Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm
|
|
|
- Dora Kelly
- 5 years ago
- Views:
Transcription
1 Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust
2 What is medical error? Medical errors can be defined as the failure of a planned action to be completed as intended or the use of a wrong plan to achieve an aim. (IOM To Err is Human Nov 1999) Mortality Morbidity Financial Reputational second victim

3 Error vs Harm Not all error leads to harm Not all harm includes an error
4 Hospital associated harm Unintended, physical injury resulting from or contributed to by medical care that requires additional monitoring, treatment or hospitalization, or that results in death. Category E: Temporary harm to the patient and required intervention Category F: Temporary harm to the patient and required initial or prolonged hospitalization Category G: Permanent patient harm Category H: Intervention required to sustain life Category I: Patient death IHI Global Trigger Tool
5 Types of error Diagnostic i. Error or delay in diagnosis ii. Failure to employ indicated tests iii. Use of outmoded tests or therapy iv. Failure to act on results of monitoring or testing Treatment i. Error in the performance of an operation, procedure, or test ii. Error in administering the treatment iii. Error in the dose or method of using a drug iv. Avoidable delay in treatment or in responding to an abnormal test v. Inappropriate (not indicated) care Preventive i. Failure to provide prophylactic treatment ii. Inadequate monitoring or follow-up of treatment Other i. Failure of communication ii. Equipment failure iii. Other system failure
6
7 Reducing error to reduce harm Multiple errors occur every day Not all errors reach the patient Some errors more likely than others Difficult to predict in a complex environment How do you know where to start?
8 How Safe is Healthcare? Health Care

9 Where Should We Be? Health Care Blood Transfusion Anesthesia
10
11 Case 1 - Sepsis First weekend in august Elderly woman presents to ED with urinary sepsis Seen by ED doctor within 30 minutes dose of antibiotics prescribed Seen by EAU consultant & junior within 80 minutes (still in ED) agreed sepsis Consultant asked junior to prescribe meds
12 Case 1 - sepsis Patient transferred to EAU (9pm) EAU nurse did not check medicines chart Patient transferred to post acute ward late due to bed pressures (11pm) Ward nurse noted no regular antibiotics prescribed Put on routine doctors job list for review as patient EWS ok
13 Case 1 - sepsis Junior doctor picks up task next day ensures antibiotics dosed and given (but 24 hours since first dose) Patient reviewed EWS 1 & seems ok Patient deteriorated acutely 6 hours later Cardiac arrest unsuccessful CPR
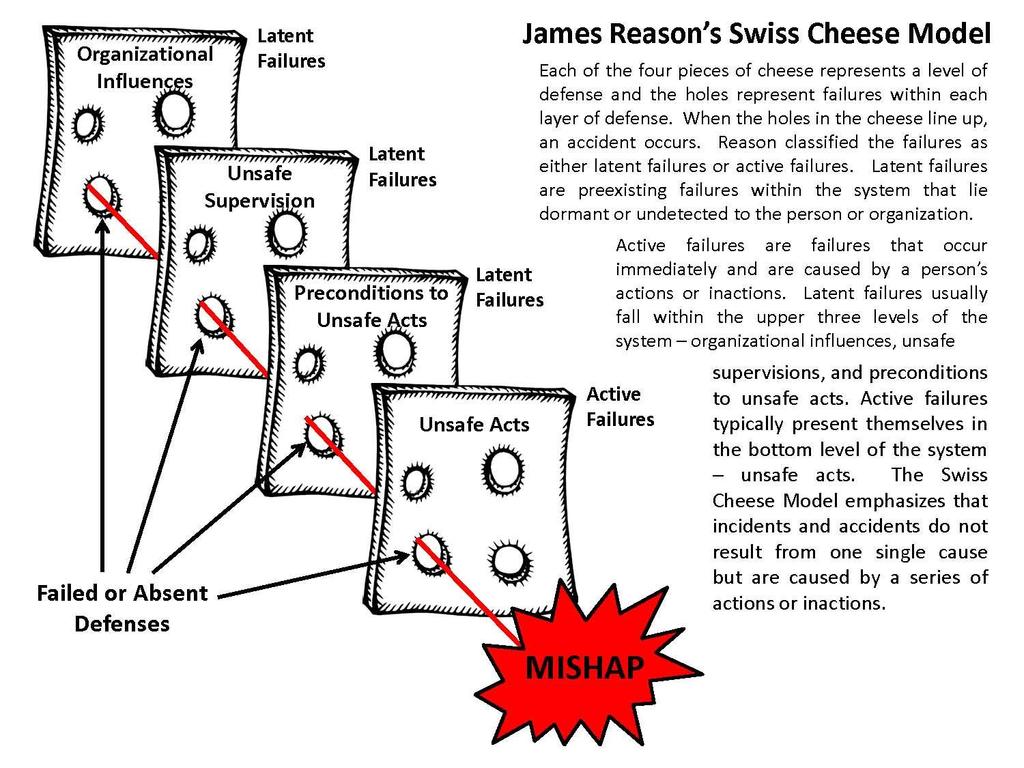
14 Case 1 - Sepsis August & weekend precondition to unsafe acts Atypical method of prescribing in ED precondition to unsafe act, unsafe supervision Seen by EAU consultant & junior together - organisational influences, precondition to unsafe act Consultant asked junior to prescribe meds (antibiotics omitted) unsafe act BUT unsafe supervision, organisational influences,
15 Case 1 - sepsis EAU nurse didn t check meds chart unsafe act organisational, precondition Patient transferred to post acute ward 2 hours later for bed pressures (11pm) organisational, preconditional Ward team noted failure, didn t act unsafe act - preconditions Put on routine doctors job list unsafe act, BUT precondition, organisational

16 Case 1 - sepsis 4 active failures omission, prescription, communication, escalation Multiple latent failures Series of reliability issues
17 Reliability Measured as the inverse of the system s failure rate Failure free operation over time Chaotic: failure in greater than 20% of events 10-1 : 1 or 2 failures out of : <5 failures per : <5 failures per : <5 failures per Chapter 4 Reliability & Resilience Roger Resar & Frank Federico The Essential Guide for Patient Safety Officers, June 13

18 Doing your best, with the best possible resources achieves reliability around 80% of the time This includes: Standard order sheets, multiple choice protocols written policies/procedures Personal check lists Feedback of compliance Working harder Awareness & training Posters in the loo
19 Reliability First process: clerking document = 80% reliable Second process: PTWR check = 80% reliable Second process should pick up 80% of slips in first process (i.e. 16%) Overall reliability = 96%
20 Step 1 simplify & standardise Step 2 controls to prevent error Step 3 errors that slip through studied & redesigned if needed. Reliability
21 Back to Case 1 Standardise: i. antibiotic prescribing across ED & EAU ii. ED EAU handover, EAU to ward handover iii. sepsis education for all clinical areas iv. communication & escalation Control: i. check of drugs chart at each handoff ii. checklist for identifying patients to move by EAU coordinator iii. Second level check for prescribing PTWR vs Meds rec vs Board round
22 Case 2 elective vs non-elective 22 year old patient presented with viral illness and headache PTWR recommended lumbar puncture to investigate? Viral meningitis LP done patient feeling much better On call junior doctor saw at about 7pm results not available Sent patient home we will write with results Patient returned next day with seizure
23 Elective vs non elective Junior doctor working on Neuro ward different population Essentially unsafe act No controls in system to prevent it However LP results were normal Independent medical opinion viral illness with lowered seizure threshold not preventable
24 Actions Standardise: 1 standard for documentation of consultant review Clear documentation of discharge/ transfer plans Control: Discharge by registrar or consultant input only No acute patients discharged without full LP results
25 Case 3 communication Patient with acute on chronic renal failure K + result 6.2 HAN allocated to on call FY1 Phoned registrar for advice Reg advised 15 units actrapid FY1 heard 50 units actrapid Nurse thought big dose but reassured that reg advised it Patient suffered hypoglycaemic fit (no long term sequelae)
26 Case 3 communication Active failure lack of knowledge Predisposition to unsafe act no available policy Latent failures unsafe supervision (did reg need to see patient or review notes) Organisational nurse knew dose wrong but felt falsely reassured Human Factors Just a routine operation:
27 Case 3 communication Simplify: Written guidelines for hyperkalaemia Made guidelines findable on intranet Control: Work with nurses around what constitutes a large dose (not just for insulin) Worked to provide psychological safety for check and challenge Junior doctor shared story for medicines safety work
28 Case 4 unexplained drowsiness 34 year old prisoner 2 officers in situ Presented Tuesday with haematemesis All medicines prescribed as per prison chart OGD Wednesday gastritis Reviewed Thursday unexpectedly drowsy Patient admitted to concealing & selling some of his diazepam in prison diazepam stopped Friday less drowsy not fully recovered Discharged to prison hospital ward Saturday readmitted large SDH

29 A pattern of deviation in judgement whereby inferences may be drawn in an illogical pattern Confirmation bias seeking information to confirm a conclusion Anchoring bias the act of relying too heavily to one piece of information Cognitive bias We all have cognitive bias & need to be aware of them
30 Bias 52 year old Polish man, poor spoken english Complains of unsteadiness, weakness & blurred vision Haemoglobin 52 Previous admission 6/12 ago with bleeding duodenal ulcer GI Bleed (alcohol?) Waldenstroms Macroglobulinaemia retinal haemorrhages, bone marrow failure
31 Bias 73 year old lady, acute episodic confusion 3 rd admission in 3 months Smells a bit.. urine dip pro and leuk?delirium & UTI Liver Abscess None of her previous urine samples showed any growth
32 Cognitive Bias Pattern recognition helps in medicine Acute medicine relies on balancing risks Personal/ reflective learning Discussion and challenge Structured approach to diagnosis Reassess diagnosis if ongoing issues Second opinion
33 A Perfect EAU Simple pathways with minimal variation Accessible information and protocols Standardisation of documentation & practices Well trained and supervised staff Early senior review Built in checks, with scheduling & role allocation Culture of openness and check/challenge Minimal handoffs Long term stable work force

34 Sound familiar?
35 Recommendations Learn (& teach) about reliability science, human factors & quality improvement Consider predictive tools when planning changes e.g. failure mode event analysis Embrace systems thinking, lose blame Reports incidents, learn from them, use the whole team. Consider mortality & morbidity reviews, global trigger tool etc to identify patterns
36 In our defence patients a month 55 beds 85% of medical take managed wholly in EAU EAU are high incident reporters & investigators Considered Outstanding by CQC High scores for patient and staff satisfaction
37 Questions?
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Sign up to Safety Drivers and Measurement
 Sign up to Safety Drivers and Measurement Expert Partner Nicola Davey Topics for today Driver diagrams Linking improvement aims to strategic objectives Generating simple improvement measures Measures
Sign up to Safety Drivers and Measurement Expert Partner Nicola Davey Topics for today Driver diagrams Linking improvement aims to strategic objectives Generating simple improvement measures Measures
This matter was initiated by a letter from the complainant received on March 20, A response from Dr. Justin Clark was received on May 11, 2017.
 COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE C Dr. Justin Clark License Number: 016409 Investigations Committee C of the College of Physicians and Surgeons
COLLEGE OF PHYSICIANS AND SURGEONS OF NOVA SCOTIA SUMMARY OF DECISION OF INVESTIGATION COMMITTEE C Dr. Justin Clark License Number: 016409 Investigations Committee C of the College of Physicians and Surgeons
Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development
 Review of National Reporting and Learning System (NRLS) incident data relating to discharge from acute and mental health trusts August 2014 NHS England INFORMATION READER BOX Directorate Medical Operations
Review of National Reporting and Learning System (NRLS) incident data relating to discharge from acute and mental health trusts August 2014 NHS England INFORMATION READER BOX Directorate Medical Operations
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
System enablers practical aspects Chair Lesley Anne Smith
 System enablers practical aspects Chair Lesley Anne Smith Time Topic Room Optional lunchtime sessions, numbers limited to 50 per room, catering provided in the room 13.15 QI Harris Level 1 Service Users
System enablers practical aspects Chair Lesley Anne Smith Time Topic Room Optional lunchtime sessions, numbers limited to 50 per room, catering provided in the room 13.15 QI Harris Level 1 Service Users
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. 170008/S Service Atypical haemolytic uraemic syndrome (ahus) (all ages) Commissioner Lead Provider Lead Period Date of Review
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. 170008/S Service Atypical haemolytic uraemic syndrome (ahus) (all ages) Commissioner Lead Provider Lead Period Date of Review
The Royal Wolverhampton Hospitals NHS Trust
 The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
Kate Beaumont. Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign.
 Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Alison Hunter. Improvement Advisor, Acute Adult Safety Programme. Healthcare Improvement Scotland
 Alison Hunter Improvement Advisor, Acute Adult Safety Programme Healthcare Improvement Scotland Acute Adult 2008 what we did Leadership Medicines Perioperative Critical Care Reduce Mortality & Harm General
Alison Hunter Improvement Advisor, Acute Adult Safety Programme Healthcare Improvement Scotland Acute Adult 2008 what we did Leadership Medicines Perioperative Critical Care Reduce Mortality & Harm General
Post-operative and Discharge Pathways for PBM Claire L J Atterbury CNS Transfusion and Haematology
 Post-operative and Discharge Pathways for PBM Claire L J Atterbury CNS Transfusion and Haematology 1 Plan for the worst and hope for the best claire.atterbury@qehkl.nhs.uk 2 Where were we? What year? The
Post-operative and Discharge Pathways for PBM Claire L J Atterbury CNS Transfusion and Haematology 1 Plan for the worst and hope for the best claire.atterbury@qehkl.nhs.uk 2 Where were we? What year? The
Thinking Differently Acting Differently. Higher staff satisfaction = better patient outcomes & better patient experience
 Thinking Differently Acting Differently Higher staff satisfaction = better patient outcomes & better patient experience Staff Satisfaction is the best indicator of a High Quality Culture Nursing contribution
Thinking Differently Acting Differently Higher staff satisfaction = better patient outcomes & better patient experience Staff Satisfaction is the best indicator of a High Quality Culture Nursing contribution
The Reliable Design of Obstetric and Gynecologic Care
 VECKAN 2015 The Reliable Design of Obstetric and Gynecologic Care Peter Cherouny, M.D. Emeritus Professor, Obstetrics, Gynecology and Reproductive Sciences University of Vermont, USA Chair, Perinatal Improvement
VECKAN 2015 The Reliable Design of Obstetric and Gynecologic Care Peter Cherouny, M.D. Emeritus Professor, Obstetrics, Gynecology and Reproductive Sciences University of Vermont, USA Chair, Perinatal Improvement
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Case study: how reliable are our healthcare systems?
 Case study: how reliable are our healthcare systems? CMSSQ Centre for Medication Safety & Service Quality Professor Bryony Dean Franklin Centre for Medication Safety and Service Quality Imperial College
Case study: how reliable are our healthcare systems? CMSSQ Centre for Medication Safety & Service Quality Professor Bryony Dean Franklin Centre for Medication Safety and Service Quality Imperial College
Coroner's Corner - Inquest into the death of Gwendoline Mead
 Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Improving medical handover at the weekend: a quality improvement project
 BMJ Quality Improvement Reports 2015; u207153.w2899 doi: 10.1136/bmjquality.u207153.w2899 Improving medical handover at the weekend: a quality improvement project Emma Michael, Chandni Patel Broomfield
BMJ Quality Improvement Reports 2015; u207153.w2899 doi: 10.1136/bmjquality.u207153.w2899 Improving medical handover at the weekend: a quality improvement project Emma Michael, Chandni Patel Broomfield
Sepsis The Silent Killer in the NHS
 Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Worcestershire Acute Hospitals NHS Trust
 Worcestershire Acute Hospitals NHS Trust Worcestershire Royal Hospital Quality Report Charles Hastings Way Worcester WR5 1DD Tel: 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit: 12,
Worcestershire Acute Hospitals NHS Trust Worcestershire Royal Hospital Quality Report Charles Hastings Way Worcester WR5 1DD Tel: 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit: 12,
This is a high level overview report to update the Board on the Acute Adult Safety Programme consisting of the following sections:
 Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
Adverse Events in Hospitals: How Many and Why Not Reported. Fran Griffin Senior Manager Clinical Programs, BD
 Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Improving Diabetes Management in Care Homes within Swale CCG
 Improving Diabetes Management in Care Homes within Swale CCG An Education Model to support Unregistered Practitioners in Diabetes Care and Delegation of Insulin Administration June 2016 Authors: Sarah
Improving Diabetes Management in Care Homes within Swale CCG An Education Model to support Unregistered Practitioners in Diabetes Care and Delegation of Insulin Administration June 2016 Authors: Sarah
Overview. Dr Stephen Gulliford & AKI Specialist Nurse Suzanne Wilson Page 1
 Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Step by step measurement guide
 Step by step measurement guide The guide has been produced under a creative commons license please use the symbols shown for guidance if you wish to use or adapt the material This edited presentation has
Step by step measurement guide The guide has been produced under a creative commons license please use the symbols shown for guidance if you wish to use or adapt the material This edited presentation has
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in
 These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in the UK and beyond. 1 The first EWS was devised in 1997
These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in the UK and beyond. 1 The first EWS was devised in 1997
Community DVT Service. Phase 3: Anticoagulation at DVT Treatment Centres
 Community DVT Service Quick Reference Guide Phase - Anticoagulation Phase : Anticoagulation at DVT Treatment Centres If a Patient has had a positive Ultrasound Scan they attend one of the DVT Treatment
Community DVT Service Quick Reference Guide Phase - Anticoagulation Phase : Anticoagulation at DVT Treatment Centres If a Patient has had a positive Ultrasound Scan they attend one of the DVT Treatment
Safe medication practice what can we learn from root cause analysis and related methods?
 Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
NHS TAYSIDE MORTALITY REVIEW PROGRAMME
 NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
@ncepod #tracheostomy
 @ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
@ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
HOSPITAL IN THE HOME (HITH) INFORMATION SHEET
 INFORMATION SHEET") What is HITH? HOSPITAL IN THE HOME (HITH) INFORMATION SHEET In 1994 the Hospital in the Home (HITH) Program was commenced as a pilot. Hospitals were invited to apply to become HITH providers and 43 were
What is HITH? HOSPITAL IN THE HOME (HITH) INFORMATION SHEET In 1994 the Hospital in the Home (HITH) Program was commenced as a pilot. Hospitals were invited to apply to become HITH providers and 43 were
A mechanism for measuring and improving patient experience on an acute medical unit
 A mechanism for measuring and improving patient experience on an acute medical unit This Future Hospital Programme case study comes from Grantham and District Hospital, part of the United Lincolnshire
A mechanism for measuring and improving patient experience on an acute medical unit This Future Hospital Programme case study comes from Grantham and District Hospital, part of the United Lincolnshire
PHARMACIST INDEPENDENT PRESCRIBING MEDICAL PRACTITIONER S HANDBOOK
 PHARMACIST INDEPENDENT PRESCRIBING MEDICAL PRACTITIONER S HANDBOOK 0 CONTENTS Course Description Period of Learning in Practice Summary of Competencies Guide to Assessing Competencies Page 2 3 10 14 Course
PHARMACIST INDEPENDENT PRESCRIBING MEDICAL PRACTITIONER S HANDBOOK 0 CONTENTS Course Description Period of Learning in Practice Summary of Competencies Guide to Assessing Competencies Page 2 3 10 14 Course
A safe system framework for recognising and responding to children at risk of deterioration. July 2016
 A safe system framework for recognising and responding to children at risk of deterioration July 2016 Background Research shows that failure to recognise and treat patients whose condition is deteriorating
A safe system framework for recognising and responding to children at risk of deterioration July 2016 Background Research shows that failure to recognise and treat patients whose condition is deteriorating
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Three steps to success
 Inpatient care for people with diabetes at Russells Hall Hospital (The Dudley Group NHS Foundation Trust) Three steps to success The ThinkGlucose team at Russells Hall Hospital developed a three-stage
Inpatient care for people with diabetes at Russells Hall Hospital (The Dudley Group NHS Foundation Trust) Three steps to success The ThinkGlucose team at Russells Hall Hospital developed a three-stage
Assessing Non-Technical Skills. A Guide to the NOTSS Tool Adapted for the Labour Ward
 Assessing Non-Technical Skills A Guide to the NOTSS Tool Adapted for the Labour Ward Acknowledgements The original NOTSS system was developed and evaluated in a multi-disciplinary project comprising surgeons,
Assessing Non-Technical Skills A Guide to the NOTSS Tool Adapted for the Labour Ward Acknowledgements The original NOTSS system was developed and evaluated in a multi-disciplinary project comprising surgeons,
NCEPOD and BTS Acute NIV
 NCEPOD and BTS Acute NIV Key points by Dr Lisa Vincent-Smith and Iain Wheatley Nurse Consultant BTS NIV Quality Standards (draft consultations Sept 17) Case study 1 An elderly patient was admitted with
NCEPOD and BTS Acute NIV Key points by Dr Lisa Vincent-Smith and Iain Wheatley Nurse Consultant BTS NIV Quality Standards (draft consultations Sept 17) Case study 1 An elderly patient was admitted with
CRAB : Big Scale Routine Data as First Alert
 Workshop 3: Patient safety and mhealth/big data/hand held services CRAB : Big Scale Routine Data as First Alert Ingo Gurcke, Dipl. Kaufmann (FH), Marsh Medical Consulting GmbH, Managing Director, Germany
Workshop 3: Patient safety and mhealth/big data/hand held services CRAB : Big Scale Routine Data as First Alert Ingo Gurcke, Dipl. Kaufmann (FH), Marsh Medical Consulting GmbH, Managing Director, Germany
Standardised handover protocol: increasing safety awareness
 Standardised handover protocol: increasing safety awareness This Future Hospital Programme case study details how Dr Shirine Boardman from Grantham and District Hospital, United Lincolnshire Hospitals
Standardised handover protocol: increasing safety awareness This Future Hospital Programme case study details how Dr Shirine Boardman from Grantham and District Hospital, United Lincolnshire Hospitals
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart
 Observation Chart") CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
NHS HIGHLAND. Significant Event Report
 ` NHS HIGHLAND Significant Event Report Report to - Quality & Patient Safety Raigmore Management Team of Findings from Significant Event Review Meeting QPS040 26/10/2011 1.0 Outline of Significant Event
` NHS HIGHLAND Significant Event Report Report to - Quality & Patient Safety Raigmore Management Team of Findings from Significant Event Review Meeting QPS040 26/10/2011 1.0 Outline of Significant Event
Overall rating for this location. Quality Report. Ratings. Overall summary. Are services safe? Are services effective? Are services responsive?
 John Munroe Hospital Rudyard Quality Report Horton Road Rudyard Leek Staffordshire ST13 8RU ST13 8RU Tel:01538 306244 Website:www.johnmunroehospital.co.uk Date of inspection visit: 11th January 2016 Date
John Munroe Hospital Rudyard Quality Report Horton Road Rudyard Leek Staffordshire ST13 8RU ST13 8RU Tel:01538 306244 Website:www.johnmunroehospital.co.uk Date of inspection visit: 11th January 2016 Date
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
Some Practical Tips on Being a Senior Pediatric Resident at McMaster
 Some Practical Tips on Being a Senior Pediatric Resident at McMaster This document is meant to provide practical information to help Junior pediatric residents transition to the Senior pediatric resident
Some Practical Tips on Being a Senior Pediatric Resident at McMaster This document is meant to provide practical information to help Junior pediatric residents transition to the Senior pediatric resident
Introductions. Welcome to the APAC Global Trigger Tool Session. Dr Carol Haraden IHI Gillian Robb CMDHB. Carol Haraden.
 Welcome to the APAC Global Trigger Tool Session Dr Carol Haraden IHI Gillian Robb CMDHB Carol Haraden Introductions Gillian Robb Outline for this session Introduction to the Global Trigger Tool What is
Welcome to the APAC Global Trigger Tool Session Dr Carol Haraden IHI Gillian Robb CMDHB Carol Haraden Introductions Gillian Robb Outline for this session Introduction to the Global Trigger Tool What is
The Scottish Public Services Ombudsman Act 2002
 Scottish Public Services Ombudsman The Scottish Public Services Ombudsman Act 2002 Investigation Report UNDER SECTION 15(1)(a) SPSO 4 Melville Street Edinburgh EH3 7NS Tel 0800 377 7330 SPSO Information
Scottish Public Services Ombudsman The Scottish Public Services Ombudsman Act 2002 Investigation Report UNDER SECTION 15(1)(a) SPSO 4 Melville Street Edinburgh EH3 7NS Tel 0800 377 7330 SPSO Information
3/9/2010. Objectives. Pharmacist Role in Medication Safety and Regulatory Compliance
 Pharmacist Role in Medication Safety and Regulatory Compliance Janet Greiwe Vice President, Systems Management Cleveland County Health System Objectives By the end of this presentation, you should be able
Pharmacist Role in Medication Safety and Regulatory Compliance Janet Greiwe Vice President, Systems Management Cleveland County Health System Objectives By the end of this presentation, you should be able
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
National Mortality Case Record Review Programme. Using the structured judgement review method A guide for reviewers (England)
") National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
MEDICINE SICK DAY RULES CARDS INTERIM EVALUATION
 INTRODUCTION MEDICINE SICK DAY RULES CARDS INTERIM EVALUATION Report by: Clare Morrison, Lead Pharmacist (North), NHS Highland Dr Martin Wilson, Consultant Physician, Raigmore Hospital, NHS Highland Correspondence
INTRODUCTION MEDICINE SICK DAY RULES CARDS INTERIM EVALUATION Report by: Clare Morrison, Lead Pharmacist (North), NHS Highland Dr Martin Wilson, Consultant Physician, Raigmore Hospital, NHS Highland Correspondence
Respiratory Clinical Review of Patients with Community Acquired Pneumonia
 Respiratory Clinical Review of Patients with Community Acquired Pneumonia DrPeter Wu Staff Specialist Department of Respiratory & Sleep Medicine Westmead Hospital Western Sydney Local Health District How
Respiratory Clinical Review of Patients with Community Acquired Pneumonia DrPeter Wu Staff Specialist Department of Respiratory & Sleep Medicine Westmead Hospital Western Sydney Local Health District How
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Wellesley Hospital Eastern Avenue, Southend-on-Sea, SS2
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Wellesley Hospital Eastern Avenue, Southend-on-Sea, SS2
PAPERLESS ED? AN EPIC EXPERIENCE. Adrian Boyle Cambridge University Hospitals Foundation
 PAPERLESS ED? AN EPIC EXPERIENCE Adrian Boyle Cambridge University Hospitals Foundation Trust @dradrianboyle We d like you to come and speak at Bournemouth Great! What on? Violence? Quality? Crowding?
PAPERLESS ED? AN EPIC EXPERIENCE Adrian Boyle Cambridge University Hospitals Foundation Trust @dradrianboyle We d like you to come and speak at Bournemouth Great! What on? Violence? Quality? Crowding?
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Online library of Quality, Service Improvement and Redesign tools. Reliable design. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Reliable design collaboration trust respect innovation courage compassion Reliable design What is it? Patients receiving the right care,
Online library of Quality, Service Improvement and Redesign tools Reliable design collaboration trust respect innovation courage compassion Reliable design What is it? Patients receiving the right care,
Kupu Taurangi Hauora o Aotearoa
 Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
Ambulatory Emergency Care A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals. The Pennine Acute Hospitals NHS Trust
 Ambulatory Emergency Care A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine Acute Hospitals NHS Trust A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine
Ambulatory Emergency Care A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine Acute Hospitals NHS Trust A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine
Quality Improvement Scorecard February 2017
 Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Medicines Reconciliation: Standard Operating Procedure
 Clinical Medicines Reconciliation: Standard Operating Procedure Document Control Summary Status: Version: Author/Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
Clinical Medicines Reconciliation: Standard Operating Procedure Document Control Summary Status: Version: Author/Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
2/15/2016. To Err is Human. Patient Safety in OB/GYN: Current Trends. At the conclusion of this talk. Published by IOM in 1999
 Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Patient Safety in OB/GYN: Current Trends Joseph R. Biggio Jr., MD Objectives At the conclusion of this talk Comprehend the underlying rationale for the increasing emphasis on patient safety Understand
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE
 DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE Ambulatory Care Unit Standard Operational Policy Document Control Reference No: First published: November 2014 Version: 004 Current Version Published:
DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE Ambulatory Care Unit Standard Operational Policy Document Control Reference No: First published: November 2014 Version: 004 Current Version Published:
To Err is Human To Delay is Deadly Ten years later, a million lives lost, billions of dollars wasted
 1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
1999 Institute of Medicine study estimated that as many as 98,000 people die in any given year from medical errors that occur in hospitals. To Err is Human To Delay is Deadly Ten years later, a million
The investigation of a complaint by Dr A against Cardiff and Vale University Health Board
 The investigation of a complaint by Dr A against Cardiff and Vale University Health Board A report by the Public Services Ombudsman for Wales Case: 201401302 Contents Page Introduction 3 Summary 4 The
The investigation of a complaint by Dr A against Cardiff and Vale University Health Board A report by the Public Services Ombudsman for Wales Case: 201401302 Contents Page Introduction 3 Summary 4 The
Mental Health Community Service User Survey 2017 Management Report
 Quality Health Mental Health Community Service User Survey 2017 Management Report Produced 1 August 2017 by Quality Health Ltd Table of Contents Background 3 Introduction 4 Observations and Recommendations
Quality Health Mental Health Community Service User Survey 2017 Management Report Produced 1 August 2017 by Quality Health Ltd Table of Contents Background 3 Introduction 4 Observations and Recommendations
Sepsis guidance implementation advice for adults
 Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Transitions in Care. Why They Are Important and How to Improve Them. U. Ohuabunwa MD
 Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
Transitions in Care Why They Are Important and How to Improve Them U. Ohuabunwa MD Learning Objectives Define transitions in care and the roles patients and providers play in safe transitions Describe
NP Discharge & Admission: Legislative Authority
 The Canadian Nurses Protective Society Admission & Discharge: Professional Liability Considerations Chantal Léonard, CEO, CNPS OHA Conference, March 29, 2012 NP Discharge & Admission: Legislative Authority
The Canadian Nurses Protective Society Admission & Discharge: Professional Liability Considerations Chantal Léonard, CEO, CNPS OHA Conference, March 29, 2012 NP Discharge & Admission: Legislative Authority
CLINICAL PROTOCOL FOR THE IDENTIFICATION OF SERVICE USERS
 CLINICAL PROTOCOL FOR THE IDENTIFICATION OF SERVICE USERS RATIONALE All Professionals/healthcare workers are personally accountable for their practice and, in the exercise of their professional accountability,
CLINICAL PROTOCOL FOR THE IDENTIFICATION OF SERVICE USERS RATIONALE All Professionals/healthcare workers are personally accountable for their practice and, in the exercise of their professional accountability,
Overall rating for this trust. Quality Report. Ratings
 Worcestershire Acute Hospitals NHS Trust Quality Report Worcestershire Royal Hospital Charles Hastings Way Worcester WR5 1DD Tel: : 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit:
Worcestershire Acute Hospitals NHS Trust Quality Report Worcestershire Royal Hospital Charles Hastings Way Worcester WR5 1DD Tel: : 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit:
West Middlesex Junior Doctors Handbook in Colorectal Surgery
 West Middlesex Junior Doctors Handbook in Colorectal Surgery Page 1 of 10 INTRODUCTION Welcome to surgery and to the colorectal team! This guide is meant to be just that, a guide and has been principally
West Middlesex Junior Doctors Handbook in Colorectal Surgery Page 1 of 10 INTRODUCTION Welcome to surgery and to the colorectal team! This guide is meant to be just that, a guide and has been principally
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
Acute kidney injury Keeping kidneys healthy: The AKI programme board. Dr Richard Fluck, National Clinical Director (Renal) NHS England
 NHS England") Acute kidney injury Keeping kidneys healthy: The AKI programme board Dr Richard Fluck, National Clinical Director (Renal) NHS England NHS Outcomes Framework NHS Five Year Forward View A vision for the
Acute kidney injury Keeping kidneys healthy: The AKI programme board Dr Richard Fluck, National Clinical Director (Renal) NHS England NHS Outcomes Framework NHS Five Year Forward View A vision for the
National clinical audit of inpatient care for adults with ulcerative colitis
 National clinical audit of inpatient care for adults with ulcerative colitis UK inflammatory bowel disease (IBD) audit Executive summary report June 2014 Prepared by the Clinical Effectiveness and Evaluation
National clinical audit of inpatient care for adults with ulcerative colitis UK inflammatory bowel disease (IBD) audit Executive summary report June 2014 Prepared by the Clinical Effectiveness and Evaluation
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Modified Early Warning Score Policy.
 Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Trust Policy and Procedure Modified Early Warning Score Policy. Document ref. no: PP(15)271 For use in (clinical areas): For use by (staff groups): For use for (patients): Document owner: Status: All clinical
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING
 Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Online library of Quality, Service Improvement and Redesign tools. Discharge planning. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
Measuring Medication Harm: Advantages of Using a Trigger Tool. Frank Federico Executive Director
 Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
Antimicrobial Stewardship in Continuing Care. Nursing Home Acquired Pneumonia Clinical Checklist
 Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
Our community nursing roles
 Our community nursing roles Community Nursing Services provide nursing care to house-bound patients within the community. Our aim is to help patients to remain healthy and independent for as long as possible,
Our community nursing roles Community Nursing Services provide nursing care to house-bound patients within the community. Our aim is to help patients to remain healthy and independent for as long as possible,
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
Reconciliation of Medicines on Admission to Hospital
 Reconciliation of Medicines on Admission to Hospital Policy Title State previous title where relevant. State if Policy New or Revised Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For
Reconciliation of Medicines on Admission to Hospital Policy Title State previous title where relevant. State if Policy New or Revised Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For
Commissioning for Quality & Innovation (CQUIN)
") Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Predict, prevent & manage AKI: A UK collaboration to detect a devastating condition AKI
 Predict, prevent & manage AKI: A UK collaboration to detect a devastating condition AKI Case Study Acute kidney injury (AKI) is a potentially devastating condition, thought to contribute to the deaths
Predict, prevent & manage AKI: A UK collaboration to detect a devastating condition AKI Case Study Acute kidney injury (AKI) is a potentially devastating condition, thought to contribute to the deaths