Accountable Care and ACOs. Len Fromer, M.D., FAAFP
|
|
|
- Gervase Hill
- 5 years ago
- Views:
Transcription
1 Accountable Care and ACOs Len Fromer, M.D., FAAFP
2 It is not the strongest of the species that survives, nor the most intelligent, but the one most responsive to change. Charles Darwin
3 The Reality: The healthcare world is changing in ways that many of us have never seen in our lifetime, with the possible exception of Medicare.
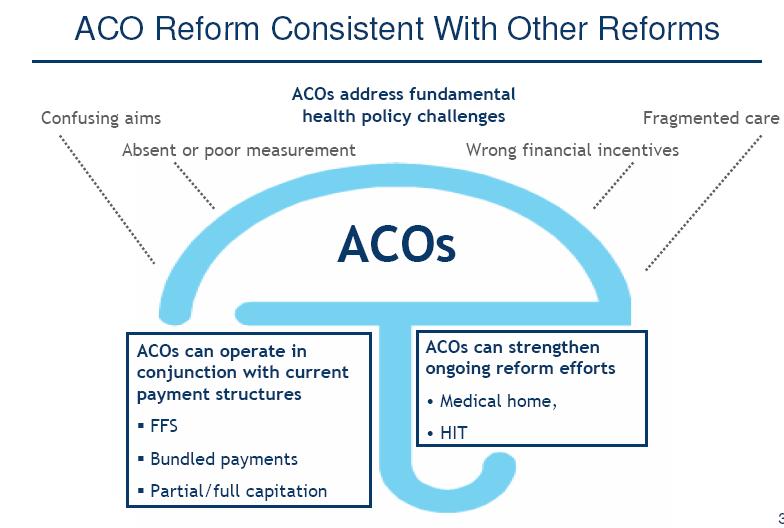
4 Drivers of Accountable Care Providers, not insurers, who are best placed to make the changes Cost and quality problems resulting from the U.S. s current system of fragmented care Variation in practice patterns Volume based payment systems Current lack of Integration Policymakers understand that the resources that flow from the decisions physicians make with patients account for a major portion of overall health care costs regardless of where that care takes place
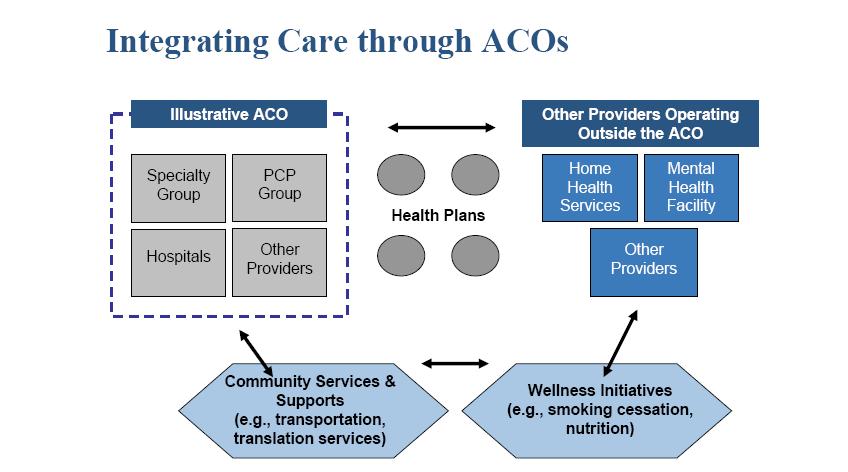
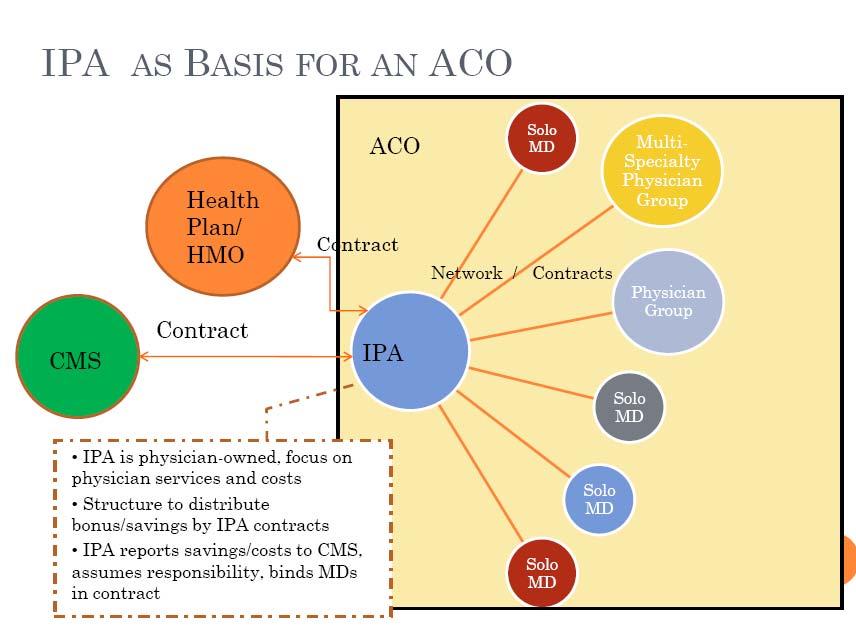
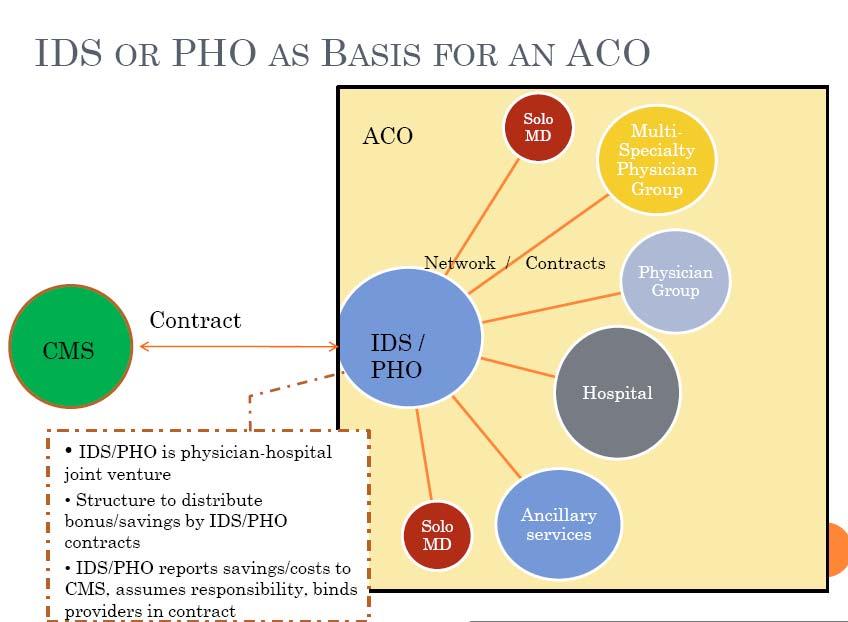
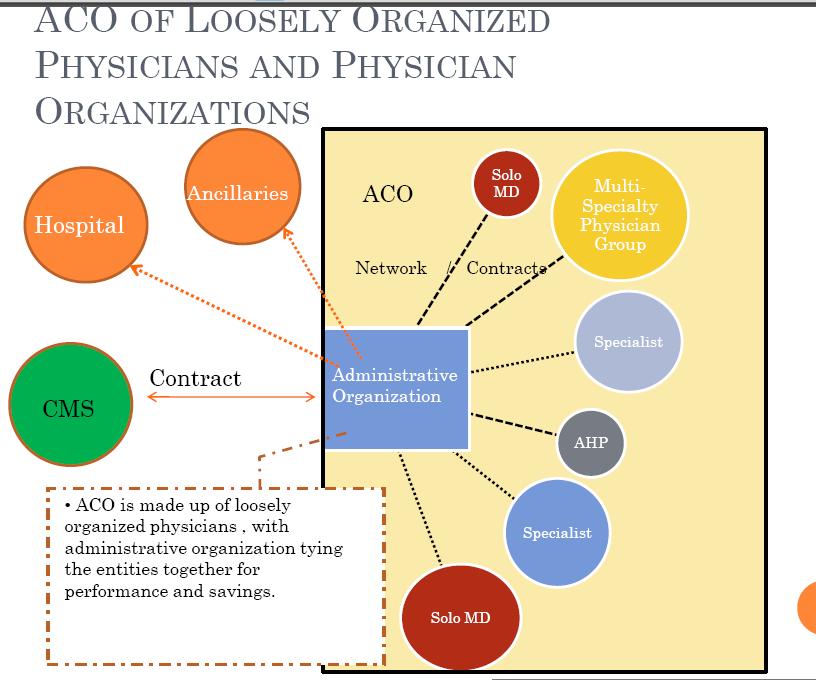
5 Principles of Accountable Care An ACO is a local health care organization and a related set of providers (at a minimum, primary care physicians, specialists, and hospitals) that can be held accountable for the cost and quality of care delivered to a defined population The goal of the ACO is to deliver coordinated and efficient care. ACOs that achieve quality and cost targets will receive some sort of financial bonus Care for patients across the continuum of care, in different institutional settings Support comprehensive, valid and reliable measurement of its performance
6 Clinical Performance Measurement is Fundamental Clinical performance measures are derived from evidencebased practice guidelines They can be used for quality improvement, public reporting, accountability or pay for performance. Reporting allows for group, regional and national comparison data In most cases, optimal performance is not known because we have not been measuring 6
7 Measuring and Improving Quality Map processes to eliminate waste and remove delays. Identify a set of balanced measures. Build performance measurement into your processes. Choose the appropriate statistics to plot. Use sampling when needed to conserve resources. Plot data in time order every month. Develop excellent visual displays. Monitor measurement results. Use small scale, rapid PDSA cycles to continuously improve.

8 Example: Dashboard
9 Conclusion: You Can t Manage what You Can t Measure Measurement is the foundation for improvement Make measurement and data collection as efficient as possible Monitor results using a dashboard that all can see Report results and look for best practices
10 What If?????? The healthcare provider had updated information on recent patient/provider encounters The healthcare provider had the most recent (even hours old) imaging studies The healthcare provider had the most recent lab data The healthcare provider actually had accurate medication lists The healthcare provider knew who was responsible for coordinating the patient s care The healthcare provider could manage and coordinate a patient s care without face to face contact Technology was utilized to capacity The healthcare provider actually knew which specialists were most effective and efficient

11 The Medical Village
12 Principles of The Patient Centered Medical Home Personal Physician trained to provide continuous, comprehensive care Physician Directed Medical Practice Whole Person Orientation Coordinated Care Quality and Safety Enhanced Access to Care Payment appropriately recognizes added value provided to the overall system

13 A Medical Home for All
14 Great Outcomes Quality Built In Patient Service Practice Management Health IT Primary Care
15 Great Outcomes Patients Office Staff Physicians Community Culture of Improvement Performance Measurement Reliable Systems Quality Built In Patient Service Convenient Access Personalized Care Care Coordination Financial Personnel Clinical Systems Practice Management Health IT Process Automation (EHR) Communication Connectivity EBM Support Clinical Information Systems Primary Care Continuous Healing Relationship Whole Person Orientation Family and Community Context Comprehensive Care
16 Principles of The Patient Centered Medical Home/Accountable Care/Clinical Integration Personal Physician trained to provide continuous, comprehensive care Physician Directed Medical Practice Whole Person Orientation Coordinated Care Quality and Safety Enhanced Access to Care Payment appropriately recognizes added value provided to the overall system Better patient care for the best price
17
18
19
20
21

22 Today Today Pilots Today 2013 Pilots* 2012 Pilots* Source: The Advisory Board, 2010 *Medicare Pilots waiver of anti-trust & anti-kickback
23
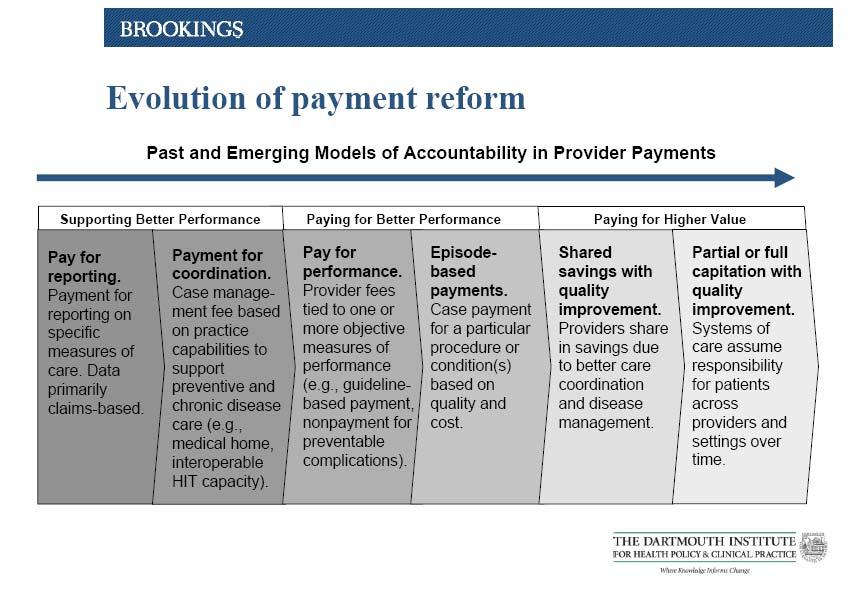
24 Payment Methodologies Enhanced fee for service Care management fees Capitated, no risk models Shared savings Targeted incentives for quality and efficiency Global or bundled payments Accountable care organizations HIT stimulus incentives
25 Shared Savings/ACO Model Downward pressure on hospital days and ER visits Concept is to share savings from reduced hospital days and other costs with referring physicians Opportunity for hospital at home concept Component of CMS pilot and some Medicare advantage projects and potentially Medicaid Managed Care
26 Global/Bundled Payments Hospitals might control total revenue from admission based on diagnosis based on Diagnosis DRG to include physician component Reimbursement for hospital admission may include 3 days before admission and 30 days after Focus on networks and systems by the government Hospital Systems are becoming active in PCMH discussions
27 Practice Payment Methods Enhanced FFS (Fee for Service) Enhanced FFS +P4P (outcomes based) Enhanced FFS + Care Management Fee (CMF) Enhanced FFS + CMF + incentives (outcomes = quality and efficiency (cost savings) and PCMH recognition) CMF (care management fee)+ incentives CMF + incentives + grants CMF + incentives + shared savings Capitation, no risk + incentives Capitation, no risk with FFS carve outs for procedures and incentives

28 Let s Make It Real for You: Prevention and Wellness Chronic Diseases Population Management Care Teams Your Patients The Patient Pathway
29 Community Resources & Policies Chronic Care Model (CCM) Clinical Information Systems Health System Health Care Organization Decision Support Delivery System Design Self- Management Support Informed, Activated Patient Productive Interactions Prepared, Proactive Practice Team Slide from E. Wagner Improved Outcomes
30 The Patient Pathway Model Office calls/ s with appointment reminder & instructions to get labs done before visit Group Medical Appointments Group Medical Appointments - Treatment Plan - Treatment Plan Terese: Terese: Diagnosed Diagnosed with with Type Type II II Diabetes Diabetes Diabetes Diabetes Coordinator Coordinator Terese: Terese: 6 6 Months Months After After Diagnosis Diagnosis Diabetes Diabetes Coordinator Coordinator Terese: Terese: 1 1 Year Year After After Diagnosis Diagnosis Diabetes Diabetes Coordinator-Led Coordinator-Led Education Education Diabetes Diabetes Coordinator Coordinator Patient Profile Dashboard Glycemic Control: A1C: 8.4% FPG: ~210mg/dL Blood pressure: 142/90 mmhg Lipids: LDL-C: 98 mg/dl; HDL-C: 37 mg/dl; TG: 151 mg/dl Treatment Physician initiated metformin 500 mg once/day Planned titrations to 500 mg twice per day over ~2 weeks Taking ACE inhibitor/thiazide diuretic at therapeutic doses for blood pressure Taking statin at therapeutic doses Diabetes Self Management Education (eg, physical activity and nutrition) Physician discusses how insulin may be introduced as a treatment option for long-term disease management EMR EMR Review Review treatment treatment plan plan and and determine determine health health literacy: literacy: +Allow +Allow patients patients to to voice voice concerns concerns uninterrup uninterrup ted ted Patient Patient selfselfmanagemen managemen t t Patient Profile Dashboard Glycemic control: A1C: 8.1%, FPG: 195 mg/dl Blood pressure: 136/86 mmhg Lipids: LDL-C: 90 mg/dl; HDL-C: 48 mg/dl; TG: 150 mg/dl Treatment Metformin dose titrated to 1000 mg bid Sulfonylurea added No change in ACE inhibitor/thiazide diuretic and statin dose Next follow-up with physician is scheduled for 3 months later Physician discusses the potential need for a second therapeutic agent and will assess patient s status at next visit EMR EMR Determine Determine patient health patient health literacy literacy Patient self Patient self management management +Does patient +Does patient pay attention pay attention to symptoms to symptoms and problems? and problems? Assess Assess medication medication adherence adherence +Brown bag +Brown bag medication medication review: Patient review: Patient brings ALL brings ALL medications in medications in (even (even supplements/ supplements/ vitamins) and vitamins) and TELLS YOU TELLS YOU how they how they take them take them +Reminder +Reminder checklists checklists Mail/ support reminders with culturally appropriate nutrition guidance & simple physical activities Terese missed last followup appointment: Teach Forward approach to reduce fear of bad news Why appointments are missed: Emotional: eg, fear of insulin Perceived disrespect: Consider flexible office hours Don t understand scheduling system: Reduce wait time Patient Profile Dashboard Glycemic control: A1C: 8.0%, FPG: 190 mg/dl Blood pressure: 132/82 mmhg Lipids: LDL-C: 85 mg/dl; HDL-C: 52 mg/dl; TG: 148 mg/dl Treatment Long-acting basal insulin at 2 units/every 3 days Metformin dose continued at 1000 mg twice daily Sulfonylurea continued DIGMA DIGMA Group Group Education Education -Insulin -Insulin education education class class - -Titration Titration education education --Foot --Foot & & eye eye exam exam EMR EMR Determine Determine patient patient health health literacy literacy Patient self Patient self manageme manageme nt nt +Blood +Blood sugar sugar testing testing and what and what to do with to do with results results Assess Assess medication medication adherence adherence +Proper +Proper insulin insulin usage usage and and storage storage Mail/ support reminders with group education networking/ support

31 Patient Care Pathway Creates a Map of the Patient Experience through the Healthcare System Coordinated care team Patient empowerment Health literacy Patient population management Electronic medical records
32 The Patient Dashboard: A Means to Assess, Monitor, and Modify Test Patient Dashboard Height 5 6" Weight BMI Average of 3 office BP measurements Treatment 160 lbs Initial Visit Data 25.8 kg/m 2 (overweight) 140/89 mm Hg HTN management: ACE inhibitor (ramipril 10 mg qd); (second medication of choice) Diabetes management: metformin 850 mg bid Test Height 5 6" Weight BMI Fasting blood glucose Average of 3 office BP measurements Treatment Patient Dashboard 155 lbs 6-Week Visit Data 25.0 kg/m 2 (slightly overweight) 110 mg/dl 127/78 mm Hg No change to meds Continue nonpharmacologic interventions Focus on lifestyle changes to control blood glucose The information presented in this case is a hypothetical example and not based on an actual patient

33 The Patient Pathway Highlights HIT/EHRs Input findings from the patient assessment Include diagnosis at current visit: uncontrolled blood pressure despite ACE inhibitor therapy Additional information Patient portal referral and explanation Nonpharmacologic measures Adherence assessment Self management tools and tips Input change in treatment Add 2 nd BP medication to ACE inhibitor Reminder: /call patient in 2 to 3 days to assess tolerability Patient Reminders Measure and record blood pressure weekly Office visits Blood work Other Referrals Nonpharmacologic measures Group visit The information presented in this case is a hypothetical example and not based on an actual patient
34 The Patient Pathway Highlights Team Based Care Models: Every Member Plays A Part Shared Responsibilities to Reach a Common Goal Patient Registry Motivational interview Checked medication adherence Updated EMR Distributed educational tools Lifestyle SMBG (diet/exerci se) Outreach to patient after appointment MD date date Nurse/NP/P A date date date date Office Staff date date date date Pharmacy CDE date date date date Sample Task List
35 Evolution of Expectations for Physicians Clinical Integration Team based care Focus on the top of license/training & interest Improved communication Improved data flow & access Right patient at the right time Patient centered aligned incentives outcomes, quality, cost External accountability outcomes, quality, cost


36 The result of the goals of higher quality, better coordinated, more efficient care via PCMH
37 The Value of Primary Care and PCMH One year data from payer pilots has demonstrated that individual practices can provide the equivalent of higher quality at lower cost as published data from large integrated systems
38 The Bottom Line: Value Quality / Cost Maximize the numerator Decrease the denominator
39
The Role of the Pharmacist in Value Based Health Care Systems. Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine
 The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Peripheral Arterial Disease: Application of the Chronic Care Model. Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario
 Peripheral Arterial Disease: Application of the Chronic Care Model Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario Objectives Provide brief overview of PAD Describe the Chronic
Peripheral Arterial Disease: Application of the Chronic Care Model Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario Objectives Provide brief overview of PAD Describe the Chronic
New Models of Care: Diabetes and the Triple Aim
 Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Advancing Care Information Measures
 Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
Participants: Advancing Care Information Measures In 2017, Advancing Care Information (ACI) measure reporting is optional for Nurse Practitioners, Physician Assistants, Clinical Nurse Specialists, CRNAs,
MEANINGFUL USE STAGE 2
 MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Accelerating the Impact of Performance Measures: Role of Core Measures
 Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Transforming to Value: One Way Forward
 Transforming to Value: One Way Forward Intermountain Healthcare s Value-Based Reimbursement and Change Management Strategy Mark Briesacher, MD Senior Administrative Medical Director Intermountain Medical
Transforming to Value: One Way Forward Intermountain Healthcare s Value-Based Reimbursement and Change Management Strategy Mark Briesacher, MD Senior Administrative Medical Director Intermountain Medical
Promoting Interoperability Measures
 Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
Promoting Interoperability Measures Previously known as Advancing Care Information for 2017 and Meaningful Use from 2011-2016 Participants: In 2018, promoting interoperability measure reporting (PI) is
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Presbyterian Healthcare Services Care Management
 Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Presbyterian Healthcare Services Care Management Kathy M. Garcia RN, BSN Director of Nursing, Primary Care Service Line November 2012 Future Healthcare Challenges Increasing number of patients Decreasing
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
Building the Universal Roadmap to Population Health Management
 Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Please stand by. There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1
 Please stand by There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1 Webinar Tips Today s webinar is a one-way audio broadcast through
Please stand by There is no audio being streamed right now. We are doing a audio/sound check before we begin the presentation 10/28/2015 1 Webinar Tips Today s webinar is a one-way audio broadcast through
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
Health Home Flow Hypothetical Patient Scenario
 Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, :00 5:00 PM
 ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, 2017 3:00 5:00 PM ACPE UAN: 0107-9999-17-105-L04-P 0.2 CEU/2.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon
ENHANCING PRESCRIBER RELATIONSHIPS: MAKING IT A WIN-WIN JULY 12, 2017 3:00 5:00 PM ACPE UAN: 0107-9999-17-105-L04-P 0.2 CEU/2.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: Upon
Quality: Finish Strong in Get Ready for October 28, 2016
 Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
CROSSWALK FOR AADE S DIABETES EDUCATION ACCREDITATION PROGRAM
 Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Procedure Code Job Aid
 Procedure Code 99211 Job Aid Definition for 99211: Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician. Usually,
Procedure Code 99211 Job Aid Definition for 99211: Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician. Usually,
Payment Reform Strategies. Ann Thomas Burnett BlueCross BlueShield of South Carolina
 Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
PCMH to ACO: Carilion Clinic s Journey
 PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Emerging Models of Care Delivery Christy Mokrohisky Ex. Dir. of PI & Emerging Models
 Emerging Models of Care Delivery Christy Mokrohisky Ex. Dir. of PI & Emerging Models 1 Sacred Encounters Perfect Care Healthiest Communities St. Joseph Heritage Healthcare Founded in 1994 Manage 7 Medical
Emerging Models of Care Delivery Christy Mokrohisky Ex. Dir. of PI & Emerging Models 1 Sacred Encounters Perfect Care Healthiest Communities St. Joseph Heritage Healthcare Founded in 1994 Manage 7 Medical
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Managing Patients with Multiple Chronic Conditions
 Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
3 Ways to Increase Patient Visits
 3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
Paving the Way for. Health Homes
 Paving the Way for Health Homes Paving the Way for Healthcare Homes Affordable Care Act The Affordable Care Act passed by Congress and signed into law by the president in March 2010, provides a variety
Paving the Way for Health Homes Paving the Way for Healthcare Homes Affordable Care Act The Affordable Care Act passed by Congress and signed into law by the president in March 2010, provides a variety
Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care
 Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care Introduction This white paper examines how new technologies are creating a fully connected point of care
Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care Introduction This white paper examines how new technologies are creating a fully connected point of care
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc.
 Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs
 HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs March 2017 Document Title: HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs (DMP) Document
HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs March 2017 Document Title: HAAD Guidelines for The Provision of Cardiovascular Disease Management Programs (DMP) Document
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018
 Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
A. DIABETES AND HEART/STROKE Data Detail
 A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Value of HIT. Pat Wise VP, Health Information Systems HIMSS North America June 21, 2017
 Value of HIT Pat Wise VP, Health Information Systems HIMSS North America June 21, 2017 Value of HIT Value Score Pat Wise RN, MA, MS, FHIMSS COL (USA ret'd) Vice President, Health Information Systems Objectives
Value of HIT Pat Wise VP, Health Information Systems HIMSS North America June 21, 2017 Value of HIT Value Score Pat Wise RN, MA, MS, FHIMSS COL (USA ret'd) Vice President, Health Information Systems Objectives
W. Douglas Weaver, MD, MACC. American College of Cardiology SENATE FINANCE COMMITTEE
 Statement of W. Douglas Weaver, MD, MACC On behalf of the American College of Cardiology Presented to the SENATE FINANCE COMMITTEE Roundtable on Medicare Physician Payments: Perspectives from Physicians
Statement of W. Douglas Weaver, MD, MACC On behalf of the American College of Cardiology Presented to the SENATE FINANCE COMMITTEE Roundtable on Medicare Physician Payments: Perspectives from Physicians
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Partners HealthCare Primary Care Quality and Patient Experience Reports 2017
 Partners HealthCare Primary Care Quality and Patient Experience Reports 2017 North Shore Health System QUALITYANDSAFETY.PARTNERS.ORG 1 INTRODUCTION Dear Patients, Colleagues and members of the Commonwealth
Partners HealthCare Primary Care Quality and Patient Experience Reports 2017 North Shore Health System QUALITYANDSAFETY.PARTNERS.ORG 1 INTRODUCTION Dear Patients, Colleagues and members of the Commonwealth
Using the Patient Activation Measure (PAM) to Promote Patient Engagement
 to Promote Patient Engagement") Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Building the Oncology Medical Home John D. Sprandio, M.D., FACP Consultants in Medical Oncology & Hematology, P.C. Oncology Management Services, LLC
 Building the Oncology Medical Home John D. Sprandio, M.D., FACP Consultants in Medical Oncology & Hematology, P.C. Oncology Management Services, LLC Oncology Patient-Centered Medical Home Update Background
Building the Oncology Medical Home John D. Sprandio, M.D., FACP Consultants in Medical Oncology & Hematology, P.C. Oncology Management Services, LLC Oncology Patient-Centered Medical Home Update Background
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Improvement Activities Data Validation Criteria
 Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
NextGen Population Health TEN TEN TEN TEN TE. Prevent Patients from Falling Through the Cracks in 10 Easy Steps
 NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
NextGen Population Health TEN TEN TEN TEN TE Prevent Patients from Falling Through the Cracks in 10 Easy Steps Proactive, automated patient engagement anytime, anywhere. Automate care management to improve
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Improvement Activities Data Validation Criteria
 Activity ID IA_EPA_1 Subcategory Name Access Activity Name Activity Description Activity Weighting Provide 24/7 access to eligible Provide 24/7 access to MIPS eligible clinicians, groups, or care teams
Activity ID IA_EPA_1 Subcategory Name Access Activity Name Activity Description Activity Weighting Provide 24/7 access to eligible Provide 24/7 access to MIPS eligible clinicians, groups, or care teams
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination
 Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Keenan Pharmacy Care Management (KPCM)
") Keenan Pharmacy Care Management (KPCM) This program is an exclusive to KPS clients as an additional layer of pharmacy benefit management by engaging physicians and members directly to ensure that the best
Keenan Pharmacy Care Management (KPCM) This program is an exclusive to KPS clients as an additional layer of pharmacy benefit management by engaging physicians and members directly to ensure that the best
MIPS; Improving Your Score with ecqi. Patty Kosednar, PMP, CPEHR, CPHIMS HIT Project Manager
 MIPS; Improving Your Score with ecqi Patty Kosednar, PMP, CPEHR, CPHIMS HIT Project Manager HealthInsight Our business is redesigning health care systems for the better HealthInsight is a private, non-profit,
MIPS; Improving Your Score with ecqi Patty Kosednar, PMP, CPEHR, CPHIMS HIT Project Manager HealthInsight Our business is redesigning health care systems for the better HealthInsight is a private, non-profit,
3/29/2013. Effective ACO Compliance. Objectives THE HEALTH CARE DILEMMA: ARE ACOS THE ANSWER? HCCA Compliance Institute April 21, 2013
 Effective ACO Compliance HCCA Compliance Institute April 21, 2013 Margaret Hambleton, MBA, CHC, CHPC Sr. Vice President, Chief Compliance Officer St. Joseph Health System 1 Objectives Understand Accountable
Effective ACO Compliance HCCA Compliance Institute April 21, 2013 Margaret Hambleton, MBA, CHC, CHPC Sr. Vice President, Chief Compliance Officer St. Joseph Health System 1 Objectives Understand Accountable
Population Health: Physician Perspective. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015
 Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012
 Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Using Data to Yield High Impact Business Intelligence Wednesday, July 25, 2012 Brent J. Estes President and CEO, Rush Health About Rush Rush University Medical Center 673 Beds 36,000 admissions 391,700
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
6/3/ National Wellness Conference. Developing Strategic Partnerships to improve the Health and Wellness of the Community. Session Objectives
 2015 National Wellness Conference Developing Strategic Partnerships to improve the Health and Wellness of the Community. Kimberly Sbardella, R.N. Manager, Community Health & Wellness Carolinas HealthCare
2015 National Wellness Conference Developing Strategic Partnerships to improve the Health and Wellness of the Community. Kimberly Sbardella, R.N. Manager, Community Health & Wellness Carolinas HealthCare
Healthy Aging Recommendations 2015 White House Conference on Aging
 Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Healthy Aging Recommendations 2015 White House Conference on Aging Chronic diseases are the leading causes of death and disability in the U.S. and account for 75% of the nation s health care spending.
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule
 Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Catholic Medical Partners
 Improving Health Outcomes Patricia Podkulski, MS,RN October 13, 2011 Catholic Medical Partners 2 Independent Practice Association WNY: Erie/Niagara counties 900 physicians Four (4) Acute Care Hospitals
Improving Health Outcomes Patricia Podkulski, MS,RN October 13, 2011 Catholic Medical Partners 2 Independent Practice Association WNY: Erie/Niagara counties 900 physicians Four (4) Acute Care Hospitals
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Future of Patient Safety and Healthcare Quality
 Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
Future of Patient Safety and Healthcare Quality Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for Medicare and Medicaid
2017 National Standards for Diabetes Self-Management Education and Support INTERPRETIVE GUIDANCE
 2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
Health Information Technology
 ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
ACO Congress Oct 25, 2010 Los Angeles, CA Patient Centered Medical Home and Accountable Care Organizations Health Information Technology David K. Nace MD, Medical Director, McKesson Corporation Co-Chair,
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
How Does This Fit into the Provisions of the Affordable Care Act? The goals are aligned
 Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies