Large scale health systems improvement to recognise and manage deteriorating patients Dr Harvey Lander and Malcolm Green
|
|
|
- Lorin Harmon
- 5 years ago
- Views:
Transcription



1 Large scale health systems improvement to recognise and manage deteriorating patients Dr Harvey Lander and Malcolm Green

2 Australia? YOU ARE HERE

3 NSW PRESENTATION NAME MONTH YYYY PRESENTER NAME 3


4 Clinical Excellence Commission The NSW health system provides the safest and highest quality care for every patient To improve healthcare for patients in NSW through leadership in safety and quality Safe, high quality patient care High performing reliable systems A culture built on improvement 1. Building system excellence together 2. Quality improvement capability and capacity 3. Knowledge-based system improvement 4. Organisational excellence Understand needs and work in partnership on agreed priorities Enhance leadership in safety and quality Enhance improvements in identified key areas Develop adaptable delivery systems with demonstrated impact Strengthen governance for safety and quality Enhance frontline capability and capacity in safety and quality Strengthen meaningful monitoring and feedback Ensure alignment of key priorities and coordination of processes across CEC Strengthen leadership and teamwork Invest in our staff Exemplify a learning organisation Improve communication Prioritise and optimise our use of resources Our Core Values Collaboration * Openness * Respect * Empowerment
5 5
6 The Quality Triangle Quality Assurance Quality Management Quality Improvement


7 A simple way to think about quality and safety the dimensions of care Raj Behal
8 Learning objectives Understand the multivalent strategy which underpins the successful implementation of the Between the Flags program Understand the impact of a large scale patient safety net system on health systems culture Share in the lessons learned from the implementation of the Between the Flags program Build system capability and leadership at scale 8

9 PRESENTATION NAME MONTH YYYY PRESENTER NAME 9
10 Designing a system a)what do you do to ensure patients deteriorate in your system? b)turn to the person next to you and compare? c) If you were to focus on three things to improve what would they be? 10
11 Failure to rescue, the problem Patient Condition The Slippery Slope (the Problem) ALS Time Source: Dr Charles Pain Death
12 What s the problem? Serious adverse events are common in hospitalized patients around the world 1-4 Documented warning signs in up to 80% of deteriorating patients 5-9 Early recognition and intervention improves outcomes Wilson et al MJA 1992, Davis et al NZ Med J 1998, Brennan / Leape 1984, Baker etal Schein et al, Chest 1990, Buist et al MJA 1999, Hodgets et al Resus 2002, Nurmi et al Act Anaes Scan 2005, Bell et al Resus GISSI Am Heart J 1999, Rivers NEJM 2001, Nardi Min. Anest 2002, NINDS NEJM 1995

13 Leadership in NSW Medical Emergency Team (MET) concept developed by Professor Ken Hillman in NSW 1 MET and Rapid Response Systems catch on across Australia, the US and the UK Lee et al, Anaesth Intensive Care Ball et al, BMJ England et al, Critical Care IHI, 100,1000 lives campaign 2006
14 But there s still a problem. Failure to recognise and respond to deteriorating patients is a significant issue 1-3 Imbalance between patient needs and available resources 4 Need to identify the root causes to inform strategies 5 1. McQuillan et al, British Medical Journal, 1998 (UK) 2. Buist et al, Medical Journal of Australia, 1999 (Australia) 3. Bell et al, Resuscitation, 2006 (Sweden) 4. Devita et al, Critical Care Medicine, Pain, CH. Johnson, JK. Amalberti, R. Stein, J. Braithwaite, J. Hughes, CF, In Safe Hands: Releasing the Potential of Clinical Teams, presented at 8 th International Organisational Behaviour in Healthcare Conference. Patient Centred Health Care Teams: Achieving Collaboration, Communication and Care [OBHC 2012], Trinity College Dublin, Ireland, April 2012
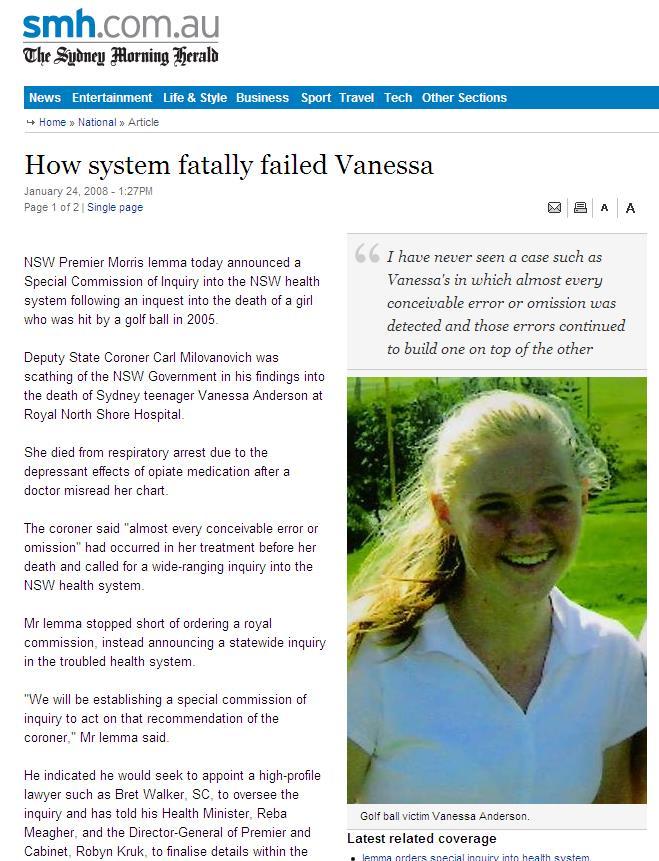
15
16 Garling on Culture I have no doubt, given the material before me, that there is a negative culture in NSW public hospitals which at worst manifests itself in bullying and harassment, but which also reflects a great divide between clinicians and administrators. Peter Garling SC, November 2008
17 What clinicians said We live in a micromanaged hell, a micromismanaged hell. It is run with a top-down culture of bullying and with the bottom-up response of fear and loathing. Senior clinician giving evidence to Garling Commission
18 Recommendation 91 A system to be put in place in NSW with the following elements: early identification escalation protocols including rapid response system; detailed education and training programs appropriate data to monitor high level support from management and clinicians; and ongoing evaluation.

19 From project to program 20
20 Transformation requires leadership Health systems face great challenges Internationally > 20 years shows that incremental improvements help But, transformation requires whole of system approach with leadership at all levels
21 22
22 Large system transformation 1 engage individuals at all levels 2 build in feedback loops 3 attend to history 4 engage clinicians 5 patients and families involvement Best et al, large system transformation: a realist review
23 Leadership at all levels Secretary NSW Health Clinical Excellence Commission Ministry of Health Local Health Districts Directors of Clinical Governance Hospital Executives Clinician leads Frontline clinicians Health care teams rapid response Chief of Ministry Statewide S&Q organisation Statewide Policy and regulation Local healthcare authority with individual boards Local hospital leadership Key clinicians Microsystem The response team

24 The launch 25
25 Aim To improve early recognition and response to clinical deterioration and thereby reduce potentially preventable deaths and serious adverse events in patients who receive their care in NSW public hospitals.










26 The System - 5 elements Policy & Governance Plan DCG s Standard Observation Charts Standard Calling Criteria Clinical Emergency Response System Clinical Review & Rapid Response Education Evaluation Awareness, DETECT, Rapid Responders 2 KPIs Evaluation Collaborative QSA Source: Colette Duff

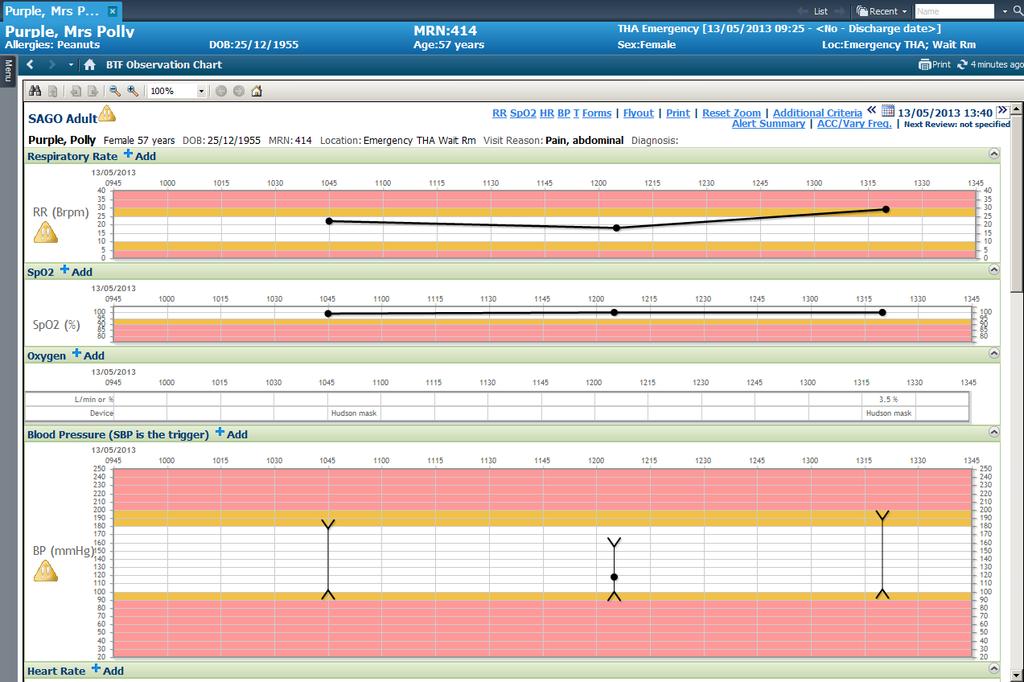
27 Standard Adult General Observation Chart
28 CEC approach Broad clinician engagement and consultation Keep it simple whether possible single trigger escalation Standardisation across NSW Allow facilities to customise their local response Promote teamwork Promote and support clinical judgement
29 Local approach a hospital Leadership is required at every level Executive top down, clinicians bottom up, between teams and units (horizontal) Support cultural conditions for effective leadership Coalition is built over time with an inclusive process Clinical outcomes
30 Local approach Governance - Clinical Council, Medical Director Committee structures Adult and Paediatric charts Response system (CERS) local policy Education DETECT and DETECT junior Evaluation CRs, RRs (times, wards), transfers to ICU, deaths 31
31
32 Is it working? 33
33 Evaluation Key Performance Indicators Rapid Response calls / 1000 admissions Cardiac Arrests calls / 1000 admissions Quality Systems Assessment (QSA) reports Hospital visits Standard Observation Chart audit tools Academic Research Partners - UNSW
34 Evaluation BETWEEN THE FLAGS EVALUATION Process Outcome IMPROVE RECOGNITION IMPROVE RESPONSE REDUCE DEATH & DISABILITY PROCESS (intervention) Track and Trigger observation chart Standard calling criteria Education package EVALUATION Audit completion Audit breaches Assess learning outcomes PROCESS (intervention) Clinical Review Rapid Response EVALUATION Measure rate of calls Audit appropriateness of calls Measure rate of calls Audit appropriateness of calls Note: 1 Unexpected deaths = all deaths minus NFR deaths 2 Potentially preventable deaths = Unexpected deaths that had breaches of calling criteria that were not acted on OUTCOME Reduce overall deaths Reduce unexpected deaths Reduce unexpected preventable deaths Reduce cardiorespiratory arrests EVALUATION Measure death rate Measure rate of unexpected deaths 1 Measure rate of unexpected potentially preventable deaths 2 Measure rate of cardiorespiratory arrests
35 Benefit to Patient Safety 100% 80% 60% 40% 20% 0% 47% 48% 21% 25% Overall the BTF has benefitted patient safety in our department/unit (Adults) Strongly agree Agree Overall the BTF program has benefitted patient safety in our department / unit (Paeds) 38% 44% Overall the BTF program has benefitted patient safety in our department / clinical unit (all)
36 Executive support/clinical leads: 100% 80% 60% 40% 20% 0% 47% 49% 28% 32% Strong executive support is an important part of the success of BTF in our dept/unit Strongly Agree Strong executive support is an important part of the success of BTF in our department / unit. Agree 39% 38% 21% 28% Our BTF clinical lead (champion) has been critical to the uptake and acceptance of the program by clinicians in our dept/unit Our BTF clinical lead (champion) has been critical to the uptake and acceptance of the program by clinicians in our dept/unit


37 Rapid Response Calls in NSW 38

38 Cardiac arrest calls in NSW 39

39 What staff say 41
40 NSW Coroner 22 August 2014 In my view, this is one of the most important reforms introduced in NSW hospitals for a generation. If properly followed, the Between the Flags program saves lives. 42
41 Lessons learned Build a large coalition of clinicians, managers and administrators Governance is key Design for the real world - staged implementation Multivalent strategy Standardisation across NSW (the foundation stone) Strike the right balance between clinical judgement and rules Moving up the Slippery Slope 43
42 Conclusions BTF has changed clinical practice in NSW and is now part of the clinical language Staff strongly believe it is making a difference Rapid Response Rates and Cardiac Arrest Rates down 20% reduction in LMDRGs BTF is unmasking the age old root causes such as cultural issues and barriers to escalation


43 Patient Condition Usual Residence / Rehabilitation Moving up the slippery slope Prevention Clinical Review Time Rapid Response 45 Advanced Life Support Death Outcomes Continued Treatment Plan Revised Treatment Plan Referral Clinical Pathway High care unit / facility End of Life care Source: Dr Charles Pain


44 SEPSIS KILLS program: reduce preventable harm to patients with sepsis RECOGNISE: Risk factors, signs and symptoms of sepsis and inform senior clinician RESUSCITATE: With rapid antibiotics and IV fluids within one hour REFER: To specialist care and initiate retrieval if needed
45 What does REACH stand for? Helps to cast the safety net wider




46 CEC End of Life (EOL) Program A standardised process for the screening of medical records of patients who have died in NSW PHOs: includes EOL measures A process is in place for: timely identification of patients at risk of dying; commencing early conversations around end of life wishes, initiation of end of life planning; and appropriate referral to support services Tools ensure that all patients receive optimal symptom control, have social, spiritual and cultural needs addressed, and bereavement support for families and carers occurs


47
48 Future Challenges & Opportunities Medical leadership/engagement at all levels Getting the balance right (rules vs judgement) Tailoring the education to real time data Continuous monitoring and its role An electronic world Building high-reliability teams 50
49 51

50 52
51 What the CEC will do next 53
52 Adult Patient safety Program Essentials of safety Hand Washing Leadership Walk Rounds Surgical timeout Huddle or Team Talk Intensive Care Unit Daily Goals Ventilator Associated Pneumonia (VAP) Bundle Deteriorating patients Central Venous Catheter (CVC) Insertion CVC Maintenance Peripheral Venous Cannula (PVC) Bundle 54
 Deteriorating Patients Heart Failure Surgical Site Infections Safer Use of Medicines")
53 Points of care VTE SEPSIS Pressure Ulcers Falls Catheter Associated Urinary Tract Infections (CAUTI) Deteriorating Patients Heart Failure Surgical Site Infections Safer Use of Medicines
54 MICRO LEVEL (Unit Huddle) Look back: individual providers report on unexpected events, medical response team calls Look forward: individual providers report on individual patients at risk for safety events Integration: charge nurse considers overall unit status, planned discharges, staffing needs Unit 2 Unit 3 MESO LEVEL (Inpatient Huddle) Look back: charge nurses from each microsystem report on unexpected events, transfers to higher levels of care Look forward: individual microsystems report on higher risk patients in mesosystem, overall unit status Integration: Manager of Patient Services (MPS) works with charge nurses to develop plans and predictions for highest risk patients, develop capacity plan through system, predict and mitigate experience failures Periop MACRO LEVEL (Daily Operations Brief) Look back: mesosystem leaders report on unexpected outcomes over last 24 hours, resolution of concerns raised at previous brief Look forward: mesosystem leaders predict and plan for big issues of day with focus on problems at intersections of mesosystems Integration: administrator of the day identifies responsible party(ies) for each concerns and sets clear follow-up Goldenhar BMJ Quality and Safety 2013
55 57
56 Five dimensions to assist monitoring and improving safety (Charles Vincent) Past harm: this encompasses both psychological and physical measures. Reliability: this is defined as failure free operation over time and applies to measures of behaviour, processes and systems. Sensitivity to operations: the information and capacity to monitor safety on an hourly or daily basis. Anticipation and preparedness: the ability to anticipate, and be prepared for, problems. Integration and learning: the ability to respond to, and improve from, safety information 58


57 Safety is a process of enquiry Are we responding & learning & improving? Has care been safe in the past? Are our clinical systems & processes reliable? Will care be safer in the future? Is care safe today? Source: Vincent C, Burnett S, Carthey J. The measurement and monitoring of safety. The Health Foundation,
58

59 We gratefully acknowledge Always swim between the red and yellow flags
60 Thank you For further information: 62
The RRS and Resident Education. Dr Daryl Jones
 The RRS and Resident Education Dr Daryl Jones Overview Patients in crisis The traditional approach RRT criteria objectify crisis Outcomes of MET patients Education phase Austin hospital Improving RRT patient
The RRS and Resident Education Dr Daryl Jones Overview Patients in crisis The traditional approach RRT criteria objectify crisis Outcomes of MET patients Education phase Austin hospital Improving RRT patient
Safety Measurement, Monitoring & Strategies
 Safety Measurement, Monitoring & Strategies Jonkoping Microsystem Festival Scientific Day March 2016 Charles Vincent Professor of Psychology University of Oxford Lead Oxford AHSN Patient Safety Collaborative
Safety Measurement, Monitoring & Strategies Jonkoping Microsystem Festival Scientific Day March 2016 Charles Vincent Professor of Psychology University of Oxford Lead Oxford AHSN Patient Safety Collaborative
Increased situational awareness to reduce undetected deterioration
 Increased situational awareness to reduce undetected deterioration SPSP Paediatric Care WebEx Patrick W. Brady, MD, MSc Associate Professor of Pediatrics Division of Hospital Medicine Objectives Understand
Increased situational awareness to reduce undetected deterioration SPSP Paediatric Care WebEx Patrick W. Brady, MD, MSc Associate Professor of Pediatrics Division of Hospital Medicine Objectives Understand
This is a high level overview report to update the Board on the Acute Adult Safety Programme consisting of the following sections:
 Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
This paper provides an update on the the recent national SPSP conference the programme of work for Tissue Viability Acute Adult Care SPSP
 Greater Glasgow and Clyde NHS Board Board Meeting December 2016 Board Paper No. 16/81 Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP) is one of the family
Greater Glasgow and Clyde NHS Board Board Meeting December 2016 Board Paper No. 16/81 Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP) is one of the family
REACH Patient and family activated escalation of care
 REACH Patient and family activated escalation of care 12 MONTHS ON AND THE SKY DID NOT FALL Dr Karen Luxford, Alison Lee & Prof Cliff Hughes ISQua 2013 Patient Based Care Model If I would have been able
REACH Patient and family activated escalation of care 12 MONTHS ON AND THE SKY DID NOT FALL Dr Karen Luxford, Alison Lee & Prof Cliff Hughes ISQua 2013 Patient Based Care Model If I would have been able
Is healthcare getting safer? Situation
 10/13/2015 Healthcare in Qatar Delivering BEST CARE ALWAYS: National ambition, energy, commitment Growing demand Capacity and infrastructure limits Diverse workforce Huge investment in healthcare Transformation
10/13/2015 Healthcare in Qatar Delivering BEST CARE ALWAYS: National ambition, energy, commitment Growing demand Capacity and infrastructure limits Diverse workforce Huge investment in healthcare Transformation
Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust
 Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust Mark Simmonds (Acute and Critical Care Medicine Consultant,
Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust Mark Simmonds (Acute and Critical Care Medicine Consultant,
Kupu Taurangi Hauora o Aotearoa
 Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
Kupu Taurangi Hauora o Aotearoa National GTT Workshop 2014 Using Data for Improvement Update Global Trigger Tool (GTT) Targeted chart reviews using triggers as flags for patient harm Provides a high level
An overview of research projects and directions of the Simpson Centre
 An overview of research projects and directions of the Simpson Centre 2014 AIHI Research Symposium Associate Professor Jack Chen MBBS PhD MBA(Exec) Simpson Centre for Health Services Research Australian
An overview of research projects and directions of the Simpson Centre 2014 AIHI Research Symposium Associate Professor Jack Chen MBBS PhD MBA(Exec) Simpson Centre for Health Services Research Australian
A safe system framework for recognising and responding to children at risk of deterioration. July 2016
 A safe system framework for recognising and responding to children at risk of deterioration July 2016 Background Research shows that failure to recognise and treat patients whose condition is deteriorating
A safe system framework for recognising and responding to children at risk of deterioration July 2016 Background Research shows that failure to recognise and treat patients whose condition is deteriorating
The deteriorating patient recognition and management Dave Story
 The deteriorating patient recognition and management Dave Story MBBS, MD, BMedSci, FANZCA Professor and Foundation Chair of Anaesthesia Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU)
The deteriorating patient recognition and management Dave Story MBBS, MD, BMedSci, FANZCA Professor and Foundation Chair of Anaesthesia Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU)
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Building Systems and Leadership for Transformation
 Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
SAFE CARE. Scottish Patient Safety Programme. SPSP Adult Acute
 SAFE CARE NHS Greater Glasgow and Clyde (NHS GGC) is committed to providing safe high quality care that our staff and patients can be proud of. Over recent years the Scottish Patient Safety Programme has
SAFE CARE NHS Greater Glasgow and Clyde (NHS GGC) is committed to providing safe high quality care that our staff and patients can be proud of. Over recent years the Scottish Patient Safety Programme has
HOW TO DO POST-HOC RESPONSE REVIEWS
 HOW TO DO POST-HOC RESPONSE REVIEWS Ken Hillman 6 th International Symposium on Rapid Response Systems and Medical Emergency Teams Pittsburgh, USA, 11 th -12 th May 2010 ACUTE HOSPITAL SYSTEM AUDIT OF
HOW TO DO POST-HOC RESPONSE REVIEWS Ken Hillman 6 th International Symposium on Rapid Response Systems and Medical Emergency Teams Pittsburgh, USA, 11 th -12 th May 2010 ACUTE HOSPITAL SYSTEM AUDIT OF
Planning and Organising End of Life Care
 GUIDE Palliative Care Network Planning and Organising End of Life Care A Guide for Clinical Model Development Collaboration. Innovation. Better Healthcare. The Agency for Clinical Innovation (ACI) works
GUIDE Palliative Care Network Planning and Organising End of Life Care A Guide for Clinical Model Development Collaboration. Innovation. Better Healthcare. The Agency for Clinical Innovation (ACI) works
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Implementation of the National Safety and Quality Health Service Standards
 Implementation of the National Safety and Quality Health Service Standards The Experience and Lessons Learnt by the Australian Council on Healthcare Standards July 2012 Introduction and overview This information
Implementation of the National Safety and Quality Health Service Standards The Experience and Lessons Learnt by the Australian Council on Healthcare Standards July 2012 Introduction and overview This information
Sepsis Management in Scotland. Calum McGregor Consultant Acute Medicine National Clinical Lead for Acute Care Healthcare Improvement Scotland
 Sepsis Management in Scotland Calum McGregor Consultant Acute Medicine National Clinical Lead for Acute Care Healthcare Improvement Scotland Sepsis Management in Scotland Outline: Background on sepsis
Sepsis Management in Scotland Calum McGregor Consultant Acute Medicine National Clinical Lead for Acute Care Healthcare Improvement Scotland Sepsis Management in Scotland Outline: Background on sepsis
How Data-Driven Safety Culture Changes Can Lower HAC Rates
 How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
SPSP: Sepsis in Primary Care Collaborative. Dr Paul Davidson Associate Medical Director Primary Care NHS Highland
 SPSP: Sepsis in Primary Care Collaborative Dr Paul Davidson Associate Medical Director Primary Care NHS Highland Collaborative Ambition Improve early recognition and timely delivery of evidence-based interventions,
SPSP: Sepsis in Primary Care Collaborative Dr Paul Davidson Associate Medical Director Primary Care NHS Highland Collaborative Ambition Improve early recognition and timely delivery of evidence-based interventions,
Improving Patient Outcomes Strategy
 Improving Patient Outcomes Strategy 2015-2018 Hertford County I Lister I Mount Vernon Cancer Centre I QEII Improving Patient Outcomes Strategy 2015-2018 Page 1. Executive Summary 1 2. Introduction 2 3.
Improving Patient Outcomes Strategy 2015-2018 Hertford County I Lister I Mount Vernon Cancer Centre I QEII Improving Patient Outcomes Strategy 2015-2018 Page 1. Executive Summary 1 2. Introduction 2 3.
NCQC PSO Safe Tables. Failure To Rescue. Failure to Rescue
 NCQC PSO Safe Tables Failure To Rescue April 2015 Failure to Rescue Term coined in Australia in 1992 Associated with hospital not pa:ent characteris:cs In response RRTs championed by IHI (100,000 Lives
NCQC PSO Safe Tables Failure To Rescue April 2015 Failure to Rescue Term coined in Australia in 1992 Associated with hospital not pa:ent characteris:cs In response RRTs championed by IHI (100,000 Lives
These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in
 These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in the UK and beyond. 1 The first EWS was devised in 1997
These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in the UK and beyond. 1 The first EWS was devised in 1997
EQuIPNational Survey Planning Tool NSQHSS and EQuIP Actions 4.
 Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Keep watch and intervene early
 IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
Policy on Learning from Deaths
 Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Intern training term assessment form
 Australian Medical Council Limited Intern training term assessment form Intern details Intern name AHPRA registration no. This form is being completed for Mid-term Intern self-assessment End of term Term
Australian Medical Council Limited Intern training term assessment form Intern details Intern name AHPRA registration no. This form is being completed for Mid-term Intern self-assessment End of term Term
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Ensuring quality outcomes
 Annual integrated report 20 64 Ensuring quality outcomes Over the past five years we have built an integrated quality management system that drives quality improvement across all Netcare divisions. More
Annual integrated report 20 64 Ensuring quality outcomes Over the past five years we have built an integrated quality management system that drives quality improvement across all Netcare divisions. More
Ramp Up or Ramp Down? Sheila K. Adam Head of Nursing, Specialist Hospitals UCLH Trust
 Ramp Up or Ramp Down? Sheila K. Adam Head of Nursing, Specialist Hospitals UCLH Trust Improving Patient Outcome (Saving lives) Prevention of Cardiac Arrest! UK and US studies of outcome for in-hospital
Ramp Up or Ramp Down? Sheila K. Adam Head of Nursing, Specialist Hospitals UCLH Trust Improving Patient Outcome (Saving lives) Prevention of Cardiac Arrest! UK and US studies of outcome for in-hospital
Can we really learn from the past?
 Can we really learn from the past? Learning Lab Sunday 10 th December 2017 SL19 Dr Jonathan Kirk, National Clinical Lead Healthcare Improvement Scotland e: Jonathan.Kirk3@nhs.net @JonathanKirk42 Professor
Can we really learn from the past? Learning Lab Sunday 10 th December 2017 SL19 Dr Jonathan Kirk, National Clinical Lead Healthcare Improvement Scotland e: Jonathan.Kirk3@nhs.net @JonathanKirk42 Professor
NHS TAYSIDE MORTALITY REVIEW PROGRAMME
 NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Quality and Safety Improvement Strategy
 Quality and Safety Improvement Strategy 2016-2021 Page 1 of 20 1. Purpose of this Strategy Patient safety and quality of care are at the heart of the NHS agenda. Treating and caring for people in a safe
Quality and Safety Improvement Strategy 2016-2021 Page 1 of 20 1. Purpose of this Strategy Patient safety and quality of care are at the heart of the NHS agenda. Treating and caring for people in a safe
Online library of Quality, Service Improvement and Redesign tools. Reliable design. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Reliable design collaboration trust respect innovation courage compassion Reliable design What is it? Patients receiving the right care,
Online library of Quality, Service Improvement and Redesign tools Reliable design collaboration trust respect innovation courage compassion Reliable design What is it? Patients receiving the right care,
A3/B3: Improvement in the Intensive Care Unit
 A3/B3: Improvement in the Intensive Care Unit Carol Peden, MD, MPH, FRCA, FFICM, Associate Medical Director for Quality Improvement, Consultant in Anesthesia and Intensive Care Session Objectives Structure
A3/B3: Improvement in the Intensive Care Unit Carol Peden, MD, MPH, FRCA, FFICM, Associate Medical Director for Quality Improvement, Consultant in Anesthesia and Intensive Care Session Objectives Structure
Guidance on End of Life Care-Updated July 2014
 Guidance on End of Life Care-Updated July 2014 INTRODUCTION Definition of End of Life Care: End of Life care helps all those with advanced, progressive, incurable illness to live as well as possible until
Guidance on End of Life Care-Updated July 2014 INTRODUCTION Definition of End of Life Care: End of Life care helps all those with advanced, progressive, incurable illness to live as well as possible until
Sign up to Safety Drivers and Measurement
 Sign up to Safety Drivers and Measurement Expert Partner Nicola Davey Topics for today Driver diagrams Linking improvement aims to strategic objectives Generating simple improvement measures Measures
Sign up to Safety Drivers and Measurement Expert Partner Nicola Davey Topics for today Driver diagrams Linking improvement aims to strategic objectives Generating simple improvement measures Measures
IHA District Meetings February-March, : Iowa Environmental Assessment in Quality and Patient Safety HEN, QIN, TCPI, SIM
 IHA District Meetings February-March, 2015 2015: Iowa Environmental Assessment in Quality and Patient Safety HEN, QIN, TCPI, SIM Looking Back 10 Years Ago IHA, AHA, CMS, IFMC, State of Iowa, JCAHO, AHRQ
IHA District Meetings February-March, 2015 2015: Iowa Environmental Assessment in Quality and Patient Safety HEN, QIN, TCPI, SIM Looking Back 10 Years Ago IHA, AHA, CMS, IFMC, State of Iowa, JCAHO, AHRQ
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
Partnering with Patients to Drive Safety and Quality
 Partnering with Patients to Drive Safety and Quality CLINICAL EXCELLENCE COMMISSION Virginia Armour Program Manager, Patient Based Care 2 November 2015 AHHA Patient engagement and the patient experience
Partnering with Patients to Drive Safety and Quality CLINICAL EXCELLENCE COMMISSION Virginia Armour Program Manager, Patient Based Care 2 November 2015 AHHA Patient engagement and the patient experience
CAREER & EDUCATION FRAMEWORK
 CAREER & EDUCATION FRAMEWORK FOR NURSES IN PRIMARY HEALTH CARE ENROLLED NURSES Acknowledgments The Career and Education Framework is funded by the Australian Government Department of Health under the Nursing
CAREER & EDUCATION FRAMEWORK FOR NURSES IN PRIMARY HEALTH CARE ENROLLED NURSES Acknowledgments The Career and Education Framework is funded by the Australian Government Department of Health under the Nursing
MORTALITY REVIEW POLICY
 MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
Safety and Quality Measures: What, Why and How? APHA Congress 2010
 Safety and Quality Measures: What, Why and How? APHA Congress 2010 Chris Baggoley 19 October 2010 Harvard study 17yrs on Although much good work has been carried out there is a sense at the coalface of
Safety and Quality Measures: What, Why and How? APHA Congress 2010 Chris Baggoley 19 October 2010 Harvard study 17yrs on Although much good work has been carried out there is a sense at the coalface of
Background. The Walton Centre NHS Foundation Trust QUALITY AND PATIENT SAFETY STRATEGY
 QUALITY AND PATIENT SAFETY STRATEGY 2015-2018 1 Background 2 In 2008, Lord Darzi s High Quality Care for All set out a vision for an NHS with quality at its heart. The report led to an understanding that
QUALITY AND PATIENT SAFETY STRATEGY 2015-2018 1 Background 2 In 2008, Lord Darzi s High Quality Care for All set out a vision for an NHS with quality at its heart. The report led to an understanding that
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Guidelines for the Management of Patients who are End of Life
 Guidelines for the Management of Patients who are End of Life This procedural document supersedes: PAT/T 65 v.1 Management of Patients who are End of Life. Did you print this document yourself? The Trust
Guidelines for the Management of Patients who are End of Life This procedural document supersedes: PAT/T 65 v.1 Management of Patients who are End of Life. Did you print this document yourself? The Trust
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
The Importance of Culture in Health Care Settings [and its relationship to safety and quality]
![The Importance of Culture in Health Care Settings [and its relationship to safety and quality]](/thumbs/80/82431804.jpg "The Importance of Culture in Health Care Settings [and its relationship to safety and quality]") The Importance of Culture in Health Care Settings [and its relationship to safety and quality] Australian Institute of Health Innovation Professor Jeffrey Braithwaite, PhD Centre for Clinical Governance
The Importance of Culture in Health Care Settings [and its relationship to safety and quality] Australian Institute of Health Innovation Professor Jeffrey Braithwaite, PhD Centre for Clinical Governance
Incident Reporting Systems and Future Strategies for Patient Safety Improvement
 WHITE PAPER: Incident Reporting Systems and Future Strategies for Patient Safety Improvement Author: Datix Date: 2016/17 Driving down harm How can healthcare providers most successfully pursue the goal
WHITE PAPER: Incident Reporting Systems and Future Strategies for Patient Safety Improvement Author: Datix Date: 2016/17 Driving down harm How can healthcare providers most successfully pursue the goal
HEI self-assessment. Completing the self-assessment - Guidance to NHS boards
 HEI self-assessment Completing the self-assessment - Guidance to NHS boards INTRODUCTION This document should be read in conjunction Healthcare Improvement Scotland healthcare associated infection (HAI)
HEI self-assessment Completing the self-assessment - Guidance to NHS boards INTRODUCTION This document should be read in conjunction Healthcare Improvement Scotland healthcare associated infection (HAI)
Healthcare quality lessons from the best small country in the world
 Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Paediatrics. PEWS & Deteriorating Patients Linda Clerihew
 Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
National Mortality Case Record Review Programme. Using the structured judgement review method A guide for reviewers (England)
") National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
Sue Brown Clinical Audit and Effectiveness Manager. Safety and Quality Committee
 Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Saving Lives with Best Practices and Improvements in Sepsis Care
 Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Betsi Cadwaladr University Health Board. Quality and Safety Committee Item QS12/60.4. Subject:
 Betsi Cadwaladr University Health Board Quality and Safety Committee14.6.12 Item QS12/60.4 Subject: Summary or Issues of Significance Wales Ombudsman s Report Section 16 aggregated review: Serious Concerns
Betsi Cadwaladr University Health Board Quality and Safety Committee14.6.12 Item QS12/60.4 Subject: Summary or Issues of Significance Wales Ombudsman s Report Section 16 aggregated review: Serious Concerns
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Sepsis The Silent Killer in the NHS
 Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Acute kidney injury Keeping kidneys healthy: The AKI programme board. Dr Richard Fluck, National Clinical Director (Renal) NHS England
 NHS England") Acute kidney injury Keeping kidneys healthy: The AKI programme board Dr Richard Fluck, National Clinical Director (Renal) NHS England NHS Outcomes Framework NHS Five Year Forward View A vision for the
Acute kidney injury Keeping kidneys healthy: The AKI programme board Dr Richard Fluck, National Clinical Director (Renal) NHS England NHS Outcomes Framework NHS Five Year Forward View A vision for the
Developing a Patient Safety Culture within the NHS Setting the Scene. Peter Davey
 University of Dundee School of Medicine Developing a Patient Safety Culture within the NHS Setting the Scene Peter Davey How Do We See Ourselves? content courtesy of Martin Marshall, Director of Clinical
University of Dundee School of Medicine Developing a Patient Safety Culture within the NHS Setting the Scene Peter Davey How Do We See Ourselves? content courtesy of Martin Marshall, Director of Clinical
CASE STUDY The Safer Patients Initiative
 CSE STUDY The Safer Patients Initiative Critical care in practice: Royal ree Hospital and the University Hospital of Wales 1. INTRODUCTION In late 4, the Health oundation funded the Institute for Healthcare
CSE STUDY The Safer Patients Initiative Critical care in practice: Royal ree Hospital and the University Hospital of Wales 1. INTRODUCTION In late 4, the Health oundation funded the Institute for Healthcare
A Step-by-Step Guide to Tackling your Challenges
 Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
PATIENT SAFETY IMPROVEMENT: THE WAY FORWARD
 PATIENT SAFETY IMPROVEMENT: THE WAY FORWARD Hong Kong May 2010 Philip Hassen, President ISQua Former CEO, CPSI Background Canadian population in 2006 was 32.5 million Canadian healthcare spending for 2007
PATIENT SAFETY IMPROVEMENT: THE WAY FORWARD Hong Kong May 2010 Philip Hassen, President ISQua Former CEO, CPSI Background Canadian population in 2006 was 32.5 million Canadian healthcare spending for 2007
April Clinical Governance Corporate Report Narrative
 April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
Using the structured judgement review method
 National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
Overall rating for this trust Good. Inspection report. Ratings. Are services safe? Requires improvement. Are services effective?
 Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Key Challenges in Implementing the 5 Priorities of Care. Monday 30 th March 2015 Cedar Court Wakefield
 Key Challenges in Implementing the 5 Priorities of Care Monday 30 th March 2015 Cedar Court Wakefield The Five Priorities for Care National Update (Bee Wee s slides adapted) Suzanne Kite 30 March 2015
Key Challenges in Implementing the 5 Priorities of Care Monday 30 th March 2015 Cedar Court Wakefield The Five Priorities for Care National Update (Bee Wee s slides adapted) Suzanne Kite 30 March 2015
Acceleration for ACS. NSTEMI Event 09 November. Outputs from Table Discussions
 Acceleration for ACS NSTEMI Event 09 November Outputs from Table Discussions 1 1. What mechanism do we need to have to identify patients early (within 6 hours of admission to hospital)? Have identification
Acceleration for ACS NSTEMI Event 09 November Outputs from Table Discussions 1 1. What mechanism do we need to have to identify patients early (within 6 hours of admission to hospital)? Have identification
DETERIORATING PATIENT POLICY GENERAL POLICY NO. 50
 DETERIORATING PATIENT POLICY GENERAL POLICY NO. 50 Applies to: Committee for Approval Date of Approval September 2012 Date Ratified: September 2012 Review Date: September 2015 Name of Lead Manager Version:
DETERIORATING PATIENT POLICY GENERAL POLICY NO. 50 Applies to: Committee for Approval Date of Approval September 2012 Date Ratified: September 2012 Review Date: September 2015 Name of Lead Manager Version:
@ncepod #tracheostomy
 @ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
@ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
1. Guidance notes. Social care (Adults, England) Knowledge set for end of life care. (revised edition, 2010) What are knowledge sets?
 Knowledge set for end of life care. (revised edition, 2010) What are knowledge sets?") Social care (Adults, England) Knowledge set for end of life care (revised edition, 2010) Part of the sector skills council Skills for Care and Development 1. Guidance notes What are knowledge sets? Knowledge
Social care (Adults, England) Knowledge set for end of life care (revised edition, 2010) Part of the sector skills council Skills for Care and Development 1. Guidance notes What are knowledge sets? Knowledge
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Sepsis Kills: The challenges & solutions to reducing mortality
 Sepsis Kills: The challenges & solutions to reducing mortality Kevin Rooney, Ahmed Labib & Brent Foreman Who are we? Declaration of Conflict of Interest We have no financial conflict of interest in presenting
Sepsis Kills: The challenges & solutions to reducing mortality Kevin Rooney, Ahmed Labib & Brent Foreman Who are we? Declaration of Conflict of Interest We have no financial conflict of interest in presenting
'Think Kidneys': Improving the management of acute kidney injury in the NHS
 WELCOME TO THIS SIGN UP TO SAFETY WEBINAR 'Think Kidneys': Improving the management of acute kidney injury in the NHS All participants lines are muted to reduce background noise Acute Kidney Injury National
WELCOME TO THIS SIGN UP TO SAFETY WEBINAR 'Think Kidneys': Improving the management of acute kidney injury in the NHS All participants lines are muted to reduce background noise Acute Kidney Injury National
Quality Strategy: Liverpool Women s NHS Foundation Trust
 Quality Strategy: 2017-2020 Liverpool Women s NHS Foundation Trust Contents Foreword... 3 Our Trust... 4 Trust Board... 4 What is our Vision and what are our Aims and Values?... 5 The drivers in developing
Quality Strategy: 2017-2020 Liverpool Women s NHS Foundation Trust Contents Foreword... 3 Our Trust... 4 Trust Board... 4 What is our Vision and what are our Aims and Values?... 5 The drivers in developing
Quality Improvement Scorecard February 2017
 Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Fitzwilliam Hospital Milton Way, South Bretton, Peterborough,
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Fitzwilliam Hospital Milton Way, South Bretton, Peterborough,
Thinking Differently Acting Differently. Higher staff satisfaction = better patient outcomes & better patient experience
 Thinking Differently Acting Differently Higher staff satisfaction = better patient outcomes & better patient experience Staff Satisfaction is the best indicator of a High Quality Culture Nursing contribution
Thinking Differently Acting Differently Higher staff satisfaction = better patient outcomes & better patient experience Staff Satisfaction is the best indicator of a High Quality Culture Nursing contribution
Violence and Aggression NICE guideline Important implications for practice. Peter Tyrer, Imperial College, London
 Violence and Aggression NICE guideline Important implications for practice Peter Tyrer, Imperial College, London Reason for update of 2005 guideline This guideline was felt to be a little too restrictive
Violence and Aggression NICE guideline Important implications for practice Peter Tyrer, Imperial College, London Reason for update of 2005 guideline This guideline was felt to be a little too restrictive
Incident reporting systems: Future strategies for patient safety improvement
 White paper Incident reporting systems: Future strategies for patient safety improvement There has been much global focus on improving patient safety in recent years but despite this, progress has been
White paper Incident reporting systems: Future strategies for patient safety improvement There has been much global focus on improving patient safety in recent years but despite this, progress has been
Patient Safety Collaboratives. Plans on a page 2016
 Patient Safety Collaboratives Plans on a page 2016 What are Patient Safety Collaboratives? The Patient Safety Collaboratives identify and spread safer care initiatives from within the NHS, as well as draw
Patient Safety Collaboratives Plans on a page 2016 What are Patient Safety Collaboratives? The Patient Safety Collaboratives identify and spread safer care initiatives from within the NHS, as well as draw
Page 1 of 26. Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - November 2014
 Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - November 2014 Clinical Quality Service Page 1 of 26 Print Date:18/11/2014 Clinical Governance
Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - November 2014 Clinical Quality Service Page 1 of 26 Print Date:18/11/2014 Clinical Governance
The Ethos Program: Re-defining Normal
 The Ethos Program: Re-defining Normal Dr Victoria Atkinson Group Chief Medical Officer Group General Manager Clinical Governance Cardiothoracic Surgeon Victoria.Atkinson@svha.org.au 1 1. Background Unprofessional
The Ethos Program: Re-defining Normal Dr Victoria Atkinson Group Chief Medical Officer Group General Manager Clinical Governance Cardiothoracic Surgeon Victoria.Atkinson@svha.org.au 1 1. Background Unprofessional
Why Shepherd? Shepherd Center Patients. Here s How We Measure Up: Shepherd Patient Population
 Center Patients Total Patients ABI Patients SCI Patients Other Patients Center specializes in medical treatment, research and rehabilitation for people with spinal cord and brain injury. In CY, had 911
Center Patients Total Patients ABI Patients SCI Patients Other Patients Center specializes in medical treatment, research and rehabilitation for people with spinal cord and brain injury. In CY, had 911
Worcestershire Acute Hospitals NHS Trust
 Worcestershire Acute Hospitals NHS Trust Worcestershire Royal Hospital Quality Report Charles Hastings Way Worcester WR5 1DD Tel: 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit: 12,
Worcestershire Acute Hospitals NHS Trust Worcestershire Royal Hospital Quality Report Charles Hastings Way Worcester WR5 1DD Tel: 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit: 12,
This guide has been produced by Dr Dave Hope, Dr Mark Smithies, Dr Alan Willson and Chris Hancock.
 Acknowledgements This guide has been produced by Dr Dave Hope, Dr Mark Smithies, Dr Alan Willson and Chris Hancock. We would particularly like to thank healthcare organisations in Wales and their teams
Acknowledgements This guide has been produced by Dr Dave Hope, Dr Mark Smithies, Dr Alan Willson and Chris Hancock. We would particularly like to thank healthcare organisations in Wales and their teams
Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath
 Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath Up to 25,000 surgical deaths per year 5-10% of surgical cases are high risk 79% of deaths occur in the high risk group Overall
Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath Up to 25,000 surgical deaths per year 5-10% of surgical cases are high risk 79% of deaths occur in the high risk group Overall
Hospital Acquired Conditions. Tracy Blair MSN, RN
 Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
The measurement and monitoring of safety
 The measurement and monitoring of safety Health Foundation summary April 2013 For more information and to download or order the full report, please visit: www.health.org.uk/measuresafety Introduction Over
The measurement and monitoring of safety Health Foundation summary April 2013 For more information and to download or order the full report, please visit: www.health.org.uk/measuresafety Introduction Over
Sepsis guidance implementation advice for adults
 Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation