LOCAL DELIVERY PLAN 2016/17
|
|
|
- Leona Joseph
- 6 years ago
- Views:
Transcription

1 LOCAL DELIVERY PLAN 2016/17 25 May 2016
2 CONTENTS Introduction Part 1 Improvement Priorities Priority 1 Health Inequalities and Prevention Priority 2 Antenatal and Early Years Priority 3 Safe Care Priority 4 Person-centred Care Priority 5 Primary Care Priority 6 Integration Priority 7 Scheduled Care Priority 8 Unscheduled Care Priority 9 Mental Health Part 2 LDP Standards Part 3 Financial Planning Part 4 Community Planning Partnerships Part 5 Workforce Appendix 1 Finance Tables
3 NHS Highland Local Delivery Plan 2016/17 Introduction Welcome to NHS Highland s Local Delivery Plan for 2016/17. This document forms our contract with the Scottish Government for the delivery of services over the coming year. Local Delivery Plans focus on the priorities for the NHS in Scotland and support delivery of the Scottish Government s national performance framework, the Health and Social care outcomes that are being developed in partnership, and the 2020 vision for high quality and sustainable health and social care. Local Delivery Plans are part of the NHS Scotland performance framework that has evolved since 2007 in line with public service reform in Scotland. They have supported the NHS in Scotland to transform waiting times for patients who continue to benefit from on-going improvement; to take decisive action to tackle Healthcare Associated Infections, to prioritise and tackle alcohol abuse and the impact it has on positive outcomes; and to achieve sound financial management. Part 1 of the NHS Highland Local Delivery Plan covers 9 improvement priority areas: Priority 1 Health Inequalities and Prevention Priority 2 Antenatal and Early Years Priority 3 Safe Care Priority 4 Person-centred Care Priority 5 Primary Care Priority 6 Integration Priority 7 Scheduled Care Priority 8 Unscheduled Care Priority 9 Mental Health The remaining Parts 2, 3, 4 and 5 cover LDP standards, Financial Planning, Community Planning Partnerships and Workforce, with the Finance tables included as appendix 1 of the document. NHS Highland continues to deliver the Triple Aim vision of Better Health, Better Care and Better Value of the Highland Quality Approach, described in the Highland Care Strategy outlining NHS Highland s vision for the future delivery of health and social care services for the people of Highland over the next 10 years. The Implementation Plan starts to describe the approach and shared focus for all the work to realise implementation of the strategy over the next 2-5 years. This plan is then supported by more detailed operational unit and corporate delivery plans. The implementation plan has been designed to maintain the focus on improving quality and to make measureable progress to deliver the Highland Care Strategy (10 year plan). At a high level it, describes the priority areas for action. It acknowledges the continuing changing financial, demographic and political environment, and the impact on the future demands for delivery and structure of health and social. There will be a clear need for care and services to be delivered in a radically different way, to ensure that NHS Highland secures the best possible outcomes for our population, maximising the use of all available resources. Our current approach recognises the complex planning arrangements that are in place for health and social care at local, regional and national level and provides a basis to govern the operational implementation across NHS Highland. By planning and working more closely in partnership, the delivery of services across traditional boundaries will help us to provide more sustainable services across Highland, the Islands and the wider North of Scotland. Key elements of the plan will require further significant work, and may be subject to consultation and have been identified as high level value streams with executive sponsorship. These work
4 streams cover the provision and model of out of hours care, transforming out-patient services, and improving the flow of adult care. Additional projects include planned major service change, challenges with Rural General Hospitals as well as wider remote and rural issues including recruitment, training and retention of staff. The Highland Quality Approach continues to capture the spirit of how NHS Highland is working to improve care and outcomes for people in Highland and will be the vehicle we will use to deliver on our implementation Plan. It recognises how important it is to improve the health of the population and get the experience of care right for individual people, every time. We will deliver this by focusing on providing person-centred care while at the same time eliminating waste, reducing harm and managing variation. This approach places an explicit emphasis on how we will make best use all of our resources, transforming care by embedding quality improvement methods at scale. Our approach encompasses that set out in the Scottish Governments 2020 Vision for Health and Social Care, which is: Our vision is that by 2020 everyone is able to live longer, healthier lives at home, or in a homely setting. We will have a healthcare system where we have integrated health and social care, a focus on prevention, anticipation and supported self management. When hospital treatment is required, and cannot be provided in a community setting, day case treatment being the norm. Whatever the setting, care will be provided to the highest standard of quality and safety, with the person at the centre of all decisions. There will be a focus on ensuring that people get back into their home or community environment as soon as appropriate, with minimal risk of re-admission. Whilst we acknowledge that 2016/17 presents a significantly challenging financial year, NHS Highland is well placed to deliver on the elements described within this Local Delivery Plan. We look forward to working with you on our journey over the next year. Elaine Mead Chief Executive
5 NHS Highland Part 1 Improvement Priorities
6 This page is intentionally blank
7 Priority 1 Health Inequalities and Prevention Procurement Effective procurement can bring a huge range of benefits for public sector organisations which go much further than the basic concepts of developing contracts and saving money. Within NHS Highland, sustainable procurement is viewed as a strategic tool which can be used to support local economic development, provide opportunities for employment and training and support enterprise and innovations which could bring benefits far beyond our borders and help to sustain our fragile rural economy. Local Priorities In 2016/17, NHS Highland has identified specific local priorities for its Procurement activity taking into account specific requirements following the introduction of the new European Procurement Directives and the Procurement Reform (Scotland) Act 2014 which support our position as one of the best performing organisations (A+ rated) as awarded in our 2015 Procurement Commercial Improvement Programme Assessment. NHS Highland supports the statutory guidance from the Scottish Government to assess the willingness all companies tendering for public contracts to pay their employees the living wage and will incorporate this into all of its contractual undertakings, NHS Highland recognises the important role played in the Scottish and Highland economies of Social Enterprises, Third Sector and Supported Businesses and supports the vital role they play in local communities providing employment opportunities and good quality goods and services, NHS Highland is keen to ensure that the awarding of its contracts can bring benefits right into the heart of local communities in new and innovative ways and adhere to its obligations under the Sustainable Procurement Duty, NHS Highland does not work in isolation and recognises the importance of procurement collaboration with other public sector partners in the Highland region and with other Health Boards across Scotland. Improvement Aims In order to deliver effective procurement which builds upon our Procurement Strategy and the 2016/17 procurement priorities, we have developed the following specific improvement aims. NHS Highland will seek to ascertain, through all of its regulated procurement activity, which of its contractors pay their employees the living wage and which don t, we will ensure that all bidders for contracts are aware of our support for the concept of a living wage. NHS Highland will undertake to establish, stronger relationships with Third Sector and Supported businesses and the Highland 3 Third Sector Forum, with an aim to exploring contracting opportunities and future contract requirements. NHS Highland will include Community Benefit Clauses in its future procurement activities which support the aims and ambitions of people in their local communities. NHS Highland will share future contract opportunities with public sector partners prior to every regulated procurement exercise to ascertain the potential for future collaboration opportunities. Levels of Activity In identifying improvement aims for procurement, we have identified areas where it is felt strong and sustained improvement can be achieved. Some of these areas are new and others are existing activities with room for improvement. NHS Highland now as a matter of routine, in most tendering activity, requests any information from contractors in relation to the living wage.
8 NHS Highland currently has some procurement activity with Third Sector and Supported businesses but this tends to be very small scale and often without a formal contract in place. NHS Highland has included Community Benefit Clauses in some of its Works contracts, but there use in contracts covered by Goods and Services regulations has not yet been explored. NHS Highland currently participates in the NHS Scotland East of Scotland Procurement Consortium, but this has brought limited opportunities for joint procurement activities to date. Joint contracting with The Highland Council tends to be on an ad-hoc basis and activity with Argyll and Bute Council is extremely limited. How we embed activity In order to deliver on our improvement aims, it s vital that we embed these in our day to day activities and our standard work practices. NHS Highland will ensure that in every contract advert published on the Public Contract Scotland Portal will include a statement of NHS Highland s support of the living wage. We will also ensure that every NHS Highland tender will ask bidders to disclose whether or not their employees employed specifically in the delivery of the contract, will be paid the living wage. NHS Highland will at the initial strategy stage of every contract opportunity undertake an assessment of requirements to see whether or not specific contracts can be reserved for participation by Third Sector and Supported Businesses only. NHS Highland will ensure that Community Benefit Clauses form a key part of the evaluation criteria of every regulated procurement exercise undertaken. NHS Highland will endeavour to share all future contract opportunities with public sector partners prior to every regulated procurement exercise to ascertain the potential for future collaboration opportunities. How we prioritise action NHS Highland will seek to engage with key stakeholders early to ensure sufficient time is allowed for the improvement aims to be embedded with partners. Internal changes such as those relating to our tendering and contracting documents will be initiated in conjunction with the NHS NSS Central Legal Office. A new Procurement Strategy will be developed and published by December 2016 with specific focus on a range of improvement aims including those covered in this section. How we monitor Progress NHS Highland will monitor the implementation of its improvement aims through existing methods such as the Scottish Government Procurement Capability Assessment and the NHS Highland Non-Pay Procurement Group. A progress update will also be published in the annual Procurement Report which is to be published at the beginning of every new financial year from 2016 onwards.
9 Employment Policies LOCAL PRIORITY & LEVEL OF PRIORITY FOR NHS HIGHLAND IMPROVEMENT AIM LEVEL OF ACTIVITY MONITORING OF PROGRESS Continue to adhere to responsive recruitment & employment practices to attract new staff to work for NHS Highland To ensure vacancies are advertised widely in order to select staff from as wide & diverse pool of suitable applicants as possible to attract & develop the best health-care teams As required following approval by vacancy monitoring committee approval- 1.Consider redeployment 2. Consider Internal Advertising or External Advertising Monitor on quarterly basis by NHS Highland s Staff Governance Committee Review recruitment & employment practices to ensure meets best practice standards & equality legislation Continue to offer work experience/ placement opportunities to people from a wide range of backgrounds including multi-disadvantaged groups To deliver positive social outcomes & to develop a more representative workforce Continue with annual assessment by Job Centre Plus to achieve the Double Tick Positive About Disabled People symbol for use on recruitment paperwork Work with partner agencies such as Job Centre Plus; Social Work; Barnardos & the Shirlie Project, Individual Placement Support Services to offer work placements, or youth employment Monitor on quarterly basis by NHS Highland s Staff Governance Committee Contribute to Health & Social Care Career programmes for School Pupils Scope opportunities for a wider range of internships across workforce groups if not already in place Offer volunteering opportunities Attending job fairs in deprived areas within NHS Highland
10 Continue to work in partnership with Trade Union/Professional Organisations to support staff, who develop Long Term Health Conditions to remain in employment through the consideration of reasonable adjustments in the work-place To deliver positive social outcomes & retain skills, knowledge and experience of staff Raise awareness with Managers about their responsibility to consider reasonable adjustments; Work with Occupational Health/ Access to work & other Charities to identify sources of funding Monitor on quarterly basis by NHS Highland s Staff Governance Committee Ensure all staff employed by NHS Highland are treated fairly & consistently and work within an organisational culture where they feel motivated, valued and free from bullying/harassment and/or any form of direct or indirect discrimination To deliver positive staff experience Consider feedback from 2015 staff Survey and I- matters 2015/16 & rollout Give Respect, Get Respect awareness programme in areas where bullying/harassment and or discrimination are of concern Raise awareness of nationally developed PIN policies across NHS Highland to ensure consistent application in supporting staff Monitor on quarterly basis by NHS Highland s HR Sub Group and/or Terms & conditions group Continue to apply national terms & conditions of service Learning & Development opportunities are made known to all staff with selection for such opportunities being free from discrimination To ensure all staff are appropriately trained to fulfil their role within NHS Highland Ensure all staff undertake an annual PDP/e-KSF review or annual appraisal in accordance with their terms and conditions of service Monitor on quarterly basis by NHS Highland s Learning & Development group
11 Supporting more individuals and their families to make choices about their health and care Making NHS Highland the employer of choice Improvement Aims Levels of activity How the activity will be embedded into routine practice Improve the Review and update Guidance contained health and breastfeeding and within PIN Policies wellbeing of our returning to work guidance staff Review an update the Violence Against Women staff policy Guidance contained within PIN Policies Monitoring progress Progress monitored through HR and partnership forum Progress monitored through HR and partnership forum Making NHS Highland a fairer place to work Develop activities aimed at helping staff and managers to recognise and manage stress Become a Cycle Friendly Employer Become a member of the Stonewall Diversity Champion Programme. Self assess the organisation against the Workplace Equality Index. Online support available to all staff. Information included within staff induction policy Through local Bike User Groups Establish an improvement group to promote equality and celebrate diversity within their own work programmes Monitoring of sickness absence where stress is given as the reason for absence Number of accredited sites Self assessment process during 2016/17 will provide a benchmark, priorities and actions for 2017/18 onwards. Develop an improvement plan by April Progress monitored through the HR Sub Group, reporting to the Highland Partnership Forum. Continuously develop our staff s knowledge and skills Deliver mandatory Violence Against Women training to our staff Included within NHS Highland policy for statutory and mandatory training and Educational Governance Framework Numbers attending training
12 Improvement Aims Supporting more individuals and families to make informed choices about food and health Levels of activity Support, promote and encourage breastfeeding with young people Support NHS Highland to maintain UNICEF BFI award including peer support and intensive interventions through infant feeding support workers How the activity will be embedded into routine practice Implement through the 3 18 curriculum programme available on GLOW Appropriate staff will be trained to ensure standards are met. Standards will be built into NHS Highland policies and procedures for ante natal and post natal care and support Monitoring progress Monitoring of breastfeeding rates On-going audit and monitoring of standards by the Maternal and Infant Nutrition Improvement group Deliver food skills courses in our most deprived communities By building capacity in staff and volunteers within communities. Quantitative evaluation of numbers trained and course delivered Pilot 1 year Food Friends, using food and meals to decrease social isolation in rural areas Partnership work with the third and voluntary sector Qualitative evaluation of experiences. 6 and 12 monthly review numbers, cost, and outcomes evaluation Support individuals and families to jointly agree priorities and approaches for health improvement and wellbeing Work with communities and hard to reach groups within them to establish structures to support resilience and positive attitudes to health Support the progression of men s sheds and monitor positive impact on mental health and wellbeing Maximise opportunities for health interventions while supporting other activities and groups Encourage and support the group to progress towards self management of a forum for men to improve physical and mental health while having the opportunity to learn some new life skills 6 and 12 monthly review numbers, interventions, cost and outcomes evaluation Qualitative evaluation of experiences
13 Widen delivery of ABIs in nonpriority settings, support those trained to deliver, and target delivery toward tackling health inequalities Target delivery for Highland, set by the Scottish Government is 3,688 ABIs. Settings split: North & West Priority (min) 737 Wider (min) 185 Maximise effective delivery by training and supporting staff to deliver ABI s Include in training for health and social care students attending Highland colleges/university Number of ABI s delivered by setting Numbers of trainers trained and delivering courses Numbers attending training Inner Moray Firth Priority (min) 1390 Wider (min) 347 Argyll &Bute Priority (min) 824 Wider (min) 205 New areas - training scheduled for Police Custody Suite and Inverness Response Team and Housing Officers Investigate the roll out of successful pilot to deliver ABI s through the Fire Service Community Safety Team Work with local agencies to deliver Discussing Drugs and Alcohol with Young People training, encouraging conversations with young people about alcohol and substance use. Integrating prevention into clinical care and improve health outcomes through implementing the Health Promoting Health Service framework Identify and support vulnerable individuals (inequalities). Promote and support smoking cessation; prevention of harmful or hazardous drinking and ensure healthier food and drink choices are the norm Encourage physical activity and active travel Ensure Health Promoting Health Service leads are identified within each hospital with clear communication links to and between all staff and networks Implement through NHS Highland policies where appropriate Quantitative and qualitative reporting annually to Scottish Government, Health Scotland and NHS Highland Board.
14 Support to enhance resilience and financial security Ensure retailers within our buildings meet the Healthcare Retail Standard Providing timely access to clinically appropriate care Improvement Aims Improve the reach of healthy weight interventions Levels of activity Increase the delivery of Well Now groups in new areas How the activity will be embedded into routine practice Recruit and train new facilitators in areas where demand is greatest Monitoring progress Numbers of participants completing the course. Achievement of course objectives Develop and pilot a Body Confidence course for teenagers Through the development of a Child Healthy Weight pathway Numbers of participants completing the course. Achievement of course objectives Improve the accessibility to services for people whose first language is not English (foreign language and BSL) Targeted delivery of interventions to individuals with long term conditions Disseminate new guidance and materials about interpretation services to all relevant Managers Run three Working With Interpreters training courses for NHSH staff Improving referral pathways including self referral Seek to embed access to interpretation within existing work programmes, e.g. out of hours and Patient Management System improvement Number of individuals completing the course with LTC (E+D questionnaire) Numbers of NHS staff attending Working With Interpreters training Monitor patient feedback about interpretation services and access to them In partnership with Highland Council procure foreign interpretation service by December 2016 and Communication Support Service by March 2017 Monitoring meetings with providers of interpretation every 6 months
15 Improving the reach of smoking cessation services Further develop and embed a smoking cessation service to inpatients within acute settings Train existing staff Include within existing quality improvement work Monitor referrals to service and successful quits through the ISD database Further develop and support a smoking cessation service within outpatients Monitor nicotine replace therapy (NRT) prescribed within the hospital setting Train and support key workers in mental health inpatient facilities to support patients to cut down or quit smoking Include in existing job roles Monitor activity through ISD database and NRT prescribing Improve our response to survivors of gender based violence Provide support to Inverness prison to support smokefree prisons Implementation of new forced marriage protocol Include in existing job roles Multi-agency guidance distributed and supported by staff training Monitor activity through ISD database Numbers trained and evaluation of training Development of clinical pathway for women affected by female genital mutilation Pathway to complement FGM protocol Service user feedback NHSH become a trauma informed service Staff receive trauma training and embedded within the sexual violence policy Staff feedback Argyll and Bute Improvement Aims Actions to support staff to support the most vulnerable people and communities What are the improvement aims that have been agreed locally? Roll out of Caring Connections within the context of an overall Organisational Development Plan (a copy of this plan is available on request) What actions will be taken to move towards that aim? Implementation of A&B HSCP Organisational Development Plan What measures will be used to assess improvements made? Review of Organisational Development Plan
16 Improvement Aims What are the improvement aims that have been agreed locally? What actions will be taken to move towards that aim? What measures will be used to assess improvements made? health improvement actions to promote healthy living and better mental health 1. multi-agency joint health improvement plan: content/uploads/2013/03/joint- Health-Improvement-Plan-2013.pdf Implementation of both plans. In addition with the integration of health and social care it has been agreed that the funding for Choose Life is within scope of the HSCP and budget for this will be mainstreamed into public health. Performance measures within the plans. 2. A&B health improvement team plan (a copy of this plan is available on request) 3. Use of the Integrated Care Fund on prevention and health improvement ICF spent on preventative and anticipatory care programmes including: management and prevention of falls All of these services will now be evaluated on what they deliver for our communities with regard to achieving our vision to help us direct funding in future years. self management reablement preventative physical activity programmes programmes improving mental health and wellbeing
17 SUBSTANCE MISUSE SERVICES Priorities 90% of clients referred for treatment will wait no longer than 3 weeks from referral received to appropriate drug or alcohol treatment that supports their recovery and no-one will wait over 6 weeks. Priorities are determined in discussion with partners within the Alcohol & Drugs Partnerships across NHS Highland area, Argyll & Bute ADP and Highland ADP. This ensures that activity matches the overall recovery strategy in both areas. Local Priorities NHS Highland has worked to achieve the above standard. The priority was to ensure that service change was sustainable in to the long term and avoided the risk of seeking short term gains. Challenges remain the geography of Highland dictates that teams are often small in number and are vulnerable to sickness or vacancies; it can be difficult to recruit. Both areas have struggled to sustain progress at or above 90% completed waits within 3 weeks. HEAT A11 Completed waits - 3 weeks 2015/16 Apr-June Q1 July-Sept Q2 NHSH 87.70% 91.60% A&BADP 96.60% 93.40% HADP 84.50% 90.80% Quarter 3 October to December data was submitted 22 nd January 2016 with expected publication at end of March. It is expected to show a drop below 90% in both ADP areas and therefore NHS Highland will be below target. Improvement Aims The priority focus is to maintain 90% in 3 weeks and achieve 100% within 6 weeks. Embedding Activity A Service Improvement Group has evolved from the Demand, Capacity, Activity and Queue process in north Highland (HADP). This group will focus on delivering the HEAT A11 standard, embed the Quality Principles and roll out the Recovery Outcomes Webtool to ensure that services are responsive and recovery focussed. The A&B ADP has a dedicated subgroup focussed on recovery. Service Level Agreements have been reviewed and updated; HEAT A11 is a specific element within the service specifications. Staff remain committed to delivering a safe and effective service. Prioritising Action A key challenge for substance misuse services across NHS Highland is in recruitment. Adverts are listed on the SHOW website to encourage staff from out with our area to join the team. There is a limited pool of Registered Mental Nurses (RMN) nationally and as a
18 result, vacancies are difficult to recruit to. RMN s are core to delivering treatment and support services. There will be a further review of the team skill mix and consideration given to alternative opportunities to develop competent staff. The Care Inspectorate is supporting ADP s in a self evaluation exercise on how well the national Quality Principles are embedded in local service delivery. This will be an invaluable exercise to create a baseline for both areas and an action plan on addressing any issues identified, providing a rapid access to treatment is reflected in this plan. The Recovery Outcomes Webtool is to be rolled out over north Highland (HADP) area with a launch date of 1 st May Events are in the process of being planned to promote this. The implementation of the Drug & Alcohol Information System (DAISy) has been moved back to January In the meantime, data quality issues are being addressed to ensure that there is accurate recording and a reduction of anonymous records in the system. There is a need to review IT requirements and NHSH are awaiting information from the DAISy steering group in order that we can match against local systems. Monitoring Progress Monthly reports are circulated to all of the teams and are checked for accuracy and compliance. Additional support can be offered where teams are struggling to maintain data input. NHS Highland are 100% compliant in data entry. An update on progress is submitted to the ADP s quarterly. The Head of Service Substance Misuse, has monthly teleconferences with Scottish Government colleagues to update on progress and challenges.
19 Priority 2 Antenatal and Early Years Strategic commissioning plans We will continue to develop the NHS Highland Balanced Score Card: Health and Well Being and Health Services for Children and Young People. (Early Years measures appended) This is informing the governance and assurance processes and the commissioning activity with the Care and Learning Service Highland Council and improvement activity across the Argyll and Bute HSCP and the Highland HSCP. We continue to work with partners to implement the recommendations in the Needs Assessment for the NHS Highland (Children and Young People Needs Assessment NHS Highland October 2014). (See Table 1 - Driver Diagram below). The Children and Young People s Commissioning Group has been revised to inform a high level strategic view of the health needs of children and young people, relevant services and commissioned relationships across the directly managed units of the HHSCP, Care and Learning Service Highland Council. Through 2016 we will develop this approach to include Argyll and Bute HSCP and tertiary contracts with other Health Boards and third sector providers. (See Table 2 - Commissioning and Improvement Priorities 2016/17 below). We are also developing a Balanced Score Card for Children and Young People s health and wellbeing and access to services (See Table 3 - Performance Measures: Early Years below). Models of service delivery The Lead Agency model for children and young people in the Highland Community Planning Partnership is moving into year five. We are furthering developing the commissioning process with clearly stated commissioning intentions for 2016/17. We continue to influence the design and delivery of services for children and young people through the commissioned elements of services for children and young people delivered by the Care and Learning Service Highland Council and as partners to the wider system of integrated children s services through For Highland s Children 4 and For Argyll and Bute s Children. We will be looking for further opportunities to better manage cost and demand and to support innovative redesign between services for children and young people in the HHSCP and Care and Learning Highland Council through further improvements to complex care assessment and planning, Child and Adolescent Mental Health and timely intervention where there are developmental/behavioural concerns in the early years. Children and Young People s Act (Scotland) 2014 We are sighted on the implications of the Children and Young People s Act (Scotland) Commissioning intentions for the Care and Learning Service Highland Council and the body corporate model in Argyll and Bute will capture the needs for services to be compliant with legislation with regard to the Named Person role. Initial planning work had already been undertaken with regard to the Health Visitor Case Load tool and additional posts have been recruited to develop capacity in the workforce. Further recruitment and training will take place as necessary during (See Tables 4 and 5 Health Visitor status reports below for further information). We will meet the named person duties under the 2014 Act with health visitor numbers as required and training for the role undertaken. Both Highland and Argyll and Bute have well established Child Plan processes and these will be refreshed in light of the legislation. Currently services, processes and practice ensure that all children under the age of five have a plan if required. The Executive Lead for Children s Services and the Child Health Commissioner are both involved in integrated children s service planning in both Highland and Argyll and Bute Community Planning Partnerships. We will fulfil the child s plan duties under the 2014 Act in both Partnerships.
20 Information sharing processes are currently being reviewed in light of the Act across both Partnerships and we will be compliant with the legislation. Both Partnerships have established Child Plan processes and these will be reviewed in light of the final guidance, being published. There will be a refreshed overarching data sharing agreement and the required protocols with regard to the Act.
21 Table 1 - Early Years (health) Driver Diagram
22 Table 2 - Commissioning and Improvement Priorities 2016/17 Input Activities Outputs Outcomes/Impact Reporting route NHS Highland Health Visitor Implementation Group Lead: Deputy Director of Nursing Highland Health Visitor Implementation Group Lead: Principal Officer Nursing Highland Council Workforce Planning Tool exercise to better understand demand and capacity and associated work force needs Workforce, Recruitment and Financial Plans for Health Visiting in Highland and Argyll and Bute (Appended) Workforce with the capacity to undertake named person service responsibilities and implement the Universal Health Visiting Pathway (2015) Area Nursing Midwifery Allied Health Leadership Committee Argyll and Bute Health Visitor Implementation Group Lead: Consultant Nurse Children and Families Senior Nurses Highland and Argyll and Bute (Training remit) Senior Nurses Highland and Argyll and Bute Head of Midwifery Lead Midwives NHSH Highland including Argyll & Bute Highland and Argyll and Bute participation in GIRFEC Health Masterclass March 2016 Input to revision of Highland Practice Model and Argyll and Bute GIRFEC Child s Plan processes Regular use of validated midwifery workforce tools and Professional Judgement tool Senior staff with skills and knowledge to build capacity in the wider health early years work force to support the implementation of legislation Revised and refreshed protocols and practice ensure that workforce is optimum to meet the needs of antenatal service provision Training skills and knowledge to support improvement across the workforce Practice guidance and protocols are legislatively compliant Area Nursing Midwifery Allied Health Leadership Committee Area Nursing Midwifery Allied Health Leadership Committee Maternity & Neonatal Services Strategy & Coordination Committee & sub groups
23 Midwifery Development Officer Highland Council Midwifery Team Leaders Midwives Health Visitors/early years teams (health) School Nurses Learning Disability Nurses Paediatricians Community Children s Nurses Specialist Nurses Specialist CAMHS Tier 1-2/3/4 AHPs GPs Dental services Clearly defined mandatory training programmes made available to relevant staff Contribute to the revision of the Highland Practice Model and GIRFEC; in particular interface between midwifery, HV & Family Nurse Partnership practice & the public health role of the midwife Health staff working with children and families undertake training and awareness raising to ensure they are aware of their responsibilities in relation to the Highland Practice Model/ Argyll and Bute GIRFEC Child s Plan processes as required by the Children and Young People s Act (Scotland ) 2014 assurance that workforce has training and skills to meet practice needs & support women and families in antenatal, intrapartum & postpartum period Maintain guidance for midwifery practice Assurance that training/updates on the Highland Practice Model has been undertaken for health staff Enable/improve collaborative interprofessional working Metrics for assurance purposes being explored Lead Midwives Group Area Nursing Midwifery Allied Health Leadership Committee Deputy Director of Nursing Associate Director of AHPS Child Health Commissioner Data and Performance Management Group Annual review and further development of Balanced Score Card Early Years measures (current measure appended) Commissioning intentions Care and Learning Highland Council Improvement priorities Directly Managed Units HHSCP and Argyll and Bute HHSCP Performance indicators and measures that demonstrate improvement to service design and outcomes for children and young people NHS Board
24 These to involve: Population Measures Outcomes that demonstrate progress in relation to service design and delivery Evidence of involving children and young people and families Evidence of involving staff improvement activity
25 Table 3 - Performance Measures: Early Years Indicator number CYP 01 Performance Measure Target Comment Percentage of maternity booking data recorded on the SBR within 14 days of booking 95% Reporting from 2017 CYP 02 CYP 03 CYP 04 CYP 05 CYP 06 The rate of LBW babies born to the most deprived compared to those born in the least deprived parts of Highland. Percentage uptake of 6-8 week Child Health Surveillance contact Percentage uptake of Child Health Surveillance contact in each quintile of deprivation 6-8 week Child Health Surveillance contact uptake between the general population and Looked After Children Percentage of new born babies exclusively breastfed at 6-8 week review A year on year reduction Annual 95% Quarterly 95% Annual 95% Annual 36% by March 2017 Target under review CYP 07 Percentage gap between the most and least deprived parts of Highland in the number of children exclusively breastfed at the 6-8 week review A reduction year on year Annual CYP 08 CYP 09 Percentage Allocation of Health Plan indicator at 6-8 week from birth Percentage uptake of primary immunisations by 12 months 95% Quarterly 95% Quarterly CYP 10 Percentage of dental registrations of 0-2 year olds An increase Quarterly CYP 11 The number of 2 years olds who have seen a dentist in the preceding 12 months An increase Quarterly CYP 12 CYP 13 Percentage increase in uptake of Healthy Start Scheme of eligible beneficiaries Percentage increase in the coverage of the month contact 85% by 2016 Target under review 95% by 2016 Target under review
26 Indicator number CYP 14 Performance Measure Target Comment Percentage of children who reach their developmental milestones at their month health review Measure on hold until 2017/18 CYP 15 CYP 21 CYP 22 CYP 31 Percentage uptake rate of MMR1 (% of 5 year olds) Percentage of statutory health assessments done within 4 weeks of becoming looked after Percentage of initial LAC health assessments included in Child s Plans within 6 weeks Percentage of children and young people attending Emergency Departments who were seen within 4 hours 95% Quarterly 95% Target under review 95% Target under review 98% Quarterly
27 Table 4 - Care and Learning Highland Council (Commissioned Service in Lead Agency Model) TEAM Baseline at integration 2015/16 establishment (FTE HV posts ) Actual qualified HVs in post HV posts covered by trainees Current HV Vacancies Expected FTE HVs by 2018 Caithness Sutherland East Ross Mid Ross Skye, Lochalsh, West Ross & Assynt Lochaber Inverness West Inverness Central, B & S Inverness East & Nairnshire Totals Table 5 - Argyll and Bute Children and Families Health Visiting Teams TEAM Baseline at integration 2015/16 establishment (FTE HV posts ) Actual qualified HVs in post HV posts covered by trainees Current HV Vacancies Expected FTE HVs by 2018 Oban, Lorn and Isles Mid Argyll, Kintyre and Islay Bute and Cowal Helenburgh & Lomond Totals
28 This page is intentionally blank

29 Priority 3 Safe Care SCOTTISH PATIENT SAFETY PROGRAMME The Scottish Patient Safety Programme forms a key part of the Highland Quality Approach. The Scottish Patient Safety Programme has expanded to include 4 major improvement programmes: Acute Adult Primary Care Mental Health Maternity, Paediatrics and Neonatal Patient safety infrastructure An SPSP Senior Leadership Team meeting takes place to provide governance and monitor progress against aims of all the improvement programmes. This meeting is chaired by the CEO or the Medical Director and meet for 2 hours on a monthly basis. Our SPSP Executive Sponsor is our Chief Executive. Reports are sent to local Operational Clinical Governance Committees, NHS Highland Clinical Governance Committee and directly to the Board when requested. The 10 patient safety essentials are monitored for reliability, sustainability using Horizon plots. They are hosted on line and can be filtered at each level from NHSH wide to individual ward run chart.
30 Each separate programme has SPSP meetings at local level. These meetings provide further governance to ensure progress against process aims and outcomes against a quality improvement timeline. Each work stream also has a defined infrastructure with regular meetings, terms of reference and a multi-disciplinary team to identify and remove barriers to improvement and success. There is a core quality improvement patient safety team which is staffed by the senior quality improvement lead, 2 quality improvement practitioner (1WTE and 1 0.6WTE), a data analyst and a project officer. NHSH have utilised the funding from HAI QIF SG funding for two further facilitator posts on a secondment basis this dedicated resource has benefited progression with the CAUTI and SSI reduction work streams. There is a robust data management system for the whole of the Scottish Patient Safety Programme hosted within the core patient safety team. Data is displayed in every ward on Quality improvement boards and is central to all SPSP reports. All data is visualised using quality improvement methodology using run chart and statistical process control chart rules. The core team continue to explore new methods of data collection, visualisation and analysis working alongside e-health and service planning colleagues. Acute Adult The New High Level Objectives for the Acute Adult Programme are: 20% Reduction in mortality (HSMR) by end % of people experiencing acute care will be free from harms as defined within the Scottish Patient Safety Indicator by the end of 2015 The SPSP aim was to have a reduction of 20 percent in the HSMR by December Progress to this date will be reported in the next quarterly ISD publication in April Nationally the current HSMR reduction is 16.5%. None of the participating hospitals in NHS Highland currently have HSMR trends in line with the percentage decrease required by the target. NHS Highland has had significant problems submitting hospital activity data to the national Standard Morbidity Recording scheme from which the HSMRs are calculated. This issue has been noted in all the reports published since the implementation of the local Trakcare patient management system. ISD estimate that data for NHS Highland for the quarter ending September 2015 is 65 percent complete. The source data is dynamic and missing hospital returns will be included in future reporting when submitted. A shortfall in data returns can result in the number of observed deaths not being accurately known, under-estimation of predicted deaths by the model and the HSMR value being inflated. The reporting of crude rates is particularly influenced by the timeliness of return of patient data. While we recognise the data recording issues it would not be safe to suggest that the most recent quarters of HSMR are data artefact without further investigation of the quality of recording and coding of key variables on the SMR01 scheme. This work is ongoing. Raigmore The quarterly data to September 2015 highlights that the Raigmore HSMR has shown a shift of six consecutive quarters above its median since April Taken alone this run of values is not sufficient to conclude that a poor quality or unsafe service is being provided at the hospital. However, this sequence will be considered by Healthcare Improvement Scotland. The current quarter HSMR at Raigmore is calculated from an incomplete submission of SMR hospital records. The data missing is of the order of 40 to 50 percent of expected activity.
31 Long-term change in mortality trends, monitored using the regression line fitted to the HSMR, indicate an overall 16% reduction. However, there has been no improvement in the HSMR at Raigmore from January Belford Simple linear regression shows a modest 4% overall improvement to date in the HSMR. The Belford Hospital HSMR shows no sustained shifts or trends over the period. The hospital has the smallest number of admissions of any of the participating NHS Highland hospitals and the HSMR data for this hospital initially showed considerable quarterly variation. Caithness General Hospital The long-term trend in the HSMR at Caithness Hospital monitored using linear regression would suggest an 8.1% decrease to date Lorn & Isles The data to September 2015 indicates that the improvement in the HSMR at Lorn and Islands RGH is only 1%t. Mortality case note reviews take place on a monthly basis with a standard set for escalation of events to appropriate system level. Leadership walk around Leadership walk rounds take place on a weekly basis in Raigmore and monthly in the RGH s they are attended by an Executive, a hospital manager, a QI representative and a scribe. The frontline teams welcome these walk rounds as it allows the opportunity to discuss patient safety successes and issues. Actions are taken and closed in a timely manner. Point of care priorities Catheter Associated Urinary Tract Infection (CAUTI) Aim: 95% or > insertion and maintenance bundles and 30% reduction in CAUTI The CAUTI insertion and maintenance bundles were rigorously tested in pilot ward which is now demonstrating high reliability in insertion and maintenance. The outcome in pilot is demonstrating a Quadruple in the median days between CAUTI.
32 Spread of the CAUTI bundles has now taken place to all wards and applicable areas in all 4 Acute Hospitals and has now launched into Community hospitals in a phased manner across NHSH. Outcome measures (utilising the new national definition) has now started to be reported across Acute Hospitals with the majority of wards now reporting catheter days as an added outcome measure. NHS Highland instigated National procurement to change the catheter connector product at factory source as was found to be faulty during point prevalence. Colo-rectal SSI reduction Aim: 95% or > with 3 SSI reduction bundles and less than 10% elective colo-rectal SSI by end December 2015 The team have produced a ward, theatre and intra operative technical bundle are now achieving high reliability across many measures. The team have achieved their ambitious aim of < 10% Colo-rectal SSI at 9.1%. Efforts to maintain outcome and continue to focus on Normothermia, normoglycaemia, on-time and repeat antibiotics continue.
33 Deteriorating Patient Aim: 95% of people with physiological deterioration in acute care will have a structured response and plan and 50% reduction in CPR attempts in general ward setting by December 2015 Structured ward round document implemented ward 7a and spreading to other surgical and medical wards and the Scottish Structured Response roll out to all Raigmore wards by Feb 2016 Principles of treatment escalation planning (TEP) supported in surgery and throughout medical wards. Further spread planned across RGH s and community hospitals throughout the next year

34 Sepsis Aim 95% or > sepsis 6 by end December 2015 Team have been challenged to achieve and maintain high reliability of the sepsis 6 bundle are currently reviewing the Sepsis 6 record and testing further versions. Spread has taken place to all admitting units across the 4 acute hospitals and further spread planned for the coming year. National outcome data demonstrated a reduction in mortality after sepsis diagnosis at Raigmore hospital.

35 Venous Thromboembolism (VTE) Aim: 95% of adult admissions achieve reliable risk assessment and appropriate thromboprophylaxis administration, Reliable re-assessment of risk and patient information NHSH have a single cross speciality VTE risk assessment and treatment protocol which is embedded within the Common Admissions Document in the 4 acute hospitals. Process measures continue to demonstrate variable reliability. The team are currently testing innovative ways to achieve patient self administration of chemical thromboprophylaxis night before surgery and extended thromboprophylaxis. NHSH are developing a system to provide outcome measures in terms of DVT and PE which may have occurred within 12 weeks of an acute hospital admission. A case note review has also taken place to understand if there is any correlation between admissions and events.
36 Heart Failure Process: 95% or > Compliance with the Heart Failure Bundle by end Dec 2015 and 15% reduction in % readmission rate within 30 days The following outcome measures remain under review: 30% decrease in median length of stay, 15% decrease in % mortality at 1 month, 6 months and 1 year by end December 2015 NHSH have provided 5 years retrospective data for all above outcome measures and will continue to provide this ongoing An Alert has been placed on all HF patients known to service on PMS for referral to HFNS when re-admitted to acute care and a system has been developed with ECHO team to inform HFNS for all new diagnosis LVSD connected to ECHO request. A patient held credit card alert has been produced to inform staff to contact HFNS on admission and HFNS service to progress with e health form stream product to enable improved and timely communication with wider multi-disciplinary team and patient. Record kept on Sci store An ECHO telephone request sticker has been designed and implemented across 3 medical wards. This work is planned to continue over next year. Falls The aim is to achieve a 25% reduction in all hospital falls and a 20% reduction in falls with harm whilst promoting recovery, independence and rehabilitation in our hospitals. Cognitive impairment, poor mobility, acute health issues and being in an unfamiliar environment contribute to hospital falls. In NHS Highland a focus on managing delirium and prevention of falls has been taken with guidance issued to Senior Charge nurses of actions they are expected to put in place in their ward area. Five falls screening questions to identify those at risk of falls are included in the NHS Highland Admission Assessment and Personal Care Record (2015) and this is used across the board area. Evidence based bundles to reduce falls are being rolled out in the 7 day assessment record documentation after being tested in a number of sites. Quality improvement facilitator posts for prevention of falls in the inpatient setting have been created within each operational unit and a Quality Improvement Breakthrough Series Collaborative is planned for 2016 to progress this work. A Learnpro module for all staff is in development and will be ready early summer to improve staff awareness and knowledge. Pressure Ulcers NHS Highland has seen an overall reduction in hospital acquired pressure ulcers Grades 2-4 since Implementation of the Pressure Ulcer prevention bundle across all sites has been underway for over 3 years, with large number of staff having completed the NES Pressure Ulcer prevention programme. Monthly reports are developed and monitored on all pressure ulcers which occur in any care setting in NHS Highland. NHS Highland will have completed adoption of the SPSP Pressure Ulcer reporting by December NHS Highland has employed 3 Tissue Viability Nurses who work closely with Care Homes and other providers to raise awareness of the risks of pressure damage and to ensure that staff and carers have the appropriate training and skills to identify and reduce risk as far as possible.
37 NHS Highland has implemented an equipment loan scheme to support short term loan of equipment to Care Homes to ensure that people are cared for appropriately when risk is identified. NHS Highland has a Care Homes Standards group which is currently developing a framework for commissioning with Care Homes and will ensure that the new standards for pressure ulcer prevention are included. The NHS Highland Tissue Viability Leadership Group is a multi disciplinary group which has representation from Care Home sectors and which oversees delivery of the prioritized work plan for pressure ulcer prevention. Medicines Management NHS Highland has brought together all the medicines management teams across the SPSP programmes under the the ADTC Medicines Safety Sub Group. This allows for cross programme discussion, e.g. primary and secondary care, mental health and primary care, community pharmacy and primary care. Many of the safety issues with medicines relate to the handover from one service to another and this new grouping allows for sharing and co-ordination of activity across NHS Highland. Pharmacist led medicines reconciliation on admission to hospital in the 3 RGHs in NHS Highland is a significant success with sustainable gains. It is more challenging in Raigmore Hospital. However sustainable gains have been made in the surgical pre-operative service and the acute medical receiving ward. Medicines reconciliation data is gathered in all other acute receiving wards. Medical leads in these areas are required to move this forward. The NHS Highland electronic discharge letter has a facility to record changes to medicines on discharge in line with SPSP principles. When completed fully the information is welcomed by GPs. Pharmacy SPSP Medicines Management Programme - NHS Highland is one of the pilot boards and is working in the remote and rural areas of the Highlands to improve medication safety. Significant success has been realised already in having community pharmacists ensure that patients are given the appropriate information on non-steroidal anti-inflammatory drugs and that prescribing of NSAIDs was safe relative to other prescribed and non-prescribed medicines. Dispensing GPs will soon be included within the pilot programme. Medicines reconciliation at the first contact after discharge from hospital continues to be a significant focus of activity for general medical practices. The gains made in reducing rates of INR >6 in Raigmore Hospital by changing practice, introducing new protocols and updating the electronic discharge letter proforma for warfarin have been sustained for several years now without any further action being required. This is a good example of an effective non-person dependent reliable system being introduced. Primary Care Programme The whole programme aim is stated as All NHS territorial boards and 95% of primary care clinical teams will be developing their safety culture and achieving reliability in 3 high-risk areas by This is in order to prevent patients being harmed by the care they receive, and if harm does occur, identify, analyse and learn to prevent it recurring. There are 100 GP practices within NHS Highland. Currently the focus is on:
38 Safer medicines: Warfarin Bundle Medicines reconciliation Bundle Safety Culture: Trigger Tool Safety Climate Survey Through the implementation of the Med Rec bundle Practice teams have gained experience in improvement methods such as process mapping exercises and the completion of reflection sheets. The reflection sheets enabled the practices to identify where improvements in their processes could be made, once implemented they were able to see the differences. The adoption of the Safety Climate Survey provided a snap shot of the overall safety climate within a practice. The results were collated and used to identify the practices strengths and weaknesses by comparison to the regional and national aggregate. The benefit of this tool acted as a diagnostic and educational tool for the whole practice to contribute. NHS Highland will continue support to the Practices that have engaged with the SPSP PC work streams whilst further utilisation of the practice manager s network in order to share good practice and offer support and information. The team plan to continue with current bundles and plan to test the Results Handing in bundle next year. Mental Health The mental health programme is currently being implemented in New Craig s Hospital and Argyll & Bute, Succoth ward. The team are testing all the new work streams in relation to reliable implementation of risk assessment and integration, reliable implementation of processes to enable effective communication, Safer medicines management including medicines reconciliation and reducing adverse medication events and appropriate use of seclusion and restraint. Physical health checks within the required timescales are in place in all wards, the roll out of As Required
39 medicines procedures to all wards is complete. Post Incident Review Form in use in test wards and working well, preparing for spread to second ward and Safety Briefs now spread to 3 wards. Medicines reconciliation has spread with full QI checks in all wards. A detailed work plan for 2015/16 is in place % of patients who have emergency detention or use of nurse holding power.
40 HOSPITAL ACQUIRED INFECTION IMPROVEMENT PROGRAMME HEAT Targets All NHS Boards carry out surveillance of Staphylococcus aureus blood stream infections (SABs), known as bacteraemias, and Clostridium difficile infections (CDI). These are serious forms of infection and there are national targets to reduce them. NHS Boards are required to reduce the healthcare associated infections so that by year ending March 2017, Staphylococcus aureus bacteraemia (including MRSA) cases are 24.0 cases or less per 100,000 acute bed days. For NHS Highland this means no more than approximately 60 cases in year ending 31st The LDP standard remains the same for 2016/17. NHS Highland will continue to reduce the incidents of Meticillin resistant and sensitive staphylococcus aureus (MRSA / MSSA). Focus will be ongoing on reducing the number of: Blood culture contaminants, Skin and soft tissue infections Vascular access device infections In relation to Clostridium difficile infections (CDI), NHS Boards are required to meet the target rate of CDI in patients aged 15 and over, of 32.0 cases or less per 100,000 total occupied bed days. For NHS Highland that means no more than approximately 78 cases in the year ending 31 st March Root cause analysis is undertaken for all applicable CDI and SAB cases using a multidisciplinary approach, and with the appointment of a data analyst for infection Control and prevention the IPCT are in a better position to scrutinise infection data for learning in real-time through the use of a standardised data management system. Work continues within the Operational Units local Infection Prevention and Control groups to review the incidence of infection within their clinical areas. The groups scrutinise the surveillance data from the individual patient case reviews in order to identify learning points, and trend analysis. This includes prescribing information for antibiotics and proton pump inhibitors, along with social and health care interventions. To reduce the incidence of healthcare associated infections a multi-modular approach is required. The correct adoption of effective infection control and prevention methods is a must, alongside maintaining a clean and safe environment, and ensuring appropriate prescribing practices are followed. The Board support the continued work by all on monitoring prescribing compliance of the CDI related antibiotics and proton pump inhibitors, by both acute and community prescribers. The Antimicrobial Management Team (AMT) is responsible for overseeing the implementation of national prescribing data, and reviewing prescribing compliance with antibiotics and proton pump inhibitors across NHS Highland. Alongside the continued monitoring of the three national indicators; Antimicrobial prescribing data, Surgical antibiotic prophylaxis data, and total antibiotic prescribing data, the AMT have also agreed a further three main areas for improvement for the coming year, as requested by the Scottish Antimicrobial Prescribing Group. These are education and training, surveillance of
41 antimicrobial resistance and use, and antibiotic ward rounds. Work on these areas commenced in 2015, and is being reviewed in Performing effective hand hygiene is a key way to prevent the spread and incidence of infection, and within NHS Highland we ask staff and visitors to adopt the use of hand washing and alcohol based hand rubs to support us in achieving this. Hand hygiene audits are undertaken in all clinical areas on a monthly basis through use of the National tool. Compliance rates are displayed in our clinical areas, and presented to our Board members bi-monthly. This process is to be reviewed in 2016 as part of work being undertaken with Healthcare Improvement Scotland in order to gain further assurance. The promotion of good hand hygiene continues to be raised through our training and awareness events. However good hand hygiene is only one part of a multi-modular approach which is required to reduce the incidence of infection. Over the past year the Infection Prevention & Control Team (IP&CT) within NHS Highland have been monitoring the implementation of best practice compliance through the use of Scottish Patient Safety Programme (SPSP) bundles, and nationally recognised audit tools. This includes the monitoring of Standard Infection Control Precautions (SICPs) including hand hygiene and the peripheral venous catheter (PVC) maintenance bundle compliance. Alongside the above specific clinical measures NHS Highland also has processes in place to monitor the clinical environment. The Healthcare Associated Infection (HAI) Monitoring walk rounds continue to occur across NHS Highland. These are led by the Lead Nurse within the Operational unit, and provide a structured framework in which to assess compliance with NHS Quality Improvement Scotland HAI Standards (2015) and the critical elements of Standard Infection Control Precautions as well as other key national policies and standards. A multidisciplinary team conducts an announced or unannounced, walk round; the action plan developed is the responsibility of the Senior Charge Nurses/Team Leaders. This process ensures that staff at the front line of care are embedded in the improvements and actions required to improve and maintain HAI standards. Actions which cannot be progressed at this level are escalated through the existing line management structure. A review of environmental cleaning and standards will be undertaken within 2016/2017 with the aim of reducing CDI. NHS BOARD LEAD: Risk The achievement of reducing the levels of Clostridium difficile infections (CDI) in patients aged 15 and over to 32.0 cases or less per 100,000 total occupied bed days will be challenging. Heidi May, Nurse Director Management of Risk Continued education of prescribers in primary and secondary care on antibiotics and proton pump inhibitors (PPIs). Explore how there can be more infection prevention engagement out with hospital settings. Continued public education to reduce their expectancy of being prescribe antibiotics and PPIs. Continue to share the learning from each case, and ensure optimal good practice is shared throughout the Board. Continued HAI Standards monitoring involving clinical, domestic, estates and infection prevention staff to ensure processes are in place and adhered too.
42 Sustaining compliance with the antimicrobial policy Continued audit to ensure antibiotic prescriptions are compliant with policy and the rationale and duration of treatment is recorded in clinical case note. Continued feedback and interaction with clinical staff by the antimicrobial pharmacists focusing on setting aims for all units to reduce antibiotic use, achieving 95% reliability with surgical prophylaxis and 95% reliability with empiric prescribing policy. The achievement of Staphylococcus aureus bacteraemia (including MRSA) cases of 24.0 cases or less per 100,000 acute bed days remains a challenge. Active support from the NHS Highland Antimicrobial Management Team to GPs, Consultants and other prescribers across Highland to comply with the antimicrobial policy and support the continued education in the use of PPIs. Carrying out root cause analysis on all healthcare associated SABs - identifying any themes for Board Wide action or learning. Gaining clinical buy in to ensure that improvement methodologies are implemented using Scottish Patient Safety Programme Improvement Methodologies. 90 day rapid improvement programmes and the robust implementation of insertion and maintenance bundles for all devices. Explore how there can be more infection prevention engagement out with hospital settings.
43 Priority 4 Person Centred Care Culture, Staff Training and Development Complaints investigation training has been delivered to Investigating officers, managers, clinical staff and other relevant staff. This includes a key focus on taking action to improve services The Can I Help You e-learning modules including how to undertake investigations has been promoted across the Board, however it has accepted that more promotion and use of these modules needs to be undertaken. The Clinical Governance Support Team has updated its resource pack for investigation officers. During the year, complaints talks have been given to a number of clinical specialities and staff groups. More are planned over the next 12 months. Complaints and Patient Feedback is included in the training provided by the Clinical Governance Support Team as part of the ILM management courses run by the Board. In March 2015 a workshop for senior managers was held on the independent Complaints Review Committee process used for social work complaints. Encouraging and Gathering Feedback NHS Highland continues to actively promote methods to encourage patients, families and services users to provide feedback. The NHS Highland website has been reviewed and further developed to provide various mechanisms to provide feedback. The feedback button sits on the opening page of the NHS Highland website and takes the reader to links for the Feedback Team, Patient Advice and Support Service (PASS), Patient Opinion and NHS Inform. In addition to the website, NHS Highland produces a hard copy newspaper which goes to all 150,000 homes across the Highland area. This newspaper provides various ways to make contact for example via Executives, Communications Team and the Feedback Team and is accompanied by positive encouragement to readers to get involved, get in touch, get informed. Patient Opinion is being actively promoted with a prominently placed link on the NHS Highland website. It is being particularly promoted across Argyll and Bute CHP, and Raigmore Hospital and for Maternity Services. An increase in Patient Opinion postings is being noted and we are getting positive feedback from Patient Opinion that we are responding and taking action in a timely and effective way. A number of senior managers have access to view postings, share with staff and provide a rapid response. Frequently an invitation is offered to the person who has posted to get in touch directly with a senior manager. The focus is now on demonstrating improvements made and for Patient Opinion to be widely promoted in all other operational units. We recognise the opportunity to identify improvements via significant event reviews and complex complaint. During 2015/16, work has been ongoing to establish systems to support the identification and spread of learning outcomes associated with significant event reviews and complex complaints. All significant events are presented to the Clinical Governance Committee and Operational Unit Quality and Patient Safety Groups. Patient Stories are increasingly being used at meetings across the Board. Learning Summaries are produced for all SAERs and complex complaint and are shared with the Operational Units. A wide range of other forms of feedback are in place and examples from 2015/16 include the following:
44 A large-scale programme of patient feedback continues using the CARE questionnaire to support medical revalidation. Realtime Feedback How Did we Do is used in the majority of our hospital with results display on local quality boards. Patient and staff feedback continues to be collected for Rapid Process Improvement Workshop (RPIW) projects being undertaken. Improvements A review of the care and treatment of a child resulted in improvements to follow up arrangements for a specific procedure, review of discharge policy and the case has been used as a learning tool for staff. Following a complaint cognitive function screening and assessment has been introduced. Poor communications with family have resulted in records being kept of discussions that have taken place with relatives Concerns were expressed by family about the pain mother suffered and as a result training in pain assessment has been undertaken and new tool being introduced Evaluation of haematology nurse led clinic led to increased focus on medication in consultations, as this had been identified as an issue where some patients were unclear. Also focus on identifying what type of contact patients wanted e.g. face-to-face, etc. In general feedback was very positive. Focus groups were run around the Enhanced Recovery Programme to collect baseline patient feedback on experiences and knowledge of the programme. This will be repeated in 2014 to compare experiences and level of understanding as the programme develops in Raigmore Hospital. Leaflets are now available in pre-assessment to provide information to patients about ERAS (however this is part of the planned ERAS implementation rather than an action as a result of the baseline feedback). Recording and Measurement All formal complaints are recorded in our risk management system Datix. This provides a consistent approach and allows for trends to be identified and linkages made. The actions module in Datix allows all actions from incidents and complaints to be recorded, assigned and monitored. This provides an improved central tracking of making improvements and closing the loop All informal complaints received by the Feedback Team will be recorded on Datix. Dashboard reporting is used to show performance in response times, themes, and number of complaints. Detailed monthly complaint reports are sent to operational unit Quality and Patient Safety Groups for discussion of findings and action. These reports identify actions which remain open, ensuring local teams do not lose sight of the remedial actions which are required to make improvements. On a bi-monthly basis a report is also prepared detailing all open and closed SPSO complaints. This also includes information on recommendations from the SPSO and action taken by the Board. This is presented to each Clinical Governance Committee and discussed at Operation Unit Quality and Patient Safety Groups. Developments from 2015/16 Continuing to pilot capturing real time patient feedback using Patient 365 in Lorn and Islands Hospital Piloting the use of a formic package to gain real time feedback in Out Patient Department Raigmore Hospital
45 Establishing a dedicated webpage on the NHS Highland intranet to sharing learning and improvements following significant adverse event reviews and complex complaints Valuing Feedback Posters are being designed by Medical Illustration to promote ways in which patients, carers and families can feedback about their experiences. These will be display across all sites within the next few months. Piloting a Feedback Cards issued by consultants at Out Patient Clinics. Patient will be asked to provide feedback via an outline site. Developing a process for executive and non executives on a six monthly basis to randomly select complaint responses and adverse event reports to check what action has been taken and feedback to patients/carers/families on outcome. Continue to provide training for staff on dealing with feedback with emphasise being given to dealing with concerns and issues at the frontline. From a strategic commissioning perspective we will be working with the Third and Independent Sector to capture real time client reported outcomes as part of our approach to improving quality in social care settings. Develop and embed person-centred assessment and care planning NHS Highland remains focused on the delivery of person centred care across all services; the Board is explicit in its requirement that individual one to one care, as well as wider service development, is co-produced with the person/people who require the services. Currently the Board is rolling out the NHS Highland Admission Assessment and Personal Care Record and there is a 3 year plan to educate staff and embed. The focus is on person centred care planning and assessment and allows staff to summarise the findings of the assessment and identify planned care. NHS Highlands Admission Assessment and Personal Care record reflects the need to involve the patient and/or their relatives in the planning of care and treatment from both the initial and the ongoing assessments. This dynamic process involves ongoing reassessment and evaluation throughout the individual s period of hospital stay whilst acknowledging their changing/ evolving needs. The NHS Highland Person Centred Assessment and Care Planning Supported Education Plan (June 2015) to support person centred care planning commenced June There is a detailed education plan available. The training plan will embed a person centred approach to assessment and care planning including training and guidance around 5 Must Do s with Me. Included in this work is the following:- Care bundles which are available for nursing assessment of falls risk, pressure area risk and Food Fluid and nutrition in line with national standards. The final work stream is the development of written evidence informed core interventions to support effective care planning. The focus is to ensure that both patients, their relatives/carers are actively encouraged to participate in MDT meetings where care planning is being progressed. Record keeping and care planning is audited across NHS Highland on an annual basis using a revised audit tool which was developed in The annual audit is undertaken more frequently where required or where audit results identify that improvement is required. The audit includes information on how patients have been involved in the planning and evaluation of their care. Results are used to inform improvement plans for each team.
46 Discussions with older people and/or their carers take place to ensure understanding of needs and plans and these are documented in the care plans and progress notes. A family and carer dialogue (as part of main document) sheet is available for staff to record within the admission and care documentation Board rounds, with the MDT (both hospital and community staff) take place in each hospital. These facilitate a more coordinated approach to ensuring that care plans are individualised and are focused on meeting the needs of patients and/or carers. Getting To Know Me The Getting To Know Me (GTKM) booklet has been developed nationally in partnership with Alzheimer Scotland and aims to record important personal information about the person with dementia and to help enhance the care and support they are given whilst they are in hospital. GTKM has been introduced to all ward areas and a prompt for its use is included in the revised nursing documentation. Small tests of change are being undertaken around the use of the GTKM to inform care delivery and to measure the impact of its use. The GTKM is being used to help assist with the communication of key information which is also shared at safety briefs. The initial national focus was on supporting the completion of the GTKM following admission into hospital however it is recognised that this is not necessarily the best time and work is ongoing to promote completion of the GTKM at the earliest opportunity. Work includes supporting the Alzheimer Scotland Post-Diagnostic Link Workers in NHS Highland who work with people newly diagnosed with dementia to complete the GTKM and an article to promote its use has been submitted for the next NHS Highland News which is delivered to all households in the Board area and it was included in the A&B version last autumn. End of Life Care NHS Highland is focused on ensuring that we meet people s wishes for their end of life care this includes discussing with them their preferred place of care, recognising this may change over the course of time. End of life care is an essential part of the person s (and carers ) journey. Treating older people with dignity, compassion and respect during this phase is an essential aspect of holistic care. We recognise that for a significant minority of people, hospital is their preferred place of care at the end of their life & sadly for some people an acute deterioration necessitates assessment & treatment in hospital which they may not recover from so ensuring excellent end of life care in hospitals is paramount. Currently the Board is updating its palliative & end of life action plan based on the Government s publication in December Areas of strength: Multi-professional teams work together with patients and/or carers/families to ensure that individual s wishes and needs are included within their care plans End of life care delivered in our hospitals is person centred, caring and compassionate. New end of life care plan being agreed as part of the new documentation. Staff have been trained in the principles of good end of life care and decision making and these are adhered to. Hospital environments are being adapted as much as possible to cater for end of life care and to facilitate carers/families being present as they require.
47 Strong support for generalist ward based teams from specialist palliative care teams this is provided through face to face contact and consultation as well as using telephone and videoconference facilities as well. Local example of good practice Raigmore - use of treatment escalation plans has increased and audit results demonstrate that this was used sensitively with those people who were going to improve from an acute episode of illness (see audit). The audit also showed good discussions with the person and their carers and completion of DNACPR documentation CPR reviews are in place and monitored through SPSP as part of monthly mortality reviews. Raigmore Hospital palliative care team is available during normal working hours (which includes a doctor from the Highland Hospice) & telephone advice from the Hospice is available 24 hours a day. National Palliative care guidelines are available on the Intranet and an app to guide good practice Plan for reflective session at ward level after a person has died with the Palliative Care Team to improve skills & confidence in caring for people who are dying & offer the opportunity to acknowledge what went well & any areas to improve upon as an ongoing improvement initiative Areas for improvement: Ensuring that everyone who is in the last year of their life has the opportunity to develop an advanced care plan and this is communicated and updated by all relevant staff involved in the person s care Include the outcomes of the treatment escalation plans in the hospital discharge summary for those older people who are discharged Testing & evaluation of the new core care plan for end of life care to improve care An End of life care plan is being developed via the Core Interventions work stream
48 This page is intentionally blank
49 Priority 5 Primary Care NHS Highland faces many challenges across all aspects of Primary Care, these challenges are felt most acutely in the remote and rural areas which often act as a barometer for the rest of Scotland. This requires NHS Highland to think creatively and imaginatively to try and come up with new solutions to ensure services are maintained in a sustainable manner across the area. Much of this creative thinking was pulled together in our submission to the Local Delivery Plan 2014/15 (Local Delivery Plan section Vision for Primary Care). NHS Highland is continuing to work through the local plans presented in the 2014/15 Local Delivery Plan these plans have been reviewed to take into account progress made in 2015/16 and reflect update for 2016/17 and will be submitted to the Scottish Government as a separate addendum to support our Local Delivery Plan.
50 This page is intentionally blank
51 Priority 6 Integration The Highland Partnership NHS Highland, with the Highland Council, has completed four years of the Lead Agency model of integration initiated in A five year plan was agreed at the time of signing the Partnership Agreement now replaced with an Integration Scheme, and the organisations are seeing the benefits of this new way of working across the services. Focussed on the National Health and Wellbeing Outcomes, the priorities for Adult Care have been the development of integrated teams and a single point of access to services, improving quality of care across all care establishments, extending services in the community and testing out new models of care in local communities. The addition of Adult Social Care to the portfolio of services delivered by NHS Highland to support adults, has been extremely valuable and enabled a more streamlined approach to care delivery as well as broadening understanding across all staff groups in relation to Health and Social Care. NHS Highland has appointed a Director of Adult Social Care to ensure the quality of Social Care is of the highest possible standard and to support the profession within the Lead Agency model. Teams working in Adult Support and Protection and the care homes across the public and Independent sectors are driving quality upwards and tackling poor quality care head on. A Large Scale Investigation protocol was developed in Highland to tackle issues of institutional abuse and this has been followed up with a risk assessment tool that will support providers and their staff in avoiding care deterioration. Contracts with the Third and Independent sectors are evolving to reflect quality outcome indicators as well as the more traditional indicators of inputs - processes, training etc. This is a very positive step and has been developed with all as valued and equal partners. The Care Standards Steering group continues to support the delivery of the highest quality care in the care home sector and draws on a number of National initiatives such as Caring for Smiles to ensure care homes and their residents have access to specialist support. With the release of the National core suite of Health and Wellbeing indicators, NHS Highland has been able to further evaluate the Balanced Scorecard which for some time has measured progress across Community Care. Making the links across these indicators and our Quality objectives has enabled us to focus on real evidence and move away from proxy indicators that did not reflect improvements in outcomes. All improvement groups established as part of the strategic commissioning approach, have agreed commissioning intentions for the second year running and are working to refine the indicators and data collected on the Community Care Balanced Scorecard to ensure improvements in outcomes can be measured and that the shifts in models of care, tested out with the aid of the Integration fund, are embedded and sustained. The Highland Partnership has embraced the HQA to Strategic Commissioning, establishing a truly cross sector approach where people who use services, those who provide them, carers and volunteers all have a voice in the planning of adult care provision. This has enabled significant shifts to take place in the provision of services, allowing greater flexibility; better quality; more choice and higher volumes of service to be delivered. District Partnership were established at the time of integration to enable clinicians, managers Elected members and the community to come together to discuss how to progress redesign at this District level and also enable the capturing of progress and issues. Though evolving at different paces, these partnerships are now seen as key platforms to support locality planning and community empowerment in line with new legislation. The Community Planning Partnership are working closely together to ensure information is readily available at District levels, support and expertise is shared from a variety of sources and that communities are able to make informed choices about services and facilities in their local area.
52 Details of how the Board will play its role in supporting Health and Social Care Partnerships in shifting the balance of care and supporting the achievement of the national health and wellbeing outcomes for Integration is contained in the Strategic Commissioning Plan and the Commissioning Intentions (2015/16) which have already been lodged with the Scottish Government. These Plans also reflect the LUCAP operational plans to change patient flow and acute hospital usage. Argyll and Bute Health and Social Care Partnership Within the Argyll & Bute Health and Social Care Partnership the decision has been taken to adopt the Pyramid Performance Management System successfully used by Argyll and Bute council. This balanced scorecard system will give the HSCP accurate and timely performance reporting information cascaded throughout the organisation both strategic and locality level incorporating local and national performance outcomes. The Integrated Joint Board (IJB) have already agreed a series of measures taken from the current Adult, Children and Families, and NHS Highland Balanced Scorecard/ A&B operational unit-ldp performance scorecard. These performance measures have been aligned against the nine national Health & Wellbeing Outcome Indicators and associated twenty three sub-indicators. It has been agreed that the IJB will receive monthly exception reporting using the Pyramid scorecard, commencing in March Performance reporting will be available to the IJB and HSCP management team as a Phase 1 development using Pyramid to give them an operational overview of their local performance against the HSCP Objectives and targets as detailed in its Strategic plan. In addition there is a wider performance review and migration plan under development which will ensure that all current performance activity is assessed and reviewed against the new Health & Wellbeing Outcomes reporting framework, this work is extensive and will be ongoing throughout This ongoing development will look to identify, review and streamline wider HSCP performance reporting associated with; Adult and Children & Families Services, Single Outcome Agreement- Community Planning Partners, Integrated Children & Young People Service Plan, Integrated Care Framework, Clinical & Care Governance and Locality Planning Groups. The reporting frequency and lines of accountability supporting the performance reporting for the HSCP have been clearly identified within the A&B HSCP Planning & Performance Management Framework (PPMF), linking all performance activity to patients and user feedback and experience. The development of Locality Planning Groups (8 in total), are developing performance core data sets alongside locality public health profiles as part of the tooling up of localities capability and capacity to support the transformation of health and social care services at locality level to deliver our vision People in Argyll and Bute will live longer, healthier, independent lives The performance management process sits alongside the HSCP planning process at both strategic and locality level to ensure the transformation activity aligns with the HSCP target and objectives and notably focusing on: Reduce avoidable emergency admissions to hospital and minimise the time people are delayed Support people to live fulfilling lives in their own homes for as long as possible Support unpaid carers to reduce the impact of their caring role on their own health and wellbeing Implement a continuous improvement approach Support staff to continuously improve the information, support and care they deliver
53 Efficiently and effectively manage all resources to deliver Best Value Thereby supporting and facilitating the change in profile of services as captured in the A&B HSCP strategic plan as to What we will look like in 3 years time These core performance data sets will be updated on a quarterly basis to support and direct locality planning groups evidencing change and service performance within the virtuous continuous improvement cycle In relation to the current reporting arrangements with NHS Highland, work will be ongoing through 2016 to establish and develop a clear reporting and governance framework in line with the national performance guidance. This will also include how analytical and system resource and services are deployed across the NHS Highland Board and the Integrated Joint Board. Finally work has commenced to address key reporting and data requirements covering acute services provided by NHS Greater Glasgow and Clyde under our SLA as an integral part of their whole system planning and commissioning of services to achieve not only shifting the balance of care but also shifting acute resource to primary and community services accordingly.
54 This page is intentionally blank
55 Priority 7 Scheduled Care North Highland A detailed programme of work has been developed to support the delivery against Scheduled care target compliance for NHS Highland this involves three distinct strands of development. 1. Treatment Times Guarantees (TTG) 2. Out-Patient (OP) waiting times 3. Raigmore Hospital Critical Services Upgrade Project 1. Treatment Time Guarantees A development programme to support the sustainable delivery against access targets for all Medical and Surgical specialities is in progress. This programme of development has already delivered a zero breach waiting times position against Treatment Time Guarantees for all Medical Specialities and a number of Surgical Specialities. A number of surgical specialities require ongoing development work to deliver reliably against Treatment Time Guarantee standards, Ear Nose and Throat (ENT), Oral Maxillo-Facial Services (OMFS), Ophthalmology, Orthopaedics, Urology and Community Dental. 2. Out-Patient Waiting Times Arrangements are in place to deliver the expected standards in relation to Out-Patient Waiting times. All medical specialities are reliably delivering a zero breach position against the out-patient waiting times standards. Trajectories have been developed to support the delivery of a zero breach position against the required waiting times standards. Monitoring arrangements are in place and the transformation programme to support the changes required to deliver sustainable and affordable Out-Patient Services are being progressed via the NHS Highland Board wide, Transforming Out Patients high level value stream. 3. Raigmore Hospital - Critical Services Upgrade Project The Critical Services Upgrade project involves the relocation of existing critical service departments to the ground and first floors of the Tower Block at Raigmore Hospital to improve adjacencies to each other and the theatres. This requires extensive refurbishment of the Ground & First floors to accommodate: Ground - CCU / MHDU / TRIAGE First - ICU & SHDU A key objective of the Critical Services Upgrade Project is to upgrade the environment of the Critical Services accommodation within Raigmore Hospital through the following: Upgrade Fire Safety, Ventilation, HAI infrastructure to modern standards Upgrade the internal environment for delivery of patient care Address deficiencies associated with current Critical Care Wards and Theatres The project deliverables will address the shortcomings noted above and provide modern healthcare facilities which will enable staff to provide a vastly improved level of service to vulnerable patients. The project also includes extensive refurbishment of the Theatre Block resulting in: Refurbishment of 9 existing theatres Construction of 1 additional fully compliant theatre 7 of 10 theatres will have Ultra-Clean Ventilation (UCV)
56 Construction of storage room on roof of theatre block Installation of new air handling units on the roof of theatre block The proposed investment allows for the replacement of the modular theatre which is currently leased by NHS Highland, with an SHTM compliant theatre within the theatre block which will provide a more efficient and productive facility in terms of adjacency to ancillary facilities and personnel. The investment will provide facilities which enable Raigmore Hospital to achieve its strategic objectives and deliver a healthcare service which is commensurate with its status as the main acute hospital in the Highland region. The construction programme for the works is anticipated to begin in April 2016 and complete in December These dates are subject to the final approval of the Full Business Case by the Scottish Government s Capital Investment Group. Argyll and Bute Argyll and Bute HSCP Strategic plan details the transformation of health and social care services delivered at locality level to achieve our vision People in Argyll and Bute will live longer, healthier, independent lives The operational services which have been delegated to it means that its Integrated Joint Board is responsible and accountable for scheduled care planning and delivery at both strategic and locality level to ensure the transformation activity aligns with the HSCP target and objectives and notably focusing on: Reduce avoidable emergency admissions to hospital and minimize the time people are delayed Support people to live fulfilling lives in their own homes for as long as possible Support unpaid carers to reduce the impact of their caring role on their own health and wellbeing Implement a continuous improvement approach Support staff to continuously improve the information, support and care they deliver Efficiently and effectively manage all resources to deliver Best Value Argyll and Bute HSCP will therefore continue to work towards achieving all of the access targets for which it is accountable for as part of a whole system approach working in Partnership with NHSGG&C who is its provider of secondary care services. Strategic level engagement is currently ongoing to strengthen, develop and sustain patient care pathways into secondary care services in Glasgow and Clyde for Argyll and Bute residents who cannot be seen or treated locally in our RGH, Community and mental health hospitals. Outpatient services. The HSCP plans to maximise patient choice by providing and commissioning services in settings that are closer to home thus more accessible to patients in remote rural and island communities. This will incorporate: Service Provision Capturing and identifying patient feedback at locality level of their experience of accessing outpatient services in: o NHSGG&C o Local clinics
57 Using this information/evidence to inform service redesign, activity modelling and identifying local alternatives where appropriate or systems and processes to ease the burden of travel e.g. appointment times, transport links etc Developing local capability and capacity to provide and a sustainable specialist outreach outpatient service, triaged and supported by practitioners and the voluntary sector e.g. Dermatology, Pain relief, Ophthalmology (Macular degeneration local Lucentis clinic) and Obstetrics, MSK and triage which are specialities under waiting time and TTG pressure Further developing the range and profile of telehealth clinics beyond teleneurology Increase the use of telephone consultations particularly for return appointments- (feedback from patients value this instead of a 4 hour journey for a 2 minute consultation) Quality, Efficiency and Effectiveness Reducing the use of waiting list initiatives which incurs excessive cost and is an unplanned burden and cost on staff and processes (in A&B and NHSGG&C) by undertaking further DCAQ work and agreeing and commissioning appropriate base line service with NHSGG&C ensuring patients safety and clinical quality of the service. The cost of Waiting list initiatives for 2015/16 was 20,375. Developing a formalised remote decision support pathway/service with secondary care triaging out unnecessary GP referrals- building from the lessons learned as part of NHS Highlands HQA. Aggressively pursuing actions to reduce our DNA rate (see graph below) by further rolling out text alerts Applying SOPs for medical record systems and developing single point of contacts for patient appointments. Taking forward in Argyll and Bute as part of a redesign of medical records exploring contact centre service with Argyll and Bute council for patient appointments possible on line appointment service. Graph 1 New and Return DNA rates in Argyll and Bute HSCP.
58 Outcome/Requirements A more focused, locality owned and strategic approach to outreach service planning and delivery has been identified by both the HSCP and NHSGG&C to provide a higher quality more sustainable, consistent and safe AND appropriate service model matching demand to supply and preventing unnecessary appointments or patients and patient activity into NHSGG&C. For 2014/15 the total number of Outpatient appointments in A&B was 9830 and the total number of outpatients seen in Glasgow was (see graph 2 below). This will require additional investment and front loading of our redesign of service models in 2016/17 and support from the national programme team to put in place these plans. Specifically we are looking at: National scheduled care programme support Collaborative working with NHSGG&C to streamline pathways A whole system review of planning and support of services with the RGH Graph 2 New Outpatient Activity A&B and NHSGGC. Elective Inpatient and Day Case services. Argyll and Bute accesses virtually all of its specialist treatment services in NHSGG&C with the exception of General Surgery and General Medicine secondary care services which are provided
59 from the Rural General Hospital in Oban for the Western catchment area of Argyll and Bute (circa 46,000) Table 1: Day case, Elective Inpatient & Non Elective Inpatient Activity General Medicine & General Surgery, Lorn & Isles Hospital 2014/15 Hospital Name Lorn and Islands Hospital Lorn and Islands Hospital Discharge Specialty General Medicine General Surgery Day case Elective Inpatient Totals Totals 1, ,757 Lorn and Islands Rural General Hospital Within the immediate 1 year and 3 year time frame these core acute service with Lorn and Islands are under significant service sustainability pressure due to inability to recruit to Consultant posts as follows: There are 2 consultant physician vacancies out of an establishment of 3 and have been unable to recruit after 2 ½ years of trying. The substantive consultant is likely to retire in the next 2 years. Anaesthetics 1 vacancy covered by fixed term locums from Poland. General surgery will have a retiral in 1yr and have experienced difficulties in recruiting (3 years previously). Outreach day case urological service Vacancy due to shortage of consultants Recent successful recruitment to one of the consultant physician posts has afforded a degree of security, within the medical services, however it is still recognised that the service is vulnerable. There is need for an urgent review and development of an appropriate RGH core service model maximizing local access as well as appropriate and rapid access to NHSGG&C supported by strong clinical pathway, professional and governance links. A review group will be established in May 2016 to undertake this work. This review will include current national best practice and models for remote and rural healthcare, while taking cognisance of local demographics. A project plan will be completed by July 16, with and 2 year implementation timescale. It is anticipated that the same requirements exist for Surgery and Anaesthetics within the 3 year window. Outcome/Requirements As detailed in the outpatient section a strategic whole system planning approach is to support this General Service as part of an obligate network and integrated clinical pathway with NHSGG&C to provide a viable and sustainable service.
60 Exploration as part of the national scheduled care programme support with regard to establishment of obligate network service alongside maximising local elective diagnostic provision, enhancing preoperative and post operative rehabilitation provision within TTG and cancer care pathways. Mental Health Scheduled care In line with current delivery of modern mental health care, a review has implemented a community focussed service, with an appropriate number of acute in-patient beds and a small IPCU in Lochgilphead. However the current mental health estate is no longer fit for purpose and the HSCP are currently considering options to improve this, by either relocation to an area within the adjacent community hospital or a new build. There are ongoing difficulties with consultant recruitment in A&B, and have requested an external review of the medical model, from the Royal College of Psychiatry and support from JIT to ensure the HSCP are implementing an appropriate mental health service for A&B. This may include consideration of the viability and appropriateness of the ICPU, and potential for closer working with NHS GG&C. The adult Mental Health Service in Helensburgh & Lomond is provided by GGC under SLA and all inpatient pathways are into NHS GG&C. The CAMHS service in A&B is provided by a small multi-disciplinary team with the exception of Cowal & Bute whether the service is provided by NHS GG&C under SLA. There is no in patient provision within A&B and any requirement for specialist in patient intervention is via the SLA with GG&C. The challenges in providing outpatient services to this patient cohort are well evidenced and some of the actions planned in 2016/17 outlined in the outpatient section above will be applied to this mental health service.
61 Priority 8 Unscheduled Care North Highland Raigmore Hospital within the Inner Moray Firth Operational Unit is engaging via the National Unscheduled Care Collaborative to support embedding improvements to facilitate the sustainable delivery of the 95% Emergency Department Four Hour Target. Within the newly developing Inner Moray Firth Operational Unit a Medical Flow value stream has been established. This improvement programme is aiming to deliver smoothed flow for medical patients into Raigmore Hospital, through the hospital and out into the community. The programme is embedding admission avoidance strategies as well as improved discharge planning with a view to reducing the number of delayed discharges that are generated as a result of hospital admission. Specific actions that are being progressed as a priority are: Daily review of the circumstances and reasons for breaches occurring within the emergency department and associated actions and improvements to support continuous improvement All patients to have a plan for exit from the emergency department by 120 minutes plus associated escalation to gain support as required for obstacles to discharge from the department Enhancing and continuous development of the Inner Moray Firth Quality and Patient Safety Huddle Closer alignment and communications of community and acute hospital management teams Enhanced discharge planning to support a higher percentage of patients to be discharged before 11am Improved information sharing in relation to patients with more complex discharge across acute and community teams to support shortening length of stay Enhanced rehabilitation and day services for older and more frail patients Enhanced Ambulatory Emergency Care Increasing the capacity for medical ward rounds to support increasing the number of weekend discharges Increasing the capacity for acute receiving at key pressure points through out the week Enhancing transport arrangements through out the week to support patients leaving the hospital Increasing capacity and sustainability of care at home services in the Inner Moray Firth Area to provide increased choices for people to remain in their own homes. The Rural General Hospitals in Wick and Fort William have also been engaging with the national collaborative work to deliver local action to improve delivery of the four hour target. Actions have included Sustained delivery of clinical leadership through acute board rounds and community huddles; Focus on the further development of community pull with enhanced discharge planning to support the creation of capacity/ improved patient flow improved integration between hospital and community to better support the patient journey Implementation of creative approaches to allow more people to be cared for in their own homes. Future initiatives in N&W will include - Review the availability of consultant ward rounds to meet acute care standards
62 Ongoing review and redesign of Caithness General Hospital to improve flow and capacity in ED and ensure improved flow across the RGH Enhancing local escalation processes to ensure that pan Highland escalation actions are aligned. Ongoing development of Integrated District Teams Enhancing Care at Home and continue to develop growth of Independent Sector Devolve Care at Home NHS provision into District Teams to provide localised Enablement The Highland Quality Approach to quality improvement and closer joint working across acute and community services will underpin these developments as will the continuing development of integrated health and social care teams with the expansion of initiatives such as virtual ward, hospital at home and the creation of additional capacity in local care facilities. As with Priority 6 (Integration), details of how the Board will support Health and Social Care Partnerships to shift the balance of care and achieve the national health and wellbeing outcomes for Integration is contained in the Strategic Commissioning Plan and the Commissioning Intentions (2015/16) which have already been lodged with the Scottish Government. These Plans also reflect the LUCAP operational plans to change patient flow and acute hospital usage. Argyll and Bute In Argyll and Bute, the unscheduled care plan focused on the 6 Essential Actions Programme. This was implemented in Lorn and Islands Hospital in Oban a Rural General Hospital, but the same principles were applied to the 5 community hospitals and the Progressive Care Centre to ensure equity. The implementation of daily huddles has ensured timely communication and planning within all hospitals. Refocusing on a patient management ethos rather than bed management ensures a more person centred approach. Key improvement areas; 4 hour target. Clinical Leadership and escalation. Short Term assessment beds. Lead Professional Model Admission, Discharge and Transfer Policy Intermediate Care Model Community Pull Through AHP ED Response. Areas for continued Improvement: Pathway for medical assessment. Decreased number of boarders and cancellations of elective procedures Implementation of the Basic Building block capacity alignment plan. Care at Home provision 7 day access to services Adults with Incapacity This programme is monitored through the Argyll and Bute Unscheduled Care and Delayed Discharge Groups.
63 Priority 9 Mental Health NHS Highland adult psychology services have reviewed waiting lists and identified the areas of particular pressure. A mental health needs assessment is complete and reported in March This work reviewed referral patterns and confirmed that depression is the main reason for referral to services. The top 2 client groups with longest waits are patients waiting for Neuropsychology assessments/ treatment and patients waiting for treatment for trauma. The service as a whole is amending its approach. The strengthening of screening and assessment of referrals will move the service towards a more matched approach with no direct referrals accepted to individual departments. We anticipate the lower level intervention, higher volume approaches, e.g. Decider Life Skills programme will successfully address a number of patients needs at the Primary Care level and remove the need for them to move on to waiting lists for other more specialist services. Expansion of psychological therapies Personality disorders we will train staff across NHS Highland and support them to provide STEPPS programmes for patients with personality disorder. Trauma we will train staff and support them to provide Survive and Thrive group courses for patients awaiting one to one therapy for trauma. We will seek resources to expand the training of staff qualified to provide therapy for patients with simple and complex trauma. The trauma Steering Group will define the clinical pathway to ensure the correct matched intervention following assessment. The aim is to develop a trauma informed service where each patient at assessment is asked if there has been a traumatic event in their life and if so, directed to the recommended level of intervention. Depression we will train and support staff to provide Behavioural activation groups for depression as the first treatment choice. We will also train and support staff to provide Mindfulness based cognitive therapy for depression. Psychosis We will implement Behavioural Family Therapy for patients with psychosis. Autism we will seek resources to provide Clinical Psychology input to autism services to assist diagnosis of adults and commence treatment Neuropsychology we will seek resources to ensure the Neuropsychology service is at the recommended level for the NHS Highland area. Technology enabled care We will explore the implementation of Beating the Blues on line based treatment as part of the Mastermind programme. This will be aimed at supporting Primary Care. The utilisation of video conferencing to deliver therapies and support to patients remote from therapists will be expanded. A model of providing initial face to face assessment appointments for Psychological therapies with treatment delivered via video conferencing/ telephone support will be expanded. The NHS Highland Eating Disorder service and Cognitive Behavioural Therapy service will adopt the use of FLORENCE as a motivational and support tool.
64 Patients in distress - NHS Highland received support via the Innovation Fund to support patients experiencing distress. This service commences on 1 July The evaluation of this will inform future development.
65 NHS Highland Part 2 LOCAL DELIVERY PLAN STANDARDS
66 NHS LDP Standards People diagnosed and treated in 1st stage of breast, colorectal and lung cancer (25% increase): 31 days from decision to treat (95%) 62 days from urgent referral with suspicion of cancer (95%) Early diagnosis and treatment improves outcomes. The Detect Cancer Early (DCE) Programme aims to increase the proportion of patients diagnosed with cancer at the earliest stage, focussing particularly on bowel, breast and lung cancer. In light of data showing that the proportion of individuals resident within NHS Highland detected with early stage lung cancer is lower than that of several other Boards, ongoing efforts will be made during 2016/17 to improve this, building on work that took place in 2015/16. A Health Promotion Officer with responsibility in relation to the DCE and cancer screening programmes was appointed during late In collaboration with colleagues across Primary and Secondary Care, they will seek to take advantage of opportunities to promote informed participation in cancer screening and encourage people with symptoms suggestive of cancer to consult their GP as soon as possible Performance against national cancer waiting times remains of concern both at Board level and at national level. These results have been for a large part due to national staffing shortages in cancer specialties, particularly within Oncology itself but also within Urology. The Board is engaged in a number of approaches to increase capacity; working closely with colleagues in NOSCAN and the other Cancer Centres with the aim of creating and sustaining a robust, sustainable service; and engaged in diagnostic and small professional workforce planning groups on a regional and national basis, to address workforce supply issues. People newly diagnosed with dementia will have a minimum of 1 year s postdiagnostic support Enable people to understand and adjust to a diagnosis, connect better and plan for future care Younger peoples memory clinic operational policy has been reviewed and people are being seen by psychiatrist, psychologist and nurse before referral to dementia support worker. A review will take place in one year to assess effectiveness of new systems. The commissioning of Alzheimer Scotland to provide the post diagnostic support service has been recently extended until March 2018 in the North Highland Operational Units. The AS Link workers are present in every area of Highland bar Caithness where the local Older Adult Mental Health Team provides the support. The service evaluates well and it is becoming clear that GPs are now referring people earlier in the disease stage as confidence in the available support grows. 12 weeks Treatment Time Guarantee (TTG 100%) 18 weeks Referral to Treatment (RTT 90%) 12 weeks for first outpatient appointment (95% with stretch 100%) Shorter waits can lead to earlier diagnosis and better outcomes for many patients as well as reducing unnecessary worry and uncertainty for patients and their relatives. 12 weeks TTG NHS Highland will continue to work with the Scottish Government to move towards the delivery of zero patients waiting over 12 weeks. 18 weeks RTT NHS Highland have made progress in resolving many of the issues arising from the implementation of TrakCare PMS, but are still not in the position to implement the RTT module. NHS Highland completed the work on admitted pathways
67 and are progressing with the non admitted and combined pathways. Improvement in this area will be assisted by improvements in 12 week TTG position and 12 week First Outpatient Appointment target. 12 week First Outpatient Appointment target NHS Highland will commence local reporting based on TTG rules in the summer and continue to work with the Scottish Government to move towards the delivery of zero patients waiting over 12 weeks. At least 80% of pregnant women in each SIMD quintile will have booked for antenatal care by the 12th week of gestation Antenatal access supports improvements in breast feeding rates and other important health behaviours. NHS Highland will continue to meet this target. Eligible patients commence IVF treatment within 12 months (90%) Shorter waiting times across Scotland will lead to improved outcomes for patients. NHS Highland will work with colleagues in NHS Grampian and NHS Greater Glasgow and Clyde to ensure that this target continues to be met for NHS Highland patients 18 weeks referral to treatment for specialist Child and Adolescent Mental Health Services (90%) Early action is more likely to result in full recovery and improve wider social development outcomes. North Highland Recruitment remains a challenge with it not being possible to recruit to a third consultant post in the Highland HSCP Service. There is a new leadership team in the service which is presenting further opportunities for service design and delivery. A RPIW was undertaken in 2015 and this identified a range of areas for improvement. The outcome has been a further refresh of administrative processes and the service is now confident that waiting list information is accurate and that administrative systems are improved. The North of Scotland Tier 4 CAMHS in patient unit opened in May Additional resource has been identified for intensive community support for Tier 4 patients working with the North of Scotland Tier 4 Service. The additional capacity will support the achievement of the 18 week RTT. Work is in progress to scope options for increasing CAMHS capacity for Looked After Children and Young People in foster care and residential units in the first instance. There is related work to start later in the year with regard to services for children and young people with distress and transitions. During 2016 there will be an extensive CAMHS process mapping exercise involving a wide range of services across the early years, school years and transitions involving CAMHS 1-4, education, adult mental health services and the police. Care and Learning Highland Council The Primary Mental Health Workers participated in the HHSCP CAMHS RPIW and are working with the HHSCP Tier 3 service to ensure seamless processes across Tier 2 and Tier 3. The team now have a manager who is leading on improvement work for the service. There will be joint work with the HHSCP service to look at the Primary Mental Health Worker contribution to Looked after children and young people.
68 Argyll and Bute The service undertook a process mapping exercise in 2015 which informed service design and operational procedures. Additional psychology resource has been added to the team. The team are scoping options to improve Tier 4 services 18 weeks referral to treatment for Psychological Therapies (90%) Timely access to healthcare is a key measure of quality and that applies equally to mental health services. The ISD statistics for the period ending December 2015 highlights that 96.1% of people were seen within 18 weeks of referral to psychological therapies treatment in NHS Highland. NHS Highland was one of five boards achieving the target. There has been a significant amount of work done with the admin team to ensure the data is as accurate as possible. The plan is to repeat the DCAQ during 2016 to maintain the progress and to match patient need with therapists. The psychological therapies strategy for NHS H has been completed and a group has been formed to develop an operational plan. Clostridium difficile infections per 1000 occupied bed days (0.32) SAB infections per 1000 acute occupied bed days (0.24) NHS Boards area expected to improve SAB infection rates during 2015/16. Research is underway to develop a new SAB standard for inclusion in LDP for 2016/17. See Priority 4 Safe Care Clients will wait no longer than 3 weeks from referral received to appropriate drug or alcohol treatment that supports their recovery (90%) Services for people are recovery focused, good quality and can be accessed when and where they are needed. See Priority 1 Health Inequalities & Prevention Sustain and embed alcohol brief interventions in 3 priority settings (primary care, A&E, antenatal) and broaden delivery in wider settings Sustain and embed successful smoking quits, at 12 weeks post quit, in the 40% SIMD areas Enabling people at risk of health inequalities to make better choices and positive steps toward better health. See Priority 1 Health Inequalities & Prevention 48 hour access or advance booking to an appropriate member of the GP team (90%) Often a patient's first contact with the NHS is through their GP practice. It is vital, therefore, that every member of the public has fast and convenient access to their local primary medical services to ensure better outcomes and experiences for patients. This is a nationally measured target.
69 Sickness absence (4%) A refreshed Promoting Attendance Partnership Information Network Policy will be published in NHS Highland continue to monitor sickness absence regularly through our Staff Governance Committee and staff at all levels in the organisation are encouraged to actively manage sickness levels appropriately. 4 hours from arrival to admission, discharge or transfer for A&E treatment (95% with stretch 98%) High correlation between emergency departments with 4 hour wait performance between 95 and 98% and elimination of long waits in A&E which result in poorer outcomes for patients NHS Highland plans to continue to meet the 95% target and work towards the 98% stretch target through 2016/17. The delivery of this target is tied in with the Local Unscheduled Care Programme (LUCAP) which has prioritised work in the community to ensure patients are maintained in their local communities for as long possible, and if patients have to be admitted they flow through the hospitals as smoothly as possible. Operate within agreed revenue resource limit; capital resource limit; and meet cash requirement Sound financial planning and management are fundamental to effective delivery of services. See Part 3 Financial Planning
70 This page is intentionally blank
71 NHS Highland Part 3 Financial Planning
72 NHS HIGHLAND FINANCIAL PLANNING 1. Headlines Break-even position over the period of the plan o Savings targets for 2016/17 total 28.8m with 2.3m currently unidentified an improvement from March submission o Compares to 16m in 2015/16 Non-recurrent savings carried forward to 2016/17 have reduced to 3.1m in 2015/16. Capital in balance but extremely challenging Cost pressures will need to be contained. 2. Revenue Core RRL NHS Highland s LDP assumes financial break-even over the five years of the plan. With a 3m expected recurrent deficit. The LDP assumes a steady reduction in the reliance on nonrecurrent resources down to an annual expectation of 3m, which will continue to be a planning assumption going forward each year. This relatively small amount (less than 0.5% of baseline) will effectively be used in a planned way rather than to underwrite recurrent resources. Assumptions and risks within the RRL are discussed below. Continued progress has been made in reducing the non-recurrent carry forward from 5.6m at the start of 2015/16 to 3.1m an improvement on the 4m expected in the LDP signed off in 2015/16. Movements in core RRL expenditure are consistent year on year to take account of inflation and planned achieved savings. 2016/17 includes uplifts as announced by SG including 1.7% general uplift 9.42m, 15.25m Social care funding see further detail below, as well as 1m of further NRAC parity adjustment. Future years assume 1.8% uplift going forward. Latest NRAC parity information show NHSH s share of the 30.5m national NRAC parity funding, for mainland Boards, is 1m whereas, to maintain its current NRAC position, Highland s NRAC share would need higher. This lower-than-nrac share means that NHSH has moved further away from parity being at 1.33% below, a further 1.75m would be required to bring NHSH to the 1% target. New medicines fund expenditure and allocations have been incorporated in line with estimates while waiting for guidance to be issued by SG finance colleagues. 1m of final brokerage repayment is also included within the financial plan for 2016/17 Argyll & Bute Integrated joint Board An Integrated Joint Board (IJB) for Argyll & Bute was formally established on 18 August The IJB is not permitted to manage resources until it has approved its Strategic Plan. The Plan was approved by the Board on 23 February 2016, Argyll & Bute Council on 17 March 2016 and is due to be approved by the IJB on 23 March Subject to this final approval the IJB will be able to manage resources and the intention is for this to become effective 1 April As part of this process, both the Board and Argyll & Bute Council are required to propose an initial payment offer to the IJB. Due to the timing of meetings (i.e. the IJB meeting on 23 March 2016
73 and the Board meeting on 5 April 2016) an offer in principle has been made by the Director of Finance, subject to Board approval. The vast majority of this offer is relatively straightforward since it is determined by Argyll & Bute s formulaic share of total Board resources. Social Care Funding In addition to the baseline uplift, the Board will receive 15.3m as its share of a national allocation of 250m in respect of Adult Social Care (ASC). Of this, 4.6m relates to Argyll & Bute and will form part of the initial payment offer referred to above. An approach to utilising this funding has been agreed in principle between the Board, Argyll & Bute Council and the IJB. This will be formally considered when the IJB meets on 23 March 2016 to consider the IJB s draft Quality & Finance Plan this includes a recommendation to accept the Board s Initial Payment offer. The remaining 10.7m relates to Northern Highland. Agreement for utilising this has been reached with The Highland Council (THC), which must be seen in the context of 2016/17 being the fifth year of the Lead Agency agreement and the third year of the three year financial agreement. The third year of the financial agreement was broadly predicated on THC receiving a flat cash settlement from the Scottish Government (SG) and then providing 1.4m increase to the funding made available to the Board in order to deliver ASC services ( the quantum ) i.e. a net increase of 1.4m. However, THC s grant settlement for 2016/17 is a reduction of 4.31%. The agreement reached with THC is that this reduction will be passed on to the Board via a 4.31% reduction in the quantum (equivalent to 4.1m). However, THC agreed to honour the 1.4m investment as planned thereby resulting in a net reduction of 2.7m. In effect, this will be the first call on the 10.7m of new funding, leaving 8m available for inflation, cost pressures and growth. A significant call on this remaining funding will be the Scottish Government s policy of introducing the Scottish Living Wage from 1 October It is anticipated that the impact of pay awards, national insurance increases, living wage, care home contracts uplifts and continuing demographic pressures will exceed the 8m available. The Board s strategic position is to protect ASC from the impact of austerity as far as possible but clearly efficiency savings will still need to be pursued where appropriate. In effect these will form part of the wider health and social care savings programme for the Inner Moray Firth and North West Highland units. 3. Revenue Non Core RRL Depreciation for 2016/17 is calculated on expected spend in year, with uplifts in future years based on proposed expenditure as per the NHS Highland Capital plan. AME impairments have been estimated at 2m in 2016/17, mostly for A&B Hospital with no impairments for future years identified at present, but this is subject to change as the timing of the redesigns for Argyll & Bute Mental Health Services, Badenoch & Strathspey and Skye, Lochalsh and South West Ross are finalised. AME provisions have been estimated using the information available to date, through closer work with SPPA around pensions and injury benefits provisions are now more robust. In line with national work on financial flexibility, the Board will be seeking further AME funding of 1.6m in relation to pre-2010 provisions. AME donated asset depreciation has an increase in 2016/17 due to the donated funding for the Children s ward at Raigmore completing at the end of 2015/ CRL Expected funding for Core Capital is 21.5m, this includes 6.6m of formula funding, 8.6m of continued investment in Raigmore Critical Care, 2m agreed return of prior years brokerage, and just over 4m of proposed developments and other schemes over 1.5m which are currently in discussion with SG colleagues.
74 Core Capital expenditure forecast for 2016/17 includes continuing costs associated with the Raigmore theatres and critical care reconfiguration, purchase of land for the proposed Badenoch and Strathspey development, and some hospital rationalisation as part of the 4m mentioned above. After legally committed schemes, there is a considerable focus on statutory compliance and backlog maintenance expenditure, which is urgently required to comply with regulations across a number of sites and despite in excess of 2m being earmarked for this purpose each year, the amount is considerably less than has been assessed as needed - however we endeavour to remain on track to eliminate all high risk backlog maintenance according to the timetable shown in the asset management strategy. For a further year and for the foreseeable future, equipment and service replacement programmes have had to be curtailed to live within the CRL and this applies to IM&T, Medical Equipment and Radiography. Any major equipment failures in year will present a considerable risk. A total of 6.7m of 2016/17 s CRL has been put against these replacement programmes though this only covers the risk prioritised as red. There is a small contingency of less than 0.3m set aside to mitigate any further potential risk. Efforts will be required to deliver the Capital programme over a number of years and work to progress this will continue throughout the year. The proposals around Raigmore - as set out above - need to be viewed in the context of the Inner Moray Firth Masterplan. This piece of work is the first of its kind in NHSScotland. It is anticipated that this will identify opportunities for improving space utilisation as well as for providing care in more appropriate settings. It may also result in opportunities for disposing of properties that require significant backlog maintenance investment. There are a significant number of schemes with varying levels of costs, currently these are not funded though are under discussion with Scottish Government, so included on the Capital plan as proposed these range from hospital and building rationalisation to ehealth national and strategy schemes. Further info on these schemes are below shown on appendix I. 5. Efficiency Savings A savings target of 28.8m is required in order to deliver breakeven. Of this 25.8m is a recurrent target and 3m non-recurrent this relates specifically to the brokerage repayment and other non recurring pressures. This target is considerably higher than 2015/16 and previous years, mainly as a result of the requirement of additional costs around employers NI in 2016/17 and continued pressures on both primary and secondary care drugs. In addition to this, there are significant costs pressures as a result of the implementation of the living wage especially in Independent Sector care homes and care at home providers as well as the FYE of Adult Social Care packages of care. 6. Assumptions A number of assumptions underpin the plan; A reduction in the non-recurrent carry forward to 3.1m Continued funding from New Medicines Fund for IPTRs New SMC approvals for drugs assumed as orphan, ultra orphan or end of life care are also funded from new medicines fund as per guidance.
75 No further increase in the national target for the treatment of Hepatitis C and therefore 45 new drug treatments in Northern Highland and 11 in Argyll & Bute are factored into the plan. Salaried Dental Services reduction in allocation of 5% Appropriate Funding is received to support the achievement of TTG Raigmore Hospital (now part of the Inner Moray Firth Operational Unit) and North & West Units are estimated to have significant levels of overspend by the end of the financial year. Whilst the plan assumes funding for around half of the recurrent overspend, both Units are required to reduce their cost base by a similar amount during the course of the financial year. Pay uplifts of 1.7%. This figure includes pay awards for staff of 1% as per current guidelines and incremental increases which have been estimated using our usual method of person by person calculations along with the implementation of living wage and these have resulted in an uplift of over 7.0m. Employers NI increase is included in the inflation calculations amounting to 6.7m. The plan assumes AME funding of 1.6m in relation to pre 2010 provisions and that SG will issue a guidance note relating to the appropriate treatment of this funding Prices include uplifts in non pay including CNORIS, prescribing of over 7% Hospital drugs of 12% (this takes account of estimated impact of drugs relating to Rare Conditions, Very Rare Conditions and Orphan Drugs). Primary care prescribing of 7% and inflationary uplifts for service contracts, SLA s and PFI s. Future years assumptions for uplifts and inflation for pay uplifts are based on current information as supplied by SG colleagues Approach The approach to savings has broadly been split into four areas: Everyday quality improvement savings in operational units 8.1m Corporate and support services savings 2.2m Central savings 5.8m Efficiencies arising from quality improvements 12.7m Everyday quality improvement savings in operational units - housekeeping savings refer to day-to-day efficiencies in operational units broadly within the framework of existing structures and service configurations. For example, by better use of contracting the supplies needed to deliver services in their current configuration can be obtained at a lower cost. Such savings have formed the backbone of the Board s savings programme for many years and there is a solid record of delivering around 10m each year from these sources. For 2016/17 the savings available from these areas will be lower due to the fact that some of the efficiency activity will be required for cost reduction rather than formal savings. Corporate Services - Corporate services have a record of delivering at least 1m of recurring savings every year. A target of 1m has again been set for 2016/17. This is becoming more challenging each year. It is anticipated that part of the savings can be made via housekeeping savings similar to those to be achieved in the operational units, but also that there may be transformational savings required too given the cumulative impact of having to make recurring savings each year. Central savings non-recurrent significant central savings have been achieved every year mainly due to the impact of unspent allocations, holding back planned funding of developments and cost pressures until costs are incurred but also as a result of technical changes in accounting policies
76 Efficiencies arising from quality improvements the Board is supportive of the Highland Quality Approach and the quality improvements that flow from this. For 2016/17, a Quality and Finance Plan is being developed for Board consideration. This follows on from the Strategic Objectives for 2016/17. It is anticipated that there will be financial efficiencies resulting as a by-product of these quality improvements. These can be categorised into the following main headings; Drugs 1.5m This will focus on generic prescribing, waste and repeat prescribing and more cost effective prescribing across both acute and secondary care. Work is well under ways in most of these areas with a number of plans already identified. Workforce - locums 2m other 1m This will focus on further controls around locum expenditure, the Managed Service model with medacs and further internal controls hope to bring the cost at least back to 2014/15 levels. Note that some of the locum reduction will be required as a cost reduction rather than a genuine saving this has been excluded from the 2m. Included is a focus on reductions in supplementary staffing costs with the emphasis on reducing locum spend, tighter vacancy control and service redesign. NHS Highland has a turnover in the region of 10% so there are significant opportunities for redesign. Length of Stay 4.9m The Board is pursuing its Highland Quality Approach. Its Strategic Objectives for 2016/17 will focus on ensuring patients are treated in the most appropriate setting and only admitted to hospital or referred to hospital when absolutely necessary. It is anticipated that this will have a beneficial impact on length of stay. In tandem with a redesign of outpatient services it is also anticipated that referrals into secondary care will reduce. Redesign of Outpatients 1.5m As above the redesign of outpatients using the Highland Quality Approach is to help fast track appointments, prevent inappropriate referrals, avoid unnecessary repeat attendances and the use of technology to reduce hospital outpatient attendance. National Initiatives 1.8m As discussed at the March Directors of Finance meeting, there are a number of national initiatives being taken forward following agreement by Chief Executives. The Board has assessed these and a very tentative estimate of a 4.0m benefit has been included. Note that this does not include 1.6m relating to AME funding in respect of pre-2010 provisions as this has been included in the Central category. The remaining 4m is not yet sufficiently progressed to be classified as identified but it is anticipated there is some potential across a range of headings. 7. Risks Broadly there are two risks areas facing the Board in 2016/17: Ability to manage underlying cost pressures Ability to deliver a very challenging savings target Underlying Cost Pressures As Highlighted previously both Raigmore and North & West Operational Units have overspent their budgets in 2015/16 due to a range of issues.
77 In N&W, this is primarily due the recruitment and service model issues around Caithness General Hospital resulting in exorbitant locum costs to maintain the level of service, A new model is being developed which should begin to impact during the course of 2016/17 which, alongside work in reducing locum costs more generally, should see a stepped reduction in costs during the year. To facilitate this, additional funding of 1.2m has been provided within the plan to help bridge this transition with the unit seeking to actively reduce costs as the model is implemented. In terms of Raigmore, the pressures there are numerous and complicated and reflect the position across the country in terms of acute hospital pressures. The hospital has had a period of sustained pressure on bed and has been running on red alert on a regular basis which cannot be sustained. This has resulted in an unsatisfactory quality of care due to the cancellations of admissions, inappropriate delayed discharges, etc. From 1 April, Raigmore will formally merge with the South & Mid Highland Operational Unit to form the Inner Moray Firth Operational Unit (IMFOU) under a single Director of Operations which will result in a Unit responsible for the full pathway of care from primary care, through acute care to community/social care and will provide the unit with the tools to directly make decisions across the entire pathway to reduce emergency admission, reduce length of stay, facilitate earlier discharge and to maintain people within their own homes. Again, additional resource of 2.5m has been invested within the unit to partially bridge this gap while initiatives begin to make an impact. Savings Target In terms of the savings target, 28.8m far exceeds any level of savings target in previous years and will be extremely challenging to deliver. In terms of housekeeping, corporate savings and central benefits, NHSH has a track history in delivering in those areas and there is a relatively high degree of confidence that the level set is challenging but deliverable. Efficiencies arising from quality improvements the Board is supportive of the Highland Quality Approach and the quality improvements that flow from this. For 2016/17, a Quality and Finance Plan is being developed for Board consideration. This follows on from the Strategic Objectives for 2016/17 and it is anticipated that there will be financial efficiencies resulting as a by-product of these quality improvements. Conclusion The Revenue position for 2016/17 requires a cash releasing target that is unprecedented for NHSH. This will clearly be a major challenge. In this final LDP, savings of 26.5m has been categorised as identified and 2.3m unidentified. There is a significant work programme required to deliver the savings identified and we would classify 3.95m as high risk, 5.55m medium risk and 17m low risk. There is also 2.3m unidentified savings. We will explore the opportunities arising from the national initiatives discussed at the Directors of Finance meeting. FINANCE TABLES attached in Appendix 1
78 This page is intentionally blank
79 NHS Highland Part 4 Community Planning Partnership
80 Highland Community Planning Partnership NHS Highland will continue to play an active role in the Highland Community Planning Partnership. We will contribute to the CPP Board and Chief Officer Group which brings together the most senior officers across the partnership to plan delivery of the priorities agreed within the Single Outcome Agreement and scrutinizes the work of the eight CPP theme groups that have been developed to deliver on these priorities. The priority themes are: Older people Health inequalities and physical activity The Environment Children and young people Economic development Safer Highland Employment Community Learning and Development We will provide leadership to the Older People s and Health Inequalities and Physical Activity theme groups and contribute to all other theme groups and their various sub/improvement groups. This will include developing and implementing specific delivery plans, contributing to implementation, providing progress reports and information for performance monitoring. During 2016/17 we will specifically: Lead the process for developing a new Active Highland strategy for Highland that will set out the partnership priorities for getting our population more active Support the partnership work to tackle substance misuse through the Highland Alcohol and Drug Partnership Lead on the partnership work to reduce gender based violence through implementation of the Highland Violence Against Women delivery plan Support partners to develop a programme of work to reduce poverty, including: o implementation of a tool that helps partners to target activity and resource at our most deprived and fragile communities o Research to explore the views of individuals and groups in fragile areas on what fragility means and what it is like to live in their community Lead on the CPP breakthrough achievement for 2016/17 which will focus on reducing social isolation and loneliness Support development of the Local Outcomes Improvement Plans as part of the implementation of the Community Empowerment Act Contribute to the work to develop a joint approach to asset transfers and participation requests as part of the implementation of the Community Empowerment Act Work with all partners to deliver the Strategic Plan as required by the Public Bodies(Joint Working)(Scotland)Act 2014 Build on the development of District Partnerships to ensure Community planning is locally driven and owned
81 Argyll and Bute Community Planning Partnership What are the improvement aims that have been agreed locally? What actions will be taken to move towards that aim? What measures will be used to assess improvements made? Role in shifting activity and spend towards tackling inequalities Role in shifting activity and spend towards prevention Role in shifting activity and spend towards community empowerment Secured agreement that inequalities is threaded throughout SOA Secured agreement that prevention is threaded throughout SOA Influential on directing resources in multi-agency arenas within the Community Planning processes to give Third Sector organisations a more robust financial footing Two outcomes of the SOA are considered in depth at each of the CPP Management Committee meetings. In this discussion, public health in particular is sighted on encouraging the CPP to be self critical as to whether there is sufficient activity on inequalities Two outcomes of the SOA are considered in depth at each of the CPP Management Committee meetings. In this discussion, public health in particular is sighted on encouraging the CPP to be self critical as to whether there is sufficient activity on prevention Work has been diverted from statutory sector and/or away from short term funding of grants or awards to a commissioned basis from the Third Sector and. This is demonstrated through A&B Alcohol & Drug Partnership with the award of the adult community alcohol and drug services Improved mortality and morbidity rates across all localities within Argyll & Bute Improved mortality and morbidity rates across all localities within Argyll & Bute This builds capacity in communities and an essential part of the measurement of that is growth of community assets overall as confidence grows. No target has been set but assets have been mapped and we can monitor how this progresses over time
82 This page is intentionally blank
83 NHS Highland PART 5 Workforce
84 5. WORKFORCE 5.1 EVERYONE MATTERS: 2020 WORKFORCE VISION IMPLEMENTATION PLAN 2016/17 NHS Highland has had in place its Everyone Matters: 2020 Workforce Vision Implementation Plan since 2014, which is overseen by the Highland Partnership Forum and the Staff Governance Committee. In line with the National Implementation Plan for 2016/17 NHS Highland will continue to implement actions from the existing plan and update the action plan to incorporate new actions as appropriate. In addition work to implement the Staff Governance Standard continues. The key focus for each work stream for 2016/17 is as follows: Healthy Organisational Culture creating a healthy organisational culture in which our NHS Highland values are embedded in everything we do, enabling a healthy, engaged and empowered workforce. The continued focus this year is on ensuring behaviours consistently live up to expectations. People Strategy is a key element of the Highland Quality Approach (HQA). Values and Behaviours have been agreed by the Board, as part of the HQA and the Board has endorsed the approach to Living our Values. A Catchball exercise has been undertaken between January and March 2016 to develop and agree the organisation s Annual Objectives for 2016/17. This has engaged staff with the aim of their understanding of the clear connection between the vision for NHS Highland and where teams and individuals focus their effort, under the three key areas of focus: People, Quality and Care. Three People objectives have been developed: o To improve our staff experience working for NHS Highland by: Making NHS Highland the employer of choice; Ensuring staff are proud of their contribution to delivering safe and effective care; Increasing the number of staff who feel engaged and valued as part of our team; Staff teams have been reflecting on the objectives as they have been developed and have been engaged in feedback about what the objectives mean for themselves and their team and how individuals and their teams will contribute to the objectives in 2016/17 and the delivery of better health, better care and better value. imatter is being rolled out and includes clinical settings and the Board leadership team. The principles of Daily Management, in line with our Lean Improvement Methodology are being rolled out and include staff Daily Huddles, investment in supervisor support to the front line; and ensuring staff are valued, supported and thanked for their contribution. The Highland Quality Awards are embedded and are awarded and celebrated on a monthly basis. Work on values based recruitment continues to be progressed. The development of a Physician s Compact has progressed and to date 9 Group sessions have taken place with 50+ staff and 4 more Group Sessions were planned. Clinicians and Managers had also been engaged and themes emerging had been
85 captured in Wordles that illustrate the current state and future state mutual expectations and behaviours expected between employee and employer. Sustainable Workforce ensuring that the right people are available to deliver the right care, in the right place, at the right time. Strengthening workforce planning continues to be the focus this year. An integrated approach to workforce planning with service, financial, ehealth and Asset Planning, through the development of an implementation plan for the Board s Clinical Strategy and its 10 Year Plan, is being progressed. Workforce Plans either exist or are being scoped to support major service redesign projects: o Reconfiguring out of hours services o Improving the flow from hospital to home o Badenoch and Strathspey Redesign o Skye Lochalsh and SW Ross Redesign o Argyll and Bute health and social care integration o Re-provisioning of community facilities o Reconfiguration of critical care in Raigmore (DGH), Inverness The focus is on developing fully integrated services to cover care both in and out of hours though skilled multi-professional teams. The quality of workforce data and contextual information will continue to be improved to inform the Board and Operational Unit Workforce Plans. Capable Workforce ensuring that everyone has the skills needed to deliver safe, effective, person-centred care. The focus this year at National level is on developing a more consistent, Scotland-wide approach to learning and development. The Board Learning and Development Plan and individual Development Programmes will reflect the Vision and the Values of NHS Highland. Work will continue to ensure that all staff have a meaningful conversation about their performance, development and career aspirations as part of KSF and other appraisal systems. Leadership Programmes and learning and development opportunities will continue to support the development of skills and behaviours for working collaboratively and flexibly across primary and secondary care and integrating health and social care. Workforce to Deliver Integrated Services developing an integrated health and social care workforce across NHS Boards, local authorities and third party providers. The focus this year is on working with colleagues and partner organisations to implement integrated health and social care workforce arrangements. The Board will continue to partner with The Highland Council and the Argyll and Bute Council to develop a shared culture, values and ways of working through effective teams and local partnership arrangements. Leadership Programmes e.g. Leading for Integration and Leading with Purpose will continue to be delivered to continue to support integration of health and social care. In
86 A&B Leading for the Future will be run as an integrated cohort to support integration of primary and secondary care including GPs, Dentists and Pharmacists. Effective Leadership and Management leaders and managers will lead by example and empower teams and individuals to deliver NHS Scotland s 2020 Vision and the Board s Clinical Strategy and its 10 Year Plan. This year the focus is on ensuring effective leadership for change. Leadership Programmes for Quality Improvement in SPSP, Lean and Staff Experience will continue to support change and continual improvement. Leadership Programmes for clinical and managerial staff will continue e.g. Leading for the Future, Leading for Purpose, Leading for Integration and ILM Programmes will help support the workforce through change. 5.2 WORKFORCE RISKS TO LDP DELIVERY Human Resources / Workforce High Level Risks have been articulated with plans articulate to mitigate against these, within the overall NHS Highland Risk Register. Workforce Risks are agreed in partnership with staff side and management and clinical representatives and are monitored on a quarterly basis by the Staff Governance Committee. The risks that are relevant to LDP delivery are as follows: Rural General Hospitals: The vulnerability and sustainability of Rural General Hospitals continues to be a key issue for the Board evidenced by significant recruitment and succession planning challenges in medical staffing, including high locum use and increasing expenditure (national trend). The Board is progressing Rural General Hospital medical workforce planning, working in partnership with Boards and NHS Education for Scotland (NES) and a number of redesign options have been developed, implemented and are being tested. GP Vacancies: The Board continues to have GP vacancies with associated impact on remote and rural primary care service delivery, including support to community hospitals. There is a continued focus on a number of initiatives to make rural practice more attractive and there has been successful recruitment outcomes from the development of a bespoke marketing campaign, Why Rural which has its own recruitment website and the Scottish National rural-track Programme for GPST training to address supply issues. The Board is also engaging on a regular basis with local communities in agreeing solutions to current workforce challenges through the Scottish Government funded Being Here programme. Cancer Services: Performance against national cancer waiting times remains of concern both at Board level and at national level. These results have been for a large part due to national staffing shortages in cancer specialties, particularly within Oncology itself but also within Urology. Radiotherapy planning recruitment has improved with the appointment of one member of staff and a second post is actively being recruited to. This will allow a return to full establishment for the first time in ten years. The Board is engaged in a number of approaches to increase capacity; working closely with colleagues in the Regional Oncology Collaborative Board and the other Cancer Centres with the aim of creating and sustaining a robust, sustainable service; and engaged in
87 diagnostic and small professional workforce planning groups on a regional and national basis, to address workforce supply issues. Sustainable Workforce: Working with partners is key to sustainable workforce. We collaborate with NHS Boards, Regions and our independent and third sector organisations to develop workforce solutions and identify workforce risks arising from new and ongoing national staff shortages / recruitment challenges in the Board or succession planning around small specialties and an ageing workforce. We have recruitment challenges in Care at Home Services and AHPs: radiography Band 5, estates/skilled trades and advanced nurse practitioner retention. 5.3 WORKFORCE DEVELOPMENT Physician Associate (PA): PA s are being considered as part of the future workforce solution to support a number of areas across NHS Highland. Internships have been developed to support the increase in clinical activity and 7 day working in Raigmore Hospital. However internships advertised for Raigmore last year has were unsuccessful in attracting applicants. A proposal is being developed to grow our own PA s and improve recruitment. Nationally there is currently a mismatch between supply and demand and an urgent need to take a Scotland wide view of the future of the profession in terms of provision of training programmes, the development of a career framework and associated funding for both. A national PA Forum is now established to support the profession & develop a cohesive strategy including the development of a career framework & active support for regulation. Care Support Workers and Care Apprentice Roles: There has been a need identified for a cohort of support staff who can deliver holistic care based on the needs of the individual service user. The rationale for this conclusion is that person-centred care demands person-centred roles which do not belong to either health or social care and so break down artificial barriers between professions. Moving the focus to outcomes for the service user helps to define the skills needed to support the achievement of those outcomes and this approach is supported by users and carers and has been incorporated into Personal Outcome Plans. Some additional work is required to support updated education frameworks that will support such roles to be developed. The extent to which Care Support Workers and Care Apprentice Roles need to be registered or regulated, and the impact on regulation of the services they work in, needs to be clarified through discussion with SSSC, NMC, HCPC and the Care Inspectorate. NES is engaged in discussions with the regulatory bodies, on behalf of the Boards so that roles can be developed. Workforce Affordability: Workforce accounts for approximately 60% of Board expenditure and it is vital that the workforce is deployed and developed appropriately to work as efficient and productively as possible. Planning workforce requirements and aligning the workforce to quality improvement and service redesign outcomes will achieve workforce efficiencies. The Highland Quality Approach is driving service change and with that comes workforce changes in terms of changes to skill mix and ensuring that staff are working at the correct roles, as well as freeing up consultant time so that care can be led, planned and delivered in the most efficient way, by the most appropriate professional.
88 Specifically, the Board has a continued focus on workforce expenditure and has plans for 2015/16 to reduce Locum spend by 6m and reduce the workforce cost base by 5m. The Board already has approaches in place and these will be further applied in 2015/16 to generate workforce affordability and efficiency. Reducing Expenditure on Flexible Workforce (effective use of flexible workforce bank, agency, locums, overtime and extra hours reduction); Reducing workforce cost base (excess basic hours, waiting time premia, extra programme activities (medical), on-call and unsocial hours, working hours, travel (use IT instead) and subsistence reduction); and Improving Productivity and Efficiency (skill mix review and applying validated workload and workforce planning tools; maximise the use of our talented workforce ensuring that individuals contribute to the top of their training and capability; ensuring our staff are as healthy and productive as possible reducing sickness absence, developing staff wellness initiatives, effective use of PIN Policies, Job Planning for medical staff and AHPs; monitoring study leave, effective use of travel time; and implementing technological solutions and service improvement. N&M Workload and Workforce Planning Tools: Review of community nursing services will be undertaken in with intention to ensure appropriately skilled workforce for the future central to the review will be planning for the future with focus on new roles to include assistant practitioner and advanced practice roles. This work will also take cognisance of the interface with general practice nursing and the implications of forthcoming changes in out of hours services and primary care. Application of the workforce planning tools is well embedded within practice across hospital and community settings. Further work has been commenced to ensure that the agreed NHS Highland principles for workforce planning are complied with on an ongoing basis and to formalise the ongoing reporting and monitoring of establishments across all settings. Changes to workforce in maternity services, health visiting, acute in patient services and mental health services have been agreed in as result of workforce reviews utilising the agreed tools. Areas for further review in include school nursing, learning disability and community nursing. The Board is engaged in the National Review of Maternity and Neonatal Services, which has a specific work stream on workforce planning and development. 5.4 INTEGRATION OF HEALTH AND SOCIAL CARE Integration arrangements in North Highland NHS Highland and Highland Council have operated a Lead Agency arrangement since 1 April In North Highland NHS Highland is the Lead Agency for services to adults, and 1470 Highland Council staff TUPE transferred to NHS Highland on that date. The Partnership Agreement with Highland Council covers the period to 31 March 2017, and the development of integrated teams and service delivery is well embedded and significant progress has already been made on workforce issues since April 2012.
89 Integration arrangements in Argyll and Bute: NHS Highland and Argyll and Bute council have agreed to establish the body corporate model of integration in what will be known and the Argyll and Bute Health and Social care partnership. The Integrated Joint Board will be accountable and responsible for the operational delivery of all adults and children s services and it will also hold the budget for all acute services commissioned from NHS Greater Glasgow and Clyde. Argyll and Bute HSCP Strategic plan details the transformation of health and social care services delivered at locality level to achieve our vision People in Argyll and Bute will live longer, healthier, independent lives. The operational services which have been delegated to it means that its Integrated Joint Board is responsible and accountable for scheduled care planning and delivery at both strategic and locality level to ensure the transformation activity aligns with the HSCP target and objectives and notably focusing on: Reduce avoidable emergency admissions to hospital and minimize the time people are delayed Support people to live fulfilling lives in their own homes for as long as possible Support unpaid carers to reduce the impact of their caring role on their own health and wellbeing Implement a continuous improvement approach Support staff to continuously improve the information, support and care they deliver Efficiently and effectively manage all resources to deliver Best Value The development of Locality Planning Groups (8 in total), are seen as the key engine of transformational change. Their involvement in the direction as a focus of workforce planning alongside service need is key in achieving the shift in the balance of care and transfer of resource/development of community and care services. The HSCP stated aim is to have in place by the end of 2016/17 a detailed and robust workforce implementation plan at locality level, and to then proceed to implement it. Ensuring we have the most capable, supported and empowered workforce to achieve our vision, which when aggregated up. 5.5 CONCLUSION Whilst a number of key workforce risks and recruitment challenges remain, considerable work is being taken forward to reduce risks, through collaboration with partners, the development of new service models and roles, innovative solutions being tested in Rural General Hospitals to support sustainability and a number of plans to support health and social care integration, quality improvement, improve workforce engagement and workforce efficiency and productivity
90 This page is intentionally blank
91 NHS Highland Appendix 1 Finance Tables

92

93

94

95
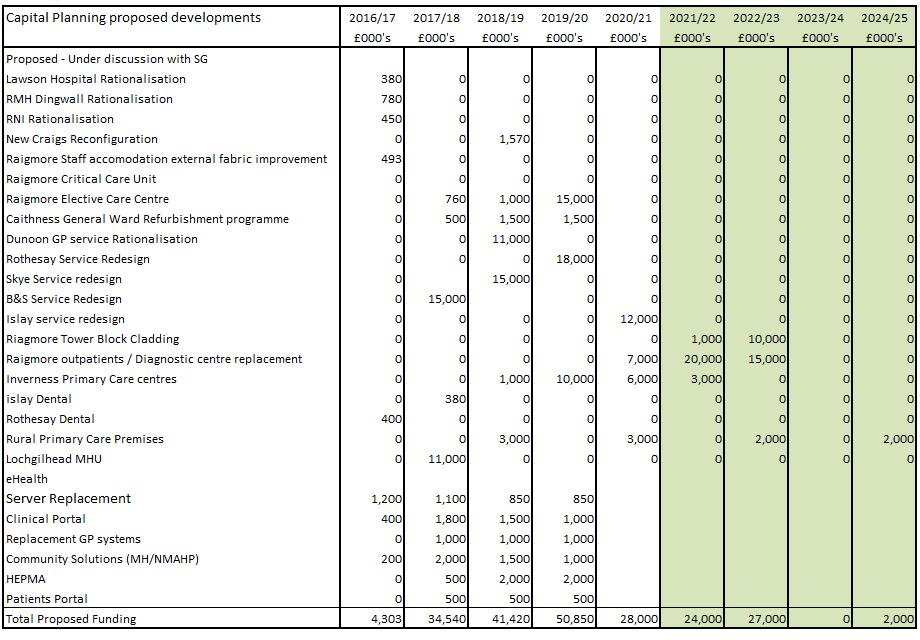
96
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
NURSING & MIDWIFERY WORKLOAD & WORKFORCE PLANNING PROJECT RECOMMENDATIONS AND ACTION PLAN NOVEMBER 2006 UPDATE
 Forma cm NHS HIGHLAND WORKLOAD AND WORKFORCE PLANNING PROJECT RECOMMENDATIONS AND ACTION PLAN NURSING & MIDWIFERY WORKLOAD & WORKFORCE PLANNING PROJECT RECOMMENDATIONS AND ACTION PLAN NHS HIGHLAND NOVEMBER
Forma cm NHS HIGHLAND WORKLOAD AND WORKFORCE PLANNING PROJECT RECOMMENDATIONS AND ACTION PLAN NURSING & MIDWIFERY WORKLOAD & WORKFORCE PLANNING PROJECT RECOMMENDATIONS AND ACTION PLAN NHS HIGHLAND NOVEMBER
Catherine Hughson Kathryn Kearney Number of supervisors relinquishing role since last report:
 Name of Local Supervising Authority: Western Isles Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising Authority
Name of Local Supervising Authority: Western Isles Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising Authority
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
EMPLOYEE HEALTH AND WELLBEING STRATEGY
 EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
NW Health & Physical Activity Forum. Martin Ashton Service Manager: Commissioning for Health Improvement NHSALW / Wigan Council
 NW Health & Physical Activity Forum Martin Ashton Service Manager: Commissioning for Health Improvement NHSALW / Wigan Council Team Purpose Strategically lead CYP Health Improvement & early intervention
NW Health & Physical Activity Forum Martin Ashton Service Manager: Commissioning for Health Improvement NHSALW / Wigan Council Team Purpose Strategically lead CYP Health Improvement & early intervention
Inequalities Sensitive Practice Initiative
 Inequalities Sensitive Practice Initiative Maternity Unit Report - 2008 Royal Alexandria Hospital 1 Acknowledgment I would like to take this opportunity to thank the staff from the maternity services in
Inequalities Sensitive Practice Initiative Maternity Unit Report - 2008 Royal Alexandria Hospital 1 Acknowledgment I would like to take this opportunity to thank the staff from the maternity services in
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
NHS GRAMPIAN. Local Delivery Plan - Mental Health and Learning Disability Services
 NHS GRAMPIAN Board Meeting 01.06.17 Open Session Item 8 Local Delivery Plan - Mental Health and Learning Disability Services 1. Actions Recommended The Board is asked to: Note the context regarding the
NHS GRAMPIAN Board Meeting 01.06.17 Open Session Item 8 Local Delivery Plan - Mental Health and Learning Disability Services 1. Actions Recommended The Board is asked to: Note the context regarding the
NHS Highland Infection Prevention & Control Annual Work Plan End of Year
 NHS Highland Board 5 April Item 5.7 NHS Highland & Control Annual Work Plan End of Year Update for COIC Prepared by Catherine Stokoe and Jonty Mills (as of 01/03/) Objective Activity Time Scale Lead Officer
NHS Highland Board 5 April Item 5.7 NHS Highland & Control Annual Work Plan End of Year Update for COIC Prepared by Catherine Stokoe and Jonty Mills (as of 01/03/) Objective Activity Time Scale Lead Officer
NHS Lothian Health Promotion Service Strategic Framework
 NHS Lothian Health Promotion Service Strategic Framework 2015 2018 Working together to promote health and reduce inequalities so people in Lothian can reach their full health potential 1 The Health Promotion
NHS Lothian Health Promotion Service Strategic Framework 2015 2018 Working together to promote health and reduce inequalities so people in Lothian can reach their full health potential 1 The Health Promotion
Alcohol Brief Interventions 2015/16
 Publication Report Alcohol Brief Interventions 2015/16 Publication date 14 June 2016 An Official Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main points... 3 Results and
Publication Report Alcohol Brief Interventions 2015/16 Publication date 14 June 2016 An Official Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main points... 3 Results and
Safeguarding Children Annual Report April March 2016
 Safeguarding Children Annual Report April 2015 - March 2016 Report Author: Andrea Anniwell, Interim Named Nurse for Safeguarding Children Date: April 2016 1 CONTENTS SECTION PAGE 1 Introduction 3 2 Overview
Safeguarding Children Annual Report April 2015 - March 2016 Report Author: Andrea Anniwell, Interim Named Nurse for Safeguarding Children Date: April 2016 1 CONTENTS SECTION PAGE 1 Introduction 3 2 Overview
Intensive Psychiatric Care Units
 NHS Highland Argyll & Bute Hospital, Lochgilphead Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity.
NHS Highland Argyll & Bute Hospital, Lochgilphead Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity.
Local Delivery Plan Guidance 2016/17
 The Scottish Government Directorate for Health Performance & Delivery Dear Colleague Local Delivery Plan Guidance 2016/17 Summary The LDP Guidance 2016-17 sets out the performance contract between the
The Scottish Government Directorate for Health Performance & Delivery Dear Colleague Local Delivery Plan Guidance 2016/17 Summary The LDP Guidance 2016-17 sets out the performance contract between the
Alcohol Brief Interventions 2016/17
 Publication Report Alcohol Brief Interventions 2016/17 Publication date 27 June 2017 A National Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main points... 3 Results and
Publication Report Alcohol Brief Interventions 2016/17 Publication date 27 June 2017 A National Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main points... 3 Results and
Child Health 2020 A Strategic Framework for Children and Young People s Health
 Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
NES NES/17/25 Item 8a (Enclosure) March 2017 NHS Education for Scotland Board Paper Summary 1. Title of Paper 2. Author(s) of Paper
 March 2017 NHS Education for Scotland Board Paper Summary 1. Title of Paper 2. Author(s) of Paper") NES Item 8a March 2017 NES/17/25 (Enclosure) NHS Education for Scotland Board Paper Summary 1. Title of Paper NHS Education for Scotland Local Delivery Plan (LDP) 2017-18. 2. Author(s) of Paper Donald
NES Item 8a March 2017 NES/17/25 (Enclosure) NHS Education for Scotland Board Paper Summary 1. Title of Paper NHS Education for Scotland Local Delivery Plan (LDP) 2017-18. 2. Author(s) of Paper Donald
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Karen King (Link) Kathleen Hamblin Carole McBurnie Frances Wright Joyce Linton Catriona Thomson
 Kathleen Hamblin Carole McBurnie Frances Wright Joyce Linton Catriona Thomson") Name of Local Supervising Authority: Dumfries and Galloway Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising
Name of Local Supervising Authority: Dumfries and Galloway Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising
Job Description. CNS Clinical Lead
 Job Description CNS Clinical Lead POST: BASE: ACCOUNTABLE TO: REPORTS TO: RESPONSIBLE FOR: CNS Clinical Lead St John s Hospice Head of Nursing and Quality Head of Nursing and Quality Community Clinical
Job Description CNS Clinical Lead POST: BASE: ACCOUNTABLE TO: REPORTS TO: RESPONSIBLE FOR: CNS Clinical Lead St John s Hospice Head of Nursing and Quality Head of Nursing and Quality Community Clinical
Healthy lives, healthy people: consultation on the funding and commissioning routes for public health
 Healthy lives, healthy people: consultation on the funding and commissioning routes for public health December 2010 The coalition Government published Healthy Lives, Health people: consultation on the
Healthy lives, healthy people: consultation on the funding and commissioning routes for public health December 2010 The coalition Government published Healthy Lives, Health people: consultation on the
Wolverhampton s 0-19 Healthy Child Programme
 Wolverhampton s 0-19 Healthy Child Programme Consultation document for a proposed new service model Public Health and Well-being August 2016 Wolverhampton s Healthy Child Programme Consultation Document
Wolverhampton s 0-19 Healthy Child Programme Consultation document for a proposed new service model Public Health and Well-being August 2016 Wolverhampton s Healthy Child Programme Consultation Document
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
Report by Liz McClurg, Infection Control Manager on behalf of Heidi May, Board Nurse Director & Executive Lead, Infection Prevention & Control
 INFECTION PREVENTION & CONTROL ANNUAL WORK PLAN (2013 2014) Highland NHS Board 4 June 2013 Item 5.5(c) Report by Liz McClurg, Infection Control Manager on behalf of Heidi May, Board Nurse Director & Executive
INFECTION PREVENTION & CONTROL ANNUAL WORK PLAN (2013 2014) Highland NHS Board 4 June 2013 Item 5.5(c) Report by Liz McClurg, Infection Control Manager on behalf of Heidi May, Board Nurse Director & Executive
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS LOTHIAN LOCAL DELIVERY PLAN Unique ID: NHS Lothian Local Delivery Plan 2016 /17 Category/Level/Type:
 NHS LOTHIAN LOCAL DELIVERY PLAN 2016-2017 Unique ID: NHS Lothian Local Delivery Plan 2016 /17 Category/Level/Type: Local Delivery Plan 2016-17 Author (s) Alex McMahon, Alyson Cumming Authorised By: Corporate
NHS LOTHIAN LOCAL DELIVERY PLAN 2016-2017 Unique ID: NHS Lothian Local Delivery Plan 2016 /17 Category/Level/Type: Local Delivery Plan 2016-17 Author (s) Alex McMahon, Alyson Cumming Authorised By: Corporate
2. This year the LDP has three elements, which are underpinned by finance and workforce planning.
 Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
grampian clinical strategy
 healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
NHS Equality Delivery System for Isle of Wight NHS Trust. Interim baseline assessment against the
 Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Mental health and crisis care. Background
 briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
briefing February 2014 Issue 270 Mental health and crisis care Key points The Concordat is a joint statement, written and agreed by its signatories, that describes what people experiencing a mental health
Victorian Labor election platform 2014
 Victorian Labor election platform 2014 July 2014 1. Background The Victorian Labor Party election platform provides positions on key elements of State Government policy. The platform offers a broad insight
Victorian Labor election platform 2014 July 2014 1. Background The Victorian Labor Party election platform provides positions on key elements of State Government policy. The platform offers a broad insight
This is a high level overview report to update the Board on the Acute Adult Safety Programme consisting of the following sections:
 Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Equality and Health Inequalities Strategy
 Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
Finance Committee. Draft Budget Submission from North Ayrshire Community Planning Partnership
 Finance Committee Draft Budget 2012-13 Submission from North Ayrshire Community Planning Partnership 1. To what extent has preventative spending been embedded within the CPP s work so that it focuses on
Finance Committee Draft Budget 2012-13 Submission from North Ayrshire Community Planning Partnership 1. To what extent has preventative spending been embedded within the CPP s work so that it focuses on
Balanced year end position. Monthly Indicators Red Amber Green No Total Status May (No. of indicators)
") From: Martin Wade Tel.: 1223 699733 Date: 11 July 218 Public Health Directorate Finance and Performance Report June 218 1 SUMMARY 1.1 Finance Previous Status Green Category Income and Expenditure Balanced
From: Martin Wade Tel.: 1223 699733 Date: 11 July 218 Public Health Directorate Finance and Performance Report June 218 1 SUMMARY 1.1 Finance Previous Status Green Category Income and Expenditure Balanced
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
This paper provides an update on the the recent national SPSP conference the programme of work for Tissue Viability Acute Adult Care SPSP
 Greater Glasgow and Clyde NHS Board Board Meeting December 2016 Board Paper No. 16/81 Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP) is one of the family
Greater Glasgow and Clyde NHS Board Board Meeting December 2016 Board Paper No. 16/81 Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP) is one of the family
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Guidelines for Maternity Services Getting it Right for Every Mother and Child
 Guidelines for Maternity Services Getting it Right for Every Mother and Child Policy Reference: 4102012 Date of issue: October 2012 Prepared by: Sandra Harrington Date of Review: October 2014 Midwifery
Guidelines for Maternity Services Getting it Right for Every Mother and Child Policy Reference: 4102012 Date of issue: October 2012 Prepared by: Sandra Harrington Date of Review: October 2014 Midwifery
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
HEALTH AND CARE (STAFFING) (SCOTLAND) BILL
 (SCOTLAND) BILL") HEALTH AND CARE (STAFFING) (SCOTLAND) BILL POLICY MEMORANDUM INTRODUCTION 1. As required under Rule 9.3.3 of the Parliament s Standing Orders, this Policy Memorandum is published to accompany the Health
HEALTH AND CARE (STAFFING) (SCOTLAND) BILL POLICY MEMORANDUM INTRODUCTION 1. As required under Rule 9.3.3 of the Parliament s Standing Orders, this Policy Memorandum is published to accompany the Health
Child & Adolescent Mental Health Services in NHS Scotland
 Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31st December 2012 26th February 2013 A National Statistics Publication for Scotland Contents Introduction...
Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31st December 2012 26th February 2013 A National Statistics Publication for Scotland Contents Introduction...
corporate management plan
 corporate management plan 2012-2013 2 Contents 1. Introduction 2. Overview of the Trust 3. Our purpose, values and core objectives 4. Safety & Quality Corporate Objectives 5. Modernisation Corporate Objectives
corporate management plan 2012-2013 2 Contents 1. Introduction 2. Overview of the Trust 3. Our purpose, values and core objectives 4. Safety & Quality Corporate Objectives 5. Modernisation Corporate Objectives
NHS Greater Glasgow and Clyde. Workforce Plan 2015/16
 NHS Greater Glasgow and Clyde Workforce Plan 2015/16 Contents 1 Section One... 5 1.1 Introduction to the Workforce Plan... 6 1.2 An overview of NHS Greater Glasgow and Clyde... 8 1.3 Staff Governance...
NHS Greater Glasgow and Clyde Workforce Plan 2015/16 Contents 1 Section One... 5 1.1 Introduction to the Workforce Plan... 6 1.2 An overview of NHS Greater Glasgow and Clyde... 8 1.3 Staff Governance...
Community Health Partnerships (CHPs) Scheme of Establishment for Glasgow City Community Health and Social Care Partnerships
 Scheme of Establishment for Glasgow City Community Health and Social Care Partnerships") EMBARGOED UNTIL MEETING Greater Glasgow NHS Board Board Meeting Tuesday 19 th April 2005 Board Paper No. 2005/33 Director of Planning and Community Care Community Health Partnerships (CHPs) Scheme of Establishment
EMBARGOED UNTIL MEETING Greater Glasgow NHS Board Board Meeting Tuesday 19 th April 2005 Board Paper No. 2005/33 Director of Planning and Community Care Community Health Partnerships (CHPs) Scheme of Establishment
Appendix 1: Public Health Business Plan: Priority One - Effective public health commissioning
 Appendix 1: Public Health Business Plan: Priority One - Effective public health commissioning Activity 1. Develop Public Health strategic commissioning plan in line with the Public health Outcomes Framework
Appendix 1: Public Health Business Plan: Priority One - Effective public health commissioning Activity 1. Develop Public Health strategic commissioning plan in line with the Public health Outcomes Framework
Staff Health, Safety and Wellbeing Strategy
 Staff Health, Safety and Wellbeing Strategy 2013-16 Prepared by: Effective From: Review Date: Lead Reviewer: Hugh Currie Head of Occupational Health and Safety 31 st January 2013 01 st April 2014 Patricia
Staff Health, Safety and Wellbeing Strategy 2013-16 Prepared by: Effective From: Review Date: Lead Reviewer: Hugh Currie Head of Occupational Health and Safety 31 st January 2013 01 st April 2014 Patricia
Child & Adolescent Mental Health Services in NHS Scotland
 Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 30 th September 2013 26 th November 2013 A National Statistics Publication for Scotland Contents
Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 30 th September 2013 26 th November 2013 A National Statistics Publication for Scotland Contents
SAFE CARE. Scottish Patient Safety Programme. SPSP Adult Acute
 SAFE CARE NHS Greater Glasgow and Clyde (NHS GGC) is committed to providing safe high quality care that our staff and patients can be proud of. Over recent years the Scottish Patient Safety Programme has
SAFE CARE NHS Greater Glasgow and Clyde (NHS GGC) is committed to providing safe high quality care that our staff and patients can be proud of. Over recent years the Scottish Patient Safety Programme has
BIRMINGHAM CITY COUNCIL
 BIRMINGHAM CITY COUNCIL PUBLIC REPORT Report to: CABINET Report of: Strategic Director for People Date of Decision: 28 th June 2016 SUBJECT: STRATEGY AND PROCUREMENT PROCESS FOR THE PROVISION OF EARLY
BIRMINGHAM CITY COUNCIL PUBLIC REPORT Report to: CABINET Report of: Strategic Director for People Date of Decision: 28 th June 2016 SUBJECT: STRATEGY AND PROCUREMENT PROCESS FOR THE PROVISION OF EARLY
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme
 The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme The Improvement Academy (IA) is one of the leading quality and safety improvement networks in the UK. The IA works across
The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme The Improvement Academy (IA) is one of the leading quality and safety improvement networks in the UK. The IA works across
Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years
 Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years Introduction 1. Islington CCG funds a range of health services for children
Islington CCG Commissioning Statement in relation to the commissioning of health services for children and young people 0-18 years Introduction 1. Islington CCG funds a range of health services for children
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
Annual Report
 Equality and Diversity Steering Group Annual Report 2012-2013 April 2013 1 Contents Page No Introduction 3 Equality Act 2010 3 NHS Lanarkshire s Equality and Diversity Reporting Structure Equality and
Equality and Diversity Steering Group Annual Report 2012-2013 April 2013 1 Contents Page No Introduction 3 Equality Act 2010 3 NHS Lanarkshire s Equality and Diversity Reporting Structure Equality and
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting. Meeting Date: 25 October Executive Lead: Rajesh Nadkarni
 Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
NHS Ayrshire and Arran. 1. Which of the following performance frameworks has the most influence on your budget decisions:
 A: Budget setting process Performance budgeting 1. Which of the following performance frameworks has the most influence on your budget decisions: National Performance Framework Quality Measurement Framework
A: Budget setting process Performance budgeting 1. Which of the following performance frameworks has the most influence on your budget decisions: National Performance Framework Quality Measurement Framework
NHS Grampian. Intensive Psychiatric Care Units
 NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHSScotland Child & Adolescent Mental Health Services
 Publication Report NHSScotland Child & Adolescent Mental Health Services Workforce Information as at 31st December 2011 27th March 2012 A National Statistics Publication for Scotland Contents About ISD...
Publication Report NHSScotland Child & Adolescent Mental Health Services Workforce Information as at 31st December 2011 27th March 2012 A National Statistics Publication for Scotland Contents About ISD...
Child & Adolescent Mental Health Services in NHS Scotland
 Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31 st December 2014 24 th February 2015 A National Statistics Publication for Scotland Contents
Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31 st December 2014 24 th February 2015 A National Statistics Publication for Scotland Contents
Driving and Supporting Improvement in Primary Care
 Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
grampian clinical strategy
 healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
Vale of York Clinical Commissioning Group Governing Body Public Health Services. 2 February Summary
 Vale of York Clinical Commissioning Group Governing Body Public Health Services 2 February 2017 Summary 1. The purpose of this report is to provide the Vale of York Clinical Commissioning Group (CCG) with
Vale of York Clinical Commissioning Group Governing Body Public Health Services 2 February 2017 Summary 1. The purpose of this report is to provide the Vale of York Clinical Commissioning Group (CCG) with
SCOTTISH AMBULANCE SERVICE LOCAL DELIVERY PLAN
 SCOTTISH AMBULANCE SERVICE 2014-15 LOCAL DELIVERY PLAN Scottish Ambulance Service National Headquarters Gyle Square 1 South Gyle Crescent Edinburgh EH12 9EB 14 March 2014 1 List of Contents Section 1:
SCOTTISH AMBULANCE SERVICE 2014-15 LOCAL DELIVERY PLAN Scottish Ambulance Service National Headquarters Gyle Square 1 South Gyle Crescent Edinburgh EH12 9EB 14 March 2014 1 List of Contents Section 1:
Performance Evaluation Report Pembrokeshire County Council Social Services
 Performance Evaluation Report 2013 14 Pembrokeshire County Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Pembrokeshire County Council
Performance Evaluation Report 2013 14 Pembrokeshire County Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Pembrokeshire County Council
Workforce Planning & Redesign
 WORKFORCE PLAN 2017-2020 Author Service Lead and Queries Executive Lead Pauline Rae Gerry Lawrie Dr Annie Ingram Workforce Planning & Redesign 1 P a g e Do you have a visual impairment or have difficulty
WORKFORCE PLAN 2017-2020 Author Service Lead and Queries Executive Lead Pauline Rae Gerry Lawrie Dr Annie Ingram Workforce Planning & Redesign 1 P a g e Do you have a visual impairment or have difficulty
Child & Adolescent Mental Health Services in NHS Scotland
 Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31 st March 2015 26 th May 2015 A National Statistics Publication for Scotland Contents Contents...
Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31 st March 2015 26 th May 2015 A National Statistics Publication for Scotland Contents Contents...
Equality and Diversity
 Equality and Diversity Vision Statement Yasmin Mahmood Senior Associate Equality and Diversity May 2016 page 1/9 Introduction NHS Merton CCG is committed to ensuring equality, diversity and inclusion are
Equality and Diversity Vision Statement Yasmin Mahmood Senior Associate Equality and Diversity May 2016 page 1/9 Introduction NHS Merton CCG is committed to ensuring equality, diversity and inclusion are
Healthy Working Lives and Health Promoting Health Service
 Healthy Working Lives and Health Promoting Health Service Purpose of Report The purpose of this report is to outline proposals and a framework for taking forward work around Healthy Working Lives and Health
Healthy Working Lives and Health Promoting Health Service Purpose of Report The purpose of this report is to outline proposals and a framework for taking forward work around Healthy Working Lives and Health
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP. Corporate Parenting Board. Date of Meeting: 23 rd Feb Agenda item: ( 7 )
") WOLVERHAMPTON CLINICAL COMMISSIONING GROUP Corporate Parenting Board Agenda Item No. 7 Health Services for Looked After Children Annual Report September 2014 -August 2015 Date of Meeting: 23 rd Feb 2016.
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP Corporate Parenting Board Agenda Item No. 7 Health Services for Looked After Children Annual Report September 2014 -August 2015 Date of Meeting: 23 rd Feb 2016.
Improving health and well being for children and families: update on the national health visiting programme - an integrated health approach
 Improving health and well being for children and families: update on the national health visiting programme - an integrated health approach Sue Hatton Workforce Development Specialist for Women and Children
Improving health and well being for children and families: update on the national health visiting programme - an integrated health approach Sue Hatton Workforce Development Specialist for Women and Children
NHS Borders. Local Report ~ November Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services
 NHS Borders Local Report ~ November 2009 Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services NHS Borders Local Report ~ November 2009 Clinical Governance
NHS Borders Local Report ~ November 2009 Clinical Governance & Risk Management: Achieving safe, effective, patient-focused care and services NHS Borders Local Report ~ November 2009 Clinical Governance
Family Nurse Partnership Caseload Management
 Standard Operating Procedure 5 (SOP 5) Family Nurse Partnership Caseload Management Why we have a procedure? Family Nurse Partnership (FNP) is an evidenced based licensed programme that was developed in
Standard Operating Procedure 5 (SOP 5) Family Nurse Partnership Caseload Management Why we have a procedure? Family Nurse Partnership (FNP) is an evidenced based licensed programme that was developed in
Job Description NHS Dumfries and Galloway Occupational Health and Safety Services
 Job Description NHS Dumfries and Galloway Occupational Health and Safety Services Part Time Occupational Health Physician 2 sessions (0.2wte) 8 hours per week 1. JOB IDENTIFICATION Job Title: Part time
Job Description NHS Dumfries and Galloway Occupational Health and Safety Services Part Time Occupational Health Physician 2 sessions (0.2wte) 8 hours per week 1. JOB IDENTIFICATION Job Title: Part time
Whittington Health Quality Strategy
 Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Public Health Skills and Career Framework Multidisciplinary/multi-agency/multi-professional. April 2008 (updated March 2009)
") Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Item No: 14. Meeting Date: Wednesday 8 th November Glasgow City Integration Joint Board
 Item No: 14 Meeting Date: Wednesday 8 th November 2017 Glasgow City Integration Joint Board Report By: David Williams, Chief Officer Contact: Susanne Millar, Chief Officer, Strategy & Operations / Chief
Item No: 14 Meeting Date: Wednesday 8 th November 2017 Glasgow City Integration Joint Board Report By: David Williams, Chief Officer Contact: Susanne Millar, Chief Officer, Strategy & Operations / Chief
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
Learning from adverse events. Learning and improvement summary
 Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
SUBJECT: QUALITY ASSURANCE AND IMPROVEMENT
 Meeting of Lanarkshire NHS Board: 31. 05. 2017 Lanarkshire NHS Board Kirklands Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: QUALITY ASSURANCE AND
Meeting of Lanarkshire NHS Board: 31. 05. 2017 Lanarkshire NHS Board Kirklands Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: QUALITY ASSURANCE AND
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
TITLE OF REPORT: Looked After Children Annual Report
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
Wolverhampton Public Health Effective Commissioning Strategy
 Date: 24 September 2014 ATTACHED: Wolverhampton Public Health Effective Commissioning Strategy 2014-2019 Executive summary. Wolverhampton Public Health Effective Commissioning Strategy 2014-2019 Executive
Date: 24 September 2014 ATTACHED: Wolverhampton Public Health Effective Commissioning Strategy 2014-2019 Executive summary. Wolverhampton Public Health Effective Commissioning Strategy 2014-2019 Executive
NHS Nursing & Midwifery Strategy
 Colchester Hospital University NHS Foundation Trust NHS Nursing & Midwifery Strategy 2015-2018 Foreword Caring with Pride is our three-year Nursing & Midwifery Strategy for Colchester Hospital University
Colchester Hospital University NHS Foundation Trust NHS Nursing & Midwifery Strategy 2015-2018 Foreword Caring with Pride is our three-year Nursing & Midwifery Strategy for Colchester Hospital University
Quality Improvement Strategy 2017/ /21
 Quality Improvement Strategy 2017/18-2020/21 Contents Section Title Page Number Foreword from Chair and Chief Executive 2 Section 1 Introduction What does Quality mean to us? What do we want to achieve
Quality Improvement Strategy 2017/18-2020/21 Contents Section Title Page Number Foreword from Chair and Chief Executive 2 Section 1 Introduction What does Quality mean to us? What do we want to achieve
HEALTH AND SAFETY POLICY
 NHS GREATER GLASGOW AND CLYDE HEALTH AND SAFETY POLICY November 2015 Lead Manager: K. Fleming Head of Health and Safety Responsible Director A. MacPherson Director of Human Resources and Organisational
NHS GREATER GLASGOW AND CLYDE HEALTH AND SAFETY POLICY November 2015 Lead Manager: K. Fleming Head of Health and Safety Responsible Director A. MacPherson Director of Human Resources and Organisational
NHS Greater Glasgow and Clyde. Workforce Plan 2014/15. New South Glasgow Hospitals. New South Glasgow Hospitals
 NHS Greater Glasgow and Clyde Workforce Plan 2014/15 New Maryhill Health Centre, opening Q1, 2015 New Possilpark Health Centre, opened Feb 14 New South Glasgow Hospitals New South Glasgow Hospitals Contents
NHS Greater Glasgow and Clyde Workforce Plan 2014/15 New Maryhill Health Centre, opening Q1, 2015 New Possilpark Health Centre, opened Feb 14 New South Glasgow Hospitals New South Glasgow Hospitals Contents
Commissioning Intentions 2019 / 20
 Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
INVERCLYDE COMMUNITY HEALTH AND CARE PARTNERSHIP - DRAFT SCHEME OF ESTABLISHMENT
 EMBARGOED UNTIL DATE OF MEETING Greater Glasgow and Clyde NHS Board Board Meeting Tuesday 17 th August 2010 Board Paper No. 2010/34 Director of Corporate Planning and Policy/Lead NHS Director Glasgow City
EMBARGOED UNTIL DATE OF MEETING Greater Glasgow and Clyde NHS Board Board Meeting Tuesday 17 th August 2010 Board Paper No. 2010/34 Director of Corporate Planning and Policy/Lead NHS Director Glasgow City
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
Transforming Mental Health Services Formal Consultation Process
 Project Plan for the Transforming Mental Health Services Formal Consultation Process June 2017 TMHS Project Plan v6 21.06.17 NOS This document can be made available in different languages and formats on
Project Plan for the Transforming Mental Health Services Formal Consultation Process June 2017 TMHS Project Plan v6 21.06.17 NOS This document can be made available in different languages and formats on
The Care Values Framework
 The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
EQuIPNational Survey Planning Tool NSQHSS and EQuIP Actions 4.
 Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement