D. Fistula First (FF) Initiative.
|
|
|
- Alan McKinney
- 5 years ago
- Views:
Transcription
1 D. Fistula First (FF) Initiative. The development of Quality Improvement Projects (QIP) is mandated in the ESRD Network contracts with CMS. The QIPs are developed and directed by the MRB, then reviewed, approved and monitored by the Board of Trustees. In 2010, the majority of quality improvement efforts were focused on continuing and improving AV fistula rates through the Fistula First Initiative. Background: In 2003, all 18 of the ESRD Networks and CMS, along with clinicians, dialysis providers, and patients, developed a three-year plan called the National Vascular Access Improvement Initiative (renamed Fistula First in 2004). This plan implements strategies for the improvement of patient vascular access outcomes to reach the CMS goal and K/DOQI guidelines for AV fistula use of >65% prevalence. Fistula First aims to build on established methods to increase fistula use, and to take advantage of system-level diagnosis and strategies for improvement. Collaboration between ESRD Networks, providers, physicians, vascular surgeons, and health professionals is key to spreading the change ideas for improving AV fistulas Primary objectives: To increase the prevalence rate of AV fistula in Network 9 from 51.1 percent in March 2010 to 54.1 percent in March 2011 (an increase of 3.0 percentage points) and to increase Network 10 from 54.2 percent in March 2010 to 56.6 percent in March 2011 (an increase of 2.4 percentage points). To increase the awareness of early referral for vascular access in the incident CKD patient. To educate providers, physicians, and vascular access surgeons on documentation of AV fistula assessment pre-hemodialysis access placement. To educate providers, physicians, and vascular access surgeons on the AV fistula improvement strategy. To provide resources and tools to providers to assist with developing initiatives for placement and assessment of AV fistula and catheter reduction. To educate medical directors, providers, and the facility interdisciplinary team on the best practices of a Quality Assessment and Performance Improvement (QAPI) program for vascular access management.
2 Progress toward these goals by December 2010 is detailed in Figure 44: Figure 44. Network 9/10 Fistula First Percentages Fistula Prevalence as of December 2010 Fistula Prevalence Network 9 Mar 10 Dec 10 Network 10 Achieved Goal Mar 10 Dec 10 K/DOQI Guidelines CMS Stretch Goal 51.1% 53.6% 54.2% 56.3% >65% 66% Actions. The national Fistula First Breakthrough Initiative (FFBI) coalition conducted an extensive root cause analysis in This root cause analysis was used to develop a strategic plan that identified priority areas to be addressed. The following seven strategies were developed into an operational plan to increase the AV fistula utilization rate to 66% in prevalent hemodialysis patients for ESRD Networks and to assist Quality Improvement Organizations (QIOs) in reducing the gap between the statewide baseline AV fistula rate and 66% for incident hemodialysis patients: Strategy 1: Nephrologist as Leader - Encourage and support nephrologists to take a leadership role and be accountable for vascular access management in all hemodialysis patients. Strategy 2: Leveraging Partnerships - Partner to improve AV fistula placement and utilization rates. Strategy 3: Hospital Systems - Modify hospital systems to promote AV fistula placement. Strategy 4: Patient Self-Management - Promote patient self-management throughout the stages of chronic kidney disease. Strategy 5: Addressing Access Problems - Promote fast-track protocols for rapid identification and referral of vascular access problems which include failure to mature, revision of the failing AV fistula, and placement of an AV fistula. Strategy 6: Practitioner Training and Credentialing - Promoting training, experience, and credentialing of healthcare professionals in the area of hemodialysis vascular access management.
3 Strategy 7: FFBI Change Concepts - Expand and endorse the current Change Concepts for education and promotion throughout the renal, surgical, and interventional communities. The staff of Network 9/10 utilized tools and resources from for education and technical support and marketed new tools that were developed through FFBI to providers and professionals. The staff of Network 9/10 participated on FFBI activities at the national, regional and local level. The Quality Improvement Department developed a vascular access management resources handbook using many of the tools provided on the FFBI Web site. The 3P s (Prevention of Catheters, Placement and Use of AVF, Preservation of AVF) of Vascular Access Success Handbook was developed using best practice protocols, algorithms, and Fistula First resources. The intent of the 3 P s handbook is to guide hemodialysis vascular access improvement efforts and change existing practices through Quality Assessment and Performance Improvement (QAPI) projects. This handbook brings together a number of best-practice concepts and suggested tools in support of those concepts. Some tools were included as hardcopy and many are available as a downloadable resource on The Renal Network, Inc. Web site, Nationally, Network 9/10 participated on the FFBI conference calls for Network Quality Improvement Directors (QIDs) on January 13, April 21, May 12, June 9, July 14, August 11, September 8, October 13, and November 11, The Quality Improvement Director attended a FFBI Learning Session development conference call on February 19, Vascular Access Advisory Panel. A panel of experts oversees the Fistula First Initiatives, under the direction of the MRB. This Vascular Access Advisory Panel (VAAP) was organized at the beginning of the Fistula First Initiative in The VAAP continued its activities during Members of the panel include: Tim Pflederer, M.D., Chair Renal Care Associates Peoria Illinois Anil Agarwal, M.D. Ohio State University Columbus Ohio George Aronoff, M.D. University of Louisville Louisville Kentucky Stephen Ash, M.D. Wellbound Lafayette Indiana Michael Brier, Ph.D. University of Louisville Louisville Kentucky
4 Luis Cespedes, M.D. RCG-Villa Park Elmhurst Illinois Deepa Chand, M.D. Akron Children s Medical Center Akron Ohio Peter DeOreo, M.D. Centers for Dialysis Care Cleveland Ohio Wendy Jagusch, R.N. Centers for Dialysis Care Cleveland Ohio Mary Hammes, D.O. Woodlawn Dialysis Chicago Illinois Richard Keen, M.D. John H. Stroger Hospital of Chicago Illinois Cook County Gordon McLennan, M.D. Cleveland Clinic Cleveland Ohio Prabir Roy-Chaudhury, M.D. University of Cincinnati Cincinnati Ohio Mary Showers, R.N. DaVita Elyria Ohio Marcia Silver, M.D. Metro Health Medical Center Cleveland Ohio Louis Thibodeaux, M.D. General & Vascular Surgical Cincinnati Ohio Specialists Jay B. Wish, M.D. University Hospitals of Cleveland Cleveland Ohio The VAAP is charged with developing and implementing strategies to achieve Fistula First goals, under the direction of the MRB. The VAAP met twice during 2010, once in May and once in October. Conference calls were scheduled during interim times to continue the work of this advisory body. Reports of VAAP activities were made continuously to the MRB. Network staff participates on the national FFBI coalition, so ideas between these two groups are shared routinely. Although at year-end the CMS contract goal in Network 9 had not been met, interim targets were achieved and the staff of Network 9/10 worked with facility staff members toward improving the AV fistula rates for the regional population of Illinois, Indiana, Kentucky and Ohio. Data Distribution. Fistula First Facility Specific Reports were sent to all hemodialysis programs in February 2010 to show fourth quarter 2009 data, June 2010 to show first quarter 2010 data, September 2010 to show second quarter, December 2010 to show third quarter 2010 data, and February 2011 to show fourth quarter 2010 data. This quarterly FF data report gives facilities the number of prevalent fistula needed to meet fistula percentage goals based on the total number of patients and the number of patients with a fistula in their facility. It displays graphs illustrating quarterly results, as well as progress over time compared to the state, Network and United States where
 so that facilities can use this report to compare themselves to other facilities of like size regarding")
 to identify patients suitable for")
5 applicable. It also graphs same population size facilities to each other in their Health Service Area (HSA) so that facilities can use this report to compare themselves to other facilities of like size regarding AV fistula rates in their area. This report provides the dialysis facilities with a tool which can be used in conjunction with other facility methods of continuous quality improvement (CQI) to identify patients suitable for conversion to a fistula. The FF data report is sent to facility medical directors, administrators, and nurse managers quarterly. These data also enable the Network to target facilities with poor outcomes for intervention. Facilities with good outcomes are utilized for positive intervention and mentoring. Communications. Stakeholders were identified as the facility medical director, administrator, nurse manager, vascular access coordinators, nephrologists, patients, vascular access surgeons, and interventional radiologists. Individual databases are continually updated and maintained to enable ongoing communications with these audiences. Information and educational materials regarding the Fistula First Initiative were sent to the various stakeholders by mail and as appropriate and necessary.
6 January QIP participant conference calls were held. Thirty-one facilities that had made quarterly interim goals were highlighted on these conference calls. Representatives from these facilities reported, providing details on their successful techniques for improvement. All facilities that attended were given the opportunity to ask questions regarding any aspect of the QIP or other challenges. January 12 & 14, A WebEx entitled QAPI & Vascular Access Management II consisted of two best practice programs describing fistula improvements based on a sound QAPI program. 159 participants representing 148 facilities attended these WebEx conferences. February 3, An announcement was ed to facility Vascular Access Coordinators (VACs) regarding the Bruit Audio educational sound bites available for patient and staff education on FFBI Web site. By listing to these sound bites the staff member can actually hear the sound of a good bruit and a bad bruit. February 9, An announcement was ed to facility medical directors, nurse managers, and VACs regarding the development of an AVF Assessment and Cannulation Resources area on the Network Web site. This Web page provides tools, training guides, protocols, master cannulator information, and PowerPoint slides to be used for staff education and training. February 11, A Medical Director/Surgeon as Partners WebEx was held. A total of 74 attended the WebEx (36 of these were surgeons or nephrologists and 38 were nurses/vacs). 66 facilities were represented and there have been 26 requests for the WebEx on CD. February 15, An announcement was ed to facility medical directors, nurse managers, and VACs regarding the development of a Successful QAPI for Vascular Access Management Resources area on the Network Web site. This Web page provides tools, protocols, and algorithms to be used to improve QAPI processes. February 16, 18, & QIP participant WebEx conference calls were held. Discussion focused on vascular access management and QAPI. Additionally, Network staff highlighted performance issues and best practice discovered during Network site visits and conference calls. February 26, Mailed a Surgical Quality Report to facility medical directors and VACs. This report displays a facility yearly fistula rate compared to region, state, Network, and US to be used to communicate to surgeon partners. March 9, A WebEx entitled Hospital Systems Change was held for representatives of hospital-based facilities. This WebEx highlighted the new Hospital Systems Change Concept developed by FFBI and two best practice
7 approaches to improving processes for placing fistulas before leaving the hospital. Attendees included 70 medical directors, 64 administrators, and 47 nurse managers. April Root Cause Analysis (RCA) QIP participant conference calls for Network 9 were held. The presentation surrounded conducting a root cause analysis and developing an action plan. All facilities that attended were given the opportunity to ask questions regarding any aspect of the QIP, the QAPI process, or other challenges. April 9, An announcement was ed to facility medical directors and VACs regarding a one page Patient Educational Vascular Access Flyer available for patient and staff education. The flyer is housed on the FFBI Web site and describes the advantages and disadvantages to all three vascular access choices. April 20 & 21, A Cannulation WebEx was held. A total of 189 participants attended the WebEx representing 144 facilities. May An announcement was ed to facility medical directors, nurse managers, VACs, nurse practitioners, and surgeons regarding the NN&I Vascular Access Management in the US Current Challenges & Potential for Improvement webinar that was held May 19, The Executive Director, Assistant Director, QID and QICs from Network staff attended this webinar. We also provided the link to the recording to above medical professionals, following the webinar. July 12, Letters were sent to identified facility medical directors informing them of their progress toward fistula goal and that they would be participating in the Promising Stars focus group. The letter reinforced the yearly goal of a four percentage point increase to be realized by March 31, August 18, An announcement was ed to facility medical directors, nurse managers/administrators, VACs, surgeons, and nurse practitioners regarding a CKD Webinar on Vascular Access Management Prior to Dialysis, sponsored by ESRD Network 7. The Network QID and QIC along with 21 participants from Network 9/10 representing 13 facilities attended this Webinar on August 19, August 24, A QAPI Vascular Access Best Practice WebEx was held. A total of 174 participants attended the WebEx representing 168 facilities. August 26, A QAPI Medical Director in Charge WebEx was held. A total of 51 participants attended the WebEx representing 48 facilities. September 7, An announcement was ed to facility medical directors, VACs, and surgeons regarding an FFBI Surgeon workshop to be held November 12, 2010 in Chicago, IL.
8 September 13, An announcement was ed to facility medical directors, nurse managers/administrators, and VACs regarding the release of the FFBI/NKDEP Vascular Access Provider videos. September 13, An announcement was ed to facility medical directors, nurse managers/administrators, and VACs regarding the release of two new FFBI tools added to Change Concept 9: a) Assessment and Monitoring of the Newly Placed AVF for Maturation and b) The Detection of Access Dysfunction in Permanent Vascular Access. September 16, The 3Ps for Vascular Access Management Handbook was mailed to facility nurse managers. The handbook houses best practices, tools and resources to be used by facilities in vascular access management and QAPI. Facility interdisciplinary teams were instructed to review the handbook at the next monthly QAPI vascular access management meeting and consider utilizing one or more tools/best practices that have been made available. September 27 & 30, The 3Ps for Vascular Access Management Handbook WebEx was held. A total of 232 participants attended the WebExes. The WebEx introduced the handbook, discussed principles of QAPI, and presented examples of how the facility interdisciplinary teams could utilize the handbook. September 24, A Vascular Access Learning Session was held in Chicago, IL. Topics included bundled payment, catheter reduction, placing and using fistula, and preserving fistula. There were 113 participants at the learning session representing 66 facilities. October 1 & 2, The Network Executive Director, Quality Improvement Director, and Quality Improvement Coordinator attended the Cincinnati Vascular Access Symposium. A total of 88 participants, representing 17 facilities, attended this symposium which satisfied their QIP learning session attendance requirement. November 4, A Fistula Placement and Assessment Intervention WebEx was held. Topics included progress toward goal, continued expectations, and QAPI principles. 19 facilities from Network 9 and 9 facilities from Network 10 attended the WebEx. An was sent to the facility nurse managers and medical directors providing a link to access the WebEx recording. 28 of the facilities from Network 9 and 4 of the facilities from Network 10 viewed the recording. The WebEx slides are on the Web site. November 4, A Vascular Access Learning Session was held in Philadelphia, PA. Network 9/10 facilities were invited to attend to satisfy their QIP learning session attendance requirement. There were five participants, representing five facilities from Network 9/10, in attendance at this learning session. Topics
9 included bundled payment, catheter reduction, placing and using fistula, and preserving fistula. November 12, An FFBI Surgeon workshop was held in Chicago, IL. Fourteen surgeons from the Network 10 area and 10 surgeons from the Network 9 area attended the workshop. Physician specific incident CKD patient vascular access data reports were sent to nephrologists in July 2010 (January 2, 2010 June 30, 2010 incident data) and February 2011 (July 1, 2010 December 31, 2010 incident data). The information provided on this report is generated from the CMS 2728 Medical Evidence and Medicare Entitlement form and displays the percent of accesses a nephrologist s patients were using when they began ESRD. The AVF Monthly Tracking Report was sent to facility VACs and medical directors every month. This report displays the facility prevalent fistula rate and shows their interim outcomes toward the final goal. Facility Vascular Access Coordinators (VAC) were sent bi-monthly electronic newsletters listing vascular access management and QAPI resources and tools. Each newsletter had a different theme/topic presented. Medical director letters were sent in February, June, July, and November 2010 providing information on vascular access interim outcomes, reminding of the goal, and stressing the importance of improving processes. To promote Fistula First goals continuously, educational resources have been developed which can be easily shared. The Fistula First page on the Network Web site was updated regularly adding the above mentioned materials as they were provided by mail or . The materials provided to our stakeholders were developed both from Networks 9/10 and the national Fistula First Breakthrough Initiative. The Network has acted as a community outreach partner by providing information on Fistula First through conference calls quarterly to state surveyor groups and the quality improvement organizations. Conference Calls, Site Visits, and Presentations. Network staff conducted many individual facility conference calls and site visits in MRB members and the CMS Regional Project Officer assisted in some of the conference calls. Staff also partnered with LDOs to present at physician meetings and quality meetings. January 19 February 1, Fourteen facility site visits were conducted in this time frame. Facilities that were visited were selected based on poor vascular access outcomes (<40% prevalent fistula/>50 patients). A packet of best practice tools was given to each facility. Facility staff and Network staff
10 discussed processes and barriers. Network staff gave suggestions to making improvements. February 2, The Quality Improvement Director was invited by FMCs Vice President of Quality Improvement to present to 59 FMC facility nurse managers in the Chicagoland area. The presentation focused on the role of the ESRD Network and expectations regarding vascular access management. Other presentations were regarding FMCs catheter reduction initiative and management and surveillance of vascular access. February 3 10, Four facility conference calls with the MRB chair and Network staff were conducted in this time frame. Facilities called were selected due to poor vascular access outcomes (<40% prevalent fistula/>50 patients). A packet of best practice tools was sent to each facility. These facilities were required to submit action plans and QAPI meeting minutes for review by the Network QI staff. During the telephone calls, facility staff and Network staff discussed processes and barriers to fistula placement. The Network staff and MRB chair provided suggestions for making improvements. February 23 March 2, Three facility conference calls with an MRB representative, Network staff, and the CMS Project Officer (PO) were conducted in this timeframe. Facilities called were selected based on poor participation in the QIP. These facilities were not sending action plans/qapi minutes and not attending required educational meetings and WebEx conferences. Action plans/qapi meeting minutes were received and reviewed by Network staff and the MRB representative. Facility staff and Network staff discussed processes and barriers. Network staff and the MRB representative gave suggestions to making improvements. The CMS PO stressed importance of participating in Network initiatives as outlined in the Conditions for Coverage. April 7, One facility conference call with a MRB representative, Network staff, and the CMS PO was conducted. The facility that was called was selected based on poor participation in the QIP. This facility was not sending action plans/qapi minutes and not attending required educational meetings and WebEx conferences. Prior to the call, the missing action plans/qapi meeting minutes were received and reviewed by Network staff and the MRB representative. Facility staff and Network staff discussed processes and barriers. Network staff and the MRB representative gave suggestions to making improvements. The CMS PO stressed importance of participating in Network initiatives as outlined in the Conditions for Coverage. May 18, The Executive Director was invited by the FMC Chief Medical Officer to present to a Chicago Nephrology Group Practice. Discussion
11 surrounded Fistula First data, Medical Director responsibilities, and overcoming barriers to fistula placement. A total of 66 nephrologists were present at this meeting. June 2 24, Ten facility site visits were conducted in this timeframe. Facilities visited were selected based on poor vascular access outcomes (<40% prevalent fistula/>35 patients). A packet of best practice tools was given to each facility. Facility staff and Network staff discussed processes and barriers. Network staff gave suggestions to making improvements. June 8, The Quality Improvement Director presented fistula improvement data and QAPI best practices at the annual Network 9/10 Pediatric Renal Group meeting. A total of 31 participants were in attendance, representing 14 pediatric centers. June 11 29, The Network staff conducted 14 facility conference calls in this timeframe. Facilities called were selected due to poor vascular access outcomes (<40% prevalent fistula/>35 patients). A packet of best practice tools was sent to each facility. These facilities were required to submit action plans and QAPI meeting minutes for review by the Network QI staff. During the telephone calls, facility staff and Network staff discussed processes and barriers to fistula placement. The Network staff provided suggestions for making improvements. June 22, The Quality Improvement Director and Quality Improvement Coordinator were invited by the FMC Vice President of Quality Improvement to present to 18 FMC facility nurse managers in the Chicagoland area. The presentation focused on the upcoming vascular access management QIPs and the QAPI process. Other presentations were given by the FMC facilities in the LDO catheter reduction initiative, surgical techniques, and a surgeon s perspective. June 29, The Executive Director was invited by the FMC Chief Medical Officer to present to several Central Indiana nephrology group practices. Discussion surrounded Fistula First data, Medical director responsibilities, and overcoming barriers to fistula placement; 40 nephrologists were present at this meeting. July 1 8, Three facility site visits were conducted in this timeframe. Facilities visited were selected based on poor vascular access outcomes (<40% prevalent fistula/>35 patients). A packet of best practice tools was given to each facility. Facility staff and Network staff discussed processes and barriers. Network staff gave suggestions to making improvements.
12 September 3-27, The Network staff conducted 12 facility conference calls in this timeframe. Facilities called were selected due to poor vascular access outcomes (<40% prevalent fistula/>35 patients). A packet of best practice tools was sent to each facility. During the telephone calls, facility staff and Network staff discussed processes and barriers to fistula placement. The Network staff provided suggestions for making improvements. September 7 29, Twenty-two facility site visits were conducted in this timeframe. Facilities visited were selected based on poor vascular access outcomes (<40% prevalent fistula/>35 patients). A packet of best practice tools was given to each facility. Facility staff and Network staff discussed processes and barriers. Network staff gave suggestions to making improvements. November 3, An Ohio Summit was held in Columbus, OH. The Network Executive Director partnered with FMC management to present medical director responsibilities regarding vascular access management and AV fistula improvement to FMC facility medical directors. December 7 17, Letters were sent to 13 medical directors on November 29, 2010 informing them they were expected to be on a conference call with an MRB representative in December Facilities called were selected based on poor vascular access outcomes (<40% prevalent fistula/>35 patients). Network staff also requested new action plans with updated actions due to poor outcomes Fistula First Completed Projects The following activities were designed as components of the Fistula First quality improvement project and were completed in March Decreasing Catheters - 51 dialysis facilities in Network 9 and 28 dialysis facilities in Network 10 with high catheter rates and low AV fistula rates participated in an initiative designed to decrease catheters. This project was part of the Quality Improvement Work Plan (QIWP) for the Fistula First initiative. In July 2009 facilities were asked to complete a root cause analysis identifying the reasons for a high catheter rate: a) High percentage of new patients starting with catheter only b) High percentage of catheter only >90 days c) High percentage of catheters with maturing AVF (AVF utilization/maintenance) OR
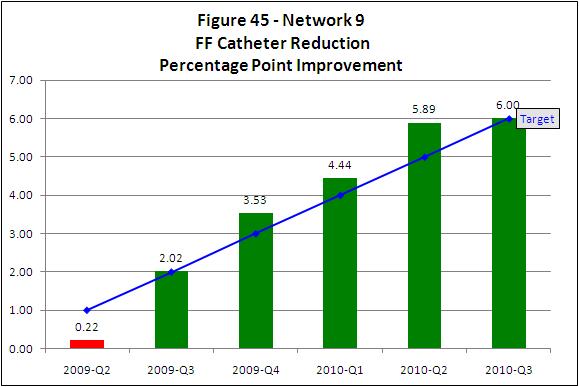
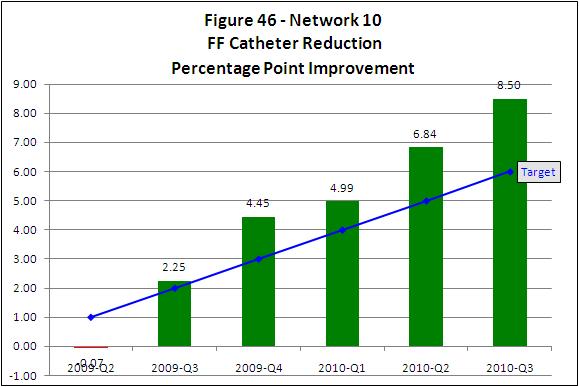
13 d) other reason that is identified The facilities were advised to initiate a process change that would address the barriers to decreased catheters/increased fistula in their facility. Network staff provided specific tools and resources to assist in process change and plan development. The project was conducted over a seven month period with monthly activities that included: Intervention-specific conference calls for participant networking and technical assistance from Network staff Evaluation of facilities monthly prevalent fistula rate increase (goal 0.33 percentage point/month) and reports to facilities Evaluation of project progress through the assessment of the facility vascular access management QAPI minutes Additionally, the following educational activities were included as part of the interventions: Month 2 -Facilities attend QAPI and Vascular Access Management I WebEx Month 3 - Facilities attend Networking for Solutions Learning Session Month 5 - Facilities attend QAPI and Vascular Access Management II WebEx Goals and timeline for the Decreasing Catheters project were: To increase by 1 percentage point each quarter to attain a four percentage point increase by March Results: The Decrease Catheter project was successful in both Networks 9 and 10. Both Networks met the goal that was set for March 2010 and continued to improve at the quarterly rate or better through September Figure 45 and Figure 46 display the results of this project at the end of the project, March 2010 and for six months after (September 2010) for Network 9 and Network 10.
14
15 2. Changing Patient Culture - 16 dialysis facilities in Network 9 and 12 dialysis facilities in Network 10 were identified as having a patient culture that contributed to low AV fistula rates. Their barriers were identified as patient refusal due to poor staff/patient communication skills, patient lack of knowledge, and/or facility culture. They participated in an initiative designed to improve patient/staff communications and patient culture. This project was part of the Quality Improvement Work Plan (QIWP) for the Fistula First initiative. The Network developed and provided two products for use by the participating facilities: a) Helping Patients Make Healthy Fistula Choices is a program designed to educate staff on techniques to help identify a patient s readiness to have a fistula placed or used and techniques in listening and empathy. Utilizing this teaching module will assist staff in discussing best care options with the patients. It will also identify patient fears and patient barriers to fistula placement and usage in order to assist staff in addressing those issues. b) The Fistula Coaching Program is designed to promote the best vascular access choice among patients through peer-to-peer education, communication, planning and problem solving. The program is provided through a trained, facility-based, patient volunteer program. Utilizing this teaching module will identify a patient champion that will be able to have a dialogue with the patient opposed to a fistula to help that patient make a best care decision. The project was conducted over a seven month period with monthly activities that included: Intervention-specific conference calls for participant networking and technical assistance from Network staff Evaluation of facilities monthly prevalent fistula rate increase (goal 0.33 percentage point/month) and reports to facilities Evaluation of project progress through the assessment of the facility vascular access management QAPI minutes Additionally, the following educational activities were included as part of the interventions: Month 2 -Facilities attend QAPI and Vascular Access Management I WebEx Month 3 - Facilities attend Networking for Solutions Learning Session Month 5 - Facilities attend QAPI and Vascular Access Management II WebEx

16 Goals and timeline for the Decreasing Catheters project were: To increase by 1 percentage point each quarter to attain a four percentage point increase by March Results: The Changing Patient Culture project was successful in both Networks 9 and 10. Both Networks met the goal that was set for March 2010 and continued to improve through September Figure 47 and Figure 48 display the results of this project at the end of the project, March 2010 and for six months after (September 2010) for Network 9 and Network 10.

17 3. Community Partnerships - 18 dialysis facilities in Network 9 and 12 dialysis facilities in Network 10 were identified as having a lack of communication between dialysis facility staff and surgeons and hospitals. This lack of communication contributed to low AV fistula rates. They participated in an initiative designed to improve communications with their identified key partners. This project was part of the Quality Improvement Work Plan (QIWP) for the Fistula First initiative. Facility staff completed a root cause analysis identifying the external ESRD stakeholder(s) who were hindering fistula rate improvements which could include: a. Vascular surgeon(s) b. Nephrology office staff c. Primary care physician d. Hospital discharge planner e. Acute dialysis staff f. Other identified stakeholder The facility staff developed plans to build a mutually rewarding relationship with their identified stakeholders. Network staff suggested techniques to begin the partnering process and provided specific tools and resources to assist in the project.
18 The project was conducted over a seven month period with monthly activities that included: Intervention-specific conference calls for participant networking and technical assistance from Network staff Evaluation of facilities monthly prevalent fistula rate increase (goal 0.33 percentage point) and reports to facilities Evaluation of project progress through the assessment of the facility vascular access management QAPI minutes Additionally, each intervention included the following educational activities: Month 2 -Facilities attend QAPI and Vascular Access Management I WebEx Month 3 - Facilities attend Networking for Solutions Learning Session Month 5 - Facilities attend QAPI and Vascular Access Management II WebEx Goals and timeline for the Community Partnerships project were: To increase by 1 percentage point each quarter to attain a four percentage point increase by March Results: The Community Partnerships project was successful in Network 10 but fell short in Network 9. Network 10 met the goal that was set for March 2010 and continued to improve through September Network 9 improved but not at the quarterly rate that was set as goal. Figure 49 and Figure 50 display the results of this project at the end of the project, March 2010 and for six months after (September 2010) for Network 9 and Network 10.
 - Because CMS imposed a")

19 Performance Improvement Plan (PIP) - Because CMS imposed a performance improvement plan (PIP) for failure to achieve 2009 vascular access goals,
20 the MRB worked during the second and third quarter of 2009 to strengthen quality improvement projects for improving fistula rates. Poor performers originally classified as a comparison group and not in a specific QIP were targeted for stronger intervention through Root Cause Analysis (RCA). A fourth QIP based on RCA was added in November 2009 to the QIWP. Network 9 had 61 newly targeted facilities and Network 10 had 18 newly targeted facilities in this RCA group. Facility staff was given an RCA tool designed to analyze their vascular access data and determine the cause of poor vascular access outcomes in their facility. They submitted the completed RCA tools to the Network for review and comment during November and December These facilities participated in the same interventions as the participants of the three original QIPs: Intervention-specific conference calls for participant networking and technical assistance from Network staff Evaluation of facilities monthly prevalent fistula rate increase (goal 0.33 percentage point) and reports to facilities Evaluation of project progress through the assessment of the facility vascular access management QAPI minutes This intervention also included the following educational activities: Facilities attend Networking for Solutions Learning Session Facilities attend QAPI and Vascular Access Management II WebEx The addition of the RCA facilities increased QIP participation numbers. Participating facilities increased in October 2009 to 216 or approximately 38% of all the facilities in Network 9/10. Goals and timeline for the RCA project were: To increase by 1 percentage point each quarter to attain a four percentage point increase by March However, this group began the RCA process in November Results: The RCA project was successful in Network 10 but fell short in Network 9. Network 10 met the goal that was set for March 2010 and continued to improve through September Even though Network 9 was unsuccessful in reaching the goal set for March 2010 it improved by 1 percentage point each quarter since the project start in November 2009 and continued to improve at the quarterly rate or better through September 2010.
21 Figure 51 and Figure 52 display the results of this project at the end of the project, March 2010 and for six months after (September 2010) for Network 9 and Network 10.
22 The PIP was closed for Network 10 in January 2010 because it was projected that the March 2010 goal would be achieved and it was in December The PIP was closed for Network 9 in October 2010 because we provided comprehensive monthly updates regarding the FF initiatives to CMS, the Network 9 AV fistula rate met the March 2010 goal in May 2010, and was well ahead of interim measures for the March 2011 goal. 5. Fistula First Quality Award: In 2005, The Renal Network established an award designed to recognize leaders of the Fistula First Initiative and provide them with a platform from which they can share their knowledge as mentors to other dialysis providers. Application for this award is voluntary and is viewed as a way for any group or individual to be recognized by providing performance processes and results in the area of placement and usage of AVF. The goal of this award is to demonstrate performance outcomes above standards in the area of promoting AV fistula and vascular access management related to the FF Initiative. The award criteria were developed using the 11 Change Concepts of the CMS National Fistula First Initiative along with the K-DOQI guidelines. Fistula First 11 Change Concepts 1. Routine CQI review of vascular access. 2. Timely referral to nephrologist 3. Early referral to surgeon for AVF only evaluation and timely placement. 4. Surgeon selection based on best outcomes, willingness, and ability to provide access services. 5. Full range of appropriate surgical approaches to AVF evaluation and placement. 6. Secondary AVF placement in patients with AV grafts. 7. AVF placement in patients with catheters where indicated. 8. Cannulation training for AV fistulas. 9. Monitoring and maintenance to ensure adequate access function. 10. Education for care givers and patients. 11. Outcomes feedback to guide practice. This performance award is defined by criteria that demonstrate rapid, sustainable improvement defined by a time-specific aim, and quantitative measures to display improvement and identification of process changes that lead to project advancement. Winners are selected based on a voluntary application that describes their processes to
23 place and maintain fistula and decrease catheters, as well as program outcomes. Winners are announced at the annual meeting of the Network Council and are used as mentors for educational activities. In 2008, in memory of Dr. Richard Breitenfield, a quality champion in Network 9, the title of the award was changed to the Dr. Richard Breitenfield Quality Award. In 2010 facilities could apply and be considered for this award if they had a prevalent AV fistula rate of 66% or higher. Eight facilities filed applications for the 2010 Dr. Richard Breitenfield Quality Award. A volunteer panel consisting of members of the MRB and VAAP reviewed the applications. Four of the award applicants had outcomes greater than their Network prevalent fistula rate and had put processes into place that helped them achieve superior results. All four award winners could extensively describe each process that assisted in their great outcomes.
24
D. Fistula First (FF) Initiative.
 Initiative.") D. Fistula First (FF) Initiative. The development of Quality Improvement Projects (QIP) is mandated in the ESRD Network contracts with CMS. The QIPs are developed and directed by the MRB, then reviewed,
D. Fistula First (FF) Initiative. The development of Quality Improvement Projects (QIP) is mandated in the ESRD Network contracts with CMS. The QIPs are developed and directed by the MRB, then reviewed,
FISTULA FIRST: PAST, PRESENT AND FUTURE. Jay Wish, MD Nephrology Clinical Consultant Fistula First Breakthrough Initiative
 FISTULA FIRST: PAST, PRESENT AND FUTURE Jay Wish, MD Nephrology Clinical Consultant Fistula First Breakthrough Initiative Jay Wish, MD: Disclosures No disclosures with regard to this presentation Wear
FISTULA FIRST: PAST, PRESENT AND FUTURE Jay Wish, MD Nephrology Clinical Consultant Fistula First Breakthrough Initiative Jay Wish, MD: Disclosures No disclosures with regard to this presentation Wear
E. Network Special Projects/Studies
 E. Network Special Projects/Studies Projects completed during 2010 included the following activities. 2009-2010 Anemia Management QIP The following activities were designed as components of the quality
E. Network Special Projects/Studies Projects completed during 2010 included the following activities. 2009-2010 Anemia Management QIP The following activities were designed as components of the quality
ESRD National Coordinating Center (NCC) Fistula First Catheter Last Learning and Action Network. October 22, 2015
 Fistula First Catheter Last Learning and Action Network. October 22, 2015") ESRD National Coordinating Center (NCC) Fistula First Catheter Last Learning and Action Network October 22, 2015 Objectives for Today The participants will be able to: 1. List 3 of the 6 components of
ESRD National Coordinating Center (NCC) Fistula First Catheter Last Learning and Action Network October 22, 2015 Objectives for Today The participants will be able to: 1. List 3 of the 6 components of
AIM 2: BETTER HEALTH FOR THE ESRD POPULATION
 AIM 2: BETTER HEALTH FOR THE ESRD POPULATION The Population Health Innovation Pilot Project: Promote Appropriate Home Dialysis in Qualified Beneficiaries The 2013 redesign of the ESRD Network Program came
AIM 2: BETTER HEALTH FOR THE ESRD POPULATION The Population Health Innovation Pilot Project: Promote Appropriate Home Dialysis in Qualified Beneficiaries The 2013 redesign of the ESRD Network Program came
IPRO ESRD Network of the South Atlantic HAI BSI/LTC QIA 2018 Kickoff Webinar
 IPRO ESRD Network of the South Atlantic HAI BSI/LTC QIA 2018 Kickoff Webinar February 7, 2018 Welcome/Opening Remarks Jeanine Pilgrim, Quality Improvement Director Housekeeping Reminders All phone lines
IPRO ESRD Network of the South Atlantic HAI BSI/LTC QIA 2018 Kickoff Webinar February 7, 2018 Welcome/Opening Remarks Jeanine Pilgrim, Quality Improvement Director Housekeeping Reminders All phone lines
2018 Increase Rate of Patients Dialyzing at Home Using the 7-Step Process Quality Improvement Activity (QIA)
") 2018 Increase Rate of Patients Dialyzing at Home Using the 7-Step Process Quality Improvement Activity (QIA) Donna DeBello, RN Quality Improvement Director Health Services Advisory Group (HSAG): End Stage
2018 Increase Rate of Patients Dialyzing at Home Using the 7-Step Process Quality Improvement Activity (QIA) Donna DeBello, RN Quality Improvement Director Health Services Advisory Group (HSAG): End Stage
Vascular Access Best Practice Sharing Stories
 Welcome to our Webinar: Presenters: Cindy Miller, RN - The Renal Network Raynel Wilson, RN - The Renal Network Vascular Access Best Practice Sharing Stories Shane Perry - The Renal Network Sue Kirschbaum,
Welcome to our Webinar: Presenters: Cindy Miller, RN - The Renal Network Raynel Wilson, RN - The Renal Network Vascular Access Best Practice Sharing Stories Shane Perry - The Renal Network Sue Kirschbaum,
Vascular Access Planning Strategies to Reduce LTC Rates. May 3, 2018
 Vascular Access Planning Strategies to Reduce LTC Rates May 3, 2018 1 Welcome/Opening Remarks Jeanine Pilgrim, Quality Improvement Director IPRO ESRD Network Program Housekeeping Reminders All phone lines
Vascular Access Planning Strategies to Reduce LTC Rates May 3, 2018 1 Welcome/Opening Remarks Jeanine Pilgrim, Quality Improvement Director IPRO ESRD Network Program Housekeeping Reminders All phone lines
How To Make A Good Vascular Access Program Even Better. Thursday, April 14, Welcome to our Webinar: Presenters: Cindy Miller, RN
 Presenters: Cindy Miller, RN - The Renal Network Raynel Wilson, RN -The Renal Network -Julie Guss, RN -FMC Heart of Ohio Welcome to our Webinar: How To Make A Good Vascular Access Program Even Better -Heidi
Presenters: Cindy Miller, RN - The Renal Network Raynel Wilson, RN -The Renal Network -Julie Guss, RN -FMC Heart of Ohio Welcome to our Webinar: How To Make A Good Vascular Access Program Even Better -Heidi
Quality Assessment & Performance. CMS Conditions for Coverage
 Quality Assessment & Performance Improvement Meeting Condition 494.110 Of CMS Conditions for Coverage Raynel Kinney, RN,CNN,CPHQ QI Director Mary Ann Webb, RN, MSN, CNN QI Coordinator Cindy Miller, RN,
Quality Assessment & Performance Improvement Meeting Condition 494.110 Of CMS Conditions for Coverage Raynel Kinney, RN,CNN,CPHQ QI Director Mary Ann Webb, RN, MSN, CNN QI Coordinator Cindy Miller, RN,
IPRO ESRD Network of New York HAI BSI/LTC QIA 2018 Kickoff Webinar
 IPRO ESRD Network of New York HAI BSI/LTC QIA 2018 Kickoff Webinar February 6, 2018 Welcome/Opening Remarks Jeanine Pilgrim, Quality Improvement Director Meet the NW2 Quality Improvement Team Improving
IPRO ESRD Network of New York HAI BSI/LTC QIA 2018 Kickoff Webinar February 6, 2018 Welcome/Opening Remarks Jeanine Pilgrim, Quality Improvement Director Meet the NW2 Quality Improvement Team Improving
Introduction BSI Prevention QIA Toolkit
 Introduction BSI Prevention QIA Toolkit In support of the Centers for Medicare & Medicaid Services (CMS ) reduction in healthcare-associated infections (HAIs) initiatives, HSAG: ESRD Network 17 (the Network)
Introduction BSI Prevention QIA Toolkit In support of the Centers for Medicare & Medicaid Services (CMS ) reduction in healthcare-associated infections (HAIs) initiatives, HSAG: ESRD Network 17 (the Network)
Welcome to the IPRO ESRD Network of New York Home Therapies QIA 2018 Kickoff Webinar. The webinar will begin momentarily!
 Welcome to the IPRO ESRD Network of New York Home Therapies QIA 2018 Kickoff Webinar The webinar will begin momentarily! IPRO ESRD Network of New York Home Therapies QIA 2018 Kickoff Webinar January 30,
Welcome to the IPRO ESRD Network of New York Home Therapies QIA 2018 Kickoff Webinar The webinar will begin momentarily! IPRO ESRD Network of New York Home Therapies QIA 2018 Kickoff Webinar January 30,
Fistula First vs. Catheter Last. Lynda K. Ball, MSN, RN, CNN March 17, 2016
 Fistula First vs. Catheter Last Lynda K. Ball, MSN, RN, CNN March 17, 2016 National Vascular Access Improvement Initiative Better known as NVAII, sponsored by the Centers for Medicare & Medicaid Services
Fistula First vs. Catheter Last Lynda K. Ball, MSN, RN, CNN March 17, 2016 National Vascular Access Improvement Initiative Better known as NVAII, sponsored by the Centers for Medicare & Medicaid Services
Network 15 Reducing Bloodstream Infections (BSIs) Quality Improvement Activity (QIA) for 2018 Orientation
 Quality Improvement Activity (QIA) for 2018 Orientation") Network 15 Reducing Bloodstream Infections (BSIs) Quality Improvement Activity (QIA) for 2018 Orientation Susan Moretti, BSN, RN Quality Improvement Nephrology Nurse Health Services Advisory Group (HSAG):
Network 15 Reducing Bloodstream Infections (BSIs) Quality Improvement Activity (QIA) for 2018 Orientation Susan Moretti, BSN, RN Quality Improvement Nephrology Nurse Health Services Advisory Group (HSAG):
Catheter Reduction Toolkit Developed by the Forum of ESRD Networks Medical Advisory Council (MAC)
") 2009 [CATHETER REDUCTION TOOLKIT] June 1, 2009 I Catheter Reduction Toolkit Developed by the Forum of ESRD Networks Medical Advisory Council (MAC) The Forum MAC has developed a series of QAPI toolkits
2009 [CATHETER REDUCTION TOOLKIT] June 1, 2009 I Catheter Reduction Toolkit Developed by the Forum of ESRD Networks Medical Advisory Council (MAC) The Forum MAC has developed a series of QAPI toolkits
ESRD Network 17. Annual Report January 1, 2014 through December 31, Contract Number: HHSM NW017C
 ESRD Network 17 Annual Report 2014 January 1, 2014 through December 31, 2014 Contract Number: HHSM-500-2013-NW017C Presented to: Centers for Medicare & Medicaid Services The mission of Western Pacific
ESRD Network 17 Annual Report 2014 January 1, 2014 through December 31, 2014 Contract Number: HHSM-500-2013-NW017C Presented to: Centers for Medicare & Medicaid Services The mission of Western Pacific
Safety in Transitions from CKD to Dialysis. Lana Spencer, BScM, RN, CDN, MBA Corporate Administrator, Dialysis Clinic, Inc.
 Safety in Transitions from CKD to Dialysis Lana Spencer, BScM, RN, CDN, MBA Corporate Administrator, Dialysis Clinic, Inc. A renal community collaboration September 11-12, 2012 Transitions from CKD to
Safety in Transitions from CKD to Dialysis Lana Spencer, BScM, RN, CDN, MBA Corporate Administrator, Dialysis Clinic, Inc. A renal community collaboration September 11-12, 2012 Transitions from CKD to
Welcome to the IPRO ESRD Network of the South Atlantic 2018 Home Dialysis QIA Kick-off Webinar. The webinar will begin at 2:00PM EST
 Welcome to the IPRO ESRD Network of the South Atlantic 2018 Home Dialysis QIA Kick-off Webinar The webinar will begin at 2:00PM EST January 31, 2018 IPRO ESRD Network of the South Atlantic 2018 Home Dialysis
Welcome to the IPRO ESRD Network of the South Atlantic 2018 Home Dialysis QIA Kick-off Webinar The webinar will begin at 2:00PM EST January 31, 2018 IPRO ESRD Network of the South Atlantic 2018 Home Dialysis
Vascular Access Planning Guide for Professionals
 Vascular Access Planning Guide for Professionals www.esrdncc.org Contents Introduction...3 Step 1: Develop Vascular Access Plan...6 Step 2: Refer for Vessel Mapping...8 Step 3: Coordinate the Surgeon Appointment...11
Vascular Access Planning Guide for Professionals www.esrdncc.org Contents Introduction...3 Step 1: Develop Vascular Access Plan...6 Step 2: Refer for Vessel Mapping...8 Step 3: Coordinate the Surgeon Appointment...11
KCER Patient SME Guide
 KCER Patient SME Guide An Introduction to Being a National Kidney Community Emergency Response (KCER) Patient and Family Engagement Learning and Action Network (N-K-PFE-LAN) Patient Subject Matter Expert
KCER Patient SME Guide An Introduction to Being a National Kidney Community Emergency Response (KCER) Patient and Family Engagement Learning and Action Network (N-K-PFE-LAN) Patient Subject Matter Expert
HOME DIALYSIS REIMBURSEMENT AND POLICY. Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation
 HOME DIALYSIS REIMBURSEMENT AND POLICY Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation Objectives Understand the changing dynamics of use of home dialysis Know the different
HOME DIALYSIS REIMBURSEMENT AND POLICY Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation Objectives Understand the changing dynamics of use of home dialysis Know the different
Renal. Outreach. Living with Renal Failure. by Della Major. Summer 2013
 LIVING WITH RENAL FAILURE PAGE 1. 5 DIAMOND PROGRAM PAGE 2 QUALITY OF LIFE PAGE 5 Renal Summer 2013 Outreach Living with Renal Failure by Della Major I t all started in 2005, when I was told that I had
LIVING WITH RENAL FAILURE PAGE 1. 5 DIAMOND PROGRAM PAGE 2 QUALITY OF LIFE PAGE 5 Renal Summer 2013 Outreach Living with Renal Failure by Della Major I t all started in 2005, when I was told that I had
Healthcare-Associated Infections (HAI) Quality Improvement Activity February Webinar
 Quality Improvement Activity February Webinar") Healthcare-Associated Infections (HAI) Quality Improvement Activity 2017 February Webinar AIM : Better Care for the Individual through Patient and Family Centered Care Patient Safety: Healthcare-associated
Healthcare-Associated Infections (HAI) Quality Improvement Activity 2017 February Webinar AIM : Better Care for the Individual through Patient and Family Centered Care Patient Safety: Healthcare-associated
IPRO ESRD Network of New York Transplant Coordination QIA 2018 Kickoff Webinar
 IPRO ESRD Network of New York Transplant Coordination QIA 2018 Kickoff Webinar January 25, 2018 Welcome/Opening Remarks Jeanine Pilgrim, Quality Improvement Director Meet the NW2 Quality Improvement Team
IPRO ESRD Network of New York Transplant Coordination QIA 2018 Kickoff Webinar January 25, 2018 Welcome/Opening Remarks Jeanine Pilgrim, Quality Improvement Director Meet the NW2 Quality Improvement Team
SERVICE SPECIFICATION 2 Vascular Access
 SERVICE SPECIFICATION 2 Vascular Access Table of Contents Page 1 Key Messages 1 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies with other specialties
SERVICE SPECIFICATION 2 Vascular Access Table of Contents Page 1 Key Messages 1 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies with other specialties
Executive Summary Heartland Kidney Network Annual Report
 2010 Annual Report End-Stage Renal Disease (ESRD) Network 12, Network Coordinating Council, Inc. DBA: Heartland Kidney Network CMS Contract Number: HHSM-500-2010-NW012C 7306 NW Tiffany Springs Pkwy, Suite
2010 Annual Report End-Stage Renal Disease (ESRD) Network 12, Network Coordinating Council, Inc. DBA: Heartland Kidney Network CMS Contract Number: HHSM-500-2010-NW012C 7306 NW Tiffany Springs Pkwy, Suite
For Dialysis Facilities
 The QIP Newsletter For Dialysis Facilities Inside this issue: What does the QIP 2 Measure? What has Changed? 3 QIP Measures 3 Clinical measure 3-5 focus Measures that 6-7 Matter Reporting measure 8 focus
The QIP Newsletter For Dialysis Facilities Inside this issue: What does the QIP 2 Measure? What has Changed? 3 QIP Measures 3 Clinical measure 3-5 focus Measures that 6-7 Matter Reporting measure 8 focus
Specialty Care Approaches to Accountable Care: A Panel Discussion. Allen R. Nissenson, MD, FACP Chief Medical Officer, DaVita
 Specialty Care Approaches to Accountable Care: A Panel Discussion Allen R. Nissenson, MD, FACP Chief Medical Officer, DaVita 1 Panel Lara M. Khouri, MBA, MPH VP, Health System Development and Integration,
Specialty Care Approaches to Accountable Care: A Panel Discussion Allen R. Nissenson, MD, FACP Chief Medical Officer, DaVita 1 Panel Lara M. Khouri, MBA, MPH VP, Health System Development and Integration,
2018 CMS Priorities, Goals, and Quality Improvement Activities. IPRO ESRD Network of New England Network Council Meeting January 17, 2018
 2018 CMS Priorities, Goals, and Quality Improvement Activities IPRO ESRD Network of New England Network Council Meeting January 17, 2018 Meeting Reminders All phone lines have been muted to avoid background
2018 CMS Priorities, Goals, and Quality Improvement Activities IPRO ESRD Network of New England Network Council Meeting January 17, 2018 Meeting Reminders All phone lines have been muted to avoid background
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule
 Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
Calendar Year 2014 Medicare Physician Fee Schedule Final Rule Non-Facility Cap After receiving many negative comments on this issue from physician groups, along with the House GOP Doctors Caucus letter
Fistula Fast Fast Fast Track What to do en h th f e i fistula wasn t first
 Fistula Fast Track What to do when the fistula wasn t first Angela Schuler, RN Fox Valley Dialysis/Tri-cities Dialysis Welcome, Today we will: Describe processes used for early placement of AVF Discuss
Fistula Fast Track What to do when the fistula wasn t first Angela Schuler, RN Fox Valley Dialysis/Tri-cities Dialysis Welcome, Today we will: Describe processes used for early placement of AVF Discuss
Reducing Infections and Improving Engagement St. Luke's Nephrology Associates. Contact Information: Robert Gayner, M.D., FASN
 BEST PRACTICES Vascular Access and CLABSI Reduction Reducing Infections and Improving Engagement St. Luke's Nephrology Associates Contact Information: Robert Gayner, M.D., FASN St. Luke's Nephrology Associates
BEST PRACTICES Vascular Access and CLABSI Reduction Reducing Infections and Improving Engagement St. Luke's Nephrology Associates Contact Information: Robert Gayner, M.D., FASN St. Luke's Nephrology Associates
Healthcare-Associated Infections (HAI) Quality Improvement Activity Project Kickoff Webinar
 Quality Improvement Activity Project Kickoff Webinar") Healthcare-Associated Infections (HAI) Quality Improvement Activity 2017 Project Kickoff Webinar QIP PY 2019 Final Measure Domain Weighting Domain Weight Measures/Measure Topics Weight (Domain) Safety
Healthcare-Associated Infections (HAI) Quality Improvement Activity 2017 Project Kickoff Webinar QIP PY 2019 Final Measure Domain Weighting Domain Weight Measures/Measure Topics Weight (Domain) Safety
ASN Dialysis Advisory Group ASN DIALYSIS CURRICULUM
 ASN Dialysis Advisory Group ASN DIALYSIS CURRICULUM 0 ASN Dialysis Curriculum The Role of Medical Directors David B. Van Wyck, MD DaVita, Inc. 1 Disclosures DaVita, Inc Employee and stockholder Affymax
ASN Dialysis Advisory Group ASN DIALYSIS CURRICULUM 0 ASN Dialysis Curriculum The Role of Medical Directors David B. Van Wyck, MD DaVita, Inc. 1 Disclosures DaVita, Inc Employee and stockholder Affymax
Network Agreement Packet
 ESRD NETWORK OF TEXAS, INC. Network Agreement Packet Forms to return: Facility Details and Primary Contacts Network Agreement Acknowledgment of Receipt Inside this packet: Goals and Objectives List of
ESRD NETWORK OF TEXAS, INC. Network Agreement Packet Forms to return: Facility Details and Primary Contacts Network Agreement Acknowledgment of Receipt Inside this packet: Goals and Objectives List of
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA)
 Case Study Scenario 1: Following Quality Assurance (QA)") Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
Infection Control Quality Assurance & Performance Improvement (QAPI) Case Study Scenario 1: Following Quality Assurance (QA) The Facility Starview Convalescent Center is a 60-bed long-term care facility.
4/26/2017. I ll Do It My Way, Thank You Performance Improvement Strategies for Home Care. Session Objectives. Session Agenda
 I ll Do It My Way, Thank You Performance Improvement Strategies for Home Care Barbara Katz, RN, MSN President, BK Health Care Consulting, LLC www.bkhealthconsulting.com Session Objectives Explain the role
I ll Do It My Way, Thank You Performance Improvement Strategies for Home Care Barbara Katz, RN, MSN President, BK Health Care Consulting, LLC www.bkhealthconsulting.com Session Objectives Explain the role
Clostridium difficile Infection (CDI) Intervention Kick-Off Webinar
 Intervention Kick-Off Webinar") Clostridium difficile Infection (CDI) Intervention Kick-Off Webinar Wednesday, January 17, 2018 National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Introduction
Clostridium difficile Infection (CDI) Intervention Kick-Off Webinar Wednesday, January 17, 2018 National Nursing Home Quality Care Collaborative (NNHQCC) Health Services Advisory Group (HSAG) Introduction
Our Journey Towards Patient Self- Management: The Patient Experience. Presented by: Dr Janet Roscoe Paulette Lewis Pat Taylor Clint Gunn
 Our Journey Towards Patient Self- Management: The Patient Experience Presented by: Dr Janet Roscoe Paulette Lewis Pat Taylor Clint Gunn Objectives To share our experiences in the development of patient
Our Journey Towards Patient Self- Management: The Patient Experience Presented by: Dr Janet Roscoe Paulette Lewis Pat Taylor Clint Gunn Objectives To share our experiences in the development of patient
CMS ESRD Data Collection. Systems Overview. Jaya Bhargava, PhD, CPHQ Operations Director
 CMS ESRD Data Collection Systems Overview Jaya Bhargava, PhD, CPHQ Operations Director Relationship Between Dialysis Facility & The Network Under conditions for coverage, ESRD providers are required to
CMS ESRD Data Collection Systems Overview Jaya Bhargava, PhD, CPHQ Operations Director Relationship Between Dialysis Facility & The Network Under conditions for coverage, ESRD providers are required to
ACO Practice Transformation Program
 ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
ACO Overview ACO Practice Transformation Program PROGRAM OVERVIEW As healthcare rapidly transforms to new value-based payment systems, your level of success will dramatically improve by participation in
Managing Your Patient Population: How do you measure up?
 Managing Your Patient Population: How do you measure up? Paul M. Palevsky, M.D. Chief, Renal Section VA Pittsburgh Healthcare System Professor of Medicine University of Pittsburgh School of Medicine Ben
Managing Your Patient Population: How do you measure up? Paul M. Palevsky, M.D. Chief, Renal Section VA Pittsburgh Healthcare System Professor of Medicine University of Pittsburgh School of Medicine Ben
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
End Stage Renal Disease Network of Texas, Inc. Facility Patient Representative Handbook
 End Stage Renal Disease Network of Texas, Inc. Facility Patient Representative Handbook 2016 Table of Contents Facility Patient Representative Handbook... 1 What is a Facility Patient Representative (FPR)?...
End Stage Renal Disease Network of Texas, Inc. Facility Patient Representative Handbook 2016 Table of Contents Facility Patient Representative Handbook... 1 What is a Facility Patient Representative (FPR)?...
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
The Renal Network Inc. CROWNWeb Network Data Reporting
 The Renal Network Inc. CROWNWeb Network Data Reporting Facility CROWNWeb Responsibilities CMS-2728 CMS-2746 Monthly PART verification Notifications & Accretions Clinical Data New enhancements/updates CMS-2728
The Renal Network Inc. CROWNWeb Network Data Reporting Facility CROWNWeb Responsibilities CMS-2728 CMS-2746 Monthly PART verification Notifications & Accretions Clinical Data New enhancements/updates CMS-2728
QIO Care Transitions Activity: the Good News so far
 QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
QIO Care Transitions Activity: the Good News so far Kim Irby, MPH; kirby@cfmc.org Senior Project Director Colorado Foundation for Medical Care www.cfmc.org/integratingcare This material was prepared by
2016 Embedded and Rapid Response Care Management
 2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
The Home Hemodialysis
 The Home Hemodialysis Cannulation Assistance Program from concept to reality. Terri Chanda R.N., CNeph(C) Renal Improvement Lead The Credit Valley Hospital and Trillium Health Centre [Poll the audience
The Home Hemodialysis Cannulation Assistance Program from concept to reality. Terri Chanda R.N., CNeph(C) Renal Improvement Lead The Credit Valley Hospital and Trillium Health Centre [Poll the audience
Home Dialysis Referral: New Shift
 Home Dialysis Referral: New Shift 2017 AIM 2 Quality Improvement Activity ANDREA MOORE Quality Improvement Coordinator Agenda CMS Statement of Work (SOW) Rewind: Another Look at the CMS Definition of Referral
Home Dialysis Referral: New Shift 2017 AIM 2 Quality Improvement Activity ANDREA MOORE Quality Improvement Coordinator Agenda CMS Statement of Work (SOW) Rewind: Another Look at the CMS Definition of Referral
Peer Review Example: Clinician 4 (Meets Expectations)
") Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Indiana Pressure Ulcer Reduction Initiative
 Indiana Pressure Ulcer Reduction Initiative Overview The IHI Breakthrough Series Collaborative is a systematic approach to healthcare quality improvement in which organizations and providers test and measure
Indiana Pressure Ulcer Reduction Initiative Overview The IHI Breakthrough Series Collaborative is a systematic approach to healthcare quality improvement in which organizations and providers test and measure
Managing Access by Generating Improvements in Cannulation
 Managing Access by Generating Improvements in Cannulation Katie Fielding, Co-Chair, BRS VA Professional Development Advisor Haemodialysis, Derby Teaching Hospitals NHS Foundation Trust MDT Fellow, UK Renal
Managing Access by Generating Improvements in Cannulation Katie Fielding, Co-Chair, BRS VA Professional Development Advisor Haemodialysis, Derby Teaching Hospitals NHS Foundation Trust MDT Fellow, UK Renal
Passport Advantage (HMO SNP) Model of Care Training (Providers)
 Model of Care Training (Providers)") Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Sandra D. Fritzsch RN JD
 Sandra D. Fritzsch RN JD Current Experience 2005-Current Consultant in the Chronic Renal Disease CKD) Industry for the development and certification of CKD dialysis facilities. Have participated in the
Sandra D. Fritzsch RN JD Current Experience 2005-Current Consultant in the Chronic Renal Disease CKD) Industry for the development and certification of CKD dialysis facilities. Have participated in the
Dialysis Laboratory Services and Reports December 2012 January 2013
 Dialysis Laboratory Services and Reports December 2012 January 2013 Excerpted Analyses From Full Report Prepared for NNI March 6, 2013 NCS Research NCSResearchCouncil@gmail.com Executive Summary Research
Dialysis Laboratory Services and Reports December 2012 January 2013 Excerpted Analyses From Full Report Prepared for NNI March 6, 2013 NCS Research NCSResearchCouncil@gmail.com Executive Summary Research
Patient Rights & Responsibilities
 Patient Rights & Responsibilities A goal of The Renal Network is to make sure that all End-Stage kidney patients in Illinois are able to receive medical care and are treated with dignity and respect. The
Patient Rights & Responsibilities A goal of The Renal Network is to make sure that all End-Stage kidney patients in Illinois are able to receive medical care and are treated with dignity and respect. The
CULTURAL OF HOME DIALYSIS
 Patient Selection What Would You Choose? Yvonne Hornyak, RN CULTURAL OF HOME DIALYSIS PATIENT SELECTION Disclosure PATIENT SELECTION Objectives Understand the relationship between social, clinical, and
Patient Selection What Would You Choose? Yvonne Hornyak, RN CULTURAL OF HOME DIALYSIS PATIENT SELECTION Disclosure PATIENT SELECTION Objectives Understand the relationship between social, clinical, and
The Intersection of PFE, Quality, and Equity: Establishing Diverse Patient and Family Advisory Councils to Improve Patient Safety
 The Intersection of PFE, Quality, and Equity: Establishing Diverse Patient and Family Advisory Councils to Improve Patient Safety OHA HIIN: Partnership for Patients (PfP) Webinar Lee Thompson, MS, AIR
The Intersection of PFE, Quality, and Equity: Establishing Diverse Patient and Family Advisory Councils to Improve Patient Safety OHA HIIN: Partnership for Patients (PfP) Webinar Lee Thompson, MS, AIR
ESRD Network 13: 2017 Performance Guidance
 ESRD Network 13: 2017 Performance Guidance This material was prepared by HSAG: ESRD Network 13, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department
ESRD Network 13: 2017 Performance Guidance This material was prepared by HSAG: ESRD Network 13, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department
QAPI Plan QAPI Plan. snits: Sanitas, Denver, CO. Effective Date: 01-Jan-2018
 QAPI Plan 2018 QAPI Plan snits: Sanitas, Denver, CO Effective Date: 01-Jan-2018 Design & Scope Statements and Guiding Principles: Vision We will be the premier providers in post-acute care. Mission Our
QAPI Plan 2018 QAPI Plan snits: Sanitas, Denver, CO Effective Date: 01-Jan-2018 Design & Scope Statements and Guiding Principles: Vision We will be the premier providers in post-acute care. Mission Our
Issue 2 2 nd Quarter 2015
 In this Issue AIM 1 AIM 2 AIM 3 Quick Links Network 13 Website CROWNWeb Online Help Dialysis Facility Compare NHSN QIP Payment Year 2017 Final Rule Materials are Available here. Network 13 All- Hazards
In this Issue AIM 1 AIM 2 AIM 3 Quick Links Network 13 Website CROWNWeb Online Help Dialysis Facility Compare NHSN QIP Payment Year 2017 Final Rule Materials are Available here. Network 13 All- Hazards
ACCME NEW MENU OF CRITERIA FOR ACCREDITATION WITH COMMENDATION. Ranae Obregon ISMA - Director of Education
 ACCME NEW MENU OF CRITERIA FOR ACCREDITATION WITH COMMENDATION Ranae Obregon ISMA - Director of Education Implementation ACCME-accredited providers receiving accreditation decisions between November 2017
ACCME NEW MENU OF CRITERIA FOR ACCREDITATION WITH COMMENDATION Ranae Obregon ISMA - Director of Education Implementation ACCME-accredited providers receiving accreditation decisions between November 2017
Accountable Care for End-Stage Renal Disease Patients 12:00 1:00, March 4, 2016
 Accountable Care for End-Stage Renal Disease Patients 12:00 1:00, March 4, 2016 Craig Schneider, Ph.D, Senior Health Researcher, Mathematica Policy Research Doug Johnson, MD, Vice Chair, DCI Conflict of
Accountable Care for End-Stage Renal Disease Patients 12:00 1:00, March 4, 2016 Craig Schneider, Ph.D, Senior Health Researcher, Mathematica Policy Research Doug Johnson, MD, Vice Chair, DCI Conflict of
Your partner in quality and patient safety. Center for Quality. Improvement. SHM s
 SHM s Center for Quality Improvement Your partner in quality and patient safety. Your People. Your Network. Your Society. Empowering hospitalists. Transforming patient care. The Society of Hospital Medicine
SHM s Center for Quality Improvement Your partner in quality and patient safety. Your People. Your Network. Your Society. Empowering hospitalists. Transforming patient care. The Society of Hospital Medicine
Congress extended Medicare coverage in
 Promoting Quality of Care for ESRD Patients: The Role of the ESRD Networks Jenna Krisher and Stephen Pastan The 18 End Stage Renal Disease (ESRD) Networks were established by Congress to oversee the care
Promoting Quality of Care for ESRD Patients: The Role of the ESRD Networks Jenna Krisher and Stephen Pastan The 18 End Stage Renal Disease (ESRD) Networks were established by Congress to oversee the care
CMS Proposed Rule Summary: ESRD PPS for CY 2017; ESRD QIP for PYs 2018, 2019, and 2020; AKI; and CEC Model
 CMS Proposed Rule Summary: ESRD PPS for CY 2017; ESRD QIP for PYs 2018, 2019, and 2020; AKI; and CEC Model On June 24, 2016, the Centers for Medicare & Medicaid Services (CMS) released a proposed rule
CMS Proposed Rule Summary: ESRD PPS for CY 2017; ESRD QIP for PYs 2018, 2019, and 2020; AKI; and CEC Model On June 24, 2016, the Centers for Medicare & Medicaid Services (CMS) released a proposed rule
Focus on Fistulas. Fistula First
 A Medical Education Institute/Life Options Publication VOL. 1 NO. 1 MARCH 2004 New Name, New Look The Renal Rehabilitation Report has gotten a makeover! After more than 10 years, we ve re-designed our
A Medical Education Institute/Life Options Publication VOL. 1 NO. 1 MARCH 2004 New Name, New Look The Renal Rehabilitation Report has gotten a makeover! After more than 10 years, we ve re-designed our
Patient Rights & Responsibilities
 Patient Rights & Responsibilities A goal of The Renal Network is to make sure that all End-Stage kidney patients in Illinois are able to receive medical care and are treated with dignity and respect. The
Patient Rights & Responsibilities A goal of The Renal Network is to make sure that all End-Stage kidney patients in Illinois are able to receive medical care and are treated with dignity and respect. The
Difference Between Lost to Follow up and Withdrawal from Care
 Difference Between Lost to Follow up and Withdrawal from Care Contents Actual Polling Questions from Webinar... 2 Questions asked on Webinar... 11 Supplemental Questions... 13 Upcoming Reminders... 15
Difference Between Lost to Follow up and Withdrawal from Care Contents Actual Polling Questions from Webinar... 2 Questions asked on Webinar... 11 Supplemental Questions... 13 Upcoming Reminders... 15
Key Performance Indicators
 Regional Nephrology System (RNS) Chronic Disease Prevention and Management Key Performance Indicators 8/9 Fiscal Year End Report Version: 1. Date published: April 7th, 9 Created by: Ethel Doyle: RNS Interim
Regional Nephrology System (RNS) Chronic Disease Prevention and Management Key Performance Indicators 8/9 Fiscal Year End Report Version: 1. Date published: April 7th, 9 Created by: Ethel Doyle: RNS Interim
NQF-Endorsed Measures for Renal Conditions,
 NQF-Endorsed Measures for Renal Conditions, 2015-2017 TECHNICAL REPORT February 2017 This report is funded by the Department of Health and Human Services under contract HHSM-500-2012-00009I Task Order
NQF-Endorsed Measures for Renal Conditions, 2015-2017 TECHNICAL REPORT February 2017 This report is funded by the Department of Health and Human Services under contract HHSM-500-2012-00009I Task Order
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies
 Improvement Strategies") Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
Follow-Up after Hospitalization for Mental Illness (FUH) Improvement Strategies 1. What efforts and/or strategies have you put in place to improve your plans performance on the Follow-Up After Hospitalization
A Year s Progress Toward ED Pediatric Readiness in Kentucky
 A Year s Progress Toward ED Pediatric Readiness in Kentucky Mark J. McDonald, M.D. Medical Director Norton Children s Hospital Associate Professor, U of L SOM Department of Pediatrics Division of Critical
A Year s Progress Toward ED Pediatric Readiness in Kentucky Mark J. McDonald, M.D. Medical Director Norton Children s Hospital Associate Professor, U of L SOM Department of Pediatrics Division of Critical
NASW/NKF Clinical Indicators for Social Work and Psychosocial Service in Nephrology Settings
 < NASW Homepage NASW/NKF Clinical Indicators for Social Work and Psychosocial Service in Nephrology Settings Advertise With NASW Contact Us Privacy Statement Prepared and approved by the National Association
< NASW Homepage NASW/NKF Clinical Indicators for Social Work and Psychosocial Service in Nephrology Settings Advertise With NASW Contact Us Privacy Statement Prepared and approved by the National Association
WELCOME: THE WEBINAR WILL BEGIN SHORTLY
 WELCOME: THE WEBINAR WILL BEGIN SHORTLY TRANSPLANT WAITLIST TRANSPLANT IMPROVEMENT PROGRAM FOR SUCCESS (TIPS) ORIENTATION WEBINAR FEBRUARY 15, 2018 1:00 PM CT DANY ANCHIA, RN, CDN CLINICAL QUALITY MANAGER
WELCOME: THE WEBINAR WILL BEGIN SHORTLY TRANSPLANT WAITLIST TRANSPLANT IMPROVEMENT PROGRAM FOR SUCCESS (TIPS) ORIENTATION WEBINAR FEBRUARY 15, 2018 1:00 PM CT DANY ANCHIA, RN, CDN CLINICAL QUALITY MANAGER
1) Goal Fellows will become competent in caring for renal transplant patients and patients with renal complications of non-renal transplants.
 Goal Fellows will become competent in caring for renal transplant patients and patients with renal complications of non-renal transplants.") Clinical curriculum: Transplant 1) Goal Fellows will become competent in caring for renal transplant patients and patients with renal complications of non-renal transplants. 2) Objectives Detailed objectives
Clinical curriculum: Transplant 1) Goal Fellows will become competent in caring for renal transplant patients and patients with renal complications of non-renal transplants. 2) Objectives Detailed objectives
Talking Control as a Method to Improve Patient Satisfaction with Staff Communication in the Dialysis Setting
 16, Volume 40, Issue 2 Talking Control as a Method to Improve Patient Satisfaction with Staff Communication in the Dialysis Setting DeeDee Velasquez-Peralta, LMSW, Anna Ramirez, MPH, CPH, Heartland Kidney
16, Volume 40, Issue 2 Talking Control as a Method to Improve Patient Satisfaction with Staff Communication in the Dialysis Setting DeeDee Velasquez-Peralta, LMSW, Anna Ramirez, MPH, CPH, Heartland Kidney
ANNUAL REPORT TO THE CONGRESSIONAL DEFENSE COMMITTEES. Support for Military Families with Special Needs. Pursuant to
 ANNUAL REPORT TO THE CONGRESSIONAL DEFENSE COMMITTEES on Support for Military Families with Special Needs Pursuant to Section 1781c(h) of Title 10, United States Code APRIL 2016 The estimated cost of this
ANNUAL REPORT TO THE CONGRESSIONAL DEFENSE COMMITTEES on Support for Military Families with Special Needs Pursuant to Section 1781c(h) of Title 10, United States Code APRIL 2016 The estimated cost of this
2014 QAPI Plan for [Facility Name]
![2014 QAPI Plan for [Facility Name]](/thumbs/74/70066237.jpg "2014 QAPI Plan for [Facility Name]") presented by: Quality Leadership for Long-Term Care 2014 QAPI Plan for [Facility Name] Vision A vision statement is sometimes called a picture of your organization in the future; it is your inspiration
presented by: Quality Leadership for Long-Term Care 2014 QAPI Plan for [Facility Name] Vision A vision statement is sometimes called a picture of your organization in the future; it is your inspiration
American Nephrology Nurses Association Comments on CMS 2015 ESRD Prospective Payment System and Quality Incentive Program
 American Nephrology Nurses Association Comments on CMS 2015 ESRD Prospective Payment System and Quality Incentive Program CY 2015 ESRD PPS System Proposed Rule ANNA Comments CY 2015 ESRD PPS System Final
American Nephrology Nurses Association Comments on CMS 2015 ESRD Prospective Payment System and Quality Incentive Program CY 2015 ESRD PPS System Proposed Rule ANNA Comments CY 2015 ESRD PPS System Final
INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP)
 DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP)") SNP MODEL OF CARE ANNUAL EVALUATIONS FOR 2013 INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP) 1 7 0 1 P O N C E D E L E O N B L V D, S
SNP MODEL OF CARE ANNUAL EVALUATIONS FOR 2013 INSTITUTIONAL/INSTITUTIONAL EQUIVALENT (I/IESNP) DUAL SPECIAL NEEDS PLAN (DSNP) CHRONIC SPECIAL NEEDS PLAN (LSNP) 1 7 0 1 P O N C E D E L E O N B L V D, S
Check-Plan-Do-Check-Act-Cycle
 Adequacy of hemodialysis 1 Adequacy of Hemodialysis Introduction Providing adequate hemodialysis treatment is dependent on numerous factors ranging from type of dialyzer used to appropriate length of treatment
Adequacy of hemodialysis 1 Adequacy of Hemodialysis Introduction Providing adequate hemodialysis treatment is dependent on numerous factors ranging from type of dialyzer used to appropriate length of treatment
2016 Complex Case Management. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
2016 Complex Case Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Complex Case Management Program Evaluation Table of Contents Program Purpose
30 E. 33rd Street New York, NY Tel Fax
 National Kidney Foundation Summary of the 2016 ESRD PPS and 2017-2019 QIP Final Rule. On Thursday, October 29, the Centers for Medicare & Medicaid Services (CMS) released the final Medicare Program; End-Stage
National Kidney Foundation Summary of the 2016 ESRD PPS and 2017-2019 QIP Final Rule. On Thursday, October 29, the Centers for Medicare & Medicaid Services (CMS) released the final Medicare Program; End-Stage
9/10/2013. The Session s Focus. Status of the NYS FIDA Initiative
 Leading Age NY Financial Manager s Conference, September 10-12, 2013 The Otesaga Resort Hotel, Cooperstown NY Paul Tenan VCC, Inc. FIDA: An Overview and Update The Session s Focus Overview of CMS national
Leading Age NY Financial Manager s Conference, September 10-12, 2013 The Otesaga Resort Hotel, Cooperstown NY Paul Tenan VCC, Inc. FIDA: An Overview and Update The Session s Focus Overview of CMS national
Technology Fundamentals for Realizing ACO Success
 Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
ESRD Network 16 Northwest Renal Network January 9, 2017
 ESRD Network 16 Northwest Renal Network January 9, 2017 Katrina Russell, RN, CNN NW16 Board Chair John Stivelman, MD NW16 Medical Review Board Chair Stephanie Hutchinson, MBA - Executive Director Barbara
ESRD Network 16 Northwest Renal Network January 9, 2017 Katrina Russell, RN, CNN NW16 Board Chair John Stivelman, MD NW16 Medical Review Board Chair Stephanie Hutchinson, MBA - Executive Director Barbara
ESRD ANNUAL FACILITY SURVEY (CMS-2744) INSTRUCTIONS FOR COMPLETION
 INSTRUCTIONS FOR COMPLETION") ESRD ANNUAL FACILITY SURVEY (CMS-2744) INSTRUCTIONS FOR COMPLETION REPORTING RESPONSIBILITY The ESRD Facility Survey is designed to capture only a limited amount of information concerning each federally
ESRD ANNUAL FACILITY SURVEY (CMS-2744) INSTRUCTIONS FOR COMPLETION REPORTING RESPONSIBILITY The ESRD Facility Survey is designed to capture only a limited amount of information concerning each federally
Strategic Plan SFY
 Strategic Plan SFY 2017-2018 DHS STRATEGY MAP SFY 2017-2018 OUR MISSION We improve the quality of life of vulnerable Oklahomans by increasing people s ability to lead safer, healthier, more independent
Strategic Plan SFY 2017-2018 DHS STRATEGY MAP SFY 2017-2018 OUR MISSION We improve the quality of life of vulnerable Oklahomans by increasing people s ability to lead safer, healthier, more independent
MDS Essentials. MDS Essentials: Content. Faculty Disclosures 5/22/2017. Educational Activity Completion
 MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
Indianapolis Transitional Grant Area Quality Management Plan (Revised)
") Indianapolis Transitional Grant Area Quality Management Plan 2017 2018 (Revised) Serving 10 counties: Boone, Brown, Hamilton, Hancock, Hendricks, Johnson, Marion, Morgan, Putnam and Shelby 1 TABLE OF CONTENTS
Indianapolis Transitional Grant Area Quality Management Plan 2017 2018 (Revised) Serving 10 counties: Boone, Brown, Hamilton, Hancock, Hendricks, Johnson, Marion, Morgan, Putnam and Shelby 1 TABLE OF CONTENTS
Local Health Department Access to the National Healthcare Safety Network. January 23, 2018
 Local Health Department Access to the National Healthcare Safety Network January 23, 2018 Learning Objectives Describe the National Healthcare Safety Network (NHSN), its functions, and uses Identify upcoming
Local Health Department Access to the National Healthcare Safety Network January 23, 2018 Learning Objectives Describe the National Healthcare Safety Network (NHSN), its functions, and uses Identify upcoming
Telehealth 101. Telehealth Summit May 24, 2018
 Telehealth 101 Telehealth Summit May 24, 2018 Tim Bickel Telehealth Director, University of Louisville Deborah Burton, Telehealth Program Manager, KentuckyOne Health, Lexington; Chair, Kentucky Teleheath
Telehealth 101 Telehealth Summit May 24, 2018 Tim Bickel Telehealth Director, University of Louisville Deborah Burton, Telehealth Program Manager, KentuckyOne Health, Lexington; Chair, Kentucky Teleheath
Navigating The End-Stage Renal Disease (ESRD) Payment System
 Payment System") Navigating The End-Stage Renal Disease (ESRD) Payment System Navigating The End-Stage Renal Disease (ESRD) Payment System Mark A. Meier, MSW, LICSW Page 1 of 13 00:00:00 Mark A. Meier: Hello, my name is
Navigating The End-Stage Renal Disease (ESRD) Payment System Navigating The End-Stage Renal Disease (ESRD) Payment System Mark A. Meier, MSW, LICSW Page 1 of 13 00:00:00 Mark A. Meier: Hello, my name is
ESRD Network 18 of Southern California January 10, 2018
 ESRD Network 18 of Southern California January 10, 2018 Kamyar (Kam) Kalantar-Zadeh, MD NW18 Medical Review Board Chair Stephanie Hutchinson, MBA - Executive Director Barbara Dommert-Breckler, RN, BSN,
ESRD Network 18 of Southern California January 10, 2018 Kamyar (Kam) Kalantar-Zadeh, MD NW18 Medical Review Board Chair Stephanie Hutchinson, MBA - Executive Director Barbara Dommert-Breckler, RN, BSN,
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
2017 Catastrophic Care. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals