Agitation Transformation
|
|
|
- Benjamin Bryan
- 5 years ago
- Views:
Transcription
1 VA Portland Health Care System Agitation Transformation Improving Behavioral Documentation on an Inpatient Psychiatric Unit Courtney Covey Lewis, RN-BSN
2 Background Project began as part of the OHSU/VA Evidence Based Practice Fellowship Develop a quality improvement project to be implemented at unit level, using EBP Attended multiple workshops Worked with Molly Archer as mentor
3 Background 5C is a 23 bed acute psychiatric unit at the Portland VA Population of Veterans Average age of 51, but ranges from early 20s to 90s Receive treatment for variety of mental health needs: Depression and suicidality, substance abuse and withdrawal, major mental illness like schizophrenia or bipolar disorder Primary focus is crisis management and stabilization
4 Background cont. This project was initially about introducing sensory based care interventions on 5C Evidence based with solid research Supported by nurses and administration However

5 The Problem The standard nursing documentation made it almost impossible to systematically evaluate the efficacy of any new intervention
6 Nursing documentation consists of a short template done every shift, and relies heavily on a narrative summary - This allows a nurse to document in detail the course of a patient s day - Inconsistent from nurse to nurse - No standardized tracking of patient behavior, and little quantifiable data in shift charting
7 For Example: Mr. B Pt mildly agitated. Recv d PRN olanzapine with moderate effect at Denies SI/HI, petc. 4 hr sleep. 0730: Pt resting in room when author assumed care at Pt appears groggy and unsteady on feet at beginning of shift at Pt awake and pacing room by 0800 but remained in room until At 0900, pt walked down to nursing station requesting cowboy boots- pt on a hospital hold so policy does not permit him to have his own cowboy boots. When request was declined, pt yelling stating "do you need me to raise my voice!" and returned to room. Pt then came back up to nursing station yelling "call the police! Call the police now!" and throwing items and linen on the ground. Pt agreeable to PRN Olanzapine 10mg PO. 1000: Pt later apologetic for cursing and behaviors stating "I'm sorry, I never meant to be so grumpy". 1100: Pt awake in room. Pt pleasant and complimenting staff ( Thank you, you girls take good care of me ) after receiving PRN Olanzapine 10mg (appears effective), although pt intermittently noted to be cursing quietly. 1200: Pt continues to talk softly and in whispered tones, difficult to understand at times. Pt appears less groggy. Pt visible in large day room.
8 The Problem, continued Nurses also lack confidence in the quality of current documentation In a survey given to 5C nurses, only 30% of responders reported that 5C nurses usually document all interventions performed for patients Only 35% felt that current documentation accurate reflects what nurses do 70% felt that documentation was regularly inconsistent, and 50% found the nursing progress note to be uninformative.
9 The Pittsburgh Agitation Scale Based on a review of available tools, the Pittsburgh Agitation Scale (PAS) was found to be the most appropriate for our population Developed in 1994, validated in a variety of settings, high inter-rater reliability Takes 1 minute or less to complete per patient Easy and intuitive to learn Standard of practice in Australia for monitoring patients with dementia
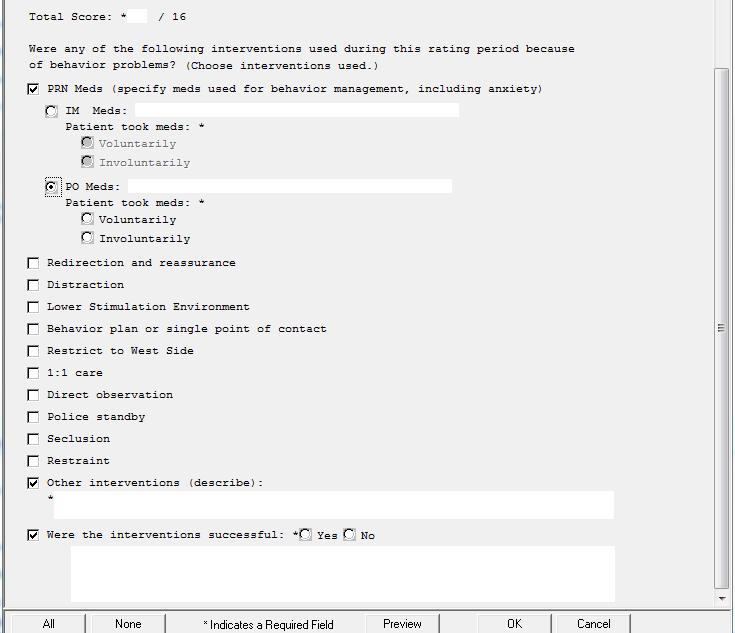
10 The PAS Measures 4 dimensions of agitated behavior Each dimension is rated from represents normal or absent behavior, 4 represents extreme example of agitated behavior Score is added for a total of 16 possible points Aberrant Vocalization Crying, shouting, inappropriate communication Motor Agitation Pacing, rate of movement, exit seeking Aggression Threats, physical violence Resistance to Care Procrastination, refusal, striking out during care
11 The PAS The PAS also requires the nurse to list what interventions were used to manage behavior Non pharmacological intervention Redirection, reassurance, therapeutic companion, lower stimulation, behavior plan, distraction Medication Was it by mouth or injectable? Did the patient willingly take the med? Restraint or seclusion
12 Data Tracking Organized into month and overall Review scales done, gather information from MD discharge summary Tracking patient demographics, diagnosis, highest and average scores Falls, forced medication, restraint and seclusion What percent of nursing notes have a completed PAS
13 Implementation Worked with IT to convert the PAS into a template Template went live early April 2015 Began education in-services in April minute sessions with time to practice the PAS on hypothetical patients Friendly competition and prizes to encourage compliance

14
15 Training Example Ms. J spent about 45 minutes in the day area this morning, crying softly. She was redirected back to her room, where she was noted to pace for about an hour. She refused lunch and afternoon meds, but later took her afternoon medications with her dinner time meds, as well as a PO PRN for anxiety. She appeared less tearful in the evening and was present in the milieu, but minimally interactive with staff and peers. Scores for Vocalization: 1, Motor Agitation: 2, Aggressiveness: 0, Resisting Care: 2 Total Score: 5 Nurse interventions performed: redirection, medication for anxiety
16 Challenges Under-rating Confusing aggression with agitation Missing resisting care Compliance New charting is always a challenge Not well integrated into charting Currently an additional template
17 Data Average of all scores since implementation is 1.1 Varies from month to month between an average of.8 to 1.4 Most common admission diagnosis for all patients is a substance abuse disorder Usually in conjunction with other mental health symptoms
18 Admission Diagnosis by Category Mania or Bipolar Spectrum 7% PTSD 7% Other or unspecified NOS 12% Substance Use D/O 26% Personality or Adjustment D/O 12% Depressive D/O or SI 15% Schzo D/O or Psychosis 21%
19 Data Veterans divided into two groups, sub-acute and acute Acute group are the veterans that have at least one score of 6 or greater during admission Why 6? Represents at minimum one episode of moderate agitation in two categories, and at least mild agitation in two others
20 Training Example, PAS of 6 Mr. D is confused, oriented to self only. He paces the hallway, and checks all the doors on the unit. He wanders into another veteran s room, and attempts to sleep in the peer s bed. The other veteran is upset, and yells at Mr. D to get out. Mr. D then spends the rest of the shift at the nurses station, trying to enter and asking for his wallet and calling out for his wife. Not directible to his room, but he is distracted by snacks in the small day area. Vocalization: 2 Motor Agitation: 3 Aggressiveness: 0 Resisting Care: 1 Total Score: 6
21 Training Example, PAS of 16 Ms. L was found in her room, attempting to fashion a ligature out of her sheets. She was placed on a hold, and moved to a security room, where she began to disrobe and rhythmically pound her head against the wall. When staff approached her to offer her fluids and PO medication, she lunged at a staff member while screaming. Due to this and the attempted self-harm, she was placed in 4 point restraints and given IM medication. She screamed and attempted to strike at staff for another 20 minutes before falling asleep. Vocalization: 4 Motor Agitation: 4 Aggressiveness: 4 Resisting Care: 4 Total Score: 16
22 Acute Group 107 out of 526 patients between April 2015 and January % of total admissions 24% of September admissions Average length of stay is 14.3 days Sub acute group average length of stay is 4.9 days
23 Acute Group Most common diagnosis for the acute group is schizophrenia/schizoaffective/psychotic disorders. Majority of the group are admitted involuntarily Higher rate of falls 26% have a neurocognitive disorder 13% of subacute group have a neurocognitive group
24 Feedback Nurses overwhelmingly report the tool as useful Integrating information in staffing methodology Interdisciplinary team uses data as well SW placement PRN medication usage
25 Next Steps Use the data! Sensory care/calming room Use data to evaluate new interventions Aromatherapy pilot project Improve practice and safety for staff and patients Create a protocol to manage acute patient group More frequent assessment Additional intervention Fall precautions for acute patients
26 Acknowledgements and References Mador, J., E., Giles, L., Whitehead, C., & Crotty, M. (2004). A randomized controlled trial of a behavior advisory service for hospitalized older patients with confusion. International Journal of Geriatric Psychiatry, 19(9), Rosen, J., Bobys, P. D., Mazumdar, S., Mulsant, B. H., Sweet, R. A., Yu, K., et al. (1999). OBRA regulations and neuroleptic use: Defining agitation using the pittsburgh agitation scale and the neurobehavioral rating scale. Annals of Long Term Care, 7(12), Rosen, J., Burgio, L., Kollar, M., Cain, M., Allison, M., Fogleman, M., et al. (1994). The pittsburgh agitation scale: A User Friendly instrument for rating agitation in dementia patients. The American Journal of Geriatric Psychiatry, 2(1), Zieber, C. G., Hagen, B., Armstrong-Esther, C., & Aho, M. (2005). Pain and agitation in long-term care residents with dementia: Use of the pittsburgh agitation scale. International Journal of Palliative Nursing, 11(2), Thanks to Molly Archer, the staff of 5C, and everyone involved with the VA/OHSU EBP Fellowship This material is the result of work supported with resources and the use of facilities at the VA Portland Health Care System, as a part of the Evidence Based Practice Fellowship collaboration between OHSU and the VA Portland Health Care System. This project was reviewed by the VA Portland Health Care System Research and Development Service and it was determined to not be research. No further research approvals were required. The contents of this presentation do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Behavioral Rapid Response Team
 May 2017 Behavioral Rapid Response Team Inpatient Behavioral Health Unit (IBHU) Presenters Michael Gallagher, BSN, NE-BC Director of Behavioral Health Services Michelle Gardner, BSN, RN-BC, NE-BC Clinical
May 2017 Behavioral Rapid Response Team Inpatient Behavioral Health Unit (IBHU) Presenters Michael Gallagher, BSN, NE-BC Director of Behavioral Health Services Michelle Gardner, BSN, RN-BC, NE-BC Clinical
Comparison of Violent or Self Destructive vs. Non-Violent Restraints
 Description Restraints can be initiated when unanticipated outbursts of severely aggressive or destructive behavior poses an imminent danger to the patient or others due to an underlying behavioral diagnosis
Description Restraints can be initiated when unanticipated outbursts of severely aggressive or destructive behavior poses an imminent danger to the patient or others due to an underlying behavioral diagnosis
Department of Veterans Affairs VHA DIRECTIVE Veterans Health Administration Washington, DC December 7, 2005
 Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
New OSU Hospital Policy on the Use of Restraints and Seclusion
 University Hospitals Office of the Medical Director 130 Doan Hall 410 West 10 th Avenue Columbus, OH 43210-1228 Phone: (614) 293-8158 FAX: (614) 293-4989 MEMORANDUM DATE: February 7, 2000 TO: FROM: RE:
University Hospitals Office of the Medical Director 130 Doan Hall 410 West 10 th Avenue Columbus, OH 43210-1228 Phone: (614) 293-8158 FAX: (614) 293-4989 MEMORANDUM DATE: February 7, 2000 TO: FROM: RE:
Dial Code Grey Pip3 Male Side This Is The Head Nurse
 Dial 77 88 Code Grey Pip3 Male Side This Is The Head Nurse By Janet Ferguson, PMHCNS-BC, Associate Director Behavioral Health Nursing, and Donna Leno-Gordon, RNMS, MPA, Director Behavioral Health Nursing
Dial 77 88 Code Grey Pip3 Male Side This Is The Head Nurse By Janet Ferguson, PMHCNS-BC, Associate Director Behavioral Health Nursing, and Donna Leno-Gordon, RNMS, MPA, Director Behavioral Health Nursing
Bridging the Gap Between Crisis and Care: How to Effectively Integrate Psychiatric Emergency Care Within a Community Hospital Emergency Department.
 Bridging the Gap Between Crisis and Care: How to Effectively Integrate Psychiatric Emergency Care Within a Community Hospital Emergency Department. Jeannine Loucks, MSN, RN BC PMHN Laura Derr, BSN, RN
Bridging the Gap Between Crisis and Care: How to Effectively Integrate Psychiatric Emergency Care Within a Community Hospital Emergency Department. Jeannine Loucks, MSN, RN BC PMHN Laura Derr, BSN, RN
From Triage to Intervention: A Crisis Care Model for Persons with IDD. Alton Bozeman, Psy.D., Clinical Psychologist Amanda Willis, LCSW-S
 From Triage to Intervention: A Crisis Care Model for Persons with IDD Alton Bozeman, Psy.D., Clinical Psychologist Amanda Willis, LCSW-S Examples of Barriers Lack of information Access to professionals
From Triage to Intervention: A Crisis Care Model for Persons with IDD Alton Bozeman, Psy.D., Clinical Psychologist Amanda Willis, LCSW-S Examples of Barriers Lack of information Access to professionals
Aurora Behavioral Health System
 Aurora Behavioral Health System Decades Program Overview Where healing starts and the road to recovery begins Aurora East 6350 S. Maple Ave. Tempe, AZ 85283 (The hospital is located on the NW corner of
Aurora Behavioral Health System Decades Program Overview Where healing starts and the road to recovery begins Aurora East 6350 S. Maple Ave. Tempe, AZ 85283 (The hospital is located on the NW corner of
ABC s of PES. Greg Miller, MD MBA CMO Unity Center for Behavioral Health
 ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
Supporting Residents Expressing Responsive Behaviours at Home, Hospital, and LTC
 Supporting Residents Expressing Responsive Behaviours at Home, Hospital, and LTC HNHB LHIN Behavioural Supports Ontario Strategy Family Council Network Four (FCN-4) Regional Meeting June 29, 2017 Objectives
Supporting Residents Expressing Responsive Behaviours at Home, Hospital, and LTC HNHB LHIN Behavioural Supports Ontario Strategy Family Council Network Four (FCN-4) Regional Meeting June 29, 2017 Objectives
PURPOSE: In accordance with SB362, Seven Hills Hospital has a documented staffing plan in place which adequately meets the needs of our patients.
 0-6 Title: Staffing Plan 9/8/203 0/29/3, 5/9/4 POC-07 PURPOSE: In accordance with SB362, Seven Hills Hospital has a documented staffing plan in place which adequately meets the needs of our patients. PERFORMED
0-6 Title: Staffing Plan 9/8/203 0/29/3, 5/9/4 POC-07 PURPOSE: In accordance with SB362, Seven Hills Hospital has a documented staffing plan in place which adequately meets the needs of our patients. PERFORMED
EMERGENCY PSYCHIATRY PROCESSES AND PROCEDURES
 EMERGENCY PSYCHIATRY PROCESSES AND PROCEDURES 1. On Call Team and Coverage a. The on call team consists of a junior resident, senior resident and staff psychiatrist. There is also usually a clinical clerk.
EMERGENCY PSYCHIATRY PROCESSES AND PROCEDURES 1. On Call Team and Coverage a. The on call team consists of a junior resident, senior resident and staff psychiatrist. There is also usually a clinical clerk.
The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing
 The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing Sharon P. Stetz MSN Marvella M. Muzik, MS PMHNP, BC Objectives
The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing Sharon P. Stetz MSN Marvella M. Muzik, MS PMHNP, BC Objectives
Organization: Solution Title: Program/Project Description, including Goals: What is this project? Why is this project important?
 Organization: Hebrew Home of Greater Washington (The Charles E. Smith Life Communities) The Hebrew Home provides post-acute services and long-term care to a daily average census of 500 residents. The Home
Organization: Hebrew Home of Greater Washington (The Charles E. Smith Life Communities) The Hebrew Home provides post-acute services and long-term care to a daily average census of 500 residents. The Home
PASRR IN SKILLED NURSING Regulatory Overview
 PASRR IN SKILLED NURSING Regulatory Overview What is the GOAL of the federally mandated PASRR? Facilitate nursing facilities in their effort to provide the necessary care and services to each resident
PASRR IN SKILLED NURSING Regulatory Overview What is the GOAL of the federally mandated PASRR? Facilitate nursing facilities in their effort to provide the necessary care and services to each resident
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
APNA elearning Center October 2017
 APNA elearning Center October 2017 New APNA elearning Center Platform! Active for the APNA Transitions in Practice Certificate Program starting 1st, then after migration of 150+ sessions from our previous
APNA elearning Center October 2017 New APNA elearning Center Platform! Active for the APNA Transitions in Practice Certificate Program starting 1st, then after migration of 150+ sessions from our previous
How can we provide the same world class care to patients with psychiatric disorders? 11/27/2016. Dec 2016 Orlando, FL
 The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
Link download full: Test bank for Varcarolis's Canadian Psychiatric Mental Health Nursing 1e Edition by Margaret Jordan Halter
 Varcarolis s Canadian Psychiatric Mental Health Nursing: Canadian Edition Test Bank Halter Link download full: Test bank for Varcarolis's Canadian Psychiatric Mental Health Nursing 1e Edition by Margaret
Varcarolis s Canadian Psychiatric Mental Health Nursing: Canadian Edition Test Bank Halter Link download full: Test bank for Varcarolis's Canadian Psychiatric Mental Health Nursing 1e Edition by Margaret
The speaker has no conflict of interest to disclose.
 APNA 3th Annual Conference Session 233: October 2. 216 The Effects of two Nursing Protocols on the Use of Continuous Special Observation Presented at: APNA 3 th annual Conference Presented on: October
APNA 3th Annual Conference Session 233: October 2. 216 The Effects of two Nursing Protocols on the Use of Continuous Special Observation Presented at: APNA 3 th annual Conference Presented on: October
The DON s & DSW s Roles in Preventing Resident to Resident Altercations
 The DON s & DSW s Roles in Preventing Resident to Resident Altercations LeadingAge New York Presenter: Linda Elizaitis, President CMS Compliance Group, Inc. T: 631.692.4422 E. lmelizaitis@cmscg.net W.
The DON s & DSW s Roles in Preventing Resident to Resident Altercations LeadingAge New York Presenter: Linda Elizaitis, President CMS Compliance Group, Inc. T: 631.692.4422 E. lmelizaitis@cmscg.net W.
Behavioural Supports Ontario (BSO)
") Behavioural Supports Ontario (BSO) What does it mean for you? Laurie Fox HNHB BSO Project Implementation Lead Hamilton Health Sciences With I am who I am, so help me continue to be me Dana Vladescu, Manager,
Behavioural Supports Ontario (BSO) What does it mean for you? Laurie Fox HNHB BSO Project Implementation Lead Hamilton Health Sciences With I am who I am, so help me continue to be me Dana Vladescu, Manager,
Absconding and inpatient suicide. Professor of Psychiatric Nursing Institute of Psychiatry
 Absconding and inpatient suicide Len Bowers Professor of Psychiatric Nursing Institute of Psychiatry AWOL/suicide research Literature reviews in 1998 and again in 2010 Exploratory research 1998 Prevention
Absconding and inpatient suicide Len Bowers Professor of Psychiatric Nursing Institute of Psychiatry AWOL/suicide research Literature reviews in 1998 and again in 2010 Exploratory research 1998 Prevention
Maine s Co- occurring Capability Self Assessment 1
 Maine s Co- occurring Capability Self Assessment August 2009 Version 3.3 Date: Rater(s): Time Spent: Agency Name: Program Name: Program Type(s): Level of Care: Address: Contact Person: Title: Telephone:
Maine s Co- occurring Capability Self Assessment August 2009 Version 3.3 Date: Rater(s): Time Spent: Agency Name: Program Name: Program Type(s): Level of Care: Address: Contact Person: Title: Telephone:
POLICY AND PROCEDURE RESTRAINT/SECLUSION, MEDICAL CENTER PATIENT CARE Effective Date: March 2010
 Number: MS 08:03:05 Submitted by: BEHAVIORAL HEALTH CLINICAL PRACTICE TEAM Issuing Department: PATIENT CARE SERVICES Approved By: Reviewed by: Date: Patient Care Practice & 12/09 Outcomes David W. Cress,
Number: MS 08:03:05 Submitted by: BEHAVIORAL HEALTH CLINICAL PRACTICE TEAM Issuing Department: PATIENT CARE SERVICES Approved By: Reviewed by: Date: Patient Care Practice & 12/09 Outcomes David W. Cress,
a. The Care Plan dated 2/16/10 documented the following:
 b. The Plan of Care dated 1/12/10 documented, "Problem: At risk for depression, related to very young to be in long term care facility and permanent brain damage R/T [related to] trauma. Approaches: Arrange
b. The Plan of Care dated 1/12/10 documented, "Problem: At risk for depression, related to very young to be in long term care facility and permanent brain damage R/T [related to] trauma. Approaches: Arrange
UnitedHealthcare Guideline
 UnitedHealthcare Guideline TITLE: CRS BEHAVIORAL HEALTH HOME CARE TRAINING TO HOME CARE CLIENT (HCTC) PRACTICE GUIDELINES EFFECTIVE DATE: 1/1/2017 PAGE 1 of 14 GUIDELINE STATEMENT This guideline outlines
UnitedHealthcare Guideline TITLE: CRS BEHAVIORAL HEALTH HOME CARE TRAINING TO HOME CARE CLIENT (HCTC) PRACTICE GUIDELINES EFFECTIVE DATE: 1/1/2017 PAGE 1 of 14 GUIDELINE STATEMENT This guideline outlines
Vanderbilt & Qsource Webinar Series
 Vanderbilt & Qsource Webinar Series Vanderbilt University Medical Center Vanderbilt University Center for Quality Aging Qsource Session #1: Introduction to Dementia Care & QAPI Session #2: Dementia & Behavioral
Vanderbilt & Qsource Webinar Series Vanderbilt University Medical Center Vanderbilt University Center for Quality Aging Qsource Session #1: Introduction to Dementia Care & QAPI Session #2: Dementia & Behavioral
Decreasing Seclusion and Increasing Restraint and Seclusion Documentation Compliance using LEAN. Sheppard Pratt Health System
 Decreasing Seclusion and Increasing Restraint and Seclusion ation Compliance using LEAN Rick Wallace MSN, RN Associate Director of Clinical Services Jacqueline Williams Porter MBA, RN Unit Director Sheppard
Decreasing Seclusion and Increasing Restraint and Seclusion ation Compliance using LEAN Rick Wallace MSN, RN Associate Director of Clinical Services Jacqueline Williams Porter MBA, RN Unit Director Sheppard
NURSING FACILITY (NF) PASRR II-B NOTIFICATION FORM (To be completed by Nursing Facilities)
 PASRR II-B NOTIFICATION FORM (To be completed by Nursing Facilities)") Attachment A NURSING FACILITY (NF) PASRR II-B NOTIFICATION FORM (To be completed by Nursing Facilities) RESIDENT NAME: J.H. NF NAME: Skilled Nursing Facility of Las Vegas NF DATE OF ADMISSION: 1/1/12 PASRR
Attachment A NURSING FACILITY (NF) PASRR II-B NOTIFICATION FORM (To be completed by Nursing Facilities) RESIDENT NAME: J.H. NF NAME: Skilled Nursing Facility of Las Vegas NF DATE OF ADMISSION: 1/1/12 PASRR
Program of Assertive Community Treatment (PACT) BHD/MH
 BHD/MH") Program of Assertive Community Treatment () BHD/MH Luis Marcano, x5343 Alan Orenstein, x0927 Program Purpose Help individuals with serious mental illness achieve and maintain community integration through
Program of Assertive Community Treatment () BHD/MH Luis Marcano, x5343 Alan Orenstein, x0927 Program Purpose Help individuals with serious mental illness achieve and maintain community integration through
ROTATION DESCRIPTION
 ROTATION TITLE Psychiatry Pediatrics (PGY2) ROTATION DESCRIPTION PURPOSE The psychiatry rotation is designed to allow the resident to further refine skills in therapeutics, pharmacokinetics, drug information,
ROTATION TITLE Psychiatry Pediatrics (PGY2) ROTATION DESCRIPTION PURPOSE The psychiatry rotation is designed to allow the resident to further refine skills in therapeutics, pharmacokinetics, drug information,
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE
 EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division
 Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division SUICIDE RISK ASSESSMENT IN THE EMERGENCY DEPARTMENT May, 2014 Background The Quality and Patient Safety
Commonwealth of Massachusetts Board of Registration in Medicine Quality and Patient Safety Division SUICIDE RISK ASSESSMENT IN THE EMERGENCY DEPARTMENT May, 2014 Background The Quality and Patient Safety
JERSEY SHORE UNIVERSITY MEDICAL CENTER DEPARTMENT OF PSYCHIATRY RULES & REGULATIONS A. QUALIFICATIONS TO BECOME A MEMBER OF THE PSYCHIATRIC DEPARTMENT
 JERSEY SHORE UNIVERSITY MEDICAL CENTER DEPARTMENT OF PSYCHIATRY RULES & REGULATIONS A. QUALIFICATIONS TO BECOME A MEMBER OF THE PSYCHIATRIC DEPARTMENT 1. INITIAL CREDENTIALING, PSYCHIATRISTS Completion
JERSEY SHORE UNIVERSITY MEDICAL CENTER DEPARTMENT OF PSYCHIATRY RULES & REGULATIONS A. QUALIFICATIONS TO BECOME A MEMBER OF THE PSYCHIATRIC DEPARTMENT 1. INITIAL CREDENTIALING, PSYCHIATRISTS Completion
Centralized Intake and Referral Application to Specialty Hospitals
 Centralized Intake and Referral Application to Specialty Hospitals CLIENT INFORMATION **** upon completion of referral please fax to 416-506-0439 **** Client Name: Gender: Male Female Other Client Preferred
Centralized Intake and Referral Application to Specialty Hospitals CLIENT INFORMATION **** upon completion of referral please fax to 416-506-0439 **** Client Name: Gender: Male Female Other Client Preferred
Psychiatric Mental Health Nursing Core Competencies Individual Assessment
 Individual Name: Orientation Start Date: Completion Date: Instructions: -the nurse will rate each knowledge, skill, or attitude (KSA) from 1 (novice) to 5 (expert) in each box. Following orientation or
Individual Name: Orientation Start Date: Completion Date: Instructions: -the nurse will rate each knowledge, skill, or attitude (KSA) from 1 (novice) to 5 (expert) in each box. Following orientation or
A PSYCHOTIC EPISODE: DRUG INDUCED? LESSONS FROM ONE CASE
 A PSYCHOTIC EPISODE: DRUG INDUCED? LESSONS FROM ONE CASE SUMMARY A middle-aged man complained to the Grand Jury that he was mistreated and possibly endangered when placed on an involuntary 72-hour hold
A PSYCHOTIC EPISODE: DRUG INDUCED? LESSONS FROM ONE CASE SUMMARY A middle-aged man complained to the Grand Jury that he was mistreated and possibly endangered when placed on an involuntary 72-hour hold
PATIENT AGGRESSION & VIOLENCE BEST PRACTICES NCQC PSO Safe Table July 2015
 PATIENT AGGRESSION & VIOLENCE BEST PRACTICES NCQC PSO Safe Table July 2015 Minimize the impact of patient aggression and violence by focusing on various phases of the care process. RECOGNITION Understand
PATIENT AGGRESSION & VIOLENCE BEST PRACTICES NCQC PSO Safe Table July 2015 Minimize the impact of patient aggression and violence by focusing on various phases of the care process. RECOGNITION Understand
Acute Crisis Units. Shelly Rhodes, Provider Relations Manager
 Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Psychiatric Patients who Abscond from Acute Care. Len Bowers Professor of Psychiatric Nursing Institute of Psychiatry
 Psychiatric Patients who Abscond from Acute Care Len Bowers Professor of Psychiatric Nursing Institute of Psychiatry AWOL research Literature reviews in 1998 and again in 2010 Exploratory research 1998
Psychiatric Patients who Abscond from Acute Care Len Bowers Professor of Psychiatric Nursing Institute of Psychiatry AWOL research Literature reviews in 1998 and again in 2010 Exploratory research 1998
Contents. Introduction 3. Required knowledge and skills 4. Section One: Knowledge and skills for all nurses and care staff 6
 Decision-making frameworks in advanced dementia: Links to improved care project. Page 2 of 17 Contents Introduction 3 Required knowledge and skills 4 Section One: Knowledge and skills for all nurses and
Decision-making frameworks in advanced dementia: Links to improved care project. Page 2 of 17 Contents Introduction 3 Required knowledge and skills 4 Section One: Knowledge and skills for all nurses and
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 8 PURPOSE To provide guidelines on: 1. rating offenders using patient acuity, 2. how to properly handle offenders who are housed in facilities with conflicting acuity levels, 3. how to properly
PAGE 1 of 8 PURPOSE To provide guidelines on: 1. rating offenders using patient acuity, 2. how to properly handle offenders who are housed in facilities with conflicting acuity levels, 3. how to properly
Region 1 South Crisis Care System
 Region 1 South Crisis Care System Region 1 South Crisis Care System Presenters: Lee Ann Reinert, LCSW Clinical Policy Specialist, DHS/DMH Patricia Palmer, LCSW, CADC Clinical Director, Collaborative Author:
Region 1 South Crisis Care System Region 1 South Crisis Care System Presenters: Lee Ann Reinert, LCSW Clinical Policy Specialist, DHS/DMH Patricia Palmer, LCSW, CADC Clinical Director, Collaborative Author:
ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-41 PSYCHIATRIC TREATMENT FACILITIES TABLE OF CONTENTS
 ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-41 PSYCHIATRIC TREATMENT FACILITIES TABLE OF CONTENTS 560-X-41-.01 560-X-41-.02 560-X-41-.03 560-X-41-.04 560-X-41-.05 560-X-41-.06 560-X-41-.07
ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-41 PSYCHIATRIC TREATMENT FACILITIES TABLE OF CONTENTS 560-X-41-.01 560-X-41-.02 560-X-41-.03 560-X-41-.04 560-X-41-.05 560-X-41-.06 560-X-41-.07
4/22/2014. Sheryl Zimmerman, Elsie Norton, Kim Broucksou. Kim Broucksou, MSW, MPA. Cognitive Care Director
 Best Practice Social Work Role Functions in Long-term Care Sheryl Zimmerman, Elsie Norton, Kim Broucksou 1. Psychosocial assessment of residents and family members. 2. Resident and family education. 3.
Best Practice Social Work Role Functions in Long-term Care Sheryl Zimmerman, Elsie Norton, Kim Broucksou 1. Psychosocial assessment of residents and family members. 2. Resident and family education. 3.
Richard E. Ray, MS, RN, PMH BC 1. The speaker has no conflict of interest to disclose.
 The Effects of two Nursing Protocols on the Use of Continuous Special Observation Presented by: Richard Ray, MS, RN, PMH-BC The speaker has no conflict of interest to disclose. Objectives Discuss uses
The Effects of two Nursing Protocols on the Use of Continuous Special Observation Presented by: Richard Ray, MS, RN, PMH-BC The speaker has no conflict of interest to disclose. Objectives Discuss uses
Dr Ihsan Kader & Dr Rachel Brown Edinburgh IHTT IK/RB
 Dr Ihsan Kader & Dr Rachel Brown Edinburgh IHTT 1 Declaration of interest none 2 Plan Brief history and evidence Edinburgh IHTT Challenges including standards Data Quality Improvement Future plans 3 4
Dr Ihsan Kader & Dr Rachel Brown Edinburgh IHTT 1 Declaration of interest none 2 Plan Brief history and evidence Edinburgh IHTT Challenges including standards Data Quality Improvement Future plans 3 4
Note: 44 NSMHS criteria unmatched
 Commonwealth National Standards for Mental Health Services linkage with the: National Safety and Quality Health Service Standards + EQuIP- content of the EQuIPNational* Standards 1 to 15 * Using the information
Commonwealth National Standards for Mental Health Services linkage with the: National Safety and Quality Health Service Standards + EQuIP- content of the EQuIPNational* Standards 1 to 15 * Using the information
MENTAL HEALTH NURSING ORIENTATION. (2) Alleviating disabling symptoms of mental disorders.
 Alleviating disabling symptoms of mental disorders.") Page 1 of 6 1. Mission Statement MENTAL HEALTH NURSING ORIENTATION a. The mission of mental health services is to provide constitutionally adequate care. Mental health care is provided to assist the inmate
Page 1 of 6 1. Mission Statement MENTAL HEALTH NURSING ORIENTATION a. The mission of mental health services is to provide constitutionally adequate care. Mental health care is provided to assist the inmate
Rowan Court. Avery Homes (Nelson) Limited. Overall rating for this service. Inspection report. Ratings. Requires Improvement
 Limited. Overall rating for this service. Inspection report. Ratings. Requires Improvement") Avery Homes (Nelson) Limited Rowan Court Inspection report Silverdale Road Newcastle under Lyme Staffordshire ST5 2TA Tel: 01782622144 Website: www.averyhealthcare.co.uk Date of inspection visit: 16 May
Avery Homes (Nelson) Limited Rowan Court Inspection report Silverdale Road Newcastle under Lyme Staffordshire ST5 2TA Tel: 01782622144 Website: www.averyhealthcare.co.uk Date of inspection visit: 16 May
TENNESSEE S CRISIS RESPITE SERVICES
 TENNESSEE S CRISIS RESPITE SERVICES Tennessee Department of Mental Health and Substance Abuse Services Office of Crisis Services and Suicide Prevention Description A facility-based, voluntary service that
TENNESSEE S CRISIS RESPITE SERVICES Tennessee Department of Mental Health and Substance Abuse Services Office of Crisis Services and Suicide Prevention Description A facility-based, voluntary service that
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
Outcome and Process Evaluation Report: Crisis Residential Programs
 FY216-217, Quarter 4 Outcome and Process Evaluation Report: Crisis Residential Programs April Howard, Ph.D. Erin Dowdy, Ph.D. Shereen Khatapoush, Ph.D. Kathryn Moffa, M.Ed. O c t o b e r 2 1 7 Table of
FY216-217, Quarter 4 Outcome and Process Evaluation Report: Crisis Residential Programs April Howard, Ph.D. Erin Dowdy, Ph.D. Shereen Khatapoush, Ph.D. Kathryn Moffa, M.Ed. O c t o b e r 2 1 7 Table of
[ ] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS.
![[ ] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS.](/thumbs/78/78464102.jpg "[ ] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS.") Sec. 4. [245.8251] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS. Subdivision 1. Rules. The commissioner of human services shall, within 24 months of enactment
Sec. 4. [245.8251] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS. Subdivision 1. Rules. The commissioner of human services shall, within 24 months of enactment
Solution Title Impact on readmission rates of psychiatric patients following pharmacist discharge counseling in a community hospital
 Organization Suburban Hospital Johns Hopkins Medicine Solution Title Impact on readmission rates of psychiatric patients following pharmacist discharge counseling in a community hospital Program/Project
Organization Suburban Hospital Johns Hopkins Medicine Solution Title Impact on readmission rates of psychiatric patients following pharmacist discharge counseling in a community hospital Program/Project
STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT EXECUTIVE SUMMARY
 STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT Prepared by: THE BUCKLEY GROUP, L.L.C. OVERVIEW The Osawatomie State Hospital (OSH) in Osawatomie
STATE OF KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES OSAWATOMIE STATE HOSPITAL OPERATIONS ASSESSMENT Prepared by: THE BUCKLEY GROUP, L.L.C. OVERVIEW The Osawatomie State Hospital (OSH) in Osawatomie
Santa Clara County, California Medicare- Medicaid Plan (MMP)
") Santa Clara County, California Medicare- Medicaid Plan (MMP) Behavioral health overview topics Topics covered: o Behavioral health (BH) covered services overview o BH noncovered services o Early and Periodic
Santa Clara County, California Medicare- Medicaid Plan (MMP) Behavioral health overview topics Topics covered: o Behavioral health (BH) covered services overview o BH noncovered services o Early and Periodic
PLACEMENT OPENINGS: Two Post-Doctoral Residency positions are available for our Integrated Behavioral Health track
 San Mateo Medical Center Medical Psychiatry Services 222 W. 39 th Ave. San Mateo, CA 94403 (650)573-2760 PLACEMENT OPENINGS: Two Post-Doctoral Residency positions are available for our Integrated Behavioral
San Mateo Medical Center Medical Psychiatry Services 222 W. 39 th Ave. San Mateo, CA 94403 (650)573-2760 PLACEMENT OPENINGS: Two Post-Doctoral Residency positions are available for our Integrated Behavioral
Hawthorne, OH Mental Health Diagnoses Provide all Diagnoses Diagnosis DSM5 OR ICD-10 Paranoid Schizophrenia F20.0
 Page 1 of 6 Referral Information Date Sent to Permedion: 1/10/16 Hospital/Facility Name: Hollywood Memorial Hospital Contact Person: Diane Smith, RN Email address: diane.smith@hmh.com Phone: 614 333 9823
Page 1 of 6 Referral Information Date Sent to Permedion: 1/10/16 Hospital/Facility Name: Hollywood Memorial Hospital Contact Person: Diane Smith, RN Email address: diane.smith@hmh.com Phone: 614 333 9823
Report to the Minister of Justice and Solicitor General Public Fatality Inquiry
 CANADA Province of Alberta Report to the Minister of Justice and Solicitor General Public Fatality Inquiry Fatality Inquiries Act WHEREAS a Public Inquiry was held at the Medicine Hat Provincial Court
CANADA Province of Alberta Report to the Minister of Justice and Solicitor General Public Fatality Inquiry Fatality Inquiries Act WHEREAS a Public Inquiry was held at the Medicine Hat Provincial Court
PRE-ADMISSION SCREENING AND RESIDENT REVIEW (PASRR) LEVEL I SCREEN
 LEVEL I SCREEN") NEW JERSEY DEPARTMENT OF HUMAN SERVICES PRE-ADMISSION SCREENING AND RESIDENT REVIEW (PASRR) LEVEL I SCREEN Please print and complete all questions. This form must be completed for all applicants PRIOR
NEW JERSEY DEPARTMENT OF HUMAN SERVICES PRE-ADMISSION SCREENING AND RESIDENT REVIEW (PASRR) LEVEL I SCREEN Please print and complete all questions. This form must be completed for all applicants PRIOR
Debriefing Activities Six Core Strategies A Tertiary Prevention Tool
 Reducing Risk and Preventing Violence, Trauma, and the Use of Seclusion and Restraint Debriefing Activities Six Core Strategies A Tertiary Prevention Tool Module created by Goetz & Huckshorn, 2003. Updated
Reducing Risk and Preventing Violence, Trauma, and the Use of Seclusion and Restraint Debriefing Activities Six Core Strategies A Tertiary Prevention Tool Module created by Goetz & Huckshorn, 2003. Updated
Patient Safety: Fall Prevention. Unlicensed Assistive Personnel
 Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
OBRA 87 & PASRR? Training Goals
 Alabama Department of Mental Health Alabama Medicaid Certified Nursing Homes Preadmission Screening & Resident Review (PASRR) for Mental Illness Intellectual Disability & Related Condition Angela Howard
Alabama Department of Mental Health Alabama Medicaid Certified Nursing Homes Preadmission Screening & Resident Review (PASRR) for Mental Illness Intellectual Disability & Related Condition Angela Howard
Reduce Readmissions & Avoidable ED Visits: Advocate Health Care s Medically Integrated Crisis Community Support
 Reduce Readmissions & Avoidable ED Visits: Advocate Health Care s Medically Integrated Crisis Community Support by Sheri Richardt, L.C.S.W. Manager for Crisis/CL/First Access/MICCS/After Care and Shastri
Reduce Readmissions & Avoidable ED Visits: Advocate Health Care s Medically Integrated Crisis Community Support by Sheri Richardt, L.C.S.W. Manager for Crisis/CL/First Access/MICCS/After Care and Shastri
REDUCTION OF PSYCHIATRIC PATIENT BOARDING IN THE ED
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 REDUCTION
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 REDUCTION
RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care. Recommendation Comparison Chart
 RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care Recommendation Comparison Chart RECOMMENDATIONS FROM SCREENING FOR DELIRIUM, DEMENTIA AND DEPRESSION IN THE OLDER ADULT (2010)
RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care Recommendation Comparison Chart RECOMMENDATIONS FROM SCREENING FOR DELIRIUM, DEMENTIA AND DEPRESSION IN THE OLDER ADULT (2010)
Assisted Living Compliance Putting it all Together
 Assisted Living Compliance Putting it all Together State of Iowa Assisted Living Codes Read, teach & understand the State of Iowa codes: 231C 481 Chapters 67 & 69 (Updated & effective on April 20, 2016)
Assisted Living Compliance Putting it all Together State of Iowa Assisted Living Codes Read, teach & understand the State of Iowa codes: 231C 481 Chapters 67 & 69 (Updated & effective on April 20, 2016)
PENNSYLVANIA PREADMISSION SCREENING RESIDENT REVIEW (PASRR) IDENTIFICATION LEVEL I FORM (Revised 9/1/2018)
 IDENTIFICATION LEVEL I FORM (Revised 9/1/2018)") PENNSYLVANIA PREADMISSION SCREENING RESIDENT REVIEW (PASRR) IDENTIFICATION LEVEL I FORM (Revised 9/1/2018) This process applies to all nursing facility (NF) applicants, regardless of payer source. All
PENNSYLVANIA PREADMISSION SCREENING RESIDENT REVIEW (PASRR) IDENTIFICATION LEVEL I FORM (Revised 9/1/2018) This process applies to all nursing facility (NF) applicants, regardless of payer source. All
San Diego County Funded Long-Term Care Criteria
 San Diego County Funded Long-Term Care Criteria Prepared By: 6/23/16 Table of Contents San Diego County Funded Long Term Care Criteria... 2 Referral Criteria by Level of Care: Institute of Mental Disease
San Diego County Funded Long-Term Care Criteria Prepared By: 6/23/16 Table of Contents San Diego County Funded Long Term Care Criteria... 2 Referral Criteria by Level of Care: Institute of Mental Disease
X Name of Patient (Please Print) X Signature of Patient (or Parent/Legal Guardian) X Name of Parent/Legal Guardian (Please Print)
 X Signature of Patient (or Parent/Legal Guardian) X Name of Parent/Legal Guardian (Please Print)") In Office Policies Identification - For the protection of our patients, and to reduce medical identity theft, all patients are required to present a valid insurance ID card and/or driver s license at the
In Office Policies Identification - For the protection of our patients, and to reduce medical identity theft, all patients are required to present a valid insurance ID card and/or driver s license at the
Dealing with Psychiatric Issues in the Emergency Department
 Dealing with Psychiatric Issues in the Emergency Department Thursday, October 28, 2010 Louisiana Hospital Association Conference Center Baton Rouge, Louisiana Dealing with Psychiatric Issues in the Emergency
Dealing with Psychiatric Issues in the Emergency Department Thursday, October 28, 2010 Louisiana Hospital Association Conference Center Baton Rouge, Louisiana Dealing with Psychiatric Issues in the Emergency
EMTALA. A 30 th Anniversary Journey. Steve Lipton. Cal. Society of Healthcare Risk Management March 10, Hooper, Lundy & Bookman, P.C.
 EMTALA A 30 th Anniversary Journey Steve Lipton Cal. Society of Healthcare Risk Management March 10, 2016 1Hooper, Lundy & Bookman, P.C. HAPPY ANNIVERSARY EMTALA The Journey 3Hooper, Lundy & Bookman, P.C.
EMTALA A 30 th Anniversary Journey Steve Lipton Cal. Society of Healthcare Risk Management March 10, 2016 1Hooper, Lundy & Bookman, P.C. HAPPY ANNIVERSARY EMTALA The Journey 3Hooper, Lundy & Bookman, P.C.
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress
 Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Improving Flow in the Emergency Department for Mental Health and Addiction Services. Session Summary
 60 Renfrew Drive, Suite 300 Markham, ON L3R 0E1 Tel: 905 948-1872 Fax: 905 948-8011 Toll Free: 1 866 392-5446 www.centrallhin.on.ca Improving Flow in the Emergency Department for Mental Health and Addiction
60 Renfrew Drive, Suite 300 Markham, ON L3R 0E1 Tel: 905 948-1872 Fax: 905 948-8011 Toll Free: 1 866 392-5446 www.centrallhin.on.ca Improving Flow in the Emergency Department for Mental Health and Addiction
Pharmacy Services. Division of Nursing Homes
 Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Managing Psychiatric Patient Throughput in the Emergency Department
 Managing Psychiatric Patient Throughput in the Emergency Department Heartland Healthcare Executive Group (HHEG) October 22, 2015 Agenda Introductions U.S. Mental Health Access Crisis Risks to Patients,
Managing Psychiatric Patient Throughput in the Emergency Department Heartland Healthcare Executive Group (HHEG) October 22, 2015 Agenda Introductions U.S. Mental Health Access Crisis Risks to Patients,
Barbara Resnick, PHD,CRNP University of Maryland School of Nursing
 Pain Careplans and Monitoring: Role of the Interprofessional Team Barbara Resnick, PHD,CRNP University of Maryland School of Nursing Disclosures I have no relevant disclosures LTC: Review Current Careplanning
Pain Careplans and Monitoring: Role of the Interprofessional Team Barbara Resnick, PHD,CRNP University of Maryland School of Nursing Disclosures I have no relevant disclosures LTC: Review Current Careplanning
Family & Children s Services. Center
 Family & Children s Services CrisisCare Center When severe psychiatric crisis makes daily life seem impossible, Family & Children s Services new CrisisCare Center can help. Services are available around
Family & Children s Services CrisisCare Center When severe psychiatric crisis makes daily life seem impossible, Family & Children s Services new CrisisCare Center can help. Services are available around
Alcohol Drug & Mental Health Services INPATIENT SERVICES
 Alcohol Drug & Mental Health Services INPATIENT SERVICES WHEN MUST COUNTY FUND MENTAL HEALTH SERVICES? 2 INPATIENT INCREASES DRIVERS Lack of psychiatric beds state & nation Increase in patients Court Ordered
Alcohol Drug & Mental Health Services INPATIENT SERVICES WHEN MUST COUNTY FUND MENTAL HEALTH SERVICES? 2 INPATIENT INCREASES DRIVERS Lack of psychiatric beds state & nation Increase in patients Court Ordered
Emergency Use of Manual Restraints Policy
 Emergency Use of Manual Restraints Policy It is the policy of this DHS licensed provider, Companion Linc, to promote the rights of persons served by this program and to protect their health and safety
Emergency Use of Manual Restraints Policy It is the policy of this DHS licensed provider, Companion Linc, to promote the rights of persons served by this program and to protect their health and safety
In Arkansas 02/20/2014 1
 In Arkansas 02/20/2014 1 Procedures for Determination of Medical Need for Nursing Home Services I. Medical Need Assessments A. Nursing Facility Procedures B. OLTC Procedures II. Pre-Admission Screening
In Arkansas 02/20/2014 1 Procedures for Determination of Medical Need for Nursing Home Services I. Medical Need Assessments A. Nursing Facility Procedures B. OLTC Procedures II. Pre-Admission Screening
Behavioral Health Initial Review Form
 Behavioral Health Initial Review Form https://providers.amerigroup.com This form is for inpatients, the Partial Hospitalization Program and the Intensive Outpatient Program. Please submit this form on
Behavioral Health Initial Review Form https://providers.amerigroup.com This form is for inpatients, the Partial Hospitalization Program and the Intensive Outpatient Program. Please submit this form on
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE RESTRAINT AS A LAST RESORT - CRITICAL CARE SCOPE Provincial: Critical Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating Officer, Glenrose Rehabilitation Hospital
TITLE RESTRAINT AS A LAST RESORT - CRITICAL CARE SCOPE Provincial: Critical Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating Officer, Glenrose Rehabilitation Hospital
Adult Family Homes. Susan L. Lakey, PharmD Pharmacy 492 January 24, 2005
 Adult Family Homes Susan L. Lakey, PharmD Pharmacy 492 January 24, 2005 Background 1995 HB 1908 Required a reduction in NH medicaid beds by 1600 over 2 years The number of older adults in nursing homes
Adult Family Homes Susan L. Lakey, PharmD Pharmacy 492 January 24, 2005 Background 1995 HB 1908 Required a reduction in NH medicaid beds by 1600 over 2 years The number of older adults in nursing homes
Frail Elderly Assessment Unit (FEAU)
") Frail Elderly Assessment Unit (FEAU) Good Practice in Care of Learning Disability and the Vulnerable Adult Event 10th February 2012 Amanda M A Futers RN Ba(Hons) Nursing Amanda.futers@uhns.nhs.uk Original
Frail Elderly Assessment Unit (FEAU) Good Practice in Care of Learning Disability and the Vulnerable Adult Event 10th February 2012 Amanda M A Futers RN Ba(Hons) Nursing Amanda.futers@uhns.nhs.uk Original
Notification Regarding BHRS Brief Treatment Services for Providers of Child and Adolescent Behavioral Health Services
 Alert #3 2008 2-03 HCNC Notification Regarding BHRS Brief Treatment Services for Providers of Child and Adolescent Behavioral Health Services Community Care will begin to allow NC BHRS providers to implement
Alert #3 2008 2-03 HCNC Notification Regarding BHRS Brief Treatment Services for Providers of Child and Adolescent Behavioral Health Services Community Care will begin to allow NC BHRS providers to implement
Background to HoNOS (extract from Trust website) Page 2. How to Rate HoNOS Page 2. The Mental Health Clustering Tool Page 3
 Page 2. How to Rate HoNOS Page 2. The Mental Health Clustering Tool Page 3") HOW TO..HoNOS and RiO Contents: Background to HoNOS (extract from Trust website) Page 2 How to Rate HoNOS Page 2 The Mental Health Clustering Tool Page 3 How to use HoNOS process flow For teams using RiO
HOW TO..HoNOS and RiO Contents: Background to HoNOS (extract from Trust website) Page 2 How to Rate HoNOS Page 2 The Mental Health Clustering Tool Page 3 How to use HoNOS process flow For teams using RiO
Behaviours Have Meaning. The Ontario Behavioural Support System Project
 Behaviours Have Meaning The Ontario Behavioural Support System Project October 2010 Submitted by the Ontario Behavioural Support System Project Team October 2010 This document contains an overview of the
Behaviours Have Meaning The Ontario Behavioural Support System Project October 2010 Submitted by the Ontario Behavioural Support System Project Team October 2010 This document contains an overview of the
ILLINOIS 1115 WAIVER BRIEF
 ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
Youth Treatment Professionals
 Realistic Job Preview Youth Treatment Professionals The mission of Devereux Colorado is to inspire growth and foster human potential in the lives of those we serve. By utilizing positive dynamic approaches
Realistic Job Preview Youth Treatment Professionals The mission of Devereux Colorado is to inspire growth and foster human potential in the lives of those we serve. By utilizing positive dynamic approaches
Forensic Assertive Community Treatment Team (FACT) A bridge back to the community for people with severe mental illness
 A bridge back to the community for people with severe mental illness") Forensic Assertive Community Treatment Team (FACT) A bridge back to the community for people with severe mental illness Gary Morse, Ph.D. Katie Thumann, L.C.S.W. Places for People: Community Alternatives
Forensic Assertive Community Treatment Team (FACT) A bridge back to the community for people with severe mental illness Gary Morse, Ph.D. Katie Thumann, L.C.S.W. Places for People: Community Alternatives
WRHA Constant Care Guidelines for Acute Care 2018
 WRHA Constant Care Guidelines for Acute Care 8. PURPOSE To establish standardized guidelines and support appropriate use of constant care in acute care settings. Separate guidelines apply to residents
WRHA Constant Care Guidelines for Acute Care 8. PURPOSE To establish standardized guidelines and support appropriate use of constant care in acute care settings. Separate guidelines apply to residents
The speaker has no conflicts of interest to disclose.
 Eliminating Restraints on a High Acuity Inpatient Behavioral Health Unit Melinda Elliott MSN, RN, NE BC The speaker has no conflicts of interest to disclose. OBJECTIVES Identify the techniques Grady s
Eliminating Restraints on a High Acuity Inpatient Behavioral Health Unit Melinda Elliott MSN, RN, NE BC The speaker has no conflicts of interest to disclose. OBJECTIVES Identify the techniques Grady s
Flexible Assertive Community Treatment (FACT)
") Flexible Assertive Community Treatment (FACT) Dutch model for recovery oriented cure & care for people with severe mental illness Dan Cohen Consensus Development Conference Edmonton 2014 Statement of Potential
Flexible Assertive Community Treatment (FACT) Dutch model for recovery oriented cure & care for people with severe mental illness Dan Cohen Consensus Development Conference Edmonton 2014 Statement of Potential
Michelle Newberry Missouri Project Director Bock Associates
 Michelle Newberry Missouri Project Director Bock Associates bockmo@embarqmail.com Kathy Schafer Registered Nurse Clinical Operations Department of Mental Health Kathy.Schafer@dmh.mo.gov Ammanda Ott FAN
Michelle Newberry Missouri Project Director Bock Associates bockmo@embarqmail.com Kathy Schafer Registered Nurse Clinical Operations Department of Mental Health Kathy.Schafer@dmh.mo.gov Ammanda Ott FAN
1. PROPOSAL NARRATIVE REQUIREMENTS (Maximum 85 points)
") Single Source Requirements for Adult Residential Care Facility Instructions: If Vendor is interested in an opportunity to contract for Adult Residential Care Facility (RCF) services in FY15 with the County,
Single Source Requirements for Adult Residential Care Facility Instructions: If Vendor is interested in an opportunity to contract for Adult Residential Care Facility (RCF) services in FY15 with the County,
Behavioral Health Services. San Francisco Department of Public Health
 Behavioral Health Services San Francisco Department of Public Health Slide 2 Agenda Behavioral Health Services in San Francisco Mental Health Services Substance Use Disorder Services Levels of Care Behavioral
Behavioral Health Services San Francisco Department of Public Health Slide 2 Agenda Behavioral Health Services in San Francisco Mental Health Services Substance Use Disorder Services Levels of Care Behavioral
Atascocita Counseling Associates Krissy Cotten, MA, LPC. Adult New Client Profile
 Adult New Client Profile Please complete the following as accurately and as completely as possible. Social Security Number is required only if you are filing with insurance. Today s Date: Name: Date of
Adult New Client Profile Please complete the following as accurately and as completely as possible. Social Security Number is required only if you are filing with insurance. Today s Date: Name: Date of