even if the family is willing to pay the difference for a private room. The additional payment would be considered income for the resident and could make the resident ineligible for OSS due to income limitations. 6
7 Resident Assessments Medical assessments are required for all OSS and OSCAP participants. Assessments will be performed by a SCDHHS nurse at the CRCF where the residents reside. The resident s assessment will occur after admission into the facility and every 24 months thereafter for OSS residents and every 18 months for OSCAP residents. 7

8 Questions. What is Optional State Supplementation? What agency is responsible for Optional State Supplementation? 8

9 OSS Steps for New Admission
10 Step 1: Who is OSS Eligible? Be 65 years or older, or 18 years of age or older and blind or disabled Be a U.S. citizen or qualified noncitizen Have a Social Security number or file for one File for any other benefits to which they may be entitled Effective January 1, 2017 meet net income limit of $1,420 Can t exceed resource limit of $2,000 for an individual QUICK FACTS Number of Consumers 3,338 (OSS & OSCAP) 49% Female & 51% Male Average Age: 63 CRCF Medicaid enrolled facilities: 313 Average Income: $811 Recurring Income : SSA: 43% SSI: 59% Top 5 Primary Diagnoses 1. Hypertension 2. Schizophrenia 3. Diabetes 4. Hyperlipidemia 5. Dementia 10
.")
11 Step 2: OSS Check Eligibility 5. Enter the one of the following in the fields indicated: Medicaid I.D.; SSN and Date of Birth; or Name and Date of Birth along with the Date of Service (auto populates with today s date). Note: The Web Tool will return SSN information only if you search eligibility using SSN. 1. Visit The Web Tool 2. Enter your username and password 3. From the Menu, click Eligibility, 4. From the submenu choose Single Query, to retrieve the Eligibility Verification Inquiry screen. 6. Click the Check Eligibility button. The Eligibility Verification Inquiry: Selection Summary screen will appear. Place a check mark in the box beside the beneficiary s Medicaid ID number. 7. Click the Display button. The Eligibility Verification Results screen will appear which contains the eligibility information of the beneficiary in question. If you wish to check eligibility for another recipient, click the Back link. This will return you to the original screen. If you wish to add this individual to your Beneficiary List, click the Add Beneficiary link. 11
12 Step 3: What documentation is needed when completing an OSS application? Forms 3401 No active Medicaid 3400A has active Medicaid t/files/fm% pdf 1728 is receiving SSI only Send Medicaid Eligibility Applications to: Fax: or Mail: SCDHHS Central Mail PO Box Columbia, SC day bank statement from previous month 2. Life Insurance policy (cash value and dividends) as of the 1st of the month 3. Burial Contract 4. Signed Authorized Representative form (Form 1282) 5. Client has to sign Form 943 (Information for Release Form) 6. Health Insurance Card (Medicare, VA, Pension) and award amounts 7. Current recurring income amount from SSA/Pension 8. Property owner have correct address and tax notice (intent to return home) 12
13 LTC Workers List of Long Term Care Coordinators (LTCCs) responsible for serving counties identified in their region throughout the state. Region LTC Worker Phone Number 1 Blue Teena Bixler BixlerT@scdhhs.gov Blue Kathi Dixon DixonK@scdhhs.gov The state is divided into four (4) regions. 2- Orange Leighann Pfannestiel Pfannla@scdhhs.gov To determine your points of contact, use the following map and identify the county in which your facility is located. Next, locate your LTCCs as listed. For example, if your facility is located in Richland County, you should contact our Region 2 team, Leighann and Melanie 2 Orange Melanie Turner TurnerMe@scdhhs.gov Green Perry Foss Foss@scdhhs.gov Green JoAnn Kearse KearseJ@scdhhs.gov Red LaRonna Bryant Faulklar@scdhhs.gov x47 4- Red Meko Williams willmeko@scdhhs.gov x229 13

14
15 Contacting Eligibility When you need to know the status of an OSS application please call Inform the customer service representative you are calling to check on the OSS status and give them the date in which you applied. The OSS program area cannot provide you with the status of your application. 15
16 Added Fax number to CRCF-02 Form Step 4: CRCF-02 Form

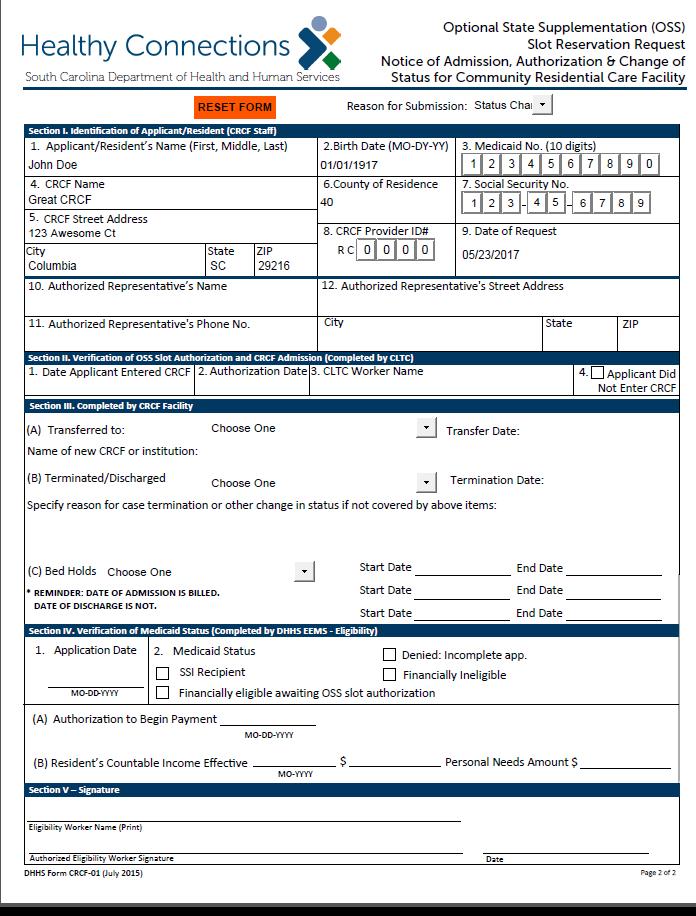
17 Step 5: Initial CRCF-01 Form Happy Feet Happy Feet 17
18 Step 6: Add Resident to TAD John Doe /17 28 The Initial CRCF 01 form must be attached to the monthly Turn Around Document (TAD) and add the new resident s name to the last page of the TAD. A copy is kept for the facility s files. 18


19 Current Resident Status Change Steps
20 When an OSS resident transfers To your facility from another CRCF? 1. Verify that the resident is already participating in the OSS program by checking Web Tool. 2. Complete a Status Change CRCF-01 Form. Complete Section I and submit to Terrell McMorris at Terrell.McMorris@scdhhs.gov or Fax to Allow 5 business days for a return forms. Please keep a copy for your records. 20
21
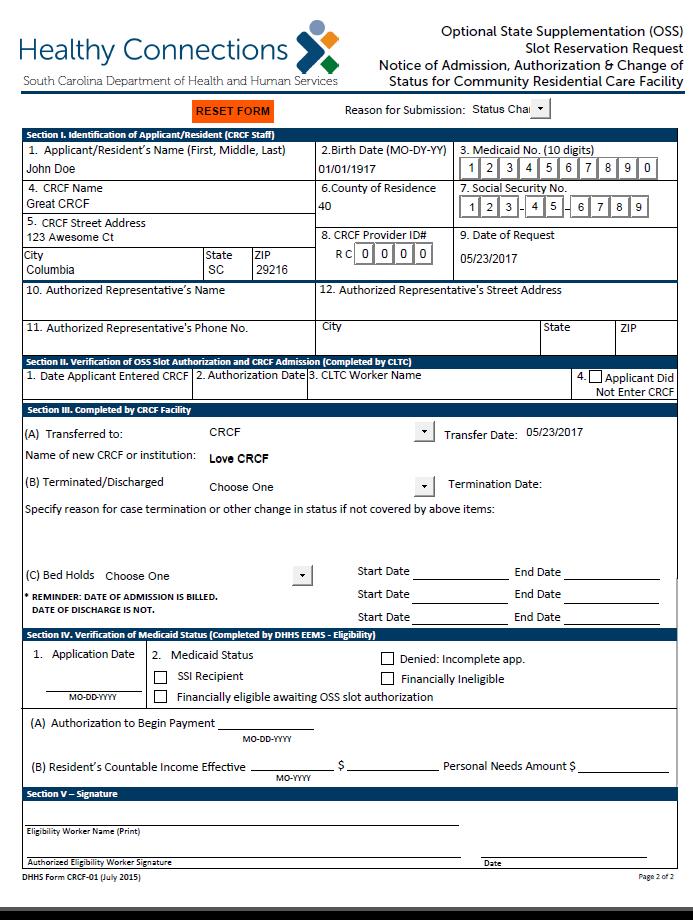
22 When an OSS resident transfers From your facility to another CRCF? Complete the following steps: 1. Complete a Status Change CRCF-01 Form Sections I and III. 2. Send the CRCF-01 form to Ms. Terrell McMorris via at Terrell.McMorris@scdhhs.gov or fax to Once a signed CRCF-01 Form is received, remove the resident s name from the TAD by placing an X in the delete column on the TAD and submit a copy of the signed CRCF-01 Form. 22
23
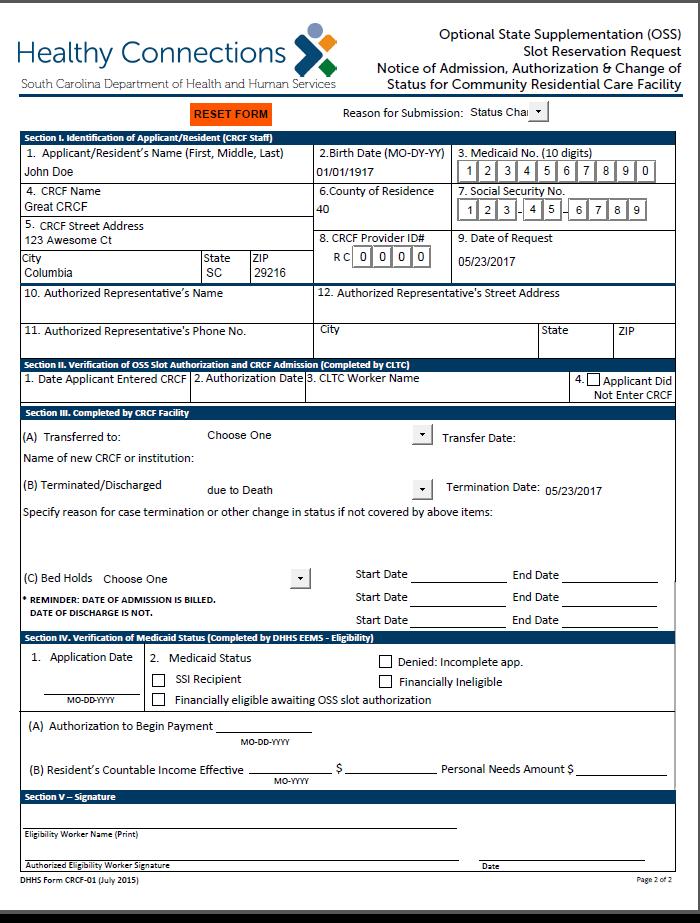
24 When a resident terminates from your facility 1. Complete the CRCF-01 Form Sections I and III (B). 2. Select the reason for termination and enter the date of termination. 3. Submit a copy of this form with your TAD and place an X in the delete column on the TAD and fax copy to eligibility department No Signature is needed for terminations on the CRCF-01 Form.
25

26 Income Change Happy Feet 06/07/17 26
27 Optional Supplemental Care For Assisted Living Participants OSCAP 27
28 What is Optional Supplemental Care For Assisted Living Participants? The Optional Supplemental Care For Assisted Living Participants (OSCAP) service provides additional reimbursement to facilities that provide assistance with personal care for OSS residents who meet the medical criteria required for participation. OSCAP gives additional reimbursement of $207 per month for each qualified resident. Current OSCAP rate is $1, 627
29 Step 1: Does my OSS resident meet the Medical Necessity Criteria? Two (2) functional dependencies One (1) cognitive and one (1) functional dependency Limited assistance with two (2) or more Activities of Daily Living (ADLs) Limited assistance with one (1) or more ADLs in addition to a cognitive impairment 29


30 How to apply for OSCAP? 1. Must be OSS approved before you can apply for OSCAP. 2. To complete OSCAP referral visit: _referrals/new 3. When applying for OSCAP, select OSS as the Reason for Referral. In the comment box type OSCAP. * OSCAP has not been added as a reason for referral. The correct choice is OSS, but be sure to enter OSCAP in the comment box. Any questions??? Best way to access referral is to google search CLTC electronic referral and select the option with Phoenix in the description. 30
31 What will the DHHS Nurse need to complete the OSCAP Assessment? A SCDHHS nurse will visit your facility to assess referred OSS participants for OSCAP. The SCDHHS nurse will need: Copy of Medication Administration Report (MAR)/Physicians Orders Copy of Individual Care Plan (ICP) Resident s chart Recent height, weight, and vital signs Interview with direct care staff Interview resident OSCAP assessments are every 18 months, unless there is a change in the level of care. 31
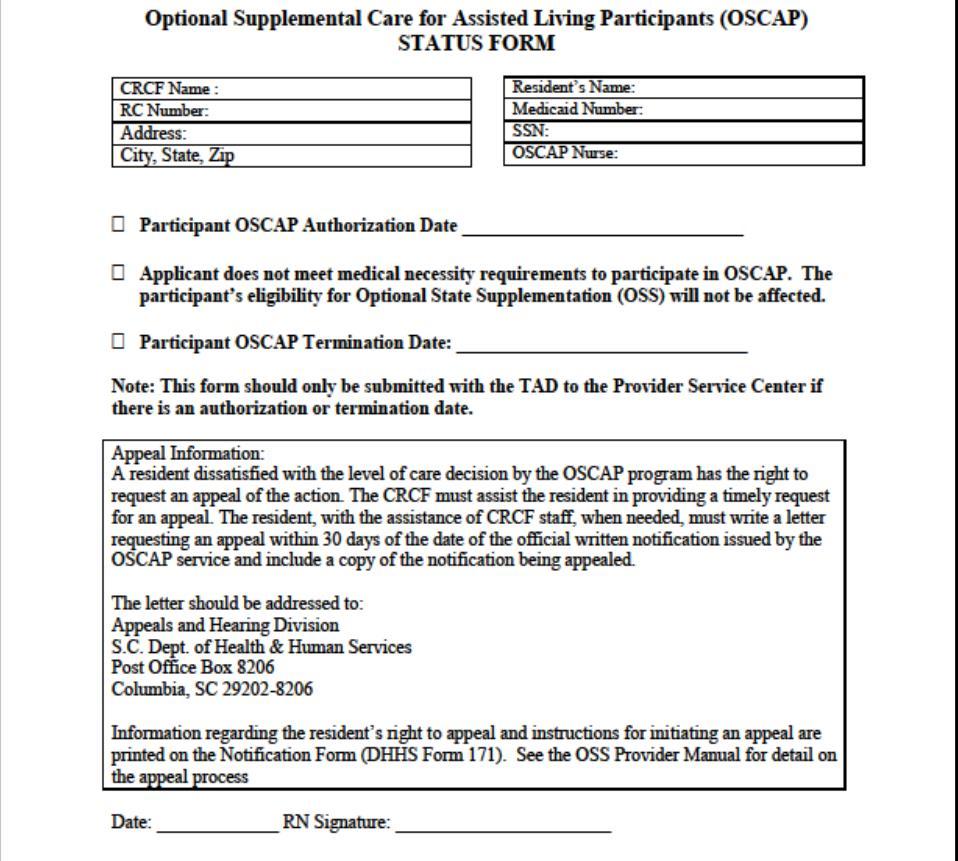
32 Status Change Form When should I expect to receive the Status Change Form? The SCDHHS nurse for your region will send the form following her assessment via fax, , or USPS mail. Do I attach this form to my TAD? You only attach the status form to the TAD if there is an authorization or termination date. A copy should be kept for your records. Should I keep a copy? A copy of the most current status form must be kept in the participant s record.
33
34 Service Plan A service plan will be individualized for each OSCAP participant by the SCDHHS nurse. Service plans will be mailed, ed, or faxed to the facility following the assessment and level of care determination. Service plan must be used as guidance to revise individual care plans and to create the Resident Monthly Task Log. A copy must be kept in the resident s file and available to any SCDHHS staff upon request. 34
35 Service Plan 35
36 Service Plan This section is used to complete the Resident Monthly Task Log
37 OSCAP Task Logs The initial OSCAP Task Log must be created by the CRCF licensed nurse. The CRCF nurse must review, revise, sign and date each monthly task log at least every 90 days. Must be completed on all OSCAP residents and kept on record. All direct care staff in contact with residents must initial all completed tasks. Administrator or designee must sign and date weekly. CRCF nurse must write a detailed nurse s note/summary every three (3) months including: height, weight, vital signs, functional/cognitive dependencies, any behavioral problems and any medical complications following face to face interaction. 37

38 Dressing Bathing Locomotion Transfer Level Name: Room No. Medicaid No. Year: 2017 Month: July Activity Lifted manually/mechanically Transfer aid Weight bearing Wheelchair/Cane/Walker x Other person wheels Put on prosthesis or brace Wandering Does not bathe appropriately In/out of tub/shower Lower body/upper body x Cueing Buttons/zippers/snaps/tying Inappropriate dressing/layers Step by step guidance x Refuses to change/reapplies dirty Put on socks/shoes Resident Monthly Task Log John Resident E L L Level of Care Key: L = Limited E= Extensive T=Total
39 Diet Cognitive Bladder & Bowel Resident Monthly Task Log All direct care staff in contact with resident should initial all completed tasks. Scheduled toileting plan Pads/briefs used Bowel program Memory problem(s) Decision making capacity Mood problem(s) Behavior problem(s) Good (75%) Fair (50%) Poor (25%) Refused Supplements Level of Care Key: L = Limited E= Extensive T=Total Signatures and Initials of all Resident Assistants providing assistance this month. Initials Signatures Initials Signatures DD x Donald Duck L DD DD DD
40 Weight & Vital Signs Resident Monthly Task Log Date & Results Date & Results Date & Results Date & Results Date & Results Date & Results Weight Blood Pressure Temperature Pulse Respiration Sugar Monitoring I certify the information on this form is correct and documented services were provided. The Administrators CRCF Signature: nurse must write a detailed nurse s Week 1 Date: note/summary Administrators Signature: Week 2 Date: every 3 months including: height, weight, vital signs, Administrators Signature: Week 3 Date: Administrators Signature: Week 4 Date: functional/cognitive dependencies, any behavioral problems I certify the information on this form is correct and documented services were provided. and any medical complications following face to face interaction. Nurse Signature: Date: Progress Note(s) Please date and initial each note.
41 Individual Care Plans (ICP) Must be in each resident s file/chart. Must be reviewed and updated every six (6) months. No changes is an unacceptable update. All ICPs/six (6) month review must be reviewed, updated, signed and dated by the CRCF nurse. Must be signed by the administrator, resident, or the responsible party/sponsoring agency. If the resident is unable to sign, then an explanation must be written on the ICP. Must be reflective of the resident s service category (OSCAP, OSS, Hospice, waiver) and current condition. Redeveloped at least every 24 months from the date of the initial ICP. 41
42 Individual Care Plans (ICP) 42

43 Individual Care Plans (ICP) John C. Resident Resident Signature Date: Responsible Party/Sponsor Facility Representative [ ] Family chose not to participate Janie Administrator / Nurse Betty,RN - DATE Sent letter on (copy attached) or Called on & spoke with
44 Individual Care Plans (ICP) INDIVIDUAL CARE PLAN REVIEW [ ] Six (6) Month Review [ ] Change in Need Comments: No changes is not an acceptable update. John C. Resident Resident Signature DATE Date: Responsible Party/Sponsor Janie Administrator / Nurse Betty,RN - DATE Facility Representative Sent letter on or Called on & spoke with 44
45 CRCF Nurse Duties OSCAP approved facilities are require to employ or contract with a licensed nurse (either a Licensed Practical Nurse or and Registered Nurse). The ICP must be reviewed, revised or updated, signed and dated by the nurse every at least every six (6) months. The initial Monthly Task Log must be created by the CRCF nurse. The CRCF nurse must review, sign and date all Monthly Task Logs at least every 90 days. Revisions to the Monthly Task Logs must be made by the CRCF Nurse as needed. The Nurse must sign and date the Monthly Task Logs when revisions/updates are made. 45
46 CRCF Nurse Duties The staff person responsible for supervision of direct care staff in the CRCF nurse s absence should be trained and determined competent and capable by the CRCF nurse. A quarterly summary of each OSCAP participant in the CRCF must be written, dated, and signed by the CRCF nurse, following a face to face evaluation of the resident. The summary must include: vitals, weight, functional/cognitive dependencies, any behavioral problems, and medical complications. All CRCF nurses are required to attend any scheduled OSCAP trainings or meetings provided by SCDHHS. 46
47 OSCAP and Hospice Services Beneficiaries of Hospice and OSCAP may only receive personal care through one service or the other; therefore, they must choose either Hospice or OSCAP. An OSCAP participant residing in a CRCF has the right to choose which service they receive. 47
48 OSCAP Provider Requirements Licensure in good standing by the South Carolina Department of Health and Environmental Control (SCDHEC) OSS Participation Agreement Facility documentation of resident funds and PNA Facility notification to the SCDHHS and MCCS of admissions, discharges, transfers, and deaths within 72 hours Monthly processing of the OSS payments Meet specific basic requirements of the Americans with Disabilities Act (ADA) including wheelchair accessibility Have a minimum of six (6) hours relevant inservice training per calendar year, in addition to SCDHEC required training Must designate, in writing, a licensed full time facility administrator and an administrator s designee Must notify SCDHHS within 10 business days in the event of a change in the administrator, OSCAP nurse, address, phone number, or an extended absence of the administrator Ensure the nurse is in good standing with the South Carolina Board of Nursing Ensure that resident to staff ratios are consistent with SCDHEC regulation at all times The facility must not be without nursing coverage for more than 90 days

49 Questions.. How are OSCAP services documented? How often must the CRCF nurse review, sign and date all Monthly Task Logs? 49
50 OSS & OSCAP Billing & Payment 50
51 Rates for 2017 Date of Service Payment Date OSS and OSCAP Rates OSS Rate : $1,420 PNA: $67 Facility Payment: $ 1,353 per month OSCAP Rate: $1,627 PNA: $67 Facility Payment: $1,560 per month January 2017 March 03, 2017 February 2017 April 7,2017 March 2017 May 5, 2017 April 2017 June 2, 2017 May 2017 July 7, 2017 June 2017 August 4, 2017 July 2017 September 1, 2017 August 2017 October 6, 2017 September 2017 November 3, 2017 October 2017 December 1, 2017 November 2017 January 5, December 2017 February 2, 2018
52 Personal Needs Allowance OSS beneficiaries who receive recurring income of SSI only are allowed to keep $67 per month for personal needs. Eligible beneficiaries who have income other than SSI are allowed to keep an extra $20 for personal needs, bringing their total to $87. PNA increases by $2 each year, if there is a COLA. Please refer to the CRCF-01 for each beneficiary to determine their PNA amount. 52
53 TAD Reminders Changes to the TAD, MUST be submitted with a CRCF-01 Form to support the action made on the TAD. OSS providers have 13 months from the date of the signed CRCF-01 Form to submit the form for billing. Any forms past the 13 month timeframe may not be processed. Failure to submit a CRCF-01 Form could result in delayed payment. Don t send CRCF-01 form in with TAD until you have completed the form from eligibility with effective date, recurring income, PNA amount, signature and date. Please verify the mailing address on the TAD to ensure the address is correct. If the address is incorrect, please contact Terrell McMorris at Terrell.McMorris@scdhhs.gov with the correct information. 53
54 TAD Mailing Address Claims Receipt CRCF Claims Section Post Office Box 67 Columbia, SC All TADs and signed CRCF-01 Forms, to include termination forms, must be sent to the address above. If your facility has not received a TAD by the second Friday in the month, you will need to contact the Provider Service Center. Please remember to submit your TAD no later than 17th of each month. PSC option 3 54
55 Daily Census This component includes documenting the daily census of all residents, regardless of pay source. The documentation must include identifiers for Medicaid participants and specify whether the participant was on medical or non-medical bed hold, admitted or discharged on that date, or was transported for emergency treatment. 55


56 Questions Where does the resident s personal needs allowance come from? What form(s) is used to communicate an OSS beneficiary s status in your facility? 56


57 OSS Quality Assurance
58 SCDHHS OSS QA Reminders Providers must meet licensing requirements as outlined in the South Carolina Department of Health and Environmental Control Regulation Providers must meet all requirements as outlined in the South Carolina Department of Health and Human Services Optional State Supplementation Manual. 58
59 Business License Every city in South Carolina requires for businesses operating in the city to obtain a business license. (There may be some exception for non-profits). County requirements vary. If your facility does not maintain a business license, please inquire if one is required (and obtain if appropriate). 59

60 Questions According to SCDHHS policy, how often must employee background checks be completed? Who cannot be hired? 60
61 Background checks are required for all employees prior to employment then at least every 5 years thereafter. -Cannot hire or have employed anyone who has a felony conviction within the last 10 years. -Stipulations for potential employees or employees with misdemeanor convictions are outlined in your Optional State Supplementation Provider Manual (Section 2, page 18). 61
62 Working Capital Working capital is the funds available for the operations of a business. It allows the Community Residential Care Facility to perform its day-to-day activities and meet its functional requirements. (Optional State Supplementation Provider Manual Section 2, page 15). The minimum working capital levels are: 4-10 Beds - $2, Beds - $5, and above $10,000 A statement from your financial institution will be required noting the minimum average balance maintained in the account. 62

63 Questions For a new admission, how long does the facility have to complete an initial assessment? Initial Individual Care Plan? 63
64 SCDHEC Regulation Based on provider reviews, Individual Care Plans are being completed prior to the initial assessment Assessment (II). A written assessment of the resident in accordance with Section 101.H shall be conducted by a direct care staff member as evidenced by his or her signature and date within a time-period determined by the facility, but no later than 72 hours after admission Individual Care Plan (II). A. Using the written assessment, the facility shall develop within seven (7) days of admission an ICP with participation of the resident, administrator (or designee), and/or the sponsor or responsible party when appropriate, as evidenced by their signatures and date. The ICP shall be reviewed and/or revised as changes in resident needs occur, but not less than semi-annually with the resident, administrator (or designee), and/or the sponsor or responsible party as evidenced by their signatures and date. 64
65 Personal Needs Allowance Specified in the Optional State Supplementation Provider Manual, Section 2, page 3 and in the SCDHEC Regulation 61-84, Section Signed and dated agreement from the beneficiary allowing the facility to manage his/her personal needs allowance. 2-The beneficiary must sign upon receiving personal needs allowance or prior to any purchase made on behalf of the resident. The date of the transaction must be present as well as the cash amount. If the beneficiary is unable to sign, the facility must have a policy in place regarding confirming personal needs allowance was given to the beneficiary. 3-Maintain receipts for all purchases made on behalf of the beneficiary. 4-Provide a quarterly report of the account balance to the beneficiary. 65
66 Personal Needs Allowance Why is the allowance documentation necessary? Financial exploitation and embezzlement are a serious matter. Allegations of embezzlement are referred to the Attorney General s Medicaid Fraud Control Unit. 66
67 Personal Needs Allowance Documentation Example Personal Needs Allowance Date Received Withdrawal Notes Balance Signature 1/1/2017 $87.00 $87.00 cash to resident $0.00 John Doe 2/1/2017 $87.00 $25.00 cash to resident $62.00 John Doe 2/15/2017 $0.00 $10.00 XYZ Pharmacy $52.00 John Doe 2/20/2017 $0.00 $15.00 Bobs Barber Shop $37.00 John Doe 3/1/2017 $87.00 $25.00 cash to resident $99.00 John Doe I authorize XYZ CRCF Administrator to maintain my personal needs allowance. John Doe 12/15/2016 XYZ Administrator- Jane Smith 12/15/2016 * Signatures are to be original 67
68 Billing Inaccuracies One provider owning multiple facilities moving residents from facility to facility but not completing appropriate forms for termination and transfer. This often causes payments to the facility in which the resident was not present. Payments must go to the provider of service (where the resident was residing). Even if this will be partial months to multiple facilities. Instances where the facility goes through a change of ownership that has not been approved by SCDHHS which results in a sharing of OSS/OSCAP payments with a non-enrolled SCDHHS facility will be referred to SCDHHS Division of Program Integrity and/or the Medicaid Fraud Control Unit of the SC Attorney General s Office. 68


69 Question Can a facility continue to receive payments for OSCAP services if the resident is not present at the facility (bed hold)? 69
70 Reimbursement for OSCAP services is not allowed for any absence from the CRCF; payment reverts to the OSS rate for any days the resident is away from the facility. (Optional State Supplementation Provider Manual Section 2, page 6). 70
71 OSCAP Provider Responsibilities The CRCF must maintain liability insurance to protect all paid and volunteer staff, including board members, from liability incurred while acting on behalf of the CRCF during the life of the OSCAP contract. The CRCF must furnish a copy of the insurance policy to SCDHHS upon request. (Optional State Supplementation Provider Manual Section 2, page 17). Providers must maintain a section in its existing policy and procedure manual describing the provision of OSCAP services. (Optional State Supplementation Provider Manual, Section 2, pages 28-30). -The OSCAP section of the facility s policy and procedure manual must be descriptive. Printing the pages out of the Optional State Supplementation Provider Manual and placing in the facility s policy and procedure manual will not be accepted. 71
72 Incontinence Supplies Incontinence Supplies (IS) referrals are made to SCDHHS. The referral is processed to determine if the participant meets the criteria for receiving the service(s). This includes a telephone assessment to determine whether the appropriate medical necessity criteria are met. 72
73 Incontinence Supplies Provider Choice Forms (PCF) CRCFs must discuss the provider choices with residents in their facility and let residents select the five (5) providers they would like to deliver their IS. The PCF Form must be returned to SCDHHS. Physician Certificate Effective July 1, 2014, Incontinence Supply providers will be responsible for obtaining the Physician Certification of Incontinence SCDHHS Form 168IS prior to delivering IS. Service Contact: Shanese Mathis

74 Bed Locator 74
75 Bed Locator If you are looking for a facility that accepts residents/patients please visit the Nursing Home Bed Locator website at ALL OSS providers must update their bed availability information at a minimum of ONCE PER MONTH at the South Carolina Long Term Care Bed Locator website Failure to report in a timely manner could result in sanctions against the facility. 75
76 Bed Locator: Steps All licensed CRCFs are listed on the South Carolina Long Term Care Bed Locator website. To update your facility information please follow the steps listed below: In order to create an account, users must go to the top right corner of the webpage and press the login button, which will take users to another page. On the new page, click on the blue hyperlink that says Register Here. This will take users to a new page where they can choose a user name, password of at least eight (8) characters, and their address. Under User Comments, users should enter the facility or facilities that they want to be associated with. Please note that in order to register, users MUST have an address. 76
77 Questions 77


78
JOB DEVELOPMENT CREDIT
 SCEDA ECONOMIC DEVELOPMENT 101 May 8, 2014 NEXSEN PRUET April C. Lucas Tushar V. Chikhliker Nexsen Pruet, LLC Nexsen Pruet, LLC 1230 Main Street, Suite 700 1230 Main Street, Suite 700 Columbia, SC 29201
SCEDA ECONOMIC DEVELOPMENT 101 May 8, 2014 NEXSEN PRUET April C. Lucas Tushar V. Chikhliker Nexsen Pruet, LLC Nexsen Pruet, LLC 1230 Main Street, Suite 700 1230 Main Street, Suite 700 Columbia, SC 29201
BlueChoice HealthPlan Medicaid An Overview Community Outreach Perspective
 BlueChoice HealthPlan Medicaid An Overview Community Outreach Perspective 1 BlueChoice HealthPlan Medicaid In the Communities We Serve! 2 BlueChoice HealthPlan Medicaid Our focus is on preventive care.
BlueChoice HealthPlan Medicaid An Overview Community Outreach Perspective 1 BlueChoice HealthPlan Medicaid In the Communities We Serve! 2 BlueChoice HealthPlan Medicaid Our focus is on preventive care.
South Carolina s. Road Map to the Future
 South Carolina s Road Map to the Future S.C. BUSINESS ROUN DTABLE To Members of the General Assembly: On December, the below-named groups delivered a letter urging your attention to one of the most important,
South Carolina s Road Map to the Future S.C. BUSINESS ROUN DTABLE To Members of the General Assembly: On December, the below-named groups delivered a letter urging your attention to one of the most important,
PRECONSTRUCTION DIRECTOR OF PRECONSTRUCTION PRATT ROBERT I ROOM 425A UPSTATE LESTER MARK C
 PRECONSTRUCTION DIRECTOR OF PRECONSTRUCTION PRATT ROBERT I 803-737-1350 ROOM 425A PRECONSTRUCTION SUPPORT RIGHT OF WAY SURVEYS ENGINEER LIFSEY MATTHEW R METTS MITCHELL D YOUNG RANDALL L LESTER MARK C EARGLE
PRECONSTRUCTION DIRECTOR OF PRECONSTRUCTION PRATT ROBERT I 803-737-1350 ROOM 425A PRECONSTRUCTION SUPPORT RIGHT OF WAY SURVEYS ENGINEER LIFSEY MATTHEW R METTS MITCHELL D YOUNG RANDALL L LESTER MARK C EARGLE
Role of SAPT Block Grant in Non- Medicaid Expansion States
 Role of SAPT Block Grant in Non- Medicaid Expansion States Stephen L. Dutton, Chief of Staff Frankie Long, Treatment Director South Carolina Department of Alcohol and Other Drug Abuse Services (DAODAS)
Role of SAPT Block Grant in Non- Medicaid Expansion States Stephen L. Dutton, Chief of Staff Frankie Long, Treatment Director South Carolina Department of Alcohol and Other Drug Abuse Services (DAODAS)
Delivery Buddy: NRP Support via Telemedicine
 Delivery Buddy: NRP Support via Telemedicine Bridget Allen, RNC, MS Carley Howard, MD, FAAP 9/19/16 Introductions Bridget Allen RNC, MS Clemson University undergraduate and graduate school. Masters Maternal
Delivery Buddy: NRP Support via Telemedicine Bridget Allen, RNC, MS Carley Howard, MD, FAAP 9/19/16 Introductions Bridget Allen RNC, MS Clemson University undergraduate and graduate school. Masters Maternal
OPERATIONS STATE EMERGENCY OPERATIONS CENTER (SEOC)
") OPERATIONS STATE EMERGENCY OPERATIONS CENTER (SEOC) OVERVIEW State Emergency Operations Center (SEOC) Purpose, and OPCONs Composition & Duties SEOC Information and Tasking Flow SEOC PURPOSE Multi Agency
OPERATIONS STATE EMERGENCY OPERATIONS CENTER (SEOC) OVERVIEW State Emergency Operations Center (SEOC) Purpose, and OPCONs Composition & Duties SEOC Information and Tasking Flow SEOC PURPOSE Multi Agency
ANNEX 1-Basic Plan ALERT AND NOTIFICATION PROCEDURES APPENDIX 2
 ANNEX 1-Basic Plan ALERT AND NOTIFICATION PROCEDURES APPENDIX 2 I. INTRODUCTION Nuclear Power Plant (NPP) licensees in conjunction with state and local emergency management organizations have established
ANNEX 1-Basic Plan ALERT AND NOTIFICATION PROCEDURES APPENDIX 2 I. INTRODUCTION Nuclear Power Plant (NPP) licensees in conjunction with state and local emergency management organizations have established
CCL E-News & E-Notes
 Serving Children and Families New Online Payment System Child Care Licensing will unveil a new online fee payment system on April 23. You will be able to pay Licensing Fees, Central Registry Fees, and
Serving Children and Families New Online Payment System Child Care Licensing will unveil a new online fee payment system on April 23. You will be able to pay Licensing Fees, Central Registry Fees, and
MEMBER HANDBOOK. Absolute Total Care (MMP) H1723_ANOCMH17_Approved_
 H1723_ANOCMH17_Approved_") 2017 Absolute Total Care (MMP) H1723_ANOCMH17_Approved_09082016 ANNUAL NOTICE OF CHANGES FOR 2017 H1723_ANOCMH17_Approved_09082017 Table of Contents A. Think about Your Medicare and Healthy Connections
2017 Absolute Total Care (MMP) H1723_ANOCMH17_Approved_09082016 ANNUAL NOTICE OF CHANGES FOR 2017 H1723_ANOCMH17_Approved_09082017 Table of Contents A. Think about Your Medicare and Healthy Connections
Surveillance, Outcomes Assessment, and Intervention Capacity
 Surveillance, Outcomes Assessment, and Intervention Capacity Participant Identification Surveillance SCI Association Clinical Center Pilot studies Project grants Bench Science/ Mechanistic Clinical and
Surveillance, Outcomes Assessment, and Intervention Capacity Participant Identification Surveillance SCI Association Clinical Center Pilot studies Project grants Bench Science/ Mechanistic Clinical and
Michael McInerney, Director of External Affairs South Carolina Department of Commerce
 Henry McMaster SOUTH CAROLINA Robert M. Hitt III G o v e r n o r D E P A R T M E N T O F C O M M E R C E S e c r e t a r y TO: FROM: Michael McInerney, Director of External Affairs South Carolina Department
Henry McMaster SOUTH CAROLINA Robert M. Hitt III G o v e r n o r D E P A R T M E N T O F C O M M E R C E S e c r e t a r y TO: FROM: Michael McInerney, Director of External Affairs South Carolina Department
May 2017 BlueNewsSM. Realignment within the BlueCross BlueShield and BlueChoice Health Plan Provider Relations and Education Team
 May 2017 BlueNewsSM for Providers The Wait Is Over! Benefit Update Meeting Winners CMS Validation Program Returns Frequently Asked Questions Claims and Billing Minute Featured Webinar Important Reminders
May 2017 BlueNewsSM for Providers The Wait Is Over! Benefit Update Meeting Winners CMS Validation Program Returns Frequently Asked Questions Claims and Billing Minute Featured Webinar Important Reminders
2017 Election Calendar
 2017 Calendar Date of Number Name of Type of 07/11/2017 20457 12-CHESTER Fort Lawn Town Council Special Special 07/11/2017 20420 19-EDGEFIELD Edgefield Council Dist. 4 Special Special 07/18/2017 20448
2017 Calendar Date of Number Name of Type of 07/11/2017 20457 12-CHESTER Fort Lawn Town Council Special Special 07/11/2017 20420 19-EDGEFIELD Edgefield Council Dist. 4 Special Special 07/18/2017 20448
FLEET STREET NEWS. G reetings Fellow. From the President s Desk...
 Volume 6, Issue 1 Spring 2012 Post Office Box 7824 Columbia, SC 29202 S o u t h e a s t G o v e r n m e n t a l F l e e t M a n a g e r s A s s o c i a t i o n FLEET STREET NEWS INSIDE THIS ISSUE: 2012
Volume 6, Issue 1 Spring 2012 Post Office Box 7824 Columbia, SC 29202 S o u t h e a s t G o v e r n m e n t a l F l e e t M a n a g e r s A s s o c i a t i o n FLEET STREET NEWS INSIDE THIS ISSUE: 2012
LTC User Guide for Nursing Facility Forms 3618/3619 and Minimum Data Set/ Long Term Care Medicaid Information (MDS/LTCMI)
") LTC User Guide for Nursing Facility Forms 3618/3619 and Minimum Data Set/ Long Term Care Medicaid Information (MDS/LTCMI) v 2018 0614 Contents Learning Objectives...1 Sequencing of Documents...2 Admission
LTC User Guide for Nursing Facility Forms 3618/3619 and Minimum Data Set/ Long Term Care Medicaid Information (MDS/LTCMI) v 2018 0614 Contents Learning Objectives...1 Sequencing of Documents...2 Admission
Consolidated Annual Performance & Evaluation Report (CAPER)
") STATE OF SOUTH CAROLINA CONSOLIDATED PLAN FOR HOUSING AND COMMUNITY DEVELOPMENT Consolidated Annual Performance & Evaluation Report (CAPER) Program Year April 1, 2011 March 31, 2012 Community Development
STATE OF SOUTH CAROLINA CONSOLIDATED PLAN FOR HOUSING AND COMMUNITY DEVELOPMENT Consolidated Annual Performance & Evaluation Report (CAPER) Program Year April 1, 2011 March 31, 2012 Community Development
FEMA CONGRESSIONAL ADVISORY November 14, 2016
 U.S. Department of Homeland Security Federal Emergency Management Agency DR-4286-SC Congressional Affairs Telephone 202-445-8820 FEMA CONGRESSIONAL ADVISORY November 14, 2016 Contents Key messages Disaster
U.S. Department of Homeland Security Federal Emergency Management Agency DR-4286-SC Congressional Affairs Telephone 202-445-8820 FEMA CONGRESSIONAL ADVISORY November 14, 2016 Contents Key messages Disaster
Provider Business Procedures. Quality. abcqualitycare.org
 Provider Business Procedures Quality abcqualitycare.org 1-800-262-4416 TABLE OF CONTENTS PAGE NO. I. Provider Selection By A Client 6 II. Maximum Care Allowed 7 III. Client Fee 7 IV. Client Transfer 7
Provider Business Procedures Quality abcqualitycare.org 1-800-262-4416 TABLE OF CONTENTS PAGE NO. I. Provider Selection By A Client 6 II. Maximum Care Allowed 7 III. Client Fee 7 IV. Client Transfer 7
Summary of Benefits. Medicare Advantage Plan (PPO) January 1, 2013 December 31, Medicare Solution. A UnitedHealthcare
 January 1, 2013 December 31, Medicare Solution. A UnitedHealthcare") 2013 Summary of Benefits January 1, 2013 December 31, 2013 Medicare Advantage Plan (PPO) A UnitedHealthcare Medicare Solution The service area for this plan includes select counties in South Carolina.
2013 Summary of Benefits January 1, 2013 December 31, 2013 Medicare Advantage Plan (PPO) A UnitedHealthcare Medicare Solution The service area for this plan includes select counties in South Carolina.
Delegation Oversight 2016 Audit Tool Credentialing and Recredentialing
 Att CRE - 216 Delegation Oversight 216 Audit Tool Review Date: A B C D E F 1 2 C3 R3 4 5 N/A N/A 6 7 8 9 N/A N/A AUDIT RESULTS CREDENTIALING ASSESSMENT ELEMENT COMPLIANCE SCORE CARD Medi-Cal Elements Medi-Cal
Att CRE - 216 Delegation Oversight 216 Audit Tool Review Date: A B C D E F 1 2 C3 R3 4 5 N/A N/A 6 7 8 9 N/A N/A AUDIT RESULTS CREDENTIALING ASSESSMENT ELEMENT COMPLIANCE SCORE CARD Medi-Cal Elements Medi-Cal
Susan G. Komen South Carolina FY18 SMALL GRANTS PROGRAM
 Susan G. Komen South Carolina FY18 SMALL GRANTS PROGRAM FOR BREAST HEALTH SUPPORT PROJECTS TO BE HELD BETWEEN APRIL 1, 2017 AND MARCH 31, 2018 SUSAN G. KOMEN AFFILIATE GRANTS TO SAVE LIVES BY MEETING THE
Susan G. Komen South Carolina FY18 SMALL GRANTS PROGRAM FOR BREAST HEALTH SUPPORT PROJECTS TO BE HELD BETWEEN APRIL 1, 2017 AND MARCH 31, 2018 SUSAN G. KOMEN AFFILIATE GRANTS TO SAVE LIVES BY MEETING THE
Chapter 11 Section 3. Hospice Reimbursement - Conditions For Coverage
 Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
Assisted Living Facility Disclosure Statement Required by the Virginia Department of Social Services
 Assisted Living Facility Disclosure Statement Required by the Virginia Department of Social Services The Standards for Licensed Assisted Living Facilities requires each assisted living facility to provide
Assisted Living Facility Disclosure Statement Required by the Virginia Department of Social Services The Standards for Licensed Assisted Living Facilities requires each assisted living facility to provide
Personal Care Services (PCS): An Overview of PCS and The Request for Independent Assessment for PCS Attestation of Medical Need Form (DMA 3051)
: An Overview of PCS and The Request for Independent Assessment for PCS Attestation of Medical Need Form (DMA 3051)") Personal Care Services (PCS): An Overview of PCS and The Request for Independent Assessment for PCS Attestation of Medical Need Form (DMA 3051) January 2018 OBJECTIVES At the conclusion of this training,
Personal Care Services (PCS): An Overview of PCS and The Request for Independent Assessment for PCS Attestation of Medical Need Form (DMA 3051) January 2018 OBJECTIVES At the conclusion of this training,
Application for Residency
 Application for Residency Date Application Mailed Date Application Received to the an Eastern Star Home A. Personal Information Applicant s Name: Maiden Name: Address: Home Phone: Birth date: / / Age:
Application for Residency Date Application Mailed Date Application Received to the an Eastern Star Home A. Personal Information Applicant s Name: Maiden Name: Address: Home Phone: Birth date: / / Age:
Alabama. Phone. Agency. Department of Public Health, Bureau of Health Provider Standards (334) Contact Kelley Mitchell (334)
 Contact Kelley Mitchell (334)") Alabama Agency Department of Public Health, Bureau of Health Provider Standards (334) 206-5575 Contact Kelley Mitchell (334) 206-5366 E-mail Kelley.Mitchell@adph.state.al.us Phone Web Site http://www.adph.org/healthcarefacilities/
Alabama Agency Department of Public Health, Bureau of Health Provider Standards (334) 206-5575 Contact Kelley Mitchell (334) 206-5366 E-mail Kelley.Mitchell@adph.state.al.us Phone Web Site http://www.adph.org/healthcarefacilities/
Ohio. Phone. Web Site. Licensure Term. Residential Care Facilities
 Ohio Phone Agency Ohio Department of Health, Division of Quality Assurance (614) 466-7713 Contact Jayson Rogers (614) 752-9156 E-mail jayson.rogers@odh.ohio.gov Web Site http://www.odh.ohio.gov/odhprograms/ltc/residential-care-facilities/main-page
Ohio Phone Agency Ohio Department of Health, Division of Quality Assurance (614) 466-7713 Contact Jayson Rogers (614) 752-9156 E-mail jayson.rogers@odh.ohio.gov Web Site http://www.odh.ohio.gov/odhprograms/ltc/residential-care-facilities/main-page
Medicaid RAC Audit Results
 Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
Medicaid RAC Audit Results Clinical Audits: The RAC Clinical audit goal was to review supporting documentation for necessity of admission and continued stay in long term care for Medicaid residents. There
SC Medicaid Health Care Performance Calendar Year 2011
 SC Medicaid Health Care Performance Calendar Year 2011 A Report on Quality, Access to Care, and Consumer Satisfaction Developed by: The Institute for Families in Society Division of Policy and Research
SC Medicaid Health Care Performance Calendar Year 2011 A Report on Quality, Access to Care, and Consumer Satisfaction Developed by: The Institute for Families in Society Division of Policy and Research
ADULT LONG-TERM CARE SERVICES
 ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
State of West Virginia DEPARTMENT OF HEALTH AND HUMAN RESOURCES Office of Inspector General Board of Review PO Box 6165 Wheeling, WV 26003
 Joe Manchin III Governor State of West Virginia DEPARTMENT OF HEALTH AND HUMAN RESOURCES Office of Inspector General Board of Review PO Box 6165 Wheeling, WV 26003 Martha Yeager Walker Secretary January
Joe Manchin III Governor State of West Virginia DEPARTMENT OF HEALTH AND HUMAN RESOURCES Office of Inspector General Board of Review PO Box 6165 Wheeling, WV 26003 Martha Yeager Walker Secretary January
MEDICARE-MEDICAID CAPITATED FINANCIAL ALIGNMENT MODEL REPORTING REQUIREMENTS: SOUTH CAROLINA-SPECIFIC REPORTING REQUIREMENTS
 MEDICARE-MEDICAID CAPITATED FINANCIAL ALIGNMENT MODEL REPORTING REQUIREMENTS: SOUTH CAROLINA-SPECIFIC REPORTING REQUIREMENTS Effective as of February 1, 2015, Issued August 13, 2015 SC-1 Table of Contents
MEDICARE-MEDICAID CAPITATED FINANCIAL ALIGNMENT MODEL REPORTING REQUIREMENTS: SOUTH CAROLINA-SPECIFIC REPORTING REQUIREMENTS Effective as of February 1, 2015, Issued August 13, 2015 SC-1 Table of Contents
ENROLLMENT, ELIGIBILITY AND DISENROLLMENT
 ENROLLMENT ENROLLMENT, ELIGIBILITY AND DISENROLLMENT Enrollment in Washington Apple Health, Apple Health Fully Integrated Managed Care (FIMC) Medicaid Programs and Behavioral Health Services Only (BHSO)
ENROLLMENT ENROLLMENT, ELIGIBILITY AND DISENROLLMENT Enrollment in Washington Apple Health, Apple Health Fully Integrated Managed Care (FIMC) Medicaid Programs and Behavioral Health Services Only (BHSO)
What is a retrospective Level of Care and what is the process for submitting a retrospective Level of Care?
 Last updated 9/14/2011 The following are Frequently Asked Questions (FAQs) associated with Connecticut Level of Care and PASRR Level I/II processes. To read to the corresponding response to the questions
Last updated 9/14/2011 The following are Frequently Asked Questions (FAQs) associated with Connecticut Level of Care and PASRR Level I/II processes. To read to the corresponding response to the questions
Services for Caregivers
 1 Services for Caregivers Caregivers often find the task of caring for another person to be overwhelming. They often develop stress-related illnesses such as heart disease, hypertension, or ulcers. An
1 Services for Caregivers Caregivers often find the task of caring for another person to be overwhelming. They often develop stress-related illnesses such as heart disease, hypertension, or ulcers. An
Clinical Coverage Policy 3L, Personal Care Services (PCS) Benefit Program
 Benefit Program") THE STATE OF NORTH CAROLINA Department of Health and Human Services Clinical Coverage Policy 3L, Personal Care Services (PCS) Benefit Program Provider Manual Effective August 2017 Table of Contents Introduction:
THE STATE OF NORTH CAROLINA Department of Health and Human Services Clinical Coverage Policy 3L, Personal Care Services (PCS) Benefit Program Provider Manual Effective August 2017 Table of Contents Introduction:
Long-Term Care Glossary
 Long-Term Care Glossary Adjudicated Claim Activities of Daily Living (ADL) A claim that has reached final disposition such that it is either paid or denied. Basic tasks individuals perform in the course
Long-Term Care Glossary Adjudicated Claim Activities of Daily Living (ADL) A claim that has reached final disposition such that it is either paid or denied. Basic tasks individuals perform in the course
TRANSITION OF NURSING HOME POPULATIONS AND BENEFITS TO MEDICAID MANAGED CARE Frequently Asked Questions March 2015
 ANDREW M. CUOMO Governor HOWARD A. ZUCKER, M.D., J.D. Acting Commissioner SALLY DRESLIN, M.S., R.N. Executive Deputy Commissioner TRANSITION OF NURSING HOME POPULATIONS AND BENEFITS TO MEDICAID MANAGED
ANDREW M. CUOMO Governor HOWARD A. ZUCKER, M.D., J.D. Acting Commissioner SALLY DRESLIN, M.S., R.N. Executive Deputy Commissioner TRANSITION OF NURSING HOME POPULATIONS AND BENEFITS TO MEDICAID MANAGED
ENROLLMENT, ELIGIBILITY AND DISENROLLMENT
 ENROLLMENT ENROLLMENT, ELIGIBILITY AND DISENROLLMENT Enrollment in Washington Apple Health Medicaid Programs: Molina Healthcare Members are enrolled in a managed care health plan after the Health Care
ENROLLMENT ENROLLMENT, ELIGIBILITY AND DISENROLLMENT Enrollment in Washington Apple Health Medicaid Programs: Molina Healthcare Members are enrolled in a managed care health plan after the Health Care
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. HCBS Frail Elderly
 Fee-for-Service Provider Manual HCBS Frail Elderly Updated 02.2016 PART II Section BILLING INSTRUCTIONS Page 7000 HCBS FE Billing Instructions................. 7-1 7010 HCBS FE Specific Billing Information.............
Fee-for-Service Provider Manual HCBS Frail Elderly Updated 02.2016 PART II Section BILLING INSTRUCTIONS Page 7000 HCBS FE Billing Instructions................. 7-1 7010 HCBS FE Specific Billing Information.............
South Carolina Fire Academy
 January - June 2013 South Carolina Fire Academy Public Fire Service Course Dates January - June 2013 South Carolina Department of Labor, Licensing and Regulation Division of Fire and Life Safety South
January - June 2013 South Carolina Fire Academy Public Fire Service Course Dates January - June 2013 South Carolina Department of Labor, Licensing and Regulation Division of Fire and Life Safety South
TRANSITION OF NURSING HOME POPULATIONS AND BENEFITS TO MEDICAID MANAGED CARE
 ANDREW M. CUOMO Governor HOWARD A. ZUCKER, M.D., J.D. Acting Commissioner SALLY DRESLIN, M.S., R.N. Executive Deputy Commissioner TRANSITION OF NURSING HOME POPULATIONS AND BENEFITS TO MEDICAID MANAGED
ANDREW M. CUOMO Governor HOWARD A. ZUCKER, M.D., J.D. Acting Commissioner SALLY DRESLIN, M.S., R.N. Executive Deputy Commissioner TRANSITION OF NURSING HOME POPULATIONS AND BENEFITS TO MEDICAID MANAGED
EW Customized Living Contract Planning Worksheet, Part I
 Purpose of This Worksheet This planning worksheet is designed to: 1. Delineate component services that can be included in EW customized living and 24 hour customized living packages. 2. Serve as a tool
Purpose of This Worksheet This planning worksheet is designed to: 1. Delineate component services that can be included in EW customized living and 24 hour customized living packages. 2. Serve as a tool
CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT
 CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT Table of Contents 1. Introduction 2. When a provider is deemed to accept Flexi Blue PFFS terms and
CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT Table of Contents 1. Introduction 2. When a provider is deemed to accept Flexi Blue PFFS terms and
Long Term Care User Guide for Hospice Providers
 Long Term Care User Guide for Hospice Providers v 2018 0802 Contents Learning Objectives...1 Forms to be Submitted...2 Hospice Form 3071 Election/Cancellation/Discharge Notice...2 How to Submit Form 3071...3
Long Term Care User Guide for Hospice Providers v 2018 0802 Contents Learning Objectives...1 Forms to be Submitted...2 Hospice Form 3071 Election/Cancellation/Discharge Notice...2 How to Submit Form 3071...3
C. The individual must be capable of assisting in the selection, training, and supervision of the attendant s scheduled activities.
 4200 ATTENDANT CARE SERVICES. 4201 General. This section addresses two types of attendant care services: A. Supportive attendant care services required to enable an individual to participate in one or
4200 ATTENDANT CARE SERVICES. 4201 General. This section addresses two types of attendant care services: A. Supportive attendant care services required to enable an individual to participate in one or
VIRGINIA DEPARTMENT OF SOCIAL SERVICES AUXILIARY GRANT PROGRAM
 VIRGINIA DEPARTMENT OF SOCIAL SERVICES AUXILIARY GRANT PROGRAM What Is an Auxiliary Grant? An Auxiliary Grant (AG) is a supplement to income (i.e., cash assistance) for recipients of Supplemental Security
VIRGINIA DEPARTMENT OF SOCIAL SERVICES AUXILIARY GRANT PROGRAM What Is an Auxiliary Grant? An Auxiliary Grant (AG) is a supplement to income (i.e., cash assistance) for recipients of Supplemental Security
Gateway Area Agency on Aging and Independent Living Policy Manual and Standard Operating Procedures
 Chapter 18 Personal Care Attendant Program Table of Contents Introduction 3 Definitions 5 Eligibility 8 Income Eligibility Standards 9 Application and Evaluation/Re-evaluation 10 Waiting List 12 Relocation
Chapter 18 Personal Care Attendant Program Table of Contents Introduction 3 Definitions 5 Eligibility 8 Income Eligibility Standards 9 Application and Evaluation/Re-evaluation 10 Waiting List 12 Relocation
Enrollment, Eligibility and Disenrollment
 Section 2. Enrollment, Eligibility and Disenrollment Enrollment: Enrollment in Medicaid Programs: The State of Florida (State) has the sole authority for determining eligibility for Medicaid and whether
Section 2. Enrollment, Eligibility and Disenrollment Enrollment: Enrollment in Medicaid Programs: The State of Florida (State) has the sole authority for determining eligibility for Medicaid and whether
DEPARTMENT OF HUMAN SERVICES AGING AND PEOPLE WITH DISABILITIES OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 33
 DEPARTMENT OF HUMAN SERVICES AGING AND PEOPLE WITH DISABILITIES OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 33 IN-HOME CARE AGENCIES PROVIDING MEDICAID IN-HOME SERVICES 411-033-0000 Purpose and Scope
DEPARTMENT OF HUMAN SERVICES AGING AND PEOPLE WITH DISABILITIES OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 33 IN-HOME CARE AGENCIES PROVIDING MEDICAID IN-HOME SERVICES 411-033-0000 Purpose and Scope
Volume 24, No. 07 July 2014
 State of New Jersey Department of Human Services Division of Medical Assistance & Health Services Volume 24, No. 07 July 2014 TO: SUBJECT: All Providers For Action For Managed Care Organizations For Information
State of New Jersey Department of Human Services Division of Medical Assistance & Health Services Volume 24, No. 07 July 2014 TO: SUBJECT: All Providers For Action For Managed Care Organizations For Information
Florida Medicaid Qualified Hospital (QH) Presumptive Eligibility. November 2016
 Presumptive Eligibility. November 2016") Florida Medicaid Qualified Hospital (QH) Presumptive Eligibility November 2016 Presentation Outline 2 Presumptive Eligibility: Section 1 LEGAL BASIS 3 What is Presumptive Eligibility? Presumptive Eligibility
Florida Medicaid Qualified Hospital (QH) Presumptive Eligibility November 2016 Presentation Outline 2 Presumptive Eligibility: Section 1 LEGAL BASIS 3 What is Presumptive Eligibility? Presumptive Eligibility
Provider Manual. Child Care Services PROVIDER MANUAL
 Child Care Services Provider Manual 1 Child Care Management Services (CCMS) Provider Manual Summary The following is a summary of the Child Care Management Services Provider Manual. This manual is the
Child Care Services Provider Manual 1 Child Care Management Services (CCMS) Provider Manual Summary The following is a summary of the Child Care Management Services Provider Manual. This manual is the
Private Duty Nursing. May 2017
 Private Duty Nursing May 2017 Overview Provider Enrollment Member Eligibility Private Duty Nursing Services Specialized Private Duty Nursing Services Billing Additional Information 2 Provider Enrollment
Private Duty Nursing May 2017 Overview Provider Enrollment Member Eligibility Private Duty Nursing Services Specialized Private Duty Nursing Services Billing Additional Information 2 Provider Enrollment
LONG TERM CARE SETTINGS
 LONG TERM CARE SETTINGS Long term care facilities assist aged, ill or disabled persons who can no longer live independently. In this section, we will briefly examine the history of long term care facilities
LONG TERM CARE SETTINGS Long term care facilities assist aged, ill or disabled persons who can no longer live independently. In this section, we will briefly examine the history of long term care facilities
Exhibit A. Part 1 Statement of Work
 Exhibit A Part 1 Statement of Work Contractor shall provide Basic Neurological services as described herein to Medicaid eligible Clients who are authorized to receive services at the Contractor s owned
Exhibit A Part 1 Statement of Work Contractor shall provide Basic Neurological services as described herein to Medicaid eligible Clients who are authorized to receive services at the Contractor s owned
CAL MEDICONNECT: Working with In-Home Supportive Services (IHSS) Physician Webinar Series
 Physician Webinar Series") CAL MEDICONNECT: Working with In-Home Supportive Services (IHSS) Physician Webinar Series Today s Webinar This webinar is part of a series designed specifically for physicians. For a general overview of
CAL MEDICONNECT: Working with In-Home Supportive Services (IHSS) Physician Webinar Series Today s Webinar This webinar is part of a series designed specifically for physicians. For a general overview of
Behavioral Health Outpatient Authorization Request Self Service. User Guide
 Behavioral Health Self Behavioral Health Outpatient Authorization Request Self Service User Guide Introduction Tufts Health Plan Network Health has created this user guide to illustrate how to navigate
Behavioral Health Self Behavioral Health Outpatient Authorization Request Self Service User Guide Introduction Tufts Health Plan Network Health has created this user guide to illustrate how to navigate
Long Term Care Nursing Facility Resource Guide
 Long Term Care Nursing Facility Resource Guide September 2014 Table of Contents Section 1: Introduction and Overview Introduction... 4 Purpose and Organization of Long Term Care Nursing Facility Resource
Long Term Care Nursing Facility Resource Guide September 2014 Table of Contents Section 1: Introduction and Overview Introduction... 4 Purpose and Organization of Long Term Care Nursing Facility Resource
FRAUD IN PERSONAL CARE PROGRAMS
 FRAUD IN PERSONAL CARE PROGRAMS JAMES G. SHEEHAN CHIEF INTEGRITY OFFICER NEW YORK CITY HUMAN RESOURCES ADMINISTRATION sheehanj@hra.nyc.gov (212) 274-5600 LEARNING OBJECTIVES Identifying personal care services.
FRAUD IN PERSONAL CARE PROGRAMS JAMES G. SHEEHAN CHIEF INTEGRITY OFFICER NEW YORK CITY HUMAN RESOURCES ADMINISTRATION sheehanj@hra.nyc.gov (212) 274-5600 LEARNING OBJECTIVES Identifying personal care services.
Policy: Supportive Care Program
 Policy: Supportive Care Program Original Approval Date: March 24, 2011 Effective Date: July 1, 2015 Approved By: Original signed by Tracey Barbrick, Associate Deputy Minister per Dr. Peter Vaughan, CD,
Policy: Supportive Care Program Original Approval Date: March 24, 2011 Effective Date: July 1, 2015 Approved By: Original signed by Tracey Barbrick, Associate Deputy Minister per Dr. Peter Vaughan, CD,
Emergency Plan Guidelines For Child Care Providers
 South Carolina Division of Early Care and Education Health. Safety. Supervision. Emergency Plan Guidelines For Child Care Providers Visit us on the Web at: www.scchildcare.org Phone Numbers Region 1 (Upstate):
South Carolina Division of Early Care and Education Health. Safety. Supervision. Emergency Plan Guidelines For Child Care Providers Visit us on the Web at: www.scchildcare.org Phone Numbers Region 1 (Upstate):
Food Stamps Caseload Distribution (FS)... 1
... 1") Table of Contents General Program Information 0210.0000 Food Stamps... 1 0210.0001 Caseload Distribution (FS)... 1 0210.0100 FOOD STAMP PROGRAM (FS)... 1 0210.0101 Legal Basis (FS)... 1 0210.0102 Program
Table of Contents General Program Information 0210.0000 Food Stamps... 1 0210.0001 Caseload Distribution (FS)... 1 0210.0100 FOOD STAMP PROGRAM (FS)... 1 0210.0101 Legal Basis (FS)... 1 0210.0102 Program
(Signed original copy on file)
") CFOP 140-10 STATE OF FLORIDA DEPARTMENT OF CF OPERATING PROCEDURE CHILDREN AND FAMILIES NO. 140-10 TALLAHASSEE, May 11, 2015 HOME CARE FOR DISABLED ADULTS This operating procedure provides guidelines for
CFOP 140-10 STATE OF FLORIDA DEPARTMENT OF CF OPERATING PROCEDURE CHILDREN AND FAMILIES NO. 140-10 TALLAHASSEE, May 11, 2015 HOME CARE FOR DISABLED ADULTS This operating procedure provides guidelines for
Massachusetts. Phone. Web Site. Licensure Term. Assisted Living Residences.
 Massachusetts Phone Agency Executive Office of Elder Affairs (617) 727-7750 Contact Patricia Marchetti (617) 222-7503 E-mail patricia.marchetti@state.ma.us Web Site http://www.mass.gov/elders/housing/assisted-living/
Massachusetts Phone Agency Executive Office of Elder Affairs (617) 727-7750 Contact Patricia Marchetti (617) 222-7503 E-mail patricia.marchetti@state.ma.us Web Site http://www.mass.gov/elders/housing/assisted-living/
CHAPTER 35. MEDICAL ASSISTANCE FOR ADULTS AND CHILDREN-ELIGIBILITY SUBCHAPTER 15. PERSONAL CARE SERVICES
 CHAPTER 35. MEDICAL ASSISTANCE FOR ADULTS AND CHILDREN-ELIGIBILITY SUBCHAPTER 15. PERSONAL CARE SERVICES 317:35-15-8.1. Agency Personal Care services; billing, and issue resolution (4-1-2009) The ADvantage
CHAPTER 35. MEDICAL ASSISTANCE FOR ADULTS AND CHILDREN-ELIGIBILITY SUBCHAPTER 15. PERSONAL CARE SERVICES 317:35-15-8.1. Agency Personal Care services; billing, and issue resolution (4-1-2009) The ADvantage
Welcome The Freedom to Succeed
 Welcome The Freedom to Succeed Liberty Healthcare PCS Provider Training May 2016 AGENDA 9:00-9:15 am Welcome and Introductions Denise Hobson, Director of Clinical Services Liberty Healthcare 9:15-9:45
Welcome The Freedom to Succeed Liberty Healthcare PCS Provider Training May 2016 AGENDA 9:00-9:15 am Welcome and Introductions Denise Hobson, Director of Clinical Services Liberty Healthcare 9:15-9:45
November 14, Chief Clinical Operating Officer Division of Medical Assistance Department of Health and Human Services
 Department of Health and Human Services Division of Medical Assistance Response To Questions from the Adult Care Home Transition Subcommittee of the Blue Ribbon Commission November 14, 2012 Presenter:
Department of Health and Human Services Division of Medical Assistance Response To Questions from the Adult Care Home Transition Subcommittee of the Blue Ribbon Commission November 14, 2012 Presenter:
MEDICARE-MEDICAID CAPITATED FINANCIAL ALIGNMENT MODEL REPORTING REQUIREMENTS: CALIFORNIA-SPECIFIC REPORTING REQUIREMENTS
 MEDICARE-MEDICAID CAPITATED FINANCIAL ALIGNMENT MODEL REPORTING REQUIREMENTS: CALIFORNIA-SPECIFIC REPORTING REQUIREMENTS Effective as of January 1, 2015, Issued August 24, 2015 CA-1 Table of Contents California-Specific
MEDICARE-MEDICAID CAPITATED FINANCIAL ALIGNMENT MODEL REPORTING REQUIREMENTS: CALIFORNIA-SPECIFIC REPORTING REQUIREMENTS Effective as of January 1, 2015, Issued August 24, 2015 CA-1 Table of Contents California-Specific
Delaware. Phone. Agency (302) Department of Health and Social Services, Division of Long Term Care Residents Protection
 Department of Health and Social Services, Division of Long Term Care Residents Protection") Delaware Agency Department of Health and Social Services, Division of Long Term Care Residents Protection (302) 421-7410 Contact Robert Smith (302) 421-7448 E-mail Robert.Smith@state.de.us Phone Web Site
Delaware Agency Department of Health and Social Services, Division of Long Term Care Residents Protection (302) 421-7410 Contact Robert Smith (302) 421-7448 E-mail Robert.Smith@state.de.us Phone Web Site
RELATIVE/NEIGHBOR PROVIDER
 TABLE OF CONTENTS 301.1 GENERAL POLICY & REGULATION 301.2 DEFINITIONS & ACRONYMS 301.3 GOALS & OBJECTIVES 301.4 P/C RESPONSIBILITIES 301.5 CCIS RESPONSIBILITIES 301.6 PROVIDER RESPONSIBILITIES 301.7 IDENTIFYING
TABLE OF CONTENTS 301.1 GENERAL POLICY & REGULATION 301.2 DEFINITIONS & ACRONYMS 301.3 GOALS & OBJECTIVES 301.4 P/C RESPONSIBILITIES 301.5 CCIS RESPONSIBILITIES 301.6 PROVIDER RESPONSIBILITIES 301.7 IDENTIFYING
Resident Name Medicaid # - - If Pending Medicaid, Social Security # - - Medicare # Date of Birth / / Responsible Party. Responsible Party Address
 URSIG FACILIT LEVEL OF CARE REQUEST FOR ADMISSIO Resident ame Medicaid # - - Room # Room Certified for Medicaid es o If Pending Medicaid, Social Security # - - Medicare # Date of Birth / / Marital Status
URSIG FACILIT LEVEL OF CARE REQUEST FOR ADMISSIO Resident ame Medicaid # - - Room # Room Certified for Medicaid es o If Pending Medicaid, Social Security # - - Medicare # Date of Birth / / Marital Status
ALABAMA CARES SCOPE OF SERVICES IN-HOME RESPITE CARE
 ALABAMA CARES SCOPE OF SERVICES IN-HOME RESPITE CARE Operating Agency-SARCOA RC-Respite Care PC-Personal Care RCW-Respite Care Worker PCW-Personal Care Worker POC-Plan of Care DSP-Direct Service Provider-(In
ALABAMA CARES SCOPE OF SERVICES IN-HOME RESPITE CARE Operating Agency-SARCOA RC-Respite Care PC-Personal Care RCW-Respite Care Worker PCW-Personal Care Worker POC-Plan of Care DSP-Direct Service Provider-(In
New provider orientation. IAPEC December 2015
 New provider orientation IAPEC-0109-15 December 2015 Welcome 2 Agenda Introduction to Amerigroup Provider resources Preservice processes Member benefits and services Claims and billing Provider responsibilities
New provider orientation IAPEC-0109-15 December 2015 Welcome 2 Agenda Introduction to Amerigroup Provider resources Preservice processes Member benefits and services Claims and billing Provider responsibilities
South Carolina Healthy Connections Prime CY 2016 Final Medicare Rate Report March 15, 2016
 The State of South Carolina, in conjunction with the Centers for Medicare and Medicaid Services (CMS), is releasing the updated Medicaid component of the CY 2016 rates for the South Carolina Healthy Connections
The State of South Carolina, in conjunction with the Centers for Medicare and Medicaid Services (CMS), is releasing the updated Medicaid component of the CY 2016 rates for the South Carolina Healthy Connections
Chapter 30, Medicaid Hospice Program 07/19/13
 Chapter 30, Medicaid Hospice Program 07/19/13 30.4. Definitions. The following words and terms, when used in this chapter, shall have the following meanings, unless the context clearly indicates otherwise.
Chapter 30, Medicaid Hospice Program 07/19/13 30.4. Definitions. The following words and terms, when used in this chapter, shall have the following meanings, unless the context clearly indicates otherwise.
Health Benefits Identification FAQs. A: All cards should be issued throughout the State by February 2007.
 1. Q: When are cards being distributed? A: All cards should be issued throughout the State by February 2007. 2. Q: What if a beneficiary has a plastic ID card and he/she goes to another county that has
1. Q: When are cards being distributed? A: All cards should be issued throughout the State by February 2007. 2. Q: What if a beneficiary has a plastic ID card and he/she goes to another county that has
Connecticut LTC Level of Care Determination Form To be maintained in the individual s medical record.
 I. Demographics A. Individual First Name: Middle Initial: Mailing Address: City: State: Zip: Phone: Social Security #: Date of Birth: _/ / Marital Status: M S W D Gender: Male Female Connecticut LTC Level
I. Demographics A. Individual First Name: Middle Initial: Mailing Address: City: State: Zip: Phone: Social Security #: Date of Birth: _/ / Marital Status: M S W D Gender: Male Female Connecticut LTC Level
FLEET STREET NEWS. From the President s Desk... S o u t h e a s t G o v e r n m e n t a l F l e e t M a n a g e r s A s s o c i a t i o n
 Volume 8, Issue 1 Winter 2014 Post Office Box 7824 Columbia, SC 29202 S o u t h e a s t G o v e r n m e n t a l F l e e t M a n a g e r s A s s o c i a t i o n FLEET STREET NEWS From the President s Desk...
Volume 8, Issue 1 Winter 2014 Post Office Box 7824 Columbia, SC 29202 S o u t h e a s t G o v e r n m e n t a l F l e e t M a n a g e r s A s s o c i a t i o n FLEET STREET NEWS From the President s Desk...
Getting Started: Creating a New Account and Logging In
 Getting Started: Creating a New Account and Logging In Welcome to Meals on Wheels America s Online Grant System! Meals on Wheels America will only accept grant applications and follow-up reports that are
Getting Started: Creating a New Account and Logging In Welcome to Meals on Wheels America s Online Grant System! Meals on Wheels America will only accept grant applications and follow-up reports that are
CDDO HANDBOOK MISSION STATEMENT
 Adopted 6-19-09 Revised 11-1-10 Revised 4-30-13 Revised 2-27-17 CDDO HANDBOOK MISSION STATEMENT Arrowhead West, Inc. is the Community Developmental Disabilities Organization (CDDO) for initial contact
Adopted 6-19-09 Revised 11-1-10 Revised 4-30-13 Revised 2-27-17 CDDO HANDBOOK MISSION STATEMENT Arrowhead West, Inc. is the Community Developmental Disabilities Organization (CDDO) for initial contact
RESIDENT SCREENING SHEET
 Department of County Human Services Aging, Disability & Veterans Services Adult Care Home Program RESIDENT SCREENING SHEET MCAR 023-080-200 through 023-080-225: To be completed by the operator before you
Department of County Human Services Aging, Disability & Veterans Services Adult Care Home Program RESIDENT SCREENING SHEET MCAR 023-080-200 through 023-080-225: To be completed by the operator before you
Wisconsin Department of Justice. Egrants System User Guide
 Wisconsin Department of Justice Egrants System User Guide Last updated 11-17/2017 What is in this guide? This guide describes technical steps describing how to apply for and manage a grant in Egrants.
Wisconsin Department of Justice Egrants System User Guide Last updated 11-17/2017 What is in this guide? This guide describes technical steps describing how to apply for and manage a grant in Egrants.
2017 CDBG Applica on Guidelines. State of South Carolina Community Development Block Grant Program
 2017 CDBG Applicaon Guidelines State of South Carolina Community Development Block Grant Program State of South Carolina Community Development Block Grant Program 2017 Application Guidelines State of South
2017 CDBG Applicaon Guidelines State of South Carolina Community Development Block Grant Program State of South Carolina Community Development Block Grant Program 2017 Application Guidelines State of South
Alzheimer s Arkansas is pleased to provide you with information about the Family
 PLEASE READ ALL INFORMATION INCLUDED IN THIS GRANT APPLICATION Dear Caregiver: Alzheimer s Arkansas is pleased to provide you with information about the 2016-2017 Family Caregiver Support Program. Funding
PLEASE READ ALL INFORMATION INCLUDED IN THIS GRANT APPLICATION Dear Caregiver: Alzheimer s Arkansas is pleased to provide you with information about the 2016-2017 Family Caregiver Support Program. Funding
Employee Matching Gift Program Online Registration and Application Guide
 TABLE OF CONTENTS Registering and Accessing the Online Matching Gift System 2 Starting and Submitting a Matching Gift Application 5 Viewing Your Matching Gift Status and History 8 Nonprofit Gift Confirmations
TABLE OF CONTENTS Registering and Accessing the Online Matching Gift System 2 Starting and Submitting a Matching Gift Application 5 Viewing Your Matching Gift Status and History 8 Nonprofit Gift Confirmations
Florida s Statewide Medicaid Managed Care Program. Patient Responsibility for Long-term Care Enrollees Residing in Assisted Living Facilities
 Florida s Statewide Medicaid Managed Care Program Patient Responsibility for Long-term Care Enrollees Residing in Assisted Living Facilities November 16, 2016 What is patient responsibility? The cost of
Florida s Statewide Medicaid Managed Care Program Patient Responsibility for Long-term Care Enrollees Residing in Assisted Living Facilities November 16, 2016 What is patient responsibility? The cost of
Ch COUNTY NURSING FACILITY SERVICES CHAPTER COUNTY NURSING FACILITY SERVICES
 Ch. 1189 COUNTY NURSING FACILITY SERVICES 55 1189.1 CHAPTER 1189. COUNTY NURSING FACILITY SERVICES Subchap. Sec. A. GENERAL PROVISIONS... 1189.1 B. ALLOWABLE PROGRAM COSTS AND POLICIES... 1189.51 C. COST
Ch. 1189 COUNTY NURSING FACILITY SERVICES 55 1189.1 CHAPTER 1189. COUNTY NURSING FACILITY SERVICES Subchap. Sec. A. GENERAL PROVISIONS... 1189.1 B. ALLOWABLE PROGRAM COSTS AND POLICIES... 1189.51 C. COST
Midlands Gives Nonprofit Handbook
 Midlands Gives Nonprofit Handbook A guide to help you navigate and prepare for the 2018 event! 4 Easy Steps to Participate! 1 2 3 4 REGISTER LEARN PLAN PROMOTE HELLO NONPROFITS! Welcome to Midlands Gives
Midlands Gives Nonprofit Handbook A guide to help you navigate and prepare for the 2018 event! 4 Easy Steps to Participate! 1 2 3 4 REGISTER LEARN PLAN PROMOTE HELLO NONPROFITS! Welcome to Midlands Gives
Section 2. Member Services
 Section 2 Member Services i. Introduction 2 ii. Programs and Enrollment Information 7 iii. Identifying HPSM Members 8 iv. Member Eligibility 10 v. Identification Cards and Co-Payments 12 vi. PCP Selection
Section 2 Member Services i. Introduction 2 ii. Programs and Enrollment Information 7 iii. Identifying HPSM Members 8 iv. Member Eligibility 10 v. Identification Cards and Co-Payments 12 vi. PCP Selection
CHILDREN S PERSONAL CARE SERVICES (CPCS): OVERVIEW & UPDATE VERMONT FAMILY NETWORK WEBINAR OCTOBER 28, 2015
: OVERVIEW & UPDATE VERMONT FAMILY NETWORK WEBINAR OCTOBER 28, 2015") 1 CHILDREN S PERSONAL CARE SERVICES (CPCS): OVERVIEW & UPDATE VERMONT FAMILY NETWORK WEBINAR OCTOBER 28, 2015 2 PROGRAM OVERVIEW: WHAT CPCS IS Medicaid benefit for children diagnosed with verifiable longterm
1 CHILDREN S PERSONAL CARE SERVICES (CPCS): OVERVIEW & UPDATE VERMONT FAMILY NETWORK WEBINAR OCTOBER 28, 2015 2 PROGRAM OVERVIEW: WHAT CPCS IS Medicaid benefit for children diagnosed with verifiable longterm
PeachCare for Kids. Handbook
 PeachCare for Kids Handbook Table of Contents What is PeachCare for Kids?...2 Who is eligible?...3 How do you apply for PeachCare for Kids?...3 Who will be your child s primary doctor?...4 Your child s
PeachCare for Kids Handbook Table of Contents What is PeachCare for Kids?...2 Who is eligible?...3 How do you apply for PeachCare for Kids?...3 Who will be your child s primary doctor?...4 Your child s
GERIATRIC SERVICES CAPACITY ASSESSMENT DOMAIN 4 ALTERNATE LIVING ARRANGEMENTS
 GERIATRIC SERVICES CAPACITY ASSESSMENT DOMAIN 4 ALTERNATE LIVING ARRANGEMENTS Table of Contents Introduction... 2 Purpose... 2 Serving Senior Medicare-Medicaid Enrollees... 2 How to Use This Tool... 2
GERIATRIC SERVICES CAPACITY ASSESSMENT DOMAIN 4 ALTERNATE LIVING ARRANGEMENTS Table of Contents Introduction... 2 Purpose... 2 Serving Senior Medicare-Medicaid Enrollees... 2 How to Use This Tool... 2
Connecticut Medical Assistance Program Refresher for Hospice Providers. Presented by The Department of Social Services & HP for Billing Providers
 Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Hospice Agenda Overview Forms Fee Schedule/Reimbursement
Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Hospice Agenda Overview Forms Fee Schedule/Reimbursement
Resident Rights in Nursing Facilities
 Your Guide to Resident Rights in Nursing Facilities 1-800-499-0229 1 Table of Contents The Ombudsman Advocate...3 You Take Your Rights with You...4 Federal Regulations Protect You...5 Medical Assessment
Your Guide to Resident Rights in Nursing Facilities 1-800-499-0229 1 Table of Contents The Ombudsman Advocate...3 You Take Your Rights with You...4 Federal Regulations Protect You...5 Medical Assessment
Printed from the Texas Medical Association Web site.
 Printed from the Texas Medical Association Web site. Medical Power of Attorney Patient and Health Care Provider Information September 1999 General Information To be read by the Patient and Health Care
Printed from the Texas Medical Association Web site. Medical Power of Attorney Patient and Health Care Provider Information September 1999 General Information To be read by the Patient and Health Care
PROVIDER TRANSMITTAL. Assistive Living Facilities and Adult Family Care Home
 PROVIDER TRANSMITTAL Transmittal Number: Provider Type: Subject: 2015-01-28-QM Assistive Living Facilities and Adult Family Care Home SMMC-MMA Assistive Living Facility ( ALF ) and Adult Family Care Home
PROVIDER TRANSMITTAL Transmittal Number: Provider Type: Subject: 2015-01-28-QM Assistive Living Facilities and Adult Family Care Home SMMC-MMA Assistive Living Facility ( ALF ) and Adult Family Care Home
REPORT OF GUARDIAN (Quarterly/Semi-Annually/Annually)
") STATE OF SOUTH CAROLINA COUNTY OF GREENVILLE IN THE MATTER OF: _ (Protected Person Guardianship Established: IN THE PROBATE COURT REPORT OF GUARDIAN (Quarterly/Semi-Annually/Annually CASE NUMBER: 2012GC2300120
STATE OF SOUTH CAROLINA COUNTY OF GREENVILLE IN THE MATTER OF: _ (Protected Person Guardianship Established: IN THE PROBATE COURT REPORT OF GUARDIAN (Quarterly/Semi-Annually/Annually CASE NUMBER: 2012GC2300120
Home and Community Based Services Mental Retardation/Developmental Disabilities Providers
 May 2008 Provider Bulletin Number 869 Home and Community Based Services Mental Retardation/Developmental Disabilities Providers Manual Updates and New Manuals Home and Community Based Services Mental Retardation/Developmental
May 2008 Provider Bulletin Number 869 Home and Community Based Services Mental Retardation/Developmental Disabilities Providers Manual Updates and New Manuals Home and Community Based Services Mental Retardation/Developmental