Improving Dementia Care and Reducing Unnecessary Use of Antipsychotic Medications in Nursing Homes
|
|
|
- Derek Brooks
- 6 years ago
- Views:
Transcription
1 1

2 Revision Date: August 2012 SMART AIM Reduce the use of Atypical Anti-Psychotics (AAPs) in Nursing Facilities by 15% by 12/12 KEY DRIVER DIAGRAM - draft Project Name: NF AAP Utilization QI Project Team Leaders: Drs. Bonnie Burman -Kantor (ODA)& Mary Applegate (OHP) KEY DRIVERS Public Awareness Clinical Expertise tied to Quality Improvement Data Transparency & Feedback Special Populations INTERVENTIONS Launch public awareness and education campaign Engage stakeholders (NFs/associations, families, prescribers, community centers, AAAs, APS, social workers) to provide input into education materials & processes Include Prevention & alternative Strategies to AAPs Create common set of evidence-based clinician-driven guidelines for AAP use in this population, including stepdown therapy Disseminate & implement Best Practice guidelines for diagnosis & treatment of dementia Provide practice alerts to prescribers in EHRs/Pharmacy Engage clinicians & NFs in proven QI processes Establish Collaborative to support QI, CME in conjunction with academic & professional organizations including Nurses and mid-level providers Include pharmacists, as required team member Telemedicine, innovative IT applications Workforce development Common data set (merge Medicaid/Medicare/MDS) Monthly meaningful prescriber & NF feedback & profiling Engage DUR & Pharmacy Benefit Managers Public reporting, prior authorization requirements Special attention to those with Dementia and Mental Health diagnoses Target High volume prescribers & providers Target Geographic trends GLOBAL AIM Improve the appropriate and effective use of psychotropic medications for elderly adults as part of the holistic strategy to improve health outcomes Family Centered Care Payment & Policy Access to non-medication alternatives Address NF culture, strengths & challenges Improve Care coordination & collaborative community referrals Begin Informed consent process with joint decision making Family mentorship Routine behavioral assessment and follow up Amend quality incentive program Tie quality to licensure requirements Improve availability, access & knowledge of alternatives Promote early screening and referral, routine assessment IT solutions Pharma marketing requirements to include non-drug options, Improving Dementia Care and Reducing Unnecessary Use of Antipsychotic Medications in Nursing Homes Alice Bonner, PhD, RN Division of Nursing Homes Center for Clinical Standards and Quality Centers for Medicare & Medicaid Services December 17 h,

3 Why this Initiative? Why Now? 5 Improving Dementia Care - Background High prevalence rates of antipsychotic drug use in nursing home residents have been reported in several studies. Much of the use is in residents with a diagnosis of dementia According to CMS s QM/QI report, between July and September 2010, 39.4% of nursing home residents nationwide who had cognitive impairment and behavioral issues but no diagnosis of psychosis or related conditions received antipsychotic drugs In addition to dangers associated with antipsychotic medications for the elderly, it can also be expensive to consumers and Medicare. Atypical antipsychotic drugs cost more than $13 billion in 2007 nearly 5% of all U.S. drug expenditures 6 3
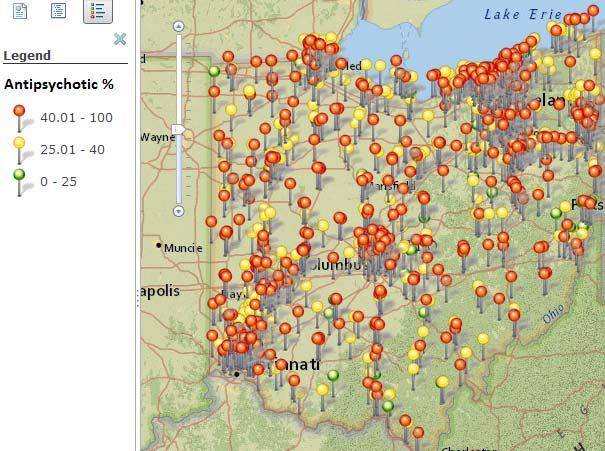
 The likelihood of a resident to receive an antipsychotic medication was related to the facility-level antipsychotic")
4 Antipsychotic Medications in Nursing Homes Prescribing Issues In one study, 17.2% had daily doses exceeding recommended levels. And 17.6% had both inappropriate indications and high dosing (Briesacher, 2005) The likelihood of a resident to receive an antipsychotic medication was related to the facility-level antipsychotic prescribing rate, even after adjustment for clinical and socio-demographic characteristics (Chen et al., 2010) 7 Antipsychotic Medication Use Varies by State Source: MDS National Quality Indicator System
5 CMS National Partnership to Improve Dementia Care CMS developed a national partnership to improve dementia care and optimize behavioral health. By improving dementia care and person-centered, individualized interventions for behavioral health in nursing homes, CMS hopes to reduce unnecessary antipsychotic medication use in nursing homes and eventually other care settings as well. While antipsychotic medications are the initial focus of the partnership, CMS recognizes that attention to other potentially harmful medications is also an important part of this initiative. 9 Partnership Overview The Partnership promotes the three R s Rethink rethink our approach to dementia care Reconnect reconnect with residents via person-centered care practices Restore restore good health and quality of life 5
6 11 CMS Updates on the National Initiative: A Public-Private Partnership Proactive efforts include collaboration with partner organizations around: provider and prescriber training surveyor training, review of surveyor guidance, protocols and challenges related to assessing compliance in these areas research quality measurement, public reporting communication strategies such as local and national conference presentations, press releases development of dissemination strategies in states and regions and a sustainable national plan for ongoing monitoring and evaluation of these issues 12 6
7 Partnership Overview Multidimensional approach includes: Public Reporting Rates of nursing homes antipsychotic drug use available on Nursing Home Compare (long-stay prevalence; short-stay incidence) First year goal: reduce prevalence rate of antipsychotic drug use in long-stay nursing home residents by 15% by end of 2012 Nursing Home Compare Quality Measures Measure: Percentage of Long-Stay Residents Who are Receiving Antipsychotic Medication Description: The percentage of long-stay residents (>100 cumulative days in the nursing facility) who are receiving antipsychotic medication Measure: Percentage of Short- Stay Patients Who Have Antipsychotics Started Incidence Description: The percentage of short-stay residents (<=100 cumulative days in the nursing facility) who have antipsychotic medications started after admission 14 7
8 Partnership Overview Research Conduct research to better understand how the team makes decisions to use antipsychotic drugs in residents with dementia Study factors that influence prescribing patterns and practices Implement approaches to improve overall health of residents with dementia based on results of study Facilitate sharing of research findings; research workgroup New grants since partnership began Commonwealth Fund small grant to compile evidence-based research on use of non-pharmacological approaches in persons with dementia to assist providers in accessing evidence-based information on these approaches and implementing them in practice (develop a toolkit) Review deficiency citations at F329 to better understand how surveyors cite noncompliance related to unnecessary antipsychotic medication use Partnership Overview Training Hand in Hand DVD series. Provides direct care workers with training that emphasizes person-centered care, prevention of abuse and individualized approaches to care of persons with dementia (FREE. Distributed to all nursing homes in December 2012; many partner organizations to receive soon as well) One Stop Shopping Multiple training programs/materials available for providers, clinicians, consumers and surveyors on Advancing Excellence website and several association, university websites as well. Many thanks to Miranda Meadows and Kris Mattivi at CFMC and Michele Laughman at CMS Site is dynamic new information added frequently 8
9
10
11
12 Partnership Overview Multidimensional approach includes: Partnerships and State-based Coalitions Engage the ongoing commitment and partnership of stakeholders including state survey agency and Medicaid agencies, provider groups, resident advocates, professional associations, QIOs, LANES, consumer groups, ombudsman and others Involve residents and families ( Nothing about us, Without us! ) Create or support existing individual state coalitions, LANES or collaboratives that will identify and spread best practices Amazing, grass roots work in many states already Frequently Asked Questions Is there an expectation that every facility will reduce the rate of antipsychotic use by 15%? Answer: No. That is a national target. Some facilities will reduce their rate by more than that, some less. There may be valid reasons why some facilities have higher than average rates of antipsychotic use, based on their population Should pharmacists change their approach to recommending gradual dose reductions (GDR) in stable residents? Answer: the approach has always been and should continue to be that the clinical team documents a systematic process for evaluating the ongoing use of the medication and clinical rationale for why a stable resident should remain on an antipsychotic. A conversation with the physician or prescriber is often helpful. Surveyors will ask about individualized approaches other than medication as well
13 The Survey Process Will surveyors be looking more intensively at persons with dementia who are on antipsychotics? Surveyor guidance has been revised with input from several professional associations (AHCA, AMDA, ASCP, NADONA, AAGP, AGS and others), advocates and other stakeholders. Surveyors will include residents with dementia who are receiving an antipsychotic in their sample. Surveyors will look for the same systematic process that providers and practitioners should be using to determine the underlying causes of behaviors in persons with dementia. Surveyors will look to see that care plans include plans for residents with dementia that address behaviors, include input from the resident (to the extent possible) and/or family or representative and that those plans are consistently carried out. Surveyors are looking for a systematic process to be evident and for that process to be followed for every resident 25 Systematic Process Get details about the patient's behavioral expressions of distress (nature, frequency, severity, and duration) and the risks of those behaviors, and discuss potential underlying causes with the care team and family Exclude potentially remediable causes of behaviors (such as delirium, infection or medications), and determine if symptoms are severe, distressing or risky enough to adversely affect the safety of residents 26 13
14 Systematic Process Try environmental and other approaches that attempt to understand and address behavior as a form of communication in persons with dementia, and modify the environment and daily routines to meet the person s needs. Assess the effects of any intervention (pharmacological or nonpharmacological) identify benefits and complications in a timely fashion. Adjust treatment accordingly. 27 Systematic Process For those residents for whom antipsychotic or other medications are warranted, use the lowest effective dose for the shortest possible duration, based on findings in the specific individual. Monitor for potential side effects, therapeutic benefit with respect to specific target symptoms/expressions of distress. Inadequate documentation: Behavior improved. Less agitated. No longer asking to go home. Include specifics, why they behaviors were harmful/dangerous/distressing and what the person is now able to do (positive) as a result of the intervention Try tapering the medication when symptoms have been stable or adjusting doses to obtain benefits with the lowest possible risk
15 The Survey Process Input from nursing assistants, nurses, social workers, therapists, family and other caregivers working closely with the resident is essential. Input from all three shifts and weekend caregivers is also important in telling the story. Surveyors will look at communication between shifts, between nurses and practitioners or prescribers. Surveyors will also look at whether medications prescribed by a covering practitioner in an urgent situation are reevaluated by the primary care team. Surveyors will look at whether or not other psychopharmacologicals are prescribed if/when antipsychotic medications are discontinued or reduced. 29 Clinical Teams are Asking Questions such as: How do I handle this situation? How do I find out about person-centered approaches and how do we train our staff? Should we use a medication? If so - Which medications should we use? How much should we give, and how often? How do we know whether those medications are working or causing complications? When should we start or stop those medications? 30 15
16 How can we reduce our rate of antipsychotic use in persons with dementia Look at the big picture consider dementia care principles Focus on each individual resident and use a careful, systematic process to evaluate his/her needs. During off-site preparation, surveyors will review the antipsychotic rate in the facility. Surveyors will ask staff about the facility s approach to persons with dementia. QIOs will be increasingly involved in phase II of the current (10 th ) SOW. 31 How can we reduce our rate of antipsychotic use in persons with dementia Consider forming a behavioral health committee or team for dementia care practices. Include the consultant pharmacist, medical director, administrator, DON, recreational and other therapy staff, social worker, direct care partners/staff (CNAs) Also include behavioral health specialists/consultants if possible Resident, family members when facility policies/practices (not individuals) are being discussed Begin by looking at each resident with dementia who is on an antipsychotic and considering the case in detail. Look for underlying causes of the behaviors. Consider whether a GDR may be indicated and communicate with the practitioner. Tools on AE. National experts are available
17 How can we reduce our rate of antipsychotic use in persons with dementia Use this team to examine nursing home practices related to dementia care and behavioral health Consider programs such as Hand in Hand Produced by CMS, this is a six-hour series of DVDs with training for nursing assistants on abuse prevention and dementia care. OASIS, Habilitation therapy, others Contact your QIO 33 CMS Challenge to Our Partners Share your existing work/resources with national leadership Curricula on dementia, behavioral health, reducing unnecessary medications Consider ways to communicate with members and encourage engagement around this issue Work with CMS to sustain and expand local, state, regional and national workgroups or collaboratives around this issue 34 17
18 Q&A, Discussion and Next Steps Set 2013 goals for the national initiative Continue engaging partners at the local, state, regional and national level Develop and refine quality measures Continue to conduct outreach to nursing homes 35 What if we don t have a lot of geriatric training or experience? HRSA funded GECs to enhance dementia training 36 18


19 Questions? Thank you! CMS staff can put you in touch with state coalition leads and state-level resources Alice Bonner Director, Division of Nursing Homes Survey and Certification Group Centers for Medicare & Medicaid Services 37 Partnership to Improve Dementia Care: The Role of Your Consultant Pharmacist Joseph G. Marek, RPh CGP FASCP Omnicare Clinical Services Clinical Manager, Northern & Central Ohio American Society of Consultant Pharmacists (ASCP) 38 Board of Directors 19
20 What Should You Expect from Your Consultant Pharmacist? Clinical and Regulatory Expertise Leadership and Support Education of the Multidisciplinary Team Resources and Tools Consultant Pharmacists Three Core Strengths: Knowledge and skills in geriatric pharmacotherapy Expertise in treating our frail seniors in the long term care setting or other settings Patient Advocates Protecting the health and quality of life of America s seniors through medication management 40 20
21 Consultant Pharmacists - Clinicians Consider the most appropriate and effective medication therapy for each resident Identify, resolve and prevent medication related problems Ensure regulatory compliance with SOM guidelines Provide medication utilization data, analysis & guidance to each facility 41 Leadership and Support Participation with the multidisciplinary team to achieve the mutual goal of enhancing the care and treatment of residents with dementia by providing: Collaboration in the medication management for each individual resident Guidance & participation in the Multidisciplinary Medication Management Meeting 21
22 Education for Multidisciplinary Team Antipsychotic Education through In Servicing: Considerations for Reducing and Eliminating Antipsychotic Medications for Behaviors in Elderly Nursing Home Residents with Dementia Non Pharmacological (non drug) interventions tip sheets The American Geriatrics Society s Guide to the Management of Psychotic Disorders and Neuropsychiatric Symptoms of Dementia in Older Patients, published in April, The AHRQ report Executive Summary: Off Label Use of Atypical Antipsychotics An Update. Education for Medical Director and Prescribing Physicians Reviewing the CMS Initiative and Regulatory Requirements through : SOM Guidance Clinical References or Research Prescriber Guide for Dose Reductions AMDA s Letter to Prescribers from Dr. Matthew Wayne, President AMDA 22
23 Treatment Algorithms Resources and Tools Reduction of Antipsychotic Medication in Dementia Residents Receiving for Behavioral Symptoms Multidisciplinary Assessment Tool Antipsychotic Use in Dementia Assessment Form Gradual Dose Reduction Tracking Report Documents indications for use, therapy start date, and next gradual dose reduction due date Algorithm for Reducing or Eliminating Antipsychotics for Residents with Behavioral Symptoms of Dementia Resident Receiving Antipsychotic for Behavioral Symptoms Assess ongoing use of non-pharmacologic interventions throughout process. Minimize use or discontinue use of medications with anticholinergic properties. Assess for depressive symptoms (PHQ-9 score on MDS 3.0) Assess for intercurrent illnesses that may be causing or contributing to behaviors (i.e. pain, constipation). Assess for condition that may have caused or contributed to behaviors that is now resolved (i.e. delirium due to UTI, etc.) Request further GDR or trial discontinuation in 3 4 months Yes GDR tolerated? No Yes GDR attempted? No Request GDR or trial discontinuation within 60 days of initiation or admission, or sooner (e.g. 3 4 weeks) if initiated to treat an acute problem (e.g. behaviors due to acute injury, infection, etc.) Monitor for behavioral symptoms and adverse medication effects. Request GDR attempt in 3 4 months if behaviors have improved or stabilized If antipsychotic GDR tolerated, request further GDR in 3 4 months. If symptoms re-emerge, assess effectiveness of non-pharmacologic interventions. If ineffective, recommend addition or dosage adjustment of adjunctive medication (e.g. antidepressant, etc.). Avoid recommending increase in antipsychotic dose if possible. If symptoms improve, consider antipsychotic GDR in 3 4 months. Where: GDR=gradual dose reduction, MDS=minimum data set, PHQ-9=patient health questionnaire, UTI=urinary tract infection 23
24 Antipsychotic Use in Dementia Assessment (Compliments of CommuniCare Family of Companies and Omnicare, Inc.) Antipsychotic Use in Dementia Assessment page 2. (Compliments of CommuniCare Family of Companies and Omnicare, Inc.) 24
25 25

26 Resources and Tools Tools to Monitor Facility Success Antipsychotic Utilization Report Trending information including acceptance rate for Consultant Pharmacists recommendations. Progress report towards CMS goal of 15% reduction Facility specific report 26
27 27
28 Progress towards Goal in State of Ohio Omnicare Serviced Facilities Percent of long stay residents who received an antipsychotic medication 3 quarter average (4/1/ /31/2011) Percent of long stay residents who received an antipsychotic medication 3 quarter average (10/1/2011 6/30/2012) 26.15% 26.35% October 2012 percent Omnicare Data 22.11% Facilities have met or exceeded a 15% reduction as of October 2012 Facilities 50% or more towards a 15% reduction as of October % 11.6% Average Pct to Goal of 15% Reduction % Summary Consultant Pharmacists can assist you: Clinical & regulatory expertise Multiple resources and tools Collaboration with your multidisciplinary team, including your medical director and psychiatrist In servicing/education of multidisciplinary team Reports & Tools to monitor success 28
29 This image cannot currently be displayed. 12/17/2012 Dementia Care & Anti-Psychotics Just The Facts Ma am December 17, 2012 Ronald A. Savrin, MD, MBA, FACS Medical Director, Ohio KePRO 58 29

30 This image cannot currently be displayed. This image cannot currently be displayed. 12/17/2012 THE MEASURE Numerator Long-stay residents who received antipsychotics Denominator All long-stay residents except those with exclusions. Exclusions Schizophrenia Tourette s Syndrome (current or prior assessment) Huntington s Disease 59 THE BOX OEI
31 This image cannot currently be displayed. This image cannot currently be displayed. 12/17/2012 The EVIDENCE Of a total of seventeen placebo controlled trials performed with olanzapine (Zyprexa),aripiprazole (Abilify), risperidone ( Risperdal), or quetiapine (Seroquel) in elderly demented patients with behavioral disorders, fifteen showed numerical increases in mortality in the drug-treated group compared to the placebotreated patients. These studies enrolled a total of 5106 patients, and several analyses have demonstrated an approximately fold increase in mortality in these studies. Examination of the specific causes of these deaths revealed that most were either due to heart related events (e.g., heart failure, sudden death) or infections (mostly pneumonia). FDA 4/11/2005 (emphasis added) 61 THE FUSS OIG May 2011 Medicare NH residents - 14% atypical antipsychotic 83% were for OFF-LABEL Use (no psychosis) 88% Black Box warning applied (dementia) 51% of claims were erroneous (no accepted indication) 22% Not in accordance with CMS standards Excessive Dose 10.4% Excessive Duration 9.4% Without Indications 8.0% Inadequate Monitoring 7.7% Adverse Consequences 4.7% (18.2% multiple) OEI May /1/07 6/30/
32 This image cannot currently be displayed. This image cannot currently be displayed. 12/17/2012 The Issue Antipsychotics Used - FOUR Possibilities Diagnosis Used On-Label for Specific Dx Diagnosis Used Off- Label for Specific Dx Evidence DOES Support Drug for Diagnosis Diagnosis Used Off- Label for Specific Dx Evidence DOES NOT Support Drug for Diagnosis No Specific Diagnosis -?? 63 The Evidence Meta-analysis 2011 Psychosis, Agitation, Global Behavioral Symptoms in Dementia BENEFITS Standardized Mean Difference (95% CI) Aripiprazole Olanzapine Quetiapine Risperidone ( ) ( ) ( ) ( ) Pooled Analysis: Neuropsychiatric Inventory (NPI) Score 35% improvement Compared to Baseline (30%) 3.41 points above placebo (4.0) JAMA. 2011;306(12):
33 This image cannot currently be displayed. This image cannot currently be displayed. 12/17/2012 The Evidence Meta-analysis 2011 Psychosis, Agitation, Global Behavioral Symptoms in Dementia RISKS OR (95% CI) Aripiprazole Olanzapine Quetiapine Risperidone Cardiovasc 1.20 ( ) 2.3 ( ) 1.10 ( ) 2.10 ( ) CVA 0.70 ( ) 1.50 ( ) 0.70 ( ) 3.12 ( ) Extrapyramidal 1.30 ( ) ( ) 1.20 ( ) 3.00 ( ) JAMA. 2011;306(12): The Evidence AHRQ Sept 2011 Aripiprazole Olanzapine Quetiapine Risperidone Dementia Mod-High Low Low Mod-High Dementia Psychosis Low Mixed Mixed Mod-High Dementia Agitation Low Mod-High Mixed Mod-High
34 This image cannot currently be displayed. This image cannot currently be displayed. 12/17/2012 The Issue Diagnosis FDA Approved On-Label Use Diagnosis Off- Label Use for Specific Dx Evidence DOES Support Drug for Diagnosis Diagnosis Off- Label Use for Specific Dx Evidence DOES NOT Support Drug for Diagnosis No Specific Diagnosis 67 The Issue Diagnosis FDA Approved On-Label Use Diagnosis Off- Label Use for Specific Dx Evidence DOES Support Drug for Diagnosis Diagnosis Off- Label Use for Specific Dx Evidence DOES NOT Support Drug for Diagnosis No Specific Diagnosis 68 34
35 This image cannot currently be displayed. This image cannot currently be displayed. 12/17/2012 American Medical Directors Association While off label prescribing in this context does not always constitute inappropriate prescribing, use of antipsychotic drugs do have significant health risks in this population reduce the unnecessary use of antipsychotic agents by refocusing the interdisciplinary team on a better understanding of the root cause of dementia related behaviors Letter June 18, Guidelines Use only if antipsychotic drug therapy is necessary to treat a specific condition as diagnosed and documented in Medical Record Unless Clinically contraindicated: Institute Gradual Dose Reductions Provide Behavioral Interventions 70 35
36 This image cannot currently be displayed. 12/17/2012 Reducing the Use of Antipsychotic Medications: First Steps on the Quality Improvement Journey December 17, 2012 Leasa Novak, LPN, BA 71 Reducing the Use of Antipsychotic Medications: First Steps on the Quality Improvement Journey December 17, 2012 Leasa Novak, LPN, BA 72 36

37 QM: Percent of Long-Stay Residents Receiving an Antipsychotic Medication Reported on Nursing Home Compare; derived from Minimum Data Set (MDS) 3.0 assessments Numerator Long-stay residents receiving antipsychotic medication Denominator All residents with target assessment, except those with exclusions Exclusions Dashes in Section N0400A or N0410A Residents with one or more of the following diagnoses in Section I: Schizophrenia Tourette s Syndrome Huntington s Disease 73 The Big Picture 74 37
38 What We Know Individualized care is still the goal. Nursing Home Reform Law (OBRA 87) Quality improvement strategies exist and can help lower QM rates. Systematic processes for improvement Systemic issues can impede improvement efforts. Disengaged leadership Unjust culture or un-empowered staff Chronic turnover Resources and assistance are available. 75 What We Think Strategies for reducing antipsychotic medications may be similar to strategies for reducing physical restraints. Must focus on residents who receive antipsychotic medication for reasons other than FDA-approved indications or evidence-based off-label uses. We have a lot to learn! (All of us.) F-329, F-501 Best practices for dementia care Diagnoses, medications Human needs (physiological, safety, connection, etc.) Quality Assurance/Process Improvement (QAPI) 76 38
39 Where We Are State rate on NH Compare: 25.3%* Does NOT include residents with Dx of Schizophrenia, Tourette s Syndrome or Huntington s Disease DOES include other residents receiving antipsychotic med: Off-label use Addressing behavioral symptom(s) An initial challenge to reduce rates by 15% Residents who have complex care needs A difficult task in a difficult landscape Opportunities Hand in Hand dementia training package Federal and state initiatives Nursing Home Quality Care Collaborative * Nursing Home Compare, 12/7/12 77 Where We re Going Quality Improvement Systematic processes No knee-jerk reactions, band-aids or quick fixes Education Diagnoses, medications, human needs Leadership, regulations, quality improvement Facility processes Facility goals, expectations Collaboration/Partnerships Disseminate resources, best practices Share successes and lessons learned 78 39
 Engage in process improvement cycles Provide education Monitor progress Celebrate successes 80")
40 Digging In 79 General QI Principles Understand the data and relevant issues Conduct facility assessment and root cause analysis (RCA) Engage in process improvement cycles Provide education Monitor progress Celebrate successes 80 40


41 Understanding the Data CASPER reports NH Compare measures Other data 81 Understanding the Relevant Issues Regulations/MDS Coding Prescribing concerns Human needs 82 41
42 Conducting a Facility Assessment Review facility policies/assessment forms Observe actual staff practices Assess culture 83 Conducting a Root Cause Analysis Determine gaps, barriers and strengths: Facility level Culture/organizational practices Prescribing practices Knowledge gaps Behavior management Resident level How many residents receive AP for off-label use? How many residents can begin GDR? How many residents have: Unmet human needs True behavioral symptoms Side effects 84 42
43 Sample Log Name Rx Dx FDAapproved indication? Off- Label Use? Plan GDR? Behavior Mary Zyprexa Bi-polar Yes - Yes Betty Geodon* Dementia No No Yes Anxious Albert Abilify* Depression No Yes Yes Suicidal Paul Mellaril Schizo. Yes - No Martha Risperdal Dementia No No Yes Confused John Haldol* Alzheimers No Yes Yes Sundowning Steven Seroquel Dementia No No Yes Combative *Prescribed after admission. 85 Process Improvement Develop a team: MD/DO, RPh, Nursing, Social Services, Activities, etc. Establish meeting structures Set a goal and create Facility Action Plan Review individual residents and determine changes to care plan For more challenging areas, select process change(s) Pilot-test the change Evaluate results Determine next steps (adopt, adapt, abandon) Repeat steps as needed Include education plan 86 43
44 Possible Change Areas Pilot-testing: Behavior /symptom assessment / care planning Nursing documentation of behaviors, side effects Non-pharmacologic interventions Social services/activities assessments Residents activity plans AIMS scales Pharmacy review process GDR documentation Process for requesting/prescribing new medications 87 Education Staff Diagnoses and nursing interventions Psychiatric diagnoses Dementia diagnoses Antipsychotic medications Indications, contraindications, warnings Side effects Non-pharmacologic interventions / behavior management Residents/families Quality improvement goals Facility protocols Non-pharmacologic interventions 88 44

45 Monitoring Progress Monitor progress Check in with staff Celebrate successes 89 DON T Assume staff are skilled in providing effective dementia care. Rotate assignments for nurses and STNAs. Permit extreme environmental noise, especially alarms. Ignore staff burnout. Burnout can lead to decreased empathy, which can ultimately lead to unmet resident needs. Contribute to a culture of blame. Instead, focus on creating a positive culture of teamwork and appreciation. Underestimate the effectiveness of nonpharmacologic approaches

46 Comparison Restraint Rates 1991: 21.1%* 2012: 1.9%** Antipsychotic Rates 2011: 25.3%*** Interventions Safety needs Individualized care Attention to seating Gate-keeping controls Active reduction efforts Interventions Human needs Individualized care Attention to Dx & Rx Prescribing controls GDRs * ** CASPER data, *** Nursing Home Compare data, Ohio rate Resources 92 46
47 Resources: The Big Picture Presentations/Training Materials: CMS broadcast March 24: nformation.aspx?cid=1098 Advancing Excellence in America s Nursing Homes campaign spx?controls=dementiacare CMS dementia training package arriving soon! Hand in Hand 93 Resources: Digging In Tools: Facility-Level Review: er%20assessment%20form%207%2027%2012.pdf ciplinary%20review%207%2027%2012.pdf Resident-Level Review: nterdisciplinarymedicationreview.pdf %20MEDICATION%20MANAGEMENT%20COMMITTEE.docx 0for%20CFMC%20(2).pdf 94 47

48 Questions 95 Ohio KePRO Rock Run Center, Suite Lombardo Center Drive Seven Hills, Ohio Tel: Fax All material presented or referenced herein is intended for general informational purposes and is not intended to provide or replace the independent judgment of a qualified healthcare provider treating a particular patient. Ohio KePRO disclaims any representation or warranty with respect to any treatments or course of treatment based upon information provided. Publication No OH /2012. This material was prepared by Ohio KePRO, the Medicare Quality Improvement Organization for Ohio, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 48

 Data portal Repository")

49 OHIO APPROACH STATE OFFICES Organization and Momentum for Quality Improvement Central Station Access to subject matter expertise and tools (e.g., dementia treatment guidelines) Data portal Repository for Systems Changes Improvements in the health care delivery system that may be identified (e.g., access to psychiatric expertise, even virtually) 49
50 PROCESS FOR LEARNING COLLABORATIVE Identify Champions Gather Teams Collect and Analyze Data Monthly Teleconferences Subjects of Interest Promising & Best Practices Quarterly Webinars Yearly Summary & Lessons Learned Conversation 50
51 CO-CHAIRS Mary S. Applegate MD, FAAP, FACP Medicaid Medical Director Beverley Laubert State LTC Ombudsman THANK YOU 51
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit
 Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
The Centers for Medicare & Medicaid Services (CMS) Partnership to Improve Dementia Care
 Partnership to Improve Dementia Care") The Centers for Medicare & Medicaid Services (CMS) Partnership to Improve Dementia Care Ohio Psychotropic Medication Nursing Facility Quality Improvement Project Ohio KePRO Nursing Home Quality Care Collaborative
The Centers for Medicare & Medicaid Services (CMS) Partnership to Improve Dementia Care Ohio Psychotropic Medication Nursing Facility Quality Improvement Project Ohio KePRO Nursing Home Quality Care Collaborative
Organization: Solution Title: Program/Project Description, including Goals: What is this project? Why is this project important?
 Organization: Hebrew Home of Greater Washington (The Charles E. Smith Life Communities) The Hebrew Home provides post-acute services and long-term care to a daily average census of 500 residents. The Home
Organization: Hebrew Home of Greater Washington (The Charles E. Smith Life Communities) The Hebrew Home provides post-acute services and long-term care to a daily average census of 500 residents. The Home
Psychotropic Drug Use To Medicate or Not to Medicate?
 Psychotropic Drug Use To Medicate or Not to Medicate? Presented by: Lydia Restivo, RN CDONA Regulatory Compliance Consultant West & Restivo Quality Consulting Cell: 516 318-9088 Email: lydrestivo@verizon.net
Psychotropic Drug Use To Medicate or Not to Medicate? Presented by: Lydia Restivo, RN CDONA Regulatory Compliance Consultant West & Restivo Quality Consulting Cell: 516 318-9088 Email: lydrestivo@verizon.net
POLICY. Use of Antipsychotic Medications in Nursing Facility Residents. Preamble. Background
 Preamble POLICY Use of Antipsychotic Medications in Nursing Facility Residents The Office of Inspector General of the U. S. Department of Health and Human Services issued a report in May 2011 finding that
Preamble POLICY Use of Antipsychotic Medications in Nursing Facility Residents The Office of Inspector General of the U. S. Department of Health and Human Services issued a report in May 2011 finding that
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications
 Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications Lisa Bridwell Program Specialist Telligen QIN-QIO March 2018 Objectives Review interpretive guidance F758 (Free from
Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications Lisa Bridwell Program Specialist Telligen QIN-QIO March 2018 Objectives Review interpretive guidance F758 (Free from
The Department of Justice s Focus on Failure of Care Fraud Cases
 The Department of Justice s Focus on Failure of Care Fraud Cases HCCA 17 TH ANNUAL COMPLIANCE INSTITUTE WASHINGTON, DC APRIL 21, 2013 SUSAN C. LYNCH, ESQ. U.S. DEPARTMENT OF JUSTICE SUSAN.LYNCH@USDOJ.GOV
The Department of Justice s Focus on Failure of Care Fraud Cases HCCA 17 TH ANNUAL COMPLIANCE INSTITUTE WASHINGTON, DC APRIL 21, 2013 SUSAN C. LYNCH, ESQ. U.S. DEPARTMENT OF JUSTICE SUSAN.LYNCH@USDOJ.GOV
Pharmacy Services. Division of Nursing Homes
 Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
3/6/2017. CMS nursing home requirements have not been comprehensively updated since 1991 despite significant changes in the industry.
 Debra Brown, PharmD Pharmaceutical Consultant II Specialist Licensing and Certification QCHF/CAHF Spring Legislative Conference March 2017 1 Describe impact of 2016 CMS Final Rule on SNF pharmacy services
Debra Brown, PharmD Pharmaceutical Consultant II Specialist Licensing and Certification QCHF/CAHF Spring Legislative Conference March 2017 1 Describe impact of 2016 CMS Final Rule on SNF pharmacy services
Nursing Home Pearls or
 Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Medication Related Changes Phase 1&2
 Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress
 Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
NURSING FACILITY ASSESSMENTS
 Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
MDS Coding. Antipsychotic Quality Measure
 MDS Coding Antipsychotic Quality Measure The information in this presentation may be subject to copyright and may not be reproduced without permission of the presenter. Introduction Jessica Mirabal, RN
MDS Coding Antipsychotic Quality Measure The information in this presentation may be subject to copyright and may not be reproduced without permission of the presenter. Introduction Jessica Mirabal, RN
CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW
 CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-242-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
CMS RULES FOR PARTICIPATION/LTC REGULATIONS: WHAT YOU NEED TO KNOW SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-242-L04-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
HOW WE GOT HERE 1935: Social Security Act Private nursing homes
 1 LeadingAge Oklahoma Annual Conference March 8, 2017 CMS Revised Pharmacy Regulations: Lessons Learned from Phase 1, Guidance for Phase 2 William M. Vaughan RN, BSN Vice President, Education and Clinical
1 LeadingAge Oklahoma Annual Conference March 8, 2017 CMS Revised Pharmacy Regulations: Lessons Learned from Phase 1, Guidance for Phase 2 William M. Vaughan RN, BSN Vice President, Education and Clinical
QAPI: Driving Quality or Just Driving You Crazy
 QAPI: Driving Quality or Just Driving You Crazy Julie Kueker, MBA, MT(ASCP) Nursing Home QIN-QIO Task Lead Objectives Review the Final Rule Changes and Updates for QAPI Describe the format of QAPI methodology
QAPI: Driving Quality or Just Driving You Crazy Julie Kueker, MBA, MT(ASCP) Nursing Home QIN-QIO Task Lead Objectives Review the Final Rule Changes and Updates for QAPI Describe the format of QAPI methodology
MISUSE AND OVERUSE OF ELDERS WITH DEMENTIA May 2018
 MISUSE AND OVERUSE OF ANTI-PSYCHOTIC DRUGS ON ELDERS WITH DEMENTIA May 2018 MITZI M CFATRICH, EXECUTIVE DIRECTOR LAURA MEYER PFEIFER, DIRECTOR OF DEVELOPMENT AND OUTREACH Kansas Advocates for Better Care
MISUSE AND OVERUSE OF ANTI-PSYCHOTIC DRUGS ON ELDERS WITH DEMENTIA May 2018 MITZI M CFATRICH, EXECUTIVE DIRECTOR LAURA MEYER PFEIFER, DIRECTOR OF DEVELOPMENT AND OUTREACH Kansas Advocates for Better Care
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
PERFORMANCE MEASURE DATE / RESULTS / ANALYSIS FOLLOW-UP / ACTION PLAN
 Resident-to-Resident Assaults AIM: To decrease incidents of Resident to Residents assaults by 5% in the Fiscal Year (FY) 2011-2012. MONITORING: Data is collected from all instances in which State of California
Resident-to-Resident Assaults AIM: To decrease incidents of Resident to Residents assaults by 5% in the Fiscal Year (FY) 2011-2012. MONITORING: Data is collected from all instances in which State of California
Minutes of the Bureau of Health Provider Standards/ Medical Directors Advisory Committee Meeting July 27, 2012
 Minutes of the Bureau of Health Provider Standards/ Medical Directors Advisory Committee Meeting July 27, 2012 ATTENDEES: James Yates, MD, CMD, President Elect Regina Harrell, MD, CMD, Secretary/Treasurer
Minutes of the Bureau of Health Provider Standards/ Medical Directors Advisory Committee Meeting July 27, 2012 ATTENDEES: James Yates, MD, CMD, President Elect Regina Harrell, MD, CMD, Secretary/Treasurer
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
Antipsychotic Use Survey Tool Supplemental Guidance
 Antipsychotic Use Survey Tool Supplemental Guidance Commonly prescribed antipsychotic medications (brand name and/or generic): First generation (typical) antipsychotic: chlorpromazine (generic only) fluphenazine
Antipsychotic Use Survey Tool Supplemental Guidance Commonly prescribed antipsychotic medications (brand name and/or generic): First generation (typical) antipsychotic: chlorpromazine (generic only) fluphenazine
Examining Inappropriate Use of Antipsychotic Drugs Part One: How Seven States Cite Antipsychotic Drug Deficiencies
 Examining Inappropriate Use of Antipsychotic Drugs Part One: How Seven States Cite Antipsychotic Drug Deficiencies The misuse of antipsychotic drug is a pervasive problem in American nursing facilities.
Examining Inappropriate Use of Antipsychotic Drugs Part One: How Seven States Cite Antipsychotic Drug Deficiencies The misuse of antipsychotic drug is a pervasive problem in American nursing facilities.
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
LTCCC Mid-Term Report to the United Nations UPR on Antipsychotic Drugging in US Nursing Homes
 Mid-Term Report: The Inappropriate Use of Antipsychotic Drugs Among Nursing Home Residents Continues to be Widespread and Immediate Action is Still Needed to Protect Residents from Chemical Restraints
Mid-Term Report: The Inappropriate Use of Antipsychotic Drugs Among Nursing Home Residents Continues to be Widespread and Immediate Action is Still Needed to Protect Residents from Chemical Restraints
March 5, March 6, 2014
 William Lamb, President Richard Gelula, Executive Director March 5, 2012 Ph: 202.332.2275 Fax: 866.230.9789 www.theconsumervoice.org March 6, 2014 Marilyn B. Tavenner Administrator Centers for Medicare
William Lamb, President Richard Gelula, Executive Director March 5, 2012 Ph: 202.332.2275 Fax: 866.230.9789 www.theconsumervoice.org March 6, 2014 Marilyn B. Tavenner Administrator Centers for Medicare
Advocating Against The Illegal and Excessive Use of Psychotropic Drugs with People with Dementia
 Advocating Against The Illegal and Excessive Use of Psychotropic Drugs with People with Dementia Kelly Bagby, AARP Foundation Litigation (202) 434-2103 OBJECTIVES Raise awareness and understanding of the
Advocating Against The Illegal and Excessive Use of Psychotropic Drugs with People with Dementia Kelly Bagby, AARP Foundation Litigation (202) 434-2103 OBJECTIVES Raise awareness and understanding of the
The CMS State Operations Manual Overview and Changes
 The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
Behavioral Health Services. Division of Nursing Homes
 Behavioral Health Services Division of Nursing Homes 483.40 Behavioral Health Services Overview F740 Introduction to Behavioral Health Services F741 Sufficient and Competent Staff F742 Treatment/Services
Behavioral Health Services Division of Nursing Homes 483.40 Behavioral Health Services Overview F740 Introduction to Behavioral Health Services F741 Sufficient and Competent Staff F742 Treatment/Services
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care
 Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Get Ready for Phase 2: How to Use the Facility Assessment to Drive Person-Centered Care Today s Objectives Analyze progress on major Arizona Nursing Home Quality Care Collaborative (NHQCC) goals. Describe
Creating the Collaborative Care Team
 Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
A Changing Landscape Regulatory Impact on Medication Management
 2015 Remedi SeniorCare Annual Conference August 30, 2018 A Changing Landscape Regulatory Impact on Medication Management William M. Vaughan RN Vice President, Education / Clinical Affairs Remedi SeniorCare
2015 Remedi SeniorCare Annual Conference August 30, 2018 A Changing Landscape Regulatory Impact on Medication Management William M. Vaughan RN Vice President, Education / Clinical Affairs Remedi SeniorCare
QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement. Patty Austin, RN, CPHQ Project Coordinator
 QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement Patty Austin, RN, CPHQ Project Coordinator QA + PI = QAPI QAPI takes a systematic, comprehensive, and data-driven
QAPI- CREATING A CULTURE FOR IMPROVMENT Guide to the Basic Principles of Quality Improvement Patty Austin, RN, CPHQ Project Coordinator QA + PI = QAPI QAPI takes a systematic, comprehensive, and data-driven
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
A Network of Long Term Care Facilities for Conducting Pharmaco-Epi Observational Studies: Experience from USA and Europe
 A Network of Long Term Care Facilities for Conducting Pharmaco-Epi Observational Studies: Experience from USA and Europe Vincent Mor, Ph.D. Giovanni Gambassi, M.D. 1 Conflicts of Interest -- Mor F PI of
A Network of Long Term Care Facilities for Conducting Pharmaco-Epi Observational Studies: Experience from USA and Europe Vincent Mor, Ph.D. Giovanni Gambassi, M.D. 1 Conflicts of Interest -- Mor F PI of
RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care. Recommendation Comparison Chart
 RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care Recommendation Comparison Chart RECOMMENDATIONS FROM SCREENING FOR DELIRIUM, DEMENTIA AND DEPRESSION IN THE OLDER ADULT (2010)
RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care Recommendation Comparison Chart RECOMMENDATIONS FROM SCREENING FOR DELIRIUM, DEMENTIA AND DEPRESSION IN THE OLDER ADULT (2010)
10/22/2015. QIO Program Restructures. QIO Program Restructures ANHA Activities/Social Services Convention Person-Centered Care
 2015 ANHA Activities/Social Services Convention Person-Centered Care Beth Greene, MSW, LGSW Quality Improvement Advisor October 28, 2015 QIO Program Restructures New multistate, five-year contract began
2015 ANHA Activities/Social Services Convention Person-Centered Care Beth Greene, MSW, LGSW Quality Improvement Advisor October 28, 2015 QIO Program Restructures New multistate, five-year contract began
DEFINITIONS (c)(1) Discharge Planning : Home Health Agency (HHA) : Inpatient Rehabilitation Facility (IRF) : Local Contact Agency :
(1) Discharge Planning : Home Health Agency (HHA) : Inpatient Rehabilitation Facility (IRF) : Local Contact Agency :") F660 483.21(c)(1) Discharge Planning Process The facility must develop and implement an effective discharge planning process that focuses on the resident s discharge goals, the preparation of residents
F660 483.21(c)(1) Discharge Planning Process The facility must develop and implement an effective discharge planning process that focuses on the resident s discharge goals, the preparation of residents
CMS Mega Rule: Implications for Pharmacists and Pharmacies
 CMS Mega Rule: Implications for Pharmacists and Pharmacies Curt Wood, RPh, BCGP, FASCP Disclosure and Conflict of Interest Curt Wood declares no conflicts of interest, real or apparent, and no financial
CMS Mega Rule: Implications for Pharmacists and Pharmacies Curt Wood, RPh, BCGP, FASCP Disclosure and Conflict of Interest Curt Wood declares no conflicts of interest, real or apparent, and no financial
Core Elements of Antibiotic Stewardship for Nursing Homes
 Core Elements of Antibiotic Stewardship for Nursing Homes Welcome! Holly Harmon, RN, MBA, LNHA Senior Director Clinical Services 1 Leonard Russ Immediate Past Chair AHCA Board of Governors Antibiotic Stewardship
Core Elements of Antibiotic Stewardship for Nursing Homes Welcome! Holly Harmon, RN, MBA, LNHA Senior Director Clinical Services 1 Leonard Russ Immediate Past Chair AHCA Board of Governors Antibiotic Stewardship
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
Nursing Home Online Training Sessions Session 4: Antibiotic Stewardship
 National Nursing Home Quality Care Collaborative Nursing Home Online Training Sessions Session 4: Antibiotic Stewardship Health Services Advisory Group (HSAG) Objectives 1 Welcome and overview. 2 Define
National Nursing Home Quality Care Collaborative Nursing Home Online Training Sessions Session 4: Antibiotic Stewardship Health Services Advisory Group (HSAG) Objectives 1 Welcome and overview. 2 Define
Reducing Harm and Healthcare Costs: A Review Of A Physician's Unlimited License To Practice
 Reducing Harm and Healthcare Costs: A Review Of A Physician's Unlimited License To Practice Generally, physicians are licensed under what is termed an "unlimited" license. Underlying the intent of unlimited
Reducing Harm and Healthcare Costs: A Review Of A Physician's Unlimited License To Practice Generally, physicians are licensed under what is termed an "unlimited" license. Underlying the intent of unlimited
PointRight: Your Partner in QAPI
 A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
A N A LY T I C S T O A N S W E R S E X E C U T I V E S E R I E S PointRight: Your Partner in QAPI J A N E N I E M I M S N, R N, N H A Senior Healthcare Specialist PointRight Inc. C H E R Y L F I E L D
2014 QAPI Plan for [Facility Name]
![2014 QAPI Plan for [Facility Name]](/thumbs/74/70066237.jpg "2014 QAPI Plan for [Facility Name]") presented by: Quality Leadership for Long-Term Care 2014 QAPI Plan for [Facility Name] Vision A vision statement is sometimes called a picture of your organization in the future; it is your inspiration
presented by: Quality Leadership for Long-Term Care 2014 QAPI Plan for [Facility Name] Vision A vision statement is sometimes called a picture of your organization in the future; it is your inspiration
Introduction Patient-Centered Outcomes Research Institute (PCORI)
") 2 Introduction The Patient-Centered Outcomes Research Institute (PCORI) is an independent, nonprofit health research organization authorized by the Patient Protection and Affordable Care Act of 2010. Its
2 Introduction The Patient-Centered Outcomes Research Institute (PCORI) is an independent, nonprofit health research organization authorized by the Patient Protection and Affordable Care Act of 2010. Its
Model of Care Scoring Guidelines CY October 8, 2015
 Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Leveraging Your Facility s 5 Star Analysis to Improve Quality
 Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State ( )
") RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
RAISING THE BAR: IPRO s Medicare Quality Improvement Report for New York State (2011 2014) The Centers for Medicare & Medicaid Services (CMS) leads a national healthcare quality improvement program, which
Advocates for Long-Term Care Residents Support Regulations to Ensure Independence of LTC Consultant Pharmacists
 Advocates for Long-Term Care Residents Support Regulations to Ensure Independence of LTC Consultant Pharmacists December 12, 2011 Marilyn B. Tavenner Acting Administrator Centers for Medicare & Medicaid
Advocates for Long-Term Care Residents Support Regulations to Ensure Independence of LTC Consultant Pharmacists December 12, 2011 Marilyn B. Tavenner Acting Administrator Centers for Medicare & Medicaid
Achieving Memory Care Certification for Your Nursing Care Center. Gina Zimmermann, MS Executive Director Nursing Care Center Accreditation Program
 Copyright, The Joint Commission Achieving Memory Care Certification for Your Nursing Care Center Gina Zimmermann, MS Executive Director Nursing Care Center Accreditation Program 1 Today s Objectives Review
Copyright, The Joint Commission Achieving Memory Care Certification for Your Nursing Care Center Gina Zimmermann, MS Executive Director Nursing Care Center Accreditation Program 1 Today s Objectives Review
2014 MASTER PROJECT LIST
 Promoting Integrated Care for Dual Eligibles (PRIDE) This project addressed a set of organizational challenges that high performing plans must resolve in order to scale up to serve larger numbers of dual
Promoting Integrated Care for Dual Eligibles (PRIDE) This project addressed a set of organizational challenges that high performing plans must resolve in order to scale up to serve larger numbers of dual
Focused Dementia Care Surveyor Worksheets
 Focused Dementia Care Surveyor Worksheets INSTRUCTIONS: The purpose of the on-site Focused Dementia Care Survey is to determine compliance with the regulations at 483.25, Appendix PP F309 Care and Services
Focused Dementia Care Surveyor Worksheets INSTRUCTIONS: The purpose of the on-site Focused Dementia Care Survey is to determine compliance with the regulations at 483.25, Appendix PP F309 Care and Services
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care
 Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
Vanderbilt & Qsource Webinar Series
 Vanderbilt & Qsource Webinar Series Vanderbilt University Medical Center Vanderbilt University Center for Quality Aging Qsource Session #1: Introduction to Dementia Care & QAPI Session #2: Dementia & Behavioral
Vanderbilt & Qsource Webinar Series Vanderbilt University Medical Center Vanderbilt University Center for Quality Aging Qsource Session #1: Introduction to Dementia Care & QAPI Session #2: Dementia & Behavioral
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
US Health Health Policy
 Memorandum US Health Health Policy Date January 22, 2015 To From Subject CMS Abt Associates MDS 3.0 Focused Survey Pilot Results Executive Summary This memo describes the results of the MDS 3.0 Focused
Memorandum US Health Health Policy Date January 22, 2015 To From Subject CMS Abt Associates MDS 3.0 Focused Survey Pilot Results Executive Summary This memo describes the results of the MDS 3.0 Focused
Antimicrobial Stewardship Program in the Nursing Home
 Antimicrobial Stewardship Program in the Nursing Home CAHF San Bernardino/Riverside Chapter May 19 th, 2016 Presented by Robert Jackson, Pharm.D. Pharmaceutical Consultant II, Specialist CDPH Licensing
Antimicrobial Stewardship Program in the Nursing Home CAHF San Bernardino/Riverside Chapter May 19 th, 2016 Presented by Robert Jackson, Pharm.D. Pharmaceutical Consultant II, Specialist CDPH Licensing
Medicaid Efficiency and Cost-Containment Strategies
 Medicaid Efficiency and Cost-Containment Strategies Medicaid provides comprehensive health services to approximately 2 million Ohioans, including low-income children and their parents, as well as frail
Medicaid Efficiency and Cost-Containment Strategies Medicaid provides comprehensive health services to approximately 2 million Ohioans, including low-income children and their parents, as well as frail
The Changing Role of Physicians in LTCF
 The Changing Role of Physicians in LTCF David Gifford MD MPH Boise ID Feb 9 th, 2017 CMS Changes to SNF Regs New rule makes extensive changes to SNF Requirements of Participation (RoP) Last major update
The Changing Role of Physicians in LTCF David Gifford MD MPH Boise ID Feb 9 th, 2017 CMS Changes to SNF Regs New rule makes extensive changes to SNF Requirements of Participation (RoP) Last major update
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Antibiotic Stewardship Program (ASP)
") Introduction: Antibiotics are among the most frequently prescribed medications in nursing centers, with up to 70% of nursing home patients receiving one or more courses of systemic antibiotics in a year.
Introduction: Antibiotics are among the most frequently prescribed medications in nursing centers, with up to 70% of nursing home patients receiving one or more courses of systemic antibiotics in a year.
4/13/2015. I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor for CMS.
 Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
Alice Bonner, PhD, RN, FAAN Northeastern University April 30 th, 2015 Photo:Alex Tenappel I am the former Director of the CMS Division of Nursing Homes. I am not currently a CMS official; I work as a contractor
INTERACT 4 Patty Abele, FNP BC
 INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
INTERACT 4 Patty Abele, FNP BC (No relevant financial relationships to disclose) TODAY WE WILL Identify the risks and disadvantages associated with avoidable hospitalizations Identify the goals of the
Local Enhanced Service Agreement 1 July March 2016
 Local Enhanced Service Agreement 1 July 2013 31 March 2016 Recognition and Management of People with Dementia and their Family/Carers in General Practices in Bristol Agreement between NHS Bristol Clinical
Local Enhanced Service Agreement 1 July 2013 31 March 2016 Recognition and Management of People with Dementia and their Family/Carers in General Practices in Bristol Agreement between NHS Bristol Clinical
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
The Role of the Agency for Healthcare Research and Quality (AHRQ) in the US Drug Safety System
 in the US Drug Safety System") The Role of the Agency for Healthcare Research and Quality (AHRQ) in the US Drug Safety System Scott R. Smith, MSPH, PhD Center for Outcomes & Evidence Agency for Healthcare Research & Quality July 20,
The Role of the Agency for Healthcare Research and Quality (AHRQ) in the US Drug Safety System Scott R. Smith, MSPH, PhD Center for Outcomes & Evidence Agency for Healthcare Research & Quality July 20,
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA)
 Case Study Scenario 1: Following Quality Assurance (QA)") Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
CMS RAI MANUAL ERRATA DOCUMENT
 CMS RAI MANUAL ERRATA DOCUMENT SECTION I UTI S In Chapter 3, page I-9, under Coding Tips in I: Active Diagnoses in the Last 7 Days, a third bullet has been added: If the diagnosis of UTI was made prior
CMS RAI MANUAL ERRATA DOCUMENT SECTION I UTI S In Chapter 3, page I-9, under Coding Tips in I: Active Diagnoses in the Last 7 Days, a third bullet has been added: If the diagnosis of UTI was made prior
Care Transitions. Objectives. An Overview of Care Transitions Efforts in Arkansas
 An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
An Overview of Care Transitions Efforts in Arkansas June 6, 2013 Christi Quarles Smith, PharmD Manager, Quality Programs Care Transitions Project Lead Arkansas Foundation for Medical Care THIS MATERIAL
The CMS Five Star Nursing Home Rating System An incomplete and inaccurate consumer tool
 The CMS Five Star Nursing Home Rating System An incomplete and inaccurate consumer tool Myth: The Centers for Medicare and Medicaid Services (CMS) 5 Star Nursing Home Quality rating system provides a useful
The CMS Five Star Nursing Home Rating System An incomplete and inaccurate consumer tool Myth: The Centers for Medicare and Medicaid Services (CMS) 5 Star Nursing Home Quality rating system provides a useful
Federal Requirements & Regulatory Provisions Relevant to Dementia Care & The Use Of Antipsychotic Drugs
 Federal Requirements & Regulatory Provisions Relevant to Dementia Care & The Use Of Antipsychotic Drugs By: Richard J. Mollot, Executive Director Daniel Butler, Public Policy & Law Intern Long Term Care
Federal Requirements & Regulatory Provisions Relevant to Dementia Care & The Use Of Antipsychotic Drugs By: Richard J. Mollot, Executive Director Daniel Butler, Public Policy & Law Intern Long Term Care
9/27/2017. Getting on the Path to Excellence. The path we are taking today! CMS Five Elements
 Getting on the Path to Excellence QAPI DESIGN AND IMPLEMENTATION Demi Haffenreffer, RN, MBA www.consultdemi.net The path we are taking today! The requirements at F944 (formerly F520) Key elements Survey
Getting on the Path to Excellence QAPI DESIGN AND IMPLEMENTATION Demi Haffenreffer, RN, MBA www.consultdemi.net The path we are taking today! The requirements at F944 (formerly F520) Key elements Survey
NURSING HOME SURVEILLANCE UPDATE
 NURSING HOME SURVEILLANCE UPDATE Shelly Glock, Acting Director Division of Nursing Homes and ICF/IID Surveillance Center for Health Care Provider Services and Oversight Office of Primary Care and Health
NURSING HOME SURVEILLANCE UPDATE Shelly Glock, Acting Director Division of Nursing Homes and ICF/IID Surveillance Center for Health Care Provider Services and Oversight Office of Primary Care and Health
Use of Antipsychotic Medications in Individuals With Alzheimer's Disease in Nursing Facilities
 Walden University ScholarWorks Walden Dissertations and Doctoral Studies Walden Dissertations and Doctoral Studies Collection 2018 Use of Antipsychotic Medications in Individuals With Alzheimer's Disease
Walden University ScholarWorks Walden Dissertations and Doctoral Studies Walden Dissertations and Doctoral Studies Collection 2018 Use of Antipsychotic Medications in Individuals With Alzheimer's Disease
Data Entry for the Advancing Excellence Campaign What you need to know
 Data Entry for the Advancing Excellence Campaign What you need to know An important step in quality improvement is to regularly review your facility s progress toward meeting its goals. In fact, this is
Data Entry for the Advancing Excellence Campaign What you need to know An important step in quality improvement is to regularly review your facility s progress toward meeting its goals. In fact, this is
Form CMS (5/2017) Page 1
 Page 1") Use this pathway for a resident who has pain symptoms or can reasonably be expected to experience pain (i.e., during therapy) to determine whether the facility has provided and the resident has received
Use this pathway for a resident who has pain symptoms or can reasonably be expected to experience pain (i.e., during therapy) to determine whether the facility has provided and the resident has received
Caring in the Carolinas 11/5/2016
 The Mega Rule: Reform of Requirements for Long- Term Care Facilities Robert Smith, Pharm D, BCPS, CGP, FASCP Director of Clinical Services Neil Medical Group Disclosures I have no conflicts of interest
The Mega Rule: Reform of Requirements for Long- Term Care Facilities Robert Smith, Pharm D, BCPS, CGP, FASCP Director of Clinical Services Neil Medical Group Disclosures I have no conflicts of interest
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
TelePsychiatry in the Long Term Care Setting
 TelePsychiatry in the Long Term Care Setting Presented by: Richard Nockowitz, M.D. Founder & President, My Psychiatric Partner, LLC rnockowitz@mypsychiatricpartner.com Mobile: 614-648-2005 1) What is telepsychiatry?
TelePsychiatry in the Long Term Care Setting Presented by: Richard Nockowitz, M.D. Founder & President, My Psychiatric Partner, LLC rnockowitz@mypsychiatricpartner.com Mobile: 614-648-2005 1) What is telepsychiatry?
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Agenda: Noon Overview of the regulatory sections affected by the Reform of RoP in Phase 2
 Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/16/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/16/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know
 New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know Presented by: Kathy Pellatt, Senior Quality Improvement Analyst LeadingAge New York
New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know Presented by: Kathy Pellatt, Senior Quality Improvement Analyst LeadingAge New York
Behavioral Health Services ( )
") Behavioral Health Services ( 483.40) Presenter: Sabine Dettlinger-Metropoulos Summary New Section CMS became aware of concerns that behavioral health services Were either not always being addressed or
Behavioral Health Services ( 483.40) Presenter: Sabine Dettlinger-Metropoulos Summary New Section CMS became aware of concerns that behavioral health services Were either not always being addressed or
Morris J. Kaplan, Esq., NHA
 Managing Behavioral Symptoms Through Best Care Practices & Behavioral Management Programs Rather Than Medication Morris J. Kaplan, Esq., NHA President, Kaplan Health Management, LLC Operating Partner,
Managing Behavioral Symptoms Through Best Care Practices & Behavioral Management Programs Rather Than Medication Morris J. Kaplan, Esq., NHA President, Kaplan Health Management, LLC Operating Partner,
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Adult Family Homes. Susan L. Lakey, PharmD Pharmacy 492 January 24, 2005
 Adult Family Homes Susan L. Lakey, PharmD Pharmacy 492 January 24, 2005 Background 1995 HB 1908 Required a reduction in NH medicaid beds by 1600 over 2 years The number of older adults in nursing homes
Adult Family Homes Susan L. Lakey, PharmD Pharmacy 492 January 24, 2005 Background 1995 HB 1908 Required a reduction in NH medicaid beds by 1600 over 2 years The number of older adults in nursing homes
Success of an MTM Program Beyond Medicare Part D: Is It Really a Pharmacy Pay for Performance Model? Jim Gartner RPh, MBA CareSource
 Success of an MTM Program Beyond Medicare Part D: Is It Really a Pharmacy Pay for Performance Model? Jim Gartner RPh, MBA CareSource 10 28 2014 Learning Objectives Understand why a health plan would want
Success of an MTM Program Beyond Medicare Part D: Is It Really a Pharmacy Pay for Performance Model? Jim Gartner RPh, MBA CareSource 10 28 2014 Learning Objectives Understand why a health plan would want
Improving Nursing Home Compare for Consumers. Five-Star Quality Rating System
 Improving Nursing Home Compare for Consumers Five-Star Quality Rating System Improving Nursing Home Compare Major Revision to Nursing Home Compare Mid-December Improved Navigation - Similar to Hospital
Improving Nursing Home Compare for Consumers Five-Star Quality Rating System Improving Nursing Home Compare Major Revision to Nursing Home Compare Mid-December Improved Navigation - Similar to Hospital
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
CMS Final Rule Pharmacy Services Update: What You Need to Know!
 CMS Final Rule Pharmacy Services Update: What You Need to Know! Presented by: Dr. William C. Hallett, Pharm.D., MBA, CGP, C-MTM Guardian Consulting Services, Inc. (855) 675-6235 whallett@guardianconsulting.com
CMS Final Rule Pharmacy Services Update: What You Need to Know! Presented by: Dr. William C. Hallett, Pharm.D., MBA, CGP, C-MTM Guardian Consulting Services, Inc. (855) 675-6235 whallett@guardianconsulting.com
Advancing Excellence Phase 2 Goals
 Advancing Excellence Phase 2 Goals Campaign participants need to select at least three goals, including one of the three clinical goals (3,4 or 5) and one of the five organizational goals (1,2,6,7,8).
Advancing Excellence Phase 2 Goals Campaign participants need to select at least three goals, including one of the three clinical goals (3,4 or 5) and one of the five organizational goals (1,2,6,7,8).
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable