Tom Abell, Deputy Chief Executive. Chris James, Assistant Director of Performance
|
|
|
- Mary Sullivan
- 5 years ago
- Views:
Transcription
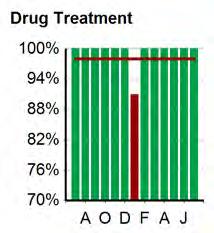
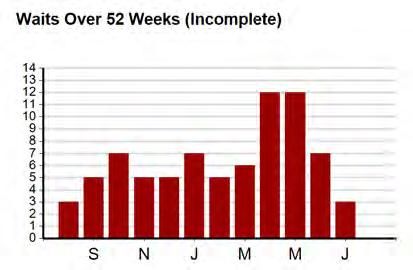
1 Meeting Title Board of Directors Meeting Date 5 October 2016 Agenda No 9 Report Title Trust Performance Report Lead Executive Director Report Author Tom Abell, Deputy Chief Executive Chris James, Assistant Director of Performance Action Required Decision Discussion Monitoring (please tick) Strategic Objective(s) Executive Summary Background / Context Objective 1 Deliver high quality acute care whenever needed The Performance Report provides the Trust s performance against the agreed metrics for: Quality, Finance, Operations and Workforce in one place. The Board is asked to: consider the content of this report and request clarification for any areas of concern; determine what additional assurance may be required from divisional and corporate leads. Previously considered by Divisional and Corporate leads as part of Trust Performance Management Framework, including at Divisional Performance meetings. Key Issue 1 (replace with a brief summary of the issue) Operational A number of KPIs across each of the four domains are not compliant against agreed standards and assurance is required that the necessary actions are being taken to recover performance and mitigate any risk of adverse quality of care. Performance concerns include: 18 weeks RTT, Diagnostic waits, Cancer 62-day performance and A&E Operational Standards including ambulance handovers to A&E staff Recovery action plans and trajectories have been agreed for each of the above in conjunction with local Trusts and commissioners, NHS Improvement and NHS England. 18 weeks incomplete was scheduled to be at or above 92% from the end of May, was not delivered in August. A&E 4-hour performance has not met the local trajectory for August. 62-day cancer performance has met its trajectory for July 6-week diagnostic wait performance was not delivered in August Operational performance will continue to be scrutinised through two Executive led weekly meetings focussing on: 54
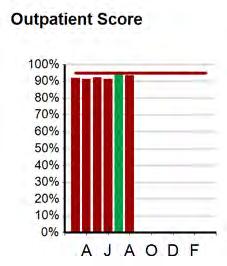
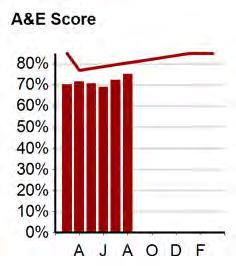
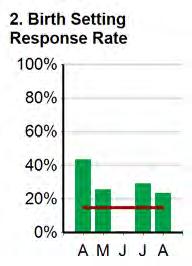
2 a) access to elective care and b) emergency care pathways An Executive led task an finish group continues focussing on improving data quality with regards to 18 weeks RTT recording, reporting and performance. Further task and finish groups to look at data quality of admitted and non-admitted performance for patient who have received treatment are proposed. Quality Timely clinic and discharge letter communication to GPs A recovery trajectory has been agreed with local commissioners, specifically in relation to electronic sharing of clinic letters to GPs. The Trust did not deliver against this trajectory in July and August. Timely Completion of RCAs and action plans following serious incidents The need to prioritise patient care has meant a decline in performance in recent months. Scrutiny of RCA and incidents is now completed via an Executive Review group Falls and pressure ulcer occurrence rates Revised KPIs and trajectories have been established for for injurious falls and pressure ulcers; with a continued focus on harm free care. Friends and Family Test Performance remains a challenge in a number of areas, however there have improvement in A&E response rates and scores.. Inpatients and outpatient scores see the vast majority of patients asked saying they would recommend their friends and family. Workforce Vacancy and Turnover rates and associated pay costs A number of recruitment initiatives are progressing well in an attempt to minimise the use of temporary staff and reduce pay costs. Mandatory training The scope of training requirements has been adjusted for and divisions performance has been reset resulting in a number of areas of non-compliance. The areas affected have committed to improving performance through support from HR Business Partners before any action is taken in line with the accountability framework Finance Financial performance was discussed at Divisional performance review meetings and as a result a number for divisions will continue to be asked to attend regular meetings with the Managing Director 55
3 and other Executive colleagues focussing on financial performance. Timescale for Benefits to be Realised n/a Assessment of Implications Financial Does this proposal have revenue (recurrent or non-recurrent) implications for the Trust? No Does this proposal have capital (recurrent or non-recurrent) implications for the Trust? No Risk Equality and Diversity Freedom of Information Other Implications Identified (including patient safety and quality, legal and regulatory compliance) Recommendation Failing to monitor and assess the performance of services provided by the Trust may result in the Trust and its Board being unaware of shortcomings in care and quality. Either : A)This proposal has been subject to an equality analysis and there are no implications for groups with protected characteristics No exemptions apply (i.e., information is in the public domain) NHS Constitution: Principle 3 - The NHS aspires to the highest standards of professionalism and excellence. Principle 4 - The NHS aspires to put patients at the heart of everything it does Monitor/CQC Compliance The Board / Committee is invited to: Appendices N/A consider the content of this report and request clarification for any areas of concern; determine what additional assurance may be required from divisional and corporate leads. 56











 Temp.")
 Workforce")
4 Performance Report: Aug 2016 Trust Mortality Screening Coverage Less than 6 wk wait - Diagnostic Patients - Incomplete Treatment Quality C-Diff Cases Inpatient Satisfaction Score Operational Patients Treated Within 4 Hrs Treated Within 62 Days Summary Vacancies Mandatory Training Variance To Budget ( m) Temp. Staff Costs ( 000) Workforce Turnover Appraisals Finance CIP ( 000) Valid NHS No field in Acute CDS 1/16 28 Sep
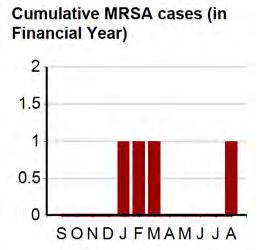
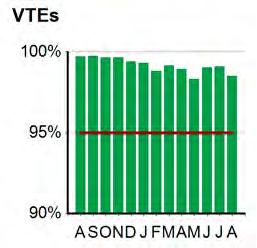
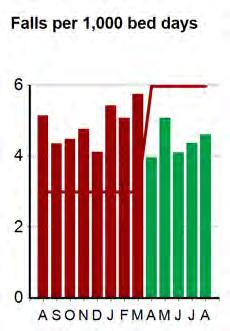
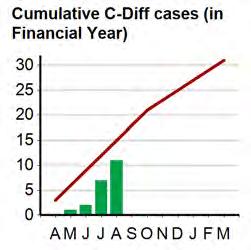
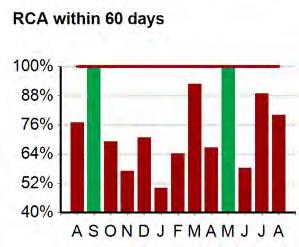
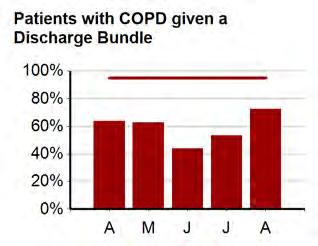
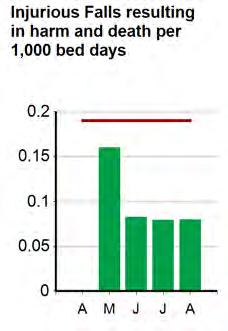
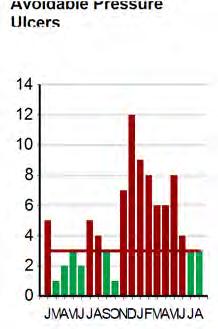
5 Performance Commentary Exception Report: August 2016 Report of the Director of Nursing & Medical Director Quality SAFE & EFFECTIVE CARE VTE Screening for VTE has fallen slightly to 98.5% in August. The divisions continue to monitor this and the paper copies continue. The electronic format requires further system changes allowing a full audit trail for changes made. Infection Prevention & Control MRSA bacteraemia and Clostridium difficile One MRSA Bacteraemia was reported in August. This case has been reviewed by the PIR process and was deemed avoidable. The case identified many areas for action and a robust action plan is being monitored through Infection Control Committee Four cases of C.difficle were reported in August. An MDT was undertaken on all cases. No lapses in care have been identified. Injurious Inpatient Falls There were no injurious inpatient falls in August 2016 resulting in severe harm (none in July). To date, activity versus falls demonstrates that the Trust consistently performs well against the national standard of 6.63 falls/1000 bed days set in the RCP audit of Inpatient falls. In August there were 4.6 falls per 1000 bed days. The FallSafe programme continues to roll out across inpatient wards. Preventable Pressure Ulcers Performance is on trajectory with 3 grade 2 preventable pressure ulcers in August. The incidences were deemed as low impact. The RCAs from the above have identified insufficient evidence that the patients heels were elevated prior the pressure ulcers occurring. A number of actions have been identified/planned including: Both wards to remind their staff of the importance of heel floatation. The Tissue Viability Team has sourced a new heel protecting device that may increase patient compliance and a trial has commenced. Teaching delivered to the ANTs (link nurses) on heel ulcer assessment and prevention strategies, micro teaching slides to be developed to enable the ANTs to deliver teaching in their clinical environment. Cardiac Arrests reviewed Cardiac Arrests data has changed for this metric to include the number of reviews completed by the NDT teams. August data shows that 12.5% of cardiac arrests were reviewed. None of these reviews have required escalation within the incident reporting system. Never Events There were no Never Events reported in August RCA within 60 working days within 60 days Performance has fallen from 89% in July to 80% in August. The Patient Safety Team continues to meet with the divisions to support the divisions to meet the target deadlines. Patients with COPD given a Discharge Bundle There was a further improvement in August s performance from at 73% (53% in July). The Respiratory nurses continue to concentrate on the assessment units to drive improvements. 58
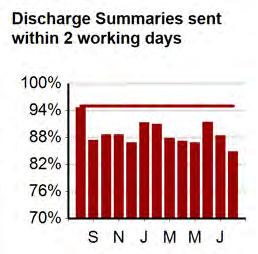
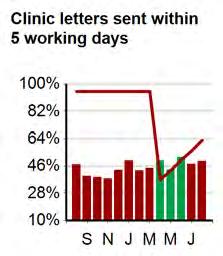
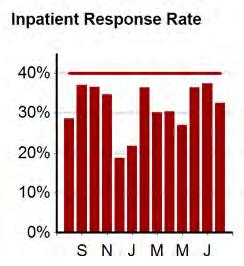
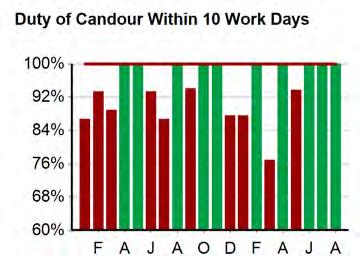
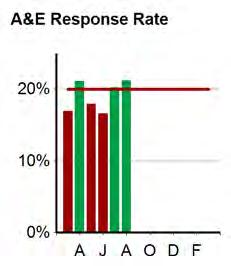
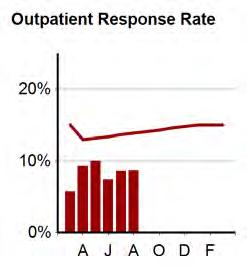
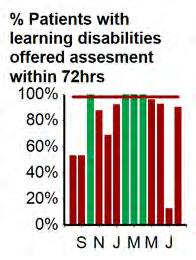
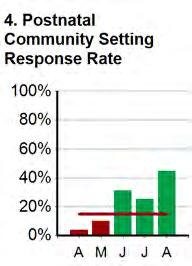
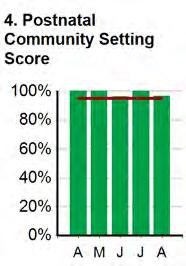
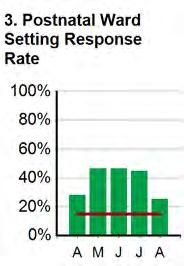
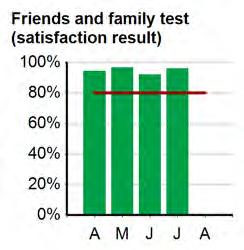
6 Report of the Director of Nursing & Medical Director Quality Catheters associated UTIs The Patient Safety Thermometer data report shows performance in August at 95%, this remains static. With an improved performance for catheter associated UTI. Completed Mortality Reviews (excl EOL pathway) The mortality reviews has fallen to 4% in August; this has been discussed at the mortality group and at divisional governance meetings. There are a number of reviews which have been completed however are not recorded on the mortality review system. Dementia Screening Performance in August was 94% and remains above the target of 90%. PATIENT EXPERIENCE Satisfaction (Friends & Family Friends & Family Test (FFT) The Inpatient response rate fell from 37% to 33% in August against the 40% target. The response rate improved further for A&E at 21.2% against the 20% national target. The internal Target of 15% for Outpatients was not achieved, in August this was 9% Duty of Candour within 10 days Performance for August was 100%. % patients with learning disabilities offered assessment within 72hrs Performance was 90% in August which is an improvement on previous months. Discharge Summaries Sent within 2-working Days The performance target increased in March 2015 to 95% from 85% in 2015/16. 95% has yet to be achieved. Performance across the year has been variable. Performance fell from 88% to 84% in August. Clinic Letters sent within 5 working days The August performance has reduced to 49%. There has been focused work being completed within the Divisions. Complaints Management There was a 21% increase in the number of new complaints received with 75 in August (62 in July). 100% of complaints were acknowledged within target and 95% of final responses were closed within target. There were 10 requests for additional investigation on closed complaints (7 in July) and 6 requests for local resolution meetings (6 in July). The complaints increases were notable in the Acute Division, Women s and Children s and Surgical Services. 59
7 Performance Report: Aug 2016 Trust Mortality Screening Coverage Infection Control Quality: Safe & Effective Care Falls (excl A&E) Never Events Serious Incidents Cardiac Arrests Pressure Ulcers Critical Care Respiratory SEPSIS 2/16 28 Sep
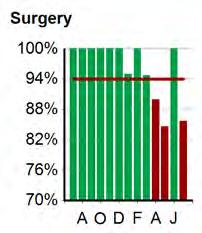
8 Performance Report: Aug 2016 Trust Satisfaction ( Friends and Family ) Complaints & Incidents Management Quality: Experience Satisfaction ( Friends and Family Maternity) Satisfaction Surgery Cancellations Communication EMSA 4/16 28 Sep
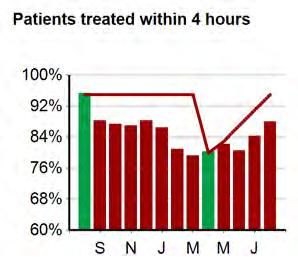
9 Performance Commentary: July 2016 Report of the Chief Operating Officer Emergency care will occur and more information on the Delivery Board will follow. Operations Performance against the 4-hour standard in Aug was disappointing, but much improved on previous months with a performance of 88.1%. We were on track to deliver 90% hut the last 3 days in August were disappointing in terms of pressure and performance resulting in the 88.1%. This compares to a national performance (in June) of 90.5%. The System action plan is reviewed fortnightly and all but one action is on track. A twice weekly meeting with all relevant partner agencies continues to take place to unblock issues and ensure that patients are moved on and placed in the most appropriate setting. The occupancy rate remains very high (100+%) and the organisation has remained on Black and Red Alert for most of August. Emergency system pressures and performance remain an area that is consuming vast amounts of staff time and energy as well as being a concern. The Managing Director convenes a weekly Emergency Pathways Group meeting to identify the key actions that will see improvement. Given historical trends in performance and recent increases in demand, financial planning has assumed there is a low probability of delivery of the improvement trajectory for the remainder of the financial year. 18-week referral to treatment The incomplete standard was not achieved for July or August against a target of 92%. There are significant data quality improvements that are assisting the recovery of this target. As at writing, the position for August has been reported as 89.2%. This compares to a national performance (in July) of 91.3%. A review of every speciality s performance is underway to ensure a complete understanding of the issues and challenges in sustainable delivery. The main risk for most specialities is workforce availability. Given recent performance, financial planning has assumed there is a low probability of delivery of the improvement trajectory for the remainder of the financial year. Staffing has been a challenge on certain days within A&E which has exacerbated performance but the appointment of a Clinical Director (who started on the 1 st August) as well as the successful recruitment to other A&E medical staff vacancies has seen medical staffing and performance improve. An urgent system summit was called on the 20 th July to ensure a better response from partner organisations and the SRG are following through on this with additional actions being agreed by other agencies. SRGs are being replaced in September with 4 hour delivery Boards chaired by the acute Trust. A re-focus of these meetings 62
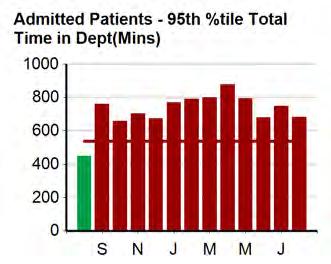
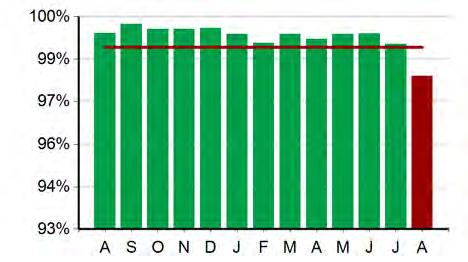
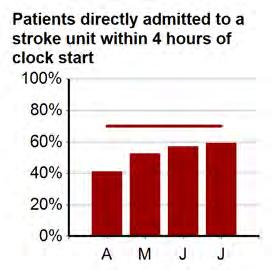
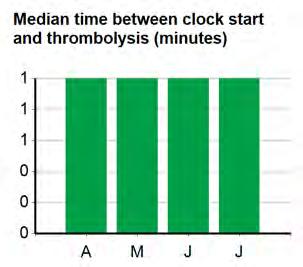
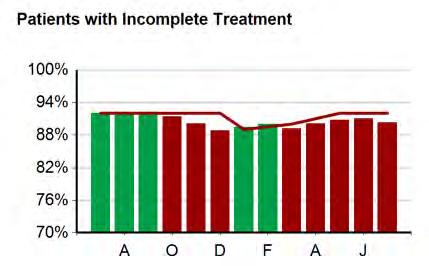
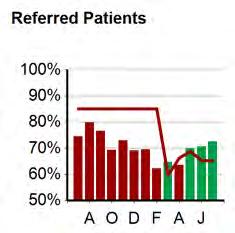
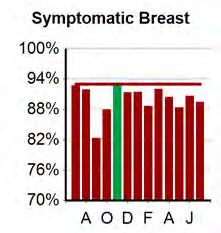
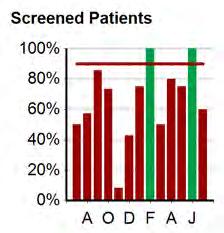
10 Performance Commentary: July 2016 Report of the Chief Operating Officer Cancer targets 6 week Diagnostic target Operations Compliance against cancer targets is a considerable challenge. The July positon for treatment within 62 day was published as 72.5%, compared to 82.2% nationally. This was ahead of the trajectory of 65.4%; with BTUH only pathways at 80.8%. An escalation meeting with NHSE / NHSI for the mid and South Essex area took place on 27 th July. In conjunction with other local Trusts, the Trust is committed to returning performance to 85% by October Given recent improvements, financial planning for STP has assumed there is a medium probability of delivery of the improvement trajectory for the remainder of the financial year. Performance at tumour site level (for 62 day performance) for Q along with the national mean performance is listed below as per the national publication by NHS England. 62-Day Cancer Performance, All Care, Q Source: NHS England Website The Trust did not achieve the 6 week diagnostic target for July with a performance of 98.1%; primarily associated with the Trust not being able to respond to increases in demand for CT, MRI and ultrasound scans. Stroke The key stroke metrics demonstrate good progress. Comparisons with other Trusts show our relative good performance. A visit to mid-essex NHS Trust has already taken place and a visit is planned to St. Georges in south London to identify any areas of shared good practice. The latest quarterly results show further improvement with the Trust now having a rating of A which has been acknowledged by the CCG. Tumour Site Basildon England All cancers 68.5% 82.4% Breast 82.0% 94.8% Lower Gastrointestinal 62.1% 72.1% Lung 44.9% 72.2% Skin 76.9% 95.9% Urological (Excluding Testicular) 61.2% 78.1% Other 68.8% 75.3% 63
11 Performance Report: Aug 2016 Trust A&E Performance Stroke Operational A Paediatric Assessment Unit (PAU) Less than 6 wk wait - Diagnostic 6/16 28 Sep
12 Performance Report: Aug 2016 Trust Patients Treated Within 18 Weeks of Referral from GP Pharmacy Cancer Waiting Times Compliance Operational B Seen within 2 weeks of referral Treated within 62 days Treatment within 31 days of decision to treat MSK 7/16 28 Sep
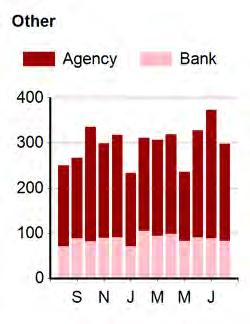
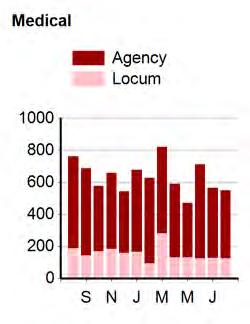
13 Performance Commentary: August 2016 Report of the Director of Workforce & Organisational Development Workforce Recruitment The Trust vacancy rate increased from 11.7% in July to 11.8% in August. Within the month of August, WTE jobs were out to advert and 141WTE were appointed, indicating a fill rate of 57%. The Trust vacancy position has not changed much since July. Trust vacant WTE is now at WTE in August compared to 556.9WTE in July. Registered nursing vacancies are currently at 282.8WTE. Recruitment plans at divisional and corporate level continue to address this. Retention is also being looked at within areas of high turnover to support recruitment and in particular to reduce turnover. There were 178 starters in August, 126 of which were trainee doctors. New starter numbers (doctors excluded) dropped between July to August from 62 to 52. There were only 8 nurse starters in August. In addition there were 15 estates staff, 9 administrative staff, 12 clinical support services staff, 7 allied health staff and 1 additional professional scientific staff. Medical Deanery rotations successfully took place in August. 31 staff grade doctors are currently being processed with projected start dates from September to November. There has been a marked increase in medical recruitment with 19 in Medicine with 4 currently being processed for the new Junior Clinical Fellow post. We expect medical vacancies to reduce significantly by the end of the year assuming turnover stays the same. Nurses We currently have a vacancy factor of 17.73% for registered Nurses and Midwives, up from 17.12% in July The greatest proportion of vacancies is at band 5 ward level. The Trust has developed a new senior staff nurse role as part of our retention strategy. Interviews and appointments to this new role are underway. Planned Nursing Job Fairs The Trust will be present at the RCN Job Fair in Glasgow on 6 & 7 October to recruit to CTC, Medicine, AE, Paediatrics and Surgery. We will also be present at the Shenfield and Thurrock Careers Fair in October and fresher fairs at local colleges. HCAs 14 HCAs commenced on 12 September with 15 due to commence in October. EU and Overseas Nursing Recruitment A further 9 EU nurses arrived on 12 September. There is a potential further intake of 10 to be commissioned to bring the total EU intake to approximately 62 by December. The first Philippine cohort arrives in November and we expect that between November and February we could have 26 additional nurses from outside the EU. Local nurse recruitment however needs to be improved to prevent an over reliance on overseas nursing. Turnover Overall turnover has increased from 15.32% in July 2016 to 15.55% in August. Sickness Absence There has been an increase from 3.72 % in June to 3.94% in July. The highest absence was in band 2 clinical areas, followed by band 7/8A in non-clinical areas. 66
14 Performance Commentary: August 2016 Report of the Director of Workforce & Organisational Development Workforce Workforce Cost Improvement Programmes/Actions The Direct Engagement project commenced on 23rd September 2015 and has yielded a saving of 533, 574 up to 31 st August Ongoing Workforce Improvement Projects National Staff Survey The National Staff Survey captures the views of staff on staff engagement including job role, management teams, health, wellbeing and safety, personal development and the Trust as an employer. The survey for 2015 closed with a total of 1448 respondents, reflecting a 34% completion rate. A paper was submitted to Trust Board in April 2016, which informed the Board of the key headlines and described the key priorities for the Trust. Below are the initiatives which we have implemented on the back of the results of the 2015 national staff survey. Each division produced a local action plan in response to the feedback given by staff in its area. We have redesigned the quarterly mini staff survey to reflect the areas of concern raised by staff in the national staff survey. The mini staff survey also contains questions relating to discrimination, staff reporting concerns and health & wellbeing which were all raised as areas requiring improvement in the national staff survey. In 2015, the Trust developed and launched a two year staff experience and engagement programme) to improve staff satisfaction and to embed a cultural shift in the way we do things at BTUH. The focus for year 2 of this staff engagement programme includes Values & Behaviours, Health & Wellbeing as well as Training and Leadership development. A staff communication is planned for October 2016, detailing the aforementioned actions taken as a result of staff feedback. Apprenticeship Levy The way the government funds apprenticeships in England is changing in spring 2017, with the introduction of an apprenticeship levy. The apprenticeship levy requires all employers operating in the UK, with a pay bill over 3 million each year, to make an investment in apprenticeships. The levy will be charged at a rate of 0.5% of the annual pay bill. There will be a levy allowance of 15,000 per year to offset against the levy you must pay Future Initiatives Talent Management The Trust is developing a talent management framework for identifying and managing the talent potential within its workforce. The aspiration is to create a resilient, agile and high performing leadership culture both now and in the future by: Investing now to develop future talent Aligning talent to organisational goals Identifying and nurturing talented leaders Identifying talent gaps Retaining and developing talent Developing career pathways and support for all staff Leadership Forum NHS Employers and the NHS Leadership Academy will be facilitating a workshop on transformational change for our senior leaders. The workshop will consider models of change, how to adapt to change, the different responses to change and managing self-resilience. The workshop is open to all senior leaders. 67





15 Performance Report: Aug 2016 Trust Appraisals Mandatory Training Core Skills Training Sickness Trust Induction Workforce Turnover Vacancies 9/16 28 Sep
16 Performance Commentary: August 16 Report of the Director of Finance Finance Key message At month five, the Trust remains behind the planned I&E position, by some 1.5milion (adverse variance). Within the YTD position is a prudent provision of a loss of 0.5m STF income for the A&E and RTT performance in July and August. The latter remains to be ratified once all counting is complete. The Year to Date financial position also includes the previously reported 0.9m benefit from the balance sheet of the finalisation of 2015/16 debts. The underlying deficit (excluding STF) is 11.0m (Which is 1.4m adverse to plan). A separate paper on the agenda details the fixed year-end block deal that has been negotiated with NHS England. The upside from this arrangement will provide for c 0.8m benefit into the Month 6 position for the year to date. Therefore, at this stage, the Trust remains on track to meet the planned Q2 position, with at least 70% of the STF funding (for financial plan) being available. It is important to note that this trust has phased its deficit correctly, professionally and in line with the NHSI guidance. But, as a result, the STF target is more challenging for the control total in Q2 and Q3. The Trust has the largest deficit planned in quarter in Q4 which is the highest cost period. There remains a significant risk to both the achievement of the 27.2m deficit control total and the requirements for the 11.6m S&T funding (STF). Full receipt of the STF reduces the net deficit down to 15.6m. A separate paper elsewhere on the agenda details the upside/downside sensitivity analysis for the forecast outturn. The risks to achieving the Control Total include the persistently high vacancy rate, particularly in nursing and scientific staff impacting bank and agency expenditure, CIP slippage risks, cost pressures, patient dependency and acuity, and most significantly of all, the CCGs demands for in-year QIPP contract income reductions against the block contract. The STF risks arise from the absolute need to meet the profiled control total plan position each quarter to receive the 70% STF and allow access to the balance of 30% STF monies. Without the control total being on plan the access to the 30% STF monies is denied. If the Trust can achieve the financial plan, then the latent risks arise specifically from attaining A&E monthly targets of 95% for the remainder of the year. RTT must also meet 92% each month. More specifically, the pressures described above manifest themselves in the adverse YTD expenditure positions in the Divisions of General Medicine, Acute Medicine, Surgery, Clinical Support Services and Women & Children s. Meanwhile CTC is recording an adverse position against income plans. Centrally held Reserves and Corporate divisions are mitigating these overspends. The Trust will take action where it can to seek to mitigate all risks, with recovery plans and strengthened controls. Divisional budgets: The heightened operational pressures and non-elective activity, together with acuity and patient dependency remains a key driver for the Trust s finances. The pay bill remains a serious concern and is above plan. This will need addressing through management action and CIP. CIP management is well-defined and schemes are now progressing. The key risk is to those plans reliant on agency staff savings. Due to the continued high-level vacancies and patient demand, these remain at considerable risk. Divisions with particular financial problems have been and continue to be escalated with Executives. Divisions are required to meet activity targets and their budget, whilst delivering safe services. The 69
17 Performance Commentary: August 16 Report of the Director of Finance excessively high vacancy rate militates against delivery of the activity plan and budget, Income: There is further risk significant financial risk to the 200m CCG block contract income arising from the CCGs planned QIPP schemes. These are being quantified but the incomplete, early CCG plans indicate that these could be c 2m to 4m. There has been early Executive-level engagement with the CCG to ensure that these schemes do in fact reduce demand and more importantly reduce hospital activity and cost. Any contract income reduction which is not matched with activity and cost changes will put the achievement of the control total at serious threat. discretionary control measures, working capital solutions, speculative procurement opportunities and income and coding improvements. Managing exceptional patient demand and increasing acuity will remain an on-going threat to the achievement of the plan. The Trust executive and management team will continue to work hard, supporting the values of the organisation to achieve the challenging financial goal set by the control total. This must be achieved without compromising clinical quality or patient experience. Finance Cash: The detailed weekly cash management will continue and, with DH cash support, the Board of Directors should be able to certify, albeit with material uncertainty, that the Trust will remain a going concern. The confirmation by NHSI of the criteria for the S&T Funds will help the Trust determine the future likely receipt. In the event that the Trust fails to meet all conditions, some of the 11.6m STF will be at risk. The funding shortfall would need to be made up with additional loan finance from the DH. The key to delivering the financial targets will be continued effective cost control, CIP delivery, contract income and QIPP negotiations, continued engagement of the organisation, performance management and continuing the financial education process to the organisation. Key actions include escalation meetings with divisions to review recovery plans to (a) arrest the deterioration and (b) to recover deficits, where possible. The Exec team are working on further temporary workforce controls, accelerated recruitment, 70
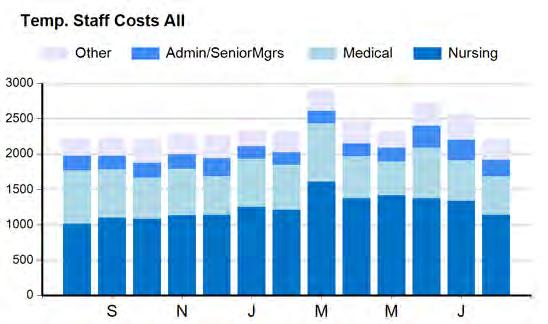
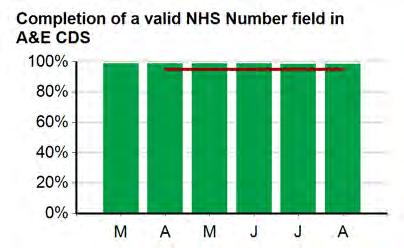
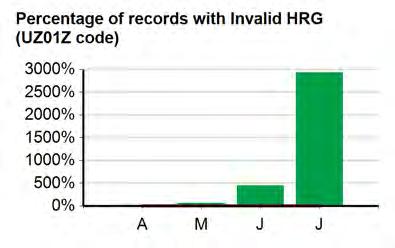
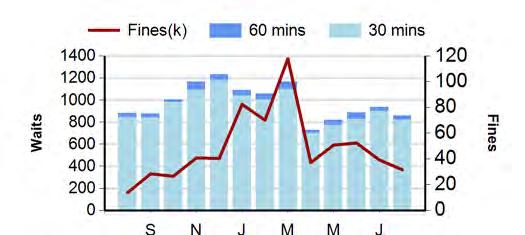
18 Performance Report: Aug 2016 Trust Earnings & Cash CIP ( 000) Ambulance Waits Temporary Staff Cost ( 000) Finance Data Quality - SUS 11/16 28 Sep
19 Meeting Title Board of Directors (Public) Date 5 th October 2016 Agenda item Report Title Clinical Governance Report (August) 11 Lead Director/ Manager Report Author Freedom of Information (FOI) Status Diane Sarkar, Director of Nursing Dawn Patience, Associate Director of Nursing & Quality Alison Kelly, Head of Litigation Public domain Action Required* Approval Decision Discussion Information Other (specify) Executive Summary The Clinical Governance Report incorporates key areas of clinical governance, in particular in the identification of areas where there can be shared learning and identify any emerging themes that are potential safety risks that require action by the Senior Management Group. Key points to note this month are as follows: Patient Satisfaction: FFT Inpatient response rates reduced from 37% in July to 33% in August. Maternity response rate has increased and exceeded target at 77%. 9 NHS Choices comments posted in August, 8 in July. 9 of these were 5 star rated. 33 plaudits logged in July. With shortages of staff in both PALS and Complaints, prioritisation of work has delayed the August plaudits being logged. Complaints: 21% increase in new complaints with 75 in August (62 in July). 5.4% increase in PALS concerns in August. Significant reduction in upheld complaints with 11% in August (24% in July). There was an increase in reopened complaints with 10 in August (7 in July). The number of requests for local resolution meetings also increased from 4 in July to 6 in August. Claims/Inquests: 12 new claims were received in August, 8 in July. 11 claims closed in August were discontinued. One inquest held in August. Narrative verdict. Incidents: 5.2% increase in incidents reported. Incidents reported as causing moderate, severe harm or death increased from 2.0% in July to 2.57% in August. Slight reduction in SIs reported with 11 in August (14 in July). The report provides a commentary in relation to performance for August Page 1 of 2 72
20 Recommendation The Board of Directors are asked to note the report Trust Strategic Objectives CQC Fundamental Standards NHS Constitution Implications Risk Legal Resources Previously Considered by Appendices Quality Care 24/7 9. Person-centred care 10. Dignity and respect 11. Need for consent 12. Safe care and treatment 13. Safeguarding service users from abuse and improper treatment 14. Meeting nutritional and hydration needs 16. Receiving and action on complaints 17. Good governance 20. Duty of candour Principle 3- The NHS aspires to the highest standards of professionalism and excellence. Nil Nil Nil Senior Management Group 29 th September 2016 Page 2 of 2 73
21 Integrated Quality Report August SAFE CARE 1.1 CARDIAC ARRESTS Current Performance Cardiac Arrests per thousand admissions (excluding ED, CCU and CTC) performance was 1.1 in July and in August was Performance over time 3 Number of Cardiac arrests per 1000 admissions(excludes CTC, Critical care and ED) The number of cardiac arrests have remained static. However, per 1000 bed days has increased due to reduced admission numbers arrests per 1000 admissions NCCA Average For the actual number of cardiac arrests occurring, there were 7 in July and 4 in August Sharing the learning & Implementing change Following actions taken to reduce deterioration in patients, many interventions have been initiated which has reduced the cardiac arrest data from 3.09 on August 2014 to 1.37 in August Number of cardiac arrests(excluding CTC, ED and Critical Care) number of cardiac arrests 8 The deteriorating patient project has multi divisional sign up. Sepsis care bundles have shown improvements in Emergency Department and Paediatrics Cardiac arrest reviews are monitored throughout divisions. The MDT team are reviewing medical and surgical cardiac arrests. Recently the incident forms raised have been for patients who had a DNACPR order which was not followed. E-observations are live on all adult wards excluding the CTC, which has a planned roll out once large TV screens are delivered and installed. 74
22 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug SAFE CARE 1.2 PRESSURE ULCERS Current Performance There were 3 grade 2 pressure ulcers declared preventable in August (2 grade 2s and 1 grade 3 in July) Performance over time Until the spike in avoidable pressure ulcers in November, there had been a month-on-month improvement in performance. The programme of work developed for Linford ward has been rolled out to Edith Cavell and Marjory Warren Analysis of performance, sharing the learning & implementing change Performance is on trajectory with 3 preventable pressure ulcers in August (3 in July). All incidences were deemed low impact. All grade 2 and above pressure ulcers are subject to RCA investigation and are reviewed by the Harm Free Care Scrutiny Group. The RCAs from the August have identified insufficient evidence that the patients heels were elevated prior to the pressure ulcers occurring. A number of actions have been identified/planned including: both wards to remind their staff of the importance of heel floatation; the Tissue Viability Team has sourced a new heel protecting device that may increase patient compliance and a trial has commenced; teaching delivered to the ANTs (link nurses) on heel ulcer assessment and prevention strategies; micro teaching slides to be developed to enable the ANTs to deliver teaching in their clinical environment. The following graph shows the total number of avoidable pressure ulcers by Grade. Total Avoidable Hospital Acquired Pressure Ulcers 2015/16 & 2016/17 Total G2 G3 G
23 1. SAFE CARE 1.3 FALLS Current Performance The Royal College of Physicians national audit report was published in October and provides the most current benchmark for total patient falls at a national rate of 6.63 falls per 1000 bed days. To date the Trust s performance continues to remain below the new national average set following the Royal College of Physicians of 6.63 falls/per 1000 bed days and below the local benchmark of For August there were no falls with severe Performance over time To date, activity versus falls demonstrates that the Trust consistently performs well against the national standard of 6.63 falls/1000 bed days set in the RCP audit of Inpatient falls. In August there were 4.6 falls per 1000 bed days. The proposed Sign Up to Safety KPI is to continue to reduce falls that result in severe injury by 50% by 2017/18 (based on the 2014/15 baseline of 28 injurious falls). In 2015/16 the target (25% reduction) was over achieved with 19 injurious falls against a target of 21. In 2016/17 the trajectory has been set at 17 injurious falls (40% reduction on 2014/15 baseline). In August there were no injurious falls resulting in severe harm (none in July). 5 BTUH Severe Injurious Falls May August Analysis of performance The Sign up to Safety workbook and KPIs remain on track and the workbook is rated as green. The Falls Safe Project team are delivering against their expected key milestones. Roll out continues to plan with all inpatient adult wards being on track to complete by end November. The assessment units will come on board in December. Competency framework plans are under review in light of the seconded individual leaving the Trust Falls with harm benchmarking Patient Safety Thermometer activity will differ from local measures, as it includes all levels of harm from minor (i.e. graze, contusion) to severe (i.e. fracture neck of femur, cerebral haemorrhage), and only on the basis of a snap shot audit once per month, this does therefore not provide a constant assessment of the overall level of injury. PST performance demonstrates the Trust is above the national benchmark. 76
24 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar SAFE CARE 1.4 Infection Prevention & Control Current Performance There was one case of MRSA bacteraemia reported in August. This case has been reviewed by the PIR process and was deemed avoidable. The case identified many areas for action and a robust action plan is being monitored through the Infection Control Committee. Four Clostridium difficile infection cases were reported in August. An MDT was undertaken on all cases and no lapses in care have been identified Performance over time The two graphs below show the Trust performance for MRSA Bacteraemia and Clostridium difficile for 2016/17. All cases of MRSA and C. Difficile infections are subject to detailed RCAs which ascertain if there were any aspects of care which failed to meet the required standards. Total Acquired C.Difficile Infections (monthly and cumulative) 2015/16 & 2016/17 Monthly Cumulative MRSA Bacteraemia (cumulative) (monthly and cumulative) 2015/16 & 2016/17 Cumulative Analysis of performance MRSA Bacteraemia There has been one case of MRSA Bactereamia Clostridium difficile The C.difficile objective for 2016/17 is set at 31 post 72 hour cases, of which there have been 10 cases to date. To comply with the Code of Practice, Criterion 1: Systems to manage and monitor the prevention and control of infection, Root Cause Analysis (RCA) have been undertaken and these are scrutinised at multi-disciplinary review meetings which include the Clinical commissioning Group (CCG). 77
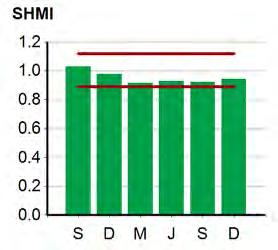
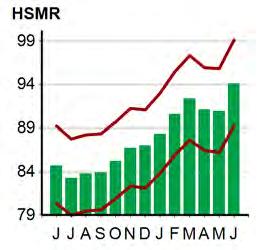
25 2. EFFECTIVE CARE 2.1 MORTALITY Current Performance Crude Mortality The Crude mortality rate for the rolling 12-month period June 2015 May 2016 is 1.92% and remains below the 2% target threshold. There was a reduction in the in-month figure with 1.74% in August compared to 1.91% in July. Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Total deaths Total discharges In-month Crude Mortality Rate 1.84% 1.74% 2.03% 1.77% 1.85% 2.36% 2.23% 2.13% 1.96% 1.87% 1.72% 1.91% 1.74% 12 Month Rolling Crude Mortality 1.89% 1.91% 1.96% 1.97% 1.92% 1.91% 1.92% 1.95% 1.93% 1.91% 1.91% 1.95% 1.95% HSMR The latest published position of HMSR for the 12 month rolling period is July 2015 to June 2016 is 93.86%, which is in the lower than expected banding. SHMI Data from HED shows SHMI at for period January-December When compared to East of England peers, the Trust is one of eight Trusts (out of 17) with SHMI below the 1000 threshold value Performance over time Crude Mortality The Crude mortality rate for the rolling 12- month period is 1.95% and remains below the 2% target threshold since November HSMR The latest published position HSMR for the 12-month rolling period, July 2015 to June 2016 is 93.86%, which is lower than expected. The HMSR trend overall appears to be static and below the 100% threshold. SHMI The SHMI preview has been released for January 2015 to December 2015 and is at 94, the banding is within expected range. For the fifth consecutive period the Trust remains below the 100 threshold. 78
26 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug EFFECTIVE CARE 2.2 DEMENTIA SCREENING Current Performance The Dementia Assessment Proforma must be completed on admission for all patients aged 75years a and over admitted as an emergency (excluding day cases). Patients unable to participate in an AMT due to impaired consciousness, critical illness or sensory impairment can be excluded. Compliance with the AMT 90% target was achieved in August at 95.23% (94% in July) % 95.00% 90.00% Dementia Assessments 85.00% 80.00% Target Compliance 75.00% In August, assessments were carried out on 23 wards. 18 wards achieved the target with many achieving 100% compliance. Wards not achieving the target were:- AMU East: 67% Elsdon: 75% Florence Nightingale: 81% Pasteur: 89% William Harvey: 86% Wards are asked to review results at their 2 at top ward meetings % 80.00% 60.00% 40.00% 20.00% 0.00% Assessments by Ward - August 2016 (datasource: PAMSBi 28/9/16) Learning and Implementing Change The Dementia Nurse has reminded the ward teams that they are responsible for copleting the assessments and that the data is uploaded to EPR 79
27 3. PERSONAL & RESPONSIVE CARE 3.1 PATIENT SATISFACTION The Trust uses a variety of sources of information to assess how we could do things differently to improve patient experience, capturing patient feedback via Friends & Family Test (FFT), We re Listening comment cards, NHS Choices, BTUH Feedback address, Facebook, Twitter, Complaints, PALS and Plaudits. Friends & Family Test (FFT) Inpatient response rate (40%) was not achieved at 33% in August representing a reduction from 37% in July. FFT results have identified that Day Case totals have been detrimental to the Trust overall response rates. The response rates for day case areas in August were:- Renal Unit Not available* BDU 38% CDU 33% Colposcopy 21% Endoscopy 14% Gynae 20% Haematology 0% Orsett DDU 10% Rheumatology 12% Thames 11% Grand Total 18% The Head of Patient Experience has discussed the results with the relevant areas and proposed actions for improving response rates. The Matron for Day Surgery has confirmed the FFT will be a standing agenda items for her admin and nurse team meetings. The results for paediatric wards has remained low. This has been due to the delay in submitting discharge information for Puffin and Wagtail wards to Healthcare Communications. This will be raised with the Trust s Information team and progress confirmed at a meeting with Healthcare Communication on 19th September. It should be noted that removing the Day Case and Paediatric ward totals, the Trust inpatient response rate was 49%. Notable improvements in areas where the response rate was not previously achieved included: AMU-East, Elizabeth Fry and Marjory Warren. The response rate is based on the number of discharges per ward and FFT forms received. James Mackenzie ward continue to report response rates above the discharge rates. This has occurred due to patients who have been transferred from the ward to elsewhere in the hospital completing the FFT forms. The ward has been reminded that these patients do not count as discharges and therefore should not be given a form the ward Bulphan, Lionel Cosins, Orsett and SRU are adult inpatient areas that experienced reductions in their response rates in August and did not achieve the 40% target. Maternity consistently achieves and exceeds the 15% response rate target. The response rate increased from 72% in July to 77% in August. There was an improvement in the A&E response rate target (20%) which has achieved and exceeded at 20.2% in July and 21.2% in August. 80
28 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 No. of new concerns Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 No. of new complaints May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 No. of plaudits logged Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 No. of postings 3. PERSONAL & RESPONSIVE CARE NHS Choices The total number of comments posted on the NHS Choices website was 8 in July and 9 in August. 9 of these were 5 star ratings. Comments included: NHS Choices 2015/16 & 2016/17 Total 5* Rating Cannot praise Breast Cancer Unit enough! Cannot praise the staff enough - all of them were incredibly friendly, amicable, trusting and made me go from feeling a nervous wreck on arrival to safe and in the correct care. Turnaround was very quick from Consultation to mammogram to ultrasound. Really wonderful unit and cannot thank not praise them enough! Thank You again! Visited in August Posted on 16 August Plaudits In addition to those logged, individual wards/ departments also receive a number of cards and letters. 80 Total Number of Formal Plaudits 2015/16 & 2016/17 A total of 33 plaudits were logged in July. Plaudits related to the standards of care provided to patients by nursing and medical staff. No plaudits were logged in August. This was due to unexpected staffing concerns whereby both PALS/Complaints were under 50% of usual staffing and concerns/complaints were prioritised. The August plaudits will be added at a later stage There is an increase in plaudits logged year to date compared to the same period in 2015/16. In addition to those logged, individual wards/departments also receive a number of cards and letters. 3.2 COMPLAINTS & PALS Current Performance 80 Total Number of Complaints 2015/16 & 2016/17 The Trust experienced a 21% increase in the number of complaints received with 75 in August compared to 62 in July. This equates to a 24% increase year to date on new complaints received for the same period in 2015/ There was a 5.4% increase in PALS cases logged with 292 in August compared to 277 in July. The total year to date is 6.7% higher than for the same period in 2015/ Total Number of PALS Concerns 2015/16 & 2016/
29 Dermatology Endocrinology Endoscopy Gastroenterology General Medicine Neurology Osler Pulmonary Physiology & Sleep Respiratory Medicine Rheumatoloy Bulphan Colorectal ENT Fracture Clinic/Ortho OPD General Surgery Neurology Oral Surgery Pain Management Surgical Doctors Trauma & Orthopaedics Urology Acute Medicine Cardiothoracic Services Clinical Support Services Environment & Infracstructure IPP Medicine QIPS Surgical Services Women & Children Other 3. PERSONAL & RESPONSIVE CARE % Divisional Complaints & PALS against Trust Total July-August 2016 Complaints % PALS % 40% 30% 20% 10% 0% Complaints Medical care/treatment Medical judgement/diagnosis Communication Attitude Clinical delay/waiting time PALS Appt delay/cancellation OPD Communication Diagnostic Tests Clinical Treatment Operation delay/cancelled August (July) 16 (19) 11 (12) 11 (8) 9 (4) 9 (6) 133 (94) 42 (48) 25 (24) 16 (25) 17 (1) Comments Medical Care/Treatment remains the highest complaint category. There was a notable increase in complaint relating to Attitude, from across all clinical divisions except Medicine, and across all staff groups. There was a significant increase in PALS cases logged under Appointment delay/cancellation OPD. This category remains the highest for all PALS cases logged. The highest proportion of those received in August related to Medicine and Surgical Services. Dermatology received the highest number of PALS concerns relating to appointment delay/cancellation OPD. The Quality Improvement Team is supporting the Medicine Division, reviewing dermatology processes including staffing Appointment delay/cancellation OPD July-August 2016 Medicine Surgical Services PALS cases relating to Communication and Diagnostic Tests remain static. There was a notable increase in PALS cases relating to Operation delay/cancelled. The highest proportion of these related to Surgical Services. The delays in Surgical Services have been attributed to capacity issues and consultant leave. The Theatre Manager is working with teams to arrange additional Saturday lists, where possible for all specialties. 82
30 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 No. of reopened complaints Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 % of upheld complaints 3. PERSONAL & RESPONSIVE CARE Acknowledgements 100% of complaints received in August were acknowledged within the statutory 3 working day target 100% of PALS concerns received in August were acknowledged within the Trust-imposed 24hours target. Responded to on time Target (90%) for complaints responses sent within agreed date was achieved with 94% in August (96% in July). The Trust achieved 81% in August (85% in July) against the Trust imposed target of resolving 90% of PALS concerns within 5 working days. Complaints Upheld There was a significant reduction in the percentage of upheld complaints with 11% (4 of 38 complaint responses) in August compared to 24% (14 of 58 responses) in July. 60% 50% % of Upheld Complaints against Responses sent 40% Many of the cases closed resulted in the identification of actions and learning. Actions from complaints are recorded on Ulysses Trusts risk database. The Complaints Team now meet weekly with Divisional leads to review of progress against actions and support closure of complaints. 30% 20% 10% 0% Trends Identified in Complaints Actions taken Stage Issues surrounding patients having to repeat information Training for staff regarding the data based in Anticoagulation Completed Communication to patients Rebuilding programme for Phlebotomy Ongoing Consultant capacity resulting in delays Communication issues Offering patients alternative surgeons with shorter waiting times Review of pre-assessment process undertaken and some basic patients receiving telephone assessments Completed Ongoing Complaints reopened There was an increase in requests for additional investigation on closed complaints with 10 in August compared to 7 in July. All complainants are given the opportunity to meet clinicians to discuss their experience, their concerns and to explain the content of complaint responses. There was also an increase in requests for local resolution meetings with 6 in August (4 in July) Reopened Complaints 0 83
Integrated Performance Report August 2017
 Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
BSUH INTEGRATED PERFORMANCE REPORT. 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain
 Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain") BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
1.1.2 Performance over time
 01/2015 02/2015 03/2015 04/2015 05/2015 06/2015 07/2015 08/2015 09/2015 10/2015 11/2015 12/2015 01/2016 02/2016 03/2016 04/2016 Number of Cardiac Arrests 01/04/2015 01/05/2015 01/06/2015 01/07/2015 01/08/2015
01/2015 02/2015 03/2015 04/2015 05/2015 06/2015 07/2015 08/2015 09/2015 10/2015 11/2015 12/2015 01/2016 02/2016 03/2016 04/2016 Number of Cardiac Arrests 01/04/2015 01/05/2015 01/06/2015 01/07/2015 01/08/2015
Integrated Performance Report
 Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Strategic KPI Report Performance to December 2017
 Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018
 Produced in February 2018") 6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
Section 1 - Key Performance Indicators
 Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
Summarise the Impact of the Health Board Report Equality and diversity
 AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
Quality & Performance Report. Public Board
 Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
Governing Body. TITLE OF REPORT: Performance Report for period ending 31st December 2012
 - Governing Body DATE OF MEETING: TITLE OF REPORT: Performance Report for period ending 31st December 2012 KEY MESSAGES: We are responsible for securing improvements in the quality of care and health outcomes.
- Governing Body DATE OF MEETING: TITLE OF REPORT: Performance Report for period ending 31st December 2012 KEY MESSAGES: We are responsible for securing improvements in the quality of care and health outcomes.
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
Integrated Performance Report
 Mid Essex, Southend and Basildon Hospitals Joint Working Board 05/04/2017, 2pm Integrated Performance Report February 2017 Mid Essex, Southend and Basildon Hospitals Introduction by CEO February 2017 The
Mid Essex, Southend and Basildon Hospitals Joint Working Board 05/04/2017, 2pm Integrated Performance Report February 2017 Mid Essex, Southend and Basildon Hospitals Introduction by CEO February 2017 The
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Newham Borough Summary report
 Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
WAITING TIMES AND ACCESS TARGETS
 NHS Board Meeting Tuesday 17 February 2015 Chief Officer (Acute Services) Board Paper No.15/08 WAITING TIMES AND ACCESS TARGETS Recommendation: The NHS Board is asked to note progress against the national
NHS Board Meeting Tuesday 17 February 2015 Chief Officer (Acute Services) Board Paper No.15/08 WAITING TIMES AND ACCESS TARGETS Recommendation: The NHS Board is asked to note progress against the national
INTEGRATED PERFORMANCE REPORT. BOARD OF DIRECTORS 20 September 2017
 INTEGRATED PERFORMANCE REPORT BOARD OF DIRECTORS 20 September 2017 1 S Section Page Executive Summary 4 Trust Performance Overview 7 Trust Performance Report by Exception 9 MSSA Bacteraemia - Actual numbers
INTEGRATED PERFORMANCE REPORT BOARD OF DIRECTORS 20 September 2017 1 S Section Page Executive Summary 4 Trust Performance Overview 7 Trust Performance Report by Exception 9 MSSA Bacteraemia - Actual numbers
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 26 March 2018 Financial Management Report for the 11 months to 28 February 2018 Author: Bob Brown, Assistant Director of Finance Governance and Shared Services
Paper 12 Ayrshire and Arran NHS Board Monday 26 March 2018 Financial Management Report for the 11 months to 28 February 2018 Author: Bob Brown, Assistant Director of Finance Governance and Shared Services
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES
 Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Quality Improvement Strategy
 / Colchester Hospital University NHS Foundation Trust Quality Improvement Strategy 2015-2018 Including our four Quality goals Strategy Author Angela Tillett, Medical Director Version 1 Date of Issue -
/ Colchester Hospital University NHS Foundation Trust Quality Improvement Strategy 2015-2018 Including our four Quality goals Strategy Author Angela Tillett, Medical Director Version 1 Date of Issue -
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST
 TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 29 th June 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 29 th June 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
Health Board Report INTEGRATED PERFORMANCE DASHBOARD
 AGENDA ITEM 4.2 27 th January 2016 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact
AGENDA ITEM 4.2 27 th January 2016 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST
 TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 25 th May 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
TAMESIDE & GLOSSOP INTEGRATED CARE NHS FOUNDATION TRUST Report to Public Trust Board meeting of the 25 th May 2017 Agenda Item 7b Title Sponsoring Executive Director Author (s) Purpose Previously considered
Executive Workforce Report
 Executive Workforce Report (v2) Safe & Effective Kind & Caring Exceeding Expectation Agenda Item No: 9.3 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 27 th November 2017 Title: Executive
Executive Workforce Report (v2) Safe & Effective Kind & Caring Exceeding Expectation Agenda Item No: 9.3 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 27 th November 2017 Title: Executive
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Integrated Performance Report
 Mid Essex, Southend and Basildon Hospitals Joint Working Board - 5 th July 17 Integrated Performance Report May 2017 Mid Essex, Southend and Basildon Hospitals Joint Working Board - 5 th July 17 Contents
Mid Essex, Southend and Basildon Hospitals Joint Working Board - 5 th July 17 Integrated Performance Report May 2017 Mid Essex, Southend and Basildon Hospitals Joint Working Board - 5 th July 17 Contents
Integrated Performance Report JULY 2017
 Integrated Performance Report JULY 2017 Executive Summary July 2017 4 hour performance We have made a commitment to sustain a >90 for the delivery of the 4 hour transit time target. This has been challenging
Integrated Performance Report JULY 2017 Executive Summary July 2017 4 hour performance We have made a commitment to sustain a >90 for the delivery of the 4 hour transit time target. This has been challenging
Report to: Trust Board 25 th April Enclosure 4. Title Integrated Performance Report March Sponsoring Executive Director
 Report to: Trust Board 25 th April 2013 Title Integrated Performance Report March 2013 Enclosure 4 Sponsoring Executive Director Author(s) Purpose Previously considered by Peter Herring Chief Executive
Report to: Trust Board 25 th April 2013 Title Integrated Performance Report March 2013 Enclosure 4 Sponsoring Executive Director Author(s) Purpose Previously considered by Peter Herring Chief Executive
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016
 NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Balanced Scorecard. Paper 5.2. TRUST BOARD 24 th September 2015 TITLE EXECUTIVE SUMMARY
 TRUST BOARD 24 th September 2015 TITLE EXECUTIVE SUMMARY Balanced Scorecard The Trust reported an in-month deficit of 0.7m against a deficit budget of 0.6m, resulting in a year to date surplus to 0.2m
TRUST BOARD 24 th September 2015 TITLE EXECUTIVE SUMMARY Balanced Scorecard The Trust reported an in-month deficit of 0.7m against a deficit budget of 0.6m, resulting in a year to date surplus to 0.2m
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Performance of the NHS provider sector for the month ended 31 December 2017
 Performance of the NHS provider sector for the month ended 31 December 2017 Contents Overview Performance comparisons 2.4 Employee expenses pay costs 2.5 NHS provider vacancies 1.0 Operational performance
Performance of the NHS provider sector for the month ended 31 December 2017 Contents Overview Performance comparisons 2.4 Employee expenses pay costs 2.5 NHS provider vacancies 1.0 Operational performance
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
Quality & Performance Report Author: John Adler Sponsor: Chief Executive Date: FIC, PPP + QAC 28 th September Executive Summary from CEO
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST PAGE 1 OF 2 Quality & Performance Report Author: John Adler Sponsor: Chief Executive Date: FIC, PPP + QAC 28 th September 2017 Executive Summary from CEO Paper
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST PAGE 1 OF 2 Quality & Performance Report Author: John Adler Sponsor: Chief Executive Date: FIC, PPP + QAC 28 th September 2017 Executive Summary from CEO Paper
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10. Date of Meeting:.24 th March 2017.
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting:.24 th March 2017. TITLE OF REPORT: CCG Corporate Performance Report AUTHOR: Melissa Laskey Director of Service
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting:.24 th March 2017. TITLE OF REPORT: CCG Corporate Performance Report AUTHOR: Melissa Laskey Director of Service
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
2017/18 Trust Balanced Scorecard
 ITEM 8b ENC 9 2017/18 Trust Balanced Scorecard Author: Performance Management Team March 2017 The purpose of this paper is to provide an update on the development of the 2017/18 Balanced Scorecard for
ITEM 8b ENC 9 2017/18 Trust Balanced Scorecard Author: Performance Management Team March 2017 The purpose of this paper is to provide an update on the development of the 2017/18 Balanced Scorecard for
QUALITY REPORT. Part A Patient Experience
 QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
Safer Nursing and Midwifery Staffing Recommendation The Board is asked to: NOTE the report
 To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
ESHT Our ambition to be outstanding by 2020
 ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Bristol, North Somerset and South Gloucestershire Clinical Commissioning Group Governing Body Meeting In-Common
 Bristol, North Somerset and South Gloucestershire Clinical Commissioning Group Governing Body Meeting In-Common Date: Tuesday 7 th November Time: 13.30 Location: Cleve Rugby Club, The Hayfields, Mangotsfield,
Bristol, North Somerset and South Gloucestershire Clinical Commissioning Group Governing Body Meeting In-Common Date: Tuesday 7 th November Time: 13.30 Location: Cleve Rugby Club, The Hayfields, Mangotsfield,
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER C Hickson, Head of Management Accounts
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Quality Improvement Scorecard December 2017
 Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 23 rd March 2017 Agenda No: 9.3 Attachment: 15 Title of Document: CCG Governing Body Assurance Report & Scorecards: Month 9 Quality &
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 23 rd March 2017 Agenda No: 9.3 Attachment: 15 Title of Document: CCG Governing Body Assurance Report & Scorecards: Month 9 Quality &
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST CHIEF EXECUTIVE S REPORT. BOARD OF DIRECTORS 21 st March 2012
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST I CHIEF EXECUTIVE S REPORT BOARD OF DIRECTORS 21 st 212 1. PERFORMANCE In overall terms, the Trust continues to perform well against both regulatory and
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST I CHIEF EXECUTIVE S REPORT BOARD OF DIRECTORS 21 st 212 1. PERFORMANCE In overall terms, the Trust continues to perform well against both regulatory and
NHS Electronic Referrals Service. Paper Switch Off an update Digital Health Webinar 4 May 2018
 NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Integrated Corporate Performance Report. August Page 1 of 9
 Integrated Corporate Performance Report August Page of 9 Integrated Corporate Performance Report... Introduction The Integrated Corporate Performance Report (ICPR) includes: An Executive Summary - highlights
Integrated Corporate Performance Report August Page of 9 Integrated Corporate Performance Report... Introduction The Integrated Corporate Performance Report (ICPR) includes: An Executive Summary - highlights
Health Board Report INTEGRATED PERFORMANCE DASHBOARD
 AGENDA ITEM 4.4 2 nd March 2016 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact
AGENDA ITEM 4.4 2 nd March 2016 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact
Quality Improvement Scorecard February 2017
 Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016)
 HR & OD Monthly Trust Report (September 2016)") Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016) Prepared by: Karen Taylor, Assistant Director of HR & Kyriacos Kyriacou, Interim Deputy Director of HR & OD Presented by: Louise Ludgrove,
Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016) Prepared by: Karen Taylor, Assistant Director of HR & Kyriacos Kyriacou, Interim Deputy Director of HR & OD Presented by: Louise Ludgrove,
Integrated Performance Report December 2015
 Portsmouth Hospitals NHS Trust QAH Hospital Page 1 Integrated Performance Report December 2015 Portsmouth Hospitals NHS Trust QAH Hospital Page 2 Contents Section Page 1 Performance Outcomes 3 2 Quality
Portsmouth Hospitals NHS Trust QAH Hospital Page 1 Integrated Performance Report December 2015 Portsmouth Hospitals NHS Trust QAH Hospital Page 2 Contents Section Page 1 Performance Outcomes 3 2 Quality
Waiting Times Report Strategic. Thematic Goals
 Strategic Improved Quality of Care Transformation - Prevention & Wellbeing Thematic Goals Waiting Times Report 2016-17 Transformation through Integration Improved Access to Services Improved Value This
Strategic Improved Quality of Care Transformation - Prevention & Wellbeing Thematic Goals Waiting Times Report 2016-17 Transformation through Integration Improved Access to Services Improved Value This
Quality Improvement Scorecard November 2017
 Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
April Clinical Governance Corporate Report Narrative
 April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST
 EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations
 No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017
 Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Trust Key Performance Indicators
 Monthly - February 2007 Patient Experience Length of Stay - Overall A Mortality Rate G Cancelled Operations R Elective A Peri-operative Mortality Rate Cancelled Operations (28 day reschedule) A Non-elective
Monthly - February 2007 Patient Experience Length of Stay - Overall A Mortality Rate G Cancelled Operations R Elective A Peri-operative Mortality Rate Cancelled Operations (28 day reschedule) A Non-elective
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
The Royal Wolverhampton NHS Trust
 Title: Safe Staffing; Planned Versus Actual Staffing by Ward September 2016 data The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 31 st October 2016 Title: Nursing Workforce Report Executive
Title: Safe Staffing; Planned Versus Actual Staffing by Ward September 2016 data The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 31 st October 2016 Title: Nursing Workforce Report Executive
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Performance of the NHS provider. sector for the quarter ended 30. June 2018
 Performance of the NHS provider sector for the quarter ended 30 June 2018 Contents Overview at Q1 2018/19 Performance comparisons 2.3 Income analysis 2.4 Employee expenses pay costs 1.0 Operational performance
Performance of the NHS provider sector for the quarter ended 30 June 2018 Contents Overview at Q1 2018/19 Performance comparisons 2.3 Income analysis 2.4 Employee expenses pay costs 1.0 Operational performance