Increased situational awareness to reduce undetected deterioration
|
|
|
- Leonard Heath
- 5 years ago
- Views:
Transcription
1 Increased situational awareness to reduce undetected deterioration SPSP Paediatric Care WebEx Patrick W. Brady, MD, MSc Associate Professor of Pediatrics Division of Hospital Medicine
2 Objectives Understand the concept of Situation Awareness and its application in health care Describe how huddles, proactive risk assessment and mitigation plans are used to improve patient safety Share ideas and ongoing work to further leverage patients, families, care teams and big data to improve situation awareness and patient safety
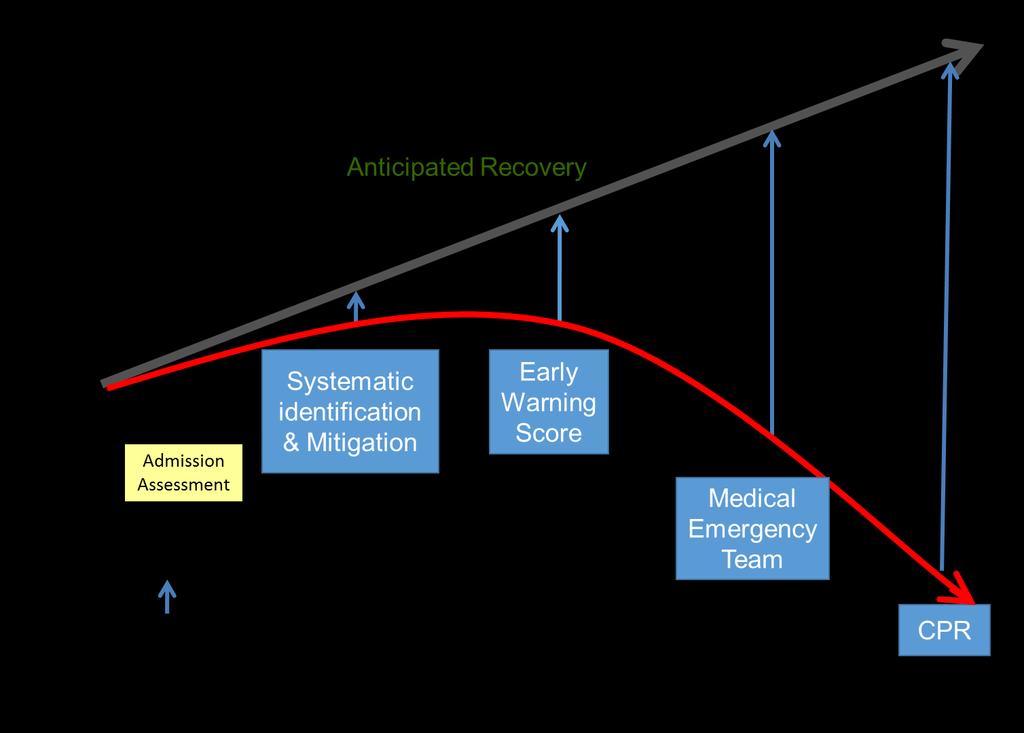
3 Clinical Example 6 month old is admitted to floor with acute gastroenteritis is initially improved after 2 fluid boluses in ED Begun on maintenance fluids but diarrhea increases Overnight parents note he is less playful Later heart rate rises from 120 to 170 On morning pre-rounds he is difficult to awake Pulses difficult to palpate and code called
4 Outcome of In-Hospital Arrest Pediatric patients that suffer a cardiopulmonary arrest have a dismal prognosis 50-67% mortality Many others with long-term neurologic morbidity Many of these arrests are preventable if we can identify patients as they begin to deteriorate
5 Patients don t suddenly deteriorate. Healthcare professionals suddenly notice.
6


7 Inattentional blindness in vigilance tasks Simons and Chabris 1999 Drew, Vo, and Wolfe 2013

8 Situation Awareness 1. Gather Information Perception What? 2. Recognize & Understand Comprehension So What? 3. Anticipate Projection What Now? Decide Act Brady Hospital Pediatrics 2014
9 What is Situation Awareness (SA)? Simple Definition: Knowing what is going on around you Having a notion of what is important Anticipation of possible future consequences of the current situation Dr. Mica Endsley (1995) Shared situation awareness: The degree to which team members have the same SA in important areas Endsley Human Factors 1995
10 So is SA a problem in healthcare? In studies looking at agreement among team members (shared SA): In a Scottish ICU, when physicians on same team predicted likelihood of deterioration, they agreed on 45% of patients 1 In a US hospital, nurses and physicians caring for the same patients agreed on 42% of medication changes and 11% of planned procedures 2 1 Reader BMJ Quality and Safety O Leary BMJ Quality and Safety 2010
11 System that improved situation awareness and reduced untreated clinical deterioration would reliably: Proactively identify patients at risk Through PEWS, gut feeling ( watchers ), high-risk therapies, etc. Mitigate risk on the unit through primary team With specific, time-bound plans and predictions Escalate risk that is not fully addressed Through rapid response teams and scheduled huddles Brady Pediatrics 2013

12 Tacit knowledge: Watchers Crandall et al 1993

13 Patient List Screen
14 Huddles Short, structured briefings designed to: look back on recent events look forward to upcoming events/emerging threats We integrate 3 tiers of huddles: Microsystem (e.g. general pediatric unit) Mesosystem (e.g. inpatient system) Macrosystem (organizational) Goldenhar BMJ Quality and Safety 2013
15 MICRO LEVEL (Unit Huddle) Look back: individual providers report on unexpected events, medical response team calls Look forward: individual providers report on individual patients at risk for safety events Integration: charge nurse considers overall unit status, planned discharges, staffing needs Unit 2 Unit 3 MESO LEVEL (Inpatient Huddle) Look back: charge nurses from each microsystem report on unexpected events, transfers to higher levels of care Look forward: individual microsystems report on higher risk patients in mesosystem, overall unit status Integration: Manager of Patient Services (MPS) works with charge nurses to develop plans and predictions for highest risk patients, develop capacity plan through system, predict and mitigate experience failures Periop MACRO LEVEL (Daily Operations Brief) Look back: mesosystem leaders report on unexpected outcomes over last 24 hours, resolution of concerns raised at previous brief Look forward: mesosystem leaders predict and plan for big issues of day with focus on problems at intersections of mesosystems Integration: administrator of the day identifies responsible party(ies) for each concerns and sets clear follow-up Goldenhar BMJ Quality and Safety 2013

16 Proactive escalation through mesosystem huddle Three times daily discussion of any concerns not fully addressed and any predicted MRTs Includes: Charge nurse from each unit Nurse manager Senior attending Safety Officer Nurse manager and safety officer coach charge nurses
")
17 Safety officer of the day (SOD) Attending-level physician with: gray hair Clinical expertise Organizational expertise Gravitas Skilled communicator and teacher OR maybe? More junior physician with clear access to and authority given from senior leader (e.g., Chief of Staff, CMO)
18 Our first year: identifying is only a start First year of journey moved from relying on individual clinicians to a system that identified >90% of patients who had UNSAFE transfers BUT in many cases risk was not successfully mitigated/reversed AND risk was not escalated even when patient was not improving Watching the watchers


19 SMART Aim Specific Measurable Actionable Relevant Time bound Some is not a number. Soon is not a time. Don Berwick

20 Robust Planning Tool Identifying the problem or concern Making responsible parties aware Forming a plan Predicting an expected outcome Setting a deadline Deciding on an escalation plan if outcome is not met
21

22 Brady Pediatrics 2013 Defined as any patient that is transferred from unit to ICU and within 1 hour is: Intubated Placed on inotropes OR Given 3 or more fluid boluses

23 Brady Pediatrics 2013 March 2010: Huddles/ Inpatient SA work spread
24 Proposed model Goldenhar BMJ Quality and Safety 2013
25 Huddle results Improved efficiencies and quality of information sharing We learned the new terminology..we learned what a watcher was, we learned what high risk therapy was, and then in practice continued to report these concerns, we began to identify who was at risk on your unit, and who wasn t. (Bedside nurse) Goldenhar BMJ Quality and Safety 2013
26 Huddle results Culture of collaboration/collegiality Anti-competition, consideration, compassion don t assume that the unit is saying no because they don t want to help, all have a better idea of what s going on other units and know that everyone is busy! (Nurse manager) Goldenhar BMJ Quality and Safety 2013
27 Improvement learnings Cincinnati Need a multidisciplinary team Nurses, doctors, improvement experts Intensivists and non-intensivists (hospitalists are often great partners) Need senior leadership support Need outcome metrics (emergency transfers, critical deterioration, etc.) Start with the willing and design healthy competition Tell stories loudly and often Even in sustain needs continued check-in points and coaching (e.g., at huddles)


28 Spread across Ohio children s hospitals
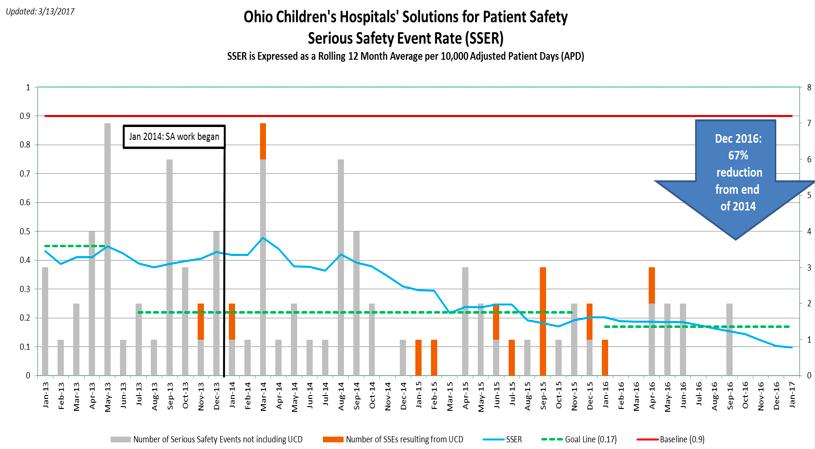
29
30 Context, context, context Organizational structure differs greatly and is tremendously important Need to find the right boots on the ground leaders as well as senior leader support Mature safety culture is needed Cannot argue about preventability for months Front-line needs some empowerment Process metric (reliability of SA bundle) is labor-intensive without an EHR


31 Take home: doing QI well, with discipline, is really hard And this is what is published!
32 Improvement learnings spread Fail often and small: 2-3 PDSAs per week, n of 1 testing It is impossible to get this right the first time or to plan it perfectly Understand your system quantitatively and qualitatively before you start What are the most common failures? When do they occur? Does a busy resident or nurse think unrecognized deterioration/situation awareness is an important challenge? Have a theory or framework connecting your intervention(s) to your specific and global aims Focus on drivers, not roles or exact processes Understand education and communication are likely necessary but not sufficient for reliable improvement

33 OHIO CHILDREN S HOPITALS SOLUTIONS FOR PT. SAFETY (OCHSPS) OHIO NETWORK Situation Awareness KDD AIM Reduce the Ohio Network s Emergency Transfer (ET) Rate per 10,000 APD from 4.4 to 2.2 by 12/31/17 KEY DRIVERS Effective Learning Structure Senior Leaders Engagement & Support Unit Leaders Engagement & Support Situation Awareness Bundle: ID, Mitigate, Escalate Unit RIsk (Process Measure: %Reliability to SA Bundle) Culture of RESPECT INTERVENTIONS 1. QTLY OCHA Board Meetings 2. Other CEO communications 3. Resource allocation 4. Accountability of leaders to uphold hospital respect standards 5. CEO s assign Sr. Leader Champions of SSE events 6. OTHER? 1. Unit Leader Rounding to Influence 2. Unit Daily Huddles 3. Unit Top 10 Problem List 1. Identify patient-level risk factors such as -PEWS -Watcher/gut feeling -High-risk therapies -Family concerns 2. OTHER??? 1. Mitigation of pt. level risk factors such as: - Unit huddles - Planning tools such as checklists, templates, and EHR tools 2. OTHER??? 1. Escalation of pt. level risk factors such as: - Inpatient huddles - Safety officer of the day - Safety rounds - Family-activation of rapid response team 2. OTHER???
34 Leadership Methods for SA Daily Organizational Safety Brief Share if you had an Emergency Transfer (formerly UNSAFE transfer) during brief Follow up on a future brief re: results of lessons learned from Emergency Transfer Senior Leader Walkaround - Senior Leaders focus (with script) on progress with SA Bundle and key lessons learned by bedside and unit leaders Unit Leaders utilize structured tools such as an Apparent Cause Analysis for each transfer
35 Leadership Methods for SA Daily Rounding to Influence at Unit Level Unit leaders round to identify barriers with the SA Bundle Talk with staff about any events and lessons learned Reinforce significance of SA work Daily Unit Huddles Review last 24 hours SA Bundle reliability, events, etc. Predict for next 24 hours Top 10 Problem List Barriers identified with implementation are placed on list Process issues from events placed on list

36 Abundance We should work not from an assumption of scarcity, but from an assumption of abundance. -Paul Batalden We have abundant & underused: Patient/family expertise Clinician expertise Data SA provides a framework to better leverage these to improve safety and quality of care
37 Questions?
Building Systems and Leadership for Transformation
 Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Building Systems and Leadership for Transformation April 7, 2016 Dr. Uma Kotagal Senior Fellow Executive Leader, Population and Community Health Efforts Cincinnati Children s Hospital Medical Center "It
Value Equation for Healthcare
 Value Equation for Healthcare Value = (Outcomes + Patient Experience) x Appropriateness Cost + Hassle Factor What Do Patients Hire Us to Provide What do they call Value Make the Right Diagnosis Deliver
Value Equation for Healthcare Value = (Outcomes + Patient Experience) x Appropriateness Cost + Hassle Factor What Do Patients Hire Us to Provide What do they call Value Make the Right Diagnosis Deliver
Large scale health systems improvement to recognise and manage deteriorating patients Dr Harvey Lander and Malcolm Green
 Large scale health systems improvement to recognise and manage deteriorating patients Dr Harvey Lander and Malcolm Green Australia? YOU ARE HERE NSW PRESENTATION NAME MONTH YYYY PRESENTER NAME 3 Clinical
Large scale health systems improvement to recognise and manage deteriorating patients Dr Harvey Lander and Malcolm Green Australia? YOU ARE HERE NSW PRESENTATION NAME MONTH YYYY PRESENTER NAME 3 Clinical
Developing HUDDLES in Healthcare
 Developing HUDDLES in Healthcare Dr Kate Pryde Consultant Paediatrician, Southampton Children s Hospital October 2017 @katepryde Huddles Healthcare HUDDLES Preparatory briefing among healthcare professionals
Developing HUDDLES in Healthcare Dr Kate Pryde Consultant Paediatrician, Southampton Children s Hospital October 2017 @katepryde Huddles Healthcare HUDDLES Preparatory briefing among healthcare professionals
4/12/2016. High Reliability and Microsystem Stress. We have no financial, professional or personal conflict of interest to disclose.
 High Reliability and Microsystem Stress Helping leaders identify and mitigate unit level stress: Next steps towards the journey of high reliability Whittney Brady RN, DNP Jackie Hausfeld, RN, MSN, NEA-BC
High Reliability and Microsystem Stress Helping leaders identify and mitigate unit level stress: Next steps towards the journey of high reliability Whittney Brady RN, DNP Jackie Hausfeld, RN, MSN, NEA-BC
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
Inpatient Flow Real Time Demand Capacity: Building the System
 Inpatient Flow Real Time Demand Capacity: Building the System Roger Resar, MD, Kevin Nolan, and Deb Kaczynski We would like to acknowledge the conceptual contributions of Diane Jacobsen, Marilyn Rudolph,
Inpatient Flow Real Time Demand Capacity: Building the System Roger Resar, MD, Kevin Nolan, and Deb Kaczynski We would like to acknowledge the conceptual contributions of Diane Jacobsen, Marilyn Rudolph,
Writing Manuscripts About Quality Improvement: SQUIRE 2.0 and Beyond
 Writing Manuscripts About Quality Improvement: SQUIRE 2.0 and Beyond Author Marilyn H. Oermann, PhD, RN, ANEF, FAAN Thelma M. Ingles Professor of Nursing, Duke University School of Nursing Editor, Journal
Writing Manuscripts About Quality Improvement: SQUIRE 2.0 and Beyond Author Marilyn H. Oermann, PhD, RN, ANEF, FAAN Thelma M. Ingles Professor of Nursing, Duke University School of Nursing Editor, Journal
Welcome Aboard: A Children s Adventure
 IHI um Virtual Site Visit to Cincinnati Children s Hospital Medical Center 1 Welcome Aboard: A Children s Adventure 2 1 The Transformation Journey: Improvement, Caring, Integration, Transparency Uma Kotagal,
IHI um Virtual Site Visit to Cincinnati Children s Hospital Medical Center 1 Welcome Aboard: A Children s Adventure 2 1 The Transformation Journey: Improvement, Caring, Integration, Transparency Uma Kotagal,
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
SITE APPLICABILITY This practice applies to all pediatric patient care areas that have been designated by your health authority.
 GUIDELINE PURPOSE To provide guidance and direction for the use of the Pediatric Early Warning System (PEWS). The PEWS system supports the recognition, mitigation, notification, and response to the pediatric
GUIDELINE PURPOSE To provide guidance and direction for the use of the Pediatric Early Warning System (PEWS). The PEWS system supports the recognition, mitigation, notification, and response to the pediatric
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Safety Huddles: Bringing fun to the frontline and reducing harm
 Safety Huddles: Bringing fun to the frontline and reducing harm Alison Lovatt Clinical Network Director, Improvement Academy Ali Cracknell Consultant Medicine For Older People, Leeds Teaching Hospitals
Safety Huddles: Bringing fun to the frontline and reducing harm Alison Lovatt Clinical Network Director, Improvement Academy Ali Cracknell Consultant Medicine For Older People, Leeds Teaching Hospitals
Paediatrics. PEWS & Deteriorating Patients Linda Clerihew
 Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
Paediatrics PEWS & Deteriorating Patients Linda Clerihew SPSP 2007 SPSPP 2010 McQIC 2013 Aim 30% reduction in avoidable harm measured by the Paediatric Serious Harm Key Indicators by December 2015 Measuring
Value, Suffering, and 10 Things I Didn t Know Before My New Job
 Value, Suffering, and 10 Things I Didn t Know Before My New Job Thomas H. Lee, MD October 28, 2013 2 1 Why We Are Stuck 3 Getting Unstuck 2 Step One: Clarifying the Overarching Goal In the absence of an
Value, Suffering, and 10 Things I Didn t Know Before My New Job Thomas H. Lee, MD October 28, 2013 2 1 Why We Are Stuck 3 Getting Unstuck 2 Step One: Clarifying the Overarching Goal In the absence of an
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
CARE DELIVERY TEAM NURSING GUIDELINES
 STANDARDS TO BE MET Team nursing is a model of care which utilises the resources within a nursing team on a shift by shift basis to deliver safe patient care within the clinical unit. The Bay of Plenty
STANDARDS TO BE MET Team nursing is a model of care which utilises the resources within a nursing team on a shift by shift basis to deliver safe patient care within the clinical unit. The Bay of Plenty
Policy for Admission to Adult Critical Care Services
 Policy Number: CCaNNI 008 Title: Policy for Admission to Adult Critical Care Services Operational Date: Review Date: December 2009 December 2012 Type of Document: EQIA Screening Date: Corporate x Clinical
Policy Number: CCaNNI 008 Title: Policy for Admission to Adult Critical Care Services Operational Date: Review Date: December 2009 December 2012 Type of Document: EQIA Screening Date: Corporate x Clinical
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
You have joined the CUSP Communication & Teamwork Tools Informational Session!
 You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
NICU Graduates: Using the Model for Improvement and Learning from Data
 NICU Graduates: Using the Model for Improvement and Learning from Data Kristin Voos, MD and Dan Benscoter, DO Learning Session May 10, 2016 Through collaborative use of improvement science methods, reduce
NICU Graduates: Using the Model for Improvement and Learning from Data Kristin Voos, MD and Dan Benscoter, DO Learning Session May 10, 2016 Through collaborative use of improvement science methods, reduce
Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management
 Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management Michelle Cline, RN, MSN, Care Model Redesign Manager Donna Litwinski, PT, Master Lean Fellow April 2018
Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management Michelle Cline, RN, MSN, Care Model Redesign Manager Donna Litwinski, PT, Master Lean Fellow April 2018
HealthONE Sepsis Program
 HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Safety Measurement, Monitoring & Strategies
 Safety Measurement, Monitoring & Strategies Jonkoping Microsystem Festival Scientific Day March 2016 Charles Vincent Professor of Psychology University of Oxford Lead Oxford AHSN Patient Safety Collaborative
Safety Measurement, Monitoring & Strategies Jonkoping Microsystem Festival Scientific Day March 2016 Charles Vincent Professor of Psychology University of Oxford Lead Oxford AHSN Patient Safety Collaborative
Healthcare Improvement Scotland. NHS Tayside
 Faculty Site Visit Report Healthcare Improvement Scotland NHS Tayside 8 th June 2011 FINAL VERSION 19 July 2011 CONTENTS 1. Key Contacts... 2 NHS Tayside... 2 Site Visit Team... 2 2. SPSP Programme Key
Faculty Site Visit Report Healthcare Improvement Scotland NHS Tayside 8 th June 2011 FINAL VERSION 19 July 2011 CONTENTS 1. Key Contacts... 2 NHS Tayside... 2 Site Visit Team... 2 2. SPSP Programme Key
Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust
 Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust Mark Simmonds (Acute and Critical Care Medicine Consultant,
Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust Mark Simmonds (Acute and Critical Care Medicine Consultant,
Implementing PEWS. With Peter Lachman, Nikki Davey and The NHS
 Implementing PEWS Sebastian Yuen Sebastian.yuen@gmail.com Consultant Paediatrician, George Eliot Hospital, Nuneaton Fellow, NHS Institute for Innovation and Improvement (2008-10) With Peter Lachman, Nikki
Implementing PEWS Sebastian Yuen Sebastian.yuen@gmail.com Consultant Paediatrician, George Eliot Hospital, Nuneaton Fellow, NHS Institute for Innovation and Improvement (2008-10) With Peter Lachman, Nikki
REACH Patient and family activated escalation of care
 REACH Patient and family activated escalation of care 12 MONTHS ON AND THE SKY DID NOT FALL Dr Karen Luxford, Alison Lee & Prof Cliff Hughes ISQua 2013 Patient Based Care Model If I would have been able
REACH Patient and family activated escalation of care 12 MONTHS ON AND THE SKY DID NOT FALL Dr Karen Luxford, Alison Lee & Prof Cliff Hughes ISQua 2013 Patient Based Care Model If I would have been able
Driving Obstetrical Excellence Through a Council Structure
 Driving Obstetrical Excellence Through a Council Structure Elizabeth Deckers, MD Director of Labor and Delivery, Hartford Hospital Deborah Feldman, M.D. Division director, Maternal Fetal Medicine, Hartford
Driving Obstetrical Excellence Through a Council Structure Elizabeth Deckers, MD Director of Labor and Delivery, Hartford Hospital Deborah Feldman, M.D. Division director, Maternal Fetal Medicine, Hartford
COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL. Sepsis Treatment Order Sets Sepsis Treatment Order Sets
 Publication Year: 2013 COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL Summary: An organized accepted approach to sepsis recognition, early management in the ED including specific
Publication Year: 2013 COMPREHENSIVE EARLY GOAL DIRECTED THERAPY IN SEPSIS ROCHESTER GENERAL Summary: An organized accepted approach to sepsis recognition, early management in the ED including specific
Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care?
 Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care? Lee Dowson Divisional Director of Medicine Royal Wolverhampton NHS Trust Clinical Associate
Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care? Lee Dowson Divisional Director of Medicine Royal Wolverhampton NHS Trust Clinical Associate
Dr. Emily Cooper Leadership Fellow, Improvement Academy Alison O Halloran Compliance Manager, Roche Healthcare Kirsty Smith Team Leader, Fieldhead
 Dr. Emily Cooper Leadership Fellow, Improvement Academy Alison O Halloran Compliance Manager, Roche Healthcare Kirsty Smith Team Leader, Fieldhead Court Nursing Home, Roche Healthcare One of the UK s leading
Dr. Emily Cooper Leadership Fellow, Improvement Academy Alison O Halloran Compliance Manager, Roche Healthcare Kirsty Smith Team Leader, Fieldhead Court Nursing Home, Roche Healthcare One of the UK s leading
System enablers practical aspects Chair Lesley Anne Smith
 System enablers practical aspects Chair Lesley Anne Smith Time Topic Room Optional lunchtime sessions, numbers limited to 50 per room, catering provided in the room 13.15 QI Harris Level 1 Service Users
System enablers practical aspects Chair Lesley Anne Smith Time Topic Room Optional lunchtime sessions, numbers limited to 50 per room, catering provided in the room 13.15 QI Harris Level 1 Service Users
Rapid Cycle Improvement
 Rapid Cycle Improvement with PDSA CPSI Forum April 30, 2009 Eileen Patterson, MCE Director - Quality Improvement Ontario Health Quality Council 1 What is it? Roots are within System of Profound Knowledge;
Rapid Cycle Improvement with PDSA CPSI Forum April 30, 2009 Eileen Patterson, MCE Director - Quality Improvement Ontario Health Quality Council 1 What is it? Roots are within System of Profound Knowledge;
Revolutionizing Patient Safety through Organizational Certification Anne Arundel Medical Center
 Revolutionizing Patient Safety through Organizational Certification Anne Arundel Medical Center 1 Anne Arundel Medical Center 1 Learning Objectives Established the Patient Safety Officer (PSO) as the focal
Revolutionizing Patient Safety through Organizational Certification Anne Arundel Medical Center 1 Anne Arundel Medical Center 1 Learning Objectives Established the Patient Safety Officer (PSO) as the focal
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
The New Right Way: Introducing New Staffing Models on Vancouver Island
 The New Right Way: Introducing New Staffing Models on Vancouver Island Talk to any nurse and you ll probably hear the same thing: patients they ain t what they used to be! Aging baby boomers have changed
The New Right Way: Introducing New Staffing Models on Vancouver Island Talk to any nurse and you ll probably hear the same thing: patients they ain t what they used to be! Aging baby boomers have changed
The Colorado ALTO Project
 Using Alternatives to Opioids (ALTOs) in Hospital Emergency Departments PRE-LAUNCH CHECKLIST Based on the 2017 Opioid Prescribing & Treatment Guidelines Colorado ALTO Project Champion Sets the direction
Using Alternatives to Opioids (ALTOs) in Hospital Emergency Departments PRE-LAUNCH CHECKLIST Based on the 2017 Opioid Prescribing & Treatment Guidelines Colorado ALTO Project Champion Sets the direction
IHI Expedition. Improving Patient Experience and Making It Stick Session 5. Expedition Coordinator
 Wednesday, August 21, 2013 These presenters have nothing to disclose IHI Expedition Improving Patient Experience and Making It Stick Session 5 Barbara Balik, RN, EDd Kelly McCutcheon Adams, LICSW Expedition
Wednesday, August 21, 2013 These presenters have nothing to disclose IHI Expedition Improving Patient Experience and Making It Stick Session 5 Barbara Balik, RN, EDd Kelly McCutcheon Adams, LICSW Expedition
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
National COPD Audit Programme
 National COPD Audit Programme COPD: Working together Clinical audit of COPD exacerbations admitted to acute hospitals in England and Wales 2017 Findings and quality improvement The audit programme partnership
National COPD Audit Programme COPD: Working together Clinical audit of COPD exacerbations admitted to acute hospitals in England and Wales 2017 Findings and quality improvement The audit programme partnership
Aligning the Outcomes of DNP Education with the Demands of DNP Practice: A Panel Discussion
 Aligning the Outcomes of DNP Education with the Demands of DNP Practice: A Panel Discussion Laura J. Wood, DNP, MS, RN Boston Children s Hospital Senior Vice President, Patient Care Services & Chief Nursing
Aligning the Outcomes of DNP Education with the Demands of DNP Practice: A Panel Discussion Laura J. Wood, DNP, MS, RN Boston Children s Hospital Senior Vice President, Patient Care Services & Chief Nursing
Learning from the Patient Safety Champions November 24, 2017
 Learning from the Patient Safety Champions November 24, 2017 1 Audio for this webinar must be accessed via telephone: Dial In Number: 1-888-289-4573 Participant Access Code: 1339131 This webinar will be
Learning from the Patient Safety Champions November 24, 2017 1 Audio for this webinar must be accessed via telephone: Dial In Number: 1-888-289-4573 Participant Access Code: 1339131 This webinar will be
IMPROVING QUALITY AND SAFETY WHERE PATIENTS, FAMILIES, AND CARE TEAMS MEET THE CLINICAL MICROSYSTEM
 IMPROVING QUALITY AND SAFETY WHERE PATIENTS, FAMILIES, AND CARE TEAMS MEET THE CLINICAL MICROSYSTEM Gautham Suresh, MD, MS Associate Professor of Pediatrics and Community & Family Medicine Medical Director,
IMPROVING QUALITY AND SAFETY WHERE PATIENTS, FAMILIES, AND CARE TEAMS MEET THE CLINICAL MICROSYSTEM Gautham Suresh, MD, MS Associate Professor of Pediatrics and Community & Family Medicine Medical Director,
Fee: The fee for the 12-month renewal is $10,000.
 CHILDHOOD CANCER AND BLOOD DISORDERS NETWORK 2017 RENEWAL TOOLS HOW TO Renew To renew, simply submit a completed Childhood Cancer & Blood Disorders Network Renewal Form to Gena Paulk via email at gena.paulk@childrenshospitals.org.
CHILDHOOD CANCER AND BLOOD DISORDERS NETWORK 2017 RENEWAL TOOLS HOW TO Renew To renew, simply submit a completed Childhood Cancer & Blood Disorders Network Renewal Form to Gena Paulk via email at gena.paulk@childrenshospitals.org.
Saving Lives in Real-time
 Saving Lives in Real-time Cincinnati Children s approach to leveraging event-driven analytics to change the outcome (on all master slides) What would you do differently? Agenda CCHMC Introduction Our Journey
Saving Lives in Real-time Cincinnati Children s approach to leveraging event-driven analytics to change the outcome (on all master slides) What would you do differently? Agenda CCHMC Introduction Our Journey
NURSING SPECIAL REPORT
 2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
Provincial Pediatric Early Warning System (PEWS) Clinical Decision Support Tool. Guideline Purpose. Practice Level / Competencies.
 Clinical Decision Support Tool. Guideline Purpose. Practice Level / Competencies.") Guideline Purpose To provide guidance and direction for the use of the British Columbia Pediatric Early Warning System (BC PEWS). The PEWS system supports the early recognition, mitigation, notification,
Guideline Purpose To provide guidance and direction for the use of the British Columbia Pediatric Early Warning System (BC PEWS). The PEWS system supports the early recognition, mitigation, notification,
If you experience any problems, please call Marilyn Nichols at the MOCPS office at , ext 221 or The Basics of CUSP
 Welcome to The Basics of CUSPCoaching Call 6 The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842#. Participants received an email this morning
Welcome to The Basics of CUSPCoaching Call 6 The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842#. Participants received an email this morning
Acute Care Workflow Solutions
 Acute Care Workflow Solutions 2016 North American General Acute Care Workflow Solutions Product Leadership Award The Philips IntelliVue Guardian solution provides general floor, medical-surgical units,
Acute Care Workflow Solutions 2016 North American General Acute Care Workflow Solutions Product Leadership Award The Philips IntelliVue Guardian solution provides general floor, medical-surgical units,
Quality Improvement: Is it for payers or patients? Michael D. Kappelman Canadian Digestive Diseases Week February 9, 2014
 Quality Improvement: Is it for payers or patients? Michael D. Kappelman Canadian Digestive Diseases Week February 9, 2014 Accreditation This event has been approved as an accredited (Section1) group learning
Quality Improvement: Is it for payers or patients? Michael D. Kappelman Canadian Digestive Diseases Week February 9, 2014 Accreditation This event has been approved as an accredited (Section1) group learning
ACTION PLANS. OHA Statewide Sepsis Initiative. January 13, 2016
 ACTION PLANS OHA Statewide Sepsis Initiative January 13, 2016 USING DRIVER DIAGRAMS FOR ACTION PLANS Used to organize theories and ideas in an improvement effort Visual display of why things are the way
ACTION PLANS OHA Statewide Sepsis Initiative January 13, 2016 USING DRIVER DIAGRAMS FOR ACTION PLANS Used to organize theories and ideas in an improvement effort Visual display of why things are the way
Copyright Scottsdale Institute All Rights Reserved.
 Copyright Scottsdale Institute 2018. All Rights Reserved. No part of this document may be reproduced or shared with anyone outside of your organization without prior written consent from the author(s).
Copyright Scottsdale Institute 2018. All Rights Reserved. No part of this document may be reproduced or shared with anyone outside of your organization without prior written consent from the author(s).
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department
 Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Keep watch and intervene early
 IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
At that moment we realized that our website wasn t optimized for mobile use; it only worked when viewed on a computer. What a mistake on our part.
 We were in the process of re-designing our adolescent psychiatry unit s website. We were really pleased with how it was turning out until we asked a young woman how she might look for information about
We were in the process of re-designing our adolescent psychiatry unit s website. We were really pleased with how it was turning out until we asked a young woman how she might look for information about
Pressure Ulcers to Zero Collaborative Guide
 Pressure Ulcers to Zero Collaborative Guide Table of Contents Page Number Purpose of the guide 2 Why get involved? 3 Pressure Ulcer Definition 5 What is the Pressure Ulcers to Zero Collaborative 6 Getting
Pressure Ulcers to Zero Collaborative Guide Table of Contents Page Number Purpose of the guide 2 Why get involved? 3 Pressure Ulcer Definition 5 What is the Pressure Ulcers to Zero Collaborative 6 Getting
Promoting Transparency, Teamwork, and Real-time Review: The Morning Safety Huddle. St. Christopher s Hospital for Children
 Promoting Transparency, Teamwork, and Real-time Review: The Morning Safety Huddle St. Christopher s Hospital for Children 1 Agenda Facility Overview Evolution of the Morning Safety Huddle Structure of
Promoting Transparency, Teamwork, and Real-time Review: The Morning Safety Huddle St. Christopher s Hospital for Children 1 Agenda Facility Overview Evolution of the Morning Safety Huddle Structure of
Alison Hunter. Improvement Advisor, Acute Adult Safety Programme. Healthcare Improvement Scotland
 Alison Hunter Improvement Advisor, Acute Adult Safety Programme Healthcare Improvement Scotland Acute Adult 2008 what we did Leadership Medicines Perioperative Critical Care Reduce Mortality & Harm General
Alison Hunter Improvement Advisor, Acute Adult Safety Programme Healthcare Improvement Scotland Acute Adult 2008 what we did Leadership Medicines Perioperative Critical Care Reduce Mortality & Harm General
The Digital ICU: Return On Innovation
 The Digital ICU: Return On Innovation Cheryl Hiddleson, MSN, RN, CCRN-E Director, Emory eicu Center May, 2017 The Digital ICU: Return on Innovation Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu
The Digital ICU: Return On Innovation Cheryl Hiddleson, MSN, RN, CCRN-E Director, Emory eicu Center May, 2017 The Digital ICU: Return on Innovation Cheryl Hiddleson MSN, RN, CCRN-E Director, Emory eicu
Patient and Family Engagement Strategy. April 10, 2013
 Patient and Family Engagement Strategy April 10, 2013 1 Webinar Agenda Overview & Introductions Kathy Wallace Why is Patient & Family Engagement the Right Thing to do? Carrie Brady Patient & Family Advisor
Patient and Family Engagement Strategy April 10, 2013 1 Webinar Agenda Overview & Introductions Kathy Wallace Why is Patient & Family Engagement the Right Thing to do? Carrie Brady Patient & Family Advisor
Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation
 Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation Potential and Mobility Plan Amy Dean, MS, RN, CCRN Kristin
Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation Potential and Mobility Plan Amy Dean, MS, RN, CCRN Kristin
Developing a measure of facilitators and barriers to rapid response team activation
 Developing a measure of facilitators and barriers to rapid response team activation Kim Schafer Astroth, PhD, RN Wendy Mann Woith, PhD, RN, FAAN Sheryl Henry Jenkins, PhD, APN Matthew Hesson- McInnis,
Developing a measure of facilitators and barriers to rapid response team activation Kim Schafer Astroth, PhD, RN Wendy Mann Woith, PhD, RN, FAAN Sheryl Henry Jenkins, PhD, APN Matthew Hesson- McInnis,
AF4Q and TCAB: An Introduction
 AF4Q and TCAB: An Introduction July 13, 2011 Ellen Interlandi, MHM, RN, NE-BC Patricia Montoya, MPA, BSN 1 What is Aligning Forces for Quality? An unprecedented commitment by the Robert Wood Johnson Foundation
AF4Q and TCAB: An Introduction July 13, 2011 Ellen Interlandi, MHM, RN, NE-BC Patricia Montoya, MPA, BSN 1 What is Aligning Forces for Quality? An unprecedented commitment by the Robert Wood Johnson Foundation
Station Name: Mrs. Smith. Issue: Transitioning to comfort measures only (CMO)
") Station Name: Mrs. Smith Issue: Transitioning to comfort measures only (CMO) Presenting Situation: The physician will meet with Mrs. Smith s children to update them on her condition and determine the future
Station Name: Mrs. Smith Issue: Transitioning to comfort measures only (CMO) Presenting Situation: The physician will meet with Mrs. Smith s children to update them on her condition and determine the future
A Rapid Team Approach: Service Recovery Team (SRT)
") Complaint Management A Rapid Team Approach: Service Recovery Team (SRT) Vicki Tiller RN MSN Glenbrook Hospital NorthShore University HealthSystem We Have a Need Defining The Problem Increased number of
Complaint Management A Rapid Team Approach: Service Recovery Team (SRT) Vicki Tiller RN MSN Glenbrook Hospital NorthShore University HealthSystem We Have a Need Defining The Problem Increased number of
Quality Improvement Plan (QIP): 2015/16 Progress Report
: 2015/16 Progress Report") Quality Improvement Plan (QIP): Progress Report Medication Reconciliation for Outpatient Clinics 1 % complete medication reconciliation on outpatient clinic visit assessments ( %; Pediatric Patients; Fiscal
Quality Improvement Plan (QIP): Progress Report Medication Reconciliation for Outpatient Clinics 1 % complete medication reconciliation on outpatient clinic visit assessments ( %; Pediatric Patients; Fiscal
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
A26/B26: Goal Zero: South Carolina s Commitment to Safety
 A26/B26: Goal Zero: South Carolina s Commitment to Safety Coleen Smith, RN, MBA, CPHQ, High Reliability Initiatives Director Joint Commission Center for Transforming Healthcare Thornton Kirby, FACHE, President
A26/B26: Goal Zero: South Carolina s Commitment to Safety Coleen Smith, RN, MBA, CPHQ, High Reliability Initiatives Director Joint Commission Center for Transforming Healthcare Thornton Kirby, FACHE, President
The Physician s Perspective
 The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 HOW WE MEASURE QUALITY 16
 Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE
 CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE Joy Goebel RN MN PhD Associate Professor of Nursing California State University Long Beach Objectives Discuss similarities
CROSSING THE CHASM: ENGAGING NURSES IN QUALITY IMPROVEMENT AND EVIDENCE BASED PRACTICE Joy Goebel RN MN PhD Associate Professor of Nursing California State University Long Beach Objectives Discuss similarities
Saving Lives with Best Practices and Improvements in Sepsis Care
 Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Provincial Pediatric Early Warning System (PEWS) Clinical Decision Support Tool. Guideline Purpose. Practice Level / Competencies.
 Clinical Decision Support Tool. Guideline Purpose. Practice Level / Competencies.") Guideline Purpose To provide guidance and direction for the use of the British Columbia Pediatric Early Warning System (BC PEWS). The PEWS system supports the early recognition, mitigation, notification,
Guideline Purpose To provide guidance and direction for the use of the British Columbia Pediatric Early Warning System (BC PEWS). The PEWS system supports the early recognition, mitigation, notification,
A Comprehensive Framework for Patient Safety
 These presenters have nothing to disclose A Comprehensive Framework for Patient Safety Allan Frankel, MD and Carol Haraden, PhD 8 October 2015 A Framework for a System of Safety Objectives 1. Link safety
These presenters have nothing to disclose A Comprehensive Framework for Patient Safety Allan Frankel, MD and Carol Haraden, PhD 8 October 2015 A Framework for a System of Safety Objectives 1. Link safety
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond. Why the focus on Sepsis?
 The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
BUILDING AN EVIDENCE-BASED NURSING ENTERPRISE: CRITICAL COMPONENTS FOR SUCCESS
 BUILDING AN EVIDENCE-BASED NURSING ENTERPRISE: CRITICAL COMPONENTS FOR SUCCESS BUILDING EBP COMPETENCE AND CAPACITY BY LEVERAGING OPPORTUNITIES AND PLANNING STRATEGICALLY Lynn Gallagher-Ford, PhD, RN,
BUILDING AN EVIDENCE-BASED NURSING ENTERPRISE: CRITICAL COMPONENTS FOR SUCCESS BUILDING EBP COMPETENCE AND CAPACITY BY LEVERAGING OPPORTUNITIES AND PLANNING STRATEGICALLY Lynn Gallagher-Ford, PhD, RN,
Barriers to Early Rehabilitation in Critically Ill Patients. Shannon Goddard, MD Sunnybrook Health Sciences Centre
 Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
TRANSFORMING CARE DELIVERY
 APRIL 2015 TRANSFORMING CARE DELIVERY THE POWER OF CLINICAL VARIATION MANAGEMENT About The Chartis Group The Chartis Group is a national advisory services firm that provides strategic planning, accountable
APRIL 2015 TRANSFORMING CARE DELIVERY THE POWER OF CLINICAL VARIATION MANAGEMENT About The Chartis Group The Chartis Group is a national advisory services firm that provides strategic planning, accountable
4/4/2012. Sign Out Competence: Easier Said Than Done. Hypothesis: Introduction. Our Program
 Introduction Information sign out is essential to patient care Sign Out Competence: Easier Said Than Done Sarah A Rawstron M.B.,B.S., Sajad Khazal M.B.,Ch.B., Cynthia Katz M.D. Duty hour restrictions (more
Introduction Information sign out is essential to patient care Sign Out Competence: Easier Said Than Done Sarah A Rawstron M.B.,B.S., Sajad Khazal M.B.,Ch.B., Cynthia Katz M.D. Duty hour restrictions (more
Creating the New Care Design L2. George Kerwin, CEO Patient of Bellin Health Bellin Health Team. Objectives
 Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Creating the New Care Design L2 George Kerwin, CEO Patient of Bellin Health Bellin Health Team Objectives Identify the five views of the Production System necessary to Create a Connected Personal Experience
Together for Health A Delivery Plan for the Critically Ill
 Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
SPSP Maternity and Children
 Healthcare Improvement Scotland s Improvement Hub SPSP Maternity and Children End of phase report August 2016 Healthcare Improvement Scotland 2016 First published August 2016 The contents of this document
Healthcare Improvement Scotland s Improvement Hub SPSP Maternity and Children End of phase report August 2016 Healthcare Improvement Scotland 2016 First published August 2016 The contents of this document
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016
 Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
This is a high level overview report to update the Board on the Acute Adult Safety Programme consisting of the following sections:
 Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Running head: LEADERSHIP ANALYSIS: ROUNDING 1
 Running head: LEADERSHIP ANALYSIS: ROUNDING 1 Leadership Analysis: Rounding Jerrene Bramble, Tara Braun, Pamela Dusseau, Angelique Kinyon, William McKinley, Noranne Morin, Nicky Reed, and Ashleigh Wash
Running head: LEADERSHIP ANALYSIS: ROUNDING 1 Leadership Analysis: Rounding Jerrene Bramble, Tara Braun, Pamela Dusseau, Angelique Kinyon, William McKinley, Noranne Morin, Nicky Reed, and Ashleigh Wash
A3/B3: Improvement in the Intensive Care Unit
 A3/B3: Improvement in the Intensive Care Unit Carol Peden, MD, MPH, FRCA, FFICM, Associate Medical Director for Quality Improvement, Consultant in Anesthesia and Intensive Care Session Objectives Structure
A3/B3: Improvement in the Intensive Care Unit Carol Peden, MD, MPH, FRCA, FFICM, Associate Medical Director for Quality Improvement, Consultant in Anesthesia and Intensive Care Session Objectives Structure
Wednesday, April 22, :00 a.m. Eastern
 Wednesday, April 22, 2015 11:00 a.m. Eastern Dial In: 888.863.0985 Conference ID: 5358648 Slide 1 Speakers Karen Harris, MD, MPH, FACOG President, North Florida Women's Physicians Medical Director of Patient
Wednesday, April 22, 2015 11:00 a.m. Eastern Dial In: 888.863.0985 Conference ID: 5358648 Slide 1 Speakers Karen Harris, MD, MPH, FACOG President, North Florida Women's Physicians Medical Director of Patient
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition
 What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
What You Need to Know About Documentation for the Must Pass Elements for NCQA PCMH Recognition Presenters: Steven Bromer, MD and Denise Anderson-Carr, MPH, RD Date: May 22, 2013 Disclaimer Presentation
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
SPSP Medicines December 2016 WebEx NHS Lothian Reducing medicines harm across transitions
 SPSP Medicines December 2016 WebEx NHS Lothian Reducing medicines harm across transitions Welcome AIM: Support the learning and sharing between boards regarding medication reconciliation as a whole system
SPSP Medicines December 2016 WebEx NHS Lothian Reducing medicines harm across transitions Welcome AIM: Support the learning and sharing between boards regarding medication reconciliation as a whole system
Version 2 15/12/2013
 The METHOD study 1 15/12/2013 The Medical Emergency Team: Hospital Outcomes after a Day (METHOD) study Version 2 15/12/2013 The METHOD Study Investigators: Principal Investigator Christian P Subbe, Consultant
The METHOD study 1 15/12/2013 The Medical Emergency Team: Hospital Outcomes after a Day (METHOD) study Version 2 15/12/2013 The METHOD Study Investigators: Principal Investigator Christian P Subbe, Consultant
NHS TAYSIDE MORTALITY REVIEW PROGRAMME
 NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
PRESSURE ULCER PREVENTION
 PRESSURE ULCER PREVENTION University of South Alabama Medical Center Mobile, AL Becky Pomrenke, RN, MSN, CNL University of South Alabama Medical Center Academic, Urban Hospital Regional Level I Trauma
PRESSURE ULCER PREVENTION University of South Alabama Medical Center Mobile, AL Becky Pomrenke, RN, MSN, CNL University of South Alabama Medical Center Academic, Urban Hospital Regional Level I Trauma
Mesosystems and pathways: Idealized design
 L14 These presenters have nothing to disclose Mesosystems and pathways: Idealized design Marjorie Godfrey PhD, MS, MSN Co-Director The Dartmouth Institute Microsystem Academy Tom Downes MB BS, MRCP, MBA,
L14 These presenters have nothing to disclose Mesosystems and pathways: Idealized design Marjorie Godfrey PhD, MS, MSN Co-Director The Dartmouth Institute Microsystem Academy Tom Downes MB BS, MRCP, MBA,
Planning guidance National Breaking the Cycle Initiative April 2015
 Background Planning guidance National Breaking the Cycle Initiative April 2015 The aim of Breaking the Cycle initiatives is to rapidly improve patient flow to produce a step-change in performance, safety
Background Planning guidance National Breaking the Cycle Initiative April 2015 The aim of Breaking the Cycle initiatives is to rapidly improve patient flow to produce a step-change in performance, safety