Multi disciplinary Team Communication and Effective Handoffs
|
|
|
- Kerry Barnett
- 6 years ago
- Views:
Transcription

1 Multi disciplinary Team Communication and Effective Handoffs Lauren Destino, MD Clinical Associate Professor Associate Medical Director of the Pediatric Hospital Medicine Division Stanford University, Lucile Packard Children s Hospital
2 Disclosures Dr. Lauren Destino has Identified that she has no conflicts of interest to disclose Documented that this presentation will not involve discussion of unapproved, off label, experimental or investigational use materials or protocols Dr. Lauren Destino will Present copyrighted materials and has obtained permission from Children s Hospital Boston and the I PASS Study Group The I PASS Handoff Study Curriculum includes materials adapted from TeamSTEPPS TM, an evidence based teamwork curriculum developed by the Department of Defense and the Agency for Healthcare Research and Quality. All materials are used with permission.
3 Objectives Describe the role of communication failures in medical errors and preventable adverse events Articulate the need for high quality patient handoffs to reduce the likelihood of communication failures Describe the implementation of I PASS evidence based handoff bundle and its impact on medical errors and patient safety Navigate communication and/or cultural barriers which can impact handoffs
4 Question For The Audience How many of you have received handoff training during your career?
5 Agenda Background Patient safety & handoffs The I PASS Study Educational Intervention Methods & Findings Dissemination and ongoing work Improving transitions of care across hospital settings
6 Background Patient Safety & Handoffs

7 Patient Safety Movement IOM Report (1999) Estimated 98,000 preventable deaths per year due to medical errors More common reason for death than Breast Cancer AIDS Motor Vehicle Accidents
8 No Change in Adverse Event Frequency North Carolina Patient Safety Study Study of 2341 randomly selected admissions from 10 randomly selected hospitals statewide Landrigan et al. NEJM 2010; 363:



9 Advances in Patient Safety Progress reducing specific types of adverse events Catheter related bloodstream infections Pronovost et al Surgical Safety Checklists Gawande et al Duty hours restrictions Landrigan et al

10 Communication Failures Joint Commission. (2011). Sentinel Event Statistics Data Root Causes by Event Type (2004 Third Quarter 2011)

11 Communication Failures and the EMR EMR was associated with BMJ 1.Decrease Quality and Safety face July 2014 to face communication 2.Worsened overall agreement about the plan of care
12 Questions For The Audience Have you witnessed a handoff like this, either between colleagues or trainees, in the past 6 months? Why was this a poor handoff?


13 Handoffs Are A Complex Skill Concept Model For Handoffs Starmer et al. Acad Med Jun;89(6):


14 We need standardized handoffs!!!
15 The I PASS Study

16 I PASS Pilot Study Boston Children s Hospital in Involved the implementation of a resident handoff bundle Starmer et al. JAMA Dec 4;310(21):
17 Results Medical Errors & Preventable Adverse Events Rates per 100 admissions Pre Post p value Medical Errors <0.001 Preventable Adverse Events Starmer et al. JAMA Dec 4;310(21):
18 Limitations Of The Pilot Study Single institution: Unclear generalizability Limited ability to control for confounding factors Learning over time Seasonal variation Mnemonic (SIGNOUT?) not memorable or sustained after research period Challenges with sustainability Lack of faculty engagement
19 Pilot Study Multisite Study IIPE PRIS Accelerating Safe Sign outs Multisite study at 9 Children s Hospitals Implemented I PASS handoff bundle for resident physician change of shift handoffs Supported by Initiative for Innovation in Pediatric Education (IIPE) Pediatric Research in Inpatient Settings (PRIS) Funded by $3 million grant from U.S. Dept of Health and Human Services (ARRA funding) September 2010
20 Challenges To Improving Handoffs Handoffs are Non standardized processes currently Not formally taught Variable Institution to institution Within institutions Implementing a change in handoff practice is a transformational change Starmer AJ et al. Resident Sign out Practices: Results from a Multisite Needs Assessment Association of Pediatric Program Directors Annual Meeting.
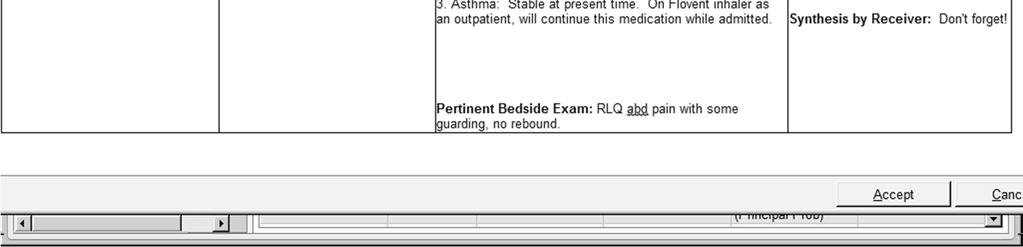
21 I The I PASS Mnemonic Illness Severity Stable, watcher, unstable P Patient Summary Summary statement Events leading up to admission Hospital course Ongoing assessment Plan A Action List To do list Timeline and ownership S Situation Awareness and Contingency Planning S Synthesis by Receiver Know what s going on Plan for what might happen Receiver summarizes what was heard Asks questions Restates key action/to do items Starmer. Pediatrics Feb;129(2):201 4.


22 I Illness Severity A Continuum Watcher: Any clinician s gut feeling that a patient is at risk of deterioration or close to the edge

23 P Patient Summary High quality patient summaries Include a summary statement/one liner Describe unique features of the patient s presentation Create a shared mental model Facilitate the transfer of information and responsibility Transmit information concisely
24 A Action List To Do: Check respiratory exam now; if still tachypneic get CXR Monitor withdrawl scores at 5pm; if still high increase ativan gtt to 3mg/hour Check ins and outs at midnight; if less than 500mL UOP give 1L Follow up 6PM electrolytes; if K still low please replace with KCl 40 Meq IVPB
25 S Situation Awareness & Contingency Planning Situation Awareness Patient level Know what s going on with your patient Status of patient s disease process Team members roles in patient s care Environmental factors Progress toward goals of hospitalization Team level Know what is going on around you Status of patients Team members Environment Progress toward team goals

26 S Situation Awareness & Contingency Planning Contingency Planning Problem solving before things go wrong If this happens, then....
27 S Synthesis By Receiver Provides an opportunity for receiver to Clarify elements of handoff Ensure there is a clear understanding Have an active role in handoff process It is not a re stating of entire verbal handoff!
28 Intervention: More Than Just A Mnemonic I PASS Handoff Bundle Components I PASS Mnemonic I PASS Campaign Introductory Workshop Faculty Observations & Feedback I PASS Handoff Bundle TeamSTEPPS Training Faculty Development Simulation Exercises I PASS Printed Handoff Document All Handoff Bundle Components Available at
29 I PASS Communication Training: TeamSTEPPS TM Brief Team Strategies and Tools to Enhance Performance and Patient Safety Debrief Technique Function Plan team activities Analyze an interim event Huddle Assertive statement Check back Solve a problem Identify potential errors Ensure accurate information transfer





30 Simulation An Integral Component Of The Curriculum


31 I PASS Printed Handoff Tools
32 I PASS Handoff Assessment Tools Development Process Expert panel identified key elements of effective handoffs Reviewed published literature for examples, items, and rating scales Created handoff assessment tool Multiple revisions Pilot tested and further revised Generated evidence to demonstrate and confirm tool validity






33 I PASS Campaign Materials Study logo Posters Screen frames Pocket cards Badge clips I PASS tips of the day Just in Time refresher training sessions
34 The I PASS Study Methods & Findings
35 I PASS Study Aims To determine if implementation of I PASS Handoff Bundle is associated with: Reduction in overall error rates and preventable adverse events (primary outcome) Improved written and verbal handoff communication (process outcomes) Change in resident workflow patterns (balancing measure)
36 Study Design General inpatient units at 9 North American pediatric residency training programs Site Name UCSF Stanford Washington University Cincinnati Utah St. Christopher s National Capital Consortium Sick Kids OHSU Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr Pre-intervention data collection I-PASS bundle implementation Post-intervention data collection
37 Methods Primary Outcome Measurement Of Error Rates Standardized error surveillance methodology Study nurse reviews patient charts Medication orders, MAR, progress notes, nursing notes, and discharge summary Hospital incident reports Daily solicited error reports from physicians Potential medical errors categorized Two MDs blinded to pre vs. post status Severity, preventability, type, non error
38 Methods Process Outcomes Verbal & Written Handoff Miscommunications Audio recordings of evening verbal handoffs Random selection of 12 per study period per site Review all patients for presence or absence of 5 key data elements Electronic copies of printed handoff documents Random selection of 24 handoff documents per study period per site Review all patients for presence or absence of 9 key data elements



39 Methods Balancing Measure Time Motion Study
40 Results Process Measures % Of Verbal Handoffs With Key Elements Present 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% All p values < * * * * * Illness Patient To do list Contingency Readback severity summary plans N = 207 verbal handoff sessions, 2281 unique patient handoffs assessment Pre-intervention Post-intervention Starmer AJ, et al. Changes in Medical Errors After Implementation of a Handoff Program. NEJM Nov 6; 371(19):
41 Results Process Measures % Of Written Handoffs With Key Data Elements All p values < % 90% 80% 70% * * * * * 60% 50% 40% * * * 30% 20% 10% * Pre-intervention Post-intervention 0% N = 432 written handoff documents, 5752 unique patient entries Starmer AJ, et al. Changes in Medical Errors After Implementation of a Handoff Program. NEJM Nov 6; 371(19):
42 Results Primary Outcome Medical Error Rates 30% reduction 23% reduction Number of errors (rate per 100 patient admissions) Pre (n=5516 admissions) Post (n=5571 admissions) P value Overall rate of medical errors <.0001 Preventable adverse events <.0001 Near misses / non harmful medical errors <.0001 Non preventable Adverse Events Starmer AJ, et al. Changes in Medical Errors After Implementation of a Handoff Program. NEJM Nov 6; 371(19):
43 Activity Results Balancing Measures Workflow % of Time per 24 hr Period Spent in Activity Pre Intervention N = 3510 hours Post Intervention N = 4618 hours P Value Patient Family Contact 11.8% 12.5% 0.41 Creating written or computerized handoff 1.6% 1.3% 0.54 document Other Computer Time 16.2 % 16.5% 0.81 Mean duration of verbal handoff per patient Pre Intervention Post Intervention P Value 2.4 min 2.5 min 0.55 Starmer AJ, et al. Changes in Medical Errors After Implementation of a Handoff Program. NEJM Nov 6; 371(19):
44 Quality Improvement Nested Within The Research Study QI methodology was embraced in order to enhance the implementation and sustainment of the handoff bundle 120 I-PASS Faculty Champion MOC Project: Percent of Residents Adhering to 5 Elements of I-PASS Mnemonic Jun (n=07) Jul (n=04) Aug (n=03) Sept (n=02) Oct (n=05) Nov (n=06) Dec (n=07) Jan (n=05) Feb (n=01) Mar (n=11) Apr (n=06) May (n=02) June (n=02) July (n=02) August (n=02) Monthly Average Monthly Averages Median Goal (90)


45 The Dissemination Of I PASS I PASS Study Website AAMC s MedEdPORTAL
46 US I PASS Downloads 0 downloads US Curricular Downloads Updated July 2, >40
47 Dissemination To Other Groups & Specialties
48 Ongoing Work AHRQ and SHM mentored implementation of I PASS across 32 institutions Adaptation for adult providers Online learning Integration into Family Centered Rounds Consultation Program MD Anderson MGH

49 AHRQ and SHM Mentored Implementation
50 AHRQ and SHM Mentored Implementation
51 AHRQ and SHM Mentored Implementation
52 AHRQ and SHM Mentored Implementation
53 Further Evidence of I PASS
54 I PASS Beyond the I PASS Study Group Variety of specialties Emergency Medicine Surgical Oncology Internal Medicine Pediatrics Hospital Wide Evidence of adaption with improvements in various handoff elements and adverse events Shahian DM. BMJ Qual Saf 2017 Fryman C. BMJ Qual Improv Rep 2017 Heilman JA. West J Emerg Med 2016 Clarke CN. Surgery2017 Huth K. Acad Pediatr 2016 Walia J. Acad Pediatr 2016
55 Transitions Throughout a Hospital: Lucile Packard Children s Hospital Stanford Focus on high risk transitions ICU to OR CVICU to Floor OR to Post op recovery areas OR to ICU Utilized I PASS format Increased information transferred Increased satisfaction among providers No change in length of handoffs Decreased hand off related care failures Sheth S et al. Pediatrics 2016 Bigham MT et al. Pediatrics 2014 Caruso TJ et al. Jt Comm J Qual Patient Saf 2015 Caruso TJ et al. Int J Health Care Qual Assur 2017
56 Key Considerations to Starting Handoff Improvement Work Multidisciplinary group Identify areas of high risk Identify areas that amenable to change Start small Long process but worth the effort for provider satisfaction and patient safety

57 In Closing

58 Summary & Take Home Points High frequency of communication and handoff errors Multi faceted approach needed to standardize and improve patient handoffs I PASS Handoff Bundle Decreased rates of medical errors and adverse events No impact on physician workflow


59 Acknowledgements The I PASS Study Group
60 Funding & Resources Primary funding Department of Health and Human Services Additional funding for I PASS provided by: Oregon Comparative Effectiveness Research K12 Program, Agency for Healthcare Research and Quality (AHRQ) Medical Research Foundation of Oregon Physician Services Incorporated Foundation (of Ontario) Pfizer (unrestricted medical education grant) Pediatric Research in Inpatient Settings (PRIS) Network Initiative for Innovation in Pediatrics Education (IIPE)
61 References Landrigan CP et al. N Engl J Med Nov 25;363(22): Starmer AJ et al. Acad Med Jun;89(6): Starmer AJ et al. JAMA Dec 4;310(21): Starmer AJ et al. Pediatrics Feb;129(2): Starmer AJ, et al. NEJM Nov 6; 371(19): pdf Shahian DM. BMJ Qual Saf 2017 Mar 9 Epub ahead of print Fryman C. BMJ Qual Improv Rep 2017 Apr 6;6(1) Heilman JA. West J Emerg Med 2016 Nov;17(6): Clarke CN. Surgery 2017 Mar;161(3): Huth K. Acad Pediatr 2016 Aug;16(6): Walia J. Acad Pediatr 2016 Aug;16(6): Sheth S et al. Pediatrics 2016 Feb;137(2):e Bigham MT et al. Pediatrics 2014 Aug;134(2): Caruso TJ et al. Jt Comm J Qual Patient Saf 2015 Jan;41(1):35 42 Caruso TJ et al. Int J Health Care Qual Assur 2017 May 8;30(4):
62 Thank You!! Questions or Comments?
I-Pass in the NICU: Operationalizing and Sustaining Improved Handoffs
 I-Pass in the NICU: Operationalizing and Sustaining Improved Handoffs Research Director Boston Children's Hospital Inpatient Pediatrics Service Director, Sleep and Patient Safety Program Brigham and Women's
I-Pass in the NICU: Operationalizing and Sustaining Improved Handoffs Research Director Boston Children's Hospital Inpatient Pediatrics Service Director, Sleep and Patient Safety Program Brigham and Women's
Optimizing Handoff Communication for Improved Patient Safety
 Optimizing Handoff Communication for Improved Patient Safety Christopher P. Landrigan, MD, MPH Professor of Pediatrics, Harvard Medical School Research Director, Inpatient Pediatrics Service, Boston Children
Optimizing Handoff Communication for Improved Patient Safety Christopher P. Landrigan, MD, MPH Professor of Pediatrics, Harvard Medical School Research Director, Inpatient Pediatrics Service, Boston Children
Better handoffs. Safer care. Just-in-time Module
 Better handoffs. Safer care. Just-in-time Module Root Causes of Sentinel Events Joint Commission. (2011). Sentinel Event Statistics Data - Root Causes by Event Type (2004 - Third Quarter 2011) 1 2 TeamSTEPPS
Better handoffs. Safer care. Just-in-time Module Root Causes of Sentinel Events Joint Commission. (2011). Sentinel Event Statistics Data - Root Causes by Event Type (2004 - Third Quarter 2011) 1 2 TeamSTEPPS
Improving Safety During Care Transitions the I-PASS Project at MGH
 Improving Safety During Care Transitions the I-PASS Project at MGH David M. Shahian, MD Vice-President, Lawrence Center for Quality & Safety Professor of Surgery, Harvard Medical School Laura Rossi RN,
Improving Safety During Care Transitions the I-PASS Project at MGH David M. Shahian, MD Vice-President, Lawrence Center for Quality & Safety Professor of Surgery, Harvard Medical School Laura Rossi RN,
Improving Transitions of Care: I-PASS Handoff Initiative
 Improving Transitions of Care: I-PASS Handoff Initiative Karin A. Sloan, MD Director of Clinical Quality, Dept of Medicine on behalf of the Core I-PASS Implementation Team for Internal Medicine: David
Improving Transitions of Care: I-PASS Handoff Initiative Karin A. Sloan, MD Director of Clinical Quality, Dept of Medicine on behalf of the Core I-PASS Implementation Team for Internal Medicine: David
A Quality Improvement Project on the Use of the I-PASS System in Written Physician Hand-Off Documents and Reduction in Unexpected Events
 A Quality Improvement Project on the Use of the I-PASS System in Written Physician Hand-Off Documents and Reduction in Unexpected Events Background Lauren Shull, MD-R In 2003, the Accreditation Council
A Quality Improvement Project on the Use of the I-PASS System in Written Physician Hand-Off Documents and Reduction in Unexpected Events Background Lauren Shull, MD-R In 2003, the Accreditation Council
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Quality, Safety and the Physician Handoff
 Quality, Safety and the Physician Handoff John M. McGregor, M.D. Department of Neurological Surgery Co-Chairman - Neuroscience Clinical Quality Management Committee Ohio State University Wexner Medical
Quality, Safety and the Physician Handoff John M. McGregor, M.D. Department of Neurological Surgery Co-Chairman - Neuroscience Clinical Quality Management Committee Ohio State University Wexner Medical
TCLHIN Standardized Discharge Summary
 TCLHIN Standardized Discharge Summary ehealth Conference June 4, 2014 Kara Kitts Quality Improvement Manager St. Michael s Hospital Ontario Healthcare System 14 Local Health Integration Networks (LHINs)
TCLHIN Standardized Discharge Summary ehealth Conference June 4, 2014 Kara Kitts Quality Improvement Manager St. Michael s Hospital Ontario Healthcare System 14 Local Health Integration Networks (LHINs)
Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship
 Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship Diane Levine, Wayne State University Allison Heacock, The Ohio State University Amy Shaheen, University of North Carolina
Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship Diane Levine, Wayne State University Allison Heacock, The Ohio State University Amy Shaheen, University of North Carolina
I-PASS tool enhances verbal handover on Pediatric General Surgery team
 I-PASS tool enhances verbal handover on Pediatric General Surgery team Lapidus-Krol E, Fallon E, Wolinska J, Kolivoshka Y, Fecteau A Division of General and Thoracic Surgery, Hospital For Sick Children,
I-PASS tool enhances verbal handover on Pediatric General Surgery team Lapidus-Krol E, Fallon E, Wolinska J, Kolivoshka Y, Fecteau A Division of General and Thoracic Surgery, Hospital For Sick Children,
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Laguna Honda Lean Transformation. Laguna Honda Strategic Performance Management November 2017
 Laguna Honda Lean Transformation Laguna Honda Strategic Performance Management November 2017 Background MAKE IT BETTER 4. 1. Performance Improvement FIX IT Do the work and make it happen 3. Create best
Laguna Honda Lean Transformation Laguna Honda Strategic Performance Management November 2017 Background MAKE IT BETTER 4. 1. Performance Improvement FIX IT Do the work and make it happen 3. Create best
Imprinting Safety and Quality Practices on Residents and Fellows. John Szymusiak, MD Gregory M. Bump, MD
 Imprinting Safety and Quality Practices on Residents and Fellows John Szymusiak, MD Gregory M. Bump, MD Introductions 2 Gregory M. Bump, MD Associate Professor of General Internal Medicine UPMC Montefiore
Imprinting Safety and Quality Practices on Residents and Fellows John Szymusiak, MD Gregory M. Bump, MD Introductions 2 Gregory M. Bump, MD Associate Professor of General Internal Medicine UPMC Montefiore
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Communication Surrounding Adverse Events: A Simulation Education Program for Resident Physicians
 Communication Surrounding Adverse Events: A Simulation Education Program for Resident Physicians, Washington, DC 1 Investigators Laura J. Sigman, MD, JD, FAAP Dr. Sigman is a physician and manages legal
Communication Surrounding Adverse Events: A Simulation Education Program for Resident Physicians, Washington, DC 1 Investigators Laura J. Sigman, MD, JD, FAAP Dr. Sigman is a physician and manages legal
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
A23/B23: Patient Harm in US Hospitals: How Much? Objectives
 A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
From Implementation to Optimization: Moving Beyond Operations
 From Implementation to Optimization: Moving Beyond Operations Session 260, March 8, 2018 Scott Aikey, Sr. Director, Core Clinical Applications Children s Hospital of Philadelphia 1 Conflict of Interest
From Implementation to Optimization: Moving Beyond Operations Session 260, March 8, 2018 Scott Aikey, Sr. Director, Core Clinical Applications Children s Hospital of Philadelphia 1 Conflict of Interest
10/23/2015. Don t drop the baton: Improving handover communication from the CMPA s perspective
 Don t drop the baton: Improving handover communication from the CMPA s perspective This is an abridged version of presentation with cases and videos removed Dr Janet Nuth, Physician Risk Manager CMPA Associate
Don t drop the baton: Improving handover communication from the CMPA s perspective This is an abridged version of presentation with cases and videos removed Dr Janet Nuth, Physician Risk Manager CMPA Associate
QUALITY IMPROVEMENT OF YOUR RESIDENCY PROGRAM: AN EXPERIENTIAL WORKSHOP
 QUALITY IMPROVEMENT OF YOUR RESIDENCY PROGRAM: AN EXPERIENTIAL WORKSHOP BROUGHT TO YOU BY: UW PEDIATRIC RESIDENCY PROGRAM DIRECTORS AND CHIEF RESIDENTS Richard, Heather, Maneesh, Susan, Emily, Celeste,
QUALITY IMPROVEMENT OF YOUR RESIDENCY PROGRAM: AN EXPERIENTIAL WORKSHOP BROUGHT TO YOU BY: UW PEDIATRIC RESIDENCY PROGRAM DIRECTORS AND CHIEF RESIDENTS Richard, Heather, Maneesh, Susan, Emily, Celeste,
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health
 Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Systems approach to Patient Safety and Experience
 Systems approach to Patient Safety and Experience Dr Alex Sia Chief Executive Officer KK Women s and Children s Hospital Professor, Duke NUS Medical School Clinical Professor, YLL School of Medicine Adjunct
Systems approach to Patient Safety and Experience Dr Alex Sia Chief Executive Officer KK Women s and Children s Hospital Professor, Duke NUS Medical School Clinical Professor, YLL School of Medicine Adjunct
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, March 2018
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, March By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing......1-2 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, March By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing......1-2 2. Emergency
L19: Improving Transitions from the Hospital to Post Acute Care Settings
 This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment. MEDCOM PS Center
 ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
ARMY DENCOM Strategic Plan for TeamSTEPPS Spread and Sustainment MEDCOM PS Center Implementing a Teamwork Initiative Department of Defense Patient Safety Program Healthcare Team Coordination Objectives
Improving Pain Center Processes utilizing a Lean Team Approach
 Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm. Kendra Folh, BSN, RNC-OB
 How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm Kendra Folh, BSN, RNC-OB Medical error has been defined as: An unintended act
How to be an ACE in Your Place: The Top Three Elements of Nursing Practice to Protect Patient Safety and Avoid Patient Harm Kendra Folh, BSN, RNC-OB Medical error has been defined as: An unintended act
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
IMPROVING RESIDENT HANDOFFS. Educating for Quality Improvement & Patient Safety
 IMPROVING RESIDENT HANDOFFS Educating for Quality Improvement & Patient Safety 1 Stephanie Reeves, DO has no relevant financial relationships with commercial interests to disclose. 2 CS&E Participant Stephanie
IMPROVING RESIDENT HANDOFFS Educating for Quality Improvement & Patient Safety 1 Stephanie Reeves, DO has no relevant financial relationships with commercial interests to disclose. 2 CS&E Participant Stephanie
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
Developing a Standardized and Sustainable Resident Sign-Out Process: An AIAMC National Initiative IV Project
 The Ochsner Journal 14:563 568, 2014 Ó Academic Division of Ochsner Clinic Foundation Developing a Standardized and Sustainable Resident Sign-Out Process: An AIAMC National Initiative IV Project Jacob
The Ochsner Journal 14:563 568, 2014 Ó Academic Division of Ochsner Clinic Foundation Developing a Standardized and Sustainable Resident Sign-Out Process: An AIAMC National Initiative IV Project Jacob
Ensuring Patient Safety and Quality Measures for RRT in AKI 2. Eileen Lischer MA, BSN, RN, CNN University of California, San Diego
 Ensuring Patient Safety and Quality Measures for RRT in AKI 2 Eileen Lischer MA, BSN, RN, CNN University of California, San Diego Today we may be doing what we can, but tomorrow we can improve Hughes,
Ensuring Patient Safety and Quality Measures for RRT in AKI 2 Eileen Lischer MA, BSN, RN, CNN University of California, San Diego Today we may be doing what we can, but tomorrow we can improve Hughes,
Click to edit Master title. style. Click to edit Master title. style. style 8/3/ Are You on Track?
 Are You on Track? Diagnostic Test Results, Consults and Referrals Click to edit Master subtitle EXPLORE Conference August 9, 2018 8/3/2018 1 EXPLORE August 9, 2018 Today s speaker is Brenda Wehrle, BS,
Are You on Track? Diagnostic Test Results, Consults and Referrals Click to edit Master subtitle EXPLORE Conference August 9, 2018 8/3/2018 1 EXPLORE August 9, 2018 Today s speaker is Brenda Wehrle, BS,
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Worth a Thousand Words: Telling a Story with Data
 A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
1. March RN VACANCY RATE: Overall 2320 RN vacancy rate for areas reported is 13.8%
 PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, April 2014 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. March 2014-2320 RN VACANCY RATE: Overall 2320 RN vacancy
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, April 2014 Terry Dentoni, RN, MSN, CNL, Interim Chief Nursing Officer 1. March 2014-2320 RN VACANCY RATE: Overall 2320 RN vacancy
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes
 Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Driving High-Value Care via Clinical Pathways. Andrew Buchert, MD Gabriella Butler, MSN, RN
 Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Driving High-Value Care via Clinical Pathways Andrew Buchert, MD Gabriella Butler, MSN, RN 1 Andrew Buchert, MD Medical Director, Clinical Resource Management Children s Hospital of Pittsburgh of UPMC
Evidence-Informed ICU Rounds. Critical Care Canada Forum October 26, 2015
 Evidence-Informed ICU Rounds Critical Care Canada Forum October 26, 2015 No disclosures or conflicts of interest Many acknowledgements Objectives 1. Summarize why we round 2. Describe current rounding
Evidence-Informed ICU Rounds Critical Care Canada Forum October 26, 2015 No disclosures or conflicts of interest Many acknowledgements Objectives 1. Summarize why we round 2. Describe current rounding
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
ACGME Institutional Requirements
 Graduate Medical Education : Focusing on Quality and Safety in a Clinical Learning Environment Developing a Standardized and Sustainable Resident Sign Out Process Better Hand Off = Safer Care Ron Amedee,
Graduate Medical Education : Focusing on Quality and Safety in a Clinical Learning Environment Developing a Standardized and Sustainable Resident Sign Out Process Better Hand Off = Safer Care Ron Amedee,
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
Corporate Services Employment Report: January Employment by Staff Group. Jan 2018 (Jan 2017 figure: 1,462) Overall 1,
 Overall 1,") Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
Corporate Services Employment Report: January Employment by Staff Group Jan (Jan 20 figure: 1,462) Jan % Overall 1,520 +58 +4.0% 8 Management (VIII+) 403 +52 4.8% Clerical & Supervisory (III to VII) 907
One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration
 One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration Presented by: Marla Husch Northwestern Memorial Hospital Northwestern Memorial Hospital Chicago, Illinois
One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration Presented by: Marla Husch Northwestern Memorial Hospital Northwestern Memorial Hospital Chicago, Illinois
From Big Data to Big Knowledge Optimizing Medication Management
 From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
Sheffield Teaching Hospitals NHS Foundation Trust
 Sheffield Teaching Hospitals NHS Foundation Trust @seamlesssurgery Seamless Surgery Team Sheffield Teaching Hospitals NHS Foundation Trust July 2017 PROUD TO MAKE A DIFFERENCE PROUD TO MAKE A DIFFERENCE
Sheffield Teaching Hospitals NHS Foundation Trust @seamlesssurgery Seamless Surgery Team Sheffield Teaching Hospitals NHS Foundation Trust July 2017 PROUD TO MAKE A DIFFERENCE PROUD TO MAKE A DIFFERENCE
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1
 Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
Aldijana Avdić, BSN, RN, PBMS, CPHQ Assistant Director, Patient Safety and Privacy 1 Program Definition The timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin
The New Clinical Research Landscape Incentives, Opportunities and Support Offered by the NIHR
 The New Clinical Research Landscape Incentives, Opportunities and Support Offered by the NIHR 1 September 2011 Dr Jonathan Gower Assistant Director CCRN The National Institute of Health Research - A real
The New Clinical Research Landscape Incentives, Opportunities and Support Offered by the NIHR 1 September 2011 Dr Jonathan Gower Assistant Director CCRN The National Institute of Health Research - A real
21 st Century Health Care: The Promise and Potential of a Learning Health System
 21 st Century Health Care: The Promise and Potential of a Learning Health System Carolyn M. Clancy, MD Director Agency for Healthcare Research and Quality National Science Foundation Learning Health System
21 st Century Health Care: The Promise and Potential of a Learning Health System Carolyn M. Clancy, MD Director Agency for Healthcare Research and Quality National Science Foundation Learning Health System
TeamSTEPPS TM National Implementation
 TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
Maimonides Medical Center Makes a Quantum Leap with Advanced Computerized Patient Record Technology
 Maimonides Medical Center Makes a Quantum Leap with Advanced Computerized Patient Record Technology Healthcare Information and Management Systems Society Electronic Poster Session CPR System Planning The
Maimonides Medical Center Makes a Quantum Leap with Advanced Computerized Patient Record Technology Healthcare Information and Management Systems Society Electronic Poster Session CPR System Planning The
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Experiential Education
 Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
at OU Medicine Leadership Development Institute August 6, 2010
 Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
Effective Patient Handovers at OU Medicine Leadership Development Institute August 6, 2010 Quality and Patient Safety Realize OU Medicine s position with respect to a culture of safety and quality. Improve
You have joined the CUSP Communication & Teamwork Tools Informational Session!
 You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
Transitions of Care: Vital to Quality Patient Care. Erica Shaver, MD WVU GME Orientation June 2017
 Transitions of Care: Vital to Quality Patient Care Erica Shaver, MD WVU GME Orientation June 2017 Goals of Session Define transition of care What makes for a good or bad handoff? ACGME expectations WVU
Transitions of Care: Vital to Quality Patient Care Erica Shaver, MD WVU GME Orientation June 2017 Goals of Session Define transition of care What makes for a good or bad handoff? ACGME expectations WVU
COPPER COUNTRY MENTAL HEALTH SERVICES ANNUAL QUALITY IMPROVEMENT REPORT FY Introduction
 COPPER COUNTRY MENTAL HEALTH SERVICES ANNUAL QUALITY IMPROVEMENT REPORT FY 2017 Introduction Copper Country Mental Health Services (CCMHS) focuses on improving the quality of our services and identifying
COPPER COUNTRY MENTAL HEALTH SERVICES ANNUAL QUALITY IMPROVEMENT REPORT FY 2017 Introduction Copper Country Mental Health Services (CCMHS) focuses on improving the quality of our services and identifying
Fee: The fee for the 12-month renewal is $10,000.
 CHILDHOOD CANCER AND BLOOD DISORDERS NETWORK 2017 RENEWAL TOOLS HOW TO Renew To renew, simply submit a completed Childhood Cancer & Blood Disorders Network Renewal Form to Gena Paulk via email at gena.paulk@childrenshospitals.org.
CHILDHOOD CANCER AND BLOOD DISORDERS NETWORK 2017 RENEWAL TOOLS HOW TO Renew To renew, simply submit a completed Childhood Cancer & Blood Disorders Network Renewal Form to Gena Paulk via email at gena.paulk@childrenshospitals.org.
NHSN: Information for Action
 NHSN: Information for Action Reducing Healthcare Associated Infections: Tennessee Marion A. Kainer MD, MPH Director, Hospital Infections Program Tennessee Department of Health marion.kainer@tn.gov 1 Outline
NHSN: Information for Action Reducing Healthcare Associated Infections: Tennessee Marion A. Kainer MD, MPH Director, Hospital Infections Program Tennessee Department of Health marion.kainer@tn.gov 1 Outline
Improving Sign-Outs in Hospital Medicine
 Improving Sign-Outs in Hospital Medicine Arpana R. Vidyarthi, MD Assistant Professor of Medicine Division of Hospital Medicine Director of Quality, Division of Hospital Medicine Director, Patient Safety
Improving Sign-Outs in Hospital Medicine Arpana R. Vidyarthi, MD Assistant Professor of Medicine Division of Hospital Medicine Director of Quality, Division of Hospital Medicine Director, Patient Safety
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Harm Across the Board Reporting: How your Hospital Can Get There
 Harm Across the Board Reporting: How your Hospital Can Get There Presentation to KHA Annual Quality Conference March 19, 2014 Jackie Conrad RN, BSN, MBA Improvement Advisor Cynosure Health Objectives Upon
Harm Across the Board Reporting: How your Hospital Can Get There Presentation to KHA Annual Quality Conference March 19, 2014 Jackie Conrad RN, BSN, MBA Improvement Advisor Cynosure Health Objectives Upon
Glenn Rosenbluth, MD. Glenn Rosenbluth, Director, Quality and Safety Programs, GME
 Patient Patient Safety Safety How How Can Can Residents Residents Prevent Prevent Medical Medical Errors Errors & & Improve Improve Quality Quality of of Care Care Glenn Rosenbluth, MD Director, Glenn
Patient Patient Safety Safety How How Can Can Residents Residents Prevent Prevent Medical Medical Errors Errors & & Improve Improve Quality Quality of of Care Care Glenn Rosenbluth, MD Director, Glenn
I-PASS, a Mnemonic to Standardize Verbal Handoffs
 CONTRIBUTORS: Amy J. Starmer, MD, MPH, a,b Nancy D. Spector, MD, c Rajendu Srivastava, MD, MPH, d April D. Allen, MPA, MA, b,e Christopher P. Landrigan, MD, MPH, b,f Theodore C. Sectish, MD b and the I-PASS
CONTRIBUTORS: Amy J. Starmer, MD, MPH, a,b Nancy D. Spector, MD, c Rajendu Srivastava, MD, MPH, d April D. Allen, MPA, MA, b,e Christopher P. Landrigan, MD, MPH, b,f Theodore C. Sectish, MD b and the I-PASS
TeamSTEPPS Introductory Webinar. July 19, 2018
 TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
Catherine Porto, MPA, RHIA, CHP Executive Director HIM. Madelyn Horn Noble 3M HIM Data Analyst
 1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
Adverse Events in Hospitals: How Many and Why Not Reported. Fran Griffin Senior Manager Clinical Programs, BD
 Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Change Management at Orbost Regional Health
 Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Change Management at Orbost Regional Health Our change management journey 1 Medication Change System Meds at Beds 2 The slightly exaggerated before process 3 Project Goals The purpose of the Meds at Beds
Utilizing FPPE and OPPE Effectively OPPE & FPPE. Joint Commission FAQs. Utilizing FPPE and OPPE Effectively. Susan Mellott PhD, RN.
 Utilizing FPPE and OPPE Effectively Susan Mellott PhD, RN, CPHQ, FNAHQ OPPE & FPPE For the sake of this presentation, OPPE and FPPE will be discussed as it pertains to physicians. However, all information
Utilizing FPPE and OPPE Effectively Susan Mellott PhD, RN, CPHQ, FNAHQ OPPE & FPPE For the sake of this presentation, OPPE and FPPE will be discussed as it pertains to physicians. However, all information
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Presentation Outline
 Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August 2016
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
HPV Vaccination Quality Improvement: Physician Perspective
 HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
Pharmaceutical Services Report to Joint Conference Committee September 2010
 Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
The CAUTI Can-Can. Hennepin County Medical Center August Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion
 Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017
 Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Effective Management of Complaints and Grievances
 October 7, 2016 Effective Management of Complaints and Grievances Jennifer Comerford, MJ, OTR/L, CHC, HEM Senior Risk Management Analyst My Own Experiences Provider Family member Manager True or False???
October 7, 2016 Effective Management of Complaints and Grievances Jennifer Comerford, MJ, OTR/L, CHC, HEM Senior Risk Management Analyst My Own Experiences Provider Family member Manager True or False???
CAMDEN CLARK MEDICAL CENTER:
 INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
Improving the Patient Experience through Key Nursing Practices and Authentic Patient Connections
 Improving the Patient Experience through Key Nursing Practices and Authentic Patient Connections Mary Del Guidice, MSN, BS, RN, CENP Chief Nursing Officer Penn Medicine, Pennsylvania Hospital Assistant
Improving the Patient Experience through Key Nursing Practices and Authentic Patient Connections Mary Del Guidice, MSN, BS, RN, CENP Chief Nursing Officer Penn Medicine, Pennsylvania Hospital Assistant
Medication Errors and Safety. Educating for Quality Improvement & Patient Safety
 Medication Errors and Safety Educating for Quality Improvement & Patient Safety 1 Mandie Tiball Svatek, MD has no relevant financial relationships with commercial interests to disclose. Rayanne Wilson,
Medication Errors and Safety Educating for Quality Improvement & Patient Safety 1 Mandie Tiball Svatek, MD has no relevant financial relationships with commercial interests to disclose. Rayanne Wilson,
Medical Education Across the Continuum: A Snapshot in Time
 2014 MMS Annual Oration Medical Education Across the Continuum: A Snapshot in Time 2004-2014 Michele P Pugnaire MD Senior Associate Dean for Educational Affairs UMass Medical School Massachusetts Medical
2014 MMS Annual Oration Medical Education Across the Continuum: A Snapshot in Time 2004-2014 Michele P Pugnaire MD Senior Associate Dean for Educational Affairs UMass Medical School Massachusetts Medical
Adverse Drug Events and Readmissions: The Global Picture
 Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
And the Evidence Shows Using Specialty Certification from The Joint Commission Improves Quality
 And the Evidence Shows Using Specialty Certification from The Joint Commission Improves Quality Leisha Buller, MSN, ACNP-BC Lindsey Canon, MSN, RNC Ashley Hodo, MSN, RN Using The Joint Commission s Certification
And the Evidence Shows Using Specialty Certification from The Joint Commission Improves Quality Leisha Buller, MSN, ACNP-BC Lindsey Canon, MSN, RNC Ashley Hodo, MSN, RN Using The Joint Commission s Certification
Implementation Model. Levels of Evidence 3/9/2011. Strategies to get Evidence into Practice EXTRACTING. Elizabeth Bridges PhD RN CCNS, FCCM, FAAN
 Implementation Model Strategies to get Evidence into Practice Extracting Summarizing Embedding g g Elizabeth Bridges PhD RN CCNS, FCCM, FAAN Clinical Nurse Researcher University of Washington Medical Center
Implementation Model Strategies to get Evidence into Practice Extracting Summarizing Embedding g g Elizabeth Bridges PhD RN CCNS, FCCM, FAAN Clinical Nurse Researcher University of Washington Medical Center
Enhancing Communication Skills: A Catalyst for Organizational Cultural Transformation Presented by William Maples, MD, Chief Medical Officer,
 Enhancing Communication Skills: A Catalyst for Organizational Cultural Transformation Presented by William Maples, MD, Chief Medical Officer, Professional Research Consultants and Executive Director, The
Enhancing Communication Skills: A Catalyst for Organizational Cultural Transformation Presented by William Maples, MD, Chief Medical Officer, Professional Research Consultants and Executive Director, The
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
PACT: The VA s Medical Home
 A5/B5 This presenter has nothing to disclose PACT: The VA s Medical Home What is working to change a big system Mike Davies, MD Director VA Systems Redesign Rich Stark, MD Director VA Primary Care Operations
A5/B5 This presenter has nothing to disclose PACT: The VA s Medical Home What is working to change a big system Mike Davies, MD Director VA Systems Redesign Rich Stark, MD Director VA Primary Care Operations
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
7-8 September 2016 Sheraton Hotel & Towers Ho Chi Minh City, Vietnam
 7-8 September 2016 Sheraton Hotel & Towers Ho Chi Minh City, Vietnam www.hospitalmanagementasia.com 2 Empower Hospital Quality Culture through Accreditation About Vinmec Mission To deliver world class
7-8 September 2016 Sheraton Hotel & Towers Ho Chi Minh City, Vietnam www.hospitalmanagementasia.com 2 Empower Hospital Quality Culture through Accreditation About Vinmec Mission To deliver world class
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
Developing Work Experience Placements for Schools. Will McConnell
 Developing Work Experience Placements for Schools Will McConnell Work experience Keen to encourage students from a wide range of backgrounds to consider a medical career Frustrations from consultant colleagues
Developing Work Experience Placements for Schools Will McConnell Work experience Keen to encourage students from a wide range of backgrounds to consider a medical career Frustrations from consultant colleagues