Using Telemedicine to Reduce Potentially Avoidable Hospitalizations of Nursing Home Residents
|
|
|
- Mavis Blankenship
- 6 years ago
- Views:
Transcription

1 Using Telemedicine to Reduce Potentially Avoidable Hospitalizations of Nursing Home Residents Steven M. Handler MD, PhD, CMD Associate Professor, Division of Geriatric Medicine and Biomedical Informatics; CMIO, UPMC Community Provider Services
2 Disclosure I am the Chief Medical and Innovation Officer for Curavi Health I do not own any equity interests in Curavi Health, nor do I have any options or other interests that are convertible into equity interests in Curavi Health 2
3 Learning Objectives 1. Describe the frequency, cost, and consequences of potentially avoidable hospitalizations (PAHs) of nursing home (NH) residents. 2. Summarize the evidence base for using telemedicine to reduce PAHs in NHs. 3. Identify and address the most significant barriers and articulate how you can use telemedicine in NHs to reduce PAHs. 3
4 Potentially Avoidable Hospitalizations (PAHs) CMS defines PAHs as hospitalizations that could have been avoided because the condition could have been prevented or treated outside of an inpatient hospital setting. Each year, approximately 25% of all long-stay and post-acute residents on a fee-for-service Medicare benefit in NHs are hospitalized, while over 20% are readmitted in 30-days following hospital discharge. NH residents are sent to the Emergency Department (ED) an average of nearly 2 times per year, and just over half of these visits do not result in hospitalization. 4 Medicare & Medicaid Research Review 2014;4.
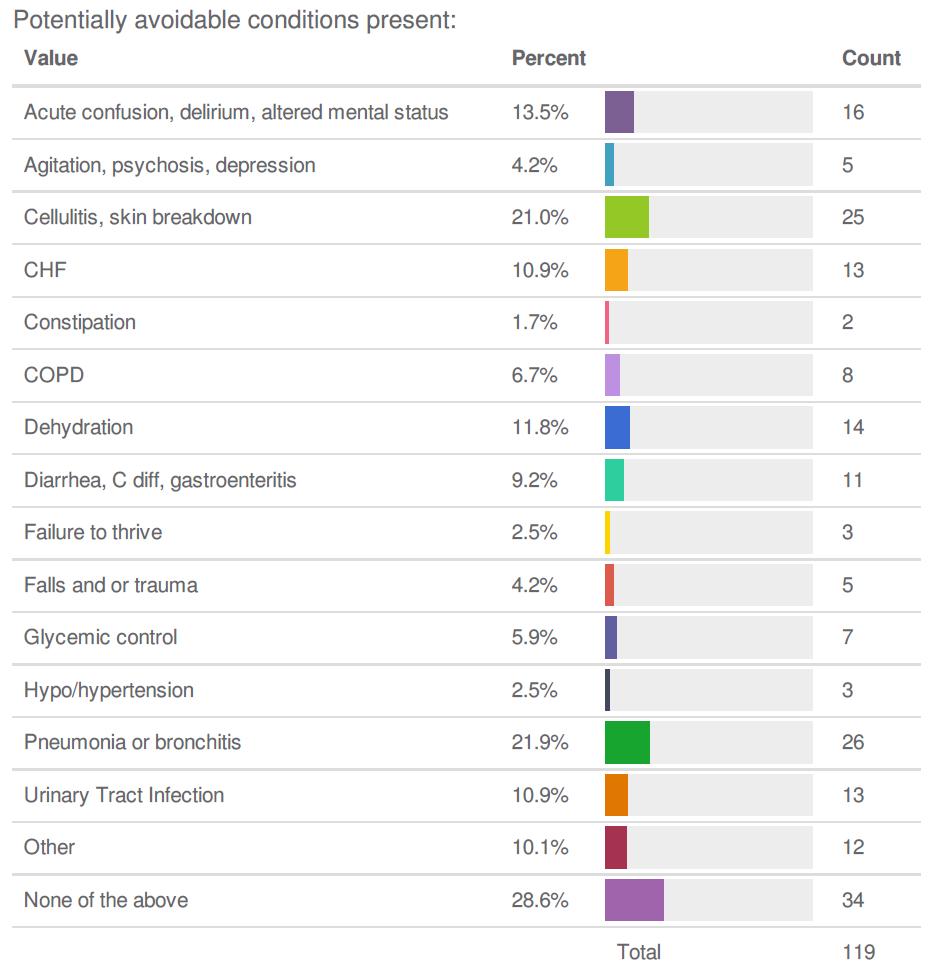
5 Most Common PAH Diagnoses Six conditions responsible for 80% of PAHs: Pneumonia (32.8%) UTI (14.2%) CHF (11.6%) Dehydration (10.3%) COPD / Asthma (6.5%) Skin Ulcers, cellulitis (4.9%) 5
6 Complete List of PAH Diagnoses Acute Renal Failure (AKI) Altered mental status Anemia Asthma C. Difficile infection Cellulitis CHF (congestive heart failure) Constipation/Impaction COPD Diarrhea/Gastroenteritis Failure to thrive Falls and Trauma HTN (hypertension) Pneumonia/Bronchitis Nutritional deficiency Poor glycemic control Psychosis Seizures Skin Ulcers UTI (urinary tract infections) 6
7 Impact of PAHs Economic Impact - Have an avg. length of stay of 6.1 days and an estimated cost of $8 billion ($11,255/ admission) to CMS (Centers for Medicare and Medicaid). Clinical Impact: Death Disability Debility Delirium Discharged to higher level of care 7


8 Potentially Avoidable Hospitalizations Affect Many Aspects of the NH Strategy 8 CONFIDENTIAL & PROPRIETARY TO CURAVI HEALTH

9 Why We Should Care: The CMS Regulatory and Reimbursement Landscape 9

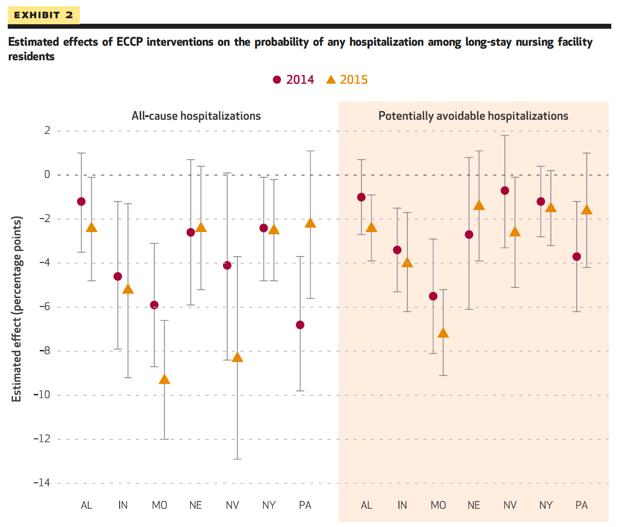
10 10 The range in rates across the states was considerable, with more than a threefold difference across states.

11 Disproportionate # of PAHs Come from NHs 16% of Medicare/ Medicaid beneficiaries were in a NH, yet comprised 45% of all PAHs Most common setting where PAHs originate from are NHs PAHs from NHs are often multifactorial 11
12 12
13 April L. Kane, MSW, LSW RAVEN Co-Director Chip Reynolds, MD RAVEN Co-Director Steven M. Handler MD, PhD, CMD Medical Director of Health Information Technology Phase 1: From CMS Cooperative Agreement 1E1CMS331081
14 Programs Designed to Reduce PAHs 1. Evercare (Optum Care Plus) model that uses NPs and Care Managers reduced hospital admissions by 47% and emergency department use by 49% (Kane et. al, 2004) 2. Medicare Advantage partnerships to waive 3-day qualifying hospital stay necessary for Part A benefit and treat in place 3. INTERACT QI program reduced hospital admissions between 17-24% (Ouslander et al, 2011) 14
15 Core Programatic Elements of RAVEN 1. Facility-based Nurse Practitioners/Enhanced Care Nurses 2. INTERACT tools to reduce avoidable hospital admission 3. Individualized educational program/simulation 4. Enhanced medication management, monitoring, and pharmacy engagement 5. Use of telemedicine to enable remote clinical assessment, and facilitate communication. 15






16 1 Ball Pavilion 2 Corry Manor 3 Oakwood Heights Sweden Valley Manor 8 Lutheran Home at Kane Sugar Creek Rest Friendship Ridge 15 Squirrel Hill Center for Rehabilitation & Healing 18 3 KaneMcKeesport Westmoreland Manor Mountainview Specialty Care Center Kane-Ross Golden Living Center Sunnyview Nursing & Rehabilitation Kane-Glen Hazel 16 2 Edison Manor Evergreen Health & Rehabilitation 9 1 Trinity Living Center

17 Technological Sophistication of NHs Approx. 60% of NHs have an EMR Majority use a fax for meds, labs, radiology, recaps 17
18 What is Telemedicine? Telemedicine is defined as the use of telecommunication and information technologies in order to provide clinical healthcare at a distance. Types of telemedicine: 1. Interactive services (synchronous) 2. Store-and-forward (asynchronous) 3. Remote monitoring (selfmonitoring) 4. mhealth (mobile devices) 18
19 Evidence-Base for Telemedicine in NHs Edirippulige et al, conducted a systematic review which provides evidence for feasibility and stakeholder satisfaction in using telemedicine in NHs across clinical specialities J Telem Telecare, 2013 Grabowksi et al., showed that an after-hours physicianbased telemedicine program can reduce hospitalization by 9.7% and yield $151K cost savings to Medicare/NH/yr. Health Aff, 2014 Hofmeyer et al., showed that NHs had on avg. 23 consults per/yr. and overall 69% of cases were not transferred. JAMDA,
20 National Telemedicine Summit Held on 3/25/15 at the UPMC Center for Connected Medicine and included 15 participants representing 91 NHs (11,842 beds) Telemedicine is critical to the future and should be viewed as the linchpin to the transformation of NHs (60.0%; 9/15) Factors influencing adoption include hospitals (8.5/10), managed care (8.4/10) and ACOs (8.1/10) making telemedicine a requirement of their NH partners, as well as the rise of value-based purchasing options (8.4/10) Driessen J, Castle NG. Handler SM. J of Appl Gerontol. (In Press) 20

21 Perceptions of Telemedicine The goal of this study was to survey NH physicians and nurse practitioners to quantify provider perceptions and desired functionality of telemedicine in NHs to reduce PAHs. Driessen, Handler, et al. J Am Med Dir Assoc 2016:17(6):
22 Perceptions of Telemedicine for PAHs Surveyed 435 physicians and nurse practitioners who attended the 2015 AMDA - The Society for Post-Acute and Long-Term Care Medicine Annual Conference Survey components: Case vignette showing how telemedicine could be used to manage acute changes of condition in NHs Perceived benefits and concerns about the use of telemedicine in NHs Attributes of a successful telemedicine program Demographic information 22


23 Perceptions and Attributes of Telemedicine 23
24 Summary: Using Telemedicine for PAHs Highly positive and strongly-held beliefs of the value of telemedicine for managing PAHs in the NH setting Suggests that there is potentially unmet demand for telemedicine and that NHs may be receptive to appropriately designed solutions Need to focus on the sociotechnical aspects of implementation and continued use of telemedicine to ensure its continued use through a highly structured change mgmt. process Limitations include self-selected sample and potential biases in the respondent population 24
25 Telemedicine for NH Specialty Consultations The goal of this study was to determine the perceived utility of providing speciality telemedicine in NHs Surveyed 522 physicians and nurse practitioners who attended the 2016 AMDA - The Society for Post-Acute and Long-Term Care Medicine Annual Conference Top 5 specialties that physicians and APPs would refer to: Derm > Geri psych > ID > Neuro > Cards Top 5 Statements of agreement: Fill an existing service gap > Improve timeliness of resident care > Increase access to appropriate care > Decrease ED/hosp > Increase overall quality of care 25 Manuscript submitted for peer-review
26 RAVEN Telemedicine Team and Approach Ashley Boots, CRNP Christa Bartos, RN, PhD Julie George, RN RAVEN CRNPs and erns Telemedicine Support Group Community Provider Services IT Facility engagement Facility and telemedicine readiness Facility telemedicine training 26
27 Case Vignette
28
29 Traditional Telephonic Clinical Case Chris Bartos is an 86 yo female (new resident) transferred to Jane St NH following a recent hospitalization for a UTI with sepsis Resident has a PMHx of diabetes, hypertension, osteoarthritis, Alzheimer s disease and malnutrition Resident has indicated FULL TREATMENT on her POLST form and would like antibiotics if life can be prolonged Family wants to send her out because they believe that the hospital can take care of sick patients better
30 30 How can we do this differently?

31 Telly the Telemedicine Cart HP All-in-one PC Washable keyboard/mouse Pan/tilt/zoom camera HD Web camera Speakerphone Bluetooth stethoscope Digital otoscope 12-lead PC-Based EKG Portable Doppler ultrasound Teleconference/med software Wireless gateway (Verizon/ATT LTE)
32 32 Video of a telemedicine consultation
33 RAVEN Telemedicine Results 15 RAVEN Partner NHs CRNP-based model; 6 hrs./day; long-stay residents (>100 days) only Completed 205 telemedicine and 2,196 telephonic-only consultations between 2/2014 and 2/2017 Percentage of hospital transfers avoided: Sep 2014 February 28, 2017 Telemedicine consults (111 of 174)* 63.8% Telephonic-only consults (212 of 2,196) 9.7%
34 Telemedicine 34

35 Post-Consult Telemedicine Survey 35

36 Post-Consult Telemedicine Survey (Cont.) 36
37 Lessons Learned Facility physician and administration support is critical for success Telemedicine is not just a technology change, but also a culture change for NH staff (sociotechnical aspects) Consistent connectivity is crucial for successful consults Keep everything as simple and intuitive as possible No individual user IDs and passwords Ongoing education and support refreshers provide repetition and keep NH staff aware 37
 Evaluation of the Initiative to Reduce Avoidable Hospitalizations among Nursing Facility Residents: Final")
38 RAVEN Phase 1 Interim Results Net savings to CMS of over $5 million (first 3 yrs. of data) Evaluation of the Initiative to Reduce Avoidable Hospitalizations among Nursing Facility Residents: Final Annual Report Project Year 3, RTI,
39 39
40 April L. Kane, MSW, LSW RAVEN Co-Director Chip Reynolds, MD RAVEN Co-Director Steven M. Handler MD, PhD, CMD RAVEN Co-Director Phase 2: From CMS Cooperative Agreement 1E1CMS331081
41 Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model CMS Cooperative Agreement 1E1CMS331491
42 Why Implement Payment Model? The initial four years of the demonstration project ( ) addressed preventing avoidable hospitalizations through various clinical quality models. 42
43 Why Implement Payment Model? HOWEVER. the initial demonstration did NOT address the existing payment policies that may be leading to avoidable hospitalizations. 43
44 Payment Reforms CMS is adding new codes to the Medicare Part B schedule specifically for this Initiative Facility payment Treatment of six qualifying conditions Practitioner payments #1 - onsite treatment of six qualifying conditions #2 - care coordination & caregiver engagement 44
45 Principal Payment Reform Goal: Six Conditions CMS states that six conditions are linked to approximately 80% of potentially avoidable hospitalizations among nursing facility residents nationally Pneumonia Urinary tract infection Congestive heart failure Dehydration COPD, asthma Skin ulcers, cellulitis 32.8% 14.2% 11.6% 10.3% 6.5% 4.9% 45
46 Facility Payment for Six Qualifying Conditions Purpose Create incentive for facility to enhance staff skills to provide higher level of service in-house Payment Onsite Acute Care Limited to 5-7 days, based on qualifying condition Limited to residents not on a covered Medicare Part A SNF stay and who meet the long stay criteria 46
47 Facility Payment for Six Qualifying Conditions (cont d) The six conditions have very specific, detailed qualifying criteria that could trigger the benefit Detection of acute change of condition documented in the medical record by a physician or a nurse at the LPN level or higher STOP AND WATCH tool, SBAR, free text note, structured clinical documentation are acceptable formats as long as they are part of the medical records 47
48 Facility Payment for Six Qualifying Conditions (cont d) Qualifying criteria that could trigger the benefit MD, NP or PA must confirm qualifying diagnosis through in-person evaluation or qualifying telemedicine assessment ANY attending practitioner can provide confirming diagnosis for the purposes of facility payment 48
49 Facility Payment for Six Qualifying Conditions (cont d) Qualifying criteria that could trigger the benefit (cont d) Evaluation or assessment must occur by the end of the 2nd day after change in condition Evaluation must be documented in resident s medical record If there is more than one qualifying diagnosis, both should be reported even though facility may only bill code once per day 49
50 Practitioner Payment #1 for Six Qualifying Conditions Purpose Create incentive for practitioner to conduct nursing facility resident visits to treat acute change in condition Equalize payment for acute change of condition visit regardless of location of service Payment Billing Code G9685; Acute Nursing Facility Care Payment will be equivalent to what would be received for a comparable visit in a hospital. Limited to first visit in response to a beneficiary who has experienced an acute change in condition (to confirm and treat the diagnosed condition) NPs & PAs reimbursed at 85% of physician 50
51 Practitioner Payment #1 for Six Qualifying Conditions (cont d) In decisions regarding provision of care, the focus should always be on providing the best setting for the resident/patient Six conditions have qualifying criteria MD, NP or PA must confirm qualifying diagnosis through in-person evaluation or qualifying telemedicine assessment Evaluation or assessment must occur by end of the 2nd day after acute change in condition Evaluation documented in resident s medical record 51
52 Practitioner Payment #1 for Six Qualifying Conditions (cont d) The new code can be billed even if the exam reveals that the resident does NOT have one of the six qualifying conditions. If ECCP staff or Telemedicine visit confirms diagnosis to allow facility payment, an eligible practitioner can still see resident for a face-toface visit by the end of the second day and bill at increased initial visit rate. 52
53 Purpose Practitioner Payment #2 for Care Coordination Payment to create incentive for practitioners to participate in nursing facility conferences, and engage in care coordination discussions with beneficiaries, their caregivers, and LTC facility interdisciplinary team. Payment Billing Code G9686; Nursing Facility Conference 53
54 Practitioner Payment #2 for Care Coordination (cont d) Code can be billed within 14 days of significant change in condition that increases likelihood of hospital admission. If billed, change in condition must be documented in beneficiary s chart and reflected in comprehensive MDS assessment. 54

55 Proposed Skilled Nursing Facilities for Phase Two 55
56 Using Telemedicine to Reduce Potentially Avoidable Hospitalizations in UPMC-Owned Nursing Homes 56
57 Telemedicine in UPMC NHs 6 UPMC NHs (~700 beds) Geriatrician-based model; 6 hrs./day; whole-house model Completed 98 telemedicine and 38 telephone consultations Since 3/15 Percentage of hospital transfers avoided: cumulative totals reflect Mar 2015 August 2016 Telemedicine (39 of 98) 40.0% After-Hours Telephone Consults (6 of 38) 16.0% 57 Thanks to Kambria Ernst, RN, MSN

58 Testimonial by Dr. Adele Towers Play video 58
59 Anecdotes NP: We can do a lot at these facilities Sometimes patients get sent out during the night and I get frustrated because we could have safely managed the resident. Nurses: This is going to be very useful. Sometimes it is just really hard to describe a residents condition on the telephone. DON: I see this is really great, it is going to let our nurses be nurses. Residents families: Aw struck and I think they were shocked. The only question I got was do we have to pay for this They were surprised. One lady said I saw this on Dr. Phil, dial a doctor. Doctors: This is great if it cuts down on the phone calls I get at night. 59
60 Implications for NH/Payor/Provider/Family Improve alignment of care to be more consistent with goals of care, advanced directives, and family preferences Increase access to appropriate care when physicians and CRNPs are not typically available on-site Expand clinical capabilities of NHs (e.g., EKG services) Reduce variability in care that is provided to NH residents by using standardized order sets 60
61 Implications for NH/Payor/Provider/Family Lower cost of care by providing it in the NHs rather than the ED or hospital which can reduce the number of PAHs and lowers readmission rates Maintain NH census stabilization and referral relationships with hospitals Reduction of pending CMS payment penalties for PAHs (value-based purchasing initiative) and alignment with other alternative payment models (bundled payments, ACOs) 61
62 Barriers to Telemedicine in NHs Physician and APP State licensure Physician and APP facility credentialing Establishment of physician/app resident relationships Lack of belief in the value or potential of the technology Limited information technology infrastructure/connectivity in NHs Administrative support/buy-in High nursing staff turnover Reimbursement 62

63 Telehealth Services Originating sites Distant site practitioners Telehealth services Billing and payment for professional services Billing and payment for originating site facility fee
64 Originating sites An originating site is the location of an eligible Medicare beneficiary at the time the service furnished via a telecommunications system occurs. Medicare beneficiaries are eligible for telehealth services only if they are presented from an originating site located in: A county outside of a Metropolitan Statistical Area (MSA) A rural Health Professional Shortage Area (HPSA) located in a rural census tract Determine if your NH is an authorized (rural non-msa) originating site:
65 Originating Sites Authorized by Law Are The offices of physicians or practitioners Hospitals Critical Access Hospitals (CAHs) Rural Health Clinics Federally Qualified Health Centers Hospital-based or CAH-based Renal Dialysis Centers Community Mental Health Centers (CMHCs) Skilled Nursing Facilities (SNFs)
66 Distant Site Practitioners Physicians Nurse practitioners (NPs) Physician assistants (PAs) Nurse-midwives Clinical nurse specialists (CNSs) Certified registered nurse anesthetists Clinical psychologists (CPs) and clinical social workers (CSWs)
67 Telehealth Services As a condition of payment, you must use an interactive audio and video telecommunications system that permits real-time communication between you, at the distant site, and the beneficiary, at the originating site. Asynchronous store and forward technology is permitted only in Federal telemedicine demonstration programs in Alaska or Hawaii.
68 Subsequent Nursing Facility Services For medical necessity, use the Subsequent Nursing Facility Care CPT E&M codes and include the GT modifier After January 1, 2017, you must use Place of Service (POS) 02: Telehealth Ensure that your H&P meets all requirements for that particular CPT E&M code and is documented in the NH medical record Limited to 1 visit per the same resident every 30 days 68
69 Advance Care Planning Services For advance care planning (ACP) services, use CPT E&M codes (first 30 min.) and (each addl. 30 min.) (starting January 2017) Include the GT modifier (via interactive audio and video telecommunications system) and POS 02 for Telehealth Ensure that your H&P meets all requirements for that particular CPT E&M code and is documented in the NH medical record There is no limits on the number of times ACP can be reported for a given beneficiary in a given time period 69
70 Originating Site Facility Fee Determine if your NH is an authorized (rural non-msa) originating site: HCPCS code Q3014, Telehealth originating site facility fee Can be billed for Short-term and LTC Medicare Beneficiaries The NH bills the MAC for the originating site facility fee, which is a separately billable Part B payment = revenue in addition to the daily RUGs rate for skilled residents Managed care companies can reimburse NHs for code Q3014 for all products if they elect to do so 70
71 Interstate Medical Licensure Compact Basic requirements do not change for state licensure of a physician seeking only one license or who chooses to become licensed in additional states through the existing process. Once a physician receives a Compact-issued license from a state, the physician still must adhere to the existing renewal and CME requirements of that state. The Compact in no way overrides a state s authority and control over the physician s practice of medicine. State participation in the Compact is voluntary, and states are free to withdraw from the Compact at any time by repealing the enacted statute. The process of licensure proposed in the Compact would reduce costs by streamlining the process for licensees. 71
72 How Can You Do Telemedicine in the NH? Communicate the value of telemedicine residents/family Work with the NH to ensure facility engagement, facility and telemedicine readiness, and facility telemedicine training Use HIPAA-compliant and secure telemedicine software and hardware (Guidance from CMS; Appendix C) Confirm that NH has notified the Dept. of Health 72
73 How Can You Do Telemedicine in the NH? Ensure that you are licensed to practice medicine in the State where the originating site is located Ensure you have notified your malpractice insurer Strongly consider becoming credentialed in the facility where you provide telemedicine services 73
74 Questions? 74
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
9/21/2017. Telemedicine vs. Telehealth. Telemedicine vs. Telehealth. Telemedicine vs. Telehealth. Time is Money. Disruptive Technology
 Telemedicine vs. Telehealth Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients health status. Telemedicine The Virtual Experience
Telemedicine vs. Telehealth Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients health status. Telemedicine The Virtual Experience
u Telemedicine The Virtual Experience
 Telemedicine The Virtual Experience April 2017 Telemedicine vs. Telehealth Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients
Telemedicine The Virtual Experience April 2017 Telemedicine vs. Telehealth Telemedicine is the use of medical information exchanged from one site to another via electronic communications to improve patients
Telemedicine and Reimbursement
 Telemedicine and Reimbursement Presented for : March 14 th 2018 About Acevedo Consulting Incorporated Acevedo Consulting Incorporated prides itself on not providing cookie-cutter programs, but a quality
Telemedicine and Reimbursement Presented for : March 14 th 2018 About Acevedo Consulting Incorporated Acevedo Consulting Incorporated prides itself on not providing cookie-cutter programs, but a quality
Cheryl A Skiffington, CCO & Interim CFO Columbia County Health System
 Cheryl A Skiffington, CCO & Interim CFO Columbia County Health System Telemedicine is A mode of delivery The service provided is basically the same as if the patient and provider were face-to-face. A modifier
Cheryl A Skiffington, CCO & Interim CFO Columbia County Health System Telemedicine is A mode of delivery The service provided is basically the same as if the patient and provider were face-to-face. A modifier
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telehealth in Peritoneal Dialysis Patient Management
 Telehealth in Peritoneal Dialysis Patient Management Susie Lew, MD George Washington University March 3, 2018 Disclosures CareFirst Foundation: grant ACT/ The App Association: Steering committee member
Telehealth in Peritoneal Dialysis Patient Management Susie Lew, MD George Washington University March 3, 2018 Disclosures CareFirst Foundation: grant ACT/ The App Association: Steering committee member
Telehealth 101. Telehealth Summit May 24, 2018
 Telehealth 101 Telehealth Summit May 24, 2018 Tim Bickel Telehealth Director, University of Louisville Deborah Burton, Telehealth Program Manager, KentuckyOne Health, Lexington; Chair, Kentucky Teleheath
Telehealth 101 Telehealth Summit May 24, 2018 Tim Bickel Telehealth Director, University of Louisville Deborah Burton, Telehealth Program Manager, KentuckyOne Health, Lexington; Chair, Kentucky Teleheath
5/1/2017. Medicare Coverage Guidelines for DSMT and MNT Telehealth. Telehealth Defined
 Medicare Coverage Guidelines for DSMT and MNT Telehealth Mary Ann Hodorowicz, RDN, MBA, CDE Certified Endocrinology Coder Mary Ann Hodorowicz Consulting, LLC 4-30-17 MEDICARE DSMT - MNT TELEHEALH KEY TOPICS
Medicare Coverage Guidelines for DSMT and MNT Telehealth Mary Ann Hodorowicz, RDN, MBA, CDE Certified Endocrinology Coder Mary Ann Hodorowicz Consulting, LLC 4-30-17 MEDICARE DSMT - MNT TELEHEALH KEY TOPICS
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents. Payment Model
 Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through Telemedicine
 PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
PACAH 2018 Spring Conference John Whitman, MBA, NHA The Wharton School Tapestry TeleHealth The TRECS Institute Why Every SNF Should Be Offering Telemedicine For Its Residents or Transforming SNF Care Through
Project: Telemedicine Engaging Your Providers in Your Telehealth Development and Program
 Project: Engaging Your Providers in Your Telehealth Development and Program Presented by: James Dunnick, MD, FACC, CHCQM, CPC, CMDP - The Dunnick Group, LLC Learning Outcome Standard: This program is based
Project: Engaging Your Providers in Your Telehealth Development and Program Presented by: James Dunnick, MD, FACC, CHCQM, CPC, CMDP - The Dunnick Group, LLC Learning Outcome Standard: This program is based
MEDICAL POLICY No R2 TELEMEDICINE
 Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Potentially Avoidable Hospitalizations among Dual Eligible Beneficiaries in Medicaid Home and Community-Based Services Waivers
 Potentially Avoidable Hospitalizations among Dual Eligible Beneficiaries in Medicaid Home and Community-Based Services Waivers Edith G Walsh, PhD Joshua Wiener, PhD Marc Freiman, PhD Susan Haber, PhD Arnold
Potentially Avoidable Hospitalizations among Dual Eligible Beneficiaries in Medicaid Home and Community-Based Services Waivers Edith G Walsh, PhD Joshua Wiener, PhD Marc Freiman, PhD Susan Haber, PhD Arnold
MEDICAL POLICY No R1 TELEMEDICINE
 Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
THE TELEMEDICINE MARKET LANDSCAPE
 How Telehealth is Changing the Care Provided to Patients Anne Cadwell, The Permanente Medical Group THE TELEMEDICINE MARKET LANDSCAPE Approximately 1 million virtual doctor visits in the U.S. in 2015 1
How Telehealth is Changing the Care Provided to Patients Anne Cadwell, The Permanente Medical Group THE TELEMEDICINE MARKET LANDSCAPE Approximately 1 million virtual doctor visits in the U.S. in 2015 1
Telemedicine and Fair Market Value What You Need to Know
 Telemedicine and Fair Market Value What You Need to Know By Chris W. David, CPA/ABV, ASA August, 2017 Telemedicine (also known as telehealth) is a rapidly-evolving trend in the healthcare delivery space
Telemedicine and Fair Market Value What You Need to Know By Chris W. David, CPA/ABV, ASA August, 2017 Telemedicine (also known as telehealth) is a rapidly-evolving trend in the healthcare delivery space
Telemedicine Policy Annual Approval Date
 Policy Number 2017R0046A Telemedicine Policy Annual Approval Date 7/13/2016 Approved By REIMBURSEMENT POLICY CMS-1500 Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You
Policy Number 2017R0046A Telemedicine Policy Annual Approval Date 7/13/2016 Approved By REIMBURSEMENT POLICY CMS-1500 Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You
Account Management, Coding, Customer Service, Legal, Medical Management, Finance, Claims, Underwriting, Network Management
 DEPARTMENT: Coding Reimbursement APPROVED DATE: POLICY DESCRIPTION: Telemedicine/Telehealth/Telecommunications/Televideo EFFECTIVE DATE: 6-24-04 PAGE: 1 of 4 REPLACES POLICY DATED: REFERENCE NUMBER: P-30
DEPARTMENT: Coding Reimbursement APPROVED DATE: POLICY DESCRIPTION: Telemedicine/Telehealth/Telecommunications/Televideo EFFECTIVE DATE: 6-24-04 PAGE: 1 of 4 REPLACES POLICY DATED: REFERENCE NUMBER: P-30
The Telemedicine Opportunity. Presented By: Marybeth McCall, MD
 The Telemedicine Opportunity Presented By: Marybeth McCall, MD 1962 Episode of the The Jetsons Presentation Objectives Identify telemedicine utilization projections Describe New York s Telemedicine Mandate
The Telemedicine Opportunity Presented By: Marybeth McCall, MD 1962 Episode of the The Jetsons Presentation Objectives Identify telemedicine utilization projections Describe New York s Telemedicine Mandate
Telemedicine and Telehealth Services
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Telemedicine and Telehealth Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 8 P U B L I S H E D : J A N U A R Y 1
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Telemedicine and Telehealth Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 8 P U B L I S H E D : J A N U A R Y 1
TELEMEDICINE POLICY. Policy Number: ADMINISTRATIVE T0 Effective Date: January 1, 2018
 TELEMEDICINE POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: ADMINISTRATIVE 114.28 T0 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 APPLICABLE LINES
TELEMEDICINE POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: ADMINISTRATIVE 114.28 T0 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 APPLICABLE LINES
REVISION DATE: FEBRUARY
 Mary Ann Hodorowicz, MBA, RDN CDE, CEC, Owner, Mary Ann Hodorowicz Consulting LLC, Palos Heights, IL Coverage: In-Person Payable Places of Services Excluded Places for Part B Payment Excluded Places: 0
Mary Ann Hodorowicz, MBA, RDN CDE, CEC, Owner, Mary Ann Hodorowicz Consulting LLC, Palos Heights, IL Coverage: In-Person Payable Places of Services Excluded Places for Part B Payment Excluded Places: 0
Telemedicine Policy. Approved By 4/08/2015
 Telemedicine Policy Policy Number 2016R0046B Annual Approval Date 4/08/2015 Approved By Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are responsible for submission
Telemedicine Policy Policy Number 2016R0046B Annual Approval Date 4/08/2015 Approved By Payment Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are responsible for submission
APNP Hospitalist Program
 APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital. Ministry Health Care. Program Objectives. Catholic Health Assembly June 23, 2014
 APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
APNP Hospitalist Program Ministry Eagle River Memorial Hospital Catholic Health Assembly June 23, 2014 Ministry Health Care An integrated Catholic Health Care system with a broad geographic footprint covering
Telemedicine: Improving Access to Specialty Care in Wisconsin s Rural Communities
 Telemedicine: Improving Access to Specialty Care in Wisconsin s Rural Communities David Guggenbuehl, RN, MBA, Director Jessica Miller, RN, Telemedicine Program Manager Department of Regional Services and
Telemedicine: Improving Access to Specialty Care in Wisconsin s Rural Communities David Guggenbuehl, RN, MBA, Director Jessica Miller, RN, Telemedicine Program Manager Department of Regional Services and
Telehealth and Telemedicine Policy
 Telehealth and Telemedicine Policy Policy Number Annual Approval Date 7/11/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Telehealth and Telemedicine Policy Policy Number Annual Approval Date 7/11/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011
 PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
Telehealth and Telemedicine Policy Annual Approval Date
 Policy Number Telehealth and Telemedicine Policy Annual Approval Date 04/12/2017 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Policy Number Telehealth and Telemedicine Policy Annual Approval Date 04/12/2017 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Telehealth and Telemedicine Policy
 Reimbursement Policy CMS 1500 Telehealth and Telemedicine Policy Policy Number 2018R0046B Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT
Reimbursement Policy CMS 1500 Telehealth and Telemedicine Policy Policy Number 2018R0046B Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT
HR Telehealth Enhancement Act of 2015
 HR 2066 - Telehealth Enhancement Act of 2015 Rep. Harper (R-MS), Rep. Thompson (D-CA), Rep. Black (R-TN) & Rep. Welch (D-VT) Author Intent: To promote and expand telehealth application under Medicare and
HR 2066 - Telehealth Enhancement Act of 2015 Rep. Harper (R-MS), Rep. Thompson (D-CA), Rep. Black (R-TN) & Rep. Welch (D-VT) Author Intent: To promote and expand telehealth application under Medicare and
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL
 TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
19 th Annual Western Regional Conference Women in Government May 21, 2016 Seattle, WA
 TELE TODAY 19 th Annual Western Regional Conference Women in Government May 21, 2016 Seattle, WA 877 707 7172 cchpca.org Mei Wa Kwong, JD Senior Policy Associate & Project Director DISCLAIMERS Any information
TELE TODAY 19 th Annual Western Regional Conference Women in Government May 21, 2016 Seattle, WA 877 707 7172 cchpca.org Mei Wa Kwong, JD Senior Policy Associate & Project Director DISCLAIMERS Any information
Opportunities to Leverage Telehealth Within Your ACO Strategy
 Opportunities to Leverage Telehealth Within Your ACO Strategy Shawn Valenta RRT, MHA Administrator of Telehealth Center for Telehealth Phillip Warr, MD Interim Chief Medical Officer Case Management and
Opportunities to Leverage Telehealth Within Your ACO Strategy Shawn Valenta RRT, MHA Administrator of Telehealth Center for Telehealth Phillip Warr, MD Interim Chief Medical Officer Case Management and
What is Telemedicine and How is It Being Used?
 What is Telemedicine and How is It Being Used? March 14, 2018 Presented by: Attorney Karina P. Gonzalez Florida Healthcare Law Firm www.floridahealthcarelawfirm.com 2016 The Law Offices of Jeff Cohen,
What is Telemedicine and How is It Being Used? March 14, 2018 Presented by: Attorney Karina P. Gonzalez Florida Healthcare Law Firm www.floridahealthcarelawfirm.com 2016 The Law Offices of Jeff Cohen,
Telehealth: An Introduction to Implementation and Policy Considerations. Angela Evatt, M.A., M.P.P
 Telehealth: An Introduction to Implementation and Policy Considerations Angela Evatt, M.A., M.P.P Overview What is telehealth, how can it be used in care delivery, and what does it aim to accomplish? Value
Telehealth: An Introduction to Implementation and Policy Considerations Angela Evatt, M.A., M.P.P Overview What is telehealth, how can it be used in care delivery, and what does it aim to accomplish? Value
Provider Handbooks. Telecommunication Services Handbook
 Provider Handbooks December 2016 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid under contract with the Texas Health
Provider Handbooks December 2016 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid under contract with the Texas Health
Aligned TeleHealth, Inc. On-site Staffing & TelePsychiatry
 Aligned TeleHealth, Inc. On-site Staffing & TelePsychiatry Aligned s History Dr. Nitin Nanda, P.C. Founded in 2000 Founded as a Private Psychiatry Practice in Los Angeles by Dr. Nitin Nanda upon Completing
Aligned TeleHealth, Inc. On-site Staffing & TelePsychiatry Aligned s History Dr. Nitin Nanda, P.C. Founded in 2000 Founded as a Private Psychiatry Practice in Los Angeles by Dr. Nitin Nanda upon Completing
Telehealth and Telemedicine Policy
 Reimbursement Policy CMS 1500 Telehealth and Telemedicine Policy Policy Number 2018R0046J Annual Approval Date 7/11/2018 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT
Reimbursement Policy CMS 1500 Telehealth and Telemedicine Policy Policy Number 2018R0046J Annual Approval Date 7/11/2018 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT
2017 Telehealth Policy for the National Rural Health Association
 2017 Telehealth Policy for the National Rural Health Association Introduction Telemedicine has been around for decades, but is just now really becoming mainstream with the congruence of technology, lower
2017 Telehealth Policy for the National Rural Health Association Introduction Telemedicine has been around for decades, but is just now really becoming mainstream with the congruence of technology, lower
19/09/2017. Telehealth Legal and Regulatory Issues in Colorado and Beyond. Nathaniel Lacktman, October 2017
 Telehealth Legal and Regulatory Issues in Colorado and Beyond Nathaniel Lacktman, Esq. @Lacktman October 2017 1 2 1 Licensing 3 Licensing Physician offering care via telemedicine is subject to licensure
Telehealth Legal and Regulatory Issues in Colorado and Beyond Nathaniel Lacktman, Esq. @Lacktman October 2017 1 2 1 Licensing 3 Licensing Physician offering care via telemedicine is subject to licensure
FACT SHEET Congressional Bill
 HR 3306 - Telehealth Enhancement Act of 2013 Rep. Gregg Harper (R-MS) Purpose: To promote and expand the application of telehealth under Medicare and other Federal health care programs. Positive Incentives
HR 3306 - Telehealth Enhancement Act of 2013 Rep. Gregg Harper (R-MS) Purpose: To promote and expand the application of telehealth under Medicare and other Federal health care programs. Positive Incentives
Telehealth. Clinical Applications 6/28/2011 TELEHEALTH UPDATE: MONTANA AND BEYOND
 TELEHEALTH UPDATE: MONTANA AND BEYOND Telehealth Telehealth is the delivery of healthrelated services via telecommunications technologies Clinical Applications Allergy Cardiology * Dermatology Oncology
TELEHEALTH UPDATE: MONTANA AND BEYOND Telehealth Telehealth is the delivery of healthrelated services via telecommunications technologies Clinical Applications Allergy Cardiology * Dermatology Oncology
LEGAL CONSIDERATIONS FOR FQHCS: REIMBURSEMENT FOR TELEMEDICINE SERVICES
 LEGAL CONSIDERATIONS FOR FQHCS: REIMBURSEMENT FOR TELEMEDICINE SERVICES SOUTH CAROLINA PRIMARY HEALTH CARE ASSOCIATION SOUTH CAROLINA PRIMARY HEALTH CARE ASSOCIATION 2017 STATE POLICY & ISSUES FORUM Jeanne
LEGAL CONSIDERATIONS FOR FQHCS: REIMBURSEMENT FOR TELEMEDICINE SERVICES SOUTH CAROLINA PRIMARY HEALTH CARE ASSOCIATION SOUTH CAROLINA PRIMARY HEALTH CARE ASSOCIATION 2017 STATE POLICY & ISSUES FORUM Jeanne
Corporate Reimbursement Policy Telehealth
 Corporate Reimbursement Policy Telehealth File Name: Origination: Last Review Next Review: telehealth 11/1997 12/2017 12/2018 Description Telehealth is a potentially useful tool that, if employed appropriately,
Corporate Reimbursement Policy Telehealth File Name: Origination: Last Review Next Review: telehealth 11/1997 12/2017 12/2018 Description Telehealth is a potentially useful tool that, if employed appropriately,
Telehealth. Administrative Process. Coverage. Indications that are covered
 Telehealth These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information
Telehealth These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information
The Future of Post-Acute Care Under Value-Based Payment
 The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
The Future of Post-Acute Care Under Value-Based Payment Robert Mechanic, MBA Brandeis University Northeast Home Health Leadership Summit January 22, 2015 Medicare Margins for Freestanding Home Health Agencies
WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH
 WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH I. CURRENT LEGISLATION AND REGULATIONS Telehealth technology has the potential to improve access to a broader range of health care services in rural and
WHITE PAPER #2: CASE STUDY ON FRONTIER TELEHEALTH I. CURRENT LEGISLATION AND REGULATIONS Telehealth technology has the potential to improve access to a broader range of health care services in rural and
Medicaid Program Administrator: Bureau for Medical Services, under the West Virginia Dept. of Health and Human Resources
 West Virginia Medicaid Program: West Virginia Medicaid Medicaid Program Administrator: Bureau for Medical Services, under the West Virginia Dept. of Health and Human Resources Regional Telehealth Resource
West Virginia Medicaid Program: West Virginia Medicaid Medicaid Program Administrator: Bureau for Medical Services, under the West Virginia Dept. of Health and Human Resources Regional Telehealth Resource
Chapter 7 Section 22.1
 TRICARE Policy Manual 6010.57-M, February 1, 2008 Medicine Chapter 7 Section 22.1 Issue Date: April 17, 2003 Authority: 32 CFR 199.4 and 32 CFR 199.14 1.0 DESCRIPTION 1.1 refers to the use of information
TRICARE Policy Manual 6010.57-M, February 1, 2008 Medicine Chapter 7 Section 22.1 Issue Date: April 17, 2003 Authority: 32 CFR 199.4 and 32 CFR 199.14 1.0 DESCRIPTION 1.1 refers to the use of information
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Outcomes Reporting: Be Ready to Negotiate with a Hospital
 Outcomes Reporting: Be Ready to Negotiate with a Hospital Tanya Procell, RN ADN Director of Clinical Services Provider Professional Services Teresa Chase President & CEO American HealthTech July 24 th,
Outcomes Reporting: Be Ready to Negotiate with a Hospital Tanya Procell, RN ADN Director of Clinical Services Provider Professional Services Teresa Chase President & CEO American HealthTech July 24 th,
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Texas Medicaid. Provider Procedures Manual. Provider Handbooks. Telecommunication Services Handbook
 Texas Medicaid Provider Procedures Manual Provider Handbooks December 2017 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid
Texas Medicaid Provider Procedures Manual Provider Handbooks December 2017 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid
Telehealth 101: Key Concepts for Starting and Sustaining
 Telehealth 101: Key Concepts for Starting and Sustaining Telehealth 101 Danielle Louder Program Director NETRC, MCD Public Health Andrew Solomon, MPH Project Manager NETRC Nina Antoniotti, PhD, MBA, RN
Telehealth 101: Key Concepts for Starting and Sustaining Telehealth 101 Danielle Louder Program Director NETRC, MCD Public Health Andrew Solomon, MPH Project Manager NETRC Nina Antoniotti, PhD, MBA, RN
Readmissions Moving beyond blame to fill the patient needs. Jackie Conrad RN, MBA, RCC Cynosure Health
 Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
Telestroke Alaska Evidence Based Care Across the Great Frontier
 Telestroke Alaska Evidence Based Care Across the Great Frontier Presented by Dr. Christie Artuso Director, Neuroscience Services Providence Alaska Medical Center 1 2 Financial Disclosures I am a speaker
Telestroke Alaska Evidence Based Care Across the Great Frontier Presented by Dr. Christie Artuso Director, Neuroscience Services Providence Alaska Medical Center 1 2 Financial Disclosures I am a speaker
Telemedicine Policy. 7/12/2017 Approved By
 Telemedicine Policy Policy Number 2018R0046A Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are responsible for submission
Telemedicine Policy Policy Number 2018R0046A Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY You are responsible for submission
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
Why Telehealth, Why Now?
 Promoting Access to Quality Care Through Technology and Innovation Why Telehealth, Why Now? Industry Webinar November 9, 2016 Panelists Bill Boling Owner/Principal Boling & Company bill@bolingandcompany.com
Promoting Access to Quality Care Through Technology and Innovation Why Telehealth, Why Now? Industry Webinar November 9, 2016 Panelists Bill Boling Owner/Principal Boling & Company bill@bolingandcompany.com
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Providing and Billing Medicare for Transitional Care Management
 PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
PYALeadership Briefing Providing and Billing Medicare for Transitional Care Management Updated November 2014 2014 Pershing Yoakley & Associates, PC (PYA). No portion of this white paper may be used or
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
H.R MEDICARE TELEHEALTH PARITY ACT OF 2017
 FACT SHEET CENTER FOR CONNECTED HEALTH POLICY The Federally Designated National Telehealth Policy Resource Center Info@cchpca.org 877-707-7172 H.R. 2550 MEDICARE TELEHEALTH PARITY ACT OF 2017 SPONSORS:
FACT SHEET CENTER FOR CONNECTED HEALTH POLICY The Federally Designated National Telehealth Policy Resource Center Info@cchpca.org 877-707-7172 H.R. 2550 MEDICARE TELEHEALTH PARITY ACT OF 2017 SPONSORS:
Why try to reduce hospitalizations? How many are avoidable?
 Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Joseph G. Ouslander, MD Professor of Clinical Biomedical Science Associate Dean for Geriatric Programs Charles E. Schmidt College of Biomedical Science Professor (Courtesy), Christine E. Lynn College of
Telehealth Legal and Compliance Issues. Nathaniel Lacktman, Anna Whites, Esq.
 Telehealth Legal and Compliance Issues Nathaniel Lacktman, Esq. @Lacktman Anna Whites, Esq. Anna Whites Law Office Attorney Advertising Prior results do not guarantee a similar outcome Models used are
Telehealth Legal and Compliance Issues Nathaniel Lacktman, Esq. @Lacktman Anna Whites, Esq. Anna Whites Law Office Attorney Advertising Prior results do not guarantee a similar outcome Models used are
08/07/2015. Next Generation ACO Model. What is an ACO? Preliminary Beneficiary Engagement Timeline
 Next Generation ACO Model National Training Program RO V and RO VII St. Louis August 10-11, 2015 What is an ACO? Accountable Care Organizations (ACOs) are groups of doctors, hospitals, and other health
Next Generation ACO Model National Training Program RO V and RO VII St. Louis August 10-11, 2015 What is an ACO? Accountable Care Organizations (ACOs) are groups of doctors, hospitals, and other health
The Telemedicine Train is Leaving the Station: Don t be left behind
 The heart and science of medicine. UVMHealth.org The Telemedicine Train is Leaving the Station: Don t be left behind Prepared by Norman Ward MD, Chief Medical Officer, OneCare Vermont Natasha Wither, DO,
The heart and science of medicine. UVMHealth.org The Telemedicine Train is Leaving the Station: Don t be left behind Prepared by Norman Ward MD, Chief Medical Officer, OneCare Vermont Natasha Wither, DO,
Telehealth And Telemedicine
 Manual: Policy Title: Reimbursement Policy Telehealth And Telemedicine Section: Medicine Subsection: None Date of Origin: 1/1/2010 Policy Number: RPM052 Last Updated: 3/17/2018 Last Reviewed: 3/17/2018
Manual: Policy Title: Reimbursement Policy Telehealth And Telemedicine Section: Medicine Subsection: None Date of Origin: 1/1/2010 Policy Number: RPM052 Last Updated: 3/17/2018 Last Reviewed: 3/17/2018
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
3/27/2017. Historical Perspective. Innovative Model of Healthcare Delivery Using Telemedicine
 Innovative Model of Healthcare Delivery Using Telemedicine Vinita Kamath MS RDN MHA Clinical Director, Nutrition Therapy Cincinnati Children s Hospital Medical Center CNM Conference March 20, 2017 Outline
Innovative Model of Healthcare Delivery Using Telemedicine Vinita Kamath MS RDN MHA Clinical Director, Nutrition Therapy Cincinnati Children s Hospital Medical Center CNM Conference March 20, 2017 Outline
Telehealth Reimbursement Policy in
 Telehealth Reimbursement Policy in New York State Greater New York Hospital Association Telehealth Webinar Series July 11, 2016 July 2016 2 Agenda Telehealth NY State Telehealth Parity Statutory Changes
Telehealth Reimbursement Policy in New York State Greater New York Hospital Association Telehealth Webinar Series July 11, 2016 July 2016 2 Agenda Telehealth NY State Telehealth Parity Statutory Changes
TELEHEALTH REIMBURSEMENT
 FACT SHEET CENTER FOR CONNECTED HEALTH POLICY The Federally Designated National Telehealth Policy Resource Center Info@cchpca.org 877-707-7172 TELEHEALTH REIMBURSEMENT Telehealth is a well-established
FACT SHEET CENTER FOR CONNECTED HEALTH POLICY The Federally Designated National Telehealth Policy Resource Center Info@cchpca.org 877-707-7172 TELEHEALTH REIMBURSEMENT Telehealth is a well-established
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Telemedicine. Important Information. Telemedicine 5/6/2016. Lauren Prew
 Telemedicine Lauren Prew Important Information This presentation is similar to any other seminar designed to provide general information on pertinent legal topics. The statements made and any materials
Telemedicine Lauren Prew Important Information This presentation is similar to any other seminar designed to provide general information on pertinent legal topics. The statements made and any materials
Telehealth: Frequently Asked Questions
 Telehealth: Frequently Asked Questions WHAT IS TELEHEALTH? Telehealth is the use of electronic information and telecommunications technology to support: THE DELIVERY OF HEALTH CARE PATIENT AND PROFESSIONAL
Telehealth: Frequently Asked Questions WHAT IS TELEHEALTH? Telehealth is the use of electronic information and telecommunications technology to support: THE DELIVERY OF HEALTH CARE PATIENT AND PROFESSIONAL
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Telehealth. Telehealth? 6/1/2016. A tool for enhancing health care, communication and information.
 Telehealth June 2016 Telehealth? A tool for enhancing health care, public Providing/receiving health, and health education health delivery care services and support, at using a distance. electronic communication
Telehealth June 2016 Telehealth? A tool for enhancing health care, public Providing/receiving health, and health education health delivery care services and support, at using a distance. electronic communication
Telemedicine and Health Reform. Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center
 Telemedicine and Health Reform Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center 1 telehealthresourcecenters.org Links to all TRCs National Webinar Series Reimbursement,
Telemedicine and Health Reform Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center 1 telehealthresourcecenters.org Links to all TRCs National Webinar Series Reimbursement,
Chapter 7 Section 22.1
 Medicine Chapter 7 Section 22.1 Issue Date: April 17, 2003 Authority: 32 CFR 199.4 and 32 CFR 199.14 Copyright: CPT only 2006 American Medical Association (or such other date of publication of CPT). All
Medicine Chapter 7 Section 22.1 Issue Date: April 17, 2003 Authority: 32 CFR 199.4 and 32 CFR 199.14 Copyright: CPT only 2006 American Medical Association (or such other date of publication of CPT). All
Telehealth in Alaska. Cindy Roleff, MS, BSN, RN-BC Telehealth Program Development Manager AFHCAN / ANTHC
 Telehealth in Alaska Cindy Roleff, MS, BSN, RN-BC Telehealth Program Development Manager AFHCAN / ANTHC Why Telehealth? Patient Empowers them with additional choices Satisfaction Decreases disparities
Telehealth in Alaska Cindy Roleff, MS, BSN, RN-BC Telehealth Program Development Manager AFHCAN / ANTHC Why Telehealth? Patient Empowers them with additional choices Satisfaction Decreases disparities
Telemedicine Compliance Maximizing Patient Care & ROI While Minimizing Legal Risks
 Live tweet - #telehealth2016 Telemedicine Compliance Maximizing Patient Care & ROI While Minimizing Legal Risks Mei Wa Kwong, JD Senior Policy Associate & Project Director Center for Connected Health Policy
Live tweet - #telehealth2016 Telemedicine Compliance Maximizing Patient Care & ROI While Minimizing Legal Risks Mei Wa Kwong, JD Senior Policy Associate & Project Director Center for Connected Health Policy
Legal Issues You Should Know April 25, 2018 In-House Counsel Conference
 1 TELEMEDICINE Legal Issues You Should Know April 25, 2018 In-House Counsel Conference Disclaimer: These materials and presentation are intended to be a general and brief summary of the law. This is not
1 TELEMEDICINE Legal Issues You Should Know April 25, 2018 In-House Counsel Conference Disclaimer: These materials and presentation are intended to be a general and brief summary of the law. This is not
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
I. LIVE INTERACTIVE TELEDERMATOLOGY
 Position Statement on Teledermatology (Approved by the Board of Directors: February 22, 2002; Amended by the Board of Directors: May 22, 2004; November 9, 2013; August 9, 2014; May 16, 2015; March 7, 2016)
Position Statement on Teledermatology (Approved by the Board of Directors: February 22, 2002; Amended by the Board of Directors: May 22, 2004; November 9, 2013; August 9, 2014; May 16, 2015; March 7, 2016)
LOUISIANA MEDICAID PROGRAM ISSUED: 06/09/17 REPLACED: CHAPTER 2: BEHAVIORAL HEALTH SERVICES SECTION 2.2: OUTPATIENT SERVICES PAGE(S) 8
 8") Licensed Practitioner Outpatient Therapy includes: Individual; Family; Group; Outpatient psychotherapy; Mental health assessment; Evaluation; Testing; Medication management; Psychiatric evaluation; Medication
Licensed Practitioner Outpatient Therapy includes: Individual; Family; Group; Outpatient psychotherapy; Mental health assessment; Evaluation; Testing; Medication management; Psychiatric evaluation; Medication
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
Admissions and Transitions Optimization Program. Nursing Facility and Practitioner Billing
 Admissions and Transitions Optimization Program Nursing Facility and Practitioner Billing November 2016 Contents Introduction... 4 Payment Reform... 5 Components... 5 Eligibility... 6 Long Term Care (LTC)
Admissions and Transitions Optimization Program Nursing Facility and Practitioner Billing November 2016 Contents Introduction... 4 Payment Reform... 5 Components... 5 Eligibility... 6 Long Term Care (LTC)
American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues. History of the Physician Fee Schedule
 American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues March 20-22, 2013 Baltimore, Maryland Sidney S. Welch, Esq. 1 History of the Physician Fee Schedule Prior to 1992,
American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues March 20-22, 2013 Baltimore, Maryland Sidney S. Welch, Esq. 1 History of the Physician Fee Schedule Prior to 1992,
CHRONIC CARE MANAGEMENT. A Guide to Medicare s New Move Toward Patient-Centric Care
 CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
CHRONIC CARE MANAGEMENT A Guide to Medicare s New Move Toward Patient-Centric Care The future of healthcare is here; Medicare has begun to shift away from fee-forservice care and move toward value based
Physician Quality Reporting System & VBPM, 2015
 Physician Quality Reporting System & VBPM, 2015 Andrew Bienstock Transformation Support Services Manager 1 Agenda 1. PQRS Penalty 2. PQRS Eligibility 3. PQRS Reporting Options 4. Value Based Payment Modifier
Physician Quality Reporting System & VBPM, 2015 Andrew Bienstock Transformation Support Services Manager 1 Agenda 1. PQRS Penalty 2. PQRS Eligibility 3. PQRS Reporting Options 4. Value Based Payment Modifier
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Expanding Urologic Practice Through Telehealth
 Expanding Urologic Practice Through Telehealth Great Lakes SUNA Chapter Spring Conference Chad Ellimoottil, MD, MS Assistant Professor of Urology Director of Telemedicine, Department of Urology ehealth
Expanding Urologic Practice Through Telehealth Great Lakes SUNA Chapter Spring Conference Chad Ellimoottil, MD, MS Assistant Professor of Urology Director of Telemedicine, Department of Urology ehealth
Telehealth and Children With Special Health Care Needs. Improving Access to Care and Care Coordination
 Telehealth and Children With Special Health Care Needs Improving Access to Care and Care Coordination Jacob Vigil, MSW Program Associate The Children s Partnership Mei Wa Kwong, JD Senior Policy Associate
Telehealth and Children With Special Health Care Needs Improving Access to Care and Care Coordination Jacob Vigil, MSW Program Associate The Children s Partnership Mei Wa Kwong, JD Senior Policy Associate
Creative Solutions to Challenging Access Issues. The State of Telehealth in Our Region
 Creative Solutions to Challenging Access Issues The State of Telehealth in Our Region Nebraska Hospital Association - October 25, 2017 Telehealth: Telemedicine Remote Monitoring Store-and-Forward Direct-to-Consumer/Primary
Creative Solutions to Challenging Access Issues The State of Telehealth in Our Region Nebraska Hospital Association - October 25, 2017 Telehealth: Telemedicine Remote Monitoring Store-and-Forward Direct-to-Consumer/Primary
Telemedicine Reimbursement. An Overview for Oregon
 Telemedicine Reimbursement An Overview for Oregon A Brief History - Medicare In 1997 the Balanced Budget Act first authorized Medicare to reimburse for telemedicine services Since 2000 there have been
Telemedicine Reimbursement An Overview for Oregon A Brief History - Medicare In 1997 the Balanced Budget Act first authorized Medicare to reimburse for telemedicine services Since 2000 there have been
TRANSFORMING HEALTH CARE WITH CONNECTED HEALTH TECHNOLOGY
 TRANSFORMING CARE WITH CONNECTED TECHNOLOGY TELE STATE TRENDS Florida Telehealth Advisory Council April 21, 2017 877-707-7172 cchpca.org Mario Gutierrez We are part of the Public Health Institute, an independent,
TRANSFORMING CARE WITH CONNECTED TECHNOLOGY TELE STATE TRENDS Florida Telehealth Advisory Council April 21, 2017 877-707-7172 cchpca.org Mario Gutierrez We are part of the Public Health Institute, an independent,