Quality Improvement Program Evaluation
|
|
|
- Shauna Barker
- 6 years ago
- Views:
Transcription
1 Denver Health Medical Plan, Inc. Quality Improvement Program Evaluation 2013 Commercial and Exchange Products 1 Page
2 Table of Contents I. Executive Summary...3 II. Quality Improvement Program Evaluation and Work Plan...4 Overview...4 Quality Improvement Objectives for QI Program Scope...5 Quality Improvement Program Accomplishments and Strengths...6 Opportunities for Improvement...8 Clinical Guidelines...8 Preventive Guidelines...8 III. Quality of Clinical Care Activities...9 Diabetes...9 Preventive Health...11 Prenatal/ Postpartum Care Indicators...11 Childhood Preventive Health...15 Preventive Cancer Screenings...21 Asthma...22 Behavioral Health...22 Complex Case Management...25 IV. Safety and Quality of Clinical Care...26 Quality of Care Concerns...26 Credentialing and Provider Networks...27 Continuity and Coordination of Care...29 V. Quality of Service Member Satisfaction (CAHPS)...29 Grievance Reporting and Trending...32 Safety of Clinical Care...33 Member Services...34 VI. Overall Structure of the QI Program...35 Committee Structure...38 Summary of Future Outcomes...39 VII. QI Activities Summary...39 VIII. Attachments: Page
3 I. Executive Summary The Denver Health Medical Plan, Inc. (DHMP) is a licensed Health Maintenance Organization (HMO), effective 1/1/97, with the responsibility for managing the following DHMP employer/member groups and their health care: City and County of Denver (CSA) Denver Health and Hospital Authority (DHHA) Denver Employees Retirement Program (DERP) Denver Police Protective Association (DPPA) DHMP established and maintains a comprehensive quality improvement (QI) program to systemically define, evaluate and monitor continuous quality improvement, ensuring high quality, cost effective care and services are provided to DMHP members. The Quality Improvement program incorporates evaluation of key indicators of care and service, identifying improvement opportunities and designing and implementing interventions to increase defined quality metrics. A multidimensional approach is utilized to measure effectiveness. Dimensions evaluated include appropriateness, efficiency, effectiveness, availability, timeliness, continuity and cost of care and services, as well as health outcomes and member and practitioner/provider satisfaction. We describe ongoing and completed quality improvement activities, analysis of our results and overall evaluation of effectiveness of our program, which are reported and reviewed in the annual program evaluation. From this evaluation process, we develop recommendations for the upcoming year, which are incorporated into the quality improvement program description and work plan. DMHP is able to assess the strengths of the program and identify opportunities for improvement, incorporating learning from the ongoing activities. In this report, DMHP quality improvement program activities are summarized and evaluated, including program accomplishments and opportunities, with tracking and trending of results and data over time. Data is systematically collected prospectively, concurrently, and/or retrospectively on clinical, safety, preventive and service performance. This data is analyzed, summarized, and presented as information, with recommendations to Quality Management Committee (QMC). QI actively collaborates with other Managed Care departments as well as our network providers to develop, implement and evaluates quality improvement initiatives. QI collaborative activities are executed and coordinated with case management, care management, member services, provider/network services, claims, marketing and product line managers for DHMP. Our network providers we work with include the Ambulatory Care Services of Denver Health, known as Community Health Services (CHS) and the expanded Cofinity Network, including University and Children s Hospital, for more expansive health plan offerings. We collaborate with Denver Health Community Health Services on QI initiatives through the Ambulatory QI Committee, the clinical design work group, disease and prevention specific work groups and the patient experience work group. In these committees and groups, we join resources and actively work together to increase the health and wellbeing of our members. 3 Page
4 For DHMP members affiliated with Ambulatory Care Services/Community Health Services, Denver Health is promoted as their medical home. A patient centered medical home is responsible for care coordination and provides health maintenance preventive care, anticipatory guidance and health education, acute and chronic illness care, coordination of medications, specialists, and therapies, and twenty-four hour telephone care. It is member centered and encourages the member to be a partner in their health care decision making. CHS is pursing National Committee on Quality Assurance Accreditation (NCQA) for their Patient Centered Medical Home (PCMH) care services in calendar year Provider and Clinician CAHPS surveys have recently begun at the CHS clinics to measure patient satisfaction with their provider and their care. The Cofinity provider network is an expanded and essential part of our new Quality Management Committee (QMC) structure. Providers within this network serve our point of service (POS) members within our commercial plan. Our quality improvement initiatives support collaboration with these practices and facilities in working together to improve the quality and patient experience for our members. II. Quality Improvement Program Evaluation and Work Plan Overview The QI Program Description and QI Work Plan provide guidance to the program structure and activities for a period of one calendar year. Input is obtained from the Operations Management Team, staff, data sources, satisfaction indicators and contract requirements. A QI work plan is prepared annually for the upcoming year for submission to the Quality Management Committee (QMC) and DHMP Board of Directors for approval. The work plan includes the following elements: Written, measurable objectives for the year. Planned quality of care and safety of clinical, preventive and services initiatives. Scope of the QI program including all clinical, safety and service indicators, responsible person, implementation, management, and timeframe of the initiatives. Schedule of reports and planned activities. Timeframe for evaluation of the effectiveness of the QI program. Quality Improvement Objectives for 2013 Deliver quality care that meets community standards and offer customer focused service to our members and practitioners and providers. Continuously measure, analyze, evaluate and improve the clinical care and administrative services of the plan and health care services delivered by contracted practitioners/providers, using Healthcare Effectiveness Data and Information Set (HEDIS) measures, QI projects and activities, and member surveys. 4 Page
5 Implement internal quality improvement activities as necessary. Adopt national and/or local public health goals as benchmarks and commit resources for QI activities that strive to meet the goals. Promote medical and preventive care delivered by contracted practitioners and providers that meets or exceeds the accepted standards or benchmarks of quality in the community. Empower members to lead a healthy lifestyle through health promotion activities, community outreach efforts and coordination with public and private community resources. Encourage safe and effective clinical practice through established care standards and applying appropriate practice guidelines. Monitor and evaluate high volume and/or high risk services to identify opportunities for improvement. Measure, evaluate, and offer interventions to address continuity and coordination of care. Coordinate delegated activities on behalf of contractual organizations. Address special needs of racial and ethnic minorities. Obtain input and participation from members as well as the interdisciplinary care team about the QI program. Maintain the health information system to comply with HIPAA and privacy laws and professional standards of health information management. QI Program Scope The QI program includes all administrative departments and services rendered to members by participating providers and practitioners, including inpatient and outpatient care, ancillary services, skilled nursing care, home health, infusion therapy, hospice, durable medical equipment, physical therapy, imaging, laboratory, pharmacy services, and behavioral health services. The program is comprehensive in scope, is ongoing and includes strategies to monitor, identify, evaluate and resolve problems that affect the accessibility, availability, continuity and quality of care and service provided to DHMP members. The QI program is integrative and designed to link structure, process, and knowledge throughout the Plan to assess and improve quality of health care services. The QI team is responsible to implement the following: Identify and prioritize quality activities based on NCQA and regulatory requirements. Reviews data annually to determine QI activities that will have a significant impact for our population. Analyze utilization of medical services as well as Case Management data to identify issues of over and underutilization. Utilize national goals as well as NCQA, HEDIS, national and regional benchmarks to establish goals for the Plan. Using geo access software to analyze access and availability of providers and pharmacies for the membership. An annual access report is completed that looks at geo access results for member access, panel sizes, telephone responsiveness, referral turnaround timeframes, and monitoring of appointment standards through the Denver Health Centralized Appointment Scheduling system. 5 Page
6 Recommendations for quality improvement initiatives from the QI team are reviewed by the QMC. The initiatives are designed to improve performance on selected aspects of clinical care and safety, continuity and coordination of care, preventive care and services to members. Quality improvement activities are conducted utilizing the following processes: Prioritize specific indicators of performance Collect appropriate data Analyze data Identify opportunities to improve performance Implement interventions to improve performance Measure effectiveness of interventions and /or conformance to guidelines Re-evaluate for further potential performance improvements The primary source of information for quality improvement initiatives are from HEDIS and Consumer Assessment of Health Providers & System (CAHPS). HEDIS clinical outcomes measures data are reviewed for diabetes, cardiovascular conditions, musculoskeletal condition, prenatal and postpartum care, respiratory conditions, medication management, behavioral health care and preventive health screenings for children and adults. For quality of service, multiple sets of data are reviewed: (i) CAHPS member satisfaction survey data and HEDIS use of services and access and availability measures (ii) grievance and appeal data and (iii) quality of care concerns and service complaints. Quality Improvement Program Accomplishments and Strengths In the past year, the QI program team members have been instrumental in the planning, assessment, implementation and review of various QI activities, highlighted below: Participated in collaborative QI work group activities with CHS on several QI interventions in disease management and prevention Began development and training to facilitate appropriate provider documentation in support of improving HEDIS scores Increased member outreach to encourage preventive health screenings Utilized innovative technology interventions (text messaging and IVR) to promote member/patient self-management of health care conditions Developed, implemented and evaluated incentives for members to engage in evidence based prenatal and postpartum care Continued enhanced collaboration with DH School Based Health Centers (SCHCs) to increase number of well child visits and immunizations within Denver Public Schools Analyzed effectiveness of member outreach, specific to mailers Collaborated with behavioral health and wellness to increase health coaching and wellness offerings for members Developed and implemented enhanced patient education materials Developed and conducted a provider satisfaction survey Collaborated with Pharmacy to evaluate and facilitate a plan to increase CAHPS scores Developed and executed a Health Fair to provide routine screening and monitoring at no cost to the member 6 Page
7 Incorporated data from CHS registries and data warehouse into supplemental files used for HEDIS reporting Maintained strong oversight and follow-up of delegated and facility credentialing relationships Enhanced reporting of quality of care concerns (QOCC) Facilitated process or system improvements identified during the QOCC review process Streamlined clinical and preventive guidelines Increased outreach to DHMP members through CHS clinics and targeted member outreach at high volume point of service offices Facilitated physician involvement in the development of clinical guidelines Continued the development, review and revision of policies and procedures annually through electronic tracking process Increased physician involvement from the Cofinity network within the Quality Management Committee (QMC) structure The overall effectiveness of the QI program increased this past year. Pursing NCQA accreditation has provided an opportunity to review our infrastructure and do critical analysis of opportunities for improvement. Evaluation of policies/procedures; workflow process improvement; restructuring of QI staff role/functions and increased outreach with our members and providers are some of the changes that have been driven, in part, by our pursuit of NCQA accreditation. The adequacy of resources for the QI program has been challenging for calendar year The Quality Improvement team has not been fully staffed for the entire calendar year, including the absence of a director for the first eight months of Fiscal challenges resulted in 2.5 positions being eliminated from the Quality Improvement team permanently, so restructuring of positions to meet deliverables has been crucial. We continue to evaluate our need for more resources, especially in HEDIS data collection, analysis and development of interventions. Increasing our HEDIS scores requires more than once a year looking at the data results to be effective and to give timely feedback to our providers on performance. As the movement towards star ratings of health plan performance occurs, DMHP will need to strategize and continuously evaluate how to best use QI resources. Alignment and collaboration with other QI initiatives being done by CHS and providers in the Cofinity network will help maximize our limited resource availability. Our committee structure continues to be a work in progress The structure change that was set up in the last six months of 2013 appears, at first blush, to be significantly better. Continuous evaluation over 2014 will be needed to monitor effectiveness and identify opportunities for improvement. The subcommittee structure, along with medical plan departments reporting up to the Quality Management Committee, provides the organization with a quality improvement focus organization-wide. Practitioner participation is a key metric to continue to evaluate in We have increased our practitioner involvement with QMC, which allows practitioner input into all aspects of health plan operations and services. Increased involvement of QI team members in ambulatory quality improvement work groups; clinical design work groups and disease and prevention work groups within CHS and outreach to Cofinity providers will need to continue and to increase in Targeted interventions to Cofinity providers, with a focus on HEDIS data outreach and training, will be an important part of the 2014 work plan. 7 Page
8 Leadership involvement, defined as the management team from DHMP, the management team from CHS and providers from our Cofinity network, has increased through several mechanisms. The restructuring of the QMC, with increased involvement from the Cofinity network, has offered an opportunity for the management team of DMHP and the provider network to interact and collaborate more closely on quality initiatives. The director of QI is involved on several quality committees and workgroups within CHS, including the ambulatory quality improvement committee; the clinical design work group (which approves all interventions); and the patient experience work group (designed to focus on increasing CAHPS scores and customer service metrics). QI team members interact on a wide variety of disease and prevention work groups with leadership staff within CHS. Opportunities for Improvement Increase engagement and training of providers in quality improvement initiatives, such as training to increase HEDIS scores through appropriate medical record documentation and coding Continue to evolve the leadership potential and role for the QMC by providing education and increasing opportunities for feedback, oversight and partnerships Review updated policies and procedures on a continual basis, developing a work/action plan to assure policy expectations and deliverables are being realized in agreed upon timeframes and documentation standards Align and partner quality improvement initiatives and interventions with our CHS and Cofinity provider networks to avoid duplication of effort and to utilize resources more effectively.. Continue evaluation of quality improvement team resources to achieve current quality improvement goals and to anticipate coming quality improvement measurement changes, such as STAR ratings for our commercial membership Clinical Guidelines Reviewed and updated the following Clinical Care Guidelines in 2013 Diabetes Management Standards Management of Asthma in Adults and Children Management of High Risk Newborns After Hospital Discharge Treatment of Depression in Adults in Primary Care Pharmacologic Management of Congestive Heart Failure Treatment of ADHD in Children and Adolescents Preventive Guidelines Reviewed and updated the following Preventive Care Guidelines in 2013 Care of Well Newborn Pediatric and Adolescent Immunization Criteria Pediatric and Adolescent Health Appraisal Adult Immunizations Prenatal Care 8 Page
9 Smoking Cessation Both Clinical and Preventive Guidelines guide the QI team in their clinical care quality activities and interventions with providers and members III. Quality of Clinical Care Activities Indicators for clinical care are based on HEDIS outcome measures and include: diabetes, cardiovascular conditions, asthma, prenatal and postpartum care, behavioral healthcare and preventive health screening measures. Review of these measures is conducted once a year. The results are available after successfully passing the HEDIS audit in June. Results are compared to the previous year and trended over several years HEDIS rates are based on 2012 data, the previous year rate, and the 90 th percentile benchmark, which is our goal and considered the gold standard. The following QI initiatives are focused on these clinical indicators with the purpose of improving the quality of clinical care for our members. Breast Cancer Screenings In June of 2013, QI made the decision to include Commercial members in a mammogram outreach reminder mailing program. Specifically, this intervention reminds members to obtain breast cancer screening in the month Denver Health claims data indicate they are due. The mailing card provides information about convenient options for mammography, including the Women s Mobile Clinic calendar and the phone number for our radiology department. Initially, the monthly mailing outreach contact list included both facets of the DHMP commercial plan (001, POS). However, after a few months of receiving privacy complaints from the members within the Cofinity Network, QI downsized the list to only include the HMO members. Health Fair Event On November 22, 2013 a Saturday Health Fair was held for the Commercial population at the Level One Physicians Clinic. This health fair provided routine screening and monitoring tests as well as an education component focusing on exercise and diet. Screenings: BMI, LDL, Blood Pressure, Breast Cancer Screening, Colorectal Cancer Screening, Well Woman Visits, and Adult Well Visits. Participation rate: At this event, providers saw 35 patients and completed nine labs for a total participation rate of 44 members. Our HEDIS 2013 rates will not include the impact of this intervention; data from HEDIS 2014 rates allow us to assess the overall impact of this project. Diabetes 2013 HEDIS Diabetes Results for Commercial Line Diabetes Indicators 2011 HEDIS 2012 HEDIS Commercial 2013 HEDIS 2013HEDIS 90 th 9 Page
10 Results Results Results percentile HbA1c Testing 89.69% 86.41% 88.22% 94.38% HbA1c Poor Control >9.0% (lower=better performance) 37.81% 39.16% 35.05% 18.18% HbA1c Control <8.0% 49.69% 46.28% 48.94% 70.99% Eye Exam 50.0% 44.34% 40.18% 74.09% LDL Testing 81.88% 80.58% 79.15% 90.02% LDL < % 44.66% 48.94% 56.2% Monitoring for Diabetic Nephropathy 85.31% 82.85% 75.53% 89.54% Blood Pressure <140/80* new for % 49.19% 56.80% 54.84% Blood Pressure <130/80* retired N/A N/A NA NA Blood Pressure <140/ % 68.28% 74.62% 77.37% HEDIS 2013 Changes There were no changes made during measurement year Summary of 2013 HEDIS Diabetes Results Comparison to 2013 HEDIS benchmarks reveals that we are well below the gold standard (90th percentile benchmark) for all diabetes indicators except for BP<140/80. A test of statistical significance revealed significant increase in BP control for the following standards: BP<140/80 (p=.05) and BP<140/90 (p<.001). There was no significant change in any other diabetes measures from HEDIS HEDIS 2013 at the p=.05 level. However, the QI team observed non-significant increase in the following diabetes measures: HbA1c testing, HbA1c control (<8.0%), and LDL-C control (<100mg/DL). DHMP Diabetes Collaborative DHMP QI staff members as well as representatives from DHMP, Denver Health, and the Federally Qualified Health Centers (FQHC) practices participate in the Denver Health Diabetes Collaborative. Participants provide regular updates, engage in discussions related to diabetic metrics, and incorporate changes in the Diabetes Registry. The workgroup approved a system for the registry to automatically flag patients who were in need of follow-up testing based on lab results and last dates of service. DHMP QI staff provided input on scripts for a self-management intervention using innovative technology including text-messaging, as well as providing expertise on the use of IVR as an intervention for promoting selfmanagement. The collaborative regularly tracks patients outcomes for diabetes control as well as blood pressure and LDL control Interventions Quality Improvement designed a health fair for Commercial members that took place on November 22 nd, Members had the opportunity to receive routine, diabetes-related monitoring tests such as HbA1c and LDL screenings. Additionally, Managed Care Behavioral Health and Wellness offers a diabetes management program called Take Control of Your Diabetes. 10 Page
11 Cardiovascular 2013 HEDIS Cardiovascular Indicator Results Cardiovascular Indicators 2011 HEDIS Results DHMP Commercial 2012 HEDIS Results 2013 HEDIS Results 2013 HEDIS 90 th percentile Controlling High Blood Pressure BP <140/ % 63.75% 64.72% 72.94% Cholesterol Management Cardiovascular Conditions (AMI, CABG, PTCA, or IVD) LDL Testing *NA 89.74% 80.00% 92.68% LDL <100 *NA 79.49% 64.44% 71.64% *NA; not reported because sample size <30 HEDIS 2013 Changes. There were no changes made during measurement year Summary of 2013 HEDIS Controlling High Blood Pressure Results There were no statistically significant differences from 2012 to However, QI observed a non-significant increase for this measure. Still, Denver Health s CBP rate still sits well below the HEDIS 90 th percentile benchmark for Preventive Health Preventive health includes the following HEDIS outcome measures: Prenatal and postpartum care Adolescent and childhood immunizations/well visits Preventive cancer screenings: colorectal, breast and cervical cancer screenings. Each measure is reviewed below with a comparison of the 2011 and 2012 results to the previous year and to the HEDIS 90 th percentile. In addition, we describe the interventions that occurred during 2013 and the activities planned for Prenatal/ Postpartum Care Indicators 2013 HEDIS Prenatal/Postpartum Indicator Results Prenatal Care in 1 st Trimester Postpartum care within days 2011 HEDIS Results DHMP Commercial 2012 HEDIS Results 2013 HEDIS Results 2013 HEDIS 90 th percentile 79.65% 85.98% 94.57% 96.97% 73.84% 69.51% 80.43% 90.25% 11 Page
12 after delivery HEDIS 2013 Changes There were no changes made during measurement year Summary of 2013 HEDIS Prenatal/Post-Partum Results For HEDIS 2013, we saw an increase in the rate of women who receive prenatal care in the first trimester as well as an increase in the rate of women who receive postpartum care within the allotted timeframe from HEDIS For Timeliness of Prenatal Care, we are above the 50 th percentile. For Postpartum Care, we are above the 25 th percentile. Medical record review indicated that women may be accessing prenatal and postpartum care, but are doing so outside of the HEDIS timeframes. To determine if the changes in the rates between HEDIS 2012 and HEDIS 2013 are statistically significant, the following analysis was done, all using a Z-test for population proportions: There was an increase of 8.59% in the rate for Timeliness of Prenatal Care. With a p-value of , this increase marks a statistically significant change. There was an increase of 10.92% in the rate for Postpartum Care. With a p-value of , this increase marks a statistically significant change QI Activities/Interventions Online Childbirth Education In 2011, DHMP Marketing and QI worked together to promote The Gift of Motherhood elearning Childbirth Education Program. The program is an interactive, web-based tool that allows expectant mothers to be more prepared for childbirth. A marketing flyer about the program is sent out monthly to women who have been identified as being pregnant through a claims report. Denver Health does not currently offer in-person prenatal classes to new mothers because the Online Childbirth Education Program gives mothers more education specific to their needs at times convenient for them. In 2011 we had 2-3 members request an online login code. We continued this outreach in 2012 with additional marketing and promotion of our new benefits for Mom & Baby. In 2012, we had 17 Commercial members request an online login code for The Gift of Motherhood elearning Childbirth Education Program. In 2013, 13 Commercial members requested an online login code for the elearning program. In 2013, Denver Health also began offering in-person birth classes at various clinics, which may account for the decrease in requests for login codes. For 2013, QI set a goal of seeing an increase in 25% from 2012 for the number of requests. With only 13 members, there was actually a decrease. For 2014, we hope to see a 25% increase from 13 members and a request for 17 login codes. In 2011, we worked with the Woman s Care Clinic to develop additional benefits available only for mothers coming in for prenatal visits at Denver Health. This program began in January 2012 and was for Commercial members only. These new benefits were distributed to women who complete a series of prenatal visits during their pregnancies. This initiative was developed in collaboration with marketing to 12 Page
13 encourage mothers to keep their prenatal care within the DH system and deliver at our state-of-the-art Labor and Delivery facilities. In 2013, Marketing at Denver Health Medical Plan, Inc. rolled out a program involving additional incentives for keeping well-child visits within the baby s first year at Denver Health. Additionally in 2013, both Quality Improvement and Marketing staff made concerted efforts to educate and inform clinics and new mothers and members about the available incentive programs through the Denver Health Medical Plan, Inc. Year 1 st Visit: Coupon Book Requests 6-10 Week Visit: Spa Kits DHMP Commercial Prenatal Benefits 20 Week Ultrasound Visit: Photo Frames Week Visit: Onesies Denver Health Tour: Umbrella Strollers After Delivery: Car Seats After Delivery: 2 Month Supply of Diapers Postpartum Visit: 1 month Supply of Diapers (54.4%) 61 (25.7%) 61 (25.7%) 60 (25.3%) 64 (27.0%) 73 (30.8%) 65 (27.4%) 51 (21.5%) For 2013, 237 commercial members had an OB intake visit that qualified them to receive the prenatal mailing. Of those who received information on the prenatal incentive program, 129 (54.4%) requested a coupon book. The participation goal for 2013 was 55%, meaning we are within our goal range. For 2014, we will continue to educate members on the availability of the prenatal incentive program, as well as provide clinics with handouts and education on the availability of the program. For 2014, we hope to have a participation rate for coupon book requests for 57%. Baby s First Year For 2013, the marketing department has expanded additional benefits to include Baby s First Year, incentives. For each newborn visit completed in the first 12 months of life, members will receive an incentive for their baby. The program began in Marketing will continue to monitor and track participation in the program for Year 2 Week Visit: Diaper Bag 2 Month Visit: Baby Monitor DHMP Commercial Baby s First Year 4 Month Visit: Healthy Baby Kit 6 Month Visit: Activity Gym 9 Month Visit: Booster Chair 1 Year Visit: 1 month Supply of Diapers (14.0%) 20 (14.7%) 15 (11.0%) 12 (8.8%) 6 (4.4%) 5 (3.6%) For 2013, 136 commercial members had a live birth. The percentages here represented the number of requested and completed incentives for 2013 based on the total number of births over the course of the year. Because live births continue throughout the year, and the Baby s First Year incentives are given based on the child meeting certain well-child visit timelines, those visits that mark the 2-month, 4-month, 6-month, 9-month, and 12-month milestones may not yet be completed for women who gave birth in We will continue to monitor our rates for participation in Baby s First Year, while continuing to 13 Page
14 educate members on the availability of the incentive program and the importance of completing timely well-child visits. The 2013 baseline goal was set at 10% for the first year of implementation. Since the highest number of women who gave birth in 2013 will have already most likely completed the 2-week visit, we can base our goal off of the 14.0%. For 2014, we hope to see a participation rate of 16%. Postpartum Intervention: DHMP identified an opportunity to improve our postpartum care visits completed within the HEDIS specifications of 21 to 56 days following delivery for our members. In August of 2009, we started mailing flyers informing the member to schedule a timely postpartum visit. If the visit is completed during the HEDIS timeframe, members receive an incentive. Once the visit information was verified, the member was sent a $25 retail gift card. Quality Improvement staff provided outreach education to clinics and clinic staff regarding timeliness of the postpartum incentive. Year Total Mailed Total Number with Visit Percent Complete Total Receive Incentive Percent Receive Incentive % 34 31% % 32 35% % 26 30% % % Analysis There was a decrease in the total number of women who received a postpartum flyer, but a large increase in the percent of women who completed a postpartum visit at all. The goal for 2013 was to have a 31% response rate for postpartum flyers and women who return the incentive. For 2013, we had a 28.4% response rate. For 2014, we will attempt to increase the response rate to the 2013 goal of 31%. Additionally, of those 90% who completed a postpartum visit in 2013, only 27 (22.0%) of women were within the HEDIS timeframe. The discrepancy between the 27 who completed the visit within the timeframe and the 35 women who received the incentive may come from the clinics, who have been distributing the postpartum flyers to women who may not have been on the mailing distribution list. Due to the fact that 96 (78.1%) of members had a postpartum visit but were outside the timeframe, we will increase our efforts to ensure visits are completed per the HEDIS specifications Interventions QI will continue to provide educating regarding prenatal and postpartum programs to the members and providers, emphasizing the importance of timely and adequate prenatal and postpartum care. QI will continue the mailing plus incentive during 2014 alongside marketing s Mom & Baby benefits. With these new incentives, we will continue to monitor our HEDIS rates for improvement. Denver Health Medical Plan, Inc. has also been collaborating with Denver Health Medical Center and partner clinics to increase PPC HEDIS rates. QI has been creating a weekly postpartum call list by collecting deliveries weekly off the Denver Health daily log and collecting faxes from outlier hospitals. DHMP will work the list each week to call members three to five days after delivery to help schedule a postpartum visit within 14 Page
15 the HEDIS timeframe. Members will also receive a call the week prior to the visit to ensure members will complete the scheduled visit. This intervention will be tracked and evaluation, and will be rolled out to delivering prenatal outreach calls if found effective. Childhood Preventive Health 2012 HEDIS Childhood Preventive Health Indicator Results Childhood Preventive Measures 2011 HEDIS Results 2012 HEDIS Results Commercial 2013 HEDIS Results 2013 HEDIS 90 th percentile Childhood Immunization Status DTP 94.29% 87.72% 86.99% 93.43% MMR 97.14% 92.98% 93.15% 95.60% OPV/IPV 97.14% 93.86% 94.52% 96.53% H Influenza Type B 95.71% 92.98% 94.52% 97.81% Hepatitis B 91.43% 85.96% 95.21% 94.74% Chicken Pox 97.14% 92.98% 91.10% 95.45% Pneumococcal Conj 92.86% 87.72% 90.41% 93.67% Hepatitis A 52.86% 44.74% 88.36% 88.67% Rotavirus 81.43% 80.70% 78.77% 85.42% Influenza 70.00% 66.67% 78.77% 76.16% Combo % 81.58% 83.56% 88.00% Combo % 78.95% 82.88% 86.00% Immunizations for Adolescents Meningococcal 79.52% 73.45% 79.03% 86.49% Tdap/Td 86.75% 87.61% 90.32% 94.51% Combo % 73.45% 78.23% 85.53% Well Child Visits 0-15 months (6+) 81.82% 80.34% 82.03% 91.43% 3-6 y/o (annual) 78.31% 75.77% 79.24% 86.52% y/o (annual) 42.50% 38.93% 41.95% 63.11% HEDIS 2013 Changes. There were changes made during measurement year 2012 to the Hepatitis A vaccination. Beginning in measurement year 2012, only one Hepatitis A vaccination is required for compliance on this component of the measure. Commercial Summary of 2013 HEDIS Child Immunization Results Childhood Immunization Status (CIS) 15 Page
16 For HEDIS 2013, DHMP rates for Hepatitis B were above the 90 th percentile when using the HEDIS 2013 benchmarks. The remainder of the immunization rates was below the 90 th percentile. All of the commercial immunizations rates, with the exception of DTaP, VZV, and Rotavirus, increased from HEDIS 2012 to HEDIS To determine if these changes were statistically significant, analysis was done using a Z-test for population proportions. The results are as follows: The rates of the following immunizations resulted in a p-value greater than p=0.05: DTaP, IPV, MMR, H influenza B, Pneumococcal Conjugate, and Rotavirus. It can be concluded that any changes seen between HEDIS 2012 and HEDIS 2013 for these measures are not statistically significant. The rate for Hepatitis B immunizations increased between HEDIS 2012 and HEDIS With a p-value of , this change is statistically significant. It can be concluded that the rate is significantly higher for HEDIS The rate for Hepatitis A immunizations increased between HEDIS 2012 and HEDIS With a p-value less than , this change is statistically significant. It can be concluded that the rate is significantly higher for HEDIS The rate for Influenza immunizations increased between HEDIS 2012 and HEDIS With a p-value of , this change is statistically significant. It can be concluded that the rate is significantly higher for HEDIS The rate for Combination #8 immunizations increased between HEDIS 2012 and HEDIS With a p-value of less than , this change is statistically significant. It can be concluded that the rate is significantly higher for HEDIS Denver Health Medical Plan, Inc. has strong immunization rates for the commercial pediatric members. For 2014, we will increase partnership with the Medication and Immunization Committee at Denver Health and Hospital Authority as well as work with the Pediatric Preventive Work Group as a way address shifts in our members immunization rates. Additionally, efforts to increase timely well child visits and newborn visits should have a positive impact on the vaccinations required to complete in the first 2 years of life. Immunizations for Adolescents (IMA) For HEDIS 2013, DHMP rates for adolescent immunizations were below the 90 th percentile. All adolescent immunizations increased from HEDIS 2012 to HEDIS To determine if these changes are statistically significant, analysis was done using a Z-test for population proportions. All p-values were found to be greater than 0.05, and therefore no changes were statistically significant. In addition to partnering with the Pediatric Prevention Work Group and the Medication and Immunization Committee, we plan to work with School Based Health Centers (SBHC) to increase the rate of adolescents receiving vaccinations. Upon discussion with various stakeholders, it was decided that an effort to increase adolescent well visits would correlate with an increase in adolescent immunization rates. 16 Page
17 Commercial Summary of 2012 HEDIS Well-child Visits Well Child Visits (W15, W34, AWC) Between HEDIS 2012 and HEDIS 2013, the rates for Well-Child Visits within the First 15 Months of Life (W15), Well-Child Visits in the Third, Fourth, Fifth and Sixth Years of Life (W34), and Adolescent Well-Care Visits (AWC) all increased. All well-child visit measures were below the 90 th percentile. To determine if these changes were statistically significant, an analysis was performed using a Z-test for population proportions. All p-values were found to be greater than 0.05, and therefore no changes were statistically significant. In 2012, HEDIS well child visit rates for 0-15 months (6+ visits) had decreased compared to the previous year and a process was put in place to count the 3 day RN well visit by having a provider cosign for the visit in order to receive validation as compliant well visit. This could attribute to the increase in the W15 rate in HEDIS Preventive Health QI Activities and Member Outreach School Based Health Centers (SBHC) Collaboration In the fall of 2008, we collaborated with 12 Denver area school based health clinics to reach out to our members in need of an annual well child visit. We provided back to school registration assistance by conducting look ups in the immunizations registry and in EDM visits to identify needed medical services. We provided a reminder card to the student with a notation of services needed and some schools were able to make the needed follow-up appointments on the spot. Each parent is required to register their child and sign a consent form that permits the SBHC to provide health care services. Each school semester DHMP QI staff request a copy of the school enrollment and match to our active enrollment and then return the list to the SBHC for follow- up for members in need of health care services. DHMP Commercial SBHC Enrollment and WCC Completion Semester Total DHMP Total with Up-todate WCC at Total DHMP Total WCC Members Performed Enrolled in Beginning of Needed WCC During Semester SBHC Semester Spring (47%) (31%) Fall (47%) (24%) Spring (35%) (37%) Spring 2012 *66 21 (32%) *45 16 (36%) Fall 2012 *52 35 (67%) *17 6 (35%) Spring (60%) 21 5 (24%) Fall (65%) (61%) 17 Page
18 *In 2012, CHP+, another line of business for Denver Health, was separated out of this report into its own standing report. This resulted in a greatly reduced enrollment for Commercial compared to years prior. For 2013, there was a decrease in the percent of members who had a well-child visit completed during the semester. For fall 2013, there was a large increase in the percent of children who received a well-child visit during the semester. There were some changes to the data collection process during the year, and that may account for some of the increase. DHMP met the goal of improving the number of well child visits need for commercial by 25%. With an additional 11 visits, the total number of children with a commercial plan enrolled in a SBHC who have a compliant well-child visit by the end of the year increased from 33 to 44, for a total of 86%. The completion of 86% of well-child visits surpasses our goal of improving the number of well-child visits by 25% from the baseline of 65%. The now 15 SBHCs are located in middle schools and high schools with another 20 satellite elementary schools that feed into the SBHCs. The age range of enrollees in the SBHC is 3 years through 21 years old. We plan to continue this intervention for 2014 and in addition will distribute the outreach list to SBHC on a monthly, rather than semi-annual, basis. The list will only be distributed back to clinics during the school year months of November through May. Additionally, DHMP is increasing collaboration with SBHC in an effort to enroll more health plan members in the SBHCs. When members go to school within Denver Public Schools, they can receive care quickly and cost-effectively at the SBHCs. The SBHCs have availability when other clinics may not, so increasing the number of members enrolled in these clinics can improve timely access to health care services. Newborn Visit Reminders for DHMP The rate for a 9 month well child visits are typically low since there are no immunization scheduled for this visit. In order to improve the 9 month well child visit rate we developed a culturally sensitive postcard reminder which is sent to the parent whose child has not completed this visit by their 10 month age. In 2012, the newborn mailings were moved to being sent to 6-month olds and included education to caregivers on the importance of completing all newborn visits within the first year of life. This is an attempt to reach members earlier in order to schedule an appointment. The analysis of 2012 showed that contacting members earlier increased visits within the 2 months of the mailer significantly. Other contributors to the higher rate of visits are the number of mailings sent was higher for 2012 then it has been in the previous years. Year Total DHMP** Postcards Mailed # Undeliverable # with visit within 2 months of mailing (40%) (31%) 2012 *126 3 *75 (60%) 2013 ** (76%) *For 2012, CHP+, another line of business for Denver Health which was combined with DHMP, was separated out of this report into its own standing report. 18 Page
19 **For 2013, CHP+ is no longer included in the report, which would account for the decline in postcards mailed. For 2013, the percent of members who completed a visit within 2 months of receiving the mailing increased from 60% in 2012 to 76% in This surpasses our goal of 50% for Additionally, 88% of members in this list had at least one well-child visit during the measurement year, surpassing our overall goal of 75%. For 2014, we will amend and evaluate the newborn mailing to be more in line with the HEDIS specifications of recommending 6 or more well-child visits in the first 15 months of life. Additionally, in 2013, the QI team conducted an evaluation of the newborn postcards divided out by line of business against a baseline historical rate from 2007 to determine if there was a significant change in the number of children coming in for a well-child visit within 2 months of turning 6 months and coming in at all when comparing the control from 2007 and the intervention group from This overall evaluation was conducted to determine mailer effectiveness with promoting an increase in well-child visits through targeted mailings. Plan A Well Child Visit within 2 Well Child Visit at All During Months of Turning 6 Months Year 2007 (Baseline) 26.3% 46.9% % 84.8% POS Well Child Visit within 2 Well Child Visit at All During Months of Turning 6 Months Year 2007 (Baseline) 15.2% 21.7% % 42.9% The intention of this intervention is to get members with less than 4 newborn well visits at the time of the mailing in for a well-child visit. Per these specifications, it seems that the intervention is effective. With p-values all less than 0.05, the proportion of members that come in for a visit (both within 2 months and at any time) is statistically significantly higher in 2012 than in The only exception is the proportion of POS members that come in for a well-child visit within 2 months of receiving the mailing. In this case, there is no statistically significant difference between the years. While the intervention seems to be effective in encouraging caregivers to bring children in for the visit nearest the one recommended at 6 months of age, the intention of the W15 HEDIS measure it to determine which members completed the recommended 6 or more visits in the first 15 months of life. Although the intervention is successful in terms of getting a member with less than 4 visits in for another visit, this does not necessarily mean that the member has come in for all 6 visits Interventions For 2014, the newborn mailing will be amended to encourage the subsequent 6 month, 9 month, 12 month, 15 month visits for those who completed less than 4 visits by 6 months of age. Additionally, DHMP will assess the availability of resources required to provide individual outreach to members and remind them of the recommended visits on an ongoing basis. 19 Page
20 Healthy Heroes Birthday Cards for DHMP/CHP+ In an effort to reach all age groups, we developed an around the world birthday card using our Healthy Heroes Program Logo. Healthy Heroes provides educational materials/health tips for enrolled children 3 to12 years of age. In addition, birthday cards remind children to come in for their annual well visit. The birthday cards are sent monthly to children ages 1 through 19. The 2012 results note a slight decrease in the average number of visits completed within 2 months of the mailing. This could also be attributed to the fact that CHP+ data is no longer incorporated into this average. For 2013, the average monthly mailing rate increased slightly per month. Among those, there was an average visit rate within 2 months of receiving the mailing of 25.2%. This surpasses our goal of 23% for Additionally, we had an overall visit goal of 56%. Of those who received the mailing, 61.1% total completed a well-child visit during the measurement year. For 2014, we expect no additional increases in well-child visits specific to this mailing. Year Avg. DHMP Postcards Mailed/Month Avg. Visit Rate within in 2 months of Mailing Visit at all During Measurement year % N/A % N/A 2012 * % N/A % 61.1% *For 2012, CHP+, another line of business for Denver Health which was combined with DHMP, was separated out of this report into its own standing report. In 2013, the QI team conducted an evaluation of the annual birthday cards divided out by line of business against a baseline historical rate from 2008 to determine if there was a significant change in the number of children coming in for their annual visit within 2 months of their birthday and coming in at all when comparing the control from 2008 and the intervention group from This overall evaluation was conducted to determine mailer effectiveness with promoting an increase in well-child visits through targeted mailings. Plan A Well Child Visit within 2 Well Child Visit at All During Months of Birthday Year 2008 (Baseline) 16.7% 60.0% % 65.0% POS Well Child Visit within 2 Well Child Visit at All During Months of Birthday Year 2008 (Baseline) 6.0% 23.6% % 23.6% With a p-value less than , the proportion of members that came in for a well-child visit within 2 months of their birthday is significantly higher in 2012 for members enrolled in Plan A. With a p-value of 0.001, the proportion of members that came in for a well-child visit at any time during the measurement year is significantly higher in 2012 for Plan A. For those members enrolled in the Point-of- Service plan, a p-value of indicated the proportion of members that came in for a well-child visit within 2 months of their birthday is not significantly different between 2008 and With a p-value of , the proportion of members that came in for a well-child visit at any time during the measurement 20 Page
21 year is not significantly different between 2008 and The mailings were found to be effective with improving members receiving well-child visits within 2 months of their birthday month and improving the well-child visit rate at all during the year for the Plan A population, but not the POS population Interventions QI team will amend the Healthy Heroes Birthday cards in 2014 to include a checklist of developmental topics the provider will cover in the well-child visit as a way of engaging the member to participate in care. We will continue to track the mailing but do not expect to see an increase in well-child visit rates attributed directly to this mailing. Preventive Cancer Screenings 2012 HEDIS Cancer Screening Indicator Results Commercial Cancer Screenings Indicators 2011 HEDIS Results 2012 HEDIS Results 2013 HEDIS Results HEDIS th Percentile Breast (42-69 y/o) 60.64% 61.36% 58.00% 78.43% Cervical (21-64y/o) 72.51% 71.59% 69.87% 81.25% Colorectal (50-80 y/o) 49.15% 46.72% 48.42% 73.86% HEDIS 2013 Changes There were no changes made during measurement year Commercial Summary of 2013 HEDIS Preventive Cancer Screening Results There was no statistically significant change in colorectal cancer screening rates between 2012 and 2013 at the p=.05 level. However, QI did note a non-significant increase during the measurement period. Also, the Quality team noted a non-significant rate decrease for breast cancer and cervical cancer screening Preventive Cancer QI Activities/Interventions Preventive Cancer Screening Workgroup: QI collaborated with the cancer screening work group that meets monthly to improve colorectal, breast and cervical cancer screenings. We continued to work on: Standardized Health Care Partner (HCP) check-in process to include identifying patients lacking breast, cervical, or colorectal cancer screenings. o HCPs schedule member for an appointment if possible and alert the provider to the tests needed. o Fecal Occult Blood Test (FOBT) kits to be given out at each visit to patients needing colorectal cancer screenings. Patient education materials about each cancer and the importance of screenings. Developed cancer metrics and implementation of registries to report screening rates on a quarterly basis to clinics. 21 Page
22 Asthma 2013 HEDIS Asthma Indicator Results Use of Appropriate Medications for People with Asthma 2011 HEDIS Results DHMP Commercial HEDIS HEDIS Results Results 2013HEDIS 90th percentile Ages 5-11 *NA *NA *NA *NA Ages N/A *NA *NA *NA Ages 12-50* retired 83.67% N/A N/A *NA Ages N/A 89.06% 82.61% 91.71% Ages N/A % 90.91% 95.16% Total 85.71% 95.04% 88.81% 93.93% *NA = Sample size <30 HEDIS 2013 Changes The groups were redefined in measurement year 2011as noted above. There were no changes made during measurement year Summary of 2013 HEDIS Asthma Results The Quality Department noted no statistically significant change for ages and ages When compared to 2013 benchmarks, DHMP rates falls well below the 90 th percentile for each age group Interventions Interventions for Asthma will be assessed in 2013 for potential interventions in Behavioral Health Take Control Program Overview The Denver Health Medical Plan Take Control disease management program aims to improve the quality of care and disease outcomes for the Denver Health Medical Plan members living with diabetes and/or depression. The program uses a multi-faceted approach to help members better manage these chronic conditions. An assessment of member needs, ongoing care monitoring, evaluation, and tailored interventions are utilized to help prevent and/or minimize the effects of the member s conditions. Through a multidisciplinary approach to care coordination and continuity of care for DHMP highest risk members, as well as self-management support for all of members to empower them to assume greater responsibility of their health, improvement in health outcomes and a reduction in costs should be realized. For a full description of the program, please refer to Attachment E. Take Control Analysis Quantitative Analysis: In total, 785 members were identified as eligible to participate in our Take Control Disease Management program for depression and of those 696 (89%) were determined to be low risk, 69 (9%) were medium risk, 15 (2%) were high risk and 5 (.6%) were determined to be critical risk. Of the 332 members identified as eligible for the Take Control Disease Management program for diabetes, 250 (75%) were determined to be low risk, 53 (16%) were medium risk, 20 (6%) were high risk, and 9 (3%) were determined to be critical risk. The majority of members were identified through the pharmacy and 22 Page
23 claims data with the HRA identifying the next largest subset of members followed by lab data. The UM and case management process as well as direct referrals either from internal staff or from the provider, member or caregiver all yielded low rates of member identification. Of the 785 members identified for the Take Control of Your Depression program, only 2 (.25%) actively participated. Similarly, of the 332 eligible members identified for the Take Control of Your Diabetes program, only 9 (.27%) actively participated. Combined, approximately 1% of commercial membership was active in the disease management program between March 1, 2013 and October 31, During this review period, March 1, 2013 through October 31, 2013, there were no member complaints or inquiries related to the Take Control Disease Management program. Behavior Health s (BH) performance on the audited HEDIS results related to the Effective Acute Phase Treatment for depression falls into the 10 th percentile and 50 th percentile for the Effective Continuation Phase Treatment. For both diabetes measures, HbA1c % Poor control (>9.0%) and HbA1c % Poor control (<8.0%), DHMP, Inc. falls into the 10 th percentile. Qualitative Analysis/Barriers/Opportunities for Improvement: Although BH has identified a significant portion of the adult commercial membership who is eligible to receive disease management services, BH has identified relatively low numbers through the UM/CM process and health coaching program as well as by direct provider and member/caregiver referrals. BH knows from experience with other medical management programs that the members who are directly referred often have better engagement and retention rates. A potential barrier could insufficient communication between the health plan and the providers either on direct education of how to refer to the disease management programs or insufficient frequency of reminders about the program. The majority of commercial members are through claims, lab and pharmacy data as well as HRA results. Currently, we have identified more than twice as many depressed members as diabetics, which is consistent with the prevalence rate reported in the literature. The majority of the identified eligible members were determined to be either low or medium risk. Only 2.6% of the members with depression fell into the high or critical categories and for the diabetic members, 9% were determined to be at high or critical risk. The subset of members identified as critical risk was very small and was equal to 14 members in total between both programs. Therefore, future efforts to engage members in the Take Control Disease Management could focus on outreach calls to the high risk group in addition to the critical risk group without requiring significant additional resources. Active participation in the Take Control disease management programs was quite low with only a total of approximately 1% of our commercial membership having been enrolled in either the depression or diabetes disease management programs between March 1, 2013 and October 31, However, given the current staffing model and limited resources, this level of participation is actually expected. Of the 10 members who completed all but the last question of the Satisfaction Survey, the majority rated all items either a 4 or 5. Only 7 of the 10 members answered the last question (for reasons unknown to us) but 100% reported being overall satisfied with the program. Two (2) members provided the following additional comments: I appreciate all of the help the Health Coach was able to give and I am very pleased with the program. This is an excellent program. 23 Page
24 There is significant room for improvement in all related depression and diabetes HEDIS measures and this remains as a high priority for the health plan as a whole. The Take Control Disease Management programs will continue to focus its efforts on the members at highest risk in an attempt to help improve these results. Proposed Actions to Address Identified Opportunities for Improvement: Based on our experience with other programs in the Behavioral Health and Wellness department, members who are directly referred tend to be the most engaged. Therefore, we plan to focus on increasing identification of members for the Take Control Disease Management programs through direct referral. This may include increasing the number of s sent to providers to solicit direct referrals as well as outreach to them through telephonic and/or other technology-based programming. Denver Health Medical Plan, Inc. hosts an online wellness program where members can access general health and wellness information and also find information and resources related to specific health conditions. We plan to update this portal to include a section devoted to the Take Control Disease Management programs which will allow us to elicit more direct referrals to the program. The program s introductory letter, flyer and pre-evaluation surveys will be uploaded and as members navigate the portal, they can click on the disease management tab and complete and mail the pre-evaluation back to us, or call the telephone number listed on the form to complete the pre-evaluation over the phone. Members enrolled in the DM programs are eligible to receive various incentives for participating in the program as well as for achieving significant health improvements during the course of their engagement in the program (i.e., decrease in A1C, decrease in BMI, increase in physical activity, decrease in tobacco use, etc). Currently, the system does not allow for easy analysis of the results and thus makes it difficult for clinicians to easily determine which members are eligible for incentives based on clinical outcomes. We are in the process of reviewing the current evaluation tools and process in our GuidingCare system to ensure it captures the information necessary to accurately determine clinical improvements based on member feedback. The incentives currently being provided may not be enticing enough for our members to stay motivated and to remain in the program as our retention rates are much lower than the initial engagement rates. We plan to further explore why members drop-out and whether greater incentives would lead to longer engagement in the program. Moreover, we need to better understand what interventions, for which population specifically, are helpful in improving the members understanding and management of their disease. We also plan to coordinate the mailings that are sent to the members with the dates that the education classes are being offered to increase the likelihood that interested members will be able to participate in that intervention if they select that option. Currently, members may request this type of intervention but remain on a waiting list for several months until the next class is scheduled to occur. Two areas in particular from the Disease Management Satisfaction Survey were found to have room for improvement such that <90% of members rated either a 4 or 5 on those specific questions. The first was related to the helpfulness of the Health Coach in improving the members health and the second was related to the helpfulness of the Health Coach in helping the member access services to get the care he/she needs. The results of the Satisfaction Survey are shared with staff in order to raise awareness of their strengths and weaknesses. Ongoing training and discussion will occur at team meetings and, if necessary, we will implement changes to the structure of the program as appropriate based on the survey results. 24 Page
25 Complex Case Management DHMP s Complex Case Management (CCM) Program has been designed to support the mission of DHMP by enhancing the quality of patient management and satisfaction, to promote continuity of care and cost effectiveness through the integrating and functions of case management. The CCM program is available to any individual enrolled into any of the Denver Health Medical Plan insurances plans. The CCM program provides intensive, personalized case management services and goal-setting for members who have complex medical needs and require a wide variety of resources to manage health and improve quality of life. Services are provided in a collaborative process that assess, plan, implement, coordinate, monitor and evaluate the options and services required to meet an individual s health needs, using communication and available resources to promote quality, cost-effective outcomes. In reviewing data from October 1, 2012 to September 30, 2013, the CCM program found areas of improvement to the CCM process that would improve coordination of care and services to members. Updates and/or changes to the CCM program and process include but are not limited to the following: Revise and expand program criteria for inclusion to include more clinical diagnoses and conditions (e.g. cancers, diabetes, trauma, complex medical conditions) Incorporate the use of predictive analytic reports from Guiding Care to increase program enrollment, including Commercial members Improve outreach to providers to increase direct referrals to the CCM program (e.g. s, newsletters, clinic presentations) Implement a new process to incorporate Nurse Advice Line data to ensure member needs are being met following contact with health information line Incorporate clinically based goals into the ongoing case management process, including staff training to improve clinical knowledge and understanding of conditions and use of those goals in the selfmanagement action plan (SMAP) Incorporate use of patient education materials into ongoing case management process to reinforce clinical education and teaching Update Initial Comprehensive Assessment to include questions that will identify and address available community resources for all lines of business, including commercial Expand the current process to address readmission rates, including implementation of a post-discharge call within 72 hours for all lines of business Provide transition letters to members of all lines of business who are admitted to inpatient hospital setting to identify those who may benefit from CCM services Update Effectiveness Review script to include evaluation of the self-management tool (SMAP At least annually, Member Satisfaction and Evaluation will be evaluated by the CCM program. The evaluation process includes, but is not limited to the following: CCM Satisfaction Survey results (member satisfaction) 25 Page
26 Member/Provider complaints The Case Management Leadership team will review the results of the program evaluation and determine appropriate interventions to address opportunities for improvement, if applicable. The team will consider both qualitative and quantitative data to identify patterns in feedback. Feedback will be specific to the complex case management program and services. (Attachment A, Attachment B) IV. Safety and Quality of Clinical Care Quality of Care Concerns All of the cases were reviewed by the DHMP Medical Director and forwarded to the appropriate physician panel of expert experts for review. All substantiated QOCC s a corrective action plan is implemented. DHMP Commercial 2013 Quality of Care Concerns (QOCCs) DHMP Plan A/ POS/CSA Q1 (Jan-Mar) Q2 (Apr-Jun) Q3 (Jul-Sep) Q4 (Oct-Dec) Total 2013 Unsubstantiated Borderline Substantiated TOTAL DHMP Analysis: Ten potential QOCCs were identified in 2013; down from the number of potential QOCCs reported last year (in 2012). Two of the ten were found to be substantiated quality of care concerns based on case review for DHMP Commercial QOCC Five Year Comparison Health Plan Denver Health Medical Plan, Inc. (DHMP) * *2013 data includes the CSA Line of Business (LOB). Prior years just include only Plan A & POS, as there were no noted QOCCs for the CSA Line of Business for years prior. In 2013 there were a total of two QOCCs for the CSA LOB. 26 Page
27 Credentialing and Provider Networks DHHA Providers The DHHA Medical Staff Office is responsible for the credentialing activities of all DHHA practitioners; following both Joint Commission and NCQA standards and guidelines. DHMP has a delegated credentialing agreement with DHHA, Cofinity network, University Hospital, Children s Hospital, Columbine Chiropractic and Take Care Clinics network that clearly defines the responsibilities of each entity. Non Denver Health providers are credentialed by the Cofinity and in some cases by University Hospital. All credentialing entities follow front Joint Commission and NCQA requirements. DHMP is responsible for the oversight of credentialing activities that includes reviewing monthly reports as specified by the delegation agreement and conducting an annual credentialing delegation site audit according to NCQA standards. In addition, DHMP credentials a number of providers and practitioners that are not part of these networks. DHHA Provider Network Physicians Allied Health Practitioners Behavioral Health Total Additions Resignations Total PCP s DHMP PCP s panel is made up of Primary Care Providers from the specialties of Family Medicine, Internal Medicine, Geriatrics, and Pediatrics. DHMP utilizes physicians, nurse practitioners, and physician assistants as PCP s. DHHA PCP's FM IM Geriatrics Ped Totals 2013 Additions Left DHHA or changed status Totals Physicians NPs PA's Grand Total *Two DHMP physicians practice in both FM and Geriatrics. Independent Network Providers DHMP maintains a panel of Independent Direct Network Providers (IDNP) consisting of non-dhha providers from various specialties. The DHMP Director of Contracting is responsible for maintaining an adequate provider network. All credentialing activities for IDNPs are conducted by the DHMP credentialing designee. DHMP follows the most current NCQA standards and regulatory requirements from the Centers for Medicare and Medicaid (CMS) & the Division of Insurance (DOI). 27 Page
28 IDNP Pediatric Speech Pediatric Optometrists Podiatrists Network Ophthalmologists Pathologists Pulmonologists Additions Resignations Total = Delegated Provider Networks: DHMP has credentialing delegation agreements with Columbine Health Plan, University Physicians Inc.(UPI) and Cofinity. DHMP Delegated Provider Networks Columbine Health Plan UPI Cofinity Delta Dental 173 Chiropractors 1914 Providers Providers 2037 Providers Results of DHMP 2013 Annual Credentialing Delegation Audits 2013 Credentialing Delegation audits were conducted for: DHHA, Columbine Health Plan, and University Physicians Inc. (UPI). DHHA scored 98%, Columbine scored 97%, and UPI scored 96% with minor deficiencies on their audits. Delta Dental scored 70% with several areas requiring corrective action and a follow-up review in 6 months. Organizational Providers DHMP follows NCQA guidelines and the State of Colorado regulatory requirements for the assessment process to credential organizational providers. According to NCQA the following types of organizational provider must be assessed: hospitals, skilled nursing facilities, home health agencies, behavioral health facilities providing mental health or substance abuse services, dialysis treatment centers, hospice/long term care centers, and home infusion. The assessment/credentialing activities for organizational providers is conducted by the DHMP credentialing designee; files are reviewed and approved by the DHMP Credentialing Committee and/or the DHMP Medical Director before a contract is executed. Ongoing monitoring is conducted monthly with a formal reassessment every three years. Refer to DHMP policy and procedure titled Assessment of Organizational Providers. Organizational Providers Adds Terms Total in Network Hospital Home Health Agencies Skilled Nursing Facilities Hospice/Long Term Care Page
29 Centers Behavioral Health Facilities Renal Dialysis Centers Home Infusion Totals Continuity and Coordination of Care Denver Health Medical Plan, Inc. (DHMP) recognizes that providing continuity and coordination of medical care and providing continuity and coordination between medical care and behavioral health care is challenging in today s health care environment. At least annually, DHMP surveys its contracted providers to identify opportunities to improve continuity and coordination of care across the health care network. Baseline: 2013 is the first time DHMP has surveyed providers related to Continuity and Coordination of Care, so there is no previous data for comparison to identify improvement or decline in performance over the past year. Goals: The goals for the survey questions are that at least 75% of the responding providers would be at least somewhat satisfied (score of 4 or 5) with the timeliness and completeness of the information received from all of the various settings. Results: The Continuity and Coordination of Medical Care survey was mailed to 759 providers with 198 providers completed the survey a return rate of 26%. The table and chart below shows the breakdown of the responding providers, by specialty type DHMP Provider Satisfaction Survey Q. 1. Which type of provider are you? Answer Options Response Count Response Percent PCP 75 38% Medical Specialist 49 25% Surgical Specialist 25 13% Behavioral Health Provider 9 5% Other 39 20% Total % DHMP did not reach the 75% satisfaction goal for any of the aspects of information exchange or the timeliness or completeness of information received from the various settings. There are numerous opportunities for improvement will be presented to the QMC and proposed actions to take will be implemented in For the full reports, please refer to attachments. (Attachment C, Attachment D) V. Quality of Service 2013 Member Satisfaction (CAHPS) Annual CAHPS Audits 29 Page
30 DHMP conducted an Adult Consumer Assessment of Health Plan Providers and Systems (CAHPS) surveys in 2013 using Morpace, an NCQA certified vendor. Morpace follows NCQA protocols and statistically appropriate methodologies to determine member satisfaction scores. The subsequent tables are the three point mean scores between 2011 and NCQA uses a three point mean as part of the NCQA accreditation process. Annual CAHPS results are compared to the National Medicaid NCQA Accreditation Scoring system using the following percentile rankings: 90th, 75th, 50th, and 25th. NCQA does not take into account regional thresholds since regional variation in these variables are not substantial. Background CAHPS measures health care consumers' satisfaction with the quality of care and customer service provided by their health plan. Denver Health Medical Plan chose the mixed mail/telephone protocol. This protocol included mailing a questionnaire with a cover letter, followed by a thank you/reminder postcard. For those selected members who did not respond to the first questionnaire, a second questionnaire with a cover letter encouraging participation was sent which was also followed by a reminder postcard. If a selected member still did not respond to the questionnaire, at least four telephone calls were made to complete the survey using trained telephone interviewers. NCQA originally designed this protocol with the goal of achieving a total response rate of at least fifty-five percent (55%). The average of response rates for all plans reporting to NCQA has been trending downward since a high in 2000 of 51% to low of 30% in In February, 1430 Denver Health Medical Plan members were randomly selected to participate in the 2013 CAHPS Adult Commercial Survey. The results below compiled from the responses of the 439 Denver Health Medical Plan members who responded to the survey (31% response rate). The table below has our member satisfaction score compared to the NCQA Quality Compass benchmark. The benchmark is based on aggregating the results of all commercial plans who submit results to NCQA and establishing the thresholds. The gold standard is the 90 th percentile. Analysis: DHMP reached the CAHPS 90 th percentile in HEDIS measures for Flu Shots (Ages 50-64) question number Q45. Most measures were at or below the 10 th percentile that means 90% of commercial plans are above this score. DHMP has many opportunities for improvement based on these results. Access and availability to primary and specialty care is a barrier that was identified in 2011 and remains consistent in This year we noted an increase in satisfaction with; how well doctors communication and Rating of Health Plan. (See quality compass comparison chart below) 30 Page
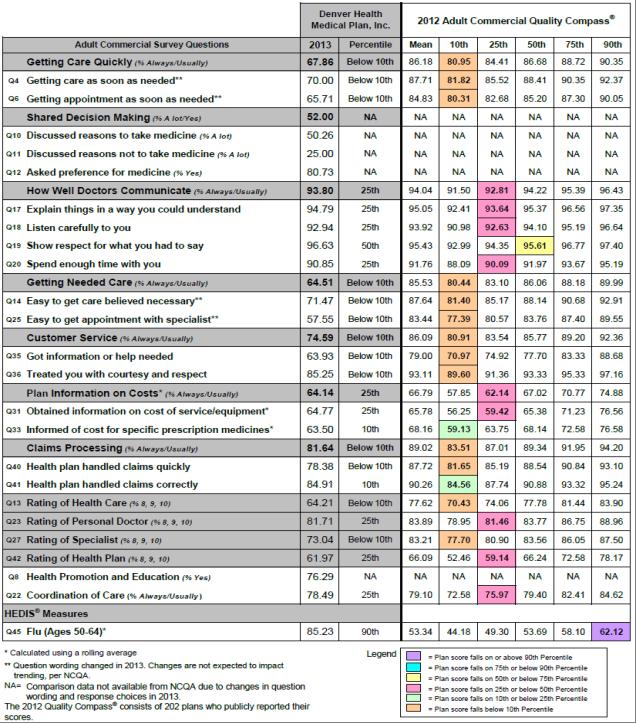
31 31 Page
32 2014 Interventions DHMP is addressing access and availability through the quarterly Access meetings. This group was started in January of 2011 and keeps minutes. The members of the committee are key leaders within DHMP and DHHA CAHPS results were presented to this committee and QMC for evaluation, discussion and recommendations, as appropriate. As a result of these discussions, process improvement objectives are in place. DHMP Secret Shopper activity will continue in 2014 to evaluate the appointment making process within the CHS clinics, pharmacy, and the Specialty Appointment clinics. The scope of Secret Shopper will expand to include our extended network facilities. To improve member satisfaction the QI staff has employed strategies to increase CAHPS and HEDIS scores when there is appropriate correlations. To improve CAHPS member satisfaction and HEDIS measure rates for annual well visits for adults and children, some clinics will be holding clinical hours on Saturdays. Provider education training on CAHPS and HEDIS will be developed around gaps in knowledge. Denver Health has hired additional primary care providers in 2013 and will do so in 2014 to help alleviate the access issues and waiting times for appointments and lean processes are being implemented to increase work efficiency in Grievance Reporting and Trending Category 1Q2013 2Q2013 3Q2013 4Q TOTAL Access Quality of Service /Customer Service Billing/Financial Benefit Package Clinical Care Rights/Legal GRAND TOTAL OF COMPLAINTS DURING REPORT PERIOD 129 DHMP gathers information (both positive and negative) from members by tracking grievances filed by members and/or their authorized representatives. Efforts are spent on analyzing not only the timeliness of the problem resolution process, whether regulatory requirements are met, whether member notification of a resolution is provided in an easy to understand and culturally competent manner, determining the root cause, but also on identifying patterns of grievances which may suggest the need for further investigation and/or performance improvement opportunities by DHMP and/or its affiliate entities and providers. 32 Page
33 Data substantiates more significant area of concern lies in the Access category. Further analysis indicates a number of members were not able to obtain an appointment in a timely manner. Members are required to schedule appointments through the Denver Health Medical Center Main Appointment Scheduling Department. To address this issue, staff in the Managed Care Grievance and Appeal Department has direct access to the Main Appointment Scheduling System. Staff can schedule primary care appointments for members. For specialty care appointments, staff developed collaborative working relationships with the practice managers over time. Inquiries for new member appointments are given priority. The second area of concern lies in the Clinical Care category. The majority of complaints within this category deal with the coordination and/or continuity of care. We receive new members from other insurance companies that may be currently receiving treatment from other medical providers that are not participating with Denver Health. In order to receive services, a member must use providers that are participating in the Denver Health provider network. When a member enrolls into our plan, we do not know at the time of enrollment if the member is currently seeking services at Denver Health or at another hospital or medical practice. To alleviate and address this issue, we have deployed patient navigators that reach out to new members, assist them in completing a health risk assessment, and authorizing any services that the new member is currently receiving from another medical provider. The patient navigator also helps in the transition of the new member to medical providers within the Denver Health network. The third area of concern is in the Quality of Service/Customer Service category. The bulk of the complaints stemmed from members experiencing discourteous and/or rude behavior from clinical and administrative staff. When this occurs, the Managed Care Grievance and Appeal Department inquires directly with the physician and/or practice manager where the complaint originated. We provide education to clinical and administrative staff about the need to provide good customer service to all of our members. Lastly, all complaint data is reviewed and discussed at the Quality Management Committee (QMC) on a quarterly basis. Accessing member understanding of DHMP Procedures The Marketing Department has a systematic and ongoing process for assessing new member understanding of DHMP key policies and procedures. Safety of Clinical Care Privacy and Confidentiality Monitoring In the course of providing quality assurance and utilization management services, the Company receives confidential information from members and from providers. In accordance with state and federal laws, the Company will receive and retain such information subject to the following conditions: At the time of initial hiring, all Company personnel shall be informed of confidentiality and the disciplinary action that will result from breach of confidentiality. At the time of hire, all staff shall sign and acknowledge understanding of the Denver Health and Hospital Authority Confidentiality Agreement on an annual basis. The Company shall treat all information as confidential to the extent that such information specifically identifies or permits identification of a certain health plan member and describes the physical, emotional, or mental conditions of such person, provided; 33 Page
34 however, that the Company may retain and use for its purposes in performance of its obligations any information it obtains relating to costs, charges, procedures, used or treatments employed by a provider in treating any member, to the extent such information does not disclose the identity of the person. Confidential information obtained in the process of performing utilization management services will be used solely for utilization and quality management and will be shared only with parties who are authorized to receive it. Any confidential information, which The Company finds it necessary to disclose, in the performance of utilization management services, shall not be disclosed to any unauthorized entity without prior consent of the member or as required by the federal law. All confidential information retained by the Company shall be held in secured and locked files or rooms. The Company in accordance with applicable State of Colorado and federal laws shall remain confidential information. In the course of performing its utilization management responsibility, it is the policy of the Company Medical Management Department not to record telephone conversations. In the event of a Conflict of Interest: No person may participate in the review, evaluation, or final disposition of any case in which he/she has been professionally involved or where judgment may be compromised. All Company employees, members of committees not employed by the organization and the board of directors are required to review and sign the Conflict of Interest statement annually. Member Services Monitoring Member Services Telephonic Performance Member Services has in place a departmental Performance Report that monitors four telephonic statistics categories to ensure that industry standards are met, specifically: Service Level at or above 85%, Average Delay of 30 seconds or less, Abandonment Rate of 5% or less, and overall Call Volume. The Member Services Performance Report monitors these telephonic statistics by each individual Denver Health Medical Plan (DHMP) and Denver Health Hospital Authority (DHHA) line of business. Tracking, comparison, and evaluation occur on a monthly as well as annual basis. The Member Services Administrative Coordinator (MSAC) pulls all telephonic statistical data from the Cisco Telephony System reporting system Cisco Unified CXX Historical Reports and prepares the report for the Director of Member Services. The Director of Member Services reviews each report and then provides a summary of monthly activity as well as an analysis of any trends in data, call volume, reason codes, deficiencies, etc. The Director presents the Performance Report as well as his or her Summary and Analysis at each quarterly Quality Management Committee meeting. For 2013, all above stated goals and standards were met and maintained. Monitoring Member Services Benefit Info for Quality and Accuracy In order to satisfy regulatory standards and monitor the telephonic quality of DHMP Member Services, the Member Services Quality Assurance Program has been instituted reporting occurring on a monthly basis. The MS QA Program allows the Member Services Leadership Team (MSLT) to determine any deficiencies in quality and service provided by the Member Services Representatives (MSRs) as well as work to correct any identified deficiencies. The QA Program serves as a valuable tool in staff development and satisfaction and is also incorporated into the annual MSR evaluation process to ensure that it is meaningful to the team and its individual members. The QA program entails monitoring and reporting on two components, telephonic productivity and performance as well as quality and accuracy of benefit information provided. Productivity is evaluated on specific metrics from the Cisco Telephony System, specifically Inbound Call Volume, Average Talk Time, Not Ready Time, and Reserved Time. The quality component of the QA Program is evaluated by direct call monitoring and evaluation by the MS Supervisor. The MS Supervisor selects 10 random calls for each MSR that occurred in the specific month out of the Call Copy Call Recording Software. The MS Supervisor will evaluate the call for the quality and accuracy of the information provided based upon 34 Page
35 various criteria (member information confirmation, identifying issues, knowledge of benefits, documenting the call, tone of voice, etc.) and scores the MSR on a sliding scale dependent upon the accuracy of the information given. The overall evaluation of MSR performance in both areas is compiled, reviewed, and provided to the MSRs on a monthly basis. One on one coaching will occur if deemed necessary. In addition, an overall departmental MS Monthly Call Quality Performance Report is compiled to track the progress of quality maintained by the MSRs from month to month on an individual as well as departmental basis. All MSRs and the department overall must maintain an accuracy rate of 85% or higher. If this is not maintained, corrective actions are taken. The MSR Quality Assurance Program was implemented beginning in December of All data will become available in January of The DHMP Member Portal audit portion of the QA Program includes monthly internal auditing conducted by the Member Services Administrative Coordinator (MSAC) to test Member Portal functionality and monitor the quality of information provided online to members. The MSAC will evaluate the quality of benefit information posted on the Member Portal on a sliding scale based upon the functionality and quality. All information available on the DHMP Member Portal must maintain 85% accuracy as well as functionality. This portion of the QA Program allows the MSLT to analyze causes of deficiencies, identify opportunities for improvement, and if needed, initiate Corrective Action Plans for specified deficient areas. The Director of Member Services includes his or her Summary and Analysis on this report at each quarterly Quality Management Committee meeting. The DHMP Member Portal Quality Assurance Program will commence once the DHMP Member Portal is online and functional. Monitoring the Nurse Advice Line The primary intent of the Member Services Nurse Advice Line Performance Monitoring Program is to track member usage of the provided services and to identify opportunities and establish priorities for improvement. DHMP Member Services receives a monthly Performance Report from the Nurse Advice Line Leadership Team that includes Nurse Advice Line phone metrics such as Service Level, Average Delay, Abandonment Rate, and Call Volume for various DHMP and DHHA lines of business. The Nurse Advice Line is held to the same industry standards as DHMP Member Services, specifically: Service Level at or above 85%, Average Delay of 30 seconds or less, and Abandonment Rate of 5%. The Nurse Advice Line Performance Report also includes data on call triage and various member utilization. In addition to monitoring the quality and productivity of the Nurse Advice Line, DHMP Member Services also completes an annual member satisfaction survey call completed by MSRs. This member feedback is recorded and provided directly to the Nurse Advice Line Leadership Team. The Director of Member Services provides the Nurse Advice Line with feedback regarding the reported metrics on a monthly basis after reviewing and analyzing the data provided to him/her. This analysis is intended to be internalized by the Nurse Advice Line Leadership Team in order to help maintain high quality standards and member satisfaction. The Director of Member presents the Nurse Advice Line Monthly Performance Report at each quarterly Quality Management Committee meeting. For 2013, all above stated goals and standards were met and maintained. For a full report, please refer to Attachment F. VI. Overall Structure of the QI Program The following Company personnel are actively involved in implementing specific aspects of the QI Program and delegating daily operational activities as needed: Medical Director, Clinical Director of Behavioral Health and Wellness Services, and Director of Utilization Management. 1. Medical Director responsibilities include, but are not limited to: 35 Page
36 Providing direction, support and oversight related to the development, implementation, and evaluation of all clinical activities of the QI department. Working in collaboration with the QI Director and the QI Intervention Managers on development and assessment of clinical interventions. Reporting findings from clinical interventions to the appropriate groups, such as the Ambulatory Quality Improvement Committee (AQIC), Quality Management Committee (QMC), and the Company Board of Directors. Working with the QI Director on preparation and dissemination of relevant information obtained on the performance of QI activities to the QMC, Operations Management Committee, AQIC, and the Company Board of Directors. Designing and implementing clinical activities in the QI Work Plan. Delegating components of the QI Work Plan to other members of the Operations Management Committee. Serving on the QMC, AQIC, Pharmacy and Therapeutics Committee (P&T), Utilization Management Committee, Credentialing Committee, Operations Management Committee, and Denver Health Physician Executive Committee. Evaluating and managing the Company s Quality of Care Concerns (QOCCs) related to physical health problems, working in conjunction with the QI RN. Overseeing all of the Company s clinical and preventive health guidelines. 2. Clinical Director of Behavioral Health and Wellness Services responsibilities include, but are not limited to: Serving on the QMC. Assisting with the development, revision, and/or implementation of the behavioral health aspects of the QI Program including the behavioral health clinical and preventive health guidelines. Collaborating with QI to review behavioral health programs and services offered by network providers to ensure adequate access to meet member needs. Reviewing behavioral health cases for appropriateness, especially related to level of care. Evaluating the Company s QOCCs related to behavioral health problems, working in conjunction with the QI RN. The Company s Quality Improvement Department 1. Quality Improvement Director responsibilities include, but are not limited to: Developing, managing, and monitoring the QI Program. Acting as staff representative to the Company s Board of Directors. Directly assuming authority and responsibility for the organization and administration of the QI Program, including annual submission of the QI Program Description, Evaluation, Work Plan and Network Adequacy Report. Coordinating, providing advice, and participating in the execution of the QI Program through collaboration with other Company and Denver Health Departments as appropriate for regulatory compliance. 36 Page
37 Reporting QOCCs to the appropriate Directors of Service at Denver Health Hospital and Authority and external network providers. Serving as Chairperson for the QMC, including determining the composition of the QMC. Directing and working with Company administrative personnel to ensure efficient recruitment of QMC membership recruitment, meeting coordination, and minute-recording. Participating in DHHA Patient Safety Committee. Annually updating policies, procedures, and guidelines related to the QI Department. Providing oversight and direction to the QI team. 2. HEDIS Program Manager responsibilities include, but are not limited to: Managing all aspects of HEDIS-related projects. Evaluating and analyzing HEDIS results. Providing recommendations to QI Director for cost efficiency, process improvements, and quality interventions. Working collaboratively with Intervention Managers on process improvements and interventions related to HEDIS. Validating the accuracy of HEDIS data. 3. Clinical Project Manager responsibilities include, but are not limited to: Managing all aspects of CAHPS-related projects. Evaluating and analyzing CAHPS results. Providing recommendations to QI Director for cost efficiency, process improvements, and quality interventions. Working collaboratively with Intervention Managers on process improvements and interventions related to CAHPS. Oversight of QI vendor contracts and delegated activities. Leading project planning activities related to regulatory and accreditation requirements. 4. QI Project Specialist responsibilities include, but are not limited to: Working in collaboration with the Statistical Research Specialist to pull data used to develop member lists for outreach projects. Analyzing the effectiveness of intervention activities. Collaborating with the Clinical Project Manager on activities related to regulatory and accreditation requirements. 5. Adult and Pediatric Intervention Managers responsibilities include, but are not limited to: Developing, managing, and evaluating all quality interventions 37 Page
38 Working collaboratively with the Medical Director, QI Director, AQCI subcommittee condition-specific work groups, HEDIS Program Manager, Clinical Project Manager, QI Project Specialist, and Statistical Research Specialist. 6. Medical Compliance Specialist responsibilities include, but are not limited to: Credentialing and re-credentialing providers for the Company. Annually reviewing and updating credentialing policies and procedures. Assisting with network adequacy reports, access plans, and other reports as needed. Managing delegation agreements and performing yearly credentialing delegation audits. 7. Statistical Research Specialist responsibilities include, but are not limited to: Pulling data from various sources to support QI program activities. Supporting staff with obtaining reports and data analysis from various systems. Assisting with interventions or special projects related to contractual requirements. Assisting with collection and interpretation of HEDIS data. 8. QI RN responsibilities include, but are not limited to: Managing QOCCs and quality of service concerns process in a timely and effective matter. Working in collaboration with HEDIS Program Manager to perform HEDIS chart review. Developing training materials, facilitating training, testing for inter-rater reliability (IRR), retraining for staff. Facilitating the HEDIS medical record audit with auditor. Providing clinical consultation for the QI team. Conducting practitioner chart review using HEDIS criteria. Overseeing multicultural health care-related activities including cultural competency training, cultural and linguistic appropriate services, and identification of any health disparities. Developing and updating all preventive and clinical guidelines. Committee Structure The Quality Management Committee (QMC) acts to plan and coordinate organization-wide improvements in quality and safety of clinical care and service to members. The QMC is charged with responsibility for oversight of all quality-related Company Medical Management activities and processes, including but not limited to: Utilization Management, Case Management, Behavioral Health and Wellness, Pharmacy, Member Services, and Provider Relations. Additionally, the Committee oversees the effectiveness of the HEDIS and CAHPS quality outcomes, QI evaluations and interventions, QOCC evaluations, and patient safety initiatives. The QMC includes primary care providers and specialty providers from both Denver Health Hospital Authority and extended practitioner network 38 Page
39 Summary of Future Outcomes The Company is going through an in-depth review of all its initiatives and intervention activities, using best practices as a guide. All approved activates will have performance measures attached with PDSA embedded into their standard work cycles. Yearly work plans will have measurable goals and/or benchmarks. All interventions that do not meet performance targets will undergo a barrier analysis and/or RCA. The Company seeks to improve member education, health literacy, and access to care and services. VII. QI Activities Summary 2013 QI activities focused on diabetes, prenatal/postpartum care, behavioral health, and preventive health measures for both children and adults. QI team members collaborated with CHS through various work groups in diabetes, weight management, children s preventive health, and preventive cancer screening. We worked with school-based health centers in the Denver Health system to improve the delivery of wellchild care to our commercial members enrolled in Denver Public Schools. Additionally, QI continues to make improvements in obtaining real time data from the warehouse and registries, which is helpful in the many interventions conducted throughout the year. In 2013 the MMC was revamped and will now be referred to as the Quality Management Committee (QMC). Furthermore, the QI Program Description and QI Work Plan were updated in accordance with NCQA standards. The QI Work Plan will have targets listed in accordance with all QI activity listed. When any interventions do not meet there intended targets a barrier analysis or RCA will be performed. All the above mentioned improvement will occur in collaboration with these departments: Utilization/Case Management, Pharmacy, Health and Wellness, and Member Services. VIII. Attachments: Attachment A_CCM_Effectiveness Report 2013.pdf Attachment B_CCM_Satisfaction Report 2013.pdf Attachment C_ Continuity and Coordination of Medical Care.pdf Attachment D_ Continuity and Coordination of BH.pdf Attachment E_Take Control Program Description.pdf Attachment F_Monitoring Member Services.pdf 39 Page
40 Effectiveness Report Complex Case Management Program Plan: All Commercial Plans Report Date: December 11, 2013 Introduction Denver Health Medical Plan Inc. (DHMP) offers several employer group plans including Medical Care HMO, Medical Care Expanded HMO and Point of Service (POS), hereafter called Commercial plans. Complex Case Management is available to all Commercial plan members. Complex Case Management (CCM) is the systematic coordination of care and services provided to members who have experienced a critical event or diagnosis that requires the extensive use of resources and who need help navigating the system to facilitate appropriate delivery of care and services. It involves a comprehensive assessment of the member s condition; determination of available benefits and resources; and development and implementation of a case management plan with prioritized performance goals, monitoring and follow-up. The goal of Complex Case Management is to help members regain optimum health or improved functional capability, in the right setting and in a cost-effective manner. Evaluation of Complex Case Management for Commercial Plans At least annually, DHMP performs an evaluation of the Complex Case Management program. The purpose of the evaluation is to determine the effectiveness the program, identify areas for improvement, and outline interventions for the following year. The plan evaluates the following three measures: 1. Member Self-Management - this is evaluated using the results of the CCM Effectiveness Review. At least quarterly, Complex Case Managers complete a CCM Effectiveness Review script in our Guiding Care system on each CCM member on their caseload. The effectiveness review is intended to capture changes in the member s health and self-management skills as a result of their involvement in the CCM Program. Additionally, a review of the Self-Management Action Plans (SMAP) conducted by complex case managers and saved in member records is conducted in order to determine the effectiveness of this program. SMAPs are self-management goals that the member and CCM are currently working. The CCM and member create the SMAP together, either face-to-face or by phone. The CCM then monitors the SMAP monthly, or as often as required, based on the goal. 1
41 2. Acute Inpatient Readmission Rate for the commercial population. The Complex Case Management program uses a multi-stage assessment process in order to engage members in care throughout their enrollment in the program. This process allows case managers to identify high-risk members and work to reduce acute inpatient readmissions. DHMP will evaluate the readmission rate (all-cause readmissions within 30 days) which is based on claims data provided by the Information Systems department. 3. Satisfaction with CCM Services Complex Case Management (CCM) is available to all DHMP members who have experienced a critical event or diagnosis that requires the extensive use of resources and who need help navigating the system to facilitate appropriate delivery of care and services. While the primary goal of CCM is to improve overall health through patient education and increased self-management, we understand that member satisfaction is vital to member engagement and a successful program. To measure this, Care Support (DHMP Patient Navigator team) conducts CCM Satisfaction surveys on all commercial DHMP members upon completion or closure from the CCM program. The survey asks a variety of questions, but the analysis will primarily be driven by the question, How helpful was your case manager in helping you understand your health better? 2

42 Current Data, Goals and Analysis 1. Member Self Management as measured by the CCM Effectiveness Review Script For the complete CCM Effectiveness results, see Appendix A. Below is the specific question, with responses, for the question related to the improvement in member s self-management. 10/01/ /30/2013 This question in the CCM Effectiveness Review demonstrates the CCM s subjective observation of the member s ability to self-manage various aspects of their health, such as: understanding their condition, navigating the health care system, and monitoring daily diet and medications. In response to our 2012 program evaluation, the Complex Case Management program has also fully implemented a new self-management tool called the Self Management Action Plan (SMAP). The SMAP is completed by the CCM with the member on the phone or in person. The intent is to use the SMAP to encourage member engagement in their plan of care, set actionable and measureable goals, and aid in the development of self-management skills. Below is the portion of the SMAP which addresses what the member will do in order to achieve the goal that they have set. The SMAP also addresses other support systems and a follow-up plan to ensure that the goal is met. See Appendix C for a full copy of the SMAP. 3
43 Goal: At least 75% of commercial members enrolled in Complex Case Management will demonstrate improvement in self-management Quantitative Analysis: During the measurement period of 10/01/ /30/2013 a total of 28 CCM Effectiveness Reviews were completed on members enrolled in Complex Case Management. Since the Plan evaluates members quarterly, these are not necessarily unique members, but rather a periodical summary of ongoing case management. Of the 28 evaluations, only 15 (53.6%) showed an improvement in self management. 5 members with self-management goals showed no improvement and 8 had no self-management goals identified. The 8 members without self-management goals are the most striking statistic. Beginning in 2013 the Complex Case Management program was updated to highly encourage self-management action plans (SMAP) on every enrolled member. Upon further investigation, 3 of the 4 evaluations indicating that there was no SMAP were for the same member and conducted by the same case manager. This member does have a SMAP on file and the record indicates that the Complex Case Manager and member were working toward this goal. Therefore, the 2013 statistics may be an internal training issue rather than an indication of CCM Effectiveness. There were also 5 members (17.8%) that have self-management goals, but made no improvement during the measurement period. Of this group only one member was evaluated twice and three different Complex Case Managers reported that their members were not improving, indicating that there is not a pattern with specific staff. 4
44 Opportunities for Improvement (Qualitative Analysis): Despite the interventions implemented in 2013, it is noted that we fall short of our goal of 75%. As a plan, DHMP needs to establish a process which fosters more member autonomy in navigating the healthcare system and understanding their own health. One opportunity is to improve member understanding of their health. Reviewing the SMAPs, DHMP recognized that the focus has primarily been on navigation of the health system and psychosocial needs rather than condition-specific goals and education. CCMs could be more instrumental in encouraging members to select more clinically focused goals. This will be a focus for improvement interventions this year. Another opportunity for improvement is to analyze the direct impact of the SMAP process. It is not currently attached to a reporting process and therefore difficult to measure. An additional opportunity identified is that there are 8 evaluations that indicate the lack of selfmanagement goals. This is nearly 30% of all evaluations completed during the review period. This is a major target for improvement in Interventions: In order to achieve the goal of 75% of members improving their self-management in 2014, DHMP has implemented two interventions. First, to address the issue of members not understanding their health, CCMs have begun sending targeted patient education materials to members enrolled in Complex Case Management. The CCM follows-up with the member on the materials to reinforce the clinical education and teaching. Second, a specific question has been added to the CCM Effectiveness Review script which specifically addresses whether or not the SMAP has been effective. This will allow the Plan to more accurately measure the success of the Self-Management Action Plan. Evaluation and Re-measurement: This measure will be re-evaluated in November 2014 as a part of the annual evaluation of the Complex Case Management program. We will evaluate reports and review the use of SMAPs and patient education material on individual case files. Results of the re-evaluation will drive interventions for improvement for the following year. 5
45 2. Population-Based Metric Readmission rates for commercial DHMP members The Denver Health Medical Plan Information Systems Department reports an annual readmission rate for all commercial members. This rate is a measure of readmissions within 30 days of discharge from any facility and for any cause. This rate includes acute medical and psychiatric inpatient admissions. Goal: The goal for all-cause readmission rates for commercial DHMP members is 5%. Quantitative Analysis: The all-cause readmission rate for all commerical plans in 2012 was 7%. More specifically, the HMO plan (DMC) readmission rate was 8% and Point of Service (POS) was 3%. There were more than twice as many inpatient cases (488) in the DH Medical group vs. the POS group (228). Overall, the total number of commerical inpatient cases is low compared to others plans. Since the DHMP HMO plan sends all members to Denver Health Medical Center for inpatient stays, it is easier for DHMP to impact the readmission rate for this population. The hospital shares information with DHMP via an electronic document management system (EDM). Therefore, staff at DHMP are notified quickly of inpatient admits and discharges. POS members are able to go to any hospital for inpatient admissions and therefore the plan does not always receive timely notification of these transitions. Opportunities for Improvement (Qualitative Analysis): The quantitative results between the HMO and POS plans are surprising since most HMO members receive inpatient care at Denver Health where medical records are shared via electronic medical records (EDM). This should mean that DHMP is notified within 24 hours of all admits and discharges and therefore be able to reach out for follow-up care quickly. POS members can go to any facility for inpatient care. Not all hospitals notify DHMP of transitions and therefore outreach to members is more difficult to complete in a timely manner. One opportunity for improvement is to reduce readmissions that occur at Denver Health Medical Center. This will mostly impact the HMO Plan, but also any POS member that admits to DHMC. 6


46 Starting with this group will have the highest impact since there are a higher volume of admits at DHMC than out-of-network facilities. Interventions: Since the transition information is available within 24 hours, the Plan can reach out to all members who discharge and complete a post-discharge call to ensure all needs regarding medications, DME and home health are met. This call will be conducted by the Care Support team unless the member is already assigned to a Complex Case Manager or Health Coach. This process has been followed for Medicare members in the past and proven to be successful. By including the commercial population in the post-discharge call process the readmission rate at DHMC should decrease. Evaluation and Re-measurement: Readmission rate results from the Information Systems department are on a 6-month lag due to claims submission. DHMP is scheduled to measure the success of this intervention in November 2014 to ensure all data from the previous year is available. 3. Satisfaction with CCM For the complete CCM Satisfaction survey results, see Appendix B. Below are a sample of questions from the CCM Satisfaction survey that exemplify overall results. 7
47 Goal: Complex Case Management strives to achieve 75% 4 s and 5 s for the question: How helpful was your Case Manager in helping you understand your health. The Care Support Department conducts the Satisfaction Survey after completion or closure of the program. Care Support asks the question, How helpful was your Case Manager in helping you understand your health better?, as a part of the CCM Satisfaction Survey. This question best demonstrates the effectiveness of the Complex Case Management program since one of the primary goals of CCM is to increase the member s self-management of their health conditions. The respondents are asked to rate their case manager on a scale of 1-5 with 5 being the highest possible score. Quantitative Analysis: During this analysis period of 10/01/ /30/2013, only 8 surveys were conducted. The small sample size poses a challenge for this year, but commercial enrollment has increased considerably over the last 6 months, so a much larger sample size is projected for next year. Out of the 8 surveys, a total of 4 members responded with either a 4 or 5, providing DHMP a score of 50%. While the DHMP CCM team is knowledgeable about health conditions, they may not make condition-specific clinical goals the primary focus, thus causing members to believe their CCM is not educating members about their health. The score alone does not reveal the reasons that members did not rate their CCM higher, so DHMP looks at responses to other questions in order to determine the specific barriers to achieving the goal. The CCMs scored 75% satisfaction on the question, How well did your case manager share important information with you when it was needed?. This could mean that the CCMs are sharing information, but not the clinical education that the member is seeking. Also, 4 members (50%) feel that the case managers did not help them connect with community resources. This may be due to the fact that the majority of resources used at DHMP cater to the Medicaid and Medicare populations. There are very few resources that commercial members would find beneficial that the Complex Case Management team currently uses. Opportunities for Improvement (Qualitative Analysis): Until recently, eligibilty requirements for Complex Case Management centered around more psycho-social conditions. This may benefit other DHMP product lines, such as Medicare and Medicaid, but not the commercial plans since these members tend to be highly employed and healthier. DHMP has now redefined the eligibility criteria for Complex Case Management to include more condition-specific criteria. In doing so, the team began to recruit more members with critical conditions, such as diabetes, cancer and heart failure. One opportunity for improvement is that DHMP did not initially conduct in-depth training for clinical staff to focus more goals on these conditions. This would cause the members perception to be that their case manager was not improving their health. Another opportunity for improvement: the community resources offered to DHMP complex case management members does not cater to the commercial population. By including more commercial-centric community resources, case managers will be able to refer more members to seek additional assistance throughout the community and therefore help members gain more knowledge and autonomy concerning their health. 8
48 Interventions: In response to the score for the question, How helpful was your Case Manager in helping you understand your health?, DHMP has implemented two interventions. First, DHMP has scheduled staff in-services covering clinical conditions that align with eligibility criteria for Complex Case Management. By keeping Complex Case Managers current with their members unique conditions, they will be better equipped to work with them on their medical goals in addition to other issues that they are currently strong at resolving. Second, several community resources have been added the the CCM Community Resource script that CCMs use to assist members with finding useful organizations within the local and national community. These resources also include offerings available through the member s health plan through DHMP such as health and wellness classes and educational meetings. This Community Resource script is now reviewed monthly as a part of the care plan review to ensure members needs are met. Evaluation and Re-measurement: This measure will be re-evaluated in November 2014 as a part of the annual Complex Case Management satisfaction evaluation. DHMP will evaluate the Satisfaction Survey results for the previous year, audit to make sure all CCMs have attended the required trainings and are using the required assessments within the Guiding Care system. 9

49 Appendix A: CCM Effectiveness Review 10
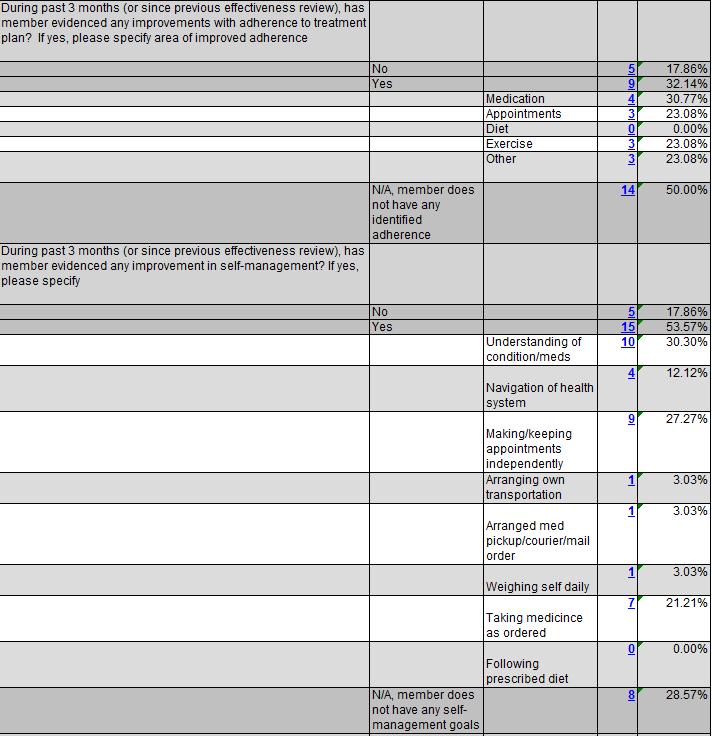
50 11
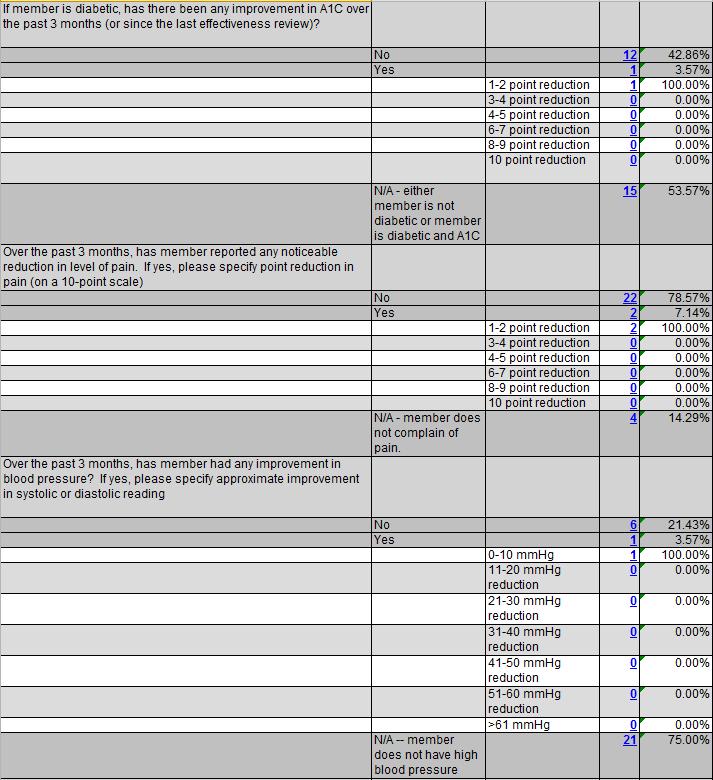

51 12

52 Appendix B: CCM Satisfaction Survey 13
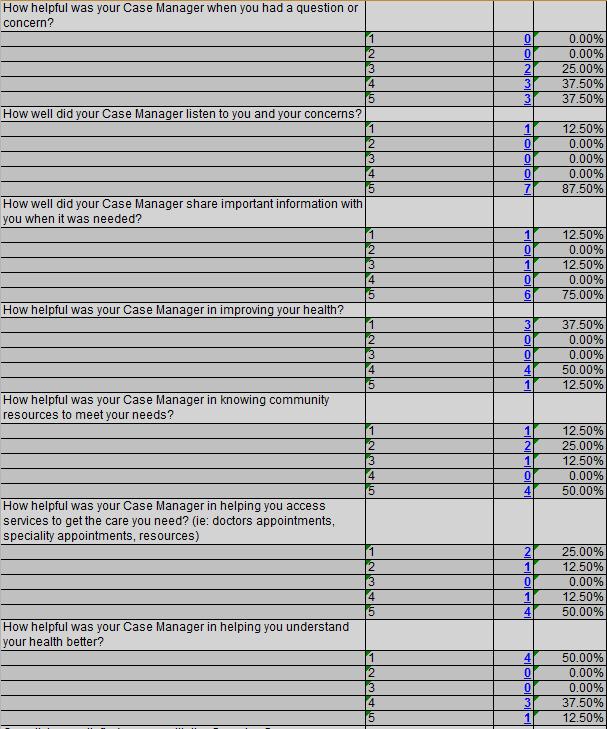
53 14
54 15
55 Appendix C: Self-Management Action Plan (SMAP) 16
56 17
57 Satisfaction Report for the Complex Case Management Program for Denver Health Commercial Plans Date of Report December 16, 2013 Period of Time Reviewed October 1, 2012 September 30, 2013 Introduction Denver Health Medical Plan (DHMP), Inc. provides health care coverage for employees of the Denver Health Authority and the Care Service Authority. DHMP offers several employer group plans including Medical Care HMO, Medical Care Expanded HMO and Point of Service (POS), hereafter called Commercial plans. Complex Case Management is available to all members of our Commercial plans. Complex Case Management (CCM) is the systematic coordination of care and services provided to members who have experienced a critical event or diagnosis that requires the extensive use of resources and who need help navigating the system to facilitate appropriate delivery of care and services. The goal of Complex Case Management is to help members regain optimum health or improved functional capability, in the right setting and in a cost-effective manner. It involves comprehensive assessment of the member s condition; determination of available benefits and resources; and development and implementation of a case management plan with performance goals, monitoring and follow-up. Member Complaints and Inquiries Members have several mechanisms in which to voice complaints or concerns. They can discuss these with their assigned case manager and/or the CCM supervisor. The members can also call Member Services (Customer Service) to file a complaint or grievance. The Appeals and Grievance Department researches the complaints and grievances to find resolution for the member. During this review period, October 1, 2012 to September 30, 2013, there were no member complaints or inquiries related to the Complex Case Management program. CCM Satisfaction Survey In 2013, the CCM program changed its process of obtaining the CCM Satisfaction Survey for members who had been engaged in the CCM program. Previously, the survey was conducted on a quarterly basis for all members who were engaged in the CCM program at some point over the past twelve months. The new process was implemented to obtain feedback from members upon case closure and avoid bias and duplication of responses by members receiving the survey more than one time. This year the survey was conducted telephonically by the Care Support staff when members were closed to the program. Members may be closed from the CCM program for reasons including but not limited to member expressing interest, member needs being addressed and goals met, termination of benefits, member being placed in long-term care facility and/or death. By completing the Survey upon case closure, the program is able to elicit unique responses from members.
 perception of the effectiveness of the CCM program.")
58 The purpose of the survey is to obtain the members perceptions about various facets of the CCM program from CM availability, to the usefulness of information provided, to CCM s impact on the member s health status. Below are the specific responses for the CCM Member Satisfaction Survey. This reflects the members (past or present) perception of the effectiveness of the CCM program.
59 Goal: The goal of the CCM Satisfaction Survey is to have 75% of responses of Question 8 be either option 4 or 5 indicating a positive response to the program. Analysis: A quick review of the CCM Satisfaction survey reveals a unique set of responses that were evenly divided between not at all satisfied and very satisfied with the CCM Program. There were no responses of a 2, 3, or 4 for overall program satisfaction. The majority of the responses are either a 1 or a 5 (on a scale from 1 to 5, with 5 being the most positive response); presenting a unique opportunity to explore the discrepancy in responses. When looking at other responses regarding the program, there were other possible positive conclusions that could be drawn. Based upon the responses, the Complex Case Managers are best at listening to member concerns, easily accessible, helping with a question or concern, sharing important information and helping members to access care. The case managers have room for improvement in helping members with community resources, improving the members health, and helping members understand their health better. Plan for improvement: The results of the CCM Satisfaction survey will be shared with the CCM staff raising their awareness of their strengths and weaknesses. As a team, staff will work to better understand the clinical knowledge and competence in providing diagnoses/condition specific interventions to improve delivery of case management services. A team action plan will be established that will incorporate well researched and proven techniques into practice. Case managers will receive clinical training (by RN or MD) to improve understanding of clinical guidelines, assessment and treatment, signs and symptoms, and management of illness. Some of the methods will include access to a knowledge library, use of patient education materials, and consistent incorporation of health related concerns in the Self-Management Action Plan (SMAP). These tools will serve as a way for staff to provide intervention in helping members improve and better understand their health. In addition to improving staff understanding and use of diagnosis-specific health information, the team will explore and utilize community resources related to those conditions. Half of those surveyed felt their case manager was not helpful in identifying resources to meet their needs. Staff will create and access a community resource repository as part of the ongoing management of health. Improving staff education and utilization of community resources available to members is expected to improve satisfaction with the CCM program in this area. Staff will develop and adopt standardized practice procedures and roles that embed clinical information, patient education and assessment of community resource needs into patient encounters. In conclusion, the implementation of a CCM Satisfaction Survey has provided valuable insight into the Program. While the sample size of 8 is small and may be statistically insignificant, this survey has provided Denver Health Medical Plan excellent feedback for growing an effective Complex Case Management program catering specifically to the needs of our unique Commercial population. The feedback from 2013 reflects strengths that are consistent throughout other programs offered by DHMP which demonstrate DHMP s establishment of strong core values. The few areas that scored lower offer an excellent opportunity for DHMP to take corrective action while our population is still small and allow for improvements as members continue to join the Complex Case Management program.
60 Continuity and Coordination of Medical Care DHMP Provider Survey 2013 Introduction Denver Health Medical Plan, Inc. (DHMP) recognizes that providing continuity and coordination of medical care is challenging in today s health care environment. At least annually, DHMP surveys its contracted providers to identify opportunities to improve continuity and coordination of care across the health care network. Methodology: At least annually, the DHMP Quality Improvement Department conducts a satisfaction survey of its contracted providers. The following questions are included in this survey to identify opportunities to improve continuity and coordination of care for our members. 1. How satisfied are you with the timeliness of the information you receive when your patients receive care in the following settings: a. Denver Health Specialists b. Non-Denver Health Specialists c. Denver Health Inpatient Hospital d. Non-Denver Health Inpatient Hospital e. Denver Health Emergency Room f. Non-Denver Health Emergency Room g. Home Health Agency h. Skilled Nursing Facility 2. How satisfied are you with the completeness of the information you receive when your patients receive care in the following settings: a. Denver Health Specialists b. Non-Denver Health Specialists c. Denver Health Inpatient Hospital d. Non-Denver Health Inpatient Hospital e. Denver Health Emergency Room f. Non-Denver Health Emergency Room g. Home Health Agency h. Skilled Nursing Facility The survey was mailed to 759 providers with 198 providers completed the survey a return rate of 26%. The table and chart below shows the breakdown of the responding providers, by specialty type. November 2013
61 2013 DHMP Provider Satisfaction Survey Q. 1. Which type of provider are you? Answer Options Response Count Response Percent PCP 75 38% Medical Specialist 49 25% Surgical Specialist 25 13% Behavioral Health Provider 9 5% Other 39 20% Total % Responding Providers, by Specialty 2013 DHMP Provider Survey Other 20% Behavioral Health Provider 4% Surgical Specialist 13% PCP 38% Medical Specialist 25% Goals: The goals for both questions are that at least 75% of the responding providers would be at least somewhat satisfied (score of 4 or 5) with the timeliness and completeness of the information they receive from all of the various settings Results: These two survey questions used Likert scale responses to measure degrees of satisfaction. To facilitate analysis, the responses were grouped into three categories Not very satisfied (score of 1 or 2), midrange (score of 3) and somewhat satisfied (score of 4 or 5). The tables and charts below provide the results. As noted in the tables and charts below, DHMP did not reach the 75% satisfaction goal for either the timeliness or completeness of information received from the various settings. November 2013
62 January DHMP Provider Satisfaction Survey How satisfied are you with the TIMELINESS of the information you receive when your patients receive care in the following settings? Answer Options 1 (Not at all satisfied) (Extremely satisfied) N/A Response Count Score of 1 or 2 -- not very satisfied Score of 4 or 5 Score of somewhat midrange satisfied Denver Health Specialists % 26% 48% Non-Denver Health Specialists % 29% 43% Denver Health Inpatient Hospital % 28% 58% Non-Denver Health Inpatient Hospital % 28% 25% Denver Health Emergency Room % 32% 42% Non-Denver Health Emergency Room % 28% 24% Home Health Agency % 25% 46% Skilled Nursing Facility % 27% 32% 70% Provider Satisfaction with the Timeliness of the information received when patients receive care in the following settings? 60% Score of 1 or 2 -- not very satisfied 50% 40% Score of 3 - midrange 30% Score of 4 or 5 - somewhat satisfied 20% 10% 0% Denver Health Specialists Non-Denver Health Specialists Denver Health Inpatient Hospital Non-Denver Health Inpatient Hospital Denver Health Emergency Room Non-Denver Home Health Health Agency Emergency Room Skilled Nursing Facility Results based on responses to the 2013 Denver Health Provider Survey November 2013
63 2013 DHMP Provider Satisfaction Survey How satisfied are you with the COMPLETENESS of the information you receive when your patients receive care in the following settings? Answer Options 1 (Not at all satisfied) (Extremely satisfied) N/A Response Count Score of 1 or 2 -- not very satisfied Score of 4 or 5 -- Score of 3 - somewhat to mid-range very satisfied Denver Health Specialists Non-Denver Health Specialists Denver Health Inpatient Hospital Non-Denver Health Inpatient Hospital Denver Health Emergency Room Non-Denver Health Emergency Room Home Health Agency Skilled Nursing Facility % 27% 58% 21% 28% 51% 10% 27% 63% 28% 35% 36% 21% 36% 43% 38% 34% 28% 33% 31% 36% 39% 31% 30% Provider Satisfaction with the Completeness of the information received when patients receive care in the following settings? 70% 60% Score of 1 or not very satisfied 50% Score of 3 - mid-range 40% 30% Score of 4 or somewhat to very satisfied 20% 10% 0% Denver Health Specialists Non-Denver Health Specialists Denver Health Inpatient Hospital Non-Denver Health Inpatient Hospital Denver Health Emergency Room Non-Denver Health Emergency Room Home Health Agency Skilled Nursing Facility Results based on responses to the 2013 Denver Health Provider Survey November 2013
64 Quantitative Analysis: This is the first time DHMP has surveyed providers related to Continuity and Coordination of Care, so there is no previous data for comparison to identify improvement or decline in performance over the past year. Timeliness Results: All of the results were below the goal of 75% satisfaction, but the providers were most satisfied with the timeliness of the information received from the Denver Health Inpatient Hospital (58%), Denver Health Specialists (48%) and Home Health Agency (46%). Providers were least satisfied with the timeliness of the information received from Non-Denver Health Emergency Room (24%), Non-Denver Health Inpatient Hospital (25%) and Skilled Nursing Facility (32%). Of note, also, are the following settings from which providers had high percentages of being not very satisfied with the timeliness of information received: Non- Denver Health Emergency Room (47%) and Non-Denver Health Inpatient Hospital (46%). Completeness Results: All of the results were below the goal of 75% satisfaction, but the providers were most satisfied with the completeness results from Denver Health Inpatient Hospital (63%), Denver Health Specialists (58%) and Non-Denver Health Specialists (51%). Providers were least satisfied with the completeness of the information received from Non- Denver Health Emergency Room (28%) and Skilled Nursing Facility (30%), Non-Denver Health Inpatient Hospital (36%) and Home Health Agency (36%). Of note, also, are the following settings from which providers had high percentages of being not very satisfied with the completeness of information received: Skilled Nursing Facility (39%) and Non-Denver Health Emergency Room (38%). The pattern of these results is somewhat expected it is easier for providers to obtain information about the patients when they receive care within the Denver Health system as compared to when their patients receive care outside of the Denver Health system. Qualitative Analysis: The setting with the lowest satisfaction ratings for both the completeness and timeliness of information is the Non-Denver Health Emergency Room (ER). Information exchange in this setting presents several barriers, including the following: There is no standard process for the non-denver Health Emergency Rooms to share member information with Denver Health. If the clinical information is sent to Denver Health, it is uploaded to the member s medical record, but the process is dependent upon the outside hospital initiating the transfer of information. Exchange of information is dependent upon members providing to the Non-Denver Health Emergency Room accurate information about their Primary Care Provider (PCP). Exchange of information often requires a signed Release of Information from the member. November 2013
65 Of concern are the scores of less than 75% for information exchange among Denver Health settings. Some of the narrative comments from the survey provide some insight to barriers which can be addressed. The Denver Health ER does not always complete notes within 24 hours The Denver Health PCP is not always notified when their patient is seen at the Denver Health ER. There is no streamlined way for the PCPs to receive information from Denver Health specialists after they have their patients. Some Denver Health Specialists are still handwriting notes, instead of dictating notes. Some of the handwriting is difficult to read. Opportunities for Improvement: There are numerous opportunities for improvement, but DHMP will concentrate on opportunities which should provide the greatest impact for the required effort. The following are opportunities to be considered: Encourage Denver Health Specialty providers to dictate clinic notes to improve readability. Explore possibility of automatic notification of Denver Health PCP when their members are seen at the Denver Health ER. Explore possibility of automatic notification of Denver Health PCP when their members are seen by a Denver Health Specialist. Educate members about the importance of providing accurate PCP information to non- Denver Health Emergency Rooms. Educate members about the importance of signing release of information forms when seen by Non-Denver Health providers. Actions: To be decided by the Quality Management Committee. Topic Continuity and Coordination of Care for DHMP Members Opportunity for Improvement Proposed Actions To Take November 2013
66 Continuity and Coordination of Between Medical Care and Behavioral Health Care DHMP Provider Survey 2013 Introduction Denver Health Medical Plan, Inc. (DHMP) recognizes that providing continuity and coordination between medical care and behavioral health care is challenging in today s health care environment, especially in light of stringent HIPAA protections. DHMP has begun to survey its contracted providers to identify opportunities to improve the coordination of care of its members Methodology: At least annually, the DHMP Quality Improvement Department conducts a satisfaction survey of its contracted providers. The following question is now included in this survey to identify opportunities to improve the coordinate the medical care and behavioral health care of its members. On average, how satisfied are you with the following aspects of the exchange of patient information between behavioral healthcare providers and other medical providers? Ease of the process Timeliness of the exchange of information Accuracy of the information Completeness of the information The survey was mailed to 759 providers with 198 providers completed the survey a return rate of 26%. The table and chart below shows the breakdown of the responding providers, by specialty type DHMP Provider Satisfaction Survey Q. 1. Which type of provider are you? Answer Options Response Count Response Percent PCP 75 38% Medical Specialist 49 25% Surgical Specialist 25 13% Behavioral Health Provider 9 5% Other 39 20% Total % November 2013
67 Responding Providers, by Specialty 2013 DHMP Provider Survey Other 20% Behavioral Health Provider 4% Surgical Specialist 13% PCP 38% Medical Specialist 25% Goals: The goal is for at least 75% of the responding providers to be at least somewhat satisfied (score of 4 or 5) with the various aspects of the exchange of patient information between behavioral healthcare providers and other medical providers. Results: This survey question used Likert scale responses to measure degrees of satisfaction. To facilitate analysis, the responses were grouped into three categories Not very satisfied (score of 1 or 2), midrange (score of 3) and somewhat satisfied (score of 4 or 5). The tables and charts below provide the results. As noted in the tables and charts below, DHMP did not reach the 75% satisfaction goal for any of the aspects of information exchange DHMP Provider Satisfaction Survey On average, how satisfied are you with the following aspects of the exchange of patient information between behavioral healthcare providers and other medical providers? Answer Options 1 (Not at all satisfied) (Extremely satisfied) N/A Response Count Score of 1 or 2 - Score of not very mid-range satisfied Score of 4 or 5 -- somewhat to very satisfied Ease of the process Timeliness of the exchange of information Accuracy of the information Completeness of the information % 30% 44% 27% 32% 41% 16% 27% 57% 18% 27% 54% November 2013

68 Provider Satisfaction with exchange of patient information between Behavioral healthcare providers and other medical providers? 60% 57% 54% Score of 1 or 2 -- not very satisfied 50% 44% 41% Score of 3 - midrange 40% 30% 30% 32% 26% 27% 27% 27% Score of 4 or 5 -- somewhat to very satisfied 20% 10% 0% Ease of the process Timeliness of the exchange of information 16% Accuracy of the information 18% Completeness of the information Results based on responses to the 2013 Denver Health Provider Survey Quantitative Analysis: This is the first time DHMP has surveyed providers related to Continuity and Coordination of Care, so there is no previous quantitative data for comparison to identify improvement or decline in performance over the past year. All of the results were below the 75% goal. The two highest scoring aspects of information exchange were Accuracy of the information (57%) and Completeness of the Information (54%). The two lowest scoring measures were Timeliness of the exchange of information (41%) and Ease of the process (44%). Qualitative Analysis: Although DHMP does not have quantitative data available to demonstrate definitive improvement or decline in this measure, the narrative comments from providers do indicate improvement over the past year. DHMP has integrated more behavioral health providers into the primary care clinics; the following comments from the Provider Survey seem to indicate that this has greatly improved the coordination between medical care and behavioral health care. November 2013
69 This has been HUGE change in the right direction since the beginning of the year. We now have a behavioral health specialist in our clinic that can help with consults and bridge the gap with psych med consults with the psychiatrists. We have an MHCD therapist and Behavioral in the clinic... awesome! With integrated care, we talk directly with the behavioral health providers. Given the challenges inherent with HIPAA regulations, the lower scores for Ease of the process and Timeliness of the exchange of information are not surprising. Of particular concern are the scores of less than 75% for the completeness and accuracy of the information exchanged. Provider comments provide some insight to the barriers to improvement: Notes are hard to decipher and the ones coming out of PES are all over the map - some excellent, some awful. I rely much more on provider-provider communication in the absence of a more modern and standardized system. Once again I am completely frustrated by the need to physically print and paste important, detailed medical information that comes in the form of correspondence and must get onto a barcoded form in order to get into the medical record. Several comments related to legibility of handwritten clinic notes Lack of a standardized process for obtaining patient information from Mental Health Center of Denver (MHCD) who provides care to many DHMP members. Opportunities for Improvement: There are numerous opportunities for improvement, but DHMP will concentrate on the opportunities which should provide the greatest impact for the required effort. The following are opportunities to be considered: Encourage behavioral health care providers to dictate clinic notes to improve readability. Explore possibility of standardizing a process for the exchange of patient information with MHCD providers. Educate members about the importance of proactively signing release of information forms when being seen by behavioral health providers. Actions: To be decided by the Quality Management Committee. Topic Continuity and Coordination of Care for DHMP Members Opportunity for Improvement Proposed Actions To Take November 2013
70 November 2013
71 Denver Health Medical Plan, Inc. Take Control Disease Management Program Description
72 Table of Contents Overview... 2 Introduction and Statement of Purpose... 2 Basis for Selection... 3 Evidence Based Guidelines... 3 Key Elements... 4 Program Design... 6 Interventions... 7 Care Coordination Approach for High-Risk Members... 9 Appendix DHMP Take Control Program Description Page 1 of 13 October 28, 2013
73 Overview Denver Health Medical Plan s (DHMP) Take Control Disease Management Program Description outlines the basis for selection of the two disease states it manages, the evidence based guidelines related to these conditions, the key elements of the program, the program structure and design as well as interventions implemented including multidisciplinary care management for our highest risk members. The Mission Statement of Denver Health Medical Plan, Inc. (DHMP) To provide quality, accessible and affordable healthcare services in the Denver area. In partnership with our providers we continually seek to improve the health and well-being of our members by: Promoting wellness and disease prevention Providing access to culturally diverse comprehensive health services Enabling members to play an active role in their health care Delivering our services with responsibility and respect to all DHMP s Take Control Disease Management Program is designed to support the mission of DHMP by improving the quality of care and disease outcomes for the Denver Health Medical Plan members. This is achieved through an assessment of member needs, provision of ongoing care monitoring, implementation of culturally appropriate and individually tailored interventions and provision of selfmanagement support so that members are empowered to play an active role in their health care. Introduction and Statement of Purpose The Denver Health Medical Plan Take Control disease management program aims to improve the quality of care and disease outcomes for the Denver Health Medical Plan members living with diabetes and/or depression. The program uses a multi-faceted approach to help members better manage these chronic conditions. An assessment of member needs, ongoing care monitoring, evaluation, and tailored interventions are utilized to help prevent and/or minimize the effects of the member s conditions. Through a multidisciplinary approach to care coordination and continuity of care for our highest risk members, as well as self-management support for all of our members to empower them to assume greater responsibility of their health, improvement in health outcomes and a reduction in costs should be realized. Self-management support has been shown to be an important component of the chronic care model and is supported in the evidence-based guidelines and recommendations. By providing patients the option to choose which type of support they would prefer to receive, it is anticipated that we will be able to achieve a higher level of engagement in our programs. Initial engagement at a lower level support option is also likely to lead to ongoing participation in a more intensive level of support at a later date. The program has been designed such that all communication related to the outreach, intake, tracking of interventions provided, ongoing monitoring, and pre and post evaluation surveys will be housed in our Guiding Care Care Management software system. This will allow for streamlined communication DHMP Take Control Program Description Page 2 of 13 October 28, 2013
74 between the multidisciplinary staff providing services related to the Take Control programs as well as reporting capabilities. Basis for Selection Disease State- Diabetes Diabetes is widely recognized as one of the leading causes of death and disability in the United States. According to the data from the 2011 National Diabetes Fact Sheet (released Jan. 26, 2011), 25.8 million children and adults in the United States, or 8.3% of the population, have diabetes. This condition accounts for almost 14% of US health care expenditures and it is associated with an increased risk for a number of serious, sometimes life-threatening, complications such as blindness, heart and blood vessel disease, stroke, kidney failure, amputations, and nerve damage. Diabetes control, which is largely achieved through health behavior change, can help reduce the risk of complications and decrease the cost of medical care. Disease State- Depression Every year, approximately 19 million Americans are affected by clinical depression. Depression affects males and females from all races, regardless of income, age, and ethnic and religious background. However, it is twice as common in women compared to men and three to five times more common in the elderly than in young people. Depression and Comorbid Diabetes The literature suggests that individuals with diabetes are twice as likely to be depressed as people without chronic disease and that depression is a risk factor for onset of type-2 diabetes. It has been shown to be associated with hyperglycemia, complications, smoking, mortality, and poorer adherence. Moreover, some research has shown that individuals with diabetes and depression are less likely than those without depression to achieve adequate levels of glycemic control. Evidence Based Guidelines Diabetes The American Diabetes Association s Standard of Medical Care in Diabetes (2009) states diabetes selfmanagement education (DSME) should be recognized as an integral component of care. Selfmanagement behavior change is the key outcome of DSME and should be measured and monitored as part of care. DSME should address psychosocial issues, since emotional well-being is strongly associated with positive diabetes outcomes. Cardiovascular disease (CVD) is the major cause of morbidity and mortality for individuals with diabetes and the largest contributor to the direct and indirect costs of diabetes. The common conditions coexisting with type-2 diabetes (e.g., hypertension and dyslipidemia) are clear risk factors for CVD, and diabetes itself confers independent risk. Depression According to the APA Practice Guideline for the Treatment of Patients with Major Depressive Disorder (2010) and the HealthTeamWorks Depression Guidelines (2011), depression increases the risk of cardiovascular disease and patients with depression have a higher mortality rate after myocardial infarction. Depression may lead to poor treatment adherence in patients with diabetes and recognizing depression must begin with symptom identification and diagnosis. Vital components of depression care DHMP Take Control Program Description Page 3 of 13 October 28, 2013
75 include patient education, helping patients and their families understand and accept a diagnosis of depression, and activating patients to seek help, adhere to treatment recommendations, and practice healthy behaviors that can promote recovery. The plan for treatment should include Shared Decision Making to tailor the treatment to the patient, provide education on diagnosis, review treatment options, discuss treatment barriers, and educate on importance of adherence. The promotion of the following health behaviors which include, but are not limited to, exercise, social support, faith/spiritual support, cessation of tobacco use, engagement in positive activities, stress management, and use of educational books and online resources is also indicated. Key Elements Program Objectives The Take Control disease management program is designed to improve the health and quality of care and disease outcomes for our members with diabetes and/or depression by providing specific information and interventions targeted at the management of these conditions, which include, but are not limited to, written patient education materials, audio/visual DVDs, education classes, and one-onone telephonic management via health coaching, telephonic counseling or complex case management. In addition, the program will strive to ensure members are well-prepared for their office visits, to assist and support members who are not adhering to the recommended treatment plan, and to increase overall patient satisfaction. As a result, the Take Control program aims to: 1. Empower patients to manage their health and health care by: a. Emphasizing the member s primary role in managing their health b. Using effective self-management support strategies that include assessment, goal setting, action planning, problem-solving and follow-up c. Facilitating coordination of internal and community resources to provide ongoing selfmanagement support to members d. Encouraging members to communicate with their providers 2. Improve healthcare outcomes though: a. Improved adherence to objective condition monitoring b. Improved medication and treatment adherence c. Identification of medical and behavioral health comorbidities d. Identification of barriers including cognitive deficits, physical limitations, and psychosocial issues 3. Lower the impact on financial expenditures through: a. Emphasis on appropriate utilization of services b. Increased primary care visits and decreased urgent/emergent visits c. Decreased readmissions and/or decreased length of stay of inpatient hospitalizations Program Goals 1. Analytically assess and stratify our member population 2. Identify and communicate gaps in care to our member population 3. Identify, provide and coordinate services 4. Ensure disease management activities which address the assessment and intervention for individual member needs as related to: health status, medical history and identified comorbidities, psychosocial issues, medication adherence and treatment, condition-specific DHMP Take Control Program Description Page 4 of 13 October 28, 2013
76 issues, cognitive and mental health status, cultural and physical preferences and limitations, identification of barriers, prioritization of goals and ongoing assessment of progress towards those goals, follow-up, and adherence to self-management action plan 5. With member consent, ensure the involvement of caregivers and provide information regarding the type and methods of support a caregiver can provide 6. Support the ongoing communication between the member and his/her health care team. 7. Provide referrals to resources as necessary 8. Maintain, evaluate and update as needed our disease management processes and resources to address members needs 9. Maintain a care management software system which supports the disease management program by: a. providing necessary evidenced-based clinical guidelines, algorithms, assessments, and documentation b. automatic prompts for follow-up c. automatic documentation of staff demographics, to include, staff members name, title date and time of input or activity 10. Formal evaluation of the program at least annually, as well ongoing informal review, to identify and monitor performance goals, measure outcomes or effectiveness and analyze results a. Action plans will be implemented to address barriers or other opportunities for improvement at the end of each evaluation and prior to the next year s rollout of the program Anticipated Outcomes As a result of our diabetes and depression disease management efforts, we anticipate the following outcomes: 1. Decreased HgA1c lab values of those members actively engaged in the health coaching program 2. Decreased PHQ-9 scores of those members actively engaged in the telephonic counseling program 3. Improved health literacy and knowledge of the disease state (as measured by pre/post knowledge tests) 4. Improved quality of life as measured by subscales of the Diabetes Distress Scale and other distress related questions on the pre/post evaluation measures 5. Decreased weight/bmi values of those members actively engaged in the health coaching program 6. Decreased tobacco use 7. Decreased ED/urgent care visits Program Design Target Population The Take Control disease management target population is active, adult members who are at risk for or who have been diagnosed with diabetes and/or depression. Method and Frequency of Member Identification Members eligible for the Take Control disease management programs will be identified at least monthly through the following data sources and referral mechanisms: DHMP Take Control Program Description Page 5 of 13 October 28, 2013
77 1. Claims and/or encounter (medical) data 2. Pharmacy data 3. Health Risk Appraisal (HRA) results 4. Laboratory results 5. Data collected through the Utilization and Case Management process 6. Internal department referrals from Care Support, Health Coaching and/or the Wellness Program 7. Information from EHRs 8. Practitioner referrals 9. Member and caregiver referrals Monthly, a report is generated which provides a list of members who have been diagnosed with diabetes and/or depression on at least two separate occasions in the last year as identified through ICD- 9 codes and claims. This report also provides clinical and laboratory information from our data warehouse including HbA1c, BMI, HDL, LDL, triglycerides and smoking status which can be used to stratify the population and identify those members who may be at greater risk based on disease severity or other markers or poorer health. Members who are identified as having a new diagnosis and/or a worsening of their diagnosis since the last data pull will be highlighted so that outreach can be made to engage them into the program. Members who exhibit non-adherence to their diabetes and/or depression medications will also be targeted for more active outreach. Denver Health's medical records system is available to all care providers in the organization and provides an individual medical record instantly for each patient. Members are incentivized to complete a Health Risk Appraisal annually through our online wellness portal. A report is generated on a monthly basis which identifies members who are at risk for or have either diabetes and/or depression based on specific questions which are positively endorsed in the HRA (i.e., the PHQ-2). Practitioner and selfreferrals, as well as referrals made from other medical management departments/programs including Care Support, Utilization and Case Management, Health Coaching and the Wellness Program to the Take Control Disease Management programs are received and tracked through the Guiding Care Care Management system. Since Denver Health is an integrated system, we have the ability to communicate with the primary care providers and other staff with whom our members may interact system-wide. This occurs through an electronic central repository of all visit and encounter documentation as well as direct , fax and/or telephonic communication. Risk Stratification Level Diabetes and Depression Members in the Take Control Disease Management programs will be stratified into four levels (low, moderate, high and critical risk) based on GuidingCare s Risk Stratification Methodology. The GuidingCare system predominantly relies on a combination of claims and pharmacy data to stratify members into various risk levels based on their propensity for future complications and/or costs. The predictive model used within GuidingCare to complete this risk analysis is the CDPS system developed by University of California, San Diego and approved by CMS for use in risk adjusted rate determination and program groupings in more than 12 states. Within this model, an initial Risk Weight for each member is calculated based on the member s age, sex and program/aid groupings (for Medicaid population only). Then based on a disease grouper within CDPS, the risk weight for specific condition groups that are active for a member driven from diagnostic codes and pharmacy codes is also added to obtain a holistic risk weight for an individual. The greater the number of conditions that a member has, the higher the DHMP Take Control Program Description Page 6 of 13 October 28, 2013
78 overall risk weight will be. The diagnostic groups cover approximately 60 condition categories including both physical health and behavioral health groups and hence, is a holistic estimation of risk across all conditions. Once this complete risk weight is calculated, outliers are eliminated by applying a standard deviation to the mean risk weight for a health plan s total membership so that outliers do not skew the risk stratification of the population. Once this is done a final risk score is assigned to each member and then the population is stratified into 4 groups Critical, High, Moderate and Low Risk Groups based on their risk scores. It must be noted that while in general, there are specific ranges of scores associated with each strata, clients can modify this based on program requirements and available resources to ensure that the right strategy for care management is deployed to the right number of members. In general 1-3 percent of the population is identified in the critical risk group, 10 percent in the high risk group, percent in the moderate risk group and the remaining fall under the low risk group. Where claims and pharmacy data is not available (new members), the system also has the capacity to use health risk assessments (HRA) analysis to determine a risk score that is dependent on the responses to the questions within the HRA. Risk Levels are as follows based on the GuidingCare Stratification Methodology: Level 1 (low risk): Risk Scores ranging from Level 2 (moderate risk): Risk scores ranging from Level 3 (high risk): Risk scores ranging from Level 4 (critical risk): Risk scores above 1,000 Refer to Appendix 1 Interventions Based on Risk Stratification. Enrollment Method All commercial members with a current diagnosis of diabetes and/or depression will be sent a welcome packet introducing them to the appropriate Take Control disease management program. This packet of information will provide basic education regarding the importance of having regular visits, exams, testing and screenings to ensure proper management of each of these conditions. Members will be able to choose from the following four self-management support options and will be sent a self-addressed postage paid return postcard to indicate their choice of intervention(s). 1. Written patient education materials specific to their condition 2. Patient education DVD specific to their condition 3. Participation in a condition-specific education class 4. One-on-one telephonic support (a referral will be made to the health coaching, telephonic counseling or complex case management program based on member s needs) In addition to providing a description of the program and how to use the services available, the introductory letter included in this welcome packet also outlines how members become eligible to participate and how they can opt out of the program. At least annually, practitioners are sent a letter which describes the disease management programs, the eligibility requirements and provides information on how to refer their patients. Periodically throughout the year, this same information is disseminated through our member and provider newsletters, through reminder blasts and is posted on the plan website as well. Interested members are asked to complete a pre-evaluation survey to assess their level of knowledge and attitudes/beliefs about their condition as well as their perceived distress related to the management of their condition. The survey also includes a screening for depression using the PHQ-2. DHMP Take Control Program Description Page 7 of 13 October 28, 2013
79 This survey can be completed on paper and returned in the mail or over the phone with one of our staff. Members are incentivized to answer the same set of questions at a later date to assess changes related to these constructs. For members who are identified as high risk and/or whose condition significantly worsens over time, an attempt is made to contact members by phone to engage them in the disease management program. Monitoring of Active Member Participation Active participation is defined as having completed the Take Control of Your Diabetes or Depression Disease Management Intake and corresponding Pre-Evaluation Survey as this interactive contact requires two-way interaction with the member. Quarterly, a report will is generated from our Guiding Care system to identify the members who have completed these assessments and is divided by the total number of members identified as eligible for participation in the Take Control Disease Management programs. Interventions Depending on the member s preferred method of self-management support, the following intervention options are available to help them improve the management of their diabetes and/or depression. Members will be incentivized for their participation in the program and for demonstrating positive health behavior changes. Patient Education Materials (Written and DVD) The Krames Diabetes book provides a general overview of diabetes and treatment, nutrition, physical activity, medications, monitoring blood glucose, preventing, detecting and treating complications, goal setting to promote health, adjusting to life with diabetes, problem solving and pregnancy. The Diabetes DVD provides an overview of type 2 diabetes and its potential complications. The program describes how people can take charge of diabetes through lifestyle changes and medications to live a longer, healthier life. It covers eating healthfully, losing weight, staying active, quitting smoking, and the importance of controlling blood sugar, blood pressure and cholesterol levels. The Krames Depression booklet offers myths and facts about depression, recognizing symptoms, diagnosis and treatment options, medications: types, uses and side effects, encouragement for patients to stick with treatment, and lifestyle changes that may help. The Depression DVD describes what people can expect from different treatment options, including self-help techniques, antidepressants, St. John s Wort for mild depression, depression counseling and combination approaches. The program provides guidance to help people decide which approach is best for them. There are also resources for locating a mental health care provider. The education classes and 1:1 telephonic support cover the same information presented above but in either a group format setting or individually over the phone. The written materials and DVD provide ongoing support as needed by the patient. The patient will have the flexibility of rereading material or re-watching the video at any time that is convenient to them. The materials offer tips and suggestions to help them overcome barriers and obstacles and the tools help the patient to create a management plan that they can stick with. DHMP Take Control Program Description Page 8 of 13 October 28, 2013
80 Disease Specific Education Classes The four week education classes offer an opportunity for patients with the same condition to meet together to discuss the daily challenges they face while trying to manage a chronic condition. The group format allows for participants to brainstorm and share ideas, it normalizes a patient's experience; it instills a sense of hope and also helps to build motivation for change. For diabetes specifically, curriculum from the Conversation Maps will be utilized. This is a structured, interactive education program that use images, metaphors, and thought-provoking conversation topics to provide a friendly learning experience for patients. It engages patients in exploring health facts through dialogue and helps them draw their own conclusions. Bilingual Health Coaches are available to conduct all classes in Spanish. Individualized Health Coaching Our Health Coaches work one-on-one with members and/or the member s caregiver, if applicable and with permission from the member, to provide individualized support and tailored interventions to help members self-manage their chronic illnesses and other health conditions by enhancing motivation and providing support and encouragement to individuals as they address chronic health care needs or lifestyle changes. Lifestyle behaviors including healthy eating, engaging in physical activity, limiting alcohol use and quitting tobacco use are assessed and motivational interviewing and other selfmanagement support techniques are used to increase the member s intrinsic motivation to improve these behaviors. When a caregiver is identified, and with permission from the member, information about the condition and treatment plan, including the type and methods of support a caregiver can offer, is provided to the respective caregiver. Bio-psychosocial assessments are conducted to gain a better understanding of the whole person, the barriers that might be preventing them from achieving their health goals, and to help inform the Health Coach of appropriate interventions for each individual. Readiness to change is assessed and a diverse array of psychological and behavioral change tools to empower individuals to become better selfmanagers of their health are employed. Interventions may include, but are not limited to, motivational interviewing for health behavior change, skills-based training, solution-focused therapy, provision of patient education, provision of information and resources, and facilitation of support groups and group visits focused on medical and behavioral issues. Health Coaches have diverse educational backgrounds and offer a wide range of clinical expertise. At a minimum, they receive specialized training in the following areas: 1) motivational interviewing for health behavior change, 2) disease education/management, 3) behavior change strategies, 4) cognitivebehavioral therapy, 5) cultural competency and diversity, 6) community resources. Working 1:1 allows for individualized support that can be tailored to meet the patient's needs. More indepth assessments are conducted which help to identify different demographic, socioeconomic, psychosocial and cultural components that may impact the patient's ability to manage their chronic condition. Patient s beliefs and concerns about their condition and treatment as well as any perceived barriers, such as access, transportation and financial barriers, to meeting the treatment recommendations are assessed. Information related to pertinent cultural, religious and ethnic beliefs that may impact the patient s care and treatment is also obtained. Various interventions, including but not limited to, the provision of patient education materials and resources, assistance scheduling transportation and appointments, motivational interviewing to increase self-efficacy and connecting to DHMP Take Control Program Description Page 9 of 13 October 28, 2013
81 community and other religious groups/resources are initiated based on the member s responses to these assessment questions. Health Coaches consistently support the ongoing communication between the member and his/her health care team. Patient handouts which discuss the importance of the communication and suggest methods of effective communication between patients and practitioners are provided. An annual health education seminar specific to this topic is also offered and presented by a physician. Telephonic Counseling for Depression and Anxiety For those members who screen positive for depression and would like further support beyond the Take Control disease management program, Behavioral Health and Wellness Services will refer these members to the Telephonic Counseling for Depression and Anxiety program. Members receive a comprehensive psychiatric assessment to screen for comorbid mental health conditions as well and 3 outcomes evaluation calls to assess changes in their depression and/or anxiety symptoms. The feedback from each of these telephone calls is provided in a report to the member s PCP which includes the identified comorbid psychiatric diagnosis(es), depression severity levels and management recommendations. Members have the opportunity to choose from 12 different counseling modules geared towards treating their depression and/or anxiety. The module topics include: Managing Stress and Anxiety, Behavioral Activation, Coping with Illness, Managing Chronic Pain, Changing Negative Thoughts, Improving Sleep, Eating Healthy, Increasing Exercise, Improving Interpersonal Relationships, Grief and Loss, and Problem Solving. Individualized Complex Case Management Although complex case managers are capable of, and often do provide health behavior change interventions consistent with those of a health coach, the goal of the program is to target members that require more intensive coordination of services. As such, high-risk members eligible for the program would include those with 1) advanced chronic diseases with multiple co-morbid conditions, 2) complicated acute diseases, 3) high utilization rates, and/or 4) severe psychological, and/or social issues or needs who require complex care coordination as well as assistance obtaining a wide range of resources. Bilingual Health Coaches, Behavioral Health Clinicians and Complex Case Managers are available to work with our Spanish-speaking members. We also have a 24/7 language line available for medical interpretation of other languages. Care Coordination Approach for High-Risk Members The Take Control program is designed as a collaborative care model with a multidisciplinary team in place to help provide self-management support to our highest risk members. The following teams will work in coordination and will communicate via our Guiding Care Care Management platform: Care Support - a team of patient navigators who will be responsible for outreach/intake and initial engagement of the members identified as eligible participants. Health Coaches see above. Behavioral Health Clinicians a team of master s level mental health clinicians who are available to provide telephonic counseling for the treatment of depression and anxiety. DHMP Take Control Program Description Page 10 of 13 October 28, 2013
82 Complex Case Managers see above. Pharmacy Case Managers a team of pharmacists, technicians, intervention managers and nurses who are available to help provide assistance with medication adherence for our members. Referrals to the Take Control programs are also made directly from this team for members identified through the prior authorization process or other inbound or outbound calls that are made to members for various reasons. Utilization/Case Managers Nurse case managers responsible for completing prior authorizations, reviewing inpatient hospital stays, assessing and appropriately facilitating discharge planning requests and completing post-discharge assessments. Nurse Advice Line The Denver Health NurseLine provides specialized nursing advice and triage for patients. 24 hours a day and 7 days a week using triage software and clinical protocols. Registered Nurses collect demographics, medical & medication history, and presenting symptoms. Using clinical guidelines, they assess the caller s symptoms to provide a comprehensive recommendation for treatment which may include a referral to the Take Control Disease Management program(s). DHMP Take Control Program Description Page 11 of 13 October 28, 2013
83 Appendix 1- Interventions Based on Risk Stratification Depression and Diabetes 1. Welcome letter and choice of the following: Written educational materials Educational DVD Disease-specific educational class 1:1 telephonic coaching 2. Ongoing monitoring of claims and other tools to re-assess risk and needs 3. Receipt of member newsletters with information about health and wellness and disease management programs and how to access services 4. Episodic educational interventions, as needed 5. Post hospitalization and emergency room assessment 6. Health Coaching/Complex Case Management: Bio-psychosocial assessments Depression screening Identification of barriers preventing one from achieving their health goals Individually tailored interventions, which employ a diverse array of psychological and behavioral change tools to empower individuals to become better self-managers of their health Readiness to change assessments Motivational interviewing for health behavior change Skills-based training Solution-focused therapy Complex care coordination Assistance obtaining resources Low Risk -Risk Score A1C < 7 -PHQ9 < 5 Med Risk -Risk Score A1C 7-8 -PHQ9 5-9 High Risk -Risk Score A1C PHQ PDC < 80% Critical Risk -Risk Score >1,000 -A1C >10 -PHQ9 > 20 -PDC < 80% Available if selfselected by member Available if selfselected by member Additional phone outreach calls made by patient navigators to attempt to engage member in services Additional phone outreach calls made by patient navigators to attempt to engage member in services DHMP Take Control Program Description Page 12 of 13 October 28, 2013
84 Monitoring Member Services Telephonic Performance Member Services has in place a departmental Performance Report that monitors four telephonic statistics categories to ensure that industry standards are met, specifically: Service Level at or above 85%, Average Delay of 30 seconds or less, Abandonment Rate of 5% or less, and overall Call Volume. The Member Services Performance Report monitors these telephonic statistics by each individual Denver Health Medical Plan (DHMP) and Denver Health Hospital Authority (DHHA) line of business. Tracking, comparison, and evaluation occurs on a monthly as well as annual basis. The Member Services Administrative Coordinator (MSAC) pulls all telephonic statistical data from the Cisco Telephony System reporting system Cisco Unified CXX Historical Reports and prepares the report for the Director of Member Services. The Director of Member Services reviews each report and then provides a summary of monthly activity as well as an analysis of any trends in data, call volume, reason codes, deficiencies, etc. The Director presents the Performance Report as well as his or her Summary and Analysis at each quarterly Quality Management Committee meeting. For 2013, all above stated goals and standards were met and maintained. Please see Report 1.1. Report MS Combined Service Level Service Level % Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Svc Lvl 08 Svc Lvl 09 Svc Lvl 10 Svc Lvl 11 Svc Lvl 12 Svc Lvl 13 *Service Level=Percentage of calls answered within 30 seconds. Standard: 80% (Industry) 85% (DMHP/MCD Choice)
85 100 MS Combined Average Delay Average Delay (Seconds) Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Avg Delay 08 Avg Delay 09 Avg Delay 10 Avg Delay 11 Avg Delay 12 Avg Delay 13 *Average Delay=How long callers wait before agent answers. Standard: 30 seconds (Industry) 30 seconds (DHMP/MCD Choice)
86 10.00% MS Combined Abandonment Rate % 8.00% 7.00% Abandonment Rate (%) 6.00% 5.00% 4.00% 3.00% 2.00% 1.00% 0.00% Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Abd Rate 08 Abd Rate 09 Abd Rate 10 Abd Rate 11 Abd Rate 12 Abd Rate 13 *Abandonment Rate=Percentage of callers that hang up before agent answers. Standard: <5% (Industry) <5% (DHMP/ MCD Choice)
87 10000 MS Combined Call Volume Number of Calls Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Call Vol 08 Call Vol 09 Call Vol 10 Call Vol 11 Call Vol 12 Call Vol 13 Monitoring Member Services Benefit Info for Quality and Accuracy In order to satisfy regulatory standards and monitor the telephonic quality of DHMP Member Services, the Member Services Quality Assurance Program has been instituted reporting occurring on a monthly basis. The MS QA Program allows the Member Services Leadership Team (MSLT) to determine any deficiencies in quality and service provided by the Member Services Representatives (MSRs) as well as work to correct any identified deficiencies. The QA Program serves as a valuable tool in staff development and satisfaction and is also incorporated into the annual MSR evaluation process to ensure that it is meaningful to the team and its individual members. The QA program entails monitoring and reporting on two components, telephonic productivity and performance as well as quality and accuracy of benefit information provided. Productivity is evaluated on specific metrics from the Cisco Telephony System, specifically Inbound Call Volume, Average Talk Time, Not Ready Time, and Reserved Time. The quality component of the QA Program is evaluated by direct call monitoring and evaluation by the MS Supervisor. The MS Supervisor selects 10 random calls for each MSR that occurred in the
88 specific month out of the Call Copy Call Recording Software. The MS Supervisor will evaluate the call for the quality and accuracy of the information provided based upon various criteria (member information confirmation, identifying issues, knowledge of benefits, documenting the call, tone of voice, etc.) and scores the MSR on a sliding scale dependent upon the accuracy of the information given. The overall evaluation of MSR performance in both areas is compiled, reviewed, and provided to the MSRs on a monthly basis. One on one coaching will occur if deemed necessary. In addition, an overall departmental MS Monthly Call Quality Performance Report is compiled to track the progress of quality maintained by the MSRs from month to month on an individual as well as departmental basis (see Report 1.2). All MSRs and the department overall must maintain an accuracy rate of 85% or higher. If this is not maintained, corrective actions are taken. The MSR Quality Assurance Program was implemented beginning in December of All data will become available in January of The DHMP Member Portal audit portion of the QA Program includes monthly internal auditing conducted by the Member Services Administrative Coordinator (MSAC) to test Member Portal functionality and monitor the quality of information provided online to members. The MSAC will evaluate the quality of benefit information posted on the Member Portal on a sliding scale based upon the functionality and quality. All information available on the DHMP Member Portal must maintain 85% accuracy as well as functionality. This portion of the QA Program allows the MSLT to analyze causes of deficiencies, identify opportunities for improvement, and if needed, initiate Corrective Action Plans for specified deficient areas (see Report 1.3). The Director of Member Services includes his or her Summary and Analysis on this report at each quarterly Quality Management Committee meeting. The DHMP Member Portal Quality Assurance Program will commence once the DHMP Member Portal is online and functional.
89 Report 1.2 EXAMPLE MS Call Quality Monthly Averages Quality Month

90 Report 1.3 Monitoring the Nurse Advice Line The primary intent of the Member Services Nurse Advice Line Performance Monitoring Program is to track member usage of the provided services and to identify opportunities and establish priorities for improvement. DHMP Member Services receives a monthly Performance Report from the Nurse Advice Line Leadership Team that includes Nurse Advice Line phone metrics such as Service Level, Average Delay, Abandonment Rate, and Call Volume for various DHMP and DHHA lines of business. The Nurse Advice Line is held to the same industry standards as DHMP Member Services, specifically: Service Level at or above 85%, Average Delay of 30 seconds or less, and Abandonment Rate of 5%. The Nurse Advice Line Performance Report also includes data on call triage and various member utilization (see Report 1.4). In addition to monitoring the quality and productivity of the Nurse Advice Line, DHMP Member Services also completes an annual member satisfaction survey call completed by MSRs. This member feedback is recorded and provided directly to the Nurse Advice Line Leadership Team (see Report 1.5).
2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary
 2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary Jai Medical Systems Managed Care Organization, Inc. (JMS) and its providers have closed out their fifteenth full year in the Maryland Medicaid HealthChoice
2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary Jai Medical Systems Managed Care Organization, Inc. (JMS) and its providers have closed out their fifteenth full year in the Maryland Medicaid HealthChoice
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
HEDIS TOOLKIT FOR PROVIDER OFFICES. A Guide to Understanding Medicaid Measure Compliance
 HEDIS TOOLKIT FOR PROVIDER OFFICES A Guide to Understanding Medicaid Measure Compliance TABLE OF CONTENTS WHAT IS HEDIS 1?... 1 ANNUAL HEDIS TIMELINE... 2 HEDIS MEDICAL RECORD REQUEST PROCESS:... 2 TIPS
HEDIS TOOLKIT FOR PROVIDER OFFICES A Guide to Understanding Medicaid Measure Compliance TABLE OF CONTENTS WHAT IS HEDIS 1?... 1 ANNUAL HEDIS TIMELINE... 2 HEDIS MEDICAL RECORD REQUEST PROCESS:... 2 TIPS
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
DENVER HEALTH MEDICAL PLAN, INC. & DENVER HEALTH MEDICAID CHOICE Medicaid Choice & CHP+ Quality Improvement Work Plan
 *2016-2017 QI Program Description-Scope The QI Program Description is reviewed annually and updated according to national and state standards and guidelines. The QI program scope, goals, objectives and
*2016-2017 QI Program Description-Scope The QI Program Description is reviewed annually and updated according to national and state standards and guidelines. The QI program scope, goals, objectives and
McLaren Health Plan Quality Improvement Update 2014
 McLaren Health Plan Quality Improvement Update 2014 Since the incorporation of McLaren Health Plan (MHP) in November 1997, the staff has continued to utilize their extensive clinical and administrative
McLaren Health Plan Quality Improvement Update 2014 Since the incorporation of McLaren Health Plan (MHP) in November 1997, the staff has continued to utilize their extensive clinical and administrative
and HEDIS Measures
 1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
HEDIS 101 for Providers
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions HEDIS 101 for Providers Aetna Better Health of Kentucky 2017 HEDIS 101 for Providers Aetna Better Health 2 HEDIS
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions HEDIS 101 for Providers Aetna Better Health of Kentucky 2017 HEDIS 101 for Providers Aetna Better Health 2 HEDIS
Quality Measures for HMO s: Understanding HEDIS
 Quality Measures for HMO s: Understanding HEDIS DANE COUNTY IMMUNIZATION COALITION MEMBERSHIP MEETING November 29, 2011 Elaine Rosenblatt MSN, FNP-BC Director, Quality and Care Management UW Medical Foundation/
Quality Measures for HMO s: Understanding HEDIS DANE COUNTY IMMUNIZATION COALITION MEMBERSHIP MEETING November 29, 2011 Elaine Rosenblatt MSN, FNP-BC Director, Quality and Care Management UW Medical Foundation/
Provider Training Quality Enhancement 2016
 Provider Training Quality Enhancement 2016 1 What s Ahead? Why Are We Here? 3 NCQA Accreditation & HEDIS 4-6 Medicare Start Rating & HEDIS 7 Provider s Role and Expectation 8-11 Staying Healthy During
Provider Training Quality Enhancement 2016 1 What s Ahead? Why Are We Here? 3 NCQA Accreditation & HEDIS 4-6 Medicare Start Rating & HEDIS 7 Provider s Role and Expectation 8-11 Staying Healthy During
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
HEDIS 101 for Providers 2018
 HEDIS 101 for Providers 2018 Improving Quality of Care HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). Author: Commercial & GBD Communication HEDIS Team Document
HEDIS 101 for Providers 2018 Improving Quality of Care HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). Author: Commercial & GBD Communication HEDIS Team Document
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
TO BE RESCINDED Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
2016 EPSDT. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
2016 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
2019 Quality Improvement Program Description Overview
 2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
2019 Quality Improvement Program Description Overview Introduction Eon/Clear Spring s Quality Improvement (QI) program guides the company s activities to improve care and treatment for the member s we
2018 Practice Improvement Program (PIP) Orientation. January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP)
 Orientation. January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP)") 2018 Practice Improvement Program (PIP) Orientation January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP) Practice Improvement Program (PIP) Leadership Team James Glauber, Chief
2018 Practice Improvement Program (PIP) Orientation January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP) Practice Improvement Program (PIP) Leadership Team James Glauber, Chief
IHCP Annual Workshop October 2017
 IHCP Annual Workshop October 2017 Pay for Performance (HEDIS) HHW-HIPP0519( 10/17) Exclusively serving Indiana families since 1994. Agenda Who is MDwise MDwise Delivery Systems HEDIS Overview Pay for Outcome
IHCP Annual Workshop October 2017 Pay for Performance (HEDIS) HHW-HIPP0519( 10/17) Exclusively serving Indiana families since 1994. Agenda Who is MDwise MDwise Delivery Systems HEDIS Overview Pay for Outcome
QUALITY IMPROVEMENT. Articles of Importance to Read: Quality Improvement Program. Winter Pages 1, 2, 3, 4 and 5 Quality Improvement
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Winter 2009 QUALITY IMPROVEMENT Quality Improvement Program The Quality
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Winter 2009 QUALITY IMPROVEMENT Quality Improvement Program The Quality
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
At the start of each HEDIS season, you will receive a fax from L.A. Care. Each fax request will stipulate what documents need to be faxed back.
 Office Manager s Guide to HEDIS 2018 L.A. CARE MEDICAL RECORD REQUESTS At the start of each HEDIS season, you will receive a fax from L.A. Care. Each fax request will stipulate what documents need to be
Office Manager s Guide to HEDIS 2018 L.A. CARE MEDICAL RECORD REQUESTS At the start of each HEDIS season, you will receive a fax from L.A. Care. Each fax request will stipulate what documents need to be
2016 Member Incentive. Program Descriptions. Our mission is to improve the health and quality of life of our members
 2016 Member Incentive Program Descriptions Our mission is to improve the health and quality of life of our members Member Incentive Program Descriptions I. Purpose Passport Health Plan (Passport) has developed
2016 Member Incentive Program Descriptions Our mission is to improve the health and quality of life of our members Member Incentive Program Descriptions I. Purpose Passport Health Plan (Passport) has developed
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Quality: Finish Strong in Get Ready for October 28, 2016
 Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Patient Centered Medical Home 2011 Standards
 PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
2016 Quality Management Annual Evaluation Executive Summary
 2016 Quality Management Annual Evaluation Executive Summary July 2017 Mission and Vision The purpose of the 2016 Annual Evaluation is to assess IEHP s Quality Program. This assessment reviews the quality
2016 Quality Management Annual Evaluation Executive Summary July 2017 Mission and Vision The purpose of the 2016 Annual Evaluation is to assess IEHP s Quality Program. This assessment reviews the quality
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Anthem Blue Cross and Blue Shield Serving Hoosier Healthwise, Healthy Indiana Plan and Hoosier Care Connect. Quality improvement strategies
 Serving Hoosier Healthwise, Healthy Indiana Plan Quality improvement strategies Learning objectives At the conclusion of this session, participants will be able to describe: Managed care products and eligible
Serving Hoosier Healthwise, Healthy Indiana Plan Quality improvement strategies Learning objectives At the conclusion of this session, participants will be able to describe: Managed care products and eligible
2017 EPSDT. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
2017 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
Practice Improvement Program 2017 Program Guide Primary Care
 Practice Improvement Program 2017 Program Guide Primary Care Community Clinic Enrollment Deadline: January 20, 2017 Last updated: June 23, 2017 Contacts: Kanelle Barreiro, Program Manager, Pay for Performance
Practice Improvement Program 2017 Program Guide Primary Care Community Clinic Enrollment Deadline: January 20, 2017 Last updated: June 23, 2017 Contacts: Kanelle Barreiro, Program Manager, Pay for Performance
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
Quality Management Utilization Management
 Aetna Better Health Aetna Better Health Kids Quality Management Utilization Management 2015 Program Evaluation EXECUTIVE SUMMARY Aetna Better Health, a Medicaid Physical Health-Managed Care Organization
Aetna Better Health Aetna Better Health Kids Quality Management Utilization Management 2015 Program Evaluation EXECUTIVE SUMMARY Aetna Better Health, a Medicaid Physical Health-Managed Care Organization
MDwise Pay-for-Performance (HEDIS)
") MDwise Pay-for-Performance (HEDIS) MDwise Quality Make it Count Exclusively serving Indiana families since 1994. HHW-HIPP0466 (8/16) Who is MDwise? MDwise is a local, not-for-profit company serving Hoosier
MDwise Pay-for-Performance (HEDIS) MDwise Quality Make it Count Exclusively serving Indiana families since 1994. HHW-HIPP0466 (8/16) Who is MDwise? MDwise is a local, not-for-profit company serving Hoosier
Assistance. Improving. Consumer Health. Strategies for
 Assistance Strategies for Improving Consumer Health A resource to help educate consumers about available preventive health incentives and eliminating barriers to receiving care www.bhpi.org www.healthsharesolutions.org
Assistance Strategies for Improving Consumer Health A resource to help educate consumers about available preventive health incentives and eliminating barriers to receiving care www.bhpi.org www.healthsharesolutions.org
Oregon's Health System Transformation
 Oregon's Health System Transformation MEASUREMENT PERIOD Baseline Year 2011 and Calendar Year 2013 JUNE 24, 2014 TABLE OF CONTENTS Executive Summary...iii 2013 CCO Performance and Quality Pool Distribution...1
Oregon's Health System Transformation MEASUREMENT PERIOD Baseline Year 2011 and Calendar Year 2013 JUNE 24, 2014 TABLE OF CONTENTS Executive Summary...iii 2013 CCO Performance and Quality Pool Distribution...1
1 Title Improving Wellness and Care Management with an Electronic Health Record System
 HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
Performance Incentives in the Southern California Permanente Medical Group (SCPMG):
:") Performance Incentives in the Southern California Permanente Medical Group (SCPMG): 1994-2007 Joel D. Hyatt, MD Assistant Medical Director Southern California Permanente Medical Group joel.d.hyatt@kp.org
Performance Incentives in the Southern California Permanente Medical Group (SCPMG): 1994-2007 Joel D. Hyatt, MD Assistant Medical Director Southern California Permanente Medical Group joel.d.hyatt@kp.org
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Medical Assistance Program Oversight Council. January 10, 2014
 Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Quality Management (QM) Program AmeriHealth Pennsylvania
 Program AmeriHealth Pennsylvania") Quality Management (QM) Program AmeriHealth Pennsylvania Goals and Objectives The goals and objectives of the Quality Management (QM) Program are to promote the quality and safety of medical and behavioral
Quality Management (QM) Program AmeriHealth Pennsylvania Goals and Objectives The goals and objectives of the Quality Management (QM) Program are to promote the quality and safety of medical and behavioral
Medical Record Review Tool Standards with Definitions
 WellCare Health Plans, Inc. WellCare of Georgia, Inc The WellCare Group of Companies Medical Record Review Tool Standards with Definitions Item # STANDARD DEFINITION SOURCE All Medical Records: 1 Patient
WellCare Health Plans, Inc. WellCare of Georgia, Inc The WellCare Group of Companies Medical Record Review Tool Standards with Definitions Item # STANDARD DEFINITION SOURCE All Medical Records: 1 Patient
HEDIS Measures and the Family Physician Office. Pablo J Calzada DO, MPH, FAAFP, FACOFP
 HEDIS Measures and the Family Physician Office Pablo J Calzada DO, MPH, FAAFP, FACOFP Disclaimer HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). NCQA and payers
HEDIS Measures and the Family Physician Office Pablo J Calzada DO, MPH, FAAFP, FACOFP Disclaimer HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). NCQA and payers
Note: Accredited is the highest rating an exchange product can have for 2015.
 Quality Overview Accreditation Exchange Product Accrediting Organization: NCQA HMO (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product can have for 215.
Quality Overview Accreditation Exchange Product Accrediting Organization: NCQA HMO (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product can have for 215.
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 2/4/2018 The following program policies are applicable to all contracted providers and practices recognized
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 2/4/2018 The following program policies are applicable to all contracted providers and practices recognized
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff
 Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
The Florida KidCare Program Evaluation
 The Florida KidCare Program Evaluation Calendar Year 2015 MED147 Deliverable # 59 12/6/16 Prepared by the Institute for Child Health Policy University of Florida Under Contract to the Agency for Health
The Florida KidCare Program Evaluation Calendar Year 2015 MED147 Deliverable # 59 12/6/16 Prepared by the Institute for Child Health Policy University of Florida Under Contract to the Agency for Health
IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM
 IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM VICE PRESIDENT, PUBLIC POLICY & EXTERNAL RELATIONS October 16, 2008 Who is NCQA? TODAY Why measure quality? What is the state of health
IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM VICE PRESIDENT, PUBLIC POLICY & EXTERNAL RELATIONS October 16, 2008 Who is NCQA? TODAY Why measure quality? What is the state of health
Quality Improvement Program
 Introduction Molina Healthcare of Michigan serves Michigan members in counties throughout Michigan since 2000. For all plan members, Molina Healthcare emphasizes personalized care that places the physician
Introduction Molina Healthcare of Michigan serves Michigan members in counties throughout Michigan since 2000. For all plan members, Molina Healthcare emphasizes personalized care that places the physician
3. Expand providers prescription capability to include alternatives such as cooking and physical activity classes.
 Maternal and Child Health Assessment 2015 In 2015, the Minnesota Department of Health conducted a Maternal and Child Health Needs Assessment for the state of Minnesota. Under the direction of a community
Maternal and Child Health Assessment 2015 In 2015, the Minnesota Department of Health conducted a Maternal and Child Health Needs Assessment for the state of Minnesota. Under the direction of a community
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives. Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018
 Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018 Why Standardization? MEDI-CAL CROSS PRODUCT San Francisco Health
Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018 Why Standardization? MEDI-CAL CROSS PRODUCT San Francisco Health
Healthy Patients/Engaged Patients
 Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Please stand by. There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1
 Please stand by There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1 Webinar Tips Today s webinar is a one-way audio broadcast through
Please stand by There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1 Webinar Tips Today s webinar is a one-way audio broadcast through
ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 CHRONIC DISEASE SPECIALTY PLAN
 ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 CHRONIC DISEASE SPECIALTY PLAN Section I. Definitions and Acronyms The definitions and acronyms in Attachment II, Section I, Definitions and
ATTACHMENT II EXHIBIT II-C Effective Date: February 1, 2018 CHRONIC DISEASE SPECIALTY PLAN Section I. Definitions and Acronyms The definitions and acronyms in Attachment II, Section I, Definitions and
Molina Healthcare Michigan Health Care Services Department Phone: (855) Fax: (800)
 Fax: (800)") Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
For Your Information. Introduction
 For Your Information Introduction We want you to be a well-informed health care consumer. The more you know about your health care coverage and how it works, the easier it will be for you to maximize the
For Your Information Introduction We want you to be a well-informed health care consumer. The more you know about your health care coverage and how it works, the easier it will be for you to maximize the
Illinois Birth to Three Institute Best Practice Standards PTS-Doula
 Illinois Birth to Three Institute Best Practice Standards PTS-Doula The Ounce recognizes that there are numerous strategies that can be employed to effectively serve pregnant and parenting teens and their
Illinois Birth to Three Institute Best Practice Standards PTS-Doula The Ounce recognizes that there are numerous strategies that can be employed to effectively serve pregnant and parenting teens and their
Developmental Screening Focus Study Results
 Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Communicator. the JUST A THOUGHT. Ensuring HEDIS-Compliant Preventive Health Services. Provider Portal Features. Peer-to-Peer Review BY DR.
 WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
Florida Medicaid: Performance Measures (HEDIS)
") Florida Medicaid: Performance Measures (HEDIS) Justin M. Senior Florida Medicaid Director Agency for Health Care Administration Senate Health Policy October 20, 2015 Statewide Medicaid Managed Care (SMMC)
Florida Medicaid: Performance Measures (HEDIS) Justin M. Senior Florida Medicaid Director Agency for Health Care Administration Senate Health Policy October 20, 2015 Statewide Medicaid Managed Care (SMMC)
OPPORTUNITIES FOR DATA INTEGRATION AND BEST PRACTICE INTERVENTIONS TO IMPROVE CLINICAL AND FINANCIAL OUTCOMES
 OPPORTUNITIES FOR DATA INTEGRATION AND BEST PRACTICE INTERVENTIONS TO IMPROVE CLINICAL AND FINANCIAL OUTCOMES Elizabeth S Miller, MPA November 2014 President BPKMiller Associates 1 2 3 HEDIS DATA IMPROVEMENT:
OPPORTUNITIES FOR DATA INTEGRATION AND BEST PRACTICE INTERVENTIONS TO IMPROVE CLINICAL AND FINANCIAL OUTCOMES Elizabeth S Miller, MPA November 2014 President BPKMiller Associates 1 2 3 HEDIS DATA IMPROVEMENT:
Federally Qualified Health Centers Rural Health Clinics. February Interim. Pay for. Quality
 Federally Qualified Health Centers Rural Health Clinics February 2018 2018 Interim Pay for Quality P R O G R A M G U I D E Table of Contents Introduction to the 2018 Primary Care Pay-for-Quality Program....2
Federally Qualified Health Centers Rural Health Clinics February 2018 2018 Interim Pay for Quality P R O G R A M G U I D E Table of Contents Introduction to the 2018 Primary Care Pay-for-Quality Program....2
2012 HEDIS/CAHPS Effectiveness of Care Report for 2011 Measures Oregon Commercial Business
 2012 HEDIS/CAHPS Effectiveness of Care Report for 2011 Measures Oregon Commercial Business About HEDIS The Healthcare Effectiveness Data and Information Set (HEDIS 1 ) is a widely used set of performance
2012 HEDIS/CAHPS Effectiveness of Care Report for 2011 Measures Oregon Commercial Business About HEDIS The Healthcare Effectiveness Data and Information Set (HEDIS 1 ) is a widely used set of performance
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Denver Health Medical Plan, Inc Access Plan for Large Group and Exchange Plans
 Denver Health Medical Plan, Inc. 2016 Access Plan for Large Group and Exchange Plans Table of Contents Page INTRODUCTION 3 I. DHMP NETWORKS OF PRIMARY CARE, SPECIALISTS, BEHAVIORAL HEALTH, HOSPITALS AND
Denver Health Medical Plan, Inc. 2016 Access Plan for Large Group and Exchange Plans Table of Contents Page INTRODUCTION 3 I. DHMP NETWORKS OF PRIMARY CARE, SPECIALISTS, BEHAVIORAL HEALTH, HOSPITALS AND
Kaleida Health 2010 One-Year Community Service Plan Update September 2010
 2010 One-Year Community Service Plan Update September 2010 1 2 Kaleida Health 2010 One-Year Community Service Plan Update September 2010 Kaleida Health hospital facilities include the Buffalo General Hospital,
2010 One-Year Community Service Plan Update September 2010 1 2 Kaleida Health 2010 One-Year Community Service Plan Update September 2010 Kaleida Health hospital facilities include the Buffalo General Hospital,
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration
 The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration January 26, 2012 1 Session Overview Partners in Innovation and Service
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration January 26, 2012 1 Session Overview Partners in Innovation and Service
From the Desk of the Medical Director Using Phone Triage to Meet Timely Access Regulations
 MD Health Plan of San Mateo Provider Newsletter Fall 2010 healthmatters From the Desk of the Medical Director Using Phone Triage to Meet Timely Access Regulations In our spring newsletter, we informed
MD Health Plan of San Mateo Provider Newsletter Fall 2010 healthmatters From the Desk of the Medical Director Using Phone Triage to Meet Timely Access Regulations In our spring newsletter, we informed
Anthem BlueCross and BlueShield
 Quality Overview BlueCross and BlueShield Accreditation Exchange Product Accrediting Organization: Accreditation Status: NCQA Health Plan Accreditation (Commercial HMO) Accredited Accreditation Commercial
Quality Overview BlueCross and BlueShield Accreditation Exchange Product Accrediting Organization: Accreditation Status: NCQA Health Plan Accreditation (Commercial HMO) Accredited Accreditation Commercial
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
Payment Transformation 2018 Measure Changes and Updates. April 4, 2018
 Payment Transformation 2018 Measure Changes and Updates April 4, 2018 1. 2018 Performance Measures 2. 2018 Engagement Measures 3. Patient Attribution & Panel Management Cozeva 4. Coreo 1. Effectively Manage
Payment Transformation 2018 Measure Changes and Updates April 4, 2018 1. 2018 Performance Measures 2. 2018 Engagement Measures 3. Patient Attribution & Panel Management Cozeva 4. Coreo 1. Effectively Manage
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies
 Advanced Primary Care Program Policies") Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Blue Cross & Blue Shield of Rhode Island (BCBSRI) Advanced Primary Care Program Policies Effective 1/1/2016 The following program policies are applicable to all contracted providers and practices participating
Requirements Document for the Blue Quality Physician Program sm Criteria Effective 08/03/2015
 All practices must reapply to the BQPP every 18 months Criteria Definition Validation Source(s) 7 Practice Elements 3 Provider Elements Practice level points: 1. PCMH/PPC/PCSP Recognition *Mandatory 2.
All practices must reapply to the BQPP every 18 months Criteria Definition Validation Source(s) 7 Practice Elements 3 Provider Elements Practice level points: 1. PCMH/PPC/PCSP Recognition *Mandatory 2.
California Pay for Performance: A Case Study with First Year Results. Tom Williams Integrated Healthcare Association (IHA) March 17, 2005
 March 17, 2005") California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
Medical Records Review & Retrieval
 Healthcare Effectiveness Data Information Set (HEDIS) Medical Records Review & Retrieval Measuring quality of care and services provided to our members! Date: November 16, 2016 Partnership HealthPlan Presenter:
Healthcare Effectiveness Data Information Set (HEDIS) Medical Records Review & Retrieval Measuring quality of care and services provided to our members! Date: November 16, 2016 Partnership HealthPlan Presenter:
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
ALL NEW ALOHACARE WEBSITE
 NEWS FOR PHYSICIANS AND PROVIDERS QUARTER 4 2017 NEW STREAMLINED PRIOR AUTHORIZATION PROCESS AlohaCare will implement a simplified and reduced list of services requiring Prior Authorization effective January
NEWS FOR PHYSICIANS AND PROVIDERS QUARTER 4 2017 NEW STREAMLINED PRIOR AUTHORIZATION PROCESS AlohaCare will implement a simplified and reduced list of services requiring Prior Authorization effective January
ALLIED PHYSICIAN IPA ADVANTAGE HEALTH NETWORK IPA ARROYO VISTA MEDICAL IPA GREATER ORANGE MEDICAL GROUP IPA GREATER SAN GABRIEL VALLEY PHYSICIANS IPA
 ALLIED PHYSICIAN IPA ADVANTAGE HEALTH NETWORK IPA ARROYO VISTA MEDICAL IPA GREATER ORANGE MEDICAL GROUP IPA GREATER SAN GABRIEL VALLEY PHYSICIANS IPA QUALITY IMPROVEMENT PROGRAM 2010 Overview The Quality
ALLIED PHYSICIAN IPA ADVANTAGE HEALTH NETWORK IPA ARROYO VISTA MEDICAL IPA GREATER ORANGE MEDICAL GROUP IPA GREATER SAN GABRIEL VALLEY PHYSICIANS IPA QUALITY IMPROVEMENT PROGRAM 2010 Overview The Quality
June Thank you for attending today s Webinar. We will begin shortly. June Brian Clark. Diana Charlton. Debbie Barkley Aetna Inc.
 June 2018 Brian Clark Diana Charlton Debbie Barkley Thank you for attending today s Webinar. We will begin shortly. June 2018 1 Brian Clark Diana Charlton Debbie Barkley Welcome Illinois, New Jersey, Florida,
June 2018 Brian Clark Diana Charlton Debbie Barkley Thank you for attending today s Webinar. We will begin shortly. June 2018 1 Brian Clark Diana Charlton Debbie Barkley Welcome Illinois, New Jersey, Florida,
Anthem BlueCross and BlueShield HMO
 Quality Overview BlueCross and BlueShield Accreditation Exchange Product Accrediting Organization: NCQA (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product
Quality Overview BlueCross and BlueShield Accreditation Exchange Product Accrediting Organization: NCQA (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home Domains of Function. Interpretive Guidelines
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home Domains of Function Interpretive Guidelines October 2009 Table of Contents Page 1.0 PATIENT-PROVIDER PARTNERSHIP 1 2.0 PATIENT REGISTRY
BCBSM Physician Group Incentive Program Patient-Centered Medical Home Domains of Function Interpretive Guidelines October 2009 Table of Contents Page 1.0 PATIENT-PROVIDER PARTNERSHIP 1 2.0 PATIENT REGISTRY
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Money and Members: Pay for Performance in a Medicaid Program
 Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
UPMC Health Plan Member Handbook
 Member Handbook Introduction UPMC Health Plan Member Handbook Introduction We prepared this booklet for you, whether you are an existing or a renewing member. While you need to read your Certificate of
Member Handbook Introduction UPMC Health Plan Member Handbook Introduction We prepared this booklet for you, whether you are an existing or a renewing member. While you need to read your Certificate of
NEW Provider Orientation
 NEW Provider Orientation About Golden Shore Medical Group Overview Golden Shore Medical Group (formerly Molina Medical Group) is owned and operated by J. Mario Molina, M.D. Dr. Molina continues his father
NEW Provider Orientation About Golden Shore Medical Group Overview Golden Shore Medical Group (formerly Molina Medical Group) is owned and operated by J. Mario Molina, M.D. Dr. Molina continues his father
Passport Advantage Provider Manual Section 8.0 Quality Improvement
 Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
Passport Advantage Provider Manual Section 8.0 Quality Improvement Table of Contents 8.1 Quality Improvement Program 8.2 Clinical Practice Guidelines 8.3 Star s 8.4 Quality of Care Concerns 8.3 Practitioner
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
National Survey of Physician Organizations and the Management of Chronic Illness II (Independent Practice Associations)
") If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP)
 DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP)") SNP MODEL OF CARE ANNUAL EVALUATIONS FOR 2013 INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP) 1 7 0 1 P O N C E D E L E O N B L V D, S
SNP MODEL OF CARE ANNUAL EVALUATIONS FOR 2013 INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP) 1 7 0 1 P O N C E D E L E O N B L V D, S
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
Part 3: NCQA PCMH 2014 Standards
 Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards