Defense Health Agency Update
|
|
|
- Duane Roberts
- 6 years ago
- Views:
Transcription














1 Defense Health Agency Update Lt Gen Doug Robb, USAF, MC Director April 2015
2 MHS Governance Reform: What We Are Undertaking Creating a more globally integrated health system built on our battlefield successes Driving enterprise-wide shared services; standardized clinical and business processes that produce better health and better health care Implementing future-oriented strategies to create a better, stronger, more relevant medical force



3 DHA: How We Got Here DoD Task Force on MHS Governance DEPSECDEF Planning Memo DHA Planning WG Report DEPSECDEF Nine Commandments Memo September 2011 March 2012 November 2012 March 2013 Recommended DHA model for MHS governance Directed planning for DHA implementation Provided DHA and Shared Services implementation plan for DEPSECDEF approval Directed implementation of DHA Medically Medically Ready Ready Force Ready Force Ready Medical Medical Force Force 3
4 DepSecDef Nine Commandments 1. Defense Health Agency (DHA) a. Designated as a Combat Support Agency b. Assumes responsibility for the functions currently undertaken by TMA c. Assumes responsibility for shared services, functions, and activities in the MHS 2.Multi-Service Markets a. Appoint a Market Manager in geographic medical markets determined by overlapping multi-service catchment areas b. Market Manager s mission: create & sustain a cost-effective, coordinated, and high-quality market health care system c. Market Manager s authorities: manage & allocate MSM budget, direct adoption of common MSM clinical & business functions, and direct movement of workload & workforce as needed between/among MSM MTFs 3.National Capital Region Medical Directorate, DHA a. Assumes authority, direction, and control over the NCR health system, to include Walter Reed National Military Medical Center, Fort Belvoir Community Hospital, and all other MTFs that are determined to reside within the NCR market b. Directors of the WRNMMC, the FBCH, and the other MTFs will be selected by the USD(P&R) (or, if delegated, the ASD(HA), Director, DHA, or Director, NCR Med Dir) from nominees provided by the Military Departments c. Military personnel for the WRNMMC, the FBCH, and the other MTFs will be provided by the Military Departments according to manning documents maintained by the DHA 4
 Policy & Oversight Execution Defense Health Agency CSA Army SG Army MEDCOM CNO Navy SG Navy BUMED CMC CSAF Air Force MAJCOMs Air Force SG MPOG MOG")
5 Military Health System Secretary of Defense USD(P&R), Vice Chiefs MHSER CJCS USD(P&R) Sec Army Sec Navy Sec Air Force ASD(HA) SGs, JSS PDASD, Deputy SGs, JSS, DD, DHA SMMAC MDAG, DASDs, JSS MDAG PAC USUHS Combat Support Agency Responsibilities ASD(HA) Policy & Oversight Execution Defense Health Agency CSA Army SG Army MEDCOM CNO Navy SG Navy BUMED CMC CSAF Air Force MAJCOMs Air Force SG MPOG MOG MBOG NCR Directorate MTFs MTFs MTFs Personnel Operations Budget Army Operational Units Navy Operational Units Marine Operational Units Air Force Operational Units MTFs MHS Governance Defense Health Agency Service Medical Organization 5









6 Defense Health Agency Leadership Team Mr. Paul Hutter Deputy Director Lt Gen Douglas Robb Director CMDCM Terry Prince Senior Enlisted Advisor MG Richard Thomas Director Healthcare Operations RADM Bruce Doll Director Research & Development Mr. David Bowen Director Health IT Brig Gen Robert Miller Director Education & Training Mr. Joseph Marshall Director Business Support RADM Raquel Bono Director NCR Medical 6
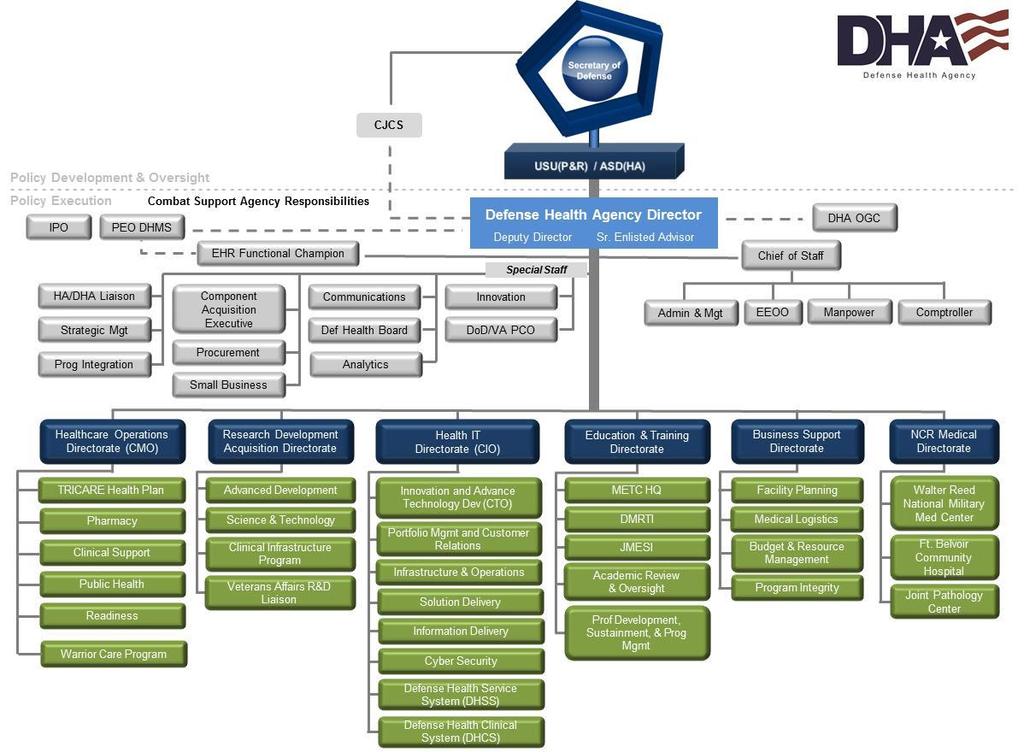
7 7

8 DHA as a Combat Support Agency Translation: DHA is to medical as DLA is to logistics as DISA is to communications 8
9 Military Health System Strategic Plan 9
10 MILITARY HEALTH SYSTEM STRATEGY MAP
11 ENDS MILITARY HEALTH SYSTEM STRATEGY MAP Medically Ready Force Ready Medical Force
12 MEANS WAYS ENDS MILITARY HEALTH SYSTEM STRATEGY MAP Medically Ready Force Ready Medical Force Healthy People
13 MEANS WAYS ENDS MILITARY HEALTH SYSTEM STRATEGY MAP Medically Ready Force Ready Medical Force Healthy People Improve Clinical Outcomes and Consistent Patient Experience Improve Stewardship
14 MEANS WAYS ENDS MILITARY HEALTH SYSTEM STRATEGY MAP Medically Ready Force Ready Medical Force Healthy People Improve Clinical Outcomes and Consistent Patient Experience Improve Stewardship
15 MEANS WAYS ENDS MILITARY HEALTH SYSTEM STRATEGY MAP PLS1 Medically Ready Force PLS2 Ready Medical Force PLS3 Healthy People PLS4 Improve Clinical Outcomes and Consistent Patient Experience PLS5 Improve Stewardship Align Resources Against Strategic Priorities \
16 MEANS WAYS ENDS MILITARY HEALTH SYSTEM STRATEGY MAP Medically Ready Force Ready Medical Force Healthy People Improve Clinical Outcomes and Consistent Patient Experience Improve Stewardship Recruit, Train, & Develop the Total Force to Meet Future Challenges Improve Information Infrastructure Optimize DHA as a Support Organization OC4 Improve Process- Based Management OC5 Align Facilities, Personnel, and Capabilities to Optimize Market Performance Align Resources Against Strategic Priorities and Ensure Fiscal Accountability
17 MEANS WAYS ENDS MILITARY HEALTH SYSTEM STRATEGY MAP Medically Ready Force Ready Medical Force Healthy People Improve Clinical Outcomes and Consistent Patient Experience Improve Stewardship Recruit, Train, & Develop the Total Force to Meet Future Challenges Improve Information Infrastructure Optimize DHA as a Support Organization Improve Process- Based Management Align Facilities, Personnel, and Capabilities to Optimize Market Performance Align Resources Against Strategic Priorities and Ensure Fiscal Accountability
18 Financial MEANS Organizational Capability WAYS ENDS MILITARY HEALTH SYSTEM STRATEGY MAP PLS1 Medically Ready Force PLS2 Ready Medical Force PLS3 Healthy People PLS4 Improve Clinical Outcomes and Consistent Patient Experience PLS5 Improve Stewardship IP1 Improve Global Health Engagement IP3 Enhance Emerging Medical Capabilities in a Joint Environment IP2 Improve Operational Medicine IP4 Enhance Strategic Partnerships IP5 Improve Healthy Behaviors IP6 Expand the Boundaries of Healthcare IP7 Improve Condition-Based Quality Care IP8 Improve Comprehensive Primary Care IP9 Improve Safety IP10 Optimize & Standardize Access & Other Care Support Processes IP11 Reform TRICARE IP12 Align Incentives to Achieve Outcomes OC1 Recruit, Train, & Develop the Total Force to Meet Future Challenges OC2 Improve Information Infrastructure OC3 Optimize DHA as a Support Organization OC4 Improve Process- Based Management OC5 Align Facilities, Personnel, and Capabilities to Optimize Market Performance F1 Align Resources Against Strategic Priorities and Ensure Fiscal Accountability
19 MEANS (Enablers) Financial Organizational Internal Process Capability WAYS ENDS Patient/Leader/ Stakeholder 1. DHA is strongly aligned to the MHS Strategy Map 2. DHA is foundation that supports the MHS as an integrated system Better Health Better Care Lower Cost Medical force ready to deliver health services anywhere, anytime, so that the total force is medically ready for, and protected during, any operational mission Improve the health of our population by fostering healthy lifestyles, preventing illness, and reducing the impact of sickness and injury Provide safe and effective patient centered healthcare that improves clinical outcomes Reducing the total cost of the MHS by continuously improving efficiency and eliminating waste DHA Directorates PLS1 Medically Ready Force IP1 Improve Global Health Engagement PLS2 Ready Medical Force IP3 Enhance Emerging Medical Capabilities in a Joint Environment IP2 Improve Operational Medicine IP4 Enhance Strategic Partnerships OC1 Recruit, Train, & Develop the Total Force to Meet Future Challenges PLS3 Healthy People IP5 Improve Healthy Behaviors OC2 Improve Information Infrastructure IP6 Expand the Boundaries of Healthcare IP7 Improve Condition-Based Quality Care IP8 Improve Comprehensive Primary Care IP9 Improve Safety IP10 Optimize & Standardize Access & Other Care Support Processes IP11 Reform TRICARE IP12 Align Incentives to Achieve Outcomes OC3 Optimize DHA as a Support Organization PLS4 Improve Clinical Outcomes and Consistent Patient Experience OC4 Improve Process-Based Management PLS5 Improve Stewardship OC5 Align Facilities, Personnel, and Capabilities to Optimize Market Performance Business Support Education & Training Healthcare Operations Health Information Technology Research & Development National Capital Region Special Staff and DHMS Contracting Human Resources Manpower Defense Healthcare Management System F1 Align Resources Against Strategic Priorities and Ensure Fiscal Accountability 10
20 COL Guy Kiyokawa Chief of Staff, DHA DHA Shared Services 20

21 DHA Shared Services 21
22 Shared Services Savings Five Year Defense Plan ( ) Shared Service IOC FY15-19 Savings FACILITIES 1 OCT 13 $537 M MEDICAL LOGISTICS 1 OCT 13 $189 M HEALTH IT 1 OCT 13 $265 M HEALTH PLAN 1 OCT 13 $456 M PHARMACY 1 OCT 13 $1,224 M CONTRACTING 1 MAR 14 $136 M BUDGET & RESOURCE MGMT 1 FEB 14 $279 M MEDICAL RESEARCH & DEV 1 JUN 14 $98 M MEDICAL EDUCATION & TNG 10 AUG 14 $ 5 M PUBLIC HEALTH 1 OCT 14 $293 M TOTAL $3.482 BILLION 22
23 FY 2014 Shared Service Savings: Covered DHA Initial Investment The DHA has achieved cost savings and paid for initial investments in FY 2014, resulting in net savings of approximately $236 million. 23
24 Shared Services FOC Criteria Developed through MHS Gov (Future Shared Services Team) Criteria Met 1. The military Services agree they are receiving the services as agreed in the Coordinated Concept of Operations (CCONOPS). The Shared Service has a mechanism (working group, committee, etc.) to elicit feedback from Services and to communicate with the Services. 2. For product line or initiative (one entry for each) as agreed to in the (CCONOPS), the Shared Service has work underway and is actively managing actions associated with this product line or initiative. 3. The Shared Service has received the resources identified in the CCONOPS, or resources have been sufficiently programmed to carry out the operation of this Shared Service 4. The Shared Service developed performance metrics to help manage actions, report progress, identify gaps, and identify areas for improvement 5. There is no substantive change required to the CCONOPS of the Shared Service 6. The Shared Service has a vision and mission statement 24
25 DHA 2 nd Year Focus Areas Achieve DHA FOC NLT 1 OCT 2015 Transition 10 Shared Services from IOC to FOC Assess the 11 th Shared Service and beyond Centers of Excellence and Executive Agents Sustain/Monitor efforts to achieve FY15-19 savings of $3.482B Develop & Sustain an MHS Performance Management System to drive MHS system-wide continuous improvement improving quality and safety where needed Enable DoD s Electronic Health Record Modernization Institute the Next Generation TRICARE Health Plan (T-2017) Institute an integrated DHA Acquisition Structure Conduct DHA Manpower Assessments to properly align resources Introduce a common cost accounting structure 25
26 Mr. John A. Becker Director, Facilities Division Facilities Medically Ready Force...Ready Medical Force 26
27 Facilities Shared Service Full Operating Capability (FOC) Status: FOC effective 3 March 2015 Governance Model: Collaborative enterprise management in coordination with Services providing integrated world-class Health Facility Life Cycle Management (FLCM) for the Military Health System MHS Governance Structure: Health Facilities Coordinating Council (HFCC) and Medical Business Operations Group (MBOG) BLUF: In close collaboration with the Services and Design/Construction Agents, DHA Facilities is improving FLCM through standardization, improved processes, and implementation of a Company Operating Model (CONOPS) Highlights: (1) Standardized demand signal and prioritization process for MilCon requirements (2) Standardized Sustainment, Restoration, and Modernization programming models (SRM) (3) Standardized IO&T programming model (4) DHA Facilities support to e-msms for future capital requirements Challenges: (1) Reacting to and accommodating impact of external forces on long lead time MilCon planning, programming, and budgeting. (e.g. Force Structure changes, mission changes. etc.) (2) Modernization and replacement of an aging inventory 27
28 Facilities Shared Service BCA and Performance Measures Area / Type Measure Reporting Frequency Notes on Current Status Current Status Expected Completion Date Cost / BCA Savings achieved vs. savings projected Annually Re-baseline savings to PB15 funding levels and revalidation of costs in progress FY14 Q2 Quality / BCA Facility Condition Index (3 Year Implementation) Quarterly Measures levels of requirements in DMLSS-FM relative to facility replacement value; Builder implementation complete in FY17 FY14 Q2 Quality / BCA Facility Functionality Index Quarterly Builder system implementation reflects facility functionality related to accreditation (safety, req d spaces, adjacencies) FY15 Q3 Quality / BCA Asset Productivity Index Quarterly Expanding portfolio management to include productivity data linked to facilities FY15 Q3 Cost / Perf Measure % of projects performed within cost & schedule Monthly Program oversight data and targets established by & reviewed monthly with Agents & Services FY14 Q3 Quality / BCA Customer Satisfaction Survey with facility environment of care Quarterly TRISS Reports reflect patient experience of cleanliness and quietness of hospital environ FY15 Q1 Under development Developed, but no baseline Baseline exists, but no target Baseline and targets exist Reporting data against targets 28
29 Facilities Shared Service BCA Costs and Projected Savings FY14-19 Projected Net Savings with FY14 Actuals Data Reviewed by the MBOG: 25 Feb 15 *FY13 YE bought ahead $40M in Implementation Costs Actual: $(4.63) FY14 - $311M IO&T Savings for MHS Redistribution 29
30 CAPT Bernie Poindexter Director, Logistics Division Medical Logistics Medically Ready Force...Ready Medical Force 30
31 Medical Logistics (MEDLOG) Shared Service Status: FOC effective 3 March 2015 Governance Model: Corporate management and compliance oversight of joint MEDLOG initiatives related to medical supply, equipment, and services MHS Governance Structure: Defense Medical Logistics Proponent Committee (DMLPC) and Medical Business Operations Group (MBOG) BLUF: In close collaboration/coordination with the Services and DLA, DHA MEDLOG is taking cost out of the medical supply chain by eliminating waste (price, excess inventory, and process) and reducing unwarranted variation through strategic sourcing and standardization Highlights: (1) Improved ordering compliance for 1,415 standardized products (2) growing e-commerce solutions for provider preference items at significant discounts (3) Healthcare Technology Joint Requirements Assessments (JRA) for the emsms (NCR planned for May 15) and (4) MEDLOG Support for NCR-MD Challenge: Medical Device (60,000+ across MHS) compatibility (interoperability and integration) with the EHR 31
32 MEDLOG Shared Service BCA and Performance Measures Area / Type Measure Reporting Frequency Notes on Current Status Current Status Expected Completion Date Cost Gross Savings Quarterly As of 31 Jan 2015: FY 14: Actual gross savings = $24.32M FY 15 Q1: Projected gross savings = $7.21M Completed Cost Use of Incentive Agreements (Formerly % of Procurement of Standardized Products) Quarterly Quarter 1 Quarter 2 Quarter 3 Quarter 4 FY 14: 77.2% 79.4% 80.8% 81.2% Completed FY 15: 83.9% Quarter 1 Quarter 2 Quarter 3 Quarter 4 Cost Use of ecommerce Quarterly FY 14: 68% 67% 67% 70% FY 15: 72% Cost Total Joint Requirements Assessment Cost Savings Annually Reported Annually Metrics Available Q2 FY15 Pending Cost Total Cost Savings from Equipment Group Purchases Annually FY 14 Army Air Force Navy NCR MD $5.15M $3.18M $.79M $1.06M $0.096M Completed Cost DoD Service Contracts Annually Reported Annually Metrics Available Q2 FY15 Pending Cost Maintenance Contract Costs to Acquisition Cost Ratio Annually Reported Annually Metrics Available Q2 FY15 Pending Quality Average Age of Equipment in DoD Inventory Annually Reported Annually Metrics Available Q2 FY15 Pending Under development Developed, but no baseline Baseline exists, but no target Baseline and targets exist Reporting data against targets 32

 13.86 15.53 22.29 31.26 36.29 43.61 50.55 197.86 Savings ($M) 0.00 5.15 4.47 11.77 16.51 17.75 18.")
33 MEDLOG Shared Service FY 14 Savings vs POM Submission $19.92 Actual FY 14 Annual Net Savings BCA Category FY14 FY14 Realized FY15 FY16 FY17 FY18 FY19 Total *Additional savings through cost avoidance are to be reinvested within the Shared Service Primary Drivers of Implementation Costs Savings ($M) IT investment (RDT&E) Supplies Cost ($M) Health Care Technology Services GRAND TOTAL NET SAVINGS RTC Savings Projections Net Savings ($M) Savings ($M) Cost ($M) Net Savings ($M) Savings ($M) Cost ($M) Net Savings ($M) Annual ($M) Cumulative ($M) Annual ($M) Cumulative ($M) IT investment (RDT&E) Contractor support (O&M) TDY Funding (O&M) 33 33
34 Dr. George E. Jones, Jr. Chief, Pharmacy Operations Division Pharmacy Medically Ready Force...Ready Medical Force 34
35 Pharmacy Shared Service Full Operating Capability (FOC) Status: FOC effective 3 March 2015 Governance Model: Corporate management and compliance oversight of Pharmacy initiatives related to all aspects of pharmacy benefit delivery MHS Governance Structure: Pharmacy Work Group (PWG) and Medical Operations Group (MOG) BLUF: A collaborative effort with the Services to reduce unwarranted variation through deliberate planning and consistent messaging and measurement of pharmacy delivery Highlights: (1) Implemented three successful initiatives in FY14 - $215M savings (2) Enhanced communication with quarterly world-wide pharmacy webinars (3) Fully deployed MTF capability to accept electronic prescriptions from community providers (4) Developed and implemented with the Services a uniform process for prescription transfers (5) Supporting pharmacy within and across emsms Challenge: Managing impact of external forces on program execution (e.g. New Drugs; Trends in therapy compounding; Drug shortages) 35
36 The MHS Spent $8.06B on pharmacy related expenditures in FY14; however, we would have spent $8.28B if not for specific initiatives undertaken by DHA Pharmacy Why have pharmacy costs increased despite pharmacy s cost saving initiatives? Specialty Drugs Cost ~$121M 1 This issue is not unique to the MHS; spending on specialty drugs increased by 14.1% and 14.7% in the commercial health industry and Medicare respectively in Compounds Cost ~$512M 3 Compound spending has increased throughout the industry; Express Scripts International, the largest pharmacy benefits manager, reported that its quarterly spending on compounds increased over 500% from 2012 to 2014 (from $28M to $171M per quarter) 4 Without pharmacy s cost saving initiatives, the enterprise would have spent an additional $215M in FY14 Channel Management (TFL Pilot) Saved $74.8M Formulary Management Saved $100.3M Compliance to Purchasing Rules Saved $39.9M We spent: $8.06B Instead of: $8.28B 36 36
37 Pharmacy Shared Service BCA and Performance Measures # Area / Type Measure Reporting Frequency Notes on Current Status Current Status Expected Completion Date 1 Cost 2 Cost 3 Cost 4 Cost Maintenance medication refills filled at all points of service with the ability to drill down to the Enhanced Multiservice Market Level (emsm) and by distribution of enrollment status MTF, retail, and mail order market share overall with the ability to drill down to the emsm level and by distribution of enrollment status The percent of pharmacy spend directed to the retail point of service Net pharmacy cost to government per member per month (PMPM) at the emsm level Quarterly - Complete Quarterly - Complete Quarterly - Complete Quarterly - Complete 5 Cost Percentage of drugs purchased as generic when generic is identified as a preferred agent, per MTF outpatient pharmacy Monthly - Complete 6 Cost Percentage of compliance with purchasing drugs via national contracts, per MTF outpatient pharmacy Monthly - Complete Under development Developed, but no baseline Baseline exists, but no target Baseline and targets exist Medically Ready Force Ready Medical Force Reporting data against targets 37
38 Dollars (in Millions) Pharmacy Shared Service FY Savings vs POM Submission $2,000 Risk- and Inflation-Adjusted Projected Savings, FY14-19 $1,500 $1,000 $500 Annual ($M) Cumulative ($M) Actual FY14 Annual Net Savings $- BCA Category FY14 #1: Phase I: Eliminate Retail Refills #2: Phase II: Eliminate Retail Refills, Optimize MTF Capacity #3: Enable MTF compliance to Pharmacy s centralized drug purchasing rules FY14 FY15 FY16 FY17 FY18 FY19 FY14 Realized FY15 FY16 FY17 FY18 FY19 Total Savings ($M) $ $74.8 $ $ $ $ $ $4, Cost ($M) $ $0.00 $ $ $ $ $ $4, Net Savings ($M) $93.00 $74.8 $ $ $ $ $ $ Savings ($M) $0.00 $0.00 $0.00 $13.19 $26.88 $41.18 $56.11 $ Cost ($M) $0.00 $0.00 $0.00 $7.39 $15.06 $23.06 $31.43 $76.94 Net Savings ($M) $0.00 $0.00 $0.00 $5.80 $11.82 $18.12 $24.68 $60.42 Savings ($M) $8.00 $39.9 $16.22 $24.75 $33.63 $42.92 $43.86 $ Cost ($M) $0.62 $0.00 $0.63 $0.64 $0.65 $0.67 $0.68 $3.90 Net Savings ($M) $7.38 $39.9 $15.59 $24.11 $32.97 $42.25 $43.18 $ Primary Drivers of Implementation Costs New drug costs at Home Delivery and MTF outpatient pharmacies New drug costs at Home Delivery and MTF outpatient pharmacies Personnel needed to implement the enabling IT solution Table continues on next slide.
39 Pharmacy Shared Service FY Savings vs POM Submission (cont.) BCA Category FY14 #4: DoD Pharmacy & Therapeutics Committee (P&T Committee) formulary management #5: Suspend coverage of newly approved FDA drugs #6: Centralize pharmacy automation contracts FY14 Realized FY15 FY16 FY17 FY18 FY19 Total Savings ($M) $60.00 $100.3 $60.84 $61.87 $63.05 $64.37 $65.79 $ Cost ($M) $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 Net Savings ($M) $60.00 $100.3 $60.84 $61.87 $63.05 $64.37 $65.79 $ Savings ($M) $0.00 $0.00 $4.06 $8.25 $8.41 $8.58 $8.77 $38.07 Cost ($M) $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 Net Savings ($M) $0.00 $0.00 $4.06 $8.25 $8.41 $8.58 $8.77 $38.07 Savings ($M) $0.10 $0.00 $6.69 $6.81 $6.94 $1.61 $1.64 $23.79 Cost ($M) $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 Net Savings ($M) $0.10 $0.00 $6.69 $6.81 $6.94 $1.61 $1.64 $23.79 Primary Drivers of Implementation Costs To be determined; implementation costs unknown at this time To be determined; proposed pharmacy regulation To be determined; implementation costs unknown at this time #7: Implement a System of Satellite MTF Pharmacy Locations GRAND TOTAL NET SAVINGS Savings ($M) $0.00 $0.00 $0.00 $0.03 $0.05 $0.07 $0.11 $0.26 Cost ($M) $0.00 $0.00 $0.00 $0.09 $0.02 $0.03 $0.05 $0.19 Net Savings ($M) $0.00 $0.00 $0.00 -$0.06 $0.03 $0.04 $0.06 $0.07 Annual ($M) $ $215.0 $ $ $ $ $ $1, Cumulative ($M) $ $215.0 $ $ $ $1, $1, To be determined; implementation costs unknown at this time 39 39

40 Metric #5 Percent Generic: Tracked Drugs 40 40
41 Metric #6 National Contract Compliance 100% Air Force Army Navy Overall 80% 75.1% 86.7% 60% 40% 20% 0% Sep-13 Oct-13 Nov-13 Dec-13 Jan-14 Feb-14 Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14
42 Outpatient Compound Costs Fraud Investigations Multiple PI investigations ongoing 42
43 Mr. David M. Bowen Director, Health Information Technology Health Information Technology 43
44 Health Information Technology (HIT) BLUF / Challenges / Wins BLUF: HIT has an all-in approach unique from other Shared Services. HIT is working towards Full Operating Capability (FOC) 1 Oct 2015 Challenges: (1) Managing cultural change TMA and Services had distinct processes (2) Standardizing the HIT infrastructure eliminating duplicative applications (3) Disrupting historical HIT funding and approval processes (4) Upgrading IT infrastructure necessary to support the Electronic Health Record (5) Establishing/maintaining the trust of our customers that we ll do this right! Wins: (1) Two huge efforts: HIT stand-up and EHR support we haven t broken anything! (2) FY14 exceeded business case by $54 million, FY15 - saved $20M to date (3) Developed and implemented metric reporting system for 90-day review actions (4) Established financial processes; gaining visibility in MTF IT spend/contracts Medically Ready Force Ready Medical Force 44
45 Health Information Technology Key Measures Area/Type Measure Reporting Frequency Notes on Current Status Current Status Expected Completion Date BCA Savings Shared Services Savings Achieved Monthly Previously reported savings achieved in FY14 was $39.19M and has been revised to $29.50M to reflect execution emerging requirements Currently Reporting Cost Total IT costs as a percentage of MHS budget Percentage of IT spending allocated to delivering new capabilities Annually Annually DHP including EHR and excluding purchased care. FY14 Budget-based Baseline=11%. Future Years Target = 15%. Actual Execution FY14 = 11 % FY14 Budget-based Baseline= 14%. Future Years Target = 29%. Actual Execution FY14 = 14 % Currently Reporting Currently Reporting Speed Percentage of software products deployed on time Quarterly Quarterly reporting based on Annual Performance Plan (APP) deployment data. Target set at 82% for FY15. Actual deployment percentage for FY15 Q1 was 83%. Currently Reporting Quality Percentage of systems meeting system availability standards Quarterly Quarterly reporting based on APP system availability standards and data, Target set at 90%. Actual percentage of systems that met their availability targets for FY15 Q1 was 80%. Currently Reporting Strategic Alignment Alignment of IT with MHS strategic objectives Annually Preliminary alignment to draft MHS objectives completed. Dependency: Final published MHS objectives Ongoing refinement Customer Service Executive Satisfaction with overall HIT Directorate performance Quarterly Third Executive Satisfaction Survey Q4 Survey was completed in January 2015 due to scheduling delays Currently Reporting Under development Developed, but no baseline Baseline exists, but no target Baseline and targets exist Reporting data against targets 45

46 Health Information Technology FY14 Savings vs FY15-19 Projected Savings Funding will need to be provided each year in order to produce net savings in FY16, and reach annual steady-state net savings in FY19. Adjusted FY16-20 Actual FY14-15 Annual Net Savings Break-even Steady state BCA Category FY14 FY14 Realized FY15 FY15 Realized FY16 FY17 FY18 FY19 Total Primary Drivers of Implementation Costs #1: Reengineering of IT Management #2: Infrastructure Consolidation #3: Portfolio Rationalization GRAND TOTAL NET SAVINGS Savings ($M) Cost ($M) $3.31 $4.37 $3.80 $0.00 $5.67 $2.58 $0.00 $0.00 $5.77 $2.10 $5.88 $2.14 $6.00 $2.18 $6.13 $0.00 $32.76 $13.37 IT costs to invest in tools (portfolio management, EA) needed to support and automate reengineered business processes. Net Savings ($M) ($1.07) $3.80 $3.09 $0.00 $3.67 $3.74 $3.82 $6.13 $19.38 Savings ($M) $3.05 $18.76 $6.19 $0.00 $14.68 $16.56 $16.91 $74.71 $ Contract support for transition planning and PMO (e.g., product line analysis, Cost ($M) $0.00 $13.78 $17.53 $0.00 $13.63 $28.85 $31.64 $0.00 $91.65 scheduling, risk management). IT costs for product line consolidation Net Savings ($M) $3.05 $4.98 ($11.34) $0.00 $1.05 ($12.29) ($14.73) $74.71 $40.45 (e.g., additional servers, storage, bandwidth). Savings ($M) $0.00 $20.72 $21.33 $0.00 $40.24 $66.21 $67.60 $69.08 $ IT costs for decommissioning and promotion of system to enterprise level Cost ($M) $23.98 $0.00 $24.32 $0.00 $32.97 $0.00 $0.00 $0.00 $81.27 (e.g., migrating/archiving data, increasing capacity of target system, hardware Net Savings ($M) ($23.98) $20.72 ($2.99) $0.00 $7.27 $66.21 $67.60 $69.08 $ disposal, training, change management, BPR). Annual ($M) ($22.00) $29.50 ($17.38) $0.00 $11.12 $56.48 $55.86 $ $ Cumulative ($M) ($22.00) $29.50 ($39.38) $0.00 ($28.26) $28.22 $84.08 $
47 CAPT Edward Simmer Deputy Chief, TRICARE Health Plans TRICARE Health Plan Medically Ready Force...Ready Medical Force 47
48 TRICARE Health Plans Shared Services BLUF / Challenges / Wins BLUF: (1) Goal: To fully integrate purchased care and direct care systems On schedule to achieve FOC 1 Aug 2015 Challenges: (1)Sole source contract extension in North limits ability to negotiate changes(2) Statutory/regulatory limitations on innovation Wins: (1) Integrated Services into T-2017 and T-20xx development, making them full partners in this process(2) TRICARE Service Center closure completed with no negative impact on customer satisfaction(3) Other Health Insurance centralized initiative about to launch(4) Established mission essential metrics focused on access, safety, readiness 48
49 Close TRICARE Service Centers (TSC) Transition Health Plan Progress Update Complete On Schedule At Risk of Missing Suspense Overall Status: Milestone Indicator Suspense Revised Suspense Completed Complete organization review of functions with Office of Strategy Management 15 Jul 14 Develop unit manning document IAW guidelines (org review started) 1 Oct 15 Develop/update position descriptions 1 Oct 15 Inventory contracts and begin identifying opportunities for rationalization for requirements 1 Oct 15 Implement performance plans aligned to organizational goals 31 Mar 14 Develop plan and metrics to monitor closure of the TRICARE Service Centers (TSC) 1 Aug Aug Jun 14 Provide quality / satisfaction data on TRICARE call centers 1 Aug Dec Jun 14 Issuance of contract modifications 29 Nov Nov Nov 13 Conclusion of Contract Negotiations 4 Mar 15 TBD Enhance Beneficiary Web Enrollment (BWE) functionality 30 Sept Mar 15 49
50 Other Health Insurance (OHI) Health Plan Progress Update (Continued) Complete On Schedule At Risk of Missing Suspense Overall Status: Milestone Indicator Suspense Revised Suspense Completed Develop PWS and Market Research 1 Oct Mar Mar 14 Document and deploy DEERS changes - New or revised reports - Technical specifications for data files Modify OHI business processes - MCSC processes - Direct Care processes - Pre-ABACUS - Post-ABACUS Award DMDC Task Order Contract and implement OHI discovery - Award of task order - Phase-In activities Award DHA Contract and implement OHI discovery - Award of task order - Contract protest - Phase-In activities 1 Apr Mar 14 1 Feb 14 1 Apr Mar 14 1 Apr 14 1 May Apr Sept 14 3rd Qtr FY15 50
51 Health Plan BCA Costs and Cost Avoidance 51
52 Health Plan BCA Costs and Projected Cost Avoidance BCA Category FY14 FY15 FY16 FY17 FY18 FY19 Total Savings ($M) #1 TSC: Cost ($M) Primary Drivers of Implementation Costs Contract-related costs #2 OHI: Net Savings ($M) Savings ($M) ** Cost ($M) Contract-related costs Net Savings ($M) GRAND TOTAL Annual ($M) NET SAVINGS Cumulative ($M) RTC PROJECTION Annual ($M) Cumulative ($M) /- FROM RTC PROJECTION Annual ($M) Cumulative ($M) *Risk-Adjusted Net Savings ** May be adjusted up for FY15 once OHI collection begins. As of 4 Mar
53 Mr. Robert Moss Budget & Resource Management Division Budget & Resource Management 53
54 Budget & Resource Management BLUF / Challenges / Wins BLUF: (1) Automated Third Party Billing and collection capability by 1 July 2015 (2) Standardize medical record coding policies/procedures for all three Military Services by 31 Mar 2015 (3) Initial implementation of common cost accounting structure by 1 Oct 2015 Challenges: (1) Operating billing and collection services as we transition to the DISA directed cloud environment (2) Development of common cost accounting structure with three distinct Military Services accounting systems (3) Transitioning to HIPAA-compliant remote medical record coding capability Wins: Services total cooperation in developing single billing/collection capability and unanimity in medical record coding policies/procedures 54
55 Establish Medical Coding Program Office Implement Joint Billing Solution (ABACUS) Implementati on of Common Cost Accounting Structure Budget and Resource Management Product Line Progress Complete On Schedule At Risk of Missing Suspense Milestone Indicator Suspense Revised Suspense Completed Award a contract for implementation support of CCAS Jun 14 - Jun 14 Initial implementation of CCAS with the services Jan 15 May 15 - Full implementation and operation of CCAS Sep Award of ABACUS contract Jan 14 - Jan 14 Deployment of ABACUS Outpatient Third Party Collections (TPC) Module (ATO 5 Mar 15) Deployment of ABACUS Inpatient TPC Module (ATO 5 Mar 15) Jun 14 Jun 15 - Sep 14 Jun 15 - Establish Coding Working Group with approved charter Oct 14 - Oct 14 Establish draft remote coding CONOPS to coordinate with HIT/DHSS Develop single DoDi guidance (Draft) on Medical Services Documentation, Coding, and Compliance Dec 14 TBD - Mar Finalize and implement approved single DoDi guidance Mar 15 Oct 15 - Develop a DHA Central IDIQ contract Sep 15 TBD - Requires back-up slide for explanation of risk and way ahead 55
 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 Contract support Cost ($M) $1.04 $1.04 $0.00 $0.00 $0.00 $0.00 $0.00 $1.04 Net Savings ($M) ($1.")
56 Budget and Resource Management FY Reimbursements vs POM Submission BCA Category FY14 Implementation of a Common Cost Accounting Structure FY14 Realized FY15 FY16 FY17 FY18 FY19 Total Primary Drivers of Implementation Costs Savings ($M) $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 Contract support Cost ($M) $1.04 $1.04 $0.00 $0.00 $0.00 $0.00 $0.00 $1.04 Net Savings ($M) ($1.04) ($1.04) $0.00 $0.00 $0.00 $0.00 $0.00 ($1.04) Implementation of a Joint Billing Solution (ABACUS) GRAND TOTAL NET REIMBURSEMENTS Reimbursements ($M) $6.02 $0.00 $43.65 $58.84 $59.95 $61.21 $62.56 $ Contract Support Cost ($M) 1,2,3 $19.83 $19.83 $15.27 $15.85 $15.64 $14.77 $11.76 $93.12 Net Reimbursements ($M) ($13.81) ($19.83) $28.38 $42.99 $44.31 $46.44 $50.80 $ Annual ($M) ($14.85) ($20.87) $28.38 $42.99 $44.31 $46.44 $50.80 $ Cumulative ($M) ($14.85) ($20.87) $13.53 $56.52 $ $ $ Initial investment costs at IOC were $6.89M due to procurement sensitivity of ABACUS; Upon award, ABACUS investments costs were $79.265M (O&M funded, Program Mgmt, Information Assurance), as detailed in the ABACUS Briefing for Lt Gen Robb dated 2 April Additional lifecycle costs were $5.47M, as detailed in the DHSS ABACUS IPR Final briefing dated 17 June Additional costs to sustain TPOCs due to ABACUS delays (3 mths FY14 and 12 mths FY15) on 18 Nov
57 Mr. Eric Thaxton Deputy Director of Acquisition Division for Procurement Procurement/Contracting 57
58 Contracting BLUF / Challenges / Wins BLUF (1) Contracting shared service strives to generate efficiencies through strategic sourcing of common requirements. (2) On Schedule to achieve Full Operating Capability 1 Oct 2015 Challenges: Moving toward strategic sourcing while executing non strategic requirements Wins (1) Enhanced Operating Model implementation 1 April; includes 101 improvement initiatives in Product Lines 1 and 2 (2) Agency wide contract data call completed; establishes demand signal rationalization process (3) Cost savings of $12.75M in personnel implementation costs 58
59 Contracting Shared Service Performance Metrics* # Metric Description 1 2 Savings attributed to DoD strategic sourcing strategies Savings attributed to developing centralized strategic sourcing solutions for Q services^ Cost of services/supplies obtained in baseline minus strategically sourced services/supplies Savings achieved in key markets (Colorado Springs, Washington State, San Antonio) through use of strategic sourcing solutions for Q services Reporting Frequency Bi-Annual Bi-Annual Current Status Status Notes Savings will not be generated until after DHA MATOs for Q and R services are awarded in FY17 and workload migrates in FY18 Savings will not be generated until after DHA MATO for Q services are awarded in FY17 and workload migrates in FY18 Expected Completion Date Q1 FY19 Q1 FY19 3 Savings attributed to utilizing existing strategic sourcing solutions for R services Savings achieved across Services' and former TMA R services R services portfolio categorized according to extent of competition prior to contract award. Bi-Annual Savings will not be generated until after DHA MATO for R services are awarded in FY17 and workload migrates in FY18 Q1 FY Savings attributed to "ordering windows (e.g., IT hardware purchases) Savings achieved through vendor base management Savings achieved by specifying timeframe in which orders can be placed for certain goods or services Savings achieved from strategically managing vendor base to eliminate passthroughs and drive down overhead costs Bi-Annual Bi-Annual D service MATO to be awarded in FY16 will establish quarterly ordering windows for IT hardware; workload will migrate in FY17 D service MATO to be awarded in FY16 will be the first opportunity for managing the vendor base to generate savings; workload will migrate in FY17 Q1 FY18 Q1 FY18 Under development Developed, but no baseline Baseline and targets exist Reporting data against targets *As outlined in CONOPS and Third Report to Congress. The five priority metrics presented here are under developed since IOC as they provide important early indicators of savings realized from Contracting shared services. Efficiencies will be baselined after the establishment of DHA Sourcing Strategies. Other metrics will be developed and tracked after IOC in a phased approach. ^Q Services savings metric timeline revised based on resource challenges and Service equities that impacted Service-level strategic MATOs. Medically Ready Force...Ready Medical Force 59
60 60
61 Contracting Shared Service Revised BCA Costs & Projected Savings Annual Projected Savings, FY14-20, Risk & Inflation Adjusted Cumulative Projected Savings, FY14-20, Risk & Inflation Adjusted $100 $50 $ -$50 -$1.43 -$1.51 $ $2.66 -$2.75 $2.48 $21.38 $19.86 $79.54 $59.93 $84.88 $200 $100 $ -$100 -$2.79 -$4.22 -$5.73 $ $2.66 -$5.41 -$2.93 $26.57 $16.93 $ $76.86 $ Rebaseline Annual Savings ($M) Original BCA Annual Savings ($M) Rebaseline Cumulative Savings ($M) Original BCA Cumulative Savings ($M) Acquisition Planning and Program Management Execution, Management, and Administration Enabler: Legal Support Opportunity FY14 FY15 FY16 FY17 FY18 FY19 FY20 Cumulative Initiative 1: Develop or identify Q Services strategic MATOs for the Initiative 2: DHA R Services Annual Savings Annual Costs Annual Net Savings Initiative 3: Establish "ordering windows" Initiative 4: Strategically manage vendor base Annual Savings Annual Costs Annual Net Savings Initiative 5: Decouple Compensation ceiling under Title Annual Savings Annual Costs Annual Net Savings Annual New Manpower Costs Total Annual Savings Total Annual Costs Net Savings Medically Ready Force...Ready Medical Force 61
62 RADM Bruce A. Doll Director, Research, Development & Acquisition Research, Development and Acquisition Directorate 62
63 BLUF / Challenges / Wins BLUF RDA is working towards Full Operating Capability (FOC) On schedule to achieve FOC 1 Oct 2015 Challenges Finalized organizational structure Predictability of funding Wins Advanced Development (AD) Concept of Operations (CONOPs) completed Initial Metrics Identified, baselines being collected Strategic Plan drafted Medically Ready Force...Ready Medical Force 63
64 Research and Development: Objectives Alignment Strategy Map Objectives Alignment Objectives Supported High Level Initiatives Supporting Initiatives IP2: Improve Operational Medicine IP3: Enhance Emerging Medical Capabilities in a Joint Environment IP4: Enhance Strategic Partnerships OC3: Optimize DHA as a Support Organization Combat Casualty Care Research Military Operational Medicine Research Hemorrhage Control and Resuscitation Program Combat Casualty Care Training Initiative Traumatic Brain Injury (TBI) Diagnosis R&D Forward Surgical Care Initiative Enroute Care research Suicide Prevention R&D Family and Community Health R&D Post Traumatic Stress Disorder (PTSD) prevention R&D Advance Medical Modeling and Simulation Collaborative Medical Modeling and Simulation R&D Enhance Research Related Strategic Partnerships Research and Development FOC Initiatives NATO engagement Armed Serviced Biomedical Evaluation and Management Committee (ASBREM) Initiatives National Research Action Plan Joint DoD-VA Review and Analysis Clinical Investigation Programs Protections Program Structures Clinical Registries Briefing Date: XX Feb
65 RDA Directorate Key Measures Area Management Question Measure Current Status Notes on Current Status Target Date to Begin Development Expected Completion Date Cost Are we maximizing the amount of research for dollars invested? Direct research dollars for total dollars spent. BCA reinvestment initiative underway Initiation of improved cost activity accounting. September 2014 Ongoing Schedule Can we speed the development and transition of research products? Institutional Review Board/Human Research Protection approval time for multi-site clinical research trials. Average time from program solicitations to award. RDA Human Research Protections and Clinical Investigations Program Working Group underway. Baselining Awards Process. Technology Transfer Improvements underway. September 2014 Annual Progress Review (October each year) Performance Are we getting the knowledge and material products we need from our RDA investment? Number of clinical trials completed. Number of products making it to Milestone Decisions. Number of fielded products (Clinical Practice Guidelines, commercial products, etc.). Advanced Development (AD) structure being implemented, Joint Program Committee tracking of outcomes underway. Armed Services Biomedical Research Evaluation Management (ASBREM) COI improving multi-agency research efforts. September 2014 Annual Progress Review (October each year) Under development Developed, but no baseline Baseline exists, but no target Baseline and targets exist Reporting data against targets 65
66 RDA Business Process Rengineering Current Status Net Savings Achieved to Date: None Status Summary: Implementation in FY 15 Next Steps Owner Status Suspense Revised Suspense Capability & Capacity Analysis Redirection of Extramural Funding Advanced Development Improvement Research Protections & Multi-Site Clinical Trials Risks and Issues Need to monitor costs to realize projected cost reinvestments Missed Original Suspense Overall Status: Complete On Schedule At Risk of Missing Suspense RDA Directorate RDA Directorate RDA Directorate RDA Directorate Sept 2014 Nov 2014 Oct 2015 Feb 2015 Oct 2015 June
67 Research, Development & Acquisition Projected Reinvestment Reinvestment Initiatives Redirection of Extramural Funding Estimated Reinvestment ($M) FY14 FY15 FY16 FY17 FY18 FY19 Cumulative Annual Reinvestment Annual Costs Annual Net Reinvestment
68 Progress Update Task Forces recommendations on: Centers of Excellence Advanced Development (AD) Clinical Infrastructure / Regulatory & Laboratories AD CONOPs completed Shared Service Working Group ongoing efforts Initial Metrics Identified, baselines being collected Strategic Plan drafted 68
69 Brig Gen (Dr.) Robert I. Miller Director, Education and Training Medical Education & Training 69
70 Education & Training (E&T) BLUF / Challenges / Wins BLUF E&T is working towards Full Operating Capability (FOC) by 1 Oct 2015 Focus on quality E&T, but cost savings expected - Learning Management System (LMS) and Modeling & Simulation (M&S) Challenges Limited DHHQ staff but increased partnering opportunities Medical Education & Training Campus (METC) a work in progress Wins Allignment of METC, Defense Medical Readiness Training Institute (DMRTI), Joint Medical Executive Skills Institute (JMESI) under E&T Directorate Single Learning Management System (Joint Knowledge Online) METC bridge programs and future academic affiliation with Uniformed Service University (USU) - Train for the Mission Educate for a Lifetime 70
71 Learning Management Systems Savings ($M) Modeling & Simulation Savings ($M) Education & Training FY14-19 Projected Savings & Implementation Costs The projected potential savings are estimated to be $7.79M from FY14 to FY19. Summary of LMS Savings* ($M) $3.00 $2.50 $2.00 $1.50 $1.00 $0.50 $- $(0.50) FY14 FY15 FY16 FY17 FY18 FY19 $(1.00) $(1.50) FY14 FY15 FY16 FY17 FY18 FY19 $6.00 $5.00 $4.00 $3.00 $2.00 $1.00 $0.00 Summary of M&S Net Savings ($M) FY14 FY15 FY16 FY17 FY18 FY19 FY14 FY15 FY16 FY17 FY18 FY19 Net Savings (Annual) $(0.03) $(0.87) $1.06 $0.95 $0.85 $0.77 Net Savings (Annual) $0.00 $0.00 $0.00 $1.05 $1.55 $2.47 Net Savings (Cumulative) $(0.03) $(0.90) $0.16 $1.11 $1.96 $2.72 Net Savings (Cumulative) $0.00 $0.00 $0.00 $1.05 $2.60 $5.07 Gross Savings FY14-19 Implementation Cost Net Savings Return on Investment** $3.62M $0.90 $2.72 ~3:1 Gross Savings Implementation Cost FY14-19 Net Savings Return on Investment** $5.07M $0*** $5.07M N/A** *Subset of HIT swg Portfolio Rationalization BCA; E&T will not formally track these savings **ROI calculated as [Net Savings/Implementation Costs] : 1 71


 Operational Training (DMRTI) Leadership Development Continuum (initial-")


72 Education & Training Organizational Chart at FOC Secretary of Defense USD (P&R) ASD (HA) Defense Health Agency Director Education and Training Director Authority, Direction and Control Coordination Policy Development Policy Execution Healthcare Inter-service Training Office (HC-ITO) *** - Facilitate training review process Military Medical Education Consortium Coordinated affiliations to facilitate the delivery of quality instruction USU* CCAF* Civilian Partners NMETC ** AMEDD C&S ** AETC/SGU ** METC DMRTI JMESI * Consortium Partners ** Consortium Partners and E&T Delivery platforms *** E&T Directorate in coordination role Professional Development, Sustainment and Program Management Graduate Med/Den Education*** MHS Leader Development (JMESI) Operational Training (DMRTI) Leadership Development Continuum (initial- Sustainment)*** Officer/Enlisted/Civilian Professional Development*** Program Standardization/ Reciprocity*** Academic Review and Policy Oversight Academic Metrics Policy and Compliance Training Agreement Management Strategic Planning Learning Modalities elearning (Learning Management System) Modeling & Simulation Regulatory Administrative Support Conference/CE/Certification approval and attendee package processing Tuition Payments/Student support CE Credit Granting JGMESB Coordination Centralized credentialing for LIP Other functions as determined by DHA E&T analysis 72
73 Education & Training Shared Service Deliverables Deliverable Measure Reporting Frequency Notes on Current Status Status Expected Completion Date #1 Align Medical Education and Training Campus to DHA E&T N/A Action Complete. METC funds transfer to DHA in FY17. FY15 #2 Align Joint Medical Executive Skills Institute to DHA E&T N/A Action Complete. JMESI funds transfer to DHA in FY17. FY15 #3 Align Defense Medical Readiness Institute to DHA E&T N/A Action Complete. DMRTI funds transfer to DHA in FY17. FY15 #4 One - Stop Learning Management System Semiannually Migrate 11 of 11 Legacy LMSs to JKO by FY18 - JMESI migration complete Dec 14 - MHS Learn migration / EDC Jun 15 FY18 #5 MHS Leadership Training Quarterly Determine standardized MHS leadership curricula development - Draft leadership curricula complete/services approved (Joint Medical Executive Skills Institute / Dr. Durica) FY17 #6 Award Degrees Semiannually Develop METC/USUHS Academic Affiliation - Meetings conducted w/key stakeholders, SEAs & DoD decision authorities; momentum steady - Unified Legislative Budget request in coordination FY17 Complete On Schedule Not On Schedule 73
74 Education &Training Shared Service Deliverables Deliverable Measure Reporting Frequency Notes on Current Status Status Expected Completion Date #7 Global Course Catalog Quarterly Complete inventory of all E&T products across the services to develop baseline - MHS Global Catalog 40% complete / EDC Oct 15 FY16 #8 METC Strategic Partnerships Semiannually Goal is to develop bridge programs with civilian schools that recognize METC training for college credit FY16 #9 Military Medical Education Consortium Semiannually Goal is to identify potential partners, develop, and establish partnerships FY16 #10 JGMESB Support Quarterly - Way forward is to formally request that Services nominate member(s) for JGMESB WG to develop POAM - Overarching E&T Work Group charter is under development FY18 #11 Combat Casualty Care Semiannually - Way forward is to conduct assessment of critical skills training and identify training gaps, then develop plan of action - Key stakeholders and SMEs have initiated & conducted meetings FY18 #12 Modeling & Simulation Quarterly - Align modeling & simulation functions across the MHS - Standardize medical training and; - Institutionalize shared Service skill sets for the enterprise to support DHA portfolio FY18 Complete On Schedule Not On Schedule 74

75 Col Carol A. Fisher Chief, Public Health Division Public Health Division 75
76 Public Health Division (PHD) BLUF / Challenges / Wins BLUF IOC: 30 Sep 2014 with 3 of 4 Branches Structured process in place to analyze 8 remaining product lines (PLs) Challenges Transition of Armed Forces Health Surveillance Center to PHD Re-baseline of projected cost savings Availability of Service Subject Matter Experts for remaining PL analyses Wins Ebola response effort Periodic Health Assessment Optimization Draft Strategic Plan 76
77 Implement PL4 Veterinary Services Implement PL3 Immunizatio n Healthcare Implement PL2 Health Surveillance Implement PL1 Deployment Health Transition Public Health Division Progress Update Milestone Indicator Suspense Revised Suspense Completed People Transfer to DHA (awaiting AFHSC) 30 Sep Jul 15 Resources Transfer to DHA 1 Oct 15 Governance Update with Services Charter, CONOPS 30 Sep 15 Public Health Division Manpower Assessment 15 Jun 15 Re-baseline projected savings and efficiencies 30 Sep 15 WG charter for Medical Readiness Systems [i.e., MEDPROS, MRRS, ASIMS] Portfolio Rationalization 1 May 15 PHA Optimization Effort DoDI out for internal coord 16 Mar 15 Awaiting transfer of AFHSC to Public Health Division 30 Sep Jul 15 Assessment of the six Immunization Regional Offices for efficiency opportunities awaiting manpower study assessment 30 Jun 15 Awaiting manpower study assessment 30 Jun Briefing Date: 10 Mar 2015 Complete On Schedule At Risk of Missing Suspense Medically Ready Force...Ready Medical Force 77 77
78 Dollars (in Millions) Public Health Division FY BCA Costs & Projected Savings $300 $200 $100 $- $(100) Risk- and Inflation-Adjusted Project Savings, FY14-19 $280.8 $191.2 $105.8 $47.3 $(0.9) $71.8 $85.5 $89.5 $33.9 $(12.4) $(13.3) FY14 FY15 FY16 FY17 FY18 FY19 Annual Net Savings Cumulative Net Savings BCA Category FY14 FY15 FY16 FY17 FY18 FY19 Total Primary Drivers of Implementation Costs Deployment Health: Eliminate ANAM assessments; streamline PHA, and deployment health assessments; and change in Optimize Health Status Health Surveillance: Eliminate redundant surveillance databases/activities and derive economies of scale from process improvements Savings ($M) $0.00 $8.68 $51.07 $77.81 $81.11 $84.68 $ Cost ($M) $8.19 $6.84 $2.35 $2.07 $2.23 $2.05 $23.73 Net Savings ($M) ($8.19) $1.84 $48.72 $75.74 $78.88 $82.63 $ Savings ($M) $0.11 $2.02 $6.74 $9.48 $9.68 $9.90 $37.94 Cost ($M) $4.30 $4.80 $8.20 $13.40 $3.10 $3.00 $36.80 Net Savings ($M) ($4.19) ($2.78) ($1.46) ($3.92) $6.58 $6.90 $ Cost savings questionable due to NDAA 2015 annual person to person mental health assessment - MBOG endorsed Deployment Health savings re-baseline effort; EDC: 30 Sept Health Surveillance (AFHSC) delayed in transfer to DHA - Implementation costs for process improvements - Identification/elimination of redundant systems 78 Medically Ready Force...Ready Medical Force Briefing Date: 10 Mar
 8 additional product lines (per CONOPs) to be analyzed for")
79 Public Health Division Product Lines: Current & Future Initial public health product lines (per CONOPs) - Deployment Health Integrated at IOC; re-baselining cost savings Status - Immunization Healthcare Integrated at IOC - Veterinary Services Integrated at IOC - Health Surveillance Pending transfer to DHA (EDC: July 2015) 8 additional product lines (per CONOPs) to be analyzed for recommended PHD FOC structure - Occupational & Environmental Health (Includes Occupational Health, Hearing Health, Industrial Hygiene, Environmental Health) Status - Clinical Preventive Medicine Analysis not initiated - Health Promotion Analysis not initiated - Public Health Laboratories Analysis in-progress - Radiation Health Analysis not initiated Initiate Analysis (Hearing Health only) March Food/Water Safety & Sanitation Initiate Analysis March Entomology Analysis not initiated - Health Risk Communication & Public Health Emergency Response Analysis not initiated Briefing Date: 10 Mar 2015 Medically Ready Force...Ready Medical Force 79
80 Enhanced Multi-Service Markets (emsm) 80
 Tidewater (Navy) San Diego (Navy) Ft.")
81 Multi-Service Markets: 2 or more Services, large beneficiary population, 45% direct care dollars, large GME & readiness platforms Puget Sound, Washington (Army) National Capital Region (DHA) Colorado Springs, Colorado (rotate Air Force/Army) Tidewater (Navy) San Diego (Navy) Ft. Bragg (Army) Oahu, Hawaii (Army) San Antonio, Texas (rotate Air Force/Army) = emsm = Single Service The Eight Largest Markets (and Service/Department Leads) 81
 2 or more Services; large beneficiary population; almost 50% of our direct care spending; and largest readiness / training platforms The Plans focused on")
82 Enhanced Multi-Service Markets (emsm) Overview Multi-Service Markets include Colorado Springs, Hawaii, the National Capital Region, Puget Sound, San Antonio, and Tidewater (with San Diego and Ft Bragg Pope as large market participants) 2 or more Services; large beneficiary population; almost 50% of our direct care spending; and largest readiness / training platforms The Plans focused on becoming an Integrated Health Delivery System, and identified opportunities to increase enrollment at military clinics, increase provider productivity, and reduce Private-Sector costs MHS leadership reviews emsm performance quarterly to enhanced accountability. If performance is below target, Service leads work with emsms to develop remediation plans

83 Executive Summary NCR emsm Walter Reed National Military Medical Center DiLorenzo TRICARE Health Clinic Branch Medical Clinic Carderock National Intrepid Center of Excellence Fort Belvoir Community Hospital Fairfax Health Center Dumfries Health Center Naval Health Clinic Quantico Naval Branch Health Clinic Washington Navy Yard Branch Medical Clinic OCS Brown Field Naval Branch Health Clinic The Basic School # MTFs Capability Overview # ORs # Total Beds Physical Staffed Physical Staffed Skill Type 1 & 2 Providers Total DHP Direct Care Funding* ,335 $1.3B * Estimated, includes MILPERS FY15 Population Kimbrough Ambulatory Care Center McNair Army Health Clinic Andrew Rader Army Health Clinic Naval Health Clinic Annapolis Naval Branch Health Clinic Bancroft Hall Eligible Population MTF-Enrolled / Empaneled MCSC-Enrolled Prime All 455K Prime 219K 34K Medicare Eligible 78K Plus 22K Johns Hopkins (FHP) Total 241K 35K 779 th Med Group Joint Base Andrews Branch Medical Clinic Naval Research Lab Washington 579 th Med Group Joint Base Anacostia-Bolling Naval Branch Health Clinic Joint Base Andrews FY15 FY16 FY17 FY18 FY19 FY20 FY16-20 Total Net Estimated Savings ($M) Savings $71.7M $109.0M $126.9M $137.9M $138.0M $138.0M $649.9M Costs $18.6M $28.3M $32.9M $35.8M $35.8M $35.8M $168.6M Net $53.1M $80.7M $94.0M $102.1M $102.2M 102.2M $481.3M Productivity Productivity Target Targeted Annual Productivity (PA wrvus) 5-Yr Change 261K 1.57M 1.73M 1.93M 2.03M 2.08M 2.08M 343K Total Enrollment Total Enrollment Target Targeted Total Annual Enrollment 5-Yr Change Prime: 277.0K 219.0K 255.8K 267.4K 277.0K 277.0K 277.0K 21.2K Plus: 23.0K 22.0K 22.2K 22.6K 23.0K 23.0K 23.0K 0.8K Total 300.0K 241.0K 278.0K 290.0K 300.0K 300.0K 300.0K 22.0K Recapture Recapture Target Annual Recapture ($M) FY16-20 Total $71.7M $109M $126.9M $138M $138M $138M $649.9M Initiative High Reliability Culture of Quality and Patient Partnership Readiness Health Impact Health Care Cost Access Quality Safety CAPT Vedral-Baron FBCH Net Savings Potential ($M) Implementation Costs ($M) Total Productivity Change Total Enrollment Change Total Recapture ($M) Quality and safety improvements have direct impact on cost (e.g., cost avoidance of repeat surgeries, complications, litigation, etc.) not reflected in this model Referral Management, Template Management, and Appointing (RM) Operating Room (OR) Optimization Patient Centered Medical Home (PCMH) 2.0 Secure Messaging Col Cantilina 779th MDG $191.9 $ K $205.1 BG Clark WRNMMC $219.2 $ K $313.1 CAPT Smith NBHC Quantico $70.2 $ K 21.9K $131.7 Lt Col Hanson 579th MDG Secure messaging and other tools (e.g., Nurse Advice Line) support the PCMH Initiative and impact cost through avoiding ED/UCC visits. Total $481.3 $ K 21.9K $649.9 Pre-Decisional Deliberative Matter -- For Official Use Only Within DoD pwc 83
84 NCR Business Plan Initiatives Summary Initiative Key Focus Areas Key Successes High Reliability Culture of Quality and Patient Partnership CAPT Vedral-Baron (FBCH) Referral Management, Template Management, and Appointing (RM) COL Cantilina (779 th ) Operating Room (OR) Optimization BG Clark (WRNMMC) Patient-Centered Medical Home (PCMH) 2.0 CAPT Smith (Quantico) Enrollment LTC Wienberg (Rader/McNair) TeamSTEPPS Patient Centered Caring Communication Initiative (PCCCI) Provider Training Expand the Partnership for Patients (PfP) to Outpatient Facilities Establish market-wide HEDIS monitoring program Inaugural Quality Summit, April 2015 Governance by Product Line Template Management & Booking Consolidate/map ancillary procedure codes and standardize review/prioritization process Establish capability for booking patient follow-up visit at checkout Reorganize Surgical Management across the Market Standardize templates and appointment types across emsm Credential surgeons at multiple MTFs NCR market approach to meet critical regional deficiencies in Physical Therapy Access to Primary Care Market-wide PCMH maturity Timely and relevant data ED/UCC usage The Enrollment team is assessing where and how to enroll new eligible beneficiaries, and determine the type and quantity of eligible beneficiaries each MTF can take on while still providing quality care. The market will increase its enrollment capacity by 10,000 enrollees by the end of FY15 Reached the 90 th percentile on Breast Cancer Screening as a market. Over 45% of the emsm has entered sustainment mode for TeamSTEPPS Completed development of all evidenced-based bundles for Partnership for Patients 50% reduction in medical Services deferrals to the network for capacity from November 2013 to November Building on the Orthopedics successes with outbound proactive booking, the NCR emsm is capitalizing on the standardization of the product line templates and processes by developing a specialized team of call center agents focused on all Orthopedic appointment needs both outbound and inbound. 26% decrease in private sector Orthopedic Surgeon encounters and 36% decrease in costs for market enrollees from FY13 to FY14 7% increase in direct care Orthopedic Surgical cases over the same timeframe Expanding its primary care footprint at two locations, Fairfax and Dumfries, both near beneficiary population centers. Realigning of the Fort Belvoir Family Practice Residency Program to maximize access to primary care FY13-14 NCR enrolled over 6,000 patients increasing total enrollment from 236,000 to 242,000. Secure Messaging Lt Col Hanson (579 th ) Patient Registration Provider Registration and Active Utilization Response time Training Policy change Nearly eliminated endocrinology leakage to the network since implementing Provider-to-Provider secure messaging at WRNMMC since March Patient adoption at 589 th is increasing and correlated with a drop in urgent care usage. 84

85
 and provides support to the three Military Services.")
86 The DHA Supports the Military Services The DHA reports to the ASD(HA) and provides support to the three Military Services. 86
The Defense Health Agency in 2015
 The Defense Health Agency in 2015 COL Scott A Svabek Acting Director of Procurement Defense Health Agency December 2014 Medically Ready Force Ready Medical Force The Why 1 the Why Not 2 Agenda MHS Governance
The Defense Health Agency in 2015 COL Scott A Svabek Acting Director of Procurement Defense Health Agency December 2014 Medically Ready Force Ready Medical Force The Why 1 the Why Not 2 Agenda MHS Governance
Enhanced Multi-Service Markets: Integrated Healthcare Readiness Focus
 Enhanced Multi-Service Markets: Integrated Healthcare Readiness Focus Paul Toland, FACHE CAPT, MSC, USN Chief Operating Officer Hawaii enhanced Multi-Service Market Disclosures The presenter has no financial
Enhanced Multi-Service Markets: Integrated Healthcare Readiness Focus Paul Toland, FACHE CAPT, MSC, USN Chief Operating Officer Hawaii enhanced Multi-Service Market Disclosures The presenter has no financial
Military Health System: The Defense Health Agency in 2016 VADM (Dr) Raquel Bono Director, Defense Health Agency December 1, 2015
 Raquel Bono Director, Defense Health Agency December 1, 2015") Military Health System: The Defense Health Agency in 2016 VADM (Dr) Raquel Bono Director, Defense Health Agency December 1, 2015 The Defense Health Agency Fully Operational / Continuity of Mission 1 The
Military Health System: The Defense Health Agency in 2016 VADM (Dr) Raquel Bono Director, Defense Health Agency December 1, 2015 The Defense Health Agency Fully Operational / Continuity of Mission 1 The
DHA & DLA-TS Supported MEDLOG Shared Services Update for AMSUS-SM September 16,
 CAPT Bernie Poindexter (DHA) Ms. Geneva Polini (DLA-TS) DHA & DLA-TS Supported MEDLOG Shared Services Update for AMSUS-SM September 16, 1 DHA Vision A joint, integrated, premier system of health, supporting
CAPT Bernie Poindexter (DHA) Ms. Geneva Polini (DLA-TS) DHA & DLA-TS Supported MEDLOG Shared Services Update for AMSUS-SM September 16, 1 DHA Vision A joint, integrated, premier system of health, supporting
DEPUTY SECRETARY OF DEFENSE 1010 DEFENSE PENTAGON WASHINGTON, DC
 DEPUTY SECRETARY OF DEFENSE 1010 DEFENSE PENTAGON WASHINGTON, DC 20301-1010 The Honorable John McCain Chairman Committee on Armed Services United States Senate Washington, DC 20510 JUN 3 0 2017 Dear Mr.
DEPUTY SECRETARY OF DEFENSE 1010 DEFENSE PENTAGON WASHINGTON, DC 20301-1010 The Honorable John McCain Chairman Committee on Armed Services United States Senate Washington, DC 20510 JUN 3 0 2017 Dear Mr.
Defense Health Agency PROCEDURAL INSTRUCTION
 Defense Health Agency PROCEDURAL INSTRUCTION NUMBER 6025.08 Healthcare Operations/Pharmacy SUBJECT: Pharmacy Enterprise Activity (EA) References: See Enclosure 1. 1. PURPOSE. This Defense Health Agency-Procedural
Defense Health Agency PROCEDURAL INSTRUCTION NUMBER 6025.08 Healthcare Operations/Pharmacy SUBJECT: Pharmacy Enterprise Activity (EA) References: See Enclosure 1. 1. PURPOSE. This Defense Health Agency-Procedural
The Defense Health Agency & Facilities Shared Service
 The Defense Health Agency & Facilities Shared Service John A. Becker Director, Facilities Division August 20, 2015 Agenda 1. Defense Health Agency (DHA) Overview 2. How does the DHA support the war fighter?
The Defense Health Agency & Facilities Shared Service John A. Becker Director, Facilities Division August 20, 2015 Agenda 1. Defense Health Agency (DHA) Overview 2. How does the DHA support the war fighter?
Department of Defense DIRECTIVE
 Department of Defense DIRECTIVE NUMBER 5136.13 September 30, 2013 DA&M SUBJECT: Defense Health Agency (DHA) References: See Enclosure 1 1. PURPOSE. Pursuant to the authority vested in the Secretary of
Department of Defense DIRECTIVE NUMBER 5136.13 September 30, 2013 DA&M SUBJECT: Defense Health Agency (DHA) References: See Enclosure 1 1. PURPOSE. Pursuant to the authority vested in the Secretary of
2016 Major Automated Information System Annual Report. Department of Defense Healthcare Management System Modernization (DHMSM)
") 2016 Major Automated Information System Annual Report Department of Defense Healthcare Management System Modernization (DHMSM) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED
2016 Major Automated Information System Annual Report Department of Defense Healthcare Management System Modernization (DHMSM) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED
DHCC Strategic Plan. Last Revised August 2016
 DHCC Strategic Plan Last Revised August 2016 Table of Contents History of DHCC... 3 Executive Summary... 4 DHCC Mission and Vision... 5 Mission... 5 Vision... 5 DHCC Strategic Drivers... 6 Strategic drivers
DHCC Strategic Plan Last Revised August 2016 Table of Contents History of DHCC... 3 Executive Summary... 4 DHCC Mission and Vision... 5 Mission... 5 Vision... 5 DHCC Strategic Drivers... 6 Strategic drivers
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 6015.17 January 13, 2012 Incorporating Change 1, November 30, 2017 SUBJECT: Military Health System (MHS) Facility Portfolio Management References: See Enclosure
Department of Defense INSTRUCTION NUMBER 6015.17 January 13, 2012 Incorporating Change 1, November 30, 2017 SUBJECT: Military Health System (MHS) Facility Portfolio Management References: See Enclosure
2016 Major Automated Information System Annual Report
 2016 Major Automated Information System Annual Report Global Combat Support System-Marine Corps Logistics Chain Management Increment 1 (GCSS-MC LCM Inc 1) Defense Acquisition Management Information Retrieval
2016 Major Automated Information System Annual Report Global Combat Support System-Marine Corps Logistics Chain Management Increment 1 (GCSS-MC LCM Inc 1) Defense Acquisition Management Information Retrieval
Session 10: Incorporating Improvement Into The Performance Plan
 Session 10: Incorporating Improvement Into The Performance Plan Ms. Sherry Stone, MHA, CDFM Army, Office of the Surgeon General Program Analysis & Evaluation Directorate sherry.j.stone2.civ@mail.mil 14-1
Session 10: Incorporating Improvement Into The Performance Plan Ms. Sherry Stone, MHA, CDFM Army, Office of the Surgeon General Program Analysis & Evaluation Directorate sherry.j.stone2.civ@mail.mil 14-1
Defense Health Program Operation and Maintenance Fiscal Year (FY) 2010 Budget Estimates Information Management
 2010 Budget Estimates Information Management") I. Description of Operations Financed: This Budget Activity Group provides for the /Information Technology resources dedicated to the operation and maintenance of Defense Health Program (DHP) facilities.
I. Description of Operations Financed: This Budget Activity Group provides for the /Information Technology resources dedicated to the operation and maintenance of Defense Health Program (DHP) facilities.
Health Policy in the U.S & the MHS. LCDR John Gardner Uniformed Services University of the Health Sciences
 Health Policy in the U.S & the MHS LCDR John Gardner Uniformed Services University of the Health Sciences Disclosures Presenter has no financial interest to disclose. This continuing education activity
Health Policy in the U.S & the MHS LCDR John Gardner Uniformed Services University of the Health Sciences Disclosures Presenter has no financial interest to disclose. This continuing education activity
Last Revised March 2017
 DHCC Strategic Plan Last Revised March 2017 Released January 2017 by Deployment Health Clinical Center, a Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury Center. This
DHCC Strategic Plan Last Revised March 2017 Released January 2017 by Deployment Health Clinical Center, a Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury Center. This
2011 Ground Robotics Capability Conference. OSD Perspective
 2011 Ground Robotics Capability Conference OSD Perspective Jose M. Gonzalez OUSD (Acquisition, Technology & Logistics) Deputy Director, Portfolio Systems Acquisition, Land Warfare and Munitions Discussion
2011 Ground Robotics Capability Conference OSD Perspective Jose M. Gonzalez OUSD (Acquisition, Technology & Logistics) Deputy Director, Portfolio Systems Acquisition, Land Warfare and Munitions Discussion
2016 Major Automated Information System Annual Report
 2016 Major Automated Information System Annual Report Logistics Modernization Program Increment 2 (LMP Inc 2) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED Table of Contents
2016 Major Automated Information System Annual Report Logistics Modernization Program Increment 2 (LMP Inc 2) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED Table of Contents
STATEMENT OF MRS. ELLEN P. EMBREY ACTING ASSISTANT SECRETARY OF DEFENSE FOR HEALTH AFFAIRS BEFORE THE HOUSE ARMED SERVICES COMMITTEE
 STATEMENT OF MRS. ELLEN P. EMBREY ACTING ASSISTANT SECRETARY OF DEFENSE FOR HEALTH AFFAIRS BEFORE THE HOUSE ARMED SERVICES COMMITTEE MILITARY PERSONNEL SUBCOMMITTEE THE MILITARY HEALTH SYSTEM: HEALTH AFFAIRS/TRICARE
STATEMENT OF MRS. ELLEN P. EMBREY ACTING ASSISTANT SECRETARY OF DEFENSE FOR HEALTH AFFAIRS BEFORE THE HOUSE ARMED SERVICES COMMITTEE MILITARY PERSONNEL SUBCOMMITTEE THE MILITARY HEALTH SYSTEM: HEALTH AFFAIRS/TRICARE
DOD INSTRUCTION JOINT TRAUMA SYSTEM (JTS)
") DOD INSTRUCTION 6040.47 JOINT TRAUMA SYSTEM (JTS) Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: September 28, 2016 Releasability: Approved by: Cleared
DOD INSTRUCTION 6040.47 JOINT TRAUMA SYSTEM (JTS) Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: September 28, 2016 Releasability: Approved by: Cleared
National Capital Region Medical Transformation Update. DoD Progress on Enhancing World-Class Healthcare Capabilities in the National Capital Region
 National Capital Region Medical Transformation Update DoD Progress on Enhancing World-Class Healthcare Capabilities in the National Capital Region VADM John Mateczun, MC, USN Commander, Joint Task Force
National Capital Region Medical Transformation Update DoD Progress on Enhancing World-Class Healthcare Capabilities in the National Capital Region VADM John Mateczun, MC, USN Commander, Joint Task Force
Prepared Statement. Lieutenant General Douglas Robb. Director, Defense Health Agency REGARDING THE MILITARY HEALTH SYSTEM BEFORE THE
 Prepared Statement of Lieutenant General Douglas Robb Director, Defense Health Agency REGARDING THE MILITARY HEALTH SYSTEM BEFORE THE HOUSE APPROPRIATIONS COMMITTEE DEFENSE SUBCOMMITTEE APRIL 14, 2015
Prepared Statement of Lieutenant General Douglas Robb Director, Defense Health Agency REGARDING THE MILITARY HEALTH SYSTEM BEFORE THE HOUSE APPROPRIATIONS COMMITTEE DEFENSE SUBCOMMITTEE APRIL 14, 2015
MHS GENESIS: EHR Modernization for Business Transformation Session 101, Tuesday, February 21, 2017
 MHS GENESIS: EHR Modernization for Business Transformation Session 101, Tuesday, February 21, 2017 Ms. Stacy Cummings, Program Executive Officer, Program Executive Office, Defense Healthcare Management
MHS GENESIS: EHR Modernization for Business Transformation Session 101, Tuesday, February 21, 2017 Ms. Stacy Cummings, Program Executive Officer, Program Executive Office, Defense Healthcare Management
Healthcare Quality Initiative within Navy Medicine
 Healthcare Quality Initiative within Navy Medicine Captain James Oberman*, M.D., FACS, CAPT, MC, USN United States Navy *This perspective is based on CAPT Oberman s experience and not endorsed by BUMED/
Healthcare Quality Initiative within Navy Medicine Captain James Oberman*, M.D., FACS, CAPT, MC, USN United States Navy *This perspective is based on CAPT Oberman s experience and not endorsed by BUMED/
UNCLASSIFIED. FY 2016 Base FY 2016 OCO
 Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Defense Information Systems Agency : February 2015 0400: Research, Development, Test & Evaluation, Defense-Wide / BA 7: Operational Systems Development
Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Defense Information Systems Agency : February 2015 0400: Research, Development, Test & Evaluation, Defense-Wide / BA 7: Operational Systems Development
DoD Biometrics Identity Management (BIdM)
") DoD Biometrics Identity Management (BIdM) Shawn Elliott Futures Branch, Biometric Task Force shawn.elliott@hqda.army.mil 28 Feb 2008 1 Purpose & Content Purpose: Share Biometric Task Force, Biometric Identity
DoD Biometrics Identity Management (BIdM) Shawn Elliott Futures Branch, Biometric Task Force shawn.elliott@hqda.army.mil 28 Feb 2008 1 Purpose & Content Purpose: Share Biometric Task Force, Biometric Identity
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach
 Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Raising the Bar On Infusion Safety: A Patient Safety Program at Baylor Scott & White Health Improving Infusion Pump Safety: A Systematic Approach July 18, 2016 AAMI Foundation Vision: To drive the safe
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 6015.23 October 30, 2002 SUBJECT: Delivery of Healthcare at Military Treatment Facilities: Foreign Service Care; Third-Party Collection; Beneficiary Counseling
Department of Defense INSTRUCTION NUMBER 6015.23 October 30, 2002 SUBJECT: Delivery of Healthcare at Military Treatment Facilities: Foreign Service Care; Third-Party Collection; Beneficiary Counseling
DATE: February 2008 Appropriation/Budget Activity R1 Item Nomenclature: 7 Defense Health Program/BA: 2 Information Technology Development HP
 Fiscal Year (FY) Budget s COST: (Dollars in Thousands) Total PE 0605013 145.665 97.099 145.654 88.859 75.322 70.875 59.560 Defense Blood Standard System (DBSS) TMA Defense Medical Human Resources System
Fiscal Year (FY) Budget s COST: (Dollars in Thousands) Total PE 0605013 145.665 97.099 145.654 88.859 75.322 70.875 59.560 Defense Blood Standard System (DBSS) TMA Defense Medical Human Resources System
2016 Major Automated Information System Annual Report
 2016 Major Automated Information System Annual Report Integrated Personnel and Pay System-Army Increment 2 (IPPS-A Inc 2) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED Table
2016 Major Automated Information System Annual Report Integrated Personnel and Pay System-Army Increment 2 (IPPS-A Inc 2) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED Table
Department of Defense Investment Review Board and Investment Management Process for Defense Business Systems
 Department of Defense Investment Review Board and Investment Management Process for Defense Business Systems Report to Congress March 2012 Pursuant to Section 901 of the National Defense Authorization
Department of Defense Investment Review Board and Investment Management Process for Defense Business Systems Report to Congress March 2012 Pursuant to Section 901 of the National Defense Authorization
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 6490.13 September 11, 2015 Incorporating Change 1, Effective March 31, 2017 USD(P&R) SUBJECT: Comprehensive Policy on Traumatic Brain Injury-Related Neurocognitive
Department of Defense INSTRUCTION NUMBER 6490.13 September 11, 2015 Incorporating Change 1, Effective March 31, 2017 USD(P&R) SUBJECT: Comprehensive Policy on Traumatic Brain Injury-Related Neurocognitive
Defense Health Agency (DHA), J7, Continuing Education Program Office (CEPO) Updates
, J7, Continuing Education Program Office (CEPO) Updates") Defense Health Agency (DHA), J7, Continuing Education Program Office (CEPO) Updates Mr. Gerald Creech Chief, Business Operations, DHA, J7, Education & Training 23 APR 2018 Governance Implementation Planning
Defense Health Agency (DHA), J7, Continuing Education Program Office (CEPO) Updates Mr. Gerald Creech Chief, Business Operations, DHA, J7, Education & Training 23 APR 2018 Governance Implementation Planning
2016 Major Automated Information System Annual Report
 2016 Major Automated Information System Annual Report Key Management Infrastructure Increment 2 (KMI Inc 2) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED Table of Contents Common
2016 Major Automated Information System Annual Report Key Management Infrastructure Increment 2 (KMI Inc 2) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED Table of Contents Common
THE DEFENSE HEALTH AGENCY
 THE DEFENSE HEALTH AGENCY 2 0 1 7 S t a k e h o l d e r R e p o r t Medically Ready Force Ready Medical Force Our Military Health System is stronger than ever Every day, in so many meaningful ways, DHA
THE DEFENSE HEALTH AGENCY 2 0 1 7 S t a k e h o l d e r R e p o r t Medically Ready Force Ready Medical Force Our Military Health System is stronger than ever Every day, in so many meaningful ways, DHA
PREPARED STATEMENT VICE ADMIRAL JOHN MATECZUN, MC, USN COMMANDER, JOINT TASK FORCE NATIONAL CAPITAL REGION MEDICAL BEFORE THE
 NOT FOR PUBLICATION UNTIL RELEASED BY THE HOUSE COMMITTEE ON APPROPRIATIONS PREPARED STATEMENT OF VICE ADMIRAL JOHN MATECZUN, MC, USN COMMANDER, JOINT TASK FORCE NATIONAL CAPITAL REGION MEDICAL BEFORE
NOT FOR PUBLICATION UNTIL RELEASED BY THE HOUSE COMMITTEE ON APPROPRIATIONS PREPARED STATEMENT OF VICE ADMIRAL JOHN MATECZUN, MC, USN COMMANDER, JOINT TASK FORCE NATIONAL CAPITAL REGION MEDICAL BEFORE
DOD INSTRUCTION DEFENSE MEDICAL LOGISTICS PROGRAM
 DOD INSTRUCTION 6430.02 DEFENSE MEDICAL LOGISTICS PROGRAM Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: August 23, 2017 Releasability: Reissues
DOD INSTRUCTION 6430.02 DEFENSE MEDICAL LOGISTICS PROGRAM Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: August 23, 2017 Releasability: Reissues
2016 Major Automated Information System Annual Report
 2016 Major Automated Information System Annual Report Defense Enterprise Accounting and Management System-Increment 1 (DEAMS Inc 1) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED
2016 Major Automated Information System Annual Report Defense Enterprise Accounting and Management System-Increment 1 (DEAMS Inc 1) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED
Last Revised February 2018
 PHCoE Strategic Plan Last Revised February 2018 Table of Contents History of PHCoE... 3 Executive Summary... 4 PHCoE Mission and Vision... 5 Mission... 5 Vision... 5 PHCoE Strategic Drivers... 6 Military
PHCoE Strategic Plan Last Revised February 2018 Table of Contents History of PHCoE... 3 Executive Summary... 4 PHCoE Mission and Vision... 5 Mission... 5 Vision... 5 PHCoE Strategic Drivers... 6 Military
Department of Defense DIRECTIVE
 Department of Defense DIRECTIVE NUMBER 6000.12E January 6, 2011 Incorporating Change 1, Effective October 3, 2013 USD(P&R) SUBJECT: Health Service Support References: See Enclosure 1 1. PURPOSE. This Directive:
Department of Defense DIRECTIVE NUMBER 6000.12E January 6, 2011 Incorporating Change 1, Effective October 3, 2013 USD(P&R) SUBJECT: Health Service Support References: See Enclosure 1 1. PURPOSE. This Directive:
OFFICE OF THE UNDER SECRETARY OF DEFENSE 4000 DEFENSE PENTAGON WASHINGTON, DC MAR
 OFFICE OF THE UNDER SECRETARY OF DEFENSE 4000 DEFENSE PENTAGON WASHINGTON, DC 20301-4000 MAR 3 1 2017 PERSONNEL AND READINESS The Honorable John McCain Chairman Committee on Armed Services United States
OFFICE OF THE UNDER SECRETARY OF DEFENSE 4000 DEFENSE PENTAGON WASHINGTON, DC 20301-4000 MAR 3 1 2017 PERSONNEL AND READINESS The Honorable John McCain Chairman Committee on Armed Services United States
OASD(HA) Mental Health Policies and Programs
 Mental Health Policies and Programs") OASD(HA) Mental Health Policies and Programs Presentation for the Defense Health Board November 27 th Dr. Jack Smith, M.D., MMM Director, Clinical and Program Policy Integration, OASD(HA) OASD (HA) Offices
OASD(HA) Mental Health Policies and Programs Presentation for the Defense Health Board November 27 th Dr. Jack Smith, M.D., MMM Director, Clinical and Program Policy Integration, OASD(HA) OASD (HA) Offices
2016 Major Automated Information System Annual Report
 2016 Major Automated Information System Annual Report Deliberate and Crisis Action Planning and Execution Segments Increment 2A (DCAPES Inc 2A) Defense Acquisition Management Information Retrieval (DAMIR)
2016 Major Automated Information System Annual Report Deliberate and Crisis Action Planning and Execution Segments Increment 2A (DCAPES Inc 2A) Defense Acquisition Management Information Retrieval (DAMIR)
Fiscal Year 2011 Defense Environmental Programs Annual Report to Congress
 Fiscal Year 2011 Defense Environmental Programs Annual Report to Congress November 2012 Office of the Under Secretary of Defense for Acquisition, Technology, and Logistics Preparation of this report/study
Fiscal Year 2011 Defense Environmental Programs Annual Report to Congress November 2012 Office of the Under Secretary of Defense for Acquisition, Technology, and Logistics Preparation of this report/study
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION SUBJECT: Distribution Process Owner (DPO) NUMBER 5158.06 July 30, 2007 Incorporating Administrative Change 1, September 11, 2007 USD(AT&L) References: (a) Unified Command
Department of Defense INSTRUCTION SUBJECT: Distribution Process Owner (DPO) NUMBER 5158.06 July 30, 2007 Incorporating Administrative Change 1, September 11, 2007 USD(AT&L) References: (a) Unified Command
Department of Defense
 Tr OV o f t DISTRIBUTION STATEMENT A Approved for Public Release Distribution Unlimited IMPLEMENTATION OF THE DEFENSE PROPERTY ACCOUNTABILITY SYSTEM Report No. 98-135 May 18, 1998 DnC QtUALr Office of
Tr OV o f t DISTRIBUTION STATEMENT A Approved for Public Release Distribution Unlimited IMPLEMENTATION OF THE DEFENSE PROPERTY ACCOUNTABILITY SYSTEM Report No. 98-135 May 18, 1998 DnC QtUALr Office of
UNCLASSIFIED R-1 ITEM NOMENCLATURE FY 2013 OCO
 Exhibit R-2, RDT&E Budget Item Justification: PB 213 Army DATE: February 212 COST ($ in Millions) FY 211 FY 212 FY 214 FY 215 FY 216 FY 217 To Complete Program Element 125.44 31.649 4.876-4.876 25.655
Exhibit R-2, RDT&E Budget Item Justification: PB 213 Army DATE: February 212 COST ($ in Millions) FY 211 FY 212 FY 214 FY 215 FY 216 FY 217 To Complete Program Element 125.44 31.649 4.876-4.876 25.655
2016 Major Automated Information System Annual Report
 2016 Major Automated Information System Annual Report Deliberate and Crisis Action Planning and Execution Segments Increment 2B (DCAPES Inc 2B) Defense Acquisition Management Information Retrieval (DAMIR)
2016 Major Automated Information System Annual Report Deliberate and Crisis Action Planning and Execution Segments Increment 2B (DCAPES Inc 2B) Defense Acquisition Management Information Retrieval (DAMIR)
Request for Proposals
 Request for Proposals Online National Resource Center Enterprise Software Platform Design and Implementation DEADLINE FOR SUBMISSION: By email: Received no later than 5:00 pm EDT, Jul 27, 2018. By mail:
Request for Proposals Online National Resource Center Enterprise Software Platform Design and Implementation DEADLINE FOR SUBMISSION: By email: Received no later than 5:00 pm EDT, Jul 27, 2018. By mail:
2016 Major Automated Information System Annual Report
 2016 Major Automated Information System Annual Report Tactical Mission Command (TMC) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED Table of Contents Common Acronyms and Abbreviations
2016 Major Automated Information System Annual Report Tactical Mission Command (TMC) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED Table of Contents Common Acronyms and Abbreviations
UNCLASSIFIED FY 2016 OCO. FY 2016 Base
 Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Air Force : February 2015 3600: Research,, Test & Evaluation, Air Force / BA 7: Operational Systems COST ($ in Millions) FY 2017 FY 2018 FY 2019 FY
Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Air Force : February 2015 3600: Research,, Test & Evaluation, Air Force / BA 7: Operational Systems COST ($ in Millions) FY 2017 FY 2018 FY 2019 FY
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation. April 4, :45 5:00 pm
 Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Three C s of Change in the Value-Based Economy: Competency, Culture and Compensation April 4, 2014 3:45 5:00 pm 1 Introduction Kevin McCune, MD Chief Medical Officer Advocate Medical Group Peg Stone Vice
Working Together for a Healthier Washington
 Working Together for a Healthier Washington Laura Kate Zaichkin, Administrator, Office of Health Innovation & Reform Health Care Authority April 29, 2015 Why do we need health system transformation? Because
Working Together for a Healthier Washington Laura Kate Zaichkin, Administrator, Office of Health Innovation & Reform Health Care Authority April 29, 2015 Why do we need health system transformation? Because
Section 727 of the Carl Levin and Howard P. Buck McKeon National Defense Authorization Act for Fiscal Year 2015 Public Law
 Section 727 of the Carl Levin and Howard P. Buck McKeon National Defense Authorization Act for Fiscal Year 2015 Public Law 113-291 Antimicrobial Stewardship Program Plan Medical Facilities Department of
Section 727 of the Carl Levin and Howard P. Buck McKeon National Defense Authorization Act for Fiscal Year 2015 Public Law 113-291 Antimicrobial Stewardship Program Plan Medical Facilities Department of
We acquire the means to move forward...from the sea. The Naval Research, Development & Acquisition Team Strategic Plan
 The Naval Research, Development & Acquisition Team 1999-2004 Strategic Plan Surface Ships Aircraft Submarines Marine Corps Materiel Surveillance Systems Weapon Systems Command Control & Communications
The Naval Research, Development & Acquisition Team 1999-2004 Strategic Plan Surface Ships Aircraft Submarines Marine Corps Materiel Surveillance Systems Weapon Systems Command Control & Communications
Joint Task Force National Capital Region Medical. Joint Pathology Center Update for the Defense Health Board
 Joint Task Force National Capital Region Medical Joint Pathology Center Update for the Defense Health Board Thomas P. Baker, M.D. COL, MC Interim Director, Joint Pathology Center 02 November 2010 Background
Joint Task Force National Capital Region Medical Joint Pathology Center Update for the Defense Health Board Thomas P. Baker, M.D. COL, MC Interim Director, Joint Pathology Center 02 November 2010 Background
Information Technology Expenditure Approval Authority
 Department of the Navy Secretariat Information Technology Expenditure Approval Authority Overview Version 1.0 15 April 2012 DEPARTMENT OF THE NAVY CHIEF INFORMATION OFFICER Table of Contents Executive
Department of the Navy Secretariat Information Technology Expenditure Approval Authority Overview Version 1.0 15 April 2012 DEPARTMENT OF THE NAVY CHIEF INFORMATION OFFICER Table of Contents Executive
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 4140.25 June 25, 2015 Incorporating Change 1, October 6, 2017 USD(AT&L) SUBJECT: DoD Management Policy for Energy Commodities and Related Services References: See
Department of Defense INSTRUCTION NUMBER 4140.25 June 25, 2015 Incorporating Change 1, October 6, 2017 USD(AT&L) SUBJECT: DoD Management Policy for Energy Commodities and Related Services References: See
UNCLASSIFIED. R-1 ITEM NOMENCLATURE PE N: Consolidated Afloat Network Ent Services(CANES) FY 2012 OCO
 FY 2012 OCO") Exhibit R-2, RDT&E Budget Item Justification: PB 2012 Navy DATE: February 2011 COST ($ in Millions) FY 2010 FY 2013 FY 2014 FY 2015 FY 2016 To Program Element 46.823 63.563 12.906-12.906 15.663 15.125
Exhibit R-2, RDT&E Budget Item Justification: PB 2012 Navy DATE: February 2011 COST ($ in Millions) FY 2010 FY 2013 FY 2014 FY 2015 FY 2016 To Program Element 46.823 63.563 12.906-12.906 15.663 15.125
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Public Health Subcommittee
 Public Health Subcommittee Decision Brief: Improving Defense Health Program Medical Research Processes Defense Health Board June 26, 2017 1 Overview Tasking Membership Timeline Findings & Recommendations
Public Health Subcommittee Decision Brief: Improving Defense Health Program Medical Research Processes Defense Health Board June 26, 2017 1 Overview Tasking Membership Timeline Findings & Recommendations
Defense Health Agency PROCEDURAL INSTRUCTION
 Defense Health Agency PROCEDURAL INSTRUCTION NUMBER 6025.03 J-3, Healthcare Operations SUBJECT: Standard Processes and Criteria for Establishing Urgent Care (UC) Services and Expanded Hours and Appointment
Defense Health Agency PROCEDURAL INSTRUCTION NUMBER 6025.03 J-3, Healthcare Operations SUBJECT: Standard Processes and Criteria for Establishing Urgent Care (UC) Services and Expanded Hours and Appointment
UNCLASSIFIED. LandWarNet Army Request for IT (ARFIT) Information Exchange Forum (IEF)
 Information Exchange Forum (IEF)") LandWarNet 2011 Army Request for IT (ARFIT) Information Exchange Forum (IEF) CIO/G-6 Governance, Acquisitions and Chief Knowledge Officer (GA&CKO) Governance Division Strategic Goals Approach Objectives
LandWarNet 2011 Army Request for IT (ARFIT) Information Exchange Forum (IEF) CIO/G-6 Governance, Acquisitions and Chief Knowledge Officer (GA&CKO) Governance Division Strategic Goals Approach Objectives
UNCLASSIFIED. FY 2016 Base FY 2016 OCO
 Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Army : February 2015 2040: Research, Development, Test & Evaluation, Army / BA 5: System Development & Demonstration (SDD) COST ($ in Millions) Years
Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Army : February 2015 2040: Research, Development, Test & Evaluation, Army / BA 5: System Development & Demonstration (SDD) COST ($ in Millions) Years
UNCLASSIFIED. R-1 ITEM NOMENCLATURE PE F: Theater Battle Management (TBM) C4I FY 2012 OCO
 C4I FY 2012 OCO") Exhibit R-2, RDT&E Budget Item Justification: PB 2012 Air Force DATE: February 2011 COST ($ in Millions) FY 2010 FY 2013 FY 2014 FY 2015 FY 2016 To Program Element 18.374 15.170 15.528-15.528 15.817 15.217
Exhibit R-2, RDT&E Budget Item Justification: PB 2012 Air Force DATE: February 2011 COST ($ in Millions) FY 2010 FY 2013 FY 2014 FY 2015 FY 2016 To Program Element 18.374 15.170 15.528-15.528 15.817 15.217
Department of Defense INSTRUCTION
 Department of Defense INSTRUCTION NUMBER 5000.55 November 1, 1991 SUBJECT: Reporting Management Information on DoD Military and Civilian Acquisition Personnel and Positions ASD(FM&P)/USD(A) References:
Department of Defense INSTRUCTION NUMBER 5000.55 November 1, 1991 SUBJECT: Reporting Management Information on DoD Military and Civilian Acquisition Personnel and Positions ASD(FM&P)/USD(A) References:
From Big Data to Big Knowledge Optimizing Medication Management
 From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
2016 Major Automated Information System Annual Report
 2016 Major Automated Information System Annual Report Teleport Generation 3 (Teleport Gen 3) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED Table of Contents Common Acronyms
2016 Major Automated Information System Annual Report Teleport Generation 3 (Teleport Gen 3) Defense Acquisition Management Information Retrieval (DAMIR) UNCLASSIFIED Table of Contents Common Acronyms
DOD INSTRUCTION PATIENT MOVEMENT (PM)
") DOD INSTRUCTION 6000.11 PATIENT MOVEMENT (PM) Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: June 22, 2018 Releasability: Cleared for public release.
DOD INSTRUCTION 6000.11 PATIENT MOVEMENT (PM) Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: June 22, 2018 Releasability: Cleared for public release.
All MHSS committees and workgroups will be sponsored by a DASD or a Deputy Surgeon General.
 OCT 17 1995 MEMORANDUM FOR: SURGEON GENERAL OF THE ARMY SURGEON GENERAL OF THE NAVY SURGEON GENERAL OF THE AIR FORCE SUBJECT: Implementation of Recommendations for Military Health Services System (MHSS)
OCT 17 1995 MEMORANDUM FOR: SURGEON GENERAL OF THE ARMY SURGEON GENERAL OF THE NAVY SURGEON GENERAL OF THE AIR FORCE SUBJECT: Implementation of Recommendations for Military Health Services System (MHSS)
Financing Army Medicine: Driving the System for Health
 Financing Army Medicine: Driving the System for Health COL Anthony S. Cooper, CDFM, FACHE, DFMCP3 MAJ Deepak J. Mathew, CDFM, DFMCP2 Slide 1 of 15 Purpose and Outline Purpose: To describe the journey of
Financing Army Medicine: Driving the System for Health COL Anthony S. Cooper, CDFM, FACHE, DFMCP3 MAJ Deepak J. Mathew, CDFM, DFMCP2 Slide 1 of 15 Purpose and Outline Purpose: To describe the journey of
Clinical Quality in Behavioral Health: A TRICARE Perspective October 15, 2010
 Clinical Quality in Behavioral Health: A TRICARE Perspective October 15, 2010 RADM C.S. Hunter, MC, USN Deputy Director TRICARE Management Activity TRICARE - Who We Are 9.6 million beneficiaries TRICARE
Clinical Quality in Behavioral Health: A TRICARE Perspective October 15, 2010 RADM C.S. Hunter, MC, USN Deputy Director TRICARE Management Activity TRICARE - Who We Are 9.6 million beneficiaries TRICARE
UNCLASSIFIED FY 2016 OCO. FY 2016 Base
 Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Air Force : February 2015 3600: Research, Development, Test & Evaluation, Air Force / BA 7: Operational s Development COST ($ in Millions) FY 2017
Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Air Force : February 2015 3600: Research, Development, Test & Evaluation, Air Force / BA 7: Operational s Development COST ($ in Millions) FY 2017
DEFENSE HEALTH AGENCY 7700 ARLINGTON BOULEVARD, SUITE 5101 FALLS CHURCH, VIRGINIA
 DEFENSE HEALTH AGENCY 7700 ARLINGTON BOULEVARD, SUITE 5101 FALLS CHURCH, VIRGINIA 22042-5101 DHA-IPM 17-004 MEMORANDUM FOR ASSISTANT SECRETARY OF THE ARMY (MANPOWER AND RESERVE AFFAIRS) ASSISTANT SECRETARY
DEFENSE HEALTH AGENCY 7700 ARLINGTON BOULEVARD, SUITE 5101 FALLS CHURCH, VIRGINIA 22042-5101 DHA-IPM 17-004 MEMORANDUM FOR ASSISTANT SECRETARY OF THE ARMY (MANPOWER AND RESERVE AFFAIRS) ASSISTANT SECRETARY
Ref: (a) MROC Decision Memorandum dtd 18 Apr 2013 (b) SECNAV M Encl: (1) Role of Performance Management and MCSHA in PPBE
 MROC Decision Memorandum dtd 18 Apr 2013 (b) SECNAV M Encl: (1) Role of Performance Management and MCSHA in PPBE") DEPARTMENT OF THE NAVY HEADQUARTERS UNITED STATES MARINE CORPS 3000 MARINE CORPS PENTAGON WASHINGTON, DC 20350-3000 MCO 5230.23 R PA&E MARINE CORPS ORDER 5230.23 From: Commandant of the Marine Corps To:
DEPARTMENT OF THE NAVY HEADQUARTERS UNITED STATES MARINE CORPS 3000 MARINE CORPS PENTAGON WASHINGTON, DC 20350-3000 MCO 5230.23 R PA&E MARINE CORPS ORDER 5230.23 From: Commandant of the Marine Corps To:
UNCLASSIFIED. FY 2016 Base FY 2016 OCO
 Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Army : February 2015 2040: Research, Development, Test & Evaluation, Army / BA 5: System Development & Demonstration (SDD) COST ($ in Millions) Years
Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Army : February 2015 2040: Research, Development, Test & Evaluation, Army / BA 5: System Development & Demonstration (SDD) COST ($ in Millions) Years
Analysis of Incurred Claims Trend and Provider Payments
 Analysis of Incurred Claims Trend and Provider Payments Board of Trustees Meeting May 24, 2013 Presentation Overview Trends in Incurred Claims Paid through March 31, 2013 Per Member Per Month (PMPM) By
Analysis of Incurred Claims Trend and Provider Payments Board of Trustees Meeting May 24, 2013 Presentation Overview Trends in Incurred Claims Paid through March 31, 2013 Per Member Per Month (PMPM) By
DOD MANUAL , VOLUME 1 DOD MANAGEMENT OF ENERGY COMMODITIES: OVERVIEW
 DOD MANUAL 4140.25, VOLUME 1 DOD MANAGEMENT OF ENERGY COMMODITIES: OVERVIEW Originating Component: Office of the Under Secretary of Defense for Acquisition and Sustainment Effective: March 2, 2018 Releasability:
DOD MANUAL 4140.25, VOLUME 1 DOD MANAGEMENT OF ENERGY COMMODITIES: OVERVIEW Originating Component: Office of the Under Secretary of Defense for Acquisition and Sustainment Effective: March 2, 2018 Releasability:
REQUIREMENTS TO CAPABILITIES
 Chapter 3 REQUIREMENTS TO CAPABILITIES The U.S. naval services the Navy/Marine Corps Team and their Reserve components possess three characteristics that differentiate us from America s other military
Chapter 3 REQUIREMENTS TO CAPABILITIES The U.S. naval services the Navy/Marine Corps Team and their Reserve components possess three characteristics that differentiate us from America s other military
GAO. DOD Needs Complete. Civilian Strategic. Assessments to Improve Future. Workforce Plans GAO HUMAN CAPITAL
 GAO United States Government Accountability Office Report to Congressional Committees September 2012 HUMAN CAPITAL DOD Needs Complete Assessments to Improve Future Civilian Strategic Workforce Plans GAO
GAO United States Government Accountability Office Report to Congressional Committees September 2012 HUMAN CAPITAL DOD Needs Complete Assessments to Improve Future Civilian Strategic Workforce Plans GAO
DoD Mentor Protégé Program. Shannon C. Jackson, Program Manager DoD Office of Small Business Programs
 DoD Mentor Protégé Program Shannon C. Jackson, Program Manager DoD Office of Small Business Programs 1 People underestimate their capacity for change. There is never a right time to do a difficult thing.
DoD Mentor Protégé Program Shannon C. Jackson, Program Manager DoD Office of Small Business Programs 1 People underestimate their capacity for change. There is never a right time to do a difficult thing.
DOD INVENTORY OF CONTRACTED SERVICES. Actions Needed to Help Ensure Inventory Data Are Complete and Accurate
 United States Government Accountability Office Report to Congressional Committees November 2015 DOD INVENTORY OF CONTRACTED SERVICES Actions Needed to Help Ensure Inventory Data Are Complete and Accurate
United States Government Accountability Office Report to Congressional Committees November 2015 DOD INVENTORY OF CONTRACTED SERVICES Actions Needed to Help Ensure Inventory Data Are Complete and Accurate
DoD Joint Federated Assurance Center (JFAC) 2017 Update
 2017 Update") DoD Joint Federated Assurance Center (JFAC) 2017 Update Thomas Hurt Office of the Deputy Assistant Secretary of Defense for Systems Engineering 20th Annual NDIA Systems Engineering Conference Springfield,
DoD Joint Federated Assurance Center (JFAC) 2017 Update Thomas Hurt Office of the Deputy Assistant Secretary of Defense for Systems Engineering 20th Annual NDIA Systems Engineering Conference Springfield,
COMPLIANCE WITH THIS PUBLICATION IS MANDATORY
 BY ORDER OF THE SECRETARY OF THE AIR FORCE AIR FORCE INSTRUCTION 41-126 6 MARCH 2014 Health Services DEPARTMENT OF DEFENSE/VETERANS AFFAIRS HEALTH CARE RESOURCE SHARING PROGRAM COMPLIANCE WITH THIS PUBLICATION
BY ORDER OF THE SECRETARY OF THE AIR FORCE AIR FORCE INSTRUCTION 41-126 6 MARCH 2014 Health Services DEPARTMENT OF DEFENSE/VETERANS AFFAIRS HEALTH CARE RESOURCE SHARING PROGRAM COMPLIANCE WITH THIS PUBLICATION
SUBJECT: Army Directive (Implementation of Acquisition Reform Initiatives 1 and 2)
") S E C R E T A R Y O F T H E A R M Y W A S H I N G T O N MEMORANDUM FOR SEE DISTRIBUTION SUBJECT: Army Directive 2017-22 (Implementation of Acquisition Reform Initiatives 1 and 2) 1. References. A complete
S E C R E T A R Y O F T H E A R M Y W A S H I N G T O N MEMORANDUM FOR SEE DISTRIBUTION SUBJECT: Army Directive 2017-22 (Implementation of Acquisition Reform Initiatives 1 and 2) 1. References. A complete
Rebalancing the Cost Structure: Progressive Health Systems, Inc. Bob Haley, CEO Steve Hall, CFO
 Rebalancing the Cost Structure: Progressive Health Systems, Inc. Bob Haley, CEO Steve Hall, CFO THE MARKET & PHS S POSITION 2 Progressive Health Systems, Inc. (dba Pekin Hospital) Pekin, IL 3 4 5 Nearby
Rebalancing the Cost Structure: Progressive Health Systems, Inc. Bob Haley, CEO Steve Hall, CFO THE MARKET & PHS S POSITION 2 Progressive Health Systems, Inc. (dba Pekin Hospital) Pekin, IL 3 4 5 Nearby
UNCLASSIFIED. FY 2016 Base
 Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Defense Health Program Date: February 2015 0130: Defense Health Program / BA 2: RDT&E COST ($ in Millions) Prior Years FY 2014 FY 2015 Complete Total
Exhibit R-2, RDT&E Budget Item Justification: PB 2016 Defense Health Program Date: February 2015 0130: Defense Health Program / BA 2: RDT&E COST ($ in Millions) Prior Years FY 2014 FY 2015 Complete Total
UNCLASSIFIED. UNCLASSIFIED Navy Page 1 of 7 R-1 Line #31
 Exhibit R2, RDT&E Budget Item Justification: PB 2015 Navy Date: March 2014 1319: Research, Development, Test & Evaluation, Navy / BA 4: Advanced Component Development & Prototypes (ACD&P) COST ($ in Millions)
Exhibit R2, RDT&E Budget Item Justification: PB 2015 Navy Date: March 2014 1319: Research, Development, Test & Evaluation, Navy / BA 4: Advanced Component Development & Prototypes (ACD&P) COST ($ in Millions)
UNCLASSIFIED R-1 ITEM NOMENCLATURE FY 2013 OCO
 Exhibit R-2, RDT&E Budget Item Justification: PB 2013 Air Force DATE: February 2012 COST ($ in Millions) FY 2011 FY 2014 FY 2015 FY 2016 FY 2017 To Program Element 42.067 6.509 5.000-5.000 41.500 30.000
Exhibit R-2, RDT&E Budget Item Justification: PB 2013 Air Force DATE: February 2012 COST ($ in Millions) FY 2011 FY 2014 FY 2015 FY 2016 FY 2017 To Program Element 42.067 6.509 5.000-5.000 41.500 30.000
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks
 Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
The Military Health System Strategic Plan
 THE MILITARY HEALTH SYSTEM The Military Health System Strategic Plan Achieving a Better, Stronger, and More Relevant Military Health System 8 OCTOBER 2014 Table of Contents 1. INTRODUCTION... 2 The Quadruple
THE MILITARY HEALTH SYSTEM The Military Health System Strategic Plan Achieving a Better, Stronger, and More Relevant Military Health System 8 OCTOBER 2014 Table of Contents 1. INTRODUCTION... 2 The Quadruple
DOD INSTRUCTION MEDICAL READINESS TRAINING (MRT)
") DOD INSTRUCTION 1322.24 MEDICAL READINESS TRAINING (MRT) Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: March 16, 2018 Releasability: Cleared for
DOD INSTRUCTION 1322.24 MEDICAL READINESS TRAINING (MRT) Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: March 16, 2018 Releasability: Cleared for
Department of Defense DIRECTIVE
 Department of Defense DIRECTIVE NUMBER 5136.12 May 31, 2001 Certified Current as of November 21, 2003 SUBJECT: TRICARE Management Activity (TMA) DA&M References: (a) Title 10, United States Code (b) DoD
Department of Defense DIRECTIVE NUMBER 5136.12 May 31, 2001 Certified Current as of November 21, 2003 SUBJECT: TRICARE Management Activity (TMA) DA&M References: (a) Title 10, United States Code (b) DoD
Subj: MEDICAL AND DENTAL TREATMENT FACILITY CUSTOMER RELATIONS PROGRAM
 DEPARTMENT OF THE NAVY BUREAU OF MEDICINE AND SURGERY 7700 ARLINGTON BOULEVARD FALLS CHURCH VA 22042 IN REPLY REFER TO BUMEDINST 6300.10C BUMED-M31 BUMED INSTRUCTION 6300.10C From: Chief, Bureau of Medicine
DEPARTMENT OF THE NAVY BUREAU OF MEDICINE AND SURGERY 7700 ARLINGTON BOULEVARD FALLS CHURCH VA 22042 IN REPLY REFER TO BUMEDINST 6300.10C BUMED-M31 BUMED INSTRUCTION 6300.10C From: Chief, Bureau of Medicine
UNCLASSIFIED. UNCLASSIFIED Defense Information Systems Agency Page 1 of 11 R-1 Line #189
 Exhibit R-2, RDT&E Budget Item Justification: PB 2015 Defense Information Systems Agency : March 2014 0400: Research, Development, Test & Evaluation, Defense-Wide / BA 7: Operational Systems Development
Exhibit R-2, RDT&E Budget Item Justification: PB 2015 Defense Information Systems Agency : March 2014 0400: Research, Development, Test & Evaluation, Defense-Wide / BA 7: Operational Systems Development
Department of Defense Consolidated Adjudications Facility
 Department of Defense Consolidated Adjudications Facility NATIONAL DEFENSE INDUSTRIAL (NDIA) AND THE AEROSPACE INDUSTRIES ASSOCIATION (AIA) DIRECTOR, NED FISH DOD CONSOLIDATED ADJUDICATIONS FACILITY November
Department of Defense Consolidated Adjudications Facility NATIONAL DEFENSE INDUSTRIAL (NDIA) AND THE AEROSPACE INDUSTRIES ASSOCIATION (AIA) DIRECTOR, NED FISH DOD CONSOLIDATED ADJUDICATIONS FACILITY November
Sustainment, Restoration and Modernization (SRM) Overview 2017 World Wide Energy Conference
 Overview 2017 World Wide Energy Conference") DEFENSE LOGISTICS AGENCY ENERGY AMERICA S COMBAT FUEL SUPPORT LOGISTICS AGENCY Sustainment, Restoration and Modernization (SRM) Overview 2017 World Wide Energy Conference AGENDA Mission Organization Processes
DEFENSE LOGISTICS AGENCY ENERGY AMERICA S COMBAT FUEL SUPPORT LOGISTICS AGENCY Sustainment, Restoration and Modernization (SRM) Overview 2017 World Wide Energy Conference AGENDA Mission Organization Processes
TITLE VII - NDAA for FY 2017
 TITLE VII - NDAA for FY 2017 SECTION 701 TRICARE SELECT AND OTHER TRICARE REFORM Establishes TRICARE Select as the self-managed, preferred provider option that would replace TRICARE Standard and Extra
TITLE VII - NDAA for FY 2017 SECTION 701 TRICARE SELECT AND OTHER TRICARE REFORM Establishes TRICARE Select as the self-managed, preferred provider option that would replace TRICARE Standard and Extra
Driving Business Value for Healthcare Through Unified Communications
 Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
Driving Business Value for Healthcare Through Unified Communications Even the healthcare sector is turning to technology to take a 'connected' approach, as organizations align technology and operational
Military Health System. The Honorable William Winkenwerder, Jr., MD, MBA Assistant Secretary of Defense for Health Affairs. and
 Not for publication until released by Committee on Armed Services United States Senate Military Health System An Overview Statement By The Honorable William Winkenwerder, Jr., MD, MBA Assistant Secretary
Not for publication until released by Committee on Armed Services United States Senate Military Health System An Overview Statement By The Honorable William Winkenwerder, Jr., MD, MBA Assistant Secretary