EMTALA. Federal Law and the Medical Staff. Shaheed Koury, MD, MBA, FACEP SVP & Chief Medical Officer Quorum Health
|
|
|
- Chastity Kelly
- 5 years ago
- Views:
Transcription

1 EMTALA Federal Law and the Medical Staff Shaheed Koury, MD, MBA, FACEP SVP & Chief Medical Officer Quorum Health
2 Objectives Review EMTALA Law Clarify Key Terms Define Hospital and Physician Responsibilities Address Special Circumstances and Challenges Discuss EMTALA Investigation and Violation Process Present Case Examples Questions 2
3 What is EMTALA? Emergency Medical Treatment and Labor Act: A Federal Law requiring Medicare participating hospitals to provide a Medical Screening Exam (MSE) and stabilizing treatment(s) for anyone that presents to the hospital s dedicated emergency department requesting medical examination or treatment, regardless of their ability to pay. 3
4 EMTALA History Enacted to prevent refusing the treatment of patients based on financial status (or other discriminatory reasons), sometimes referred to as patient dumping. EMTALA is not simply an anti-dumping law. EMTALA is a federally mandated standard of practice for hospitals and physicians. 4
5 What must the hospital provide? 1. An appropriate Medical Screening Exam (MSE) to anyone who comes to the emergency department and requests an exam or treatment. 2. Necessary stabilizing treatment to a person with an emergent medical condition (EMC), including an individual in labor, regardless of their ability to pay. 5
6 What must the hospital provide? 3. An appropriate transfer if: The individual requests the transfer, OR The hospital does not have the capability or capacity to provide the treatment necessary to stabilize the EMC, and/or have the capability or capacity to admit the individual for treatment, AND the benefits of the transfer outweigh the risk 6
7 Additional requirements 4. The treatment must be the same that would be provided to any patient arriving with those signs and symptoms. 5. Treatment decisions must be made in a nondiscriminatory manner regardless of diagnosis (e.g., labor, AIDS), financial status (e.g., uninsured, Medicaid), race, color, national origin (e.g. Hispanic or Native American surnames), and/or disability. 7
8 Hospital Property Main hospital campus Parking lot Sidewalk Driveway Hospital departments Definitions Any building owned by the hospital within 250 yards of the main building. 8
9 Definitions Comes to the Emergency Department An individual requests examination or treatment, OR A prudent layperson would believe that the individual needs emergency examination or treatment. 9
10 Definitions Medical Screening Exam A Medical Screening Exam (MSE) is an exam performed by a qualified medical practitioner, to determine the presence, or absence, of an emergent medical condition. This includes the presence, or absence, of labor. 10
11 Definitions Appropriate Screening An MSE is the process required to reach, with reasonable clinical confidence, the point at which it can be determined whether the individual has an Emergency Medical Condition or not. 11
12 Definitions Proper Screening An MSE is an ongoing process, not an isolated event. May be a brief history and physical examination, or can include ancillary studies and procedures. 12
13 Definitions Emergency Medical Condition (EMC) A medical condition manifesting itself by acute symptoms of sufficient severity (including severe pain) such that the absence of immediate medical attention could reasonably be expected to result in: Placing the health of the individual (or, with respect to a pregnant woman, the health of the woman or her unborn child) in serious jeopardy, Serious impairment to bodily functions, or Serious dysfunction of any bodily organ or part. 13
14 Definitions Emergency Medical Condition (EMC) With respect to a pregnant woman who is having contractions: There is inadequate time to effect a safe transfer to another hospital before delivery, or The transfer may pose a threat to the health or safety of the woman or her unborn child. 14
15 Medical Screening Examination Triage is not a Medical Screening Exam! Triage simply means to sort the patient based on acuity. Only a Registered Nurse can triage a patient. Only a Qualified Medical Provider can perform a MSE. 15
16 Medical Screening Examination Every patient is considered emergent until determined otherwise by a Medical Screening Exam performed by a QMP. 16
17 Medical Screening Examination You cannot delay the MSE to inquire about insurance or ability to pay for care. Even if it causes no delay, you cannot seek authorization from an insurer until the MSE is complete and stabilizing treatment is initiated. 17
18 The QMP has performed the Medical Screening Exam Does an EMC Exist? If No, the patient is determined to have a non-emergent condition. No further obligation under EMTALA. If Yes, or EMC is not ruled out, then must: STABILIZE, ADMIT, or TRANSFER* *Appropriate Transfer 18
19 Definitions Stabilized Emergency Medical Conditions: No material deterioration of the patient s condition is likely to result from discharge. Patients in Active Labor: The infant and the placenta have been delivered. Psychiatric Patients: Protected and prevented from injuring or harming him/herself or others. 19
20 Stabilizing Treatment Asthma Management Bronchospasm resolved Psychiatric Patient No longer a danger to self or others Broken Bone Pain managed, fracture splinted Woman in Labor Delivery of child and placenta 20
21 Stabilized If a patient comes to the Hospital and is determined to have an EMC following a MSE, the Hospital must provide further medical examination and treatment, including hospitalization if necessary, as required to stabilize the EMC within the capabilities of the staff and facilities available at the Hospital, including on-call physicians. 21
22 Within The Capabilities The hospital resources and staff available to inpatients All resources available in the emergency department. the capability of its emergency department includes the services of its on-call physicians. The capability of the hospital includes that of the hospital as a whole 22
23 When a Transfer Occurs: The hospital does not have the capacity or capability to provide the treatment needed to stabilize the patient for a discharge disposition, and the benefits of the transfer outweigh the risk, Patient request OR 23
24 Stabilized Discharge versus Transfer Confusing Terminology! Stabilized for Discharge: No material deterioration of the patient s condition is likely to result. Stabilized for Transfer: Benefits of transfer outweigh risks of transfer. SO. Unstable then means: Unstable for Discharge: Material deterioration of the patient s condition is likely to result. Unstable for Transfer: Risks of transfer outweigh the benefits of transfer. 24
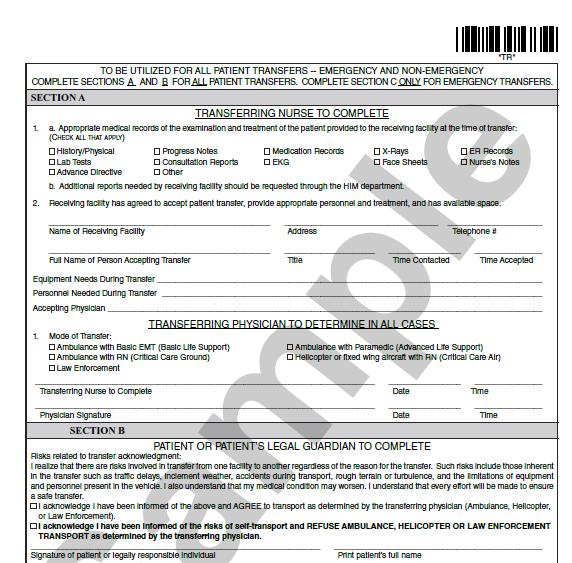
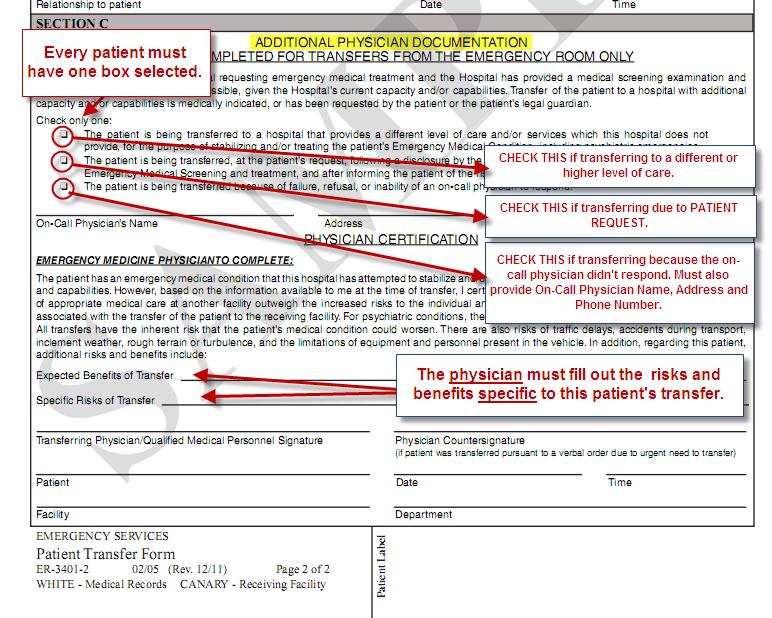
25 Steps to ensuring an Appropriate Transfer 1. Provide stabilizing treatment to the extent possible given the hospital s current capacity and capability. 2. Obtain an accepting hospital with the capability and capacity to treat the patient. 3. Completion of the EMTALA Transfer Form. 4. Send copies of the medical records/chart. 5. If the on call physician refused to respond need to list their name and address on the form. 25
26 Related to Private Vehicles: REMEMBER, when transferring a patient, the sending hospital is ultimately responsible for ensuring that the transfer is effected appropriately. There is no way to ensure that a patient will arrive at the intended destination when transported by private vehicle. Ask yourself: What is the best way to ensure that the patient arrives at the receiving hospital? 26
27 A Note about Private Vehicles: When transferring a patient, the sending hospital is ultimately responsible for ensuring that the transfer is effected appropriately. There is no way to ensure that a patient will arrive at the intended destination when transported by private vehicle. CMS does not consider private vehicle an appropriate mode of transportation for an EMTALA transfer. Patients can make their own decision including deciding to self-transport (unless special circumstance such as involuntary psychiatric admission). The appropriate box is checked under section B and the patient disposition is transfer.

28 Example: Standard Transfer Form NOTE: PRIVATE VEHICLE not considered Appropriate Mode of Transfer and therefore not an option to select. 28
29 29 NEW 29
30 30
31 Note about Non-EMTALA Transfers Applies to areas other than the ED, such as the inpatient unit (EMTALA obligation ceases on good faith inpatient admission). ED Transfers are treated as EMTALA Transfers. 31
32 On-Call Coverage Obligations The hospital is responsible for maintaining an on-call list in a manner that best meets the needs of its patients in accordance with the resources available to the hospital. The hospital must have written policies and procedures to respond to situations where a particular specialty is not available; where a hospital permits on-call physicians to provide simultaneous call; where a hospital permits physicians to schedule elective surgery during call. 32
33 On-Call Coverage Obligations Each Hospital must establish a process for identifying those physicians on-call for a given specialty. On-call physicians, after being called, must respond to the Dedicated Emergency Department as specified in the Hospital s Medical Staff Bylaws. 33
34 On-Call Coverage Obligations The Hospital must document on the transfer form the name and address of any on-call physician who has refused or failed to appear within a reasonable time to provide necessary stabilizing treatment, and must report such information to Hospital administration as soon as possible. 34
35 Does a hospital violate EMTALA if a patient refuses treatment? No, an individual may refuse to consent to examination and treatment, but only after the hospital offers to provide further medical examination and treatment and informs the individual of the risks and benefits of refusing examination and treatment. The hospital MUST take all reasonable steps to secure the individual s written consent to refusal of further medical examination and treatment. 35
36 Notice and Record Keeping Hospitals are required to maintain all records related to persons transferred for a minimum of 5 years. Maintain the list of on-call physicians. Maintain a central log on each patient who comes to the DED to track the care provided. 36
37 Recipient hospital responsibilities: A hospital is required to report to CMS or the State survey agency within 72 hours of the occurrence when it suspects it may have received an improperly transferred individual. Failure to report improper transfers may subject the receiving hospital to termination of its provider agreement. 37
38 Recipient hospital responsibilities: A hospital that has specialized capabilities or facilities (including, but not limited to, facilities such as burn units, shock trauma units, neonatal intensive case units, or, with respect to rural areas, regional referral centers) may not refuse to accept from a referring hospital an appropriate transfer if the receiving hospital has the capacity to treat the individual. 38
39 The patient s visit to the ED should contain the following to meet CMS expectations: 1. Central log entry with disposition 2. Triage record 3. On-going vitals recorded 4. Oral history 5. Physical exam of affected systems 6. Physical exam of potentially affected systems and known chronic conditions 7. Any testing necessary to rule out the presence of a legally defined Emergency Medical Condition 8. Use of on-call personnel PRN to complete above 9. Use of on-call physician PRN to diagnose and stabilize patient 10. Resolution of abnormal findings or test results by normalization (serial values) or explanation of why they are not significant to the presentation 11. Discharge/transfer vitals 12. Adequate documentation of all above 39
40 Who is the Enforcer? CMS Sanctions include: Termination of hospital s provider agreement. Civil money penalties ($50,000 if over 100 beds, $25,000 if less than 100 beds) against both hospital and physician. Exclusion of physician. Malpractice suit. Physicians are not covered under their Malpractice insurance for a violation of EMTALA. 40
41 Suspected Violation? What to do? Contact your direct supervisor, and follow normal event reporting protocol. Administration, in conjunction with corporate, will development a corrective action plan and complete a root cause analysis. 41
42 Example: A Texas hospital paid a $20,000 fine after a patient left the ED without getting a medical screening exam ( MSE ) because a desk clerk recommended he go to his family physician. Takeaway: no matter how small an injury appears, all patients seeking emergency care must get an appropriate MSE. 42
43 Example: In Texas, a suicidal patient presented with underlying hypotension. The hospital treated the psychiatric condition and transferred the patient to a specialty hospital, but they failed to fully treat the hypotension. The hospital paid $20,000. Takeaway: when a patient has multiple conditions, the hospital must stabilize each one within its capability. 43
44 OIG Example: An on-call surgeon at a large academic medical center in Tennessee (AMC) refused to accept a patient. The patient was transferred to another facility and died. The AMC agreed to pay $45,000, and the physician was personally fined $35,000. Takeaway: make sure physicians know they must accept patients if the facility has the capacity and capability to treat them. 44
45 On-Call Scenario On-call physician asked to come in to see an ED patient, responds with instructions to admit or to run various testing and that the on-call physician will see the patient at a later time. EMTALA requires prompt response within a "reasonable" time to be specified by the bylaws. These times are not extended by necessary or prudent testing or by admission. Delays will lead to violations for failure to promptly evaluate or stabilize the patient. 45
46 On-Call Scenario On-call physician asked to come in to see an ED patient, debates with ED physician over the necessity of coming in. Once the request is made to come in, the duty attaches. In addition, EMTALA places the decision power with the physician with eyes on the patient. Response is not negotiable or debatable. 46
47 EMTALA Q/A When covering more than one hospital on-call, asking a patient be sent to the hospital where the on-call physician is currently seeing patients instead of going to the patient s location. EMTALA requires all care to be rendered in the hospital where the patient presents. The only circumstances where the request to transfer would be valid would be if the needs of the patient could not be met in timely fashion where the patient presented, and the requested transfer would allow more timely intervention for patient safety and response of the on-call physician was not possible (i.e. currently involved in surgery). Thorough documentation would be important. 47
48 Interpretive Guidelines Who Must Take Call? CMS will consider all relevant factors, including the number of physicians on staff, other demands on these physicians, the frequency with which the hospital s patients typically require services of on-call physicians, and the provisions made for situations in which a physician specialty is not available. 48

49 Simultaneously On-Call On-call docs can be oncall at more than one institution. Must be a plan for when the on-call physician is not available. 49
50 Interpretive Guidelines The best practice for hospitals, which offer particular services to the public, should be available through on-call coverage of the ED. CMS Phone Contact: Any specialty with a significant presence on a medical staff, offering services to the community, available for inpatient care, will be represented on the on-call schedule. 50
51 EMTALA Q/A When asked to come in to see an E.D. patient, declining on the basis that the patient was previously discharged from the physician s practice for non-compliance, prior litigation, or non-payment. While the patient has the right to decline the on-call physician, the on-call physician does not have the right under EMTALA to decline the patient. He/she may arrange for someone else to present in his/her stead. 51
52 Transfer Acceptance Scenario #1 ER attending physician receives a call from a small rural hospital wanting to transport a 50 yo male with chest pain to your facility. The rural hospital has done an EKG and performed blood work. ER attending denies the transport suggesting that the patient be admitted to the rural hospital for observation. Rural hospital does not have a cardiologist on staff. Is this an EMTALA violation? 52
53 Transfer Acceptance Scenario #1 EMTALA Violation : YES The transferring hospital determines that the patient requires further examination and treatment in order to stabilize the emergency medical condition A hospital with specialized capabilities may not refuse to accept an appropriate transfer if patient requires specialized capabilities and there is capacity and capability. 53
54 Transfer Acceptance Scenario #2 45 yo male with a subdural hematoma from a fall. ED physician calls the regional trauma center to transfer. Resident from trauma facility refuses the transfer even though hospital has NS coverage. Is this an EMTALA violation? 54
55 Transfer Acceptance Scenario #2 EMTALA Violation : YES The transferring physician determines that the patient requires further examination and treatment in order to stabilize the emergency medical condition. A hospital with specialized capabilities may not refuse to accept an appropriate transfer if patient requires specialized capabilities and there is capacity and capability. 55
56 Transfer Acceptance Scenario #3 35 yo female with ovarian torsion. Local facility does not have GYN services. ED physician called the referral hospital which refused to accept the patient since they did not participate in her insurance. Advised to call other facilities which delayed ultimate care. Is this an EMTALA violation? 56
57 Transfer Acceptance Scenario #3 EMTALA Violation : YES A hospital with specialized capabilities may not refuse to accept an appropriate transfer if patient requires specialized capabilities and there is capacity and capability. Cannot inquire about financial status. 57
58 Transfer Acceptance Scenario #4 85 yo male presents with a ruptured AAA. Local hospital has no general or vascular surgery backup. Patient is unstable with hypotension and tachycardia. ED physician speaks to CV surgeon at referral hospital. Surgeon states patient is too ill and unstable for transfer and refuses transfer. Patient expires 8 hours later after multiple attempts to transfer fail. Is this an EMTALA violation? 58
59 Transfer Acceptance Scenario #4 EMTALA Violation : YES When a hospital has exhausted all of its capabilities in attempting to resolve the EMC, it must effect an appropriate transfer of the individual (see Tag A-2409/C-2409). If an individual s EMC has not been stabilized, prior to transferring the individual to another hospital, the sending hospital is required under EMTALA to pursue a transfer because either: the individual requests the transfer; or the expected benefits of the transfer outweigh the increased risks of the transfer. 59
60 Frequent ED patient example A frequent Flyer patient was seen, treated and discharged from the ED. Patient returned to the same ED within minutes of discharge with different complaints and threats of self-harm, asking to be seen. The same ED doctor who was still on duty refused to see the patient and went to lobby and told the patient to leave. Patient went to the parking lot and called 911 and reported intent to kill himself, had a knife in his hand when police arrived. Police returned patient to ED registration and asked for a psychiatric/medical evaluation and treatment on patient s behalf. Doctor again came to lobby and told police she had seen this patient earlier, and refused to see the patient again. Police took patient to another ED in the same city and filed EMTALA complaint with the state department of health. 60
61 EMTALA Example (Medical Screening) Patient #1 stated she presented at the hospital ED on 11/07/16 and asked if there was a doctor who specialized in kidney failure. Patient #1 stated she was told to go next door to see a doctor as a walk-in as the ED is only for emergencies. 61
62 References 1. Centers for Medicare and Medicaid (2005), Social Security Act Section 1867 (42 USC 1395dd), Regulations: 42 CFR State Operations Manual,(Rev. 60, ) : Appendix V Interpretive Guidelines Responsibilities of Medicare Participating Hospitals in Emergency Cases Guidance/Guidance/Manuals/Downloads/som107ap_v_ emerg.pdf 62

 371-7979")
63 Contact Us Shaheed Koury, MD, MBA, FACEP Senior Vice President & Chief Medical Officer (615) (615)
EMTALA Emergency Medical Treatment and Active Labor Act
 EMTALA Emergency Medical Treatment and Active Labor Act William F. Jourdain EMTALA BASICS! Federal law enacted in 1986! Where a person comes to the dedicated emergency department (DED) or hospital property
EMTALA Emergency Medical Treatment and Active Labor Act William F. Jourdain EMTALA BASICS! Federal law enacted in 1986! Where a person comes to the dedicated emergency department (DED) or hospital property
Pali Lipoma-Director, Corporate Compliance September 2017
 Pali Lipoma-Director, Corporate Compliance September 2017 Review the intent of the Emergency Medical Treatment and Labor Act (EMTALA). Review key definitions used for EMTALA compliance. Review requirements
Pali Lipoma-Director, Corporate Compliance September 2017 Review the intent of the Emergency Medical Treatment and Labor Act (EMTALA). Review key definitions used for EMTALA compliance. Review requirements
Emergency Medical Treatment and Active Labor Act. Deirdre Newton Senior Counsel NYC Health + Hospitals Office of Legal Affairs
 Emergency Medical Treatment and Active Labor Act Deirdre Newton Senior Counsel NYC Health + Hospitals Office of Legal Affairs What is EMTALA? The Emergency Medical Treatment and Active Labor Act is a 1986
Emergency Medical Treatment and Active Labor Act Deirdre Newton Senior Counsel NYC Health + Hospitals Office of Legal Affairs What is EMTALA? The Emergency Medical Treatment and Active Labor Act is a 1986
Slide 1 DN1. Emergency Medical Treatment and Active Labor Act Deirdre Newton, 8/24/2012
 DN1 Slide 1 DN1 Emergency Medical Treatment and Active Labor Act Deirdre Newton, 8/24/2012 Costs associated with health insurance plans and the increased numbers of uninsured or underinsured persons seeking
DN1 Slide 1 DN1 Emergency Medical Treatment and Active Labor Act Deirdre Newton, 8/24/2012 Costs associated with health insurance plans and the increased numbers of uninsured or underinsured persons seeking
EMTALA TRAINING. Emergency Medical Treatment and Labor Act
 EMTALA TRAINING Emergency Medical Treatment and Labor Act Sometimes called: Anti-Dumping Law or COBRA August 2014 Overview of EMTALA The purpose of EMTALA is to prevent "'patient dumping, the practice
EMTALA TRAINING Emergency Medical Treatment and Labor Act Sometimes called: Anti-Dumping Law or COBRA August 2014 Overview of EMTALA The purpose of EMTALA is to prevent "'patient dumping, the practice
EMTALA. Mark Reiter MD MBA FAAEM
 EMTALA Mark Reiter MD MBA FAAEM Residency Director, U. Tennessee Murfreesboro/Nashville Past President, American Academy of Emergency Medicine CEO, Emergency Excellence Objective To educate on EMTALA using
EMTALA Mark Reiter MD MBA FAAEM Residency Director, U. Tennessee Murfreesboro/Nashville Past President, American Academy of Emergency Medicine CEO, Emergency Excellence Objective To educate on EMTALA using
What is EMTALA? Emergency Medical Treatment & Active Labor Act. Federally-mandated requirement [42 CFR ]. Known as the Anti-Dumping Law.
![What is EMTALA? Emergency Medical Treatment & Active Labor Act. Federally-mandated requirement [42 CFR ]. Known as the Anti-Dumping Law.](/thumbs/82/84983217.jpg "What is EMTALA? Emergency Medical Treatment & Active Labor Act. Federally-mandated requirement [42 CFR ]. Known as the Anti-Dumping Law.") Emergency Medical Treatment t and Active Labor Act (EMTALA) What Physicians Need to Know January 2017 What is EMTALA? Emergency Medical Treatment & Active Labor Act. Federally-mandated requirement [42
Emergency Medical Treatment t and Active Labor Act (EMTALA) What Physicians Need to Know January 2017 What is EMTALA? Emergency Medical Treatment & Active Labor Act. Federally-mandated requirement [42
EMTALA. Santa Rosa Memorial Hospital Medical Staff May 9, 2017
 EMTALA Santa Rosa Memorial Hospital Medical Staff May 9, 2017 Reflection "Your success in life isn't based on your ability to simply change. It is based on your ability to change faster than your competition,
EMTALA Santa Rosa Memorial Hospital Medical Staff May 9, 2017 Reflection "Your success in life isn't based on your ability to simply change. It is based on your ability to change faster than your competition,
Learning Objectives. The EMTALA Framework. EMTALA Update: Challenges in Community and Specialty Hospitals. Originally known as Anti-Dumping Law
 EMTALA Update: Challenges in Community and Specialty Hospitals Presented by Jan Corcoran, RN, BS, CEN Divisional Director of Clinical Services Learning Objectives 1) Describe the definition and history
EMTALA Update: Challenges in Community and Specialty Hospitals Presented by Jan Corcoran, RN, BS, CEN Divisional Director of Clinical Services Learning Objectives 1) Describe the definition and history
A Review of Current EMTALA and Florida Law
 A Review of Current EMTALA and Florida Law South Carolina Hospital Fined $1.28 Million for EMTALA violations Doctor fined $40,000 for not showing up at Emergency Room Chicago Hospital and Docs settle EMTALA
A Review of Current EMTALA and Florida Law South Carolina Hospital Fined $1.28 Million for EMTALA violations Doctor fined $40,000 for not showing up at Emergency Room Chicago Hospital and Docs settle EMTALA
EMERGENCY ROOM TREATMENT
 SCOPE Individuals requiring Emergency Services at University Medical Center New Orleans. PURPOSE To provide emergency medical treatment to individuals in compliance with section 1921 of The Consolidated
SCOPE Individuals requiring Emergency Services at University Medical Center New Orleans. PURPOSE To provide emergency medical treatment to individuals in compliance with section 1921 of The Consolidated
Revised and Amended Statement of Gina G. Greenwood, J.D. 1 Baker Donelson Bearman Caldwell and Berkowitz, PC 2
 Revised and Amended Statement of Gina G. Greenwood, J.D. 1 Baker Donelson Bearman Caldwell and Berkowitz, PC 2 This Statement is provided to the United States Commission on Civil Rights regarding the Emergency
Revised and Amended Statement of Gina G. Greenwood, J.D. 1 Baker Donelson Bearman Caldwell and Berkowitz, PC 2 This Statement is provided to the United States Commission on Civil Rights regarding the Emergency
EMTALA: SCREENING, STABILIZATION AND TRANSFER
 PAGE: 1 of 21 TABLE OF CONTENTS Section Page Numbers 1. Purpose 2 2. Scope 2 3. Definitions 2-4 4. Policy 4-5 5. Procedures 5-20 Cross References; Owner; References; Prior Version Dates 20 Appendices Appendix
PAGE: 1 of 21 TABLE OF CONTENTS Section Page Numbers 1. Purpose 2 2. Scope 2 3. Definitions 2-4 4. Policy 4-5 5. Procedures 5-20 Cross References; Owner; References; Prior Version Dates 20 Appendices Appendix
HealthStream Regulatory Script
 HealthStream Regulatory Script [EMTALA] Version: [May 2005] Lesson 1: Introduction Lesson 2: History and Enforcement Lesson 3: Medical Screening Lesson 4: Stabilizing Care Lesson 5: Appropriate Transfer
HealthStream Regulatory Script [EMTALA] Version: [May 2005] Lesson 1: Introduction Lesson 2: History and Enforcement Lesson 3: Medical Screening Lesson 4: Stabilizing Care Lesson 5: Appropriate Transfer
Primer: Overview of the Emergency Medical Treatment and Active Labor Act (EMTALA) Overview:
 Overview:") Primer: Overview of the Emergency Medical Treatment and Active Labor Act (EMTALA) Overview: In 1986, Congress enacted EMTALA as part of the Consolidated Omnibus Budget Reconciliation Act (COBRA). Often
Primer: Overview of the Emergency Medical Treatment and Active Labor Act (EMTALA) Overview: In 1986, Congress enacted EMTALA as part of the Consolidated Omnibus Budget Reconciliation Act (COBRA). Often
EMTALA: Transfer Policy, RI.034
 Current Status: Active PolicyStat ID: 1666780 POLICY: Origination: 12/2011 Last Approved: 01/2012 Last Revised: 12/2011 Next Review: 12/2013 Owner: Policy Area: References: Applicability: Lisa O'Connor:
Current Status: Active PolicyStat ID: 1666780 POLICY: Origination: 12/2011 Last Approved: 01/2012 Last Revised: 12/2011 Next Review: 12/2013 Owner: Policy Area: References: Applicability: Lisa O'Connor:
EL PASO COUNTY HOSPITAL POLICY: P-2 DISTRICT POLICY EFFECTIVE DATE: 02/05 LAST REVIEW DATE: 03/17
 POLICY The policy of the El Paso County Hospital District (EPCHD) is to provide services in compliance with applicable federal and state laws, rules and regulations regarding the appropriate medical screening
POLICY The policy of the El Paso County Hospital District (EPCHD) is to provide services in compliance with applicable federal and state laws, rules and regulations regarding the appropriate medical screening
SACRED HEART HEALTHCARE SYSTEM SACRED HEART HOSPITAL 421 CHEW STREET ALLENTOWN, PA GENERAL POLICY AND PROCEDURE MANUAL
 SACRED HEART HEALTHCARE SYSTEM SACRED HEART HOSPITAL 421 CHEW STREET ALLENTOWN, PA 18102-3490 GENERAL POLICY AND PROCEDURE MANUAL Subject: On- Call Physician Policy Policy Number: GEN_693 Approval: Initial
SACRED HEART HEALTHCARE SYSTEM SACRED HEART HOSPITAL 421 CHEW STREET ALLENTOWN, PA 18102-3490 GENERAL POLICY AND PROCEDURE MANUAL Subject: On- Call Physician Policy Policy Number: GEN_693 Approval: Initial
DEACONESS HOSPITAL, INC Evansville, Indiana
 DEACONESS HOSPITAL, INC Evansville, Indiana Policy and Procedure No. 40-06 Revised Date: February 10, 2014 Reviewed Date: February 10, 2014 EMERGENCY MEDICAL TRANSFER AND ACTIVE LABOR (EMTALA) GUIDELINES
DEACONESS HOSPITAL, INC Evansville, Indiana Policy and Procedure No. 40-06 Revised Date: February 10, 2014 Reviewed Date: February 10, 2014 EMERGENCY MEDICAL TRANSFER AND ACTIVE LABOR (EMTALA) GUIDELINES
Cheri Benander, MSN, RN, CHC, NHCE-C Director of Compliance Consulting Services, HealthTechS3
 December 2016 COMPLIANCE NEWSLETTER Cheri Benander, MSN, RN, CHC, NHCE-C Director of Compliance Consulting Services, HealthTechS3 NAVIGATING THE MAZE Cheri Benander, MSN, RN, CHC, NHCE-C Director of Compliance
December 2016 COMPLIANCE NEWSLETTER Cheri Benander, MSN, RN, CHC, NHCE-C Director of Compliance Consulting Services, HealthTechS3 NAVIGATING THE MAZE Cheri Benander, MSN, RN, CHC, NHCE-C Director of Compliance
The Emergency Medical Treatment and Labor Act (EMTALA)
") The Emergency Medical Treatment and Labor Act (EMTALA) Presentation to the 2016 Nurse Leaders in Native Care Conference Mary Ellen Palowitch MHA,RN Division of Acute Services Survey & Certification Group
The Emergency Medical Treatment and Labor Act (EMTALA) Presentation to the 2016 Nurse Leaders in Native Care Conference Mary Ellen Palowitch MHA,RN Division of Acute Services Survey & Certification Group
SYSTEM POLICY EMERGENCY MEDICAL TREATMENT AND ACTIVE LABOR ACT ( EMTALA )
") BAPTIST HEALTHCARE SYSTEM CATEGORY EFFECTIVE DATE 11-10-03 REVISED 10-29-09 INDEX PAGE Pages SYSTEM POLICY SUBJECT: SCOPE: EMERGENCY MEDICAL TREATMENT AND ACTIVE LABOR ACT ( EMTALA ) All Baptist Healthcare
BAPTIST HEALTHCARE SYSTEM CATEGORY EFFECTIVE DATE 11-10-03 REVISED 10-29-09 INDEX PAGE Pages SYSTEM POLICY SUBJECT: SCOPE: EMERGENCY MEDICAL TREATMENT AND ACTIVE LABOR ACT ( EMTALA ) All Baptist Healthcare
EMTALA: Taking the high road BRANDON LEWIS, DO, MBA, FACOEP, FACEP
 EMTALA: Taking the high road BRANDON LEWIS, DO, MBA, FACOEP, FACEP Objectives Provide a better understanding of the background and definitions of EMTALA Provide a better understanding of how these regulations
EMTALA: Taking the high road BRANDON LEWIS, DO, MBA, FACOEP, FACEP Objectives Provide a better understanding of the background and definitions of EMTALA Provide a better understanding of how these regulations
CASEY COUNTY HOSPITAL EMERGENCY MEDICAL TREATMENT AND ACTIVE LABOR ACT ( EMTALA )
") CASEY COUNTY HOSPITAL EMERGENCY MEDICAL TREATMENT AND ACTIVE LABOR ACT ( EMTALA ) SCOPE: This Policy and Procedure applies to the hospital and rural health clinics including Casey County Primary Care and
CASEY COUNTY HOSPITAL EMERGENCY MEDICAL TREATMENT AND ACTIVE LABOR ACT ( EMTALA ) SCOPE: This Policy and Procedure applies to the hospital and rural health clinics including Casey County Primary Care and
EMERGENCY HEALTH CARE SERVICES AND URGENT CARE CENTER SERVICES (MARYLAND ONLY)
") UnitedHealthcare Community Plan Coverage Determination Guideline EMERGENCY HEALTH CARE SERVICES AND URGENT CARE CENTER SERVICES (MARYLAND ONLY) Guideline Number: CS038.J Effective Date: January 1, 2018
UnitedHealthcare Community Plan Coverage Determination Guideline EMERGENCY HEALTH CARE SERVICES AND URGENT CARE CENTER SERVICES (MARYLAND ONLY) Guideline Number: CS038.J Effective Date: January 1, 2018
EMERGENCY HEALTH CARE SERVICES AND URGENT CARE CENTER SERVICES
 UnitedHealthcare Commercial Coverage Determination Guideline EMERGENCY HEALTH CARE SERVICES AND URGENT CARE CENTER SERVICES Guideline Number: CDG.010.11 Effective Date: January 1, 2018 Table of Contents
UnitedHealthcare Commercial Coverage Determination Guideline EMERGENCY HEALTH CARE SERVICES AND URGENT CARE CENTER SERVICES Guideline Number: CDG.010.11 Effective Date: January 1, 2018 Table of Contents
Current Status: Pending PolicyStat ID:
 Current Status: Pending PolicyStat ID: 2196545 Origination: Last Review: Effective: Expiration: Author: This policy reflects guidance under the Emergency Medical Treatment and Labor Act ("EMTALA") and
Current Status: Pending PolicyStat ID: 2196545 Origination: Last Review: Effective: Expiration: Author: This policy reflects guidance under the Emergency Medical Treatment and Labor Act ("EMTALA") and
State Operations Manual Appendix V Interpretive Guidelines Responsibilities of Medicare Participating Hospitals in Emergency Cases
 State Operations Manual Appendix V Interpretive Guidelines Responsibilities of Medicare Participating Hospitals in Emergency Cases (Rev. 60, 07-16-10) Transmittals for Appendix V Part I- Investigative
State Operations Manual Appendix V Interpretive Guidelines Responsibilities of Medicare Participating Hospitals in Emergency Cases (Rev. 60, 07-16-10) Transmittals for Appendix V Part I- Investigative
Emergency Medical Treatment and Active Labor Act ( EMTALA )
") Emergency Medical Treatment and Active Labor Act ( EMTALA ) Kim C. Stanger Compliance Bootcamp (2-18) This presentation is similar to any other legal education materials designed to provide general information
Emergency Medical Treatment and Active Labor Act ( EMTALA ) Kim C. Stanger Compliance Bootcamp (2-18) This presentation is similar to any other legal education materials designed to provide general information
EMERGENCY HEALTH SERVICES AND URGENT CARE CENTER SERVICES
 EMERGENCY HEALTH SERVICES AND URGENT CARE CENTER SERVICES UnitedHealthcare Commercial Coverage Determination Guideline Guideline Number: CDG.010.08 Effective Date: January 1, 2017 Table of Contents Page
EMERGENCY HEALTH SERVICES AND URGENT CARE CENTER SERVICES UnitedHealthcare Commercial Coverage Determination Guideline Guideline Number: CDG.010.08 Effective Date: January 1, 2017 Table of Contents Page
AHLA. C. Great Expectations: CMS Enforcement of EMTALA. Jesse Neil Senior Operations Counsel Community Health Systems Franklin, TN
 AHLA C. Great Expectations: CMS Enforcement of EMTALA Jesse Neil Senior Operations Counsel Community Health Systems Franklin, TN Sandra J. Sands Senior Counsel US Department of Health and Human Services
AHLA C. Great Expectations: CMS Enforcement of EMTALA Jesse Neil Senior Operations Counsel Community Health Systems Franklin, TN Sandra J. Sands Senior Counsel US Department of Health and Human Services
CMS Will Show No Mercy:
 CMS Will Show No Mercy: Ensuring EMTALA Compliance for Psychiatric Patients in the ED Presentation for Missouri Hospital Association Gregg J. Lepper Greensfelder, Hemker & Gale, P.C. September 14, 2017
CMS Will Show No Mercy: Ensuring EMTALA Compliance for Psychiatric Patients in the ED Presentation for Missouri Hospital Association Gregg J. Lepper Greensfelder, Hemker & Gale, P.C. September 14, 2017
State Operations Manual. Appendix V Interpretive Guidelines Responsibilities of Medicare Participating Hospitals In Emergency Cases
 State Operations Manual Appendix V Interpretive Guidelines Responsibilities of Medicare Participating Hospitals In Emergency Cases PART I- Investigative Procedures I. General Information II. Principal
State Operations Manual Appendix V Interpretive Guidelines Responsibilities of Medicare Participating Hospitals In Emergency Cases PART I- Investigative Procedures I. General Information II. Principal
EMTALA and Behavioral Health. Catherine Greaves
 EMTALA and Behavioral Health Catherine Greaves Need for EMTALA As individuals moved from tradition indemnity coverage to managed case plans, hospitals were forced to absorb cost of emergency care. ERs
EMTALA and Behavioral Health Catherine Greaves Need for EMTALA As individuals moved from tradition indemnity coverage to managed case plans, hospitals were forced to absorb cost of emergency care. ERs
EMTALA (The Emergency Medical Treatment and Active Labor Act: Screening, Stabilization, and Transfer of Individuals with Emergency Medical Conditions)
") EMTALA (The Emergency Medical Treatment and Active Labor Act: Screening, Stabilization, and Transfer of Individuals with Emergency Medical Conditions) Type: TIER # 1 Original Effective Date: 11/2001 Current
EMTALA (The Emergency Medical Treatment and Active Labor Act: Screening, Stabilization, and Transfer of Individuals with Emergency Medical Conditions) Type: TIER # 1 Original Effective Date: 11/2001 Current
EMERGENCY HEALTH CARE SERVICES AND URGENT CARE CENTER SERVICES
 UnitedHealthcare of California (HMO) UnitedHealthcare Benefits Plan of California (IEX EPO, IEX PPO) UnitedHealthcare of Oklahoma, Inc. UnitedHealthcare of Oregon, Inc. UnitedHealthcare Benefits of Texas,
UnitedHealthcare of California (HMO) UnitedHealthcare Benefits Plan of California (IEX EPO, IEX PPO) UnitedHealthcare of Oklahoma, Inc. UnitedHealthcare of Oregon, Inc. UnitedHealthcare Benefits of Texas,
All UW Medicine hospitals and provider-based urgent care centers qualifying as Dedicated Emergency Departments (DED), as defined in this policy.
, as defined in this policy.") Applicability: Policy Title: Policy Number: Entity Policies: UW Medicine hospitals Application of and Compliance with the Emergency Medical Treatment and Labor Act (EMTALA) COMP.301 Harborview Medical
Applicability: Policy Title: Policy Number: Entity Policies: UW Medicine hospitals Application of and Compliance with the Emergency Medical Treatment and Labor Act (EMTALA) COMP.301 Harborview Medical
Current Status: Pending PolicyStat ID: LL.EM.001.EMTALA Definitions
 Current Status: Pending PolicyStat ID: 2196568 SCOPE: Origination: Last Review: Effective: Expiration: Author: AdministrationHospital-Based Entities N/A N/A N/A 3 years after approval Quincey Garcia: Medial
Current Status: Pending PolicyStat ID: 2196568 SCOPE: Origination: Last Review: Effective: Expiration: Author: AdministrationHospital-Based Entities N/A N/A N/A 3 years after approval Quincey Garcia: Medial
2016 EMTALA UPDATE: A Practical Look at the Impact of EMTALA
 2016 EMTALA UPDATE: A Practical Look at the Impact of EMTALA Gregg Lepper, J.D. Greensfelder, Hemker & Gale, P.C. St. Louis Provided by MHA Center for Education 1 Overview of the Day Morning EMTALA Overview.
2016 EMTALA UPDATE: A Practical Look at the Impact of EMTALA Gregg Lepper, J.D. Greensfelder, Hemker & Gale, P.C. St. Louis Provided by MHA Center for Education 1 Overview of the Day Morning EMTALA Overview.
WHO YOU GONNA CALL? PHYSICIAN CALL COVERAGE OBLIGATIONS UNDER WYOMING AND FEDERAL LAW. By Nick Healey Dray, Dyekman, Reed & Healey, P.C.
 WHO YOU GONNA CALL? PHYSICIAN CALL COVERAGE OBLIGATIONS UNDER WYOMING AND FEDERAL LAW By Nick Healey Dray, Dyekman, Reed & Healey, P.C. Wyoming physicians have for many years regarded call coverage as
WHO YOU GONNA CALL? PHYSICIAN CALL COVERAGE OBLIGATIONS UNDER WYOMING AND FEDERAL LAW By Nick Healey Dray, Dyekman, Reed & Healey, P.C. Wyoming physicians have for many years regarded call coverage as
TODAY S WEBINAR Ebola and the Law: What Hospitals Can Do Now to Prepare
 TODAY S WEBINAR Ebola and the Law: What Hospitals Can Do Now to Prepare Joe Geraci 512.703.5774 Stephen Cockerham 214.999.6167 Lisa Luetkemeyer 314.345.6248 Edward Barker 816.983.8356 Agenda Lessons Learned
TODAY S WEBINAR Ebola and the Law: What Hospitals Can Do Now to Prepare Joe Geraci 512.703.5774 Stephen Cockerham 214.999.6167 Lisa Luetkemeyer 314.345.6248 Edward Barker 816.983.8356 Agenda Lessons Learned
PRACTICE RESOURCE EMTALA
 Journal of Health Law Summer Volume 38, No. 3 Articles PRACTICE RESOURCE EMTALA Compliance Andrea M. Kahn-Kothmann Paige Kesman PRACTICE RESOURCE EMTALA Compliance Andrea M. Kahn-Kothmann Paige Kesman*
Journal of Health Law Summer Volume 38, No. 3 Articles PRACTICE RESOURCE EMTALA Compliance Andrea M. Kahn-Kothmann Paige Kesman PRACTICE RESOURCE EMTALA Compliance Andrea M. Kahn-Kothmann Paige Kesman*
We Get Letters May 2004 Number 11
 We Get Letters May 2004 Number 11 Sharing office space Psychiatric medication management EMTALA changes To reach MIEC This newsletter is written in response to numerous questions the Loss Prevention Department
We Get Letters May 2004 Number 11 Sharing office space Psychiatric medication management EMTALA changes To reach MIEC This newsletter is written in response to numerous questions the Loss Prevention Department
Key EMTALA Concepts for ED Staff
 Key EMTALA Concepts for ED Staff Background In the early 1980s, some emergency departments were refusing medical care to uninsured patients. Essentially, unstable patients were being turned away either
Key EMTALA Concepts for ED Staff Background In the early 1980s, some emergency departments were refusing medical care to uninsured patients. Essentially, unstable patients were being turned away either
Resident/Fellow Training Orientation Policies
 Resident/Fellow Training Orientation Policies Restraint or Seclusion: Violent Behavior Prevention and Reporting of Patient Abuse Blood Component Indications & Critical Tests HIPAA Privacy and Security
Resident/Fellow Training Orientation Policies Restraint or Seclusion: Violent Behavior Prevention and Reporting of Patient Abuse Blood Component Indications & Critical Tests HIPAA Privacy and Security
PAT Quality Through Compliance. Policies and Procedures. HAWAII HEALTH SYSTEMS C O R P O R A T I O N Touching Lives Everyday" N/A
 HAWAII HEALTH SYSTEMS C O R P O R A T I O N Touching Lives Everyday" Policies and Procedures Subject: Emergency Care, Transfers (COBRA) Quality Through Compliance Issued by: Corporate Compliance Committee
HAWAII HEALTH SYSTEMS C O R P O R A T I O N Touching Lives Everyday" Policies and Procedures Subject: Emergency Care, Transfers (COBRA) Quality Through Compliance Issued by: Corporate Compliance Committee
Chapter 3. Covered Services
 Chapter 3 Covered Services This chapter covers the services for which hospitals may receive reimbursement through the Health Care Responsibility Act (HCRA). HCRA reimburses out-of-county hospitals for
Chapter 3 Covered Services This chapter covers the services for which hospitals may receive reimbursement through the Health Care Responsibility Act (HCRA). HCRA reimburses out-of-county hospitals for
Implementing EMTALA: Strategies for Compliance. Study Guide
 4573 Implementing EMTALA: Strategies for Compliance Study Guide Special Thanks Sue Dill, RN, MSN, JD Vice President of Legal Services Memorial Hospital of Union County Marysville, OH Charles Keeran Operations
4573 Implementing EMTALA: Strategies for Compliance Study Guide Special Thanks Sue Dill, RN, MSN, JD Vice President of Legal Services Memorial Hospital of Union County Marysville, OH Charles Keeran Operations
EMTALA. A 30 th Anniversary Journey. Steve Lipton. Cal. Society of Healthcare Risk Management March 10, Hooper, Lundy & Bookman, P.C.
 EMTALA A 30 th Anniversary Journey Steve Lipton Cal. Society of Healthcare Risk Management March 10, 2016 1Hooper, Lundy & Bookman, P.C. HAPPY ANNIVERSARY EMTALA The Journey 3Hooper, Lundy & Bookman, P.C.
EMTALA A 30 th Anniversary Journey Steve Lipton Cal. Society of Healthcare Risk Management March 10, 2016 1Hooper, Lundy & Bookman, P.C. HAPPY ANNIVERSARY EMTALA The Journey 3Hooper, Lundy & Bookman, P.C.
INDIAN HEALTH SERVICE (IHS) ADDENDUM TWO (2) SOONERCARE O-EPIC PRIMARY CARE PROVIDER/CASE MANAGEMENT
 ADDENDUM TWO (2) SOONERCARE O-EPIC PRIMARY CARE PROVIDER/CASE MANAGEMENT") INDIAN HEALTH SERVICE (IHS) ADDENDUM TWO (2) SOONERCARE O-EPIC PRIMARY CARE PROVIDER/CASE MANAGEMENT for AI/AN MEMBERS 1.0 PURPOSE The purpose of this Addendum (hereafter ADDENDUM 2) is for OHCA and PROVIDER
INDIAN HEALTH SERVICE (IHS) ADDENDUM TWO (2) SOONERCARE O-EPIC PRIMARY CARE PROVIDER/CASE MANAGEMENT for AI/AN MEMBERS 1.0 PURPOSE The purpose of this Addendum (hereafter ADDENDUM 2) is for OHCA and PROVIDER
Legal/Regulatory Overview EMTALA Anti-Dumping
 Legal/Regulatory Overview EMTALA Anti-Dumping The National Congress on the Un and Under Insured September 23, 2008 Washington, D.C. Charlotte S. Yeh, MD, FACEP Chief Medical Officer AARP Services, Inc.
Legal/Regulatory Overview EMTALA Anti-Dumping The National Congress on the Un and Under Insured September 23, 2008 Washington, D.C. Charlotte S. Yeh, MD, FACEP Chief Medical Officer AARP Services, Inc.
ARTICLE II. HOSPITAL/CLINIC AGREEMENT INCORPORATED
 REIMBURSEMENT AGREEMENT FOR PRIMARY CARE PROVIDER SERVICES Between OKLAHOMA HEALTH CARE AUTHORITY And SOONERCARE AMERICAN INDIAN/ALASKA NATIVE TRIBAL HEALTH SERVICE PROVIDERS ARTICLE 1. PURPOSE The purpose
REIMBURSEMENT AGREEMENT FOR PRIMARY CARE PROVIDER SERVICES Between OKLAHOMA HEALTH CARE AUTHORITY And SOONERCARE AMERICAN INDIAN/ALASKA NATIVE TRIBAL HEALTH SERVICE PROVIDERS ARTICLE 1. PURPOSE The purpose
Patient Rights & Responsibilities and Advance Directives. Annual Training Program
 Patient Rights & Responsibilities and Advance Directives Annual Training Program Background on Patient Rights The legal interests of persons who submit to medical treatment. For many years, common medical
Patient Rights & Responsibilities and Advance Directives Annual Training Program Background on Patient Rights The legal interests of persons who submit to medical treatment. For many years, common medical
EMTALA Technical Advisory Group (TAG) Update David Siegel, M.D., J.D., FACEP, FACP Chair
 Update David Siegel, M.D., J.D., FACEP, FACP Chair") EMTALA Technical Advisory Group (TAG) Update David Siegel, M.D., J.D., FACEP, FACP Chair Section 945 of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) requires the Secretary
EMTALA Technical Advisory Group (TAG) Update David Siegel, M.D., J.D., FACEP, FACP Chair Section 945 of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) requires the Secretary
Policies and Procedures
 1 Policies and Procedures THE MENNINGER CLINIC Finance & Admissions Policy MC-241 Financial Assistance Policy Effective Date: June 2016 Mission Statement The Menninger Clinic (The Clinic) is a leading
1 Policies and Procedures THE MENNINGER CLINIC Finance & Admissions Policy MC-241 Financial Assistance Policy Effective Date: June 2016 Mission Statement The Menninger Clinic (The Clinic) is a leading
EMTALA Technical Advisory Group
 AMERICAN ASSOCIATION OF NEUROLOGICAL SURGEONS THOMAS A. MARSHALL, Executive Director 5550 Meadowbrook Drive Rolling Meadows, IL 60008 Phone: 888-566-AANS Fax: 847-378-0600 info@aans.org President ROBERT
AMERICAN ASSOCIATION OF NEUROLOGICAL SURGEONS THOMAS A. MARSHALL, Executive Director 5550 Meadowbrook Drive Rolling Meadows, IL 60008 Phone: 888-566-AANS Fax: 847-378-0600 info@aans.org President ROBERT
Crisis Triage, Walk-ins and Mobile Crisis Services
 Section 10.15 Crisis Triage, Walk-ins and Mobile Crisis Services 10.15.1 Introduction 10.15.2 References 10.15.3 Scope 10.15.4 Did you know? 10.15.5 Definitions 10.15.6 Procedures 10.15.6-A Triage 10.15.6-B
Section 10.15 Crisis Triage, Walk-ins and Mobile Crisis Services 10.15.1 Introduction 10.15.2 References 10.15.3 Scope 10.15.4 Did you know? 10.15.5 Definitions 10.15.6 Procedures 10.15.6-A Triage 10.15.6-B
Policies and Procedures
 1 Policies and Procedures THE MENNINGER CLINIC Finance & Admissions Policy MC-241 Financial Assistance Policy Effective Date: November 1, 2016 Mission Statement The Menninger Clinic (The Clinic) is a leading
1 Policies and Procedures THE MENNINGER CLINIC Finance & Admissions Policy MC-241 Financial Assistance Policy Effective Date: November 1, 2016 Mission Statement The Menninger Clinic (The Clinic) is a leading
National Uninsured Audioconference. EMTALA Anti-Dumping Update
 National Uninsured Audioconference EMTALA Anti-Dumping Update March 5, 2008 Overview Patient Transfers -- Unintended Consequences Behavioral Health -- A Mighty Wind Blows between EMTALA and State Laws
National Uninsured Audioconference EMTALA Anti-Dumping Update March 5, 2008 Overview Patient Transfers -- Unintended Consequences Behavioral Health -- A Mighty Wind Blows between EMTALA and State Laws
EXPERT REPORTS ON THE NEW EMTALA GUIDELINES. from Emergency Physician LEGAL BULLETIN Volume 9, Number 5, 1999
 EXPERT REPORTS ON THE NEW EMTALA GUIDELINES from Emergency Physician LEGAL BULLETIN Volume 9, Number 5, 1999 "EMTALA, known as COBRA to physicians, governs everything we do in the ED," said Robert Bitterman,
EXPERT REPORTS ON THE NEW EMTALA GUIDELINES from Emergency Physician LEGAL BULLETIN Volume 9, Number 5, 1999 "EMTALA, known as COBRA to physicians, governs everything we do in the ED," said Robert Bitterman,
Cape Cod Hospital, Falmouth Hospital Financial Assistance Policy
 Introduction This policy applies to Cape Cod Hospital, Falmouth Hospital and any other specific locations and providers as identified in this policy. The hospital is the frontline caregiver providing medically
Introduction This policy applies to Cape Cod Hospital, Falmouth Hospital and any other specific locations and providers as identified in this policy. The hospital is the frontline caregiver providing medically
Patient Financial Services Policy
 Patient Financial Services Policy Policy: Purpose: Billing & Collection Policy MaineHealth hospitals and physician practices are the frontline caregivers providing medically necessary care for all people
Patient Financial Services Policy Policy: Purpose: Billing & Collection Policy MaineHealth hospitals and physician practices are the frontline caregivers providing medically necessary care for all people
Protocols and Guidelines for the State of New York
 Protocols and Guidelines for the State of New York UnitedHealthcare would like to remind health care professionals in the state of New York of the following protocols and guidelines: Care Provider Responsibilities
Protocols and Guidelines for the State of New York UnitedHealthcare would like to remind health care professionals in the state of New York of the following protocols and guidelines: Care Provider Responsibilities
Illinois Association of Defense Trial Counsel P.O. Box 7288, Springfield, IL IDC Quarterly Vol. 14, No. 2 (14.2.
 Health Law By: Roger R. Clayton Heyl, Royster, Voelker & Allen Peoria What Every Litigator Needs to Know About Recent Changes in EMTALA Introduction The Emergency Medical Treatment and Active Labor Act
Health Law By: Roger R. Clayton Heyl, Royster, Voelker & Allen Peoria What Every Litigator Needs to Know About Recent Changes in EMTALA Introduction The Emergency Medical Treatment and Active Labor Act
31470 Federal Register / Vol. 67, No. 90 / Thursday, May 9, 2002 / Proposed Rules
 31470 Federal Register / Vol. 67, No. 90 / Thursday, May 9, 2002 / Proposed Rules about the individual s payment method or insurance status. Section 1867 of the Act also provides for the imposition of
31470 Federal Register / Vol. 67, No. 90 / Thursday, May 9, 2002 / Proposed Rules about the individual s payment method or insurance status. Section 1867 of the Act also provides for the imposition of
UTILIZATION MANAGEMENT Section 4. Overview The Plan s Utilization Management (UM)
") Overview The Plan s Utilization Management (UM) Program is designed to meet contractual requirements and comply with federal regulations while providing members access to high quality, cost effective medically
Overview The Plan s Utilization Management (UM) Program is designed to meet contractual requirements and comply with federal regulations while providing members access to high quality, cost effective medically
EMERGENCY HEALTH SERVICES AND URGENT CARE CENTER SERVICES
 COVERAGE DETERMINATION GUIDELINE EMERGENCY HEALTH SERVICES AND URGENT CARE CENTER SERVICES Guideline Number: CDG.010.02 Effective Date: August 1, 2014 Table of Contents COVERAGE RATIONALE... DEFINITIONS
COVERAGE DETERMINATION GUIDELINE EMERGENCY HEALTH SERVICES AND URGENT CARE CENTER SERVICES Guideline Number: CDG.010.02 Effective Date: August 1, 2014 Table of Contents COVERAGE RATIONALE... DEFINITIONS
You recently called the Medicare Rights helpline for assistance with a denial from your Medicare private health plan.
 Date: Dear Helpline Caller: The Medicare Rights Center is a national, nonprofit organization. We help older adults and people with disabilities with their Medicare problems. We support caregivers and train
Date: Dear Helpline Caller: The Medicare Rights Center is a national, nonprofit organization. We help older adults and people with disabilities with their Medicare problems. We support caregivers and train
Precertification: Overview
 Precertification: Overview Introduction Precertification determines whether medical services are: Medically Necessary or Experimental/Investigational Provided in the appropriate setting or at the appropriate
Precertification: Overview Introduction Precertification determines whether medical services are: Medically Necessary or Experimental/Investigational Provided in the appropriate setting or at the appropriate
Blue Choice PPO SM Provider Manual - Preauthorization
 In this Section Blue Choice PPO SM Provider Manual - The following topics are covered in this section. Topic Page Overview E 3 What Requires E 3 evicore Program E 3 Responsibility for E 3 When to Preauthorize
In this Section Blue Choice PPO SM Provider Manual - The following topics are covered in this section. Topic Page Overview E 3 What Requires E 3 evicore Program E 3 Responsibility for E 3 When to Preauthorize
Lahey Clinic Hospital, Inc. Financial Assistance Policy
 Lahey Clinic Hospital, Inc. Financial Assistance Policy This policy applies to Lahey Clinic Hospital, Inc. DBA Lahey Hospital and Medical Center ( the hospital ) and specific locations and providers as
Lahey Clinic Hospital, Inc. Financial Assistance Policy This policy applies to Lahey Clinic Hospital, Inc. DBA Lahey Hospital and Medical Center ( the hospital ) and specific locations and providers as
Refusal Protocol. Christopher J. Bosche, MD FACEP Medical Director Mehlville Fire Protection District
 Refusal Protocol Christopher J. Bosche, MD FACEP Medical Director Mehlville Fire Protection District I am not a lawyer Advice to Me The law is vague for a reason. ex: Appropriate medical screening exam
Refusal Protocol Christopher J. Bosche, MD FACEP Medical Director Mehlville Fire Protection District I am not a lawyer Advice to Me The law is vague for a reason. ex: Appropriate medical screening exam
UNITED STATES DISTRICT COURT DISTRICT OF NEVADA
 Case :0-cv-0-LDG-PAL Document Filed /0/0 Page of JACOB L. HAFTER, ESQ. Nevada State Bar No. 0 MICHAEL NAETHE, ESQ. Nevada State Bar No. LAW OFFICE OF JACOB L. HAFTER, P.C. W. Lake Mead Boulevard, Suite
Case :0-cv-0-LDG-PAL Document Filed /0/0 Page of JACOB L. HAFTER, ESQ. Nevada State Bar No. 0 MICHAEL NAETHE, ESQ. Nevada State Bar No. LAW OFFICE OF JACOB L. HAFTER, P.C. W. Lake Mead Boulevard, Suite
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Boston Medical Center Financial Assistance Policy. Introduction
 Boston Medical Center Financial Assistance Policy Introduction The mission of Boston Medical Center (the Hospital or BMC ), in partnership with its licensed Community Health Centers, is to provide consistently
Boston Medical Center Financial Assistance Policy Introduction The mission of Boston Medical Center (the Hospital or BMC ), in partnership with its licensed Community Health Centers, is to provide consistently
DIGNITY HEALTH GOVERNANCE POLICY AND PROCEDURE
 DIGNITY HEALTH GOVERNANCE POLICY AND PROCEDURE Dignity Health 9.101 FROM: Dignity Health Board of Directors SUBJECT: EFFECTIVE DATE: January 1, 2017 REVISED: January 1, 2016; (60.4.006) January 17, 2012
DIGNITY HEALTH GOVERNANCE POLICY AND PROCEDURE Dignity Health 9.101 FROM: Dignity Health Board of Directors SUBJECT: EFFECTIVE DATE: January 1, 2017 REVISED: January 1, 2016; (60.4.006) January 17, 2012
Application of Proposals in Emergency Situations
 March 27, 2018 Alex Azar Secretary Department of Health and Human Services Hubert H. Humphrey Building Room 509F 200 Independence Avenue, SW. Washington, DC 20201 Re: RIN 0945-ZA03 Re: Protecting Statutory
March 27, 2018 Alex Azar Secretary Department of Health and Human Services Hubert H. Humphrey Building Room 509F 200 Independence Avenue, SW. Washington, DC 20201 Re: RIN 0945-ZA03 Re: Protecting Statutory
Objectives. Emergency Medicine Risk Factors
 The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
OASIS HOSPITAL GOVERNANCE POLICY AND PROCEDURE
 OASIS HOSPITAL GOVERNANCE POLICY AND PROCEDURE FROM: SUBJECT: OASIS Hospital Board of Directors Financial Assistance Policy - Arizona EFFECTIVE DATE: REVISED: 7/16 REVIEWED WITH NO CHANGES: 7/16 ORIGINAL
OASIS HOSPITAL GOVERNANCE POLICY AND PROCEDURE FROM: SUBJECT: OASIS Hospital Board of Directors Financial Assistance Policy - Arizona EFFECTIVE DATE: REVISED: 7/16 REVIEWED WITH NO CHANGES: 7/16 ORIGINAL
TORRANCE MEMORIAL MEDICAL STAFF
 BYLAWS COMMITTEE: APPROVED WITH NO CHANGES 10/3/2017 Dates Approved: Medical Executive Committee 09/14/2010; 12/9/2014 PATIENT ATTRIBUTION PLAN: This Attribution Plan assures that all staff are able to
BYLAWS COMMITTEE: APPROVED WITH NO CHANGES 10/3/2017 Dates Approved: Medical Executive Committee 09/14/2010; 12/9/2014 PATIENT ATTRIBUTION PLAN: This Attribution Plan assures that all staff are able to
EMTALA: AN OVERVIEW OF ITS ENDURING ROLE IN EMERGENCY CARE
 RiskRx Clinical Risk Management Newsletter Fall 2016 EMTALA: AN OVERVIEW OF ITS ENDURING ROLE IN EMERGENCY CARE By Irma Spaho, LLB, LLM Introduction: The following article is intended to provide general
RiskRx Clinical Risk Management Newsletter Fall 2016 EMTALA: AN OVERVIEW OF ITS ENDURING ROLE IN EMERGENCY CARE By Irma Spaho, LLB, LLM Introduction: The following article is intended to provide general
#507 Do It Yourself EMTALA Auditing April 21, 2015
 #507 Do It Yourself EMTALA Auditing April 21, 2015 Robert S. Brown Manager UW Medicine Compliance University of Washington Seattle, Washington 1 LEARNING OBJECTIVES Understand the background and basics
#507 Do It Yourself EMTALA Auditing April 21, 2015 Robert S. Brown Manager UW Medicine Compliance University of Washington Seattle, Washington 1 LEARNING OBJECTIVES Understand the background and basics
Signage/Notices. Claire Lester BA CRCE Baycare Health Systems
 Signage/Notices Claire Lester BA CRCE Baycare Health Systems This is not a complete representation of all Signage/Notices. EMTALA Signage IT'S THE LAW EMTALA Sign State Operations Manual Appendix V. Basic
Signage/Notices Claire Lester BA CRCE Baycare Health Systems This is not a complete representation of all Signage/Notices. EMTALA Signage IT'S THE LAW EMTALA Sign State Operations Manual Appendix V. Basic
Provider Evaluation of Performance. Plan. Tennessee
 Provider Evaluation of Performance Plan Tennessee 2018 Executive Summary UnitedHealthcare Community Plan is committed to ensuring the services members receive from network providers meet the requirements
Provider Evaluation of Performance Plan Tennessee 2018 Executive Summary UnitedHealthcare Community Plan is committed to ensuring the services members receive from network providers meet the requirements
EMTALA Compliance In Disaster Circumstances
 EMTALA Compliance In Disaster Circumstances Prepared by: Steve Gravely, J.D., M.H.A. Erin Whaley, J.D., M.A. Troutman Sanders LLP Prepared for: Virginia Hospital and Healthcare Association March 2, 2007
EMTALA Compliance In Disaster Circumstances Prepared by: Steve Gravely, J.D., M.H.A. Erin Whaley, J.D., M.A. Troutman Sanders LLP Prepared for: Virginia Hospital and Healthcare Association March 2, 2007
State of New Jersey DEPARTMENT OF BANKING AND INSURANCE INDIVIDUAL HEALTH COVERAGE PROGRAM PO BOX 325 TRENTON, NJ
 CHRIS CHRISTIE Governor KIM GUADAGNO Lt. Governor State of New Jersey DEPARTMENT OF BANKING AND INSURANCE INDIVIDUAL HEALTH COVERAGE PROGRAM PO BOX 325 TRENTON, NJ 08625-0325 TEL (609) 633-1882 FAX (609)
CHRIS CHRISTIE Governor KIM GUADAGNO Lt. Governor State of New Jersey DEPARTMENT OF BANKING AND INSURANCE INDIVIDUAL HEALTH COVERAGE PROGRAM PO BOX 325 TRENTON, NJ 08625-0325 TEL (609) 633-1882 FAX (609)
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
EMTALA A Guide to Patient Anti-Dumping Laws
 EMTALA A Guide to Patient Anti-Dumping Laws 2018 9th Edition Written by M. Steven Lipton Hooper, Lundy & Bookman, PC Published by California Hospital Association CHA Publications Several helpful publications
EMTALA A Guide to Patient Anti-Dumping Laws 2018 9th Edition Written by M. Steven Lipton Hooper, Lundy & Bookman, PC Published by California Hospital Association CHA Publications Several helpful publications
Training Bulletin: When to Conduct an Exam or Interview Why Are We Prodding Victims to Keep Them Awake?
 We often receive questions from health care providers, law enforcement officers, and victim advocates about when they should conduct an exam or detailed interview with a victim of a sexual assault. In
We often receive questions from health care providers, law enforcement officers, and victim advocates about when they should conduct an exam or detailed interview with a victim of a sexual assault. In
INFORMATION ABOUT YOUR OXFORD COVERAGE REIMBURSEMENT PART I OXFORD HEALTH PLANS OXFORD HEALTH PLANS (NJ), INC.
, INC.") OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Passport Advantage Provider Manual Section 5.0 Utilization Management
 Passport Advantage Provider Manual Section 5.0 Utilization Management Table of Contents 5.1 Utilization Management 5.2 Review Criteria 5.3 Prior Authorization Requirements 5.4 Organization Determinations
Passport Advantage Provider Manual Section 5.0 Utilization Management Table of Contents 5.1 Utilization Management 5.2 Review Criteria 5.3 Prior Authorization Requirements 5.4 Organization Determinations
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
VOLUME II/MA, MT51 01/17 SECTION
 2054 POLICY STATEMENT Emergency Medical Assistance (EMA) provides medical coverage to individuals who meet all requirements for a Medicaid Class of Assistance (COA) except for citizenship/immigration status
2054 POLICY STATEMENT Emergency Medical Assistance (EMA) provides medical coverage to individuals who meet all requirements for a Medicaid Class of Assistance (COA) except for citizenship/immigration status
Workers Compensation Health Care Network
 The Hartford s Texas Workers Compensation Health Care Network Employee Enrollment Package Includes: 1. Employee Notification Letter 2. Attachment A - Healthcare Provider Listing 3. Attachment B - Description
The Hartford s Texas Workers Compensation Health Care Network Employee Enrollment Package Includes: 1. Employee Notification Letter 2. Attachment A - Healthcare Provider Listing 3. Attachment B - Description
Hospital On-Call Responsibilities: A Urology Group Practice Analysis
 Hospital On-Call Responsibilities: A Urology Group Practice Analysis Case Study This case study manuscript is being submitted in partial fulfillment of the requirement for ACMPE Fellowship Hospital On-Call
Hospital On-Call Responsibilities: A Urology Group Practice Analysis Case Study This case study manuscript is being submitted in partial fulfillment of the requirement for ACMPE Fellowship Hospital On-Call
Appendix A: Requirements and Best Practices for Reportable Incidents
 Appendix A: Requirements and Best Practices for Reportable Incidents Reporting Incidents The table below shows what events must and must not be reported to achieve compliance with 55 Pa.Code 2600.16(c).
Appendix A: Requirements and Best Practices for Reportable Incidents Reporting Incidents The table below shows what events must and must not be reported to achieve compliance with 55 Pa.Code 2600.16(c).
AMENDATORY SECTION (Amending WSR , filed 8/27/15, effective. WAC Inpatient psychiatric services. Purpose.
 AMENDATORY SECTION (Amending WSR 15-18-065, filed 8/27/15, effective 9/27/15) WAC 182-550-2600 Inpatient psychiatric services. Purpose. (1) The medicaid agency, on behalf of the mental health division
AMENDATORY SECTION (Amending WSR 15-18-065, filed 8/27/15, effective 9/27/15) WAC 182-550-2600 Inpatient psychiatric services. Purpose. (1) The medicaid agency, on behalf of the mental health division
MEMBER WELCOME GUIDE
 2015 Dear Patient; MEMBER WELCOME GUIDE The staff of Scripps Health Plan and its affiliate Plan Medical Groups (PMG), Scripps Clinic Medical Group, Scripps Coastal Medical Center, Mercy Physician Medical
2015 Dear Patient; MEMBER WELCOME GUIDE The staff of Scripps Health Plan and its affiliate Plan Medical Groups (PMG), Scripps Clinic Medical Group, Scripps Coastal Medical Center, Mercy Physician Medical
AMBULANCE SERVICES. Guideline Number: CS003.F Effective Date: January 1, 2018
 AMBULANCE SERVICES UnitedHealthcare Community Plan Coverage Determination Guideline Guideline Number: CS003.F Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
AMBULANCE SERVICES UnitedHealthcare Community Plan Coverage Determination Guideline Guideline Number: CS003.F Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...