Implementation Practices: Motivating and Training Your Staff. Enhanced Services Boot Camp
|
|
|
- Aldous Stevenson
- 6 years ago
- Views:
Transcription

1
2 Implementation Practices: Motivating and Training Your Staff Enhanced Services Boot Camp
3 Objectives Develop mechanisms for getting buy in on your pharmacy culture. Apply best practices for engaging and training the pharmacy team to streamline operations. Develop mechanisms for giving feedback and managing resistance to change.
4 Panel Discussion Panelists: Tripp Logan, Pharm.D., L and S Pharmacy Joe Moose, Pharm.D., CPESN USA and Moose Pharmacy Denise Pratt, Pharm.D., First Pharmacy Services Moderator: Bri Morris, Pharm.D., NCPA Innovation Center
5 Workflow Best Practices Enhanced Services Boot Camp Ashley Branham, Pharm.D. & Joe Moose, Pharm.D. CPESN USA and Moose Pharmacy
6 Objectives Discuss how a med sync program can positively affect pharmacy operations. Outline staffing/workflow considerations needed for enhanced service delivery.
7

8 Everyone Must Work at the Top of Their License We need to re-engineer our practices to align with new payment models Technology should support us all moving to work at the top of our abilities


9 Different Approach to Payment and Delivery Fee for Service Population Health Management

10 Case Study When considering a patient population of 50,000
11 Technology to Help Me Fill Scripts Fast, Accurately, & Cheap Finding from NC State School of Industrial Engineering: If you are not efficient at the filling prescription process you will never get the enhanced services and clinical support process optimized. We don t address problems/opportunities at the time we find them. We wait until the end of the filling process.
: Coordinating all of a patient s prescription medications to be")
12 What is the ABM? Appointment-Based Model (ABM): Coordinating all of a patient s prescription medications to be picked up on the same date each month, coupled with communications from the pharmacy.
13 Best Thing Since Sliced Bread Patient Improved: Communication Patient adherence Quality of care Health outcomes Workflow/efficiencies Inventory management Coordinated refill program Completes triad of care Business differentiator Win-win-win model Improved patient outcomes Prescriber satisfaction Increased business efficiencies and margins Pharmacist Business margins Physician
14 ABM Impact on Workflow Reactive proactive Optimizes dispensing process the way we do business here Scripts patients Are we optimizing therapy? How s the patient s adherence? Facilitates the patient appointment Opportunity for revenue each month Additional time for meaningful patient interaction
15 Hello, Goodbye What you can expect: Streamlined workflow Predictable workload Decreased delivery runs Better inventory control Healthier bottom line More time for enhanced services What you won t miss: Manic Mondays Frequent flyers Waiting for patients to remember to call in a refill Last-minute call-ins on Friday afternoons or before holidays Taking care of patients who run out of pills
16 Synchronization: How It Works Action 1. Determine and list the chronic monthly prescriptions the patient will be taking. Example Lisinopril 20mg daily (due 4 th ) Synthroid 137mcg daily (due 16 th ) Metformin 500mg BID (due 22 nd ) 2. The medication with the highest copay should become the anchor prescription. Synthroid 137mcg (due 16 th ) 3. Calculate the quantity needed for each medication to synchronize it with the anchor prescription. Lisinopril 20mg (12 tablets) Metformin 500mg (50 tablets)
17 Synchronization: How It Works 4. Contact the patient s prescriber, explain your ABM program, and request two prescriptions for each synchronized medication: One for the quantity required for synchronization A second for the normal monthly quantity 5. Short/long fill the appropriate prescription(s) to synchronize with the anchor prescription. Document on the hard copy the one-time short fill was for the adherence program.
18 7-10 Days Prior to the Appointment Call patient to review medications Assess adherence Have you been to the doctor in the last month? Have you been in the hospital in the last month? Are you taking any new prescription or over-the-counter medications? Are there any other changes we need to be aware of at this time?
19 3-7 Days Prior to the Appointment Initiate refill requests, PAs; contact prescribers as needed Update the patient profile in the pharmacy management system Pharmacist reviews orders and resolves any drug therapy problems identified by the program manager
 Call and remind patient to pick up")
20 1-2 Days Prior to the Appointment Review inventory/order products Dispense product(s) Call and remind patient to pick up prescriptions

21 Appointment Date Patient picks up medications Pharmacist addresses any clinical issues Are we optimizing patient therapy? How s the patient s adherence? What services can we add on?
22 ABM is more than syncing medications. Leveraging the patient appointment for enhanced service delivery is key.

23 Tips from the Experts Designate a technician to run the daily operations Best use of staff time Something for them to own Vested interest in success Leverage your technology Identify non-adherent patients Group patients by sync date Reports to help with patient calls Robust sync programs
24 Med Sync Pearls Submission clarification codes for Medicare D Patients allow for prorated copays for <30 supply 47 use on first attempt (short fill) 48 use on subsequent usual fill (if you get a RTS reject for being <30 days) Figure out your anchor Highest copay med Delivery area Disease state drive to enhanced services Pay schedule
25 Free Tools/Resources Simplify My Meds Operations manual, patient forms Marketing kit Free to NCPA members ( Implementing Med Sync video series <25 minutes Step by step training Great for pharmacy staff
26 Failing Forward: Our Guide to Prepare Community Pharmacy for Delivering Value Rethink Workflow Operations Population Management Strategies Shifting the Patient s Expectation of the Pharmacy Experience
27 Rethink Workflow Operations Involvement of Pharmacy Staff This CPESN model will remain a disruption until all staff are educated to participate. Pharmacists need to engage and train pharmacy technicians, delivery drivers, and cashiers for roles supporting CPESN. You go into this project thinking you can be a super pharmacist, but you quickly realize that it needs to be a team effort.
28 Community Pharmacy Care Management Community Pharmacy Care Management Services provided locally by a community pharmacy in close coordination with other care team members, including other care managers that focus on optimal drug use. The objective of Community Pharmacy Care Management is to procure, update and re-enforce a team-based, patientcentered pharmacy care plan over time. This service line is longitudinal and coordinated with the rest of the care team. Confidential Do not reproduce or reuse without consent.
29 Intensity Intensity Intensity Transformational Change in Frequency & Nature of Clinical Patient Interactions Part D CMR Steady State Community Pharmacy Care Management Model Time (6+ months) Initial NC CPESN attempts at Community Pharmacy Care Management Time (6+ months) Time (6+ months) Confidential Do not reproduce or reuse without consent.

30 Meet Karrie We take a proactive approach for our patients. We start the process by calling them each month and finding out what medications they need, what has changed and what concerns they may have Adherence Technician They feel like they know me and they feel like they have a connection with our pharmacy. They know when they call Moose Pharmacy, they are more than a refill number.
31 Glimpse into Operations Input & Counting Typical Day 8:30AM-6:00PM Run queue for the day. Drug therapy problems (DTPs) identified in adherence and medication list discrepancy. 11:00AM-6:00PM- DTP follow up queue in dispensing system. Call patients, prescriber offices, insurance companies and comment on progress in dispensing system.
32 Getting in the Habit of Documentation Technician Tool: DTP Short Form 1. Form placed at technician work station 2. Technician to complete form if potential DTP s are identified 3. Technician to send form in basket to the pharmacist 4. Pharmacist investigate the issue and takes necessary steps to resolve DTP 5. DTP documented in platform
33 Glimpse into Operations Adherence Technician Typical Day 8:30-9:30AM: Identify patients for daily phone calls on call list. 9:30-1:30PM: Call patients- DTPs identified while reviewing adherence and medication list discrepancies. DTPs input added to dispensing system DTP queue via MTM Actions. Advise pharmacists on complex medication list and therapeutic considerations 1:30PM-5:00PM: Process patient medications-primary DTPs during this part of the day will be system failure (insurance reject, PA required) DTPs added to dispensing system DTP queue via MTM Actions. Help with DTP queue as allowed

34 Scripts Pfor Technician Touch Points
35 Vaccine Screening Form Instructions: By checking a box below, I am indicating that I have screened this patient and he/she is eligible to receive the marked vaccine. Section 1: Zoster (Shingles) Zostavax The patient is 60 years old AND has not received Zostavax at any point in the past. Section 2: Influenza (Flu) Fluzone (Trivalent), Fluvirin (Trivalent), Flulaval (Quadrivalent), Fluzone HD (High Dose) The patient has not had the influenza vaccine AND is 14 YO Section 3: Pneumococcal Conjugate Prevnar13 (PCV13) The patient has never received Prevnar13 (PCV13) AND any one of the following: 65 years old years old AND has one of the following conditions: congenital/acquired immunodeficiency (including B-,T-lymphocyte, or complement deficiencies, phagocytic disorders). leukemia, lymphoma, Hodgkin s disease, generalized cancer, multiple myeloma. HIV infection. chronic renal failure, nephrotic syndrome, or solid organ transplant. iatrogenic immunosuppression (including long-term corticosteroids and radiation therapy). anatomical or functional asplenia. cerebrospinal fluid leak. cochlear implant. Section 4: Pneumococcal Polysaccharide Pneumovax23 (PPSV23) The patient is: 65 years old AND one of the following: has never received Pneumovax23 (PPSV23) AND has received Prevnar13 (PCV13) 1 year ago. received Pneumovax23 (PPSV23) when they were < 65 YO AND it has been 5 years since the previous PPSV23 dose years old AND has a high risk medical condition: chronic heart condition (chronic heart failure or cardiomyopathies, excluding hypertension). diabetes. chronic lung disease (COPD, emphysema, asthma). alcoholism. chronic liver disease (cirrhosis). immunocompromising conditions (HIV, long-term steroids, chronic renal failure). smokes cigarettes. anatomical or functional asplenia. Section 5: Tetanus Boostrix (Tdap) or Tenivac (Td) The patient is 18 years old AND any one of the following: pregnant. has not received the Tdap vaccine. received Tdap 10 years ago. it is unknown if they have received Tdap. Section 6: Hepatitis B (Engerix-B) The patient is 18 years old AND any one of the following: has not received the hepatitis B series or did not receive the full hepatitis B series. is at high risk for acquiring the infection (i.e. diabetes, healthcare professional, household contacts with HBV, end -stage renal disease, kidney dialysis, HIV, chronic liver disease, seeking/receiving STD treatment). Section 7: Meningococcal Menactra The patient is years old AND any one of the following: has no previous meningococcal vaccination. has not received a dose of meningococcal vaccine after their 16 th birthday and requires catch up vaccination. is a first year college student who lives in a dorm or plans to live in a dorm. 18 YO AND plans to travel to an area of the world where meningococcal disease is common. Vaccine Screening Form Created by Laura A. Rhodes, PharmD, Moose Pharmacy of Concord Rhodes, L. A., Branham, A. R., Dalton, E. E., Moose, J. S., & Marciniak, M. W. (2017). Implementation of a vaccine screening program at an independent community pharmacy. Journal of the American Pharmacists Association, 57(2), Revised: 02/10/2016
36 Glimpse into Operations Dispensing Pharmacist 8:30AM-9:30AM Work on DTP follow up queue 9:30AM-6:00PM- Identify DTPs while dispensing. Risk score of 75 warrants checking to see if a CMR has been completed within a year. If no CMR, notify cashier or delivery drive and attempt to complete if time permits or schedule. Notify cashier if RPh needs to speak w/ patient to address DTP when in the store Delivery driver to call RPh when he arrives at patient home to address DTP Scheduled CMR should be added to dispensing system queue. If dispensing pharmacist is unable to complete CMR with patient, then clinical pharmacist will assist
37 Glimpse into Operations Cashier 8:30-9:30AM: Tag bags for potential face to face CMRs from report given by pharmacist or technician. 8:30AM-6:00PM: Schedule CMR for pharmacist at point of sale if no time to do CMR. Pull return to stock medications if remaining in will call bin for 10 days or more (call patient to determine if still need medication or reason for denial). Notify staff if patient chooses not to get a medication or if returned by delivery driver.
38 Glimpse into Operations Delivery Drivers Call pharmacist or technician after arrival at patient home per pharmacist/technician request. Share any compelling social/health status changes with pharmacist. Notify technicians of new phone numbers of any points of contact for patient (extended family, neighbor) for difficult to reach patients. Notify cashier of address change so it can be changed in dispensing system.

39 Different Expectations of Our Pharmacy Team If we are going to be different in the marketplace We need to deliver services differently
40 Identifying Drug Therapy Problems- It s a Team Approach Prescription ON HOLD for Simvastatin 40mg and Aspirin 325mg Prescriber office (different from the PCP) was contacted. Told that the patient was recently discharged from the rehabilitation center. Patient s PCP was also notified to discuss discrepancies in medication regimen. PCP unaware of patient s most recent discharge from rehabilitation center. Patient was notified and fill was initiated Medication was delivered to the patient s home
41 Identifying Drug Therapy Problems- It s a Team Approach Prescription ON HOLD for Simvastatin 40mg and Aspirin 325mg Student Pharmacist Discovery through Data Mining Project
42 Identifying Drug Therapy Problems- It s a Team Approach Prescription ON HOLD for Simvastatin 40mg and Aspirin 325mg Prescriber office (different from the PCP) was contacted. Told that the patient was recently discharged from the nursing home Consulted with Pharmacist and Adherence Technician Notified Prescriber
43 Identifying Drug Therapy Problems- It s a Team Approach Prescription ON HOLD for Simvastatin 40mg and Aspirin 325mg Prescriber office (different from the PCP) was contacted. Told that the patient was recently discharged from the nursing home Patient s PCP was also notified to discuss discrepancies in medication regimen. PCP unaware of patient s most recent discharge from nursing home. Consulted with Pharmacist again and Adherence Technician Notified PCP
44 Identifying Drug Therapy Problems- It s a Team Approach Patient was notified and fill was initiated Medication was delivered to the patient s home Pharmacist discussed with patient and alerted Technician to fill the medications Delivery Driver
45 Targeting Patients and Populations

46 Importance of Targeting and Channeling Patients to High Performing Pharmacies

47 Panel Management & Risk Stratification Managing a panel of patients is new to community pharmacy Adequate training is needed to acclimate to this model Patients at different levels of risk need different types of intensities of services from enhanced service pharmacies Assists with targeting intensive activities toward highest risk, most complex patients
48 Well Informed Protocols. Risk Scores Algorithms Protocols Risk of Admission (30 Days) 6 or More Medications If X, then Schedule Appt. Risk of Admission (12 Months) High Risk Medications If X, then Med Sync Risk of Low Adherence Preferred Payer If X, then phone f/u Risk of Therapeutic Consideration Preferred Clinician/Provider If X, ask if they would like Risk of Discrepancy Discharged & >3 Chronic Meds If CMR Due, Task. Composite Medication Chaos Risk Low PDC for >2 Classes If High Risk for Hosp., Offer Potential Savings From CPCM 6 Or More Opioids in 90 days If Overdose Risk Offer Naloxone
49 Using Risk Scores in Your Community Pharmacy Obtain report with spreadsheet of risk scores organized from highest to lowest Proactively engage patients at high risk (alert staff, conduct medication reviews, reach out by phone for check-in) For those not reached, flag in the system to alert staff at next point of contact
50 No Population Management Tool? Do you have patients that fit any of the following criteria? Trends of poor adherence to chronic medications Recurrent visits to ED or hospital Transportation challenges Literacy challenges Complex medication regimens Looking to reduce number of visits to the pharmacy
51 Changing Patient Expectations The patient experience in this model may be different than how the patient previously worked with his or her pharmacy. - Intensive monitoring - Initial attempts to engage patients in this way should be acknowledged to help set new expectations
52 Strategies for Patient Engagement Leverage information about their recent health care utilization or concern with their medications Leveraging a referral from their care manager or provider Using a connection point such as an immunization or assistance with Medicare Part D plan selection to build trust
53 Referral from Provider to Provider
54 Ashley Branham, PharmD CPESN USA Joe Moose, PharmD CPESN USA
55 Financial Planning: Building the Business Case for Expanded Services Enhanced Services Boot Camp Tripp Logan, Pharm.D. L and S Pharmacy

56 My Background: COMMUNITY PHARMACIST / PHARMACY OWNER 2 nd generation multi-pharmacy owner in Southeast Missouri Strong focus on appropriate medication use Quality focused pharmacy practices Residency program, care coordination, disease state management, diabetes support group, medication use monitoring, MTM, compliance packaging, TOC, etc. PHARMACY QUALITY CONSULTANT / PARTNER MedHere Today is a healthcare quality and performance consulting firm created to help healthcare stakeholders expand and grow their quality and value based initiatives by leveraging community pharmacy. SERVICE ORGANIZATIONS Pharmacy Quality Alliance (PQA) Board Liaison NCPA Innovation Center Board Member CPESN USA National Luminary CPESN Missouri Lead Luminary Local Department of Health Board of Directors
57 Disclosures Tripp Logan, PharmD NCPA Innovation Center Board Member CPESN USA National Luminary Partner, MedHere Today Consulting Vice President, Logan & Seiler Inc. (L&S Pharmacy / Medical Arts Pharmacy)
58 Disclosures Tripp Logan, PharmD does not have (nor does any immediate family member have) actual or potential conflict of interest, within the last twelve months, a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with an organization whose philosophy could potentially bias this presentation.
59 Personal Disclaimer The content of this presentation reflects my personal experiences in our pharmacies, our consulting firm, and my service within pharmacy advocacy groups. Each pharmacist & pharmacy is unique, with a unique payer mix, unique set of offered services, unique opportunities, and most of all unique patient populations. The purpose of this presentation is to walk you through our ROI exploration process in our businesses. The purpose of this presentation IS NOT for it to be used as specific guidance on how you should operate your pharmacy practice, how you work within your current or future pharmacy contracts, or how you care for your unique set of patients. --Tripp Logan, PharmD
60 Most Taboo Words in Health Care: Provider Profitability
61 Pharmacy Staff Orientation Speech: As a community pharmacy, our primary responsibility is to the patients that walk through our doors. If we make poor business decisions, we close our doors, and FAIL EVERY PATIENT WE SERVE.
62 The Community Pharmacy Conundrum: Pharmacies must: 1. Think PATIENT FIRST PAYER SECOND, 2. While we ensure that our patients have access to the medication they need, 3. And maintain pharmacy profitability at the same time.
63

64 Pharmacy Service Litmus Test How Do You Identify a Return On Investment?


65 Good Investments are Typically: Good for Prescribers Good for Employers Good for Third Parties Good for Pharmacy Staff Good for Pharmacy Good for Patients

66 Standard Question: How Can I Afford This? Pharmacist time is limited Pharmacist time is expensive Enhanced pharmacy service reimbursement is not always available My dispensing reimbursement is shrinking and my DIR fees are rising
67 Begin With a Business Plan How much time will this service take to implement? Can I start small and scale? What is my target market? What will this cost in labor? What will this cost to implement? Will this service also provide advertising? What is the short term & long term program budget?

68 Begin With a Business Plan There is a How much time will this service take to implement? Can I start small and scale? What is my target market? What will this cost in labor? What will this cost to implement? Will this service also provide advertising? What is the short term & long term program budget? difference between REIMBURSABLE and PROFITABLE
69 Consider Services That Are Profitable and/or Marketable Profitable Marketable Adherence monitoring program with packaging Transition of care with hospital Care coordination with mental health provider Immunizations Medication Therapy Management Clinical services (blood pressure, blood glucose testing, Etc.)

70 Ask yourself: Is This? Good for my patients? Revenue producing & profitable? Good for my pharmacy s image? Something my staff will buy in to? Is this sustainable? If the answer is NO, that s OK. Don t force it.
71 What s Out There? To seize opportunities, you MUST look beyond the counter at things like: Your current business model and processes Your unique patient mix Your exposure to national markets Your exposure to LOCAL markets



72 Key Universal Targets: Patients Rx Volume / New Patients / Foot Traffic Pharmacy Operations Workflow / Efficiency / Labor / Wages Providers Health Systems / Clinics / Prescribers Payers Health Plans / PBMs / Employers
73 Adherence Monitoring: ROI Increase in ADDITIONAL program-driven Rx volume Number of patients enrolled in program Additional Rxs per patient annually * 2900 *Armstrong T., Impact of the MedHere Today Program on Persistence and Adherence, A Descriptive Report; Pfizer, May 2011.
74 Adherence Monitoring: ROI Cash flow savings for pro-active medication management of 20 patients $ $10000 Pharmacy cost of Each Prescription Number of patients filling one $500 Rx/mo

75 Adherence Monitoring: ROI Cash flow savings for pro-active medication management of 20 patients $10,000/mo = $120,000/year $ That s a Pharmacist Salary!!!! $10000 Pharmacy cost of Each Prescription Number of patients filling one $500 Rx/mo

76 All Rxs ARE NOT Created Equal

77 All Rxs ARE NOT Created Equal
78 All Rxs ARE NOT Created Equal
79 Targeting Exercise 1. Who is my most profitable third party payer? 2. Which prescriber accounts for the most prescriptions from that payer? 3. What is my average margin per patient per month from this third party payer and prescriber 4. How many patients do I have from that prescriber and how could I get more?
80 Targeting Exercise 1. Who is my most profitable third party payer? 2. Which prescriber accounts for the most prescriptions from that payer? 3. What is my average margin per patient per month from this third party payer and prescriber 4. How many patients do I have from that prescriber and how could I get more? 1. State Medicaid Local Results 2. Multi-Site Mental and Behavioral Health Clinic 3. Average 4 Rx/patient but most see multiple prescribers ($63 avg margin/mo) 4. We see 88 patients/month
81 Targeting Exercise 1. Who is my most profitable third party payer? 2. Which prescriber accounts for the most prescriptions from that payer? 3. What is my average margin per patient per month from this third party payer and prescriber 4. How many patients do I have from that prescriber and how could I get more? 1. State Medicaid Local Results 2. Multi-Site Mental and Behavioral Health Clinic 3. Average 4 Rx/patient but most see multiple prescribers ($63 avg margin/mo) 4. We see 88 patients/month
82 Targeting Exercise 1. Who is my most profitable third party payer? 2. Which prescriber accounts for the most prescriptions from that payer? 3. What is my average margin per patient per month from this third party payer and prescriber 4. How many patients do I have from that prescriber and how could I get more? 1. State Medicaid Local Results 2. Multi-Site Mental and Behavioral Health Clinic 3. Average 4 Rx/patient but most see multiple prescribers ($63 avg margin/mo) 4. We see 88 patients/month
83 Targeting Exercise 1. Who is my most profitable third party payer? 2. Which prescriber accounts for the most prescriptions from that payer? 3. What is my average margin per patient per month from this third party payer and prescriber 4. How many patients do I have from that prescriber and how could I get more? 1. State Medicaid Local Results Don t Forget to Factor in average DIR Fees 2. Multi-Site Mental and Behavioral Health Clinic 3. Average 4 Rx/patient but most see multiple prescribers ($63 avg margin/mo) 4. We see 88 patients/month
84 Internal DIR Fee Assessment Plan A $0.00 / Rx Plan E $2.76 / Rx Plan B $0.00/ Rx Plan F $5.00 / Rx Plan C $0.00 / Rx Plan G $7.00 / Rx Plan D $2.17 / Rx Plan H $20.16 / Rx
85 Targeting Exercise 1. Who is my most profitable third party payer? 2. Which prescriber accounts for the most prescriptions from that payer? 3. What is my average margin per patient per month from this third party payer and prescriber 4. How many patients do I have from that prescriber and how could I get more? 1. State Medicaid Local Results 2. Multi-Site Mental and Behavioral Health Clinic 3. Average 4 Rx/patient but most see multiple prescribers ($63 avg margin/mo) 4. We see 88 patients/month
86 Targeting Exercise 1. Started with Research in Mental Health, Medicaid, the Clinic 2. Became familiar with some pharmacy best practices in mental and behavioral health 3. Learned who was on the board and who was in administration 4. Explored common barriers and pharmacy solutions that could positively impact mental and behavioral health
87 Targeting Exercise: Gaps Primary non-adherence Never get first fill Routine non-adherence Doesn t continue medication Formulary issues patients unable to acquire medication Lack of Care Coordination Patients unable to navigate the health care maze Transportation Patients struggle with acquisition of meds Lack of communication among providers Patients receive sub optimal care due to health care silos Limited continuity of care Treatment often stops once the patient walks out of the clinic

88 Targeting Exercise: Use What You Have Our care coordination and adherence monitoring leads to improvements in medication adherence across multiple chronic conditions *Armstrong T., Impact of the MedHere Today Program on Persistence and Adherence, A Descriptive Report; Pfizer, May 2011.
89 Targeting Exercise: Solutions? Adherence Packaging

90 Targeting Exercise: Adherence Packaging Business Planning How much does a vial cost? How much does a cap cost? How much does a label cost? How much does a package / card cost? How many vials equal the cost of one package / card? How many cards will each new clinic patient purchase?
91 Targeting Exercise: Adherence Packaging Results Found packaging solution that allowed us to start with minimal investment and automation upgrade opportunities Estimated that patients with 10 or more prescriptions would cost us around $20/year to covert to packaging Estimated that each new clinic Medicaid patient is worth the cost of around 870 packages/cards
92 Targeting Exercise: Questions for Clinic What can we do to help you? Adherence packaging? 28 vs 30 day supply packages? Increasing communication with the pharmacy? Reporting back on dispensing, refill status, adherence, clinical markers, etc? Would extra patient monitoring post-visit help? PHQs, waist circumference, weight, blood glucose, 7,14,28 day package pickup/delivery to increase touch points, etc? Patient bring in package to office visit? Suggestions?
93 Targeting Exercise: Secondary Solutions Medication Reconciliation 28 vs 30 day dispensing Consolidation of medication + home visit Coordinate & communicate with clinic & PCPs Patient Health Questionnaire PHQ2 used on previous project to target depression in DM and could be used here PHQ9 could be used if preferred Metabolic monitoring Waist circumference Weight BG checks Medicaid MTM Interventions Standardized reporting back to Clinic after assessment and medication is delivered Referrals to Clinic for at risk patients not currently receiving mental health care
94 Targeting Exercise: ROI Held meetings with administrator for clinic needs assessment and pharmacy service detailing Hosted in service for case managers to detail pharmacy services Immediately began receiving referrals from case managers for packaging, care coordination, and other pharmacy services Prescription volume & referrals from target clinic and target payer increased Ongoing communication with clinic exploring new collaboration opportunities, despite clinic opening an on site pharmacy
95 Payer Programs: ROI? Is the program Pay for Performance or Pay to Play? Is it the program an Incentive Program or a Penalty Program? Are the metrics movable? Is the workflow process achievable and sustainable? Is the program in the best interest of your target patients? Will the program bring you patients? Revenue? Volume? Marketing? Is the Rx volume worth the investment with this payer? Is the program worth investing time, money, and valuable resources?


96 ROI: The Payers Themselves Began by looking at the payers themselves BEFORE we looked at their programs. Specifically looked at: Average margin per Rx Average DIR per Rx Our pharmacy s cost to dispense Average annual Rx volume per Rx Determined which plans had patients we wanted more of, and which plans we were losing money on. Created a list of positive ROI partners and poor ROI partners


 are")
97 ROI: Payer Programs Examples: 90 day supply conversion FFS Traditional Medicare Part D FFS Medication Therapy Management Medicare Part D adherence interventions through MTM vendors Medicare Part D performance program using health plan quality metrics Per member per month disease state management programs Enhanced MTM opportunities, Chronic Care Management, Etc. Patient attribution for enhanced pharmacy services Drug Manufacturers (PHARMA) are becoming payers Currently LOTS of innovation and experimentation in this space!!!!
98 Payer Strategies There is more value in hitting the measure's star rebate level, than a focus on the medical cost reduction -Medicare Part D Plan Executive, August 2017

99 Pharmacy Strategies Claims Based Fill reminders Med sync Fill gaps in care Medication safety CMR Packaging Days supply DIR reduction Patient Based Copay assistance Medication access Transition of care Health literacy/social Care coordination Transportation Education Empathy
100 Positive ROI: Current & Future Examples: Outcomes based programs, contracts, and collaboration opportunities A1C, BP, Lipids, Asthma, Admissions, Readmissions, CHF, etc Drug manufacturer programs Surveys, trainings, education, etc. Medicare Part D programs BEYOND claims based metrics Admissions per 1000, ER visits/1000, Complaints to Medicare, $PMPM (medical & drug), etc. Community Pharmacy Enhanced Service Network expansion The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) Risk sharing with Health Systems & Hospitals No one knows what the future holds is it Amazon?


101 Good Investments Are Typically: Good for Prescriber Good for Employers Good for Third Parties Good for Pharmacy Staff Good for Pharmacy Good for Patients
102 Tripp Logan, Pharm.D. L & S Pharmacy tlogan@semorx.com
103 Making Connections, Developing Your Brand Enhanced Services Boot Camp Jay Williams CPESN USA
104 Objectives Articulate your pharmacy elevator speech. Create a plan to build relationships with other health care professionals in your area that can lead to opportunities for your pharmacy.
105 Importance of a Marketing Strategy Why should you invest the time? Articulate your brand clearly and consistently Assess your uniqueness Manage a clear set of marketing deliverables
106 Elements of a Successful Strategy 1. Identify your target groups 2. Create your brand position 3. Take action

107 1. Identify Your Target Groups 1. Group targets by characteristics not job titles Example: Physicians in Dublin, Ohio verses Plain City, Ohio 2. Understand targets based on their needs/desires Example: Care Managers typically have homebound patients, so pharmacies that deliver are needed 3. Create a Message Map


108 Attract Your Ideal Patient Identify your ideal patient Lure the ideal patient into your store Create a retention strategy to keep ideal patients

109 Target Groups The aim of marketing is to know and understand the customer so well that the product or service fits and sells itself. Peter Drucker


110 2. Create Your Brand Position
111 2. Create Your Brand Position 1. Consider the needs of all target groups 2. Create your key messages 3. Evaluate your Brand Strength How well does it resonate with your target groups? How different is it from your competition s position?

112 SWOT Analysis Strengths Weaknesses Opportunities Threats

113 Create Your Key Messages



114 Gallup Poll 2016

115 J.D. Power 2016 Independents were #1 overall Independents were #1 in 4 out of 5 categories
116 Boehringer Ingleheim 2013 Independents were rated #1 overall #1 in Pharmacist Engagement, Pharmacy Staff

117 Consumer Reports 2016 Independents* were rated #1 overall * Non-Medicine Shoppe Independents #1 in Personalized Service among others
118 Physician Messaging Be responsive to immediate needs Help foster medication adherence Make it easier to manage complicated patients Keep it simple

119 Messages that Resonate
120 Payer Messaging One size does not fit all Listen to (and understand) the payer s pain points Emphasize your situational adaptability & readiness Be prepared with an ask

121 Messages that Resonate

122 Messaging "People don't buy what you do. They buy why you do it. Simon Sinek
123 3. Take Action 1. Build your brand 2. Create a Strategy on a Page 1. Simple, easy-to-draft, easy-to-implement document 2. Establish clear deliverables for your teams 3. Test effectiveness, evaluate, then try new approaches 3. Try and try again
124 Build Your Brand 1. Focus on everything you do 2. Train and retrain team members 3. Be consistent!

125 Brand A brand for a company is like a reputation for a person. You earn a reputation by trying to do hard things well. Jeff Bezos
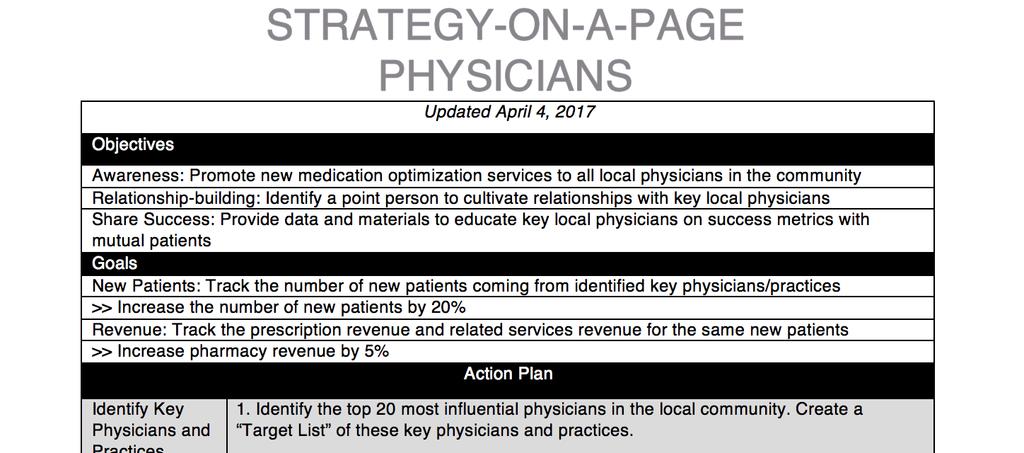
126 Strategy-on-a-Page

127 Taking Action/Risks There are risks and costs to action. But they are far less than the long range risks of comfortable inaction. John F. Kennedy

128 Taking Action/Risks The biggest risk is not taking any risk... In a world that changing really quickly, the only strategy that is guaranteed to fail is not taking risks. Mark Zuckerberg


129 Summary 1. Identify your target audiences 2. Create your brand position 3. Take action!
130 Jay Williams CPESN USA
131 How to Make It Work: Billing for Services in Tennessee Enhanced Services Boot Camp Micah Cost, Pharm.D., Tennessee Pharmacists Association Jacqueline Woeppel, TennCare
132 Objectives Describe the pharmacist payment structure within the TennCare program. Outline a plan for incorporating this new opportunity into the community pharmacy setting.
133 Micah Cost, Pharm.D. Tennessee Pharmacists Association
134 Update on Chronic Care Management: Opportunities and Challenges Enhanced Services Boot Camp Aaron Garst, Pharm.D. Seamless Healthcare PLLC
135 Objectives Discuss chronic care management and transitional care management opportunities for revenue in delivering clinical pharmacy services. Demonstrate how businesses are able to implement these programs while remaining profitable.
136 Chronic Care Management (CCM) Non-face-to-face, time-based services Billing Code Payment Clinical Staff Time Billing Practitioner Work $43 20 minutes Ongoing oversight, direction and management $94 60 minutes +moderate-high complexity $ minutes +moderate-high complexity G0506 $64 N/A Personally performs extensive assessment and CCM care planning beyond the usual effort described by the separately billable CCM initiating visit Initiating Visit $ Face-to-face work required by the initiating visit code
")
137 Evaluation of a Collaborative Pharmacy Practice Model for Community Pharmacist- Provided Chronic Care Management (CCM) Services

138 Med Review Physician Visit Care Plan Unnecessary Referrals CCM Call
139 Results Pharmacist-Provided Medication Reconciliation and CCM Services Insurance Patients Seen Enrolled Declined Enrollment % Reimbursed Medicare Only % 5 Medicare w/ Supplement % 15 Dual Eligible % 3 Total % 23
140 Final Thoughts Community pharmacists should consider a Hybrid Collaborative Pharmacy Practice (HCPP) model Must ensure the ability to provide billable services at the physician s office Focus on providing CCM services with primary care practices instead of specialists Insist on receiving at least the amount paid by Medicare (i.e. 80% of the billable code) and let the practice manage copay collection
141 Community Pharmacy Foundation (CPF) Synopsis and Toolkit on CPF website What s Next? Implementation of a Hybrid Collaborative Pharmacy Practice (HCPP) Model with Community Pharmacies Utilizing Technician Product Verification (TPV) Workflow Selection of at least two, but not more than seven, CPhT pilot project sites to receive additional support in establishing a HCPP model of care
142 Aaron Garst, PharmD Owner, Seamless Healthcare PLLC
143 Aaron Garst, Pharm.D. Tennessee Pharmacists Association
144 Community Pharmacy Enhanced Services Networks Enhanced Services Boot Camp Ashley Branham, Pharm.D. & Joe Moose, Pharm.D. CPESN USA and Moose Pharmacy
145 Objectives Discuss common characteristics of pharmacies in a community pharmacy enhanced service network Discuss the role of community pharmacy in providing medication management resources to the highest risk populations. Describe how pharmacies are positioning themselves to integrate with care teams to lower health care costs and participate in new models of care and reimbursement.


146 Healthcare Spend in in America Medication/Pharmacy Spend Medication/Pharmacy Spend 10% 10% Medical/Non-Pharmacy Spend Medical/Non-Pharmacy Spend 90%


147 Threats to Community Pharmacy

148 Patient Access
149 Strategic Considerations for Community- Based Pharmacy Networks History of NC CPESN Model Overview of States with CPESN Development Underway
150 How did Community Pharmacy Enhanced Services Networks Begin? Goal: Create a network of community pharmacies who are willing to provide enhanced services and coordinate care with the broader care team Started in January 2014 with official network launch in April 2014 Open network which includes ~ 280 North Carolina community-based pharmacies Confidential Do not reproduce or reuse without consent.
151 Types of Enhanced Services Medication Synchronization Adherence Packaging Home Delivery Home Visits Point-of-Care Testing Collection of Vital Signs Nutritional Counseling Smoking Cessation Compounding Long-Acting Injections 24-Hour Emergency Services Multi-Lingual Capabilities

152 CPESN Network Structure


153 Clinically Integrated Network Pharmacy Benefit Payer

154 Building a Network of Networks
155 Minimum CPESN Network Service Set Comprehensive Medication Reviews A systemic assessment of medications, including prescription, over-the-counter, herbal medications and dietary supplements to identify medication-related problems, prioritize a list of medication therapy problems and create a patient-specific plan to resolve medication therapy problems working with the extended healthcare team. Medication Synchronization Program Aligning a patient s routine medications to be filled at the same time each month. The pharmacists will provide clinical medication management and monitoring for progression toward desired therapeutic goals during the patient appointment at time of medication pick-up or delivery.
156 Minimum CPESN Network Service Set Immunizations- Act of screening patients for ACIP recommended immunizations, educate patients about needed immunizations and administer immunizations when appropriate. Medication Reconciliation- The process of comparing a patient s medication orders to all of the medications that the patient has been taking (active, chronic, as needed and OTC including herbal) to avoid medication errors. This service is especially important during transitions of care when patients are most vulnerable to medication errors or mishaps. Personal Medication Record- Ability to create a comprehensive list of current patient medications manually or from dispensing software
 Home Delivery Immunizations In-Depth Counseling/Coaching Medication Synchronization Program Personal Medication Record Medication")
157 CPESN Tennessee Minimum Requirements Adherence Packaging & Counseling Collection of Vital Signs Comprehensive Medication Review (10 step process) Home Delivery Immunizations In-Depth Counseling/Coaching Medication Synchronization Program Personal Medication Record Medication Reconciliation
158 The Big Picture Form a nationwide Network of Networks Increase, develop and sustain Networks of high performing pharmacies that provide enhanced services Create a marketplace presence of & dependency on CPESN networks Facilitate local value propositions to other care team members to establish positive referral patterns Establish relationships and reimbursement models with the Medical Benefit side of payer infrastructure
159 CPESN USA A Network of Networks CPESN USA will focus on providing services and solutions to the local network where scale and aggregation make the most sense 3 Main Areas of Support: Subject Matter Expertise & Network Consultation Value Expression & Marketing Support Quality Assurance & Best Practice Identification
160 Deployment of the CPESN Model Care Team Integration Pharmacy ecare Plan

161 The Health Care System with Convenience Care vs. Chronic Care / CPESN Pharmacies Confidential Do not reproduce or reuse without consent.
162 Care Team Collaboration Joint home visits may be a way to establish a coordinated care plan for complex patients Pharmacies can assist care managers with patient engagement and longitudinal management Care managers and CPESN pharmacies can work together to address: Barriers preventing optional medication adherence Health literacy challenges, cognitive deficits, or lack of caregiver support that require pill box fills, special packaging, or special labeling Other specialized medication-related needs that could be fulfilled by a CPESN pharmacy Patient understanding of special instructions for administration or storage
163 Opportunity for Pharmacies Today Typical Referred Patient: 10 Rx/Pt/Month Estimated Profit per Rx: ~$10 How it Breaks Down: patients/day referred to NC CPESN ~$1200/patient/year X 200 patients =
164 Opportunity for Pharmacies Today Typical Referred Patient: 10 Rx/Patient/Month Estimated Profit per Rx: ~$10 How it Breaks Down: patients/day referred to NC CPESN ~$1200/patient/year X 200 patients = $240,000 in annual net profit per day
165 Pharmacist ecare Plan Goal of the Project: Create a new standard for electronic pharmacist care plans called Pharmacist Care Plan which is a further constraint on a standard in the Interoperability Standards Advisory. Integrate the pharmacist care plan into coordination efforts for patient care across the health continuum.
166 Group III Group II Group I Pharmacist ecare Plans Pharmacist ecare Plans are essential to quality assurance, quality improvement and Clinically Integrated Networks status. Vendors that are now certifying:
167 What Makes the CPESN Model Different? Community-based pharmacies that focus on high risk patients in a chronic care model Patient targeting Panel management Patients instead of prescriptions Accountability on global outcomes and quality Shared metrics with the rest of the care team Local care team integration and care coordination Change packages and network support to enable practice transformation Workflow changes related to panel management, care team integration, and weaving together clinical components with enhanced services Approach to HIT Pharmacist ecare Plans Confidential Do not reproduce or reuse without consent.
168 Lessons Learned Network Size: A SMALL, HIGHLY ENGAGED AND HIGH-PERFORMING NETWORK is better than a larger network with variable quality. Workflow: Enhanced services and Community Pharmacy Care Management MUST BE INTEGRATED INTO WORKFLOW FOR EFFECTIVE, EFFICIENT DEPLOYMENT; this includes HIT and efforts to coordinate with the care team Staff Engagement: CPESN concepts, including Community Pharmacy Care Management, are TRANSFORMATIONAL CHANGES in the way the pharmacy operates THAT REQUIRE A CULTURE SHIFT. To be successful, ALL STAFF SHOULD BE TRAINED AND ENGAGED.
169 ings Newsroom Innovation Center LTC s Pharmacy Assessment Survey Tool Join/Renew 018 Pharmacy Self-Assessment

170 Ashley Branham, PharmD CPESN USA Joe Moose, PharmD CPESN USA
171
Workflow Best Practices. Ashley Branham, PharmD, BCACP Bri Morris, PharmD
 Workflow Best Practices Ashley Branham, PharmD, BCACP Bri Morris, PharmD Disclosures Ashley Branham is receiving an honorarium for this program. The conflict of interest was resolved by peer review of
Workflow Best Practices Ashley Branham, PharmD, BCACP Bri Morris, PharmD Disclosures Ashley Branham is receiving an honorarium for this program. The conflict of interest was resolved by peer review of
Dimmy Sokhal, PharmD 9/28/2016. Clinical Pharmacist, Hayat Pharmacy. Building Enhanced Services into Your Existing Medication Synchronization Program
 Building Enhanced Services into Your Existing Medication Synchronization Program Sponsored by Merck Dimmy Sokhal, PharmD Laura Patterson, PharmD Amina Abubakar, PharmD Dimmy Sokhal, PharmD Clinical Pharmacist,
Building Enhanced Services into Your Existing Medication Synchronization Program Sponsored by Merck Dimmy Sokhal, PharmD Laura Patterson, PharmD Amina Abubakar, PharmD Dimmy Sokhal, PharmD Clinical Pharmacist,
Clinical Service Networks Re-Engineering Your Pharmacy Practice Bootcamp August 13, 2016
 Clinical Service Networks Re-Engineering Your Pharmacy Practice Bootcamp August 13, 2016 Ashley Branham, PharmD, BCACP Joe Moose, PharmD Disclosures Ashley Branham is receiving an honorarium for this program.
Clinical Service Networks Re-Engineering Your Pharmacy Practice Bootcamp August 13, 2016 Ashley Branham, PharmD, BCACP Joe Moose, PharmD Disclosures Ashley Branham is receiving an honorarium for this program.
Leading By Example. Begin with a vision. Disclosures. Learning Objectives 3/25/2017. Tripp Logan, PharmD
 Leading By Example Melissa Somma McGivney, PharmD, FAPhA, FCCP Associate Dean for Community Partnerships; Associate Professor University of Pittsburgh Tripp Logan, PharmD Senior Quality Consultant - MedHere
Leading By Example Melissa Somma McGivney, PharmD, FAPhA, FCCP Associate Dean for Community Partnerships; Associate Professor University of Pittsburgh Tripp Logan, PharmD Senior Quality Consultant - MedHere
Pharmacists Improve Care Through Team Collaboration
 Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Pharmacists Improve Care Through Team Collaboration Trista Pfeiffenberger, PharmD, MS Director, Network Pharmacy Programs Community Care of North Carolina Disclosure and Conflict of Interest I am an employee
Keenan Pharmacy Care Management (KPCM)
") Keenan Pharmacy Care Management (KPCM) This program is an exclusive to KPS clients as an additional layer of pharmacy benefit management by engaging physicians and members directly to ensure that the best
Keenan Pharmacy Care Management (KPCM) This program is an exclusive to KPS clients as an additional layer of pharmacy benefit management by engaging physicians and members directly to ensure that the best
Synergy Through Integration:
 WHITEPAPER Synergy Through Integration: Complementary Roles of MTM and Medication Synchronization With the myriad of strategies aimed at reforming our nation s healthcare system receiving mixed results,
WHITEPAPER Synergy Through Integration: Complementary Roles of MTM and Medication Synchronization With the myriad of strategies aimed at reforming our nation s healthcare system receiving mixed results,
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Yes You Can! How Community Pharmacies Have Profitably Implemented Enhanced Care Services. Introduction
 Yes You Can! How Community Pharmacies Have Profitably Implemented Enhanced Care Services Bruce Kneeland June 30, 2018 Introduction The Road Trip Guy 1 Disclosure Bruce Kneeland is the Community Pharmacy
Yes You Can! How Community Pharmacies Have Profitably Implemented Enhanced Care Services Bruce Kneeland June 30, 2018 Introduction The Road Trip Guy 1 Disclosure Bruce Kneeland is the Community Pharmacy
ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, :00 5:00 PM
 ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, 2017 3:00 5:00 PM ACPE UAN: 0107-9999-17-105-L04-P 0.2 CEU/2.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon
ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, 2017 3:00 5:00 PM ACPE UAN: 0107-9999-17-105-L04-P 0.2 CEU/2.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon
Pharmacy Quality Measures: What They Are and How Community Pharmacies Can Impact Them in Their Practice
 Pharmacy Quality Measures: What They Are and How Community Pharmacies Can Impact Them in Their Practice Zac Renfro, PharmD, Pharmacy Quality Consultant Pharmacy Quality Solutions Disclosure and Conflict
Pharmacy Quality Measures: What They Are and How Community Pharmacies Can Impact Them in Their Practice Zac Renfro, PharmD, Pharmacy Quality Consultant Pharmacy Quality Solutions Disclosure and Conflict
Pharmacy Operations Manual
 Pharmacy Operations Manual Version 1.5 (February 2018) Copyright 2018. National Community Pharmacists Association (NCPA). All rights reserved. Summary This manual provides pharmacists with the tools necessary
Pharmacy Operations Manual Version 1.5 (February 2018) Copyright 2018. National Community Pharmacists Association (NCPA). All rights reserved. Summary This manual provides pharmacists with the tools necessary
Jake Olson, PharmD 9/28/2016. Improving Patient Care Through Improved Pharmacist-Prescriber Relationships. President/CEO, Skywalk Pharmacy
 Improving Patient Care Through Improved Pharmacist-Prescriber Relationships Sponsored by Merck Jake Olson, PharmD Hamid Abbaspour, RPh, MBA Amanda Faber, PharmD, MBA Briana P. Murray, PharmD Jake Olson,
Improving Patient Care Through Improved Pharmacist-Prescriber Relationships Sponsored by Merck Jake Olson, PharmD Hamid Abbaspour, RPh, MBA Amanda Faber, PharmD, MBA Briana P. Murray, PharmD Jake Olson,
Enhance Your Pharmacy Performance Performance Tips from a Fellow Good Neighbor Pharmacy Owner
 Enhance Your Pharmacy Performance Performance Tips from a Fellow Good Neighbor Pharmacy Owner Series 4 Medication Therapy Management: An Opportunity to Engage Presented By Jason Turner, PharmD Moundsville
Enhance Your Pharmacy Performance Performance Tips from a Fellow Good Neighbor Pharmacy Owner Series 4 Medication Therapy Management: An Opportunity to Engage Presented By Jason Turner, PharmD Moundsville
Objectives. Medication Therapy Management: The Important Role of the Pharmacy Technician. Medication Therapy Management (MTM)
") Medication Therapy Management: The Important Role of the Pharmacy Technician Nancy Myers, PharmD, MBA, BCPS, CDE Katrina Harper, PharmD, MBA Objectives Define Medication Therapy Management () and its Core
Medication Therapy Management: The Important Role of the Pharmacy Technician Nancy Myers, PharmD, MBA, BCPS, CDE Katrina Harper, PharmD, MBA Objectives Define Medication Therapy Management () and its Core
The New Frontier: Value- Based Payment Models
 The New Frontier: Value- Based Payment Models Target Audience: Pharmacists and Pharmacy Technicians ACPE#: 0202-0000-18-026-L04-P/T Activity Type: Knowledge-based Target Audience: ACPE#: Activity Type:
The New Frontier: Value- Based Payment Models Target Audience: Pharmacists and Pharmacy Technicians ACPE#: 0202-0000-18-026-L04-P/T Activity Type: Knowledge-based Target Audience: ACPE#: Activity Type:
NAVIGATING THE BILLING MAZE: THE BASICS OF MEDICARE PART B BILLING JULY 13, :00 10:00 AM
 NAVIGATING THE BILLING MAZE: THE BASICS OF MEDICARE PART B BILLING JULY 13, 2017 9:00 10:00 AM ACPE UAN: 0107-9999-17-079-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
NAVIGATING THE BILLING MAZE: THE BASICS OF MEDICARE PART B BILLING JULY 13, 2017 9:00 10:00 AM ACPE UAN: 0107-9999-17-079-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
8/28/18. "Organizing Pharmacy to Prepare for Payment Reform" Disclosure and Conflict of Interest
 "Organizing Pharmacy to Prepare for Payment Reform" Troy Trygstad, PharmD MBA PhD VP, Pharmacy and Provider Partnerships Community Care of North Carolina Executive Director CPESN USA, LLC Disclosure and
"Organizing Pharmacy to Prepare for Payment Reform" Troy Trygstad, PharmD MBA PhD VP, Pharmacy and Provider Partnerships Community Care of North Carolina Executive Director CPESN USA, LLC Disclosure and
INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE
 INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE ACPE UAN: 0107-9999-17-101-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon completion
INTEGRATING CHRONIC CARE MANAGEMENT INTO COMMUNITY PHARMACY PRACTICE ACPE UAN: 0107-9999-17-101-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon completion
Pharmacy s Appointment Based Model. Implementation Guide for Pharmacy Practices
 Pharmacy s Appointment Based Model Implementation Guide for Pharmacy Practices Pharmacy s Appointment Based Model Implementation Guide for Pharmacy Practice Module XX Authors Lindsay L. Watson, PharmD
Pharmacy s Appointment Based Model Implementation Guide for Pharmacy Practices Pharmacy s Appointment Based Model Implementation Guide for Pharmacy Practice Module XX Authors Lindsay L. Watson, PharmD
Patient Centric Model (PCM)
") Patient Centric Model (PCM) Operations Manual A product of your state pharmacy association For more information, contact: PCM Project Manager 804-285-4431 PCM@naspa.us Background The typical pharmacy model
Patient Centric Model (PCM) Operations Manual A product of your state pharmacy association For more information, contact: PCM Project Manager 804-285-4431 PCM@naspa.us Background The typical pharmacy model
CPhT Program Recognition Attestation Form
 About this Form Beginning in 2020, CPhT applicants must have completed a PTCB-recognized education/training program or have equivalent work experience in order to be eligible for certification. The purpose
About this Form Beginning in 2020, CPhT applicants must have completed a PTCB-recognized education/training program or have equivalent work experience in order to be eligible for certification. The purpose
3 Ways to Increase Patient Visits
 3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
Connecticut Department of Public Health and Community Pharmacists Medication Management Services
 Connecticut Department of Public Health and Community Pharmacists Medication Management Services MODERATOR: Marie Smith, PharmD Palmer Professor and Assistant Dean, Practice and Public Policy Partnerships,
Connecticut Department of Public Health and Community Pharmacists Medication Management Services MODERATOR: Marie Smith, PharmD Palmer Professor and Assistant Dean, Practice and Public Policy Partnerships,
10/10/2017. Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP
 Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP") Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
CEOCFO Magazine. Andy Reeves, RPh Chief Executive Officer OptiMed Specialty Pharmacy
 CEOCFO Magazine ceocfointerviews.com All rights reserved! Issue: October 30, 2017 Q&A with Andy Reeves, RPh, CEO of OptiMed Specialty Pharmacy, a National Specialty and Infusion Pharmacy dedicated to Managing
CEOCFO Magazine ceocfointerviews.com All rights reserved! Issue: October 30, 2017 Q&A with Andy Reeves, RPh, CEO of OptiMed Specialty Pharmacy, a National Specialty and Infusion Pharmacy dedicated to Managing
Success of an MTM Program Beyond Medicare Part D: Is It Really a Pharmacy Pay for Performance Model? Jim Gartner RPh, MBA CareSource
 Success of an MTM Program Beyond Medicare Part D: Is It Really a Pharmacy Pay for Performance Model? Jim Gartner RPh, MBA CareSource 10 28 2014 Learning Objectives Understand why a health plan would want
Success of an MTM Program Beyond Medicare Part D: Is It Really a Pharmacy Pay for Performance Model? Jim Gartner RPh, MBA CareSource 10 28 2014 Learning Objectives Understand why a health plan would want
eprescribing Information to Improve Medication Adherence
 eprescribing Information to Improve Medication Adherence April 2017 (revised) About Point-of-Care Partners Executive Summary Point-of-Care Partners (POCP) is a leading management consulting firm assisting
eprescribing Information to Improve Medication Adherence April 2017 (revised) About Point-of-Care Partners Executive Summary Point-of-Care Partners (POCP) is a leading management consulting firm assisting
Page 2 of 29 Questions? Call
 Revised 7.29.2018 Contents Introduction. 3 OutcomesMTM Participation.. 3 User Access to Protected Health Information (PHI) 3 Participation from Various Settings..3 Retail 3 LTC/Assisted Living 3 Ambulatory
Revised 7.29.2018 Contents Introduction. 3 OutcomesMTM Participation.. 3 User Access to Protected Health Information (PHI) 3 Participation from Various Settings..3 Retail 3 LTC/Assisted Living 3 Ambulatory
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
Medication Management Services in Connecticut
 Medication Management Services in Connecticut Connecticut Department of Public Health, UConn School of Pharmacy and Community Pharmacies Mehul Dalal, MD, MSc, MHS - Chronic Disease Director, CT Department
Medication Management Services in Connecticut Connecticut Department of Public Health, UConn School of Pharmacy and Community Pharmacies Mehul Dalal, MD, MSc, MHS - Chronic Disease Director, CT Department
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
The Future of Pharmacy. Troy Trygstad NYSCHP Saturday April 21st, 2018
 The Future of Pharmacy Troy Trygstad NYSCHP Saturday April 21st, 2018 The Future of Pharmacy (objectives) Objectives 1. Describe the Essential Care Process Elements for Effective Population Management
The Future of Pharmacy Troy Trygstad NYSCHP Saturday April 21st, 2018 The Future of Pharmacy (objectives) Objectives 1. Describe the Essential Care Process Elements for Effective Population Management
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project
 Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care
 Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care Introduction This white paper examines how new technologies are creating a fully connected point of care
Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care Introduction This white paper examines how new technologies are creating a fully connected point of care
Specialty Pharmacy How is Traditional Pharmacy Practice Positioned
 Specialty Pharmacy How is Traditional Pharmacy Practice Positioned Nick Calla Vice President, Industry Relations Cardinal Health Specialty Solutions August 19, 2016 Today s Learning Objectives Understand
Specialty Pharmacy How is Traditional Pharmacy Practice Positioned Nick Calla Vice President, Industry Relations Cardinal Health Specialty Solutions August 19, 2016 Today s Learning Objectives Understand
38 May June 2014 OI
 38 www.accc-cancer.org May June 2014 OI BY MICHAEL J. REFF, RPH, MBA Physician Dispensing Adding value to patients and the practice While oral oncolytics are serious medications prescribed to help patients
38 www.accc-cancer.org May June 2014 OI BY MICHAEL J. REFF, RPH, MBA Physician Dispensing Adding value to patients and the practice While oral oncolytics are serious medications prescribed to help patients
Medication Adherence: Strategies for Improving Outcomes
 Medication Adherence: Strategies for Improving Outcomes Thursday, June 16, 2016, 12:00 p.m. to 1:00 p.m. Andrea H. Williams, RPh, MBA President, RX CONSULTANTS LLC, Wilmington, DE EDUCATIONAL OBJECTIVES
Medication Adherence: Strategies for Improving Outcomes Thursday, June 16, 2016, 12:00 p.m. to 1:00 p.m. Andrea H. Williams, RPh, MBA President, RX CONSULTANTS LLC, Wilmington, DE EDUCATIONAL OBJECTIVES
Evaluation of Pharmacy Delivery Models
 Evaluation of Pharmacy Delivery Models As Required By House Bill 1, 84th Legislature, Regular Session, 2015 (Article II, Health and Human Services Commission, Rider 83) Health and Human Services Commission
Evaluation of Pharmacy Delivery Models As Required By House Bill 1, 84th Legislature, Regular Session, 2015 (Article II, Health and Human Services Commission, Rider 83) Health and Human Services Commission
Partnering with Pharmacists to Enhance Medication Management
 Partnering with Pharmacists to Enhance Medication Management Tamara Ravn PharmD BCACP Staff Pharmacist Clinical Cancer Pharmacy Froedtert & The Medical College of Wisconsin April 6, 2016 Objectives Describe
Partnering with Pharmacists to Enhance Medication Management Tamara Ravn PharmD BCACP Staff Pharmacist Clinical Cancer Pharmacy Froedtert & The Medical College of Wisconsin April 6, 2016 Objectives Describe
Medication Therapy Management
 Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Piedmont Access to Health Services. Standing Orders for Patient Work-ups
 Piedmont Access to Health Services Policy Number: 01-09-014 SUBJECT: Standing Orders for Patient Work-ups EFFECTIVE DATE: 8/3/09 REVIEWED/REVISED : 4/10/2012 POLICY: PATHS is committed to allowing each
Piedmont Access to Health Services Policy Number: 01-09-014 SUBJECT: Standing Orders for Patient Work-ups EFFECTIVE DATE: 8/3/09 REVIEWED/REVISED : 4/10/2012 POLICY: PATHS is committed to allowing each
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Falcon Quality Payment Program Checklist- 2017
 Falcon Quality Payment Program Checklist- 2017 DISCLAIMER: This material is provided for informational purposes only and should not be relied upon as legal or compliance advice. If legal advice or other
Falcon Quality Payment Program Checklist- 2017 DISCLAIMER: This material is provided for informational purposes only and should not be relied upon as legal or compliance advice. If legal advice or other
Draft 2014 CMS Advanced Notice and Call Letter to Medicare Advantage and Part D Prescription Drug Plans
 Jonathan Blum Center for Medicare Center for Medicare and Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, SW, MS:314G Washington, DC 20201 [Submitted electronically to: AdvanceNotice2014@cms.hhs.gov]
Jonathan Blum Center for Medicare Center for Medicare and Medicaid Services Hubert H. Humphrey Building 200 Independence Avenue, SW, MS:314G Washington, DC 20201 [Submitted electronically to: AdvanceNotice2014@cms.hhs.gov]
Emerging Opportunities: Pharmacy Care. NACDS Total Store Expo August 20, 2017
 Emerging Opportunities: Pharmacy Care NACDS Total Store Expo August 20, 2017 Presentation Objectives Current value based healthcare landscape Medication management as a critical component to achieve value
Emerging Opportunities: Pharmacy Care NACDS Total Store Expo August 20, 2017 Presentation Objectives Current value based healthcare landscape Medication management as a critical component to achieve value
PHCY 471 Community IPPE. Student Name. Supervising Preceptor Name(s)
") PRECEPTOR CHECKLIST /SIGN-OFF PHCY 471 Community IPPE Student Name Supervising Name(s) INSTRUCTIONS The following table outlines the primary learning goals and activities for the Community IPPE. Each student
PRECEPTOR CHECKLIST /SIGN-OFF PHCY 471 Community IPPE Student Name Supervising Name(s) INSTRUCTIONS The following table outlines the primary learning goals and activities for the Community IPPE. Each student
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model. ACO Congress November 5, 2013 Charles Kennedy
 Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
UPDATE ON MEANINGFUL USE. HITECH Stimulus Act of 2009: CSC Point of View
 HITECH Stimulus Act of 2009: CSC Point of View UPDATE ON MEANINGFUL USE Introduction The HITECH provisions of the American Recovery and Reinvestment Act of 2009 provide a commanding $36 billion dollars
HITECH Stimulus Act of 2009: CSC Point of View UPDATE ON MEANINGFUL USE Introduction The HITECH provisions of the American Recovery and Reinvestment Act of 2009 provide a commanding $36 billion dollars
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
The Pharmacist s Role in Reducing Readmissions
 The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
The Pharmacist s Role in Reducing Readmissions John Vinson, Pharm.D. UAMS West Family Medical Center Fort Smith, Arkansas Assistant Professor Co-Chair Clinical Leadership Committee UAMS Regional Programs
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
Medication Therapy Management (MTM) Solution
 Solution") Medication Therapy Management (MTM) Solution Service Overview Updated 5.5.16 Congratulations on your decision to partner with Cardinal Health to help ensure that your patients receive beneficial Medication
Medication Therapy Management (MTM) Solution Service Overview Updated 5.5.16 Congratulations on your decision to partner with Cardinal Health to help ensure that your patients receive beneficial Medication
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care
 Includes Suggestions for Leveraging Improved BP Measurements to Achieve Quality Metrics Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care Introduction This
Includes Suggestions for Leveraging Improved BP Measurements to Achieve Quality Metrics Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care Introduction This
Medication Synchronization Change Package
 Medication Synchronization Change Package December 2017 Project Lead: Stefanie Ferreri, PharmD, CDE, BCACP, FAPhA Funding Opportunity Notice: The project described was supported by Grant Number 1C1CMS331338
Medication Synchronization Change Package December 2017 Project Lead: Stefanie Ferreri, PharmD, CDE, BCACP, FAPhA Funding Opportunity Notice: The project described was supported by Grant Number 1C1CMS331338
Administrators. Medical Directors. 61% The negative impact on our hospital-based program s. 44% We will need to consider the most appropriate or most
 2016 This annual survey, which began in 2009, provides key insight into nationwide developments in the business of cancer care. To better capture information from its multidisciplinary membership, this
2016 This annual survey, which began in 2009, provides key insight into nationwide developments in the business of cancer care. To better capture information from its multidisciplinary membership, this
Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population
 Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population Marie Smith, PharmD UConn School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists Association 4th National Medicaid Congress
Enhancing E Prescribing and Medication Adherence in the CT Medicaid Population Marie Smith, PharmD UConn School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists Association 4th National Medicaid Congress
A PRIMER ON MEDICATION SYNCHRONIZATION JULY 14, :45 8:45 AM
 A PRIMER ON MEDICATION SYNCHRONIZATION JULY 14, 2017 7:45 8:45 AM ACPE UAN: 0107-9999-17-085-L04-P 0.1 CEU/1.0 hr 0107-9999-17-085-LO4-T 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives
A PRIMER ON MEDICATION SYNCHRONIZATION JULY 14, 2017 7:45 8:45 AM ACPE UAN: 0107-9999-17-085-L04-P 0.1 CEU/1.0 hr 0107-9999-17-085-LO4-T 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
We Simplify Medication Management
 The Dose We Simplify Medication Management November 2016 Moving Forward with Marketing Wow, hello November! The air is cooler and leaves are beginning to fall. As we wrap up the current year and look
The Dose We Simplify Medication Management November 2016 Moving Forward with Marketing Wow, hello November! The air is cooler and leaves are beginning to fall. As we wrap up the current year and look
The Role of Pharmacy Technician in Patient Care Services
 By: Wendy Mobley-Bukstein PharmD, CDE Assistant Professor of Pharmacy Practice Drake University College of Pharmacy and Health Sciences Dr. Wendy Mobley-Bukstein PharmD is Assistant Professor of Pharmacy
By: Wendy Mobley-Bukstein PharmD, CDE Assistant Professor of Pharmacy Practice Drake University College of Pharmacy and Health Sciences Dr. Wendy Mobley-Bukstein PharmD is Assistant Professor of Pharmacy
LSU First & WebTPA: Working Together
 LSU First & WebTPA: Working Together 2016 LSU First Health Plan Changes 2016 LSU First Health Plan Changes New ID Card Specialty drug copay $150 90 day timely filing period (medical and pharmacy) Home
LSU First & WebTPA: Working Together 2016 LSU First Health Plan Changes 2016 LSU First Health Plan Changes New ID Card Specialty drug copay $150 90 day timely filing period (medical and pharmacy) Home
PBM SOLUTIONS FOR PATIENTS AND PAYERS
 PBM SOLUTIONS FOR PATIENTS AND PAYERS Reducing Prescription Drug Costs Designing Solutions for Employers, Unions, and Government Programs Delivering High Patient Satisfaction and Improved Outcomes Improving
PBM SOLUTIONS FOR PATIENTS AND PAYERS Reducing Prescription Drug Costs Designing Solutions for Employers, Unions, and Government Programs Delivering High Patient Satisfaction and Improved Outcomes Improving
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
2017 Oncology Insights
 Cardinal Health Specialty Solutions 2017 Oncology Insights Views on Reimbursement, Access and Data from Specialty Physicians Nationwide A message from the President Joe DePinto On behalf of our team at
Cardinal Health Specialty Solutions 2017 Oncology Insights Views on Reimbursement, Access and Data from Specialty Physicians Nationwide A message from the President Joe DePinto On behalf of our team at
All ACO materials are available at What are my network and plan design options?
 ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement. Craig J. Wilson
 Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Integrated Health System
 Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
Integrated Health System Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital Association and Health Forum. Page 2
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
MEDICARE PART D STAR RATINGS & PHARMACY PERFORMANCE
 MEDICARE PART D STAR RATINGS & PHARMACY PERFORMANCE LISA R. ERWIN, R.PH., CGP SENIOR CONSULTANT AUGUST 21, 2015 WHO IS GORMAN HEALTH GROUP? Gorman Health Group is the leading solutions and consulting firm
MEDICARE PART D STAR RATINGS & PHARMACY PERFORMANCE LISA R. ERWIN, R.PH., CGP SENIOR CONSULTANT AUGUST 21, 2015 WHO IS GORMAN HEALTH GROUP? Gorman Health Group is the leading solutions and consulting firm
Driving the value of health care through integration. Kaiser Permanente All Rights Reserved.
 Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Pharmacists' Impact on Quality Measures and Opportunities for Pharmacy Enhanced Services
 CONTINUING EDUCATION Pharmacists' Impact on Quality Measures and Opportunities for Pharmacy Enhanced Services by Blair Thielemier, PharmD, and Alexander Tu, PharmD May 1, 2017 (expires May 1, 2018) Activity
CONTINUING EDUCATION Pharmacists' Impact on Quality Measures and Opportunities for Pharmacy Enhanced Services by Blair Thielemier, PharmD, and Alexander Tu, PharmD May 1, 2017 (expires May 1, 2018) Activity
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
The Role of Pharmacy in Alternative Payment Models
 The Role of Pharmacy in Alternative Payment Models July 15, 2015 Disclaimer Organizations may not re use material presented at this AMCP webinar for commercial purposes without the written consent of the
The Role of Pharmacy in Alternative Payment Models July 15, 2015 Disclaimer Organizations may not re use material presented at this AMCP webinar for commercial purposes without the written consent of the
ACTIVITY DISCLAIMER. Improving Patient Portal Use DISCLOSURE. Learning Objectives. Audience Engagement System Step 1 Step 2 Step 3
 ACTIVITY DISCLAIMER Improving Patient Portal Use William Manard, MD, FAAFP The material presented here is being made available by the American Academy of Family Physicians for educational purposes only.
ACTIVITY DISCLAIMER Improving Patient Portal Use William Manard, MD, FAAFP The material presented here is being made available by the American Academy of Family Physicians for educational purposes only.
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Fundamentals of Medication Therapy Management (MTM) Services By Bruce R. Siecker, Ph.D., R.Ph.
 Services By Bruce R. Siecker, Ph.D., R.Ph.") Fundamentals of Medication Therapy Management (MTM) Services By Bruce R. Siecker, Ph.D., R.Ph. Bruce Siecker is president of Paradigm Research & Advisory Services, Inc. based in Stone Ridge, Virginia.
Fundamentals of Medication Therapy Management (MTM) Services By Bruce R. Siecker, Ph.D., R.Ph. Bruce Siecker is president of Paradigm Research & Advisory Services, Inc. based in Stone Ridge, Virginia.
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Prescription for Healthy Communities: CARRYING OUT SUCCESSFUL MEDICATION MANAGEMENT SERVICES IN COMMUNITY PHARMACIES
 Prescription for Healthy Communities: CARRYING OUT SUCCESSFUL MEDICATION MANAGEMENT SERVICES IN COMMUNITY PHARMACIES Deborah Pestka, PharmD Caitlin Frail, PharmD, MS, BCACP Laura Palombi, PharmD, MPH,
Prescription for Healthy Communities: CARRYING OUT SUCCESSFUL MEDICATION MANAGEMENT SERVICES IN COMMUNITY PHARMACIES Deborah Pestka, PharmD Caitlin Frail, PharmD, MS, BCACP Laura Palombi, PharmD, MPH,
E1. STUDENTS IN-NO-VA-TION 10:45-11:45AM
 E1. STUDENTS IN-NO-VA-TION 10:45-11:45AM Speaker: Randy P. McDonough, PharmD, MS, CGP, BCPS, FAPhA, is Co-owner of Towncrest and Towncrest Compounding Pharmacies in Iowa City and Solon Towncrest Pharmacy
E1. STUDENTS IN-NO-VA-TION 10:45-11:45AM Speaker: Randy P. McDonough, PharmD, MS, CGP, BCPS, FAPhA, is Co-owner of Towncrest and Towncrest Compounding Pharmacies in Iowa City and Solon Towncrest Pharmacy
Pitch Perfect: Selling Your Services to LTC Facilities
 Pitch Perfect: Selling Your Services to LTC Facilities Lou Ann Brubaker, President Brubaker Consulting www.brubakerconsulting.com 301 535 5449 brubak97@aol.com Linkedin Disclosure Lou Ann Brubaker is the
Pitch Perfect: Selling Your Services to LTC Facilities Lou Ann Brubaker, President Brubaker Consulting www.brubakerconsulting.com 301 535 5449 brubak97@aol.com Linkedin Disclosure Lou Ann Brubaker is the
Fueling Pharmacy Change: From Community Pharmacy Foundation (CPF) Grants to Action
 Grants to Action") Fueling Pharmacy Change: From Community Pharmacy Foundation (CPF) Grants to Action Community Pharmacy Foundation Anne Marie Kondic, PharmD Executive Director Disclosures Anne Marie Kondic, PharmD, is the
Fueling Pharmacy Change: From Community Pharmacy Foundation (CPF) Grants to Action Community Pharmacy Foundation Anne Marie Kondic, PharmD Executive Director Disclosures Anne Marie Kondic, PharmD, is the
Journey in managing practice variation in Diabetes and Hypertension (Part 2/2)
") Journey in managing practice variation in Diabetes and Hypertension (Part 2/2) For Part 1 of this presentation, go to http://rightcare.berkeley.edu/sacramento-university-of-best-practices Parag Agnihotri,
Journey in managing practice variation in Diabetes and Hypertension (Part 2/2) For Part 1 of this presentation, go to http://rightcare.berkeley.edu/sacramento-university-of-best-practices Parag Agnihotri,
Decreasing Medical. Costs. Are your members listening to you? PRESENTED BY: September 22, 2016
 Decreasing Medical Costs Are your members listening to you? PRESENTED BY: Aaron Crowell, Executive Vice President, MTM, Inc. Gary Jacobs, Executive Vice President, CareCentrix Dan Masciopinto, SVP of Product,
Decreasing Medical Costs Are your members listening to you? PRESENTED BY: Aaron Crowell, Executive Vice President, MTM, Inc. Gary Jacobs, Executive Vice President, CareCentrix Dan Masciopinto, SVP of Product,
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
TABLE H: Finalized Improvement Activities Inventory
 TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
Strategic Plan for Enabling Pharmacist-Provided Medication Therapy Management & Wellness Services throughout Ohio
 Strategic Plan for Enabling Pharmacist-Provided Medication Therapy Management & Wellness Services throughout Ohio PREMISE: FOR MEDICATION THERAPY MANAGEMENT /WELLNESS SERVICES TO BE A PHARMACIST-PROVIDED
Strategic Plan for Enabling Pharmacist-Provided Medication Therapy Management & Wellness Services throughout Ohio PREMISE: FOR MEDICATION THERAPY MANAGEMENT /WELLNESS SERVICES TO BE A PHARMACIST-PROVIDED
Medicare Coverage That Works for You
 Medicare Coverage That Works for You A simple guide to your University of California benefits Health Net Seniority Plus (Employer HMO) CA_19_8249EGBROC_C 08132018 Helping You Make the Right Choice For
Medicare Coverage That Works for You A simple guide to your University of California benefits Health Net Seniority Plus (Employer HMO) CA_19_8249EGBROC_C 08132018 Helping You Make the Right Choice For
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care