KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. Hospital
|
|
|
- Nicholas Harmon
- 6 years ago
- Views:
Transcription
1 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital
2 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions Submission of Claim MS-2126 Billing Instructions Hospital Specific Billing Information State Institution for Mental Health Billing Instructions BENEFITS AND LIMITATIONS 8100 Copayment Medical Assessment Benefit Plans Medicaid Medicaid-Inpatient Only Medicaid-Outpatient Only Family Planning/Sterilization HCPCS Procedure Codes and Nomenclature Ambulatory Surgery/Outpatient Surgery - Procedure Codes and Nomenclature DME/Medical Supplies in a Swing Bed NF Hospital Cost Report Appendix I Appendix II Appendix III Appendix IV FORMS SECTION DRG RATES AND WEIGHTS
3 PART II This is the provider specific section of the manual. This section (Part II) was designed to provide information and instructions specific to hospital providers. It is divided into three subsections: Billing Instructions, Benefits and Limitations, and Appendices. The Billing Instructions subsection gives examples of the billing forms applicable to hospital services. The forms are followed by directions for completing and submitting them. The Benefits and Limitations subsection defines specific aspects of the scope of hospital services allowed within the Kansas Medical Assistance Program (KMAP). The Appendix subsection contains information concerning procedure codes, emergency diagnosis codes and swing bed nursing facility supplies. The appendices were developed to make finding and using codes easier for the biller. HIPAA Compliance As a KMAP participant, providers are required to comply with compliance reviews and complaint investigations conducted by the Secretary of the Department of Health and Human Services as part of the Health Insurance Portability and Accountability Act (HIPAA) in accordance with section 45 of the code of regulations parts 160 and 164. Providers are required to furnish the Department of Health and Human Services all information required by the Department during its review and investigation. The provider is required to provide the same forms of access to records to the Medicaid Fraud and Abuse Division of the Kansas Attorney General's Office upon request from such office as required by K.S.A and amendments thereto. A provider who receives such a request for access to or inspection of documents and records must promptly and reasonably comply with access to the records and facility at reasonable times and places. A provider must not obstruct any audit, review or investigation, including the relevant questioning of employees of the provider. The provider shall not charge a fee for retrieving and copying documents and records related to compliance reviews and complaint investigations.
4 7000. HOSPITAL BILLING INSTRUCTIONS Updated 03/08 Introduction to the UB-04 Claim Form Hospital providers must use the UB-04 red claim form when requesting payment for medical services and supplies provided under the Kansas Medical Assistance Program. Any UB-04 claim not submitted on the red claim from will be returned to the provider. An example of the UB-04 claim form is in the Forms section at the end of this manual. Instructions for completing this claim form are included in the following pages. The Kansas MMIS will be using electronic imaging and optical character recognition (OCR) equipment. Therefore, information will not be recognized if not submitted in the correct fields as instructed. EDS does not furnish the UB-04 claim form to providers. Refer to Section The following numbered form locators (FL) are to be completed when required or if applicable. Completing the UB-04 Claim Form: FL 1 FL 3A FL 3B FL 4 Required. Enter the name and address of the billing provider. Patient Control No. Enter a patient account number if desired. (This number will be referenced on the Remittance Advice [RA].) Medical Record No.-Desired. Enter the patient s medical record number. (This number will appear on the provider s RA.) Type of Bill - Required. Enter the 3-digit number specific to the type of claim. 1st digit indicates facility. (Always a "1".) 2nd digit indicates location within facility. 3rd digit indicates the frequency of the claim billed. Medicaid allowed codes: 1st digit: 1 Hospital (IP/OP) 8 Outpatient Critical Access 2nd digit: 1 Inpatient 3 Outpatient 5 Critical Access Hospital 8 Swing bed NF 3rd digit: 0 Nonpayment/zero claim 1 Admit through discharge claim 2 Interim - first claim 3 Interim - continuing claim 4 Interim - last claim (thru date is discharge date) BILLING INSTRUCTIONS 7-1
5 7000. Updated 5/07 FL 6 FL 7 FL 8 FL 12 8B FL FL FL FL FL FL Statement Covers Period - From/Through - Required. Enter inpatient dates of admission and discharge or outpatient from and through dates in MM/DD/YY format. Covered Days - Required - Inpatient Only. Enter the number of days for which you are billing. NOTE: Count date of admission, but not date of discharge. Non-Covered Days - Required - Enter the total number of non-covered days. Patient Name - Required - Enter patient's last name, first name and middle initial exactly as it appears on the ID card. If patient is a newborn, enter "newborn", "baby boy", or "baby girl" in the first name field and enter the last name. Birthdate - Required. Enter patient's date of birth in MM/DD/YYYY format. If newborn, enter baby's date of birth (not mother's). Sex - Required. Enter "M" for male or "F" for female. If newborn services, enter "M" or "F" for the baby. Admission Date - Required. Enter date patient was admitted as inpatient or date of outpatient care in MM/DD/YY format. Admission Hour - Required - Inpatient Only. Enter treatment hour using the continental time system (i.e., 6:00 p.m. = 1800 hours). Admission Type - Required - Inpatient Only. Enter a one-digit code to indicate type of admission. 1 Emergency 3 Elective 2 Urgent, etc. 4 Newborn 5 Trauma Admission Source - Required - Enter a one digit code to indicate admission source. 4 - Transfer from Hospital 5 - Transfer from Nursing Home 6 - Transfer from Another Facility BILLING INSTRUCTIONS 7-2
6 7000. Updated 03/08 FL 17 Patient Status - Required - Inpatient Only. Enter a two-digit code to indicate status of patient: 01 Discharged to home or self care (routine discharge). 02 Discharged/transferred to another short-term general hospital for inpatient care. 03 Discharged/transferred to skilled nursing facility (SNF) with Medicare certification. 04 Discharged/transferred to an Intermediate Care Facility (ICF). 05 Discharge/transfer to a designated cancer center or children s hospital. Discharged/transferred to a non-medicare PPS children s hospital or non-medicare PPS cancer hospital for inpatient care. 06 Discharged/transferred to a home under care of organized home health service organization. 07 Left against medical advice or discontinued care. 08 Discharged/transferred to home under care of a home IV drug therapy provider. This is not a certified Medicare provider. 09 Admitted as an inpatient to this hospital (for use on Medicare Outpatient Hospital claims only). 20 Expired (or did not recover - Christian Science Patient). 30 Still patient. 40 Expired at home. (Hospice claims only.) 41 Expired in a medical facility, such as a hospital, SNF, ICF, or freestanding hospice. (Hospice claims only.) 42 Expired - place unknown. (Hospice claims only.) 43 Discharge/transferred to a Federal Health Care Facility. 50 Discharge to hospice home. 51 Discharge to hospice - medical facility. 61 Discharged/transferred within this institution to a hospital-based, Medicare-approved, swing bed. 62 Discharged/transferred to another rehabilitation facility an inpatient rehabilitation facility (IRF) including rehabilitation distinct part units of a hospital. 63 Discharged/transferred to a Medicare certified long term care hospital (LTCH). 64 Discharge/transferred to a nursing facility certified under Medicaid but not certified under Medicare. 65 Discharged/transferred to a psychiatric hospital or psychiatric distinct part unit of a hospital (for future use). Providers shall continue to use Patient Status Code 05 until further notice. 66 Discharged/transferred to a Critical Access Hospital (CAH) for discharge dates on or after January 1, Discharge/transfer to another type of health care institution not defined elsewhere in the code list. BILLING INSTRUCTIONS 7-3
7 7000. Updated 12/07 Note: Hospitals will be eligible for full DRG reimbursement when a discharge occurs using discharge code 01, 03, 04, 05, 06, 07, 08, 20, 50, or 51. Distinct claim forms must be submitted for each discharge. In the case of transfers to same specialty providers (discharge code 02), the transferring hospital s reimbursement may be reduced, based upon a transfer prorated reimbursement determination, and the receiving hospital will be eligible to receive a full DRG reimbursement. FL Condition Codes - Enter one of these two-digit codes to indicate a condition(s) relating to inpatient or outpatient claims, special programs or procedures (e.g., KAN Be Healthy, sterilization, etc.) Note: This is not a complete list. For a complete list of Condition Codes contact EDS Customer Service. 01 Military service related 02 Condition is employment related 03 Patient covered by insurance not reflected here 67 Beneficiary elects not to use life time reserve (LTR) days Note: This will now replace the Z1 Medicare Part A benefits exhausted condition code. The verbiage in the explanation of condition code 67 means the patient s benefits are exhausted. 80 Home Dialysis Nursing Facility A1 KAN Be Healthy (EPSDT) A4 Family Planning AA Abortion performed due to rape AB Abortion performed due to incest AI Sterilization D9 Any other change Note: This will now replace the XO swing bed condition code. FL Occurrence Codes/Dates: OCCURRENCE CODES CAN ONLY BE SUBMITTED ON LINE A. The following occurrence codes must be indicated if reporting information on type of accident, crime victim, other insurance denial or date of TPR termination, or aborted surgery, false labor or nondelivery claim where associated services are indicated. 01 Accident/medical coverage 02 No fault insurance involved including auto accident/other 03 Accident/tort liability 04 Accident/employment related 05 Accident/no medical or liability coverage 06 Crime victim 24 Date insurance denied 25 Date benefits terminated by primary payer A3 Benefits exhausted, Payer A B3 Benefits exhausted, Payer B C3 Benefits exhausted, Payer C BILLING INSTRUCTIONS 7-4
8 7000. Updated 12/07 All EDS/SRS guidelines remain the same regarding attachments required for TPR proof and SSA/Medicare EOMBs. FL 39 FL 42 FL 44 FL 45 FL 46 FL 47 Value Codes/Amount Required if applicable (for State Institutions Only). Enter D3 for nonpatient obligation as the value code. Enter the nonpatient obligation dollar amount in the Amount field. Examples of nonpatient obligation are Parental, Spousal, and Trust. Enter 80 for covered days and enter the number of covered days in the Amount field. Note: Count the date of admission but not the date of discharge. Rev. Cd. - Required - Inpatient Only. Enter the three-digit number identifying the type of accommodation and ancillary service(s). DO NOT INDICATE REVENUE CODE(S) IF THE SERVICE IS NONCOVERED. Note: Revenue codes are not to be indicated for outpatient services. HCPCS/Rates/HIPPS Code - Required - Outpatient Only. List the HCPCS procedure code for each specific outpatient procedure. DO NOT INDICATE PROCEDURE(S) IF THE SERVICE IS NONCOVERED. Serv. Date - Required - Outpatient Only. Enter the date services were provided in MM/DD/YY format. Serv. Units - Required. Enter number of days for each accommodation revenue code or appropriate units for each outpatient service billed. Total Charges - Required. Enter total charges for each coded line item. List each outpatient procedure with a specific (itemized) charge. DO NOT INDICATE CHARGES FOR NONCOVERED SERVICES. Enter the total claim charge on the last line of this detail section with a revenue code of 001 in FL 42 and total charges in FL 47. FL 48 FL 50 Noncovered Charges - Optional. Enter noncovered charges. Payer Name - Required. Indicate all third party resources (TPR). If TPR does exist, it must be billed first. Lines B and C should indicate secondary and tertiary coverage. Medicaid will be either the secondary or tertiary coverage and the last payer. When B and C are completed, the remainder of this line must be completed as well as FL Medicare needs to always be the last entry. BILLING INSTRUCTIONS 7-5
9 7000. Updated 12/07 FL 54 FL 56 FL 57 FL 60 FL FL 63 FL 64 FL 67A-Q FL 74 FL 74A-E FL 76 Prior Payments - Required if other insurance is involved. Enter amount paid by other insurance. Medicare needs to always be the last entry. (Do not enter spenddown or copayment amounts. These reductions will be made automatically during claim processing.) NPI: Enter the billing provider s NPI. Other Provider ID: Enter either qualifier 1D and the billing provider s KMAP provider ID or qualifier ZZ and the taxonomy code. Insured s Unique ID Required. Enter the 11-digit beneficiary number from patient's medical ID card on line C. If newborn services, use mother's beneficiary number if newborn's ID number is unknown. Group Name/Insurance Group No. - Required if Medicaid is not primary payer. Enter the primary insurance information on line A and Medicare on line C. Treatment Authorization Codes - Leave blank. (This number, if applicable, is system generated.) Document Control Number Desired if this claim is a resubmission. Enter the previous ICN. Note: This field is for timely filing purposes. DX - Required. Enter the ICD-9-CM code indicating the primary diagnosis and additional diagnoses. Principal Procedure - Required - Inpatient/Outpatient, if applicable. Enter the ICD-9-CM procedure code for the primary procedure and date of service. DO NOT INDICATE THE PROCEDURE IF THE SERVICE IS NONCOVERED. Other Procedure - Required - Inpatient/Outpatient, if applicable. Enter other procedures performed, using ICD-9-CM procedure codes and date of service. DO NOT INDICATE THE PROCEDURE IF THE SERVICE IS NONCOVERED. Attending - Required. a. Enter attending physician's NPI, or the appropriate qualifier and physician s KMAP provider ID or taxonomy code. b. Enter attending physician's Medicaid provider name as last name and then first name. Note: DO NOT ENTER A GROUP PROVIDER NUMBER. BILLING INSTRUCTIONS 7-6
10 7000. Updated 12/07 FL 77 FL Operating - Required if applicable. a. Enter operating physician's NPI, or the appropriate qualifier and physician s KMAP provider ID or taxonomy code. b. Enter operating physician's Medicaid provider name as last name and then first name. Other - Required if applicable. a. Enter other physician's NPI or the appropriate qualifier and physician s KMAP provider ID or taxonomy code. b. Enter other physician's Medicaid provider name as last name and then first name. Note: If the claim is for a sterilization, the surgeon performing the sterilization procedure must be identified by their KMAP provider ID in field 78. FL 80 Remarks - Specify additional information as necessary. BILLING INSTRUCTIONS 7-7
11 7000. Updated 12/07 Submission of Claim: Send completed claim to: Kansas Medical Assistance Program Office of the Fiscal Agent P.O. Box 3571 Topeka, Kansas BILLING INSTRUCTIONS 7-8
12 7010. MS-2126 BILLING INSTRUCTIONS Updated 5/07 Introduction to the Notification of Nursing Facility Admission/Discharge MS-2126 The completion of the MS-2126 (Notification of Nursing Facility Admission/Discharge) shall be completed by the provider and a copy sent to the local SRS office Economic & Employment Specialist (EES). Submission of the MS-2126 is not required as a prerequisite for a hospital "reserve day" (Section IV). However, the MS-2126 must be retained in the beneficiary's file for documentation. Completion of the MS-2126 is not required for payment of a therapeutic reserve day. This form will need to be copied or duplicated by providers since neither the fiscal agent nor the state will furnish the form to providers. When to Use the MS-2126: Sections I, II, and III, "Facility Placement/Discharge" shall be initiated by the nursing facility when: 1. An eligible Kansas Medical Assistance Program resident is initially admitted to or discharged from the nursing facility (NF), nursing facility for mental health (NF/MH) or intermediate care facility for the mentally retarded (ICF/MR). 2. A resident of an NF, NF/MH, or ICF/MR becomes eligible for Kansas Medical Assistance Program. 3. An eligible Kansas Medical Assistance Program resident transfers from one facility to another facility. 4. A resident's eligibility has been reinstated after suspension for more than two months. (If two calendar months or less, a new form will be needed.) 5. An eligible Kansas Medical Assistance Program resident is out of the facility for more than 30 days. (This is the same as a new admission.) When a resident returns to the facility on the 31st day, a new form will not be required. When a resident fails to return on the 31st day, a new form is required. 6. An eligible Kansas Medical Assistance Program resident has a change in his/her level of care. Section IV, Hospital Leave Information shall be initiated by the facility to report any hospital admission and to report reserve days for a medical leave being claimed by the facility. Completion of this section is not required for therapeutic (home) leave days. When a single hospital stay exceeds 30 days, the facility shall send another form to the local SRS office indicating the stay has exceeded 30 days and listing the estimated number of days the consumer will remain in the hospital. BILLING INSTRUCTIONS 7-9
13 7010. Updated 5/07 Return to the Facility: Whether Section III or IV is being completed, the EES retains a copy of this form for their files. The original MS-2126, completed by the facility, and the Notice of Action must be retained by the nursing facility. How to Complete the MS-2126: Section I: Name: Enter the resident's first name, middle initial, and last name as it appears on the medical identification (ID) card. SSN: Enter the resident's Social Security number. If the resident does not have a Social Security number, enter the "NA." Date of Birth: Enter the resident's birth date in month, day, and year - MM/DD/YYYY format. (Example: May 15, 1925 should appear as ) Sex: Indicate "M" for male and "F" for female. Client ID Number: Enter the 11-digit resident number from the individual's Kansas Medical Assistance Program card. Responsible Person's Name: Enter the first and last name of the responsible party. Responsible Person's Address: Enter the responsible person's street address, P.O. Box number, along with his/her city, state, and zip code. Phone: Enter the responsible party's area code and phone number. Section II: Facility Name: Enter the name under which the facility operates. Provider Number: Enter your 10-digit Medicaid provider number. Address: Enter the street address, city, and zip code where the facility is located BILLING INSTRUCTIONS 7-10
14 7010. Updated 5/07 Date of Placement: Date resident was admitted to the facility. Anticipated Length of Stay: Enter the number of months the resident is expected to be in the facility. If unknown, write "unknown." Screened By: Enter the name of the person or facility completing the assessment. The State of Kansas requires that "each individual prior to admission to an NF... receive assessment and referral services." To achieve this, the CARE program was created "for the data collection and individual assessment and referral to community-based services and appropriate placement in long-term care facilities. Date: Date screening was completed (if known). Signature: The facility administrator or his/her designee signs here. Phone: In the event there are questions, please indicate the area code and telephone number to call. Section III: Enter a check mark in the appropriate space to indicate (A) Admission, (B) Discharge, or (C) Deceased. Providers will also need to indicate the method of payment in place at the time of admission or discharge. Section IV: A1. Admitted From: Indicate where the resident is being admitted to and the name of the facility they are coming from. A2. Indicate method of payment at time of admission. B1. Discharged On: Check the appropriate space to indicate where the resident is being discharged to, name of facility, and date of discharge. B2. Indicate method of payment at time of discharge. C. Deceased Date: Enter the resident's date of death. A. Entered: Enter the name of the hospital and the date entered. B. Reason Admitted: If known, indicate reason for admission. If unknown, write "UNKNOWN". C. Estimated Days in Hospital: Indicate the number of days the admitting physician reasonably believes the resident will be in the hospital BILLING INSTRUCTIONS 7-11
15 7010. Updated 5/07 Reserve Day Notice - Once the facility has completed this form, it should be submitted to the local SRS office. Since the information sent to the SRS office will not be returned, it is important for the facility to keep the original in their files. Nursing Facility Processes Form III. Facility Placement/Discharge: The facility is required to retain the completed form in the facility. These records shall be made available to SRS and/or the fiscal agent upon request. Suspension of payment to the facility may result in the absence of this form. IV. Hospital Leave Day Form: Retain the completed form in the beneficiary's records for documentation of medical reserve day approval BILLING INSTRUCTIONS 7-12
16 7020. HOSPITAL SPECIFIC BILLING INFORMATION Updated 03/08 Inpatient Accommodation and Ancillary Charges: If the individual accommodation and ancillary services exceed the detail lines on the UB-04 claim form, providers may combine all similar revenue code charges together (e.g., lab, radiology) when necessary. Accommodation codes may also be 'lumped' together when necessary. This will not affect the reimbursement of the claim. Admission and Readmission (Same Day): Admission An inpatient admission starts when the physician writes an order for an inpatient admission. It is not considered inpatient until that order has been written. Documented verbal admission orders are considered the same as written orders. Scenario #1: A patient is sent to the medical floor on September 23 at 11:00 p.m. The physician writes an order to admit the patient on September 24 at 3:00 a.m. According to KMAP, the inpatient admission starts on September 24 at 3:00 a.m. Scenario #2: A physician writes an order for a patient to be admitted inpatient on September 23 at 11:00 p.m. The patient arrives on the medical floor on September 24 at 3:00 a.m. According to KMAP, the inpatient admission starts on September 23 at 11:00 p.m. Scenario #3: A physician contacts a hospital on September 23 at 11:00 p.m. about a direct admission and gives a verbal order for admission once the patient arrives at the hospital. The patient arrives at the hospital on September 24 at 3:00 a.m. According to KMAP, the inpatient admission starts on September 24 at 3:00 a.m. Readmission (Same Day) When a patient is discharged or transferred from an inpatient hospital and is readmitted to the same inpatient hospital on the same day for symptoms related to or for evaluation and management of the prior stay s medical condition, hospitals must adjust the original claim generated by the original stay by combining the original and subsequent stay onto a single claim. When a patient is discharged or transferred from an inpatient hospital and is readmitted to the same inpatient hospital on the same day for symptoms unrelated to and not for evaluation and management of the prior stay s medical condition, hospitals must bill for two separate stays on two separate claims. Emergency Renal Dialysis: Inpatient emergency renal dialysis must be billed utilizing revenue code 809 in FL 42 of the UB-04 claim form. Interim Billing: Interim billing is restricted to once every 180 days. Interim bills received more frequently than 180 days will be denied. When interim billing, be sure to enter the appropriate 'Type of Bill' code (e.g., 112, 113, 114). A 'Patient Status' code of 30 (still a patient) must be indicated when 'Type of Bill' is 112 or 113. Medicare B Services: When Medicare B payment is made on an inpatient claim, indicate the amount paid as Prior Payment in FL 54 on the UB-04 claim form. BILLING INSTRUCTIONS 7-13
17 7020. Updated 03/08 Newborn Services (When the Mother Is NOT in an HMO): When billing for a newborn who does not have a beneficiary ID number, use "Newborn", "Baby Girl", or "Baby Boy" in the first name field of patient name. Use the newborn's date of birth and the mother's beneficiary ID number. The claim will suspend in the claims processing system for up to 45 days pending the fiscal agent's receipt of the newborn's beneficiary ID number from the local SRS office. If the newborn's beneficiary ID number is received within the 45 days, the claim will be processed using that number. If the newborn's beneficiary ID number is not received within the 45 days, the claim will complete processing with the mother's beneficiary ID number. Newborn Services (When the Mother Is in an HMO): Notify the HMO that is on the mother's Medicaid ID card of the birth. The HMO will provide further instructions if the provider is part of that HMO's network. The mother's HMO will notify KHPA and the fiscal agent of the birth. Outpatient/Inpatient: Outpatient procedures (i.e., surgery, X-rays, EKGs) provided within three days of a hospital admission or discharge for the same or similar diagnosis are considered 'content of service' and should be billed on the same inpatient hospital claim. The outpatient procedure date should be changed on the claim to correspond with the actual hospital admission date. Note: There is one exception to this policy. Complications from an outpatient sterilization resulting in an inpatient admission. In this instance, the outpatient charges and the inpatient charges should be billed on two separate claims. This is necessary in order for the service dates on the claim form to match the service dates on the sterilization consent form. Outpatient Services Provided During Inpatient Admission: Outpatient services provided during an inpatient hospital stay must be included by the hospital on the UB-04 claim form and reimbursed through the DRG. The outpatient provider should receive reimbursement from the hospital. Outpatient services provided to residents of state institutions shall be billed by the hospital providing the outpatient service. Psychiatric Observation Beds: When an inpatient hospital admission follows a psychiatric observation stay, the observation days should be billed on the inpatient claim. The observation bed days then become part of the DRG payment to the hospital. Transfers: When billing medically necessary incoming transfers, in FL 80 on claims for incoming transfers from other hospitals under "Remarks" enter "direct transfer from (hospital, city)". Swing Bed Nursing Facility: When billing for a swing bed nursing facility (NF), the following must be observed: 1) Your hospital must be certified by the Kansas Department of Health and Environment as a swing bed NF hospital. BILLING INSTRUCTIONS 7-14
18 7020. Updated 5/07 2) Notify the local SRS Income Maintenance (IM) Worker immediately when an SRS consumer is placed in a swing bed NF. Notification shall be performed by completing parts I and II of the MS (Refer to Section 7010.) Once the IM Worker has received the MS-2126, the consumer's case will be budgeted for longterm care. The hospital will then be notified via a "Notice of Action" as to the consumer's liability to the hospital while in the swing bed NF. Providers must bill the full amount and patient liability will be deducted during processing. When billing for a Swing bed, a separate claims must be submitted for each calendar month. Do not attach a copy of either the MS-2126 or Notice of Action to your claim form. 3) Bill all NF days for eligible Medicare patients to Medicare first. Medicaid can be billed for any remaining amounts using the inpatient Medicare claim crossover method. (Refer to Section 3200.) If Medicare will not pay for the NF days, a copy of either the Medicare Report of Eligibility (ROE) or a Medicare denial must be attached to the Medicaid billing supporting non-payment by Medicare. 4) Before a transfer to a swing bed NF occurs, the patient must be discharged from the inpatient unit. Use the appropriate 3-digit type of bill code in FL 4 on the UB-92 UB-04 claim form. (Refer to Section 7000.) Remember, the inpatient unit is not reimbursed for the date of discharge since the swing bed NF will be reimbursed for the date of admission. 5) The appropriate accommodation revenue code applicable to the patient's level of care shall be entered in FL 42. Bill the total number of days in FL 46 (units). In FL 47, place the total charge of days billed. Ancillary charges: Cannot be billed on the swing bed NF claim. Any ancillary services received by the patient while in a swing bed NF, must be billed on a UB-92 UB-04 claim form using the outpatient type of bill code (FL 4) and the correct HCPCS code and revenue code for the ancillary services provided. (See items 7 and 8 for supplies/services which are content of service for swing bed NF and cannot be billed separately). Indicate condition code D9 (any other change) X0 (swing bed ancillary) in FL , and enter the from and through dates of service in FL 6 on the UB-92 UB-04 claim form. When multiple dates of service are being billed, enter only the first date of service in FL 45 on the UB-92 UB-04 claim form. BILLING INSTRUCTIONS 7-15
19 7020. Updated 5/07 Pharmacy: Pharmacy services for swing bed claims need to be billed on a pharmacy claim form from a Medicaid-enrolled outpatient pharmacy. Refer to the Pharmacy Provider Manual for billing instructions. Supplies: When billing for supplies provided by the swing bed facility over and above the supplies included in the reimbursement rate, use procedure code bill one unit per day. Claims must include both revenue codes and HCPCS codes. Therapy: Physical, occupational and speech therapy may be billed as outpatient hospital services for clients in hospital swing beds and long term care units attached to hospitals. 6) With the exception of the billing guidelines addressed above, the remainder of the claim form is to be completed in the same manner as an inpatient submission. Refer to instructions in Section 7000 of this manual. 7) A hospital may not charge Medicaid consumers for providing routine supplies and services since: (1) The hospital is required to provide routine supplies and services to Medicaid swing bed patients; and (2) the cost of providing routine supplies and services is included in the hospital's swing bed per diem reimbursement. 8) "Routine" is defined as an item that is commonly stocked for use by anyone. It is an item that may or may not be specifically assigned or prescribed to any one patient. Routine items covered by the drug program when ordered by a physician for occasional use are included in the per diem reimbursement. Since items considered to be routine for residents of adult care homes are also considered to be routine for swing bed NF patients, refer to Appendix III for a descriptive list of routine items. Any routine item billed on the outpatient hospital claim form will be denied. "Non-routine" is defined as a specifically prescribed item for a resident for an acute or chronic need. Medication orders may be considered non-routine if: (1) It is not a stock item of the facility; or (2) it is a stock item with unusually high usage by the individual. BILLING INSTRUCTIONS 7-16
20 7020. Updated 05/07 Outpatient NOTE: Outpatient hospital claims which require medical necessity documentation may be billed electronically. Medical necessity documentation must be retained in the provider's file and made available for review on a post-pay basis. Refer to your EMS Operators manual for additional information. It is not required that providers roll-up their charges into the covered HCPCS code they are billing. Providers can bill the HCPCS code they are providing and the processing system will allow the covered charges and deny the services that are content or non-covered. Durable Medical Equipment/Prosthetics and Orthotics: Hospitals must enroll as DME or P&O providers and bill on the professional claim form (HCFA-1500 CMS-1500) when providing these services. Contact the Provider Assistance Unit at or (785) (local). DME, prosthetic and orthotic items cannot be billed as ancillary services on the UB-92 UB-04 claim form. Exception: Prosthesis implanted by a surgical procedure may be billed on the hospital claim form for inpatient services. Procedure codes for covered items can be found in Appendix I of the Durable Medical Equipment and Prosthetic and Orthotic manuals. Emergency Renal Dialysis: Outpatient emergency renal dialysis must be billed utilizing the following diagnosis codes in FL 67 and/or 68 of the UB-92 UB-04 claim form. Diagnosis Codes Emergency Room/Department Services: Enter the time of day (using the Continental Time System, i.e., ) in FL 13 18, admission hour. Emergency services provided in the emergency department shall be billed using the appropriate Evaluation and Management (E&M) emergency department or critical care procedure code from the CPT manual BILLING INSTRUCTIONS 7-17
21 7020. Updated 5/07 Please reference the Physician's Current Procedural Terminology (CPT) manual for information on the Centers for Medicare & Medicaid Services (CMS) Health Care Financing Administration (HCFA) and American Medical Association's (AMA) documentation guidelines as well as directions for assigning codes for emergency services. Copies of "detailed" documentation guidelines have been published by CMS HCFA, Blue Cross & Blue Shield (BCBS), and the Kansas Foundation for Medical Care (KFMC). E&M procedure codes applicable to emergency department services include: Refer to the CPT manual for procedure code nomenclature. Mid-Level Practitioners: Physician Assistants (PA) and Advanced Registered Nurse Practitioners (ARNP) must be enrolled as a Medicaid provider to bill for services. Indicate the PA s or ARNP s number as the attending physician on the UB-92 UB-04 claim form. ARNPs and PAs are reimbursed 75% of the Medicaid allowed amount for services provided. Modifiers for ER Services: The ET modifier must be added to the base E&M procedure code when billing the hospital ER/observation room and supplies. When billing for the hospital-based physician, indicate the base code only (no modifier). Non-Emergency: A revenue code is not required for any outpatient service. Use HCPCS procedure codes. In the instance of a non-emergent visit, procedure code may be used. Submit only your charges for the hospital-based physician professional fee and covered diagnostic tests, endoscopic procedures, therapy, etc. BILLING INSTRUCTIONS 7-18
22 7020. Updated 5/07 Enter the time of day using the Continental Time System if the services are provided between 6:00 p.m. and 8:00 a.m. (1800 and 0800 hours) in FL 13 18, admission hour Hospital- based physician professional fee in a non-emergency situation 99281ET Emergency department encounters 99070ET Medical supplies required for non-emergency treatment Bilateral Procedures: Bilateral procedures performed during the same operative session shall be billed with the appropriate procedure code. To be consistent with Medicare, if a procedure is identified in the CPT manual as one that should have a '50' modifier added when performed bilaterally, bill the procedure as a single line item with the '50' modifier. For example, to bill the excision of bilateral nasal polyps, the provider should indicate procedure code ' ' on one detail line on the claim. Reimbursement will be made for the bilateral procedure. 'E' Diagnosis Codes: External causes of injury and poisoning diagnosis ('E') codes are accepted on a claim as a secondary diagnosis when billed in conjunction with a covered primary diagnosis code. Observation Room: Procedure code 99218WP ET should be billed for any service which requires monitoring a patient's condition beyond the usual amount of time in an outpatient setting. This code shall not be used to bill for the recovery room. Sterilization Procedures: When a sterilization is performed in conjunction with, or secondary to an inpatient procedure (e.g., delivery) and the sterilization is not covered (e.g., failure to obtain the sterilization consent form), remove all procedure codes and charges related to the sterilization from the claim and bill the primary procedure only. Carefully document in the medical record the reason the sterilization was not billed on the claim. BILLING INSTRUCTIONS 7-19
23 7020. Updated 05/07 Physician Clinic Services: Currently, some physicians make scheduled visits once or twice a week to rural hospitals and see patients in the emergency room which functions as their office. Physician clinic services provided in a hospital location are considered content of the physician service and should not be billed to Medicaid or the consumer. However; in this instance the hospital can bill procedure code (supplies and materials) for use of room and supplies. Professional Fees: The only physician services which can be billed by the hospital on the UB-92 UB-04 claim form are hospital based physicians assigned to the emergency department. Professional/Technical Component Billing: Components: Professional: Enter the HCPCS base code for services rendered, including modifier "26". (Example: ). Technical: Enter the HCPCS base code of the service performed, including modifier "TC". (Example: 72070TC). Note: Hospitals that bill the base code for radiology procedures will be reimbursed at the TC rate. Professional and Technical: Enter the HCPCS base code of the radiology service performed. (Example: 72070) The same procedures performed on the same day: Must be billed on the same claim. Must clarify the reason for billing more than one procedure (e.g., 2 x-rays at two different times; left arm, right arm). When same procedures are not billed on the same claim, the additional claim(s) will be denied as a duplicate. To seek reimbursement for additional services when this occurs: Submit an underpayment adjustment using the Internal Control Number (ICN) from the Remittance Advice (RA) of the paid claim, and state on the adjustment request that more than one procedure was performed on the same day. Refer to Section 5600 for details. Unit Billing: When billing for outpatient hospital services, round units to the nearest whole number. Do not bill fractions of units. BILLING INSTRUCTIONS 7-20
24 7030. STATE INSTITUTION FOR M/H BILLING INSTRUCTIONS Updated 02/08 Introduction to the UB-04 Claim Form State institution for mental health providers must use the UB-04 red claim form (or accepted electronic equivalent) when requesting payment for medical services and supplies provided under the Kansas Medical Assistance Program. Any UB-04 claim not submitted on the red claim form will be returned to the provider. An example of the UB-04 claim form is in the Forms section at the end of this manual. Instructions for completing this form are included in the following pages. The Kansas MMIS will be using electronic imaging and optical character recognition (OCR) equipment. Therefore, information will not be recognized if not submitted in the correct fields as instructed. EDS does not furnish the UB-04 claim form to providers. Refer to Section The following numbered form locators (FL) fields are to be completed when required or if applicable. Billing Instructions: FL 1 FL 3A FL 3B FL 4 (No Field Name) - Required. Enter the name and address of the billing provider. Patient Control No. Enter a patient account number if desired. (This number will be referenced on the Remittance Advice [RA].) Medical Record No.-Desired. Enter the patient s medical record number. (This number will appear on the provider s RA.) Type of Bill - Required. Enter the 3-digit number specific to the type of claim. 1st digit indicates facility. (Always a 2 or 6.) 2nd digit indicates location within facility. 3rd digit indicates the frequency of the claim billed. Medicaid allowed codes: 1st digit: 1 Hospital (IP/OP) 2nd digit: 3rd digit: 1 Inpatient 0 Non-payment/zero claim 1 Admit through discharge claim 2 Interim - first claim 3 Interim - continuing claim 4 Interim - last claim (thru date is discharge date) FL 6 Statement Covers Period - From/Through - Required. Enter dates of admission and discharge from and through dates in MM/DD/CCYY format. BILLING INSTRUCTIONS 7-21
25 7030. Updated 03/08 FL 7 FL 8B FL 10 FL 12 FL 17 Covered Days - Required - Inpatient Only. Enter the number of days for which you are billing. Note: Count date of admission, but not date of discharge. Patient Name - Required - Enter patient's last name, first name and middle initial exactly as it appears on the ID card. Birthdate - Required. Enter patient's date of birth in MM/DD/YYYY format (i.e. October 1, 1957 would be listed as 10/01/1957). Admission Date - Required. Enter date patient was admitted to the facility in MM/DD/CCYY format. Patient Status - Required - Inpatient Only. Enter a two-digit code to indicate status of patient: 01 Discharged to home or self care (routine discharge). 02 Discharged/transferred to another short-term general hospital for inpatient care. 03 Discharged/transferred to skilled nursing facility (SNF) with Medicare certification. 04 Discharged/transferred to an Intermediate Care Facility (ICF). 05 Discharge/transfer to a designated cancer center or children s hospital. Discharged/transferred to a non-medicare PPS children s hospital or non-medicare PPS cancer hospital for inpatient care. 06 Discharged/transferred to a home under care of organized home health service organization. 07 Left against medical advice or discontinued care. 08 Discharged/transferred to home under care of a home IV drug therapy provider. This is not a certified Medicare provider. 09 Admitted as an inpatient to this hospital (for use on Medicare Outpatient Hospital claims only). 20 Expired (or did not recover - Christian Science Patient). 30 Still patient. 40 Expired at home. (Hospice claims only.) 41 Expired in a medical facility, such as a hospital, SNF, ICF, or freestanding hospice. (Hospice claims only.) 42 Expired - place unknown. (Hospice claims only.) 43 Discharge/transferred to a Federal Health Care Facility. 50 Discharge to hospice home. 51 Discharge to hospice - medical facility. 61 Discharged/transferred to a hospital-based, Medicare-approved, swing bed. BILLING INSTRUCTIONS 7-22
26 7030. Update 03/08 62 Discharged/transferred to an inpatient rehabilitation facility (IRF) distinct part units of a hospital. 63 Discharged/transferred to a Medicare certified long term care hospital (LTCH). 64 Discharge/transferred to a nursing facility certified under Medicaid but not certified under Medicare. 65 Discharged/transferred to a psychiatric hospital or psychiatric distinct part unit of a hospital (for future use). Providers shall continue to use Patient Status Code 05 until further notice. 66 Discharged/transferred to a Critical Access Hospital (CAH) for discharge dates on or after January 1, Discharge/transfer to another type of health care institution not defined elsewhere in the code list. FL Condition Codes Optional. Enter one of these two-digit codes to indicate a condition(s) relating to inpatient or outpatient claims, special programs or procedures (e.g. KAN Be Healthy, sterilization, etc.). Note: This is not a complete list. For a complete list of Condition Codes contact EDS Customer Service. 01 Military service related 02 Condition is employment related 03 Patient covered by insurance not reflected here 67* Beneficiary elects not to use life time reserve (LTR) days *This will now replace the Z1 Medicare Part A benefits exhausted condition code. The verbiage in the explanation of condition code 67 means the patient s benefits are exhausted. 80 Home Dialysis Nursing Facility A1 KAN Be Healthy (EPSDT) A4 Family Planning AA Abortion performed due to rape AB Abortion performed due to incest AI Sterilization D9* Any other change *This will now replace the XO swing bed condition code. BILLING INSTRUCTIONS 7-23
27 7030. Updated 12/07 FL Occurrence Codes/Dates: OCCURRENCE CODES CAN ONLY BE SUBMITTED ON LINE A. The following occurrence codes must be indicated if reporting information on type of accident, crime victim, other insurance denial or date of TPR termination, or aborted surgery, false labor or nondelivery claim where associated services are indicated. Note: This is not a complete list. For a complete list of Occurrence Codes contact EDS Customer Service. 01 Accident/medical coverage 02 No fault insurance involved including auto accident/other 03 Accident/tort liability 04 Accident/employment related 05 Accident/no medical or liability coverage 06 Crime victim 24 Date insurance denied 25 Date benefits terminated by primary payer A3 Benefits exhausted, Payer A B3 Benefits exhausted, Payer B C3 Benefits exhausted, Payer C All EDS/SRS guidelines remain the same regarding attachments required for TPR proof and SSA/Medicare EOMBs. FL 39 *FL 42 *FL 45 *FL 46 Value Codes/Amount Required if applicable (for State Institutions Only). Enter D3 for nonpatient obligation as the value code. Enter the nonpatient obligation dollar amount in the Amount field. Examples of nonpatient obligation are Parental, Spousal, and Trust. Enter 80 for covered days and enter the number of covered days in the Amount field. Note: Count the date of admission but not the date of discharge. Revenue Code Required. Enter the three-digit code identifying the type of accommodation services. Use only the revenue codes listed below: 101 All inclusive room and board 180 NF/MH reserve days 181 Home therapeutic reserve days ICF/MH 21 days per calendar year 183 Home leave days / Therapeutic leave days 185 Hospital leave days 189 Noncovered days Service Date Required. Enter first date of service for the detail line. Service Units - Required. Enter the total number of days for each detail line. BILLING INSTRUCTIONS 7-24
28 7030. Updated 09/07 FL 47 FL 50 FL 54 FL 57 FL 60 FL FL 67A-Q FL 76 FL 80 Total Charges - Required. Enter total charges billed. Payer Name - Required. Enter all third party resources (TPR). If TPR does exist, it must be billed first. Lines B and C should indicate secondary and tertiary coverage. Medicaid will be either the secondary or tertiary coverage and the last payer. When B and C are completed, the remainder of this line must be completed as well as FL Medicare needs to always be the last entry. Prior Payments - Required if other insurance is involved. Enter amount paid by other insurance. Medicare needs to always be the last entry. Do not enter patient liability amount. It is automatically deducted during claim processing. Other Provider ID: Enter either qualifier 1D and the billing provider s KMAP provider ID or qualifier ZZ and the taxonomy code. Insured s Unique ID: Enter the 11-digit number from the beneficiary s medical card on line C. Group Name/Insurance Group No. - Required if Medicaid is not primary payer. Enter the primary insurance information on line A and Medicare on line C. Prin. Diag. Cd. - Required. Enter the ICD-9-CM code indicating the primary diagnosis and additional diagnoses. Attending - Optional. a. Enter attending physician's NPI, or the appropriate qualifier and physician s KMAP provider ID or taxonomy code. b. Enter attending physician's Medicaid provider name as last name and then first name. Remarks Optional. Specify additional information as necessary. Submission of Claim: Send completed claim to: Kansas Medical Assistance Program Office of the Fiscal Agent P.O. Box 3571 Topeka, Kansas BILLING INSTRUCTIONS 7-25
29 7030. Updated 9/07 STATE INSTITUTION FOR M/H SPECIFIC BILLING INFORMATION Accommodation and Ancillary Charges: If the individual accommodation and ancillary services exceed the detail lines on the UB-04 claim form, providers may combine all similar revenue code charges together (e.g., lab, radiology) when necessary. Accommodation codes may also be 'lumped' together when necessary. This will not affect the reimbursement of the claim. State institutions may bill for ancillary services without indicating an accommodation code. Medicare B Services: When Medicare B payment is made on an inpatient claim, indicate the amount paid as "Prior Payment" in FL 54 on the UB-04 claim form. Other Insurance: When a consumer has other insurance, proof of payment or denial is required. Enter the amount paid by the other insurance carrier in FL 54 on the claim form. Refer to Section 3300 for specific instructions on submitting claims when other insurance is involved. Patient/Parental Liability: Indicate any patient or parental liability in FL 54 on the UB-04 claim form. Payment will be deducted accordingly. Transfers: When billing medically necessary incoming transfers, the following should be entered on claims for incoming transfers from other hospitals: In FL 84 "Remarks", enter "direct transfer from (hospital, city)". Reserve Days: Indicate revenue code 189 in FL 42 when billing for reserve days. BILLING INSTRUCTIONS 7-26
30 8100. COPAYMENT Updated 11/03 BENEFITS AND LIMITATIONS General hospital inpatient services require a copayment of $48.00 per inpatient admission. General hospital outpatient surgery requires a copayment of $3.00 per surgery. General hospital non-emergency outpatient services in place of a doctor's office visit require a copayment of $3.00 per visit. Ambulatory surgical center services require a copayment of $3.00 per day. Inpatient free standing private psychiatric facility services require a copayment of $48.00 per admission. Specialty hospital (rehabilitation facilities, teaching facilities, etc.) inpatient services require a copayment of $48.00 per inpatient admission. State psychiatric facility consumers are exempt from copayment requirements. Transferring inpatient hospital admissions are exempt from copayment requirements. Copayment will be deducted from the receiving hospital. Bill all services occurring on the same date on the same claim form. If multiple claims are submitted for the same date(s) of service, the copayment requirement will be deducted for each claim submitted. Do not reduce charges or balance due by the copayment amount. This reduction will be made automatically during claim processing. Refer to Section 3000 for exceptions. BENEFITS & LIMITATIONS 8-1
31 BENEFITS AND LIMITATIONS MEDICAL ASSESSMENT Updated 08/07 Documentation: To verify services provided in the course of a postpayment review, documentation in the patient's medical record must support the service billed. Documentation can be requested at any time to verify that services have been provided within program guidelines. Refer to Section 5000 of the General Billing Provider Manual. Autoauthentication (computerized authentication) of documentation for the medical record is acceptable documentation for the Kansas Medical Assistance Program. Autoauthentication must meet federal guidelines. It may be necessary to contact the ordering physician for medical necessity information. Federal regulation 42 CFR (c) (1) (i) requires that there must be a method of determining that the physician authenticated the document after transcription. All entries must be legible and complete and must be authenticated and dated promptly by the person (identified by name and discipline) who is responsible for ordering, providing, or evaluating the service furnished. The author of each entry must be identified and must authenticate his or her entry. Authentication may include the author's signature, written initials, or computer entry. The information below indicates medical information which may be necessary to document medical necessity of those diagnoses designated as sometimes payable on the screen. Abdominal Plain Films and Ultrasound: Abdominal plain films and ultrasound are medically necessary if the diagnosis indicates abdominal pain, nausea/vomiting, complications associated with ulcers, intestinal obstruction, gall bladder disease, malignant neoplasm of the abdominal organs, injury to the abdomen or nephrolithiasis. It may be necessary to contact the ordering physician for medical necessity information. An abdominal plain film may be warranted in a pregnant patient if: Fetal position is questionable Obstetrical ultrasound is unavailable and patient is in labor Electrocardiograms (EKGs): Electrocardiograms (up to 12 leads) are considered medically necessary when the diagnosis and/or condition clearly indicates one or more of the following: Relevant cardiopulmonary diagnosis Significant electrolyte imbalance Drug induced EKG changes (identify the drug) Progressive renal disease Unstable thyroid disease Specific central nervous system (CNS) disorders causing EKG changes BENEFITS & LIMITATIONS 8-2
32 8200. Updated 9/06 Congenital disorders causing EKG changes Symptomatic hypothermia Shortness of breath Fainting spells Monitoring the effects of psychotropic drugs for potential cardiac effects (identify the drug) Preoperative EKGs are medically necessary for patients over age 40, or those patients under 40 with a history of cardiac problems. It may be necessary to contact the ordering physician for medical necessity information. Cardiac Rehabilitation: Phase II Cardiac Rehabilitation is covered using procedure code This procedure is covered when performed in an outpatient or cardiac rehabilitation unit setting, with the following criteria: Beneficiary must have a recent cardiology consultation within three months of starting the cardiac rehabilitation program. Beneficiary must have completed Phase I Cardiac Rehabilitation: Beneficiary must have one or more of the following diagnoses/conditions. o Acute myocardial infarction ( , 414.8) within the preceding three months, post inpatient discharge o Coronary bypass (V45.81) surgery within the preceding three months, post inpatient discharge o Stable angina pectoris (413.9 and 413.0) within three months post diagnosis Chest X-Rays: Chest X-rays are determined medically necessary if: History or indication of cardiopulmonary disease, malignancy, cardiovascular accident (CVA), or long bone fracture Recent thoracic surgery Thoracic injury Chronic cough of over one month duration o (Specify as chronic in the diagnosis field. If this designation is not supplied, the condition will be considered acute and the X-ray denied.) Pre-operative and routine admission chest X-rays are non-covered unless documentation of medical necessity (one or more of the following factors) is noted on the claim: Sixty years of age or older Pre-existing or suspected cardiopulmonary disease Smoker over age forty Acute medical/surgical conditions such as malignancy or trauma BENEFITS & LIMITATIONS 8-3
33 8200. Updated 9/06 Claims denied because other factors are listed, will be reconsidered if appealed (refer to Section 5300). It may be necessary to contact the ordering physician for medical necessity information. CT Scans - Abdominal: A CT scan of the abdomen is medically necessary if the diagnosis indicates a malignant neoplasm of the intra-abdominal cavity, lung or genital organs, lymphoma, diseases of the spleen, liver abscess, peritonitis, pancreatitis, abdominal trauma, or abdominal mass. A CT scan of the abdomen may be medically necessary for abdominal pain, abdominal aneurysm, acute lymphocytic leukemia, or any malignant neoplasm not located in the intraabdominal cavity, lung or genital organs. Inclusion of the following documentation will assist in the adjudication of your claim. Abdominal Pain: Indicate the severity and chronicity of the pain, presenting symptoms and suspected conditions or complications. Abdominal Aneurysms: Indicate the presenting symptoms and suspected complications. Acute Lymphocytic Leukemia: Indicate the presenting symptoms and a detailed description of area(s) involved. Malignant Neoplasm not located in the Intra-Abdominal Cavity, Lung or Genital Organs: Indicate pertinent symptoms and if performed as part of staging the disease process. It may be necessary to contact the ordering physician for medical necessity information. CT Scans - Head or Brain: CT scan of the head or brain is medically necessary if the diagnosis indicates intracranial masses/tumors, intracranial congenital anomalies, hydrocephalus, brain infarcts, parencephalic cyst formation, open or closed head injury, progressive headache with or without trauma, intracranial bleeding, aneurysms, or the presence of a neurological deficit. A CT scan of the head or brain may also be medically necessary with the indication of headache, epilepsy, syncope, dizziness, or acute lymphocytic leukemia. Inclusion of the following documentation will assist in adjudication of your claim: Headache - Indicate length of chronicity and any accompanying Central Nervous System (CNS) symptoms. Epilepsy - Specify if initial or repeat scan, indicate if suspected injury occurred during seizure. Syncope - Specify if recurrent or single episode. Dizziness - Specify if recurrent or single episode. Acute Lymphocytic Leukemia - Indicate any accompanying CNS symptoms. It may be necessary to contact the ordering physician for medical necessity information. BENEFITS & LIMITATIONS 8-4
34 8200. Updated 3/06 Hyperbaric Oxygen Therapy Hyperbaric oxygen therapy is a covered service under KMAP with prior authorization. The following criteria must be met before a PA will be approved. 1. the services must be for one of the following conditions: a. Acute carbon monoxide intoxication b. Decompression illness c. Gas embolism d. Gas gangrene e. Acute traumatic peripheral ischemia f. Compromised skin grafts g. Chronic refractory osteomyelitis h. Osteoradionecrosis i. Soft tissue radionecrosis j. Cyanide poisoning k. Actinomycosis l. Crush injuries and suturing of severed limbs m. Progressive necrotizing infections n. Acute peripheral arterial insufficiency o. Diabetic wounds of lower extremities 2. It must be documented that other treatments have been attempted with no improvement. Facilities bill for this procedure using either (one unit equals 30 minutes) or C1300 (four units equals one session, up to two hours). The facility must choose which procedure code they will bill prior to the approval of the PA. If there are multiple sessions on the same day (more than four units for facilities), each subsequent session must be billed on a separate line detail with a 76 modifier. MRI - Head or Brain: MRI scan of the head or brain is medically necessary if the diagnosis indicates intracranial injury, intracranial mass/tumor, CNS malignancies, cerebrovascular disorder, cerebral malformations, disorders of the cerebral hemispheres and higher brain functions, demyelinating diseases, extrapyramidal and cerebellar disorders, brain abscesses, encephalitis, tuberculous meningitis, or the presence of a neurological deficit. MRI scan of the head or brain may also be medically necessary with the indication of headache, seizure disorders, syncope, dizziness, or non-cns malignancies. Inclusion of the following information will assist in adjudication of your claim: Headache - Indicate length of chronicity and any accompanying neurologic symptoms. Seizure - Specify if initial or repeat scan, and if seizures (or convulsions) are of Disorders - (or convulsions) are of recent onset, frequency of their occurrence, and any accompanying neurologic symptoms. Syncope - Specify if recurrent or single episode and any accompanying neurologic symptoms. BENEFITS & LIMITATIONS 8-5
35 8200. Updated 3/06 Dizziness - Specify if recurrent or single episode and any accompanying neurologic symptoms. Non-CNS Malignancies - Indicate any accompanying neurologic symptoms. It may be necessary to contact the ordering physician for medical necessity information. MRI - Breast MRI of the breast will be covered with the following indications: Staging and therapy planning in patients diagnosed with breast cancer Occult primary breast cancer when there are positive axillary nodes and no known primary tumor Inconclusive diagnosis after a standard mammography evaluation, for example when scar tissue from previous surgery, dense breast tissue of breast implants render mammographic images inconclusive MRI used for screening for breast cancer is not justified. Skull X-Rays: Skull X-rays are medically necessary if diagnosis indicates cranial trauma, primary or metastatic tumors of the skull, or tumors of the pituitary gland. A skull X-ray may also be medically necessary for indication of chronic sinusitis, trigeminal neuralgia, or anomalies relating to the head. Inclusion of the following documentation will assist in the adjudication of your claim: Chronic Sinusitis - Indicate any pertinent specific suspected complications resulting from chronicity. Trigeminal Neuralgia - Specify type of lesion suspected. Anomalies relating to the head - Specify if done as a scout film for non-cosmetic reconstructive surgery. Indicate type of surgery under consideration. It may be necessary to contact the ordering physician for medical necessity information. Sonograms - Non-Obstetrical Pelvic: Non-obstetrical pelvic sonograms are determined medically necessary if the diagnosis indicates pelvic mass or pain, ovarian cyst, pelvic inflammatory disease, endometriosis, possible retained products of conception, or question/history of metastatic disease. Non-obstetrical pelvic sonograms may be medically necessary if there is an indication of vaginal bleeding or irregular menstrual cycles. It may be necessary to contact the ordering physician for medical necessity information. BENEFITS & LIMITATIONS 8-6
36 8200. Updated 05/07 Obstetrical Pelvic Sonograms: Routine obstetrical sonograms for a normal pregnancy are not covered. Primary diagnosis shall support medical necessity for an OB sonogram. Some examples are: indication of vaginal bleeding, multiple birth, diabetes, size/date discrepancy, fetal anomalies, threatened abortion, placental/uterine abnormalities, fetal demise, or maternal drug/alcohol/tobacco use; history of previous miscarriage, Cesarean Section, stillbirth, ectopic pregnancy, eclampsia, or intra-uterine growth retardation. Medical necessity may also be determined based on maternal age, maternal weight or fetal position. If applicable, this information should be submitted with the claim. It may be necessary to contact the ordering physician for medical necessity information. A biophysical profile will not be reimbursed when a complete OB sonogram has been billed for the same date of service. Upper Gastrointestinal Series: Upper Gastrointestinal (UGI) series, which require precertification, are medically necessary if the primary diagnosis indicates persistent dysphagia, melena, symptoms of UGI tract bleeding or signs and symptoms of ulcers affecting the UGI tract after a trial of medicinal therapy has failed to relieve the symptoms. State guidelines allow one UGI series per day, per beneficiary, regardless of provider. UGI series may also be medically necessary when diagnoses such as abdominal pain and dyspepsia are used. When these common non-specific diagnosis codes are used, additional symptoms and/or circumstances that relate to the medical necessity of the procedure must be indicated. Examples of additional information which will assist in adjudication of your claim are as follows: Is the symptom persistent? If so, how long has the symptom persisted? Is the symptom recurrent? When was the last episode? Has the symptom or condition increased in severity? Was medicinal therapy initiated prior to any procedure being performed? If so, indicate the date each therapy was initiated, name(s) of medication (list all GI related medications tried) and the length of time each medication was tried. What was the patient's response to each treatment? If a chronic condition, has there been a change in symptoms? If so, describe the change(s). If cancer diagnosis codes are used, what symptoms are present that indicate UGI involvement? Claims for UGI X-rays are denied reimbursement when the diagnosis code on the claim is either too non-specific or is the result, rather than the reason, for the procedure. Whenever possible, use the symptoms that most clearly describe the reason for the test. It may be necessary to contact the ordering physician for medical necessity information. BENEFITS & LIMITATIONS 8-7
37 8200. Updated 3/06 Emergency Room/Department (Outpatient Hospital): General Information: The State of Kansas defines emergency services as follows: KAR (42) "Emergency services are those services provided after the sudden onset of a medical condition manifested by symptoms of sufficient severity, including severe pain, that the absence of immediate medical attention could reasonably be expected to result in placing the patient's health in serious jeopardy, serious impairment of bodily functions, or serious dysfunction of any bodily organ or part." KAR (b) (4) "Services provided in the Emergency Department shall be emergency services." Emergency status is determined based on conditions relating to the emergency visit, not the patient's age and time of admission to the emergency department. Emergency department claims are limited to one visit per consumer, per date of service unless accompanying documentation verifies the necessity for more than one emergency room/department visit. Direct physical attendance by a physician or mid-level practitioner is required in "emergency" situations. If the physician or mid-level practitioner has not made entries on the record other than his/her signature and/or diagnosis and documentation does not indicate that he/she had examined the patient, the visit will not be considered emergent. Phone or standing orders do not support emergency treatment. Axillary temperatures are not considered accurate and will be disregarded when determining emergent status. Consumers may go to the emergency room without a referral from their physician based on the definition of an emergency according to a prudent layperson (as defined by the Balanced Budget Act, 1997): What a layperson would consider an emergency in the absence of medical knowledge. Such an emergency could include, but is not limited to: serious impairment to bodily functions; serious dysfunction of any bodily organ or part; severe pain; or an injury/illness that places the health of the individual in serious jeopardy (and in the case of a pregnant woman, her health or that of her unborn child). Other Examples of Emergencies are: o Initial treatment for medical emergencies including indications of severe chest pain, dyspnea, gastrointestinal hemorrhage, spontaneous abortion, loss of consciousness, status epilepticus or other conditions considered "life-threatening." o Patients who require transfer to another facility for further treatment or who expire. BENEFITS & LIMITATIONS 8-8
38 8200. Updated 3/06 Non-Emergent Situations: o Intentional non-compliance with previously ordered medications and treatments resulting in continued symptoms of the same condition. o Refusal to comply with currently ordered procedures/treatments such as drawing blood for laboratory work. o Leaving the emergency room against medical advice. o Scheduled visits to the emergency room for procedures, examinations or medication administration. Examples include cast changes, suture removal, dressing changes, follow-up examinations and second opinion consultations. o Visits made to receive a "tetanus" injection in the absence of other emergent conditions. o Visits made to obtain medication(s) in the absence of other emergent conditions. The following conditions will not be considered emergent unless the criteria described has been met: Alcoholism in and of itself is considered nonemergent unless documentation supports an emergent status (i.e., gastric bleeding or coma/stupor). Ambulance: A patient brought in by ambulance does not necessarily justify an emergency room visit. Guidelines for Use of Air Ambulance Services: Time: If time is a critical factor in the patient s recovery or survival, or duration of ground transport would be excessive and potentially detrimental, air transport may be indicated. In general, if the ground ambulance can arrive at the destination institution within 20 minutes, it is the preferred mode of transport. Expertise: If the health care institution does not possess the expertise to provide the definitive care required to stabilize the patient (i.e., advanced life support) and the ground ambulance providers in the near vicinity cannot provide assistance in providing that care, air transport may be indicated. Coverage: If ground ambulance utilization leaves the service area without adequate ground coverage and patient outcome will be compromised by arranging other ground transport, air transport may be indicated. Documentation: The above guidelines serve as a guide to documentation which is necessary to determine proper reimbursement and must specify the indication and justification for air transport. If guidelines are not met, or are met but not documented, the billed transportation will be reimbursed at ground ambulance rates or denied altogether. Depression/Anxiety: Documentation must support the individual to be an immediate danger to self or others. BENEFITS & LIMITATIONS 8-9
39 8200. Updated 3/06 Disposition: If a patient's disposition is one of the following, the visit would be considered emergency: a) requires transfer to another facility for further treatment, b) has expired, expires enroute to the hospital or in the emergency room, c) requires extended observation or admission. Fevers must be considered with other documented symptoms. Generally, temperatures less than 103 rectally (children) or 102 orally (adults) are not considered emergent. Ear and axillary temperatures will be considered along with additional symptoms. Reported temperatures by patients are not acceptable for determining emergent status. Insect Bites, Stings, Embedded Ticks: Minor insect bites (tick) with simple local reactions only (i.e., erythema, local edema, itching) are not considered emergent. Medical Emergency: Initial treatment and/or stabilization for medical emergencies including indications of severe chest pain, dyspnea, gastrointestinal hemorrhage, spontaneous abortion, loss of consciousness, status epilepticus or other conditions considered "life-threatening" would be considered emergent. Just because these conditions may be considered "lifethreatening" at times, does not automatically indicate a Level of Care III. The Level of Care assignment is dependent upon the severity of the situation and the services provided. Mental Disorders such as depression or anxiety as an individual diagnosis is considered nonemergency unless the patient is noted to be suicidal or of immediate risk to self or others. Minor Burns/Sunburns: Minor burns/sunburns are considered nonemergent unless documentation supports the presence of complications such as severe swelling, infection, or the young age of the patient. Eye and chemical burns are considered emergent. Otitis Media: If tympanic membrane is bulging or ruptured, drainage from the ear(s), fever of 103 or above or is a child of age 3 or under and is crying inconsolably, a visit to the emergency room would be considered emergent for consideration of otitis media. If the physical examination reveals evidence of acute otitis media (after office hours or on the weekend), but does not meet any of the above criteria, the ED visit may be considered emergent because of the time of day/week. Patient Non-Compliance: Intentional non-compliance with previously ordered medications and treatments resulting in continued symptoms of the same condition are considered nonemergent. Refusal to comply with currently ordered procedures/treatments such as drawing blood for laboratory work will also be considered nonemergent. BENEFITS & LIMITATIONS 8-10
40 8200. Updated 3/06 Removal of Cutaneous Foreign Bodies: Removal of cutaneous foreign bodies (i.e., simple splinters, cactus needles) are considered nonemergent unless sedation or the use of extensive medical supplies such as cutdowns are required. Seizures are considered emergent when: a) this is an initial seizure b) there is a secondary diagnosis noted (i.e., infection or headache) c) the patient is 12 years old or younger d) the seizure is still in progress or status epilepticus e) this is a febrile seizure f) the condition is aggravated by alcohol/drug ingestion g) this is a previously undiagnosed condition Scheduled Visits: Scheduled visits to the emergency department for procedures, examinations or medication administration (i.e., cast changes, suture removal, dressing changes, follow-up examinations and second opinion consultations) are considered nonemergent. When a patient leaves the emergency department against medical advice (AMA) the service is generally considered nonemergent. However, if the facility provided considerable services before the patient left AMA, the visit will be given consideration as emergent. Sickle Cell Anemia: If a person has sickle cell anemia and presents with suspicion of an infectious or hypoxic process, or complains of pain, the visit may be considered emergent. Skin Rash/Hives: Documentation must support presence of systemic complications beyond the local skin discomforts resulting from the rash. If the rash causes eye complications or the beneficiary has a history of anaphylactic (allergic) reactions, the visit is considered emergent. If the rash causes eye edema or impairment to eye function and the visit is over a weekend when there is no access to a physician's office, the visit may be considered emergent. A history of anaphylaxis along with the rash is considered emergent. Trauma/Injury: Recent trauma or injury is considered emergent. Recent is defined as an injury occurring within 48 hours prior to the emergency room visit. Minor abrasions/lacerations not requiring suture or other injuries not requiring treatment are not emergent. If the injury is older than 48 hours and symptoms have deteriorated to the point of requiring emergency care, consider as emergent. BENEFITS & LIMITATIONS 8-11
41 8200. Updated 3/06 An injury that requires only simple first aid treatment that can be done in the home (such as cleansing and/or bandaging an abrasion) is not considered emergent. A laceration requiring steri-strips indicates a gaping wound and would be considered emergent. X-rays do not define the level of care. Tetanus Injection: A tetanus injection is not considered emergent, and does not change the visit to emergent. However, the patient should not have to make two visits (one to the emergency room and one to an office or public health department) in order to receive the tetanus injection. When needed, a tetanus injection should be given within hours of the injury, if possible. Time of Visit: The time of the visit is a consideration in determining emergent vs. nonemergent status. If the condition require immediate attention and it is after office hours, a weekend, or holiday, consider as emergent. If a patient is brought in by the police at any time, consider as emergent. If a patient had previously been in the same or different emergency department or physician's office for the same condition and the condition has not worsened, the visit will be considered nonemergent. Vital Signs: If the vital signs are outside a reasonable range for the age, consider the visit as emergent (see "fever"). Emergency Department/Room Guidelines for E&M Codes: History: The age of a patient is a component of every medical record. Documentation of age in relationship to issues such as antisocial behavior or mental status is important; however, age alone is not considered a social history. Examination: A "comprehensive exam" is considered a "hands on" specialist examination. Telephone consultation with a specialist is not the equivalent of comprehensive exam (per Dr. Aaron Primack, HCFA/AMA consultant). Medical Decision Making: Transfers from the emergency department to another facility for additional care should be considered in management options as either the "new problem, additional work-up" or the category of "established problem, worsening" (per Dr. Aaron Primack, HCFA/AMA consultant). A vascular examination is included in the cardiovascular category. BENEFITS & LIMITATIONS 8-12
42 8200. Updated 3/06 A notation that the patient should "follow-up" with his family physician in the morning or return to the physician's office for stitch removal does not justify use of the "additional workup" statement when considering management options (per Dr. Aaron Primack, HCFA/AMA consultant). In evaluating the "Table of Risk", infection is the usual risk that pops into mind when talking about minor surgery. To consider infection as a "risk" from minor surgery, there must be documentation to support increased risk due to the quality or condition of the injury or illness (per Dr. Aaron Primack, HCFA/AMA consultant). "Self-limited/minor problems" are defined as those representative of basic emergency department care such as lacerations, stings, insect bites (per Dr. Aaron Primack, HCFA/AMA consultant). "New problems with or without additional work-up" is defined as representing new, longstanding problems that will need attention again at some time (per Dr. Aaron Primack, HCFA/AMA consultant). Observation Room: Observation in the outpatient setting is a service which requires monitoring the patient's condition beyond the usual amount of time in an outpatient setting. Examples of the appropriate use of the observation room include: monitoring head trauma, drug overdose, cardiac arrhythmias and false labor. A physician or mid-level practitioner must see the patient within two hours prior to admission to the observation room except for obstetrical labor or scheduled administration of IV medication or blood products. The observation room stay must be medically necessary. There is no time limit restriction for the observation room. The same reimbursement rate applies regardless of the number of hours required for monitoring. This reimbursement is all inclusive of services and supplies. If there is a discharge and readmission to the observation room from midnight to midnight, only one reimbursement rate will be allowed. Observation room is content of service of a minor surgery. ER physician fee, non-scheduled fetal oxytocin stress tests and fetal non-stress tests are content of service of the observation room. Additional reimbursement for these services will not be made. Observation room should not be billed for the following: o Recovery room services following inpatient or outpatient surgery. o Recovery/observation following scheduled diagnostic tests such as arteriograms, cardiac catherization, etc. o Scheduled fetal oxytocin stress tests and fetal non-stress tests. BENEFITS & LIMITATIONS 8-13
43 8200. Updated 3/06 NOTE: Additional information may be added to the face of your claim if applicable. Tape billers who have had initial billings denied with EOB 548 (Service denied. This claim and all attachments have been reviewed by the medical staff and the medical necessity of the service rendered is not supported by the documentation provided. Refer to the provider manual section 8200 for further discussion.), may resubmit a paper claim with the applicable documentation noted on the face of the claim. If the claim and/or attachments do not support the medical necessity of the service rendered, the service will be denied. BENEFITS & LIMITATIONS 8-14
44 8300 Benefit Plan Updated 11/03 BENEFITS AND LIMITATIONS Kansas Medical Assistance beneficiaries will be assigned to one or more Medical Assistance benefit plans. The assigned plan or plans will be listed on the beneficiary ID card. These benefit plans entitle the beneficiary to certain services. From the provider's perspective, these benefit plans are very similar to the type of coverage assignment in the previous MMIS. If there are questions about service coverage for a given benefit plan, contact the Medical Assistance Customer Service Center at or (785) For example all policies and coverages under the current Medicaid Program apply to the MediKan benefit plan except: Inpatient general hospital services are covered for MediKan consumers for the following conditions only: Alcohol and Drug Detoxification Burns Mental Health Severe Traumatic Injuries Tuberculosis DRGs for covered inpatient hospital services are , , and 447. Additional DRGs are covered when the hospital admission is related to tuberculosis and a TB diagnosis is billed on the claim. Claims for MediKan consumers that group to any of the following DRGs will be reviewed: 002, 217, 443, , 472, Coverage determination is based on the nature of the injury indicated by the diagnosis on the claim. Psychiatric Admissions: The only psychiatric services covered are those for acute psychotic episodes. Inpatient psychiatric admissions to acute care general and specialty hospitals are covered only after a psychiatric preadmission assessment has been completed and a determination made that the most appropriate treatment setting is the hospital. Only the following diagnosis codes are covered for MediKan consumers: Coverage determinations are based on the emergent nature of the service. BENEFITS & LIMITATIONS 8-15
45 BENEFITS AND LIMITATIONS MEDICAID - INPATIENT/OUTPATIENT Updated 11/03 Enrollment: Hospitals must sign a Hospital/Peer Review Organization Agreement with the Utilization Review Contractor before becoming enrolled as a Kansas Medical Assistance provider. Change of Ownership: Each hospital must notify the Adult and Medical Services, SRS, in writing at least 60 days prior to the change of ownership closing transaction date. Failure to do so may result in: 1) the forfeiture of rights to payment for covered services provided to consumers by the previous owner or owners in the 60-day period prior to the effective date of the change of ownership; and 2) the new owner or owners assuming responsibility for any overpayment made to previous owner(s) before the effective date of the change of ownership. (This shall not release the previous owner of responsibility for such overpayment.) The new owner (and affiliated providers) must apply for a Medicaid provider number through the Adult and Medical Services by contacting: Department of Social and Rehabilitation Services Adult and Medical Services, Medical Programs The Docking State Office Building, 6th Floor 915 S.W. Harrison Topeka, Kansas The new owner will receive the full reimbursement for any patients admitted before and discharged after the change of ownership effective date. The old owner shall not receive Medicaid payment for these services. Advance Directives: Hospital providers participating in the Kansas Medical Assistance Program must comply with federal legislation (OBRA 1990, Sections 4206 and 4751) concerning advance directives. An "advance directive" is otherwise known as a living will or durable power of attorney. Every hospital provider must maintain written policies, procedures and materials about advance directives. Specific Requirements 1. Each hospital must provide written information to every adult individual receiving medical care by or through the hospital. This information must contain: the individual's right to make decisions concerning his or her own medical care. - the individual's right to accept or refuse medical or surgical treatment. BENEFITS & LIMITATIONS 8-16
46 8400. Updated 11/03 - the individual's right to make advanced directives. - the Department of Social and Rehabilitation Services' "Description of the Law of Kansas Concerning Advance Directives." SRS does not provide copies of the description to providers. It is up to providers to reproduce the description. Providers are free to supplement this description as long as they do not misstate Kansas law. 2. Additionally, each hospital must provide written information to every adult individual about the hospital's policy on implementing these rights. 3. A hospital must document in every individual's medical record whether the individual has executed an advance directive. 4. A hospital may not place any conditions on health care or otherwise discriminate against an individual based upon whether that individual has executed an advance directive. 5. Each hospital must comply with State law about advance directives. 6. Each hospital must provide for educating staff and the community about advance directives. This may be accomplished by brochures, newsletters, articles in the local newspapers, local news reports or commercials. Incapacitated Individuals An individual may be admitted to a facility in a comatose or otherwise incapacitated state, and be unable to receive information or articulate whether he or she has executed an advance directive. If this is the case, families of, surrogates for, other concerned persons of the incapacitated individual must be given the information about advance directives. If the incapacitated individual is restored to capacity, the hospital must provide the information about advance directives directly to him or her even though the family, surrogate or other concerned person received the information initially. If an individual is incapacitated, otherwise unable to receive information or articulate whether he or she has executed an advance directive, the hospital must note this in the medical record. Mandatory Compliance with the Terms of the Advanced Directive When a patient, relative, surrogate or other concerned/related person presents a copy of the individual's advance directive to the hospital, the facility must comply with the terms of the advance directive to the extent allowed under State law. This includes recognizing powers of attorney. BENEFITS & LIMITATIONS 8-17
47 8400. Updated 11/03 Description of the Law of Kansas Concerning Advance Directives: There are two types of "advance directives" in Kansas. One is commonly called a "living will" and the second is called a "durable power of attorney for health care decisions." The Kansas Natural Death Act, K.S.A ,106, et seq. This law provides that adult persons have the fundamental right to control decisions relating to their own medical care. This right to control medical care includes the right to withhold life-sustaining treatment in case of a terminal condition. Any adult may take a declaration which would direct the withholding of life-sustaining treatment in case of a terminal condition. Some people call this declaration a "living will." The declaration must be: 1. In writing; 2. Signed by the adult making the declaration; 3. Dated; and 4. Signed in front of two adult witnesses, or notarized. There are specific rules set out in the law about the signature in case of an adult who can't write. There are specific rules about the adult witnesses. Relatives by blood or marriage, heirs, or people who are responsible for paying for the medical care may not serve as witnesses. A woman who is pregnant may not make a declaration. The declaration may be revoked in three ways: 1. By destroying the declaration; 2. By signing and dating a written revocation; and 3. By speaking an intent to revoke in front of an adult witness. The witness must sign and date a written statement that the declaration was revoked. Before the declaration becomes effective, two physicians must examine the patient and diagnose that the patient has a terminal condition. The desires of a patient shall at all times supersede the declaration. If a patient is incompetent, the declaration will be presumed to be valid. The Kansas Natural Death Act imposes duties on physicians and provides penalties for violations of the laws about declarations. BENEFITS & LIMITATIONS 8-18
48 8400. Updated 11/03 The Kansas Durable Power of Attorney for Health Care Decisions Law, K.S.A , et seq. A "durable power of attorney for health care decisions" is a written document in which an adult gives another adult (called an "agent") the right to make health care decisions. The power of attorney applies to health care decisions even when the adult is not in a terminal condition. The adult may give the agent the power to: 1. Consent or to refuse consent to medical treatment; 2. Make decisions about donating organs, autopsies, and disposition of the body; 3. Make arrangements for hospital, nursing home, or hospice care; 4. Hire or fire physicians and other health care professionals; or 5. Sign releases and receive any information about the adult. A "durable power of attorney for health care decisions" may give the agent all those five powers or may choose only some of the powers. The power of attorney may not give the agent the power to revoke the adult's declaration under the Kansas Natural Death Act ("living will"). The power of attorney only takes effect when the adult is disabled unless the adult specifies that the power of attorney should take effect earlier. The adult may not make a health care provider treating the adult the agent except in limited circumstances. The power of attorney may be made by two methods: 1. In writing; 2. Signed by the adult making the declaration; 3. Dated; 4. Signed in front of two adult witnesses; Or: Written and notarized. Relatives by blood or marriage, heirs, or people who are responsible for paying for the medical care may not serve as witnesses. The adult, at the time the power of attorney is written, should specify how the power of attorney may be revoked. BENEFITS & LIMITATIONS 8-19
49 8400. Updated 02/07 The Patient Self-Determination Act, Section 1902(w) of the Social Security Act This federal law, codified at 42 U.S.C. Sec. 1396a(w), was effective December 1, It applies to all Medicaid and Medicare hospitals, nursing facilities, home health agencies, hospices, and prepaid health care organizations. It requires these organizations to take certain actions about a patient's right to decide about health care and to make advance directives. This law also required that each state develop a written description of the State law about advance directives. This description was written by the Health Care Policy Section of the Kansas Department of Social and Rehabilitation Services to comply with that requirement. If you have any questions about your rights to decide about health care and to make advance directives, please consult with your physician or attorney. Third Edition: January 14, 2003 Abortions: Abortions are covered only under the following conditions: In the case where a woman suffers from a physical disorder, physical injury, or physical illness, including a life-endangering physical condition caused by or arising from the pregnancy itself. If the pregnancy is the result of an act of rape or incest. The physician must complete the abortion necessity form below to certify that the woman's physical health is in danger, or that this pregnancy is a result of rape or incest. A copy of the form can be found in the forms section at the end of this manual. The form, located at the end of this manual in the Forms section, Abortion_necessity_form, or on the Provider Web site under Publications/Forms/Abortion necessity form may be photocopied for your use. All blanks must be completed, including the patient's complete address. Claims submitted for abortions due to rape or incest must be accompanied by a statement signed by the physician stating that he/she was informed by the patient that the pregnancy was the result of rape or incest. No further documentation is required to process the claim. However, all pertinent information must be retained with the medical record. Children and Family Services (CFS) Contractors: Medicaid reimbursable services will not be paid by child welfare contractors. All services for children assigned to contractors, including behavior management and mental health, must be billed directly to the Kansas Medical Assistance Program and will be reimbursed at the approved Medicaid rate. Prior authorization and other restrictions apply. Refer to Section 2900 of your General Provider Manual for an all-inclusive list of the categories of service covered under the CFS contract. BENEFITS & LIMITATIONS 8-20
50 8400. Updated 09/07 Immunization/Vaccine: Reimbursement for covered immunizations for children is limited to the administration of the vaccine only. Vaccines are supplied at no cost to the provider through Vaccines for Children, a federal program administered by the Kansas Department of Health and Environment. Intrathecal Baclofen Pump: Intrathecal baclofen pumps are covered for Medicaid beneficiaries. This includes the initial and all subsequent implantation(s), revision(s), repairs, catheters, batteries, refills, removals, and maintenance of the intrathecal baclofen pumps when indicated. Three services require prior authorization, 62350, 62351, and The following conditions must be met: The beneficiary must have responded favorably to a trial of intrathecal baclofen and documentation of previously used medication The beneficiary s ICD diagnosis code must be a covered code and the source of the spasticity must be documented The beneficiary must be over the age of four years or there must be documentation that there is sufficient space within the child s chest wall for the pump to be implanted. Contraindications include pregnancy and active infection at time of surgery Procedure codes 62311, 62319, 62355, 62365, 95990, 95991, and do not require PA but HealthConnect beneficiaries do need a referral from their PCPs. Renal Dialysis and Kidney Transplant: When it has been determined a beneficiary has chronic renal disease (CRD) requiring renal dialysis, the beneficiary or his representative should apply for Medicare CRD eligibility. Medicare allows for payment of claims for eligible beneficiaries with chronic renal disease and will reimburse for maintenance dialysis the third month after the maintenance dialysis starts. Medicare will reimburse for maintenance dialysis in the first three months if the beneficiary has been involved in self training in a self-care dialysis unit or through a self-care home dialysis support service provided by a qualified provider. They also reimburse for expenses incurred for a kidney transplant including those for the kidney donor. Medicaid will reimburse claims for services related to chronic renal dialysis and/or kidney transplants only after proof has been attached to one claim that the beneficiary has applied for Medicare and coverage has been approved or denied. The Medicare CRD eligibility information will be retained in the claims processing system. Therefore, subsequent claims do not need to have proof of Medicare CRD eligibility approval or denial attached. Acceptable proof of application and coverage or denial by Medicare are: Medicare EOMB/RA Beneficiary Health Insurance Card Report of Confidential Social Security Benefit Information Letter from Medicare or Social Security explaining that the beneficiary has applied for Medicare and whether beneficiary is eligible BENEFITS & LIMITATIONS 8-21
51 8400. Updated 09/07 Hospitals Qualifying For Federal Renal Program: Univ. of Kansas Med. Center St. Francis Regional Med. Center 39th & Rainbow Boulevard 929 North St. Francis Kansas City, Kansas Wichita, Kansas St. Luke's Hospital Research Hospital & Medical Ctr. 44th and Wornall Road Meyer Boulevard & Prospect Kansas City, Missouri Kansas City, Missouri St. Francis Hosp. & Health Center* Humana Hospital Dodge City* 1700 West Seventh Street Dodge City, Kansas Topeka, Kansas Children's Mercy Hospital Kansas City Dialysis & Training 24th at Gillham Road Center* Kansas City, Missouri Located at Research Hospital (CAPD Training & Support Services) Meyer Boulevard & Prospect Kansas City, Missouri Salina Regional Health Center 400 S. Santa Fe Salina, Kansas FOR VETERANS: Kansas City V.A. Hospital Wichita V.A. Hospital 4801 Linwood Boulevard 5500 East Kellogg Kansas City, Missouri Wichita, Kansas * Approved for dialysis only BENEFITS & LIMITATIONS 8-22
52 8400. Updated 09/07 Surgery - Ambulatory/Outpatient: Ambulatory surgery centers and outpatient hospitals will be reimbursed for multiple unrelated outpatient surgical procedures performed on the same day as follows: 100% of the current Medicaid rate for the highest value procedure; 50% of the current Medicaid rate for the second procedure; and 25% of the current Medicaid rate for all subsequent procedures. IV's, medications, supplies and injections provided on the same day as an ambulatory/outpatient surgery procedure are considered content of service of the surgery and cannot be billed separately. EXCEPTION: The following thrombolytic enzymes are not considered content of service when billed in conjunction with outpatient surgery: Alteplase- J2997, Reteplase-J2993, Urokinase-J3364, Streptokinase-J2995, and Anistreplase-J0350. Anesthesia (equipment and supplies), drugs, surgical supplies and other equipment of the operating room and the recovery room are considered content of service of the ambulatory/outpatient surgical procedure. Surgery - Breast Reconstruction: Breast reconstruction is covered when the beneficiary had a mastectomy for breast cancer on or after March 1, Only the breast reconstruction procedure codes listed in Appendix II are covered. This coverage is limited to one breast reconstruction process per breast per lifetime. Surgery - Cosmetic: All surgeries which are cosmetic in nature (and related complications) are not covered. Any medically necessary procedure which could ever be considered cosmetic in nature must receive prior authorization (PA). The hospital must have a copy of the physician's PA for claim processing purposes. Surgery - Elective: The Medicaid program will not reimburse for inpatient/outpatient elective surgery unless the beneficiary is a KAN Be Healthy participant. Certain surgical procedures will be reviewed on a post-pay random sample basis by the KHPA physician. Retain all documentation supporting the non-elective nature of the surgery for review. Supporting documentation includes admission notes/history and physical, operative report and pathology report. If the documentation does not support the non-elective nature of the surgery, reimbursement for all claims relating to the surgery will be recovered. Therapy: Therapy treatments are not covered for a psychiatric diagnosis. Habilitative - Therapy is covered for any birth defects/developmental delays only when approved and provided by an Early Childhood Intervention (ECI), Head Start or Local Education Agency (LEA) program. Therapy treatments performed in the Local Education Agency (LEA) settings may be habilitative or rehabilitative for disabilities due to birth defects or physical trauma/illness. Therapy of this type is covered only for participants age 0 to under the age of 21. Therapy must be medically necessary. The purpose of this therapy is to maintain maximum possible functioning for children. BENEFITS & LIMITATIONS 8-23
53 8400. Updated 09/07 Rehabilitative - All therapies must be physically rehabilitative. Therapies are covered only when rehabilitative in nature and provided following physical debilitation due to an acute physical trauma or physical illness and prescribed by the attending physician. Therapy services are limited to 6 months for non-kan Be Healthy participants (except the provision of therapy under HCBS), per injury, to begin at the discretion of the provider. There is no limitation for KAN Be Healthy participants. Effective with dates of service on and after December 1, 2006, providers of rehabilitative therapy can submit claims with a combination of the following rehabilitation therapy procedure codes and a diagnosis code in the range of V57.0-V57.9 as the primary diagnosis. Providers are required to submit a secondary diagnosis code to describe the origin of the impairment for which rehabilitative therapy is needed when one of these V-codes is billed as a primary diagnosis Transplants: Liver transplants for Medicaid beneficiaries will only be reimbursed at the University of Kansas Medical Center or at a hospital recommended by their staff. Heart, lung, and heart/lung transplants performed in approved in-state or border city hospitals are covered for KAN Be Healthy participants only. Heart transplants will be allowed at St. Luke's Hospital in Kansas City, Missouri or Via Christi (St. Francis Campus) in Wichita, Kansas, or at a hospital recommended by either of these facilities. Bone marrow, cornea, kidney, and pancreas transplants performed in approved in-state or border city hospitals are covered and do not require prior authorization. Pancreas transplants are only covered when performed simultaneously with or following a kidney transplant. Tuberculosis: Inpatient services related to a tuberculosis diagnosis, including physician and laboratory services, are covered for beneficiaries with the TB benefit plan. Inpatient hospitalization, including physicians services for diagnostic evaluation of beneficiaries highly suspected of tuberculosis, is covered for completion of the diagnosis. BENEFITS & LIMITATIONS 8-24
54 8400. Updated 09/07 Tuberculosis continued: Acute problems, which are present on admission or arise during hospitalization, are covered services. Hospitalization for monitoring toxicity of anti-tuberculosis drugs is covered. Inpatient claims may be billed directly to KMAP. Coverage and payment of inpatient or outpatient services are subject to compliance with infectious disease reporting requirements as directed by K.A.R Coverage and payment of outpatient services are coordinated between Kansas Department of Health and Environment (KDHE) and KMAP in accordance with the current interagency agreement. Contact KDHE at (785) for determination of coverage. Anti-tuberculosis drugs to treat the beneficiary and family members are provided at no cost by KDHE. Contact your local health department or KDHE at (785) Vagal Nerve Stimulators: Vagal nerve stimulators (VNS) are covered for beneficiaries with epileptic disorders. With the exception of procedure codes and 95974, all services must be prior authorized VNS services must meet the following conditions: The beneficiary must have an epileptic disorder. VNS will not be covered for individuals with previous epileptic brain surgery or individuals with progressive disorders. Mental retardation with epilepsy is not a contraindication for VNS but must be considered with other factors. The beneficiary must be over the age of 12, with documentation showing that the VNS will improve quality of life. All other courses of treatment must be documented, such as conventional and anticonvulsant drugs. Refer to Appendix II for a list of covered codes. Vacuum Assisted Wound Closure Therapy: Vacuum assisted wound closure therapy is covered for specific benefit plans. Prior authorization is required and criteria must be met. Refer to the KMAP DME Provider Manual for criteria For questions about service coverage for a given benefit plan, contact the KMAP Customer Service Center at or All prior authorization must be requested in writing by a KMAP DME provider. All medical documentation must be submitted to the KMAP DME provider. BENEFITS & LIMITATIONS 8-25
55 BENEFITS AND LIMITATIONS MEDICAID - INPATIENT ONLY Updated 09/07 General Hospital Reimbursement Policies: Payment for general inpatient hospital services is based on the following equation: DRG weight times (X) group payment rate plus (+) outlier costs, if appropriate. Medicaid does not reimburse for days not medically necessary or deemed "not payable" by federal or state laws, regulations, or state policy. All DRGs have the potential for day or cost outliers. When a stay is eligible for both day and cost outliers, the greater of the two is paid. Only day outlier payment is made for hospitalization extending beyond 360 days. If a Medicaid beneficiary is transferred from one hospital to another, the transferring hospital will receive outlier payments when the length of stay is greater than the DRG day or cost outlier. The hospital billing the final discharge receives the standard DRG payment including outliers, if applicable. When a Medicaid beneficiary is discharged prematurely and subsequently readmitted within 30 days, only the DRG payment for the first stay will be made if the discharging and readmitting hospital are the same. If the discharging and readmitting hospitals are not the same, only the readmitting hospital will be reimbursed. When the Medicaid beneficiary is not eligible for the entire inpatient stay, the DRG payment is prorated and reimbursement is made only for the days the beneficiary was eligible. Reimbursement shall not exceed the standard DRG payment plus any applicable outlier payment. (Only covered days are used to calculate outliers.) Hospitals can issue a continued stay denial to a beneficiary only after the attending physician has written a discharge order. The hospital must supply the beneficiary with the necessary notification that the beneficiary will assume responsibility for payment since a continued stay is not considered medically necessary and is no longer a covered service. Admissions or day outliers found to be unnecessary by the utilization review contractor cannot be billed to the beneficiary. BENEFITS & LIMITATIONS 8-26
56 8410. Updated 09/07 Dental Admissions: Dental admissions are covered when medically necessary. Documentation supporting the medical or dental condition making hospitalization necessary must be in the medical record. Prior authorization is required for adults. Medical review is required for children age 21 and under. Claims for this service are to be billed with procedure code and must include a detailed description of the actual service provided. Emergency Renal Dialysis: Emergency renal dialysis (revenue code 809) is only allowed once in an 18 month period per beneficiary. State Institutions for Mental Health: State institution services are only covered for Medicaid beneficiaries under 21 years of age, or 65 years of age and older. (However, if a beneficiary is an inpatient in a state institution on their 21st birthday, state institution services will be covered until the age of 22.) State institutions are reimbursed 100% of the amount billed. Long-Term Care Units: Long-term care units must be a distinct or separate unit of a hospital certified to provide skilled and/or intermediate care under the Kansas Medical Assistance Program subject to the same federal and state rules and regulations as a free-standing adult care home. This includes compliance with federal regulations for standards of care and related reimbursement. Non-Covered Services: Take home drugs. Non-medical hospital supplies (e.g., hospital kits). Psychiatric: A psychiatric preadmission assessment is not required for inpatient medical treatment when the admission was the result of a medical manifestation of a psychiatric disorder and the beneficiary was not admitted to the psychiatric unit. Inpatient general hospital psychiatric admissions are covered only after a psychiatric preadmission assessment has been completed and a determination made that the most appropriate treatment setting is the hospital. [As required by Mental Health Reform, Community Mental Health Centers (CMHCs) review all admissions to state hospitals.] No payment will be made for the hospital admission or related physician services without the completion of the preadmission assessment and determination that the hospital admission meets criteria. When seeking to admit a Kansas Medical Assistance Program beneficiary for inpatient treatment call to arrange for the assessment to be completed. This toll free number is staffed 24 hours a day by the Mental Health Consortium (MHC). BENEFITS & LIMITATIONS 8-27
57 8410. Updated 09/07 All individuals, determined by the hospital, to be potentially eligible for Kansas Medical Assistance Program benefits must have a psychiatric preadmission assessment performed prior to admission into an acute care general or special hospital. The following criteria is a guideline that should assist hospitals in determining which individuals are potential candidates for Kansas Medical Assistance Program benefits: Individuals receiving Supplemental Security Income (SSI) or have applied for SSI, Individuals on Social Security, Individuals who have been unemployed longer than six months, Individuals who have applied or will be applying for Kansas Medical Assistance Program. After receiving a request for a psychiatric preadmission assessment the MHC will contact the appropriate CMHC, or other approved provider if the admission is out of state, to complete the assessment face-to-face with the patient. The hospital and admitting physician will be notified of the results verbally and via a letter from the MHC. If the admission is approved a prior authorization (PA) number will be included in the letter for the hospital to utilize when billing for the admission and related services. A referral from the beneficiary's primary care provider is not required for a psychiatric hospital stay or related physician and ancillary services provided during the psychiatric hospitalization approved through the preadmission assessment process. Free Standing Psychiatric Hospitals: Federal regulations classify free standing psychiatric hospitals as Institutions for Mental Disease (IMDs). Medicaid reimbursement to IMDs is restricted to treatment of beneficiaries 20 years of age and younger, or 65 and older. Even though an admission may be authorized by a pre-admission screening, Medicaid reimbursement to free standing psychiatric hospital providers (with a specialty of B3) will be made only for beneficiaries under the age of 21, or 65 and older at admission. Emergency Psychiatric: Screening for inpatient services following the sudden onset of severe psychiatric symptoms, which could reasonably be expected to make the individual harmful to self or others if not immediately under psychiatric care. The individual is in crisis and not currently in a place of safety. A screening is completed immediately (no later than 3 hours) to determine appropriate placement. Urgent Psychiatric: Screening is initiated if the individual meets one of the four independent criteria and is currently in a place of safety. An observation bed may be used to provide security and observation for individuals in imminent danger and to assist in the determination of the need for psychiatric hospitalization. In this instance, the screening must be completed as soon as possible and within two (2) days of the Consortium s receipt of the request. BENEFITS & LIMITATIONS 8-28
58 8410. Updated 09/07 Planned Psychiatric: Noncrisis in nature, the screening must be completed within two (2) days of the Consortium s receipt of the request. The admission must occur within two (2) days of the completion of the screening. Retroactive Psychiatric: Individuals whose Medicare or other primary insurance denied payment for treatment, and who were Medicaid eligible at the time of admission. Other retroactive screens may be authorized for denied requests when eligibility is in question. If the individual receives a valid Medicaid card after a hospital admission has been completed, the Consortium requests the admission information, and completes a pre-admission screening within five (5) working days of the receipt of that information. Cases Involving Retroactive Eligibility: The assessment must be requested and completed prior to the admission and related services being billed to Medicaid. The assessment will not be face-to-face and will be completed by the MHC. The MHC must complete the assessment within five (5) working days of receiving the request. Cases Involving Other Insurance or Medicare: If the admission and related services are billed to other insurance or Medicare first, the psychiatric preadmission assessment is not necessary. If the other insurance or Medicare makes no payment on the claim, prior to the claim being billed to Medicaid, an assessment must be completed. The MHC will complete the assessment within five (5) working days of receiving the request. The assessment will not be face-to-face. A face-to-face psychiatric preadmission assessment consists of a psychiatric diagnostic interview examination including history, mental status examination, and communication with family members and other collateral contacts in order to develop an appropriate treatment plan. Placement problems for children in SRS custody: The SRS office suggests that efforts to make arrangements for placement in a state hospital or appropriate long-term care facility should begin as soon as the need for prolonged non-acute inpatient care becomes apparent. The local SRS office, the physician, or the hospital should contact the Adult and Medical Services for assistance in placement, if necessary. Please request this assistance by the 6-10th day of stay in an acute hospital. Substance Abuse: Acute detoxification is covered in any acute general hospital, when medically necessary. Alcohol and drug addiction treatment services provided in an inpatient hospital setting are not covered. BENEFITS & LIMITATIONS 8-29
59 8410. Updated 09/07 Utilization Review General Hospitals: Utilization review (UR) is performed on a postpayment basis for general hospitals with the exception of some readmissions, some interim bills and some adjustments. (Utilization reviews are performed internally at state institutions.) Review of outlier cases are conducted on all cases with day or cost outliers. Reviews are performed on a post-pay basis, unless interim bills are submitted and the beneficiary is still an inpatient. Readmissions within 30 days of a discharge are reviewed on a postpayment basis. All patient initiated transfers are subject to utilization review. When a patient is transferred from an inpatient hospital bed to a swing-bed unit and acute care continues to be provided, payment for the swing-bed will be denied or recouped. The only purpose for this type of transfer is for the hospital to obtain reimbursement beyond the DRG payment. Following DRG coding evaluation and adjustment by the UR contractor, payment of claims will be adjusted upward or downward. In this instance, the fiscal agent will initiate the adjustment. When a hospital admission is determined to be nonmedically necessary by the Medicaid utilization review contractor (KFMC), resulting in recoupment of payment, the provider shall not rebill the claim as an outpatient service. UR may be performed either on-site or by reviewing records sent as required to the UR contractor. If a hospital fails to provide the UR contractor with the complete requested information within the allowable time frames, the case will be denied, resulting in recoupment of payment. These "technical denials" are not eligible for reconsideration. If the facility supplies the UR contractor the information within 90 days of the "technical denial" date, the case may be reopened for review. Pending the review results, repayment for the case may occur. Discharge Day Not Medically Necessary: When a beneficiary's hospital discharge day is determined by the UR contractor to not be medically necessary, the discharge day is redefined as the last medically necessary day. This redefined discharge day is not reimbursed. BENEFITS & LIMITATIONS 8-30
60 BENEFITS AND LIMITATIONS MEDICAID - OUTPATIENT ONLY Updated 09/07 Emergency Medical Services for Aliens (SOBRA): In addition to inpatient hospital and emergency room hospital, emergency services performed in outpatient facilities and related physician, lab, and x-ray services will be allowed for the following places of service: office, outpatient hospital, Federally Qualified Health Clinics, state or local public health clinics, Rural Health Clinics, ambulance, and lab for SOBRA claims. Inpatient hospital reimbursement will not be limited to 48 hours. Follow-up care will not be allowed once the emergent condition has been stabilized. Blood: Refer to Section 2040 of the General Provider Manual for specific information. Blood transfusions, including whole blood, red blood cells, plasma, platelets and cryoprecipitate, and IV infusions are covered services. Set-ups including volume controller cassettes are content of service of the procedure billed. Crisis Resolution Services: Hospitals may be reimbursed when Medicaid patients are admitted to observation/stabilization beds for crisis resolution services in accordance with the following conditions: There is an affiliation agreement between the admitting hospital and the licensed community mental health center. The patient must be referred by the primary care case manager, agency, or health professional currently providing care (whichever is applicable). The patient shall have demonstrated an acute change in mood or thought that is reflected in behavior, indicating the need for crisis intervention to stabilize and prevent hospitalization. The patient must have a diagnosed psychiatric disorder. The patient shall not be in need of acute detoxification or experiencing withdrawal symptoms. The patient must be medically stable. The following documentation shall be completed: - nursing assessment (including physical review, mental status, and medication) - strength assessment - personal crisis plan, and - at least one progress note Crisis resolution services are covered up to two consecutive days and shall be billed under procedure code H2013. Developmental Testing Providers are reimbursed one visit per day, up to three visits per beneficiary per year for developmental testing: extended (which includes assessment of motor, language, social, adaptive, and/or cognitive functioning by standardized developmental instruments), with interpretation and report. The procedure code for this service is BENEFITS & LIMITATIONS 8-31
61 8420. Updated 03/08 Diagnostic Tests: Although not all HCPCS codes are covered, most procedure codes for laboratory, radiology, EKG, EEG, hearing and speech testing (if provided following physical debilitation) are covered. Drugs: All drugs are content of service of surgery. Oral drugs are content of service of emergency treatment. Take home drugs are noncovered. Injections, IVs, blood infusions, and aerosol inhalant additives are covered if not associated with surgery. Electro-Convulsive Treatments: Electro-convulsive treatments are covered and include all ancillary services needed to provide the treatment, including the charge for use of a bed. Emergency Room Services: Emergency room encounters will not deny based on ICD-9 diagnosis codes. Nonemergent claims will be reduced to the rate. Medical necessity documentation must accompany the claim when more than one ER visit is made on the same day for the same individual. The ER visit is content of service to any surgical and therapeutic treatment procedures performed in an emergency room. Laboratory: Handling fee (drawing/collection) is considered content of service of the outpatient visit/lab procedure and is not covered if billed separately. The beneficiary cannot be billed for the drawing or collection since it is considered content of another service or procedure. Laboratory procedures performed on inpatients are content of service of the DRG reimbursement to the hospital and should not be billed by either the independent laboratory or hospital. Pathologists not contracted by the hospital may bill the professional component (modifier 26) for pathology services provided on inpatients. Reimbursement will only be made for one complete blood count (CBC) per day. The Kansas Medical Assistance Program considers the following procedures to be component parts of a CBC. Refer to the CPT manual for a complete description of these procedures Only the provider performing the laboratory analysis can bill. BENEFITS & LIMITATIONS 8-32
62 8420. Laboratory continued: Updated 11/07 When ordered laboratory tests make up a panel or profile, the all-inclusive procedure code should be used to bill. Components should not be billed separately. Three or more multichannel tests are considered a SMA/SMAC profile when performed on the same date of service. Medicaid follows the guidelines outlined in the CPT manual to identify automated multichannel tests (SMACs, profiles) performed. When billing for a multichannel test use the appropriate CPT procedure code ( ). Urinalysis (UA) is considered content of service of the reimbursement to the physician for antepartum care when the UA is obtained for a diagnosis of pregnancy. The hospital/independent laboratory will not be reimbursed by Medicaid for the UA in this situation. Cytogenetic (chromosome) studies are covered for pregnant women (when medically necessary) and KAN Be Healthy participants only. A medical necessity form must accompany the claim when billing for a cytogenetic study for a pregnant woman older than 21 years of age. The following HIV testing is limited to four per calendar year, regardless of provider. Refer to the CPT manual for complete description of these procedures: 86701, 86702, HIV-1, viral load, quantitative, HCPCS code is covered. HIV-1, Infectious agent genotype analysis by nucleic acid (DNA or RNA), reverse transcriptase and protease (87901) is covered. Medical necessity documentation must include information that the patient meets at least one of the following criteria: (1) that the patient presents with virologic failure during Highly Active Antiretroviral Therapy (HAART), and/or (2) that the patient has suboptimal suppression of viral load after initiation of antiretroviral therapy. Testing is limited to two per calendar year. Life Sustaining Therapy: Chemotherapy, radiation therapy and renal dialysis are covered. Non-Covered Services: Medical supplies used in conjunction with outpatient surgery and/or the emergency room/observation room are considered content of service and cannot be billed separately. The rental or sale of DME and certain prosthetic and orthotic items. Operating Room: Anesthesia (equipment and supplies), drugs, surgical supplies and other equipment of the operating room, the recovery room and supplies are considered content of service of the operating and/or delivery room charges. Outpatient Procedures: Outpatient services provided within three days of an admission or discharge from the same hospital for the same or similar diagnosis are considered 'content of service' of the inpatient hospital stay. In this instance, bill the outpatient charges together on the inpatient claim. BENEFITS & LIMITATIONS 8-33
63 8420. Outpatient Procedures cont. Updated 09/07 There is one exception to this policy, complications from an outpatient sterilization resulting in an inpatient admission. In this instance the outpatient charges and the inpatient charges should be billed on two separate claims. HealthConnect/Managed Care Documentation: Acceptable outpatient hospital referral documentation includes an entry in the hospital outpatient or emergency department medical record noting that the primary care provider (PCP) was contacted at the time the service was rendered and approval was given. The statement must be signed by the individual who received the approval. If the PCP cannot be reached, approval must be secured from one of his/her covering physicians. Prosthetic & Orthotic Services: Outpatient hospitals will be allowed to bill the following prosthetic & orthotic codes: L3700 Elbow orthoses, elastic with stays, prefabricated, includes fitting and adjustment L3720 Elbow orthoses, double upright with forearm/arm cuffs, free motion, customfabricated L3845 Wrist-hand-finger orthoses, addition to short and long opponens, thumb I.P. extension assist, with M.P. stop L3906 Wrist-hand orthoses, wrist gauntlet, custom-fabricated L3907 Wrist-hand-finger orthosis, wrist gauntlet with thumb spica, custom-fabricated L3908 Wrist-hand orthoses, wrist extension control cock-up, non-molded, prefabricated, includes fitting and adjustment L3912 Hand-finger orthoses, flexion glove with elastic finger control, prefabricated, includes fitting and adjustment L3914 Wrist-hand orthoses, wrist extension cock-up, prefabricated, includes fitting/adjustment L3916 Wrist-hand-finger orthoses, wrist extension cock-up, with outrigger, prefabricated, includes fitting and adjustment L3918 Hand-finger orthoses, knuckle bender, prefabricated, includes fitting and adjustment L3928 Hand-finger orthoses, finger extension, with clock spring, prefabricated, includes fitting and adjustment L3930 Wrist-hand-finger orthoses, finger extension, with wrist support, prefabricated, includes fitting and adjustment L3934 Finger orthoses, safety pin, modified, prefabricated, includes fitting and adjustment L3938 Wrist-hand-finger othoses, dorsal wrist, prefabricated, includes fitting and adjustment L3942 Hand-finger orthoses, reverse knuckle bender, prefabricated, includes fitting and adjustment L3948 Finger orthoses, finger knuckle bender, prefabricated, includes fitting and adjustment L3954 Hand-finger orthoses, spreading hand, prefabricated, includes fitting and adjustment L3980 Upper extremity fracture orthosis, humeral, prefabricated, includes fitting and adjustment DeFlux, an injectable medical device, is covered with prior authorization. Use procedure code L8606. BENEFITS & LIMITATIONS 8-34
64 8420. Updated 09/07 Psychiatric Observation Beds: Psychiatric observation beds are covered up to two consecutive days. During the observation period the patient shall receive: a physical examination history and psychiatric assessment containing recommendations for ongoing treatment an initial nursing assessment nursing progress notes written each shift a discharge summary A physician must admit the patient to an observation bed and discharge him/her at the end of the observation stay. When an admission follows an observation stay, the physical examination report and the psychiatric assessment must be included in the patient's medical record. The observation bed stay becomes part of the DRG payment to the hospital. Refer to Section 7020 for billing instructions. Psychiatric Partial Hospitalization: These services are covered only in those hospitals where such a program has been approved by SRS. BENEFITS & LIMITATIONS 8-35
65 8430. FAMILY PLANNING/STERILIZATIONS Updated 09/07 Family Planning: Family planning is any medically approved treatment, counseling, drugs, supplies, or devices which are prescribed or furnished by a provider to individuals of child-bearing age for purposes of enabling such individuals to freely determine the number and spacing of their children. Insertion or removal of an implantable contraceptive requires medical necessity documentation when performed in an outpatient setting. Complete the family planning block on the claim form whenever a procedure or service is performed which relates to family planning. The following information is provided to facilitate coding the FL of the UB-04 claim form. The two-digit indicator "A4" is to be placed in this field. The following procedures are family planning related. The sterilization consent form must be attached to the surgeon's claim at the time of submission. Related claims (anesthesia, assistant surgeon, ambulatory surgery center, hospital or Rural Health Clinic) do not require an attached sterilization consent form. However, if not attached, processing will be delayed until the consent form with the surgeon's claim is reviewed and determined to be correct. ICD-9-CM Procedure Code (IP) Description HCPCS / Procedure Code Vasectomy, unilateral or bilateral (separate procedure), including post-op examinations. Ligation (percutaneous) of vas deferens unilateral or bilateral, (separate procedure) Vasectomy, unilateral or bilateral (separate procedure), including post-op examinations. Ligation (percutaneous) of vas deferens unilateral or bilateral, (separate procedure) 66.39, Ligation or transection of fallopian tube(s), abdominal or vaginal approach, unilateral or bilateral. Ligation or transection of fallopian tube(s), abdominal or vaginal approach, postpartum, unilateral or bilateral, during the same hospitalization (separate procedure) V25.2 Laparoscopy, surgical; with removal of adnexal structures (partial or total oophorectomy and/or salpingectomy) , 66.29, Laparoscopy, surgical, with fulguration of the , 66.39, oviducts (with or without transection) Laparoscopy, surgical, with occlusion of the oviducts by device (e.g. band, clip or Falope ring) BENEFITS & LIMITATIONS 8-36
66 8430. Updated 03/08 Sterilizations: Hysterectomy: Hysterectomies are covered only for medically indicated reasons. Medicaid will reimburse for this service only if at least one of the following three conditions is met and documented. One of the following conditions must also be met and documented. If one of these three options does not apply to the situation for which you have provided service, you may not be reimbursed. 1. The individual or her representative signs the Hysterectomy Necessity Form acknowledging receipt of information that the surgery will make her permanently incapable of reproducing. The Sterilization Consent Form is not an acceptable substitute. 2. The physician shall certify in writing that the individual was already sterile and state the cause or reason for the sterility on an attachment to the claim. The signature in field 85 of the claim form will not suffice. 3. For the sterilization consent form only, the physician shall certify in writing that the surgery was performed under a life-threatening situation and individual certification was not possible. Include a description of the nature of the emergency. The signature in field 85 of the claim form will not suffice. Refer to Section A copy of the Hysterectomy Necessity Form must be attached to the surgeon's claim at the time of submission. The form is located at the end of this manual in the Forms section, Hysterectomy_Necessity_Form, or on the KMAP Web site under Publications, Forms, Hysterectomy Necessity Form. It may be photocopied for your use. A copy of the Hysterectomy Necessity Form does not have to be attached to related claims (anesthesia, assistant surgeon, hospital, or Rural Health Clinic) at the time of submission. However, a related claim will not be paid until the Hysterectomy Necessity Form with the surgeon's claim has been reviewed and determined to be correct, unless the related claim has the correct Hysterectomy Necessity Form attached. All Sterilizations: Guidelines: Sterilizations on mentally incompetent individuals or individuals institutionalized for mental illness are not covered. The following guidelines must be accurately followed before reimbursement can be made for any sterilization procedure (including, but not limited to, hysterectomy, tubal ligation sterilization, and vasectomy). If each item is not followed completely, it will result in the denial of your claim. KMAP or other authorized agencies may ask for documentation at any time, either during the claims processing period or after payment of a claim, to verify that services have been provided within program guidelines. 1) The sterilization consent form mandated by federal regulation is located at the end of this manual in the Forms section, Sterilization Consent_Form or on the KMAP Web site under Publication, Forms, Sterilization Consent Form. All voluntary sterilization claims submitted without this specific sterilization consent form will be denied. 2) The sterilization consent form must be signed so that 30 days have passed before the date the sterilization is performed with the following exceptions: BENEFITS & LIMITATIONS 8-37
67 8430. Updated 09/07 Premature Delivery: The date of the beneficiary s consent must be at least three (3) calendar days prior to the date the sterilization was performed. The expected date of delivery must be indicated on the consent form and the date of the beneficiary s consent must be at least 30 days prior to the expected date of delivery. Emergency Abdominal Surgery: The date of the beneficiary s consent must be at least three (3) calendar days prior to the date the sterilization was performed. The circumstances of the emergency abdominal surgery must be described by the physician sufficiently to substantiate the waiver of the 30 day requirement. Three (3) calendar days is used in the above exceptions to guarantee compliance with the minimum federal requirement of 72 hours. 3) The sterilization consent form is valid for 180 days from the date it is signed by the beneficiary. Sterilization claims for individuals that reflect dates of service beyond 180 days from the date the consent form was signed will be denied. 4) The individual must be at least 21 years of age or older on the date the consent form is signed, or the sterilization claim will be denied. (This includes those situations in which the individual has misrepresented his or her age on the consent form to the provider.) The birth date information provided by SRS will be used to determine whether the individual meets the age requirement. This information can be obtained through KMAP Customer Service. 5) Sterilizations on mentally incompetent individuals are not covered. "Mentally incompetent individual" is defined as an individual who has been declared mentally incompetent by a federal, state or local court of competent jurisdiction for any purpose, unless the individual has been declared competent for purposes which include the ability to consent to sterilizations (42 CFR ). 6) The sterilization is not covered when consent is obtained from anyone in "labor", under the influence of alcohol or other drugs, or seeking or obtaining an abortion. 7) Interpreters must be provided when there are language barriers, and special arrangements must be made for handicapped individuals. 8) The physician's statement must be signed and dated no more than two (2) days prior to the surgery, the day of the surgery, or any day after sterilization was performed. 9) The physician statement on the consent form must be signed by the physician who performed the sterilization. No other signatures will be accepted. BENEFITS & LIMITATIONS 8-38
68 8400. Updated 01/08 When sterilization results from the treatment of a medical condition, a consent form is not required. However, there must be a note on the face of the claim that states what medical condition caused the sterility. Claims billed involving these situations will be denied for no sterilization consent form when an explanatory notation is not present on the face of the claim. The form must be legible in its entirety. Providers may photocopy this form from the manual. Refer to the Forms section at the end of the manual for a copy of the sterilization consent form. Note: Instruction on how to complete the Sterilization form is posted following the forms. Transcervical Sterilizations: Procedure code is not covered for transcervical sterilization procedures. Procedure code is to be used. The procedure must meet all sterilization requirements. Prior authorization is required. The Essure Kit is included in procedure code and should not be billed separately. The invoice does not need to be attached to the claim. Procedure code (SIS/HSG test) is covered as part of the transcervical sterilization process. This code will be paid only if the transcervical sterilization has been paid previously and the sterilization was performed more than three months prior to the date of service. If a beneficiary has had a transcervical hysteroscopy sterilization, a federal sterilization consent form is required. Additionally, three months must have passed before having the catheterization and introduction of saline or contrast material for saline infusion sonohysterography (SIS) or hysterosalpingography (HSG) - procedure code To indicate proof of sterilization, ICD-9 CM diagnosis code V25.2 must be used. Prior authorization is not required. BENEFITS & LIMITATIONS 8-39
69 APPENDIX I Updated 5/07 HCPCS PROCEDURE CODES The Health Care Policy / Medical Policy unit at SRS, requires Kansas Medical Assistance Program hospital billers to submit claims using the Health Care Financing Administration Common Procedure Code System (HCPCS). HCPCS is a combination of codes which includes CPT (Current Procedural Terminology) codes created and controlled by the American Medical Association; Centers for Medicare & Medicaid Services (CMS) Health Care Finance Administration (HCFA) codes created and controlled by CMS HCFA; and local codes created and controlled by the regional CMS HCFA office. HCPCS codes consist of a 5-digit base code with the capability of being up to 9 digits in length when modifiers are used. A modifier code is a two-digit code that identifies a specific type of service, for example anesthesia, or a variation of the service identified by the base code. Certain services require a modifier code be given in addition to the HCPCS base code. The modifier codes listed below are the only covered hospital modifier codes; use of any other modifier codes may cause your claim to be denied. Modifier Description 26 Professional Component 50 Bilateral Procedure *TC Technical Component 59 Multiple Surgeries thru Separate Incisions ET Emergency Services *Note: Hospitals that bill the base code for radiology procedures will be reimbursed at the TC rate Hospital billers should use CPT codes (refer to Section 1300) for outpatient services when available or when specifically instructed to do so; otherwise the CMS HCFA or local codes printed in the following pages should be used. Not all CPT procedure codes are covered. Contact the EDS Provider Assistance Unit with questions regarding coverage (refer to Section 1000). When a CPT, CMS HCFA or local code is not available, the service is non-covered by Kansas Medical Assistance Program. NOC (not otherwise classified) codes are non-covered. (Refer to Section 4200.) APPENDIX I AI-1
70 PROCEDURE CODES AND NOMENCLATURE Updated 9/04 PA - Prior authorization is required. COVERAGE INDICATORS PROCEDURE COV. CODE NOMENCLATURE P9010 P9012 P9016 P9017 P9019 P9021 P9022 P9023 P9031 P9032 P9033 P9034 P9035 P9036 P9037 P9038 P9039 P9040 P9041 P9043 P9044 P9045 P9046 P9047 P9048 P9050 P9051 P9052 P9053 P9054 LABORATORY SERVICES - BLOOD Blood (whole), for transfusion, per unit Cryoprecipitate, each unit Red blood cells, leukocytes reduced, each unit Fresh frozen plasma ((single donor), frozen within 8 hours of collection, each unit Platelet concentrate, each unit Red blood cells, each unit Washed red blood cells, each unit Plasma, pooled multiple donor, solvent/detergent treated, frozen, each unit Platelets, leukocytes reduced, each unit Platelets, irradiated, each unit Platelets, leukocytes reduced, irradiated, each unit Platelets, pheresis, each unit Platelets, pheresis, leukocytes reduced, each unit Platelets, pheresis, irradiated, each unit Platelets, pheresis, leukocytes reduced, irradiated, each unit Red blood cells, irradiated, each unit Red blood cells, deglycerolized, each unit Red blood cells, leukocytes reduced, irradiated, each unit Infusion, albumin (human), 5%, 50 ml Infusion, plasma protein fraction (human), 5%, 50 ml Plasma, cryoprecipitate reduced, each unit Infusion, albumin (human), 5%, 250 ml Infusion, albumin (human), 25%, 20 ml Infusion, albumin (human), 25%, 50 ml Infusion, plasma protein fraction (human), 5%, 250ml Granulocytes, pheresis, each unit Whole blood or red blood cells, leukocytes reduced CMVnegative, each unit Platelets, HLA-matched leukocytes reduced, apheresis/pheresis, each unit Platelets, pheresis, leukocytes reduced,cmv-negative, irradiated each unit Whole blood or red blood cells, leukocytes reduced, frozen, glycerol, washed, each unit APPENDIX I AI-2
71 PROCEDURE Updated 4/05 COV. CODE NOMENCLATURE P9055 Platelets, leukocytes reduced, CMV-negative, apheresis/pheresis, each unit P9056 Whole blood, leukocytes reduced, irradiated, each unit P9057 Ted blood cells, frozen/deglycerolized/washed, leukocytes reduced, irradiated, each unit P9058 Red blood cells, leukocytes reduced, CMV-negative, irradiated, each unit P9059 Fresh frozen plasma between 8-24 hours of collection each unit P9060 Fresh frozen plasma, donor retested, each unit (The above codes include processing and collection for transfusion; IV infusion sets include volume controller cassettes and buretrols.) MISCELLANEOUS PSYCHIATRIC SERVICES SUPPORTIVE PSYCHIATRIC SERVICES H2013 Psychiatric Health Facility, per diem DENTOALVEOLAR STRUCTURES PA* Unlisted Procedure, Dentoalveolar Structures is covered for the following procedures. Claims must include a detailed description of the actual service provided. If the description of the service is other than what is included on the list below, the service will be noncovered. Surgical removal, soft tissue impact each additional Pediatric dental procedures Simple extractions Full mouth extractions Dental service for non KAN Be Healthy recipients *Prior authorization is required for adults. Medical review is required for children age 21 and under. APPENDIX I AI-3
72 INJECTIONS Updated 12/07 Injection procedures listed below are placed in alphabetical order by generic name. Reference this listing using the generic drug name to find the procedure code. Utilize units to designate the dosage administered if there is not a specific injection code for the dosage. COVERAGE INDICATORS KBH - Covered for KAN Be Healthy participants only MCD - Injection covered for Medicaid recipients only MN - Medical Necessity documentation required PA - Prior authorization is required PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY PA J0129 Abatacept 10 mg J1120 Acetazolamide Sodium up to 500 mg vial Q047S Acyclovir, Zovirax up to 500 mg Q4075 Acyclovir 5 mg J0135 Adalimumab 20 mg J0150 Adenosine for therapeutic use, 6 mg (not to be used to report any J0152 adenosine phosphate compounds, instead use A9270) Adenosine for diagnostic use, 30 mg (not to be used to report any adenosine phosphate compounds; instead use A9270) J0170 Adrenalin, Epinephrine up to 1 ml 1 cc J0180 Agalsidase beta 1 mg J0200 Alatrofloxacin Mesylate 100 mg J7609 Albuterol (unit dose) 1 mg J7610 Albuterol (concentrated form) 1 mg PA J0215 Alefacept 0.5 mg J9015 Aldesleukin vial MCD J0205 Alglucerase units C9234 Alglucosidase Alfa 10 mg J0220 Alglucosidase Alfa 10 mg J2997 Alteplase Recombinant 1 mg J0207 Amifostine 500 mg * Administration only (patient brings own medication). Medication shall not be billed in conjunction with this procedure. APPENDIX I AI-4
73 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY S0072 Amikacin Sulfate up to 500 mg S0017 Aminocaproic 250 mg 1 cc J0280 Aminophyllin up to 250 mg J0282 Amiodarone HCL 30 mg J1320 Amitriptyline HCL up to 20 mg 2 cc J0300 Amobarbital up to 125 mg vial J0285 Amphotericin B 50 mg J0287 Amphotericin B lipid complex 10 mg J0289 Amphotericin B Liposome 10 mg J0290 Ampicillin Sodium 500 mg vial J0295 Ampicillin Sodium/Sulbactam 1.5 gm vial J0348 Anadulafungin 1 mg J0350 Anistreplase 30 units vial J7197 Antithrombin III (Human) unit MCD Z2064 Antivenin Polyvant (crotalide) ml J0128 Arbarelix 10 mg J0400 Aripiprazole, intramuscular 0.25 mg J9020 Asparaginase, Elspar up to 10, cc units J2910 Aurothioglucose up to 50 mg 1 cc J7501 Azathioprine (e.g., Imuran)- 100 mg 20 ml parenteral, vial J0456 Azithromycin 500 mg J3490 Aztreonam 500 mg 15 cc J3490 Bacitracin 50,000 units vial MCD J0475 Baclofen 10 mg (NDC and product name must be provided) J0476 Baclofen, for intrathecal trial 50 mcg J9025 Azacitidine 1 mg J9031 BCG Live (Intravesical) 50 mg vial J9050 BCNU, Bischlorethyl Nitrosourea, 100 mg vial Carmustine J0515 Benztropine 1 mg 1 cc J0702 Betamethasone Acetate and 3 mg 1 cc Betamethasone Sodium Phosphate J0704 Betamethasone Sodium Phosphate 4 mg 1 cc J0520 Bethanechol Chloride, up to 5 mg 1 cc Myotonachol or Urecholine APPENDIX I AI-5
74 PROCEDURE Updated 12/06 COV. CODE NOMENCLATURE STRENGTH QUANTITY J9035 Bevacizumab, 10 mg J0583 Bivalirudin 1 mg J9040 Bleomycin Sulfate 15 units amp J9041 Bortezomib 0.1 mg PA J0585 Botulinum Toxin Type A per unit PA J0587 Botulinum Toxin Type B per 100 units J0595 Butorphanol Tartrate 1 mg J7626 Budesonide Inhalation Solution, 0.5 mg Non-compounded, Administered Through DME, Unit Dose Form J7633 Budesonide Inhalation Solution 0.25 mg Administered through DME, Concentrated form J7634 Budesonide Inhalation Solution, 0.25 mg Compounded product, Administered Through DME, Concentrated Form S0020 Bupivacaine Hydrochloride 0.5 % J0592 Buprenorphine Hydrochloride 0.1 mg J0592 Buprenorphine 0.3 mg 1 cc J0595 Butorphanol Tartrate 1 mg 1 cc J0706 Caffeine Citrate 5 mg J0630 Calcitonin Salmon up to units J0636 Calcitriol 0.1mcg J3490 Calcium Chloride 1 gm 10 cc J3490 Calcium Gluceptate standard 5 cc J0610 Calcium Gluconate 10% 10 cc J9045 Carboplatin 50 mg vial J0637 Caspofungin Acetate 5 mg J0690 Cefazolin Sodium 500 mg 10 cc J0692 Cefepime Hydrochloride 500 mg S0021 Cefoperazone, Cefobid up to 1 gm J0698 Cefotaxime Sodium 1 gm vial S0074 Cefotetan Disodium (Cefotan) 1 gm vial J0694 Cefoxitin up to 1 gm 10 cc J0713 Ceftazidime 500 mg J0715 Ceftazidime Sodium 500 mg J0696 Ceftriaxone Sodium 250 mg vial J1890 Cephalothin Sodium up to 1 gm 10 cc J0710 Cephapirin Sodium up to 1 gm vial J9055 Cetuximab 10 mg J0720 Chloramphenicol Sodium up to 1 gm Siccomate APPENDIX I AI-6
75 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY J1205 Chlorothiazide Sodium 500 mg 20 cc J3230 Chlorpromazine HCL up to 50 mg Cholera vaccine for injectable use standard 1 cc J0725 Chorionic Gonadotropin 100 units J0743 Cilastatin Sodium; Imipenem 250 mg vial J0744 Ciprofloxacin for Intravenous Infusion 200 mg J9060 Cisplatin 10 mg vial J9062 Cisplatin 50 mg S0077 Clindamycin up to 300 mg J0745 Codeine Phosphate 30 mg 1 cc J0760 Colchicine up to 2 mg 2 cc J0770 Colistimethate Sodium up to 150 mg 2 cc J0835 Cosyntropin 0.25 mg J9070 Cyclophosphamide 100 mg 10 cc J9080 Cyclophosphamide 200 mg 20 cc J9090 Cyclophosphamide 500 mg 30 cc J9091 Cyclophosphamide 1 gm J9092 Cyclophosphamide 2 gm J9093 Cyclophosphamide, Lyophilized 100 mg J9094 Cyclophosphamide, Lyophilized 200 mg J9095 Cyclophosphamide, Lyophilized 500 mg J9096 Cyclophosphamide, Lyophilized 1.0 gm J9097 Cyclophosphamide, Lyophilized 2.0 gm J7516 Cyclosporine (e.g., Sandimmune)- 250 mg Parentera J9098 Cytarabine 10 mg J9100 Cytarabine 100 mg J9110 Cytarabine 500 mg J9130 Dacarbazine 100 mg 10 cc J9140 Dacarbazine 200 mg 10 cc J7513 Daclizumab, parenteral 25 mg J9120 Dactinomycin, Actinomycin D 0.5 mg 3 cc MCD J1645 Dalteparin Sodium 2500 IU J0878 Daptomycin 1 mg J9150 Daunorubicin 10 mg vial J9151 Daunorubicin Citrate 10 mg Liposomal Formulation Q0137 Darbepoetin Alfa 1 mcg (non ESRD use) J0894 Decitabine 1 mg J0895 Deferoxamine Mesylate 500 mg amp J9160 Denileukin Diftitox 300 mcg APPENDIX I AI-7
76 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY J1060 Depandrogyn standard 1 cc J1000 Depo-Estradiol Cypionate up to 5 mg 1 cc J1094 Dexamethasone Acetate 1 mg J1100 Dexamethasone Sodium 1 mg 1 cc Phosphate J1100 & J0670 Dexamethasone Acetate.5 cc and standard Mepivacaine Hydrochloride 1%.5 cc J1190 Dexrazoxane HCL 250 mg J0500 Dicyclomine up to 20 mg 2 cc J9165 Diethylstilbestrol Diphosphate 250 mg J1160 Digoxin up to 0.5 mg 1 cc J1110 Dihydroergotamine up to 0.1 mg 1 cc MCD J1240 Dimenhydrinate up to 50 mg J1200 Diphenhydramine HCL up to 50 mg 1 cc J1245 Dipyridamole 10 mg 2 ml J1250 Dobutamine HCL 250 mg 1 cc J9170 Docetaxel (Taxotere) 20 mg 1 ml J1260 Dolasetron Mesylate 10 mg J1270 Doxercalciferol 1 mcg J9000 Doxorubicin HCL 10 mg vial J9001 Doxorubicin HCL, all lipid formulations 10 mg J1810 Droperidol and Fentanyl Citrate up to 2 ml amp (NDC and product name/description must be provided) J1300 * Eculizumab 10 mg J3520 Edetate Disodium 150 mg PA J1324 Enfuvirtide 1 mg MCD J1650 Enoxaparin Sodium 30mg 1 ml J0170 Epinephrine Hydrochloride 1:200 mg 0.3 cc J9178 Epirubicin HCL 2 mg MCD J1325 Epoprostenol 0.5 mg J1330 Ergonovine Maleate up to 0.2 mg 1 cc J1335 Ertapenem Sodium 500 mg J1364 Erythromycin Lactobionate 500 mg J0885 Injection, epoetin alfa, 1000 units (for non-esrd use) *This code will be placed on medical review until the Drug Utilization Review (DUR) Board meets to set PA criteria. Once PA criteria has been determined, the code will be taken off of medical review. Providers will be notified when the code is removed from medical review. APPENDIX I AI-8
77 PROCEDURE Updated 4/04 COV. CODE NOMENCLATURE STRENGTH QUANTITY J1380 Estradiol Valerate up to 10 mg 1 cc J1390 Estradiol Valerate up to 20 mg 1 cc J0970 Estradiol Valerate up to 40 mg 1 cc J1410 Estrogen Conjugated 25 mg J1435 Estrone 1 mg PA J1438 Etanercept 25 mg J3490 Ethacrynic Acid 50 mg 1 cc J1436 Etidronate Disodium 300 mg 6 ml amp J9181 Etoposide 10 mg 2.5 cc J9182 Etoposide 100 mg 5 cc J7190 Factor VIII (Antihemophilic Factor per i.u (NDC and product name/description must be provided) J7191 Factor VIII (Antihemophilic Factor per i.u [Porcine]) J7192 Factor VIII (Antihemophilic Factor per unit [Recombinant]) J7193 Factor IX (Antihemophilic Factor, per i.u. Purified, Non-Recombinant) J7195 Factor IX (Antihemophilic Factor, per i.u. Recombinant) MCD S0028 Famotidine 10 mg/ml 1 ml J3010 Fentanyl Citrate 0.1 mg 2 cc MCD J1440 Filgrastim (G-CSF) 300 mcg MCD J1441 Filgrastim (G-CSF) 480 mcg J9200 Floxuridine 500 mg 5 cc J1450 Fluconazole 200 mg J9185 Fludarabine Phosphate 50 mg 1 ml J7641 Flunisolide, Inhalation Solution per mg Administered Through DME, Unit Dose Form APPENDIX I AI-9
78 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY J7311 Fluocinolone acetonide 0.59 mg J9190 Fluorouracil 500 mgm amp J2680 Fluphenazine Decanoate up to 25 mg 1 cc J1452 Fomivirsen Sodium, Intraocular 1.65 mg J1652 Fondaparinux Sodium 0.5 mg J1455 Foscarnet Sodium 1000 mg vial J9395 Fulvestrant 25 mg J1940 Furosemide up to 20 mg 2 cc J1458 Galsulfase 1 mg J1460 Gamma Globulin, Intramuscular standard 1 cc J1470 Gamma Globulin, Intramuscular standard 2 cc J1480 Gamma Globulin, Intramuscular standard 3 cc J1490 Gamma Globulin, Intramuscular standard 4 cc J1500 Gamma Globulin, Intramuscular standard 5 cc J1510 Gamma Globulin, Intramuscular standard 6 cc J1520 Gamma Globulin, Intramuscular standard 7 cc J1530 Gamma Globulin, Intramuscular standard 8 cc J1540 Gamma Globulin, Intramuscular standard 9 cc J1550 Gamma Globulin, Intramuscular standard 10 cc J1560 Gamma Globulin, Intramuscular standard 10 cc J1570 Ganciclovir Sodium 500 mg vial J1580 Garamycin, Gentamycin up to 80 mg 2 cc J1590 Gatifloxacin 10 mg J9201 Gemcitabine HCL 200 mg J9300 Gemtuzumab, Ozogamicin 5 mg J1610 Glucagon Hydrochloride 1 mg 1 cc J1600 Gold Sodium Thiomaleate up to 50 mg 1 ml J1620 Gonadorelin Hydrochloride 100 mcg J9202 Goserelin Acetate Implant 3.6 mg 1 MCD J1626 Granisetron Hydrochloride 100 mcg 1 ml J1631 Haloperidol Decanoate 50 mg 1 cc J1642 Heparin Sodium (Heparin 10 units tubex Lock Flush) J1644 Heparin Sodium 1000 units vial J1571 Hepatitis B immune globulin 0.5 ml (Hepagam B), intramuscular J1573 Hepatitis B immune globulin 0.5 ml (Hepagam B), intravenous Q4090 Hepatitis B immune globulin (Hepagam B), intramuscular, 0.5ml Q4083 Hyaluronan or derivative, hyalgan or supartz, for intra-articular injection, per dose Q4084 Hyaluronan or derivative, synvisc, for intra-articular injection, per dose Q4085 Hyaluronan or derivative, euflexxa, for intra-articular injection, per dose Q4086 Hyaluronan or derivative, orthovisc, for intra-articular injection, per dose APPENDIX I AI-10
79 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY J7321 Hyaluronan or derivative, hyalgan or supartz, for intra-articular injection, per dose J7322 Hyaluronan or derivative, synvisc, for intra-articular injection, per dose J7323 Hyaluronan or derivative, euflexxa, for intra-articular injection, per dose J7324 Hyaluronan or derivative, orthovisc, for intra-articular injection, per dose J3470 Hyaluronidase up to 150 units 1 cc J0360 Hydralazine HCL up to 20 mg amp J1700 Hydrocortisone Acetate, up to 25 mg 1 cc J1720 Hydrocortisone Sodium Succinate up to 100 mg 2 cc J1710 Hydrocortisone Sodium Phosphate up to 50 mg 1 cc J1170 Hydromorphone up to 4 mg 1 cc J3410 Hydroxyzine HCL up to 25 mg 1 cc J7320 * Hylan G-F (Synvisc ) 16 mg J1740 Ibandronate Sodium 1 mg MCD J9211 Idarubicin Hydrochloride 5 mg vial C9232 Idursulfase 1 mg J1743 Idursulfase 1 mg J9208 Ifosfomide per gm 1 gm vial MCD J1785 Imiglucerase unit Q4087 Immune globulin, intravenous, non-lyophilized, 500mg Q4088 Immune globulin, (Gammagard), intravenous, non-lyophilized, 500mg Q4091 Immune globulin, (Flebogamma), intravenous, non-lyophilized, 500mg Q4092 Immune globulin, (Gamunex), intravenous, non-lyophilized, 500mg Q9941 Immune globulin, intravenous, lyophilized 1 g Q9942 Immune globulin, intravenous, lyophilized 10 mg Q9943 Immune globulin, intravenous, 1 g non-lyophilized Q9944 Immune globulin, intravenous, 10 mg non-lyophilized J1561 Immune globulin (gamunex), 500 mg intravenous, non-lyophilized (e.g. liquid) J1562 Immune globulin (vivaglobin) 100 mg Subcutaneous J1568 Immune globulin (octagam), 500 mg intravenous, non-lyophilized (e.g. liquid) J1569 Immune globulin (gammagard 500 mg liquid), intravenous, non-lyophilized (e.g. liquid) J1572 Immune globulin (flebogamma), 500 mg intravenous, non-lyophilized (e.g. liquid) PA J1745 Infliximab (Remicade) 10 mg vial J9213 Interferon, Alfa-2A, Recombinant 3 mill. units vial J9214 Interferon, Alfa-2B, Recombinant 1 mill. units *Second series requires prior authorization APPENDIX I AI-11
80 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY J9215 Interferon, Alfa-N3 (Human 250,000 units Leukocyte Derived) J9212 Interferon, Alfacon-1, Recombinant 1 mcg J1825 Interferon Beta-1A 33 mcg MCD J1830 Interferon Beta 1-B 0.25 mg J9216 Interferon, Gamma 1-B 3 mill. units vial J9206 Irinotecan HCI 20 mg/ml 1 ml J1751 Iron Dextran mg J1752 Iron Dextran mg J1756 Iron Sucrose 21 mg J7647 Isoetharine HCL concentrated form per mg J7650 Isoetharine HCL unit dose form per mg J7657 Isoproterenol HCL concentrated form per mg J7657 Isoproterenol HCL unit dose form per mg J7658 Isoproterenol Hydrochloride per mg conc. form J7659 Isoproterenol Hydrochloride, unit dose per mg form (NDC and product name/description must be provided) J1835 Itraconazole 50 mg J1840 Kanamycin Sulfate up to 500 mg 2 cc J1850 Kanamycin Sulfate up to 75 mg 2 cc J1885 Ketorolac Tromethamine 15 mg ml (NDC and product name/description must be provided) J1931 Laronidase 0.1 mg J0640 Leucovorin Calcium 50 mg vial J1950 Leuprolide Acetate (For Depot) 3.75 mg Suspension) J9218 Leuprolide Acetate 1 mg 1 ml J9217 Leuprolide Acetate, For Depot 7.5 mg/ml 1.5 ml Suspension J9219 Leuprolide Acetate Implant 65 mg (NDC and product name/description must be provided) J7607 Levalbuterol concentrated form 0.5 mg J7615 Levalbuterol unit dose form 0.5 mg C9238 Levetiracetam 10 mg J1956 Levofloxacin 250 mg J2001 Lidocaine HCL (For intravenous infusion) 10 mg J2010 Lincomycin HCL up to 300 mg 1 cc MCD J2001 Lidocaine HCL per ml (Lidocaine HCL w/epinephrine) J2020 Linezolid 200 mg J7511 Lymphocyte Immune Globulin, 25 mg Antihymocyte Globulin, Rabbit, Parenteral APPENDIX I AI-12
81 PROCEDURE Updated 04/07 COV. CODE NOMENCLATURE STRENGTH QUANTITY J3475 Magnesium Sulfate 500 mg J2150 Mannitol 25% 50 ml J2170 Mecasermin 1 mg J9230 Mechlorethamine HCL (Nitrogen 10 mg 20 cc Mustard), HN2 J1051 Medroxyprogesterone Acetate 50 mg J1055 Medroxyprogesterone Acetate 150 mg 1 cc For Contraceptive Use J1056 Medroxyprogesterone Acetate/ Estradiol Cypionate, 5 mg/25 mg J2180 Meperidine and Promethazine HCL up to 50 mg 2 cc J2175 Meperidine 100 mg 1 cc J0670 Mepivacaine 1% 1 cc J2185 Meropenem 100 mg J9209 Mesna 200 mg vial J3490 Mesoridazine Besylate 25 mg 1 cc J7667 Metaproterenol Sulfate concentrated form per 10 mg J7670 Metaproterenol Sulfate unit dose form per 10 mg J0380 Metaraminol up to 10 mg 1 cc J2800 Methocarbamol up to 10 ml 10 cc J9250 Methotrexate 5 mg J9260 Methotrexate Sodium Mix 50 mg 2 cc J2210 Methylergonovine Maleate up to 0.2 mg 1 cc J1020 Methylprednisolone Acetate 20 mg 1 cc J1040 Methylprednisolone Acetate 80 mg 2 cc J2920 Methylprednisolone Sodium up to 40 mg 1 cc Succinate J2930 Methylprednisolone Sodium up to 125 mg 2 cc Succinate J2765 Metoclopramide HCL up to 10 mg 2 cc S0030 Metronidazole up to 500 mg 100 ml J2248 Micafungin Sodium 1 mg J2260 Milrinone Lactate 5 mg J9280 Mitomycin 5 mg J9290 Mitomycin 20 mg J9291 Mitomycin 40 mg J9293 Mitoxantrone HCL 5 mg 10 ml J2270 Morphine Sulfate up to 10 mg 1 cc J2271 Morphine Sulfate 100 mg MCD J2275 Morphine Sulfate, preservative-free 10 mg ml sterile solution) J2280 Moxifloxacin 100 mg J2300 Nalbuphine HCL 10 mg 2 cc APPENDIX I AI-13
82 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY J2310 Naloxone HCL 1 mg 1 cc J2315 Naltrexone, depot form 1 mg J2320 Nandrolone Decanoate up to 50 mg 0.5 cc J2321 Nandrolone Decanoate up to 100 mg 1 cc J2322 Nandrolone Decanoate up to 200 mg 2 cc J2710 Neostigmine Bromide 1:1000 (1 mg) 1 cc J2710 Neostigmine Methylsulfate up to 0.5 mg 1 cc J2353 Octreotride (Depot form) 1 mg J2354 Octreotride (non-depot form) 25 mg J2357 Omalizumab 5 mg MCD J2405 Ondansetron Hydrochloride 1 mg 0.5 ml J2355 Oprelvekin 5 mg J2700 Oxacillin Sodium up to 250 mg vial J9263 Oxaliplatin 0.5 mg J2410 Oxymorphone HCL up to 1 mg 1 cc J2460 Oxytetracycline HCL up to 50 mg 1 ml J2460 Oxytetracycline HCL 500 mg 10 cc J2590 Oxytocin up to 10 units 1 cc J9264 Paclitaxel protein-bound particles 1 mg J9265 Paclitaxel 30 mg 5 ml KBH,PA Palivizumab (Synagis) up to 50 mg vial J2469 Palonosetron hcl 25 mcg J2430 Pamidronate Dissodium 30 mg vial C9235 Panitumumab 10 mg J9303 Panitumumab 10 mg J2440 Papaverine HCL up to 60 mg 2 cc J2501 Paricalacitol 1 mcg J2505 Pegfilgrastim 6 mg J9305 Pemetrexed 10 mg J0530 Penicillin G Benzathine & Penicillin up to 600,000 1 cc G Procaine units J0540 Penicillin G Benzathine & Penicillin up to 1,200,000 2 cc G Procaine units J0550 Penicillin G Benzathine & Penicillin up to 2,400,000 4 cc G Procaine units J0560 Penicillin G Benzathine up to 600,000 1 cc units J0570 Penicillin G Benzathine up to 1,200,000 2 cc units J0580 Penicillin G Benzathine up to 2,400,000 4 cc units J2540 Penicillin G Potassium up to 600,000 1 cc units APPENDIX I AI-14
83 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY J2510 Penicillin G Procaine, Aqueous up to 600,000 1 cc J3070 Pentazocine HCL up to 30 mg 1 cc J2515 Pentobarbital Sodium 50 mg 1 cc J3310 Perphenazine up to 5 mg 1 cc units J2560 Phenobarbital Sodium up to 120 mg 2 cc J1165 Phenytoin Sodium 100 mg 2 cc J2543 Piperacillin Sodium/Tazobactum Sodium 1 gm/0.125 gm vial J9270 Plicamycin (Mithramycin) 2.5 mg Z2069 Polymyxin B Sulfate 500,000 units vial J9600 Porfimer Sodium 75 mg J3480 Potassium Chloride 2 meq J2650 Prednisolone Acetate up to 1 ml J0743 Primaxin 250 mg J2690 Procainamide HCL up to 1 gm 2 cc J0780 Prochlorperazine up to 10 mg 2 cc J3490 Prolixin Enanthate 25 mg 1 cc J2550 Promethazine HCL up to 50 mg 1 cc J1800 Propranolol HCL up to 1 mg 1 cc J2720 Protamine Sulfate 10 mg J2724 Protein C concentrate, intravenous, human 10 IU J3415 Pyridoxine 100 mg Rabies Immune Globulin (RIG), human for intramuscular and/or subcutaneous use Rabies Immune Globulin, heat-treated (RIG-HT), human for intramuscular and/or subcutaneous use C9233 Ranibizumab 0.5 mg J2778 * Ranibizumab 0.1 mg J2780 Ranitidine HCL 25 mg J2783 Rasburicase 0.5 mg J1565 Resp Sync Vir Immug (Respigam) 50 mg/ml 1 ml Respiratory Synctyial Virus Immune 50 mg Globulin (RSV-IGIM), for intramuscular use, each *This code will be placed on medical review until the Drug Utilization Review (DUR) Board meets to set PA criteria. Once PA criteria has been determined, the code will be taken off of medical review. Providers will be notified when the code is removed from medical review APPENDIX I AI-15
84 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY J2993 Reteplase (two single use vials) 18.1 mg Rho(D) immune globulin (RhIg), human, full-dose for intramuscular use J2788 Rho(D) immune globulin, human, mini-dose 50 mg Rho(D) immune globulin (RhIg), human, mini-dose, for intramuscular use Rho(D) immune globulin (RhIgIV), human, for intravenous use J2791 Rho(D) immune globulin, human 100 IU (rhophylac) intramuscular or intravenous J2792 Rho(D) immune globulin, human 100 IU solvent detergent Q4089 Rho(D) Immune Globulin, Human, (Rhophylac), intravenous, 100 IU J2794 Risperidone, long acting 0.5 mg J9310 Rituximab 100 mg MCD J2820 Sargramostin (GM-CSF) 50mcg vial J2912 Sodium Chloride 0.9% 2 ml J2916 Sodium Ferric Gluconate 12.5 mg PA,KBH J2940 Somatrem 1 mg J2941 Somatropin 1 mg J3320 Spectinomycin Dihydrochloride up to 2 gm 3.2 cc J0697 Sterile Cefuroxime Sodium 750 mg vial S0040 Sterile Ticarcillin Disodium and 3.1 gm vial Clavulanate J2995 Streptokinase 250,000 unit vial J0330 Succinycholine Chloride up to 20 mg vial J3030 Sumatriptan Succinate 6 mg J7525 Tacrolimus, Parenteral 5 mg C9239 Temsirolimus 1 mg J3100 Tenecteplase 50 mg Q2017 Teniposide ml APPENDIX I AI-16
85 Updated 09/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY J3105 Terbutaline Sulfate up to 1 mg J3140 Testosterone Suspension up to 50 mg 1 cc J1060 Testosterone Cypionate & up to 1 ml 1 ml Estradiol Cypionate J1070 Testosterone Cypionate up to 100 mg 1 cc J1080 Testosterone Cypionate 200 mg 1 cc J3120 Testosterone Enanthate up to 100 mg.5 cc J3130 Testosterone Enanthate up to 200 mg 1 cc J0900 Testosterone Enanthate and up to 1 cc Estradiol Valerate J3150 Testosterone Propionate up to 100 mg 2 cc Tetanus Immune Globulin (TIG), Human, For Intramuscular Use Measles, Mumps and Rubella virus vaccine (MMR), live for subcutaneous use Therapeutic or diagnostic injection (NDC and product name/description must be provided) J3280 Thiethylperazine Maleate up to 10 mg 2 cc J9340 ThioTepa 15 mgm J3243 Tigecycline 1 mg J1655 Tinzaparin Sodium 1000 IU J3246 Tirofiban HCL 0.25mg J3260 Tobramycin Sulfate up to 80 mg 2 cc MCD J9350 Topotecan HCL (Hycamtin) 4 mg vial J9355 Trastuzumab (Herceptin) 10 mg J3302 Triamcinolone Diacetate 5 mg/ml 1 ml J3303 Triamcinolone Hexacetonide 5 mg/ml 1 ml J3400 Triflupromazine HCL up to 20 mg 1 cc J3250 Trimethobenzamide HCL up to 200 mg 2 cc J3315 Triptorelin Pamoate 3.75 mg Typhoid Vaccine, Live, Oral Typhoid Vaccine, VI Capsular Polysaccharide (VICPS), For Intramuscular Use Typhoid Vaccine, Heat- and Phenol-Inactivated (H-P) For Subcutaneous or Intradermal Use J3364 Urokinase 5000 units 1 ml J9357 Valrubicin, intravesical 200 mg J3370 Vancomycin HCL 500 mg 10 cc J3490 Verapamil Hydrochloride 5 mg/2 ml 2 ml J3396 Verteporfin 0.1 mg APPENDIX I AI-17
86 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE STRENGTH QUANTITY J9360 Vinblastine Sulfate 1 mg 1 cc J9370 Vincristine Sulfate 1 mg/ml 1 ml vial J9375 Vincristine Sulfate 2 mg 2 ml vial J9380 Vincristine Sulfate 5 mg 5 ml vial J9390 Vinorelbine Tartrate 10 mg 1 ml J3420 Vitamin B-12 Cyanocobalamin up to 1000 mcg J3430 Vitamin K, Phytonadione, up to 10 mg 1 cc Menadione, Menadiol Sodium Diphosphate J3486 Zipasidone 10 mg J3487 Zoledronic acid (Zometa) 1 mg J3488 Zoledronic acid (Reclast) 1 mg Q4095 Zoledronic Acid (Reclast) 1 mg IV INFUSIONS PROCEDURE CODE NOMENCLATURE DOSE J7030 Infusion, normal saline soln cc J7040 Infusion, normal saline soln. 500 ml J7042 5% dextrose/normal saline 500 ml J7050 Infusion, normal saline soln. 250 cc J7060 5% dextrose/water 500 ml = 1 unit J7070 Infusion, D5W 1000 cc MCD J7100 Infusion, Dextran ml MCD J7110 Infusion, Dextran ml J7120 Ringers lactate infusion up to 1000 cc J7130 Hypertonic saline soln 50 or 100 meq., 20 cc vial J3490 J7303 J7599 J8499 J8999 J9999 NOT OTHERWISE CLASSIFIED INJECTIONS Unclassified drugs Contraceptive supply, hormone containing vaginal ring, each Immunosuppressive drug, not otherwise classified Prescription drug, oral, non-chemotherapeutic, not otherwise classified Prescription drug, oral, chemotherapeutic, not otherwise classified Antineoplastic drug, not otherwise classified NOTE: The NDC and drug name must be included on the claim or the claim will deny. APPENDIX I AI-18
87 AEROSOL ADDITIVES Updated 12/07 FOR OUTPATIENT HOSPITAL USE ONLY PROCEDURE CODE NOMENCLATURE DOSE J3535 Drug administered through a metered dose inhaler (NDC and product name/description must be provided) J7602 Albuterol, all formulations including separated isomers, inhalation solution, FDA-approved final product, non-compounded, administered through DME, concentrated form, per 1 mg (Albuterol) or per 0.5 mg (Levalbuterol) J7603 Albuterol, all formulations including separated isomers, inhalation solution, FDA-approved final product, non-compounded, administered through DME, unit dose, per 1 mg (Albuterol) or per 0.5 mg (Levalbuterol) J7604 Acetylcysteine, inhalation solution, compounded product, administered through DME, unit dose form, per gram J7619 Albuterol Inhalant Solution, unit dose form 1 mg J7620 Albuterol, up to 2.5 mg and ipratropium bromide, up to 0.5 mg, non-compounded inhalation solution, administered through DME J7622 Beclomethasome, inhalation solution per mg administered through DME, unit dose form J7624 Betamethasome, inhalation solution per mg administered through DME, unit dose form J7632 Cromolyn sodium, inhalation solution, 10 mg compounded product, administered through DME, unit dose form Q4093 Albuterol, all formations including separated per mg isomers, inhalation solution, FDA-approved final product, non-compounded, administered through DME, concentrated form Q4094 Albuterol, all formations including separated per mg isomers, inhalation solution, FDA-approved final product, non-compounded, administered through DME, unit dose J7648 Isoetharine HCL, Inhalation Soln. Conc. form per mg J7649 Isoetharine HCL, Inhalation Soln. unit dose form per mg (NDC and product name/description must be provided) J7645 Ipratropium Bromide, inhalation solution, per mg compounded product, administered through DME, unit dose form J7668 Metaproterenol sulfate, Inhalation Soln. 10 mg Conc. form J7669 Metaproterenol sulfate, Inhalation Soln. 10 mg unit dose form Pentamidine, aerosol inhalation 300 mg APPENDIX I AI-19
88 AEROSOL ADDITIVES continued Updated 12/07 FOR OUTPATIENT HOSPITAL USE ONLY PROCEDURE CODE NOMENCLATURE DOSE J7676 Pentamidine isethoionate, inhalation solution, 300 mg compounded product, administered through DME, unit dose form J7608 Acetylcysteine, inhalation solution, FDA-approved per gram final product, non-compounded, administered per mg through DME, unit dose form APPENDIX I AI-20
89 IMMUNIZATION ADMINISTRATION Updated 12/07 Providers must bill the appropriate administration code in addition to the vaccine and toxoid code for each dose administered. CPT codes for vaccines covered under the VFC program will be noncovered for children 18 years of age and younger. ADLT VFC COVERAGE INDICATORS Vaccine covered for adults (19 years of age and older). Vaccine covered by VFC (18 years of age and younger). PROCEDURE COV. CODE NOMENCLATURE ADMINISTRATION CODES Immunization administration (includes percutaneous, intradermal, subcutaneous, or intramuscular injections); one vaccine (single or combination vaccine/toxoid) each additional vaccine (single or combination vaccine/toxoid) (List separately in addition to code for primary procedure) Immunization administration by intranasal or oral route; one vaccine (single or combination vaccine/toxoid) each additional vaccine (single or combination vaccine/toxoid) )List separately in addition to code for primary procedure) Immunization administration younger than 8 years of age (includes percutaneous, intradermal, subcutaneous, or intramuscular injections) when the physician counsels the patient/family; first injection (single or combination vaccine/toxoid), per day each additional injection (single or combination vaccine/toxoid), per day (List separately in addition to code for primary procedure) Immunization administration younger than age 8 years (includes intranasal or oral routes of administration) when the physician counsels the patient/family; first administration (single or combination vaccine/toxoid), per day each additional administration (single or combination vaccine/toxoid), per day (List separately in addition to code for primary procedure) VACCINE CODES VFC Diphtheria, tetanus toxoids, acellular pertussis vaccine, haemophilus influenza Type B, and poliovirus vaccine, inactivated (DTaP-Hib-IPV), for intramuscular use VFC Diphtheria, tetanus toxoids and acellular pertussis vaccine (DTaP), when administered to individuals younger than 7 years, for intramuscular use ADLT Diphtheria, tetanus toxoids, and whole cell pertussis vaccine (DTP), for intramuscular use VFC Diphtheria and tetanus toxoids (DT) adsorbed when administered to individuals younger than 7 years, for intramuscular use VFC Diphtheria, tetanus toxoids, and whole cell pertussis vaccine and hemophilus influenza B vaccine (DTP-Hib), for intramuscular use APPENDIX I AI-21
90 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE VACCINE CODES (cont.) VFC Diphtheria, tetanus toxoids, acellular pertussis vaccine, Hepatitis B, and poliovirus vaccine, inactivated (DTaP-HepB-IPV), for intramuscular use ADLT Hepatitis A vaccine, adult dosage, for intramuscular use VFC Hepatitis A vaccine, pediatric/adolescent dosage-2 dose schedule, for intramuscular use VFC Hepatitis A vaccine, pediatric/adolescent dosage-3 dose schedule, for intramuscular use ADLT Hepatitis A and hepatitis B vaccine (HepA-HepB), adult dosage, for intramuscular use ADLT Hepatitis B vaccine, dialysis or immunosuppressed patient dosage (3 dose schedule), for intramuscular use VFC Hepatitis B vaccine, adolescent (2 dose schedule), for intramuscular use VFC Hepatitis B vaccine, pediatric/adolescent dosage (3 dose schedule), for intramuscular use ADLT Hepatitis B vaccine, adult dosage, for intramuscular use ADLT Hepatitis B vaccine, dialysis or immunosuppressed patient dosage (4 dose schedule), for intramuscular use VFC Hepatitis B and Hemophilus influenza b vaccine (HepB-Hib), for intramuscular use VFC Hemophilus influenza b vaccine (Hib), HbOC conjugate (4 dose schedule), for intramuscular use VFC Hemophilus influenza b vaccine (Hib), PRP-D conjugate, for booster use only, intramuscular use VFC Hemophilus influenza b vaccine (Hib), PRP-OMP conjugate (3 dose schedule), for intramuscular use VFC Hemophilus influenza b vaccine (Hib), PRP-T conjugate (4 dose schedule), for intramuscular use VFC, Human Papilloma virus (HPV) vaccine, types 6, 11, 16, 18 ADLT (quadrivalent), 3 dose schedule, for intramuscular use VFC Influenza virus vaccine, split virus, preservative free, when administered to children 6-35 months of age, for intramuscular use VFC, Influenza virus vaccine, split virus, preservative free, when administered ADLT to individuals 3 years and older, for intramuscular use VFC Influenza virus vaccine, split virus, when administered to children 6-35 months of age, for intramuscular use VFC, Influenza virus vaccine, split virus, when administered to individuals 3 years ADLT of age and older, for intramuscular use VFC, Influenza virus vaccine, live, for intranasal use ADLT VFC, Influenza virus vaccine, derived from cell cultures, subunit, preservative ADLT and antibiotic free, for intramuscular use VFC, Influenza virus vaccine, split virus, preservative free, enhanced ADLT immunogenicity via increased antigen content, for intramuscular use APPENDIX I AI-22
91 Updated 12/07 PROCEDURE COV. CODE NOMENCLATURE VACCINE CODES (cont.) VFC, Influenza virus vaccine, pandemic formulation ADLT VFC, Measles, mumps, and rubella virus vaccine (MMR), live, for subcutaneous ADLT use VFC, Measles, mumps, rubella, and varicella vaccine (MMRV), live, for ADLT subcutaneous use VFC Meningococcal polysaccharide vaccine (any groups[s]), for subcutaneous use VFC, Meningococcal conjugate vaccine, serogroups A, C, Y and W-135 ADLT (tetravalent), for intramuscular use VFC Pneumococcal conjugate vaccine, polyvalent, when administered to children younger than 5 years, for intramuscular use VFC, Pneumococcal polysaccharide vaccine, 23-valent, adult or ADLT immunosuppressed patient dosage, when administered to individuals 2 years or older, for subcutaneous or intramuscular use VFC Poliovirus vaccine, inactivated, (IPV), for subcutaneous or intramuscular use Rabies vaccine, for intramuscular use VFC Rotavirus vaccine, pentavalent, 3 dose schedule, live, for oral use VFC Tetanus toxoid absorbed, for intramuscular use VFC, Tetanus and diphtheria toxoids (Td) adsorbed, preservative free, when ADLT administered to 7 years or older, for intramuscular use VFC, Tetanus, diphtheria toxoids and acellular pertussis vaccine (Tdap), when ADLT administered to 7 years or older, for intramuscular use VFC, Tetanus and diphtheria toxoids (Td) adsorbed, when administered to ADLT individuals 7 years or older, for intramuscular use VFC, Varicella virus vaccine, live, for subcutaneous use ADLT ADLT Zoster (shingles) vaccine, live, for subcutaneous injection APPENDIX I AI-23
92 Updated 12/07 Defibrillator codes: G0297 Insertion of single chamber pacing cardioverter defibrillator pulse generator G0298 Insertion of dual chamber pacing cardioverter defibrillator pulse generator G0299 Insertion or repositioning of electrode lead for single chamber pacing cardioverter defibrillator and insertion of pulse generator G0300 Insertion or repositioning of electrode lead(s) for dual chamber pacing cardioverter defibrillator and insertion of pulse generator Pacemaker surgical Codes: Insertion of epicardial electrode(s); endoscopic approach Insertion or replacement of permanent pacemaker with transvenous electrode(s); atrial Insertion or replacement of permanent pacemaker with transvenous electrode(s); ventricular Insertion or replacement of permanent pacemaker with transvenous electrode(s); atrial and ventricular APPENDIX I AI-24
93 APPENDIX II Updated 6/05 AMBULATORY SURGERY/OUTPATIENT SURGERY PROCEDURE CODES AND NOMENCLATURE COVERAGE INDICATORS KBH - Services covered for KAN Be Healthy participants only. PROCEDURE COV. CODE NOMENCLATURE BREAST RECONSTRUCTION OUTPATIENT CODES Delayed Insertion of Breast Prosthesis Nipple/Areola Reconstruction Breast Reconstruction with Tissue Expander Breast Reconstruction with other Technique PHYSICIAN CODES Immediate Insertion of Breast Prosthesis Following Mastopexy, Mastectomy, or in Reconstruction Delayed Insertion of Breast Prosthesis Following Mastopexy, or in Reconstruction Nipple/Areola Reconstruction Breast Reconstruction, Immediate or Delayed, With Tissue Expander Breast Reconstruction with Latisimus Dorsi Flap, With or Without Prosthetic Implant Breast Reconstruction with Free Flap Breast Reconstruction with Other Technique Breast Reconstruction with Transverse Rectus Abdominis Myocutaneous Flap (TRAM), Single Pedicel, Including Closure of Donor Site Breast Reconstruction with Transverse Rectus Abdominis Myocutaneous Flap (TRAM), Single Pedicel, Including Closure of Donor Site; with Micro Vascular Anastomosis Breast Reconstruction with Transverse Rectus Abdominis Myocutaneous Flap (TRAM), Double Pedicel, Including Closure of Donor Site APPENDIX II AII-1
94 Updated 12/06 PROCEDURE COV. CODE NOMENCLATURE MASTECTOMY CODES Mastectomy, Partial (eg Lumpectomy, Tylectomy, Quadrantectomy, Segmentectomy); Mastectomy, Partial (Quadrectomy or more); with Axillary Lymphadenectomy Mastectomy, Simple, Complete Mastectomy, Subcutaneous Mastectomy, Radical, Including Pectoral Muscles, Axillary Lymph Nodes Mastectomy, Radical, Including Pectoral Muscles, Axillary and Internal Mammary Lymph Nodes Mastectomy, Modified Radical, Including Axillary Lymph Nodes, with or without Pectoralis Minor Muscle, but Excluding Pectoralis Major Muscle Mastectomy; partial Mastectomy; partial with axillary lymphadenectomy Mastectomy, simple, complet Mastectomy, subcutaneous Mastectomy, radical, including pectoral muscles, axillary lymph nodes Mastectomy, radical, including pectoral muscles, axillary and internal mammary lymph nodes Mastectomy, modified radical, including axillary lymph nodes, with or without pectoralis minor muscle, but excluding pectoralis major muscle BREAST CANCER DIAGNOSES Malignant Neoplasm of the Breast Secondary Malignant Neoplasm of Skin 217 Benign Neoplasm of Breast Carcinoma in situ of Breast Neoplasm of Unspecified Nature of Breast APPENDIX II AII-2
95 Updated 12/06 DENTOALVEOLAR STRUCTURES PA* Unlisted Procedure, Dentoalveolar Structures is covered for the following procedures. Claims must include a detailed description of the actual service provided. If the description of the service is other than what is included on the list below, the service will be noncovered. Surgical removal, soft tissue impact each additional Pediatric dental procedures Simple extractions Full mouth extractions Dental service for non KAN Be Healthy recipients *Prior authorization is required for adults. Medical review is required for children age 21 and under. APPENDIX II AII-3
96 Updated 12/06 PROCEDURE COV. CODE NOMENCLATURE VAGAL NERVE STIMULATOR CODES PA Incision and subcutaneous placement of cranial neurostimulator pulse generator or receiver, direct or inductive coupling; with connection to a single electrode array PA Revision or removal or cranial neurostimulator pulse generator receiver PA Incision for implantation of neurostimulator electrodes; cranial nerve PA Revision or removal of peripheral neurostimulator electrodes PA Incision and subcutaneous placement of peripheral neurostimulator pulse generator or receiver, direct or indicative coupling PA Revision or removal of peripheral neurostimulator pulse generator or receiver Electronic analysis of implanted neurostimulator pulse generator system (such as rate, pulse, amplitude and duration, configuration of wave form, battery status, electrode selectability, output modulation, cycling impedance, and patient compliance measures); simple or complex brain, spinal cord, or peripheral (such as neuromuscular) neurostimulator pulse generator/transmitter without reprogramming Complex cranial nerve neurostimulator pulse generator/transmitter, with intraoperative or subsequent programming, with or without nerve interface testing, first hour PA Complex cranial nerve neurostimulator pulse generator/transmitter, with intraoperative or subsequent programming, each additional 30 minutes after first hour APPENDIX II AII-4
97 APPENDIX III Updated 11/03 DME/MEDICAL SUPPLIES IN A SWING BED NF PROGRAM Nutritional Therapy: Total nutritional replacement therapy is covered with prior authorization when billed through a durable medical equipment provider. (Enteral or parenteral nutrition must be the sole source of nutrition.) Nutritional supplements are not covered and are a part of the adult care home per diem rate. Oxygen Concentrator: This will be covered for rental when billed through the durable medical equipment provider and only when it is more economical than the tank oxygen method. Blood gas levels must demonstrate the medical necessity for oxygen. Refer to Section Urinary Supplies: Urinary supplies and accessories are covered services when billed through the durable medical equipment provider. Wheelchairs: Wheelchairs are included in the per diem rate with the exception that coverage through the Durable Medical Equipment Program will be considered by prior authorization for cases of exceptional wheelchair requirements. The following DME/medical supply items are considered routine and the responsibility of the Swing bed NF Program (unless used in excessive quantities): Alternating pressure pads and pumps Armboards Bedpans, urinals, basins Bed rails, beds & mattress and mattress covers Blood glucose, monitors and supplies Canes Commodes Compressors Crutches Denture Cups Dialysis, supplies & maintenance Dressing items (applicators, tongue blades, tape, gauze, bandages, bandaids, pads and compresses, ace bandages, vaseline gauze, cotton balls, slings, triangle APPENDIX IV AIII-1 bandages, pressure pads, and tracheostomy care kits) Emesis basins, bath basins Enemas and enema equipment Facial tissues & toilet paper First aid type ointments (e.g, Vaseline, Metholatum, Ben-Gay, K-Y Jelly) Footboards Footcradles Gel pads or cushion (e.g., Action Cushion) Geri-chairs Gloves, rubber or plastic Heating pads Heat lamps, examination light Humidifiers Ice bags, hot water bottles Intermittent Positive Pressure Breathing (IPPB) machines Irrigation solution (i.e., H2O normal saline) I.V. stands, clamps
98 Lifts Updated 11/03 Lotions, creams and powders (e.g., Dermassage, Noxema, baby lotion, oil and powders) Nebulizers Orthotics and splints to prevent or correct contractures Oxygen Masks, stands, tubing, regulators, hoses, catheters, cannulas, and humidifiers Parenteral, enteral infusion pumps Patient gowns, pajamas, bed linens Restraints Sheepskins, foam pads Skin antiseptics (e.g., Tinc of Benzoine, Tinc of Zephrin, Betadine, alcohol) Sphygmomanometers, stethoscopes, & other examination equipment Stretchers Suction pumps and tubing Syringes & needles (except insulin syringes and needles for diabetics that are covered by pharmacy program) Thermometers Traction apparatus & equipment Underpads & adult diapers (disposable/non-disp.) Walkers Water pitchers, glasses, Weighing scales Wheelchairs (manual) APPENDIX IV AIII-2
99 APPENDIX IV Updated 5/06 Hospital Cost Report To be eligible for payment from the Kansas Medical Assistance Program (KMAP), each hospital located in Kansas must complete, sign, and submit a copy of the cost report form (CMS ). An electronic copy of the Electronic Cost Report (ECR) and Print Image (PI) files are required along with the signed certification page. This must be done annually. The cost report and its instructions can be obtained from Medicare. Numerous private vendors offer services to assist in completing this cost report. KMAP has adopted this cost report, since it is already used by hospitals enrolled in the Medicare program. KMAP does not require any Medicaid specific schedules to be completed, although they may be referred to in the instructions. All general schedules of the report must be completed. Submit the report to the following address: Myers and Stauffer, LC. Certified Public Accountants 4123 SW Gage Center Drive, Suite 200 Topeka, KS For questions regarding the cost report, contact the above company at: Telephone: Telephone: Fax: KSCOST@mslc.com APPENDIX IV AIV-1
100 FORMS SECTION UB-04 MS-2126 ABORTION NECESSITY HYSTERECTOMY NECESSITY FORM NDC DETAIL ATTACHMENT FORM STERILIZATION CONSENT (ENGLISH) STERILIZATION CONSENT (SPANISH) HOW TO COMPLETE THE STERILIZATION FORM
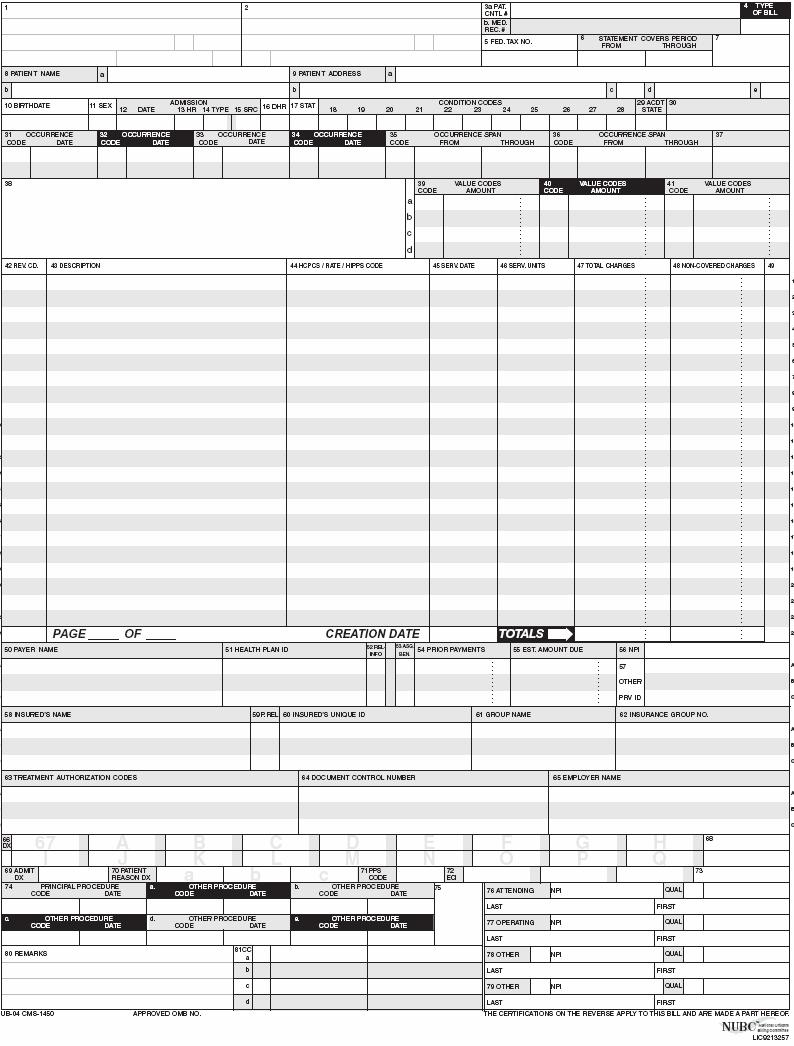
101
102 MS-2126 NOTIFICATION OF FACILITY ADMISSION/DISCHARGE Rev RESIDENT INFORMATION Name: SSN: Sex: Date of Birth: Client ID #: Responsible Person or Agency: Relationship: Responsible Person Address: II. FACILITY INFORMATION Facility Name/Location: Phone: Name of Agency/Person Placing Resident: Facility Fax: CARE or Screening Completed? Yes Date No Reason: Administrator s Signature (or Designee): Date: III. FACILITY PLACEMENT/DISCHARGE A. ADMISSION 1. Admission Date: Anticipated Length of Stay: 2. Admitted From (check one): NF ICF/MR NF/MH Hospital Private Home Swing Bed State Institution Assisted Living Other If admitted from facility, name of facility: 3. Pay Status on Admission (check one): Private Pay Medicare or Private Insurance Medicaid Other 4. Current Level of Care in Your Facility: Nursing Facility (NF SN) NF - Mental Health (NF MH) State Hospital - MR (SH SD) Swing Bed (NF SB) Head Injury/Rehb. (NF HI) State Hospital - MH (SH SM) PRTF (BF MH) ICF/MR (NF SD) B. DISCHARGE INFORMATION 1. Discharged to: (check one) 2. Discharge Date: 3. Date Deceased: Private Home Facility Swing Bed Assisted Living Hospital Other 3. If discharged to facility or hospital, name of facility: Level of Care: IV. HOSPITAL LEAVE (Complete for absences over 30 days only): Hospital: Date Admitted: Estimated: This form must be filed with the local SRS office within five working days of the date of admission, discharge, death, or hospital leave. Distribution: Original to Facility; Copy to Local SRS Office.
103 MS-2126 Instructions 1. The facility initiates the MS-2126 under the conditions specified in KEESM within five days of the event/request. Specific conditions prompting an MS-2126 include: A medical recipient is admitted or discharged from the facility A resident files an application for medical assistance A resident has been absent from the facility for 30 days or longer A resident changes level of care 2. Sections I and II are always completed. Sections III or IV are completed as necessary. 3. If the resident is in SRS or JJA custody, note this in Section 1 under responsible person/agency. Contact the designated individual in the SRS Regional Service Center if additional information is needed. 4. For Psychiatric Rehabilitation Treatment Facility, follow processing guidelines outlined in the appropriate KMAP provider manual regarding prior authorization and prescreening. 5. Indicate the results of any required pre-admission screening. It is the responsibility of the admitting facility to ensure these requirements are met. Note: A CARE assessment is NOT required for swing bed placements. 6. The facility shall retain the original MS-2126 and submit a copy to the SRS eligibility contact. 7. SRS will notify the facility when the MS-2126 is approved or denied. The facility will also be notified of the effective date and any applicable patient liability.
104 KANSAS HEALTH INSURANCE PROGRAM ABORTION NECESSITY FORM I, (Please print name of physician), certify that on the basis of my professional judgment, the pregnancy of (Name of patient) of (address), 1. Is endangering the life of the mother. 2. Is a result of rape. 3. Is a result of incest. (Signature of Physician) (Physician s Address) (Date)
105 Hysterectomy Necessity Form To be completed by the individual receiving the hysterectomy or her representative, if any:.(please print name and relation to patient) Please select one of the following choices and place your initials on the line next to the statement that best describes your situation. Prior to surgery, I received, orally and in writing, information stating that the hysterectomy would render me permanently incapable of reproducing. I understand that I will not be able to become pregnant or bear children. I am already sterile and incapable of bearing children. My physician and I have orally discussed my illness and he/she has given me written information on my illness that has led to the decision for this surgery. The illness/disease/symptoms that I have is called:. (Signature of Patient or Representative) (Date 00/00/00) (Signature of Physician ) (Date 00/00/00)

106 Kansas Medical Assistance Programs P. O. Box 3571 Topeka, KS Provider Line: Consumer Line: From the office of the Fiscal Agent NDC Detail Attachment This form is a required attachment for any Kansas Medicaid paper claim billed using a drug HCPCS code on a CMS-1500 or a UB-92 Provider Name Provider Number Beneficiary Name Beneficiary ID Number Date of Service LINE NDC DESCRIPTION UNITS BASIS OF MEASUREMENT *UNIT PRICE Please fill in: GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ GR ML UN F2 $ Legend: The corresponding line number from the CMS-1500 (HCFA-1500) or the UB-92 GR Gram NDC number used ML - Milliliter The drug description UN - Unit The actual quantity (units) given to the patient F2 International Unit Circle the appropriate basis of measurement * The unit price (If known)
107 Mo-8812 NOTICE CONSENT FORM YOUR DECISION AT ANY TIME NOT TO BE STERILIZED WILL NOT RESULT IN THE WITHDRAWAL OR WITHHOLDING OF ANY BENEFITS PROVIDED BY THE PROGRAMS OR PROJECTS RECEIVING FEDERAL FUNDS. 8 CONSENT TO STERILIZATION 8 I have asked for and received information about sterilization from when I first asked for the Doctor or Clinic information I was told the decision to be sterilized is completely up to me. I was told that I could decide not to be sterilized. If I decide not to be sterilized my decision will not affect my right to future care or treatment. I will not lose any help or benefits from programs receiving federal funds such as A.F.D.C. or Medicaid that I am now getting or for which I may become eligible. I UNDERSTAND THAT THE STERILIZATION MUST BE CONSIDERED PERMANENT AND NOT REVERSIBLE. I HAVE DECIDED THAT I DO NOT WANT TO BECOME PREGNANT, BEAR CHILDREN OR FATHER CHILDREN. I was told about those temporary methods of birth control that are available and could be provided to me which will allow me to bear or father children in the future. I have rejected these alternatives and chosen to be sterilized. I understand that I will be sterilized by an operation known as a. The discomforts, risks, and benefits associated with the operation have been explained to me. All my questions have been answered to my satisfaction. I understand that the operation will not be done until at least thirty days after I sign this form. I understand that I can change my mind at any time and that my decision at any time not to be sterilized will not result in the withholding of any benefits or medical services provided by federally funded programs. I am at least 21 years of age and was born on I hereby consent of my own free will to be sterilized by by a method called. My consent expires 180 days from the date of my signature below. I also consent to the release of this form and other medical records about the operation to: Representatives of the Department of Health and Human Services, or Employees of programs or projects funded by that Department but only for determining if Federal laws were observed. I have received a copy of this form. Date Signature Month Day Year You are requested to give the following information, but it is not required: 0 American Indian or 0 Black (not of Hispanic origin) Alaska Native 0 Hispanic 0 Asian or Pacific Islander 0 White (not of Hispanic origin) 8 INTERPRETER'S STATEMENT8 If an interpreter is provided to assist the individual to be sterilized: I have translated the information and advice presented orally to the individual to be sterilized b the person obtaining this consent I have also read to him/her the consent form in language and explained its contents to him/her. To the best of my knowledge and belief he/she understood this explanation. Interpreter Date (Revised 1/79) 8 STATEMENT OF PERSON OBTAINING CONSENT 8 Before signed the consent form. I explained to him/her the nature of the sterilization operation, the fact that it is intended to be a final and irreversible procedure and the discomforts, risks, and benefits associated with it. I counseled the individual to be sterilized that alternative methods of birth control are available which are temporary. I explained that sterilization is different because it is permanent. I informed the individual to be sterilized that his/her consent can be withdrawn at any tine and that he/she will not lose any health services or any benefits provided by Federal funds. To the best of my knowledge and belief the individual to be sterilized is at least 21 years old and appears to be mentally competent. He/she knowingly and voluntarily requested to be sterilized and appears to understand the nature and consequences of the procedure. signature Date Facility Address 8 PHYSICIANS STATEMENT 8 Shortly before I performed a sterilization operation upon on, I explained to him/her the nature of the sterilization operation, the fact that it is intended to be a final and irreversible procedure and the discomforts, risks, and benefits associated with it. I counseled the individual to be sterilized that alternative methods of birth control are available which are temporary. I explained that sterilization is different because it is permanent. I informed the individual to be sterilized that his/her consent can be withdrawn at any time and that he/she will not lose any health services or benefits provided by Federal funds. To the best of my knowledge and belief the individual to be sterilized is at least 21 years old and appears to be mentally competent. He/she knowingly and voluntarily requested to be sterilized and appears to understand the nature and consequences of the procedure. (Instructions for use of alternative final paragraphs: Use the first paragraph below except in the case of premature delivery or emergency abdominal surgery where the sterilization is performed less than 30 days after the date of the individual's signature on the consent form. In those cases, the second paragraph below must be used. Cross out the paragraph not used.) (1) At least thirty days have passed between the date of the individual's signature on this consent form and the date the sterilization was performed. (2) This sterilization was performed less than 30 days but not more than 72 hours after the date of the individual's signature on this consent form because of the following circumstances (check applicable box and fill in information requested) 0 Premature delivery 0 Individual's expected date of delivery: 0 Emergency abdominal surgery: (describe circumstances): Physician Date Provider Number
108
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. Hospital
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim................
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim................
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. Hospital
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim..................
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim..................
UPDATED Nursing/Intermediate Care Facility Providers
 December 2008 Provider Bulletin Number 8160 UPDATED Nursing/Intermediate Care Facility Providers Revenue Codes The revenue codes listed under field 42 for the UB-04 form were inadvertently deleted with
December 2008 Provider Bulletin Number 8160 UPDATED Nursing/Intermediate Care Facility Providers Revenue Codes The revenue codes listed under field 42 for the UB-04 form were inadvertently deleted with
Tips for Completing the UB04 (CMS-1450) Claim Form
 Claim Form") Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Subject: Updated UB-04 Paper Claim Form Requirements
 INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 2 J A N U A R Y 3 0, 2 0 0 7 To: All Providers Subject: Updated UB-04 Paper Claim Form Requirements Overview The following
INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 2 J A N U A R Y 3 0, 2 0 0 7 To: All Providers Subject: Updated UB-04 Paper Claim Form Requirements Overview The following
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Podiatry
 Fee-for-Service Provider Manual Podiatry Updated 03.2014 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Podiatry Billing Instructions.................. 7-1 Submission of Claim..................
Fee-for-Service Provider Manual Podiatry Updated 03.2014 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Podiatry Billing Instructions.................. 7-1 Submission of Claim..................
KANSAS MEDICAL ASSISTANCE PROGRAM. Provider Manual. Podiatry
 Provider Manual Podiatry Updated 07/2012 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Podiatry Billing Instructions.................. 7-1 Submission of Claim.................. 7-1 7010 Podiatry
Provider Manual Podiatry Updated 07/2012 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Podiatry Billing Instructions.................. 7-1 Submission of Claim.................. 7-1 7010 Podiatry
HOW TO SUBMIT OWCP-04 BILLS TO ACS
 HOW TO SUBMIT OWCP-04 BILLS TO ACS The following services should be billed on the OWCP-04 Form: General Hospital Hospice Nursing Home Rehabilitation Centers As a provider you have the option of sending
HOW TO SUBMIT OWCP-04 BILLS TO ACS The following services should be billed on the OWCP-04 Form: General Hospital Hospice Nursing Home Rehabilitation Centers As a provider you have the option of sending
Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims
 Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims Skilled Nursing Facility Services Custodial Care, SLP and Hospice R&B
Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims Skilled Nursing Facility Services Custodial Care, SLP and Hospice R&B
Archived 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION BILLING PROCEDURES FOR MEDICARE/MO HEALTHNET...5
 SECTION 15 - BILLING INSTRUCTIONS Contents 15.1 ELECTRONIC DATA INTERCHANGE...4 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION...4 15.3 UB-04 (CMS-1450) CLAIM FORM...5 15.4 PROVIDER COMMUNICATION UNIT...5 15.5
SECTION 15 - BILLING INSTRUCTIONS Contents 15.1 ELECTRONIC DATA INTERCHANGE...4 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION...4 15.3 UB-04 (CMS-1450) CLAIM FORM...5 15.4 PROVIDER COMMUNICATION UNIT...5 15.5
UB-92 Billing Instructions
 August 26, 2005 UB-92 Billing Instructions 2005 Hospital Provider Workshop Conduent MS Medicaid Project Government Healthcare Solutions Objective & Definition To explain how to complete a UB-92 claim form
August 26, 2005 UB-92 Billing Instructions 2005 Hospital Provider Workshop Conduent MS Medicaid Project Government Healthcare Solutions Objective & Definition To explain how to complete a UB-92 claim form
PARTNERSHIP HEALTHPLAN OF CALIFORNIA MEDI-CAL PROVIDER MANUAL CLAIMS DEPARTMENT
 III.A. CMS 1500 Billing Form Effective April 1, 2014, the information listed below are the CMS 1500 fields that must be completed accurately and completely in order to avoid claim suspense or denial. A
III.A. CMS 1500 Billing Form Effective April 1, 2014, the information listed below are the CMS 1500 fields that must be completed accurately and completely in order to avoid claim suspense or denial. A
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04 Claim Form Instructions
 UB-04 Claim Form This document explains the UB-04 claim form, which is used for submitting claims for reimbursement for specially designated facilities. The instructions included in this section are excerpts
UB-04 Claim Form This document explains the UB-04 claim form, which is used for submitting claims for reimbursement for specially designated facilities. The instructions included in this section are excerpts
Tips for Completing the CMS-1500 Version 02/12 Claim Form
 Tips for Completing the CMS-1500 Version 02/12 Claim Form NOTE: FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM. Enter in the white, open carrier
Tips for Completing the CMS-1500 Version 02/12 Claim Form NOTE: FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM. Enter in the white, open carrier
Format Specifications For the MHA DMS Publish Date: 11/20/2017
 Specifications For the MHA DMS 10 1.00.10 Publish Date: 11/20/2017 This document is updated periodically. If you are not reading this on the web but are instead reading a printed copy, please check our
Specifications For the MHA DMS 10 1.00.10 Publish Date: 11/20/2017 This document is updated periodically. If you are not reading this on the web but are instead reading a printed copy, please check our
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Non-PIHP Alcohol and Substance Abuse Community Based Services
 Fee-for-Service Provider Manual Non-PIHP Alcohol and Substance Abuse Community Based Services Updated 08.2015 PART II Introduction Section 7000 7010 8100 8200 8300 8400 Appendix BILLING INSTRUCTIONS Alcohol
Fee-for-Service Provider Manual Non-PIHP Alcohol and Substance Abuse Community Based Services Updated 08.2015 PART II Introduction Section 7000 7010 8100 8200 8300 8400 Appendix BILLING INSTRUCTIONS Alcohol
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. HCBS Autism Waiver
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL HCBS Autism Waiver Introduction Section 7000 7010 8100 8300 8400 BILLING INSTRUCTIONS HCBS Autism Waiver Billing Instructions... Submission of Claim...
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL HCBS Autism Waiver Introduction Section 7000 7010 8100 8300 8400 BILLING INSTRUCTIONS HCBS Autism Waiver Billing Instructions... Submission of Claim...
Connecticut interchange MMIS
 Connecticut interchange MMIS Provider Manual Chapter 8 Hospital Claim Submission Instructions Connecticut Department of Social Services (DSS) 55 Farmington Avenue Hartford, CT 06105 HP Enterprise Services
Connecticut interchange MMIS Provider Manual Chapter 8 Hospital Claim Submission Instructions Connecticut Department of Social Services (DSS) 55 Farmington Avenue Hartford, CT 06105 HP Enterprise Services
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File
 North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (Diag1, fac, ptzip)
North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (Diag1, fac, ptzip)
WYOMING MEDICAID PROVIDER MANUAL. Medical Services HCFA-1500
 WYOMING MEDICAID PROVIDER MANUAL Medical Services HCFA-1500 Medical Services March 01,1999 Table of Contents AUTHORITY... 1-1 Chapter One... 1-1 General Information... 1-1 How the Billing Manual is organized...
WYOMING MEDICAID PROVIDER MANUAL Medical Services HCFA-1500 Medical Services March 01,1999 Table of Contents AUTHORITY... 1-1 Chapter One... 1-1 General Information... 1-1 How the Billing Manual is organized...
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. HCBS TBI Cognitive Therapy
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL HCBS TBI Cognitive Therapy PART II TBI COGNITIVE THERAPY PROVIDER MANUAL Section BILLING INSTRUCTIONS Page 7000 TBI Cognitive Therapy Billing Instructions............
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL HCBS TBI Cognitive Therapy PART II TBI COGNITIVE THERAPY PROVIDER MANUAL Section BILLING INSTRUCTIONS Page 7000 TBI Cognitive Therapy Billing Instructions............
May 2007 Provider Bulletin Number 753. Hospice Providers. Changes to ICF/MR Room and Board Charges for Hospice Beneficiaries
 May 2007 Provider Bulletin Number 753 Hospice Providers Changes to ICF/MR Room and Board Charges for Hospice Beneficiaries This is an update to bulletin 743. A correction has been made regarding how to
May 2007 Provider Bulletin Number 753 Hospice Providers Changes to ICF/MR Room and Board Charges for Hospice Beneficiaries This is an update to bulletin 743. A correction has been made regarding how to
North Carolina Emergency Department Visit Data - Data Dictionary FY2012 Alphabetic List of Variables and Attributes Standard Research File
 North Carolina Emergency Department Visit Data - Data Dictionary FY2012 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (diag1, fac, or
North Carolina Emergency Department Visit Data - Data Dictionary FY2012 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (diag1, fac, or
Chapter 6 Section 3. Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment)
") Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
CMS-1500 Billing and Reimbursement. HP Provider Relations/October 2013
 CMS-1500 Billing and Reimbursement HP Provider Relations/October 2013 Agenda Common Denials for CMS-1500 CMS-1500 Claims Billing Types of CMS-1500 Claims Paper Claim Billing Fee Schedule Crossover Claims
CMS-1500 Billing and Reimbursement HP Provider Relations/October 2013 Agenda Common Denials for CMS-1500 CMS-1500 Claims Billing Types of CMS-1500 Claims Paper Claim Billing Fee Schedule Crossover Claims
Nursing Facility UB-04 Paper Billing Guide
 Nursing Facility UB-04 Paper Billing Guide Oregon Medicaid Nursing Facilities November 2008 1 Effective 11/17/08 TABLE OF CONTENTS Introduction... 3 Claims Processing General Information... 4 Required
Nursing Facility UB-04 Paper Billing Guide Oregon Medicaid Nursing Facilities November 2008 1 Effective 11/17/08 TABLE OF CONTENTS Introduction... 3 Claims Processing General Information... 4 Required
Rural Health Clinic Overview
 TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS
 SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 REQUIRED ATTACHMENTS...3 14.1.A RESUBMISSIONS...3 14.1.B HOW TO ORDER ATTACHMENTS...3 14.2 CERTIFICATION OF MEDICAL NECESSITY FOR ABORTION...4 14.2.A
SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 REQUIRED ATTACHMENTS...3 14.1.A RESUBMISSIONS...3 14.1.B HOW TO ORDER ATTACHMENTS...3 14.2 CERTIFICATION OF MEDICAL NECESSITY FOR ABORTION...4 14.2.A
Home and Community Based Services Mental Retardation/Developmental Disabilities Providers
 May 2008 Provider Bulletin Number 869 Home and Community Based Services Mental Retardation/Developmental Disabilities Providers Manual Updates and New Manuals Home and Community Based Services Mental Retardation/Developmental
May 2008 Provider Bulletin Number 869 Home and Community Based Services Mental Retardation/Developmental Disabilities Providers Manual Updates and New Manuals Home and Community Based Services Mental Retardation/Developmental
HCBS MRDD Home Modifications
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL HCBS MRDD Home Modifications PART II MR/DD HOME MODIFICATIONS PROVIDER MANUAL Section BILLING INSTRUCTIONS Page 7000 MR/DD Home Modifications Billing Instructions.........
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL HCBS MRDD Home Modifications PART II MR/DD HOME MODIFICATIONS PROVIDER MANUAL Section BILLING INSTRUCTIONS Page 7000 MR/DD Home Modifications Billing Instructions.........
Place of Service Code Description Conversion
 Place of Conversion CMS Place of Code Place of Name The place of service field indicates where the services were performed Possible values include: Code Description Inpatient Outpatient Office Home 5 Independent
Place of Conversion CMS Place of Code Place of Name The place of service field indicates where the services were performed Possible values include: Code Description Inpatient Outpatient Office Home 5 Independent
Administrative Guide. KanCare Program Chapter 11: Hospice. Physician, Health Care Professional, Facility and Ancillary. UHCCommunityPlan.
 KanCare Program Physician, Health Care Professional, Facility and Ancillary Administrative Guide Doc#: PCA-1-003044_06202016 UHCCommunityPlan.com Welcome to UnitedHealthcare This administrative guide is
KanCare Program Physician, Health Care Professional, Facility and Ancillary Administrative Guide Doc#: PCA-1-003044_06202016 UHCCommunityPlan.com Welcome to UnitedHealthcare This administrative guide is
Targeted Case Management- Mental Health
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Targeted Case Management- Mental Health Part II TARGETED CASE MANAGEMENT-MENTAL HEALTH PROVIDER MANUAL Introduction Section 7000 7010 8100 8300 8400 Forms
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Targeted Case Management- Mental Health Part II TARGETED CASE MANAGEMENT-MENTAL HEALTH PROVIDER MANUAL Introduction Section 7000 7010 8100 8300 8400 Forms
Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Amended Date: October 1, Table of Contents
 Amended Date: October 1, Table of Contents") Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 2.0 Eligibility Requirements...
Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 2.0 Eligibility Requirements...
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Rural Health Clinic/ Federally Qualified Health Center
 Fee-for-Service Provider Manual Rural Health Clinic/ Federally Qualified Health Center Updated 08.2013 PART II RURAL HEALTH CLINIC AND FEDERALLY QUALIFIED HEALTH CENTER FEE-FOR-SERVICE PROVIDER MANUAL
Fee-for-Service Provider Manual Rural Health Clinic/ Federally Qualified Health Center Updated 08.2013 PART II RURAL HEALTH CLINIC AND FEDERALLY QUALIFIED HEALTH CENTER FEE-FOR-SERVICE PROVIDER MANUAL
AMBULATORY SURGERY FACILITY GENERAL INFORMATION
 AMBULATORY SURGERY FACILITY GENERAL INFORMATION I. BCBSM s Ambulatory Surgery Facility Programs Traditional BCBSM s Traditional Ambulatory Surgery Facility Program includes all facilities that are licensed
AMBULATORY SURGERY FACILITY GENERAL INFORMATION I. BCBSM s Ambulatory Surgery Facility Programs Traditional BCBSM s Traditional Ambulatory Surgery Facility Program includes all facilities that are licensed
Florida Medicaid. State Mental Health Hospital Services Coverage Policy. Agency for Health Care Administration. January 2018
 Florida Medicaid State Mental Health Hospital Services Coverage Policy Agency for Health Care Administration Table of Contents 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions...
Florida Medicaid State Mental Health Hospital Services Coverage Policy Agency for Health Care Administration Table of Contents 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions...
District of Columbia Medicaid Specialty Hospital Project Frequently Asked Questions
 District of Columbia Medicaid Specialty Hospital Project Frequently Asked Questions Version Date: September 22, 2014 UPDATE: The District of Columbia Department of Health Care Finance (DHCF) is submitting
District of Columbia Medicaid Specialty Hospital Project Frequently Asked Questions Version Date: September 22, 2014 UPDATE: The District of Columbia Department of Health Care Finance (DHCF) is submitting
Hospital Refresher Workshop. Presented by The Department of Social Services & HP Enterprise Services
 Hospital Refresher Workshop Presented by The Department of Social Services & HP Enterprise Services 1 Training Topics Provider Bulletins Outpatient Claim Billing Changes Explanation of Benefit Codes Web
Hospital Refresher Workshop Presented by The Department of Social Services & HP Enterprise Services 1 Training Topics Provider Bulletins Outpatient Claim Billing Changes Explanation of Benefit Codes Web
Policies Regarding Network Provider Payment
 CLAIMS PAYMENT (NOTE: Below please find guidelines ValueOptions follows when processing claims for most accounts. If you believe there may be a specific set of guidelines that need to be followed for your
CLAIMS PAYMENT (NOTE: Below please find guidelines ValueOptions follows when processing claims for most accounts. If you believe there may be a specific set of guidelines that need to be followed for your
BCBSNC Best Practices
 BCBSNC Best Practices Thank you for attending today! We value your commitment of caring for our members your patients and our shared goals for their improved health An independent licensee of the Blue
BCBSNC Best Practices Thank you for attending today! We value your commitment of caring for our members your patients and our shared goals for their improved health An independent licensee of the Blue
Nebraska pays for telepsychiatry + a separate transmission fee ($.08/minute).
.") Nebraska pays for telepsychiatry + a separate transmission fee ($.08/minute). Nebraska Telehealth Statutes 2014 Legislative Bill 1076 enacted in 2014 allows Medicaid payment for telehealth when patient
Nebraska pays for telepsychiatry + a separate transmission fee ($.08/minute). Nebraska Telehealth Statutes 2014 Legislative Bill 1076 enacted in 2014 allows Medicaid payment for telehealth when patient
Administrative Billing Data
 Administrative Billing Data Patient Identification and Demographic Information: From UB-04 Data or Medical Record Face Sheet. Note: When you go to enter data on this case, the information below will already
Administrative Billing Data Patient Identification and Demographic Information: From UB-04 Data or Medical Record Face Sheet. Note: When you go to enter data on this case, the information below will already
Chapter 9 Section 1. Ambulatory Surgical Center (ASC) Reimbursement
 Reimbursement") Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
FHCA 2014 Annual Conference & Trade Show
 FHCA 2014 Annual Conference & Trade Show CE Session #49 Medicaid Managed Care Billing: Purely A Provider s Perspective Thursday, July 10 4:00 to 6:00 p.m. Crystal N/J2 Finance/Development Upon completion
FHCA 2014 Annual Conference & Trade Show CE Session #49 Medicaid Managed Care Billing: Purely A Provider s Perspective Thursday, July 10 4:00 to 6:00 p.m. Crystal N/J2 Finance/Development Upon completion
AMBULATORY SURGICAL CENTERS PROVIDER MANUAL Chapter Twenty-nine of the Medicaid Services Manual
 AMBULATORY SURGICAL CENTERS PROVIDER MANUAL Chapter Twenty-nine of the Medicaid Services Manual Issued November 1, 2010 Claims/authorizations for dates of service on or after October 1, 2015 must use the
AMBULATORY SURGICAL CENTERS PROVIDER MANUAL Chapter Twenty-nine of the Medicaid Services Manual Issued November 1, 2010 Claims/authorizations for dates of service on or after October 1, 2015 must use the
VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION
 VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION GENERAL INFORMATION Primary Practice Facility Location The type of application being submitted: Please choose facility type (check all that apply):
VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION GENERAL INFORMATION Primary Practice Facility Location The type of application being submitted: Please choose facility type (check all that apply):
Section 7. Medical Management Program
 Section 7. Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent fraud, waste and abuse in its programs.
Section 7. Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent fraud, waste and abuse in its programs.
Table of Contents. 1.0 Description of the Procedure, Product, or Service Definitions Hospice Terminal illness...
 Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 1.1.1 Hospice... 1 1.1.2 Terminal illness... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1
Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 1.1.1 Hospice... 1 1.1.2 Terminal illness... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1
Chapter 11 Section 3. Hospice Reimbursement - Conditions For Coverage
 Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Non- PAPH Outpatient Mental Health
 Fee-for-Service Provider Manual Non- PAPH Outpatient Mental Health Updated 05.2014 PART II Introduction Section 7000 7010 8100 8200 8300 8400 8410 Appendix BILLING INSTRUCTIONS Non-PAHP Outpatient Mental
Fee-for-Service Provider Manual Non- PAPH Outpatient Mental Health Updated 05.2014 PART II Introduction Section 7000 7010 8100 8200 8300 8400 8410 Appendix BILLING INSTRUCTIONS Non-PAHP Outpatient Mental
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Facilities and Ancillaries This supplement of the Optima Health Provider Manual provides information of specific interest to Optima Health contracted
Optima Health Provider Manual Supplemental Information For Facilities and Ancillaries This supplement of the Optima Health Provider Manual provides information of specific interest to Optima Health contracted
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:
 Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:") Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Provider-Based RHC Billing June 8, 2018
 Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
BCBSNC Provider Application for Participation
 BCBSNC Provider Application for Participation This application is to be used if you wish to become a participating provider facility with BCBSNC. This application is not a contract. Please follow the applicable
BCBSNC Provider Application for Participation This application is to be used if you wish to become a participating provider facility with BCBSNC. This application is not a contract. Please follow the applicable
CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT
 CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT Table of Contents 1. Introduction 2. When a provider is deemed to accept Flexi Blue PFFS terms and
CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT Table of Contents 1. Introduction 2. When a provider is deemed to accept Flexi Blue PFFS terms and
Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) Care Healthcare and VNSNY CHOICE Transition
 Claim Submission Instructions (MLTC) Care Healthcare and VNSNY CHOICE Transition") 2018 Provider Manual VNSNY CHOICE Appendix V Claims CMS-1500 Form (Sample) UB-04 Form (Sample) Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) ICD-10 FAQ Care Healthcare
2018 Provider Manual VNSNY CHOICE Appendix V Claims CMS-1500 Form (Sample) UB-04 Form (Sample) Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) ICD-10 FAQ Care Healthcare
Chapter 9 Section 1. Ambulatory Surgical Center (ASC) Reimbursement
 Reimbursement") Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
INSTITUTIONAL. Covered services and limitations module
 INSTITUTIONAL Covered services and limitations module UB-92 Covered Services and Limitations Module Comprehensive Outpatient Rehabilitation Facility (CORF)...2 Critical Access Hospital (CAH)...3 End Stage
INSTITUTIONAL Covered services and limitations module UB-92 Covered Services and Limitations Module Comprehensive Outpatient Rehabilitation Facility (CORF)...2 Critical Access Hospital (CAH)...3 End Stage
CHAPTER 3: EXECUTIVE SUMMARY
 INDIANA PROVIDER MANUAL EXECUTIVE SUMMARY Indiana Family and Social Services Administration (FSSA) contracts with Anthem Insurance Companies, Inc. (dba Anthem Blue Cross and Blue Shield) for the provision
INDIANA PROVIDER MANUAL EXECUTIVE SUMMARY Indiana Family and Social Services Administration (FSSA) contracts with Anthem Insurance Companies, Inc. (dba Anthem Blue Cross and Blue Shield) for the provision
This letter gives notice of an adopted rule: MaineCare Benefits Manual, Chapters II & III, Section 45, Hospital Services.
 Department of Health and Human Services MaineCare Services 242 State Street 11 State House Station Augusta, Maine 04333-0011 Tel.: (207) 287-2674; Fax: (207) 287-2675 TTY Users: Dial 711 (Maine Relay)
Department of Health and Human Services MaineCare Services 242 State Street 11 State House Station Augusta, Maine 04333-0011 Tel.: (207) 287-2674; Fax: (207) 287-2675 TTY Users: Dial 711 (Maine Relay)
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Local Education Agency
 Fee-for-Service Provider Manual Local Education Agency Updated 07.2018 Introduction PART II Section Page 7000 Local Education Agency Billing Instructions............ 7-1 7010 Local Education Agency Billing
Fee-for-Service Provider Manual Local Education Agency Updated 07.2018 Introduction PART II Section Page 7000 Local Education Agency Billing Instructions............ 7-1 7010 Local Education Agency Billing
Section A Identification Information
 r Minimum Data Set (MDS) 3.0 Instructor Guide Section A Identification Information Objectives State the intent of Section A Identification Information. Describe the information required to complete Section
r Minimum Data Set (MDS) 3.0 Instructor Guide Section A Identification Information Objectives State the intent of Section A Identification Information. Describe the information required to complete Section
Medical Management Program
 Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent Fraud, Waste and Abuse in its programs. The Molina
Medical Management Program Introduction Molina Healthcare maintains a medical management program to ensure patient safety as well as detect and prevent Fraud, Waste and Abuse in its programs. The Molina
2018 Northern California HMO Provider Manual Kaiser Foundation Health Plan, Inc.
 2018 Northern California HMO Provider Manual Kaiser Foundation Health Plan, Inc. Welcome from Kaiser Permanente It is our pleasure to welcome you as a contracted provider (Provider) participating under
2018 Northern California HMO Provider Manual Kaiser Foundation Health Plan, Inc. Welcome from Kaiser Permanente It is our pleasure to welcome you as a contracted provider (Provider) participating under
OFFICIAL NOTICE DMS-2003-A-2 DMS-2003-II-6 DMS-2003-SS-2 DMS-2003-R-12 DMS-2003-O-7 DMS-2003-L-8 DMS-2003-KK-9 DMS-2003-OO-7
 Arkansas Department of Human Services Division of Medical Services Donaghey Plaza South PO Box 1437 Little Rock, Arkansas 72203-1437 Internet Website: www.medicaid.state.ar.us Telephone: (501) 682-8292
Arkansas Department of Human Services Division of Medical Services Donaghey Plaza South PO Box 1437 Little Rock, Arkansas 72203-1437 Internet Website: www.medicaid.state.ar.us Telephone: (501) 682-8292
District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions
 District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions Version Date: July 20, 2017 Updates for October 1, 2017 Effective October 1, 2017 (the District s fiscal year
District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions Version Date: July 20, 2017 Updates for October 1, 2017 Effective October 1, 2017 (the District s fiscal year
Florida Medicaid. Outpatient Hospital Services Coverage Policy. Agency for Health Care Administration. Draft Rule
 Florida Medicaid Agency for Health Care Administration Draft Rule Table of Contents Florida Medicaid 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions... 1 2.0 Eligible
Florida Medicaid Agency for Health Care Administration Draft Rule Table of Contents Florida Medicaid 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions... 1 2.0 Eligible
Managed Care Referrals and Authorizations (Central Region Products)
") In this section Page Overview of Referrals and Authorizations 10.1 Referrals 10.1! Referrals: SelectBlue only 10.1! Definition of referrals 10.1! Services not requiring a referral 10.1! Who can issue a
In this section Page Overview of Referrals and Authorizations 10.1 Referrals 10.1! Referrals: SelectBlue only 10.1! Definition of referrals 10.1! Services not requiring a referral 10.1! Who can issue a
Molina Healthcare MyCare Ohio Prior Authorizations
 Molina Healthcare MyCare Ohio Prior Authorizations Agenda Eligibility Medicare Passive Enrollment Transition of Care Definition Submission Time Frame Standard vs. Urgent How to Submit a Prior Authorization
Molina Healthcare MyCare Ohio Prior Authorizations Agenda Eligibility Medicare Passive Enrollment Transition of Care Definition Submission Time Frame Standard vs. Urgent How to Submit a Prior Authorization
Medi-Pak Advantage: Reimbursement Methodology
 Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
Medi-Pak Advantage: Reimbursement Methodology The information located on the following pages is intended to summarize the reimbursement methodologies for Medi-Pak Advantage: Medi-Pak Advantage reimburses
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
Nursing facility/swing bed
 Nursing facility/swing bed KSPEC-2176-18 August 2018 We will cover Client assessment, referral and evaluation (CARE) assessments Quick Fax Sheet Level of care (LOC) MS-2126 Form Eligibility verification
Nursing facility/swing bed KSPEC-2176-18 August 2018 We will cover Client assessment, referral and evaluation (CARE) assessments Quick Fax Sheet Level of care (LOC) MS-2126 Form Eligibility verification
OptumHealth Operations Guide
 OptumHealth Operations Guide Kidney Resource Services Table of Contents Operations Guide Overview...3 KIDNEY RESOURCE SERVICES PROGRAM OVERVIEW...3 HEALTH CARE PROVIDER ON-BOARDING PROCESS...3 CLINICAL
OptumHealth Operations Guide Kidney Resource Services Table of Contents Operations Guide Overview...3 KIDNEY RESOURCE SERVICES PROGRAM OVERVIEW...3 HEALTH CARE PROVIDER ON-BOARDING PROCESS...3 CLINICAL
Care Plan Oversight Services and Physician Services for Certification
 Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
Blue Choice PPO SM Physician, Professional Provider, Facility and Ancillary Provider - Provider Manual Table of Contents (TOC)
") THIS MANUAL CONTAINS A REQUIRED DISCLOSURE CONCERNING BLUE CROSS AND BLUE SHIELD OF TEXAS CLAIMS PROCESSING PROCEDURES Blue Choice PPO SM Physician, Professional Provider, Facility and Ancillary Provider
THIS MANUAL CONTAINS A REQUIRED DISCLOSURE CONCERNING BLUE CROSS AND BLUE SHIELD OF TEXAS CLAIMS PROCESSING PROCEDURES Blue Choice PPO SM Physician, Professional Provider, Facility and Ancillary Provider
Version 5010 Errata Provider Handout
 Version 5010 Errata Provider Handout 5010 Bringing Clarity & Consistency To Your Electronic Transactions Benefits Transactions Impacted Changes Impacting Providers While we have highlighted the HIPAA Version
Version 5010 Errata Provider Handout 5010 Bringing Clarity & Consistency To Your Electronic Transactions Benefits Transactions Impacted Changes Impacting Providers While we have highlighted the HIPAA Version
CMS , Ch 13, Sec
 Direct supervision by a provider is required Must be in clinic, not in same room being in the hospital when attached to clinic is NOT incident to Part of provider s services previously ordered integral,
Direct supervision by a provider is required Must be in clinic, not in same room being in the hospital when attached to clinic is NOT incident to Part of provider s services previously ordered integral,
NJDDCS VERSION 2 DATA DICTIONARY And DATA EXTRACT FILE LAYOUT Version 17.2
 NJDDCS VERSION 2 DATA DICTIONARY And DATA EXTRACT FILE LAYOUT Version 17.2 Table of Contents Introduction... 5 Accident State... 6 Acute Days... 7 Admission Hour... 8 Admission/Start of Care Date (Admission
NJDDCS VERSION 2 DATA DICTIONARY And DATA EXTRACT FILE LAYOUT Version 17.2 Table of Contents Introduction... 5 Accident State... 6 Acute Days... 7 Admission Hour... 8 Admission/Start of Care Date (Admission
Place of Service Codes (POS) and Definitions
 and Definitions") 2950 Robertson Ave, Suite 200 Cincinnati, OH 45209 (P): 513-281-4400 www.medicalreimbursementinc.com www.linkedin.com/company/medical-reimbursement-inc www.twitter.com/medreimburse www.facebook.com/medicalreimbursementinc
2950 Robertson Ave, Suite 200 Cincinnati, OH 45209 (P): 513-281-4400 www.medicalreimbursementinc.com www.linkedin.com/company/medical-reimbursement-inc www.twitter.com/medreimburse www.facebook.com/medicalreimbursementinc
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
CRS Report for Congress Received through the CRS Web
 CRS Report for Congress Received through the CRS Web Order Code RS20386 Updated April 16, 2001 Medicare's Skilled Nursing Facility Benefit Summary Heidi G. Yacker Information Research Specialist Information
CRS Report for Congress Received through the CRS Web Order Code RS20386 Updated April 16, 2001 Medicare's Skilled Nursing Facility Benefit Summary Heidi G. Yacker Information Research Specialist Information
OBSERVATION CARE EVALUATION AND MANAGEMENT CODES POLICY
 OBSERVATION CARE EVALUATION AND MANAGEMENT CODES POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: ADMINISTRATIVE 232.10 T0 Effective Date: March 1, 2017 Table of Contents Page INSTRUCTIONS
OBSERVATION CARE EVALUATION AND MANAGEMENT CODES POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: ADMINISTRATIVE 232.10 T0 Effective Date: March 1, 2017 Table of Contents Page INSTRUCTIONS
Chapter 02 Hospital Based Care
 Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
9.1.1 Medicaid Managed Care Enrollment Prior Authorization Emergency Ambulance Services
 Section 9Ambulance 9 9.1 Enrollment........................................................ 9-2 9.1.1 Medicaid Managed Care Enrollment................................. 9-2 9.2 Reimbursement....................................................
Section 9Ambulance 9 9.1 Enrollment........................................................ 9-2 9.1.1 Medicaid Managed Care Enrollment................................. 9-2 9.2 Reimbursement....................................................
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL
 TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
Observation Services Tool for Applying MCG Care Guidelines
 In the event of a conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include
In the event of a conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include
Health Management Policy
 Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Chapter. CPT only copyright 2008 American Medical Association. All rights reserved. 30Radiation Therapy Services
 Chapter 30Radiation Therapy Services 30 30.1 Enrollment...................................................... 30-2 30.2 Benefits, Limitations, and Authorization Requirements...................... 30-2
Chapter 30Radiation Therapy Services 30 30.1 Enrollment...................................................... 30-2 30.2 Benefits, Limitations, and Authorization Requirements...................... 30-2
All Indiana Health Coverage Programs Providers. Package C Claim Submission and Coverage Information
 P R O V I D E R B U L L E T I N B T 2 0 0 0 0 6 J A N U A R Y 2 0, 2 0 0 0 To: Subject: All Indiana Health Coverage Programs Providers Package C Claim Submission and Coverage Information Overview The purpose
P R O V I D E R B U L L E T I N B T 2 0 0 0 0 6 J A N U A R Y 2 0, 2 0 0 0 To: Subject: All Indiana Health Coverage Programs Providers Package C Claim Submission and Coverage Information Overview The purpose
Blue Shield High Deductible Plan
 Blue Shield High Deductible Plan Benefit Booklet Stanford University Group Number: 170293, 976184 & 976185 Effective Date: January 1, 2014 An independent member of the Blue Shield Association Claims Administered
Blue Shield High Deductible Plan Benefit Booklet Stanford University Group Number: 170293, 976184 & 976185 Effective Date: January 1, 2014 An independent member of the Blue Shield Association Claims Administered
LifeWise Reference Manual LifeWise Health Plan of Oregon
 11 UB-04 Billing Description This chapter contains participation, claims and billing information for providers who bill on a UB-04 (CMS 1450) claim form. This chapter supplements information contained
11 UB-04 Billing Description This chapter contains participation, claims and billing information for providers who bill on a UB-04 (CMS 1450) claim form. This chapter supplements information contained
KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance. UM Retrospective Review Services.
 KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance UM Retrospective Review Services Provider Manual August 2017 This page intentionally blank Table of Contents KDHE-DHCF:
KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance UM Retrospective Review Services Provider Manual August 2017 This page intentionally blank Table of Contents KDHE-DHCF:
Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services(CMS) Transmittal 1361 Date: NOVEMBER 2, 2007
 Centers for Medicare & Medicaid Services(CMS) Transmittal 1361 Date: NOVEMBER 2, 2007") CMS Manual System Pub 100-04 Medicare Claims Processing Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services(CMS) Transmittal 1361 Date: NOVEMBER 2, 2007 Change Request
CMS Manual System Pub 100-04 Medicare Claims Processing Department of Health & Human Services (DHHS) Centers for Medicare & Medicaid Services(CMS) Transmittal 1361 Date: NOVEMBER 2, 2007 Change Request
Connecticut Medical Assistance Program Refresher for Hospice Providers. Presented by The Department of Social Services & HP for Billing Providers
 Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Training Topics Hospice Agenda HIPAA 5010 Hospice Form
Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Training Topics Hospice Agenda HIPAA 5010 Hospice Form
Chapter. CPT only copyright 2009 American Medical Association. All rights reserved. 31Radiation Therapy Services
 Chapter 31Radiation Therapy Services 31 31.1 Enrollment...................................................... 31-2 31.2 Benefits, Limitations, and Authorization Requirements...................... 31-2
Chapter 31Radiation Therapy Services 31 31.1 Enrollment...................................................... 31-2 31.2 Benefits, Limitations, and Authorization Requirements...................... 31-2