HOW TO SUBMIT OWCP-04 BILLS TO ACS
|
|
|
- Hillary Allison
- 6 years ago
- Views:
Transcription
1 HOW TO SUBMIT OWCP-04 BILLS TO ACS The following services should be billed on the OWCP-04 Form: General Hospital Hospice Nursing Home Rehabilitation Centers As a provider you have the option of sending your bills either electronically or by paper. PAPER BILLS SHOULD BE SENT TO: US Department of Labor P O Box 8300 DFEC Central Mailroom London, KY ELECTRONIC BILL SUBMISSION Submitting DOL bills via electronic media offers the advantage of speed in processing. Providers may submit electronic bills or choose a billing agent that offers electronic bill submission services. Billing agents must enroll as DOL providers. The Electronic Data Interchange (EDI) Support Unit assists providers who have questions about electronic bill submission. ACS s EDI Support Unit is available to all providers Monday through Friday from 8:00 a.m. to 8:00 p.m. Eastern Standard Time at EDI Support will: Provide information on available services. Assist in enrolling users for electronic bills submission and report retrieval. Process test transmissions. Provide technical assistance on transmission difficulties
2 AUTHORIZATION REQUIREMENTS The FECA Program pays for medical services rendered for work-related injury or disease. Some services require prior authorization. Listed below are some of the services that require prior authorization: All inpatient admissions Some durable medical equipment Emergency admissions within 48 hours of admission All surgical procedures Some injections Home health services Physical/Occupational therapy services Physical/Occupational therapy authorization requests must be accompanied by a physician s prescription and a treatment plan. Authorization will be given for the number of modalities to be done per day and the number of days requested. Anesthesia CPT codes and Routine services such as office/clinic visits, diagnostic tests and laboratory service do not require prior authorization. Please call (850) , fax (800) using the attached authorization forms, or access our website owcp.dol.acs-inc.com to request an authorization.
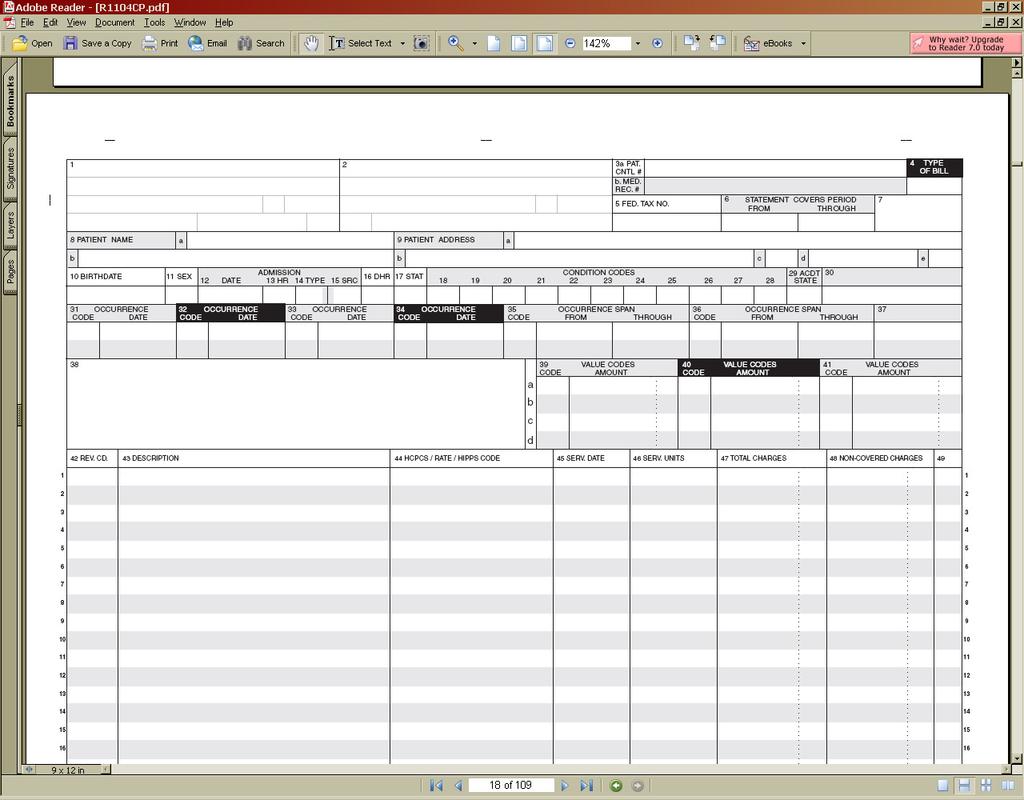
3 BILLING REQUIREMENTS 1. All bills must contain the Federal Employees' Compensation (FECA) 9-digit case number of your patient or client as well as, the 9-digit ACS Provider Number. 2. Laboratory, x-ray, physical therapy, and clinical test such as ECGs, etc. must be identified with the correct CPT code. 3. Facility charges for outpatient surgery billing must be billed using the surgical CPT code. 4. Inpatient bills must include the 9-digit ACS Provider Number in block 51a of the OWCP-04 form. 5. Inpatient bills must include the Medicare number in block 51b of the OWCP-04 form. 6. It is recommended that the NPI number is included in block 56 on the OWCP-04 form. 7. Please refer to the attached OWCP-04 list and the required fields for additional instructions.
4
5 OWCP- 04 CLAIM ITEM TITLE ACTION 1 Provider Name, Address, and Telephone Number 2 Pay-to Name, address, and Secondary Identification Fields 3 a Patient Control Number 3 b Medical/Health Record Number Enter the provider s name and address as well as the telephone number. Required when the pay-to name and address information is different than the Billing Provider information. Enter the claimant's Patient Control Number. (Optional) The number assigned to the patient s medical/health record by the provider. 4 Type of Bill Enter the appropriate three-digit code for the Type of Bill. 5 Federal Tax Number Enter the Federal Tax Number 6 Statement Covers Period Mandatory field. Inpatient: Enter the service dates in MM/DD/YY format. 7 Not Used Reserved 8 Patient s Name Enter the patient s last name, first name, and, if any, middle initial, along with patient ID (if different than the subscriber/insured s ID). 9 Patient s Address Enter the claimant s address. (Optional) 10 Patient s Date of Birth Enter the patient's date of birth in the eight-digit MM/DD/YY format. If full birth date is unknown; indicate zeros for all eight digits. 11 Patient s Sex 12 Admission Date Enter the date the patient was admitted for inpatient care (MMDDYY). 13 Admission Hour 14 Type of Admission/Visit Required on Inpatient bills only. Code Structure: 1 Emergency 2 Urgent 3 Elective 4 Newborn 5 Trauma Center 6-8 Reserved for National Assignment 9 Information Not Available 15 Source of Admission The provider enters the code indicating the source of the referral for this admission or visit. (Optional) 16 Discharge Hour
6 17 Patient Status This code indicates the patient s status as of the Through date of the billing period (FL 6). Outpatient no entry required Patient Status Codes: 01 Discharged to home or self care (routine discharge) 02 Discharged/transferred to another short-term general hospital for inpatient care 03 Discharged/transferred to skilled nursing facility 04 Discharged/transferred to an intermediate care facility 05 Discharged/transferred to another type of institution for inpatient care or referred for outpatient services to another institution 06 Discharged/transferred to home under care of organized home health service organization 07 Left against medical advice or discontinued care Outpatient: No Entry Required Condition Codes No Entry Required 29 Accident State Occurrence Codes and Dates 35 and 36 Occurrence Span Code and Dates Required when there is a condition code that applies to this claim. (Optional) Required For Inpatient. The provider enters codes and associated beginning and ending dates defining a specific event relating to this billing period. Event codes are two alpha-numeric digits and dates are shown numerically as MMDDYY. (Optional) 37 (Untitled) 38 Responsible Party Name and Address Value Codes and Amounts 42 Revenue Code Mandatory Field. Enter the appropriate three-digit revenue code(s) itemizing all services and/or items furnished to the patient in your facility. 43 Revenue Description Enter a narrative description or standard abbreviation for each revenue code included on this bill. 44 HCPCS/Rates/HIPPS Rate Codes 45 Service Date When coding HCPCS for outpatient services, the provider enters the HCPCS code describing the procedure here. On inpatient hospital bills the accommodation rate is shown here. No Entry Required for Inpatient Services. 46 Units of Service Inpatient: Enter the number of units of service and number of days for accommodations. A late discharge may not be billed as an additional day. Outpatient: Enter the units of service for each revenue code.
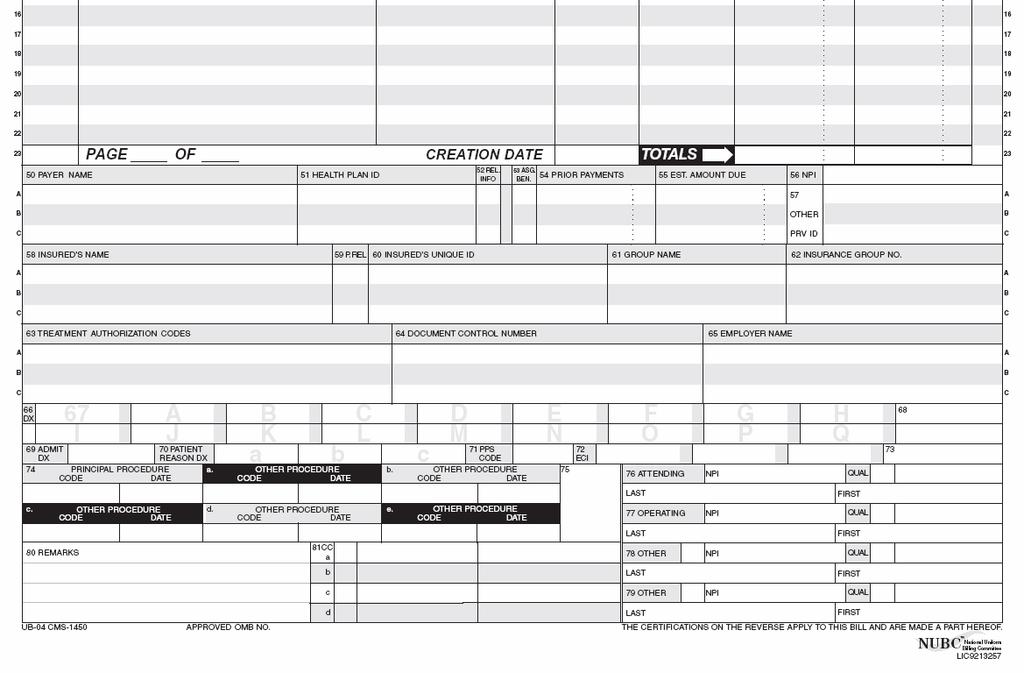
7 47 Total Charges - Not Applicable for Electronic Billers Mandatory Field. Enter the total charge for each revenue code or procedure code entry. This entry must be the sum of the individual charges. Decimal Point required ( ) 48 Noncovered Charges 49 Untitled 50 A, B, C Payer Identification If Medicare is the primary payer, the provider must enter Medicare on line A. Entering Medicare indicates that the provider has developed for other insurance and determined that Medicare is the primary payer. If Medicare is the secondary or tertiary payer, the provider identifies the primary payer on line A and enters Medicare information on line B or C as appropriate. 51 A, B, C Health Plan ID ACS Provider Number is required. Medicare number is required for inpatient services. 52 A, B, C Release of Information Certification Indicator A Y code indicates that the provider has on file a signed statement permitting it to release data to other organizations in order to adjudicate the claim. Required when state or federal laws do not supersede the HIPAA Privacy Rule by requiring that a signature be collected. An I code indicates Informed Consent to Release Medical Information for Conditions or Diagnoses Regulated by Federal Statutes. Required when the provider has not collected a signature and state or federal laws do not supersede the HIPAA Privacy Rule by requiring a signature be collected. 53 A, B, C Assignment of Benefits Certification Indicator 54 A, B, C Prior Payments Situational. For all services other than inpatient hospital or SNF the provider must enter the sum of any amounts collected from the patient toward deductibles (cash and blood) and/or coinsurance on the patient (fourth/last line) of this column. 55 A, B, C Estimated Amount Due From Patient 56 NPI National Provider ID-Recommended for Inpatient Services. 57 Other Provider ID (primary, secondary, and/or tertiary) Situational. Use this field to report other provider identifiers as assigned by a health plan (as indicated in FL50 lines 1-3) prior to May 23, 2007.
8 OWCP- 04 TITLE CLAIM ITEM 58 A, B, C Insured s Name 59 A, B, C Patient s Relationship to Insured 60 A, B, C Insured s Unique ID (Certificate/Social Security Number/HI Claim/Identification Number (HICN)) ACTION Enter the insured s last name first. Mandatory Field. Claimant s 9-digit Claimant ID 61 A, B, C Insurance Group Name 62 A, B, C Insurance Group Number 63 Treatment Authorization Code 64 Document Control Number (DCN) 65 Employer Name 66 Diagnosis and Procedure code Qualifier (ICD Version Indicator) Required. The qualifier that denotes the version of International Classification of Diseases (ICD) reported. 67 Principal Diagnosis Code The hospital enters the ICD code for the principal diagnosis. The code must be the full ICD-9 diagnosis code, including all five digits where applicable. 67A - 67Q Other Diagnoses (Other Than Principal) 68 (Untitled) 69 Admitting Diagnosis Inpatient Required. The hospital enters the full ICD codes for up to eight additional conditions if they co-existed at the time of admission or developed subsequently, and which had an effect upon the treatment or the length of stay. Reserved For inpatient hospital claims the admitting diagnosis is required. 70A 70C Patient s Reason for Visit Situational. Patient s Reason for Visit is required for all un-scheduled outpatient visits for outpatient bills. 71 Prospective Payment System (PPS) Code 72 External Cause of Injury (ECI) Codes 73 Untitled 74 Principal Procedure Code and Date 75 Untitled Situational. Required on inpatient claims when a procedure was performed. Not used on outpatient claims. 76 Attending Provider Name and Identifiers (including NPI) 77 Operating Provider Name and Identifiers (including Required when claim contains any services other than nonscheduled transportation services. Required when a surgical procedure code is listed on this claim.
9 NPI) 78 and 79 Other Provider Name and Identifiers (including NPI) The name and ID number of the individual corresponding to the qualifier category indicated in this section of the claim. 80 Remarks Provider Type Qualifier Codes/Definition/Situational Usage Notes: DN - Referring Provider. The provider who sends the patient to another provider for services. Required on an outpatient claim when the Referring Provider is different than the Attending Physician. If not required, do not send. ZZ - Other Operating Physician. An individual performing a secondary surgical procedure or assisting the Operating Physician. Required when another Operating Physician is involved. If not required, do not send Rendering Provider. The health care professional who delivers or completes a particular medical service or non-surgical procedure. Report when state or federal regulatory requirements call for a combined claim, i.e., a claim that includes both facility and professional fee components (e.g., a Medicaid clinic bill or Critical Access Hospital claim). If not required, do not send. Secondary Identifier Qualifiers: 0B - State License Number 1G - Provider UPIN Number EI - Employer s Identification Number SY - Social Security Number Situational. For DME billings the provider shows the rental rate, cost, and anticipated months of usage so that the provider s FI may determine whether to approve the rental or purchase of the equipment. Where Medicare is not the primary payer because WC, automobile medical, no-fault, liability insurer or an EGHP is primary, the provider enters special annotations. In addition, the provider enters any remarks needed to provide information that is not shown elsewhere on the bill but which is necessary for proper payment. For Renal Dialysis Facilities, the provider enters the first month of the 30-month period during which Medicare benefits are secondary to benefits payable under an EGHP. (See Occurrence Code 33.) 81 Code-Code Field Situational. To report additional codes.
UB-04 Claim Form Instructions
 UB-04 Claim Form This document explains the UB-04 claim form, which is used for submitting claims for reimbursement for specially designated facilities. The instructions included in this section are excerpts
UB-04 Claim Form This document explains the UB-04 claim form, which is used for submitting claims for reimbursement for specially designated facilities. The instructions included in this section are excerpts
Tips for Completing the UB04 (CMS-1450) Claim Form
 Claim Form") Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Subject: Updated UB-04 Paper Claim Form Requirements
 INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 2 J A N U A R Y 3 0, 2 0 0 7 To: All Providers Subject: Updated UB-04 Paper Claim Form Requirements Overview The following
INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 2 J A N U A R Y 3 0, 2 0 0 7 To: All Providers Subject: Updated UB-04 Paper Claim Form Requirements Overview The following
UB-92 Billing Instructions
 August 26, 2005 UB-92 Billing Instructions 2005 Hospital Provider Workshop Conduent MS Medicaid Project Government Healthcare Solutions Objective & Definition To explain how to complete a UB-92 claim form
August 26, 2005 UB-92 Billing Instructions 2005 Hospital Provider Workshop Conduent MS Medicaid Project Government Healthcare Solutions Objective & Definition To explain how to complete a UB-92 claim form
Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims
 Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims Skilled Nursing Facility Services Custodial Care, SLP and Hospice R&B
Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims Skilled Nursing Facility Services Custodial Care, SLP and Hospice R&B
AWCC TABLE OF DATA REQUIREMENTS
 December 1, 2011 Advisory 2011-2 Billing for Provider Services (Rule 30) Effective January 1, 2012, to be considered a properly submitted medical bill, [Rule 30, I, F, 55; I, I, 7], all information submitted
December 1, 2011 Advisory 2011-2 Billing for Provider Services (Rule 30) Effective January 1, 2012, to be considered a properly submitted medical bill, [Rule 30, I, F, 55; I, I, 7], all information submitted
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. Hospital
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim................
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim................
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
North Carolina Emergency Department Visit Data - Data Dictionary FY2012 Alphabetic List of Variables and Attributes Standard Research File
 North Carolina Emergency Department Visit Data - Data Dictionary FY2012 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (diag1, fac, or
North Carolina Emergency Department Visit Data - Data Dictionary FY2012 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (diag1, fac, or
Archived 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION BILLING PROCEDURES FOR MEDICARE/MO HEALTHNET...5
 SECTION 15 - BILLING INSTRUCTIONS Contents 15.1 ELECTRONIC DATA INTERCHANGE...4 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION...4 15.3 UB-04 (CMS-1450) CLAIM FORM...5 15.4 PROVIDER COMMUNICATION UNIT...5 15.5
SECTION 15 - BILLING INSTRUCTIONS Contents 15.1 ELECTRONIC DATA INTERCHANGE...4 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION...4 15.3 UB-04 (CMS-1450) CLAIM FORM...5 15.4 PROVIDER COMMUNICATION UNIT...5 15.5
Tips for Completing the CMS-1500 Version 02/12 Claim Form
 Tips for Completing the CMS-1500 Version 02/12 Claim Form NOTE: FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM. Enter in the white, open carrier
Tips for Completing the CMS-1500 Version 02/12 Claim Form NOTE: FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM. Enter in the white, open carrier
North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File
 North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (Diag1, fac, ptzip)
North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (Diag1, fac, ptzip)
Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) Care Healthcare and VNSNY CHOICE Transition
 Claim Submission Instructions (MLTC) Care Healthcare and VNSNY CHOICE Transition") 2018 Provider Manual VNSNY CHOICE Appendix V Claims CMS-1500 Form (Sample) UB-04 Form (Sample) Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) ICD-10 FAQ Care Healthcare
2018 Provider Manual VNSNY CHOICE Appendix V Claims CMS-1500 Form (Sample) UB-04 Form (Sample) Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) ICD-10 FAQ Care Healthcare
Chapter 12 Section 6
 Home Health Care (HHC) Chapter 12 Section 6 Home Health Benefit Coverage And Reimbursement - Claims And Billing Submission Under Home Health Agency Prospective Payment System (HHA PPS) Issue Date: Authority:
Home Health Care (HHC) Chapter 12 Section 6 Home Health Benefit Coverage And Reimbursement - Claims And Billing Submission Under Home Health Agency Prospective Payment System (HHA PPS) Issue Date: Authority:
Kentucky HIPAA HEALTH CARE CLAIM: INSTITUTIONAL Companion Guide 837
 Kentucky HIPAA HEALTH CARE CLAIM: INSTITUTIONAL Companion 837 Version 1.4 Final RECORD OF CHANGE VERSION NUMBER DATE REVISED DESCRIPTION OF CHANGE PERSONS INVOLVED 1.0 10/25/02 Creation and first view
Kentucky HIPAA HEALTH CARE CLAIM: INSTITUTIONAL Companion 837 Version 1.4 Final RECORD OF CHANGE VERSION NUMBER DATE REVISED DESCRIPTION OF CHANGE PERSONS INVOLVED 1.0 10/25/02 Creation and first view
UPDATED Nursing/Intermediate Care Facility Providers
 December 2008 Provider Bulletin Number 8160 UPDATED Nursing/Intermediate Care Facility Providers Revenue Codes The revenue codes listed under field 42 for the UB-04 form were inadvertently deleted with
December 2008 Provider Bulletin Number 8160 UPDATED Nursing/Intermediate Care Facility Providers Revenue Codes The revenue codes listed under field 42 for the UB-04 form were inadvertently deleted with
Format Specifications For the MHA DMS Publish Date: 11/20/2017
 Specifications For the MHA DMS 10 1.00.10 Publish Date: 11/20/2017 This document is updated periodically. If you are not reading this on the web but are instead reading a printed copy, please check our
Specifications For the MHA DMS 10 1.00.10 Publish Date: 11/20/2017 This document is updated periodically. If you are not reading this on the web but are instead reading a printed copy, please check our
Nursing Facility UB-04 Paper Billing Guide
 Nursing Facility UB-04 Paper Billing Guide Oregon Medicaid Nursing Facilities November 2008 1 Effective 11/17/08 TABLE OF CONTENTS Introduction... 3 Claims Processing General Information... 4 Required
Nursing Facility UB-04 Paper Billing Guide Oregon Medicaid Nursing Facilities November 2008 1 Effective 11/17/08 TABLE OF CONTENTS Introduction... 3 Claims Processing General Information... 4 Required
LifeWise Reference Manual LifeWise Health Plan of Oregon
 11 UB-04 Billing Description This chapter contains participation, claims and billing information for providers who bill on a UB-04 (CMS 1450) claim form. This chapter supplements information contained
11 UB-04 Billing Description This chapter contains participation, claims and billing information for providers who bill on a UB-04 (CMS 1450) claim form. This chapter supplements information contained
CMS-1500 Billing and Reimbursement. HP Provider Relations/October 2013
 CMS-1500 Billing and Reimbursement HP Provider Relations/October 2013 Agenda Common Denials for CMS-1500 CMS-1500 Claims Billing Types of CMS-1500 Claims Paper Claim Billing Fee Schedule Crossover Claims
CMS-1500 Billing and Reimbursement HP Provider Relations/October 2013 Agenda Common Denials for CMS-1500 CMS-1500 Claims Billing Types of CMS-1500 Claims Paper Claim Billing Fee Schedule Crossover Claims
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. Hospital
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim................
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim................
PARTNERSHIP HEALTHPLAN OF CALIFORNIA MEDI-CAL PROVIDER MANUAL CLAIMS DEPARTMENT
 III.A. CMS 1500 Billing Form Effective April 1, 2014, the information listed below are the CMS 1500 fields that must be completed accurately and completely in order to avoid claim suspense or denial. A
III.A. CMS 1500 Billing Form Effective April 1, 2014, the information listed below are the CMS 1500 fields that must be completed accurately and completely in order to avoid claim suspense or denial. A
Version 5010 Errata Provider Handout
 Version 5010 Errata Provider Handout 5010 Bringing Clarity & Consistency To Your Electronic Transactions Benefits Transactions Impacted Changes Impacting Providers While we have highlighted the HIPAA Version
Version 5010 Errata Provider Handout 5010 Bringing Clarity & Consistency To Your Electronic Transactions Benefits Transactions Impacted Changes Impacting Providers While we have highlighted the HIPAA Version
Medicare Hospice Billing 2015 & Beyond!
 Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first
Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first
CareFirst ICD-10 Claim Submission Guidelines
 CareFirst ICD-10 Claim Submission Guidelines Introduction The U.S. Department of Health and Human (HHS) has released a HIPAA administration simplification mandate requiring all HIPAA entities to adopt
CareFirst ICD-10 Claim Submission Guidelines Introduction The U.S. Department of Health and Human (HHS) has released a HIPAA administration simplification mandate requiring all HIPAA entities to adopt
Florida Medicaid. Outpatient Hospital Services Coverage Policy. Agency for Health Care Administration. Draft Rule
 Florida Medicaid Agency for Health Care Administration Draft Rule Table of Contents Florida Medicaid 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions... 1 2.0 Eligible
Florida Medicaid Agency for Health Care Administration Draft Rule Table of Contents Florida Medicaid 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions... 1 2.0 Eligible
FHCA 2014 Annual Conference & Trade Show
 FHCA 2014 Annual Conference & Trade Show CE Session #49 Medicaid Managed Care Billing: Purely A Provider s Perspective Thursday, July 10 4:00 to 6:00 p.m. Crystal N/J2 Finance/Development Upon completion
FHCA 2014 Annual Conference & Trade Show CE Session #49 Medicaid Managed Care Billing: Purely A Provider s Perspective Thursday, July 10 4:00 to 6:00 p.m. Crystal N/J2 Finance/Development Upon completion
Place of Service Code Description Conversion
 Place of Conversion CMS Place of Code Place of Name The place of service field indicates where the services were performed Possible values include: Code Description Inpatient Outpatient Office Home 5 Independent
Place of Conversion CMS Place of Code Place of Name The place of service field indicates where the services were performed Possible values include: Code Description Inpatient Outpatient Office Home 5 Independent
A Revenue Cycle Process Approach
 A Revenue Cycle Process Approach VALERIUS BAYES NEWBY Education BLOCHOWIAK Preface x Parti Chapter1 WORKING WITH MEDICAL INSURANCE AND BILLING Chapter 3 Introduction to the Revenue Cycle 2 1.1 Working
A Revenue Cycle Process Approach VALERIUS BAYES NEWBY Education BLOCHOWIAK Preface x Parti Chapter1 WORKING WITH MEDICAL INSURANCE AND BILLING Chapter 3 Introduction to the Revenue Cycle 2 1.1 Working
Rural Health Clinic Overview
 TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
Place of Service Codes (POS) and Definitions
 and Definitions") 2950 Robertson Ave, Suite 200 Cincinnati, OH 45209 (P): 513-281-4400 www.medicalreimbursementinc.com www.linkedin.com/company/medical-reimbursement-inc www.twitter.com/medreimburse www.facebook.com/medicalreimbursementinc
2950 Robertson Ave, Suite 200 Cincinnati, OH 45209 (P): 513-281-4400 www.medicalreimbursementinc.com www.linkedin.com/company/medical-reimbursement-inc www.twitter.com/medreimburse www.facebook.com/medicalreimbursementinc
Choice PPO Retired Employees Health Program Non-Medicare Eligible Retired Members
 Choice PPO Retired Employees Health Program Non-Medicare Eligible Retired Members DEDUCTIBLE (per calendar year) Annual in-network deductible must be paid first for the following services: Imaging, hospital
Choice PPO Retired Employees Health Program Non-Medicare Eligible Retired Members DEDUCTIBLE (per calendar year) Annual in-network deductible must be paid first for the following services: Imaging, hospital
Summary of benefits Health Net. seniority plus green. Benefits effective January 1, 2009 H0562 Medicare Advantage HMO
 2009 Health Net Summary of benefits Los Angeles, Orange, Riverside and San Bernardino counties s effective January 1, 2009 H0562 Medicare Advantage HMO Material ID H0562-09-0041 CMS Approval 9/08 Section
2009 Health Net Summary of benefits Los Angeles, Orange, Riverside and San Bernardino counties s effective January 1, 2009 H0562 Medicare Advantage HMO Material ID H0562-09-0041 CMS Approval 9/08 Section
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. Hospital
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim..................
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim..................
Administrative Billing Data
 Administrative Billing Data Patient Identification and Demographic Information: From UB-04 Data or Medical Record Face Sheet. Note: When you go to enter data on this case, the information below will already
Administrative Billing Data Patient Identification and Demographic Information: From UB-04 Data or Medical Record Face Sheet. Note: When you go to enter data on this case, the information below will already
Policies Regarding Network Provider Payment
 CLAIMS PAYMENT (NOTE: Below please find guidelines ValueOptions follows when processing claims for most accounts. If you believe there may be a specific set of guidelines that need to be followed for your
CLAIMS PAYMENT (NOTE: Below please find guidelines ValueOptions follows when processing claims for most accounts. If you believe there may be a specific set of guidelines that need to be followed for your
FBLP will include all provider types for the provider look-up with the exception of provider type 53, non-medical vendors from the search.
 Dear Provider: Thank you for your interest in participating as a provider of medical services for programs administered by the U.S. Department of Labor s Office of Workers Compensation Compensation Programs
Dear Provider: Thank you for your interest in participating as a provider of medical services for programs administered by the U.S. Department of Labor s Office of Workers Compensation Compensation Programs
US Department of Labor OWCP/FECA P.O. Box 8300 London, KY DEEOIC P.O. Box 8304 London, KY
 Dear Provider: Thank you for your interest in participating as a provider of medical services for programs administered by the U.S. Department of Labor s Office of Workers Compensation Programs (OWCP).
Dear Provider: Thank you for your interest in participating as a provider of medical services for programs administered by the U.S. Department of Labor s Office of Workers Compensation Programs (OWCP).
All but Part A Deductible. Medicare Part A Deductible. Nothing. Inpatient Hospital All but Part A Medicare Part A Nothing.
 Summary of Signature 65 Benefits Signature 65 is a Medicare-complimentary benefit program that fills in the coverage gaps and cost sharing of the traditional Medicare program (Medicare Part A and ). In
Summary of Signature 65 Benefits Signature 65 is a Medicare-complimentary benefit program that fills in the coverage gaps and cost sharing of the traditional Medicare program (Medicare Part A and ). In
Chapter 13 Section 2. Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups
 Groups") Outpatient Prospective Payment System (OPPS)-Ambulatory Payment Classification (APC) Chapter 13 Section 2 Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups Issue Date:
Outpatient Prospective Payment System (OPPS)-Ambulatory Payment Classification (APC) Chapter 13 Section 2 Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups Issue Date:
AMBULATORY SURGICAL CENTERS PROVIDER MANUAL Chapter Twenty-nine of the Medicaid Services Manual
 AMBULATORY SURGICAL CENTERS PROVIDER MANUAL Chapter Twenty-nine of the Medicaid Services Manual Issued November 1, 2010 Claims/authorizations for dates of service on or after October 1, 2015 must use the
AMBULATORY SURGICAL CENTERS PROVIDER MANUAL Chapter Twenty-nine of the Medicaid Services Manual Issued November 1, 2010 Claims/authorizations for dates of service on or after October 1, 2015 must use the
MEDICAL POLICY No R2 TELEMEDICINE
 Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims
 Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims Transmittals for Chapter 11 Table of Contents (Rev. 3326, 08-14-15) (Rev. 3378, 10-16-15) 10 - Overview 10.1 - Hospice Pre-Election
Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims Transmittals for Chapter 11 Table of Contents (Rev. 3326, 08-14-15) (Rev. 3378, 10-16-15) 10 - Overview 10.1 - Hospice Pre-Election
(a) The provider's submitted charge; or
 The provider's submitted charge; or") ACTION: Final DATE: 12/20/2013 11:35 AM 5101:3-1-60 Medicaid reimbursement. (A) The medicaid payment for a covered service constitutes payment in full and may not be construed as a partial payment when
ACTION: Final DATE: 12/20/2013 11:35 AM 5101:3-1-60 Medicaid reimbursement. (A) The medicaid payment for a covered service constitutes payment in full and may not be construed as a partial payment when
Screening, Brief Intervention and Referral to Treatment (SBIRT) Program
 Program") Screening, Brief Intervention and Referral to Treatment (SBIRT) Program (SBIRT) Services... 1 Program Overview... 1 Billing Information... 1 National Provider Identifier (NPI)... 1 Paper Claims... 1 Electronic
Screening, Brief Intervention and Referral to Treatment (SBIRT) Program (SBIRT) Services... 1 Program Overview... 1 Billing Information... 1 National Provider Identifier (NPI)... 1 Paper Claims... 1 Electronic
North Carolina Inpatient Hospital Discharge Data - Data Dictionary FY2011 Standard Research File Alphabetic List of Variables and Attributes
 North Carolina Inpatient Hospital Discharge Data - Data Dictionary FY2011 Standard Research File Alphabetic List of Variables and Attributes One of these three variables must be suppressed (diag1, fac,
North Carolina Inpatient Hospital Discharge Data - Data Dictionary FY2011 Standard Research File Alphabetic List of Variables and Attributes One of these three variables must be suppressed (diag1, fac,
Summary of Benefits Advantra Freedom PEBTF
 Advantra Freedom is a Medicare Advantage Private Fee-For-Service (PFFS) Plan. This Summary of Benefits tells you some features of our Plan. It doesn't list every service that we cover or list every limitation
Advantra Freedom is a Medicare Advantage Private Fee-For-Service (PFFS) Plan. This Summary of Benefits tells you some features of our Plan. It doesn't list every service that we cover or list every limitation
PHYSICIAN S RECOMMENDATION FOR PEDIATRIC CARE INSTRUCTIONS FOR COMPLETING THE PEDIATRIC CARE FORM DMA-6(A)
") PHYSICIAN S RECOMMENDATION FOR PEDIATRIC CARE INSTRUCTIONS FOR COMPLETING THE PEDIATRIC CARE FORM DMA-6(A) This section provides detailed instructions for completion of the Form DMA-6 (A). Before payment
PHYSICIAN S RECOMMENDATION FOR PEDIATRIC CARE INSTRUCTIONS FOR COMPLETING THE PEDIATRIC CARE FORM DMA-6(A) This section provides detailed instructions for completion of the Form DMA-6 (A). Before payment
Summary of Benefits. New York: Bronx, Kings, New York, Queens and Richmond Counties
 Summary of Benefits New York: Bronx, Kings, New York, Queens and Richmond Counties January 1, 2006 - December 31, 2006 You ve earned the right to live life on your own terms. And that includes the right
Summary of Benefits New York: Bronx, Kings, New York, Queens and Richmond Counties January 1, 2006 - December 31, 2006 You ve earned the right to live life on your own terms. And that includes the right
Chapter 11 Section 4. Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
 Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
Standardized Prior Authorization Form Instructions
 Standardized Prior Authorization Form Instructions The Standardized one-page Prior Authorization Request Form is to be used by all NH Medicaid Fee for Service (FFS) and Managed Care Organization (MCO)
Standardized Prior Authorization Form Instructions The Standardized one-page Prior Authorization Request Form is to be used by all NH Medicaid Fee for Service (FFS) and Managed Care Organization (MCO)
INPATIENT/COMPREHENSIVE REHAB AUDIT DICTIONARY
 Revised 11/04/2016 Audit # Location Audit Message Audit Description Audit Severity 784 DATE Audits are current as of 11/04/2016 The date of the last audit update Information 1 COUNTS Total Records Submitted
Revised 11/04/2016 Audit # Location Audit Message Audit Description Audit Severity 784 DATE Audits are current as of 11/04/2016 The date of the last audit update Information 1 COUNTS Total Records Submitted
Chapter 11 Section 4. Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
 Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: C-6, October 20, 2017 1.0 APPLICABILITY
Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: C-6, October 20, 2017 1.0 APPLICABILITY
Provider Handbooks. Telecommunication Services Handbook
 Provider Handbooks December 2016 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid under contract with the Texas Health
Provider Handbooks December 2016 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid under contract with the Texas Health
Reimbursement for Anticoagulation Services
 Journal of Thrombosis and Thrombolysis 12(1), 73 79, 2001. # 2002 Kluwer Academic Publishers, Manufactured in The Netherlands. Reimbursement for Anticoagulation Services Paul W. Radensky McDermott, Will
Journal of Thrombosis and Thrombolysis 12(1), 73 79, 2001. # 2002 Kluwer Academic Publishers, Manufactured in The Netherlands. Reimbursement for Anticoagulation Services Paul W. Radensky McDermott, Will
Reimbursement Policy. Subject: Consultations. Committee Approval Obtained: Section: Evaluation and 07/01/17. Effective Date:
 Subject: Consultations https://providers.amerigroup.com Reimbursement Policy Effective Date: Committee Approval Obtained: Section: Evaluation and 07/01/17 06/06/16 Management *****The most current version
Subject: Consultations https://providers.amerigroup.com Reimbursement Policy Effective Date: Committee Approval Obtained: Section: Evaluation and 07/01/17 06/06/16 Management *****The most current version
Provider Portal Hints & Tips Frequently Asked Questions
 Provider Portal Hints & Tips Frequently Asked Questions 1 Medical Review-Claim Appeal Hints & Tips Claim Appeals The Dean Health Plan Medical Affairs Department reviews the claim and associated medical
Provider Portal Hints & Tips Frequently Asked Questions 1 Medical Review-Claim Appeal Hints & Tips Claim Appeals The Dean Health Plan Medical Affairs Department reviews the claim and associated medical
Super Blue Plus 2000 WVHTC High Option-B (Non-Grandfathered) $200 Deductible
 $200 Deductible") BENEFIT HIGHLIGHTS 1 Super Blue Plus 2000 WVHTC High Option-B (Non-Grandfathered) $200 Group Effective Date December 1, 2017 Benefit Period (used for and Coinsurance limits) January 1 through December
BENEFIT HIGHLIGHTS 1 Super Blue Plus 2000 WVHTC High Option-B (Non-Grandfathered) $200 Group Effective Date December 1, 2017 Benefit Period (used for and Coinsurance limits) January 1 through December
AMBULANCE SERVICES. Guideline Number: CS003.F Effective Date: January 1, 2018
 AMBULANCE SERVICES UnitedHealthcare Community Plan Coverage Determination Guideline Guideline Number: CS003.F Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
AMBULANCE SERVICES UnitedHealthcare Community Plan Coverage Determination Guideline Guideline Number: CS003.F Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 BENEFIT CONSIDERATIONS...
Objectives. Observation: Exploring the MOON and Charge Capture. Aurora Health Care 10/11/2016
 Observation: Exploring the MOON and Charge Capture Lynn Sisler, Senior Director Case Management Manpreet Lehn, Manager Revenue Assurance Objectives Understand the CMS requirements for the Medicare Outpatient
Observation: Exploring the MOON and Charge Capture Lynn Sisler, Senior Director Case Management Manpreet Lehn, Manager Revenue Assurance Objectives Understand the CMS requirements for the Medicare Outpatient
CLASSIC BLUE SECURE/BLUE CROSS BLUE SHIELD COMPLEMENTARY Monroe County Benefit Summary/Comparison (Over 65 Retirees)
") WHO IS COVERED Enrollment Requirement Members must be enrolled in both Medicare Parts A and B Members must be enrolled in both Medicare Parts A and B Type of Tier Single only Single only Dependent/Student
WHO IS COVERED Enrollment Requirement Members must be enrolled in both Medicare Parts A and B Members must be enrolled in both Medicare Parts A and B Type of Tier Single only Single only Dependent/Student
EFFECTIVE 4/1/ Texas Administrative Code Chapter GENERAL MEDICAL PROVISIONS
 28 Texas Administrative Code Chapter 133 - GENERAL MEDICAL PROVISIONS Subchapter B - HEALTH CARE PROVIDER BILLING PROCEDURES AMENDED: 133.10 Adopted: 12/16/2013 Effective: 4/1/2014 Adoption: http://texashistory.unt.edu/ark:/67531/metapth379970/m1/186/?q=133.10
28 Texas Administrative Code Chapter 133 - GENERAL MEDICAL PROVISIONS Subchapter B - HEALTH CARE PROVIDER BILLING PROCEDURES AMENDED: 133.10 Adopted: 12/16/2013 Effective: 4/1/2014 Adoption: http://texashistory.unt.edu/ark:/67531/metapth379970/m1/186/?q=133.10
Healthcare Eligibility Benefit Inquiry and Response. 270/ Companion Guide
 Healthcare Eligibility Benefit Inquiry and Response 270/271 5010 Companion Guide Table of Contents Purpose...1 Contact Information...1 Preparation and Testing Requirements...1 System Availability...2 Batch
Healthcare Eligibility Benefit Inquiry and Response 270/271 5010 Companion Guide Table of Contents Purpose...1 Contact Information...1 Preparation and Testing Requirements...1 System Availability...2 Batch
Chapter 02 Hospital Based Care
 Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
INPATIENT HOSPITAL REIMBURSEMENT
 HCRA CLAIMS PROCESSING Reimbursement: HCRA is not Medicaid; however, HCRA covered services are reimbursed at the hospital s outpatient or inpatient reimbursement rate allowed for Florida Medicaid. The
HCRA CLAIMS PROCESSING Reimbursement: HCRA is not Medicaid; however, HCRA covered services are reimbursed at the hospital s outpatient or inpatient reimbursement rate allowed for Florida Medicaid. The
Reimbursement Policy. Subject: Consultations Effective Date: 05/01/05
 Reimbursement Policy Subject: Consultations Effective Date: 05/01/05 Committee Approval Obtained: 06/06/16 Section: Evaluation and Management *****The most current version of the Reimbursement Policies
Reimbursement Policy Subject: Consultations Effective Date: 05/01/05 Committee Approval Obtained: 06/06/16 Section: Evaluation and Management *****The most current version of the Reimbursement Policies
Care Management. Billing March 2017
 Care Management Title Billing March 2017 Subtitle The information contained herein is the proprietary information of BCBSM. Any use or disclosure of such information without the prior written consent of
Care Management Title Billing March 2017 Subtitle The information contained herein is the proprietary information of BCBSM. Any use or disclosure of such information without the prior written consent of
Connecticut interchange MMIS
 Connecticut interchange MMIS Provider Manual Chapter 8 Hospital Claim Submission Instructions Connecticut Department of Social Services (DSS) 55 Farmington Avenue Hartford, CT 06105 HP Enterprise Services
Connecticut interchange MMIS Provider Manual Chapter 8 Hospital Claim Submission Instructions Connecticut Department of Social Services (DSS) 55 Farmington Avenue Hartford, CT 06105 HP Enterprise Services
NJDDCS VERSION 2 DATA DICTIONARY And DATA EXTRACT FILE LAYOUT Version 17.2
 NJDDCS VERSION 2 DATA DICTIONARY And DATA EXTRACT FILE LAYOUT Version 17.2 Table of Contents Introduction... 5 Accident State... 6 Acute Days... 7 Admission Hour... 8 Admission/Start of Care Date (Admission
NJDDCS VERSION 2 DATA DICTIONARY And DATA EXTRACT FILE LAYOUT Version 17.2 Table of Contents Introduction... 5 Accident State... 6 Acute Days... 7 Admission Hour... 8 Admission/Start of Care Date (Admission
Welcome to Kaiser Permanente: NAME (Please Print):
:") Welcome to Kaiser Permanente: NAME (Please Print): You have made a great choice for your health! We value each and every member and aim to make your transition from your prior insurance company to Kaiser
Welcome to Kaiser Permanente: NAME (Please Print): You have made a great choice for your health! We value each and every member and aim to make your transition from your prior insurance company to Kaiser
SmartSaver. A Medicare Advantage Medical Savings Account Plan. Summary of Benefits and Other-Value Added Services. From Blue Cross of California
 SmartSaver From Blue Cross of California A Medicare Advantage Medical Savings Account Plan Service Area C Summary of Benefits and Other-Value Added Services H5769 2007 CO 415 09/22/06 Introduction to the
SmartSaver From Blue Cross of California A Medicare Advantage Medical Savings Account Plan Service Area C Summary of Benefits and Other-Value Added Services H5769 2007 CO 415 09/22/06 Introduction to the
SUMMARY OF BENEFITS 2009
 HEALTH NET VIOLET OPTION 1, HEALTH NET VIOLET OPTION 2, HEALTH NET SAGE, AND HEALTH NET AQUA SUMMARY OF BENEFITS 2009 Southern Oregon Douglas, Jackson, and Josephine Counties, Oregon Benefits effective
HEALTH NET VIOLET OPTION 1, HEALTH NET VIOLET OPTION 2, HEALTH NET SAGE, AND HEALTH NET AQUA SUMMARY OF BENEFITS 2009 Southern Oregon Douglas, Jackson, and Josephine Counties, Oregon Benefits effective
Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications
 Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications Complete and correct coding of claims will become more important, and will have an effect on claim payment. The
Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications Complete and correct coding of claims will become more important, and will have an effect on claim payment. The
Pulmonary Intake Form
 Pulmonary Intake Form Name DOB Date Please list the referring physician or other physicians that you would like this office visit to be shared with. Pharmacy Name, Location, and Phone Number Reason for
Pulmonary Intake Form Name DOB Date Please list the referring physician or other physicians that you would like this office visit to be shared with. Pharmacy Name, Location, and Phone Number Reason for
HEALTH INFORMATION TECHNOLOGY (HIT) COURSES
 COURSES") HEALTH INFORMATION TECHNOLOGY (HIT) COURSES HIT 110 - Medical Terminology This course is an introduction to the language of medicine. Course emphasis is on terminology related to disease and treatment
HEALTH INFORMATION TECHNOLOGY (HIT) COURSES HIT 110 - Medical Terminology This course is an introduction to the language of medicine. Course emphasis is on terminology related to disease and treatment
COMPLIANCE MONITORING CHECKLIST
 HOSPITAL COMPLIANCE MONITORING CHECKLIST Return To: Year Ending: December 31, 2005 Email: Affiliate: Person Completing: Fax: All "No" answers should include an explanation in the General Comments column.
HOSPITAL COMPLIANCE MONITORING CHECKLIST Return To: Year Ending: December 31, 2005 Email: Affiliate: Person Completing: Fax: All "No" answers should include an explanation in the General Comments column.
Federal Employee Program Service Benefit Plan An independent licensee of the Blue Cross and Blue Shield Association
 Federal Employee Program Service Benefit Plan 2009 An independent licensee of the Blue Cross and Blue Shield Association Federal Employee Program Two PPO Products Basic Option with (in-network benefits
Federal Employee Program Service Benefit Plan 2009 An independent licensee of the Blue Cross and Blue Shield Association Federal Employee Program Two PPO Products Basic Option with (in-network benefits
MEDICARE. 32 nd Annual Open Season Seminar
 MEDICARE 32 nd Annual Open Season Seminar What is Medicare and who is eligible? Federal Health Insurance Program for aged and disabled o Over age 65 o Disabled workers o Patients with End Stage Renal Disease
MEDICARE 32 nd Annual Open Season Seminar What is Medicare and who is eligible? Federal Health Insurance Program for aged and disabled o Over age 65 o Disabled workers o Patients with End Stage Renal Disease
Inpatient Psychiatric Facility (IPF) Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016
 Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016") Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Medicare Plus Blue SM Group PPO
 2018 Medicare Plus Blue SM Group PPO Evidence of Coverage Your Medicare Health Benefits and Services as a Member of Medicare Plus Blue SM Group PPO This booklet gives you the details about your Medicare
2018 Medicare Plus Blue SM Group PPO Evidence of Coverage Your Medicare Health Benefits and Services as a Member of Medicare Plus Blue SM Group PPO This booklet gives you the details about your Medicare
Therapies (e.g., physical, occupational and speech) Medical social worker (MSW) 3328ALL0118-F 1
 Medical social worker (MSW) 3328ALL0118-F 1") 1. Q: Why is Humana implementing this utilization management (UM) program? A: Humana is implementing this program to help coordinate home health care for its Medicare Advantage members in Oklahoma and
1. Q: Why is Humana implementing this utilization management (UM) program? A: Humana is implementing this program to help coordinate home health care for its Medicare Advantage members in Oklahoma and
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Texas Medicaid. Provider Procedures Manual. Provider Handbooks. Telecommunication Services Handbook
 Texas Medicaid Provider Procedures Manual Provider Handbooks December 2017 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid
Texas Medicaid Provider Procedures Manual Provider Handbooks December 2017 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL
 TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
Medicare 101. Lisa Satterfield, ASHA director, health care regulatory advocacy Neela Swanson, ASHA director, health care coding policy
 Medicare 101 Lisa Satterfield, ASHA director, health care regulatory advocacy Neela Swanson, ASHA director, health care coding policy Neela Swanson Director, Health Care Coding Policy, ASHA Disclosure
Medicare 101 Lisa Satterfield, ASHA director, health care regulatory advocacy Neela Swanson, ASHA director, health care coding policy Neela Swanson Director, Health Care Coding Policy, ASHA Disclosure
CHAPTER 59B-9 PATIENT DATA COLLECTION, AMBULATORY SURGERY AND EMERGENCY DEPARTMENT
 CHAPTER 59B-9 PATIENT DATA COLLECTION, AMBULATORY SURGERY AND EMERGENCY DEPARTMENT 59B-9.030 59B-9.031 59B-9.032 59B-9.033 59B-9.034 59B-9.035 59B-9.036 59B-9.037 59B-9.038 59B-9.039 Purpose of Ambulatory
CHAPTER 59B-9 PATIENT DATA COLLECTION, AMBULATORY SURGERY AND EMERGENCY DEPARTMENT 59B-9.030 59B-9.031 59B-9.032 59B-9.033 59B-9.034 59B-9.035 59B-9.036 59B-9.037 59B-9.038 59B-9.039 Purpose of Ambulatory
Amarillo Endoscopy Center Srinivas Pathapati, MD., PA 6833 Plum Creek Drive Amarillo, TX (806)
") Today s Date: / / PATIENT INFORMATION Patient s Last Name First Middle Mr. Miss Mrs. Ms. Marital Status (Circle one) Single / Mar / Div / Sep / Widow Legal Name (If applicable) Maiden Name Birth Date Age
Today s Date: / / PATIENT INFORMATION Patient s Last Name First Middle Mr. Miss Mrs. Ms. Marital Status (Circle one) Single / Mar / Div / Sep / Widow Legal Name (If applicable) Maiden Name Birth Date Age
Evidence of Coverage:
 January 1 December 31, 2013 Evidence of Coverage: Your Medicare Health Benefits and Services as a Member of Health Net Aqua (PPO) This booklet gives you the details about your Medicare health care coverage
January 1 December 31, 2013 Evidence of Coverage: Your Medicare Health Benefits and Services as a Member of Health Net Aqua (PPO) This booklet gives you the details about your Medicare health care coverage
ATTENTION PROVIDERS. Billing & Reimbursement Requirements for Observation Services
 EqualityCareNews November 2005 ATTENTION PROVIDERS Provider Bulletin 05-005 Billing & Reimbursement Requirements for Observation Services Effective October 1, 2005, under Outpatient Prospective Payment
EqualityCareNews November 2005 ATTENTION PROVIDERS Provider Bulletin 05-005 Billing & Reimbursement Requirements for Observation Services Effective October 1, 2005, under Outpatient Prospective Payment
Chapter 9 Section 1. Ambulatory Surgical Center (ASC) Reimbursement
 Reimbursement") Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Telemedicine and Telehealth Services
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Telemedicine and Telehealth Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 8 P U B L I S H E D : J A N U A R Y 1
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Telemedicine and Telehealth Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 8 P U B L I S H E D : J A N U A R Y 1
MEDICAL POLICY No R1 TELEMEDICINE
 Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
SCHEDULE OF MEDICAL BENEFITS
 Annual Deductibles Annual Out-of-Pocket Maximums Inpatient Hospital Copayment (Excludes Deductible) $250 Individual $1,000 Individual $100 per day, not to exceed $500 Family $2,000 Family $600 per admission
Annual Deductibles Annual Out-of-Pocket Maximums Inpatient Hospital Copayment (Excludes Deductible) $250 Individual $1,000 Individual $100 per day, not to exceed $500 Family $2,000 Family $600 per admission
Best Practice Recommendation for
 Best Practice Recommendation for Submitting & Processing Claims (5010 version) WorkSMART A program of the Washington Healthcare Forum operated by OneHealthPort 1 For use with ASC X12N 837 (005010X222)
Best Practice Recommendation for Submitting & Processing Claims (5010 version) WorkSMART A program of the Washington Healthcare Forum operated by OneHealthPort 1 For use with ASC X12N 837 (005010X222)
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
04/03/03 Health Care Claim: Institutional - 837
 837 Health Care Claim: Institutional Companion Guide LA Medicaid HIPAA/V4010X096A1/837: 837 Health Care Claim: Institutional Version: 1.3 Update 06/08/04 Author: Publication: EDI Department LA Medicaid
837 Health Care Claim: Institutional Companion Guide LA Medicaid HIPAA/V4010X096A1/837: 837 Health Care Claim: Institutional Version: 1.3 Update 06/08/04 Author: Publication: EDI Department LA Medicaid
Chapter 11 Section 4. Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care
 Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy
Hospice Chapter 11 Section 4 Hospice Reimbursement - Guidelines For Payment Of Designated Levels Of Care Issue Date: February 6, 1995 Authority: 32 CFR 199.14(g) Revision: 1.0 APPLICABILITY This policy