Credentialing Application and Process
|
|
|
- Esmond Hopkins
- 6 years ago
- Views:
Transcription

1 Credentialing Application and Process
2 What is Credentialing? Credentialing is the process of obtaining, verifying and assessing the qualifications of a healthcare practitioner to provide patient care services in or for a healthcare entity. To ensure consistency of credentialing, recredentialing, and privileging, a routine process should be followed. This assures accuracy of approach and process as well as minimize the variation in references received. Use of the same process for each new applicant or re-applicant also reduces the opportunity of charges of discrimination (from the applicant) if there is a negative outcome.
3 Reasons for Credentialing Patient Safety-This is the number one concern. The patient is put before anything else. Every organization as part of their mission statement refers to providing high quality patient care. Only those providers who meet high quality standards should be providing care to your members. Risk Management-If a patient suffers an adverse outcome in a healthcare setting, the healthcare entity can be held liable. If the provider has problems that would have been revealed by credentialing, but the credentialing was not performed, the entity may be liable for any patient harm caused by the substandard clinician. Required by Accrediting and Regulatory Agencies-Federal Regulations protect patient health and safety. To ensure quality of care, Medicare Conditions of Participation (CoP), Joint Commission Standards (JCAHO), National Committee for Quality Assurance (NCQA) Standards and Health Plan Policies all require practitioner credentialing.
4 Who Needs to Be Credentialed? Licensed Independent Practitioner-An individual permitted by law to provide care and services without direction or supervision, within the scope of the individual s license and consistent with individually granted clinical privileges. (MD, DO, DPM, DC, DDS, OD, PhD, LCSW, MFCC, MFT, MHC, PT, OT, SLT) Licensed or Certified Healthcare Practitioner-An individual who is licensed, registered, or certified but is not permitted by law to provide patient care services without direction or supervision. (Certified Nurse Midwife, Physician Assistant, Nurse Practitioner)
5 Non Discriminatory Practice Practitioner participation is a privilege which is afforded to professionally licensed or certified, qualified and competent practitioners, contingent upon the approval of their credentials according to policy. ¹Gender, race, ethnicity, religious conviction, national identity/origin, age, marital status, sexual orientation or any other criteria lacking professional justification shall not be considered in determining a practitioner s qualifications for employment or contract. ¹This information will be used for consumer information only.
6 Confidentiality Practitioner Credential files, Peer Review Work Product and Credentialing Committee minutes are treated as confidential and kept in locked files and/or secured electronically. Documents in these files may not be reproduced or distributed, except for confidential peer review and credentialing purposes consistent with Section 1157 of the California Evidence Code. The Health Insurance Portability and Accountability Act of 1996 (HIPAA) requireshealth information be protected. Patient information, physician health information and patient complaints are often times a part of the practitioner credentials file. All those involved in the credentialing process must protect the confidentiality and integrity of credentials files and guard against unauthorized access to and modification of credentials files.

7 The Application-Page 1 Section I: Instructions This form should be typed or legibly printed in black or blue ink. If more space is needed than provided, attach additional sheets and reference the question being answered. Please do not use abbreviations when completing the application. Section II: Demographics Demographic and personal information about the applicant and his/her area of practice. Section III: Practice Information Practice/Clinic address, phone, fax and contact information.

8 The Application-Page 2 Section III: Continued Any additional practice addresses are listed here. Section IV: Pre-Medical Education Section V: Medical/Professional Education Section VI: Internship/PGY1
9 The Application-Page 3 Section VII: Residencies/Fellowships Include Residencies, Fellowships, Preceptorships, Teaching/Faculty appointments (indicate whether clinical or academic), Research programs and postgraduate education in chronological order. Include all programs you attended, whether or not completed. Section VIII. Board Certification Any certifying, specialty board you have been certified through. If certification has expired, must provide a brief explanation

10 The Application-Page 4 Section IX. Other Certifications Section X. Medical/Professional Licensure/Registration Section XI. All other State/Medical Licensure Section XII. Professional Liability Current insurance carrier information maybe clinic s coverage. List all previous insurance carriers from previous five years.


11 The Application-Page 5 Section XIII. Hospital and Other Institutional Affiliations Please list your current affiliation(s) first, followed by any affiliations you have previously had in the past ten (10) years.
12 The Application-Page 6 Section XIV. Peer References List four references, which are directly familiar with your work, either via direct clinical observation or through close working relations. Section XV. Work History Chronologically list all work history activities since completion of postgraduate training (use extra sheets if necessary). This information must be complete. A curriculum vita is sufficient provided it is current and contains all information requested below. Please explain in writing any gaps in professional work history over six months. Work History MUST INCLUDE practice address.


13 The Application-Page 7 Section XVI. Attestation Questions A practitioner must personally attest to the application s correctness and completeness. In addition, these questions relate to his or her health status and any history of loss or limitations of license or privileges. If your answer to questions B through N is yes or if your answer to A, O or P is no, please provide full details on a separate sheet.

14 The Application-Page 8 Information Release and Acknowledgement Consent to the inspection of records and documents pertinent to his or her licensure, specific training, and current competence.

15 Addendum A-Page 1 Section I. Identifying Information Section II. Billing Information Section III. Practice Information

16 Addendum A-Page 2 Section III. Continued Section IV. Office Hours Section V. Coverage of Practice

17 Addendum A-Page 3 Section VI. Foreign Languages Spoken Section VII. Laboratory Services Section VIII. Professional Organizations
 years, whether the lawsuit or arbitration is pending, settled or otherwise concluded, and whether or not any payment was made on")
18 Addendum B-Page 1 Professional Liability Action Explanation Please complete this form for each pending, settled or otherwise concluded professional liability lawsuit or arbitration filed and served against you, in which you were named a party in the past seven (7) years, whether the lawsuit or arbitration is pending, settled or otherwise concluded, and whether or not any payment was made on your behalf by any insurer, company, hospital or other entity. All questions must be answered completely in order to avoid delay in expediting your application. If there is more than one professional liability lawsuit or arbitration action, please photocopy this form prior to completing, and complete a separate form for each lawsuit.
19 Addendum B-Page 2 Professional Liability Action Explanation Summarizethe circumstances giving rise to the action. If the action involves patient care, provide a narrative, with adequate clinical detail, including your description of your care and treatment of the patient. If more space is needed, attach additional sheet(s). Include 1) condition and diagnosis at time of incident, 2) dates and description of treatment rendered, and 3) condition of patient subsequent to treatment. Please print.

20 Provider Rights Addendum 1. Right of Review 2. Notification of Discrepancy 3. Correction of Erroneous Information 4. Status of Application
21 Primary Care Experience Addendum Please indicate below the age of the patients for whom you have provided primary care services to in the last 5 years. In order for a category to apply, it must represent at least 20% of your average practice and you must be familiar with and routinely follow standard preventive services, such as CHDP and the American Academy of Pediatrics (AAP), both for pediatrics only, and the United States Preventive Task Force (USPTF).
22 Physician Extender Attestation I attest to compliance with all laws, regulations, standards and contract provisions governing supervision of my activities as a physician extender by the state licensed physician referenced above; that this state licensed physician provides legally required collaboration, consultation and supervision consistent with my license; and that there is a written agreement that delineates medical services which I may appropriately provide within my scope of practice, as determined by the respective licensing board; and written supervisory guidelines are in place that are appropriately utilized for supervision Signature required from both the extender and the supervisor
23 HIV Specialty Designation Attestation Identifies appropriately qualified specialists who meet the Department of Managed Health Care (DMHC) definition of an HIV/AIDS specialist under Regulation LS-34-01
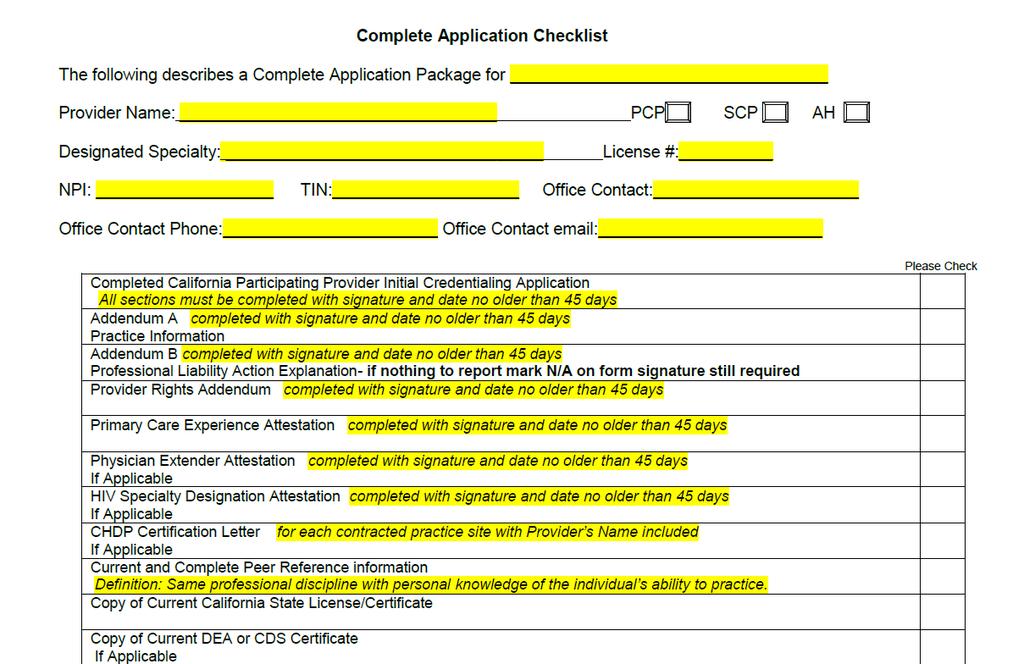
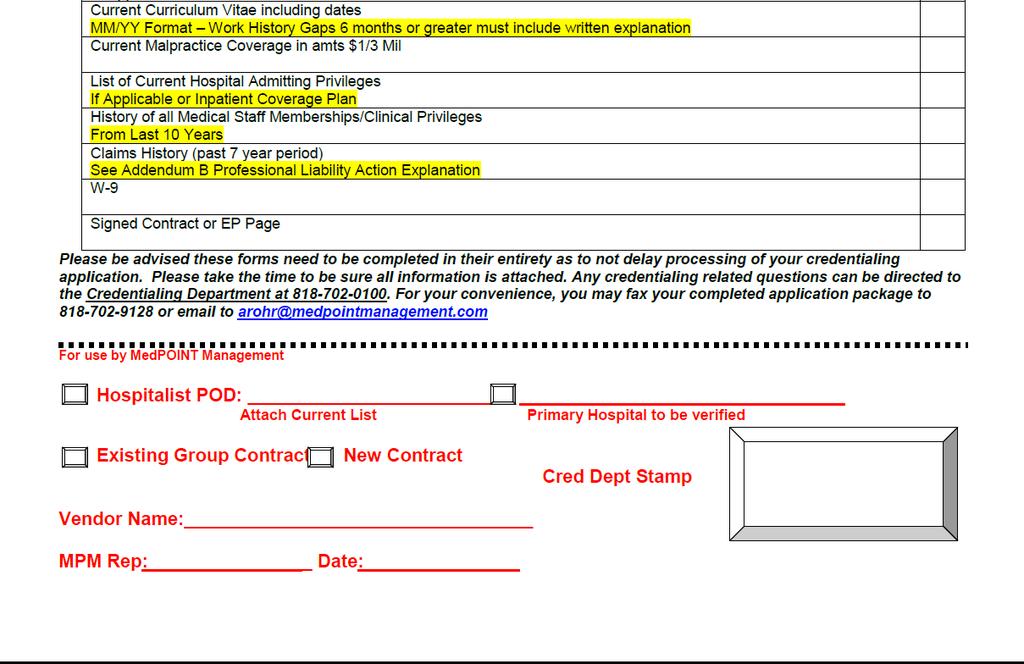
24 Tips for Completing Application Type or legibly complete the application in black or blue ink Sign and date all signature pages, No Stamped Signatures! If a section of the application does not apply, write N/A in the first box of the section If changes must be made to the completed application, use a black or blue pen to strike-out information and write in modified information. All changes must be initialed and dated. DO NOT WHITE-OUT Submit any requested addenda and do not relay on attached information unless requested (i.e. writing See CV in sections) Attach copies of supporting documents Use the checklist to determine the completeness of the application package Always provide contact information, including address in case follow up is necessary Best Practice:scan application and other documents to a PDF and complete package to arohr@medpointmanagement.com
25 Supporting Documents o Copy of Current State License or Certificate o Copy of Current DEA Certificate (if applicable) o Current Curriculum Vitae including dates o Current Malpractice Coverage o CHDP Certification Letter (if applicable) osigned Contract or EP Page ow-9
26
27 These indicators will not necessarily result in denial, only that an explanation is required. A practitioner should be afforded the opportunity to submit additional information in support of the application. The Credentialing Committee will consider all factors when reviewing practitioner credentials. Red Flags Missing dates or gaps in training or professional practice Discrepancies between information provided on application and verified information Suspension, reprimand, revocation, or challenge to licensure Excessive professional liability history, either in the number of claims filed or judgments awarded Reference verification letters that refer only to the fact that the dates are correct
28 Remember the burden is on the applicant to provide complete information. Insufficient or conflicting information may cause delay in the credentialing process. Often, these issues can be resolved by contacting the applicant and requesting additional information.
29 Full Credentialing Process MPM logs receipt of application MPM reviews for completeness MPM requests necessary additional information or clarification MPM complete data entry Forward to Gemini Diversified CVO Written verification is received from primary sources and results are forwarded to MedPOINT Management Credentialing Specialist sends written verification requests to Education and Training Facilities; Hospitals and other Institutions; Past Employers; and Liability Carriers Verifies License, DEA, Board Certification Query NPDB for Malpractice Claims Confirm Good Standing with State and Federal Programs Cred. Dept. conducts final review of file; compare and contrast to standards Obtain missing required documentation or data elements Prepare and forward for review and recommendation by Credentialing Committee Credentialing Committee Approval is sent to Provider Services MedPOINT Management sends Approval Letter Provider Services updates data base and sends notification to contracted Health Plans
30 On-Going Monitoring MedPOINT Management will regularly, obtain and review documentation on practitioner sanctions, complaints, adverse events and quality issues and implement appropriate interventions when poor quality, safety issues or limitations on licensure or exclusion from participation are identified. Among the types of media used, these sources have been identified as pertinent information used in the ongoing assessment of Practitioners. Reports publicized by licensing boards OIG Exclusions and Reinstatement Report/Database Medi-Cal Suspended and Ineligible Provider List maintained on the Medi-Cal web site Medicare Opt Out Report SAM (System for Award Management) formerly known as Excluded Parties List System (EPLS) Member complaints, filed with the Health Plan or MedPOINT Management Quality of Care issues, identified by the Health Plan or MedPOINT Management Adverse Events, identified by Health Plan or MedPOINT Management
31 Updating Expireables Time sensitive documents such as primary state license, DEA certificate, malpractice insurance coverage and board certification will be kept current at all times. California state license must be updated no more than five days of expiration DEA will be verified with the next available update from the primary source Insurance coverage will be verified with the next available update from the carrier Board certification will be verified with the next available update from the primary source.
32 Recredentialing Process One hundred and eighty (180) days prior to the end of the three-year appointment period, you will receive the Practitioner s pre-populated recredentialing application. The practitioner is required to review the information; make any necessary updates or corrections; then sign and date where it is indicated. THAT S IT! Return the completed recredentialing application and any supporting documents as requested. The reapplication will be processed, information verified, reviewed by Credentialing Committee and updated in our data base.
33 Questions? Linda Deaktor V.P. Quality Management MedPOINT Management Ph , Option 4 Fx credentialing_hsi@medpointmanagement.com
Please Note: Please send all documentation related to the credentialing portion of this documentation to:
 Please ote: The application process is split into different actions. Please send all documentation related to the contracting portion of this documentation to: Fax to: (916)350-8860 Or email to: BSCproviderinfo@blueshieldca.com
Please ote: The application process is split into different actions. Please send all documentation related to the contracting portion of this documentation to: Fax to: (916)350-8860 Or email to: BSCproviderinfo@blueshieldca.com
EFFECTIVE DATE: 10/04. SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31
 SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31 EFFECTIVE DATE: 10/04 Applies to all products administered by the plan except when changed by contract Policy Statement:
SUBJECT: Primary Care Nurse Practitioners SECTION: CREDENTIALING POLICY NUMBER: CR-31 EFFECTIVE DATE: 10/04 Applies to all products administered by the plan except when changed by contract Policy Statement:
Values Accountability Integrity Service Excellence Innovation Collaboration
 n00256 Recredentialing Process Values Accountability Integrity Service Excellence Innovation Collaboration Abstract Purpose: The purpose of recredentialing is to assure that Network Health Plan/Network
n00256 Recredentialing Process Values Accountability Integrity Service Excellence Innovation Collaboration Abstract Purpose: The purpose of recredentialing is to assure that Network Health Plan/Network
Delegation Oversight 2016 Audit Tool Credentialing and Recredentialing
 Att CRE - 216 Delegation Oversight 216 Audit Tool Review Date: A B C D E F 1 2 C3 R3 4 5 N/A N/A 6 7 8 9 N/A N/A AUDIT RESULTS CREDENTIALING ASSESSMENT ELEMENT COMPLIANCE SCORE CARD Medi-Cal Elements Medi-Cal
Att CRE - 216 Delegation Oversight 216 Audit Tool Review Date: A B C D E F 1 2 C3 R3 4 5 N/A N/A 6 7 8 9 N/A N/A AUDIT RESULTS CREDENTIALING ASSESSMENT ELEMENT COMPLIANCE SCORE CARD Medi-Cal Elements Medi-Cal
OREGON PRACTITIONER CREDENTIALING APPLICATION (Not an Employment Application)
") OREGON PRACTITIONER CREDENTIALING APPLICATION (Not an Employment Application) Prior to completing this credentialing application, please read and observe the following: Healthcare Organizations may contract
OREGON PRACTITIONER CREDENTIALING APPLICATION (Not an Employment Application) Prior to completing this credentialing application, please read and observe the following: Healthcare Organizations may contract
Name of Sex: M F Applicant: Last First Middle. Date of Birth: Social Security Number: Phone: ( ) City State Zip. Phone: ( ) City State Zip
 City State Zip. Phone: ( ) City State Zip") SCHNEIDER REGIONAL MEDICAL CENTER 9048 SUGAR ESTATE ST. THOMAS, U.S.V.I 00802 APPLICATION FOR TEMPORARY PRIVILEGES (USED FOR URGENT PATIENT NEED AND LOCUM TENENS) COMPLETE THE APPLICATION IN FULL. PRINT
SCHNEIDER REGIONAL MEDICAL CENTER 9048 SUGAR ESTATE ST. THOMAS, U.S.V.I 00802 APPLICATION FOR TEMPORARY PRIVILEGES (USED FOR URGENT PATIENT NEED AND LOCUM TENENS) COMPLETE THE APPLICATION IN FULL. PRINT
Practitioners may be recredentialed at any time, but in no circumstance longer than a 36 month period.
 SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN RECREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-02 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed by contract
SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN RECREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-02 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed by contract
The Plan will not credential trainees who do not maintain a separate and distinct practice from their training practice.
 SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN INITIAL CREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-01 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed
SUBJECT: PRIMARY CARE AND SPECIALTY PHYSICIAN INITIAL CREDENTIALING SECTION: CREDENTIALING POLICY NUMBER: CR-01 EFFECTIVE DATE: 1/01 Applies to all products administered by the Plan except when changed
This letter is to let you know that you are due for re-credentialing as a participating provider for AmeriHealth Caritas Louisiana of Louisiana.
 ATTN: AmeriHealth Caritas Louisiana Providers RE: Provider Re-Credentialing CAQH ID: Dear Credentialing Contact: This letter is to let you know that you are due for re-credentialing as a participating
ATTN: AmeriHealth Caritas Louisiana Providers RE: Provider Re-Credentialing CAQH ID: Dear Credentialing Contact: This letter is to let you know that you are due for re-credentialing as a participating
Additional Information / Documents Required
 Initial Credentialing Application Checklist If you are a CAQH (Council for Affordable Quality Healthcare) provider please provide your CAQH number CAQH#: California Participating Physician Application
Initial Credentialing Application Checklist If you are a CAQH (Council for Affordable Quality Healthcare) provider please provide your CAQH number CAQH#: California Participating Physician Application
Subject: Re-Credentialing Verification (Page 1 of 5)
") Subject: Re-Credentialing Verification (Page 1 of 5) Objective: I. To ensure that initial credentialed Health Share/Tuality Health Alliance (THA) providers have the continuing legal authority and relevant
Subject: Re-Credentialing Verification (Page 1 of 5) Objective: I. To ensure that initial credentialed Health Share/Tuality Health Alliance (THA) providers have the continuing legal authority and relevant
CREDENTIALING PLAN SECTION ONE INDIVIDUAL PROVIDERS
 CREDENTIALING PLAN SECTION ONE INDIVIDUAL PROVIDERS I. STATEMENT OF POLICY II. SCOPE A. The purpose of Avera Credentialing Verification Service (CVS) is to provide credentialing and recredentialing primary
CREDENTIALING PLAN SECTION ONE INDIVIDUAL PROVIDERS I. STATEMENT OF POLICY II. SCOPE A. The purpose of Avera Credentialing Verification Service (CVS) is to provide credentialing and recredentialing primary
LIBERTY DENTAL PLAN. Provider Credentialing Application. (* Required Fields) *OFFICE PHONE #: ( ) EMERGENCY PHONE #: ( ) *FAX #: ( )
 *OFFICE PHONE #: ( ) EMERGENCY PHONE #: ( ) *FAX #: ( )") (Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
(Complete one application per Provider) (* Required Fields) Credentialing Information: Owner: Associate: *PROVIDER NAME: DDS DMD Other (specify) *DATE OF BIRTH: / / Gender: Male Female Owning Dentist Name:
Provider Credentialing
 I. Purpose The purpose of this Policy and Procedure is to establish the process including written guidelines and standards for the credentialing and re-credentialing of all clinicians defined in this policy.
I. Purpose The purpose of this Policy and Procedure is to establish the process including written guidelines and standards for the credentialing and re-credentialing of all clinicians defined in this policy.
VNSNY CHOICE PRACTITIONER CREDENTIALING APPLICATION
 Attached please find an application for participation with VNSNY CHOICE. Upon completion, please forward this application to: VNSNY CHOICE Attn: Provider Relations Network Development 1250 Broadway - 11th
Attached please find an application for participation with VNSNY CHOICE. Upon completion, please forward this application to: VNSNY CHOICE Attn: Provider Relations Network Development 1250 Broadway - 11th
CREDENTIALING Section 4
 Overview Credentialing is the process by which the appropriate peer-review bodies of Ohana Health Plan (the Plan) evaluate the credentials and qualifications of providers, i.e., physicians, allied health
Overview Credentialing is the process by which the appropriate peer-review bodies of Ohana Health Plan (the Plan) evaluate the credentials and qualifications of providers, i.e., physicians, allied health
SAMPLE - Medical Staff Credentialing and Initial Appointment Policy
 Subject: Medical Staff Credentialing and Initial Appointment Number: Effective Date: Supersedes SPP# Dated: Approved by: (signature) Distribution: Medical Staff, Credentialing Manual, Medical Staff Office
Subject: Medical Staff Credentialing and Initial Appointment Number: Effective Date: Supersedes SPP# Dated: Approved by: (signature) Distribution: Medical Staff, Credentialing Manual, Medical Staff Office
Credentialing Standards
 Credentialing Standards Presenters: Mei Ling Christopher Veronica Harris Royal Agenda Definitions vs. 2017 Regulatory Updates Understanding the Standards SB 137 Provider Directories Reminders Questions
Credentialing Standards Presenters: Mei Ling Christopher Veronica Harris Royal Agenda Definitions vs. 2017 Regulatory Updates Understanding the Standards SB 137 Provider Directories Reminders Questions
HONORHealth CREDENTIALING PROCEDURES MANUAL 2017
 HONORHealth CREDENTIALING PROCEDURES MANUAL 2017 Table of Contents Part 1 APPOINTMENT PROCEDURES 1.1 Application 1 1.2 Application Content 1 1.3 References 2 1.4 Effect of Application 2 1.5 Application
HONORHealth CREDENTIALING PROCEDURES MANUAL 2017 Table of Contents Part 1 APPOINTMENT PROCEDURES 1.1 Application 1 1.2 Application Content 1 1.3 References 2 1.4 Effect of Application 2 1.5 Application
Medicare Manual Update Section 2 Credentialing (pg 15-23) SECTION 2: CREDENTIALING. 2.1 : Credentialing Policies & Procedures
 SECTION 2: CREDENTIALING. 2.1 : Credentialing Policies & Procedures") SECTION 2: CREDENTIALING The credentialing program applies to all direct-contracted and those who are affiliated with Care1st through their relationship with a contracted PPG (delegated IPA/MG). Care1st
SECTION 2: CREDENTIALING The credentialing program applies to all direct-contracted and those who are affiliated with Care1st through their relationship with a contracted PPG (delegated IPA/MG). Care1st
Idaho Practitioner Credentials Verification Checklist
 Idaho Practitioner Credentials Verification Checklist The following documentation is required when submitting a practitioner credentialing application. Please complete the information below and return
Idaho Practitioner Credentials Verification Checklist The following documentation is required when submitting a practitioner credentialing application. Please complete the information below and return
UnitedHealthcare of Insurance Company of New York The Empire Plan. CREDENTIALING and RECREDENTIALING PLAN
 UnitedHealthcare of Insurance Company of New York The Empire Plan CREDENTIALING and RECREDENTIALING PLAN 2013-2014 2013 UnitedHealth Group The Empire Plan All Rights Reserved This Credentialing and Recredentialing
UnitedHealthcare of Insurance Company of New York The Empire Plan CREDENTIALING and RECREDENTIALING PLAN 2013-2014 2013 UnitedHealth Group The Empire Plan All Rights Reserved This Credentialing and Recredentialing
2015 Complete Overview of the NCQA Standards Session Code: TU13 Time: 2:30 p.m. 4:00 p.m. Total CE Credits: 1.5 Presenter: Frank Stelling, MEd, MPH
 2015 Complete Overview of the NCQA Standards Session Code: TU13 Time: 2:30 p.m. 4:00 p.m. Total CE Credits: 1.5 Presenter: Frank Stelling, MEd, MPH Introduction to NCQA Credentialing Standards NAMSS Educational
2015 Complete Overview of the NCQA Standards Session Code: TU13 Time: 2:30 p.m. 4:00 p.m. Total CE Credits: 1.5 Presenter: Frank Stelling, MEd, MPH Introduction to NCQA Credentialing Standards NAMSS Educational
Medi-cal Manual Update Section 9.14 Credentialing Program (pg )
") 9.14: Credentialing Program Purpose To ensure that all network practitioners/providers meet the minimum credentials requirements set forth by Care1st and the regulatory agencies including, but not limited
9.14: Credentialing Program Purpose To ensure that all network practitioners/providers meet the minimum credentials requirements set forth by Care1st and the regulatory agencies including, but not limited
SC Uniform Managed Care Provider Credentialing Application
 SC Uniform Managed Care Provider Credentialing Application I. PERSONAL INFORMATION Solo Practice Group Practice Name: Last First M.I. Suffix Degree Maiden and/or other name List W-9 name if different Place
SC Uniform Managed Care Provider Credentialing Application I. PERSONAL INFORMATION Solo Practice Group Practice Name: Last First M.I. Suffix Degree Maiden and/or other name List W-9 name if different Place
CREDENTIALING APPLICATION Please complete all sections. Incomplete applications may delay the credentialing process.
 CREDENTIALING APPLICATION Please complete all sections. Incomplete applications may delay the credentialing process. PERSONAL IDENTIFICATION DATA Last Name: First: MI: Degree: Date of Birth: Social Security
CREDENTIALING APPLICATION Please complete all sections. Incomplete applications may delay the credentialing process. PERSONAL IDENTIFICATION DATA Last Name: First: MI: Degree: Date of Birth: Social Security
Molina Healthcare of Wisconsin, Inc. Practitioner Application
 Molina Healthcare of Wisconsin, Inc. Practitioner Application 1. INSTRUCTIONS This form should be: Typed or legibly printed in black or blue ink. Keep a copy of the application on file for future requests.
Molina Healthcare of Wisconsin, Inc. Practitioner Application 1. INSTRUCTIONS This form should be: Typed or legibly printed in black or blue ink. Keep a copy of the application on file for future requests.
CREDENTIALING Section 5
 Overview Credentialing is the process used by the Plan to evaluate the qualifications and credentials of providers, physicians, allied health professionals, hospitals and ancillary facilities/health care
Overview Credentialing is the process used by the Plan to evaluate the qualifications and credentials of providers, physicians, allied health professionals, hospitals and ancillary facilities/health care
This document describes the internal Harbor Health Plan's criteria for credentialing and recredentialing.
 vc I. SCOPE: This document describes the internal 's criteria for credentialing and recredentialing. II. POLICY: 's criteria for credentialing and recredentialing will be compliant with legal and accreditation
vc I. SCOPE: This document describes the internal 's criteria for credentialing and recredentialing. II. POLICY: 's criteria for credentialing and recredentialing will be compliant with legal and accreditation
The University Hospital Medical Staff BYLAWS
 The University Hospital Medical Staff BYLAWS October 2008 Page 1 of 77 The University Hospital Medical Staff Bylaws PREAMBLE WHEREAS, University Hospital is a health care entity of the University of Medicine
The University Hospital Medical Staff BYLAWS October 2008 Page 1 of 77 The University Hospital Medical Staff Bylaws PREAMBLE WHEREAS, University Hospital is a health care entity of the University of Medicine
Legal Last Name First Middle Professional Title/Degree
 IOWA STATEWIDE UNIVERSAL PRACTITIONER RECREDENTIALING APPLICATION Type or print responses in ink. A CV or See CV may not be use in lieu of completing any answers on this application. Review or complete
IOWA STATEWIDE UNIVERSAL PRACTITIONER RECREDENTIALING APPLICATION Type or print responses in ink. A CV or See CV may not be use in lieu of completing any answers on this application. Review or complete
CREDENTIALING Section 8. Overview
 Overview Credentialing is the process by which the appropriate peer review bodies of the Plan evaluate an individual applicant s background, education, post-graduate training, experience, work history,
Overview Credentialing is the process by which the appropriate peer review bodies of the Plan evaluate an individual applicant s background, education, post-graduate training, experience, work history,
Idaho Practitioner Application
 Idaho Practitioner Application To use the Idaho Practitioner Application (IPA), follow these instructions: Keep an unsigned and undated copy of the application on file for future requests. When a request
Idaho Practitioner Application To use the Idaho Practitioner Application (IPA), follow these instructions: Keep an unsigned and undated copy of the application on file for future requests. When a request
Washington Practitioner Application
 Washington Practitioner Application To use the Washington Practitioner Application (WPA), follow these instructions: Keep an unsigned and undated copy of the application on file for future requests. When
Washington Practitioner Application To use the Washington Practitioner Application (WPA), follow these instructions: Keep an unsigned and undated copy of the application on file for future requests. When
Washington Practitioner Application
 Washington Practitioner Application To use the Washington Practitioner Application (WPA), follow these instructions: Keep an unsigned and undated copy of the application on file for future requests. When
Washington Practitioner Application To use the Washington Practitioner Application (WPA), follow these instructions: Keep an unsigned and undated copy of the application on file for future requests. When
BCBS NC Blue Medicare Credentialing Instructions
 BCBS C Blue Medicare Credentialing Instructions Licensed Certified Social Worker (LCSW) Certified Substance Abuse Counselor (CSAC) Licensed Clinical Addiction Specialist (LCAS) Licensed Marriage and Family
BCBS C Blue Medicare Credentialing Instructions Licensed Certified Social Worker (LCSW) Certified Substance Abuse Counselor (CSAC) Licensed Clinical Addiction Specialist (LCAS) Licensed Marriage and Family
UnitedHealthcare. Credentialing Plan
 UnitedHealthcare Credentialing Plan 2015-2016 Table of contents Section 1.0 Introduction... 1 Section 1.1 Purpose...1 Section 1.2 Credentialing Policy...1 Section 1.3 Authority of Credentialing Entity
UnitedHealthcare Credentialing Plan 2015-2016 Table of contents Section 1.0 Introduction... 1 Section 1.1 Purpose...1 Section 1.2 Credentialing Policy...1 Section 1.3 Authority of Credentialing Entity
2014 Complete Overview of the URAC Standards
 2014 Complete Overview of the URAC Standards Session Code: TU09 Time: 10:00 a.m. 11:30 a.m. Total CE Credits: 1.5 Presented by: Sandra Greenwalt, RN, BSN, MCHA, CCM, CCP, CPHQ URAC Provider Credentialing,
2014 Complete Overview of the URAC Standards Session Code: TU09 Time: 10:00 a.m. 11:30 a.m. Total CE Credits: 1.5 Presented by: Sandra Greenwalt, RN, BSN, MCHA, CCM, CCP, CPHQ URAC Provider Credentialing,
CREDENTIALING PROCEDURES MANUAL MEMORIAL HOSPITAL OF SOUTH BEND, INC. SOUTH BEND, INDIANA
 MEMORIAL HOSPITAL OF SOUTH BEND, INC. SOUTH BEND, INDIANA January 16, 1984 Revised: October 18, 1984 January 19, 1989 April 17, 1989 April 26, 1990 December 20, 1990 January 21, 1993 May 27, 1993 July
MEMORIAL HOSPITAL OF SOUTH BEND, INC. SOUTH BEND, INDIANA January 16, 1984 Revised: October 18, 1984 January 19, 1989 April 17, 1989 April 26, 1990 December 20, 1990 January 21, 1993 May 27, 1993 July
LIBERTY DENTAL PLAN. Dental Hygienist - Credentialing Application. City: State: DEGREE: City: State: DEGREE:
 *Required Fields LIBERTY DENTAL PLAN Dental Hygienist - Credentialing Application Please complete one application per Dental Hygienist Demographic Information: Male Female *HYGIENIST NAME: RDH Other *DATE
*Required Fields LIBERTY DENTAL PLAN Dental Hygienist - Credentialing Application Please complete one application per Dental Hygienist Demographic Information: Male Female *HYGIENIST NAME: RDH Other *DATE
Subject: Initial Credentialing Verification (Page 1 of 5)
") Subject: Initial Credentialing Verification (Page 1 of 5) Objective: I. To ensure that Health Share/Tuality Health Alliance (THA) practitioners/providers have the legal authority and relevant training
Subject: Initial Credentialing Verification (Page 1 of 5) Objective: I. To ensure that Health Share/Tuality Health Alliance (THA) practitioners/providers have the legal authority and relevant training
Effective Date: 1/13
 North Shore-LIJ Health System is now Northwell Health POLICY TITLE: Disaster Privileging ADMINISTRATIVE POLICY AND PROCEDURE MANUAL POLICY #: 100.002 System Approval Date: 6/18/15 Site Implementation Date:
North Shore-LIJ Health System is now Northwell Health POLICY TITLE: Disaster Privileging ADMINISTRATIVE POLICY AND PROCEDURE MANUAL POLICY #: 100.002 System Approval Date: 6/18/15 Site Implementation Date:
PRACTICE INFORMATION AND LETTER AGREEMENT FORM. COMPLETE, SIGN AND RETURN TO: One Huntington Quadrangle Suite 1N09 Melville, NY 11747
 PRACTICE INFORMATION AND LETTER AGREEMENT FORM COMPLETE, SIGN AND RETURN TO: One Huntington Quadrangle Suite 1N09 Melville, NY 11747 PERSONAL DATA Last Name First Name License Number Tax I.D. Number for
PRACTICE INFORMATION AND LETTER AGREEMENT FORM COMPLETE, SIGN AND RETURN TO: One Huntington Quadrangle Suite 1N09 Melville, NY 11747 PERSONAL DATA Last Name First Name License Number Tax I.D. Number for
Network Participant Credentialing Application
 Please: Type or print legibly Complete all items. If an item does not apply, enter NA. Do not leave any items blank. Include the following with your application, if applicable: Copy of professional license(s)
Please: Type or print legibly Complete all items. If an item does not apply, enter NA. Do not leave any items blank. Include the following with your application, if applicable: Copy of professional license(s)
MEDICAL STAFF CREDENTIALING APPLICATION FORM For MD; DO; DDS; DMD; DC; DPM; PharmD; PhD; PsyD; OD.
 MEDICAL STAFF CREDENTIALING APPLICATION FORM For MD; DO; DDS; DMD; DC; DPM; PharmD; PhD; PsyD; OD. APPLICANT NAME: SPECIALTY: In order to expedite the credentialing process, please complete every item
MEDICAL STAFF CREDENTIALING APPLICATION FORM For MD; DO; DDS; DMD; DC; DPM; PharmD; PhD; PsyD; OD. APPLICANT NAME: SPECIALTY: In order to expedite the credentialing process, please complete every item
MEDICAL STAFF CREDENTIALS MANUAL
 MEDICAL STAFF CREDENTIALS MANUAL Adopted by the Medical Staff: July 27, 2009 Adopted by the Board of Directors: July 31, 2009 AHMC ANAHEIM REGIONAL MEDICAL CENTER (ARMC) CREDENTIALS MANUAL TABLE OF CONTENTS
MEDICAL STAFF CREDENTIALS MANUAL Adopted by the Medical Staff: July 27, 2009 Adopted by the Board of Directors: July 31, 2009 AHMC ANAHEIM REGIONAL MEDICAL CENTER (ARMC) CREDENTIALS MANUAL TABLE OF CONTENTS
THE UNIVERSITY OF MISSISSIPPI MEDICAL CENTER
 INSTRUCTIONS FOR NEW APPLICATIONS AND REAPPOINTMENT APPLICATIONS FOR CLINICAL PRIVILEGES AT THE UNIVERSITY OF MISSISSIPPI MEDICAL CENTER Applicant: Department: Please return this form with your application
INSTRUCTIONS FOR NEW APPLICATIONS AND REAPPOINTMENT APPLICATIONS FOR CLINICAL PRIVILEGES AT THE UNIVERSITY OF MISSISSIPPI MEDICAL CENTER Applicant: Department: Please return this form with your application
10111 Richmond Avenue, Suite 400, Houston, Texas (713) / (866) (Toll Free) / (713) (Fax)
 / (866) (Toll Free) / (713) (Fax)") Application Date: \ \ Date Available: \ \ Provider s Name: O MD O DO O PA O NP SS # : City: State: Zip: Home Phone ( ) Work Phone ( ) Pager ( ) Cell Phone ( ) E-Mail address: Driver s Lic. # Expires: \
Application Date: \ \ Date Available: \ \ Provider s Name: O MD O DO O PA O NP SS # : City: State: Zip: Home Phone ( ) Work Phone ( ) Pager ( ) Cell Phone ( ) E-Mail address: Driver s Lic. # Expires: \
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION
 INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must be completed in its entirety 3. Must be signed and dated 4.
INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must be completed in its entirety 3. Must be signed and dated 4.
Department: Legal Department. Approved by:
 HAWAII HEALTH SYSTEMS C O R P O R A T I O N Touching Lives Everyday" Policies and Procedures Subject: Credentialing Requirements Department: Legal Department Issued by: Rene McWade, Esq. VP & General Counsel
HAWAII HEALTH SYSTEMS C O R P O R A T I O N Touching Lives Everyday" Policies and Procedures Subject: Credentialing Requirements Department: Legal Department Issued by: Rene McWade, Esq. VP & General Counsel
COMMUNITY HOWARD REGIONAL HEALTH KOKOMO, INDIANA. Medical Staff Policy POLICY #4. APPOINTMENT, REAPPOINTMENT AND CREDENTIALING POLICY
 COMMUNITY HOWARD REGIONAL HEALTH KOKOMO, INDIANA Medical Staff Policy POLICY #4. APPOINTMENT, REAPPOINTMENT AND CREDENTIALING POLICY 1.1 PURPOSE The purpose of this Policy is to set forth the criteria
COMMUNITY HOWARD REGIONAL HEALTH KOKOMO, INDIANA Medical Staff Policy POLICY #4. APPOINTMENT, REAPPOINTMENT AND CREDENTIALING POLICY 1.1 PURPOSE The purpose of this Policy is to set forth the criteria
Keywords: Credentialing, Practitioner, PSV. Last Review Date: 10/11/2004, 1/31/2005, 3/28/2005, 3/13/2006, 4/24/2006
 3/28/2005, Page 1 of 7 I. Purpose: A. To describe and outline the initial credentialing process for all independent practitioners and to ensure that new independent practitioners meet ValueOptions of California
3/28/2005, Page 1 of 7 I. Purpose: A. To describe and outline the initial credentialing process for all independent practitioners and to ensure that new independent practitioners meet ValueOptions of California
UH Medical Staff Bylaws April Medical Staff BYLAWS. Last Updated: April Page 1 of 72
 Medical Staff BYLAWS Last Updated: Page 1 of 72 The University Hospital Medical Staff Bylaws PREAMBLE WHEREAS, University Hospital is a health care entity of the University of Medicine and Dentistry of
Medical Staff BYLAWS Last Updated: Page 1 of 72 The University Hospital Medical Staff Bylaws PREAMBLE WHEREAS, University Hospital is a health care entity of the University of Medicine and Dentistry of
MENTAL HEALTH MENTAL RETARDATION OF TARRANT COUNTY. Operating Procedure MC-033 Effective: January 1999 Managed Care Revised: April 2008 Page 1
 MENTAL HEALTH MENTAL RETARDATION OF TARRANT COUNTY Operating Procedure MC-033 Effective: January 1999 Managed Care Revised: April 2008 Page 1 CREDENTIALING/RECREDENTIALING OF PROFESSIONALS I. PURPOSE:
MENTAL HEALTH MENTAL RETARDATION OF TARRANT COUNTY Operating Procedure MC-033 Effective: January 1999 Managed Care Revised: April 2008 Page 1 CREDENTIALING/RECREDENTIALING OF PROFESSIONALS I. PURPOSE:
Credentialing Standards Presenters: Mei Ling Christopher Veronica Harris Royal
 Credentialing Standards Presenters: Mei Ling Christopher Veronica Harris Royal Agenda Introductions Definitions vs. 2016 Regulatory Updates Survey Process Reminders Questions and Answers 222 Introduction
Credentialing Standards Presenters: Mei Ling Christopher Veronica Harris Royal Agenda Introductions Definitions vs. 2016 Regulatory Updates Survey Process Reminders Questions and Answers 222 Introduction
Stanford Health Care Lucile Packard Children s Hospital Stanford
 Practitioners Page 1 of 11 I. PURPOSE To outline individuals who are authorized to provide care as an Allied Health Provider as well as describe which categories of individuals who will be processed under
Practitioners Page 1 of 11 I. PURPOSE To outline individuals who are authorized to provide care as an Allied Health Provider as well as describe which categories of individuals who will be processed under
YORK HOSPITAL CREDENTIALS POLICY AND PROCEDURE MANUAL
 YORK HOSPITAL CREDENTIALS POLICY AND PROCEDURE MANUAL Updated January 25, 2012 TABLE OF CONTENTS YORK HOSPITAL CREDENTIALS POLICY AND PROCEDURE MANUAL PROCEDURE MANUAL DEFINITIONS ARTICLE I. APPOINTMENT
YORK HOSPITAL CREDENTIALS POLICY AND PROCEDURE MANUAL Updated January 25, 2012 TABLE OF CONTENTS YORK HOSPITAL CREDENTIALS POLICY AND PROCEDURE MANUAL PROCEDURE MANUAL DEFINITIONS ARTICLE I. APPOINTMENT
Bylaws. of the. Medical Staff. Crouse Health Hospital, Inc. including amendments approved through June 28, 2016
 Bylaws of the Medical Staff of Crouse Health Hospital, Inc. including amendments approved through June 28, 2016 Crouse Health Hospital, Inc. 736 Irving Avenue, Syracuse, New York 13210 {H1058039.33} MEDICAL
Bylaws of the Medical Staff of Crouse Health Hospital, Inc. including amendments approved through June 28, 2016 Crouse Health Hospital, Inc. 736 Irving Avenue, Syracuse, New York 13210 {H1058039.33} MEDICAL
CR-01 Credentialing Program
 PNO-CR-01 Credentialing Program Provider Network Operations CR-01 Credentialing Program Effective Date: January 1, 2015 Revision Date: January 25, 2016 Review and Approved by Credentialing Committee: February
PNO-CR-01 Credentialing Program Provider Network Operations CR-01 Credentialing Program Effective Date: January 1, 2015 Revision Date: January 25, 2016 Review and Approved by Credentialing Committee: February
UPMC PINNACLE PROVIDER ENROLLMENT CREDENTIALING POLICIES AND PROCEDURES
 SUBJECT: Provider Enrollment Delegated Credentialing & Recredentialing PURPOSE Credentialing/recredentialing is the process by which UPMC Pinnacle ensures the quality of all providers of health care services
SUBJECT: Provider Enrollment Delegated Credentialing & Recredentialing PURPOSE Credentialing/recredentialing is the process by which UPMC Pinnacle ensures the quality of all providers of health care services
To Apply for BlueCross BlueShield of South Carolina and BlueChoice HealthPlan
 To Apply for BlueCross BlueShield of South Carolina and BlueChoice HealthPlan 1. Complete the SC Uniform Managed Care Provider Credentialing Application. 2. Enclose copies of the following items: A. State
To Apply for BlueCross BlueShield of South Carolina and BlueChoice HealthPlan 1. Complete the SC Uniform Managed Care Provider Credentialing Application. 2. Enclose copies of the following items: A. State
This policy applies to: Stanford Health Care Stanford Children s Health. Date Written or Last Revision: Oct 2017
 Providers Page 1 of 15 I. PURPOSE To establish mechanisms for gathering relevant data that will serve as the basis for decisions regarding credentialing and privileging of licensed independent practitioners
Providers Page 1 of 15 I. PURPOSE To establish mechanisms for gathering relevant data that will serve as the basis for decisions regarding credentialing and privileging of licensed independent practitioners
CLINICAL STAFF CREDENTIALING AND PRIVILEGING MANUAL
 CLINICAL STAFF CREDENTIALING AND PRIVILEGING MANUAL January 20, 2012 TABLE OF CONTENTS Introduction...1 I. Clinical Staff Membership...1 II. Clinical Staff Privileges...2 III. Procedures for Initial Appointment
CLINICAL STAFF CREDENTIALING AND PRIVILEGING MANUAL January 20, 2012 TABLE OF CONTENTS Introduction...1 I. Clinical Staff Membership...1 II. Clinical Staff Privileges...2 III. Procedures for Initial Appointment
Organizational Provider Credentialing Application
 Prior to completing this credentialing application, please read and observe the following: INSTRUCTIONS This form should be typed (using a different font than the form) or legibly printed in black or blue
Prior to completing this credentialing application, please read and observe the following: INSTRUCTIONS This form should be typed (using a different font than the form) or legibly printed in black or blue
UCSF Medical Staff Advanced Health Practitioners (AHPs) Credentialing Policy & Procedure
 Credentialing Policy & Procedure") Medical Staff Services UCSF Medical Staff Advanced Health Practitioners (AHPs) Credentialing Policy & Procedure Office of Origin: Medical Staff Office (415) 885 7268 I. PURPOSE: UCSF Medical Staff (UCSF)
Medical Staff Services UCSF Medical Staff Advanced Health Practitioners (AHPs) Credentialing Policy & Procedure Office of Origin: Medical Staff Office (415) 885 7268 I. PURPOSE: UCSF Medical Staff (UCSF)
I. PERSONAL INFORMATION. Degree and/or Title SS# . Non-physician Practitioner (Please specify )
") Pennsylvania Standard Application This form should be typed or legibly printed in black or blue ink. Please answer all questions completely and fully. If more space is needed than provided on this application,
Pennsylvania Standard Application This form should be typed or legibly printed in black or blue ink. Please answer all questions completely and fully. If more space is needed than provided on this application,
C. HUMAN RESOURCES LIASON MCCMH administrative employee who communicates with the Macomb County Human Resource and Labor Relations Department.
 IV. DEFINITIONS A. CLINICAL STRATEGIES AND CLINICAL IMPROVEMENT DIVISION The Clinical Strategies and Clinical Improvement ( CSI ) Division is the MCCMH administrative division responsible for the credentialing
IV. DEFINITIONS A. CLINICAL STRATEGIES AND CLINICAL IMPROVEMENT DIVISION The Clinical Strategies and Clinical Improvement ( CSI ) Division is the MCCMH administrative division responsible for the credentialing
STONY BROOK UNIVERSITY HOSPITAL CREDENTIALING POLICY - REVISIONS 2014
 STONY BROOK UNIVERSITY HOSPITAL CREDENTIALING POLICY - REVISIONS 2014 Stony Brook University Hospital (SBUH) has established policy guidelines for credentialing and recredentialing providers of patient
STONY BROOK UNIVERSITY HOSPITAL CREDENTIALING POLICY - REVISIONS 2014 Stony Brook University Hospital (SBUH) has established policy guidelines for credentialing and recredentialing providers of patient
Texas Credentialing Application Checklist
 APPLICANT NAME: Texas Credentialing Application Checklist TYPE OF DENTIST: In order to facilitate a prompt credentialing process, please complete every item on this application. Please, DO NOT write, See
APPLICANT NAME: Texas Credentialing Application Checklist TYPE OF DENTIST: In order to facilitate a prompt credentialing process, please complete every item on this application. Please, DO NOT write, See
BYLAWS OF THE MEDICAL STAFF UNIVERSITY OF NORTH CAROLINA HOSPITALS
 7 1 BYLAWS OF THE MEDICAL STAFF UNIVERSITY OF NORTH CAROLINA HOSPITALS Approved by the Executive Committee of the Medical Staff, November 5, 2001. Approved by the Medical Staff, December 5, 2001. Approved
7 1 BYLAWS OF THE MEDICAL STAFF UNIVERSITY OF NORTH CAROLINA HOSPITALS Approved by the Executive Committee of the Medical Staff, November 5, 2001. Approved by the Medical Staff, December 5, 2001. Approved
CRNA INITIAL CREDENTIALING APPLICATION
 CRNA INITIAL CREDENTIALING APPLICATION Revised 01/12 GENERAL INSTRUCTIONS LocumTenens.com CVO must credential all providers prior to placement into any practice location. All information requested in this
CRNA INITIAL CREDENTIALING APPLICATION Revised 01/12 GENERAL INSTRUCTIONS LocumTenens.com CVO must credential all providers prior to placement into any practice location. All information requested in this
CHAPTER 6: CREDENTIALING PROCEDURES
 We want to help you become or continue as a participating in-network provider for our members. Please refer to this chapter for information about: Provider credentialing Provider recredentialing Provider
We want to help you become or continue as a participating in-network provider for our members. Please refer to this chapter for information about: Provider credentialing Provider recredentialing Provider
Verify and Comply: CMS, JC, NCQA, HFAP, and DNV Credentialing Standards Compared and Contrasted
 Verify and Comply:, JC,,, and DNV Credentialing Standards Compared and Contrasted Session Code: MN10 Date: Monday, October 23 Time: 12:45 p.m. - 2:15 p.m. Total CE Credits: 1.5 Presenter(s): Sally Pelletier,
Verify and Comply:, JC,,, and DNV Credentialing Standards Compared and Contrasted Session Code: MN10 Date: Monday, October 23 Time: 12:45 p.m. - 2:15 p.m. Total CE Credits: 1.5 Presenter(s): Sally Pelletier,
Massachusetts Integrated Application for Re-Credentialing/Re-Appointment
 Massachusetts Integrated Application for Re-Credentialing/Re-Appointment Name (Please type or print) Degrees MA License. Are you currently in the United States on a temporary visa? ** **Identify type of
Massachusetts Integrated Application for Re-Credentialing/Re-Appointment Name (Please type or print) Degrees MA License. Are you currently in the United States on a temporary visa? ** **Identify type of
Credentialing Application
 Credentialing Application 1. NAME Last First MI Degree Gender 2. BIRTH, SOCIAL SECURITY & E-MAIL ADDRESS Date of Birth Social Security # E-Mail Address 3. PRACTICE, OFFICE & SPECIALTY INFORMATION 3.1 Please
Credentialing Application 1. NAME Last First MI Degree Gender 2. BIRTH, SOCIAL SECURITY & E-MAIL ADDRESS Date of Birth Social Security # E-Mail Address 3. PRACTICE, OFFICE & SPECIALTY INFORMATION 3.1 Please
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION
 HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must
TIFT REGIONAL MEDICAL CENTER MEDICAL STAFF POLICIES & PROCEDURES
 Title: Allied Health Professionals Approved: 2/02 Reviewed/Revised: 11/04; 08/10; 03/11; 5/14 Definition TIFT REGIONAL MEDICAL CENTER MEDICAL STAFF POLICIES & PROCEDURES P & P #: MS-0051 Page 1 of 7 For
Title: Allied Health Professionals Approved: 2/02 Reviewed/Revised: 11/04; 08/10; 03/11; 5/14 Definition TIFT REGIONAL MEDICAL CENTER MEDICAL STAFF POLICIES & PROCEDURES P & P #: MS-0051 Page 1 of 7 For
Ohio Department of Insurance
 Ohio Department of Insurance STANDARDIZED CREDENTIALING FORM Please complete each section thoroughly. Attach additional sheets where necessary. Type or print clearly in black ink. Sign and date the application.
Ohio Department of Insurance STANDARDIZED CREDENTIALING FORM Please complete each section thoroughly. Attach additional sheets where necessary. Type or print clearly in black ink. Sign and date the application.
PROVIDER CREDENTIALING APPLICATION
 PROVIDER CREDENTIALING APPLICATION We appreciate your interest in becoming a TRICARE network provider, offering medical services for Prime Beneficiaries. STEP 1. Contact your Provider Education and Relations
PROVIDER CREDENTIALING APPLICATION We appreciate your interest in becoming a TRICARE network provider, offering medical services for Prime Beneficiaries. STEP 1. Contact your Provider Education and Relations
***CAPS will not begin processing your application until ALL of the above items (numbers 1-4) are returned***
 are returned***") As a service to providers and the community, the Greater Louisville Medical Society (GLMS) offers a Centralized Application Processing Service (CAPS). The GLMS CAPS department verifies: education, training,
As a service to providers and the community, the Greater Louisville Medical Society (GLMS) offers a Centralized Application Processing Service (CAPS). The GLMS CAPS department verifies: education, training,
Credentialing Application for Hospitals and Facilities
 Instructions Credentialing Application for Hospitals and Facilities 1. Please accurately and legibly complete all sections of this Credentialing Application, and mark non-applicable fields with N/A. If
Instructions Credentialing Application for Hospitals and Facilities 1. Please accurately and legibly complete all sections of this Credentialing Application, and mark non-applicable fields with N/A. If
Provider Rights. As a network provider, you have the right to:
 NETWORK CREDENTIALING AND SANCTIONS ValueOptions program for credentialing and recredentialing providers is designed to comply with national accrediting organization standards as well as local, state and
NETWORK CREDENTIALING AND SANCTIONS ValueOptions program for credentialing and recredentialing providers is designed to comply with national accrediting organization standards as well as local, state and
Medical Staff Bylaws
 Medical Staff Bylaws Allen Hospital Waterloo, IA Revised/Reviewed: November 2015 Previous editions: March, 2015, December, 2013, November 2011, December 2009, November 2007, November 2006, May 2006, December
Medical Staff Bylaws Allen Hospital Waterloo, IA Revised/Reviewed: November 2015 Previous editions: March, 2015, December, 2013, November 2011, December 2009, November 2007, November 2006, May 2006, December
Oncology Nurse Practitioner Fellowship Application
 Oncology Nurse Practitioner Fellowship Application I. General Information Use this form to apply for full time appointment to the Nurse Practitioner Fellowship in Oncology at Sylvester Comprehensive Cancer
Oncology Nurse Practitioner Fellowship Application I. General Information Use this form to apply for full time appointment to the Nurse Practitioner Fellowship in Oncology at Sylvester Comprehensive Cancer
Eye Medical Provider Practice Application
 and subsidiaries Eye Medical Provider Practice Application How to Join the Avesis Network. Complete and sign the application Complete and sign the W-9 Complete and sign the Credential Verification Release
and subsidiaries Eye Medical Provider Practice Application How to Join the Avesis Network. Complete and sign the application Complete and sign the W-9 Complete and sign the Credential Verification Release
Facility and Ancillary Credentialing Application INSTRUCTIONS
 Facility and Ancillary Credentialing Application INSTRUCTIONS Please complete the application thoroughly in its entirety. The checklist below may not be exhaustive of all materials, but is provided as
Facility and Ancillary Credentialing Application INSTRUCTIONS Please complete the application thoroughly in its entirety. The checklist below may not be exhaustive of all materials, but is provided as
GENERAL INFORMATION. English Spanish Arabic Chinese French German Hmong Hindi Laotian Philippine Vietnamese Other
 **INCOMPLETE APPLICATIONS WILL DELAY THE CREDENTIALING PROCESS** 1. Please print or type ALL responses. 2. If you need additional space to complete a section, please attach additional sheets. 3. If you
**INCOMPLETE APPLICATIONS WILL DELAY THE CREDENTIALING PROCESS** 1. Please print or type ALL responses. 2. If you need additional space to complete a section, please attach additional sheets. 3. If you
Parkview Hospital Medical Staff Bylaws Supplement Allied Health Practitioner Manual
 Parkview Hospital Medical Staff Bylaws Supplement Allied Health Practitioner Manual PVH AHP Manual December 9, 2014 Table of Contents A. Comparison of Advanced and Dependent AHP 3 B. Authorizations of
Parkview Hospital Medical Staff Bylaws Supplement Allied Health Practitioner Manual PVH AHP Manual December 9, 2014 Table of Contents A. Comparison of Advanced and Dependent AHP 3 B. Authorizations of
Delegated Credentialing A Solution to the Insurer Credentialing Waiting Game?
 Chapter EE Delegated Credentialing A Solution to the Insurer Credentialing Waiting Game? Charles J. Chulack, Esq. Horty, Springer & Mattern, P.C. Pittsburgh EE-1 EE-2 Table of Contents Chapter EE Delegated
Chapter EE Delegated Credentialing A Solution to the Insurer Credentialing Waiting Game? Charles J. Chulack, Esq. Horty, Springer & Mattern, P.C. Pittsburgh EE-1 EE-2 Table of Contents Chapter EE Delegated
Clinical Credentialing & Recredentialing
 7 Clinical Credentialing & Recredentialing Clinical Credentialing and Recredentialing Preface Harvard Pilgrim Medicare Advantage cannot employ or contract with individuals excluded from participation in
7 Clinical Credentialing & Recredentialing Clinical Credentialing and Recredentialing Preface Harvard Pilgrim Medicare Advantage cannot employ or contract with individuals excluded from participation in
NCQA STANDARDS & SURVEY PROCESS UPDATES
 NCQA STANDARDS & SURVEY PROCESS UPDATES Presenter: Tammy L. White, CPCS CPMSM President, Gemini Diversified Services, Inc. Partner, Optimal Revenue Cycle Management, LLC Partner, MyAPPSTAT Provider Enrollment
NCQA STANDARDS & SURVEY PROCESS UPDATES Presenter: Tammy L. White, CPCS CPMSM President, Gemini Diversified Services, Inc. Partner, Optimal Revenue Cycle Management, LLC Partner, MyAPPSTAT Provider Enrollment
Provider Credentialing and Termination
 PROVIDER CREDENTIALING AND TERMINATION PROVIDER CREDENTIALING Subject to limited exceptions, Fidelis Care is required to credential each health care professional, prior to the professional providing services
PROVIDER CREDENTIALING AND TERMINATION PROVIDER CREDENTIALING Subject to limited exceptions, Fidelis Care is required to credential each health care professional, prior to the professional providing services
Standardized. Credentialing Form To Be Used By Health Maintenance Organizations Licensed in the State of Missouri
 I. GENERAL INFORMATION Standardized Credentialing Form To Be Used By Health Maintenance Organizations Licensed in the State of Missouri COMPLETE EACH SECTION AS THOROUGHLY AS POSSIBLE. PLEASE TYPE OR PRINT
I. GENERAL INFORMATION Standardized Credentialing Form To Be Used By Health Maintenance Organizations Licensed in the State of Missouri COMPLETE EACH SECTION AS THOROUGHLY AS POSSIBLE. PLEASE TYPE OR PRINT
SAMPLE - Verifying Credentialing Information Policy
 Subject: Number: Effective Date: Supersedes SPP# Approved by: (signature) Distribution: Verifying Credentialing Information Dated: Medical Staff, Credentialing Manual, Medical Staff Office I. STATEMENT
Subject: Number: Effective Date: Supersedes SPP# Approved by: (signature) Distribution: Verifying Credentialing Information Dated: Medical Staff, Credentialing Manual, Medical Staff Office I. STATEMENT
UNIVERSITY MALAYA MEDICAL CENTER (UMMC) CREDENTIALING AND RECREDENTIALING OF ALLIED HEALTH STAFF APPLICATION PROCEDURE
 CREDENTIALING AND RECREDENTIALING OF ALLIED HEALTH STAFF APPLICATION PROCEDURE") APPENDIX 2 UNIVERSITY MALAYA MEDICAL CENTER (UMMC) CREDENTIALING AND RECREDENTIALING OF ALLIED HEALTH STAFF APPLICATION PROCEDURE 1.0 OBJECTIVE To define the policies and procedures used in the appointment,
APPENDIX 2 UNIVERSITY MALAYA MEDICAL CENTER (UMMC) CREDENTIALING AND RECREDENTIALING OF ALLIED HEALTH STAFF APPLICATION PROCEDURE 1.0 OBJECTIVE To define the policies and procedures used in the appointment,
ALLIED HEALTH PROFESSIONAL CREDENTIALING APPLICATION FORM
 ALLIED HEALTH PROFESSIONAL CREDENTIALING APPLICATION FORM Independent Practitioners: Acupuncturist, Audiologist, Dietitian, Licensed Clinical Social Worker, Licensed Marriage and Family Therapist, Licensed
ALLIED HEALTH PROFESSIONAL CREDENTIALING APPLICATION FORM Independent Practitioners: Acupuncturist, Audiologist, Dietitian, Licensed Clinical Social Worker, Licensed Marriage and Family Therapist, Licensed
2016 CREDENTIALING PLAN
 2016 CREDENTIALING PLAN Reviewed by Cred Committee: April 2016 Adopted by Board Approval: May 2016 Reviewed by Cred Committee: November 2016 Amended by Board Approval: December 2016 Reviewed by Cred Committee:
2016 CREDENTIALING PLAN Reviewed by Cred Committee: April 2016 Adopted by Board Approval: May 2016 Reviewed by Cred Committee: November 2016 Amended by Board Approval: December 2016 Reviewed by Cred Committee:
Behavioral Health Facility and Ancillary Credentialing Application
 Behavioral Health Facility and Ancillary Credentialing Application Please complete the application thoroughly in its entirety. The checklist below may not be exhaustive of all materials, but is provided
Behavioral Health Facility and Ancillary Credentialing Application Please complete the application thoroughly in its entirety. The checklist below may not be exhaustive of all materials, but is provided
2018 CREDENTIALING COMMITTEE PROGRAM DESCRIPTION
 2018 CREDENTIALING COMMITTEE PROGRAM DESCRIPTION Purpose The purpose of the Credentialing Committee is to develop, monitor, and maintain standards of education, training, licensure, and experience of the
2018 CREDENTIALING COMMITTEE PROGRAM DESCRIPTION Purpose The purpose of the Credentialing Committee is to develop, monitor, and maintain standards of education, training, licensure, and experience of the
APPLICATION FOR REAPPOINTMENT RESEARCH ASSOCIATE
 APPLICATION FOR REAPPOINTMENT RESEARCH ASSOCIATE Enclosed is an application for reappointment to the position of Research Associate. We ask that you review the shaded areas to assure that all current information
APPLICATION FOR REAPPOINTMENT RESEARCH ASSOCIATE Enclosed is an application for reappointment to the position of Research Associate. We ask that you review the shaded areas to assure that all current information