Clinical Risk Assessment and Management Policy
|
|
|
- Holly Carr
- 6 years ago
- Views:
Transcription
1 Clinical Risk Assessment and Management Policy For Individual Service Users Version: 8 Executive Lead: Lead Author: Approved Date: Approved By: Ratified Date: Ratified By: Issue Date: Review Date: Executive Director of Quality & Safety Consultant Psychiatrist 19 November 2015 Clinical Risk & Learning Lessons Group 17 th December 2015 Policy Panel 17 th December th December 2018 Target Audience: This policy is to be followed by:- All medical staff, nursing and health care professionals and Support staff who are involved in the assessment and management of clinical risk. 1
2 Preface P1 - Version Control History: Version Date of Issue Author Status Comment V7 9 th September 2013 Consultant Psychiatrist Superseded Full review and inclusion of implementation of Paris Electronic Patient Record V7.1 1 st May 2015 Consultant Superseded Updated for Care Act 2014 Psychiatrist V8 17 Dec 2015 Head of Practice Governance Update Updated in consultation with key colleagues to reflect changes in recording P2 - Relevant Standards: a) CQC Fundamental Standards Regulation 9 Person-centered Care and Regulation 12 Safe Care and Treatment b) Equality and RESPECT: The Trust operates a policy of fairness and RESPECT in relation to the treatment and care of service users and carers; and support for staff.. Symbols used in Policies: = internally agreed, that this is a rule & must be done the way described RULE STANDARD = a national standard which we must comply with, so must be followed Managers must bring all relevant policies to the attention of their staff, where possible, viewing and discussing the contents so that the team is aware of what they need to do. Individual staff/students/learners are responsible for implementing the requirements appropriate to their role, through reading the Policy and demonstrating to their manager that they understand the key points. All Trust Policies will change to these formats as Policies are reviewed every 3 years, or when national Policy or legislation or other change prompts a review. All expired & superseded documents are retained & archived and are accessible through the Compliance and Risk Facilitator Policies@hpft.nhs.uk All current Policies can be found on the Trust Policy Website via the Green Button or 2
3 PART: CONTENTS PAGE: Preface Preface concerning the Trust Policy Management System: PART 1 PART 2 P1 - Version Control History P2 - Relevant Standards P3 - The 2012 Policy Management System & Document Format Preliminary Issues: 1. Summary 2. Purpose 3. Definitions 4. Duties and Responsibilities 5. Key Standards What needs to be done and who by: 6. Procedures 6.1 Background 6.2 Risk Assessment and Care Coordination 6.3 The process of Risk Assessment and Risk Management 6.4 Gathering Information 6.5 Identifying situations and circumstances known to present increased risk (critical indicators) 6.6 Risk to Self 6.7 Risk to Others 6.8 Risk of Abuse 7. Recording the risk assessment 7.1 Use of the tools 7.2 Adult Mental Health Risk Assessment 7.3 Child and Adolescent Mental Health Services Risk Assessment 7.4 Forensic Services 7.5 Other Specialist Tools 8. Formulating a care plan to manage risk 9. Monitoring and reviewing the situation 9.1 Risk Review 9.2 Risk Management Panel 10. Support to Staff 11. Communication and Confidentiality 12. Carers 13. Inter-professional Disagreements 14. Health Professionals Regulatory Guidance 15. Training /Awareness 16. Equality and RESPECT 17. Process for monitoring compliance with this document PART 3 Associated Issues 18. Version Control 19. Archiving Arrangements 20. Associated Documents 21. Supporting References 22. Comments and Feedback Appendices 33 3
4 PART 1 - Preliminary Issues: 1. Summary Hertfordshire Partnership University NHS Foundation Trust (referred to in this document as HPFT or the Trust) is committed to the safety and wellbeing of service users, staff and all people visiting or working within the Trust. Clinical Risk Assessment and Management is part of the Trust's overall risk management strategy and is fundamental to patient safety. This policy defines the overarching standards to be employed within all local services relating to the risk assessment and management of individual service users. It should be used by all staff involved in the assessment and management of clinical risk. 2. Purpose The policy sets out the framework for the management of risk related to individual service users in all clinical areas. The policy is followed by procedures which provide more detailed guidance on risk assessment and risk management within services. The procedures are also reflected in relevant Operational Policies. The policy aims to: Provide a framework which enables staff to use best practice in assessing and managing clinical risk Enable staff to practice in such a way that their own professional judgment is encouraged Enable staff to practice in such a way that service users (and carers whenever possible) are genuine partners in considering and addressing their own areas of risk, so that they are supported to find ways to keep themselves and those around them free from harm The guidance is not intended as a substitute for specific training of staff in this area of work. Training on the assessment and management of risk remains a priority area for the Trust. The procedures to be followed are described in Part 2. These apply to all services in the Trust other than the Enhanced Primary care Mental Health Services, who work with a different group of service users. They have developed separate procedures, summarised here in appendix 3. Procedures are designed to support structured clinical judgment (defined below), the approach to clinical risk assessment and management that is favoured both by the Department of Health (DH) (Best Practice in Managing Risk March 2009) and the Trust. This policy should be considered in the context of several other Trust policies, which are listed below under Associated Documents. 3. Definitions Clinical Risk Assessment and Management is defined by the Trust as a continuous and dynamic process for judging risk and subsequently making appropriate plans considering the risks identified. For convenience the term mental health professional may be used, but this should 4
5 be taken as referring to all staff working with service users in this Trust. 4. Duties and Responsibilities The Chief Executive is ultimately responsible for Trust delivery of services in accordance with this policy. The Clinical Risk and Learning Lessons Group, reporting to the Quality and Risk Management Committee, is responsible for monitoring implementation of and compliance with this policy. All operational managers are responsible for ensuring staff who report to them are familiar with this policy. All operational staff are expected to comply with this policy. Each service is responsible for: The implementation and evaluation of risk assessment and management procedures described in Part 2 The supervision of staff in the use of procedures and risk assessment tools Contributing to the audits, learning from incidents and other initiatives which will enable continual improvement of practice 5. Key Standards STANDARD The Trust employs the Department of Health s best practice points Basic ideas in risk management and Individual practice and team working : Basic Ideas in Risk Management: Risk management involves developing flexible strategies aimed at preventing any negative event from occurring or, if this is not possible, minimizing the harm caused. Risk management should take into account that risk can be both general and specific, and that good management can reduce and prevent harm. Knowledge and understanding of mental health legislation is an important component of risk management. The risk management plan should include a summary of all risks identified, formulations of the situations in which identified risks may occur, and actions to be taken by practitioners and the service user in response to crisis. Where suitable tools are available, risk management should be based on assessment using the structured clinical judgment approach. 5
6 Risk assessment is integral to deciding on the most appropriate level of risk management and the right kind of intervention for the service user. Individual practice and team working: Risk management plans should be developed by multi-disciplinary teams and multi-agency teams operating in an open, democratic and transparent culture that embraces reflective practice. All staff involved in risk management should receive relevant training, which should be updated at least every 3 years. A risk management plan is only as good as the time and effort put into communicating its findings to others. In addition, the Trust has set the following standards which are integral to how we approach risk: Be a joint exercise between staff, service user and (where agreed), carers Be empowering for service users and recognize the value of positive risk-taking: Inform and guide the process of care with the service user at the centre Generate fresh ideas for positive risk management which make sense to the service user and which he or she can use Be dynamic and on-going with reviews triggered by needs or events Be recorded in a clear accessible form, and be communicated appropriately Be integral to the wider assessment and care planning process for each service user. (e.g. should be fully compatible with the Care Programme Approach and other care planning processes.) Be carried out by suitably trained and competent staff unqualified staff may not complete risk assessments independently Ensure that the care plan including the risk management plan is guided by the risk assessment. 6
7 PART 2 - What needs to be done and who by: 6. PROCEDURES 6.1. Background Risk and risk taking are intrinsic to practice in Mental Health and Learning Disability Trusts. Properly managed they are a means of encouraging autonomy, choice and participation for users of mental health services and combating their stigmatisation and social exclusion. It is the policy of Hertfordshire Partnership University NHS Foundation Trust that all mental health professionals will undertake or contribute to the assessment and management of clinical risk. 6.2 Risk Assessment and Care Coordination For those with mental health problems, the Care Programme Approach (CPA) was introduced in 1991 and reviewed in 1999 and again in CPA is the approach to care coordination that is applicable to those people under the care of Mental Health Trusts with mental health problems and the most complex needs, whether they are receiving adult (working age or older people s) mental health services, specialist learning disability services, or child and adolescent mental health services. From 2008 there is only one level of CPA. Consideration of risk issues plays an important role in deciding eligibility for CPA. The Trust continues to provide care and treatment to service users who will no longer receive care co-ordination through CPA. These now receive care through Standard Care, supported by a named professional. Many service users in older people s mental health services and in specialist learning disabilities services have their care coordinated through the Single Assessment Process (SAP). Those with dual diagnosis, mental health and substance misuse, should be care coordinated in mental health services and are likely to be on CPA. They may at the same time receive treatment from Substance Misuse Services provided by other agencies. Those receiving enhanced primary care mental health services (Well-being Services), from the Trust, and some of those under the care of CAMHS or specialist learning disability services, will be exempt from CPA and will not require any other formal system of care co-ordination. They should however all have an assessment of needs including risk assessment once accepted into the service, and they should all know who to contact in the Trust if they have a problem. All these approaches to care coordination place the service user at the centre of their own care planning and reflect Trust values and the principles of the recovery approach as adapted by the Trust, encouraging staff to recognise fully the strengths of those with whom they are working and to treat them as individuals. The Delivery of Care Policy (April 2015) describes how risk assessments can be recorded in different ways depending on whether a service user is on the CPA or not. 7
8 6.3 The Process of Risk Assessment and Risk Management The Trust endorses the use of structured clinical judgment as an approach to assessing risk. This approached is encouraged by the Department of Health and the Royal College of Psychiatrists. It involves the use of clinical judgment that is guided by a standardised format, potentially complemented by the use of clinical risk assessment tools. When assessing risk, practitioners are expected to use the relevant forms to guide the process of collating and considering information, and formulating the plan with regard to the relevant risks and associated contributory factors. Some important steps in risk assessment include: Consider the clinical risk management policy and procedures Gather information from the service user, carers and other relevant agencies as appropriate Identify situations and circumstances known to present increased risk Make an assessment of the risk and record the assessment Formulate a plan in collaboration with the service user and carer to manage the identified risks and include a Contingency/Crisis Plan Take the risk assessment into account in deciding if care should be provided under CPA or Standard care (see Delivery of Care policy) 6.4. Gathering Information. The quality of the risk assessment depends on the information available. The amount and accuracy of the information available may vary considerably according to the circumstances and setting where it is carried out. For example, the information available to make an informed risk assessment on an unknown patient newly admitted to a hospital ward in the middle of the night may greatly contrast with the extent of information known about a patient already subject to CPA. The three main sources of information available to staff are: Clinical interview and observation Information from informants (these may be relatives or carers and people from any agency involved in the person s care). Carers provide important information available to make an informed risk assessment, including concerns about the possible risk of deterioration in service users. Documentary evidence available in care records Therefore, in certain cases, staff will not have full information and will have to make the best possible assessment based upon what information is available. As more information comes to light, and with the person better known, the risk assessment and 8
9 care plan should be reviewed and updated. Anyone assessed as posing a risk of harm to self or others should not suffer discrimination because of that assessment. The behavior may be assessed as potentially harmful or dangerous and may legitimately restrict certain services options. It may also entitle the person assessed to special provision because of those needs. When considering information about history of harm to self or others, there are four components which should be considered: Severity Recency Frequency Pattern Attention must be paid not only to actual past harm committed by the person but also to the potential of likely harm and acts of harm which were intended but prevented. These must be given proper consideration and weight so as to avoid the tendency to minimise the potential of harm Identifying Situations and Circumstances Known to Present Increased Risk (Critical Indicators) There are certain general circumstances that may increase a level of risk, such as violence being more likely when drug or alcohol abuse co-exist with major mental illness or when a patient has multiple psychiatric diagnoses. Research has also shown that certain factors including socio-demographic data, past history, and situational factors can particularly be associated with increased likelihood of violence and suicide. As well as general circumstances it is also often possible to identify circumstances in which, based on past experience, it is likely that a particular person will present an increased risk. For example, (but not exclusively): When a person stops medication and has previously been aggressive during an acute phase of an illness When a person who has been suicidal in one particular situation, such as the ending of a close relationship, is faced with another similar situation When a person who has previously offended under the influence of drugs and alcohol starts drinking again, or enters an environment where drugs or alcohol are available When there is an apparent improvement in health though history suggests that this maybe short lived and requires careful monitoring over a longer period of time Where a service user with a learning disability previously inclined to challenging behavior after bereavement suffers a further loss Environmental conditions or events which have been associated with dangerous behaviour or risks in the past should be considered. Situational factors can include loss of employment, financial difficulties, the ending of a 9
10 relationship and sexual exploitation. Evidence of perpetration of, or risk of being subject to, domestic violence should be included in risk assessment. Personal triggers are factors internal to the person which have been historically identified as related to risk e.g. deterioration in mental state stress reactions, loneliness or other emotional states. These should also be considered. The person may demonstrate warning signs of risk behaviours. They are observable behaviours which have been noted to be present when harm is about to happen. For example, pacing, swearing, threats of self-harm, stalking, refusal to eat, refusal of medication. Wherever possible, staff should consider both general factors and information relevant to the individual based on their history. Staff must use their professional judgment to decide on the weight to give each factor. Wherever possible this should be done in a multi-disciplinary setting in order to capture the most complete picture of risk Risk to Self This can be considered under separate headings: suicide, deliberate self-harm, accidental self-harm, and self-neglect. Suicide Three elements are especially important in assessing the risk of suicide: Knowledge of general risk factors for suicide Knowing the individual well their history, and their protective and vulnerability factors Skills in making direct enquiries about suicidal intent, based on a close and trusting therapeutic relationship An example of general risk factors for suicide is the knowledge that at present in the UK males aged 35 to 70 are known to be at particularly high risk for suicide. This demographic factor should be taken into account in practice. The Patient Safety and Practice Governance Leads will keep staff informed about any significant demographic trends of this kind. Patient Safety and PG leads will also use reports such as those by the National Confidential Inquiry into Suicides and Homicides to keep staff appraised of trends. The period around inpatient discharge can be a time of particular high risk of suicide, emphasizing the need for proper assessment prior to discharge and effective follow up (see Discharge and Transfer of Service Users within the Care Planning Process Policy and Procedures (incorporating 7 day follow-up requirements). A breakdown in the continuity of care by either carers or professionals can significantly increase the risk of suicide post discharge. This could include key personnel being on leave or leaving or a change of Consultant since the admission. The most obvious warning sign is a direct statement of intent. This should never be ignored, although it needs to be carefully assessed with each service user each time such a statement is made. Those who are suicidal can fluctuate between a wish to live and a wish to die. More 10
11 than half of those under the care of the Trust who commit suicide have contact with a member of staff within 7 days of the event. With skilled questioning on the basis of a strong therapeutic relationship, staff can be well placed to elicit signs of high suicidal intent. However an expression of lack of suicidal intent does not necessarily indicate lack of risk. It may be that the service user is trying to avoid accessing services so that they can commit an act of self-harm or suicide, or their intent may be fluctuating. It is important always to be psychologically-minded in assessing risk for suicide. In this context, hopelessness is known to be a key factor. More recently, the feeling of being a burden to others has been confirmed as often very important. A care plan to manage the risk must urgently be put in place when risk of suicide is expressed. The care co-coordinator and the Consultant Psychiatrist (where there is one) may need to be informed and this will trigger a review of the risk assessment and care plan. Carers must always be involved at this stage, with the service user s consent or without it if the risks are grave. Consideration should be given to whether the use of the Mental Health Act is appropriate. Deliberate Self Harm People who have committed non-fatal acts of self-harm are at an increased risk of committing suicide at a later date. The highest risk is in the first three years, especially the first six months following an overdose. Factors associated with a higher risk of repetition of deliberate self-harm include: Substance misuse problems Diagnosis of personality disorder Previous psychiatric inpatient treatment For those in longer term care, deliberate self-harm can be a feature of frustration and boredom. For those with limited verbal skills, this pattern of behavior may be adopted by people who cannot otherwise express their distress. These factors may be prevalent in services for adults with learning disabilities. Deliberate self-harm is also a common pattern of behavior amongst adolescents and such incidents should always be carefully assessed. Accidental Self Harm Desperate or reckless behaviour can be expected to be more common in those with a diagnosis of borderline personality disorder and those with drug and/or alcohol issues. It may be hard to separate out what behaviours are intended and what are accidental. Whether the risk is of deliberate or accidental self-harm (or a mixture of the two), it should be assessed with equal care as in each scenario the outcome can be fatal. Service users especially but not only frail elderly people may be at risk of falls and pressure ulcers. See relevant practice policies. For those with learning disabilities there is a strong role for programmes and individual support in self-care in all settings including kitchens, traffic and other potentially hazardous environments, to help service users develop their skills in staying safe. 11
12 Risk of Self-neglect. Assessment of risk of self-neglect may include assessment of: Hygiene Diet Infestation Household safety Warmth Hoarding behaviours A failure to eat or drink adequately may be acute, severe and life threatening. On the other hand, it may result in slow deterioration in health and nutritional status and not be recognised initially by professionals or carers. This is a complex area for assessment. Professionals have to balance an acknowledgement of relative standards and the service user s right to be protected from unnecessary interference against the need for accurate assessment of a person s circumstances and responsibility for intervention where severe self-neglect is likely. Active follow up in the community may be necessary and a contingency plan should be in place when a service user who is considered high risk does not keep an appointment or is not at home when visited. Wherever possible interventions should be with the consent of the service user however when the situation may be life threatening then consideration needs to be given to the use of the Mental Health Act Risks to Others General. Predicting dangerous or violent behaviour is an inexact science. The most reliable long term predictor of violent behaviour is previous violent behaviour, hence the importance of full, accurate and up to date information, communication and recording. This should include any incidents of harm to others (including history of offending) and any history of carrying of instruments that have potential to cause harm, including knives. Victims are more likely to be family members or those trying to deliver care and support. In assessing risk of violence, consideration should be given to the risk for family and carers and in addition the need to protect any particularly vulnerable adults or children in the household. Assessing the Risks of Violence: Identifying situations or circumstances in which, based on previous experience, the service user is likely to become violent. Trying to see the behaviour from a service user s point of view can be very revealing in terms of risk assessment. Liaison may occur with the probation and police service if they are currently involved with the service user or have had previous involvement in order to exchange appropriate information and to develop a jointly agreed risk management plan. (Multiagency public protection panels should be used where appropriate). The Trust s Community Forensic Service can advise staff on the process for obtaining criminal records from the Police. When assessing individuals for risk of violence and when 12
13 concerns are great, it is reasonable to seek such information through the advice of the Forensic Team Attention must be paid not only to actual past harm committed by the person, but also to the potential for harm. Acts that were intended to harm or could have harmed but which were prevented, must be given proper consideration and weight so as to avoid the tendency to minimise the potential risk of harm. The assessment should aim to identify not only the nature of the risk of violence but also identify who is at risk. In specific forensic settings, appropriately trained staff are expected to use the HCR 20 to assist in the assessment of risk of violence to others Carers. Carers are often particularly at risk of violence from the person they care for and staff should be sensitive to this (see section 11 below) Risk to Staff Managers within the Trust must comply with the legislative requirements set out in the Health and Safety procedures relevant to their Departments. In particular this requires managers to undertake health and safety risk assessments to identify hazards and evaluate risks to staff. Physical and verbal violence towards staff requires immediate management action. Trust managers are responsible for the development, implementation, monitoring and review of safe working practices and procedures in all environments where staff have contact with service users. This is particularly important where staff are working alone in the person s home or in community settings such as dispersed day care activities. Each team should review its safe working procedures annually or more often if the need arises. Staff also have responsibilities and need to ensure they consider the risks that may occur during the course of their work. In order to do this they need to check on current risk status before interviewing a service user and take all appropriate steps to ensure their own safety during any encounter. They should also comply with Trust policy and use the protective devices now provided (see Lone Working Policy). Alerts should be placed on the service user s electronic patient record when significant risks have been identified, especially when these are about the safety of others Risk to staff in other Provider Agencies It is essential that with any referral to a care provider within the Trust or outside the Trust, consideration should be given to provision of an unambiguous, accessible and up to date risk assessment and management plan, with the new provider s responsibilities clear, and agreed by them. When someone is transferred from inpatient status to community services including CATT, this decision should in all cases be informed by an updated risk assessment. Likewise, when someone is transferred from CATT to non-acute community services, this decision should be supported by an updated risk assessment, completed within 48hours of the transfer. 13
14 Service users must be consulted, understand the reasons for sharing the information and agree to this action. If service users refuse to share the information then it may not be possible to commission a particular service. There are some particularly dangerous situations when information needs to be shared without consent. Professionals should adhere to the principles and guidance offered by their professional body that clarifies the circumstances in which confidential information may be shared with other agencies in the public interest. Further information regarding this can be found in HPFT Policy, Procedure and Guidance on the Management of Care Records and Inter-agency guidance on sharing information Risk to a Child or Young Person (under 18yrs old) Parental mental ill-health is known to be a significant factor in many cases of child abuse. Thus, risk assessments of adult service users must include gathering all child identifiable data in every case. Information about identified children needs to be reviewed during significant changes of circumstances and care reviews, as part of the risk assessment. On the basis of the information included within this document, a decision should then be made with regards to whether a referral to Children s Services may be necessary. This is of particular importance when the adult is a lone parent or the main carer of children. Where possible the mental health professional involved in the case should meet the children and observe their physical condition and behaviour. Concerns should always be discussed with the parent. However, where doubts remain the line manager must always be informed and advice should be sought from the Trust s Safeguarding Children Lead (Named Nurse or Named Doctor). If a referral to Children s Social Care is required, there should be two separate but integrated care plans - one, focusing on the needs of the child managed by the children's service and another focusing on the needs of the adult managed by the Trust services. The respective care co-ordinators should work in close liaison and attend care planning and review meetings for both child and adult as necessary. The welfare of a child is paramount (Children s Act 2014).Timely communication and the sharing of information is a key factor in ensuring that children are protected from harm. Confidentiality of the parent or service user may be overridden in these circumstances. The team manager must be informed about concerns in the response by children's social care to a referral. If the team manager cannot resolve the concerns through discussions with the other agency it must be escalated to the Trust Safeguarding Children Lead (Named Nurse or Named Doctor). In all cases a further referral must be made if new concerns arise. Consultant Psychiatrists must always be informed and directly involved in clinical decisions for service users who express delusional beliefs or suicidal ideation that may involve and pose a risk to children. Where the service user is an inpatient this will include any decision regarding discharge, leave, CPA reviews or contact arrangements with children. These decisions must not be delegated to a junior doctor. The above cases are likely to be the small minority. Therefore, Care Coordinators must have a low threshold for acting in cases where there may be a significant risk to children. 14
15 All such cases must be discussed in the multi-disciplinary team meeting to ensure a group decision is taken about how to manage risks and plan actions. When a Consultant Psychiatrist is not present at the meeting the discussion must include whether it is necessary for the Consultant to be alerted to the case to make a decision about whether there is a need for direct Consultant involvement and / or oversight of the case. If urgent action is required to safeguard a child, before the routine team meeting, the clinician must seek advice from the manager or senior clinician immediately and make a referral to Children s Social Care. If in any doubt advice should be sought from the Trust Safeguarding Children Lead (Named Nurse or Named Doctor), although this should never cause a delay to safeguard a child. When considering the risk presented by mental illness or substance misuse from someone who is also a parent, or is significantly involved in the care of children, it is important to consider specifically the risks that the children may encounter as a result of the parent s potentially impaired parenting abilities. The following are examples of specific risks to children: Severe postnatal depression and Puerperal Psychosis carry particular risks for babies and children. Adults with moderate to severe learning disabilities may lack the knowledge and skills to provide adequate parental care. Continuous or frequent intoxication due to alcohol or drug misuse can lead to dangerously low levels of parental care and supervision. Psychosis can result in physical or emotional neglect or abuse of children. The risk is high if an adult has delusional beliefs which involve a child Severe obsessive compulsive disorder can place children under intolerable pressure to comply with rituals and routines resulting in impaired social development and schooling. Suicidal thinking that includes a child in a suicide pact Children should not be expected to be the main carers for adults to the detriment of their own needs for care and development Risk of Abuse or Exploitation by Others Safeguarding Adults All staff, agencies and service providers must work within the law and must not support or condone abuse to vulnerable adults. Where abuse is occurring or believed to be occurring then staff must pass their concerns on to a responsible person. The Safeguarding Adults from Abuse procedures must be followed where there is concern that abuse of a vulnerable adult may have occurred. In all cases where there is actual or risk of potential abuse or exploitation, staff should consult the HPFT Safeguarding Adults link policy read in conjunction with the following policies and procedures: For staff working in Hertfordshire, the HPFT policy and procedure is adapted from and must be used in conjunction with the Hertfordshire Interagency Procedure for the Protection of Vulnerable Adults (Safeguarding Adults from Abuse) which is established as the one procedure in the county, used by public agencies and private voluntary services in the protection of vulnerable adults from abuse. For staff working in Norfolk, the HPFT policy and procedure is adapted from and must be used in conjunction with the Norfolk Vulnerable Adults at Risk of Abuse, Joint 15
16 Policy and Operational Procedures developed by Norfolk Social Services, Norfolk Constabulary and Norfolk Primary Care Trust. For staff working in Essex, the HPFT policy and procedure is adapted from and must be used in conjunction with the Southend Essex Thurrock (SET) Safeguarding Adults Guidelines. In situations where staff have concerns about a vulnerable adult it is essential to consider whether there are grounds for using legal powers to protect the service user and/or their assets. Risk assessment and protection planning are of paramount importance in supporting and reducing any further risk of abuse to the vulnerable adult. Further guidance and contact details can be obtained from the HPFT link Safeguarding Adults From Abuse Policy and the Head of Safeguarding. A significant proportion of service users may be at risk of domestic violence. Whether or not the victim is considered vulnerable, staff should take the necessary steps to help the individual be safe according to policy. Finally in this section, the Prevent Policy guides staff on their responsibilities in being vigilant to service users being groomed into extremism or terrorist activity. 7. Recording the Risk Assessment The nature of the risk assessment will be dependent upon how well known the service user is to the professionals completing the assessment. A risk assessment that takes place within an initial interview in Accident and Emergency or when someone is admitted as an emergency in the middle of the night will be different from a risk assessment that is part of the ongoing management of a long term case. In a similar manner a service user who is only seen in an outpatient clinic and is assessed as low risk and maintained on Standard Care, will not need a complex care plan or complex risk assessment. A record of a risk assessment: Provides an explanation of how conclusions about risk are reached which can inform the practice of all Captures the risk history which needs to be available to all colleagues dealing with the service user Captures the protective factors and strengths of the service user as a basis for them to be developed further Allows for reports on completion of risk assessments to be provided to managers so that good practice can be maintained The Care Co-coordinator is normally responsible for ensuring the appropriate risk assessment is completed (during an in-patient admission the role may be delegated to the Named Nurse). For Standard Care this may be an individual worker. For CPA (or equivalent) this will be the designated Care Co-coordinator or Named Nurse in discussion and agreement with the multi-disciplinary team where appropriate. When a risk assessment has to be completed at the time of an emergency, such as an unplanned admission to hospital, the person responsible will be the most senior professional involved in the emergency. This is likely to be the admitting doctor and the most senior nurse present. All professionals involved in emergency admissions should jointly participate in the completion of the risk assessment and sign the record. Risk 16
17 assessments made during emergencies should clearly state the review date and consideration should be given to an early review. When necessary, in high-risk situations, this may need to be within 72 hours. 17
18 Assessing risk and the attendant management plan will have a slightly different focus dependent upon whether the service user has a mental illness, a substance misuse problem or a learning disability, and on whether they are a child, young person, or adult Use of the tools RULE A risk assessment should be completed at the following points in the service user s care pathway: a. On referral to the Trust, the Single Point of Access service will complete a risk assessment as part of their triage. This is not comprehensive and its prime purpose is to ascertain the level of urgency of each referral b. A full risk assessment will be completed as part of the assessment process alongside the needs agreement c. A full risk assessment will be completed whenever a CPA review takes place that is, when there are significant changes of need and at least annually. d. For those on Standard Care, the GP letter may be used as the risk assessment record rather than the separate form; this must be done at least annually e. A full risk assessment will be completed when a service user is transferred between services under CPA. This will generally be completed by the receiving team when they take over the case. The exception to this is in inpatient services, where both the risk assessment on admission and the one on transfer out of inpatient care will be completed by the named nurse. f. In the case of transfers from all inpatient care, when the transfer destination is a funded health or social care placement, there must be a risk assessment that the manager has signed off as up to date before transfer to the placement takes place The descriptions of the risk assessment tools that follow are to be considered just that; tools to assist in the process of risk assessment. They are not a format to record risk, but act as a structure to guide the clinician in their thinking, so that the risk assessment can be as comprehensive as possible. The document is intended to be live that is, not something that is completed once the risks have been assessed but a tool that structures the consideration of the risks with the information presented. By prompting the clinician to consider details that are relevant to risk assessment that may be over looked, e.g. history of substance using behaviour, it supports the clinicians in considering a variety of possibilities. Clinicians are then better placed to make more sophisticated and meaningful management plans. This is the essence of structured clinical judgment Adult Mental Health Risk Assessment Form (Appendix 1) It is to be used for: New mental health service users at initial assessment Those on CPA whenever the risk assessment needs to be repeated It may be used for those on Standard Care. 18
19 Who records and signs: The person conducting the initial assessment, or the Care Coordinator. Who receives a copy: HPFT staff who need to know will access the risk assessment on the EPR. With whom should the information be shared: This is a professional decision however in situations of high risk it is important to consider the need to share information with other agencies, carers, and providers of other services. See section 11 Communication and Confidentiality. When completing the form for new users of the service consideration should be given to the appropriate level of CPA or whether no further input is required by the specialist services. The management plan should detail these issues. For example: If high risk has been recorded the assessor may then be discussing the case in a multi-disciplinary forum such as a ward or CMHT meeting. This would form part of the immediate management plan. If risk is assessed as low and the person does not require specialist mental health services but social or family factors cause some concern the immediate management plan may be giving information on community agencies such as CAB and Relate and referring back to the GP. Care Act responsibilities are significant here. Information recorded on all risk assessment forms should be verified and the source identified on the record Child and Adolescent Mental Health Services Risk Assessment Form ( Appendix 2). CAMHS service users may experience the full range of clinical risks associated with mental ill health, including suicide. High rates of deliberate self-harm and of self-neglect associated with eating disorders can be expected, as well as risk from others including abuse and exploitation. All service users under the care of CAMHs will receive an initial risk assessment, including Forest House and C- CATT, using the specialised CAMHS Risk Assessment Tool on the EPR. Please see tool at Appendix 3. Those managed under CPA should have further risk assessments at review or when circumstances significantly change, documented on the same EPR form. For those not on CPA documentation of risk and its management in the GP letter is acceptable, or else the risk assessment form must be used Forensic Services In all HPFT forensic services, Structured Professional Judgment risk assessment will commence prior to admission. The mainstay of this will be a combination of HCR-20 and START. At pre-admission meetings the (H) score of the HCR-20 will be initially rated based on the preadmission assessment. This will be reviewed and updated prior to initial CPA, at 6 to 12 weeks post-admission. Initial START risk assessment will take place prior to the first 19
20 CPA. HCR-20 and START will be reviewed prior to every subsequent CPA meeting. CPA reviews will take place at minimum once every six months. A CPA/117 meeting will take place prior to discharge from inpatient care, at which all risk assessments will be reviewed in light of the proposed discharge destination. Where an individual is due to be discharged into the care of an HPFT team or clinician, the HPFT risk assessment tool will be completed at the CPA prior to discharge, for familiarity of communication. Other Structured Professional Judgment tools, such as SAPROF, SVR-20 will be completed as necessary, based on the clinical scenario Other Specialist Tools For specialist settings, or for individuals with particular areas of risk, many tools have been developed to assist in the risk assessment. A selection of such tools has been made by the Department of Health (see Best Practice Guidance June 2007). The Trust has centrally approved for use the Beck Hopelessness Scale and has organised licenses for teams. All services are now able to use this tool to inform their risk assessment if they feel it is appropriate. Manuals for use have been distributed to teams along with the assessment forms. If practitioners use this scale, it is appropriate to scan the original form onto the electronic care record. Reference to the use of the scale should be made in the Risk Assessment form. Use of any such tools would complement the regular Trust risk assessment procedures outlined above, and not replace them. A range of other tools may be helpful in assessing clinical factors relevant to risk. These include: Beck Depression Inventory HCR - 20 Hare Psychopathy Checklist Edinburgh Post-natal Depression Scale MHSOP Falls Risk Assessment Tool Waterlow Pressure Sore scale HPFT Dysphagia and Nutrition Screening Tool Clifton Assessment Procedures for the Elderly Geriatric Depression Scale START (Short-Term Assessment of Risk & Treatability) It is the responsibility of individual staff to ensure that they are appropriately trained and that if required they are covered by a licence, before using these tools. 8. Formulating a Care Plan to Manage Risk In order to be effective a risk assessment must be communicated and acted upon. Risk management is about evaluating the risks identified in the risk assessment process, taking into account the possible beneficial and harmful outcomes, and subsequently planning and implementing appropriate strategies to reduce these identified risks. The aim should be to identify the vulnerabilities and strengths of the service user which contribute to the risk 20
21 equation, and develop or reduce these proportionately; the risks should alter accordingly. This is an integral part of Care Co-ordination, and the Care Plan produced needs to clearly specify how needs are to be met and the risks managed. It should ideally be planned in collaboration with the service user and carer (where appropriate), and copies of the written plan should be provided to the service user and carer (if the service user consents). Using the information gained from the risk assessment and the assessment of need, the care plan is formulated and recorded by the Care Co-ordinator or named professional. This may be undertaken in a multi-disciplinary forum for service users monitored on CPA and in a clinical interview or meeting for those maintained on Standard Care. The risk management plan often known as Staying Safe forms a core part of the care plan, which is developed with and shared with the service user and carer as appropriate. This forms the basis for a partnership between staff and service user, working together to build strengths, avoid harms and move towards independence. 9. Monitoring and Reviewing the Situation 9.1. Risk Review CPA A review should also use Structured Clinical Judgment, following the guidance above. A new Risk Assessment form should be completed at each CPA review and at other times when risks significantly change, which should bring forward historical information from previous assessments and include new history since the last assessment. Who records and signs: Care Coordinator with input from any other professional involved in the care plan. Who receives a copy: All those present at the CPA or Professional Review Meeting. Where separate records are held by other disciplines a copy of the new risk assessment should be placed on each file. With whom should the information be shared: All those contributing to the care plan should receive the information. In situations of high risk it is important to consider the need to share information with other agencies, carers, and any providers of other services who may need to know. See section 10 Communication and Confidentiality. Standard Care As with initial risk assessments, risk assessments at review for those on Standard Care do not have to be recorded on the risk assessment EPR document. They can be recorded in the GP letter. In all cases: risk assessments should be reviewed when there are any changes that cause concern. when someone is transferred from inpatient status to community services including CATT, 21
22 this decision should in all cases be informed by an updated risk assessment. Likewise, when someone is transferred from CATT to non-acute community services, this decision should be supported by an updated risk assessment, completed within 48 hours of the transfer. (See Transfer and Discharge Policy section 5). when someone is transferred from inpatient care to a funded placement, there should always either be a new risk assessment within 48 hours of the placement starting or a signed checklist stating that the previous risk assessment remains valid as a minimum all risk assessments should be reviewed annually. In urgent situations the Care Coordinator, or during in-patient admissions the Named Nurse, may need to take immediate decisions in managing clinical risks without a formal review of the care plan and in these circumstances this should be communicated to the multi-disciplinary team and a formal review arranged as soon as possible. Changes in risk also should prompt consideration of a review of the level of Care Coordination. 9.2 Risk Management Panel From time to time a team may be faced with a challenging case where they have an ongoing duty to provide care and treatment to a service user, but where it is extremely difficult to ensure that the service user and those around her or him including Trust staff can remain safe. In some parts of the Trust risk meetings often known as professionals meetings are already used to enable complex and high risk situations to be though through by a range of staff. Psychiatrists will also sometimes seek a second opinion when faced with a challenging or especially complex case. The Risk Panel is available to staff when all other sources of extra advice have been exhausted. The Panel Function - The panel s main function is to provide expert advice to the care co-ordinator and other Trust staff contributing to the care plan, on the future management of an individual service user. It will: Provide a broader perspective on a case in a situation where the local ward/team may be finding it difficult to maintain a clear objective view of the needs of the service user Make available professional advice which brings additional expertise to the case and also a multi-disciplinary perspective More detail is provided in Appendix Support to Staff Working with high risk can be stressful and time consuming. To support this process, staff and their managers must ensure the following are in place: All HPFT staff must have regular training on the management of violence and 22
23 aggression Staff training in risk assessment will occur at a minimum of 3 yearly as recommended by the National Confidential Inquiry into Suicide and Homicide by people with Mental Illness and the Department of Health All staff involved in risk assessment and management should receive regular supervision as set out in the HPFT Performance, Review and Development Policy. High-risk cases should only be allocated to suitably experienced staff as judged by the line manager Staff should alert their line managers to all cases that are assessed as high risk by the multidisciplinary team Risk status should be considered when cases are allocated Careful workload management should ensure staff have sufficient time for the work required in such cases Staff should be clear about line management accountability and to whom they should report any clinical concerns. In the case of any situation which is identified as high unmanaged risk this must always be reported immediately Staff should be proactive in bringing high risk cases to supervision Staff should be made aware of internal and external staff support systems 11. Communication and Confidentiality Issues of good communication and of sharing relevant information amongst members of the multi-disciplinary team are fundamental to the operation of an effective coordinated service and yet may appear, at times, to be at odds with the safeguards around confidentiality which are required by many professional organisations. The key to successfully treading this course is to ensure the service user is consenting to the sharing of relevant information with other agencies that have legitimate grounds for being advised of such information. By the nature of some meetings, such as multidisciplinary CPA meetings, this may be self-evident to the service user, particularly if thorough and adequate introductions are undertaken at the commencement of the meeting. In other cases, often those at Standard Care level where there is pre-dominantly unidisciplinary working it may be much less clear to a person that information may need to be shared with other agencies. Therefore the agreement and consent of the person to relevant disclosure, needs to be sought explicitly. In situations of high risk, there needs to be a final judgment by the relevant Consultant and/or Care Co-coordinator as to whether there may be sufficiently strong grounds for over-ruling the request of a service user who has asked that information not be shared with other disciplines or agencies. This may be considered appropriate where it is judged that the public interest outweighs the duty of confidentiality. Issues of safety to the public, carers, staff and children may take priority over the right to confidentiality. For further information please see Care Records Management Policy. 12. Carers Staff should routinely work in partnership with carers in assessing and managing risk. 23
24 Carers can often contribute very sensitive information about risk factors for the person they care for, and they are also often in a position to be managing most of the risks presented on a daily basis. Carers provide important information to make an informed risk assessment in relation to concerns about the possible risk of deterioration in service users. When attending an appointment with the service user, a carer should be offered time to discuss privately any concerns they might have, including risks for the service user. It is not necessary for the service user to have given permission when the carer is simply sharing information that they have which helps Trust staff assess and manage any risks. Confidentiality rules should not be used as an automatic barrier to communicating with carers. Staff should explain to service users both the importance of confidentiality rules but also the advantages of permission being given for carers to be given clinical and risk information so that they are fully equipped to help ensure the safety of the person they care for ( and also of themselves). Carers should be treated as key allies in the risk management plan. Once identified, they should always be offered a carer s assessment. Further details can be found in the Consensus Statement: Information Sharing and Suicide Prevention( Department of Health, January 2014). 13. Inter Professional Disagreements It is important that all agencies involved in the care of service users clearly and openly debate the issues involved in risk assessment and risk management and agree a single care plan which is owned by all parties. Staff of the Trust have a responsibility to ensure that their professional and/or employing agencies concerns are taken note of and fully considered in drawing up a risk management plan. Where local discussions within a multi-disciplinary team cannot resolve inter-professional differences, staff should inform their line managers so that issues can be addressed at a higher management level. Such disputes will be rare. 14. Health Professionals Regulatory Guidance Health professionals of all disciplines have an ongoing requirement to fulfill the registration requirements of their own professional regulatory body i.e. the GMC (medical staff), NMC (nursing staff) or HPC (AHPs). These regulatory bodies may periodically issue their own guidance, standards, advice or position statements with which professionals are required to comply as a condition of their continuing professional registration. This policy is not intended to supersede or override guidance as provided by a regulatory body. 15. Training / Awareness STANDARD Training will be available to all members of staff who are involved in the assessment and management of clinical risk. 24
25 Following training needs analysis, these categories of training have been agreed: New practitioners including doctors, will be introduced to the clinical risk policy and procedures as part of local induction All practitioners will receive refresher training at least every 3 years Staff in specialist settings, and/or who need to use specialist risk assessment tools, will receive additional training as necessary The Trust will ensure that such training is provided, and staff will attend as directed. Further support and advice for staff in risk assessment and management practices, will be available through supervision and informal support, and if necessary through the Risk Panel. In carrying out risk assessment and management, professionals will refer to the guidance given by the Department of Health ( Best Practice in Managing Risk (March 2009)), the Royal Colleges, the Nursing and Midwifery Council or other professional organisations. Training Template: Course For Renewal Period Clinical Risk Assessment for Individual Service Users Bespoke Training in Clinical Risk Assessment All clinical staff Key teams eg. CATTs (Band 5 and above) Every 3 years Every 3 years Delivery Mode Taught course half day Taught course half day Contact Information For taught courses, contact the Learning & Development Team: Learning@hertspartsft.nhs.uk You can check for future dates here, and request a specific date. 16. Embedding a culture of Equality & RESPECT The Trust promotes fairness and RESPECT in relation to the treatment, care & support of service users, carers and staff. RESPECT means ensuring that the particular needs of protected groups are upheld at all times and individually assessed on entry to the service. This includes the needs of people based on their age, disability, ethnicity, gender, gender reassignment status, relationship status, religion or belief, sexual orientation and in some instances, pregnancy and maternity. 25
26 Working in this way builds a culture where service users can flourish and be fully involved in their care and where staff and carers receive appropriate support. Where discrimination, inappropriate behaviour or some other barrier occurs, the Trust expects the full cooperation of staff in addressing and recording these issues through appropriate Trust processes. Access to and provision of services must therefore take full account of needs relating to all protected groups listed above and care and support for service users, carers and staff should be planned that takes into account individual needs. Where staff need further information regarding these groups, they should speak to their manager or a member of the Trust Inclusion & Engagement team. Where service users and carers experience barriers to accessing services, the Trust is required to take appropriate remedial action.. Service user, carer and/or staff access needs (including disability) The Clinical Risk Policy and procedure has been developed based on feedback from service users and carers and piloted in service areas with service users. As an important part of the clinical process, it is important that all staff working within the Trust are aware of issues relating to equality and diversity for service users and carers and are able to understand how to ask the questions to ensure the needs of protected groups are upheld at all times and assessed appropriately whilst under Trust services. A minimum requirement consistent with the promotion of equality of opportunity for service users and carers is to make all reasonable efforts to ensure that an appropriate interpreter is able to facilitate communication between Trust staff and service users and carers if their preferred spoken language is not English including ensuring availability of British Sign Language (BSL) interpreters. Being aware of alternative methods of communication for profoundly deaf services users during the clinical risk assessment process. Ensuring that people with learning disabilities do not suffer disadvantages and are supported appropriately during the risk assessment process. Understanding the needs of all protected groups and what issues they might be experiencing that has led to them accessing the service. Observing the principles of the RESPECT campaign at all times. Involvement The development of the clinical risk assessment process has been based on trials involving a diverse range of staff, service users and groups in shaping and testing the tools. This has enable consultation that is informative and meaningful, and ensures there has been no unlawful discrimination in the development of policy and procedures. 26
27 Relationships & Sexual Orientation Culture & Ethnicity Spirituality Age Gender & Gender Reassignment Advancing equality of opportunity Clinical risk assessment is an assessment tool and as such take into account the needs of service users. Staff will document any risks associated with relationships, existing or not, for the information of staff responsible for the care and treatment and they may be factored into the risk management plan. They will likewise take account of any issues around sexual orientation (and any barriers for people around their orientation) as well as any relevant issues regarding nearest relatives and family carer or pregnancy during the risk assessment. Trust staff will take account of the needs of people based culture and ethnicity gathering relevant information such as language, and diet and any other cultural needs identified during the risk assessment process. Trust staff will take account of any expressed spirituality that is identified in the initial clinical risk assessment. Clinical risk assessment is undertaken to all service users regardless of age and will ensure that older adults and young people do not suffer disadvantage and are supported appropriately through the service and communicated with in a way that they respond to. Trust staff will take account of the gender of all service users they undertake a clinical risk assessment on and consider the needs and risks associated with transgender service users and carers. This will be used to inform appropriate gender of onward care givers/assessors/clinicians. Staff have a responsibility to challenge any discrimination they may witness and report back in accordance with risk management and incidents processes. Promoting and considering individual wellbeing Under the Care Act 2014, Section 1, the Trust has a duty to promote wellbeing when carrying out any of their care and support functions in respect of a person. Wellbeing is a broad concept and is described as relating to the following areas in particular: Personal dignity (including treatment of the individual with respect); Physical and mental health and emotional wellbeing; Protection from abuse and neglect; Control by the individual over day to day life including over the care and support provided and the way in which it is provided; Participation in work, training, education, or recreation; Social and economic wellbeing; Domestic, family and personal; Suitability of living accommodation; The individual s contribution to society. There is no hierarchy and all should be considered of equal importance when considering an individual s wellbeing. How an individual s wellbeing is considered will depend on their individual circumstances including their needs, goals, wishes and personal choices and how these impact on their wellbeing. In addition to the general principle of promoting wellbeing there are a number of other key principles and standards which the Trust must have regard to when carrying out activities or functions: The importance of beginning with the assumption that the individual is best placed to judge their wellbeing; The individual s views, wishes, feelings and beliefs; 27
28 The importance of preventing or delaying the development of needs for care and support and the importance of reducing needs that already exist; The need to ensure that decisions are made having regard to all the individual s circumstances; The importance of the individual participating as fully as possible; The importance of achieving a balance between the individuals wellbeing and that of any carers or relatives who are involved with the individual; The need to protect people from abuse or neglect; The need to ensure that any restriction on the individuals rights or freedom of action that is involved in the exercise of the function is kept to the minimum necessary 17. Process for monitoring compliance with this document Action: Lead Method Frequency Report to: Review of compliance with this policy PACE Team Audit Annually Clinical Risk and Learning Check policies compliance via serious incident investigations Use of the new supervision tools in AMH community ssservicesservi Patient Safety Manager Root cause analysis investigation On going SLLs Supervision Ongoing Lessons, Quality and Risk Management Committee Service users, staff and carers are encouraged to express any safety and security risks to staff at a local level. Information should be gathered to highlight concerns which may trigger the need for local audit and review, or to highlight good practice. 28
29 PART 3 Associated Issues: 18. Version Control STANDARD Version Date of Issue Author Status Comment V4 Oct 2005 Head of Superseded Practice Governance V5 July 2008 Head of Practice Governance Superseded Approved Trust Executive Team V5.1 August 09 Head of Practice Governance V6 V7 20 th August th September 2013 Consultant Psychiatrist Consultant Psychiatrist V7.1 1 st May 2015 Consultant Psychiatrist V8 17 Dec 2015 Head of PG Governance Superseded Superseded Superseded Current Interim update Archived Executive agreement Appendix 4 Procedure for placing a risk of violence marker on electronic and paper records included Minor amendments will need review and rewrite following implementation of Paris Electronic Patient Record Updated for Care Act 2014 Addendum Updated in consultation with key colleagues to reflect changes in recording 19. Archiving Arrangements STANDARD: All policy documents when no longer in use must be retained for a 29
30 period of 10 years from the date the document is superseded as set out in the Trust Business and Corporate (Non-Health) Records Retention Schedule available on the Trust Intranet A database of archived policies is kept as an electronic archive administered by the Policy Coordinator. This archive is held on a central server and copies of these archived documents can be obtained from the Policy Coordinator on request. 20. Associated Documents This Policy and associated procedures should be used in conjunction with the following Hertfordshire Partnership NHS Foundation Trust policies all of which can be accessed via the staff intranet or the local Policy Guardian: a. Supportive Observation of Service Users at Risk b. Non Physical and Physical Assaults (Violence and Aggression) c. Lone Worker Policy d. Delivery of Care Policy (Incorporating the Care Programme Approach) e. Falls Prevention Policy f. Pressure Ulcer Prevention Policy g. Learning from Incidents h. Risk Management Policy i. Safeguarding Adults and Children j. Care Records Management k. Lone Working Policy l. Searching Service Users and their Property m. Advance Directives Policy n. Health and Safety Policies (HPT and ACS) o. Discharge and Transfer Policy p. Operational Policy, Adult Mental Health Community Services q. Operational Policy, Mental Health Teams for Older People r. Acute Ward Operational Policy s. Dysphagia and Nutrition Policy t. Physical Health Assessment and Physical Monitoring 21. Supporting References STANDARD The risk management process should take into account relevant legislation and existing guidance: The Mental Health Act 1983 and Codes of Practice The Mental Health Act 2007 The Mental Capacity Act 2005 The Human Rights Act 1998 The Data Protection Act 1998 The Health and Safety at Work Act 1976 The Race Relations Amendment Act 2000 The Disability Discrimination Act 2005 The Equality Act 2006 The Children s Act
31 The Care Act 2014 Preventing Suicide: A toolkit for Mental Health Services 2003 Safeguarding Adults from Abuse: a Hertfordshire Inter-agency protocol 31
32 Avoidable Deaths: Five Year report of the national Confidential Inquiry into suicide and homicide by People with mental Illness (2006) Best Practice in Managing Risk: Department of Health (2009) Refocussing the Care Programme Approach (2008) 22. Comments and Feedback STANDARD Comments and Feedback on this document were obtained from: Head of Social Work and Safeguarding Associate medical Director Associate Medical Director (Practice Governance) Deputy Director Safer Care and Standards 32
33 APPENDICES Appendices Appendix 1 Risk Assessment Form AMHS Appendix 2 - Risk Assessment Form CAMHS Appendix 3 Risk Assessment Form LD Appendix 4 - Procedures for Well-being/IAPT services Appendix 5 - Risk Management Panel Guidance Appendix 6 Learning from Serious Incidents 33
34 Appendix 1 AMH Risk Assessment Tool Amh/Camhs Risk Assessment USER(141885) PROFESSOR. TEST SERVICE Person Details Name PROFESSOR. TEST SERVICE USER DoB/Gender 25/04/1999, FEMALE Address 5TL HERTFORDSHIRE PARTNERSHIP NHS TRUST, 99 WAVERLEY ROAD, ST. ALBANS, HERTFORDSHIRE, AL3 Telephone ID NHS No Status Header Details Type AMH/CAMHS RISK ASSESSMENT Date Started 18/12/2014 End Date Time Started Reason for Assess. Location End Time Outcome Planned Comp Date. Team INFORMATICS2 Reason for Delay Carried Out By ROBERT XXHARRIS Link Info Ref Recorded By ROBERT XXHARRIS Assessment ID Referral ID Planned Next Review Date Goal at Time of Ass. Which HPFT Service Please Select if this is an AMH/CAMHS Assessment AMH 34
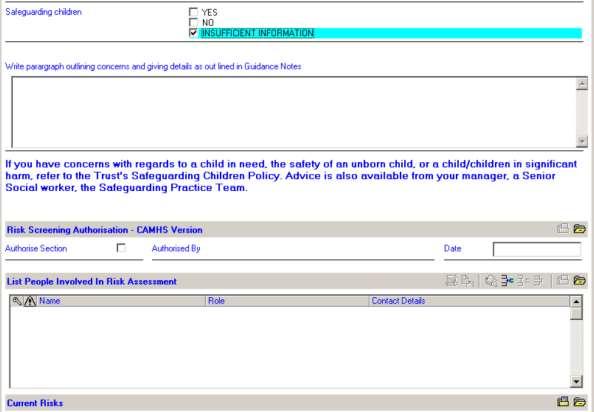
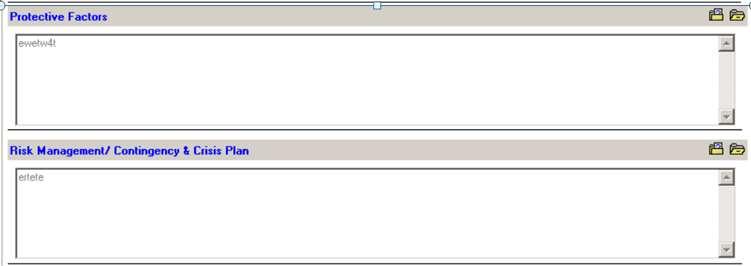
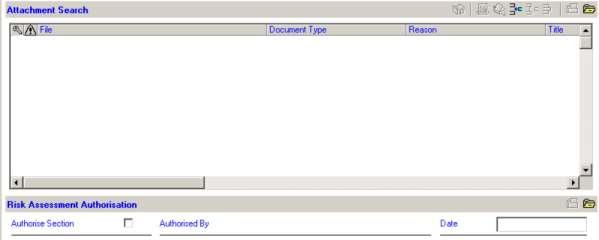
35 Risk Screening - AMH Version Risk of self harm or suicide Risk of self neglect Risk of harm to others Risk of abuse or neglect by others Does the patient have children under the age of 18, are they pregnant, do they have close contact with children? YES NO INSUFFICIENT INFORMATION YES NO INSUFFICIENT INFORMATION YES NO INSUFFICIENT INFORMATION YES NO INSUFFICIENT INFORMATION YES NO Risk Screening Authorisation - AMH Version Authorise Section Authorised By Date List People Involved In Risk Assessment Name Role Contact Details Amh/Camhs Risk Assessment PROFESSOR. TEST SERVICE USER(141885) Patients with suicidal ideas/thoughts please consider completing Beck Hopelessness Scale and attaching to this Risk Assessment. History Of Risks dsadsawrtgwrh Other Concerns asdasdewt4yw4 Protective Factors ewetw4t Risk Management/ Contingency & Crisis Plan ertete Please Select To Indicate The Following Has Been Discussed Information sharing / confidentiality discussed with Service User YES NO Consent to sharing risk assessment given by Service User YES NO Service User and/or Carer informed of this plan YES NO With whom will this risk assessment and management plan be shared? Carer GP Service User Other Agencies (Please specify) Attachment Search File Document Type Reason Title Recorded By Recorded On Recorded At 35
36 Risk Assessment Authorisation Authorise Section Authorised By Date 36

37 Appendix 2 CAMHS Risk Assessment Tool 37

38 38
39 39

40 Print Date: 06/10/2015 Page: 40
41 Appendix 3 LD Risk Assessment Tool Ld Risk Assessment PROFESSOR. TEST SERVICE USER(141885) Person Details Name PROFESSOR. TEST SERVICE USER DoB/Gender 25/04/1999, FEMALE Address HERTFORDSHIRE PARTNERSHIP NHS TRUST, 99 WAVERLEY ROAD, ST. ALBANS, HERTFORDSHIRE, AL3 5TL Telephone ID NHS No Status Header Details Type LD RISK ASSESSMENT Date Started 13/10/2014 End Date Time Started Reason for Assess. Location Outcome Planned Comp Date. Team INFORMATICS2 Reason for Delay Carried Out By Link Info Ref Recorded By ALIJA XXHAMULIC Assessment ID Referral ID Planned Next Review Date Goal at Time of Ass. List People Involved In Risk Assessment Name Role Contact Deatils History Of Risk No Change Current Risks No Change Early Warning Signs No Change Physical Health No Change Mental Health. No Change Print Date: 06/10/2015 Page: 41
42 Current Personal And Contextual Risk Factors No Change Ld Risk Assessment PROFESSOR. TEST SERVICE USER(141885) Factors Potentially Reducing Risk No Change Child Need Screening Date of Completion 07/04/2014 Carried Out By DR ADEELA ABBASI Is the service user pregnant or have dependant children or close contact with children? (e.g. adult who lives with another person who has children, adult who is given responsibility by the parent for caring for the children, adult who is engaged in close relationship with a parent and spends time in the home where children reside). Children's Details Name Dob Age Primary Carer Gp Current School YES Associated People Contact Name Relationship Association DoB / Age / Sex Ethnicity Client / Person Status Client / Person ID Parental Responsibility? PR Reason Association From To Address Primary Contact lbltel1 lbltel2 Contact Name Relationship Association DoB / Age / Sex Ethnicity Client / Person Status Client / Person ID Parental Responsibility? PR Reason Association From To Address Primary Contact lbltel1 lbltel2 Contact Name Relationship Association DoB / Age / Sex Ethnicity Print Date: 06/10/2015 Page: 42
43 Client / Person Status Client / Person ID Parental Responsibility? PR Reason Association From To Ld Risk Assessment PROFESSOR. TEST SERVICE USER(141885) Address Primary Contact lbltel1 lbltel2 Child Need Screening Assessment Mental Health Act Is the mental health of the service user likely to impact significantly on his/her ability to meet the needs of the child/children Assessment of mental health should take into account: - The present mental state of the service user and any relevant history - The service user s use of/attitude towards use of treatment and the impact of treatment: Some things you might consider are the ages of the children, support networks and capacities for parenting Alternative Parenting Arrangements If the parent/service user is unable to fulfil one or more of these, is there an identified parent/carer (such as co-parent or grandparent) who is able to and does fulfil these needs? Concern Child Needs Not Being Met Could the presenting behaviour of the adult impact on the Childs needs not being met? (If 'Yes' then action taken must be specified below) Additional Comments Including relationship, age of child/children, and frequency of contact, it the service user does not have parental responsibility for the child/children Action Required Refer to trust s Safeguarding Children Policy, it provides all contact details about who to discuss concerns with and how to make a referral, if necessary to Children s Services (If 'No' please explain) Other Relevant Assessments Including relationship, age of child/children, and frequency of contact, it the service user does not have parental responsibility for the child/children (Consider referral to Children's Services) If 'Yes' initiate a Young Carer s Assessment and consider a referral to Children s Services This document must be reviewed and re-assessed at Care Coordination meetings and at any change of circumstances. Risk Assessment : Sign Off Section Completed? Completed By Completed When On Behalf Of Print Date: 06/10/2015 Page: 43
44 Ld Risk Assessment PROFESSOR. TEST SERVICE USER(141885) Contingency And Crisis Plan Trigger Contingency/crisis Plan By When By Whom Su's Views Of The Risk Management Plan No Change Carers View Of Risk Mgmnt Plan No Change Please Select To Indicate The Following Has Been Discussed Service User and/or Carer informed of this plan YES NO Information sharing / confidentiality discussed with service user YES NO Consent to sharing risk assessment given by service user YES NO With whom will this risk assessment and management plan be shared? Carer CLDT Other HPFT Staff Other Agencies (Please specify) Risk Management : Sign Off Section Completed Completed By Completed When On Behalf Of Attachment Search File Document Type Reason Title Recorded By Recorded On Recorded At Print Date: 06/10/2015 Page: 44
45 Appendix 4 Procedures for Well-being/IAPT Services Assessing whether clients are a risk to themselves or others is an area which should be prioritised within the IAPT service. Although level of risk will have been assessed at Triage, the client s level of risk may change on a daily basis, and therefore workers should maintain a constant awareness of this issue. For this reason risk assessment is a mandatory field for every contact on PC-Mis. In assessing risk the following areas are good indicators of level of risk to self: Level of ideation and hopelessness Extent of planning Likelihood of action and previous attempts At each contact the IAPT minimum data set questionnaires should be completed. Attend particularly to PHQ 9 item 9: Thoughts that you would be better off dead or thoughts of hurting yourself in some way. If the response is 1 or above (several days or more), then the following questions from PC-Mis should be asked: Q1. Do you ever feel that bad that you think about harming or killing yourself? Q2. Do you ever feel that life is not worth living? Q3. Have you made plans to end your life? Q4. Do you know how you would kill yourself? Q5. Have you made any actual preparations to kill yourself? Q6. Have you ever attempted suicide in the past? Q7. How likely is it that you will act on such thoughts and plans? (0 10, 10 being certain) Q8. What is stopping you killing or harming yourself at the moment? In particular if the client answers yes to questions 1, 3, 4, or 5 then this together with the intent rating on question 7 may indicate a high level of risk. If you think that the client may present a level of risk to themselves or others or then speak to the duty worker or a qualified clinician as soon as possible. In terms of risk to others supplementary questions will need to be asked if there are indications that the client may pose a risk to others. eg anger problems. Also consider child protection issues. Again, areas to assess include level of ideation, extent of planning and previous history. The police may need to be informed if a serious crime is planned or disclosed. If that is the case, the duty worker should be consulted. If for any reason a qualified clinician is not available and you feel that there is a high level of risk then phone the crisis team. The client can also access the crisis team by attending the local hospital A & E department. The GP should also be informed in writing by fax as soon as possible. For further guidance please refer to the CORE guidance on risk assessment Print Date: 06/10/2015 Page: 45
46 Appendix 5 Risk Management Panel Guidance 1. Background. From time to time a team may be faced with a challenging case where they appear to have an on-going duty to provide care and treatment to a service user, but where it is extremely difficult to ensure that the service user and those around her/him including Trust staff can remain safe. With regard to inpatients, various options are available to ward staff to ensure patient safety. These include a range of medical and psychological treatments, use of the provisions of the Mental Health Act, use of increased observation levels with where necessary extra staff to undertake the role, and the interventions described in detail in the Non-physical and Physical Assault Policy (July 2012). Despite this, data shows that significant numbers of incidents of actual or threatened aggression from service users to staff or to other service users take place, especially on older people s inpatient units and inpatient units for people with learning disabilities. The Trust is committed to reducing these incidents so that staff can feel safe and confident in their practice. In community services, there can be high risk cases where a team is faced with clinical, legal and at times ethical dilemmas about how to continue to provide care when risk factors appear unmanageable. In such scenarios, the risks can be more entrenched and well known, but the options available to staff, and the ability to control the behaviour of the service user, are often more limited. The risk management panel aims to better support staff in inpatient and community settings in the sometimes very pressurized work that they do. 2. The Panel 2.1. Function. The panel s main function is to provide expert advice to the care co-ordinator and other Trust staff contributing to the care plan, on the future management of an individual service user. It will: Provide a broader perspective on a case in a situation where the local ward/team may be finding it difficult to maintain a clear objective view of the needs of the service user Make available professional advice which brings additional expertise to the case and also a multi-disciplinary perspective It will not: Provide an emergency service e.g. dealing with inappropriate placements of service users or dilemmas about acute admission.and bed availability Replace the standard responsibilities of the care co-ordinator and their team to assess and manage clinical risks in line with this policy 47
47 2.2. Panel Membership A pool of Trust staff will be available to act on the panel of 3. This will comprise: Head of practice governance Practice governance leads Consultant Psychiatrists Heads of Nursing Personality Disorder Therapists Incident Investigator Senior social worker Consultant clinical psychologist Allied health professional Lead for prevention and management of violence and aggression In exceptional circumstances the chair will co-opt others onto the panel. Legal advice may also be sought via the Patient Safety manager Criteria. The Multidisciplinary Team should consider referring a case to the panel when the following applies: The care team is facing a dilemma in terms of safe and clinically appropriate management of an individual All available options in terms of staffing levels, statutory powers, specialist services and treatments appear to have been exhausted There are likely to have been recent incidents of threatened or actual assault or other unacceptable behaviour under the RESPECT standards If a second opinion could be expected to facilitate a solution this should be arranged first (see Second Opinions and Transfer of Consultant Psychiatrist Policy July 2009). The panel will meet monthly with 3 slots Process. Referrals to the panel should always be made by the care co-ordinator or Named Nurse, and with the agreement of the responsible manager. Referrals should be made on the referral form (see below), to the Head of Practice Governance, who will organise the panel response. The panel will comprise a chair and at least two others from the membership list above. The care co-ordinator or Named Nurse will attend and will organise attendance of key colleagues as necessary. The meeting will examine the impact of the current care plan, and generate ideas for proactive interventions which will enable staff to gain greater control of the risks being presented by the service user. The chair will therefore ensure that the meeting is solution-focussed. 48
48 The service user and carers will not attend, but the care co-ordinator or Named Nurse will inform them the meeting is taking place and feedback the outcome. The panel chair will provide a written record of the meeting to the care co-ordinator or Named Nurse who will enter it into the patient record.. Name of service user Risk Management Panel Care co-ordinator Team Named nurse (if appropriate) Consultant Psychiatrist Is service user an inpatient at present? Yes/No If Yes, name of ward Current care plan Current risks Form completed by Name of manager (taken as their consent to the referral) Date of completion 49
49 Appendix 6 Shown below are the main recommendations that have arisen from Serious Incidents involving unexpected deaths in the past year. These give important pointers for all staff about how to manage such cases most effectively. Further information is available from the Patient Safety team or Practice Governance leads. Unexpected Deaths 1. Consideration of stepping up from Wellbeing to secondary MH services when clinically indicated 2. Engagement with, and support of, families/carers post incident 3. Access to all available information on different EPR systems to inform assessment of risk 4. Evidencing that carers assessments are being offered, undertaken and recorded 5. Recording of key decisions in the electronic record 6. All identified risks had not been documented on the latest risk assessment 7. A paper file was in use by some staff involved in the care pathway and not all information in that file had been added to the electronic record 8. Key risk information not shared between teams which led to a missed opportunity to review the risk management plan 9. No record of carer/next of kin in the electronic record 10. Recording of rationale for discharge in the electronic record 11. Decision to discharge did not involve all key individuals 12. Information not always shared with the GP 13. Missed opportunity for case review prior to discharge 14. Risk factors and safeguarding issues were not properly identified, acknowledged or addressed 15. Absence of a risk assessment used to formulate a suitable follow-up care plan in accordance with the DNA policy 16. Joint working with D&A services service user discharged from Spectrum and HPFT at the same time removing all support 17. Accessing all available corroborative information to inform the assessment and management plan 50

50 51
Clinical Risk Assessment and Management in Mental Health & Learning Disability Services Policy
 Clinical Risk Assessment and Management in Mental Health & Learning Disability Services Policy Document Author Written By: MH & LD Clinical Quality & Safety Leads Authorised Authorised By: Chief Executive
Clinical Risk Assessment and Management in Mental Health & Learning Disability Services Policy Document Author Written By: MH & LD Clinical Quality & Safety Leads Authorised Authorised By: Chief Executive
Page 1 of 18. Summary of Oxfordshire Safeguarding Adults Procedures
 Page 1 of 18 Summary of Oxfordshire Safeguarding Adults Procedures Page 2 of 18 Introduction This part of the procedures sets out clear expectations regarding the standards roles and responsibilities of
Page 1 of 18 Summary of Oxfordshire Safeguarding Adults Procedures Page 2 of 18 Introduction This part of the procedures sets out clear expectations regarding the standards roles and responsibilities of
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
Unless this copy has been taken directly from the Trust intranet site (Pandora) there is no assurance that this is the most up to date version
 there is no assurance that this is the most up to date version") Policy No: MH27 Version: 2.0 Name of Policy: Care Programme Approach & Care Co-ordination Effective From: 25/08/2015 Date Ratified 24/07/2015 Ratified Mental Health Committee Review Date 01/07/2017 Sponsor
Policy No: MH27 Version: 2.0 Name of Policy: Care Programme Approach & Care Co-ordination Effective From: 25/08/2015 Date Ratified 24/07/2015 Ratified Mental Health Committee Review Date 01/07/2017 Sponsor
Safeguarding Vulnerable Adults Policy
 POLICY & PROCEDURES PROTECTION OF VULNERABLE ADULTS This policy was written in conjunction with the Multi-Agency Safeguarding of Vulnerable Adults in Lincolnshire Policy STATEMENT The welfare of all vulnerable
POLICY & PROCEDURES PROTECTION OF VULNERABLE ADULTS This policy was written in conjunction with the Multi-Agency Safeguarding of Vulnerable Adults in Lincolnshire Policy STATEMENT The welfare of all vulnerable
Document Title Clinical Risk Assessment and Management Policy. Electronic Systems Development & Training Consultant Risk and Assurance Facilitator
 Document Title Clinical Risk Assessment and Management Policy Document Description Document Type Policy Service Application Trust Wide Version 1.2 Policy Reference no. POL 025 Lead Author(s) Name Bob Yardley
Document Title Clinical Risk Assessment and Management Policy Document Description Document Type Policy Service Application Trust Wide Version 1.2 Policy Reference no. POL 025 Lead Author(s) Name Bob Yardley
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Grampian. Intensive Psychiatric Care Units
 NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
Refocusing CPA: a summary of the key changes. Bernadette Harrison CPA Manager Bedfordshire & Luton Mental Health & Social Care Partnership NHS Trust
 Refocusing CPA: a summary of the key changes Bernadette Harrison CPA Manager Bedfordshire & Luton Mental Health & Social Care Partnership NHS Trust Introduction In March 2008, the Department of Health
Refocusing CPA: a summary of the key changes Bernadette Harrison CPA Manager Bedfordshire & Luton Mental Health & Social Care Partnership NHS Trust Introduction In March 2008, the Department of Health
NHS Borders. Intensive Psychiatric Care Units
 NHS Borders Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Borders Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
Care Programme Approach Policies and Procedures. Choice, Responsiveness, Integration & Shared Care
 Care Programme Approach Policies and Procedures Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose:
Care Programme Approach Policies and Procedures Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose:
Policy for the use of Leave under Section 17 of the Mental Health Act 1983 (as amended) Version: 9
 Version: 9") SH CP 52 Policy for the use of Leave under Section 17 of the Mental Health Act 1983 (as amended) Version: 9 Summary: Keywords (minimum of 5): (To assist policy search engine) Target Audience: Policy for
SH CP 52 Policy for the use of Leave under Section 17 of the Mental Health Act 1983 (as amended) Version: 9 Summary: Keywords (minimum of 5): (To assist policy search engine) Target Audience: Policy for
Managing deliberate self-harm in young people
 Managing deliberate self-harm in young people Council Report CR64 March 1998 Royal College of Psychiatrists, London Due for review: March 2003 1 2 Contents Background 4 Commissioning services 5 Providing
Managing deliberate self-harm in young people Council Report CR64 March 1998 Royal College of Psychiatrists, London Due for review: March 2003 1 2 Contents Background 4 Commissioning services 5 Providing
THE ROLE OF COMMUNITY MENTAL HEALTH TEAMS IN DELIVERING COMMUNITY MENTAL HEALTH SERVICES
 THE ROLE OF COMMUNITY MENTAL HEALTH TEAMS IN DELIVERING COMMUNITY MENTAL HEALTH SERVICES Interim Policy Implementation Guidance and Standards [July 2010] - 1 - CONTENTS 1. Introduction... 3 2. The guiding
THE ROLE OF COMMUNITY MENTAL HEALTH TEAMS IN DELIVERING COMMUNITY MENTAL HEALTH SERVICES Interim Policy Implementation Guidance and Standards [July 2010] - 1 - CONTENTS 1. Introduction... 3 2. The guiding
SAFEGUARDING CHILDEN POLICY. Policy Reference: Version: 1 Status: Approved
 SAFEGUARDING CHILDEN POLICY Policy Reference: Version: 1 Status: Approved Type: Clinical Policy Policy applies to : All services within SCH Serco Policy applies to (staff groups): All SCH Serco staff Policy
SAFEGUARDING CHILDEN POLICY Policy Reference: Version: 1 Status: Approved Type: Clinical Policy Policy applies to : All services within SCH Serco Policy applies to (staff groups): All SCH Serco staff Policy
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care in England. Core Values and Principles
 National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care in England Core Values and Principles Contents Page No Paragraph No Introduction 2 1 National Policy on Assessment 2 4 The Assessment
National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care in England Core Values and Principles Contents Page No Paragraph No Introduction 2 1 National Policy on Assessment 2 4 The Assessment
Summary guide: Safeguarding Adults: Pan Lancashire and Cumbria Multi Agency Policy and Procedures. For partner agencies staff and volunteers
 Summary guide: Safeguarding Adults: Pan Lancashire and Cumbria Multi Agency Policy and Procedures For partner agencies staff and volunteers 1 1. Introduction This Summary Guide is designed to provide straightforward
Summary guide: Safeguarding Adults: Pan Lancashire and Cumbria Multi Agency Policy and Procedures For partner agencies staff and volunteers 1 1. Introduction This Summary Guide is designed to provide straightforward
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
Luton Psychiatric Liaison Service (PLS) Job Description & Person Specification
 Job Description & Person Specification") Luton Psychiatric Liaison Service (PLS) Job Description & Person Specification Job Title: Psychiatric Liaison Nurse Practitioner Grade: Band 6 Hours: Responsible To: Accountable To: Location 37.5 Hours
Luton Psychiatric Liaison Service (PLS) Job Description & Person Specification Job Title: Psychiatric Liaison Nurse Practitioner Grade: Band 6 Hours: Responsible To: Accountable To: Location 37.5 Hours
Lone worker policy. Director of Nursing Therapies Patient Partnership Author and contact number Safety and Security Lead
 Document level: Trustwide (TW) Code: GR33 Issue number: 3 Lone worker policy Lead executive Director of Nursing Therapies Patient Partnership Author and contact number Safety and Security Lead 01244 397618
Document level: Trustwide (TW) Code: GR33 Issue number: 3 Lone worker policy Lead executive Director of Nursing Therapies Patient Partnership Author and contact number Safety and Security Lead 01244 397618
1. Guidance notes. Social care (Adults, England) Knowledge set for end of life care. (revised edition, 2010) What are knowledge sets?
 Knowledge set for end of life care. (revised edition, 2010) What are knowledge sets?") Social care (Adults, England) Knowledge set for end of life care (revised edition, 2010) Part of the sector skills council Skills for Care and Development 1. Guidance notes What are knowledge sets? Knowledge
Social care (Adults, England) Knowledge set for end of life care (revised edition, 2010) Part of the sector skills council Skills for Care and Development 1. Guidance notes What are knowledge sets? Knowledge
Safeguarding Adults Policy March 2015
 Safeguarding Adults Policy 2015-16 March 2015 Document Control: Description Comment Title Document Number 1 Author Lindsay Ratapana Date Created March 2015 Date Last Amended Version 1 Approved By Quality
Safeguarding Adults Policy 2015-16 March 2015 Document Control: Description Comment Title Document Number 1 Author Lindsay Ratapana Date Created March 2015 Date Last Amended Version 1 Approved By Quality
SAFEGUARDING CHILDREN POLICY
 SAFEGUARDING CHILDREN POLICY The child s needs are paramount, and the needs and wishes of each child, be they a baby or infant, or an older child, should be put first Working Together 2015 p 8 Keeping
SAFEGUARDING CHILDREN POLICY The child s needs are paramount, and the needs and wishes of each child, be they a baby or infant, or an older child, should be put first Working Together 2015 p 8 Keeping
JOB DESCRIPTION. As specified in the job advertisement and the Contract of. Lead Practice Teacher & Clinical Team Leader
 JOB DESCRIPTION JOB TITLE: Student Health Visitor BAND: Agenda for Change Band 5 HOURS AND: DURATION As specified in the job advertisement and the Contract of Employment AGENDA FOR CHANGE (reference No)
JOB DESCRIPTION JOB TITLE: Student Health Visitor BAND: Agenda for Change Band 5 HOURS AND: DURATION As specified in the job advertisement and the Contract of Employment AGENDA FOR CHANGE (reference No)
Care Programme Approach (CPA) Policy
 Policy") Care Programme Approach (CPA) Policy DOCUMENT CONTROL: Version: 10 Ratified by: Quality and Safety Sub Committee Date ratified: 3 May 2017 Name of originator/author: Nurse Consultant, AMHS Name of responsible
Care Programme Approach (CPA) Policy DOCUMENT CONTROL: Version: 10 Ratified by: Quality and Safety Sub Committee Date ratified: 3 May 2017 Name of originator/author: Nurse Consultant, AMHS Name of responsible
Specialist mental health services
 How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
Informal Patients to take Leave from Adult Mental Health Inpatient Wards. Standard Operating Procedure
 Informal Patients to take Leave from Adult Mental Health Inpatient Wards Standard Operating Procedure DOCUMENT CONTROL: Version: 1 Ratified by: Quality Committee Date ratified: 16 June 2016 Name of originator/author:
Informal Patients to take Leave from Adult Mental Health Inpatient Wards Standard Operating Procedure DOCUMENT CONTROL: Version: 1 Ratified by: Quality Committee Date ratified: 16 June 2016 Name of originator/author:
Kent and Medway Ambulance Mental Health Referral Pathway Protocol
 Kent and Medway Ambulance Mental Health Referral Pathway Protocol Introduction This protocol has been developed jointly by Kent and Medway NHS and Social Care Partnership Trust (KMPT) and South East Coast
Kent and Medway Ambulance Mental Health Referral Pathway Protocol Introduction This protocol has been developed jointly by Kent and Medway NHS and Social Care Partnership Trust (KMPT) and South East Coast
Policies, Procedures, Guidelines and Protocols
 Title Policies, Procedures, Guidelines and Protocols Document Details Trust Ref No 2078-28878 Local Ref (optional) Main points the document covers Who is the document aimed at? Author Approved by (Committee/Director)
Title Policies, Procedures, Guidelines and Protocols Document Details Trust Ref No 2078-28878 Local Ref (optional) Main points the document covers Who is the document aimed at? Author Approved by (Committee/Director)
Reducing Risk: Mental health team discussion framework May Contents
 Reducing Risk: Mental health team discussion framework May 2015 Contents Introduction... 3 How to use the framework... 4 Improvement area 1: Unscheduled absence and managing time off the ward... 5 Improvement
Reducing Risk: Mental health team discussion framework May 2015 Contents Introduction... 3 How to use the framework... 4 Improvement area 1: Unscheduled absence and managing time off the ward... 5 Improvement
DELIVERING THE CARE PROGRAMME APPROACH IN WALES
 DELIVERING THE CARE PROGRAMME APPROACH IN WALES Interim Policy Implementation Guidance [July 2010] - 2 - CONTENTS PART 1 Introduction and background... 5 1. Introduction... 5 2. Mental Health (Wales) Measure,
DELIVERING THE CARE PROGRAMME APPROACH IN WALES Interim Policy Implementation Guidance [July 2010] - 2 - CONTENTS PART 1 Introduction and background... 5 1. Introduction... 5 2. Mental Health (Wales) Measure,
PROTOCOL FOR LOCATING A CAMHS TIER 4 BED AT CRISIS PRESENTATION
 PROTOCOL FOR LOCATING A CAMHS TIER 4 BED AT CRISIS PRESENTATION Title: Protocol for locating a CAMHS Tier 4 Bed at crisis presentation Reference Number: Version No: V1 Issue Date: December 2017 Review
PROTOCOL FOR LOCATING A CAMHS TIER 4 BED AT CRISIS PRESENTATION Title: Protocol for locating a CAMHS Tier 4 Bed at crisis presentation Reference Number: Version No: V1 Issue Date: December 2017 Review
SAFEGUARDING ADULTS POLICY
 SAFEGUARDING ADULTS POLICY This document may be made available in alternative formats and other languages, on request, as is reasonably practicable to do so. Policy Owner: Approved by: POVA Operational
SAFEGUARDING ADULTS POLICY This document may be made available in alternative formats and other languages, on request, as is reasonably practicable to do so. Policy Owner: Approved by: POVA Operational
Framework for Managing Care Care Coordinators Handbook
 Ymddiriedolaeth GIG Gogledd Cymru North Wales NHS Trust (Central Area) Division of Mental Health, Learning Disability and Psychology Including Ymddiriedolaeth GIG Siroedd Conwy a Dinbych Adult Mental Health
Ymddiriedolaeth GIG Gogledd Cymru North Wales NHS Trust (Central Area) Division of Mental Health, Learning Disability and Psychology Including Ymddiriedolaeth GIG Siroedd Conwy a Dinbych Adult Mental Health
Learning from Deaths - Mortality Report
 Learning from Deaths - Mortality Report NHS Improvement and the National Quality Board have requested all NHS Trusts to publish a review of mortality by. This is our Trust report. 1. Background In line
Learning from Deaths - Mortality Report NHS Improvement and the National Quality Board have requested all NHS Trusts to publish a review of mortality by. This is our Trust report. 1. Background In line
Intensive Psychiatric Care Units
 NHS Greater Glasgow and Clyde Stobhill Hospital, Glasgow Intensive Psychiatric Care Units Service Profile Exercise ~ November 009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and
NHS Greater Glasgow and Clyde Stobhill Hospital, Glasgow Intensive Psychiatric Care Units Service Profile Exercise ~ November 009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and
Care and Treatment Review: Policy and Guidance
 Care and Treatment Review: Policy and Guidance With policy and guidance on Care, Education and Treatment Reviews for children and young people Easy Read Version 2017 1 Contents Foreword from Gavin Harding...
Care and Treatment Review: Policy and Guidance With policy and guidance on Care, Education and Treatment Reviews for children and young people Easy Read Version 2017 1 Contents Foreword from Gavin Harding...
Performance and Quality Committee
 Title: NHS Continuing Health Care Choice Policy (addendum to Cornwall Wide Patient Choice, Equity and Fair Access Policy) Developed by: Document type: Policy library: NHS Kernow Policy Policies Sub Section:
Title: NHS Continuing Health Care Choice Policy (addendum to Cornwall Wide Patient Choice, Equity and Fair Access Policy) Developed by: Document type: Policy library: NHS Kernow Policy Policies Sub Section:
Intensive Psychiatric Care Units
 NHS Tayside Carseview Centre, Dundee Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have
NHS Tayside Carseview Centre, Dundee Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have
Safeguarding Vulnerable Adults Policy and Procedures
 155-159 Freeman Street, Grimsby, North East Lincolnshire, DN32 7AR Tel: 01472 240440 Safeguarding Vulnerable Adults Policy and Procedures The CPO Media policy adheres to the multi-agency policy, procedures
155-159 Freeman Street, Grimsby, North East Lincolnshire, DN32 7AR Tel: 01472 240440 Safeguarding Vulnerable Adults Policy and Procedures The CPO Media policy adheres to the multi-agency policy, procedures
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7.Optional to use, detail for local determination
SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7.Optional to use, detail for local determination
ISLE OF WIGHT SAFEGUARDING CHILDREN BOARD WORKFORCE DEVELOPMENT POLICY
 ISLE OF WIGHT SAFEGUARDING CHILDREN BOARD WORKFORCE DEVELOPMENT POLICY Version 1 Ratified March 2014 Reviewed and updated January 2016 For review January 2017 Contents 1. Introduction... 3 2. Purpose...
ISLE OF WIGHT SAFEGUARDING CHILDREN BOARD WORKFORCE DEVELOPMENT POLICY Version 1 Ratified March 2014 Reviewed and updated January 2016 For review January 2017 Contents 1. Introduction... 3 2. Purpose...
Staffordshire and Stoke on Trent Adult Safeguarding Partnership Board Safeguarding Adult Reviews (SAR) Protocol
 Protocol") Staffordshire and Stoke on Trent Adult Safeguarding Partnership Board Safeguarding Adult Reviews (SAR) Protocol SAR Process July 2014 (revised August 2017) Page 1 Contents 1. Introduction 2. Criteria 3.
Staffordshire and Stoke on Trent Adult Safeguarding Partnership Board Safeguarding Adult Reviews (SAR) Protocol SAR Process July 2014 (revised August 2017) Page 1 Contents 1. Introduction 2. Criteria 3.
Mental health and crisis care. Background
 briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
Practice Guidance: Large Scale Investigations
 Practice Guidance: Large Scale Investigations Version: Version 1: April 2014 Ratified by: Leeds Safeguarding Adults Board Date ratified: April 2014 Author/Originator of title Safeguarding Policy, Protocols
Practice Guidance: Large Scale Investigations Version: Version 1: April 2014 Ratified by: Leeds Safeguarding Adults Board Date ratified: April 2014 Author/Originator of title Safeguarding Policy, Protocols
CARERS POLICY. All Associate Director of Patient Experience. Patient & Carers Experience Committee & Trust Management Committee
 CARERS POLICY Department / Service: Originator: All Associate Director of Patient Experience Accountable Director: Chief Nursing Officer Approved by: Patient & Carers Experience Committee & Trust Management
CARERS POLICY Department / Service: Originator: All Associate Director of Patient Experience Accountable Director: Chief Nursing Officer Approved by: Patient & Carers Experience Committee & Trust Management
Core Domain You will be able to: You will know and understand: Leadership, Management and Team Working
 DEGREE APPRENTICESHIP - REGISTERED NURSE 1 ST0293/01 Occupational Profile: A career in nursing is dynamic and exciting with opportunities to work in a range of different roles as a Registered Nurse. Your
DEGREE APPRENTICESHIP - REGISTERED NURSE 1 ST0293/01 Occupational Profile: A career in nursing is dynamic and exciting with opportunities to work in a range of different roles as a Registered Nurse. Your
Forensic Mental Health Service. Referrals to and Discharges from the Leicestershire Partnerships NHS Trust
 Referrals to and Discharges from the Leicestershire Partnerships NHS Trust Contents 1. Introduction... 3 2. Aims and Objectives of the Policy... 3 3. Referral Criteria... 3 4. Referral Procedure... 3 5.
Referrals to and Discharges from the Leicestershire Partnerships NHS Trust Contents 1. Introduction... 3 2. Aims and Objectives of the Policy... 3 3. Referral Criteria... 3 4. Referral Procedure... 3 5.
Non Attendance (Did Not Attend-DNA ) Policy. Executive Director of Nursing and Chief Operating Officer
 Policy. Executive Director of Nursing and Chief Operating Officer") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Non Attendance (Did Not Attend-DNA) NTW(C)06 Executive Director of Nursing and Chief Operating Officer Ann Marshall
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Non Attendance (Did Not Attend-DNA) NTW(C)06 Executive Director of Nursing and Chief Operating Officer Ann Marshall
Policy Document Control Page
 Policy Document Control Page Title: Section 17 (Leave of Absence) Policy Version: 9 Reference Number: CL7 Supersedes Supersedes: Section 17 (Leave of Absence) Policy V8 Description of Amendment(s): Updated
Policy Document Control Page Title: Section 17 (Leave of Absence) Policy Version: 9 Reference Number: CL7 Supersedes Supersedes: Section 17 (Leave of Absence) Policy V8 Description of Amendment(s): Updated
EXECUTIVE SUMMARY OF THE INDEPENDENT INVESTIGATION INTO THE MENTAL HEALTH CARE AND TREATMENT OF PATIENT E COMMISSIONED BY THE FORMER NORTH EAST
 EXECUTIVE SUMMARY OF THE INDEPENDENT INVESTIGATION INTO THE MENTAL HEALTH CARE AND TREATMENT OF PATIENT E COMMISSIONED BY THE FORMER NORTH EAST STRATEGIC HEALTH AUTHORITY 1 Contents Page The Panel 3 1
EXECUTIVE SUMMARY OF THE INDEPENDENT INVESTIGATION INTO THE MENTAL HEALTH CARE AND TREATMENT OF PATIENT E COMMISSIONED BY THE FORMER NORTH EAST STRATEGIC HEALTH AUTHORITY 1 Contents Page The Panel 3 1
Care Coordination and Care Programme Approach Practice Guidance Note Learning Disability Admissions Urgent Care Only V02
 Care Coordination and Care Programme Approach Practice Guidance Note Learning Disability Admissions Urgent Care Only V02 Date issued Issue 2 Dec 15 Issue 3 Dec 17 Author/Designation Responsible Officer
Care Coordination and Care Programme Approach Practice Guidance Note Learning Disability Admissions Urgent Care Only V02 Date issued Issue 2 Dec 15 Issue 3 Dec 17 Author/Designation Responsible Officer
Short Break (Respite ) Care Practice and Procedure Guidance
 Care Practice and Procedure Guidance") Short Break (Respite ) Care Practice and Procedure Guidance 1 Contents 1. Introduction 2. Definition 2.1 Definition of a Carer 3. Legislation 3.1 Fair Access to care Services and the Duty to Provide 4.
Short Break (Respite ) Care Practice and Procedure Guidance 1 Contents 1. Introduction 2. Definition 2.1 Definition of a Carer 3. Legislation 3.1 Fair Access to care Services and the Duty to Provide 4.
HEALTHCARE INSPECTORATE WALES SAFEGUARDING AND PROTECTING CHILDREN IN WALES:
 HEALTHCARE INSPECTORATE WALES SAFEGUARDING AND PROTECTING CHILDREN IN WALES: A Review of the arrangements in place across the Welsh National Health Service ACTION PLAN - UPDATED August 2010 RECOMMENDATION
HEALTHCARE INSPECTORATE WALES SAFEGUARDING AND PROTECTING CHILDREN IN WALES: A Review of the arrangements in place across the Welsh National Health Service ACTION PLAN - UPDATED August 2010 RECOMMENDATION
Safeguarding & Wellbeing Policy
 Safeguarding & Wellbeing Policy 4.0 June 17 June 19 (unless an earlier review is required by legislative changes) All Midland Staff, Contractors and Volunteers Rebekah Newton, Director of Retirement Living
Safeguarding & Wellbeing Policy 4.0 June 17 June 19 (unless an earlier review is required by legislative changes) All Midland Staff, Contractors and Volunteers Rebekah Newton, Director of Retirement Living
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Hospital Discharge and Transfer Guidance. Choice, Responsiveness, Integration & Shared Care
 Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
This policy should be read in conjunction with all related policies and procedures. See the separate list in the Policies and Procedures file.
 Safeguarding Adults Policy and Procedure Related policies and procedures This policy should be read in conjunction with all related policies and procedures. See the separate list in the Policies and Procedures
Safeguarding Adults Policy and Procedure Related policies and procedures This policy should be read in conjunction with all related policies and procedures. See the separate list in the Policies and Procedures
Note: 44 NSMHS criteria unmatched
 Commonwealth National Standards for Mental Health Services linkage with the: National Safety and Quality Health Service Standards + EQuIP- content of the EQuIPNational* Standards 1 to 15 * Using the information
Commonwealth National Standards for Mental Health Services linkage with the: National Safety and Quality Health Service Standards + EQuIP- content of the EQuIPNational* Standards 1 to 15 * Using the information
Adult Psychiatric Liaison Service Operational Policy. Version No. 2
 Livewell Southwest Adult Psychiatric Liaison Service Operational Policy. Version No. 2 Notice to staff using a paper copy of this guidance The policies and procedures page of LSW intranet holds the most
Livewell Southwest Adult Psychiatric Liaison Service Operational Policy. Version No. 2 Notice to staff using a paper copy of this guidance The policies and procedures page of LSW intranet holds the most
SAFEGUARDING CHILDREN POLICY 2016
 POL 022 SAFEGUARDING CHILDREN POLICY 2016 Version 3.0 Ratified By Date Ratified NHS Wirral Clinical Commissioning Group :Quality, Performance & Finance Committee Author(s) Responsible Committee / Officers
POL 022 SAFEGUARDING CHILDREN POLICY 2016 Version 3.0 Ratified By Date Ratified NHS Wirral Clinical Commissioning Group :Quality, Performance & Finance Committee Author(s) Responsible Committee / Officers
BSc (Hons) Adult Nursing. Practice Assessment Document: Year 1
 Adult Nursing. Practice Assessment Document: Year 1") UNIVERSITY CAMPUS SUFFOLK School of Nursing and Midwifery Division of Nursing BSc (Hons) Adult Nursing Practice Assessment Document: Year 1 Student Name: Programme: Cohort: School of Nursing and Midwifery
UNIVERSITY CAMPUS SUFFOLK School of Nursing and Midwifery Division of Nursing BSc (Hons) Adult Nursing Practice Assessment Document: Year 1 Student Name: Programme: Cohort: School of Nursing and Midwifery
(NAME OF HOME) 2.1 This policy is based on the Six Principles of Safeguarding that underpin all our safeguarding work within our service.
 2.1 This policy is based on the Six Principles of Safeguarding that underpin all our safeguarding work within our service.") Title: SAFEGUARDING POLICY 1.0 INTRODUCTION 1.1 Safeguarding means protecting people's health, wellbeing and human rights, and enabling them to live free from harm, abuse and neglect. It's fundamental
Title: SAFEGUARDING POLICY 1.0 INTRODUCTION 1.1 Safeguarding means protecting people's health, wellbeing and human rights, and enabling them to live free from harm, abuse and neglect. It's fundamental
Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process
 Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process 10.1 Definition Risk is the likelihood that a person may be harmed or suffers adverse effects if exposed
Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process 10.1 Definition Risk is the likelihood that a person may be harmed or suffers adverse effects if exposed
Integrated Care Pathways for Child and Adolescent Mental Health Services. Final Standards June Evidence
 Integrated Care Pathways for Child and Adolescent Mental Health Services Final Standards June 2011 Evidence Healthcare Improvement Scotland is committed to equality and diversity. We have assessed these
Integrated Care Pathways for Child and Adolescent Mental Health Services Final Standards June 2011 Evidence Healthcare Improvement Scotland is committed to equality and diversity. We have assessed these
Action required: To agree the process by which Governors will meet with the inspection team.
 Airedale NHS Foundation Trust Council of Governors: 28 th January 2016 Title: CQC Inspection Briefing Author: Jane Downes, Company Secretary As you will be aware, the Care Quality Commission ( CQC ) have
Airedale NHS Foundation Trust Council of Governors: 28 th January 2016 Title: CQC Inspection Briefing Author: Jane Downes, Company Secretary As you will be aware, the Care Quality Commission ( CQC ) have
SAFEGUARDING ADULTS POLICY
 SAFEGUARDING ADULTS POLICY (Working with adults who have care and support needs to keep them safe from abuse or neglect) Version Ratified By Date Ratified Author(s) FINAL APPROVED NHS Wirral CCG Commissioning
SAFEGUARDING ADULTS POLICY (Working with adults who have care and support needs to keep them safe from abuse or neglect) Version Ratified By Date Ratified Author(s) FINAL APPROVED NHS Wirral CCG Commissioning
Worcestershire Early Intervention Service. Operational Policy
 Worcestershire Early Intervention Service Operational Policy Document Type Service Operational Unique Identifier CL-158 Document Purpose To Outline The Operation Of The Early Intervention Service Document
Worcestershire Early Intervention Service Operational Policy Document Type Service Operational Unique Identifier CL-158 Document Purpose To Outline The Operation Of The Early Intervention Service Document
How CQC monitors, inspects and regulates NHS GP practices
 How CQC monitors, inspects and regulates NHS GP practices March 2018 Updates to this guidance since October 2017: NEW annual provider information collection (for practices rated as good and outstanding)
How CQC monitors, inspects and regulates NHS GP practices March 2018 Updates to this guidance since October 2017: NEW annual provider information collection (for practices rated as good and outstanding)
Thresholds for initiating Adult Safeguarding Referrals or Care Concerns
 September 2012 Thresholds for initiating Adult Safeguarding Referrals or Care Concerns Establishing whether or not abuse of a vulnerable adult has taken place is not always straightforward. In some cases,
September 2012 Thresholds for initiating Adult Safeguarding Referrals or Care Concerns Establishing whether or not abuse of a vulnerable adult has taken place is not always straightforward. In some cases,
The Cornwall Framework for the Assessment of Children, Young People and their Families
 The Cornwall Framework for the Assessment of Children, Young People and their Families Background 1. Under Section 17 of the Children Act 1989, local authorities are required to provide services for children
The Cornwall Framework for the Assessment of Children, Young People and their Families Background 1. Under Section 17 of the Children Act 1989, local authorities are required to provide services for children
BARNSLEY CHILD AND ADOLESCENT MENTAL HEALTH SERVICE (CAMHS) CHILDREN IN CARE (CiC) PATHWAY
 CHILDREN IN CARE (CiC) PATHWAY") BARNSLEY CHILD AND ADOLESCENT MENTAL HEALTH SERVICE (CAMHS) CHILDREN IN CARE (CiC) PATHWAY Date issued: June 2017 Author: Children in Care Pathway Lead & General Manager In consultation with Children in
BARNSLEY CHILD AND ADOLESCENT MENTAL HEALTH SERVICE (CAMHS) CHILDREN IN CARE (CiC) PATHWAY Date issued: June 2017 Author: Children in Care Pathway Lead & General Manager In consultation with Children in
Care Programme Approach (CPA): Standard Operating Procedure
: Standard Operating Procedure") Clinical Care Programme Approach (CPA): Standard Operating Procedure Document Control Summary Status: New Version: v1.2 Date: 22/09/15 Author/Owner/Title: Kenny Laing Deputy Director of Nursing Approved
Clinical Care Programme Approach (CPA): Standard Operating Procedure Document Control Summary Status: New Version: v1.2 Date: 22/09/15 Author/Owner/Title: Kenny Laing Deputy Director of Nursing Approved
Bedfordshire and Luton Mental Health Street Triage. Operational Policy
 Bedfordshire and Luton Mental Health Street Triage Operational Policy 1 1. Introduction Mental Health Street Triage (MHST) is a collaborative service between mental health professionals (MHPs) paramedics
Bedfordshire and Luton Mental Health Street Triage Operational Policy 1 1. Introduction Mental Health Street Triage (MHST) is a collaborative service between mental health professionals (MHPs) paramedics
Safeguarding Adults Policy. General Policy GP12
 Safeguarding Adults Policy General Policy GP12 Applies to: All staff in contact with patients Committee for Approval Quality and Governance Committee Date Ratified: July 2012 Review Date: October 2013
Safeguarding Adults Policy General Policy GP12 Applies to: All staff in contact with patients Committee for Approval Quality and Governance Committee Date Ratified: July 2012 Review Date: October 2013
The Cornwall Framework for the Assessment of Children, Young People and their Families
 The Cornwall Framework for the Assessment of Children, Young People and their Families Background 1. Under the Children Act 1989, local authorities are required to provide services for children in need
The Cornwall Framework for the Assessment of Children, Young People and their Families Background 1. Under the Children Act 1989, local authorities are required to provide services for children in need
Warwickshire. Domestic Abuse Multi-Agency Risk Assessment Conference (MARAC) Operating Protocol
 Operating Protocol") Warwickshire Domestic Abuse Multi-Agency Risk Assessment Conference (MARAC) Operating Protocol Contents 1 Introduction... 4 1.1 Multi-Agency Risk Assessment Conferences... 4 1.2 Multi Agency Risk Assessment
Warwickshire Domestic Abuse Multi-Agency Risk Assessment Conference (MARAC) Operating Protocol Contents 1 Introduction... 4 1.1 Multi-Agency Risk Assessment Conferences... 4 1.2 Multi Agency Risk Assessment
The following staff are involved in your friend or relatives care. Their names and contact details are below.
 The Orchard Clinic The Royal Edinburgh Hospital: An information guide for relatives and carers Useful contacts for you The following staff are involved in your friend or relatives care. Their names and
The Orchard Clinic The Royal Edinburgh Hospital: An information guide for relatives and carers Useful contacts for you The following staff are involved in your friend or relatives care. Their names and
Section 117 Policy The Mental Health Act 1983
 Section 117 Policy The Mental Health Act 1983 [as amended by the Mental Health Act 2007] DOCUMENT CONTROL: Version: 1 Ratified by: Mental Health Legislation Committee Date ratified: 2 November 2016 Name
Section 117 Policy The Mental Health Act 1983 [as amended by the Mental Health Act 2007] DOCUMENT CONTROL: Version: 1 Ratified by: Mental Health Legislation Committee Date ratified: 2 November 2016 Name
Choice on Discharge Policy
 Choice on Discharge Policy Reference No: P_CIG_19 Version 1 Ratified by: LCHS Trust Board Date ratified: 13 th September 2016 Name of originator / author: Sarah McKown Name of responsible committee / Individual
Choice on Discharge Policy Reference No: P_CIG_19 Version 1 Ratified by: LCHS Trust Board Date ratified: 13 th September 2016 Name of originator / author: Sarah McKown Name of responsible committee / Individual
ASSOCIATED TRUST POLICIES Treatment Risk Assessment and Management of Treatment Risk Training Policy 15.09
 SECTION: 1 PATIENT CARE POLICY & PROCEDURE: 1.05 NATURE AND SCOPE: SUBJECT: POLICY TRUSTWIDE CARE PROGRAMME APPROACH (CPA) POLICY IN PARTNERSHIP WITH NOTTINGHAM ADULT SERVICES HOUSING AND HEALTH AND NOTTINGHAMSHIRE
SECTION: 1 PATIENT CARE POLICY & PROCEDURE: 1.05 NATURE AND SCOPE: SUBJECT: POLICY TRUSTWIDE CARE PROGRAMME APPROACH (CPA) POLICY IN PARTNERSHIP WITH NOTTINGHAM ADULT SERVICES HOUSING AND HEALTH AND NOTTINGHAMSHIRE
Independent Investigation Action Plan for Mr L STEIS Ref No: 2014/7319. Report published: NHE to complete
 Independent Investigation Action Plan for Mr L STEIS Ref No: 2014/7319 Statement from Oxleas NHS Foundation Trust The Trust would like to offer sincere condolenses to the family and friends of Mr Parsons.
Independent Investigation Action Plan for Mr L STEIS Ref No: 2014/7319 Statement from Oxleas NHS Foundation Trust The Trust would like to offer sincere condolenses to the family and friends of Mr Parsons.
SCDHSC0042 Lead practice for health and safety in the work setting
 Lead practice for health and safety in the work setting Overview This standard identifies the requirements when leading practice for health and safety in settings where children, young people or adults
Lead practice for health and safety in the work setting Overview This standard identifies the requirements when leading practice for health and safety in settings where children, young people or adults
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
North East Hampshire and Farnham Clinical Commissioning Group Safeguarding Framework
 North East Hampshire and Farnham Clinical Commissioning Group Safeguarding Framework North East Hampshire and Farnham Clinical Commissioning Group Safeguarding Strategic Framework Page 3 of 27 Contents
North East Hampshire and Farnham Clinical Commissioning Group Safeguarding Framework North East Hampshire and Farnham Clinical Commissioning Group Safeguarding Strategic Framework Page 3 of 27 Contents
DOCUMENT CONTROL Title: Use of Mobile Phones and Tablets (by services users & visitors in clinical areas) Policy. Version: Reference Number: CL062
 Policy. Version: Reference Number: CL062") DOCUMENT CONTROL Title: Version: Reference Number: Use of Mobile Phones and Tablets (by services users & visitors in clinical areas) Policy 5 CL062 Scope: This Policy applies all employees of the Trust,
DOCUMENT CONTROL Title: Version: Reference Number: Use of Mobile Phones and Tablets (by services users & visitors in clinical areas) Policy 5 CL062 Scope: This Policy applies all employees of the Trust,
JOB DESCRIPTON. Multisystemic Therapy Child Abuse & Neglect (MST-CAN) Supervisor. Therapists, Support Worker, Family Engagement Worker
 Supervisor. Therapists, Support Worker, Family Engagement Worker") JOB DESCRIPTON Post Title Multisystemic Therapy Child Abuse & Neglect (MST-CAN) Supervisor Service MST - CAN Job Number Grade 12 Responsible to Programme Manager Responsible for Therapists, Support Worker,
JOB DESCRIPTON Post Title Multisystemic Therapy Child Abuse & Neglect (MST-CAN) Supervisor Service MST - CAN Job Number Grade 12 Responsible to Programme Manager Responsible for Therapists, Support Worker,
Central Alerting System (CAS) Policy
 Policy") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Management of Violence and Aggression Policy
 Management of Violence and Aggression Policy Approved by: Trust Health and Safety Committee Date First Issued: August 2000 Reviewed July 2006 TABLE OF CONTENTS Section Page No 1 STATEMENT OF POLICY 2 SCOPE
Management of Violence and Aggression Policy Approved by: Trust Health and Safety Committee Date First Issued: August 2000 Reviewed July 2006 TABLE OF CONTENTS Section Page No 1 STATEMENT OF POLICY 2 SCOPE
A thematic review of six independent investigations. A report for NHS England, North Region
 A thematic review of six independent investigations A report for NHS England, North Region November 2014 Authors: Chris Brougham Liz Howes Verita 2014 Verita is a management consultancy that works with
A thematic review of six independent investigations A report for NHS England, North Region November 2014 Authors: Chris Brougham Liz Howes Verita 2014 Verita is a management consultancy that works with
TRUST WIDE CARE PROGRAMME APPROACH POLICY (INCLUDING ARRANGEMENTS FOR STANDARD CARE PLAN)
") TRUST WIDE CARE PROGRAMME APPROACH POLICY (INCLUDING ARRANGEMENTS FOR STANDARD CARE PLAN) Date effective from: 1 st May 2014 Review date: 28 th April 2016 Version number: 3.0 See Document Summary Sheet
TRUST WIDE CARE PROGRAMME APPROACH POLICY (INCLUDING ARRANGEMENTS FOR STANDARD CARE PLAN) Date effective from: 1 st May 2014 Review date: 28 th April 2016 Version number: 3.0 See Document Summary Sheet
Adult Mental Health Team AMHT Standard Operating Procedure
 SH CP 198 Adult Mental Health Team AMHT Standard Operating Procedure Summary: Keywords: Target Audience: This Standard Operating Procedure describes the roles and functions of The Acute Mental Health Teams
SH CP 198 Adult Mental Health Team AMHT Standard Operating Procedure Summary: Keywords: Target Audience: This Standard Operating Procedure describes the roles and functions of The Acute Mental Health Teams
Solent. NHS Trust. Allied Health Professionals (AHPs) Strategic Framework
 Strategic Framework") Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Open Door Policy (replacing policy no. 030/Clinical)
") A member of: Association of UK University Hospitals Open Door Policy (replacing policy no. 030/Clinical) THIS POLICY IS CURRENTLY UNDER REVIEW WITH THE POLICY AUTHOR POLICY NUMBER 138/Clinical POLICY VERSION
A member of: Association of UK University Hospitals Open Door Policy (replacing policy no. 030/Clinical) THIS POLICY IS CURRENTLY UNDER REVIEW WITH THE POLICY AUTHOR POLICY NUMBER 138/Clinical POLICY VERSION
CARE PROGRAMME APPROACH POLICY. Care Programme Approach. Quality and Safety Committee. Disclaimer
 CARE PROGRAMME APPROACH POLICY Reference No: UHB 118 Version No: 1 Previous Trust / LHB Ref No: T/226 Documents to read alongside this Policy Care Programme Approach Procedures Classification of document:
CARE PROGRAMME APPROACH POLICY Reference No: UHB 118 Version No: 1 Previous Trust / LHB Ref No: T/226 Documents to read alongside this Policy Care Programme Approach Procedures Classification of document:
Child and Adolescent Mental Health Services (CAMHS)
") Crisis Assessment & Treatment Team (C-CATT) Operational Policy Child and Adolescent Mental Health Services (CAMHS) Version: 2.1 Executive Lead: Lead Author: Executive Director Operations CAMHS Community
Crisis Assessment & Treatment Team (C-CATT) Operational Policy Child and Adolescent Mental Health Services (CAMHS) Version: 2.1 Executive Lead: Lead Author: Executive Director Operations CAMHS Community
Adult Therapy Services. Community Services. Roundshaw Health Centre. Team Lead / Service Manager. Service Manager / Clinical Director
 THE ROYAL MARSDEN NHS FOUNDATION TRUST Job Description Job Title Specialist Neuro Physiotherapist - Community Neuro Therapy Service Area of Specialty Adult Therapy Services Directorate Community Services
THE ROYAL MARSDEN NHS FOUNDATION TRUST Job Description Job Title Specialist Neuro Physiotherapist - Community Neuro Therapy Service Area of Specialty Adult Therapy Services Directorate Community Services
The Scottish Public Services Ombudsman Act 2002
 Scottish Public Services Ombudsman The Scottish Public Services Ombudsman Act 2002 Investigation Report UNDER SECTION 15(1)(a) SPSO 4 Melville Street Edinburgh EH3 7NS Tel 0800 377 7330 SPSO Information
Scottish Public Services Ombudsman The Scottish Public Services Ombudsman Act 2002 Investigation Report UNDER SECTION 15(1)(a) SPSO 4 Melville Street Edinburgh EH3 7NS Tel 0800 377 7330 SPSO Information