Introductions. Welcome to the APAC Global Trigger Tool Session. Dr Carol Haraden IHI Gillian Robb CMDHB. Carol Haraden.
|
|
|
- Bertina Willis
- 6 years ago
- Views:
Transcription
1 Welcome to the APAC Global Trigger Tool Session Dr Carol Haraden IHI Gillian Robb CMDHB Carol Haraden Introductions Gillian Robb
2 Outline for this session Introduction to the Global Trigger Tool What is the Global Trigger Tool Using the Global Trigger Tool Examples / Case studies of improvement initiatives First Do No Harm
3 Patient Harm Common Median incidence of in hospital adverse events: 9.2% Median percentage of preventability: 43.5% Lethal: 7.4% (de Vries st al 2008) Costly In NZ: $10,000 per patient Cost of preventable adverse events was estimated at around $590 million 30% of public hospital expenditure goes toward treating preventable events (Brown et al 2002) Do we have the full picture about patient harm in our DHBs? How many harmed? What are the most common harms? What are the common issues? Where do they occur? Are we successfully improving patient safety?
4 Window on patient harm Voluntary Reporting Internal Incident reporting system Serious & Sentinel Event Morbidity & Mortality Meetings Metrics Routine data Surveillance systems Audits External ACC treatment injury claims Inquests HDC investigations Patient Administration System Coding data Patients Patient complaints Patient surveys Focus groups Qualitative Global Trigger Tool Harms per 1000 patient days Harms per 100 admissions % patients Quantitative harmed Increase the volume of data Broaden the perspective
5 What is the GTT 9 Background Computerized triggers for ADE identification and concurrent intervention David Classen (1990) ADE review identifying 14 triggers accounting for majority of ADE s David Classen (1994) Adverse drug event trigger tool developed for the IHI Idealized Design of the Medication System (1999) ICU Adverse event trigger tool, IHI Idealized Design ICU (2002) Global Trigger Tool testing and spread to US and international hospitals (2004)
6 Why Use Trigger Tools? Traditional reporting of errors, incidents, or events does not reliably occur in the best of cultures in healthcare Voluntary methods underestimate events and concentrate on what is interpreted as being preventable Easily identifies events without complex technology Can be integrated into a good sampling methodology Global Trigger Tool Modules Cares (General) Critical Care Medication Surgery L&D ED
7 C1 C2 C3 C4 C5 C6 C7 C8 C9 C10 C11 C12 C13 C14 C15 Cares Module Triggers Transfusion or use of blood products Any Code or arrest Dialysis Positive blood culture X-Ray or Doppler studies for emboli Abrupt drop of greater than 25% in Hg or Hemtocrit Patient fall Decubiti Readmission within 30 days Restraint use Infection of any kind In hospital Stroke Transfer to higher level of care Any procedure complication Other E Category of Harm NCCMERP Index Temporary harm, intervention required F Temporary harm, initial or prolonged hospitalization G Permanent patient harm H Life sustaining intervention required I Contributing to Death
8 Global Trigger Tool Examples Readmit within 30 days with recurrence of abscess right hip. Readmit next day w/ileus s/p exp lap for tumor. Stopped lasix-acute renal failure. Readmitted in 30 days for wound revision due to incisional seroma. Readmit related with wound infection. Volume Depletion with altered mental status caused by Lasix -resulted in hospital admission. ARF due to nephrotoxicity due to combination of ACE and NSAIDS taken at home. Ischemic colitis had rt hemicolectomy. New onset CP=MI. Unresponsive, coded. Decreased loc & sats on Morphine PCA. Rec'd Narcan. Global Trigger Tool Using the GTT
9 Outline Getting Started Chart review process Data entry & analysis Reporting Next steps GTT in NZ Getting Started: People Organisational commitment to patient safety Executive Sponsor Steering group to support the process Programme lead / Coordinator Reviewers

10 Roles & responsibilities Role Responsibility Time commitment Per month Executive Sponsor Steering Committee Championthe GTT; provide resources ; remove roadblocks Endorse & promote GTT; engage support and participation; supportprogramme lead. 1 hour per month 1 hour per month Programme Lead Coordination of programme & process, oversees data entry, data analysis & reporting 8-10 days per month (0.4 FTE) Review team Completes chart reviews within specified timeframes & meets with team doctor hours month (includes meetings) Physicians Authenticates findings of the reviewers 3-4 hours per month Getting Started: Resources Dedicated space Secure Access to computers Process for managing charts Training & support for reviewers Initial Training Ongoing training and refreshers Data collection tool Database Excel spreadsheet Dedicated database

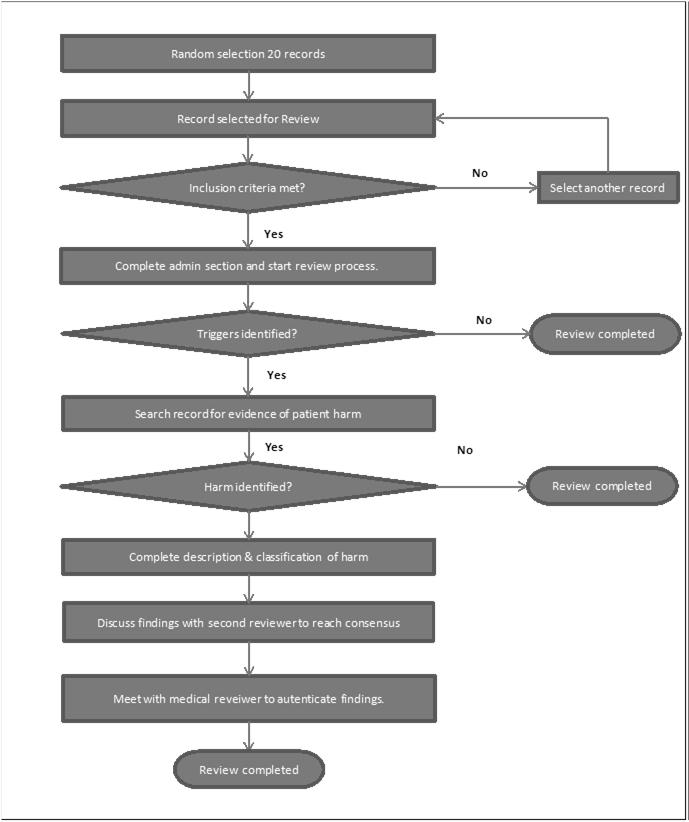
11 Chart Review Process
.")
12 Chart review process 20 minute limit Discharge summary Laboratory results Medication chart & administration record Operative record Nursing notes Physician progress notes If time permits, any other areas of the record (such as History & Physical, Consult notes, or Emergency Department notes). The GTT is not designed to identify all harms, but by using the recommended IHI systematic process, sufficient harms are identified to provide useful information for the organisation Flags for harm Filtering process Modules in GTT Cares Medication Laboratory Surgery Intensive Care Emergency Care Triggers

13 Harm Categories Harm Category E F G H I Description Temporary harm to the patient and required intervention Temporary harm to the patient and required initial or prolonged hospitalisation Permanent patient harm Intervention required to sustain life. Patient death National Coordinating Council for Medication Error Reporting and Prevention Index Managing the data: Data collection tool
14 Florida Hospital AE sub-categories Events related to: Medication Laboratory Patient Care Hospital Acquired infection Surgery & Other procedures Intensive Care When harm occurred Code In Pt Definition AE occurred during this hospital admission Adm 1 Adm 2 AE present on admission, occurred within 30 days of this admission. AE present on admission, occurred between 30 days and 12 months of this admission. Adm 3 AE present on admission, occurred greater than 1 year of this admission. Re- Admit AE present on admission, related to prior discharge, occurred within 30 days of admission.
, Another DHB, Private Hospital, Aged Care Facility, Primary Care Provider, At Home etc Ward X (prior admission at")
15 Where harm occurred Code In Pt Definition EC, ICU, Theatre, Ward X, AT&R etc (during this admission) Adm 1 Adm 2 Adm 3 Re- Admit Ward X (prior admission at CMDHB), Another DHB, Private Hospital, Aged Care Facility, Primary Care Provider, At Home etc Ward X (prior admission at CMDHB), Another DHB, Private Hospital, Aged Care Facility, Primary Care Provider, At Home etc Ward X (prior admission at CMDHB), Another DHB, Private Hospital, Aged Care Facility, Primary Care Provider, At Home etc Ward X (prior admission at CMDHB), Another DHB, Private Hospital, Aged Care Facility, Primary Care Provider, At Home Managing the data: Database


16 Reporting: Metrics Adverse events per 1000 patient days Adverse events per 100 patient admissions Percent admissions with an adverse event. Events by Categories of harm
17 Results Records Reviewed 339 Total events: 152 Events/1,000 bed days: Events/100 admissions: Percent Patients harmed: Event categories: E: 81 (53.29 %) F: 65 (42.76 %) G: 2 (1.32 %) H: 3 (1.32 %) I: 1 (0.66 %)
18 Harm Category E F G H I Description Temporary harm to the patient and required intervention Temporary harm to the patient and required initial or prolonged hospitalisation Permanent patient harm Intervention required to sustain life. Patient death
19 Frontline clinicians Reporting: Who Executive Team Board Purpose of GTT Reporting: What Key results (Metrics + Context) Examples of harms in each category What you are doing about it
20 Next Steps: Drilling down Focus on harms not triggers Start simply Inpatient / non-inpatient Events by sub-categories Common medications Drill deeper Events related to sub-classifications Further record reviews enriched sample Next Steps: Drilling Down Sub-Category Adverse Events Severity N=152 E F G H J Medication/IV Fluids Hospital Acquired Infection Surgery or Other Procedure Patient Care Other
21 Medication Related Events Total Harms 152 % Medication Related (n = 104) 68% Inpatient Events (n=67) 64% Events present on admission occurring within 30 days: (n= 22) Events associated with a re-admission (n=15) 21% 15% Percent 25.00% 20.00% 15.00% 10.00% 5.00% 0.00% Frequency of Medication Related Events % 90.00% 80.00% 70.00% 60.00% 50.00% 40.00% 30.00% 20.00% 10.00% 0.00% Events
 Aspirin (45%) Enoxaparin (20%) Warfarin (20%) Morphine (58%) Oxycodone (8%) Improvement Plan: Focus on prescribing of opiates Establish a team Do a more in depth analysis Demographics (age,")
22 Medications Implicated Event No Events (%) Primary Drug Involved Secondary Drug involved Constipatio n 24 (23%) Morphine (37.5%) Oxycodone (21% ) Bleeding 20 (19%) Nausea & Vomiting 12 (11.5% ) Aspirin (45%) Enoxaparin (20%) Warfarin (20%) Morphine (58%) Oxycodone (8%) Improvement Plan: Focus on prescribing of opiates Establish a team Do a more in depth analysis Demographics (age, gender, ethnicity) Case weights Length of stay Service area Process / system issues Variation in prescribing



23 GTT in NZ Brief History Current DHBs doing GTT HQSC Support Future Harm and Error 46
24 Adverse Events Harm and Error HARM Harm is the focus of discussion Looks at all unintended results Measurement is clear and direct Nothing is theoretically unpreventable ERROR Errors and humans are the focus of discussion Tends to focus on those outcomes felt to be related to error Measurement relies on self-reporting Many AEs seen as unpreventable Accepting the Harm Burden Adverse Event and Errors Error definition bears upon concept of preventability and human mistake Adverse event describes harm to the patient regardless of error and is often system-based Relationship between errors and adverse events: Adverse Events Errors Mortality
 transferred to ICU Placed on Bi-Pap Received standard Demerol and Versed for procedure Given Romazicon; stayed in unit 12 hours.")
25 Finding the triggers exercise Example of a trigger: Transfer to higher level of care Endoscopy Post procedure somnolent and hypotensive (BP 80) transferred to ICU Placed on Bi-Pap Received standard Demerol and Versed for procedure Given Romazicon; stayed in unit 12 hours.
26 Exercise 51 Question #1 A patient on chronic anticoagulation has a INR of 8.2. Does that represent an adverse event? 1 - Yes 2 - No
27 Analysis of a Trigger (INR 8.2) In itself, the abnormal INR is not an adverse event The appropriate portion of the chart must be reviewed to determine if an adverse event has occurred Large retroperitoneal bleed has been diagnosed The event has caused a prolongation of the hospitalization and has been classified as a category? Question #2 Given the previous description of an event and the categories, how would you categorize the event? 1 - E 2 - F 3 - G 4 - H 5 - I
28 Question #3 Given the previous description of an event and the categories, how would you categorize the event? 1 - E 2 - F 3 - G 4 - H 5 - I Question #4 Given your understanding of the hospital you work in, guess as to your adverse event rate? 1 - Significantly less than 100 events/1000 patient days 2 - Slightly less than 100 events/1000 patient days 3 - About the average, 100 events/1000 patient days 4 - More than 100 events/1000 patient days
29 Experience with the GTT 57 Exemplar Hospital Validation Review Hospital A Hospital B Hospital C Events/1000 patient days Events/100 admissions % of admissions with an event % 28% 32% 32%
30 Additional GTT Reviews Plus Exemplar Hospitals Events/1000 Days 3 Exemplar Hospitals (900Charts) 40 Bed rural Hospital (300 Charts 10 Hospital Research Project (240 charts) 7 Hospital System (3000 Charts) NA Multi-state Tertiary System (2000 charts) Events/100 admissions Admissions with adverse events 32% 30% 30% 29% 30%
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD September 2012 This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies: - Blame - Denial - And the
Diagnostics for Patient Safety and Quality of Care
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD Vice President Institute for Healthcare Improvement Cindy Hupke, BSN, MBA Director Institute for Healthcare Improvement Objectives
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD Vice President Institute for Healthcare Improvement Cindy Hupke, BSN, MBA Director Institute for Healthcare Improvement Objectives
Diagnostics for Patient Safety and Quality of Care
 Session L17 The presenters have nothing to disclose Diagnostics for Patient Safety and Quality of Care Carol Haraden Kate Jones Pat O Connor Orlando, FL December 09, 2012 Objectives P3 Describe the current
Session L17 The presenters have nothing to disclose Diagnostics for Patient Safety and Quality of Care Carol Haraden Kate Jones Pat O Connor Orlando, FL December 09, 2012 Objectives P3 Describe the current
Measuring Medication Harm: Advantages of Using a Trigger Tool. Frank Federico Executive Director
 Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
November The Global Trigger Tool. A Practical Implementation Guide for New Zealand District Health Boards
 November 2012 The Global Trigger Tool A Practical Implementation Guide for New Zealand District Health Boards Published in November 2012 by the Health Quality & Safety Commission, PO Box 25496, Wellington
November 2012 The Global Trigger Tool A Practical Implementation Guide for New Zealand District Health Boards Published in November 2012 by the Health Quality & Safety Commission, PO Box 25496, Wellington
Kupu Taurangi Hauora o Aotearoa
 Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
A23/B23: Patient Harm in US Hospitals: How Much? Objectives
 A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
A23/B23: Patient Harm in US Hospitals: How Much? 23rd Annual National Forum on Quality Improvement in Health Care December 6, 2011 Objectives Summarize the findings of three recent studies measuring adverse
Practical Tools in Patient Safety Tools Carol Haraden Amelia Brooks Jennifer Lenoci-Edwards
 Session Code These presenters have nothing to disclose Practical Tools in Patient Safety Tools Carol Haraden Amelia Brooks Jennifer Lenoci-Edwards December 5 th 8:30 4:00 #IHIFORUM Introduction 2 Morning
Session Code These presenters have nothing to disclose Practical Tools in Patient Safety Tools Carol Haraden Amelia Brooks Jennifer Lenoci-Edwards December 5 th 8:30 4:00 #IHIFORUM Introduction 2 Morning
Adverse Events in Hospitals: How Many and Why Not Reported. Fran Griffin Senior Manager Clinical Programs, BD
 Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
April Clinical Governance Corporate Report Narrative
 April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
National Programme to Prevent Central-Line Associated Bacteraemia. Project Charter October 2011 to April 2013
 National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
2018 Optional Special Interest Groups
 2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
Go for the Gold. Incorporating Regulatory Issues into the Quality Management Process. June 9 11, 2008 Starr Pass Resort Tucson, Arizona
 Go for the Gold June 9 11, 2008 Starr Pass Resort Tucson, Arizona Incorporating Regulatory Issues into the Quality Management Process Recent regulatory changes have impacted the traditional hospital Quality
Go for the Gold June 9 11, 2008 Starr Pass Resort Tucson, Arizona Incorporating Regulatory Issues into the Quality Management Process Recent regulatory changes have impacted the traditional hospital Quality
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
The Primary Care Trigger Tool: Practical Guidance
 The Primary Care Trigger Tool: Practical Guidance Reviewing clinical records to detect and reduce patient safety incidents Index Content Page Introduction 2 What is a Trigger Tool Review? 2 What types
The Primary Care Trigger Tool: Practical Guidance Reviewing clinical records to detect and reduce patient safety incidents Index Content Page Introduction 2 What is a Trigger Tool Review? 2 What types
Hospital Authority Key Performance Indicator Annual Review
 - 1 - For decision on 25.1.2018 AOM-P1352 Hospital Authority 2017 Key Performance Indicator Annual Review Purpose This paper informs Members of the progress of the 2017 Key Performance Indicator (KPI)
- 1 - For decision on 25.1.2018 AOM-P1352 Hospital Authority 2017 Key Performance Indicator Annual Review Purpose This paper informs Members of the progress of the 2017 Key Performance Indicator (KPI)
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
What are the potential ethical issues to be considered for the research participants and
 What are the potential ethical issues to be considered for the research participants and researchers in the following types of studies? 1. Postal questionnaires 2. Focus groups 3. One to one qualitative
What are the potential ethical issues to be considered for the research participants and researchers in the following types of studies? 1. Postal questionnaires 2. Focus groups 3. One to one qualitative
Scoring Methodology FALL 2016
 Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Centralizing Multi-Hospital Mortality Reviews
 December 7, 2016 Session Codes: D4 (9:30am-10:45am) & E4 (11:15am - 12:30pm) Centralizing Multi-Hospital Mortality Reviews IHI 28 th National Forum Mark P Jarrett, MD, MBA, MS SVP, Chief Quality Officer,
December 7, 2016 Session Codes: D4 (9:30am-10:45am) & E4 (11:15am - 12:30pm) Centralizing Multi-Hospital Mortality Reviews IHI 28 th National Forum Mark P Jarrett, MD, MBA, MS SVP, Chief Quality Officer,
WHY OFFER SAME DAY DISCHARGE FOR NON-RECONSTRUCTIVE BREAST CANCER SURGERY?
 WHY OFFER SAME DAY DISCHARGE FOR NON-RECONSTRUCTIVE BREAST CANCER SURGERY? Jo Marsden, Consultant Breast Surgeon, Kings College Hospital NHS Foundation Trust, London LENGTH OF STAY FOR NON-RECONSTRUCTIVE
WHY OFFER SAME DAY DISCHARGE FOR NON-RECONSTRUCTIVE BREAST CANCER SURGERY? Jo Marsden, Consultant Breast Surgeon, Kings College Hospital NHS Foundation Trust, London LENGTH OF STAY FOR NON-RECONSTRUCTIVE
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
National Patient Safety Goals & Quality Measures CY 2017
 National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
The Nexus of Quality and Finance
 The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
MORTALITY REVIEW POLICY
 MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development
 Review of National Reporting and Learning System (NRLS) incident data relating to discharge from acute and mental health trusts August 2014 NHS England INFORMATION READER BOX Directorate Medical Operations
Review of National Reporting and Learning System (NRLS) incident data relating to discharge from acute and mental health trusts August 2014 NHS England INFORMATION READER BOX Directorate Medical Operations
Introduction. Singapore and its Quality and Patient Safety Position. Singapore 2004: Top 5 Key Risk Factors. High Body Mass
 Introduction Singapore and its Quality and Patient Safety Position Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking (7.4%; 28,000)
Introduction Singapore and its Quality and Patient Safety Position Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking (7.4%; 28,000)
Scoring Methodology SPRING 2018
 Scoring Methodology SPRING 2018 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 6 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician
Scoring Methodology SPRING 2018 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 6 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician
NHS TAYSIDE MORTALITY REVIEW PROGRAMME
 NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
2017 LEAPFROG TOP HOSPITALS
 2017 LEAPFROG TOP HOSPITALS METHODOLOGY AND DESCRIPTION In order to compare hospitals to their peers, Leapfrog first placed each reporting hospital in one of the following categories: Children s, Rural,
2017 LEAPFROG TOP HOSPITALS METHODOLOGY AND DESCRIPTION In order to compare hospitals to their peers, Leapfrog first placed each reporting hospital in one of the following categories: Children s, Rural,
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY
 CONDITIONS IN THE COMMUNITY") THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
February New Zealand Health and Disability Services National Reportable Events Policy 2012
 February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
GTT from manual to automated processes & - From patient injuries as a management tool to a clinical relevant tool
 GTT from manual to automated processes & - From patient injuries as a management tool to a clinical relevant tool Jan Terje Henriksen Nordland Hospital Trust Agenda Why ASJ/GTT What is GTT & ASJ/NCAF?
GTT from manual to automated processes & - From patient injuries as a management tool to a clinical relevant tool Jan Terje Henriksen Nordland Hospital Trust Agenda Why ASJ/GTT What is GTT & ASJ/NCAF?
IHI Skilled Nursing Facility Trigger Tool for Measuring Adverse Events
 IHI Skilled Nursing Facility Trigger Tool for Measuring Adverse Events AN IHI RESOURCE 20 University Road, Cambridge, MA 02138 ihi.org How to Cite This Document: Adler L, Moore J, Federico F. IHI Skilled
IHI Skilled Nursing Facility Trigger Tool for Measuring Adverse Events AN IHI RESOURCE 20 University Road, Cambridge, MA 02138 ihi.org How to Cite This Document: Adler L, Moore J, Federico F. IHI Skilled
Avoidable Hospitalisation
 Avoidable Hospitalisation Introduction Avoidable hospitalisation is used to measure the occurrence of a severe illness that theoretically could have been avoided by either; Ambulatory sensitive hospitalisation
Avoidable Hospitalisation Introduction Avoidable hospitalisation is used to measure the occurrence of a severe illness that theoretically could have been avoided by either; Ambulatory sensitive hospitalisation
Measuring Harm. Objectives and Overview
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3. Measuring Harm
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Review for Required Monitors
 Review for Required Monitors The Joint Commission Hospital Accreditation Manual, 2009 Medicare Conditions of Participation, Hospitals Update: February 2009 Indicator / Monitor Restraint, Medical (non-specific
Review for Required Monitors The Joint Commission Hospital Accreditation Manual, 2009 Medicare Conditions of Participation, Hospitals Update: February 2009 Indicator / Monitor Restraint, Medical (non-specific
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Scoring Methodology FALL 2017
 Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
How to conduct second line assessments. Barry Beiles-Clinical Director VASM
 How to conduct second line assessments Barry Beiles-Clinical Director VASM ASM receives notification of death Surgical case form sent to surgeon for completion by paper or Fellows Interface Completed paper
How to conduct second line assessments Barry Beiles-Clinical Director VASM ASM receives notification of death Surgical case form sent to surgeon for completion by paper or Fellows Interface Completed paper
QUALITY ACCOUNTS 2013/2014
 QUALITY ACCOUNTS 2013/2014 Northland District Health Board Quality Accounts 2013/2014 Quality is important to us all and we are making steady progress against each of our nominated priorities. We have
QUALITY ACCOUNTS 2013/2014 Northland District Health Board Quality Accounts 2013/2014 Quality is important to us all and we are making steady progress against each of our nominated priorities. We have
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals
 Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
HEALTHCARE ASSOCIATED INFECTION PREVENTION AND CONTROL REPORT JUNE 2016
 Appendix--75 Borders NHS Board HEALTHCARE ASSOCIATED INFECTION PREVENTION AND CONTROL REPORT JUNE Aim The purpose of this paper is to update Board members of the current status of Healthcare Associated
Appendix--75 Borders NHS Board HEALTHCARE ASSOCIATED INFECTION PREVENTION AND CONTROL REPORT JUNE Aim The purpose of this paper is to update Board members of the current status of Healthcare Associated
Where There s a Spark
 Where There s a Spark Counties Manukau District Health Board THERE S A WAY FORWARD Changing our Game Geraint Martin, CEO, Counties Manukau District Health Board Ron Pearson, Deputy CEO, Counties Manukau
Where There s a Spark Counties Manukau District Health Board THERE S A WAY FORWARD Changing our Game Geraint Martin, CEO, Counties Manukau District Health Board Ron Pearson, Deputy CEO, Counties Manukau
Surgical Performance Tracking in a Multisource Data Environment
 Surgical Performance Tracking in a Multisource Data Environment Kiley B. Vander Wyst, MPH Jorge I. Arango, MD Madison Carmichael, BS Shelley Flecky, PA P. David Adelson, MD, FACS, FAAP Disclosures No conflicts
Surgical Performance Tracking in a Multisource Data Environment Kiley B. Vander Wyst, MPH Jorge I. Arango, MD Madison Carmichael, BS Shelley Flecky, PA P. David Adelson, MD, FACS, FAAP Disclosures No conflicts
Quality Provisions in the EPM Final Rule. Matt Baker Scott Wetzel
 Quality Provisions in the EPM Final Rule Matt Baker Scott Wetzel Overview Quality Scoring Overview Quality Metrics in AMI and CABG EPMs Quality Metrics in SHFFT EPMs COTH Performance in these programs
Quality Provisions in the EPM Final Rule Matt Baker Scott Wetzel Overview Quality Scoring Overview Quality Metrics in AMI and CABG EPMs Quality Metrics in SHFFT EPMs COTH Performance in these programs
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI
 COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI Sample CHNA. This document is intended to be used as a reference only. Some information and data has been altered
COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI Sample CHNA. This document is intended to be used as a reference only. Some information and data has been altered
CRAB : Big Scale Routine Data as First Alert
 Workshop 3: Patient safety and mhealth/big data/hand held services CRAB : Big Scale Routine Data as First Alert Ingo Gurcke, Dipl. Kaufmann (FH), Marsh Medical Consulting GmbH, Managing Director, Germany
Workshop 3: Patient safety and mhealth/big data/hand held services CRAB : Big Scale Routine Data as First Alert Ingo Gurcke, Dipl. Kaufmann (FH), Marsh Medical Consulting GmbH, Managing Director, Germany
C. difficile Infection and C. difficile Lab ID Reporting in NHSN
 C. difficile Infection and C. difficile Lab ID Reporting in NHSN MARY ANDRUS, BA, RN, CIC Infection Preventionist Consultant Learning Objectives Review the structure and of the MDRO/CDAD Module within
C. difficile Infection and C. difficile Lab ID Reporting in NHSN MARY ANDRUS, BA, RN, CIC Infection Preventionist Consultant Learning Objectives Review the structure and of the MDRO/CDAD Module within
Enhanced Recovery: Measurement for Improvement Monthly Data Submission Guidance. Version 1.0
 Enhanced Recovery: Measurement for Improvement Monthly Data Submission Guidance Version 1.0 Document Control Version Version 1.0 Date Issued January 2014 Document To provide guidance for the monthly collection
Enhanced Recovery: Measurement for Improvement Monthly Data Submission Guidance Version 1.0 Document Control Version Version 1.0 Date Issued January 2014 Document To provide guidance for the monthly collection
Healthcare Reform Hospital Perspective
 Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
Healthcare Reform Hospital Perspective Susan DeVore President and CEO, Premier, Inc. March 8, 2010 1 The end of an illusion 2 Current landscape for healthcare reform 3 Specific policies require a paradigm
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
National Update on Malnutrition
 National Update on Malnutrition Dr Trevor Smith Consultant Gastroenterologist University Hospital Southampton BAPEN Executive Officer Chair, British Artificial Nutrition Survey British Association for
National Update on Malnutrition Dr Trevor Smith Consultant Gastroenterologist University Hospital Southampton BAPEN Executive Officer Chair, British Artificial Nutrition Survey British Association for
Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE
 Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE Acknowledgement and disclaimer Funding acknowledgement: This project is funded by the National Institute for Health Research Health
Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE Acknowledgement and disclaimer Funding acknowledgement: This project is funded by the National Institute for Health Research Health
IHI Open School Advanced Case Study October 14, 2010 Clemson University
 IHI Open School Advanced Case Study October 14, 2010 Clemson University Catherine Simmons 1, Drew Sargent 1, and Kate Wright 1 Public Health Science Hallie Bagnal 2 and Megan Hohenberger 2 Biological Science
IHI Open School Advanced Case Study October 14, 2010 Clemson University Catherine Simmons 1, Drew Sargent 1, and Kate Wright 1 Public Health Science Hallie Bagnal 2 and Megan Hohenberger 2 Biological Science
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm
 Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
Reducing emergency admissions
 A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System
 Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 HOW WE MEASURE QUALITY 16
 Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
SUPPORTING TREATMENT SAFETY TREATMENT INJURY INFORMATION APRIL
 SUPPORTING TREATMENT SAFETY TREATMENT INJURY INFORMATION APRIL 2018 www.acc.co.nz/treatmentsafety 978-0-478-36290-9 Supporting Patient Safety (printed version) 978-0-478-36291-6 Supporting Patient Safety
SUPPORTING TREATMENT SAFETY TREATMENT INJURY INFORMATION APRIL 2018 www.acc.co.nz/treatmentsafety 978-0-478-36290-9 Supporting Patient Safety (printed version) 978-0-478-36291-6 Supporting Patient Safety
Banner Health Friday, February 20, 2015
 Banner Health Friday, February 20, 2015 Leveraging the Power of Clinical and Business Intelligence: A Primer Presented by: Dr. Maxine Rand, DNP, RN-BC, CPHIMS, Director, Clinical Education, Practice and
Banner Health Friday, February 20, 2015 Leveraging the Power of Clinical and Business Intelligence: A Primer Presented by: Dr. Maxine Rand, DNP, RN-BC, CPHIMS, Director, Clinical Education, Practice and
Policy on Learning from Deaths
 Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Review Process. Introduction. InterQual Level of Care Criteria Long-Term Acute Care Criteria
 InterQual Level of Care Criteria Long-Term Acute Care Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of Long-Term Acute Care (LTAC) admission,
InterQual Level of Care Criteria Long-Term Acute Care Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of Long-Term Acute Care (LTAC) admission,
Admissions and Readmissions Related to Adverse Events, NMCPHC-EDC-TR
 Admissions and Readmissions Related to Adverse Events, 2007-2014 By Michael J. Hughes and Uzo Chukwuma December 2015 Approved for public release. Distribution is unlimited. The views expressed in this
Admissions and Readmissions Related to Adverse Events, 2007-2014 By Michael J. Hughes and Uzo Chukwuma December 2015 Approved for public release. Distribution is unlimited. The views expressed in this
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB)
") Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES. James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Comprehensive Program and 5 Key Aspects James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Comprehensive Program and 5 Key Aspects James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Medication Reconciliation
 Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Quality Strategy (Refreshed March 2015)
") Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
O U T C O M E. record-based. measures HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT
 HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT record-based O U Michael Goldacre, David Yeates, Susan Flynn and Alastair Mason National Centre for Health Outcomes Development
HOSPITAL RE-ADMISSION RATES: APPROACH TO DIAGNOSIS-BASED MEASURES FULL REPORT record-based O U Michael Goldacre, David Yeates, Susan Flynn and Alastair Mason National Centre for Health Outcomes Development
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Provide Safe and Effective Medicines Management in Primary Care
 Primary Drivers Secondary Drivers Aim Safe and reliable prescribing, monitoring and administration of high risk medications that require systematic monitoring Implement systems for reliable prescribing
Primary Drivers Secondary Drivers Aim Safe and reliable prescribing, monitoring and administration of high risk medications that require systematic monitoring Implement systems for reliable prescribing
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
Coroner's Corner - Inquest into the death of Gwendoline Mead
 Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
The How to Guide for Reducing Surgical Complications
 The How to Guide for Reducing Surgical Complications Post operative wound (surgical site) infections Maintaining perioperative normothermia Main contacts for Reducing Surgical Complications Campaign Director:
The How to Guide for Reducing Surgical Complications Post operative wound (surgical site) infections Maintaining perioperative normothermia Main contacts for Reducing Surgical Complications Campaign Director:
Page 1 of 26. Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - November 2014
 Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - November 2014 Clinical Quality Service Page 1 of 26 Print Date:18/11/2014 Clinical Governance
Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - November 2014 Clinical Quality Service Page 1 of 26 Print Date:18/11/2014 Clinical Governance
THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING. Australasian Rehabilitation Nurses Association June 26 th 2015
 THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING Australasian Rehabilitation Nurses Association June 26 th 2015 Conflict of Interest and affiliations No conflicts of interest regarding this topic. Current
THE DETERIORATING PATIENT IN THE SUB-ACUTE SETTING Australasian Rehabilitation Nurses Association June 26 th 2015 Conflict of Interest and affiliations No conflicts of interest regarding this topic. Current
UTILIZATION MANAGEMENT AND CARE COORDINATION Section 8
 Overview The focus of WellCare s Utilization Management (UM) Program is to provide members access to quality care and to monitor the appropriate utilization of services. WellCare s UM Program has five
Overview The focus of WellCare s Utilization Management (UM) Program is to provide members access to quality care and to monitor the appropriate utilization of services. WellCare s UM Program has five
Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference
 Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference INGA AIKMAN, MD, MPH PEDIATRIC CHIEF RESIDENT EAST CAROLINA UNIVERSITY Second Annual REACH Medical
Utilizing the Fish-Bone Model to Identify Systems Errors During Pediatric Morbidity and Mortality Conference INGA AIKMAN, MD, MPH PEDIATRIC CHIEF RESIDENT EAST CAROLINA UNIVERSITY Second Annual REACH Medical
MIPS, MACRA, & CJR: Medicare Payment Transformation. Presenter: Thomas Barber, M.D. May 31, 2016
 MIPS, MACRA, & CJR: Medicare Payment Transformation Presenter: Thomas Barber, M.D. May 31, 2016 Michael Porter- Value Based Care Delivery, Annals of Surgery 2008 Principals: Define Value as a Goal Care
MIPS, MACRA, & CJR: Medicare Payment Transformation Presenter: Thomas Barber, M.D. May 31, 2016 Michael Porter- Value Based Care Delivery, Annals of Surgery 2008 Principals: Define Value as a Goal Care
Patients Experience of Emergency Admission and Discharge Seven Days a Week
 Patients Experience of Emergency Admission and Discharge Seven Days a Week Abstract Purpose: Data from the 2014 Adult Inpatients Survey of acute trusts in England was analysed to review the consistency
Patients Experience of Emergency Admission and Discharge Seven Days a Week Abstract Purpose: Data from the 2014 Adult Inpatients Survey of acute trusts in England was analysed to review the consistency
The Management and Control of Hospital Acquired Infection in Acute NHS Trusts in England
 Report by the Comptroller and Auditor General The Management and Control of Hospital Acquired Infection in Acute NHS Trusts in England Ordered by the House of Commons to be printed 14 February 2000 LONDON:
Report by the Comptroller and Auditor General The Management and Control of Hospital Acquired Infection in Acute NHS Trusts in England Ordered by the House of Commons to be printed 14 February 2000 LONDON:
Medicine Management Policy
 INDEX Prescribing Page 2 Dispensing Page 3 Safe Administration Page 4 Problems & Errors Page 5 Self Administration Page 7 Safe Storage Page 8 Controlled Drugs Best Practice Procedure Page 9 Controlled
INDEX Prescribing Page 2 Dispensing Page 3 Safe Administration Page 4 Problems & Errors Page 5 Self Administration Page 7 Safe Storage Page 8 Controlled Drugs Best Practice Procedure Page 9 Controlled
Serious Adverse Event Report 1 July June 2015
 Serious Adverse Event Report 1 July 2014 30 June 2015 Category Brief description Main findings There were no clear gaps in care delivery identified, but there were a Falls Unwitnessed patient fall resulting
Serious Adverse Event Report 1 July 2014 30 June 2015 Category Brief description Main findings There were no clear gaps in care delivery identified, but there were a Falls Unwitnessed patient fall resulting
HAEMOVIGILANCE POLICY
 REASON FOR ISSUE: New document describing Haemovigilance System 1. INTRODUCTION NZBS has adopted the Council of Europe definition that states that haemovigilance is: The organised surveillance procedures
REASON FOR ISSUE: New document describing Haemovigilance System 1. INTRODUCTION NZBS has adopted the Council of Europe definition that states that haemovigilance is: The organised surveillance procedures
Value-Based Purchasing & Payment Reform How Will It Affect You?
 Value-Based Purchasing & Payment Reform How Will It Affect You? HFAP Webinar September 21, 2012 Nell Buhlman, MBA VP, Product Strategy Click to view recording. Agenda Payment Reform Landscape Current &
Value-Based Purchasing & Payment Reform How Will It Affect You? HFAP Webinar September 21, 2012 Nell Buhlman, MBA VP, Product Strategy Click to view recording. Agenda Payment Reform Landscape Current &
Medication Reconciliation. Peggy Choye, Pharm.D., BCPS
 Medication Reconciliation Peggy Choye, Pharm.D., BCPS What is it? Medication reconciliation The process of identifying the most accurate list of all medications that a patient is taking including name,
Medication Reconciliation Peggy Choye, Pharm.D., BCPS What is it? Medication reconciliation The process of identifying the most accurate list of all medications that a patient is taking including name,
Glasgow City CHP Item No. 6
 Glasgow City CHP Item No. 6 CHP Committee Meeting Date: Thursday, 28 th February 2013 Paper No 2013/006 Subject: Presented by: Recommendation(s) Summary/ Background Scottish Patient Safety Programme -
Glasgow City CHP Item No. 6 CHP Committee Meeting Date: Thursday, 28 th February 2013 Paper No 2013/006 Subject: Presented by: Recommendation(s) Summary/ Background Scottish Patient Safety Programme -
National clinical audit of inpatient care for adults with ulcerative colitis
 National clinical audit of inpatient care for adults with ulcerative colitis UK inflammatory bowel disease (IBD) audit Executive summary report June 2014 Prepared by the Clinical Effectiveness and Evaluation
National clinical audit of inpatient care for adults with ulcerative colitis UK inflammatory bowel disease (IBD) audit Executive summary report June 2014 Prepared by the Clinical Effectiveness and Evaluation
Home administration of intravenous diuretics to heart failure patients:
 Quality and Productivity: Proposed Case Study Home administration of intravenous diuretics to heart failure patients: Increasing productivity and improving quality of care Provided by: British Heart Foundation
Quality and Productivity: Proposed Case Study Home administration of intravenous diuretics to heart failure patients: Increasing productivity and improving quality of care Provided by: British Heart Foundation
Reliability of Evaluating Hospital Quality by Surgical Site Infection Type. ACS NSQIP Conference July 22, 2012
 Reliability of Evaluating Hospital Quality by Surgical Site Infection Type ACS NSQIP Conference July, 01 Surgical Site Infection Common cause of patient morbidity 5%-6% for colorectal procedures Significant
Reliability of Evaluating Hospital Quality by Surgical Site Infection Type ACS NSQIP Conference July, 01 Surgical Site Infection Common cause of patient morbidity 5%-6% for colorectal procedures Significant
Research on nurse practitioner diagnostic reasoning
 Clinical Stream Research on nurse practitioner diagnostic reasoning Alison Pirret Research on nurse practitioner diagnostic reasoning Alison Pirret (NP, BA, MA, PGCert, PhD) Introduction Nurse practitioners
Clinical Stream Research on nurse practitioner diagnostic reasoning Alison Pirret Research on nurse practitioner diagnostic reasoning Alison Pirret (NP, BA, MA, PGCert, PhD) Introduction Nurse practitioners
The History of the development of the Prometheus Payment model defined Potentially Avoidable Complications.
 The History of the development of the Prometheus Payment model defined Potentially Avoidable Complications. In 2006 the Prometheus Payment Design Team convened a series of meetings with physicians that
The History of the development of the Prometheus Payment model defined Potentially Avoidable Complications. In 2006 the Prometheus Payment Design Team convened a series of meetings with physicians that