Together with Somali Health Authorities
|
|
|
- Herbert Gallagher
- 6 years ago
- Views:
Transcription


1 Together with Somali Health Authorities
2
3 Overview Programme/Project Name Somali Joint Health and Nutrition Programme (JHNP) Location Somaliland/North West Zone (NWZ), Puntland/North East Zone (NEZ) and Central South Zone (CSZ) of Somalia Participating UN Organizations Implementing Authorities Currently Engaged Donors United Nations Children Fund (UNICEF) United Nations Population Fund (UNFPA) World Health Organization (WHO) Ministry of Health, Federal Government of Somalia (CSZ); Ministry of Health, Puntland (NEZ); Ministry of Health, Somaliland (NWZ) The Government of the United Kingdom of Great Britain and Northern Ireland/ Department for International Development (DFID); The Government of Sweden/ Swedish International Development Cooperation Agency (Sida); The United States Agency for International Development (USAID); and the Government of Australia/ Australian Agency for International Development (AusAID) Grant Agreement Number XI UNICEF Ref (PBA Number) UNFPA Projects and Fund code SC (DFID and Sida); SC (USAID) SOM2R21A, SOM2R22A, SOM2R23A, (UCJ11) WHO Ref (Award Number) Report Type Annual Report Report Number 3 Report Due Date 31 May 2014 Period Covered by Report 1 January December 2013 Contribution during Reporting period/ Amount in Original Currency and USD and date received by UNICEF Contribution in Amount in Original Currency and USD Total Contribution from all donors (February 2012 to December 2013) DFID GBP11,523,157 = US$ 18,615,775 April 2013 Sweden SEK 36,600,000 = US$ 5,556,246 July 2013 DFID GBP 7,850,000 = US$ 12,661,290 November 2013 (for 2014 s Work Plan) TOTAL = US$ 36,833, DFID GBP 1,487,000 = US$ 2,352,850 June 2012 AusAID AUD 3,000,000 = US4 3,131,520 June 2012 Sweden SEK 15,000,000 = US4 2,250,600 October 2012 USAID = US$ 1,149,963 October 2012 Sweden SEK 17,000,000 = US4 2,554,080 December 2012 TOTAL = US$ 11,439,013 in 2012 US$ 48,272,325 Funds Disbursed UNICEF: UNFPA: WHO: Administrative Agent (AA) fee: US$ 48,272,325 US$ 26,369,860 US$ 8,859,339 US$ 12,571,902 US$ 471,223 Page 1 of 80
4 Major Breakdown of Funds Disbursed For Activities in CSZ: US$ 15,550,387 For Activities in NEZ: US$ 10,774,389 For Activities in NWZ: US$ 11,555,940 UN Direct and Indirect Cost: US$ 9,920,386 AA fee: US$ 471,223 TOTAL US$ 48,272,325 ~ Fund utilisation rate of funds received by October 2013: per cent ~ Fund utilisation rate including funds received by December 2013: per cent Official expenditures to be communicated by UNICEF HQ. Expected Programme Duration 5 Years ( ) Inception Phase: February July 2012 Continuation Phase: August December 2016 Budget Forecast over 5 years ~US$ 236 million Programme s Objectives Geographical Focus Impact: Improved health and nutrition status of Somali people contributing to reduction in maternal and child mortality. Outcome: Increased use of reproductive, maternal, new-born and child health (RMNCH) and nutrition services that are available, accessible, affordable, of acceptable quality and adaptable. Results are set out in the Programme Document 1 and logical framework (revised in 2013) to align programming with in-country health sector strategic plans. All three Somali zones. Focus of service delivery is initially in the following nine regions: Lower Juba, Galgadud and Banadir - CSZ Nugaal, Mudug and Bari - NEZ Togdheer, Awdal and Sanaag (Erigavo and El-Afweyn districts) - NWZ Agency Contacts Ministry of Health (MoH) Contacts JHNP - Joint Coordination Unit (JCU) Anirban Chatterjee (Chief of Health) UNICEF, achatterjee@unicef.org Humayun Rizwan (PHC Medical Officer) WHO, rizwanh@nbo.emro.who.int Achu Lordfred (Maternal Health Advisor) UNFPA, lordfred@unfpa.org Mohamed Abdi Farah (Acting Director General, FGS), drfarah2011@gmail.com Abdirizak Hirsi (Director General NEZ), abdirizak30@yahoo.com Ousman Warsame (Director General NWZ), ousmanwarsame@gmail.com Raza Zaidi (Senior Programme Manager JHNP), razaidi@unicef.org Esther Waters-Crane (Programme & Planning Specialist), ewaterscrane@unicef.org Administrative Agent (UNICEF) Sarah Elamin Ng inja (Donor Relations Specialist), snginja@unicef.org 1 JHNP Programme Document Control: Initial Proposal: Developed with input from donors, authorities and United Nations partners; Shared with stakeholders in January/February 2012; Strategic concept and design document: Formally submitted to donors in February/March 2012; Programme document: Finalised in August 2013 after the development of the three Health Sector Strategic Plans; Approval of Programme document by the Steering Committee: 4 October Page 2 of 80
5 Table of Contents Overview...1 Table of Contents...3 Acronyms...5 Executive Summary Introduction...11 What support is the JHNP providing? What are the expected results? What is the context in which JHNP support is provided? Planned Outputs, Activities and Results...15 Output 1: Governance and Leadership Output 2: Health Workforce Output 3: RMNCH and Nutrition Service Delivery Output 4: Health Financing Output 5: Medicines, Vaccines, RH and Nutrition Commodities and Technologies Output 6: Health Information Overall Performance and Value for Money...49 Annual Outcome Assessment Financial Outcome Assessment Evidence and Evaluation Risks Performance on VfM measures Programme Management...65 Key Functions of the JCU and Progress made during 2013: Links to Other Programmes Lessons Learnt and the Way Forward : Working with Partners : Best Practice and Innovation : Programme Management Programme Priorities for JHNP: List of Reference Documents...73 Page 3 of 80

6 Page 4 of 80
7 Acronyms AA AusAID AWP AYCS+MH BEmONC BNSP CEmONC CEDAW CEP CHD CHF CHW CRC CSO CSS CSZ DFID DPT3 EC EPHS EPI EMRO FP FGM/C FGS FHW FRA FSNAU GAVI GFATM HAB HAs HC HCS HMIS HRH HSAT HSC HSCO HSS HSSP iccm IMAM IYCF JAR JCU JHNP JPLG M&E Administrative Agent Australian Agency for International Development Annual Work Plan Accelerated Young Child Survival and Maternal Health Basic Emergency Obstetric and New-born Care Basic Nutrition Services Package Comprehensive Emergency Obstetric and New-born Care Convention on the Elimination of All Forms of Discrimination against Women Community Empowerment Programme Child Health Day Common Humanitarian Fund Community Health Worker Convention on the Rights of the Child Civil Society Organizations Central South Somalia Central South Zone UK s Department for International Development Diphtheria, Pertussis and Tetanus third dose European Commission Essential Package of Health Services Expanded Programme on Immunization Eastern Mediterranean Regional office of WHO Family Planning Female Genital Mutilation/Cutting Federal Government of Somali Republic Community based Female Health Worker Fiduciary Risk Assessment Food Security and Nutrition Analysis Unit Global Alliance for Vaccines and Immunization Global Fund to fight AIDS, Tuberculosis and Malaria Health Advisory Board Health Authorities Health Centre Health Consortium Somalia (DFID project) Health Management Information System Human Resources for Health Health Systems Analysis Team Health Sector Committee Health Sector Coordination Office Health Systems Strengthening Health Sector Strategic Plan Integrated Community Case Management Integrated Management of Acute Malnutrition Infant & Young Child Feeding Joint Annual Review JHNP - Joint Coordination Unit Joint Health and Nutrition Programme Joint Programme on Local Governance Monitoring and Evaluation Page 5 of 80
8 MCH MDGs MoH MoHDPS MoU MoWDFA MICS NHHP NHPC NGO OPD OTP PCA PDRC PFM PL PSG RMNCH RUTF SC SCODO SIDA SL SOP SRCS TBA TCG TFG THET ToR ToT UN UNDP UNICEF UNFPA UNRC UNSAS USAID WASH WB WHO WVi ZWG Mother and Child Health (facility) Millennium Development Goals Ministry of Health Ministry of Human Development and Public Services, FGS Memorandum of Understanding Ministry of Women Development and Family Affairs Multiple Indicator Cluster Survey Nutrition Hygiene and Health Promotion National Health Professions Commission, NWZ Non-Governmental Organization Out Patient Department Out-Patient Therapeutic Programme Partnership Cooperation Agreement Puntland Development Research Centre Public Financial Management Puntland - NEZ Peacebuilding and State-building Goal Reproductive, Maternal, New-born and Child Health Ready-to-Use Therapeutic Foods Steering Committee Somaliland Community Development Organization Swedish International Development Agency, the Government of Sweden Somaliland - NWZ Standard Operating Procedure Somali Red Crescent Society Traditional Birth Attendant Technical Coordination Group Transitional Federal Government Tropical Health & Education Trust Terms of Reference Training of Trainers United Nations United Nations Development Programme United Nations Children s Fund United Nations Population Fund United Nations Resident Coordinator United Nations Somalia Assistance Strategy United States Agency for International Development Water, Sanitation and Hygiene World Bank World Health Organization World Vision International Zonal Working Group Page 6 of 80
9 Executive Summary Somalia continues to operate with a rudimentary health sector, a fragile and unstable social sector and a governmental structure with a weak economic base, facing security and humanitarian challenges. The fragility of the country over the past two decades has resulted in the collapse of the health sector and a subsequent focus on emergency response interventions to recurrent crises. The Somali people have some of the worst health and nutrition indicators in the world and the country is completely off-track to reach the Millennium Development Goals (MDGs). The Somali health status is poor due to multiple factors including fragmented approaches, low emphasis on community participation and behaviour change, inadequate resource allocation and human resource development as well as inadequate focus on health system strengthening. Key health sector challenges: 1. Every two hours, a Somali mother dies due to pregnancy complications (3,800 Somali mothers die per year, which is nearly more than double the conflict related deaths in Somalia 2,158 in 2010). 2. For every 1,000 Somali children born, 180 will not live to see their fifth birthday (70,000 Somali children die every year). 3. Every fourth Somali child (approximately 348,000 children) suffers from chronic undernourishment, whereas every sixth child (more than 240,000 children) suffers from severe acute malnutrition (SAM), leading to poor learning, growth retardation, increased health care costs and lower economic productivity. 4. High maternal, new-born and child mortality are attributed to high fertility rates, inadequate access to quality maternal and child health and nutrition services, low skilled birth attendance rate, inadequate emergency obstetric and new-born care (EmONC), low female literacy, poverty, social barriers, urban-rural disparities, under-nutrition and a heavy burden of communicable diseases primarily as a result of poor water, sanitation and hygiene (WASH) services. 5. Most deaths and diseases occur among the poor and the disadvantaged segments of the population. Access to an essential package of health, nutrition, social protection and WASH services is a basic human right and its delivery is the primary responsibility of the Somali Authorities. In acknowledgement of the same, Development Partners and UN agencies (UNICEF, WHO and UNFPA) decided to work together with the Somali authorities to design and implement the Somali Joint Health and Nutrition Programme (JHNP) The JHNP aims to support sustained and improved RMNCH and nutrition outcomes for Somali women, girls, children and their communities - resulting in a measurable impact of reduced maternal and child mortality. It also aims to improve the capacity and leadership of the Somali Health Authorities in managing and coordinating the health sector s development. The programme supports critical elements of the New Deal initiative the Somali Compact ; the Somali Six pillar policy for peace-building and state-building; and more specifically implementation of the incountry developed Health and Nutrition Policies, Health Sector Strategic Plans (HSSPs), relevant United Nations (UN) cooperation strategies, as well as other aligned strategies. The programme s implementation considers the specific context of NWZ, NEZ and CSZ and on-going health sector initiatives including the Essential Package of Health Services (EPHS) framework; Global Fund for AIDS, Tuberculosis and Malaria (GFATM); GAVI Health Systems Strengthening (GAVI-HSS); Health Consortium Page 7 of 80
10 Somalia (HCS); humanitarian health initiatives and the Joint Programme on Local Governance and Decentralised Service Delivery (JPLG). The three implementing UN agencies have worked with the Somali health authorities and development partners to develop new ways of engagement, which has led to increasingly inclusive country-led health and nutrition sector reforms; improved results delivery; effective harmonization; enhanced coordination with the donor community; and a strengthened system of mutual accountability and transparency. The continuation phase of JHNP followed the completion of the inception phase at the end of The purpose of the first year (2013) of the continuation phase was to fully activate the JHNP governance and management mechanism that was conceptualized during the inception phase; institutionalize the leadership of the Somali Health Authorities; support the creation of wide reaching HSSPs; finalize the JHNP programme document aligned to the HSSPs; and to strengthen planning, implementation and monitoring components. The first year of the continuation phase focused on commencing a significant service delivery component through the roll-out of EPHS, alongside on-going activities and new work streams related to the six building blocks of the health system. An annual progress report of 2012 was submitted in May 2013 covering the initial programme set-up period and start of the continuation phase. The reporting period of this report is January to December 2013 and provides an overview of performance against the revised JHNP Logical Framework milestones for the year. Key achievements during 2013 included: Leadership and Governance: HSSPs ( ) of CSZ, NEZ and NWZ along with 2013 annual work plans were finalized and implementation commenced. Nutrition Plans of Action were developed for all three zones in alignment with the HSSPs. Assessments for the Public Health Law and on Right to Health for CSZ, NEZ and NWZ were completed. The evaluation of the TOSTAN Female Genital Mutilation/Cutting (FGM/C) intervention for NWZ and NEZ was completed and findings were shared with stakeholders. Technical assistance was provided to the three zones on Reproductive Health (RH) issues. RH units were established with RH working groups and FGM task forces activated at zonal level. Revision of Reproductive Health Strategy completed. Support was provided to strengthen health and nutrition sector coordination mechanisms at national and zonal levels. Furthermore, consensus was reached to further strengthen in-country health coordination mechanisms, with empowerment of the Somali health authorities to play an effective leadership role. Health Workforce: Human Resource for Health (HRH) assessment work in CSZ and NEZ were completed along with consultations to develop HRH policies and plans for CSZ and NEZ, in partnership with the Banadir University and the Puntland Development and Research Centre (PDRC). Page 8 of 80
11 The Review of compensation, salaries, incentives and benefits for Health Personnel was completed and recommendations, which are endorsed by the Health Advisory Board (HAB), are being used to establish a uniform salary top-up mechanism. Standard treatment guidelines and clinical guidelines for the three zones were finalized. A draft curricula Diploma on CEmONC for clinical staff was developed. Support was provided to strengthen nine Midwifery schools in all three zones. 15 post-basic midwives in NWZ and 17 in CSZ completed their training. 90 midwives in NWZ and 45 in NEZ have completed their basic midwifery training. Training of trainers on modern contraception and birth spacing counselling was completed for the three zones. More than 120 health workers were trained on maternal health and child health services in all three zones. 46 midwives and nurses were trained in basic emergency obstetric and neonatal care (BEmONC) in NEZ and 40 midwives were trained in NWZ. A curriculum for Community Health Workers (CHWs) was developed. EPHS/ RMNCH and Nutrition Service Delivery: EPHS contracts were finalized and signed for the roll-out of services in Togdheer. An EPHS assessment and micro-planning exercise was completed for three regions in CSZ, two regions in NEZ and one region in NWZ. Three maternity waiting homes providing basic obstetric, ante/post natal services and neonatal care have been made functional. Fourteen facilities were supported to provide BEmONC services. Missing equipment and supplies in two CEmONC hospitals in Banadir and Galgadug were replaced. RH kits and equipment was provided for CEmONC and BEmONC services in referral hospitals in NWZ and NEZ. With partial support from JHNP, activities in relation to the Child Health Days (CHD) were completed in CSZ in December Polio vaccine was administered to 923,580 children, measles vaccine to 744,077 children and pentavalent vaccine to 177,079 children in CSZ. Additionally, 885,822 women were immunized against tetanus. Furthermore, 686,486 children were de-wormed, 789,762 children were given Vitamin-A whereas oral rehydration salt (ORS) was provided to 917,254 children. Through JHNP support21 more communities in NEZ declared abandonment of FGM/C. Policy and legislation on FGM/C was drafted for NEZ and NWZ. Community-based birth spacing interventions were initiated in Gaalkacyo, Bossasso and Garowe. Health Financing: A health financing workshop took place in November 2013 and a health financing road map was developed. Essential Medicines, Vaccines, Commodities and Supplies: Essential medicines, supplies and nutrition commodities, as well as RH commodities, were made available for EPHS health facilities. Co-financing for the procurement of pentavalent vaccine ensured sufficient stocks of the vaccines in 2013 for all Somali children in all three zones. Support was provided to establish a cold chain in NEZ. Essential drug list was developed for all three zones. Page 9 of 80
 of the HSSPs and to develop the annual work plan for 2014.")
12 Health Information: The Review/Assessment of EPI in NWZ and NEZ was completed. A task force was established to conduct the first Joint Annual Review (JAR) of the HSSPs and to develop the annual work plan for Tools and indicators were finalized, pilot testing was completed and tools were translated for a baseline survey in CSZ. Programme Management: A JHNP specific Somali Compact for Achieving the Health MDS was agreed between all partners and was signed on 4 October The JHNP Programme document was aligned to the HSSPs and the Logical Framework was revised. Standard Operating Procedures (SOP) SOP 002 on Implementing Partner Selection and SOP 003 on Long Term Technical Assistance were developed, approved and is being implemented. A joint annual rolling plan and budget (to replace the tranche based planning mechanism) was developed and approved by the Steering Committee. Roles and responsibilities of the Joint Coordination Unit (JCU) were agreed and the unit was fully staffed. The risk assessment of the JHNP was completed and a Risk Register was developed. Work on Fund Raising Strategy of the Programme initiated. Page 10 of 80
13 1. Introduction What support is the JHNP providing? The Somali Joint Health and Nutrition Programme (JHNP) , with an overall estimated budget of US$ 236 million, is a comprehensive multi-partner five-year development programme aimed towards achieving the health MDG and following the principles of the New Deal 2. While scaling-up the delivery of the EPHS and more specifically RMNCH and nutrition services for women, young girls and children, the JHNP addresses the six building blocks for efficient health system functioning, building and strengthening foundations in order to improve the health and nutritional status of Somali people. Critical aspects of JHNP support include Somali ownership of the strategic and policy process, to provide conflict-sensitive programming in support of Somali priorities and to help build Somali capacity in health. Critical activities and services under JHNP are delivered through the health systems approach and due consideration is given to the specific contexts of NWZ, NEZ and CSZ. The JHNP is supporting the Somali authorities to sustain momentum in the health, nutrition, social protection and WASH sectors ensuring provision of basic services and capacity development, thus contributing to resilience and economic development. The JHNP initially supported the health authorities to put in place a sector road map in the form of a Health Sector Policy framework, followed by the development of three HSSPs which present a practical approach to achieving health sector objectives. The programme has since fully aligned to the approaches identified in the HSSPs and other strategies. Interventions in the HSSPs and JHNP prioritize and adapt cost effective approaches and approaches that are viable in the context. What are the expected results? The programme was designed to help Somali authorities to make progress on MDG 4 and 5 by improving maternal and child health. In harmonization with the ongoing development and humanitarian programming, it is estimated that JHNP results would contribute to averting about 6,000 maternal deaths and 105,000 deaths of children over the period In other words, by the end 2016, it is anticipated that Somali s maternal mortality will reduce by at least 10 per cent, the under-5 mortality rate will reduce by 15 per cent, the number of underweight children will reduce by 10 per cent and the incidence of Female Genital Mutilation/Cutting (FGM/C) will reduce by 10 per cent. The expected outcome of the programme is Increased use of RMNCH and Nutrition services and these services will be more available, accessible, affordable, of acceptable quality and adaptable. Expected outcome results 180,000 additional deliveries through skilled birth attendants (SBA) including more than 170,000 deliveries in public or private health facilities, 170,000 additional couples using birth spacing services, 130,000 additional children immunized against DPT/Pentavalent III vaccine, 170,000 additional children prevented from malnutrition. 2 Page 11 of 80
14 The programme was developed to achieve outcomes through the following six outputs: 1. Improved governance and leadership at all levels of the health sector, 2. Skilled and motivated health workforce distributed equally and equipped to deliver quality RMNCH and nutrition services through a continuum of care approach, 3. RMNCH and nutrition services available, accessible, affordable, of acceptable quality and adaptable, within the EPHS framework, 4. Steady progress made to an equitable and efficient health financing system, 5. Improved access, availability, acceptability, quality and use of health information that covers disease surveillance as well as management information system, 6. Improved access, availability, quality and rational use of essential medicines, vaccines, medical equipment and physical structures. While all Somalis will benefit from strengthened health systems, the focus of these interventions is initially on nine key regions across the three zones: Galgadud, Banadir and Lower Juba regions (CSZ); Nugaal, Mudug and Bari regions (NEZ); Togdheer, Awdal and Sanaag (Erigavo and El-Afweyn districts) regions (NWZ). Expected output results Core Health sector policies, frameworks and plans in place and applied, Health and nutrition sector strategic priorities supported through legislation and health sector coordination mechanism, Health workforce policy and plans in place and 90 per cent of facilities in EPHS regions having skilled/ trained health workforce as per acceptable standards, 480 new midwives completed their training, Improved management capacity at zonal and regional level, Functional health workforce registration and accreditation mechanism, Roll-out of EPHS in all nine targeted regions, with more than 85 per cent of the facilities meeting core EPHS standards, In each targeted region, at least one hospital providing round-the-clock comprehensive emergency obstetric and new born care (CEmONC) services, with a minimum two hospitals offering round-theclock basic EmONC (BEmONC) services, Five time increase in health facility utilization rate, with significant increase in immunization coverage, use of multi-micronutrients, breastfeeding initiation, etc., 75 per cent of EPHS health facilities offering birth spacing services, A minimum of 7 regions having at least 90 per cent of Integrated Management of Acute Malnutrition (IMAM) services, More than 300 communities engaged to declare abandonment of FGM/C, along with enabling environment through legislation and policy measures, Health financing strategy developed and proportion of national budget on health increased to 5-8 per cent, National Drug Policy and quality control procedures in place and being implemented, Essential medicines, supplies, vaccines, RH and nutrition commodities available in health facilities, More than 60 per cent of the facilities meeting WASH standards as per EPHS guidelines, Monitoring and Evaluation Framework developed and implemented. Page 12 of 80
15 What is the context in which JHNP support is provided? The Joint Health and Nutrition Programme was initiated during 2012, when Somalia s eight year political transition ended with the adoption of a provisional constitution, selection of new Parliament and formation of a new government. The political climate remained uncertain in 2013 but with positive developments. The political systems in NWZ and NEZ have shown signs of further stability and maturity. The most recent example is that of a peaceful election in NEZ and the transfer of power to the new Government. Somalia is experiencing a new phase of peace consolidation which provides the best opportunity for sustainable peace and development. The implementation of the continuation phase of the programme started in August However, the country continued to face major development challenges in 2013 with a high level of poverty headcount, slow economic growth and after-effects of the humanitarian crisis especially as a result of 2011 s drought. The health situation in Somalia is among the worst in the world and the country is unlikely to achieve its MDGs on health (4, 5 and 6), education (2 and 3) and nutrition (1) by Some 3,800 pregnant women 3 and 70,000 children 4 under-5 die every year - maternal and child mortality rates are among the highest in the world. The country also faces a nutrition emergency: 26.7 per cent 5 of children under-5 in the CSZ have stunted growth (indicating chronic malnutrition) per cent of children in NWZ, 10.7 per cent in NEZ and 16.5 per cent in CSZ suffer from acute malnutrition 6. With approximately 10 million people, Somalia has one of the highest total fertility rate in the world, whereas life expectancy is only around 51 years. Over the last two decades, risks related to internal and external conflict increased significantly, and have negatively affected the already weak health system in the country. The security gains of the past two years are real but remain incomplete and reversible. Somalia, especially CSZ, remains under the influence of anti-government groups and areas recovered from the insurgency are especially volatile. The authorities, being aware of the risk, are in process of establishing several policy frameworks and legislation that may support the stabilization process. However, Government structures have weak capacity to pursue reconciliation, and to guarantee basic services, security and justice for the population. The Brussels Conference, A New Deal for Somalia, was held on 16 September 2013, co-hosted by the Federal Government of Somali Republic (FGS) and the European Union (EU) and was attended by a wide range of stakeholders. The conference endorsed the Somali Compact, pledging support to enable its implementation and re-commit to the Somali political and socio-economic process with financial pledges of over billion. The Compact priorities are drawn from the existing Six Pillar Programme of the FGS, the second five-year Development Plan of NEZ and the NWZ National Development Plan. These priorities are framed according to the five Peacebuilding and State-building Goals (PSGs) of the Compact to demonstrate measurable progress both by national authorities and by the international community. The PSG 5 Revenues and Services relate to managing revenue and building capacity for fair and accountable service delivery (including health). 3: Trends in Maternal Mortality: 1990 to 2013; Estimates developed by WHO, UNICEF, UNFPA and The World Bank; : Levels & Trends in Child Mortality; Estimates Developed by the UN Inter-agency Group for Child Mortality Estimation; : Micro-Nutrient Survey; : FSNAU/ Deyr Assessment 2012/2013 Page 13 of 80
16 Somali macroeconomic performance is in a very poor state and resources for the health sector are mainly out-of-pocket or through donors support. The investment in health is negatively affected by a number of factors such as the global economic crunch, competing crises in the region and overall global reduction in aid by 4 per cent during This creates a very difficult operating environment for effective delivery of basic services in Somalia. Diaspora communities are a significant contributing factor to the un-documented economy and impact on households dependence on remittances. Large proportions of meagre national resources are spent on security, rather than basic social services. A narrow tax base and persistent inequality in resource allocation has led to a long-running neglect of these services. At the same time, corruption is a major risk and generates popular anger that threatens to further exacerbate tension and conflict. Transparency International (TI) indicates that the perceived level of public sector corruption (on a scale of 0-100), 7 is very low (eight) for Somalia the country ranked on the bottom of 177 countries in According to WHO s estimates 8, the total expenditure on health is only US$ 17 per person per year, much below the recommended figure of US$ 40 per person. The overall Government allocation is significantly lower than the 5 to 7 per cent average allocation to the health sector by East African counterparts and far lower than the 15 per cent requirement of the 2001 Abuja declaration. The biggest proportion of total expenditure on health is either out-of-pocket or through donor assistance. In CSZ, the health sector allocation progressively increased from 0.99 per cent in 2011 to 1.98 per cent in 2012 and 2.2 per cent in NEZ has allocated 1.73 per cent (US$ 313,719) of the national budget to health in In 2010, the figure was lower at 1.45 per cent (US$ 361,520) of the overall national budget of US$ 25 million. It was again lower in 2011, with just 1.38 per cent (US$ 412,129). Although, in nominal terms, the national health budget has increased due to increased revenue collection, it remains less than a mere 2 per cent of the overall national budget. In NWZ, the overall picture looks better with an increasing budgetary allocation for health. In 2009, the government allocated 2.72 per cent (US$ 687,008) of its national budget to the health sector. In 2010, the allocation was slightly higher at 2.83 per cent (US$ 836,553) and in 2011 the allocation increased to 3.08 per cent (US$ 1,556,647) of the total Government budget. In the recently announced 2014 budget for NWZ, a total of 14.4 per cent has been allocated to social sectors. Of this, the greatest share (81 per cent) has been earmarked for Education and Health, which represents 7.7 per cent and 4 per cent of the total budget respectively. Health sector fiduciary risks include budget variations, payment arrears, unreported operations, limited access to key fiscal information, weak payroll controls, internal audit functions, procurement controls, external audit scrutiny and legislative scrutiny etc. 7 Where 0 means that a country is perceived as highly corrupt and 100 means it is perceived as very clean/not corrupt. 8 WHO EMRO health system observatory Page 14 of 80

17 2. Planned Outputs, Activities and Results Output 1: Governance and Leadership Improved governance and leadership at all levels of the health sector 1.1: Core Health Sector Policies, Framework, Strategies and Plans in place Milestone: i: Annual work plans with budget in place, ii: NWZ: Human Resource Policy developed, Legal framework and Public Health Law drafted, National Health Act approved; NEZ: Health Policy, Operational Plan and Human Resource Policy developed; CSZ: Health Policy and Human Resource Policy developed. Progress: WHO and UNICEF, with the support of a Strategic Planning Task Force in each zone, supported the Health Authorities in developing their first zonal HSSPs. The three HSSPs were finalized in early 2013 along with three zonal Annual Work Plans (AWP) for Implementation of the strategic priorities and activities started with the support of multiple funding channels including JHNP, GFATM, GAVI and HCS etc. Limited public sector financing was available and implementation remained largely dependent on the donors financing NWZ has already developed its Health Policy with the support of Tropical Health & Education Trust (THET) but the three zonal health authorities agreed to develop a Somali Health Policy, for which consultations were completed and a draft made available in the first quarter of Nutrition Plans of Action were developed for all three zones in alignment with the HSSPs, and provided an estimation of the financial costs for priority at scale nutrition interventions. This is envisaged to strengthen the planning process within the sector and contribute to the development of investment cases for child and maternal nutrition. Final endorsement of the plans is still pending Assessment work of Human Resource for Health (HRH) in CSZ and NEZ was completed along with consultations on HRH policy and plans for CSZ and NEZ in partnership with the Banadir University and the Puntland Development Research Centre (PDRC). The HR policies and plans were finalized by March 2014 but need endorsement of the health authorities. The HR policy in NWZ was developed and is operational with the support of THET under the HCS project. Page 15 of 80
18 1.1.5 TOSTAN s activities related to Female Genital Mutilation/Cutting (FGM/C) in Somalia began in 2006, when UNICEF provided support to the pilot Community Empowerment Programme (CEP) titled Ending Female Genital Mutilation/Cutting in Somalia. CEP aimed to empower communities to create healthier, more gender sensitive, environmentally sound and financially secure lives. In 2013, the evaluation of the programme was completed for NWZ and NEZ through JHNP support. Evidence is being used to learn lessons for the improvement of programmatic interventions and to support the Somali authorities to develop legislation and policy on FGM/C. Drafts of FGM/C abandonment policy and legislation were developed with the Puntland authorities in 2013 and the policy was approved in February JHNP continued to support FGM/C taskforce monthly meetings to develop and implement activities - working closely with the Ministry of Women Development and Family Affairs (MoWD&FA), the Directorate of Gender (DoG) and the MoHs UNFPA completed the consultations on the revision of the Somali RH Strategy the draft was shared with stakeholders for review. UNICEF has completed consultations for the development of the Micronutrient Strategy and WHO selected a firm for the development of the Community Based Health Strategy WHO completed assessments for the Public Health Law and on Right to Health for CSZ, NEZ and NWZ using WHO tools. The assessments present a range of international instruments that cover basic public health obligations, which have been applied at international and country level to secure the rights for its citizens. Reports are currently under review for quality assurance, after which WHO plans to support the drafting of the Public Health Law/National Health Legislation Framework with the support of WHO/JHNP. These assessments are likely to set the road map for a series of legislation/laws required in the health sector and all three UN partners will be supporting health authorities in this regard FGS organized the National Health Conference in Mogadishu (7-9 November 2013), to which it invited key health stakeholders from the Government, Somali health professionals from within and outside the country, universities, private sector and other partners. The aim of the Conference was to deliberate on supporting the vision of universal health coverage through revitalization of the national health system towards current and anticipated health needs of individuals, families, communities and the country as a whole. Following three days of intensive discussions and deliberation, the stakeholders agreed on the National Health Conference Declaration and committed to the resolute implementation of the recommendations outlined in the declaration. 1.2: Health Sector Coordination is functioning at Central/Nairobi, Zonal and Regional Level Milestone: i: MoH leading/conducting Annual Joint Health Sector Review, ii: Health Sector Committee (HSC), the Health Advisory Board (HAB), JHNP s Technical Coordination Group (TCG) and Steering Committee (SC) meetings regularly held, iii: Roll-out of annual work plans, iv: Leadership and Capacity Building plan developed and implementation started. Progress: The first Joint Annual Review of HSSP/AWP-2013 was planned with the following three core objectives: Page 16 of 80
19 1. To assess the progress of the three HSSPs/AWPs-2013 and the contribution of both public sector financing and the four key aligned programmes i.e. GFATM, GAVI-HSS, JHNP and Health Sector Coordination (HSC), against specific outcomes, outputs and activities, 2. To identify potential constraints to the implementation of HSSPs, 3. To support the three Somali health authorities in developing AWPs for A task force led by the health authorities was formed to work with a team of consultants to deliver the above-mentioned outputs. Bids were invited for the selection of a team of consultants but after limited responses, the committee decided to re-invite bids to ensure fair competition. The Joint Annual Review took place in Puntland and Somaliland in early 2014 but delayed in CSZ for security reasons. Programmespecific Annual Work Plans of the JHNP and other core development programmes have already been developed and were agreed with the health authorities these will become an integral part of the AWPs Following review and development of AWPs-2014, the task force will decide on the revision of the three HSSPs, considering gaps and recommendations of the review In the initial phase, the JHNP supported individual supervisory activities related to MCH, EPI and Nutrition etc. It was later agreed that Zonal Health and Nutrition Coordination Forums (ZHNCF) and JHNP Zonal Working Groups (ZWGs) will conduct quarterly joint supervisory visits to regions and districts to review the performance and implementation of AWPs. The joint supervisory teams will use the supervisory tools developed under the GAVI-HSS programme. GAVI plans to train supervisory teams on these tools by mid The HAB met twice, in March and September 2013, as scheduled. The HSC meeting convened three times in March, June and September Efforts were made to hold the June HSC in Mogadishu, but due to security concerns the meeting was eventually convened in NEZ with NWZ representatives unable to attend. Rest of the meetings were held in Nairobi and all parties were represented Between 2012 and 2013 the Health Sector Coordination Office (HSCO) and staff was funded by DFID through UNOPS. The cost of coordination meetings (HAB and HSC) was supported by JHNP through WHO. DFID support through UNOPS ended in September In a JHNP SC meeting held in July 2013, the three UN partners representatives proposed the option of a stronger leadership role for the zonal health authorities moving forward. The proposal was supported by the Somali health authorities. In the following JHNP SC meeting held on 1 November 2013, the UN agencies reiterated the agreement with the three ministers and donors, and it was agreed that WHO will release a communiqué to all stakeholders to this affect JHNP s TCG meetings were held on 18 February, 1 July, 6 September and 28 October 2013 in addition to a number of e-polls to make decisions on urgent issues. Efforts were made to organize these meetings within Somalia and the July meeting was hosted by the MoH NEZ. However, NWZ s representatives were unable to attend. Four SC meetings were held in 2013 (on 20 March, 30 August, 4 October and 1 November). Key strategic and financial allocation decisions were made in these meetings. In a SC meeting in November 2013, it was agreed to reduce the number of SC meetings to every six months rather than every quarter. This cycle has since been followed Meetings of JHNP s Zonal Working Groups (ZWG) were held almost monthly in all three zones, in order to expedite the roll-out of the EPHS in targeted regions and to plan other JHNP activities. Similarly, meetings of zonal health sector committee (ZHSC) were held regularly in NWZ and less regularly in NEZ. However, ZHSC meetings were not held in CSZ on a regular basis due to security Page 17 of 80
20 concerns and financial constraints. Support to working groups, especially the Reproductive and Maternal Health Working Groups, as well as the Nutrition and the FGM/C working groups, continued during the reporting period. Coordination mechanisms have helped not only in developing consensus but also in the roll-out of HSSPs AWP-2013, JHNP planned activities and other programmatic interventions Effective governance, leadership and management is widely recognised as a prerequisite to an effective and equitable health system. Health authorities in the three zones are currently developing their respective roles in governance and stewardship of the health sector. While challenges remain, discussions took place on how to establish a more effective and equitable health system. In 2011, GFATM supported a participatory process to develop a plan to strengthen governance, leadership and management within health authorities. The process was led by the three zonal health authorities and supported by WHO in collaboration with other development partners. The draft plan was finalized in 2013 with a total cost implication of US$ 11,442,862 over four years. Considering the high cost implication, the health authorities agreed on the following strategic priorities to be supported through JHNP in the initial phase: Training programme of Leadership and Management capacity-building i.e., o e-mph courses for senior managers in three ministries, o cost effective international/regional tailored programme for mid-level managers (while building the capacity of Somali institutions), Clarity on roles and responsibilities in the MoH, especially in CSZ, Development/upgrading of systems and linking them to capacity-building through learning by doing, Long-term technical assistance and support to strengthen management role. Some capacity building priorities related to roles and responsibilities are under implementation now, while the modalities of others are being finalized The zonal health authorities identified three areas for long-term technical assistance, i.e. RH advisers, monitoring and evaluation (M&E) advisers and advisers to support contracting of EPHS. Three RH Advisors who are based in the three zonal Ministries of Health play an active role in the JHNP s ZWGs and RH groups by contributing to the revision of RH policy (to include birth spacing and related issues), provide technical support to the implementation of RMNCH activities and train clinical staff on birth spacing, EmONC etc. Selection of M&E advisors took place and came on board in early To roll out EPHS, the three MOHs led the ZWGs in completing all processes including assessment, micro planning, and selection of NGOs and proposals review. This was a learning by doing exercise where the role of the health authorities was central and key to success. Senior UN staff from the three agencies (both Nairobi and Zonal based) were actively involved with the health authorities/zwgs to provide back-stopping. Output progress against expected results: Overall, the programme has largely achieved both milestones under output 1, in addition to delivering significant additional milestones which, while not set out in the Log Frame for 2013, helped position the programme on a positive trajectory to meet the overall output objectives by the end of the programme life cycle. Page 18 of 80
21 Milestones End of 2013 status Core Health Sector Policies, Framework, Strategies and Plans in place i: Annual work plans with budget in place. Fully met Performance Trajectory by end 2013 ii: NWZ: Human Resource Policy developed, Legal framework and Largely met Public Health Law drafted, National Health Act approved; NEZ: Health Policy, Operational Plan and Human Resource Policy developed; CSZ: Health Policy and Human Resource Policy developed. 1.2: Health Sector Coordination is functioning at Central/Nairobi, Zonal and Regional Level: i: MoH leading/conducting Annual Joint Health Sector Review. Partially met ii: HSC, HAB, JHNP s TCG and SC meetings regularly held. iii: Roll-out of Annual work plans. iv: Leadership and capacity-building plan developed and implementation started. Largely met Fully met Largely met Positive progress was made despite the following constraints: Change and volatility in the security situation; changes in political leadership; change in management; and ambiguity about roles and responsibilities in health authorities, Non-availability/un-willingness of consultants/firms to work in conflict affected areas, A changing mind-set from a humanitarian to a more development approach, Financial constraints and un-predictability in funding. The above notwithstanding, the programme has prioritised interventions and focused on those activities that are expected to better contribute towards the expected outcomes. Recommendations: A series of policy and strategic documents are in their final stages of development/revision in consultation with stakeholders; the health authorities should prioritize their approval in a reflection of commitment for improved Somali health provision; As decided, strengthen the leadership role of the zonal health authorities as the way forward for the new coordination mechanism especially in CSZ; Health authorities should strengthen inter-sectoral coordination activities and prioritize social issues such as FGM/C and WASH, through the health sector, as these have long-lasting impact on the health outcomes especially for women and children; Engage top Somali political leadership to prioritise health as the entry point for peacebuilding and state-building initiatives; Constrained activities to be reviewed more frequently to develop consensus and remove hurdles. Impact weighting (per cent): 20 per cent Revised since last Annual Review: The output was updated, revised and approved by SC in Page 19 of 80
22 Risk: HIGH. Risk continues to be HIGH, especially in light of the political and security context. The peaceful election process and subsequent smoothly implemented changes in the Government are positive signs. However, institutional risks and ambiguity about roles and responsibilities continue to prevail. The new Government needs to express their commitment to address health and especially RMNCH and nutrition issues through endorsement of newly developed policies, strategic documents, legislation and enhanced public sector financing/expenditure in future. Technical support on policy and strategic issues is available, mainly through UN agencies and international NGOs. Economic and fiduciary risks remain high and health outcomes are largely dependent on donor financing. Donors committed more funding during the 2013 Brussels conference, however, overall there is a sharp decline in humanitarian support. Availability of qualified managers and planners (especially female) in the health authorities is another constraint. Output 2: Health Workforce Skilled and trained public health workforce produced and distributed equitably to deliver RMNCH and nutrition services 2.1: Proportion of public health facilities having skilled health care providers according to EPHS guidelines Milestone: i: CSZ and NEZ - HR policy developed; ii: CSZ and NWZ - Health workforce plan developed; iii: CSZ and NEZ - Levels of remuneration standardized, published and circulated to donors and NGOs. Progress: The formulation of HRH policies for CSZ and NEZ is a major milestone achieved in 2013, providing an opportunity to develop an important component of the health system. The HRH assessment and policy development process was closely coordinated by a team of senior consultants from the Banadir University and the Puntland Development Research Centre (PDRC) - both contracted by WHO. The human resource departments of the two MoHs acted as the focal points coordinating the stakeholder workshops conducted during the course of this study. The HRH policy development process was organized in two principal phases: (i) Human Resources assessment phase and (ii) HRH policy analysis and formulation. A consultative process was ensure, with contributions from senior Ministry staff; regional medical offices; hospitals and health facilities; various professional associations; representatives from universities and academic institutions with health training programmes; the Somali diaspora; the Somali Federal Parliament Social Committee; the National Civil Service Commission; UN agencies and international and national NGOs. The assessment highlighted that the coverage rate of doctors, nurses and midwives per 1,000 population in CSZ and NEZ is only 0.29 and 0.4 respectively, compared to the minimum threshold of 2.3 doctors, nurses and midwives per 1,000 population which is considered by WHO to support the achievement of the MDGs. Accordingly, the two HRH policies emphasized the production and supply of health workers, aligned with the HRH goals of the health system as outlined in the national EPHS, thus Page 20 of 80
23 forming the basis for improving the promotive, preventive, curative and rehabilitative services of the health system, during the ensuing nation-building phase of health sector recovery. The HRH policy triggered the development of health workforce strategic plans both for CSZ and NEZ and translated the set policy aspirations into action. HRH assessments, policies and plans for the two zones are currently under review by the two ministries before final approval. The health workforce strategic plan for NWZ was developed by the MOH NWZ with the support of THET under the HCS project UNICEF hired a consultancy firm (Mannion Daniels) in November 2012 to gather information on the remuneration of health staff and to design a remuneration framework along with recommendations concerning future remuneration levels. The consultants visited Nairobi, Hargeisa, Garowe and Mogadishu, interviewed representatives of Government, at central and local levels, implementing partners, funders, service delivery staff, academics and others about their remuneration practices and their views on the future of remuneration of health workers. In parallel, a detailed questionnaire was circulated to partners, seeking information on the staff they paid or funded, remuneration levels, pay and human resource management processes. Interviews also included questions on remuneration rates paid and proposed for principal health cadres in order to understand the range of remuneration practices and proposals. The Review of Compensation, Salaries, Incentives and Benefits for Health Personnel in Somalia report was drafted in January 2013 and shared with all stakeholders. The report was finalized in March 2013 and all stakeholders endorsed the report, highlighting the two key elements as the salary scale (medium scenario) and the building/strengthening of adequate management systems within the health institutions The JHNP s TCG met in July 2013 and asked JCU to facilitate the development of a payroll format for salary top-up support through JHNP. The format was developed in consultation with the three UN agencies and agreed in the subsequent TCG meeting. However, health authorities faced difficulties in identifying the core staff to be supported through JHNP. Salary top-ups were paid to the nutrition team at zonal and regional level in 2013 through JHNP funds. In future this will be a part of MoH payroll for the JHNP. UNICEF has aligned salary top-up support for the district and facility staff with the medium scenario through the Partnership Cooperation Agreement (PCA) process with the implementing agencies. A DFID-led working group on HR also reviewed the issue across the sector through regular meetings of stakeholders. 2.2: Number of health workers securing professional accreditation Milestone: Progress: i: NWZ - standards for registration, accreditation and licensing in place, voluntary registration system and operational NHPC database, ii: CSZ and NEZ - business plan for professional associations in place The NWZ National Health Professions Commission (NHPC) is a statutory body with the mandate of regulating, accrediting and licensing health facilities, health training institutions and health workers in the country, formed under an act passed by the NWZ parliament in Since its formation in 2001, Page 21 of 80
24 the HNPC has gone through a spate of challenges and remained non-functional until 2008 when efforts were made to reconstitute it. In January 2013, NWZ s president signed into law the much-debated amendment of the Health Regulatory Act. This achievement meant that the commission could implement its core activities and operationalize its mandate. The commission has been operating with the support of THET under the Somalia Health Consortium. In addition, the commission received JHNP support through WHO (amounting to US$ 48,200) to support ongoing work on the following three activities: Relay a series of media awareness about the Health Regulatory Act, Conduct a baseline assessment and pre-registration workshops, Technical support for the commission to exercise its mandate The HRH plans for NEZ and CSZ identified the strategic need of Improving HRH regulation and professional standards in the health sector and accordingly activities have been planned. The proposed activities include the formation of Professional Health Associations to address the processes of certification; registration of health professionals with established by-laws; acts and codes of practice. An assessment for the legislative framework was completed by WHO/JHNP, which identified the need for legislation to regulate professional standards. Some of the activities are expected to be the part of HSSP s AWPs : Number of health workers trained in RMNCH and nutrition by accredited training institutes: Milestone: i: Training of 80 midwives completed in seven midwifery schools, ii: Preparation completed for the first intake of clinical officers diploma training. Progress The shortage of female health care providers and especially Skilled Birth Attendants (SBAs) is a critical constraint to the functioning of the Somali health system. The programme is targeting midwifery schools as a long-term investment. However, strengthening of these schools would be important for training of nurses and other paramedics in future. Through UNFPA, support was provided to strengthen eight out of nine planned midwifery schools in all three zones: four in NWZ, three in NEZ and one in CSZ. One more midwifery school became functional in Baidoa (Bay) in early Two newly established midwifery schools: one in Mogadishu (August 2012) and one in Gaalkacyo (August 2013) are now functional. Midwifery schools currently getting JHNP support (both for strengthening/running cost of schools for midwifery training and the stipend of student midwives and post-midwives) are as follows: NWZ: 1. Hargeisa School of Health Sciences - Maroodi-Jeex 2. Edna Adan University Hospital - Maroodi-Jeex 3. Amoud University School of Nursing and Midwifery - Awdal 4. Burao School of Health Sciences - Togdheer NEZ: 1. College/University of Health Science, Bossasso - Bari 2. Haji Abdi Nursing and Midwifery School - Nugaal 3. Gaalkacyo Midwifery/Nursing School - Mudug Page 22 of 80

25 CSZ: 1. Mogadishu Midwifery School - Banadir 2. Baidoa Midwifery School - Bay By the end of December 2013, 135 students completed their basic midwifery training from the above mentioned schools, 194 new students are currently undergoing training. Similarly, 32 midwives have completed post-basic training in NWZ and CSZ - 55 are currently in class in all three zones. The Basic midwifery training is two years long whereas post-basic midwifery training is of 18 months duration. Details of midwifery training are as follows: Page 23 of 80
26 S. N o Table: MIDWIFERY SCHOOLS AND MIDWIFERY TRAINING SUPPORTED BY UNFPA/ JHNP AND STATUS IN MARCH 2014 Name of Midwifery school 1 Hargeisa School of Health Sciences 2 Edna Adan University Hospital 3 Amoud University School of Nursing and Midwifery 4 Burao School of Health Sciences Region Date of establish ment Midwives completed training (Basic) Midwifery students - currently in class (Basic) Graduation due date Midwives completed training (Post-Basic) Maroodi-Jeex October 2014 Maroodi-Jeex Awdal October 2015 Midwifery students Currently in Class (Post-Basic) Note: UNFPA is supporting the strengthening/ running cost of midwifery schools and stipend of students. However, stipend of some students and infrastructure development support has also been provided by some International NGOs. Graduation due date Togdheer due in October 2014, October July 2014 Bossaso, Bari February 2015 Nugaal September 2014 Mudug September 5 College/University of Health Science 6 Haji Abdi Nursing and Midwifery School 7 Gaalkacyo Midwifery/ Nursing School Mogadishu Midwifery Banadir February School Baidoa Midwifery Bay December School 2015 TOTAL: December 2015 Page 24 of 80

27 2.3.2 One of the key barriers to the provision of comprehensive reproductive and obstetric care services is the lack of skilled providers. To address the challenge, Somali Health Authorities identified the need for the development of an Emergency Obstetric Care Diploma which aims at building capacity of the clinical officers to complement EmONC which are important components of the EPHS. A nine month training course has been developed with course materials consisting of i) Trainer Manual, ii) Guide for the trainer, and iii) A Participant Manual. The course consists of a theoretical phase, a practical phase and a clinical phase and focuses on following skills: Essential and basic EmONC, Clinical training for Emergency RH, Emergency obstetric surgery, including postpartum hysterectomy and laparotomy for ectopic pregnancy, New-born care and resuscitation, and The acquisition of life-saving skills. WHO has identified the training facilities and tutors, and plans to start the training in In 2013, UNFPA supported the health authorities in developing Birth Spacing Guidelines for Somalia in a workshop in Kampala, Uganda. These guidelines are now ready for further review at the zonal level before final endorsement and distribution. WHO completed the activity of revision of Standard Treatment Guidelines for Somalia and is planning to start the training of health staff when funds are available. WHO developed a training curriculum for Community Health Workers (CHWs) and shared it with zonal authorities in NEZ and CSZ for their final endorsement Short training courses: UNFPA completed the training of 46 midwives and nurses in NEZ and 40 midwives in NWZ on BEmONC. 40 midwives in NEZ and 80 midwives in NWZ completed the training of trainers on modern contraceptive methods and birth spacing counselling techniques. Trickle down of these training for facility staff is planned for Page 25
28 JHNP funds contributed to Nutrition, Health and Hygiene Promotion (NHHP) trainings conducted from May through December This included cascade trainings for six IPs and 18 MoH/UNICEF staff in NEZ, as well as four IPs and 18 MoH/NICEF staff in NWZ. The programme supported the development and piloting of an integrated package for NHHP. Standardized, integrated, and comprehensive NHHP is an important part to the joint WASH and nutrition approach, as it increases adequate nutrition, hygiene and health-seeking behaviours. The package was specifically designed to improve the quality of promotion activities at nutrition sites and at health facility level. To date, UNICEF has supported the development of 134 master trainers from 103 partners covering almost all regions of Somalia. At least 16 of these partners have been supervised to conduct roll-out trainings for 79 promoters. The programme also contributed to Integrated Management of Acute Malnutrition (IMAM) trainings in NEZ for four Nutrition IPs and MoH staff. IMAM trainings ensure enhanced adherence to admission and discharge protocols, while promoting key aspects of a holistic Basic Nutrition Services Package (BNSP). Progress against expected results: Overall, the programme has achieved all three milestones under output 2. Given the substantive additional work undertaken to help the programme achieve its overall outcome, the programme is currently on a positive trajectory and is substantially exceeding expectations, given the targets set. Milestone End of 2013 status Performance Trajectory by end Proportion of public health facilities having skilled health care providers according to EPHS guidelines: i: CSZ and NEZ: HR policy developed. Fully met ii: CSZ and NWZ: Health workforce plan developed. Fully met iii: CSZ and NEZ: Levels of remuneration standardized, published Fully met and circulated to donors and NGOs. 2.2: Number of health workers securing professional accreditation: i: NWZ: standards for registration, accreditation and licensing in Fully met place, voluntary registration system and operational NHPC database. ii: CSZ and NEZ: business plan for professional associations in place. Fully met 2.3: Number of health workers trained in RMNCH and nutrition by accredited training institutes: i: Training of 80 midwives completed in seven midwifery schools. Exceeded milestone ii: Preparation completed for first intake of clinical officers Fully met diploma training. Health authorities and UN agencies have prioritised interventions to achieve targets and should maintain the pace as future milestones are more challenging and critical to contribute towards the outcomes. Page 26
29 Recommendations: High-level advocacy required to implement the HRH policies and plans, as there is scarcity of resources, Health authorities to work with UN agencies and partners to standardize all public health and nutrition trainings and to institutionalize in-service training with a knowledge and skill monitoring mechanism, Need to explore options to further scale up midwifery training especially in CSZ, Plan to scale-up community level multi-purpose health workforce, Health authorities to finalize and share payroll with partners to ensure transparency in the use of funds. Impact Weighting (per cent): 20 per cent Revised since last Annual Review: The output was updated, revised and approved by the SC in Risk: HIGH. Risk continues to be HIGH. Sustained commitment of the Government is required to invest in human capital. Political and security risks are the major factors for the brain drain of health workforce and low investment in human capital. Good progress was made on developing policies and plans, at the same time these need to be implemented - considering efficiency and equity needs. Private sector and civil society have limited capacity but openness of the Government to encourage them could be helpful. The Somali diaspora needs to be attracted to contribute to nation-building. Institutional risks and ambiguity about roles and responsibilities is affecting the performance in this output. Economic and fiduciary risks remain high. The Governments need to be proactive and transparent in the use of public and donors funds e.g. to pay salary top-up and incentives, liquidation of released funds on time with proper documentation and to take disciplinary actions against malpractices. Output 3: RMNCH and Nutrition Service Delivery RMNCH and nutrition services available and utilized 3.1: Proportion of health facilities providing EPHS services in targeted regions of JHNP Milestone: i: NWZ: EPHS phase 1 started in two regions, ii: CSZ: 10 per cent of assessed health facilities in pilot areas providing EPHS services, iii: NEZ: 70 per cent of health services in two regions provide EPHS services. Progress: The critical steps and responsibilities in the roll-out of EPHS through JHNP were agreed as the following: 1. Assessment/situation analysis of the health system in a region: Responsibility sits with the ZWG led by Director of Planning, the MoH and participation of senior MoH staff, zonal UNICEF, UNFPA, WHO staff and observers. 2. Micro-planning based on situation analysis: ZWG led by Health Authorities. 3. Selection of NGO to implement EPHS: ZWG led by Health Authorities (one NGO per district to avoid multiple small contracts at health facility level). 4. Review of the process at zonal level: TCG led by the Health Directorate and participated by senior UNICEF, UNFPA and WHO staff and one donor as observer. Page 27
30 5. Prioritization of districts in a region to roll-out EPHS considering funds availability: ZWG led by Health authorities. 6. Proposal development and submission: selected NGO to UNICEF. 7. Review of the proposal: feedback to NGO, resubmission of proposal, negotiations on the work-plan and budgets, completion of PCA formalities and submission - Health authorities and UNICEF. 8. Final Review: UNICEF Risk committee and PCA committee (independent of UNICEF technical team). 9. Agreement and signing of PCA - UNICEF and partner NGO. The following table shows the progress on EPHS roll-out by end 2013: Actions Assessment (date) Micro planning (date) ZWG meeting to pre-select/select NGOs UNICEF and NGO discussions on proposal and budget completed Tentative PCA signing date Responsible Parties Health Auth Health Auth Health Auth/ UN agencies UNICEF / Health Auth Nugal Jun-13 Jul-13 Jul-13 Oct-13 Oct-13 UNICEF PUNTLAND Bari Feb-14 Mar-14 Apr-14 May-14 May-14 Mudug Jun-13 Sep-13 Oct-13 Apr-14 Apr-14 Togdheer Jun-13 Jul-13 Jul-13 Aug-13 Sep-13 SOMALILAND Awdal Dec-13 Mar-14 Oct 13/ Apr 14 Sanaag (Erigavo & El-Afweyn) Apr-14 May-14 Feb-14 Apr-14 Apr-14 May-14 May-14 Gedo Jul-13 Sep-13 Oct-13 Lower Juba timeline to be agreed CENTRAL SOUTH Galgadud Jul-13 Sep-13 Oct-13 Feb/Mar-14 Apr-14 Banadir Jul-13 Sep-13 Oct-13 Mar/Apr-14 Apr-14 Activity completed in 2013 Activity to be completed by The table shows that in 2013 in NWZ, EPHS has been rolled out in Togdheer under JHNP. The ZWG in CSZ has shown a good progress in completing the formalities before final agreement with the NGOs. As a result, EPHS contracts were finalized in Banadir and Galgadud in the first quarter of In NEZ, EPHS was rolled-out in Nugaal under JHNP. Sahil in NWZ, Karkar in NEZ and Gedo in CSZ are already covered under the DFID funded HCS programme. Page 28
 and Somalia Red Crescent Society (SDCS).")
31 The implementing partners in Togdheer are World Vision International (WVI) and Somali Red Crescent Society (SRCS). In Nugaal implementing partners are NWZ Community Development Organization (SCODO) and Somalia Red Crescent Society (SDCS). It is expected that EPHS will be rolled-out in eight of the targeted nine regions by end of the second quarter of However, scaling up of services depends on the availability of funds. 3.2: Proportion of health facilities providing round-the-clock EmONC services in targeted regions Milestone: i: 10 per cent of targeted hospitals offering round-the-clock EmONC services. Progress: In 2013, UNFPA/MOH-CSS (with JHNP funding) signed contract agreements with WAHA International and Swisso Kalmo to strengthen round-the-clock EmONC services in Banadir Hospital and Page 29
32 Galgadud Hospital. Hospitals were upgraded, new qualified staff was employed, equipment and RH kits and supplies were made available to be used in maternity wards, Outpatient Department (OPD) and operation theatres. Monthly progress reports indicate a rise in admission, deliveries and caesareansection rates in the hospitals Through JHNP funding, UNFPA provided kits and equipment for referral hospitals in NWZ and NEZ for CEmOC and BEmOC services. Three maternity waiting rooms, providing basic obstetric, ante- and postnatal services and neo-natal care are now functional in Garowe, Gaalkacyo and Bossaso UNICEF supported two facilities in Bossasso, two in Garowe, two in Gaalkacyo, and seven facilities in Boroma and one in Burtinle for BEmONC services through JHNP and EC funding To work in a more systematic way, it was decided in a TCG meeting that health authorities will share list of hospitals to be upgraded for CEmONC services in the targeted regions with UNFPA/JHNP. UNFPA will present a plan on how to improve CEmONC services in a phased manner and monitor activities. WHO will work with UNFPA to ensure blood bank services in those hospitals in case support is not available through GFATM. Furthermore, UNICEF ensured provision of BEmONC services in health facilities covered under the EPHS roll-out. 3.3: Health Facility Utilization Rate (HFUR): Milestone: i: 0.4 visits per person per year. Progress: There are three critical factors which influence the health facility utilization rate of the three zones, and these must be taken into account: i. Knowledge of the total population of a zone or region as currently no reliable information exists preventing an accurate estimation for HFUR from being calculated. ii. Information from PHU/Health posts is not available as HMIS is not operational at that level. iii. Data of all expected HMIS reports is not available - for example HMIS have no reports from hospitals in CSS. In NWZ, OPD data from MCH/HC was available but not from hospitals. Based on the limited data available, HFUR in the three zones is calculated as per the table below. However, where full reports are made available, it is estimated that HFUR for all the three zones was more than 0.35 visits per person for the year Table: Health Facility Utilization Rate % of HMIS reports for 2013 received by mid Feb 2014 Total OPD visits in 2013 OPD visits per month Health Facility Utilization Rate 2013 Somaliland (only MCH/HC) 70.1% 573,998 47, Puntland (MCH/HC and Hospitals) 73.7% 485,516 40, Central South (only MCH/HC) 12.5% 200,386 16, Female: male ratio varies from female patients as compared to 100 male patients in three zones. Page 30

33 3.4: Number of children immunized for Measles in targeted regions: Milestone: i: NWZ: 30 per cent, ii: NEZ; 20 per cent, iii: CSZ: 20 per cent. Progress: Due to lack of funds, no survey was conducted in 2013 to show progress of zonal or regional immunization coverage. HMIS 2013 s data was used to estimate the number of children immunized in the targeted regions of the three zones. While interpreting the data, the HMIS reporting pattern needs to be considered. Table: Children Immunised against Measles at MCH/HC through routine services in 2013 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total Average/ month SOMALILAND Awdal , Togdheer , Sanaag , PUNTLAND Bari , Nugal , Mudug , CENTRAL SOUTH Galgadud , Banadir , Lower Juba Overall, the immunization coverage for measles is showing a positive trajectory in the targeted regions as shown in the above table. It is expected that with the roll-out of EPHS in 2014, the services will improve further. The 2013 data will be used as a baseline for the effectiveness of immunization services. It is critical to improve HMIS reporting to monitor the trend correctly along with validation/ verification of HMIS data on a regular basis. Page 31

34 3.5: Proportion of women receiving multiple micronutrients during pregnancy and lactation: Milestone: i: Reporting started on performance. Progress: Considering the high level of micronutrient deficiency, the health authorities and UN agencies are promoting the use of multi-micronutrients especially during pregnancy and lactation. HMIS 2013 s data for the targeted regions was used to estimate visits of pregnant and lactating women provided with multimicronutrients at MCH/HC level. Table: Visits of Preganant and Lactating women provided Multi-micronutrients (MMN) in 2013 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total Average/ month SOMALILAND Awdal , Togdheer , Sanaag , PUNTLAND Bari , Nugal , Mudug , CENTRAL SOUTH Galgadud Banadir , Lower Juba Overall trajectory of prescription of multi-micronutrient to women visiting MCH/HC is positive and the HMIS 2013 s data will serve as a baseline to review the effectiveness of EPHS in Micronutrient activities have significantly increased the availability and uptake of micronutrient supplementation, especially zinc for diarrhoea treatment and multiple micronutrients for women. The programme continued to ensure that health workers are equipped with knowledge on micronutrients (especially multiple micronutrients, deworming and zinc) in order to enable them to make appropriate recommendations to beneficiaries at MCHs and other facilities. Since January 2013, 113,379 pregnant women have been supplied with multiple micro-nutrient tablets during antenatal care visits in health facilities in NWZ and NEZ. Health interventions through the JHNP and other programmes will ensure better coverage and quality at the facility level for multiple micronutrients. The new emphasis on community based programming and the preventative and promotion aspects will help to ensure compliance with supplementation regimes, and significantly improve coverage. Page 32

35 3.6: Proportion of mothers initiating breastfeeding within one hour after birth Milestone: i: NWZ: 62 per cent, ii: NEZ; 58 per cent, iii: CSZ:20 per cent. Progress: HMIS 2013 s data indicates a sharp increase in breastfeeding promotion activities at MCH/HC. However, the quality of the counselling and behaviour change needs to be reviewed through formative research. Communication materials need to be provided. The trend of the indicator in the targeted regions is as follows: Table: Mothers initiating Breast Feeding within one hour after birth in MCH/HC in 2013 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total Average/ month SOMALILAND Awdal , , Togdheer , Sanaag , PUNTLAND Bari , Nugal , Mudug , CENTRAL SOUTH Galgadud Banadir , Lower Juba However, when this was compared with the number of deliveries in MCH/HC, the proportion was above 100 per cent. This indicates misreporting in HMIS or lack of understanding of definition or issues in filling the reports. Regular use of information, analysis at all levels and HMIS validation/verification exercises can improve the quality of data, which will be helpful for the monitoring of programmatic interventions IYCF activities, harmonized with the IYCF Strategy and Action Plan for NWZ, NEZ, and CSS, continued to take place within health facilities and communities. They are considered within all emergency response plans. IYCF counsellors were instrumental in addressing necessary aspects of maternal nutrition. 3.7: Number of health facilities offering birth spacing services Milestone: i: EPHS (including birth spacing) rolled out in health facilities in targeted regions. Page 33
36 Progress: Progress on roll-out of EPHS is shown above. Birth spacing interventions is integral to EPHS. UNFPA has procured RH commodities in 2013 and supplied these to zonal health offices. Training of Trainers (ToT) on modern birth spacing methods was completed and trickle-down training for facility staff is planned in : Number of regions with at least 90 per cent coverage of Integrated Management of Acute Malnutrition (IMAM) services Milestone: i: EPHS including IMAM rolled out in targeted regions. Progress: A number of strategic rationalization exercises were conducted in 2013 in order to ensure that the geographic coverage is applied in a rational fashion with a service available within 15 km of a large number of population centres and 25 km for up to 95 per cent of population centres. This strategic reduction and repositioning of nutrition centres resulted in a minimum fixed site service plan that ensured optimal geographic coverage while minimizing overlap in services. This allowed for the delivery of consolidated services that economize available resources, while improving the effectiveness of a holistic basic nutrition package in line with the changing nutrition situation and the recently formulated HSSPs From January through December 2013, UNICEF supported the treatment of 16,816 severely malnourished children under-5 in NWZ and 9,597 severely malnourished children under-5 in NEZ. Of this, JHNP funds contributed to the treatment of 3,689 children in NWZ and 106 children in NEZ. 3.9: Number of communities declaring abandonment of FGM/C Milestone: i: 21 communities in NEZ declare abandonment of FGM/C. Progress: In the Somali context, the primary reasons for the continuation of the FGM/C practice include tradition, perceived religious demand (not actually required), passage to womanhood, marriage eligibility, social standing and lack of knowledge about medical consequences. The FGM/C is a right infringement because girls are afforded no autonomy in which to decide whether or not to undergo the procedure which is unjust and against the United Nations Convention on the Rights of the Child (UN CRC); the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW); the African Charter on the Rights and Welfare of the Child; the African Charter on Human and People s Rights; and the Additional Protocol on Women s Rights (Maputo protocol). Therefore, Government has a right to intervene on behalf of affected girls and women through policies and legislation prohibiting all forms of the FGM/C practice. Page 34

 and 21 in NEZ (2013) were identified for community empowerment along with advocacy interventions with JHNP support.")
37 TOSTAN was contracted by UNICEF in 2006 to implement the TOSTAN Community Empowerment Programme (CEP). The goal of the project was to contribute to the reinforcement of community-led development in Somalia and contribute to the abandonment of FGM/C. TOSTAN developed an approach that precipitated documented positive social transformation in rural and urban areas. Twenty-one communities in NWZ (2012) and 21 in NEZ (2013) were identified for community empowerment along with advocacy interventions with JHNP support. The programme was evaluated in 2013 with JHNP support. BCC material was developed and used for the CEP. The support was also provided to develop policy and legislation on the FGM/C. FGM policy and FGM legislation were drafted for NEZ in 2013 and are currently under review by the government for approval Considering the need for more CEP interventions along with further work on advocacy, legislation and policy development JHNP submitted a proposal to USAID to scale-up the intervention in 80 new communities in Funding was approved and further investment has been included in the Joint Rolling Plan to access JHNP pooled funds from other donors for this activity. 3.10: Percentage of patients/clients satisfied with the provision of services from the health facilities in the targeted regions Milestone: i: Baseline established in CSZ Page 35
38 Progress: The information on the satisfaction level is being collected through a baseline survey in CSZ. Initial results are in The Programme has approved another activity of Annual Health Facility Assessment, through which the information will be collected from all the three zones in future. This will commence in : Percentage of mothers and caregivers attending OTPs with good knowledge for household sanitation and hygiene: Milestone: i: EPHS rolled-out in targeted regions. Progress: The EPHS package includes outpatient therapeutic programme (OTP) services. UNICEF continued training health workers on key aspects of the BNSP, in particular IYCF training, IMAM and NHHP. 3.12: Considering the low immunization coverage and poor health outcomes as highlighted in the MICS 2011 results, the health authorities proposed another round of Child Health Days (CHDs) in all three zones. US$ 500,000 was allocated for the operational cost of CHDs, provided UN agencies were able to generate additional required resources from other means. It is estimated that one round of CHD costs about US$ 7 million. Major funding for the activity came from Common Humanitarian Fund (CHF) and other sources identified by UNICEF and WHO. CHDs were successfully organized in CSZ from 22 to 26 December Polio vaccine was administered to 923,580 children, measles vaccine to 744,077 children and pentavalent vaccine to 177,079 children in CSZ. 885,822 women were also immunized against tetanus. In addition, 686,486 children were dewormed, 789,762 were given Vitamin-A supplements and Oral Rehydration salt (ORS) was provided to 917,254 children. CHDs for NEZ and NWZ were planned and completed successfully in February Table: Coverage of different services during CHD in CSZ (December 2013): Polio Measles Penta TT 1-5 Deworming Regions in CSZ (<5 year) (<5 years) (<2 years) (CBA) (12-59m) Vit A (6-59m) ORS (<5 years) GALGADUD 87,495 68,728 20,053 73,838 61,598 73,596 87,495 BAKOOL 16,539 13,666 3,318 16,541 12,429 14,408 16,539 BAY 101,328 82,930 18,252 94,835 79,421 87,226 96,138 HIRAN 45,643 35,530 8,872 36,892 36,515 41,942 45,643 LOWER SHABELLE 115,382 95,024 24, ,095 91, , ,382 MIDDLE SHABELLE 89,272 70,714 16,358 85,086 60,303 69,290 89,272 BANADIR 346, ,899 65, , , , ,921 GEDO 67,206 49,422 11,393 50,586 47,117 54,504 66,339 MIDDLE JUBA LOWER JUBA 53,794 41,164 8,735 46,534 38,730 45,730 53,525 TOTAL 923, , , , , , ,254 Page 36
39 Progress against expected results: Overall, the programme has largely achieved milestones under output 3. The main constraint is the delay in the roll-out of EPHS, mainly as a result of the paradigm shift from a traditional humanitarian process to a government-led development approach to engage NGOs for EPHS. This is a learning by doing exercise where the role of the government authorities is central and key for the success. Child Health Days were supported in 2013 to cover the gaps in service provision through the delay in EPHS. Milestone End of 2013 status 3.1: Proportion of health facilities providing EPHS services in targeted regions of JHNP: i: NWZ: EPHS phase 1 started in two region. Largely met ii: CSZ: 10 per cent of assessed health facilities in pilot areas Not met providing EPHS services. iii: NEZ: 70 per cent of health services in two regions provide EPHS Largely met services. Performance Trajectory by end : Proportion of health facilities providing 24/7 emergency obstetric care services in targeted regions: i: 10 per cent of targeted hospitals offering 24/7 EmONC services. Fully met 3.3: Health Facility Utilization Rate (HFUR): i: 0.4 visits per person per year. Largely met 3.4: Number of children immunized for Measles in targeted regions: i: NWZ: 30 per cent. ii: NEZ: 20 per cent. iii: CSZ: 20 per cent. Fully met as per HMIS data 3.5: Proportion of women receiving multiple micronutrient during pregnancy and lactation: i: Reporting started on performance Fully met 3.6: Proportion of mothers initiating breastfeeding within one hour after birth: i: NWZ: 62 per cent ; ii: NEZ: 58 per cent ; iii: CSZ: 20 per cent. 3.7: Number of health facilities offering birth spacing services: i: EPHS including (birth spacing) rolled out in health facilities in targeted regions. Fully met but HMIS data not conclusive Largely met 3.8: Number of regions with at least 90 per cent coverage of Integrated Management of Acute Malnutrition (IMAM) services: i: EPHS including IMAM rolled out in targeted regions Largely met 3.9: Number of communities declaring abandonment of FGM/C: i: 21 communities in NEZ declare abandonment of FGM/C Fully met and exceeded expectations Page 37
40 3.10: per cent of patients/ clients satisfied with the provision of services from the health facilities in the targeted regions: i: Baseline established in CSS (need to establish baseline in all Partially met zones).. (work in progress) 3.11: per cent of mothers and caregivers attending OTPs with good knowledge for household sanitation and hygiene: i: EPHS rolled-out in targeted regions. Largely met Recommendations: a. Due diligence and transparency in the EPHS roll-out process should be ensured for timely delivery of results, b. While ensuring Learning by doing development partners should also help Government in defining clear procurement rules and regulations, especially for procurement of services, c. Donors should scale up funding for the Somali health sector while ensuring predictability so as to ensure continuation of essential services, d. Cross-sectoral linkages between different ministries should be improved, e. Results of service delivery should be reviewed at zonal and regional level on a quarterly basis to monitor progress and to identify challenges in time. f. Health authorities to prioritize hospitals to be upgraded for round-the-clock comprehensive EmONC services and lessons should be learnt from scaling up services in different regions, g. Cost of medicines, supplies, vaccines and commodities should be included in the AWPs of HSSPs to have a comprehensive picture of needs versus resources available. Impact Weighting (per cent): 30 per cent Revised since last Annual Review: The output was updated, revised and approved by the SC in Risk: HIGH. Risk continues to be HIGH. Political and security risks are the major factors that affect service delivery. Health authorities are interested in scaling up service delivery but required resources are not available. Economic and fiduciary risks remain high and there is hardly enough fiscal space in the public sector to divert resources for service delivery in health. Services are largely dependent on out-of-pocket expenditure or donors financing. Overall donors support for the health sector appears to be declining especially on the humanitarian front thus putting more financial burden on recovery/development interventions. The situation in the north of the country is more stable but humanitarian risks continue in all areas. Availability and deployment of health workforce for service delivery continued to be a challenge but health authorities are making efforts to address the issue through strategy formulation and strengthening the leadership role of government. More commitment is required to focus on preventive and primary health care interventions compared to curative care. Page 38
41 Output 4: Health Financing Equitable and efficient health financing system in place 4.1: Robust health financing framework and harmonization of financial support Milestone: i: Pro-poor health financing study published, joint financing agreement for HSSPs, preliminary national health accounts discussions held, ii: Central South Somalia health financing option paper/draft health financing strategy produced by MoH, draft joint financing agreement, iii: NEZ: data for the preparation of national accounts, analysis performed on availability of information on social protection mechanism. Progress: In all three HSSPs, the Development of a Health Financing System that relies more on local financing and local resources, that aligns funding to the country s priorities and is based on sound financial management, that allocates budget to priorities, accounts for spending accurately and uses national and internationals funds more efficiently is articulated as one of the top priorities. Reliable data on the health-financing situation on which to base a health-financing strategy is not available. Crude analysis indicates that major expenditure in Somali health is out-of-pocket or dependent on donors support mainly for humanitarian intervention. Overall government revenue is very small with a notional share for the health sector. In 2013, the programme considered collecting basic information through household and income expenditure to understand the status of health financing in the country. However, as the initial cost for this survey was very high (approximately US$ 1 million), it was agreed to hold consultation of stakeholders to develop understanding on the subject and to agree on a roadmap. A joint workshop with the Somali authorities and supported by DFID, World Bank and WHO/JHNP was organized on November 2013 to engage in a high level discussion on Governance and Finance in Somali Health to harness greater buyin and collective support on the key issues, and to agree consensus on the next steps. The plenary recommended a gradual approach firstly focusing on obtaining a better understanding of the health financing situation and secondly formulating a national strategy for heath financing and finally to move towards Universal Health Coverage through implementation of the strategy. Under step 1, the following activities were agreed and work initiated: WHO to lead the work on the analysis of public health allocation and expenditure, UNICEF/JCU to work on the mapping of donors assistance as a part of fundraising strategy for JHNP and work on different financing scenarios, WHO to work on the proposal for the first round of National Health Account (NHA). Related parallel activities under different outputs will be building the capacity of health authorities on health financing as a part of Leadership and Management plan, review of public financial management system under a fiduciary risk assessment and development of fiduciary risk mitigation plan and aligning JHNP activities with the Public Financial Reforms under the Somali Compact. It is planned that under the activity of Joint Annual Review and Development of AWPs 2014, all Somali health development financing through multiple channels will be aligned behind HSSPs. Page 39
42 4.2: Proportion of national budget spent on health Milestone: i: NWZ: National health budget (with 4 per cent share of health) submitted by November 2013, ii: CSZ: 4 per cent of national budget allocated for health and annual health sector budget submitted on time, iii: NEZ: increase of 3 per cent shown in health accounts. Progress: In NWZ, the overall picture looks better with an increasing budgetary allocation for health. In 2009, the Government allocated 2.72 per cent (US$ 687,008) of its national budget to the health sector. In 2010, the allocation was slightly higher at 2.83 per cent (US$ 836,553) and even higher again in 2011 with an allocation of 3.08 per cent (US$ 1,556,647) of the total government budget. In the recently announced 2014 budget for NWZ, a total of 14.4 per cent has been allocated to the social sectors. Of this, the greatest share (81 per cent) has been earmarked for Education and Health, which represents 7.7 per cent and 4 per cent of the total budget respectively. Ministry of Finance submitted the budget for approval on time In CSZ, allocation had progressively increased from less than 1 per cent (0.99 per cent) in 2011 to 1.98 per cent in 2012 and to 2.2 per cent in The NEZ allocated 1.73 per cent (US$ 313,719) of the national budget to health in 2009 (excluding off-budgets). In 2010, the figure was lower at 1.45 per cent (US$ 361,520) of the overall national budget of US$ 25 million. It was again lower in 2011, with just 1.38 per cent (US$ 412,129) allocation, although, in normative terms, the national health budget has increased due to increased revenue collection but remains less than a mere 2 per cent of the overall national budget The programme initiated work through WHO to collect and analyse the information of public sector allocation and expenditure in the three zones to monitor the trend and to use the information for health financing strategy development. Progress against expected results: Overall, the programme has partially achieved milestones under output 4. The main constraint is shortage of funds in JHNP to collect basic information for the development of a health financing strategy. However, a roadmap was agreed to collect the information in a more cost effective way. NWZ has shown progress in allocating the desired budget for the health sector but the progress in CSZ and NEZ is very slow. Milestone End of 2013 status Performance Trajectory by end : Robust health financing framework and harmonization of financial support: i: Pro-poor health financing study published, joint financing agreement for HSSPs, preliminary national health accounts discussions held. Not met Milestone unrealistic Partially met Page 40
43 ii: CSZ: health financing option paper/ draft health financing strategy produced by MoH, draft joint financing agreement. iii: NEZ: data for the preparation of national accounts, analysis performed on availability of information on social protection mechanism. 4.2: Proportion of national budget spent on health: i: NWZ National health budget (with 4 per cent share of health) submitted by Nov ii: CSZ: 4 per cent of national budget allocated for health and annual health sector budget submitted on time. iii: NEZ: increase to 3 per cent shown in health accounts. Not met Milestone unrealistic Fully met in NWZ but not met in Central South Somalia and NEZ Recommendations: a. Need to move some of the recurrent health expenditures in the Government budget through new investment under the Somali Compact, b. Analytical work needs to be prioritised considering value-for-money and before initiating work on the health financing strategy development, c. Align JHNP reform initiatives with the expected Public Financial Management (PFM) reforms across the Government, d. Allocate more funds for this output or revise milestones. Impact Weighting (per cent): 10 per cent Revised since last Annual Review The output was updated, revised and approved by the SC in Risk: HIGH. Risk continues to be HIGH. Economic and fiduciary risks remain high and there is hardly enough fiscal space in the public sector to divert resources for health and the sector remained largely dependent on out-of-pocket expenditure and donors financing. Donors support is declining sharply especially on the humanitarian side and there are limited donors with interest on the development side. Political and security risks are major factors influencing economic situation. Page 41
44 Output 5: Medicines, Vaccines, RH and Nutrition Commodities and Technologies Improved availability and quality of essential medicines, vaccines, RH and nutrition commodities, medical equipment and physical structures 5.1: National drugs policy and quality control procedures in place and being implemented Milestone: i: NWZ: pharmaceutical registration and import control system functioning in two additional regions, ii: CSZ: updated essential drug list and treatment guidelines, medicines steering committee, basic quality control system introduced, development plan for drug regulatory facility, iii: NEZ: develop import regulations and inform wholesalers, submit regulations to Parliament for approval, licensing and registration of drug wholesalers and retailers. Progress: NWZ surrendered the activity (establish pharmaceutical inspectorate) considering the need for completion of assessment and development of legislative framework first. WHO completed assessments for the Public Health Law and on Right to Health which will set a roadmap to draft a series of legislation/laws required in the health sector including those related to the pharmaceutical sector Standard Treatment Guidelines and Essential Drugs List developed and under final review of Ministries of Health. Health Authorities also plan to train clinical providers on the rational use of drugs and use of Standard treatment guidelines Work on other regulatory issues is in progress through WHO support outside of JHNP. 5.2: Availability of medicines, vaccines, RH and nutrition commodities and supplies in EPHS health facilities in targeted regions: Milestone: i: Contribution for Pentavalent vaccine; ii: RH commodities supplied for service delivery; iii: Medicines and supplies procured and supplied for service delivery. Progress: As Government co-financing for the procurement of pentavalent vaccine, US$ 300,000 was released in 2013 from the JHNP. The GAVI Alliance has approved the Country s request for the supply of vaccines and related injection safety material with a programme budget of US$ 7,450,500 ( ). For 2013, the programme budget was US$ 2,891,500 for the purchase of 1,321,000 pentavalent doses, 1,296,400 auto-destructible syringes and 14,400 safety boxes. In accordance with the GAVI Co-financing Policy, the Country agreed to make the required contribution to co-financing vaccine doses in 2013 and the amount for 2013 was released through JHNP. This has ensured availability of the vaccine and other material in all parts of the country. The next instalment of Government co-financing is expected in the second quarter and the approved activity is part of the JHNP plan UNFPA procured RH commodities including contraceptives, essential medicines, equipment and supplies for obstetric care etc. worth US$ 611,975 and initial shipments supplied to all three zones for Page 42

45 onward distribution to regions and health facilities. While ensuring RH commodities, UNFPA is also implementing a training plan through a trickle down approach to ensure effective service delivery related to birth spacing, obstetric care and management of complicated cases of FGM/C. Considering the need for RH commodities in 2014, UNFPA placed further orders worth US$ 250,000 in December UNICEF procured medicines, supplies and nutrition commodities to ensure effective delivery of EPHS interventions in the targeted regions amounting to US$ 1.29 million for medicines and US$118,000 for nutrition commodities. New orders worth US$ 508,613 were placed against the planned allocation for procurement of medicines and supplies for the year Nonetheless, funding is not enough for EPHS medicines and supplies to be able to sustain services in JHNP regions. The issue is emerging as a result of declining investment on humanitarian interventions and inadequate funds are available for procurement of EPHS medicines, supplies and nutrition commodities Funds from JHNP contributed to the provision of therapeutic feeding supplies for 7,400 severely malnourished children under-5 through the procurement of 360 cartons of F-100 and 250 cartons of F-75. Standard protocols for the treatment of severe malnutrition consist of three phases: The Acute Phase, where the patient is treated with F-75; the Transition Phase, which includes treatment with F-100 or Ready-to-Use Foods (RUTF); and the Recovery Phase, which includes treatment with RUTF (in-patient and out-patient treatment) or F-100 (in-patient settings only). Some of the beneficiaries reflected above have also received F-75 or F-100, while some beneficiaries received both F-75 and F-100. JHNP support also contributed to the purchase of other essential supplies, including Mid-Upper Arm Circumference (MUAC) tapes and ID bracelets for the therapeutic feeding programme. 5.3: Proportion of health facilities meeting EPHS standards in having WASH facilities Milestone: i: NWZ: 10 per cent increase of facilities meeting standards, ii: CSZ: undertake infrastructure assessment for CSS and infrastructure development plan in place. Page 43
46 Progress: While rolling out of EPHS in Togdheer and Nugaal funds were approved for minor refurbishment of health facilities including WASH facilities. Status of WASH standards are reviewed on an annual basis during an annual health facility assessment exercise CSZ completed its internal assessment and development of infrastructure development plan. However, funding support to implement the plan is not available so far. 5.4: UNICEF completed the Cold Chain Facility in Garowe, NEZ, for which JHNP provided partial support. Support for revitalising and upgrading of Cold Chain Facility in CSZ is at planning stage and funds have been released for the activity. Progress against expected results: Overall, the programme has largely achieved milestones under output 5 and is showing a positive trajectory. The main constraint is shortage of funds in JHNP to procure essential medicines, vaccines, RH and nutrition commodities and supplies. There are needs for infrastructure development but funds are not available. Milestone End of 2013 Performance status Trajectory by end : National drugs policy and quality control procedures in place and being implemented: i: NW: pharmaceutical registration and import control system Fully met functioning in two additional regions. ii: CSZ: updated essential drug list and treatment guidelines, Largely met medicines steering committee, basic quality control system introduced, development plan for drug regulatory facility. iii: NEZ: develop import regulations and inform wholesalers, Not met submit regulations to Parliament for approval, licensing and registration of drug wholesalers and retailers. milestone unrealistic 5.2: Availability of medicines, vaccines, RH and nutrition commodities and supplies in EPHS health facilities in targeted regions: i: Contribution for Pentavalent vaccine, Fully met ii: RH commodities supplied for service delivery, Fully met iii: Medicines and supplies procured and supplied for service Fully met delivery. 5.3: Proportion of health facilities meeting EPHS standards in having WASH facilities: i: NWZ 10 per cent increase of facilities meeting standards, ii: CSS - undertake infrastructure assessment for CSS and infrastructure development plan in place. Not met Information not available Fully met Plan available but no funds Page 44
47 Recommendations: a. Comprehensive need assessment for medicines, vaccines, RH and nutrition commodities should be done (during Joint Annual Review exercise) along with identification of possible source of funding, b. Different programmatic interventions should work jointly to strengthen supply chain management system of the health ministries, c. Health authorities should lead the dialogue with donors to generate more funding support for the procurement of medicines, supplies and commodities, d. Donors need to be identified for health infrastructure development. Impact Weighting (per cent): 10 per cent Revised since last Annual Review? The output was updated, revised and approved by the SC in Risk: HIGH. Risk continues to be HIGH. Economic and fiduciary risks remain high and public sector funds are not available for procurement of medicines, vaccines, supplies and commodities. Availability of these essential items is completely dependent on donors and UN support. UN agencies are facing difficulties to ensure availability of medicines and supplies. Political, institutional and security risks are also affecting the situation negatively. Output 6: Health Information Improved availability, quality and use of health information that covers disease surveillance as well as management information system 6.1: Percentage of regions and health facilities submitting timely, complete and accurate reports to zonal health authorities Milestone: i: 30 per cent of EPHS facilities in targeted regions provide regular reports, ii: NWZ: improved data collection and management, HMIS expanded to primary health units in EPHS regions, HR workforce indicators staff needs integrated into HMIS and piloted, computerized system introduced at facility level. Progress: Overall, 70.1 per cent of the expected 2013 HMIS reports in NWZ were submitted by mid- February 2014; 73.7 per cent in NEZ and 15.1 per cent in CSZ. Both NWZ and NEZ have good reporting rate and CSZ has shown gradual but consistent improvement. Page 45



48 6.1.2 The HMIS reporting rate in JHNP regions is above 50 per cent in NWZ and NEZ. However, the reporting rate is much below the expectation in all three regions of CSZ. The overall trend was positive in 2013 and with the roll-out EPHS, the reporting rate is expected to improve. Page 46
49 6.1.3 HMIS information is still not generated from Primary Health Units (PHUs). Global Fund, which mainly provides support for the implementation of HMIS, is currently conducting the review of HMIS. The review will help in setting the future direction of HMIS including way forward for its expansion to cover other areas. 6.2: Health System Analysis Team (HSAT) fully functional, serving MOH and partners: Milestone: i: HSAT core staff recruited and performing core functions at MOH/Nairobi levels; prioritized and approved agenda of analysis in support of Health Authorities and JHNP. Progress: The HSAT unit was established in 2012 under a Memorandum of Understanding (MoU) between DFID and UNOPS. The support ended in The HSAT was revived with JHNP funding in A new HSAT team leader was selected and appointed in The work plan of HSAT was developed and shared with all stakeholders. Some of the research activities identified for 2013 and 2014 were included in the work plan of HSAT. To strengthen the zonal MoH capacity in health system analysis, the selection process of zonal HSAT technical officers started HSAT has been given a task to design and implement an Annual Health Facility Assessment and start the first round in Other research activities supported by JHNP are as follows: Maternal Mortality study in NWZ: Initial results expected in Q2, Baseline survey in Central South Somalia Initial results expected in Q2, EPI Review in NWZ and NEZ: study completed. 6.3: A functional Monitoring and Evaluation mechanism established: Milestone: i: First Joint Annual Review (JAR) conducted and finding shared with stakeholders. Progress: Somali Health Authorities and other stakeholders decided to conduct the first Joint Annual Review of the three HSSPs/AWPs 2013 with following three core objectives: i. To assess the progress of the three HSSPs/AWPs-2013 and the contribution of both public sector financing and the four key aligned programmes i.e. GFATM, GAVI-HSS, JHNP and HCS, against specific outcomes, outputs and activities, ii. To identify potential constraints to implementation of the HSSPs, iii. To support the Somali health authorities in developing AWPs for It was decided to identify a consultancy firm to conduct the review with support/supervision of a Task Force consisting of Health authorities, UN Agencies, Donors and the four Programmes. ToRs of the Task Force and the Technical Assistance were developed and agreed. WHO led the procurement process to identify a consultancy firm. The process was delayed as a suitable firm was not identified in the first round. Eventually the firm was selected and actual work is expected to start in the first quarter of Health authorities, with the support of WHO, initiated the work of developing a Somali Monitoring and Evaluation Framework with three Zonal M&E plans. ToRs were developed, agreed and a consultant identified for the work. Page 47
50 6.3.3 The JCU drafted the Standard Operating Procedure (SOP004) - Monitoring and Review of Joint Health and Nutrition Programme. It sets out processes which use the existing HMIS mechanism and not replace, duplicate, or change the terms of reference of HMIS officers within the MoH/ UN agencies. The SOP empowers the existing zonal MoHs bureaucracy, including the regional and district health offices. It also seeks to decentralize programme monitoring and oversight to the JHNP s ZWGs. Progress against expected results: Overall, the programme has largely achieved milestones under output 6, with a positive trajectory. The main constraint is availability of health information from CSZ. However, the situation is gradually improving and the baseline survey is likely to generate critical information for the design and implementation of the project activities. HSAT is fully operational at Nairobi level and HSAT technical officers at zonal level were on board in March There are delays in organising the first JAR but started in Q1, Milestone End of 2013 status Performance Trajectory by end : Percentage of regions and health facilities submitting timely, complete and accurate reports to zonal health authorities: i: 30 per cent of EPHS facilities in targeted regions provide regular reports, ii: NWZ: improved data collection and management, HMIS expanded to primary health units in EPHS regions, HR workforce indicators staff needs integrated into HMIS and piloted, computerized system introduced at facility level. Fully met Not met Activity led by GFATM 6.2: Health System Analysis Team (HSAT) fully functional, serving MOH and partners: i: HSAT core staff recruited and performing core functions Largely met at MOH/Nairobi levels, prioritized and approved agenda of analysis in support of Health Authorities and JHNP. 6.3: A functional Monitoring and Evaluation mechanism established: i: First Joint Annual Review (JAR) conducted and finding shared with stakeholders. Partially met process started Recommendations: a. All monitoring and evaluation activities in the health sector should be aligned with the Somali M&E plan, once developed and agreed by all stakeholders, b. Considering more clarity in strategic priorities and better access to information, the JHNP Log Frame should be revised and be made more realistic with regards to stakeholder consultation, c. Zonal monitoring team consisting of Zonal HMIS officer, M&E advisor and HSAT technical officer should be responsible to regularly collect, review, verify, present, share and ensure use HMIS data, d. Conduct JAR on annual basis and use findings of the review for the development of joint and consolidated AWPs under the HSSP with inputs from all programmatic interventions, e. Implementing partners should proactively share information with the zonal health authorities on a regular and timely basis. Page 48

51 Impact Weighting (per cent): 10 per cent Revised since last Annual Review: The output was updated, revised and approved by the SC in Risk: HIGH. Risk continues to be HIGH. The culture of evidence based decision-making will take time in the Somali context. There is a positive trend in availability of information but most of the time basic information is not available on time nor regularly. The security situation, especially CSZ, poses a high risk to a functioning M&E system, although communication technology is available in all areas. The political-economic situation of the country and availability of resources for the sector are critical risks. Page 49
52 3. Overall Performance and Value for Money The JHNP Programme is on-track, as is evident from the progress made to deliver its outputs, which are expected to contribute to the outcome of the programme. A summary of progress on the six outputs is as following: Outputs Output 1: Improved governance and leadership at all levels of the health sector. Output 2: Skilled and trained public health workforce produced and distributed equitably to deliver RMNCH and nutrition services. Output 3: RMNCH and nutrition services available and utilized. Output 4: Equitable and efficient health financing system in place. Output 5: Improved availability and quality of essential medicines, vaccines, RH and nutrition commodities, medical equipment and physical structures. Output 6: Improved availability, quality and use of health information that covers disease surveillance as well as management information system. End of 2013 status of Milestones Fully met - 2 Largely met - 3 Partially met - 1 Not met - 0 Fully met - 7 Largely met - 0 Partially met - 0 Not met - 0 Fully met - 5 Largely met - 6 Partially met - 1 Not met - 1 Fully met - 1 Largely met - 0 Partially met - 1 Not met - 4 Fully met - 5 Largely met - 1 Partially met - 0 Not met - 2 Fully met - 1 Largely met - 2 Partially met - 1 Not met - 0 Performance Trajectory by end 2013 Significant progress has been made during the last year. Nonetheless, there is still a need to focus on complete roll-out of EPHS and effective delivery services both at health facility and community level. Health authorities and UN agencies were able to resolve many operational issues which emerged as a result of devolution of powers to the JHNP s ZWGs under the leadership of health authorities. New evidence is being generated and partners are currently considering this to make adjustments in policy and programmatic choices. The Joint Annual Review is expected to present a more cohesive picture of the health sector and alignment of different programmatic interventions behind HSSPs. Zonal health authorities are in a process of restructuring, enabling them to meet new challenges and to ensure strengthening of all six system blocks of the health system. While prioritizing the provision of health services, the programme also plans to focus on the demand-side interventions in coming years. Page 50
53 Funds transfer and utilization has improved significantly. However, there are expected funding gaps in the programme in coming years especially with the roll-out EPHS. Predictability and availability of required funds are be a major challenge for full implementation of the programme. The programme has taken on a consultant to develop a fundraising strategy to map out donor assistance and to explore partnership opportunities with new development partners to fill the funding gap. All three UN partners are working coherently and involve each other in activities and decision-making process. Health authorities are increasingly involved and contributing significantly to leading the programme. In terms of division of labour, UNICEF s focus is on ensuring the provision of services under the framework of EPHS while at the same time giving due attention to nutritional and social protection issues. UNFPA focuses on provision of reproductive and comprehensive EmONC services while ensuring availability of midwives in the health system. WHO s focus is on evidence based policy, strategic, legislative, governance, system and capacity-building aspects of the programme including training and deployment of community based female health workers. Areas where further focus is required: 1. Development, approval and implementation of policies, strategies and plans which should guide reforms focusing on a) quality, b) integrated approach, c) behaviour change communication, d) ignored service delivery areas e.g. birth spacing and FGM/C and d) nutritional crises, 2. Development of future plans which are based on the needs of beneficiaries and encourage partnerships between the public and private sector for delivery of cost effective interventions, 3. Coherence and integration of the different interventions supported by different programmes/ investments; and make strategic decisions to achieve international coverage indicators, 4. Further prioritisation around cost-effective activities with a strong focus on decentralization and delivery of results, 5. Strengthening linkages between a) zonal MoHs and other social sector ministries, b) the community based and facility based EPHS and c) among the community level workers i.e. FHWs, CMW, vaccinators and others, 6. Implementation of a comprehensive training plan of action to further improve skills of health providers in a systematic way to ensure provision of quality care; zonal authorities to develop basic training and continued support packages for regional, district and facility based staff, 7. Introduction of reforms in the training and examination system of midwives to ensure competency, clinical and service standards in place and are implemented and monitored, 8. Enhancing donor support and release of committed funds on time to ensure predictability and smooth implementation of programme, 9. Mitigate fiduciary risks and ensure transparent and equitable use of resources in the sector, 10. The Government to proactively harmonise donor activities and harness incoming finances by developing clear guidelines, whereby donors support is governed by a common agenda and must not be used to replace public financing; Government to bear the recurrent cost in the sector up to a maximum possible extent. Annual Outcome Assessment The programme has four outcome level indicators: 1. Proportion of institutional deliveries attended by skilled birth attendants - disaggregated by location. Proxy indicator: Annual number of deliveries in MCH/HC and hospitals. 2. Contraceptive prevalence rate - disaggregated by location. Proxy indicator: Annual number of birth spacing clients in MCH/HC. Page 51
54 3. Proportion of (12-23 months) children having received DPT/ Pentavalent III - disaggregated by location. Proxy indicator: Annual number of children immunized for DPT/Pentavalent III in MCH/HC 4. Proportion of acutely malnourished children (<5yr) who were treated through routine services. Proxy indicators: Annual number of moderately and severely malnourished children attended in MCH/HC. Since the last Multiple Indicator Cluster Surveys (MICS 2011) for NWZ and NEZ, no information is available at the national level. However, in the area of nutrition, information is available through FSNAU results published in It is currently not possible to comment on overall progress against outcomes, but the results of 2013 s HMIS data (received in mid-february 2014) on the proxy indicators indicate some improvement in the outcome level indicators. It is important to understand limitations and assumptions in the data collection and analysis before reaching any conclusion. HMIS data needs validation/ verification through a regular process at the zonal and regional level. Outcome results for 2013 are as follows: Page 52

55 Page 53

56 Page 54
57 The table below shows a summary of proxy indicators from HMIS of the three zones in the year 2013: Table: Summary of Proxy Outcome Indicators Proxy Outcome Indicators Central South Puntland Somaliland Total JHNP No. of Deliveries in MCH/HC 6,467 34,788 42,528 83,783 13,405 Antenal Care visits in MCH/HC 112, , , ,928 70,868 TT 1 immunization to women in MCH/HC 19,293 15,965 71, ,263 17,002 No. of Birth spacing clients in MCH/HC 1,030 3,053 8,666 12,749 2,040 No. of Children immunized for DPT/Penta III in MCH 29,687 20,088 85, ,812 21,570 Children immunized for Measles in MCH/HC 25,803 30,903 48, ,583 16,893 No. of Moderately and Severely under-noursihed children provided care in MCH/HC 52,479 NA 9,768 62,247 9,960 Women provided with Multi-micro nutrients 32,259 40, , ,690 40,430 % of HMIS reports submitted of expected reports 15.10% 73.70% 70.10% 40.56% In spite of financial constraints and high economic, political, institutional, social and fiduciary risks, there appears to be some progress on the outcomes. It is estimated that the share of JHNP out of total health expenditure (and therefore JHNP s contribution to results) during 2013 is roughly 16 per cent and is expected to rise to above 30 per cent in The Programme intends to collect detailed information of budget allocation and expenditure in 2014 which will help to estimate JHNP attribution to outcome results more accurately. As the programme is focusing on long-term reforms and is expected to further contribute to enhanced health outcomes in 2014, especially with the complete roll-out of EPHS. At that stage, the 2013 s HMIS data will work as a baseline to monitor trend. The programme is still not well placed to focus on some inter-related aspects e.g. birth spacing, behaviour change communication, community based interventions and cross-sectoral interventions focusing especially on WASH and FGM/C. Financial Outcome Assessment The programme is off-track against the financial forecasts because of the amount of donor funding available; less availability of public funds for the health sector; decline in humanitarian funding leading to pressure on the programme to fill the gaps; delayed start and delayed completion of the inception phase resulting in delayed start of the continuation phase. However, the programme has with the resources available - picked up the pace and has resolved many governance and financial management issues. In spite of a complex governance structure, the Steering Committee was able to make strategic decisions which contributed to better implementation of the programme. The programme was able to place satisfactory safeguards on fiduciary risks by using the financial management system of the three UN agencies, which have effective mechanism for checks and balances (both internal and external) and ensure value for money (VfM). For some minor activities, funds were transferred by the UN agencies to health authorities in limited tranches. In order to safeguard against Page 55
58 misuse of these funds, liquidation of the funds released (with proof of transactions) was required by the UN agencies before transferring additional tranches, as per fiduciary risk mitigation measures of the UN agencies. In some instances, delay in liquidation by the health authorities resulted in the delay of some activities. The programme has planned a fiduciary risk assessment in the health sector in collaboration with DFID along with the development of a fiduciary risk mitigation plan. This will help not only building the capacity of the public sector to manage funds properly but will be another step towards a government led programme implementation. Key cost drivers of the programme are as per the six building blocks of the health system. The programme is monitoring cost drivers by sub-outputs and activities on a quarterly basis. The information is shared with stakeholders on a quarterly basis during review meetings. There is over-expenditure for some of the sub-outputs which is due to the consideration of approved plan for 2014 and availability of DFID tranche in November 2013 for 2014 activities. Considering needs, implementation of the 2014 activities were therefore started already in December 2013, especially CHDs and procurement of medicines and supplies. The cost drivers, allocations and expenditures by the end of December 2013 are as follows: Page 56
59 S. No. Output and Sub-output wise Allocations, Releases, Estimated Expenditure/ Commitment by end December 2013 Sub-outputs TOTAL FUNDS REQUIRED AS PER ROLLING PLAN Output 1: Improved governance and leadership at all levels of the health sector ** FUNDS RELEASED EXPENDITURE/ COMMITMENT BY END DEC 2013 BALANCE / FUNDS AVAILABLE % EXPENDITURE OF RELEASED Amount in US$ FORECAST FOR 2014 AS PER ROLLING PLAN 1 Support to Policy, Strategies and Legal Frameworks 5,138,314 2,492,850 1,883, , % 2,493,947 2 Improved Management and Institutional Capacities 4,634, , , , % 1,908,000 3 Effective Partnership and Coordination 5,070,324 1,220, , , % 1,678,124 4 Better Citizens engagement/ involvement in Health System (Voice & Accountability) 950, ,000 OUTPUT 1 15,793,138 4,674,074 2,858,971 1,815, % 6,580,071 Output 2: Skilled and motivated health workforce distributed equally and equipped to deliver quality RMNCH & nutrition services through a Continuum of Care 1 Improved Human Resource Planning and Management 3,520, , , , % 1,420,000 2 Health Professionals registered, licensed and accredited 848,200 48, , ,200 3 Harmonize incentives and allowances 3,132,546 1,082, , , % 1,172,000 4 Availability of training guidelines, material and protocols 5 Sufficient skilled health professionals and workers to implement EPHS/RMNCH services 639, , , , % 350,496 17,400,392 3,943,518 1,226,450 2,717, % 5,774,782 OUTPUT 2 25,540,493 5,962,577 2,022,455 3,940, % 9,175,478 Output 3: EPHS/ RMNCH and Nutrition Services available, accessible, affordable, of acceptable quality and adaptable services, within the EPHS framework 1 EPHS Assessment and Micro planning 360, , ,594-21, % 360,000 2 Roll out of EPHS Core Programmes in Target Regions 72,940,756 9,760,756 3,471,320 6,289, % 17,540,756 3 Basic health services maintained in regions 2,164,867 1,770,000 2,164, , % 500,000 4 Improved Healthy Behaviours and Practices of the communities 5 Improved Health & Nutrition for women, children & adolescents 1,750, ,000 97,265 2, % 452,735 7,280, , , , % 2,080,000 Page 57
60 S. No. Sub-outputs 6 Health Emergency Preparedness Plan and System in place + Partnership with Private sector TOTAL FUNDS REQUIRED AS PER ROLLING PLAN ** FUNDS RELEASED EXPENDITURE/ COMMITMENT BY END DEC 2013 BALANCE / FUNDS AVAILABLE % EXPENDITURE OF RELEASED FORECAST FOR 2014 AS PER ROLLING PLAN 2,460, ,500,000 OUTPUT 3 86,955,623 12,590,756 6,567,914 6,022, % 22,133,491 Output 4: Steady progress made to an equitable and efficient health financing system 1 Robust Health Financing Framework and Harmonization 1,840, ,000 50, , % 1,240,000 2 Sound Financial Management and Accounting system 1,050, ,000 OUTPUT 4 2,890, ,000 50, , % 1,890,000 Output 5: Improved access, availability, quality and rational use of essential medicines, vaccines, commodities, medical equipment and physical structures 1 Ensure EPHS, Reproductive Health and Nutrition Supplies 2 Effective Procurement, Logistics and Supply chain system/ Physical structures 8,127,757 1,937,757 3,076,318-1,138, % 2,150, , ,000 84,001 75, % 400,000 3 Improved / Rational Use of Drugs 1,272,000 36, , ,000 OUTPUT 5 9,899,757 2,133,757 3,160,319-1,026, % 3,536,000 Output 6: Improved access, availability, acceptability, quality and use of health information that covers disease surveillance, policy research as well as HMIS 1 Effective M&E system to track Health System Performance 2 Improved Research capacity and priority review, research & survey plan 2,965, ,000 35, , % 1,295,000 4,432,396 1,239,965 1,138, , % 779,965 3 Timely, complete and accurate HMIS at all levels 640,000 60, , ,000 4 Effective Disease Early Warning and Surveillance System 600, ,000 OUTPUT 6 8,637,396 2,084,965 1,174, , % 2,764,965 TOTAL OF COST FOR ACTIVITIES UNDER OUTPUT 1-6 (excluding UN cost) 149,716,407 27,596,129 15,834,066 11,762, % 46,080,005 GRAND TOTAL OF COST (including UN Cost) 182,206,675 35,611,034 23,517,706 12,093, % 57,044,727 **: Note: The Funds Released does not include DFID Last Tranche released in Nov 2013 as the same is part of 2014 Plan Page 58

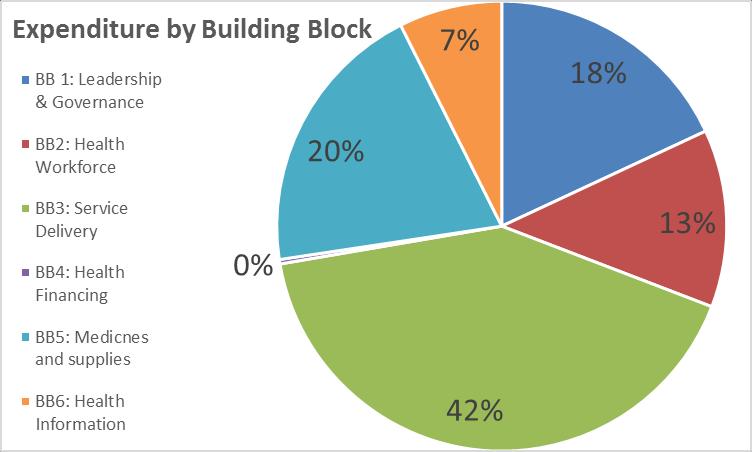

61 Page 59
62 Evidence and Evaluation The programme is using multiple tools to generate evidence about progress. These include: National Surveys (MICS, FSNAU reports), Health Management Information System, Quarterly monitoring system of the Programme - information shared by the three UN agencies, Documents and deliverables of the JHNP activities (please refer to Appendix A), Analytical and research work carried out by JHNP and other programmes and organizations, Third party assessment reports, Financial monitoring data including quarterly expenditure updates, Joint supervision visits and reviews, Programme documents, SOPs and guidelines. Joint Annual Review of the HSSPs/AWPs is likely to generate information about the progress and challenges faced by the health sector including JHNP. The programme is also planning to conduct the first round of Health Facility Assessment in 2014 through HSAT to observe and monitor changes at service delivery level. The programme will rely upon the next round of MICS to observe changes in the impact and outcome level indicators. A Maternal Mortality study will provide information related to maternal mortality ratio (MMR) in Global Inter-agency estimates are also used to monitor impact level indicators. The programme has a plan to conduct a mid-term evaluation in 2015, which may help to estimate the impact of JHNP at the outcome level. Evidence generated will be used to develop successor programmes along with associated reforms in the health sector. Risks Overall output level risk rating is HIGH as mentioned against each output. In addition to risk assessments carried out by the UN agencies, the programme is monitoring the following risks (impact and probability) on a six-monthly basis: Political, Conflict, Economic, Fiduciary, Corruption, Institutional, Partnership, Behavioural and Disasters. The health authorities have planned the first fiduciary risk assessment in the health sector for 2014 along with development of fiduciary risk mitigation plans. The programme needs to mitigate Climate and Environment Risks for which a detailed assessment of the infection control measures will be required. This activity will be planned soon after completion of EPHS rollout in targeted regions. The development of Infection Control protocols for different levels (hospitals to community) of service delivery will be required along with guidelines to implement these protocols. Performance on VfM measures A VfM analysis as a part of the Joint Annual Review is planned for An initial VfM assessment of the programme found that: Budget allocations were less than envisaged in the programme document. The programme only received US$ 35.6 million during 2012 and 2013 and expects to receive another US$ 40 million for 2014 against the total requirement of US$ 236 million ( ). Nonetheless, the programme is on track to achieve the target of midwifery training, EPHS roll-out and the provision of EmONC and RH services along with Page 60
63 policy and strategic work. The programme is likely to ensure good VfM, provided required resources are available on time and service provision as per standards is not interrupted. Allocation of funds to essential services in all three zones is likely to contribute to an equalizing effect, improving the equity of the system. Investment on Leadership and Governance, Health Workforce and Health Information is likely to improve the equity and parts of the three zones will benefit from it. For service delivery, the programme is prioritising investment in CSZ which is another way of improving equity. For service delivery, 43 per cent of the resources have been allocated to CSZ compared to 28 per cent for NEZ and 29 per cent for NWZ. However, there is a need to invest more in CSZ as this will help in state-building and peace-building efforts. The analysis for the EPHS roll-out in 2013 indicates that the unit cost per beneficiary ranges from US$ 12 to US$ 17 per person per year - this includes contributions from the implementing partners which varies from 4.4 per cent to 34 per cent of the cash component. The unit cost to the programme is US$ 8 to US$ 11 for the cash component and US$ to US$ 6 for the supply component. Variation in the unit cost depends upon the number and type of facilities covered under the PCA. These are just an initial estimate and a more concrete unit cost will be shared after the roll-out of EPHS in other regions. PCAs are finalised as per standard global guidelines of UNICEF, which are implemented through a comprehensive process and mechanism of scrutiny. The cost of comprehensive EmONC services is not included as an activity within EPHS unit costs and is managed separately by UNFPA. Even then, unit costs are much below US$ 40 per person per year for the provision of essential health services as recommended by the Commission on Macroeconomics and Health. Other gaps in provision of essential services are likely to be in the community based interventions and behaviour change communication. To ensure VfM and efficiency in the procurement of medicines and supplies, UNICEF furthermore uses its own data for procurement, considering past trends. The unit costs for medicines and supply kits are at different levels for the year Table: UNICEF Cost US$ of Kits per facility per year in 2013 Type Primary Health Unit / Health post unicef material UNICEF Revised pre-packed kits unit cost Offshore Inland freight / warehousing clearance / logistic 15% 25% Total kit cost per facility per year (if quarterly distribution) S Somalia, PHU kit medicines 1, , , S Somalia, PHU kit renewable S Somalia, PHU kit equipment cost per facility per year US$ 8,455 S Somalia, HC kit medicines 2, , , Health Center / MCH S Somalia, HC kit renewable , ,871 S Somalia, HC kit equipment Additional supplies - Only for facilities conducting institutional deliveries S Midwifery kit, 1 - drugs: , S Midwifery kit, Supplementary 1a - drugs: S Midwifery kit, 2 - equipment: S Midwifery kit, 3 - renewable: , ,152 iccm Kit - equipment iccm 1,103 iccm Kit - Renewable Pinted material (HMIS registers, vaccination cards, ANC cards, EPI cards, IEC material, etc) 500 This does not include equipment like hospital beds, delivery tables, etc., which are one time supplies for health facilities. Page 61
64 Another key intervention in the programme is training 480 midwives by the end of Two types of midwifery trainings are supported by UNFPA/JHNP: Basic (24 month duration) and Post-Basic (18 month duration) midwifery training. The programme is currently supporting nine midwifery schools and the support is both to strengthen (upgrade training centre, provide equipment, teaching aid and the running cost) midwifery schools as well as to provide scholarships for students. It is estimated that the unit cost per midwife student varies from US$ 2,626 to US$ 4,349 per year depending on whether it is a running institute or a newly established school which needs more support for running costs. The cost per midwife student includes the cost of stipends which is US$ 1,200 per year (US$ 100 per month). Value for Money considerations of consultancy services - procurement through UN agencies: For contractual and consultancy services, the HR Manual on Remuneration and payment of fees to international consultants and individual contractors is applied which is revised on a regular basis considering market rates, Corporate sections or regional offices ensure quality checks (independent of country technical team) before award of any contract for consultancy services, Procurement of consultancy services is mostly through open tendering offering, When setting the consultant's or individual contractor s rate of pay, the following factors are considered: (i) level of work in terms of responsibilities and complexity of the assignment, (ii) degree of specialization required by the assignment, (iii) knowledge, qualifications, experience and skills required, (iv) Fees paid to the consultant for previous assignments with UN agency. Once the equivalent level of the assignment has been estimated, a Fee Range - for the purpose of negotiating the contract with the consultant or individual contractor is determined within the minimum and maximum of the range based on the complexity of the assignment, the degree of specialization, knowledge, qualifications, experience and skills required. International Consultants and Individual Contractor Fee Ranges: Levels Fee Range Daily Rate Monthly Rate A Junior (P1/P2) Minimum Maximum $ $ $3, $6, B Middle (P3/P4/P5) Minimum Maximum $ $ $5, $11, C Senior (D1/D2) Minimum Maximum $ $ $10, $13, Market Rates Fee is determined based on local market conditions The daily and monthly rates are updated whenever there is a revision to the gross annual salary rates for professional and higher grades. On Economy: Cost of consultancy is judged as acceptable as UN rules/ guidance are followed. On Efficiency: UN agencies are globally judged to be operating at a satisfactory level. On Effectiveness: Client feedback is invited to assess satisfaction and areas need to be addressed to increase effectiveness. There is scope for increasing VfM by clarification of ToRs in the new devolved environment where health authorities/ ZWGs are empowered, more focus on ZWG s decision makers, greater attention to capacity building and developing government s ownership. Page 62
65 Commercial activity and Value for Money: The bulk of procurement (medicines, vaccines, supplies, RH and nutrition commodities) for the programme activities is done by the UN agencies, utilizing their standard mechanisms and procedures. Items are procured through international competitive process and in bulk quantities for different countries. Rates are always competitive and ensuring quality standards is an added value. This may not be immediately possible through the Government mechanism (or even NGOs) considering capacity constraints. The Government needs assistance from development partners in making improvement in their procurement, logistics and supply chain management. Role of JHNP partners: The implementing UN agencies are responsible (under an MoU with the AA) for effectively and efficiently using funding as per the MoU signed between the AA (UNICEF) and donors. Activities are identified by the JHNP s ZWGs under the leadership of the health authorities and finalized in the Technical Coordination Group (TCG) - with equal representation of health authorities and UN agencies with donors attending the meeting as observers. Strategic decisions and approval of the plan is the responsibility of the SC, chaired by UN Resident Coordinator (UNRC) and consisting of three MoHs, representatives of the three UN organizations and JHNP donors. The JCU facilitates the development of SOPs which are agreed at all levels and signed between health authorities and the UN agencies. The implementing UN agencies are responsible and accountable to carry out activities in close collaboration with health authorities and partner UN agencies, according to their own rules and procedures. UN agencies are responsible for the final contractual agreements with the implementing partners and have a joint responsibility with the health authorities to monitor their performance. In Summary, the programme offers good VfM especially in the Somali context. It is too early to comment on impact as evidence is not available/conclusive and the programme needs time to mature enough. However, the programme is showing a positive trajectory on outputs and VfM considering the challenges the Somali context inhibit and the programme has faced. The programme s technical support is utilised by the three Governments in driving policy changes. Page 63

66 Page 64
67 4. Programme Management A three-tier governance structure executes the programme with strategic decentralization of decision making to the zones. The three ZWGs, as the first tier, have taken a more structured and formalized role by prioritizing activities for inclusion in the joint annual plan. ZWGs also facilitate implementation of the planned activities through a joint consultative and decision-making process. The second tier is the Technical Coordination Group contributing to most policy recommendations, technical and financial decision-making. The third-tier is the SC of the programme, making all policy and strategic decisions and final approval of plans. UNICEF is the Administrative Agent of the JHNP, and the programme is implemented through a joint UN mechanism comprising of UNICEF, UNFPA and WHO. The JCU ensures the technical oversight of programme implementation and serves as a coordinating mechanism between health authorities, UN agencies, donors and NGOs. Endorsement of the 2012 Inception Phase Report in September 2012, and the subsequent initiation of the continuation phase by the JHNP donors, allowed UNICEF to recruit fixed term positions for the roles of Senior Programme Manager and Programme & Planning Specialist to take over from the temporary management arrangement. The Senior Programme Manager joined the programme in June 2013 whereas the Programme & Planning Specialist commenced in September 2013, thus making the unit fully functional. In April 2013, DFID supported an independent external review of the JHNP. The review strongly recommended defining key functions, roles and responsibilities of the JCU. Following detailed consultations, key functions, roles and responsibilities of the JCU were agreed and included in the Programme document and approved by the Steering Committee on 4 October Key Functions of the JCU and Progress made during 2013: 1: General Coordination: JCU regularly coordinated with external partners. Key forums were the Health Sector Coordination meetings, quarterly meetings of the HCS, the HR working group, the RH working group and HMIS working group. Ad-hoc meetings with NGOs (especially in the context of SOP002 development) and implementing partners were attended as and when required. On the decision of the SC in August 2012 to focus the Steering Committee agenda on strategic and political issues, quarterly donor briefings were instigated in November 2012, as an important addition to the programme structure. The aim of the quarterly donor briefings is for the JCU, along with the UN agencies, to update JHNP donors on programme achievements per quarter, and discuss matters of strategic and technical nature. These meetings were regularly convened during 2013 (a week prior to SC meetings), in addition to ad-hoc meetings on a needs basis. The SC has now decided to only meet twice a year. The JCU nevertheless intends to continue formal donor briefings on a quarterly basis. As planned, JCU organized four meetings (18 February, 1 July, 6 September and 28 October 2013) of the TCG in 2013, in addition to e-polls to make decisions on urgent issues. Efforts were made to organize these meetings within Somalia and the July 2014 meeting was hosted by the MoH NEZ. Four SC meetings Page 65

 and learn lessons from each other.")
68 (20 March, 30 August, 4 October and 1 November 2013) were organized. Key strategic and financial allocation decisions were made in these meetings. Minutes of all meetings were prepared and shared with all stakeholders. In addition, a number of meetings of the UN agencies were organized to develop consensus on technical and implementation issues. The programme ensured that all three UN agencies were available to take joint decisions related to agreements on ToRs, bid evaluation, selection of firms/consultants, developing guidelines, protocols, standards, etc. JCU also made efforts to organize a joint mission of UN agencies to review progress on ground (in NWZ) and learn lessons from each other. JCU ensured regular communication with the Somali health authorities through briefings, facilitating preformal and formal meetings to develop consensus in addition to disseminating documents, minutes, and information. All TCG and SC meetings were held with representation of all three health authorities. JCU adopted the approach of Roadmap actions to regularly present progress on these and ensuring that actions are closed. Minutes were regularly reviewed in the following meeting to provide an update on actions taken. Constrained activities were identified and highlighted in the meetings for discussion and decision-making. 2: Planning, Programming and Budgeting: JCU facilitated priority setting through the development and finalization of the JHNP Compact, Programme document and revised Log Frame in consultation with stakeholders. The annual review 2013 recommended moving from tranche-based planning to annual planning. Accordingly, guidelines for the development of a Joint Rolling Plan was developed in consultation with stakeholders. Based on these guidelines, ZWGs started planning processes by identifying activities aligned to their respective HSSP. JCU facilitated further discussions of the ZWGs in a workshop in Nairobfollowed Page 66
69 by a special meeting of TCG to prioritise activities along with budget allocations. Through a consultative process, the Joint Rolling Plan ( ) was finalized and approved by the SC on 1 November A mechanism of re-appropriation/surrender of funds was defined to ensure effective use of available resources. Programme implementation was monitored on a regular basis through quarterly review of activities and funds utilization. Constrained activities were identified and progress presented in the TCG and donor briefings. Deviations from the SOPs and protocols were raised in the TCG meetings and corrective measures were proposed accordingly. Issues and constraints were documented in minutes and followed up upon. 3: Fund Management: The new planning process introduced in 2013, facilitated better information of funds requirement but also linked activities with the donors disbursement plan. Accordingly activities were prioritized and implemented in a phased manner. Allocations and expenditures of all activities approved by the SC were monitored on a quarterly basis and updates were shared in the TCG and donor briefing meetings. This task was complex given different financial management systems of partners but with the support of the UN agencies, a fund-tracking mechanism was agreed and implemented giving a fair reflection of expenditure. ToRs for a fundraising strategy were developed and approved by the SC. Funds for this were identified and the selection process to identify a suitable consultant/firm was initiated. In the first round, a suitable firm/consultant was not identified and the process needed to be repeated which resulted in a delay of the activity. A consultant was identified in the second round. Current donors are committed to continuing support to the programme. Dialogue was initiated with the Government of Sweden to scale-up their financing as all committed funds were released by mid The Government of Sweden announced more support in the SC meeting in November It is expected that Sweden will release US$ 11 million in July USAID committed more funds towards the end of The Swiss Agency for Development and Cooperation (SDC) and the Government of Finland has expressed interest to engage. 4: Financial Management: JCU facilitated a standard financial reporting format in consultation with partners and has started reporting against this in quarterly donor briefings. Financial outcomes are also included in this report. However, the official expenditure report is shared by UNICEF Headquarters, based on the UNICEF Financial Information System. All the three agencies ensure fiduciary safeguards as per their agency rules and procedures. This is facilitated by the development of SOPs which further ensure safeguards. A new activity of conducting a fiduciary risk assessment in the public health sector along with development of fiduciary risk mitigation plan was agreed and likely to be completed in : Monitoring of SOPs: The SOP002 on Implementing Partner Selection within the JHNP and the SOP003 on Recruitment, Remuneration and Performance Management of long-term (six months or more) Technical Assistance for Page 67
70 Health Authorities within the JHNP were developed, approved and implementation has started. The SOP004 Monitoring and Review for the JHNP was developed and shared with stakeholders for comments before approval. JCU through TCG ensured implementation of these SOPs by highlighting irregularities where necessary with suggestions for corrective measures. 6: Risk Management: Risks were identified along with mitigation measures during the programme document development. A Risk Register is maintained and reviewed on a six-monthly basis in consultation with UN agencies. Risks are also reviewed during work on the Annual Progress Report. After the annual review in 2013, the programme agreed on a performance improvement plan with donors with an objective to show commitment and to make positive progress on the successful implementation of the Programme. Actions were followed up upon and targets were achieved on time. 7: Value for Money: JCU is working with the three UN agencies to develop a quarterly monitoring mechanism as proposed in the draft SOP004. Furthermore, the HMIS results for 2013 were reviewed in detailed and findings were shared with partners. VfM analysis, based on the information available for 2013, was conducted and included in this report. 8: Monitoring and Evaluation: JCU is working with partners for the development of an M&E framework for HSSPs, proposing a monitoring and review mechanism under SOP004, revision of the Log Frame and inclusion of the review of HMIS work led by GFATM. Information has been generated through the review of HMIS data which will be used to monitor trends in health outputs in the coming years (both in JHNP and non-jhnp regions). JCU worked with the UN agencies to draft initial ToRs of the JAR and the Task Force. JCU plans to start work on the mid-term assessment of the Programme by the end of Links to Other Programmes Careful consideration is taken to ensure there is no unnecessary duplication of services and that the JHNP supported facilities and activities complement other initiatives. Linkages within the JHNP work plan to other UN run initiatives in health are documented in regular JHNP planning and reporting events: The EPHS has been identified as a flagship programme in the health sector under PSG-5 of the Somali Compact and JHNP is the key delivery mechanism for this, The DFID supported HCS programme is a development initiative and works through a NGOs consortium. The JHNP has coordinated with the HCS and participated in its quarterly briefings and an annual best practice sharing forum so as to be able to accommodate the lessons learned from the HCS programme. The JHNP will work closely with the programme to ensure that there is no risk of duplication of effort and resources and that the two programmes complement each other, UNICEF is implementing the EC Supported Continuum of Care Programme for Reproductive and Sexual Health (SRH) and the two programmes are complementing each other in the regions of Nugaal (NEZ) and Awdal (NWZ). The same implementing partners were engaged for EPHS services, Page 68
71 Focus of GFATM is mainly disease (TB, Malaria and HIV) specific programmatic interventions whereas JHNP focuses on (RMNCH and nutrition) interventions. The two programmes complement each other to ensure delivery of comprehensive and essential service delivery package. The Health System strengthening (HSS) component of the GFATM overlaps with the JHNP programmatic areas of health system. However, the two programme coordinate with each other to avoid any duplication of activities and complement each other, The WHO/UNICEF GAVI HSS was launched in 2012 and interventions take place in Nugaal and Galgadud regions. The two programme work together to avoid duplication of activities and learn lessons and best practices from each other, The focus of Joint Programme on Local Governance (JPLG) is on strengthening of service delivery through a decentralized approach. The two programmes are interacting with each other on a quarterly basis and expect a more coordinated response in future through Community Management Strategy for the health sector, The UNFPA/UNICEF Joint Programme on FGM/C was launched in 2007 with the aim of contributing to reduction in the FGM/C practice among girls aged 0-12 years. The JHNP provides support to critical parts of the FGM/C prevention and response strategy that are not covered or are underfunded by the global initiative: o Social mobilization through the Community Empowerment Programme, o Support to Medical Health Professionals, o FGM/C policy and family planning policies, o Community dialogues on FGM/C abandonment in CSZ, o Capacity building for Child Protection Advocates/Child Protection Committees, o C4D strategy and implementation. UNFPA Maternal Health Trust Funds were used by UNFPA to complement JHNP funds in providing support to training of health providers and to support the fistula programme in NEZ and CSZ. DANIDA & Brazil humanitarian response funds were utilized by UNFPA to support maternal mortality reduction interventions in NEZ and CSZ and 24 Maternity Waiting Homes were established. The JHNP through UNFPA is supporting three homes in NEZ. Page 69
72 5. Lessons Learnt and the Way Forward Programme specific lessons in the three categories are as following: 1: Working with Partners The health authorities led the governance mechanism at the Zonal and Technical level with full participation of key stakeholders (government officials, three UN agencies, and observers). Donors participate in TCG meetings as observers and for their strategic inputs quarterly donor briefings are held. The SC is the final decision making body chaired by UNRC and is attended by three MoHs, Representatives of three UN agencies and all JHNP donors. This has contributed to greater understanding of the programme, improved coordination and a progressive decision-making process. This will help to pave the way for increased harmonisation of health sector support to the government. The joint planning process and related coordination models could also be a useful entry point for improved sector-wide coordination, harmonization and alignment in coming years. 2: Best Practice and Innovation Development of the cadre of Midwives is based on theoretical and practical training. The need has been highlighted in the recent HRH assessment and Policy. The investment is directly linked to RMNCH outcomes and partners are coordinating with the programme to ensure consistent support. It is expected that this intervention will lead to an increase in skilled birth attendance, and a significant reduction in maternal and neonatal mortality levels. The programme is also providing an opportunity to strengthen coordination both with the public and private sector. Through JHNP, UN agencies aim to increase access to an EPHS in the nine targeted regions of the three zones of Somalia, mainly focusing on the two major health priorities (maternal and child health) of the agreed EPHS strategy. Through EPHS roll-out, the health sector is currently undergoing a paradigm shift from a traditional humanitarian operating environment to a post recovery setting, where partners are supporting the government structures to deliver EPHS through implementing partners such as NGOs. This is learning by doing exercise where the role of the government authorities is central and key for the success. This is the first time that an approach (government-led process), setting up mechanisms for their involvement at different levels, zonal, regional, TCG and SC has been applied in such a scale. The process has faced some challenges/changes and there are important lessons to be learnt, which include: Changes in operating modalities from humanitarian to development: The development approach is comparatively slow but likely to be sustainable, more effective and contributing to stability, Close coordination of the three UN agencies and commitment is the best practice to speed up the process (as an example the working of the ZWG in CSZ). Considering weak capacity, the standard operating procedures helps in ensuring a check and balance system and follow good procurement practices, Regular interaction of country level and zonal staff and on-the-job support helps in better understanding of rules and procedures and to avoid ambiguous messages. Political factors affecting the process: Follow DO NO HARM principles especially in a fragile country like Somalia, Regularly review political risks and allow local leadership/authorities to reach a conclusion through mutual consultation and without compromising on the principles, Regularly interaction with NGOs to sensitize them and to understand the challenges faced by them. Page 70
73 Challenges faced to ensure Delivery of Results : Continue to focus on delivery of results but provide technical support if difficulties are faced, Remain committed to ensure delivery of results, At the contractual stage, clarify linkage of payments with the delivery of results/ performance and its process, Strengthen and support monitoring and review system of the authorities rather than creating another vertical system. Changes in funding modalities and high expectations: In the meetings with authorities and NGOs, donors should highlight the need for prioritization and the factual funding status, Both humanitarian and development approaches need continued support from donors in the rehabilitation phase, The unit cost analysis is helpful to convince partners to suggest reasonable cost, Gradually move towards open competitive process while considering the Somali context. Changes in organizational structures influencing work stream: Involve NGOs through a constructive dialogue at different levels to facilitate understanding of the challenges, Regular risk assessment of partners helps in the success of contractual agreements. 3: Programme Management There are some key lessons that have been learnt during the implementation. Since the beginning of any such programme, the following needs to be considered: In a programme led by multiple agencies, strong coherence should be shown by the top leadership, which has a very positive trickle-down effect on the success of a programme, Carefully develop the programme governance structure and ensure regular, consistent consultations which are critical for the success of a programme, Three management areas should be focused from the start of the programme: i) Transparency in the use of resources, ii) Simple but effective planning mechanism with involvement of stakeholders at different levels and iii) focusing on the delivery of results. Programme Priorities for 2014 Considering lessons learnt during 2013, key Programmatic priorities for the year 2014 are as following: Finalize Policy and Strategic documents on which work has initiated and get the endorsement of health authorities to initiate action, Complete the process of EPHS roll-out in targeted regions and focus on provision of quality essential RMNCH and nutrition services, Further scale-up training of midwives and strengthen in-service training of health providers, Scale-up community based integrated essential services, Prioritize cross-cutting issues including WASH and FGM/C, Conduct Joint Annual Review of HSSPs AWPs-2013 and develop AWPs-2014, Develop and implement a Fund Raising Strategy for JHNP, Revise the JHNP Log Frame, Conduct the next round of Joint Rolling Plan through a comprehensive consultative process, Page 71
74 Initiate the process to strengthen Regional Health Management Teams. Finalize SOP004 and strengthen monitoring and review system at all levels to ensure delivery of results; Review SOP001 to further strengthen governance mechanism based on lessons learnt. Harmonize programme activities with the reforms under Somali Compact initiatives, Identify fiduciary risks and strengthen financial management systems of the health authorities, Continue to identify constrained activities and further improve implementation of agreed activities, Effective coordination with other programmes and interventions. Page 72
75 ANNEXURE A JHNP: List of Reference Documents Code Title Month/ Year Lead Organization Partner Organization Output 01: Leadership and Governance OP TFG Health Policy Framework Apr 2012 MoH CSS WHO OP Puntland Health Policy Framework Apr 2012 MoH PL WHO OP Central South Somalia Health Sector Strategic Plan Feb 2013 MoH CSS WHO & UNICEF and AWP 2013 OP Puntland Health Sector Strategic Plan and Feb 2013 MoH PL WHO & UNICEF AWP 2013 OP Somaliland Health Sector Strategic Plan and Feb 2013 MoH SL WHO & UNICEF AWP 2013 OP Prioritization of Health Policy Actions in the Somali Mar 2013 MoH CSS, PL and SL WHO Health Sector (Draft) OP Tostan Evaluation report combined Northwest and Northeast Zones Dec 2013 Family Support Institute (FASI) UNICEF OP Tostan Evaluation report Northwest zone Dec 2013 Family Support Institute (FASI) UNICEF OP Tostan Evaluation report Northeast zone Dec 2013 Family Support Institute (FASI) UNICEF OP Female Genital Mutilation/ Cutting Policy (Draft) Feb 2013 MoWDFA UNICEF Government of Puntland OP The Prohibition of Female Genital Mutilation Act Feb 2013 MoWDFA UNICEF (Draft) - Puntland OP Revised Reproductive Health Policy and action plans Feb 2013 MoH CSS, PL and SL UNFPA (Draft) 0P National Action Plan for Nutrition for all three zones Aug 2013 Go CSS, PL and SL UNICEF 0P Micronutrient Strategy (Draft) Jan 2013 Go CSS, PL and SL UNICEF 0P ToRs for the Development of Somali Community Jul 2013 Go CSS, PL and SL WHO based health care Strategy OP Tool to Assess Health Law - EMRO Jul 2013 WHO EMRO OP Right to Health assessment tool - EMRO Jul 2013 WHO EMRO OP Public Health Law Assessment for Somaliland, Jan 2014 MoH CSS, PL and SL WHO Puntland and Central South Somalia (Draft) OP Right to Health assessment report for Somaliland, Jan 2014 MoH CSS, PL and SL - WHO Puntland and Central South Somalia (Draft) OP Conference Declaration National Health Nov 2014 FGS, MoHDPS - WHO Conference for Somalia Transforming Somali s Health Sector OP ToRs of Joint Annual Review Nov 2013 JAR Task Force OP ToRs of Joint Annual Review Task Force Dec 2013 JAR Task Force OP GAVI Supervisory Tools 2013 MoH CSS, PL and SL - GAVI-HSS OP Minutes of HSC and HAB meetings 2013 MoH CSZ, PL and SL - WHO OP Health Sector Coordination - Institutional Analysis of May 2013 MoH CSZ, PL and SL - DFID Organizational and Governance Arrangements OP Joint Communiqué to Stakeholders on Somali Health Sector Coordination (Draft) Dec 2013 MoH CSS, PL and SL/ UN agencies - WHO OP Minutes of ZWGs and ZHSCs meetings 2013 MoH CSS, PL and SL - UNICEF Page 73
76 Code Title Month/ Year Lead Organization Partner Organization OP A Programme for Improving Governance, Leadership Feb 2013 MoH CSS, PL and SL - GFATM/WHO and Management Capacity of the three health authorities in Somalia OP ToRs of Long term TA RH advisers Dec 2012 MoH CSS, PL and SL - UNFPA OP ToRs of Long term TA M&E advisers Oct 2013 MoH CSS, PL and SL - WHO OP ToRs of Assessing Capacities of Somali Health Authorities for Contracting Health Services Oct 2013 MoH CSS, PL and SL - WHO Output 02: Health Workforce OP Human Resources for Health Assessment and Policy Feb 2014 MoH CSS - WHO for CSS (Draft) OP Human Resources for Health Strategic Plan for CSS Feb 2014 MoH CSS - WHO (Draft) OP Human Resources for Health Assessment and Policy Feb 2014 MoH PL - WHO for Puntland (Draft) OP Human Resources for Health Strategic Plan for Feb 2014 MoH PL - WHO Puntland (Draft) OP Review of Compensation, Salaries, Incentives and Mar 2013 MoH CSS, PL and SL - UNICEF Benefits for Health Personnel in Somalia OP Proposal of Somaliland National Health Professionals Nov 2013 NHPC - WHO Commission (NHPC) OP Progress reports on Midwifery training/ schools 2013 Partners - UNFPA OP Training material for Emergency Obstetric care Feb 2014 MoH CSS, PL and SL - WHO Diploma: a: Trainers manual b: Guide for trainers c: Participants manual OP Birth spacing guidelines for all zones (Draft) Dec 2013 MoH CSS, PL and SL - UNFPA OP Training material for CHW: Aug 2013 MoH CSS and PL - WHO a: Trainers manual b: Participants manual OP Somaliland CHW TOT manual and curriculum Mar 2013 MoH SL - THET OP BEmONC training reports Jun 2013 MoH PL - UNFPA Output 03: RMNCH and Nutrition services OP Assessment to roll out EPHS in Togdheer, SL Jul 2013 ZWG SL - UNICEF OP Assessment to roll out EPHS in Nugal, PL Jun 2013 ZWG PL - UNICEF OP Assessment to roll out EPHS in Galgadud, Banadir Jul 2013 ZWG CSS - UNICEF and Gedo, CSS OP Assessment to roll out EPHS in Mudug, PL Oct 2013 ZWG PL - UNICEF OP Assessment to roll out EPHS in Awdal, SL Dec 2013 ZWG SL - UNICEF OP PCA with SRCS(2) & SCODO(2), Togdheer, SL Sep 2013 UNICEF OP PCA with WVi(2) & SRCS(2), Nugal, PL Oct 2013 UNICEF OP PCA with SWISSO KALMO(1), Galgadud, CSS Mar 2013 UNICEF OP PCA with CISP(1), Banadir, CSS Mar 2013 UNICEF OP Progress reports on CEmONC services from hospitals 2013 Partners - UNFPA in CS OP Advocacy material for FGM/C abandonment interventions: May 2012 UNICEF - FGM/C MYTHS & FACTS handbill - Poster (Girl) - Poster (Mother & daughter) - Talking points for religious leaders - Pictorial story the protected one OP CHD 2013 coverage data from CSS Dec 2013 MoH CSS - UNICEF/WHO Page 74
77 Code Title Month/ Year Lead Organization Partner Organization Output 04: Health Financing OP Health Financing discussion meeting - notes and recommendations Nov 2013 MoH CSS, PL and SL - WHO, DFID, WB OP ToRs of Health Sector Expenditure review Mar 2014 MoH CSS, PL and SL - WHO OP ToRs of Fiduciary Risk Assessment (Draft) Mar 2014 MoH CSS, PL and SL - WHO Output 05: Medicines, Vaccines, RH & Nutrition Commodities and supplies OP Somali Standard Treatment Guidelines for April 2013 MoH CSS, PL and SL - WHO Management and Referral of Common Conditions at Primary Health Care OP GAVI-New Vaccines Support-Pentavalent vaccine- Nov 2012 MoH CSS, PL and SL - GAVI/UNICEF Decision Letter for Vaccine Support OP UNICEF Kit cost Nov 2013 UNICEF OP UNICEF WASH proposal to Go Spain Feb 2014 UNICEF - CSS OP Assessment of Medical Supply Systems in Somalia May 2013 GFATM - WHO OP Sustainable health care Reconstruction and Recovery- Infrastructure Development Plan Dec 2013 MoH CSS Output 06: Health Information OP HMIS 2013 data summary sheets for SL Feb 2013 MoH SL OP HMIS 2013 data summary sheets for PL Feb 2013 MoH PL OP HMIS 2013 data summary sheets for CSS Feb 2013 MoH CSS OP HMIS Assessment Report (MD) Mar 2014 MoH CSS, PL and SL - GFATM/UNICEF OP HSAT Work plan 2014 Jan 2014 HSAT OP Somaliland Emergency Obstetric Care Survey Report, 2012 MoH SL - UNFPA 2012 OP Routine Immunisation Non-Participation Survey April 2013 MoH SL, PL - UNICEF (RINPS), Somaliland and PL OP Baseline Survey CSS Concept Note and Tools Nov 2013 MoH CSS - WHO OP ToRs of HSAT technical officer May 2013 MoH CSS, PL and SL-WHO JHNP Documents JCU-001 MoU between Participating UN agencies (WHO, UNICEF and UNFPA) and UNICEF regarding Operational Aspects of a Somali Joint Health and Nutrition Programme - Addendum No. 1 JCU-002 Standard Administrative Arrangement between Government of United Kingdom of Great Britain and Northern Ireland and UNICEF regarding JHNP - Addendum No.1 - Addendum No. 2 JCU-003 JCU-004 Standard Administrative Arrangement between Government of Australia/ AusAID and UNICEF regarding JHNP Standard Administrative Arrangement between Government of Sweden (represented by SIDA) and UNICEF regarding JHNP - Addendum No.1 - Addendum No. 2 - Addendum No. 3 Feb 2012 Jan 2013 Mar 2012 Nov 2012 Mar 2012 June 2012 Dec 2012 May 2013 May 2013 UNICEF, UNFPA and WHO UNICEF and Government of UK/ DFID UNICEF and Government of Australia/ AusAID UNICEF and Government of Sweden/ SIDA JCU-005 JHNP proposal to USAID (1) Sep 2012 UNICEF and USAID Page 75
78 Code Title Month/ Year JHNP proposal to USAID - Modification (2) Aug MOD 1 Dec MOD 2 Feb 2014 UN Agency to UN Agency Contribution Agreement (USAID Grant) Nov 2012 Lead Organization Partner Organization UNICEF and WHO/UNFPA JCU-006 Initial JHNP proposal Jan 2012 Inputs from Somali Health Authorities, UN agencies and Donors JCU-007 Strategic concept and design document Mar 2012 UN agencies with inputs from SHAs and Donors JCU-008 JHNP Programme Document (developed in Aug 2013 Oct 2013 All JHNP partners - JCU and approved by SC on 4 Oct 2013) JCU-009 JHNP Compact A Somali compact for achieving the Oct 2014 All JHNP partners - JCU Health MDGs JCU-010 Risk Register JHNP Aug 2013 UNICEF, UNFPA and WHO - JCU JCU-011 SOP001 - Programme activity prioritization and budget allocation within the JHNP Jan 2013 MoH CSS, PL and SL/ UN agencies (UNICEF, UNFPA and WHO) - JCU - ToRs of Steering Committee Aug ToRs of TCG Aug ToRs of ZWGs Sep 2012 JCU-012 SOP002 - Implementing partner selection within the JHNP Oct 2013 MoH CSS, PL and SL/ UN agencies (UNICEF, UNFPA and WHO) - JCU JCU-013 SOP003 - Recruitment, remuneration and performance management of Long term TA for health authorities within JHNP Oct 2013 JCU-014 SOP004 - Monitoring and review for the JHNP (draft Feb 2014 cleared by TCG) JCU-015 Minutes of Steering Committee meetings Mar, Aug, Oct, Nov 2013 JCU-016 Minutes of Technical Coordination Group meetings Feb, Jul, Sep, Oct 2013 Feb 2014 JCU-017 Briefing papers and minutes of Donors briefings Nov 2012 Mar, Jul, Oct, Nov 2013 Jan 2014 MoH CSS, PL and SL/ UN agencies (UNICEF, UNFPA and WHO) - JCU MoH CSS, PL and SL/ UN agencies (UNICEF, UNFPA and WHO) - JCU All Partners - JCU HAs, UN agencies - JCU Donors and UN agencies - JCU JCU-018 JHNP - Inception phase progress report Jun 2012 JHNP - JCU JCU-019 JHNP - Annual Progress report 2012 May 2013 JHNP - JCU JCU-020 JHNP - Annual Progress report 2013 (Draft) Mar 2014 JHNP - JCU JCU-021 JHNP - External annual review 2012 Jun 2013 DFID JCU-022 JHNP - Performance Improvement Plan and updates Aug 2013 DFID - JCU Feb 2014 JCU-023 Guiltiness for development of Joint Rolling Plan of JHNP JCU-024 Annual Joint Rolling Plan Nov 2013 ZWGs, TCG and SC - JCU JCU-025 Quarterly financial and activities updates Oct 2013, HAs, UN agencies - JCU Jan 2014 JCU-026 JHNP - Fund Raising Strategy (Draft) Mar 2014 JCU JCU-027 Challenges and lessons learnt during EPHS roll out Mar 2014 UNICEF - JCU JCU-028 Principles and Operational guidelines for payment of Ministry of Health Core staff (Draft) Mar 2014 TCG - JCU Page 76
79 Page 77




80 Expression of Thanks The UN Resident Coordinator for Somalia, Ministries of Health of Somaliland, Puntland and Federal Government of Somalia and United Nation Agencies of UNICEF, UNFPA and WHO would like to extend their sincere gratitude to the Governments of United Kingdom, Sweden, Australia and United States of America for their strategic support and generous contribution towards improved health systems for Somalis. Page 78
UHC. Moving toward. Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES. Public Disclosure Authorized
 Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
Health and Nutrition Public Investment Programme
 Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
 -DDA-3485-726-2334-Proposal 1 of 7 3/13/2015 9:46 AM Project Proposal Organization Project Title Code WFP (World Food Programme) Targeted Life Saving Supplementary Feeding Programme for Children 6-59 s,
-DDA-3485-726-2334-Proposal 1 of 7 3/13/2015 9:46 AM Project Proposal Organization Project Title Code WFP (World Food Programme) Targeted Life Saving Supplementary Feeding Programme for Children 6-59 s,
In 2012, the Regional Committee passed a
 Strengthening health systems for universal health coverage In 2012, the Regional Committee passed a resolution endorsing a proposed roadmap on strengthening health systems as a strategic priority, as well
Strengthening health systems for universal health coverage In 2012, the Regional Committee passed a resolution endorsing a proposed roadmap on strengthening health systems as a strategic priority, as well
Harmonization for Health in Africa (HHA) An Action Framework
 An Action Framework") Harmonization for Health in Africa (HHA) An Action Framework 1 Background 1.1 In Africa, the twin effect of poverty and low investment in health has led to an increasing burden of diseases notably HIV/AIDS,
Harmonization for Health in Africa (HHA) An Action Framework 1 Background 1.1 In Africa, the twin effect of poverty and low investment in health has led to an increasing burden of diseases notably HIV/AIDS,
Egypt. MDG 4 and Beyond. Emad Ezzat, MD Head of PHC Sector. Ministry of Health & Population
 Egypt Ministry of Health & Population MDG 4 and Beyond Lessons Learnt Emad Ezzat, MD Head of PHC Sector EMRO high-level meeting, Dubai, Jan 2013 Trends of Under 5, Infant and Neonatal Mortality (1990 2008)
Egypt Ministry of Health & Population MDG 4 and Beyond Lessons Learnt Emad Ezzat, MD Head of PHC Sector EMRO high-level meeting, Dubai, Jan 2013 Trends of Under 5, Infant and Neonatal Mortality (1990 2008)
Somalia Is any part of this project cash based intervention (including vouchers)? Conditionality:
? Conditionality:") Somalia 2018 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives HEALTH POVERTY ACTION (HPA) Emergency Nutrition Interventions for IDPs in Somaliland 2018 (NutriSom) SOM-18/N/121295
Somalia 2018 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives HEALTH POVERTY ACTION (HPA) Emergency Nutrition Interventions for IDPs in Somaliland 2018 (NutriSom) SOM-18/N/121295
Lessons learned in. Somalia Nutrition Cluster. Exercise conducted by the Global Nutrition Cluster
 Somalia Nutrition Cluster Lessons learned in Somalia Nutrition Cluster Exercise conducted by the Global Nutrition Cluster Synthesis Report 8 th September 2014 by GNC and Somalia Nutrition Cluster. Table
Somalia Nutrition Cluster Lessons learned in Somalia Nutrition Cluster Exercise conducted by the Global Nutrition Cluster Synthesis Report 8 th September 2014 by GNC and Somalia Nutrition Cluster. Table
Ethiopia Health MDG Support Program for Results
 Ethiopia Health MDG Support Program for Results Health outcome/output EDHS EDHS Change 2005 2011 Under 5 Mortality Rate 123 88 Decreased by 28% Infant Mortality Rate 77 59 Decreased by 23% Stunting in
Ethiopia Health MDG Support Program for Results Health outcome/output EDHS EDHS Change 2005 2011 Under 5 Mortality Rate 123 88 Decreased by 28% Infant Mortality Rate 77 59 Decreased by 23% Stunting in
Sudan Ministry of Health Capacity Development Plan
 Sudan Ministry of Health Capacity Development Plan Progress Report: January June 2016 1 Photograph Hassan Bablonia Contents Background 2 Partnership between FMOH and UNDP 3 CD Plan Implementation Arrangements
Sudan Ministry of Health Capacity Development Plan Progress Report: January June 2016 1 Photograph Hassan Bablonia Contents Background 2 Partnership between FMOH and UNDP 3 CD Plan Implementation Arrangements
The Syrian Arab Republic
 World Health Organization Humanitarian Response Plans in 2015 The Syrian Arab Republic Baseline indicators* Estimate Human development index 1 2013 118/187 Population in urban areas% 2012 56 Population
World Health Organization Humanitarian Response Plans in 2015 The Syrian Arab Republic Baseline indicators* Estimate Human development index 1 2013 118/187 Population in urban areas% 2012 56 Population
Puntland Nutrition Working Group
 N U T RITIO N CL U S T E R M E ET I N G M I N U T ES 29 TH DECEMBER 2013, MOH-HQ CONFERENCE HALL, GAROWE PUNTLAND, SOMALIA Overall Objectives The overall objective of the Nutrition Cluster meeting is to
N U T RITIO N CL U S T E R M E ET I N G M I N U T ES 29 TH DECEMBER 2013, MOH-HQ CONFERENCE HALL, GAROWE PUNTLAND, SOMALIA Overall Objectives The overall objective of the Nutrition Cluster meeting is to
Mongolia. Situation Analysis. Policy Context Global strategy on women and children/ commitment. National Health Sector Plan and M&E Plan
 COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment* Manila, Philippines Accountability Workshop, March 19-20, 2012 Information updated: April 19, 2012 Policy Context Global strategy on women and children/ commitment
COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment* Manila, Philippines Accountability Workshop, March 19-20, 2012 Information updated: April 19, 2012 Policy Context Global strategy on women and children/ commitment
Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder
 Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder Newborn Health in Humanitarian Settings: Background Newborn Health in Humanitarian Settings 16 February 2017 An
Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder Newborn Health in Humanitarian Settings: Background Newborn Health in Humanitarian Settings 16 February 2017 An
Period of June 2008 June 2011 Partner Country s Implementing Organization: Federal Cooperation
 Summary of Terminal Evaluation Results 1. Outline of the Project Country: Sudan Project title: Frontline Maternal and Child Health Empowerment Project (Mother Nile Project) Issue/Sector: Maternal and Child
Summary of Terminal Evaluation Results 1. Outline of the Project Country: Sudan Project title: Frontline Maternal and Child Health Empowerment Project (Mother Nile Project) Issue/Sector: Maternal and Child
Saving Every Woman, Every Newborn and Every Child
 Saving Every Woman, Every Newborn and Every Child World Vision s role World Vision is a global Christian relief, development and advocacy organization dedicated to improving the health, education and protection
Saving Every Woman, Every Newborn and Every Child World Vision s role World Vision is a global Christian relief, development and advocacy organization dedicated to improving the health, education and protection
UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION
 COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION") UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION UNICEF H&NH Outcome: UNICEF H&N OP #: 3 UNICEF Work Plan Activity: Objective:
UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION UNICEF H&NH Outcome: UNICEF H&N OP #: 3 UNICEF Work Plan Activity: Objective:
Mauritania Red Crescent Programme Support Plan
 Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
PROJECT INFORMATION DOCUMENT (PID) APPRAISAL STAGE
 APPRAISAL STAGE") PROJECT INFORMATION DOCUMENT (PID) APPRAISAL STAGE Report No.: AB7702 Project Name System Enhancement for Health Action in Transition (SEHAT) - Additional Financing Region SOUTH ASIA Country Afghanistan
PROJECT INFORMATION DOCUMENT (PID) APPRAISAL STAGE Report No.: AB7702 Project Name System Enhancement for Health Action in Transition (SEHAT) - Additional Financing Region SOUTH ASIA Country Afghanistan
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r
 RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
TERMS OF REFERENCE: PRIMARY HEALTH CARE
 TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
SOMALIA NUTRITION CLUSTER
 SOMALIA NUTRITION CLUSTER QUARTER II, 2016 AFTER ACTION REVIEW MEETING Meeting Proceeding and Highlights 15 th - 16 th August 2016, Jacaranda Nairobi, Kenya Page 0 Contents Introduction... 2 Day 1, Session
SOMALIA NUTRITION CLUSTER QUARTER II, 2016 AFTER ACTION REVIEW MEETING Meeting Proceeding and Highlights 15 th - 16 th August 2016, Jacaranda Nairobi, Kenya Page 0 Contents Introduction... 2 Day 1, Session
USAID/Philippines Health Project
 USAID/Philippines Health Project 2017-2021 Redacted Concept Paper As of January 24, 2017 A. Introduction This Concept Paper is a key step in the process for designing a sector-wide USAID/Philippines Project
USAID/Philippines Health Project 2017-2021 Redacted Concept Paper As of January 24, 2017 A. Introduction This Concept Paper is a key step in the process for designing a sector-wide USAID/Philippines Project
SOMALIA. In Brief. Appeal no /2003; Appeal target: CHF 2,365,686 Programme Update No. 1; Period covered: January to March, 2003
 SOMALIA Appeal no. 01.09/2003; Appeal target: CHF 2,365,686 Programme Update No. 1; Period covered: January to March, 2003 16 June 2003 The Federation s mission is to improve the lives of vulnerable people
SOMALIA Appeal no. 01.09/2003; Appeal target: CHF 2,365,686 Programme Update No. 1; Period covered: January to March, 2003 16 June 2003 The Federation s mission is to improve the lives of vulnerable people
How can the township health system be strengthened in Myanmar?
 How can the township health system be strengthened in Myanmar? Policy Note #3 Myanmar Health Systems in Transition No. 3 A WPR/2015/DHS/003 World Health Organization (on behalf of the Asia Pacific Observatory
How can the township health system be strengthened in Myanmar? Policy Note #3 Myanmar Health Systems in Transition No. 3 A WPR/2015/DHS/003 World Health Organization (on behalf of the Asia Pacific Observatory
Contracting Out Health Service Delivery in Afghanistan
 Contracting Out Health Service Delivery in Afghanistan Dr M.Nazir Rasuli General director Care of Afghan Families,CAF. Kathmando Nepal 12 Jun,2012 Outline 1. Background 2. BPHS 3. Contracting with NGOs,
Contracting Out Health Service Delivery in Afghanistan Dr M.Nazir Rasuli General director Care of Afghan Families,CAF. Kathmando Nepal 12 Jun,2012 Outline 1. Background 2. BPHS 3. Contracting with NGOs,
SOMALILAND NUTRITION WORKING GROUP
 NUTRITION WORKING GROUP MEETING MINUTES Thursday, 5 th of December 2013 at 10:30am Ambassador Hotel Meeting Hall, Hargeisa, Somaliland 1. Welcome and Introductions: The meeting was chaired by Dr Ahmed
NUTRITION WORKING GROUP MEETING MINUTES Thursday, 5 th of December 2013 at 10:30am Ambassador Hotel Meeting Hall, Hargeisa, Somaliland 1. Welcome and Introductions: The meeting was chaired by Dr Ahmed
Solomon Islands experience Final 5 June 2004
 Solomon Islands experience Final 5 June 2004 1. Background Information Solomon Islands is a Pacific island nation with a total population of 409,042, an annual growth rate of 2.8% and a life expectancy
Solomon Islands experience Final 5 June 2004 1. Background Information Solomon Islands is a Pacific island nation with a total population of 409,042, an annual growth rate of 2.8% and a life expectancy
Monitoring and Evaluation (M&E) Strategy. April 2013
 Strategy. April 2013") Monitoring and Evaluation (M&E) Strategy April 2013 Disclaimer The document is an internal document aimed to cover all consortium members, County partners as well as linkages with DFID where appropriate.
Monitoring and Evaluation (M&E) Strategy April 2013 Disclaimer The document is an internal document aimed to cover all consortium members, County partners as well as linkages with DFID where appropriate.
Summary of UNICEF Emergency Needs for 2009*
 UNICEF Humanitarian Action in 2009 Core Country Data Population under 18 (thousands) 11,729 U5 mortality rate 73 Infant mortality rate 55 Maternal mortality ratio (2000 2007, reported) Primary school enrolment
UNICEF Humanitarian Action in 2009 Core Country Data Population under 18 (thousands) 11,729 U5 mortality rate 73 Infant mortality rate 55 Maternal mortality ratio (2000 2007, reported) Primary school enrolment
In , WHO technical cooperation with the Government is expected to focus on the following WHO strategic objectives:
 VANUATU Vanuatu, a Melanesian archipelago of 83 islands and more than 100 languages, has a land mass of 12 189 square kilometres and a population of 234 023 in 2009 (National Census). Vanuatu has a young
VANUATU Vanuatu, a Melanesian archipelago of 83 islands and more than 100 languages, has a land mass of 12 189 square kilometres and a population of 234 023 in 2009 (National Census). Vanuatu has a young
Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan
 Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan Date: Prepared by: February 7, 2017 Dr. Taban Martin Vitale I. Demographic Information
Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan Date: Prepared by: February 7, 2017 Dr. Taban Martin Vitale I. Demographic Information
DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL
 DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL The fight against malnutrition and hunger in the Democratic Republic of Congo (DRC) is a challenge that Action Against Hunger has worked to address
DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL The fight against malnutrition and hunger in the Democratic Republic of Congo (DRC) is a challenge that Action Against Hunger has worked to address
ANNEX. 2. RATIONALE This proposal is financed by the Special Funds for Sudan (SFS), allocated by Council Decision number 2010/406/EU.
, allocated by Council Decision number 2010/406/EU.") ANNEX 1. IDENTIFICATION Title/Number Total cost Aid method / Method of implementation SUDAN: Rider - Strengthening Sudan Health Services (SSHS) - CRIS No SD/FED/023-301 EUR 12 000 000 (no modification)
ANNEX 1. IDENTIFICATION Title/Number Total cost Aid method / Method of implementation SUDAN: Rider - Strengthening Sudan Health Services (SSHS) - CRIS No SD/FED/023-301 EUR 12 000 000 (no modification)
REVIEW ARTICLE Human Resource Requirement Under the Context of Universal Health Coverage (UHC) in Bangladesh: Current Situation and Future Challenges
 in Bangladesh: Current Situation and Future Challenges") REVIEW ARTICLE Human Resource Requirement Under the Context of Universal Health Coverage (UHC) in Bangladesh: Current Situation and Future Challenges *MHK Talukder 1, MM Rahman 2, M Nuruzzaman 3 1 Professor
REVIEW ARTICLE Human Resource Requirement Under the Context of Universal Health Coverage (UHC) in Bangladesh: Current Situation and Future Challenges *MHK Talukder 1, MM Rahman 2, M Nuruzzaman 3 1 Professor
A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH
 EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
National Health Strategy
 State of Palestine Ministry of Health General directorate of Health Policies and Planning National Health Strategy 2017-2022 DRAFT English Summary By Dr. Ola Aker October 2016 National policy agenda Policy
State of Palestine Ministry of Health General directorate of Health Policies and Planning National Health Strategy 2017-2022 DRAFT English Summary By Dr. Ola Aker October 2016 National policy agenda Policy
South Sudan Country brief and funding request February 2015
 PEOPLE AFFECTED 6 400 000 affected population 3 358 100 of those in affected, targeted for health cluster support 1 500 000 internally displaced 504 539 refugees HEALTH SECTOR 7% of health facilities damaged
PEOPLE AFFECTED 6 400 000 affected population 3 358 100 of those in affected, targeted for health cluster support 1 500 000 internally displaced 504 539 refugees HEALTH SECTOR 7% of health facilities damaged
Incorporating the Right to Health into Health Workforce Plans
 Incorporating the Right to Health into Health Workforce Plans Key Considerations Health Workforce Advocacy Initiative November 2009 Using an easily accessible format, this document offers guidance to policymakers
Incorporating the Right to Health into Health Workforce Plans Key Considerations Health Workforce Advocacy Initiative November 2009 Using an easily accessible format, this document offers guidance to policymakers
NUTRITION. UNICEF Meeting Myanmar/2014/Myo the Humanitarian Needs Thame of Children in Myanmar Fundraising Concept Note 5
 NUTRITION Improving Equitable Access to Essential Nutrition Interventions for Conflict-Affected Populations in Rakhine, Kachin and Northern Shan States 1 UNICEF Meeting Myanmar/2014/Myo the Humanitarian
NUTRITION Improving Equitable Access to Essential Nutrition Interventions for Conflict-Affected Populations in Rakhine, Kachin and Northern Shan States 1 UNICEF Meeting Myanmar/2014/Myo the Humanitarian
Biennial Collaborative Agreement
 Biennial Collaborative Agreement between the Ministry of Health of Kazakhstan and the Regional Office for Europe of the World Health Organization 2010/2011 Signed by: For the Ministry of Health Signature
Biennial Collaborative Agreement between the Ministry of Health of Kazakhstan and the Regional Office for Europe of the World Health Organization 2010/2011 Signed by: For the Ministry of Health Signature
INTRODUCTION. 76 MCHIP End-of-Project Report. (accessed May 8, 2014).
.") Redacted INTRODUCTION Between 1990 and 2012, India s mortality rate in children less than five years of age declined by more than half (from 126 to 56/1,000 live births). The infant mortality rate also
Redacted INTRODUCTION Between 1990 and 2012, India s mortality rate in children less than five years of age declined by more than half (from 126 to 56/1,000 live births). The infant mortality rate also
Minister. Secretaries of State. Department of Planning and Health Information. Department of Human Resources Development
 KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
Maternal, infant and young child nutrition: implementation plan
 SIXTY-FOURTH WORLD HEALTH ASSEMBLY A64/22 Provisional agenda item 13.13 24 March 2011 Maternal, infant and young child nutrition: implementation plan Report by the Secretariat 1. In May 2010, the Health
SIXTY-FOURTH WORLD HEALTH ASSEMBLY A64/22 Provisional agenda item 13.13 24 March 2011 Maternal, infant and young child nutrition: implementation plan Report by the Secretariat 1. In May 2010, the Health
WORLD HEALTH ORGANIZATION. Strengthening nursing and midwifery
 WORLD HEALTH ORGANIZATION FIFTY-SIXTH WORLD HEALTH ASSEMBLY A56/19 Provisional agenda item 14.11 2 April 2003 Strengthening nursing and midwifery Report by the Secretariat 1. The Millennium Development
WORLD HEALTH ORGANIZATION FIFTY-SIXTH WORLD HEALTH ASSEMBLY A56/19 Provisional agenda item 14.11 2 April 2003 Strengthening nursing and midwifery Report by the Secretariat 1. The Millennium Development
Uzbekistan: Woman and Child Health Development Project
 Validation Report Reference Number: PVR-331 Project Number: 36509 Loan Number: 2090 September 2014 Uzbekistan: Woman and Child Health Development Project Independent Evaluation Department ABBREVIATIONS
Validation Report Reference Number: PVR-331 Project Number: 36509 Loan Number: 2090 September 2014 Uzbekistan: Woman and Child Health Development Project Independent Evaluation Department ABBREVIATIONS
CONSOLIDATED RESULTS REPORT. Country: ANGOLA Programme Cycle: 2009 to
 CONSOLIDATED RESULTS REPORT Country: ANGOLA Programme Cycle: 2009 to 2014 1 1. Key Results modified or added 2. Key Progress Indicators 3. Description of Results Achieved PCR 1: Accelerated Child Survival
CONSOLIDATED RESULTS REPORT Country: ANGOLA Programme Cycle: 2009 to 2014 1 1. Key Results modified or added 2. Key Progress Indicators 3. Description of Results Achieved PCR 1: Accelerated Child Survival
MALAWI. COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment*, Dar-es-Salaam, Tanzania, February 13-15, 2012
 COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment*, Dar-es-Salaam, Tanzania, February 13-15, 2012 Policy Context Global strategy on women and children/ commitment National Health policy/national Health Plan/Strategies
COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment*, Dar-es-Salaam, Tanzania, February 13-15, 2012 Policy Context Global strategy on women and children/ commitment National Health policy/national Health Plan/Strategies
Global Health Workforce Crisis. Key messages
 Global Health Workforce Crisis Key messages - 2013 Despite the increased evidence that health workers are fundamental for ensuring equitable access to health services and achieving universal health coverage,
Global Health Workforce Crisis Key messages - 2013 Despite the increased evidence that health workers are fundamental for ensuring equitable access to health services and achieving universal health coverage,
CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES. Tajikistan
 CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES Tajikistan In 2010, a string of emergencies caused by natural disasters and epidemics affected thousands of children and women in Tajikistan,
CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES Tajikistan In 2010, a string of emergencies caused by natural disasters and epidemics affected thousands of children and women in Tajikistan,
Shaping the future of health in the WHO Eastern Mediterranean Region: reinforcing the role of WHO WHO-EM/RDO/002/E
 Shaping the future of health in the WHO Eastern Mediterranean Region: reinforcing the role of WHO WHO-EM/RDO/002/E WHO-EM/RDO/002/E Shaping the future of health in the WHO Eastern Mediterranean Region:
Shaping the future of health in the WHO Eastern Mediterranean Region: reinforcing the role of WHO WHO-EM/RDO/002/E WHO-EM/RDO/002/E Shaping the future of health in the WHO Eastern Mediterranean Region:
GUIDELINES FOR HEALTH SYSTEM ASSESSMENT
 GUIDELINES FOR HEALTH SYSTEM ASSESSMENT Myanmar June 13 2009 Map: Planned Priority Townships for Health System Strengthening 2008-2011 1 TABLE OF CONTENTS BOOK 1 SURVEYOR GUIDELINES List of Figures...
GUIDELINES FOR HEALTH SYSTEM ASSESSMENT Myanmar June 13 2009 Map: Planned Priority Townships for Health System Strengthening 2008-2011 1 TABLE OF CONTENTS BOOK 1 SURVEYOR GUIDELINES List of Figures...
Frequently Asked Questions Funding Cycle
 Frequently Asked Questions 2017-2019 Funding Cycle November 2017 Table of Contents The Funding Model... 1 Eligibility and Allocations... 3 Differentiated Application Process... 6 Preparing a Funding Request...
Frequently Asked Questions 2017-2019 Funding Cycle November 2017 Table of Contents The Funding Model... 1 Eligibility and Allocations... 3 Differentiated Application Process... 6 Preparing a Funding Request...
Nurturing children in body and mind
 Nurturing children in body and mind Dr Rachel Devi National Advisor for Family Health Ministry of Health and Medical Services, Fiji 11 th Pacific Health Ministers Meeting 15-17 April 2015 Yanuca Island,
Nurturing children in body and mind Dr Rachel Devi National Advisor for Family Health Ministry of Health and Medical Services, Fiji 11 th Pacific Health Ministers Meeting 15-17 April 2015 Yanuca Island,
Senegal Humanitarian Situation Report
 Senegal Humanitarian Situation Report Highlights 4,015 children have been admitted to treatment in January and February, or 11% of the annual target. The national Infant and Young Child Feeding policy
Senegal Humanitarian Situation Report Highlights 4,015 children have been admitted to treatment in January and February, or 11% of the annual target. The national Infant and Young Child Feeding policy
Islamic Republic of Afghanistan Ministry of Public Health
 21 April 2007 Islamic Republic of Afghanistan Ministry of Public Health National Strategic Plan for the Monitoring and Evaluation Department 1386 1390 National Strategy for Monitoring and Evaluation 1386-1390
21 April 2007 Islamic Republic of Afghanistan Ministry of Public Health National Strategic Plan for the Monitoring and Evaluation Department 1386 1390 National Strategy for Monitoring and Evaluation 1386-1390
Primary objective: Gain a global perspective on child health by working in a resource- limited setting within a different cultural context.
 Global health elective competency- based objectives for pediatric residents (These objectives can be adapted by the resident s institution to pertain to a specific elective site) Primary objective: Gain
Global health elective competency- based objectives for pediatric residents (These objectives can be adapted by the resident s institution to pertain to a specific elective site) Primary objective: Gain
HEALTH SYSTEMS FUNDING PLATFORM - WORK PLAN OCTOBER 2010 JUNE 2011 BACKGROUND
 HEALTH SYSTEMS FUNDING PLATFORM - WORK PLAN OCTOBER 2010 JUNE 2011 BACKGROUND Countries, partners, global health initiatives, and funding agencies increasingly recognize that weak health systems are an
HEALTH SYSTEMS FUNDING PLATFORM - WORK PLAN OCTOBER 2010 JUNE 2011 BACKGROUND Countries, partners, global health initiatives, and funding agencies increasingly recognize that weak health systems are an
Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan
 Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan Date: June 13, 2016 Prepared by: Dr. Taban Martin Vitale 1. City & State Bor, Jonglei
Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan Date: June 13, 2016 Prepared by: Dr. Taban Martin Vitale 1. City & State Bor, Jonglei
Water, sanitation and hygiene in health care facilities in Asia and the Pacific
 Water, sanitation and hygiene in health care facilities in Asia and the Pacific A necessary step to achieving universal health coverage and improving health outcomes This note sets out the crucial role
Water, sanitation and hygiene in health care facilities in Asia and the Pacific A necessary step to achieving universal health coverage and improving health outcomes This note sets out the crucial role
UNICEF Senegal Situation Report 23 July 2012 Highlights
 UNICEF Senegal Situation Report 23 July 2012 Highlights A national nutrition SMART survey completed to update the nutrition situation countrywide. The preliminary results are to be released by MoH on 25
UNICEF Senegal Situation Report 23 July 2012 Highlights A national nutrition SMART survey completed to update the nutrition situation countrywide. The preliminary results are to be released by MoH on 25
Strengthening Midwifery Education and Practice in Post-conflict Liberia. Nancy Taylor Moses ICM Triennial Congress Prague, Czech Republic June 2014
 Strengthening Midwifery Education and Practice in Post-conflict Liberia Nancy Taylor Moses ICM Triennial Congress Prague, Czech Republic June 2014 Objectives Describe strengthening midwifery education
Strengthening Midwifery Education and Practice in Post-conflict Liberia Nancy Taylor Moses ICM Triennial Congress Prague, Czech Republic June 2014 Objectives Describe strengthening midwifery education
5. The Regional Committee examined and adopted the actions proposed and the related resolution. AFR/RC65/6 24 February 2016
 24 February 2016 REGIONAL COMMITTEE FOR AFRICA ORIGINAL: ENGLISH Sixty-fifth session N Djamena, Republic of Chad, 23 27 November 2015 Agenda item 10 RESEARCH FOR HEALTH: A STRATEGY FOR THE AFRICAN REGION,
24 February 2016 REGIONAL COMMITTEE FOR AFRICA ORIGINAL: ENGLISH Sixty-fifth session N Djamena, Republic of Chad, 23 27 November 2015 Agenda item 10 RESEARCH FOR HEALTH: A STRATEGY FOR THE AFRICAN REGION,
Health: UNDAP Plan. Report Summary Responsible Agency # Key Actions Action Budget UNFPA 8 15,900,000 UNICEF 15 39,110,000 WFP 2 23,250, ,085,000
 Health: UNDAP Plan Report Summary Responsible Agency # Key Actions Action Budget 8 5,900,000 5 9,0,000 WFP,50,000 6 5 50,85,000 9,085,000 Relevant MDAs and LGAs develop, implement and monitor policies,
Health: UNDAP Plan Report Summary Responsible Agency # Key Actions Action Budget 8 5,900,000 5 9,0,000 WFP,50,000 6 5 50,85,000 9,085,000 Relevant MDAs and LGAs develop, implement and monitor policies,
Managing Programmes to Improve Child Health Overview. Department of Child and Adolescent Health and Development
 Managing Programmes to Improve Child Health Overview Department of Child and Adolescent Health and Development 1 Outline of this presentation Current global child health situation Effective interventions
Managing Programmes to Improve Child Health Overview Department of Child and Adolescent Health and Development 1 Outline of this presentation Current global child health situation Effective interventions
SOMALILAND NUTRITION WORKING GROUP
 Minutes of Nutrition Working Group Meeting Thursday, 4 th of July 2013 at 9:00am Ambassador Hotel Meeting Hall, Hargeisa, Somaliland AGENDA: 1 Welcome and Introductions. MOH Dr Ahmed 2 Review of the previous
Minutes of Nutrition Working Group Meeting Thursday, 4 th of July 2013 at 9:00am Ambassador Hotel Meeting Hall, Hargeisa, Somaliland AGENDA: 1 Welcome and Introductions. MOH Dr Ahmed 2 Review of the previous
#HealthForAll ichc2017.org
 #HealthForAll ichc2017.org 1 Positioning CHW s within HRH Strategies: Key Issues and Opportunities Liberia Case Study Ochiawunma Ibe, MD, MPH, Msc (MCH), FWACP Background Outline Demographic profile and
#HealthForAll ichc2017.org 1 Positioning CHW s within HRH Strategies: Key Issues and Opportunities Liberia Case Study Ochiawunma Ibe, MD, MPH, Msc (MCH), FWACP Background Outline Demographic profile and
#HealthForAll ichc2017.org
 #HealthForAll ichc2017.org Tamba Boima, Director of Community Health Services Division, Liberia Ministry of Health Mallika Raghavan, Director of National Community Health Systems, Last Mile Health Joint
#HealthForAll ichc2017.org Tamba Boima, Director of Community Health Services Division, Liberia Ministry of Health Mallika Raghavan, Director of National Community Health Systems, Last Mile Health Joint
RWANDA. COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment*, Dar-es-Salaam, Tanzania, February 13-15, 2012
 COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment*, Dar-es-Salaam, Tanzania, February 13-15, 2012 Policy Context Global strategy on women and children/ commitment National Health policy/national Health Plan/Strategies
COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment*, Dar-es-Salaam, Tanzania, February 13-15, 2012 Policy Context Global strategy on women and children/ commitment National Health policy/national Health Plan/Strategies
The World Breastfeeding Trends Initiative (WBTi)
") The World Breastfeeding Trends Initiative (WBTi) Name of the Country: Swaziland Year: 2009 MINISTRY OF HEALTH KINGDOM OF SWAZILAND 1 Acronyms AIDS ART CBO DHS EGPAF FBO MICS NGO AFASS ANC CHS CSO EPI HIV
The World Breastfeeding Trends Initiative (WBTi) Name of the Country: Swaziland Year: 2009 MINISTRY OF HEALTH KINGDOM OF SWAZILAND 1 Acronyms AIDS ART CBO DHS EGPAF FBO MICS NGO AFASS ANC CHS CSO EPI HIV
AUDIT OF THE UNDP AMKENI WAKENYA PROGRAMME KENYA. Report No Issue Date: 10 January 2014
 UNITED NATIONS DEVELOPMENT PROGRAMME AUDIT OF THE UNDP AMKENI WAKENYA PROGRAMME IN KENYA Report No. 1246 Issue Date: 10 January 2014 Table of Contents Executive Summary i I. Introduction 1 II. About the
UNITED NATIONS DEVELOPMENT PROGRAMME AUDIT OF THE UNDP AMKENI WAKENYA PROGRAMME IN KENYA Report No. 1246 Issue Date: 10 January 2014 Table of Contents Executive Summary i I. Introduction 1 II. About the
STRONG SYSTEMS SAVE LIVES
 STRONG SYSTEMS SAVE LIVES Health Systems Strengthening Component USAID Maternal and Child Health Program PAKISTAN August 2017 Competency and skills play a vital role in improving quality of care. Here,
STRONG SYSTEMS SAVE LIVES Health Systems Strengthening Component USAID Maternal and Child Health Program PAKISTAN August 2017 Competency and skills play a vital role in improving quality of care. Here,
BUILDING AN EFFECTIVE HEALTH WORKFORCE THROUGH IN-SERVICE TRAINING DELIVERED BY REGIONAL TRAINING HUBS: LESSONS FROM KENYA
 BUILDING AN EFFECTIVE HEALTH WORKFORCE THROUGH IN-SERVICE TRAINING DELIVERED BY REGIONAL TRAINING HUBS: LESSONS FROM KENYA January 2017 Peter Milo, Caroline Karutu, Peter Abwao, Stephen Mbaabu, and Isaac
BUILDING AN EFFECTIVE HEALTH WORKFORCE THROUGH IN-SERVICE TRAINING DELIVERED BY REGIONAL TRAINING HUBS: LESSONS FROM KENYA January 2017 Peter Milo, Caroline Karutu, Peter Abwao, Stephen Mbaabu, and Isaac
3MDG Strategy for Transition and to Address Sustainability 2
 3MDG Support to MNCH Service Delivery A Strategy for Transition and to Address Sustainability for work being currently financed in Delta and Magway updated 7 June 2016 This document consists of three main
3MDG Support to MNCH Service Delivery A Strategy for Transition and to Address Sustainability for work being currently financed in Delta and Magway updated 7 June 2016 This document consists of three main
RBF in Zimbabwe Results & Lessons from Mid-term Review. Ronald Mutasa, Task Team Leader, World Bank May 7, 2013
 RBF in Zimbabwe Results & Lessons from Mid-term Review Ronald Mutasa, Task Team Leader, World Bank May 7, 2013 Outline Country Context Technical Design Implementation Timeline Midterm Review Results Evaluation
RBF in Zimbabwe Results & Lessons from Mid-term Review Ronald Mutasa, Task Team Leader, World Bank May 7, 2013 Outline Country Context Technical Design Implementation Timeline Midterm Review Results Evaluation
IMCI and Health Systems Strengthening
 Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI and Health Systems Strengthening 7 IMCI and Health Systems Strengthening What components of the health
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI and Health Systems Strengthening 7 IMCI and Health Systems Strengthening What components of the health
Background Paper & Guiding Questions. Doctors in War Zones: International Policy and Healthcare during Armed Conflict
 Background Paper & Guiding Questions Doctors in War Zones: International Policy and Healthcare during Armed Conflict JUNE 2018 This discussion note was drafted by Alice Debarre, Policy Analyst on Humanitarian
Background Paper & Guiding Questions Doctors in War Zones: International Policy and Healthcare during Armed Conflict JUNE 2018 This discussion note was drafted by Alice Debarre, Policy Analyst on Humanitarian
WHO supports countries to develop responsive and resilient health systems that are centred on peoples needs and circumstances
 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 Service delivery Health workforce WHO supports countries to develop responsive and resilient health systems that are centred on peoples needs and circumstances Information
4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 Service delivery Health workforce WHO supports countries to develop responsive and resilient health systems that are centred on peoples needs and circumstances Information
Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012
 Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012 1 What has India achieved so far? Goals Achievements National Rural Health Mission (By
Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012 1 What has India achieved so far? Goals Achievements National Rural Health Mission (By
Comprehensive Evaluation of the Community Health Program in Rwanda. Concern Worldwide. Theory of Change
 Comprehensive Evaluation of the Community Health Program in Rwanda Concern Worldwide Theory of Change Concern Worldwide 1. Program Theory of Change Impact Sexual and Reproductive Health Maternal health
Comprehensive Evaluation of the Community Health Program in Rwanda Concern Worldwide Theory of Change Concern Worldwide 1. Program Theory of Change Impact Sexual and Reproductive Health Maternal health
Framework for the implementation of the Ouagadougou Declaration on Primary Health Care and Health Systems in Africa
 Framework for the implementation of the Ouagadougou Declaration on Primary Health Care and Health Systems in Africa Framework for the implementation of the Ouagadougou Declaration on Primary Health Care
Framework for the implementation of the Ouagadougou Declaration on Primary Health Care and Health Systems in Africa Framework for the implementation of the Ouagadougou Declaration on Primary Health Care
Investment Case for Reproductive, Maternal, Neonatal, Child, Adolescent Health & Nutrition (RMNCAH&N)
") República de Moçambique Ministério da Saúde Investment Case for Reproductive, Maternal, Neonatal, Child, Adolescent Health & Nutrition (RMNCAH&N) GFF IG meeting, November 8, 2017 O Nosso maior valor é
República de Moçambique Ministério da Saúde Investment Case for Reproductive, Maternal, Neonatal, Child, Adolescent Health & Nutrition (RMNCAH&N) GFF IG meeting, November 8, 2017 O Nosso maior valor é
Islamic Republic of Afghanistan. Ministry of Public Health
 Islamic Republic of Afghanistan Ministry of Public Health NATIONAL HEALTH POLICY -2009 AND NATIONAL HEALTH STRATEGY -2006 A policy and strategy to accelerate implementation TABLE OF CONTENTS NATIONAL HEALTH
Islamic Republic of Afghanistan Ministry of Public Health NATIONAL HEALTH POLICY -2009 AND NATIONAL HEALTH STRATEGY -2006 A policy and strategy to accelerate implementation TABLE OF CONTENTS NATIONAL HEALTH
WORLD BREASTFEEDING TRENDS INITIATIVE (WBTi) DATABASE QUESTIONNAIRE
 DATABASE QUESTIONNAIRE") WORLD BREASTFEEDING TRENDS INITIATIVE (WBTi) DATABASE QUESTIONNAIRE Part I (1) Percentage of babies breastfed within one hour of birth (26.3%) (2) Percentage of babies 0
WORLD BREASTFEEDING TRENDS INITIATIVE (WBTi) DATABASE QUESTIONNAIRE Part I (1) Percentage of babies breastfed within one hour of birth (26.3%) (2) Percentage of babies 0
Provisional agenda (annotated)
") EXECUTIVE BOARD EB140/1 (annotated) 140th session 21 November 2016 Geneva, 23 January 1 February 2017 Provisional agenda (annotated) 1. Opening of the session 2. Adoption of the agenda 3. Report by the
EXECUTIVE BOARD EB140/1 (annotated) 140th session 21 November 2016 Geneva, 23 January 1 February 2017 Provisional agenda (annotated) 1. Opening of the session 2. Adoption of the agenda 3. Report by the
Evidence Based Practice: Strengthening Maternal and Newborn Health
 Evidence Based Practice: Strengthening Maternal and Newborn Health Address Mauakowa Malata PhD RNM FAAN Kamuzu College of Nursing International Confederation of Midwives 1 University of Malawi Kamuzu College
Evidence Based Practice: Strengthening Maternal and Newborn Health Address Mauakowa Malata PhD RNM FAAN Kamuzu College of Nursing International Confederation of Midwives 1 University of Malawi Kamuzu College
Lessons Learned. Grant Management
 Lessons Learned Grant Management Introduction NSRP is a five year programme to support the initiatives of Nigerian actors and institutions to manage conflicts non-violently and reduce the impact of violent
Lessons Learned Grant Management Introduction NSRP is a five year programme to support the initiatives of Nigerian actors and institutions to manage conflicts non-violently and reduce the impact of violent
The USAID portfolio in Health, Population and Nutrition (HPN)
") The USAID portfolio in Health, Population and Nutrition (HPN) Goal: Promote and improve health and well-being of Malawians through investing in sustainable, high-impact health initiatives in line with
The USAID portfolio in Health, Population and Nutrition (HPN) Goal: Promote and improve health and well-being of Malawians through investing in sustainable, high-impact health initiatives in line with
Terms of Reference. Consultancy to support the Institutional Strengthening of the Frontier Counties Development Council (FCDC)
") Terms of Reference Consultancy to support the Institutional Strengthening of the Frontier Counties Development Council (FCDC) 1. Introduction August 2016 to August 2018 1. Supporting Kenya s devolution
Terms of Reference Consultancy to support the Institutional Strengthening of the Frontier Counties Development Council (FCDC) 1. Introduction August 2016 to August 2018 1. Supporting Kenya s devolution
Ballia Rural Integrated Child Survival (BRICS) Project World Vision of India Dr. Beulah Jayakumar
 Project World Vision of India Dr. Beulah Jayakumar") Ballia Rural Integrated Child Survival (BRICS) Project World Vision of India Dr. Beulah Jayakumar Email: ballia_india_adp@wvi.org The Ballia Rural Integrated Child Survival (BRICS) Project was implemented
Ballia Rural Integrated Child Survival (BRICS) Project World Vision of India Dr. Beulah Jayakumar Email: ballia_india_adp@wvi.org The Ballia Rural Integrated Child Survival (BRICS) Project was implemented
Health System Analysis for Better. Peter Berman The World Bank Jakarta, Indonesia February 8, 2011 Based on Berman and Bitran forthcoming 2011
 Health System Analysis for Better Health System Strengthening Peter Berman The World Bank Jakarta, Indonesia February 8, 2011 Based on Berman and Bitran forthcoming 2011 Health Systems Analysis: Can be
Health System Analysis for Better Health System Strengthening Peter Berman The World Bank Jakarta, Indonesia February 8, 2011 Based on Berman and Bitran forthcoming 2011 Health Systems Analysis: Can be
National Hygiene Education Policy Guideline
 ISLAMIC REPUBLIC OF AFGHANISTAN Ministry of Rural Rehabilitation & Development And Ministry of Public Health National Hygiene Education Policy Guideline Developed by: Hygiene Education Technical Working
ISLAMIC REPUBLIC OF AFGHANISTAN Ministry of Rural Rehabilitation & Development And Ministry of Public Health National Hygiene Education Policy Guideline Developed by: Hygiene Education Technical Working
Health system strengthening, principles for renewal of primary health care and lessons learned
 Plans for implementation of resolution WHA62.12 on primary health care Progress report from the WHO Regional Office for Europe Health system strengthening, principles for renewal of primary health care
Plans for implementation of resolution WHA62.12 on primary health care Progress report from the WHO Regional Office for Europe Health system strengthening, principles for renewal of primary health care
Somalia Is any part of this project cash based intervention (including vouchers)? Conditionality:
? Conditionality:") Somalia 2018 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives MERCY CORPS (MERCY CORPS) Provision of live saving and sustainable WASH interventions to conflict and
Somalia 2018 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives MERCY CORPS (MERCY CORPS) Provision of live saving and sustainable WASH interventions to conflict and
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region. Community IMCI. Community IMCI
 Implementation in the Western Pacific Region. Community IMCI. Community IMCI") Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Getting it Done for Maternal and Newborn Health. Innovations in Health Systems Strengthening
 The UN Secretary General s Global Strategy for Women s and Children s Health: Getting it Done for Maternal and Newborn Health Innovations in Health Systems Strengthening Pat Riley, CNM, MPH, FACNM Nagesh
The UN Secretary General s Global Strategy for Women s and Children s Health: Getting it Done for Maternal and Newborn Health Innovations in Health Systems Strengthening Pat Riley, CNM, MPH, FACNM Nagesh
Vacancy: Pediatrician Terms of Reference Re-advertisement
 Vacancy: Pediatrician Terms of Reference Re-advertisement I. General Information Position: Pediatrician Beneficiary Institution: Garowe General Hospital Duty Station: Garowe (Puntland State of Somalia)
Vacancy: Pediatrician Terms of Reference Re-advertisement I. General Information Position: Pediatrician Beneficiary Institution: Garowe General Hospital Duty Station: Garowe (Puntland State of Somalia)
A Review on Health Systems in Transition in Myanmar
 A Review on Health Systems in Transition in Myanmar Resources and Services Dr. Nilar Tin Physical and human resources Physical Resources Capital stocks and investment no: of Infrastructure (as of 2013)
A Review on Health Systems in Transition in Myanmar Resources and Services Dr. Nilar Tin Physical and human resources Physical Resources Capital stocks and investment no: of Infrastructure (as of 2013)
A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH
 FAST FACTS THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL STATE OF THE WORLD S MIDWIFERY CHALLENGES The 73 countries
FAST FACTS THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL STATE OF THE WORLD S MIDWIFERY CHALLENGES The 73 countries
TERMS OF REFERENCE FOR INDIVIDUAL CONTRACTORS/ CONSULTANTS/ SSAs
 TERMS OF REFERENCE FOR INDIVIDUAL CONTRACTORS/ CONSULTANTS/ SSAs PART I Title of Assignment To provide support to the evidence based scale up of the 3 feet work across select provinces and linking the
TERMS OF REFERENCE FOR INDIVIDUAL CONTRACTORS/ CONSULTANTS/ SSAs PART I Title of Assignment To provide support to the evidence based scale up of the 3 feet work across select provinces and linking the