Principles of Revenue Cycle Management and Utilization Management. For Children s Providers
|
|
|
- Ariel West
- 5 years ago
- Views:
Transcription
1 Principles of Revenue Cycle Management and Utilization Management For Children s Providers
2 Introduction & Housekeeping Housekeeping: Slides will be posted at MCTAC.org after the last of these events Questions not addressed today will be: Reviewed and incorporated into future trainings and presentations Reminder: Information and timelines are current as of the date of the presentation
3 Agenda/Objectives I. Intro - 9:30AM II. Revenue Cycle Management - 9:35-10:45AM III. Break: 15 minutes IV. Utilization Management :15PM V. Questions
")

4 Children's Transition Timeline JULY 1 ST JULY 1 ST JANUARY 1 ST SYSTEM TRANSITION READINESS Preparatory activities for children s system transition to include: Obtainment of NPI number Enrollment in NYS Medicaid Program Designation Contracting Fairs SPECIALTY BH BENEFITS TRANSITION TO MANAGED CARE Exemption from enrollment in managed care removed for children in all 1915(c) waivers Care Coordination services and staff fully transition to HH care management NEW SPA & ALIGNED HCBS SERVICES GO LIVE Six new Behavioral Health Children s Specialty Services available for children under 21 who meet medical necessity criteria Newly aligned children s HCBS services available through FFS and managed care Providers begin delivering services under new array VOLUNTARY FOSTER CARE TRANSITION & HCBS EXPANSION All children receiving foster care services will move into the managed care environment. Expansion of eligibility criteria for aligned children s HCBS to include children who meet Level of Need (LON)
5 Revenue Cycle Management
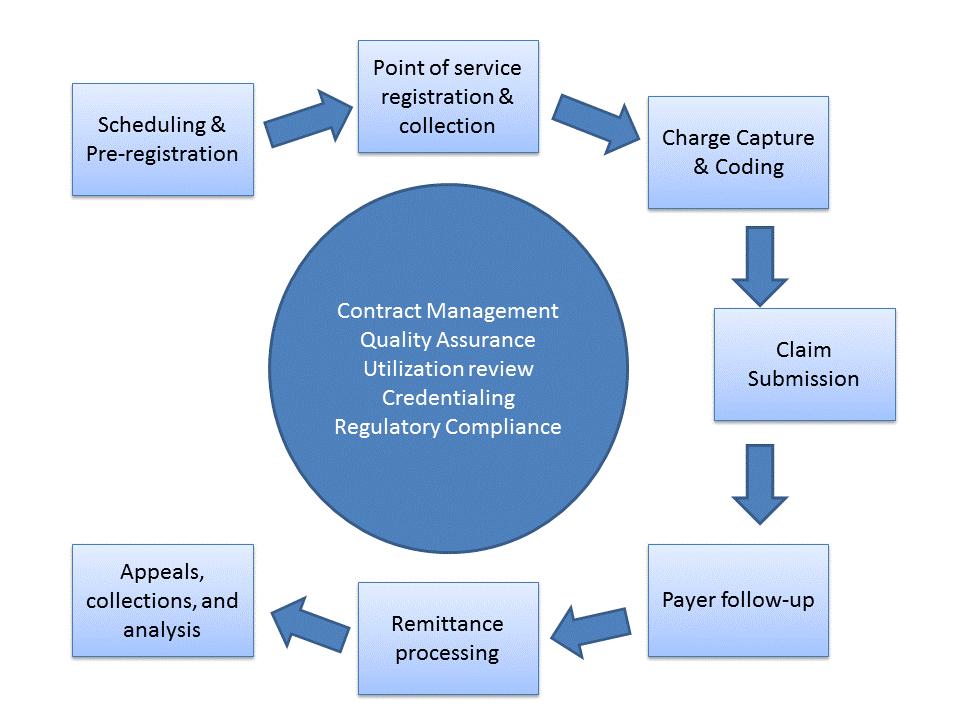
6 Revenue Cycle Defined All administrative and clinical functions that contribute to the capture, management, and collection of client service revenue. This describes the life cycle of a client account from creation to payment collection and resolution. The client account cycle is supported by a number of additional activities necessary to assure that all encounters are billable, meet regulatory requirements and revenue collection is maximized.
7 How is The Revenue Cycle Unique as an Organizational Process? Brings together workgroups and staff who do not work together in any other context Interdependencies exist across non- naturally occurring workgroups Revenue generation is the cornerstone of fiscal viability Inefficiencies, errors, and oversights can have a devastating impact Clinical priorities and fiscal/billing priorities are not always aligned
8
9 Phases of the Revenue Cycle Prior to Service Pre-registration including eligibility verification and authorization Scheduling During Services New client registration Eligibility verification Collection of fees Charge capture and coding Following Services Claims submission Payer follow-up Remittance processing and posting Ongoing Analysis Process improvement
10 Prior to Service Eligibility verification When possible insurance eligibility and benefit verification should take place before the initial visit and checked regularly after that. Staff should have a working knowledge of the most commonly seen insurance plans and coverage options Many payers have their own web portals or phone verification systems that can be used to verify eligibility Authorization Some plans may require clinical authorizations that should be identified when verifying eligibility Each payer will have a unique process for securing authorizations Most authorizations will have visit limits that will need to be tracked
11 Prior to Service (continued) Scheduling When possible scheduling should be centralized and electronic If an insurance plan requires specific staff credentials, care must be taken to schedule clients with providers that are reimbursable under the plan Efficiencies can be gained through medical model scheduling. In this model initial appointments are scheduled by front office staff, follow-up visits are set by front office staff based upon the clinicians instructions, and processes are put in place to back fill canceled visits.
12 During Service New client registration Efficiently collect information necessary to establish a new client record including basic demographics, financial information, and financial agreements. Clients need to be made aware of fee policies and any payment responsibility they may have. Important to check eligibility
13 Eligibility Verification Medicaid Fee for service and Medicaid Managed care verifications can be done by: Telephone VeriFone Vx570 epaces Batch upload (270) The most efficient means to verify Medicaid eligibility is the electronic transmission of a 270 directly from the billing component of your EMR/EHR or billing software. A 271 will be returned to your billing system which should create a variance report for reconciliation. Eligibility verification is also a service that can be provided by a billing clearinghouse.
14 Charge Capture and Coding Charge capture and coding Documenting the type and duration of the client encounter and transforming that into a data set necessary to support a clean claim. Whenever possible charge capture should be standardized. One of the approaches is to develop and implement a Chargemaster. EHR/EMR setup should make it easy to identify when a modifier should be applied to the basic charge. The proper selection of modifiers is critical to revenue maximization because in many instances they are associated with higher reimbursement rates.
15 Charge Capture and Coding (continued) If charge are not captured through the EHR/EMR then: Staff should be provided with a Chargemaster that they can use to cross walk from the service they provided to the proper billing code. An efficient process must be in place to record, verify, and accurately report services provided to be entered into the billing program. Care must be taken to assure that minimum duration standards are met and that the CPT code for the transaction matches the start and end time on the clinical documentation.
16 Improper or Inaccurate Coding Improper or inaccurate coding carries a significant risk of disallowance upon subsequent audit Strong quality assurance programs must be in place to assure codes are correct and supported by the clinical documentation. It is essential that staff understand the billing rules that guide their practice and documentation
17 After Services Claim submission Submission of billable fees to the insurance company via the required universal claim form. o Claim data can be submitted directly to the payer or through a clearinghouse o Processes must be in place to scrub claims to assure that they are clean. o Some common tests should be: Was the claim formatted correctly and are all required data elements present Was the service of the required duration for the code Was the documentation completed properly: Progress note was completed Service was on the treatment plan Treatment plan was up to date o Claims should be submitted as soon as feasible
18 Improper Claiming Improper claiming can be very costly Each claim that is rejected due to improper formatting must be touched and resubmitted Claims that are submitted without adherence to documentation regulations create a huge risk for disallowance upon audit Clearinghouses can do a good job at scrubbing claims with technical errors but only an EMR with a billing component can evaluate claims for compliance with documentation requirements. An EMR can suspend claims and alert staff to errors that renders the claim unbillable and support quality improvement efforts and regulatory compliance. If there is no EMR scrubbing of claims it is essential that there is an active Quality Assurance process that identifies improper claims and voids them when necessary.
19 Denials Review each denied claim and determine the cause Some common denials are: Claim was submitted after the allowable time period Visit was not authorized Client was not eligible Provider was not credentialed Claim had incorrect client or provider data Provider technical error Payer technical error Adjudicate claims, correct errors and resubmit promptly Identify preventable denials and apply a quality improvement process to correct
20 Not Just Denials Not Billed Due to EHR/EMR billing rules, claims might be held back. These are not denials Clearinghouse can also hold claims back due to their rules Rejection Due to numerous errors, claims might not be processed (never get to the payer) at all and fall into rejection category, for example, wrong ID or Name on the claim. Pending Sometimes the payer, including Medicaid, will Pend the claim due to missing information or further reviews internally
21 Remittance Process and Posting Posting and applying payments and adjustments to client accounts and posting payments in aggregate amounts to the General Ledger o Post payments in a timely fashion o Compare payments received to amounts billed and reconcile differences o Review adjustments made by the payer to individual claim. Appeal adjustments when warranted
22 Ongoing Analysis Review and evaluate the effectiveness of your revenue cycle management and the performance of your payers. o Create an analysis standard metrics to identify issues and processes that may need improvement o Quantify issues related to payers and discuss with your customer service representatives o Some standard metrics Collection ratio: a total collected to total billed reviewed by payer and payer class
23 Ongoing (continued) Aged accounts receivable: Dollar value of accounts receivables tracked by amount of time they have been outstanding: Less than 30 days days days days Denial report percentage and amount of claims denied by reason, clinician, and payer Percentage of claims paid upon initial submission Process improvement Formalized process using your analytics to identify problems, create solutions, implement change, and measure the results.
24 How Might You Address the Operational Challenges? Clearly articulate measurable performance standards for all staff with involvement in the revenue cycle process Measure against these standards regularly and differentiate people problems from system problems Address people problems quickly and effectively
25 How Might You Address The Operational Challenges? Provide staff with the tools and information they need to successfully carry out their tasks Implement a quality improvement process to address system problems. Assure that Executive, Clinical, and Finance leadership are on the same page and speak with a single voice regarding revenue and the critical role it plays in supporting the mission of the organization
26 Tools to Support Revenue Cycle Management A full featured properly implemented EHR/EMR with a strong billing component can bring significant efficiencies and accuracy to the revenue cycle process: Provide electronic scheduling to maximize the use of clinical capacity Efficiently evaluate insurance eligibility Track authorizations and alert staff when they are approaching thresholds Behind the scenes management of charge capture and coding to eliminate errors, maximize revenue and minimize audit risk Catch and suspend claims that do not meet payer and documentation requirements minimizing audit risk Efficiently post payments to maintain accurate client accounts Provide reports necessary to address staff, system, and payer performance issues
27 Tools to support RCM (continued) Short of a fully functional EMR/EHR a strong Revenue Cycle Management system, here are some essentials: Outsourcing billing services is an option In house stand alone billing systems are available A combination of in house billing systems (either EMR/EHR or stand alone based) and a clearinghouse claims processer is a popular option.
28 MCO Tips for successful RCM Develop a good relationship with your clearinghouse vendor Review HIPAA requirements for electronic claim submissions Review and respond to clearinghouse reports (i.e. acceptance and denials) Promptly make corrections and submit the claim(s) to clearinghouse Review and respond to payer provider remittance advices to allow time to make corrections and appeals Remember timely filing deadlines Review and update your 837i or UB-04 claim form and make adjustments to ensure correct information is in each field to avoid delay/denial of payment with managed care payers Be mindful that claims forms often have pre-populated fields which worked for FFS but won t work with MCO s Sign up for Electronic Payments and Statements with each payer Know about the unlicensed practitioner number for OMH and OASAS
29 Lessons Learned Clearinghouse Plan Providers Providers should contact the Electronic Data Interchange (EDI) to assist in the remediation of rejected claims. Know the capabilities of the Electronic Health Record as it relates to receiving payments from multiple payers.


30 Remember CLAIMS TESTING CLAIMS TESTING CLAIMS TESTING

31 Break 15 mins
32 Utilization Management Overview What is UM and Why Is It Important?
33 What is Utilization Management?
34 What is Utilization Management? A set of techniques used by Managed Care Organizations to manage health care costs by determining the appropriateness of care (level of care, intensity, duration) of services covered under an enrollee s plan Primary purpose is to ensure that services are medically necessary and cost-effective Maintains fidelity and integrity of service provisions

35 What s The Difference? Utilization Management Function performed by MCO as a payer VS. Utilization Review Regulatory requirement performed by provider that stipulates periodic re-examination of open cases
36 Why do MCOs Conduct Utilization Management? Role An integrated system that manages health services for an enrolled population. Puts processes in place to assist in determining whether identified services are medically necessary based on specific criteria. Function Ensure individual receives the least restrictive care Confirm services provided are medically necessary Certify treatment is appropriate to diagnosis, member needs, and member wishes. Make certain payment rendered is for only those services that are medically necessary. Review for the appropriate length of care.
37 What does Medical Necessity Mean? Is defined as accepted health care services and supplies provided by health care entities, appropriate to the evaluation and treatment of a disease, condition, illness or injury and consistent with the applicable standard of care. Appropriate services and supplies are those that are neither more nor less than what the individual requires at a specific point in time. Medical necessity is the standard terminology that all health care professionals and entities will use in the review process when determining if medical care is appropriate and essential.
38 Medical Necessity Principles Consistent Management of: Clinical effectiveness - Treatment of illness, injury, disease or symptom must be proven to be clinically effective. Appropriateness - Type, frequency, extent and duration of services must be appropriate for the individual enrollee. Cost effectiveness - Services must not be more costly than alternative services that are just as likely to produce equivalent therapeutic and diagnostic results. Cost Effectiveness Clinical Effectiveness Appropriateness All Components are needed for authorization
39 What does Medical Necessity Mean? New York State Department of Health requires the following definition of Medically Necessary: Medically necessary means health care and services that are necessary to prevent, diagnose, manage or treat conditions in the person that cause acute suffering, endanger life, result in illness or infirmity, interfere with such person s capacity for normal activity, or threaten some significant handicap. (N.Y. Soc. Serv. Law, 365-a).
40 Types of Reviews? UM will occur at different points in the healthcare delivery cycle: Prior authorization: provider must request permission from the MCO before delivering a service in order to receive payment Concurrent review: occurs during an ongoing course of treatment (such as inpatient hospital admission) to ensure that such treatment remains appropriate Discharge Review: For inpatient, this review occurs prior to discharge to assure that plans are in place for a safe and supported re-entry into the community Retrospective review: review that takes place, on an individual or aggregate basis, after the service is provided
41 Utilization Management Process 1) Prior to calling the MCO Review Level of Care (LOC) criteria for the service being requested/discussed Review the specific information regarding the individual (presenting problem, current symptoms, medications, recent treatment) and formulate a rationale for the requested service(s) and anticipated service units 2) Contact the MCO representative Provide patient name, Date of Birth (DOB), Medicaid number (CIN) and your name, facility name and contact number Identify the start date for treatment being requested Request the services and number of service units (days, visits, etc.) necessary to deliver these services Present rationale for request
42 Utilization Management Process 3) Discuss planned treatment changes (if any) and anticipated service units. 4) Always include overview of the long term treatment/support plan (including discharge planning steps if the individual is in an inpatient setting) Communication with treatment providers (new, existing) Family meetings Medications (new, existing, changes) Patient involvement (family driven, youth guided, person centered approach) If inpatient, discharge plans: to home, transfer to another facility, etc..
43 Utilization Management Process 5) Obtain decision from MCO, document and schedule next review if necessary If adverse decision: request rationale request alternative services consider MD to MD review appeal
44 When Parties Disagree? Dealing with Denials: Appeal and Grievance Process 1) What if your organization cannot support the decision of the MCO? Conflict Resolution (both external and internal) Are there liability issues in not providing a service, even if the MCO denies payment? 2) If the respective clinicians do not agree on a plan of action, the next step is to formally submit an expedited appeal. Mandated timeframes guide this process for both the facility making the appeal as well as the MCO and must be adhered to. 3) The next steps in the appeal process is the Standard Appeal or External Appeal.
45 When Parties Disagree? Dealing with Denials: Appeal and Grievance Process Each Managed Care Organization may have specific guidelines for initiating any of these options. They will all be similar but it is important for you to become familiar with the process for each MCO you work with. Medicaid Managed Care Provider Guide index.aspx Note: More on Appeal and Grievance in January

46 A reminder: The Member Bill of Rights...




47 Utilization Management and Payment for Services In a nutshell The Member is not liable for payment of these services NO PAYMENT If it is not authorized it will not be paid for The facility will not be reimbursed

48 Role of Agency in UM Process Secure the optimal care for your clients
49 Utilization Management Expectations Medicaid Managed Care Transformation
50 NYS State UM Expectations The State has provided guidelines for Utilization Management practices for the Behavioral Health Benefit Administration of the Medicaid Managed Care Program. Plans will use Medical Necessity Criteria (MNC) to determine appropriateness of new and ongoing services for Specialty BH services. Family Driven, Youth Guided, and Person Centered approaches will be the expectation when providing services.
51 NYS State UM Expectations The Plan s UM system shall follow national and state standards and guidelines, promote quality of care, and adhere to standards of care, including protocols that address the following: Review of clinical assessment information, treatment planning, concurrent review, and treatment progress Promotion of recovery principles Promotion of relapse/crisis prevention planning
52 Medicaid Managed Care Organization Children s System Transformation Requirements and Standards Final published July 2017 See section 3.8 on Utilization Management, pp n/behavioral_health/children/docs/ _mc_plan_rqmts.pdf
53 More about the OASAS LOCADTR
54 LOCADTR: Background Transition to Managed Care Carve In Want to ensure access to care Need tool for provider-patient-plan communication Tool aligned with NY treatment system Goals Reliable/valid/credible Include collective understanding of level determination Placement in least restrictive yet appropriate setting Simplified and expedient administration
55 LOCADTR Reflects OASAS clinical judgment about the appropriate level of care Based on ASAM Tailored to NY: Policy to increase MAT for opioids Residential redesign Required for MMC services OASAS would like to extend beyond Medicaid Training Needs: Diverse workforce: Designed for someone with SUD clinical background Eventually will be used by other providers Working with managed care to develop workflow
56 LOC Principles Treatment should occur in the least restrictive setting that is likely to be successful. Resources may be added to increase the likelihood that the client can succeed in a lower level of care including care coordination through a health home, peer or other support services. Failure at an outpatient level of care, by itself, should not necessarily lead to a higher level of care. Access to a higher level of care that is needed should not be denied because the client has not failed at a lower level of care.
57 What We Want in a Tool Speed- Able to be completed in minutes Relevance- Includes Levels of Care known and understood in New York Reliability- Predictability and accurately recommends the best level of care Credibility- Plans and providers accept the tool and agree that there is evidence to support the tool, face validity and empirical support Clinical Support- Provides information to clinicians to support level of care decisions to payers and auditors
58 LOCADTR: Online Tool Health Commerce System: The LOCADTR is a web-based application Currently found on the Department of Health-Health Commerce System (HCS) Users need to have a health commerce account with a user name and password Online tool offers an opportunity for streamlined conversations with Plans: Plans will have access to LOCADTR Ability to speak the same language to help with conversations with managed care plans

59 LOCADTR Assessment Layers

60 LOCADTR Schematic
61 Strategies for Maximizing Utilization Management Outcomes What Can Providers Do Today To Prepare For UM?
62 Top 10 things to consider 1. Understand medical necessity criteria per service 2. Documentation integrity (i.e., dx and tx must match) 3. Examine level of intensity per service, identify outliers 4. Reference EBTs/Best Practices 5. Be able to provide a concise clinical presentation demonstrating how level requested is needed and will be used.
63 Top 10 things to consider 6. Proactively staff cases of concern/high risk and have practical, individualized crisis plans that are up to date 7. Participate in any MCO workgroups 8. Have fully functional IT systems for reports and tracking 9. Be prepared for appeals, & know how to staff a case 10. Bump up any concerns!
64 UM Strategies: Prepare Your Agency Staff Understand any requirements or qualifications for staff delivering the services and address any gaps in staff preparedness For example: Family and Youth Peer Support Services Review and fully understand Level of Care admission, continuing stay and discharge criteria Understand MCO expectations for the review process Understand and embrace the MCO language tied to UM Practice reviews with Case Studies to gain comfort with the process
65 UM Strategies: Effective Agency Practices Develop internal workflows with responsibilities clearly designated for staff members Develop population level reporting strategies to identify outliers by program by staff and client level Routinely monitor the quality of the service being provided and look for improvement opportunities. Seek feedback (degree of satisfaction) from those individuals receiving the services
66 UM Strategies: Effective Staffing for UM The Agency s Utilization Management staff member: Is a member of the treatment team and a part of the conversation Effectively communicates MCO concerns to the team Understands MCO terminology, treatment volume caps and effectively communicates with the MCO. Understands the treatment being provided and is not just extracting information from a client note or record Is familiar with all covered services under the Plan: OMH/OASAS Inpatient, Outpatient, clinic, PROS, HCBS, etc.. Well informed of treatment modalities being utilized including medications Tracks the success of the individual in the service being provided and can articulate the success to the MCO Able to articulate the long term services plan developed to move the individual towards recovery and how the current service supports the long term plan.
67 MCO Tips for Successful UM Make sure front line staff making the calls and submitting the documentation are as aware of regulations as supervisors Remember that the member ID card may not broadcast that the member is on Medicaid; Providers should attend MCO orientations to become more familiar with each Plan s Medicaid name, logo or other identifying feature and know how to contact that specific MCO for member authentication and/or service authorization Identify yourself as a Provider, in any communication with MCO: Caller/Sender name Name of treating Provider/Facility Provider Tax ID # Address Expedite a member authentication with this 2-point PHI validation process: Option 1: Option 2: o Subscriber/Medicaid ID #; AND ONE of the following: o Member s full DOB (month/day/year); AND ONE of the following: o Member s full DOB (month/day/year) o Subscriber/Medicaid or Member ID o SSN (last 4 digits suffice) o SSN (last 4 digits suffice) o Address; or o Address; or o Full phone # o Full phone #
68 Future Trainings SPA and HCBS Rates and Codes SPA and HCBS In-Depth Service Specific Implementation Support Billing Rules and Manual Utilization Management, Medical Necessity, Prior Authorization/Concurrent Review Criteria for Specialty Children s Services Want additional training? MCTAC+ focuses on providing individualized and hands-on training and technical assistance to BH providers throughout NYS on the successful transition to Medicaid Managed Care. This includes topics such as the Children s System Transformation.

 designed to facilitate and improve use of evidence based")
69 Tools Managed Care Plan Matrix comprehensive resource for MCO contact information relevant to adults and children Billing Tool Children System specific updates coming soon! Output to Outcomes Database access to standardized outcome measurement tools and metrics (database) designed to facilitate and improve use of evidence based practices.

70 Questions and Discussion Please send questions to: Logistical questions usually receive a response in 1 business day or less. Longer & more complicated questions can take longer. We appreciate your interest and patience! Visit to view past trainings, sign-up for updates and event announcements, and access resources
Medicaid Managed Care Utilization Management and Integrated Billing Overview
 Medicaid Managed Care Utilization Management and Integrated Billing Overview March, 23 2016 The Managed Care Technical Assistance Center of New York 1 st webinar in series about UM and Billing. In- person
Medicaid Managed Care Utilization Management and Integrated Billing Overview March, 23 2016 The Managed Care Technical Assistance Center of New York 1 st webinar in series about UM and Billing. In- person
David W. Eckert, LMHC, NCC, CRC Senior Consultant at CCSI s Center for Collaboration in Community Health
 David W. Eckert, LMHC, NCC, CRC Senior Consultant at CCSI s Center for Collaboration in Community Health The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation,
David W. Eckert, LMHC, NCC, CRC Senior Consultant at CCSI s Center for Collaboration in Community Health The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation,
Adult BH Home & Community Based Services (HCBS) Foundations Webinar JUNE 29, 2016
 Foundations Webinar JUNE 29, 2016") Adult BH Home & Community Based Services (HCBS) Foundations Webinar JUNE 29, 2016 June 30, 2016 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Adult BH Home & Community Based Services (HCBS) Foundations Webinar JUNE 29, 2016 June 30, 2016 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Implementing Medicaid Behavioral Health Reform in New York
 Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York Conference of Local Mental Hygiene Directors November 19, 2013 Agenda Goals Timeline BH Benefit Design Overview
Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York Conference of Local Mental Hygiene Directors November 19, 2013 Agenda Goals Timeline BH Benefit Design Overview
Implementing Medicaid Behavioral Health Reform in New York
 Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York HIV Health and Human Services Planning Council of New York March 19, 2014 Agenda Goals Timeline BH Benefit
Redesign Medicaid in New York State Implementing Medicaid Behavioral Health Reform in New York HIV Health and Human Services Planning Council of New York March 19, 2014 Agenda Goals Timeline BH Benefit
Children's System MCO Contracting Fair. November 6, 2017
 Children's System MCO Contracting Fair November 6, 2017 2 Guiding Principles Behind Children s Health and Behavioral Health MC Transition Key components of the managed care transition is to: Early identification
Children's System MCO Contracting Fair November 6, 2017 2 Guiding Principles Behind Children s Health and Behavioral Health MC Transition Key components of the managed care transition is to: Early identification
GUIDE TO BILLING HEALTH HOME CLAIMS
 GUIDE TO BILLING HEALTH HOME CLAIMS 1 GUIDE TO BILLING HEALTH HOME CLAIMS DEFINITIONS...1 BILLING TIPS...2 EDI TRANSACTIONS GUIDE...5 ATTACHMENT A SERVICE GRID...6 ATTACHMENT B FEE SCHEDULE...8 EXHIBIT
GUIDE TO BILLING HEALTH HOME CLAIMS 1 GUIDE TO BILLING HEALTH HOME CLAIMS DEFINITIONS...1 BILLING TIPS...2 EDI TRANSACTIONS GUIDE...5 ATTACHMENT A SERVICE GRID...6 ATTACHMENT B FEE SCHEDULE...8 EXHIBIT
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives
 Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
Draft Children s Managed Care Transition MCO Requirements
 Draft Children s Managed Care Transition MCO Requirements OVERVIEW On February 1 st, New York State released for stakeholder feedback a draft version of the Medicaid Managed Care Organization (MCO) Children
Draft Children s Managed Care Transition MCO Requirements OVERVIEW On February 1 st, New York State released for stakeholder feedback a draft version of the Medicaid Managed Care Organization (MCO) Children
Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) Care Healthcare and VNSNY CHOICE Transition
 Claim Submission Instructions (MLTC) Care Healthcare and VNSNY CHOICE Transition") 2018 Provider Manual VNSNY CHOICE Appendix V Claims CMS-1500 Form (Sample) UB-04 Form (Sample) Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) ICD-10 FAQ Care Healthcare
2018 Provider Manual VNSNY CHOICE Appendix V Claims CMS-1500 Form (Sample) UB-04 Form (Sample) Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) ICD-10 FAQ Care Healthcare
October 5 th & 6th, The Managed Care Technical Assistance Center of New York
 October 5 th & 6th, 2015 The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that offers resources to all mental health
October 5 th & 6th, 2015 The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that offers resources to all mental health
A McKesson Perspective: ICD-10-CM/PCS
 A McKesson Perspective: ICD-10-CM/PCS Its Far-Reaching Effect on the Healthcare Industry Executive Overview While many healthcare organizations are focused on qualifying for American Recovery & Reinvestment
A McKesson Perspective: ICD-10-CM/PCS Its Far-Reaching Effect on the Healthcare Industry Executive Overview While many healthcare organizations are focused on qualifying for American Recovery & Reinvestment
UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS
 UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS November 18, 2013 NYS OMH Behavioral Health Transition 2 Key MRT initiative to move fee-for-service populations and services into managed
UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS November 18, 2013 NYS OMH Behavioral Health Transition 2 Key MRT initiative to move fee-for-service populations and services into managed
Joining Passport Health Plan. Welcome IMPACT Plus Providers
 Joining Passport Health Plan Welcome IMPACT Plus Providers Agenda Passport Behavioral Health Services Overview Steps to Joining Passport Health Plan s Network Getting a Medicaid Number Enrolling in the
Joining Passport Health Plan Welcome IMPACT Plus Providers Agenda Passport Behavioral Health Services Overview Steps to Joining Passport Health Plan s Network Getting a Medicaid Number Enrolling in the
4/7/2016. Provider Leadership Update. Reminder: Information and timelines are current as of the date of the presentation
 Provider Leadership Update The Managed Care Technical Assistance Center of New York Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will be: reviewed and incorporated into future
Provider Leadership Update The Managed Care Technical Assistance Center of New York Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will be: reviewed and incorporated into future
Children s Medicaid System Transformation: HCBS Rates & SPA Rate Code Review. December 21, 2017
 Children s Medicaid System Transformation: HCBS Rates & SPA Rate Code Review December 21, 2017 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
Children s Medicaid System Transformation: HCBS Rates & SPA Rate Code Review December 21, 2017 Introduction & Housekeeping Housekeeping: Slides are posted at MCTAC.org Questions not addressed today will
HMSA Physical and Occupational Therapy Utilization Management Guide
 HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
Residential Rehabilitation Services (RRS) Level 3.1 Frequently Asked Questions (Updated 4/5/2018)
 Level 3.1 Frequently Asked Questions (Updated 4/5/2018)") Contracting Residential Rehabilitation Services (RRS) Level 3.1 Frequently Asked Questions (Updated 4/5/2018) Q: I haven t heard from the MBHP contracting department. What should I do? A: Applications
Contracting Residential Rehabilitation Services (RRS) Level 3.1 Frequently Asked Questions (Updated 4/5/2018) Q: I haven t heard from the MBHP contracting department. What should I do? A: Applications
Behavioral Health Provider Training: Program Overview & Helpful Information
 Behavioral Health Provider Training: Program Overview & Helpful Information Overview The Passport Behavioral Health Program provides members with access to a full continuum of recovery and resiliency focused
Behavioral Health Provider Training: Program Overview & Helpful Information Overview The Passport Behavioral Health Program provides members with access to a full continuum of recovery and resiliency focused
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction
 Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
Residential Re-Design Readiness Guide
 Residential Re-Design Readiness Guide Developed by the OASAS Residential Redesign Workgroup to assist programs in their discussions as they evaluate strategies towards implementation of the element(s)
Residential Re-Design Readiness Guide Developed by the OASAS Residential Redesign Workgroup to assist programs in their discussions as they evaluate strategies towards implementation of the element(s)
Chapter 2 Provider Responsibilities Unit 6: Behavioral Health Care Specialists
 Chapter 2 Provider Responsibilities Unit 6: Health Care Specialists In This Unit Unit 6: Health Care Specialists General Information 2 Highmark s Health Programs 4 Accessibility Standards For Health Providers
Chapter 2 Provider Responsibilities Unit 6: Health Care Specialists In This Unit Unit 6: Health Care Specialists General Information 2 Highmark s Health Programs 4 Accessibility Standards For Health Providers
HMSA Physical and Occupational Therapy Utilization Management Authorization Guide
 HMSA Physical and Occupational Therapy Utilization Management Authorization Guide Published Landmark's provider materials are available online at www.landmarkhealthcare.com. The online Physical and Occupational
HMSA Physical and Occupational Therapy Utilization Management Authorization Guide Published Landmark's provider materials are available online at www.landmarkhealthcare.com. The online Physical and Occupational
New York s 1115 Waiver Programs Downstate Public Comment and PAOP Working Session. Comments of Christy Parque, MSW.
 New York s 1115 Waiver Programs Downstate Public Comment and PAOP Working Session Comments of Christy Parque, MSW President and CEO November 29, 2017 The Coalition for Behavioral Health, Inc. (The Coalition)
New York s 1115 Waiver Programs Downstate Public Comment and PAOP Working Session Comments of Christy Parque, MSW President and CEO November 29, 2017 The Coalition for Behavioral Health, Inc. (The Coalition)
Provider Frequently Asked Questions
 Provider Frequently Asked Questions Strengthening Clinical Processes Training CASE MANAGEMENT: Q1: Does Optum allow Case Managers to bill for services provided when the Member is not present? A1: Optum
Provider Frequently Asked Questions Strengthening Clinical Processes Training CASE MANAGEMENT: Q1: Does Optum allow Case Managers to bill for services provided when the Member is not present? A1: Optum
Blue Care Network Physical & Occupational Therapy Utilization Management Guide
 Blue Care Network Physical & Occupational Therapy Utilization Management Guide (Also applies to physical medicine services by chiropractors) January 2016 Table of Contents Program Overview... 1 Physical
Blue Care Network Physical & Occupational Therapy Utilization Management Guide (Also applies to physical medicine services by chiropractors) January 2016 Table of Contents Program Overview... 1 Physical
Behavioral Health Provider Training: BHSO updates
 Behavioral Health Provider Training: BHSO updates Agenda Diagnosis Code 799 Laboratory Work CPT Code Q3014- Telehealth BHSO Claims submission Process Targeted Case Management Diagnosis Codes Diagnosis
Behavioral Health Provider Training: BHSO updates Agenda Diagnosis Code 799 Laboratory Work CPT Code Q3014- Telehealth BHSO Claims submission Process Targeted Case Management Diagnosis Codes Diagnosis
Hospital-Based Ambulatory Care
 C H A P T E R 2 Hospital-Based Ambulatory Care ANSWERS TO KNOWLEDGE-BASED QUESTIONS 1. What has been the trend in the utilization of hospital-based services? What factors help to account for this trend?
C H A P T E R 2 Hospital-Based Ambulatory Care ANSWERS TO KNOWLEDGE-BASED QUESTIONS 1. What has been the trend in the utilization of hospital-based services? What factors help to account for this trend?
Inland Empire Health Plan Quality Management Program Description Date: April, 2017
 Inland Empire Health Plan Quality Management Program Description Date: April, 2017 Page 1 of 35 Table of Contents Introduction.....3 Mission and Vision........3 Section 1: QM Program Overview........4
Inland Empire Health Plan Quality Management Program Description Date: April, 2017 Page 1 of 35 Table of Contents Introduction.....3 Mission and Vision........3 Section 1: QM Program Overview........4
Behavioral Health Provider Training: Program Overview & Helpful Information
 Behavioral Health Provider Training: Program Overview & Helpful Information Overview The Passport Behavioral Health Program provides members with access to a full continuum of recovery and resiliency focused
Behavioral Health Provider Training: Program Overview & Helpful Information Overview The Passport Behavioral Health Program provides members with access to a full continuum of recovery and resiliency focused
Boosting Your Bottom Line
 Boosting Your Bottom Line Making More Money for Clinics Lisa Clark, MBA NYS Office of Mental Health 7/26/16 Partners in CTAC and MCTAC include: Agenda Introduction Review of Revenue Maximization Basics
Boosting Your Bottom Line Making More Money for Clinics Lisa Clark, MBA NYS Office of Mental Health 7/26/16 Partners in CTAC and MCTAC include: Agenda Introduction Review of Revenue Maximization Basics
Long Term Care (LTC) Claims Forwarding Webinar for Nursing Facility Users Frequently Asked Questions (FAQ)
 Claims Forwarding Webinar for Nursing Facility Users Frequently Asked Questions (FAQ)") Long Term Care (LTC) Claims Forwarding Webinar for Nursing Facility Users Frequently Asked Questions (FAQ) 1. What assistance is available if providers have additional questions regarding claims billing
Long Term Care (LTC) Claims Forwarding Webinar for Nursing Facility Users Frequently Asked Questions (FAQ) 1. What assistance is available if providers have additional questions regarding claims billing
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL
 TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
TELECOMMUNICATION SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 TELECOMMUNICATION SERVICES Table of Contents 38.1 Enrollment......................................................................
NEW YORK STATE CHILDREN S HEALTH AND BEHAVIORAL HEALTH (BH) SERVICES CHILDREN S MEDICAID SYSTEM TRANSFORMATION BILLING AND CODING MANUAL
 SERVICES CHILDREN S MEDICAID SYSTEM TRANSFORMATION BILLING AND CODING MANUAL") NEW YORK STATE CHILDREN S HEALTH AND BEHAVIORAL HEALTH (BH) SERVICES CHILDREN S MEDICAID SYSTEM TRANSFORMATION BILLING AND CODING MANUAL 1 Table of Contents General... 5 Purpose of this Manual... 5 New
NEW YORK STATE CHILDREN S HEALTH AND BEHAVIORAL HEALTH (BH) SERVICES CHILDREN S MEDICAID SYSTEM TRANSFORMATION BILLING AND CODING MANUAL 1 Table of Contents General... 5 Purpose of this Manual... 5 New
HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012
 HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
October 5 th & 6th, The Managed Care Technical Assistance Center of New York
 October 5 th & 6th, 2015 The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that offers resources to all mental health
October 5 th & 6th, 2015 The Managed Care Technical Assistance Center of New York What is MCTAC? MCTAC is a training, consultation, and educational resource center that offers resources to all mental health
ValueOptions Presents: An Administrative Orientation for VNSNY CHOICE SelectHealth Providers
 ValueOptions Presents: An Administrative Orientation for VNSNY CHOICE SelectHealth Providers 2013 1 Objectives Welcome and Introductions Overview of ValueOptions Overview of VNSNY CHOICE SelectHealth &
ValueOptions Presents: An Administrative Orientation for VNSNY CHOICE SelectHealth Providers 2013 1 Objectives Welcome and Introductions Overview of ValueOptions Overview of VNSNY CHOICE SelectHealth &
KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance. UM Retrospective Review Services.
 KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance UM Retrospective Review Services Provider Manual August 2017 This page intentionally blank Table of Contents KDHE-DHCF:
KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance UM Retrospective Review Services Provider Manual August 2017 This page intentionally blank Table of Contents KDHE-DHCF:
Utilization Management Program California Edition
 Utilization Management Program California Edition 2018 ACN Group of California, Inc. Originator Chantal Russel, D.C. Effective Date March 2018 Department Utilization Management Revision Date March 2018
Utilization Management Program California Edition 2018 ACN Group of California, Inc. Originator Chantal Russel, D.C. Effective Date March 2018 Department Utilization Management Revision Date March 2018
Connecticut Medical Assistance Program Refresher for Hospice Providers. Presented by The Department of Social Services & HP for Billing Providers
 Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Hospice Agenda Overview Forms Fee Schedule/Reimbursement
Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Hospice Agenda Overview Forms Fee Schedule/Reimbursement
Our general comments are listed below, and discussed in greater depth in the appropriate Sections of the RFP.
 Deborah Cave, Executive Director Colorado Coalition of Adoptive Families (COCAF) Comments on Accountable Care Collaborative (ACC) Phase II DRAFT RFP Submitted January 13, 2017 (In Format Requested by HCPF)
Deborah Cave, Executive Director Colorado Coalition of Adoptive Families (COCAF) Comments on Accountable Care Collaborative (ACC) Phase II DRAFT RFP Submitted January 13, 2017 (In Format Requested by HCPF)
State of Montana. Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES
 State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT January 31, 2013 Children s Mental Health
State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT January 31, 2013 Children s Mental Health
Navigating New York State s Transition to Managed Care
 Navigating New York State s Transition to Managed Care December 3, 2014 Mary McKernan McKay, Ph.D Andrew F. Cleek, Psy.D. Meaghan E. Baier, LMSW Agenda Introduction of the Managed Care Technical Assistance
Navigating New York State s Transition to Managed Care December 3, 2014 Mary McKernan McKay, Ph.D Andrew F. Cleek, Psy.D. Meaghan E. Baier, LMSW Agenda Introduction of the Managed Care Technical Assistance
LifeWise Reference Manual LifeWise Health Plan of Oregon
 11 UB-04 Billing Description This chapter contains participation, claims and billing information for providers who bill on a UB-04 (CMS 1450) claim form. This chapter supplements information contained
11 UB-04 Billing Description This chapter contains participation, claims and billing information for providers who bill on a UB-04 (CMS 1450) claim form. This chapter supplements information contained
Implementation Issues of the Physician Practice. for ICD-10-CM
 Implementation Issues of the Physician Practice for ICD-10-CM What are ICD-10-CM and the Version 5010? The Centers for Medicare & Medicaid Services (CMS) is driving the industry to upgrade core HIPAA transactions
Implementation Issues of the Physician Practice for ICD-10-CM What are ICD-10-CM and the Version 5010? The Centers for Medicare & Medicaid Services (CMS) is driving the industry to upgrade core HIPAA transactions
Medicaid Managed Care Readiness For Agency Staff --
 Medicaid Managed Care Readiness 101 -- For Agency Staff -- To Understand: Learning Objectives Basic principles of Managed Care as a payment vehicle for health care services The structure of the current
Medicaid Managed Care Readiness 101 -- For Agency Staff -- To Understand: Learning Objectives Basic principles of Managed Care as a payment vehicle for health care services The structure of the current
Alternative Managed Care Reimbursement Models
 Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Medicaid and CHIP Managed Care Final Rule MLTSS
 Medicaid and CHIP Managed Care Final Rule MLTSS John Giles, Technical Director Division of Quality and Health Outcomes Children and Adult Health Programs Group Debbie Anderson, Deputy Director Division
Medicaid and CHIP Managed Care Final Rule MLTSS John Giles, Technical Director Division of Quality and Health Outcomes Children and Adult Health Programs Group Debbie Anderson, Deputy Director Division
TRANSITION OF NURSING HOME POPULATIONS AND BENEFITS TO MEDICAID MANAGED CARE
 ANDREW M. CUOMO Governor HOWARD A. ZUCKER, M.D., J.D. Acting Commissioner SALLY DRESLIN, M.S., R.N. Executive Deputy Commissioner TRANSITION OF NURSING HOME POPULATIONS AND BENEFITS TO MEDICAID MANAGED
ANDREW M. CUOMO Governor HOWARD A. ZUCKER, M.D., J.D. Acting Commissioner SALLY DRESLIN, M.S., R.N. Executive Deputy Commissioner TRANSITION OF NURSING HOME POPULATIONS AND BENEFITS TO MEDICAID MANAGED
UNIVERSITY OF CALIFORNIA, SAN FRANCISCO AUDIT SERVICES. UCSF Medical Center Hospital Charge Capture - Emergency Services Project #
 , SAN FRANCISCO AUDIT SERVICES UCSF Medical Center Hospital Charge Capture - Emergency Services Project #13-024 June 2013 Performed by: Sugako Amasaki, Principal Auditor Julia Travous, Manager (Protiviti)
, SAN FRANCISCO AUDIT SERVICES UCSF Medical Center Hospital Charge Capture - Emergency Services Project #13-024 June 2013 Performed by: Sugako Amasaki, Principal Auditor Julia Travous, Manager (Protiviti)
Section VII Provider Dispute/Appeal Procedures; Member Complaints, Grievances, and Fair Hearings
 Section VII Provider Dispute/Appeal Procedures; Member Complaints, Grievances, and Fair Hearings Provider Dispute/Appeal Procedures; Member Complaints, Grievances and Fair Hearings 138 Provider Dispute/Appeal
Section VII Provider Dispute/Appeal Procedures; Member Complaints, Grievances, and Fair Hearings Provider Dispute/Appeal Procedures; Member Complaints, Grievances and Fair Hearings 138 Provider Dispute/Appeal
IV. Clinical Policies and Procedures
 A. Introduction The role of ValueOptions NorthSTAR is to coordinate the delivery of clinical services. There are three parties to this care coordination process: the Enrollee, the Provider(s), and the
A. Introduction The role of ValueOptions NorthSTAR is to coordinate the delivery of clinical services. There are three parties to this care coordination process: the Enrollee, the Provider(s), and the
Mississippi Medicaid Outpatient Hospital Mental Health Services Provider Manual
 Mississippi Medicaid Outpatient Hospital Mental Health Services Effective Date: January 1, 2009 Revised: January 2017 Table of Contents: Hospital Outpatient Mental Health I. Getting Started Helpful Tips
Mississippi Medicaid Outpatient Hospital Mental Health Services Effective Date: January 1, 2009 Revised: January 2017 Table of Contents: Hospital Outpatient Mental Health I. Getting Started Helpful Tips
FOUR TIPS: THE INVISIBLE IMPACT OF CREDENTIALING
 FOUR TIPS: THE INVISIBLE IMPACT OF CREDENTIALING The Invisible Impact of Credentialing Four Tips: The past 8 to 10 years have been transformative in the business of providing healthcare. The 2009 American
FOUR TIPS: THE INVISIBLE IMPACT OF CREDENTIALING The Invisible Impact of Credentialing Four Tips: The past 8 to 10 years have been transformative in the business of providing healthcare. The 2009 American
Butte County Department of Behavioral Health
 Butte County Department of Behavioral Health Quality Assurance and Performance Improvement Work Plan FY 17-18 Introduction As required by the California State Department of Health Care Services and the
Butte County Department of Behavioral Health Quality Assurance and Performance Improvement Work Plan FY 17-18 Introduction As required by the California State Department of Health Care Services and the
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
John W. Gahan Jr. Department of Health
 John W. Gahan Jr. Department of Health Indigent Care Pool Electronic Health Record Medicaid Reimbursement FQHC s Other Clinics Appeals Meaningful Use Primary Medical Home General Billing 2010 AHCF-1 Questions
John W. Gahan Jr. Department of Health Indigent Care Pool Electronic Health Record Medicaid Reimbursement FQHC s Other Clinics Appeals Meaningful Use Primary Medical Home General Billing 2010 AHCF-1 Questions
Presented to you by The Cooperative of American Physicians, Inc.
 ICD-10 Action Guide for Medical Practices PAGE 1 Presented to you by The Cooperative of American Physicians, Inc. Table of Contents Introduction... 3 What Is Changing and Why?... 4 What Are the Main Provisions
ICD-10 Action Guide for Medical Practices PAGE 1 Presented to you by The Cooperative of American Physicians, Inc. Table of Contents Introduction... 3 What Is Changing and Why?... 4 What Are the Main Provisions
HealthChoice Radiology Management. March 1, 2010
 HealthChoice Radiology Management March 1, 2010 Introduction Acting on behalf of our Medicaid customers in Maryland (HealthChoice), UnitedHealthcare has worked with external physician advisory groups to
HealthChoice Radiology Management March 1, 2010 Introduction Acting on behalf of our Medicaid customers in Maryland (HealthChoice), UnitedHealthcare has worked with external physician advisory groups to
Behavioral Health Provider Training: Program Overview & Helpful Information
 Behavioral Health Provider Training: Program Overview & Helpful Information Agenda Passport Behavioral Health Services Overview Steps to Joining Passport Health Plan s Network Getting a Medicaid Number
Behavioral Health Provider Training: Program Overview & Helpful Information Agenda Passport Behavioral Health Services Overview Steps to Joining Passport Health Plan s Network Getting a Medicaid Number
Welcome to the Cenpatico 2017 Provider Newsletter
 Improving Lives 2017 ISSUE You want to help your patients. We re here to help you. This newsletter will provide you with information regarding our clinical and operational resources, and programs, all
Improving Lives 2017 ISSUE You want to help your patients. We re here to help you. This newsletter will provide you with information regarding our clinical and operational resources, and programs, all
FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy
 FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014,
FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014,
State Medicaid Recovery Audit Contractor (RAC) Program
 Program") State Medicaid Recovery Audit Contractor (RAC) Program Section 6411 of the Patient Protection and Affordable Care Act 2010 (ACA) requires by December 31, 2010 each state Medicaid program to contract with
State Medicaid Recovery Audit Contractor (RAC) Program Section 6411 of the Patient Protection and Affordable Care Act 2010 (ACA) requires by December 31, 2010 each state Medicaid program to contract with
Quality Improvement Work Plan
 NEVADA County Behavioral Health Quality Improvement Work Plan Mental Health and Substance Use Disorder Services Fiscal Year 2017-2018 Table of Contents I. Quality Improvement Program Overview...1 A. QI
NEVADA County Behavioral Health Quality Improvement Work Plan Mental Health and Substance Use Disorder Services Fiscal Year 2017-2018 Table of Contents I. Quality Improvement Program Overview...1 A. QI
Behavioral health provider overview
 Behavioral health provider overview KSPEC-1890-18 February 2018 Agenda Provider manual and provider website Behavioral Health (BH) program goals Access and availability standards Care coordination and
Behavioral health provider overview KSPEC-1890-18 February 2018 Agenda Provider manual and provider website Behavioral Health (BH) program goals Access and availability standards Care coordination and
Providing and Documenting Medically Necessary Behavioral Health Services
 Providing and Documenting Medically Necessary Behavioral Health Services Presented by: David Reed, Office Chief, Division of Behavioral Health and Recovery Marc Bollinger, LISCW, CEO, Great Rivers BHO
Providing and Documenting Medically Necessary Behavioral Health Services Presented by: David Reed, Office Chief, Division of Behavioral Health and Recovery Marc Bollinger, LISCW, CEO, Great Rivers BHO
CorCare PPO Provider Manual. Updated 12/19/2016
 CorCare PPO Provider Manual 2017 Updated 12/19/2016 TABLE OF CONTENTS TABLE OF CONTENTS 1. Summary of Procedures, Resources, Claims Submissions... 3 2. Claims Completion... 4 3. Prepayment and Balanced
CorCare PPO Provider Manual 2017 Updated 12/19/2016 TABLE OF CONTENTS TABLE OF CONTENTS 1. Summary of Procedures, Resources, Claims Submissions... 3 2. Claims Completion... 4 3. Prepayment and Balanced
SEVEN SEVEN. Credentialing tips designed to help keep costs down and ensure a healthier bottom line.
 Seven Tips to Succeed in the Evolving Credentialing Landscape SEVEN SEVEN Credentialing tips designed to help keep costs down and ensure a healthier bottom line. 7The reimbursement shift from fee-for-service
Seven Tips to Succeed in the Evolving Credentialing Landscape SEVEN SEVEN Credentialing tips designed to help keep costs down and ensure a healthier bottom line. 7The reimbursement shift from fee-for-service
Behavioral Health Redesign. 1. Progress toward transformation 2. Readiness to go live January 1, Contingency plan for provider payment
 Behavioral Health Redesign 1. Progress toward transformation 2. Readiness to go live January 1, 2017 3. Contingency plan for provider payment Behavioral Health Redesign The goal is to integrate physical
Behavioral Health Redesign 1. Progress toward transformation 2. Readiness to go live January 1, 2017 3. Contingency plan for provider payment Behavioral Health Redesign The goal is to integrate physical
Observation vs. Inpatient: How to Get it Right. November 5, 2013
 Observation vs. Inpatient: How to Get it Right November 5, 2013 Learning Objectives Understand how the Inpatient Prospective Payment System (IPPS) Final Rule impacts your facility Integrate leading practice
Observation vs. Inpatient: How to Get it Right November 5, 2013 Learning Objectives Understand how the Inpatient Prospective Payment System (IPPS) Final Rule impacts your facility Integrate leading practice
Mississippi Medicaid Inpatient Services Provider Manual
 Mississippi Medicaid Inpatient Services Provider Manual Effective Date: November 2015 Revised: June 2016 Inpatient Services Provider Manual Introduction eqhealth Solutions (eqhealth) is the Utilization
Mississippi Medicaid Inpatient Services Provider Manual Effective Date: November 2015 Revised: June 2016 Inpatient Services Provider Manual Introduction eqhealth Solutions (eqhealth) is the Utilization
UTILIZATION MANAGEMENT POLICIES AND PROCEDURES. Policy Name: Substance Use Disorder Level of Care Guidelines Policy Number: 7.08
 SALISH BHO UTILIZATION MANAGEMENT POLICIES AND PROCEDURES Policy Name: Substance Use Disorder Level of Care Guidelines Policy Number: 7.08 Reference: WAC 388-877B, Contract requirements DSM-5, ASAM, SBHO
SALISH BHO UTILIZATION MANAGEMENT POLICIES AND PROCEDURES Policy Name: Substance Use Disorder Level of Care Guidelines Policy Number: 7.08 Reference: WAC 388-877B, Contract requirements DSM-5, ASAM, SBHO
ABOUT FLORIDA MEDICAID
 Section I Introduction About eqhealth Solutions ABOUT FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency) is the single
Section I Introduction About eqhealth Solutions ABOUT FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency) is the single
Stewardship Policy No. 16
 Page 1 of 16 REVIEW BY: 12/07/19 POLICY It is the policy of Catholic Health Initiatives (CHI), and each of its tax-exempt Direct Affiliates, 1 and tax-exempt Subsidiaries 2 that Operates a Hospital Facility
Page 1 of 16 REVIEW BY: 12/07/19 POLICY It is the policy of Catholic Health Initiatives (CHI), and each of its tax-exempt Direct Affiliates, 1 and tax-exempt Subsidiaries 2 that Operates a Hospital Facility
State of Montana. Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES
 State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT October 1, 2012 Children s Mental Health
State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT October 1, 2012 Children s Mental Health
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
State advocacy roadmap: Medicaid access monitoring review plans
 State advocacy roadmap: Medicaid access monitoring review plans Background Federal Medicaid law requires states to ensure Medicaid beneficiaries are able to access the healthcare providers they need through
State advocacy roadmap: Medicaid access monitoring review plans Background Federal Medicaid law requires states to ensure Medicaid beneficiaries are able to access the healthcare providers they need through
Rehabilitation (PSR/CPST) & Habilitation. November 13 th & 16 th The Managed Care Technical Assistance Center of New York
 & Habilitation. November 13 th & 16 th The Managed Care Technical Assistance Center of New York") Rehabilitation (PSR/CPST) & Habilitation November 13 th & 16 th 2015 The Managed Care Technical Assistance Center of New York Welcome MCTAC Overview Business/Billing Rules Services Definition Service Components
Rehabilitation (PSR/CPST) & Habilitation November 13 th & 16 th 2015 The Managed Care Technical Assistance Center of New York Welcome MCTAC Overview Business/Billing Rules Services Definition Service Components
Benchmarking Patient Access Performance
 Revenue Cycle Solutions Benchmarking Patient Access Performance Compare your patient access performance to our 15 best practice benchmarks Advisory Board estimates that the average 350 bed hospital stands
Revenue Cycle Solutions Benchmarking Patient Access Performance Compare your patient access performance to our 15 best practice benchmarks Advisory Board estimates that the average 350 bed hospital stands
Redesign Medicaid in New York State. Behavioral Health Medicaid Managed Care Kick-Off Forums
 Redesign Medicaid in New York State Behavioral Health Medicaid Managed Care Kick-Off Forums Presented by: Gary Weiskopf, Associate Commissioner for Managed Care, NYS Office of Mental Health Donna Bradbury,
Redesign Medicaid in New York State Behavioral Health Medicaid Managed Care Kick-Off Forums Presented by: Gary Weiskopf, Associate Commissioner for Managed Care, NYS Office of Mental Health Donna Bradbury,
WellCare FL_ Encounters. Florida 2016 Module 2: AHCA Rules and Guidelines
 WellCare 2016. FL_061516. Encounters Florida 2016 Module 2: AHCA Rules and Guidelines Provider Validation and Registration Medicaid ID Registration Process 2 National Provider Identifier (NPI) & Medicaid
WellCare 2016. FL_061516. Encounters Florida 2016 Module 2: AHCA Rules and Guidelines Provider Validation and Registration Medicaid ID Registration Process 2 National Provider Identifier (NPI) & Medicaid
3. Does the institution have a dedicated hospital-wide committee geared towards the improvement of laboratory test stewardship? a. Yes b.
 Laboratory Stewardship Checklist: Governance Leadership Commitment It is extremely important that the Laboratory Stewardship Committee is sanctioned by the hospital leadership. This may be recognized by
Laboratory Stewardship Checklist: Governance Leadership Commitment It is extremely important that the Laboratory Stewardship Committee is sanctioned by the hospital leadership. This may be recognized by
Texas Medicaid. Provider Procedures Manual. Provider Handbooks. Telecommunication Services Handbook
 Texas Medicaid Provider Procedures Manual Provider Handbooks December 2017 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid
Texas Medicaid Provider Procedures Manual Provider Handbooks December 2017 Telecommunication Services Handbook The Texas Medicaid & Healthcare Partnership (TMHP) is the claims administrator for Texas Medicaid
Clinical Quality Review Team (CQRT) Training
 Training") 1 Clinical Quality Review Team (CQRT) Training A Guide to the Authorization Process for Alameda County Behavioral Health Plan Members 2 Learning Objectives Understand the purpose of the CQRT and its function
1 Clinical Quality Review Team (CQRT) Training A Guide to the Authorization Process for Alameda County Behavioral Health Plan Members 2 Learning Objectives Understand the purpose of the CQRT and its function
Full speech capability, allowing you to speak your information and inquiries or use your touchtone
 NEW YORK 2015 ISSUE IV PROVIDER Newsletter NEW PROVIDER SERVICES TECHNOLOGY WellCare is excited to announce some major technology improvements within our call centers, making it easier for providers to
NEW YORK 2015 ISSUE IV PROVIDER Newsletter NEW PROVIDER SERVICES TECHNOLOGY WellCare is excited to announce some major technology improvements within our call centers, making it easier for providers to
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
GUIDELINES FOR CRITERIA AND CERTIFICATION RULES ANNEX - JAWDA Data Certification for Healthcare Providers - Methodology 2017.
 GUIDELINES FOR CRITERIA AND CERTIFICATION RULES ANNEX - JAWDA Data Certification for Healthcare Providers - Methodology 2017 December 2016 Page 1 of 14 1. Contents 1. Contents 2 2. General 3 3. Certification
GUIDELINES FOR CRITERIA AND CERTIFICATION RULES ANNEX - JAWDA Data Certification for Healthcare Providers - Methodology 2017 December 2016 Page 1 of 14 1. Contents 1. Contents 2 2. General 3 3. Certification
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule
 CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
Health UM Accreditation v7.4. Workers Compensation UM Accreditation v7.4. Copyright 2018 URAC All Rights Reserved
 Health UM Accreditation v7.4 Workers Compensation UM Accreditation v7.4 Copyright 2018 URAC All Rights Reserved Learning Objectives Attendees at this webinar should be able to: Understand the accreditation
Health UM Accreditation v7.4 Workers Compensation UM Accreditation v7.4 Copyright 2018 URAC All Rights Reserved Learning Objectives Attendees at this webinar should be able to: Understand the accreditation
9/10/2016. What is a Cycle? Learning Objectives
 Keep the Cycle Going: Maintaining a Healthy Long Term Care Revenue Cycle and Key Strategies for Successful Reimbursement Management September 29, 2016 What is a Cycle? By law of periodical repetition,
Keep the Cycle Going: Maintaining a Healthy Long Term Care Revenue Cycle and Key Strategies for Successful Reimbursement Management September 29, 2016 What is a Cycle? By law of periodical repetition,
Clinical documentation is the core of every patient encounter. The
 Cornerstone of CDI success: Build a strong foundation WHITE PAPER Summary: Clinical documentation improvement (CDI) programs play a vital role in today s healthcare environment. The growth of the U.S.
Cornerstone of CDI success: Build a strong foundation WHITE PAPER Summary: Clinical documentation improvement (CDI) programs play a vital role in today s healthcare environment. The growth of the U.S.
TABLE OF CONTENTS. Therapy Services Provider Manual Table of Contents
 Table of Contents TABLE OF CONTENTS Table of Contents...1 About AHCA...2 About eqhealth Solutions...2 Accessibility and Contact Information...5 Review Requirements and Submitting PA Requests...9 First
Table of Contents TABLE OF CONTENTS Table of Contents...1 About AHCA...2 About eqhealth Solutions...2 Accessibility and Contact Information...5 Review Requirements and Submitting PA Requests...9 First
Amerigroup Kansas Provider Training Program
 Amerigroup Kansas Provider Training Program Agenda About NIA The Provider Partnership The Program Components How the Program Works: The Precertification Process The Precertification Appeals Process The
Amerigroup Kansas Provider Training Program Agenda About NIA The Provider Partnership The Program Components How the Program Works: The Precertification Process The Precertification Appeals Process The
Molina Healthcare Michigan Health Care Services Department Phone: (855) Fax: (800)
 Fax: (800)") Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
The Transition to Version 5010 and ICD-10
 The Transition to Version 5010 and ICD-10 An Overview Denise M. Buenning, MsM Director, Administrative Simplification Group Office of E-Health Standards and Services Centers for Medicare & Medicaid Services
The Transition to Version 5010 and ICD-10 An Overview Denise M. Buenning, MsM Director, Administrative Simplification Group Office of E-Health Standards and Services Centers for Medicare & Medicaid Services
Understanding and Using the Adult BH HCBS Billing Rates and Codes. February 22, The Managed Care Technical Assistance Center of New York
 Understanding and Using the Adult BH HCBS Billing Rates and Codes February 22, 2016 The Managed Care Technical Assistance Center of New York Housekeeping Slides are posted at MCTAC.org Questions not addressed
Understanding and Using the Adult BH HCBS Billing Rates and Codes February 22, 2016 The Managed Care Technical Assistance Center of New York Housekeeping Slides are posted at MCTAC.org Questions not addressed
UW MEDICINE ICD-10 Program UW MEDICINE ICD-10
 UW MEDICINE ICD-10 Program UW MEDICINE ICD-10 There and back again INTEGRATION OF MANDATES ACO Quality Based Reimbursement Meaningful Use, P4P, etc. ICD-10 HIPAA, 5010 2 STRATEGIC OPPORTUNITIES Significant
UW MEDICINE ICD-10 Program UW MEDICINE ICD-10 There and back again INTEGRATION OF MANDATES ACO Quality Based Reimbursement Meaningful Use, P4P, etc. ICD-10 HIPAA, 5010 2 STRATEGIC OPPORTUNITIES Significant
General Who is National Imaging Associates, Inc. (NIA)?
?") National Imaging Associates, Inc. (NIA) Frequently Asked Questions (FAQ s) For Managed Health Services (MHS) Providers Post Service Therapy Review Program Question Answer General Who is National Imaging
National Imaging Associates, Inc. (NIA) Frequently Asked Questions (FAQ s) For Managed Health Services (MHS) Providers Post Service Therapy Review Program Question Answer General Who is National Imaging
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership