Crash Course in Medical Necessity for E/M Coders. Regional Conference
|
|
|
- Claud Lynch
- 6 years ago
- Views:
Transcription

1 Crash Course in Medical Necessity for E/M Coders Regional Conference

2 About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions that allow coders to help physicians to best pursue their hard-earned art in the practice of medicine. She is an executive level healthcare sales, operations, and public speaking expert with significant & broad ambulatory healthcare business experience with emphasis on multispecialty physician groups and payers. She has served as a senior executive for over 15 years. In prior roles: as VP of Coding Operations with Aviacode, overseeing the coding operation of more than 30 million claims per year. As Chief Audit Officer for Parses, Inc, she assured physician medical coding audit accuracy & quality control for payer driven recovery audits of professional fees and was responsible for driving sales & managing new coding audit programs. Stephanie lives in Salt Lake City, Utah with her husband Jim and their three children. Stephanie is LION (Linked In Open Network).
3 You Learn how to confidently code the correct E/M level ---every time Discover when documentation becomes a compliance problem Stop over-coding or under-coding claims based on Medical Necessity Gain an essential understanding of regulations that effect E/M documentation Combat today s most challenging E/M leveling errors with actionable info Learn 5 things every coder should do to accurately code for Medical Necessity 3

4 Drowning in Documentation. Dying of thirst for information.
5 Thousands of Pages in legalese Federal Register OIG Compliance Guidance ICD 10 Official Guidelines CMS.gov Internet-Only Manuals (IOMs) Chapter 12 Physicians Medicare Claims Processing Manual CMS Medicare Benefit Policy Manual CPT guidelines CMS 1995 and 1997 DGs for EM HIPAA CCI National Correct Coding Initiative (NCCI) False Claims Act and Qui Tam Social Security Act (Medical Necessity)

6 Mixed Messages & Documentation Medical Necessity & Value Based Laws & Malpractice EMR HITECH Act & CMS DGs & Non Clinical Work

7 The Truth In Soapy Coding Subjective: Opinions Medical Necessity is a clinically required action It is the reason for a service It validates the provision of service o It is open for interpretation by all parties involved
8 Objective: Facts Medical Decision Making E/M Component is a measurement of work It is defined by: o 1995 and 1997 Documentation Guidelines o Marshfield Clinic audit tool. Medical Decision Making is the mathematically formulated result of all documented components of the physician s service, whether medically needed or not. o It is the data driven outcome of a patient visit and not a substitute for determining the appropriateness of the services rendered or the Medical Necessity.

9 Assessment: Judgements The best way to stay compliant with Medical Necessity related laws is to think of each element of the patient s history and physical exam as a separate procedure that should be performed only if there is a clear medical reason to do so. This requires making a clinical judgement. A coder, while better educated than most non-clinicians, is not able to make that judgment with the certainty of a medical peer.

10 Plan: Strategies In an effort to bridge the gap between the clinical savvy of a documenting provider and a clinically untrained coder some coding administrators have exchanged the definition of Medical Necessity with the MDM component of E/M services. This mistake can leave money on the table or result in overpayments. A different strategy is needed
11 The Medical Necessity Problem Incorrect E/M coding resulted in $1.4B in overpayments in Problem code had a 50.4% error rate in 2015 Problem code had a 14.3% error rate in 2015 Problem code had a 16.5% error rate in 2015 Medical Necessity errors are nearly twice as common as are coding errors. CMS 1995 and 1997 Documentation Guidelines are not statutes Medical need for services rendered is the authoritative factor o Medical necessity is not defined
12 How is Medical Necessity Defined? Government: Per the Social Security Act 42 U.S.C. 1395y(a)(1)(A), SSA Medicare only pays for medical items and services that are "reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member", unless there is another statutory authorization for payment. National coverage determinations (NCDs) and Local Coverage Determinations (LCDs). Section 522 of the Benefits Improvement and Protection Act (BIPA) defines an LCD as a decision by a Medicare carrier whether to cover a particular service in accordance with the SSA
13 AMA Health care services or products that a prudent physician would provide to a patient for the purpose of preventing, diagnosing, or treating an illness, injury, disease or its symptoms in a manner that is: (a) in accordance with generally accepted standards of medical practice; (b) clinically appropriate in terms of type, frequency, extent, site and duration; and (c) not primarily for the convenience of the patient, physician, or other health care provider.
14 Generally Accepted What is common acknowledged as generally accepted? Standards that are based on credible scientific evidence published in peer-reviewed, medical literature generally recognized by the relevant medical community; Physician specialty society recommendations; The views of physicians practicing in the relevant clinical area.
15 Evidence Based Guidelines Industry standard guidelines for evidence based determinations of Medical Necessity by payers include MCG (formerly Milliman Care Guidelines) by MCG Health LLC of the Hearst Health network, and InterQual by McKesson. o InterQual provides a structure of criteria for "severity of illness (SI) and "intensity of service (IS)" to help determine if a patient is sick enough to be admitted an inpatient. These standards are helpful insights, however are incomplete substitutes for the clinical judgment of the physician.
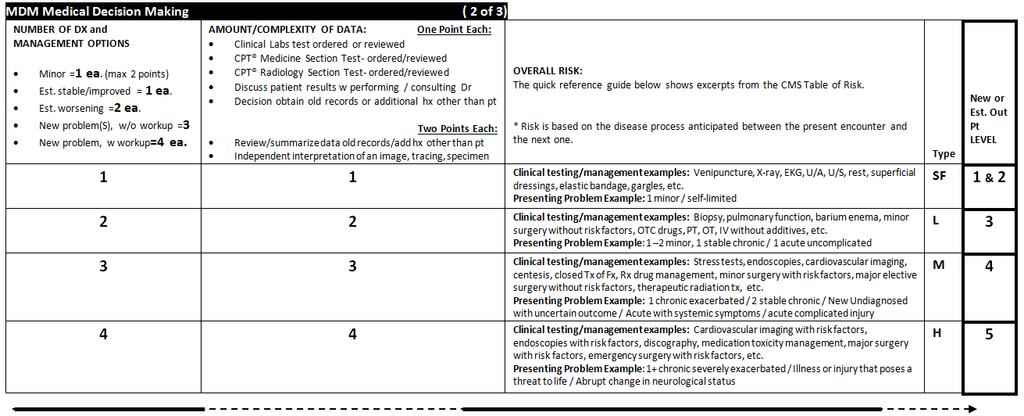
16 CPT Nature of the Presenting Problem Minimal: A problem that may not require the presence of the physician or other qualified health care professional, but service is provided under the physician s or other qualified health care professional s supervision. Self-limited or minor: A problem that runs a definite and prescribed course, is transient in nature, and is not likely to permanently alter health status OR has a good prognosis with management/compliance. Low severity: A problem where the risk of morbidity without treatment is low; there is little to no risk of mortality without treatment; full recovery without functional impairment is expected. Moderate severity: A problem where the risk of morbidity without treatment is moderate; there is moderate risk of mortality without treatment; uncertain prognosis OR increased probability of prolonged functional impairment. High severity: A problem where the risk of morbidity without treatment is high to extreme; there is a moderate to high risk of mortality without treatment OR high probability of severe, prolonged functional impairment.

17 MDM as a MN Driver? Example: Number of Diagnoses and Management Options: o A patient with a new problem is diagnosed during the same encounter with a problem that is more severe than a minor problem. This is worth 3 on the MDM scale of Number of Diagnoses and Management Options. Amount/Complexity of Data: o The physician ordered and reviewed a medical test in his office. This is worth 1 on the Amount and Complexity of Data Overall Risk: o The problem requires a prescription medication, which the physician orders.
18 Clinically Stated The patient has sudden central vision loss and is sent to a Retina specialist for diagnosis and treatment. A history is obtained and both eyes are thoroughly examined. Several optic tests are used, including an Amsler grid and optical coherence tomography. A new diagnosis is made by the physician of sub choroidal neovascularization for which he recommends a monthly injection of Avastin. He explains the risk of the injections, and shares with the patient the risk of continued vision loss with or without the injection. The patient elects to have the injection the same day. Follow-up in 3 weeks for evaluation and repeat injection.

19 MDM as a MN Driver? 19
20 Answer is a Level Four, right? Well What if the patient was sent by the physician to be worked up at an outside facility, and the patient returned with the test results for final diagnosis with the results on the same day? What if the provider decides that the risk of the problem is not classifiable as that associated with Prescription drug management, but rather with the risk associated with an acute illness or injury that poses a threat to bodily function (in this case vision)? In terms of code selection for Medical Necessity with an MDM driver, this could now support a Level Five new or established Outpatient patient. Another example: 45-year-old, otherwise healthy male returns for a non-resolved problem first seen 5 days ago.a cough x 7 days which is now productive. This patient is also under the physician s care for well controlled hypertension and hypercholesterolemia. The diagnosis today is URI. She reviews all the patient s current medications and adds to it by ordering an antibiotic. No follow-up requested MDM is moderate.is this a Level Four clinical example?

21 Five Secrets to Success Accept That There Is No Tool That Can Replace A Physician In Medical Necessity Determinations on E/M codes.


22 Five Secrets to Success Understand why the topic of payment is a source of physician frustration Let s take a closer look

23 Only the best Can be a physician.

24 Devaluation of the work by a physician 50% of physicians feel devalued RVUs are used in the Physician Fee Schedule The Physician Work RVU is based on government estimates on time and complexity RVUs are used by employers who measure productivity and calculate salaries or bonuses To generate income a physician must be actively providing an allowed service. o No payments for work solely humanistic in nature, such as time with a grieving family o No payments for time in meeting required documentation requirements o Can take 3 or more hours per day

25 Five Secrets to Success Communicate with physicians quickly, concisely and in terms they can relate to



26 Inspire me Provide a clear vision o What makes your heart sing? Energy, Energize, Edge, and Execution o Dopamine Be memorable o Work in emotionally charged moments o Teach in a new way, or an unusual place Be novel o Fresh, new and unexpected twist o Tell a story o Tell someone else s story


27 Scale of 1-5 Levels 3-5* are reserved for sick or injured patients. Lower levels are for patients who present with minor and/or well controlled condition/s. *This presentation refers to levels of service for outpatient visits.
28 Sickest (5/3) Presenting Problem: An illness or injury that poses a threat to life, chronic severely exacerbated, abrupt change in neurological status Typically the patient s situation is serious, imminent, and uncertain o Severe exacerbation of CHF o Patient presents confused in diabetic ketoacidosis o Morphine Sulfate IVP ordered for chest pain not controlled by Nitro o Patient brought by parents after a failed suicide attempt o Patient post fall on ski slopes with extradural hematoma o hospital inpatient who is rapidly declining
29 Sick (3/1) Typical Presenting Problem: 1 2 minor, 1-2 stable chronic, 1-2 acute uncomplicated Typically the diagnosis is known and/or made during the encounter Future follow up is often classifiable as routine o Patient returns with productive cough x 10 days for antibiotic o Patient with choroidal revascularization to assess efficacy of anti-vegf o Follow up Patient with cystocele not requiring treatment o Patient in follow up with stable angina and no new symptoms o Return visit for patient with worsening plantar fasciitis o Non pregnant female with resolving hyperemesis o Patient with well controlled hypertension and hypercholesterolemia o Hospital patient who is getting better and progressing to discharge
30 Sicker (4/2) Presenting Problem: 2-3 stable chronic, chronic exacerbated, acute with systemic symptoms or injury Typically the diagnosis is known and worsening/complicated or further testing is required Future follow up is often classifiable as routine or sooner o Patient with choroidal revascularization now with new central vision loss o Patient in follow up with stable angina, not tolerating medication o Patient with suspected cellulitis of the lower leg o Patient with heel ulcer and drainage o Hospital inpatient who isn t getting better or progressing to discharge but is not declining

31 Five Secrets to Success Master the Art of Asking the Right Questions
32 CDI: The Physician Interview The best way to communicate with physicians is to ask questions that allow them to draw their own conclusions. Your goal is to promote effective communication Ask questions that are not answered with yes or no what made you more concerned about this patient encounter than the other one? versus did you understand what makes this a Level Four?
33 Effective Communication Listen: Don t think about what you will say next while the physician is talking Have a clear idea of what you want to say so you can be organized in your delivery Example: o Doctor, I have reviewed this patient encounter, and your superbill. You selected a Level Four. You saw this patient 1 month ago for premenopausal syndrome mood swings and prescribed Zoloft. You saw her again today in follow-up. You repeated a comprehensive history and exam. She is doing well with reduced mood swings and will continue with sertraline 50MG. You ask to see her back in 12 months or PRN if there is a change. I am concerned that an auditor might question the higher Level of service being billed because you are not seeing her back for 12 months and there are no other problems documented. o What was it about this patient that put her at a higher Level of concern to be coded at a Level Four?
34 Provider Interview Always customize CDI Run a productivity report of the last one to three months of Outpatient visits that shows the top diagnosis codes used and the frequency of their use. Ask Questions: Dr., what about these diagnoses make you more (i.e. 4) or less (i.e. 3) concerned about a patient? Code Count of Occurrence Short Description Threat to Life/Function D Anemia Yes/No E Congenital hypothyroidism s goiter Yes/No F Generalized anxiety disorder Yes/No I10 42 Essential (primary) hypertension Yes/No
35 Sample Interview Questions Do any of these pose a threat to life or bodily function within hours? (Level Five) Under what circumstances would you see a patient in follow-up sooner than typically required? (Level Four) Which patient problems have you very concerned for the patient but do not pose an imminent threat to life or bodily function? (Level Four) Which of these can commonly be diagnosed on the first encounter and do not usually require a prompt follow-up? (Level Three) Which of these problems might you bring a patient back for a quick check, and on doing so discover no further medical management is needed? (Level Two) Which of these diagnoses are self-limited and require reassurance with no active medical management? (Level One) Would a non-friendly medical peer agree with your decisions?


36 Five Secrets to Success Address the problems head on ---and use effective tools to communicate effectively and code confidently. Let s address the 2 main problems:
37 Over-coding Problem MN is a 3

38 Under-coding Problem MN is a 5 Confidential Planning Document - IP - DO NOT DISTRIBUTE 9/28/2016

39 The Solution: Communication Improvement Fixing the communication problem Medical Necessity Noted in the Record o Coder can prevent over-coding o Coder can identify CDI needs to prevent under-coding
40 Level 1 I attest that I am billing for what was medically necessary for this patient. The severity of illness and the intensity of service provided by me today is associated with medical needs that were. Level 1 Out Pt: For a new Pt with a CC 1) That required reassurance with no active medical management (or) 2) Time based: counseling or coordinating care for the patient equal to the Level
41 Level 2 I attest that I am billing for what was medically necessary for this patient. The severity of illness and the intensity of service provided by me today is associated with medical needs that were. Level 2 Out Pt: For a new or established Pt: 1) With a minor CC (or) 2) To follow up to ensure efficacy of previous care AND Who required little or no active medical management OR Time based: counseling/coordinating care equal to the level
42 Level 3/1 I attest that I am billing for what was medically necessary for this patient. The severity of illness and the intensity of service provided by me today is associated with medical needs that were. Level 3 Out Pt/Level 1 In Pt.: For a new or established Pt: AND OR 1) With a CC diagnosed during this encounter (or) 2) To follow up on known problem/s that are progressing as expected Where the planned return is routine, and/or the problem/s presented no unusual or unexpected concerns for the medical outcome Time based: counseling/coordinating care equal to the level
43 Level 4/2 I attest that I am billing for what was medically necessary for this patient. The severity of illness and the intensity of service provided by me today is associated with medical needs that were. Level 4 Out Pt/Level 2 In Pt: For a new or established Pt: AND OR 1) With a CC requiring consideration of multiple comorbidities (or) 2) With a CC not progressing as expected, (or) 3) With a CC in a rule out stage pending outside tests With medical management requiring consideration of the added risk to the patient s medical outcomes Time based: counseling/coordinating care equal to the level
44 Level 5/3 I attest that I am billing for what was medically necessary for this patient. The severity of illness and the intensity of service provided by me today is associated with medical needs that were. Level 5 Out Pt/Level 3 In Pt: For a new or established Pt: AND OR 1) With a CC that is a probable threat to life within hours (or) 2) With a CC that is a probable threat to limb within hours (or) 3) With a CC that is a probable threat to organ function within hours (or) With medical management requiring consideration of the imminent risk or rapid decline in the patient s medical outcomes Time based: counseling/coordinating care equal to the level
45 Communication is Key To accuracy in medical necessity coding To preventing overpayments To minimizing underpayments with clinical documentation improvement training To reducing the need to query physicians or turn them into coders To increasing the accuracy and confidence of the coder
46 Thank you for your work and for supporting the delivery of excellent healthcare Stephanie Cecchini, CPC, CEMC, CHISP is LION (Linked In Open Network).
Crash Course in Medical Necessity for E/M Coders
 Crash Course in Medical Necessity for E/M Coders Stephanie Cecchini, CPC, CEMC, CHISP About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions
Crash Course in Medical Necessity for E/M Coders Stephanie Cecchini, CPC, CEMC, CHISP About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing solutions
CRASH COURSE MEDICAL NECESSITY SKILLS FOR NON PROVIDERS
 CRASH COURSE MEDICAL NECESSITY SKILLS FOR NON PROVIDERS PRESENTED BY: MAGGIE MAC CPC, CEMC, CHC, CMM, ICCE, AHIMA APPROVED ICD 10 CM/PCS TRAINER STEPHANIE CECCHINI, CPC, CEMC, CHISP, APPROVED ICD 10 TRAINER
CRASH COURSE MEDICAL NECESSITY SKILLS FOR NON PROVIDERS PRESENTED BY: MAGGIE MAC CPC, CEMC, CHC, CMM, ICCE, AHIMA APPROVED ICD 10 CM/PCS TRAINER STEPHANIE CECCHINI, CPC, CEMC, CHISP, APPROVED ICD 10 TRAINER
In the Shark Tank: When Coding Compliance Goes on Attack
 In the Shark Tank: When Coding Compliance Goes on Attack Stephanie Cecchini, CPC, CEMC, CHISP About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing
In the Shark Tank: When Coding Compliance Goes on Attack Stephanie Cecchini, CPC, CEMC, CHISP About the Presenter Stephanie Cecchini, CPC, CEMC, CHISP, is VP of Products at AAPC. Her passion is providing
Medical Necessity verses Medical Decision Making. Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC
 Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
Advanced E/M Auditing: Secrets to Success
 Advanced E/M Auditing: Secrets to Success Presented by Carrie Severson CPC, CPC-H, CPMA, CPC-I Senior Auditor, AAPC Client Services Why We Are Here OIG Report (OEI-04-10-00180) Coding Trends of Medicare
Advanced E/M Auditing: Secrets to Success Presented by Carrie Severson CPC, CPC-H, CPMA, CPC-I Senior Auditor, AAPC Client Services Why We Are Here OIG Report (OEI-04-10-00180) Coding Trends of Medicare
Medical Decision Making
 Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Demonstrating the Chain of Medical Necessity. Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President
 Demonstrating the Chain of Medical Necessity Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science,
Demonstrating the Chain of Medical Necessity Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC QCC CPC-I MCS-P CPMA CMHP AAPC Fellow Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science,
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
6/14/2017. Evaluation and Management Coding. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA
 Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
The presenter has owns Kelly Willenberg, LLC in relation to this educational activity.
 Kelly M Willenberg, MBA, BSN, CCRP, CHC, CHRC 1 The presenter has owns Kelly Willenberg, LLC in relation to this educational activity. 2 1 Medical Necessity when you submit claims Coding for qualifying
Kelly M Willenberg, MBA, BSN, CCRP, CHC, CHRC 1 The presenter has owns Kelly Willenberg, LLC in relation to this educational activity. 2 1 Medical Necessity when you submit claims Coding for qualifying
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
AAPC Richardson, TX Chapter. Monthly Meeting. 6pm. Location:
 AAPC Richardson, TX Chapter Monthly Meeting 4/17/2017 @ 6pm Location: Methodist Richardson/Renner Medical Center-Physician Pavilion I 2821 E President George-Physician Services Building, 2nd floor Conference
AAPC Richardson, TX Chapter Monthly Meeting 4/17/2017 @ 6pm Location: Methodist Richardson/Renner Medical Center-Physician Pavilion I 2821 E President George-Physician Services Building, 2nd floor Conference
3/16/2016. No Treble. OIG Reports. Highlights OIG Report Coding Trends. Presented by Maggie Mac CPC, CEMC, CHC, CMM, ICCE
 It s All About That E/M No Treble Presented by Maggie Mac CPC, CEMC, CHC, CMM, ICCE OIG Reports Coding Trends of Medicare Evaluation and Management Services ~ May 2012 Improper Payments for Evaluation
It s All About That E/M No Treble Presented by Maggie Mac CPC, CEMC, CHC, CMM, ICCE OIG Reports Coding Trends of Medicare Evaluation and Management Services ~ May 2012 Improper Payments for Evaluation
Quarterly CERT Error Findings Report WPS GHA Part B J8 MAC ~ Indiana and Michigan ~
 Quarterly CERT Error Findings Report WPS GHA Part B J8 MAC ~ Indiana and Michigan ~ This report provides details of Comprehensive Error Rate Testing (CERT) errors assessed April 1, 2017, through June 30,
Quarterly CERT Error Findings Report WPS GHA Part B J8 MAC ~ Indiana and Michigan ~ This report provides details of Comprehensive Error Rate Testing (CERT) errors assessed April 1, 2017, through June 30,
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
Medical Necessity: Not just LCD. Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC
 Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
CODING vs AUDITING Does it all boil down to Medical Necessity?
 PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
PSYCHIATRY SERVICES: MD FOCUSED
 PSYCHIATRY SERVICES: MD FOCUSED CY2013 Risk Based Scheduled Review Agenda 2 Overview of New Risk Based Scheduled Reviews Initial review findings PhD summary MD summary Examples Template/Psychotherapy Time
PSYCHIATRY SERVICES: MD FOCUSED CY2013 Risk Based Scheduled Review Agenda 2 Overview of New Risk Based Scheduled Reviews Initial review findings PhD summary MD summary Examples Template/Psychotherapy Time
2019 Evaluation and Management Coding Advisor. Advanced guidance on E/M code selection for traditional documentation systems
 2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
The E/M Essentials Pocket Guide
 The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CCS-P, CEMC The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CEMC, CCS-P The E/M Essentials Pocket Guide is published by HCPro, a division
The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CCS-P, CEMC The E/M Essentials Pocket Guide Peggy S. Blue, MPH, CPC, CEMC, CCS-P The E/M Essentials Pocket Guide is published by HCPro, a division
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Evaluation and Management
 Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Outpatient Observation Services
 Outpatient Observation Services Presented by: Gina Hobert, MBA, CHC, CPC-I, CPMA, CEMC, CRC Sr. Manager, Baker Newman Noyes Definition MCR Benefit Policy Manual, CMS 100-02, Chapter 6, 20.6 A. Outpatient
Outpatient Observation Services Presented by: Gina Hobert, MBA, CHC, CPC-I, CPMA, CEMC, CRC Sr. Manager, Baker Newman Noyes Definition MCR Benefit Policy Manual, CMS 100-02, Chapter 6, 20.6 A. Outpatient
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness. October 12, 2009
 Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness October 12, 2009 Betty B. Bibbins, MD, CHC, FACOG, C-CDI, C CDI, CPEHR, CPHIT President & Chief
Clinical Documentation Improvement Programs and Physician Advisors: Working Together to Improve Effectiveness October 12, 2009 Betty B. Bibbins, MD, CHC, FACOG, C-CDI, C CDI, CPEHR, CPHIT President & Chief
The Business of Medicine
 The Business of Medicine Coding as a profession Objectives How the coder fits in Hospital vs. physician services Hierarchy of providers Reimbursement aspects Payers Medical necessity ABN 1 Regulations
The Business of Medicine Coding as a profession Objectives How the coder fits in Hospital vs. physician services Hierarchy of providers Reimbursement aspects Payers Medical necessity ABN 1 Regulations
EMTALA. Federal Law and the Medical Staff. Shaheed Koury, MD, MBA, FACEP SVP & Chief Medical Officer Quorum Health
 EMTALA Federal Law and the Medical Staff Shaheed Koury, MD, MBA, FACEP SVP & Chief Medical Officer Quorum Health Objectives Review EMTALA Law Clarify Key Terms Define Hospital and Physician Responsibilities
EMTALA Federal Law and the Medical Staff Shaheed Koury, MD, MBA, FACEP SVP & Chief Medical Officer Quorum Health Objectives Review EMTALA Law Clarify Key Terms Define Hospital and Physician Responsibilities
Transition Care Management Update: Practical Applications for 2016
 60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
Coding, Corroboration, and Compliance How to assure the 3 C s are met
 Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Cotiviti Approved Issues List as of April 27, 2017
 Cotiviti Approved Issues List as of April 27, 2017 Ambulatory Surgery Center (ASC); Outpatient Hospital 23 Inpatient Hospital 25 Inpatient Hospital; Inpatient Psychiatric Facility 27 Inpatient; Outpatient;
Cotiviti Approved Issues List as of April 27, 2017 Ambulatory Surgery Center (ASC); Outpatient Hospital 23 Inpatient Hospital 25 Inpatient Hospital; Inpatient Psychiatric Facility 27 Inpatient; Outpatient;
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC
 Service in RHC") How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
Getting paid properly requires a thorough knowledge of the rules.
 Selecting E/M Codes For Established Patients Getting paid properly requires a thorough knowledge of the rules. Kenneth F. Malkin, D.P.M. Bio: Dr. Malkin is a diplomate of the American Board of Quality
Selecting E/M Codes For Established Patients Getting paid properly requires a thorough knowledge of the rules. Kenneth F. Malkin, D.P.M. Bio: Dr. Malkin is a diplomate of the American Board of Quality
Care Transition Strategies: The 2013 Transition Care Management Codes
 Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
9/17/2018. Critical to Practices
 Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
AMBULANCE SERVICES. Guideline Number: CS003.F Effective Date: January 1, 2018
 AMBULANCE SERVICES UnitedHealthcare Community Plan Coverage Determination Guideline Guideline Number: CS003.F Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
AMBULANCE SERVICES UnitedHealthcare Community Plan Coverage Determination Guideline Guideline Number: CS003.F Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
Conquering Consults. Objectives. Kim Reid,, CPC,, CPC-I,, CEMC
 Conquering Consults Kim Reid,, CPC,, CPC-I,, CEMC Objectives Clearing up p cons consult lt conf confusion sion Understanding the consult requirements How do we code/document now that Medicare no longer
Conquering Consults Kim Reid,, CPC,, CPC-I,, CEMC Objectives Clearing up p cons consult lt conf confusion sion Understanding the consult requirements How do we code/document now that Medicare no longer
Are they coming to get you! Todd Thomas, CCS-P
 Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
601-Audit Plan for Medicare s Shared Visit Rule
 601-Audit Plan for Medicare s Shared Visit Rule Elin Baklid-Kunz, MBA, CPC, CCS Health Care Compliance Association 6500 Barrie Road, Suite 250, Minneapolis, MN 55435 888-580-8373 www.hcca-info.org Presentation
601-Audit Plan for Medicare s Shared Visit Rule Elin Baklid-Kunz, MBA, CPC, CCS Health Care Compliance Association 6500 Barrie Road, Suite 250, Minneapolis, MN 55435 888-580-8373 www.hcca-info.org Presentation
Coding for the Practitioner
 Coding for the Practitioner Prepared for Coalition of State Rheumatology Organizations National Rheumatology Fellows Conference February 2018 Presented by: Jean Acevedo, LHRM, CPC, CHC, CENTC Disclaimer
Coding for the Practitioner Prepared for Coalition of State Rheumatology Organizations National Rheumatology Fellows Conference February 2018 Presented by: Jean Acevedo, LHRM, CPC, CHC, CENTC Disclaimer
The Medicare Local Coverage Determination Process and Clinical Trials
 The Medicare Local Coverage Determination Process and Clinical Trials Richard K. Baer, M.D. Medical Director, National Government Services Health Care Compliance Association 6500 Barrie Road, Suite 250,
The Medicare Local Coverage Determination Process and Clinical Trials Richard K. Baer, M.D. Medical Director, National Government Services Health Care Compliance Association 6500 Barrie Road, Suite 250,
10/7/2014. Agenda. Big picture Internal Medicine Update. The Two Midnight Rule: One Year Later
 2014 Internal Medicine Update SC Chapter Scientific Meeting The Two Midnight Rule: One Year Later Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case Management, SRHS Agenda Define status
2014 Internal Medicine Update SC Chapter Scientific Meeting The Two Midnight Rule: One Year Later Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case Management, SRHS Agenda Define status
Polling Question #1. Denials and CDI: A Recovery Auditor s Perspective
 1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
Coding and Billing for Lifestyle Medicine
 Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Evaluation & Management
 Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
Billing and Coding Tidbits for Not Leaving $$ on the Table
 Billing and Coding Tidbits for Not Leaving $$ on the Table Presented by Sarah Reed BSE, CPC, CPC-I Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Presentation Objectives Review some
Billing and Coding Tidbits for Not Leaving $$ on the Table Presented by Sarah Reed BSE, CPC, CPC-I Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Presentation Objectives Review some
Getting Paid for What You Do! Coding 2010
 Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
Start with the Problem
 Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Preparing for ICD 10 Compliance While Living in ICD 9 A Challenge to Overcome
 Preparing for ICD 10 Compliance While Living in ICD 9 A Challenge to Overcome Betty B. Bibbins, MD, BSN, CHC, C CDI, CPEHR, CPHIT President & Chief Medical Officer Physician Executive Educator DocuComp
Preparing for ICD 10 Compliance While Living in ICD 9 A Challenge to Overcome Betty B. Bibbins, MD, BSN, CHC, C CDI, CPEHR, CPHIT President & Chief Medical Officer Physician Executive Educator DocuComp
See the Time chapter for complete instructions on how to code using time as the controlling factor when selecting an E/M code.
 2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
Focus On Observation
 Focus On Observation Introduction CPT and CMS Requirements CPT Codes Documentation Requirements Observation Coding: Facility Considerations 2 LogixHealth s unsurpassed service stems from the fact that
Focus On Observation Introduction CPT and CMS Requirements CPT Codes Documentation Requirements Observation Coding: Facility Considerations 2 LogixHealth s unsurpassed service stems from the fact that
Documentation for ED Visits with "Additional Work-Up" Planned. Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS
 Documentation for ED Visits with "Additional Work-Up" Planned Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS Course Objectives Discuss gray areas for E/M selection for the professional
Documentation for ED Visits with "Additional Work-Up" Planned Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS Course Objectives Discuss gray areas for E/M selection for the professional
THE ART OF DIAGNOSTIC CODING PART 1
 THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
THE ART OF DIAGNOSTIC CODING PART 1 Judy Adams, RN, BSN, HCS-D, HCS-O June 14, 2013 2 Background Every health care setting has gone through similar changes in the need to code more thoroughly. We can learn
General Information. Overview. Purpose. Table of Contents
 Blue Cross and Blue Shield of Georgia, Inc. and Blue Cross Blue Shield Healthcare Plan of Georgia, Inc.engage Inovalonto conduct outreach efforts for ouraca individual and small group on and off exchange
Blue Cross and Blue Shield of Georgia, Inc. and Blue Cross Blue Shield Healthcare Plan of Georgia, Inc.engage Inovalonto conduct outreach efforts for ouraca individual and small group on and off exchange
UTILIZATION MANAGEMENT Section 4. Overview The Plan s Utilization Management (UM)
") Overview The Plan s Utilization Management (UM) Program is designed to meet contractual requirements and comply with federal regulations while providing members access to high quality, cost effective medically
Overview The Plan s Utilization Management (UM) Program is designed to meet contractual requirements and comply with federal regulations while providing members access to high quality, cost effective medically
1:35. NPP April Young Medical Consulting, LLC. Non-Physician Practitioner Coding and Billing. Disclaimer
 Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
Non-Physician Practitioner Coding and Billing Jill Young - CPC, CEDC, CIMC, East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing. The information
Cotiviti Approved Issues List as of February 26, 2018
 Cotiviti Approved Issues List as of February 26, 2018 All physician/npp specialties 32 Ambulance Providers 34 Ambulatory Surgery Center (ASC), Outpatient Hospital 38 Inpatient Hospital 40 Inpatient Hospital,
Cotiviti Approved Issues List as of February 26, 2018 All physician/npp specialties 32 Ambulance Providers 34 Ambulatory Surgery Center (ASC), Outpatient Hospital 38 Inpatient Hospital 40 Inpatient Hospital,
Observation Services Tool for Applying MCG Care Guidelines
 In the event of a conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include
In the event of a conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include
Updates in Coding & Billing Strategies.
 Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
The World of Evaluation and Management Services and Supporting Documentation
 The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
Special Fall/Winter 2016 Presentation Medical Necessity Crash Course for E/M Coders
 Special Fall/Winter 2016 Presentation Medical Necessity Crash Course for E/M Coders 1 Medical Necessity Crash Course for E/M Coders Written By: Stephanie Cecchini, CPC, CEMC, CHISP, AHIMA Approved ICD
Special Fall/Winter 2016 Presentation Medical Necessity Crash Course for E/M Coders 1 Medical Necessity Crash Course for E/M Coders Written By: Stephanie Cecchini, CPC, CEMC, CHISP, AHIMA Approved ICD
Critical Care What Makes this so Difficult
 Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
ICD-9 (Diagnosis) Coding
 Coding") 1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
1 Disclaimer This presentation is intended only for use by Tulane University faculty, staff, and students. No copy or use of this presentation should occur without the permission of Tulane University.
Sharpen coding skills and reimbursement strategies during ICD-10 delay The Centers for Medicare & Medicaid Services (CMS) once again has extended the
 once again has extended the") Ambulatory Surgery Centers Sharpen coding skills and reimbursement strategies during ICD-10 delay The Centers for Medicare & Medicaid Services (CMS) once again has extended the deadline to begin using
Ambulatory Surgery Centers Sharpen coding skills and reimbursement strategies during ICD-10 delay The Centers for Medicare & Medicaid Services (CMS) once again has extended the deadline to begin using
Medicare: This subset aligns with the requirements defined by CMS and is for the review of Medicare and Medicare Advantage beneficiaries
 InterQual Level of Care Criteria Subacute & SNF Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
InterQual Level of Care Criteria Subacute & SNF Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
RULES OF TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT WORKERS COMPENSATION DIVISION
 RULES OF TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT WORKERS COMPENSATION DIVISION CHAPTER 0800-02-25 WORKERS COMPENSATION MEDICAL TREATMENT TABLE OF CONTENTS 0800-02-25-.01 Purpose and Scope
RULES OF TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT WORKERS COMPENSATION DIVISION CHAPTER 0800-02-25 WORKERS COMPENSATION MEDICAL TREATMENT TABLE OF CONTENTS 0800-02-25-.01 Purpose and Scope
PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE
 PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE IN-ACC October 13, 2018 Linda Gates-Striby CCS-P, ACS-CA St. Vincent Medical Group Director Quality Assurance Lggates@ascension.org
PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE IN-ACC October 13, 2018 Linda Gates-Striby CCS-P, ACS-CA St. Vincent Medical Group Director Quality Assurance Lggates@ascension.org
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Communicator. the JUST A THOUGHT. Ensuring HEDIS-Compliant Preventive Health Services. Provider Portal Features. Peer-to-Peer Review BY DR.
 WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
FindACode.com Presents: Integrating NPP into E/M for Compliance and Quality Care. Excerpts from:
 FindACode.com Presents: Integrating NPP into E/M for Compliance and Quality Care Excerpts from: Practical E/M: Documentation and Coding Solutions for Quality Patient Care by Dr. Stephen R. Levinson To
FindACode.com Presents: Integrating NPP into E/M for Compliance and Quality Care Excerpts from: Practical E/M: Documentation and Coding Solutions for Quality Patient Care by Dr. Stephen R. Levinson To
FAQ for Coding Encounters in ICD 10 CM
 FAQ for Coding Encounters in ICD 10 CM Topics: Encounter for Routine Health Exams Encounter for Vaccines Follow Up Encounters Coding for Injuries Encounter for Suture Removal External Cause Codes Tobacco
FAQ for Coding Encounters in ICD 10 CM Topics: Encounter for Routine Health Exams Encounter for Vaccines Follow Up Encounters Coding for Injuries Encounter for Suture Removal External Cause Codes Tobacco
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
Appendix A WORK PROCESS SCHEDULE AND RELATED INSTRUCTION OUTLINE. Health Information Management (HIM) Professional Fee Coder Apprenticeship
 Professional Fee Coder Apprenticeship") Appendix A WORK PROCESS SCHEDULE AND RELATED INSTRUCTION OUTLINE Health Information Management (HIM) Professional Fee Coder Apprenticeship O*NET-SOC CODE: 29-2071.00 RAPIDS CODE: Type of Training: Competency-based
Appendix A WORK PROCESS SCHEDULE AND RELATED INSTRUCTION OUTLINE Health Information Management (HIM) Professional Fee Coder Apprenticeship O*NET-SOC CODE: 29-2071.00 RAPIDS CODE: Type of Training: Competency-based
Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims
 March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
Preventive and Sick Visits Same Day. Objectives
 Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
SECTION 9 Referrals and Authorizations
 SECTION 9 Referrals and Authorizations General Information The PAMF Utilization Management (UM) Program is carried out by the Managed Care department. The UM Program is designed to ensure that all Members
SECTION 9 Referrals and Authorizations General Information The PAMF Utilization Management (UM) Program is carried out by the Managed Care department. The UM Program is designed to ensure that all Members
Addressing Documentation Insufficiencies
 Objectives Addressing Documentation Insufficiencies ICAHN June 9,2015 Glenn Krauss, BBA, RHIA, CCS, FCS, PCS,CCS-P, CPUR, C-CDI, CCDS, C- DAM Understand and appreciate physician frustrations with the EHR
Objectives Addressing Documentation Insufficiencies ICAHN June 9,2015 Glenn Krauss, BBA, RHIA, CCS, FCS, PCS,CCS-P, CPUR, C-CDI, CCDS, C- DAM Understand and appreciate physician frustrations with the EHR
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance?
 Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
NEXTGEN E&M CODING DEMONSTRATION
 NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: observation_room_services 2/1997 3/2013 3/2014 3/2013 Description of Procedure or Service Observation services
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: observation_room_services 2/1997 3/2013 3/2014 3/2013 Description of Procedure or Service Observation services
NEXTGEN E&M CODING DEMONSTRATION
 NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
OUTPATIENT DOCUMENTATION IMPROVEMENT
 OUTPATIENT DOCUMENTATION IMPROVEMENT Pam Brooks, MHA, COC, PCS, CPC Coding Manager Wentworth-Douglass Hospital Dover NH Disclaimer This presentation is for general education purposes only. The information
OUTPATIENT DOCUMENTATION IMPROVEMENT Pam Brooks, MHA, COC, PCS, CPC Coding Manager Wentworth-Douglass Hospital Dover NH Disclaimer This presentation is for general education purposes only. The information
Procedure Code Job Aid
 Procedure Code 99211 Job Aid Definition for 99211: Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician. Usually,
Procedure Code 99211 Job Aid Definition for 99211: Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician. Usually,
Certified Ophthalmic Executive (COE) Review Day
 Review Day") Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
3M Health Information Systems. A case study in coding compliance: Achieving accuracy and consistency
 3M Health Information Systems A case study in coding compliance: Achieving accuracy and consistency A case study in coding compliance: Achieving accuracy and consistency The challenge Coding compliance
3M Health Information Systems A case study in coding compliance: Achieving accuracy and consistency A case study in coding compliance: Achieving accuracy and consistency The challenge Coding compliance
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule. Grace Wilson, RHIA
 Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
EMERGENCY HEALTH CARE SERVICES AND URGENT CARE CENTER SERVICES (MARYLAND ONLY)
") UnitedHealthcare Community Plan Coverage Determination Guideline EMERGENCY HEALTH CARE SERVICES AND URGENT CARE CENTER SERVICES (MARYLAND ONLY) Guideline Number: CS038.J Effective Date: January 1, 2018
UnitedHealthcare Community Plan Coverage Determination Guideline EMERGENCY HEALTH CARE SERVICES AND URGENT CARE CENTER SERVICES (MARYLAND ONLY) Guideline Number: CS038.J Effective Date: January 1, 2018
9 TIPS FOR SURVIVING AFTER THE ICD-10 GRACE PERIOD ENDS. By Aine Cryts
 9 TIPS FOR SURVIVING AFTER THE ICD-10 GRACE PERIOD ENDS By Aine Cryts BE SPECIFIC IN YOUR CODING "Specificity in documentation and diagnosis coding since the ICD-10 implementation is to be encouraged.
9 TIPS FOR SURVIVING AFTER THE ICD-10 GRACE PERIOD ENDS By Aine Cryts BE SPECIFIC IN YOUR CODING "Specificity in documentation and diagnosis coding since the ICD-10 implementation is to be encouraged.
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
What To Do When An Audit Letter Comes
 What To Do When An Audit Letter Comes Sarah Reed BSE,CPC,CPC-I AAPC Fellow 2 The speaker has no financial relationship to any products or services referenced in this program. This program is intended to
What To Do When An Audit Letter Comes Sarah Reed BSE,CPC,CPC-I AAPC Fellow 2 The speaker has no financial relationship to any products or services referenced in this program. This program is intended to
Presentation Overview
 MISSING VITALS: IMPORTANT INFORMATION FOR UTILIZATION REVIEW 2011/2012 Presentation Overview Utilization Review HFS Requirements Vital Information for Review Clinical information necessary Completeness
MISSING VITALS: IMPORTANT INFORMATION FOR UTILIZATION REVIEW 2011/2012 Presentation Overview Utilization Review HFS Requirements Vital Information for Review Clinical information necessary Completeness