Organization: Solution Title: Program/Project Description, including Goals: What is this project? Why is this project important?
|
|
|
- Horace Lewis
- 5 years ago
- Views:
Transcription
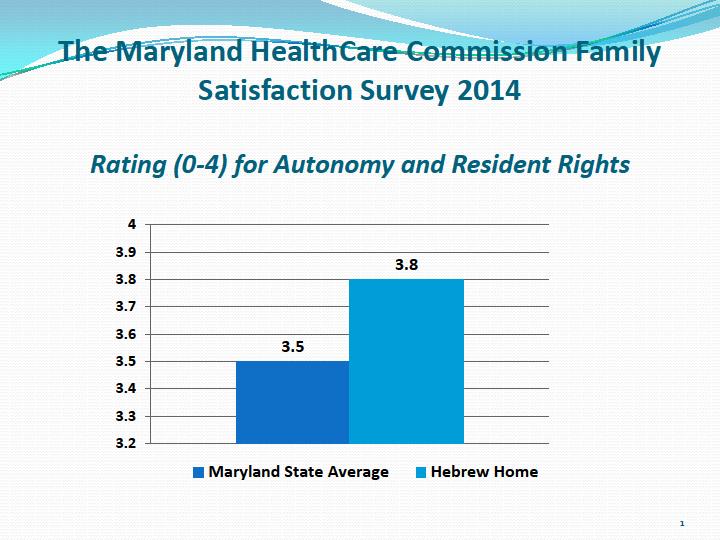
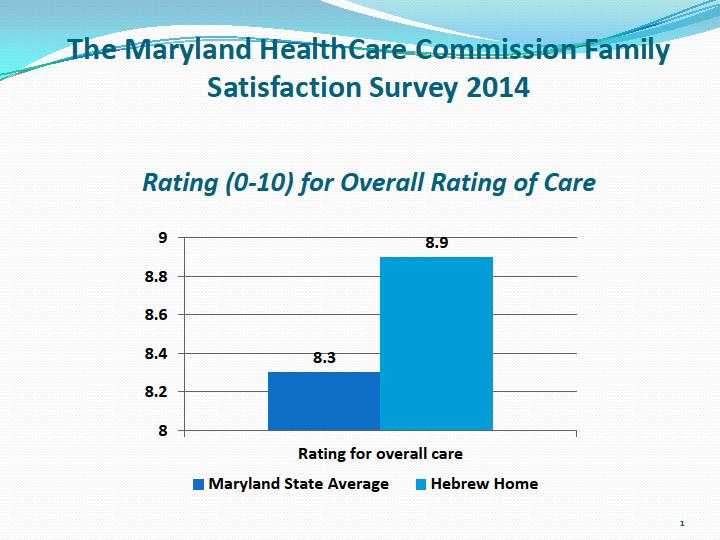
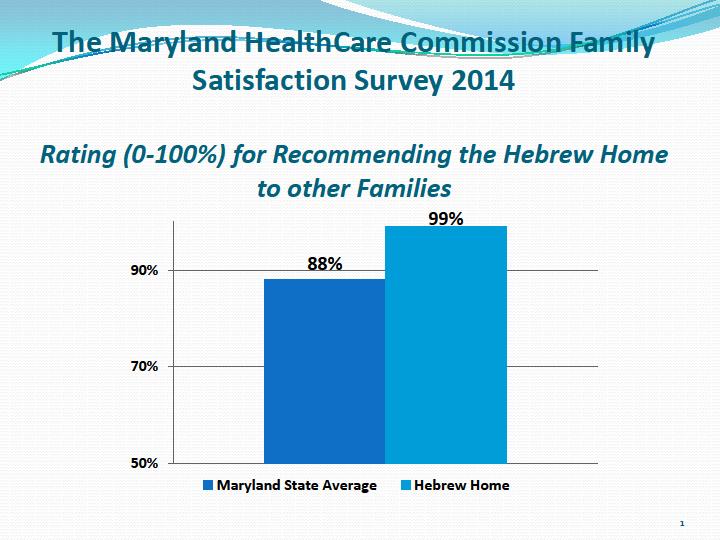
1 Organization: Hebrew Home of Greater Washington (The Charles E. Smith Life Communities) The Hebrew Home provides post-acute services and long-term care to a daily average census of 500 residents. The Home is located on a 34-acre campus in Rockville, Maryland. Solution Title: Improving the Safety of Dementia Care by Reducing the Use of Antipsychotic Medication in the Long-Term Care Setting Program/Project Description, including Goals: What is this project? Antipsychotic medications help suppress psychotic symptoms in individuals with schizophrenia. While these medications can help some people with dementia who do have psychosis, frequently the medications are used when a person acts in a way that is challenging or disturbing to others such as hitting, yelling, screaming, refusing care, walking around, crying, banging, or throwing things. Antipsychotic medications can be harmful though, in this vulnerable population causing significant side effects. Many elderly individuals are admitted to the Hebrew Home already prescribed these medications by their primary care physicians. Individuals suffering from dementia deserve better than merely to be given these drugs as a first line of choice. The Hebrew Home has embraced the notion that no resident should be prescribed an antipsychotic medication without an assessment for the underlying cause of the behavior it seeks to minimize. Consistent with its mission and core values, clinical leaders at the Hebrew Home of Greater Washington identified this opportunity to improve the safety of dementia care by reducing its use of antipsychotic medications as a priority quality initiative. Progress was determined by monitoring two sets of outcomes: first, the monthly assessment of anti-psychotic utilization percentage throughout 2014; and second, the 2014 Maryland HealthCare Commission Family Satisfaction Survey results. These results were also examined to look at rating of Autonomy and Resident Rights, Overall Rating of Care, and Whether families would recommend the Hebrew Home to others compared to the Maryland State averages for over 200 nursing home facilities. Why is this project important? Antipsychotic medications can be dangerous when used in the elderly population. Some of these side effects include cardiac conduction disturbances, sedation, anticholinergic reactions, stroke, parkinsonian events, cognitive slowing, tardive dyskinesia, orthostatic hypotension, earlier death, and reduced bone mineral density. In addition, this group of medications is expensive to consumers and Medicare, costing billions of dollars (more than $13 billion in 2007 and $7.6 billion in 2011). The literature confirms that there is a high prevalence of antipsychotic medication use in nursing home residents, especially in residents with a diagnosis of dementia. Moreover, daily dosing often exceeds recommended levels and includes inappropriate indications (Briesacher, 2005). A correlation has also been drawn between the likelihood of a resident to receive an antipsychotic medication with facility-level
2 antipsychotic prescribing rates, even after adjustment has been made for clinical and sociodemographic characteristics (Chen et al., 2010). Who embraced this project? This project was led by an interdisciplinary team which worked together throughout the year to improve the safety of dementia care by reducing the use of antipsychotic medication in the geriatric population receiving long-term care. The team consisted of: 1. VP of Quality and Corporate Compliance 2. Director of Nursing 3. Medical Staff 4. Performance Improvement Managers 5. Recreation Therapy 6. Social Work 7. Pharmacist Consultant 8. Consultant Psychiatrist The team s goal was to reduce the use of antipsychotic medications by turning to effective and safe non-pharmacological, behavioral approaches to the care of residents with dementia. Antipsychotic medications could be considered for residents with dementia, but only after medical, physical, functional, psychological, emotional, psychiatric, social and environmental causes had been identified and addressed. Process: The team approached this performance improvement project from the perspective of the three Rs of Rethinking, Reconnecting, Restoring within the Plan Do Study Act Quality Model framework: 1. Rethinking our approach to dementia care: Transforming the culture to rethink the care team s approach to dementia care. This involved engagement of all stakeholders with daily discussion at the Stand-up meetings between the care team, monthly discussion at the Quality Assurance/Performance Improvement Meetings and quarterly discussion at the Quality Improvement Committee of the Board. 2. Reconnecting with residents through person-centered care practices: Incorporating a comprehensive team-based approach to provide care. This was accomplished by starting with new employee orientation, including education on person-centered care scenarios. All employees also participated in mandatory dementia education (8 hours for clinical staff and 2 hours for non-clinical staff). 3. Restoring good health and quality of life: Supporting a safe and optimal quality of life by introducing a person-centered approach, assessing triggers for behavior changes, introducing behavioral interventions (e.g. walking with resident, massage therapy, provision of snacks), restricting anti-psychotic medication as a last resort. Solution:
3 1. Engagement of Quality leadership. In order to succeed, the team prioritized the need to reduce the use of anti-psychotic medication. Strong support was offered by the Board of Governor s Quality Improvement Committee and Executive Leadership. 2. Provision of Mandatory Dementia Education to all employees. One of the first steps was to re-focus the care team and ancillary staff on person-centered care, prevention of abuse, and the need to customize individualized approaches to care of persons with dementia. Mandatory 8-hour dementia education was provided to all clinical staff and mandatory 2-hour dementia education was provided to all non-clinical staff. The primary components of the dementia education included, but were not limited to the following: a. Introduction to Dementia Understanding cognitive impairment and mental illness, the normal aging process, the conditions affecting cognitive impairment and mental illness, the clinical definition of dementia and how it impacts behavior, communication and basic needs; it also included a discussion of how to develop a realistic approach to dealing with people who have cognitive impairment as well as understanding that depression can be mistaken for dementia. b. Medical Considerations Related to the Care of Persons with Dementia This component included recognition of reversible causes of dementia, different types of dementia, prevalence in nursing home settings, diagnostic criteria, physical exam for arriving at a diagnosis, tests for dementia, non-verbal pain recognition in dementia, and discussion of competence and capacity within the framework of a dementia diagnosis c. Making Activities Meaningful for Our Residents The coursework also covered developing an understanding of the important role that activity programs play in the day-to-day life of those residents with dementia. d. Communication, Behavior and De-Escalation Finally, the program concluded with discussion of the behavioral symptoms found within dementia, causes and reactions--- what they can signal, developing care based on principles of person-centered care, developing awareness of the verbal and non-verbal message, reality orientation vs. validation therapy approach, and interventions grounded in understanding these principles.
4 3. A Systematic Process was defined. The following approach was provided for each resident: a. Identify the resident s behavioral expression of distress, including the nature, frequency, severity, and duration and the risks of those behaviors and discussion of potential underlying causes with the care team and family b. Exclude potentially remediable causes of behaviors such as delirium, infection or other medication) and determine if symptoms are severe, distressing, or risky enough to adversely affect the safety of residents c. Identify environments and other approaches that attempt to understand and address behavior as a form of communication and in persons with dementia, and modify the environment and daily routines to meet the person s needs d. Assess the effects of any intervention (pharmacological or non-pharmacological); identify benefits and complications in a timely fashion; adjust treatment accordingly e. Use gradual dose reduction (team approach including the clinical pharmacist, attending physician, and clinical team manager) to transition a resident off the medication f. All residents admitted on an antipsychotic medication were re-evaluated at the time of admission and/or within two weeks of admission to consider a reduction in dose or discontinuation. 4. Discussion of findings at daily Stand-up meeting between members of the care team. The Stand-up meeting occurs daily at 8:30 a.m. in the Social Hall of either the Wasserman or Smith-Kogod Residence. The 24-hour summary report within the electronic medical record (Point Click Care or PCC ) is projected on a large screen for all attendees to view. The interdisciplinary team discusses all reported behaviors and potential interventions as well as ongoing status of other interventions already in place. The team learned that many of the residents actions were indicating that they needed something such as needing a nap because they were tired, fluids because they were thirsty, food because they were hungry, activity or change in environment because they were bored, and/or a visit to the bathroom because they needed to urinate. 5. Review of project status at monthly Quality Assurance/Performance Improvement ( QAPI ) meetings, quarterly Board of Governors Quality Improvement Committee meetings, and quarterly Pharmacy and Therapeutics Committee. Monthly stats regarding the percentage of residents on anti-psychotic medication and the gradual dose reduction report from the consultant pharmacist was reviewed.
5 Measurable Outcomes: The measures used reflect two separate outcomes (both described below). The first, percentage utilization, takes into account all antipsychotics; the common medications including Haldol, Quetiapine (Seroquel), Olanzapine (Zyprexa), Aripiprazole (Abilify), and Risperidone (Risperidal). The second outcome measurement includes three measures from the Maryland Health Care Commission (MHCC) Survey. This survey measures the family or responsible party s experience and satisfaction regarding care of the resident at the nursing home. The team examined the Hebrew Home s performance in three different areas as noted below: the score for Autonomy and Residents Rights (0-4 scale), the Overall Rating of Care (0-10 scale), and the Overall percentage of parties who would recommend the Hebrew Home to others (0-100% scale) compared to the State average scores. 1. Measure: Percentage of Long Stay Residents who are receiving antipsychotic medication per month Description of Measure: Percentage of long stay residents (>100 cumulative days in the nursing facility) who are receiving antipsychotic medication. 2. Measure: MHCC Survey score for Autonomy and Resident Rights Description of Measure Two questions were asked of the respondents and scores were calculated by averaging the responses for each question across all respondents for that facility survey. This resulted in a score averaged from 1 = never to 4 = always. The two questions focused on privacy during visits with clergy or family as well as privacy during the care of the resident such as showering, bathing, dressing. This all reflects content of education received during the mandatory dementia education. 3. Measure: MHCC Survey score for Overall Rating of Care Description of Measure: The respondents were asked to rate the care of the resident received at the nursing home on a scale of 1 to 10, 1 being the worst possible care and 10 being the best possible care. 4. Measure: MHCC score for Percentage of families who would recommend facility to others Description of Measure: This measure reflects the percentage of respondents answering Definitely yes or "Probably yes to whether they would recommend the nursing facility to others. Sustainability: To date, the following practices continue to sustain the improvement: 1. The pharmacist consultant generates a gradual dose reduction report which is sent to the VP of Quality and Corporate Compliance. That report is then disseminated to each Performance Improvement Manager overseeing quality improvement within the 14 nursing units at the Hebrew Home. The report helps the Performance Improvement
6 Manger and Nurse Manager of each unit to gauge the unit s progress as well as identify which residents are currently prescribed an anti-psychotic medication; 2. Monthly and quarterly review of progress at the QAPI and QIC meetings, respectively; 3. The behavioral assessment tool has been built into the electronic medical record, Point Click Care ( PCC ) so that the use of the tool is used routinely as part of continuous nursing care. Staff identifies and document specific target behaviors, expressions of distress and desired outcomes. Individualized, person-centered interventions are implemented and documented. The care plan of these interventions is communicated throughout all shifts establishing continuity of care. 4. Education regarding (1) use of the behavioral assessment tool; and (2) person-centered approaches to care is included in the new nursing employee orientation; 5. Mandatory Dementia Education (8 hours for clinical staff, 2 hours for non-clinical staff) with annual re-education. Role of Collaboration and Leadership: As noted above, team engagement was critical to the success of this improvement effort. The Board and Executive Leadership s support were both strong and supportive from the initial start-up of the project. Innovation: Several Innovative approaches contributed to the success of this improvement: 1. Collaboration between multiple disciplines (quality, nursing, medical, pharmacy, behavioral health) 2. Monthly audits of all residents currently prescribed a routine and/or anti-psychotic medication 3. Monthly audits of all residents undergoing gradual dose reduction of antipsychotic medication 4. Board involvement (Board s Quality Improvement Committee) 5. Monthly (and Quarterly) progress reports using measurement graphics 6. Incorporating a behavioral assessment tool into the electronic medical record 7. Discussion of behavioral issues at daily Stand-up Meeting led by Director of Nursing and attended by Nurse Managers, Performance Improvement Managers, Social Work, Recreation Therapy, and Medical Staff
7 Related Tools and Resources: 1. Measurement Graphs (see below) 2. Behavior Assessment Tool Contact Person: Barbara Hirsch, BSN, JD, VP, Quality and Corporate Compliance
8
9
10 Behavior Monitoring Pathway Tool
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit
 Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Part 1: Overview of AHCA/NCAL Clinical Considerations of Antipsychotic Management Toolkit Dr. Cathy Lipton, MD Dr. Anna Fisher, PhD Holly Harmon, RN, MBA, LNHA Introduction Holly Harmon 1 Objectives Summarize
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress
 Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
POLICY. Use of Antipsychotic Medications in Nursing Facility Residents. Preamble. Background
 Preamble POLICY Use of Antipsychotic Medications in Nursing Facility Residents The Office of Inspector General of the U. S. Department of Health and Human Services issued a report in May 2011 finding that
Preamble POLICY Use of Antipsychotic Medications in Nursing Facility Residents The Office of Inspector General of the U. S. Department of Health and Human Services issued a report in May 2011 finding that
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Psychotropic Drug Use To Medicate or Not to Medicate?
 Psychotropic Drug Use To Medicate or Not to Medicate? Presented by: Lydia Restivo, RN CDONA Regulatory Compliance Consultant West & Restivo Quality Consulting Cell: 516 318-9088 Email: lydrestivo@verizon.net
Psychotropic Drug Use To Medicate or Not to Medicate? Presented by: Lydia Restivo, RN CDONA Regulatory Compliance Consultant West & Restivo Quality Consulting Cell: 516 318-9088 Email: lydrestivo@verizon.net
NURSING FACILITY ASSESSMENTS
 Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
Department of Health and Human Services OFFICE OF INSPECTOR GENERAL NURSING FACILITY ASSESSMENTS AND CARE PLANS FOR RESIDENTS RECEIVING ATYPICAL ANTIPSYCHOTIC DRUGS Daniel R. Levinson Inspector General
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care
 Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
Antipsychotic Use Survey Tool Supplemental Guidance
 Antipsychotic Use Survey Tool Supplemental Guidance Commonly prescribed antipsychotic medications (brand name and/or generic): First generation (typical) antipsychotic: chlorpromazine (generic only) fluphenazine
Antipsychotic Use Survey Tool Supplemental Guidance Commonly prescribed antipsychotic medications (brand name and/or generic): First generation (typical) antipsychotic: chlorpromazine (generic only) fluphenazine
Pharmacy Services. Division of Nursing Homes
 Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Form CMS (5/2017) Page 1
 Page 1") Use this pathway for a resident who has pain symptoms or can reasonably be expected to experience pain (i.e., during therapy) to determine whether the facility has provided and the resident has received
Use this pathway for a resident who has pain symptoms or can reasonably be expected to experience pain (i.e., during therapy) to determine whether the facility has provided and the resident has received
Reducing Harm and Healthcare Costs: A Review Of A Physician's Unlimited License To Practice
 Reducing Harm and Healthcare Costs: A Review Of A Physician's Unlimited License To Practice Generally, physicians are licensed under what is termed an "unlimited" license. Underlying the intent of unlimited
Reducing Harm and Healthcare Costs: A Review Of A Physician's Unlimited License To Practice Generally, physicians are licensed under what is termed an "unlimited" license. Underlying the intent of unlimited
MISUSE AND OVERUSE OF ELDERS WITH DEMENTIA May 2018
 MISUSE AND OVERUSE OF ANTI-PSYCHOTIC DRUGS ON ELDERS WITH DEMENTIA May 2018 MITZI M CFATRICH, EXECUTIVE DIRECTOR LAURA MEYER PFEIFER, DIRECTOR OF DEVELOPMENT AND OUTREACH Kansas Advocates for Better Care
MISUSE AND OVERUSE OF ANTI-PSYCHOTIC DRUGS ON ELDERS WITH DEMENTIA May 2018 MITZI M CFATRICH, EXECUTIVE DIRECTOR LAURA MEYER PFEIFER, DIRECTOR OF DEVELOPMENT AND OUTREACH Kansas Advocates for Better Care
Behavioral Health Services. Division of Nursing Homes
 Behavioral Health Services Division of Nursing Homes 483.40 Behavioral Health Services Overview F740 Introduction to Behavioral Health Services F741 Sufficient and Competent Staff F742 Treatment/Services
Behavioral Health Services Division of Nursing Homes 483.40 Behavioral Health Services Overview F740 Introduction to Behavioral Health Services F741 Sufficient and Competent Staff F742 Treatment/Services
Behavior Problems: Dementia and Mental Illness in Long Term Care and Assisted Living
 Behavior Problems: Dementia and Mental Illness in Long Term Care and Assisted Living Module II Dr. David A. Smith, M.D., FAAFP, CMD mmlearn.org is a program of Morningside Ministries Cell Phones and Pagers
Behavior Problems: Dementia and Mental Illness in Long Term Care and Assisted Living Module II Dr. David A. Smith, M.D., FAAFP, CMD mmlearn.org is a program of Morningside Ministries Cell Phones and Pagers
NHS Norfolk Medicines Management in Care Homes. Sue Woodruff Senior Clinical Pharmacist Co-ordinator (care homes)
") NHS Norfolk Medicines Management in Care Homes Sue Woodruff Senior Clinical Pharmacist Co-ordinator (care homes) susan.woodruff@nhs.net Background Almost 400 care homes in NHS-N area Care for over 8000
NHS Norfolk Medicines Management in Care Homes Sue Woodruff Senior Clinical Pharmacist Co-ordinator (care homes) susan.woodruff@nhs.net Background Almost 400 care homes in NHS-N area Care for over 8000
PERFORMANCE MEASURE DATE / RESULTS / ANALYSIS FOLLOW-UP / ACTION PLAN
 Resident-to-Resident Assaults AIM: To decrease incidents of Resident to Residents assaults by 5% in the Fiscal Year (FY) 2011-2012. MONITORING: Data is collected from all instances in which State of California
Resident-to-Resident Assaults AIM: To decrease incidents of Resident to Residents assaults by 5% in the Fiscal Year (FY) 2011-2012. MONITORING: Data is collected from all instances in which State of California
3/6/2017. CMS nursing home requirements have not been comprehensively updated since 1991 despite significant changes in the industry.
 Debra Brown, PharmD Pharmaceutical Consultant II Specialist Licensing and Certification QCHF/CAHF Spring Legislative Conference March 2017 1 Describe impact of 2016 CMS Final Rule on SNF pharmacy services
Debra Brown, PharmD Pharmaceutical Consultant II Specialist Licensing and Certification QCHF/CAHF Spring Legislative Conference March 2017 1 Describe impact of 2016 CMS Final Rule on SNF pharmacy services
Psychiatric Mental Health Nursing Core Competencies Individual Assessment
 Individual Name: Orientation Start Date: Completion Date: Instructions: -the nurse will rate each knowledge, skill, or attitude (KSA) from 1 (novice) to 5 (expert) in each box. Following orientation or
Individual Name: Orientation Start Date: Completion Date: Instructions: -the nurse will rate each knowledge, skill, or attitude (KSA) from 1 (novice) to 5 (expert) in each box. Following orientation or
Nursing Home Pearls or
 Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
c) Facilities substantially in compliance with the requirements of this Subpart will receive written recognition from the Department.
 Facilities substantially in compliance with the requirements of this Subpart will receive written recognition from the Department.") TITLE 77: PUBLIC HEALTH CHAPTER I: DEPARTMENT OF PUBLIC HEALTH SUBCHAPTER c: LONG-TERM CARE FACILITIES PART 300 SKILLED NURSING AND INTERMEDIATE CARE FACILITIES CODE SECTION 300.7000 APPLICABILITY Section
TITLE 77: PUBLIC HEALTH CHAPTER I: DEPARTMENT OF PUBLIC HEALTH SUBCHAPTER c: LONG-TERM CARE FACILITIES PART 300 SKILLED NURSING AND INTERMEDIATE CARE FACILITIES CODE SECTION 300.7000 APPLICABILITY Section
Examining Inappropriate Use of Antipsychotic Drugs Part One: How Seven States Cite Antipsychotic Drug Deficiencies
 Examining Inappropriate Use of Antipsychotic Drugs Part One: How Seven States Cite Antipsychotic Drug Deficiencies The misuse of antipsychotic drug is a pervasive problem in American nursing facilities.
Examining Inappropriate Use of Antipsychotic Drugs Part One: How Seven States Cite Antipsychotic Drug Deficiencies The misuse of antipsychotic drug is a pervasive problem in American nursing facilities.
a. The Care Plan dated 2/16/10 documented the following:
 b. The Plan of Care dated 1/12/10 documented, "Problem: At risk for depression, related to very young to be in long term care facility and permanent brain damage R/T [related to] trauma. Approaches: Arrange
b. The Plan of Care dated 1/12/10 documented, "Problem: At risk for depression, related to very young to be in long term care facility and permanent brain damage R/T [related to] trauma. Approaches: Arrange
The Department of Justice s Focus on Failure of Care Fraud Cases
 The Department of Justice s Focus on Failure of Care Fraud Cases HCCA 17 TH ANNUAL COMPLIANCE INSTITUTE WASHINGTON, DC APRIL 21, 2013 SUSAN C. LYNCH, ESQ. U.S. DEPARTMENT OF JUSTICE SUSAN.LYNCH@USDOJ.GOV
The Department of Justice s Focus on Failure of Care Fraud Cases HCCA 17 TH ANNUAL COMPLIANCE INSTITUTE WASHINGTON, DC APRIL 21, 2013 SUSAN C. LYNCH, ESQ. U.S. DEPARTMENT OF JUSTICE SUSAN.LYNCH@USDOJ.GOV
QAA/QAPI Meeting Agenda Guide
 QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
QAA/QAPI Meeting Agenda Guide Date of Meeting The facility is required to have a QAA committee (do not need to use this name) that meets at least quarterly and as needed to coordinate and evaluate activities
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
Local Enhanced Service Agreement 1 July March 2016
 Local Enhanced Service Agreement 1 July 2013 31 March 2016 Recognition and Management of People with Dementia and their Family/Carers in General Practices in Bristol Agreement between NHS Bristol Clinical
Local Enhanced Service Agreement 1 July 2013 31 March 2016 Recognition and Management of People with Dementia and their Family/Carers in General Practices in Bristol Agreement between NHS Bristol Clinical
Medication Related Changes Phase 1&2
 Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Improving Dementia Care and Reducing Unnecessary Use of Antipsychotic Medications in Nursing Homes
 1 Revision Date: August 2012 SMART AIM Reduce the use of Atypical Anti-Psychotics (AAPs) in Nursing Facilities by 15% by 12/12 KEY DRIVER DIAGRAM - draft Project Name: NF AAP Utilization QI Project Team
1 Revision Date: August 2012 SMART AIM Reduce the use of Atypical Anti-Psychotics (AAPs) in Nursing Facilities by 15% by 12/12 KEY DRIVER DIAGRAM - draft Project Name: NF AAP Utilization QI Project Team
The DON s & DSW s Roles in Preventing Resident to Resident Altercations
 The DON s & DSW s Roles in Preventing Resident to Resident Altercations LeadingAge New York Presenter: Linda Elizaitis, President CMS Compliance Group, Inc. T: 631.692.4422 E. lmelizaitis@cmscg.net W.
The DON s & DSW s Roles in Preventing Resident to Resident Altercations LeadingAge New York Presenter: Linda Elizaitis, President CMS Compliance Group, Inc. T: 631.692.4422 E. lmelizaitis@cmscg.net W.
MENTAL HEALTH NURSING ORIENTATION. (2) Alleviating disabling symptoms of mental disorders.
 Alleviating disabling symptoms of mental disorders.") Page 1 of 6 1. Mission Statement MENTAL HEALTH NURSING ORIENTATION a. The mission of mental health services is to provide constitutionally adequate care. Mental health care is provided to assist the inmate
Page 1 of 6 1. Mission Statement MENTAL HEALTH NURSING ORIENTATION a. The mission of mental health services is to provide constitutionally adequate care. Mental health care is provided to assist the inmate
Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications
 Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications Lisa Bridwell Program Specialist Telligen QIN-QIO March 2018 Objectives Review interpretive guidance F758 (Free from
Developing and Action Plan: Person Centered Dementia Care and Psychotropic Medications Lisa Bridwell Program Specialist Telligen QIN-QIO March 2018 Objectives Review interpretive guidance F758 (Free from
UNDERSTANDING THE CONTENT OUTLINE/CLASSIFICATION SYSTEM
 BOARD OF PHARMACY SPECIALTIES PSYCHIATRIC PHARMACY SPECIALIST CERTIFICATION CONTENT OUTLINE/CLASSIFICATION SYSTEM FINALIZED FEBRUARY 2017/FOR USE ON FALL 2017 EXAMINATION AND FORWARD UNDERSTANDING THE
BOARD OF PHARMACY SPECIALTIES PSYCHIATRIC PHARMACY SPECIALIST CERTIFICATION CONTENT OUTLINE/CLASSIFICATION SYSTEM FINALIZED FEBRUARY 2017/FOR USE ON FALL 2017 EXAMINATION AND FORWARD UNDERSTANDING THE
Solution Title Impact on readmission rates of psychiatric patients following pharmacist discharge counseling in a community hospital
 Organization Suburban Hospital Johns Hopkins Medicine Solution Title Impact on readmission rates of psychiatric patients following pharmacist discharge counseling in a community hospital Program/Project
Organization Suburban Hospital Johns Hopkins Medicine Solution Title Impact on readmission rates of psychiatric patients following pharmacist discharge counseling in a community hospital Program/Project
Advocating Against The Illegal and Excessive Use of Psychotropic Drugs with People with Dementia
 Advocating Against The Illegal and Excessive Use of Psychotropic Drugs with People with Dementia Kelly Bagby, AARP Foundation Litigation (202) 434-2103 OBJECTIVES Raise awareness and understanding of the
Advocating Against The Illegal and Excessive Use of Psychotropic Drugs with People with Dementia Kelly Bagby, AARP Foundation Litigation (202) 434-2103 OBJECTIVES Raise awareness and understanding of the
9/8/2017. Making the Connection: Linking the Facility Assessment and QAPI Plan. Cindy Mason VP Provider Services. Final Rule. Providigm, LLC,
 Making the Connection: Linking the Facility Assessment and QAPI Plan Cindy Mason VP Provider Services Final Rule Providigm, LLC, 2017 1 Final Rule Effective Date These regulations are effective as of November
Making the Connection: Linking the Facility Assessment and QAPI Plan Cindy Mason VP Provider Services Final Rule Providigm, LLC, 2017 1 Final Rule Effective Date These regulations are effective as of November
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02
 Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Nursing homes: a case study of prescribing in older people. Carmel M. Hughes
 Nursing homes: a case study of prescribing in older people Carmel M. Hughes Objectives of lecture To highlight issues with nursing home care, focussing on use of medicines To highlight influences on prescribing
Nursing homes: a case study of prescribing in older people Carmel M. Hughes Objectives of lecture To highlight issues with nursing home care, focussing on use of medicines To highlight influences on prescribing
Achieving Memory Care Certification for Your Nursing Care Center. Gina Zimmermann, MS Executive Director Nursing Care Center Accreditation Program
 Copyright, The Joint Commission Achieving Memory Care Certification for Your Nursing Care Center Gina Zimmermann, MS Executive Director Nursing Care Center Accreditation Program 1 Today s Objectives Review
Copyright, The Joint Commission Achieving Memory Care Certification for Your Nursing Care Center Gina Zimmermann, MS Executive Director Nursing Care Center Accreditation Program 1 Today s Objectives Review
INTRODUCTION Reduce falls Improve patient outcomes Establish a baseline of falls in home care
 INTRODUCTION The Missouri Alliance for Home Care (MAHC) has developed a set of standardized tools for reporting and monitoring falls in patients under the care of home health. The program which began as
INTRODUCTION The Missouri Alliance for Home Care (MAHC) has developed a set of standardized tools for reporting and monitoring falls in patients under the care of home health. The program which began as
MDS Coding. Antipsychotic Quality Measure
 MDS Coding Antipsychotic Quality Measure The information in this presentation may be subject to copyright and may not be reproduced without permission of the presenter. Introduction Jessica Mirabal, RN
MDS Coding Antipsychotic Quality Measure The information in this presentation may be subject to copyright and may not be reproduced without permission of the presenter. Introduction Jessica Mirabal, RN
OIG Risk Areas: Comprehensive Care Plans, Restorative/Personal Care Services & Medication Management
 OIG Risk Areas: Comprehensive Care Plans, Restorative/Personal Care Services & Medication Management Presented by: Nan Impink, Esq. Kelly Priegnitz, Esq. Harvey Tettlebaum, Esq. Where We ve Been & Today
OIG Risk Areas: Comprehensive Care Plans, Restorative/Personal Care Services & Medication Management Presented by: Nan Impink, Esq. Kelly Priegnitz, Esq. Harvey Tettlebaum, Esq. Where We ve Been & Today
Finding Clarity in the Midst of Uncertainty
 Using Technology to Improve Outcomes for Patients-Part II: Discussion and Case Study Sandra Vale, M.D. Adult Behavioral Health Medical Director The Center for Health Care Services Finding Clarity in the
Using Technology to Improve Outcomes for Patients-Part II: Discussion and Case Study Sandra Vale, M.D. Adult Behavioral Health Medical Director The Center for Health Care Services Finding Clarity in the
Event Name: More Music! Less Medication! Event Date: 04/11/2018 Event Time: 11:30am-12:30pm ET
 Event Name: More Music! Less Medication! Event Date: 04/11/2018 Event Time: 11:30am-12:30pm ET Good morning again my name is Doreen Ostapchuk from the New England QIO, and I will be your moderator for
Event Name: More Music! Less Medication! Event Date: 04/11/2018 Event Time: 11:30am-12:30pm ET Good morning again my name is Doreen Ostapchuk from the New England QIO, and I will be your moderator for
role profiles PART 5 CONTENTS 259 fast track LPN 261 community foot care LPN 263 total care worker
 PART 5 role profiles Three distinct LPN and care aide roles are described in this section. One profile describes the job of an LPN in a fast track emergency unit at a regional acute care facility. Another
PART 5 role profiles Three distinct LPN and care aide roles are described in this section. One profile describes the job of an LPN in a fast track emergency unit at a regional acute care facility. Another
UCARE MODEL OF CARE SUMMARY FOR MH-TCM (February 2009)
") UCARE MODEL OF CARE SUMMARY FOR MH-TCM (February 2009) The UCare Model of Care for Mental Health Targeted Case Management is designed to provide care for the child member and their families and adult members,
UCARE MODEL OF CARE SUMMARY FOR MH-TCM (February 2009) The UCare Model of Care for Mental Health Targeted Case Management is designed to provide care for the child member and their families and adult members,
CMHC Conditions of Participation
 CMHC Conditions of Participation Mary Rossi-Coajou Center for Clinical Standards and Quality/Clinical Standards Group The Centers for Medicare and Medicare Services March 4,2014 Key Themes The CMHC NPRM
CMHC Conditions of Participation Mary Rossi-Coajou Center for Clinical Standards and Quality/Clinical Standards Group The Centers for Medicare and Medicare Services March 4,2014 Key Themes The CMHC NPRM
Proposed Accreditation Requirements Related to the Care of Patients or Residents with Dementia
 Proposed Accreditation Requirements Related to the Care of Patients or Residents with Dementia Nursing and Rehabilitation Center Accreditation Program EC.0001 1 The organization manages safety and security
Proposed Accreditation Requirements Related to the Care of Patients or Residents with Dementia Nursing and Rehabilitation Center Accreditation Program EC.0001 1 The organization manages safety and security
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Inpatient Psychiatric Services for Under Age 21 Arkansas Medicaid Regulations and Documentation
 Inpatient Psychiatric Services for Under Age 21 Arkansas Medicaid Regulations and Documentation Presented by: Shelly Rhodes Shelly.Rhodes@beaconhealthoptions.com Disclaimer Disclaimer: This presentation
Inpatient Psychiatric Services for Under Age 21 Arkansas Medicaid Regulations and Documentation Presented by: Shelly Rhodes Shelly.Rhodes@beaconhealthoptions.com Disclaimer Disclaimer: This presentation
Antibiotic Stewardship Program (ASP)
") Introduction: Antibiotics are among the most frequently prescribed medications in nursing centers, with up to 70% of nursing home patients receiving one or more courses of systemic antibiotics in a year.
Introduction: Antibiotics are among the most frequently prescribed medications in nursing centers, with up to 70% of nursing home patients receiving one or more courses of systemic antibiotics in a year.
Tag Description Page. F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125. F622 Transfer & Discharge 155
 Tag Description Page F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125 F622 Transfer & Discharge 155 F626 Permitting Residents to Return to Facility 170 F656 Comprehensive Care Plans
Tag Description Page F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125 F622 Transfer & Discharge 155 F626 Permitting Residents to Return to Facility 170 F656 Comprehensive Care Plans
RALF Behavior Management Rules IDAPA
 RALF Behavior Management Rules IDAPA 16.03.22 DEFINITIONS: 010.10. Assessment. The conclusion reached using uniform criteria which identifies resident strengths, weaknesses, risks and needs, to include
RALF Behavior Management Rules IDAPA 16.03.22 DEFINITIONS: 010.10. Assessment. The conclusion reached using uniform criteria which identifies resident strengths, weaknesses, risks and needs, to include
Project of: Seniors Health Strategic Clinical Network (SCN) in collaboration with Addiction & Mental Health SCN
 in collaboration with Addiction & Mental Health SCN") Project of: Seniors Health Strategic Clinical Network (SCN) in collaboration with Addiction & Mental Health SCN This PowerPoint describes the steps and strategies developed by the Appropriate use of Antipsychotics
Project of: Seniors Health Strategic Clinical Network (SCN) in collaboration with Addiction & Mental Health SCN This PowerPoint describes the steps and strategies developed by the Appropriate use of Antipsychotics
Teepa Snow, Positive Approach, LLC to be reused only with permission.
 Handouts are intended for personal use only. Any copyrighted materials or DVD content from Positive Approach, LLC (Teepa Snow) may be used for personal educational purposes only. This material may not
Handouts are intended for personal use only. Any copyrighted materials or DVD content from Positive Approach, LLC (Teepa Snow) may be used for personal educational purposes only. This material may not
The CMS State Operations Manual Overview and Changes
 The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
Behavioral and Emotional Status Critical Element Pathway
 Behavioral and Emotional Status Critical Element Pathway Use this pathway to determine if the facility is providing necessary behavioral, mental, and/or emotional health care and services to each resident.
Behavioral and Emotional Status Critical Element Pathway Use this pathway to determine if the facility is providing necessary behavioral, mental, and/or emotional health care and services to each resident.
Standards of Care Standards of Professional Performance
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Standards of Care Standard 1 Assessment Standard 2 Diagnosis Standard 3 Outcomes Identification Standard 4 Planning Standard 5 Implementation
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Standards of Care Standard 1 Assessment Standard 2 Diagnosis Standard 3 Outcomes Identification Standard 4 Planning Standard 5 Implementation
STROKE REHAB PROGRAM
 STROKE REHAB PROGRAM Allied Rehab Hospital is part of Allied Services Integrated Health System, the premier post-acute health-care system in Northeast Pennsylvania, and is the region s leading provider
STROKE REHAB PROGRAM Allied Rehab Hospital is part of Allied Services Integrated Health System, the premier post-acute health-care system in Northeast Pennsylvania, and is the region s leading provider
What are the potential ethical issues to be considered for the research participants and
 What are the potential ethical issues to be considered for the research participants and researchers in the following types of studies? 1. Postal questionnaires 2. Focus groups 3. One to one qualitative
What are the potential ethical issues to be considered for the research participants and researchers in the following types of studies? 1. Postal questionnaires 2. Focus groups 3. One to one qualitative
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities Proposed Rule
 Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities Proposed Rule Summary of Major Provisions Summary adapted from Proposed Rule (with AHCA Comments) July 14, 2015 Updates
Medicare and Medicaid Programs; Reform of Requirements for Long-Term Care Facilities Proposed Rule Summary of Major Provisions Summary adapted from Proposed Rule (with AHCA Comments) July 14, 2015 Updates
Advocates for Long-Term Care Residents Support Regulations to Ensure Independence of LTC Consultant Pharmacists
 Advocates for Long-Term Care Residents Support Regulations to Ensure Independence of LTC Consultant Pharmacists December 12, 2011 Marilyn B. Tavenner Acting Administrator Centers for Medicare & Medicaid
Advocates for Long-Term Care Residents Support Regulations to Ensure Independence of LTC Consultant Pharmacists December 12, 2011 Marilyn B. Tavenner Acting Administrator Centers for Medicare & Medicaid
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE MEDICATION ORDERS SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Provincial Medication Management Committee PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
TITLE MEDICATION ORDERS SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Provincial Medication Management Committee PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
PURPOSE: In accordance with SB362, Seven Hills Hospital has a documented staffing plan in place which adequately meets the needs of our patients.
 0-6 Title: Staffing Plan 9/8/203 0/29/3, 5/9/4 POC-07 PURPOSE: In accordance with SB362, Seven Hills Hospital has a documented staffing plan in place which adequately meets the needs of our patients. PERFORMED
0-6 Title: Staffing Plan 9/8/203 0/29/3, 5/9/4 POC-07 PURPOSE: In accordance with SB362, Seven Hills Hospital has a documented staffing plan in place which adequately meets the needs of our patients. PERFORMED
CAREGIVING COSTS. Declining Health in the Alzheimer s Caregiver as Dementia Increases in the Care Recipient
 CAREGIVING COSTS Declining Health in the Alzheimer s Caregiver as Dementia Increases in the Care Recipient National Alliance for Caregiving and Richard Schulz, Ph.D. and Thomas Cook, Ph.D., M.P.H. University
CAREGIVING COSTS Declining Health in the Alzheimer s Caregiver as Dementia Increases in the Care Recipient National Alliance for Caregiving and Richard Schulz, Ph.D. and Thomas Cook, Ph.D., M.P.H. University
Delirium management initiative: Guarding the minds of our patients
 Delirium management initiative: Guarding the minds of our patients Introduction This past January (2014), in response to requests from a number of our physicians, a new effort began at Baptist Health,
Delirium management initiative: Guarding the minds of our patients Introduction This past January (2014), in response to requests from a number of our physicians, a new effort began at Baptist Health,
9/27/2017. Getting on the Path to Excellence. The path we are taking today! CMS Five Elements
 Getting on the Path to Excellence QAPI DESIGN AND IMPLEMENTATION Demi Haffenreffer, RN, MBA www.consultdemi.net The path we are taking today! The requirements at F944 (formerly F520) Key elements Survey
Getting on the Path to Excellence QAPI DESIGN AND IMPLEMENTATION Demi Haffenreffer, RN, MBA www.consultdemi.net The path we are taking today! The requirements at F944 (formerly F520) Key elements Survey
Violence and Aggression NICE guideline Important implications for practice. Peter Tyrer, Imperial College, London
 Violence and Aggression NICE guideline Important implications for practice Peter Tyrer, Imperial College, London Reason for update of 2005 guideline This guideline was felt to be a little too restrictive
Violence and Aggression NICE guideline Important implications for practice Peter Tyrer, Imperial College, London Reason for update of 2005 guideline This guideline was felt to be a little too restrictive
Sexuality in Nursing Homes Healthy Sex Lives v. Sexually Aggressive, Demented Residents
 Sexuality in Nursing Homes Healthy Sex Lives v. Sexually Aggressive, Demented Residents http://hereandnow.wbur.org/2013/08/01/nur sing-home-sex 1 Question Research shows that nursing home residents are
Sexuality in Nursing Homes Healthy Sex Lives v. Sexually Aggressive, Demented Residents http://hereandnow.wbur.org/2013/08/01/nur sing-home-sex 1 Question Research shows that nursing home residents are
A REVIEW OF THE USE OF ANTIPSYCHOTIC DRUGS IN BRITISH COLUMBIA RESIDENTIAL CARE FACILITIES. Ministry of Health
 A REVIEW OF THE USE OF ANTIPSYCHOTIC DRUGS IN BRITISH COLUMBIA RESIDENTIAL CARE FACILITIES Ministry of Health December 2011 An adult person in care has the right to the protection and promotion of his
A REVIEW OF THE USE OF ANTIPSYCHOTIC DRUGS IN BRITISH COLUMBIA RESIDENTIAL CARE FACILITIES Ministry of Health December 2011 An adult person in care has the right to the protection and promotion of his
Palliative and Hospice Care In the United States Jean Root, DO
 Palliative and Hospice Care In the United States Jean Root, DO Hello. My name is Jean Root. I am an Osteopathic Physician who specializes in Geriatrics, or care of the elderly. I teach and practice Geriatric
Palliative and Hospice Care In the United States Jean Root, DO Hello. My name is Jean Root. I am an Osteopathic Physician who specializes in Geriatrics, or care of the elderly. I teach and practice Geriatric
Link download full: Test bank for Varcarolis's Canadian Psychiatric Mental Health Nursing 1e Edition by Margaret Jordan Halter
 Varcarolis s Canadian Psychiatric Mental Health Nursing: Canadian Edition Test Bank Halter Link download full: Test bank for Varcarolis's Canadian Psychiatric Mental Health Nursing 1e Edition by Margaret
Varcarolis s Canadian Psychiatric Mental Health Nursing: Canadian Edition Test Bank Halter Link download full: Test bank for Varcarolis's Canadian Psychiatric Mental Health Nursing 1e Edition by Margaret
Texas Administrative Code
 RULE 19.1201 Physician Services A physician must personally approve in writing a recommendation that an individual be admitted to a facility. Each resident must remain under the care of a physician. The
RULE 19.1201 Physician Services A physician must personally approve in writing a recommendation that an individual be admitted to a facility. Each resident must remain under the care of a physician. The
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/16/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/16/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
STATE OF CONNECTICUT DEPARTMENT OF DEVELOPMENTAL SERVICES
 STATE OF CONNECTICUT DEPARTMENT OF DEVELOPMENTAL SERVICES Procedure No. I.E.PR.003 Issue Date: October 28, 2003 Subject: Behavior Modifying Medications Effective Date: Upon Release Section: Health and
STATE OF CONNECTICUT DEPARTMENT OF DEVELOPMENTAL SERVICES Procedure No. I.E.PR.003 Issue Date: October 28, 2003 Subject: Behavior Modifying Medications Effective Date: Upon Release Section: Health and
ROTATION DESCRIPTION
 ROTATION TITLE Psychiatry Pediatrics (PGY2) ROTATION DESCRIPTION PURPOSE The psychiatry rotation is designed to allow the resident to further refine skills in therapeutics, pharmacokinetics, drug information,
ROTATION TITLE Psychiatry Pediatrics (PGY2) ROTATION DESCRIPTION PURPOSE The psychiatry rotation is designed to allow the resident to further refine skills in therapeutics, pharmacokinetics, drug information,
Mental Health Centers
 SECTION 2 Table of Contents 1. GENERAL POLICY... 3 1-1 Authority... 3 1-2 Qualified Mental Health Providers... 3 1-3 Definitions... 3 1-4 Scope of Services... 4 1-5 Provider Qualifications... 4 1-6 Evaluation
SECTION 2 Table of Contents 1. GENERAL POLICY... 3 1-1 Authority... 3 1-2 Qualified Mental Health Providers... 3 1-3 Definitions... 3 1-4 Scope of Services... 4 1-5 Provider Qualifications... 4 1-6 Evaluation
The policy applies to all SHS employees involved in direct patient care and medical staff.
 Restraints Use of Violent - System Introduction Restraints, Use of Violent System Introduction SCOPE The policy applies to all SHS employees involved in direct patient care and medical staff. Implementation
Restraints Use of Violent - System Introduction Restraints, Use of Violent System Introduction SCOPE The policy applies to all SHS employees involved in direct patient care and medical staff. Implementation
ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists
 DECLINE Facility Assessment Checklists") ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to activities of daily living
ACTIVITIES OF DAILY LIVING (ADL) DECLINE Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to activities of daily living
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS
 MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
PART 512 Personalized Recovery Oriented Services
 PART 512 Personalized Recovery Oriented Services (Statutory authority: Mental Hygiene Law 7.09[b], 31.04[a], 41.05, 43.02[a]-[c]; and Social Services Law, 364[3], 364-a[1]) Sec. 512.1 Background and intent.
PART 512 Personalized Recovery Oriented Services (Statutory authority: Mental Hygiene Law 7.09[b], 31.04[a], 41.05, 43.02[a]-[c]; and Social Services Law, 364[3], 364-a[1]) Sec. 512.1 Background and intent.
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL
 CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
NURS 147A NURSING PRACTICUM PSYCHIATRIC/MENTAL HEALTH NURSING CLINICAL EVALUATION CRITERIA. SAN JOSE STATE UNIVERSITY School of Nursing
 SAN JOSE STATE UNIVERSITY School of Nursing NURS 147A - Nursing Practicum IVA - 2 Units Psychiatric/Mental Health Nursing Based on Scope and Standards of Psychiatric-Mental Health Nursing Practice (AP,
SAN JOSE STATE UNIVERSITY School of Nursing NURS 147A - Nursing Practicum IVA - 2 Units Psychiatric/Mental Health Nursing Based on Scope and Standards of Psychiatric-Mental Health Nursing Practice (AP,
RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care. Recommendation Comparison Chart
 RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care Recommendation Comparison Chart RECOMMENDATIONS FROM SCREENING FOR DELIRIUM, DEMENTIA AND DEPRESSION IN THE OLDER ADULT (2010)
RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care Recommendation Comparison Chart RECOMMENDATIONS FROM SCREENING FOR DELIRIUM, DEMENTIA AND DEPRESSION IN THE OLDER ADULT (2010)
Highlights of the New LTCSP and Regulations
 Highlights of the New LTCSP and Regulations New York State Department of Health Division of Nursing Homes and ICF/IID Surveillance November 15, 2017 November 15, 2017 2 Resources https://www.cms.gov/medicare/provider-enrollment-andcertification/guidanceforlawsandregulations/nursinghomes.html
Highlights of the New LTCSP and Regulations New York State Department of Health Division of Nursing Homes and ICF/IID Surveillance November 15, 2017 November 15, 2017 2 Resources https://www.cms.gov/medicare/provider-enrollment-andcertification/guidanceforlawsandregulations/nursinghomes.html
4. Hospital and community pharmacies
 4. Hospital and community pharmacies As FIP is the international professional organisation of pharmacists, this paper emphasises the role of the pharmacist in ensuring and increasing patient safety. The
4. Hospital and community pharmacies As FIP is the international professional organisation of pharmacists, this paper emphasises the role of the pharmacist in ensuring and increasing patient safety. The
APPENDIX I HOSPICE INPATIENT FACILITY (HIF)
") INTRODUCTION APPENDIX I HOSPICE INPATIENT FACILITY (HIF) The principles and standards in all chapters of the Standards of Practice for Hospice Programs apply to hospice care provided in an inpatient facility.
INTRODUCTION APPENDIX I HOSPICE INPATIENT FACILITY (HIF) The principles and standards in all chapters of the Standards of Practice for Hospice Programs apply to hospice care provided in an inpatient facility.
SECTION P: RESTRAINTS
 SECTION P: RESTRAINTS Intent: The intent of this section is to record the frequency over the 7-day look-back period that the resident was restrained by any of the listed devices at any time during the
SECTION P: RESTRAINTS Intent: The intent of this section is to record the frequency over the 7-day look-back period that the resident was restrained by any of the listed devices at any time during the
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care
 Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
POLICY AND PROCEDURE RESTRAINT/SECLUSION, MEDICAL CENTER PATIENT CARE Effective Date: March 2010
 Number: MS 08:03:05 Submitted by: BEHAVIORAL HEALTH CLINICAL PRACTICE TEAM Issuing Department: PATIENT CARE SERVICES Approved By: Reviewed by: Date: Patient Care Practice & 12/09 Outcomes David W. Cress,
Number: MS 08:03:05 Submitted by: BEHAVIORAL HEALTH CLINICAL PRACTICE TEAM Issuing Department: PATIENT CARE SERVICES Approved By: Reviewed by: Date: Patient Care Practice & 12/09 Outcomes David W. Cress,
Vanderbilt & Qsource Webinar Series
 Vanderbilt & Qsource Webinar Series Vanderbilt University Medical Center Vanderbilt University Center for Quality Aging Qsource Session #1: Introduction to Dementia Care & QAPI Session #2: Dementia & Behavioral
Vanderbilt & Qsource Webinar Series Vanderbilt University Medical Center Vanderbilt University Center for Quality Aging Qsource Session #1: Introduction to Dementia Care & QAPI Session #2: Dementia & Behavioral
APPENDIX B. Physician Assistant Competencies: A Self-Evaluation Tool
 APPENDIX B Physician Assistant Competencies: A Self-Evaluation Tool Rate your strength in each of the competencies using the following scale: 1 = Needs Improvement 2 = Adequate 3 = Strong 4 = Very Strong
APPENDIX B Physician Assistant Competencies: A Self-Evaluation Tool Rate your strength in each of the competencies using the following scale: 1 = Needs Improvement 2 = Adequate 3 = Strong 4 = Very Strong
DIVISION OF MENTAL HEALTH AND ADDICTION SERVICES ADMINISTRATIVE BULLETIN A.B. 5:04B
 DIVISION OF MENTAL HEALTH AND ADDICTION SERVICES ADMINISTRATIVE BULLETIN A.B. 5:04B EFFECTIVE DATE: June 4, 2012 SUBJECT: The Non-Emergent Administration of Psychotropic Medication to Non-Consenting Involuntary
DIVISION OF MENTAL HEALTH AND ADDICTION SERVICES ADMINISTRATIVE BULLETIN A.B. 5:04B EFFECTIVE DATE: June 4, 2012 SUBJECT: The Non-Emergent Administration of Psychotropic Medication to Non-Consenting Involuntary
The Good Samaritan Society CHOICE Program. Client Handbook. In Co-operation with Alberta Health Services
 The Good Samaritan Society CHOICE Program Client Handbook In Co-operation with Alberta Health Services We Want to Hear from You We are committed to providing a high standard of care, tailored to fit your
The Good Samaritan Society CHOICE Program Client Handbook In Co-operation with Alberta Health Services We Want to Hear from You We are committed to providing a high standard of care, tailored to fit your