|
|
|
- Tobias Higgins
- 5 years ago
- Views:
Transcription
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57 AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2010 B E T W E E N: NORTH SIMCOE MUSKOKA LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) - and - MUSKOKA ALGONQUIN HEALTHCARE (the Hospital ) WHEREAS the LHIN and the Hospital (together the Parties ) entered into a two year service accountability agreement that took effect April 1, 2008 (the H-SAA ); AND WHEREAS given economic uncertainties, funding allocations by the Ministry of Health and Long-Term Care which form the basis for the negotiation of the H-SAA have not yet been confirmed; AND WHEREAS the OHA, LHINs and the Ministry of Health and Long-Term Care have agreed to adjust the H-SAA process for 2010/11, as set out in the letter dated February 1, 2010 and attached as Appendix A; AND WHEREAS the Parties acknowledge a mutual commitment to pursuing needed operational efficiencies over the course of the agreement; AND WHEREAS the LHIN and the Hospital have agreed to extend the H-SAA for a third year; NOW THEREFORE in consideration of mutual promises and agreements contained in this Agreement and other good and valuable consideration, the Parties agree as follows: 1.0 Definitions. Except as otherwise defined in this Agreement, all terms shall have the meaning ascribed to them in the H-SAA. 2.0 Amendments. 2.1 Agreed Amendments. The Parties agree that the H-SAA shall be amended as set out in this Article Title and Headers. The Parties agree that the title of the H-SAA and the headers within the H-SAA shall be amended by deleting and replacing it with H-SAA Amending Agreement Page 1 of 14
58 2.3 Definitions. The definition for HAPS in Article 2.1 shall be amended with the addition of the following text immediately after and before the semicolon: and the Board approved hospital accountability planning submission provided by the Hospital to the LHIN for the Fiscal Year Term. The reference to 2010 in Article 3.2, shall be deleted and replaced with March 31, Planning Cycle. The words for Fiscal Years 2010/11 and 2011/12 in Article 7.1 shall be deleted. 2.6 Schedules. (a) Schedule A shall be deleted and replaced with the Schedule A included in this Agreement. (b) Schedule B shall be supplemented with the addition of Schedule B-1 included in this Agreement. (c) Schedule C shall be supplemented with the addition of Schedule C-1 included in this agreement. (d) Schedule D shall be supplemented with the addition of Schedule D-1 included in this agreement. (e) Schedule E shall be supplemented with the addition of Schedule E-1 included in this agreement. (f) Schedule F shall be supplemented with the addition of Schedule F-1 included in this agreement. (g) Schedule G shall be supplemented with the addition of Schedule G-1 included in this agreement. (h) Schedule H shall be supplemented with the addition of Schedule H-1 included in this agreement. 2.7 Renegotiation of Schedules. The Parties agree that it is their intention to negotiate and to further amend the Schedules following the announcement of funding allocations by the Ministry of Health and Long-Term Care. It is recognized that a waiver to the balanced budget obligation may need to be negotiated. 3.0 Effective Date. The Parties agree that the amendments set out in Article 2 shall take effect on April 1, All other terms of the H-SAA, including but not limited to current funding levels and those provisions in Schedules A-H not amended by s. 2.6, above, shall remain in full force and effect. H-SAA Amending Agreement Page 2 of 14
59
60 Schedule A Planning and Funding Timetable OBLIGATIONS Part I - Funding Obligations Party Timing Announcement of multi-year funding allocation (confirmation of 2008/09 Schedule C funding, reinforcement of 2009/10 Schedule C funding) LHIN The later of June 30, 2008 or 14 days after confirmation from the Ministry of Health and Long Term Care Announcement of multi-year funding allocation (confirmation of 2009/10 Schedule C funding) LHIN The later of June 30, 2009 or 14 days after confirmation from the Ministry of Health and Long Term Care Announcement of multi-year funding allocation (confirmation of 20010/11 Schedule C funding) LHIN The later of June 30, 2010 or 14 days after confirmation from the Ministry of Health and Long Term Care H-SAA Amending Agreement Page 4 of 14
61 Schedule A Planning and Funding Timetable Part II - Planning Obligations Party Timing Announcement of 2010/11 planning target for hospital planning purposes LHIN The later of June 30, 2008 or 14 days after confirmation from the Ministry of Health and Long Term Care Publication of the Hospital Annual Planning Submission Guidelines for LHIN No later than June 30, 2009 Announcement of multi-year funding allocation (reaffirm 2010/11 and announce 2011/12 planning targets for HSAA negotiations) LHIN The later of June 30, 2009 or 14 days after confirmation from the Ministry of Health and Long-Term Care Indicator Refresh (including detailed hospital calculations) LHIN (in conjunction with MOHLTC) No later than November 30, 2009 Refresh related Schedules for Hospital/LHIN No later than February 26, 2010 Sign 1 year extension to the 2008/10 H-SAA Hospital/LHIN No later than March 31, 2010 Announcement of multi-year funding allocation for 2010/11 and announce, if possible, planning targets for 2011/13 HSAA negotiations) Submission of Hospital Annual Planning Submission for LHIN Hospital 14 days after confirmation from the Ministry of Health and Long-Term Care To be determined Publication of the Hospital Annual Planning Submission Guidelines for 2011/13 LHIN No later than June 30, 2010 Announcement of multi-year planning targets for 2011/13 H-SAA negotiations) LHIN 14 days after confirmation from the Ministry of Health and Long-Term Care Submission of Hospital Annual Planning Submission for Hospital No later than October 31, 2010 Indicator Refresh (including detailed hospital calculations) LHIN (in conjunction with MOHLTC) No later than November 30, 2010 Refresh the Hospital Annual Planning Submission for and related Schedules Hospital/LHIN No later than January 31, 2011 Sign Hospital Service Accountability Agreement Hospital/LHIN No later than March 31, 2011 H-SAA Amending Agreement Page 5 of 14
62 Schedule A Planning and Funding Timetable Obligation Timeline Diagram Definitions: Planning Target = For negotiations Confirm = Confirm signed agreement amounts after appropriation of monies by the Legislature of Ontario Funding Year 06/07 07/08 08/09 09/10 10/11 11/12 12/13 13/ /08 HAA H-SAA June 06 Confirm Schedule C Funding Planning Target Planning Target June 07 Confirm Schedule C Funding Planning Target (Oct) Planning Target (Oct) Feb. 08 Negotiated Schedule C Funding Negotiated Schedule C Funding June 08 Confirm Schedule C Funding Reaffirm Schedule C Funding Planning Target June 09 Confirm Schedule C Funding Planning Target Feb. 10 Negotiated Schedule C Funding June 10 Confirm Schedule C Funding Funding Obligations are shaded Planning Obligations are not shaded H-SAA Amending Agreement Page 6 of 14
63 Schedule B-1 Performance Obligations for 10/ PERFORMANCE CORRIDORS FOR SERVICE VOLUMES AND PERFORMANCE INDICATORS 1.1 The provisions of Article 1 of Schedule B apply in fiscal year 10/11 with all references to Schedule D being read as referring to Schedule D PERFORMANCE CORRIDORS FOR PERFORMANCE INDICATORS 2.1 The provisions of Article 2 of Schedule B apply in fiscal year 10/11 subject to the following amendments: (a) sub articles 2.2, 2.3 and 2.6 shall be deleted; and (b) all references to Schedule D shall be read as referring to Schedule D PERFORMANCE OBLIGATIONS WITH RESPECT TO NURSING ENHANCEMENT/CONVERSION 3.1 The provisions of Article 3 of Schedule B apply in fiscal year 10/11with all references to Schedule D being read as referring to Schedule D PERFORMANCE OBLIGATIONS WITH RESPECT TO CRITICAL CARE 4.1 The provisions of Article 4 of Schedule B apply in fiscal year 10/11 subject to the following amendments: (a) references to 2008/09 and 2009/10 shall be read as referring to 2010/11. (b) all references to Schedule E shall be read as referring to Schedule E PERFORMANCE OBLIGATIONS WITH RESPECT TO POST CONSTRUCTION OPERATING PLAN FUNDING AND VOLUME 5.1 The provisions of Article 5 of Schedule B apply in fiscal year 10/11, subject to the following amendments: (a) references to Schedule F shall be read as referring to Schedule F-1; (b) references to 2008/09 and 09/10 shall be read as referring to 2010/ PERFORMANCE OBLIGATIONS WITH RESPECT TO PROTECTED SERVICES 6.1 The Performance Obligations set out in Article 6 of Schedule B apply in fiscal year 10/11, subject to the following amendments: (a) (b) All references to Schedule D or Schedule G shall be read as referring to Schedules D-1 and G-1 respectively; and All references to 2008/09 and 09/10 shall be read as referring to 2010/11 H-SAA Amending Agreement Page 7 of 14
64 7.0 PERFORMANCE OBLIGATIONS WITH RESPECT TO WAIT TIME SERVICES 7.1 The Performance Obligations set out in Article 7 of Schedule B apply to fiscal year 10/11 with all references to Schedules A, G, or H being read as referring to Schedules A-1, G-1 or H-1 respectively. 8.0 REPORTING OBLIGATIONS 8.1 The reporting obligations set out in Article 8 of Schedule B apply to fiscal year 10/ The following reporting obligations are added to Article 8 of Schedule B: (a) French Language Services. If the Hospital is required to provide services to the public in French under the provisions of the French Language Services Act, the Hospital will be required to submit a French language implementation report to the LHIN. If the Hospital is not required to provide services to the public in French under the provisions of the French Language Service Act, it will be required to provide a report to the LHIN that outlines how the Hospital addresses the needs of its local Francophone community. 9.0 LHIN SPECIFIC PERFORMANCE OBLIGATIONS 9.1 Except where specifically limited to a given year, the obligations set out in Article 9 of Schedule B apply to fiscal 10/11. Without limiting the foregoing, waivers or conditional waivers for 08/09 and 09/10 do not apply to 10/11. H-SAA Amending Agreement Page 8 of 14
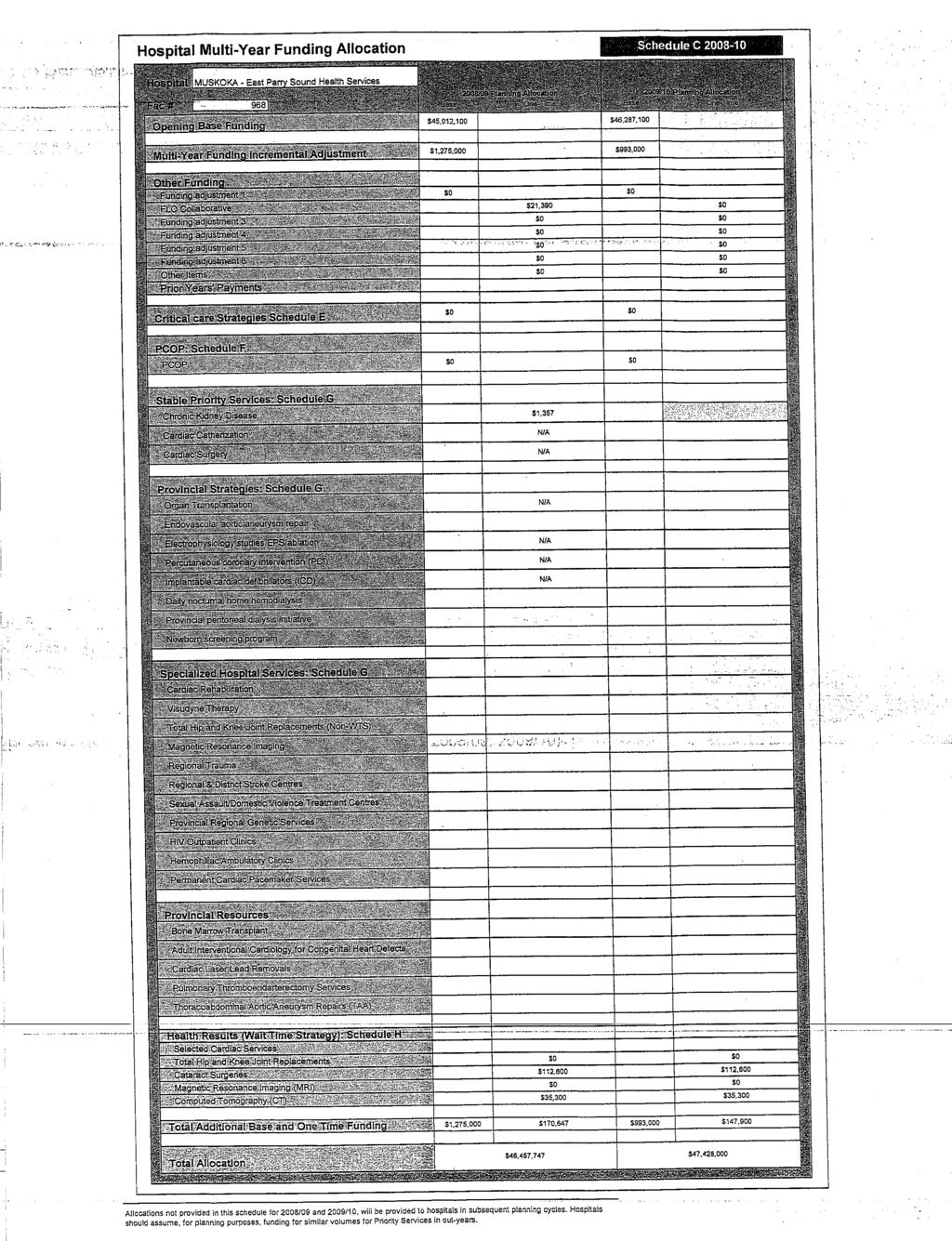
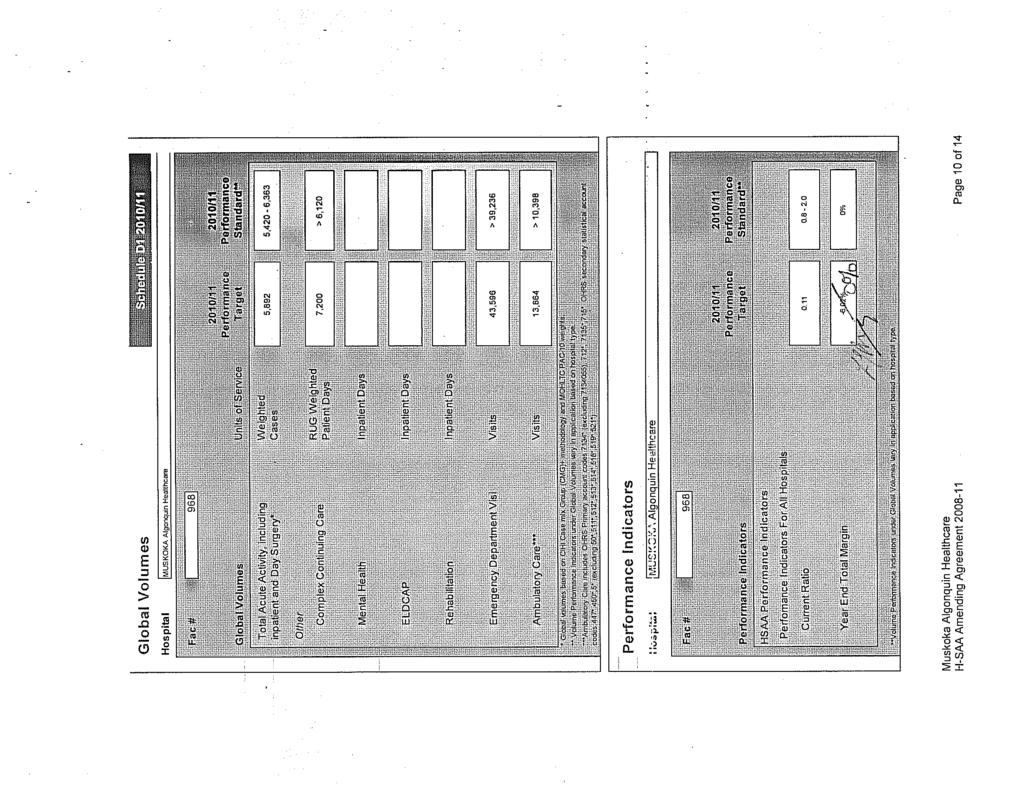
65 Hospital Multi-Year Funding Allocation Schedule C1 2010/11 Hospital MUSKOKA Algonquin Healthcare 2010/11 Planning Allocation Fac # 968 Base One-Time Opening Base Funding $47,488,800 Multi-Year Funding Incremental Adjustment Other Funding Funding Formula Increases $738,000 Nurse Practitioners $123,000 Aging at Home Strategy: Transitional Care Beds $240,000 Pay for Results Program - Initial Allocation $464,800 Funding to address Structural Deficit $4,500,000 Funding adjustment 6 ( ) Funding adjustment 7 ( ) Other Items Prior Years' Payments Critical care Strategies Schedule E PCOP: Schedule F PCOP Stable Priority Services: Schedule G Chronic Kidney Disease Cardiac Catherization Cardiac Surgery Provincial Strategies: Schedule G Organ Transplantation Endovascular aortic aneurysm repair Electrophysiology studies EPS/ablation Percutaneous coronary intervention (PCI) Implantable cardiac defibrillators (ICD) Daily nocturnal home hemodialysis Provincial peritoneal dialysis initiative Newborn screening program Specialized Hospital Services: Schedule G Cardiac Rehabilitation Visudyne Therapy Total Hip and Knee Joint Replacements (Non-WTS) Magnetic Resonance Imaging Regional Trauma Regional & District Stroke Centres Sexual Assault/Domestic Violence Treatment Centres Provincial Regional Genetic Services HIV Outpatient Clinics Hemophiliac Ambulatory Clinics Permanent Cardiac Pacemaker Services Provincial Resources Bone Marrow Transplant Adult Interventional Cardiology for Congenital Heart Defects Cardiac Laser Lead Removals Pulmonary Thromboendarterectomy Services Thoracoabdominal Aortic Aneurysm Repairs (TAA) Health Results (Wait Time Strategy): Schedule H Selected Cardiac Services Total Hip and Knee Joint Replacements Cataract Surgeries (147 volumes) $110,300 Magnetic Resonance Imaging (MRI) Computed Tomography (CT 148 hours) $37,000 Total Additional Base and One Time Funding $5,361,000 $852,100 Total Allocation $53,701,900 Allocations not provided in this schedule for 2010/11, will be provided to hospitals in subsequent planning cycles. Hospitals should assume, for planning purposes, funding for similar volumes for Priority Services in out-years. H-SAA Amending Agreement Page 9 of 14
66
67 Critical Care Funding Schedule E1 2010/11 Hospital MUSKOKA Algonquin Healthcare This section has been intentionally left blank Once negotiated, an amendment will be made under section 15.3 of the Agreement to include these targets and any additional conditions not otherwise set out in Schedule B or B1. This funding would be an additional in-year allocation contemplated by section 5.3 of the Agreement H-SAA Amending Agreement Page 11 of 14
68 Post-Construction Operating Plan Funding and Volum Schedule F1 2010/11 Hospital MUSKOKA Algonquin Healthcare This section has been intentionally left blank Once negotiated, an amendment (Sch F1.1) will be made under section 15.3 of the Agreement to include these targets and any additional conditions not otherwise set out in Schedule B or B1. This funding would be an additional in-year allocation contemplated by section 5.3 of the Agreement H-SAA Amending Agreement Page 12 of 14
69 Protected Services Schedule G1 2010/11 Hospital Fac # MUSKOKA Algonquin Healthcare 968 Stable Priority Services Units of Service 2010/11 Performance Target 2010/11 Performance Standard 2011/12 LHIN Plan Chronic Kidney Disease Weighted Units 3,122 3,122 3,122 Cardiac Catherization Cardiac Surgery Procedures Weighted Units Provincial Strategies Organ Transplantation* Endovascular aortic aneurysm repair Electrophysiology studies EPS/ablation Percutaneous coronary intervention (PCI) Implantable cardiac defibrillators (ICD) Daily nocturnal home hemodialysis Provincial peritoneal dialysis initiative Newborn screening program Cases Specialized Hospital Services Cardiac Rehabilitation Visudyne Therapy Total Hip and Knee Joint Replacements (Non-WTS) Magnetic Resonance Imaging Regional Trauma Number of patients treated Number of insured Visudyne vials Number of Implant Devices Hours of operation Cases Regional & District Stroke Centres Sexual Assault/Domestic Violence Treatment Centres Provincial Regional Genetic Services HIV Outpatient Clinics Hemophiliac Ambulatory Clinics Permanent Cardiac Pacemaker Services Provincial Resources Bone Marrow Transplant Adult Interventional Cardiology for Congenital Heart Defects Cardiac Laser Lead Removals Pulmonary Thromboendarterectomy Services Thoracoabdominal Aortic Aneurysm Repairs (TAA) * Organ Transplantation - Funding for living donation (kidney & liver) included as part of organ transplantation funding. Hospitals are funded retrospectively for deceased donor management activity, reported and validated by the Trillium Gift of Life Network. Note: Additional accountabilities assigned in Schedule B, B1 Funding and volumes for these services should be planned for based on 2009/10 approved allocations. Amendments, pursuant to section 5.2 of this Agreement, may be made during the quarterly submission process. H-SAA Amending Agreement Page 13 of 14
70 Wait Time Services Schedule H1 2010/11 Hospital MUSKOKA Algonquin Healthcare Fac # /10 Funded 2010/11 Funded Base Volumes Incremental Volumes ** Base Volumes Incremental Volumes ** Selected Cardiac Services Refer to Schedule G for Cardiac Service Volumes and Targets Total Hip and Knee Joint Replacements (Total Implantations) Cataract Surgeries (Total Procedures) Magnetic Resonance Imaging (MRI) (Total Hours) Computed Tomography (CT) (Total Hours) 1, , * The 2009/10 Funded volumes are as a reference only ** Once negotiated, an amendment will be made under section 15.3 of the Agreement to include these targets and any additional conditions not otherwise set out in Schedule B, B1. This funding would be an additional in-year allocation contemplated by section 5.3 of the Agreement. H-SAA Amending Agreement Page 14 of 14
71
72
73
74 H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2011 B E T W E E N: NORTH SIMCOE MUSKOKA LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND MUSKOKA ALGONQUIN HEALTHCARE (the Hospital ) WHEREAS the LHIN and the Hospital (together the Parties ) entered into a two year hospital service accountability agreement that took effect April 1, 2008 (the H-SAA ); AND WHEREAS pursuant to an amending agreement effective as of April 1, 2010 (the "1st Amending Agreement") the H-SAA was amended and extended effective April 1, 2010; AND WHEREAS the LHIN and the Hospital have agreed to extend the H-SAA for a fourth year; NOW THEREFORE in consideration of mutual promises and agreements contained in this Agreement and other good and valuable consideration, the parties agree as follows: 1.0 Definitions. Except as otherwise defined in this Agreement, all terms shall have the meaning ascribed to them in the H-SAA. References in this Agreement to the H-SAA mean the H-SAA as amended and extended by the 1 st Amending Agreement. 2.0 Amendments. 2.1 Agreed Amendments. The Parties agree that the H-SAA shall be amended as set out in this Article Title and Headers. The Parties agree that the title of the H-SAA and the headers within the H-SAA shall be amended by deleting and replacing it with Definitions. (a) The following new definition will be added: Explanatory Indicator means a measure of hospital performance for which no Performance Target is set. H-SAA Amending Agreement Page 1 of 31
75 (b) The definition for HAPS in Article 2.1 shall be deleted and replaced with: HAPS means the Board-approved hospital accountability planning submission provided by the Hospital to the LHIN for the Fiscal years , , and ; (c) The following new definition will be added: Accountability Agreement means the Accountability Agreement in effect between the LHIN and the MOHLTC during a Fiscal Year. (d) The terms Performance Indicator and Performance Indicators shall be deleted and replaced with Accountability Indicator and Accountability Indicators respectively. 2.4 Term. The reference to March 31, 2011 in Article 3.2 shall be deleted and replaced with March 31, Remedies for Non-Compliance. The words for Fiscal Year 2009/10 shall be deleted from Article 12.1(i)(a). 2.6 Schedules. (a) (b) (c) (d) (e) (f) (g) (h) Schedule A shall be supplemented with the addition of Schedule A1 attached to this Agreement. Schedules B and B1 shall be supplemented with the addition of Schedule B2 attached to this Agreement. Schedules C and C1 shall be supplemented with the addition of Schedule C2 attached to this Agreement. Schedules D and D1 shall be supplemented with the addition of Schedule D-2 attached to this Agreement. Schedules E and E1 shall be supplemented with the addition of Schedule E2 attached to this Agreement. Schedules F and F1 shall be supplemented with the addition of Schedule F2 attached to this Agreement. Schedules G and G1 shall be supplemented with the addition of Schedule G2 attached to this Agreement. Schedules H and H1 shall be supplemented with the addition of Schedule H2 attached to this Agreement. 2.7 Renegotiation of Schedules. The Parties agree that it is their intention to negotiate and to further amend the Schedules following the announcement of funding allocations by the MOHLTC. H-SAA Amending Agreement Page 2 of 31
76
77 Schedule A1 Planning and Funding Timetable OBLIGATIONS Part I - Funding Obligations Party Timing Announcement of hospital-specific base funding allocation LHIN The later of June 30, 2011or 21 Days after confirmation from the MOHLTC Part II - Planning Obligations Party Timing Sign 1 year extension to the Hospital Service Accountability Agreement Announcement of multi-year planning targets for Hospital Service Accountability Agreement negotiations* Publication of the Hospital Accountability Planning Submission Guidelines for * Hospital/LHIN No later than March 31, 2011 LHIN LHIN Contingent upon MOHLTC announcement and direction Fiscal quarter following MOHLTC direction regarding new multi-year agreements Indicator Refresh (including detailed hospital calculations)* Submission of Hospital Accountability Planning Submission for * LHIN (in conjunction with MOHLTC) Hospital Contingent upon announcement and timing of multi-year planning targets Contingent upon announcement and timing of multi-year planning targets and provincial HAPS /Hospital Service Accountability Agreement process Sign Hospital Service Accountability Agreement * Hospital/LHIN No later than March 31, 2012 * Intended process based on timely announcement of multi-year planning targets from the MOHLTC. Actual process may change to adapt to timing and duration of the planning targets actually announced by the MOHLTC. H-SAA Amending Agreement Page 4 of 31
78 Schedule B2 Performance Obligations for 11/ PERFORMANCE CORRIDORS FOR SERVICE VOLUMES AND ACCOUNTABILITY INDICATORS 1.1 The provisions of Article 1 of Schedule B apply in Fiscal Year 11/12 with all references to Schedule D being read as referring to Schedule D PERFORMANCE CORRIDORS FOR ACCOUNTABILITY INDICATORS 2.1 The provisions of Article 2 of Schedule B, as amended by B1, apply in Fiscal Year 11/12 subject to the following amendments: (a) new sub articles 2.7, 2.8 and 2.9 shall be added as set out below; th Percentile Emergency Room (ER) Length of Stay for Admitted Patients a) Definition. The total emergency room (ER) length of stay (LOS) where 9 out of 10 admitted patients completed their visits. ER LOS is defined as the time from triage or registration, whichever comes first, to the time the patient leaves the ER. Steps: 1: Calculate ER LOS in hours for each patient. 2: Apply inclusion and exclusion criteria. 3: Sort the cases by ER LOS from shortest to highest. 4: The 90 th percentile is the case where 9 out of 10 admitted patients have completed their visits. Excludes: 1. ER visits where Registration Date/Time and Triage Date/Time are both missing; 2. ER visits where Left ER Date/Time and Disposition Date/Time are both missing; 3. ER visits where patients are over the age of 125 on earlier of triage or registration date; 4. Negative ER LOS (earlier of registration or triage after date/time patient left ER); 5. Duplicate records within the same functional centre where all data elements have the same values, except Abstract ID number; 6. Non-Admitted Patients (Disposition Codes and 08 15); and H-SAA Amending Agreement Page 5 of 31
79 7. Admitted Patients (Disposition Codes 06 and 07) with missing patient left ER Date/Time. b) LHIN Target (i) (ii) For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Target: maintain or improve current performance For hospitals performing above the LHIN s Accountability Agreement target: Performance Target: To be negotiated locally taking into consideration contribution to the MLPA target c) Performance Corridor (i) (ii) For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Corridor: equal to or less than the LHIN s Accountability Agreement target For hospitals performing above the LHIN s Accountability Agreement target: Performance Corridor: 10% th Percentile ER Length of Stay for Non-Admitted Complex (CTAS I-III) Patients a) Definition. The total emergency room (ER) length of stay (LOS) where 9 out of 10 non-admitted complex (Canadian Triage and Acuity Scale (CTAS) levels I, II and III) patients completed their visits. ER LOS is defined as the time from triage or registration, whichever comes first, to the time the patient leaves ER. Steps 1. Calculate ER LOS in hours for each patient. 2. Apply inclusion and exclusion criteria. 3. Sort the cases by ER LOS from shortest to highest. 4. The 90 th percentile is the case where 9 out of 10 nonadmitted patients have completed their visits. Excludes: 1. ER visits where Registration Date/Time and Triage Date/Time are both missing; H-SAA Amending Agreement Page 6 of 31
80 2. ER visits where Left ER Date/Time and Disposition Date/Time are both missing; 3. ER visits where patients are over the age of 125 on earlier of triage or registration date; 4. Negative ER LOS (earlier of registration or triage after date/time patient left ER); 5. Duplicate records within the same functional centre where all data elements have the same values; 6. ER visits identified as the patient has left ER without being seen (Disposition Codes 02 and 03); 7. Admitted Patients (Disposition Codes 06 and 07); 8. Non-Admitted Patients (Disposition Codes 01, and 08 15) with assigned CTAS IV and V; 9. Non-Admitted Patients (Disposition Codes 01, and 08 15) with missing CTAS; and 10. Transferred Patients (Disposition Codes 08 and 09) with missing patient left ER Date/Time. b) LHIN Targets (i) (ii) For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Target: maintain or improve current performance For hospitals performing above the LHIN s Accountability Agreement target with Pay for Results Funding: Performance Target: To be negotiated locally taking into consideration contribution to the LHIN s Accountability Agreement target c) Performance Corridors (i) (ii) For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Corridor: equal to or less than the LHIN s Accountability Agreement target For hospitals performing above the LHIN s Accountability Agreement target: Performance Corridor: 10% th Percentile ER Length of Stay for Non-admitted Minor Uncomplicated (CTAS IV-V) Patients a) Definition. The total emergency room (ER) length of stay (LOS) where 9 out of 10 non-admitted minor/uncomplicated (Canadian Triage and Acuity Scale (CTAS) levels IV and V) patients completed their visits. ER LOS is defined as the time from triage H-SAA Amending Agreement Page 7 of 31
81 or registration, whichever comes first, to the time the patient leaves the ER. Steps 1. Calculate ER LOS in hours for each patient. 2. Apply inclusion and exclusion criteria. 3. Sort the cases by ER LOS from shortest to highest. 4. The 90 th percentile is the case where 9 out of 10 nonadmitted patients have completed their visits. Excludes: 1. ER visits where Registration Date/Time and Triage Date/Time are both missing; 2. ER visits where Left ER Date/Time and Disposition Date/Time are both missing; 3. ER visits where patients are over the age of 125 on earlier of triage or registration date; 4. Negative ER LOS (earlier of registration or triage after date/time patient left ER); 5. Duplicate records within the same functional centre where all data elements have the same values; 6. ER visits identified as the patient has left ER without being seen (Disposition Codes 02 and 03); 7. Admitted Patients (Disposition Codes 06 and 07); 8. Non-Admitted Patients (Disposition Codes 01, and 08 15) with assigned CTAS I, II and III; 9. Non-Admitted Patients (Disposition Codes 01, and 08 15) with missing CTAS; and 10. Transferred Patients (Disposition Codes 08 and 09) with missing patient left ER Date/Time. b) LHIN Target (i) (ii) For hospitals performing at the LHIN s Accountability Agreement target or better: PerformanceTarget: maintain or improve current performance For hospitals performing above the LHIN s Accountability Agreement target: Performance Target: To be negotiated locally taking into consideration contribution to the LHIN s Accountability Agreement target c) Performance Corridor (i) For hospitals performing at the LHIN s Accountability Agreement target or better: H-SAA Amending Agreement Page 8 of 31
82 Performance Corridor: less than or equal to the LHIN s Accountability Agreement target (ii) For hospitals performing above the LHIN s Accountability Agreement target with Pay for Results Funding: Performance Corridor: 10% and (b) All references to Schedule D1 shall be read as referring to Schedule D PERFORMANCE OBLIGATIONS WITH RESPECT TO NURSING ENHANCEMENT/CONVERSION 3.1 The provisions of Article 3 of Schedule B, as amended by B1 apply in Fiscal Year 11/12 subject to the following amendments: (a) subsection 3.1 and 3.2(b) shall be deleted; and (b) all references to Schedule D1 shall be read as referring to Schedule D PERFORMANCE OBLIGATIONS WITH RESPECT TO CRITICAL CARE 4.1 The provisions of Article 4 of Schedule B, as amended by B1, apply in Fiscal Year 11/12 subject to the following amendments: (a) references to 2010/11 shall be read as referring to 2011/12 ; and (b) all references to Schedule E1 shall be read as referring to Schedule E PERFORMANCE OBLIGATIONS WITH RESPECT TO POST CONSTRUCTION OPERATING PLAN FUNDING AND VOLUME 5.1 The provisions of Article 5 of Schedule B, as amended by B1, apply in Fiscal Year 11/12, subject to the following amendments: (a) references to Schedule F1 shall be read as referring to Schedule F2; and (b) references to 2010/11 shall be read as referring to 2011/ PERFORMANCE OBLIGATIONS WITH RESPECT TO PROTECTED SERVICES 6.1 The Performance Obligations set out in Article 6 of Schedule B, as amended by B1, apply in Fiscal Year 11/12, subject to the following amendments: (a) All references to Schedule D1 or Schedule G1 shall be read as referring to Schedules D2 and G2 respectively; and (b) All references to 2010/11 shall be read as referring to 2011/ PERFORMANCE OBLIGATIONS WITH RESPECT TO WAIT TIME SERVICES 7.1 The Performance Obligations set out in Article 7 of Schedule B, as amended by B1 apply to Fiscal Year 11/12 subject to the following amendments. (a) Sub article 7.2 shall be amended with the addition of the following eight H-SAA Amending Agreement Page 9 of 31
83 new sub paragraphs (c)-(i): (c) 90 th Percentile Wait Times for Cancer Surgery (i) Definition. This indicator measures the time between a patient s and surgeon s decision to proceed with surgery, and the time the procedure is conducted. The 90 th percentile is the point at which 90% of the patients received their treatment while the other 10% waited longer. The 90 th percentile wait time is an actual wait time of a patient and is not estimated. Steps: 1. Wait Days = Procedure Date Decision to Treat Date Patient Unavailable Days. 2. Sort the records in ascending order (i.e. patients with short wait days on top and patients with long wait days at the bottom). 3. Count the total number of cases and multiply by 0.90 to get the 90 th percentile patient. If this value has a decimal digit greater than zero, then round up (ex. 6.6 ~ 7, 6.0 ~ 6, ~ 18). 4. The number of wait days for the 90 th percentile patient is the indicator value Excludes: 1. Procedures no longer required; 2. Diagnostic, palliative and reconstructive cancer procedures; 3. Procedures on skin - carcinoma, skin-melanoma, and lymphomas; 4. Procedures assigned as priority level 1; 5. Wait list entries identified by hospitals as data entry errors; and 6. If unavailable days fall outside the decision to treat date up to procedure date, unavailable days are not deducted from patients wait days. These are considered data entry errors. (ii) LHIN Targets 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Target: maintain or improve current performance 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: H-SAA Amending Agreement Page 10 of 31
84 Performance Target: Accountability Agreement target or better (iii) Performance Corridors 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Corridor: less than or equal to the LHIN s Accountability Agreement target 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Corridor: 10% (d) 90 th Percentile Wait Times for Cardiac Bypass Surgery (i) Definition. 90 th percentile wait times for cardiac bypass surgery. This indicator measures the time between a patients acceptance for bypass surgery, and the time the procedure is conducted. The 90 th percentile is the point at which 90% of the patients received their treatment while the other 10% waited longer. The 90 th percentile wait time is an actual wait time of a patient and is not estimated. Waiting periods are counted from the date a patient was accepted for bypass surgery by the cardiac service or cardiac surgeon. Includes: Elective patients who have been accepted for bypass surgery who are Ontario residents. Excludes: Time spent investigating heart disease before a patient is accepted for a procedure. For example, the time it takes for a patient to have a heart catheterization procedure before being referred to a heart surgeon is not part of the waiting time shown for heart surgery. (ii) LHIN Target 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Target: maintain or improve current performance 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding Performance Target: the LHIN s Accountability Agreement target or better H-SAA Amending Agreement Page 11 of 31
85 (iii) Performance Corridor 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Corridor: less than or equal to the LHIN s Accountability Agreement target 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Corridor: 10% (e) 90 th Percentile Wait Times for Cataract Surgery (i) Definition. This indicator measures the time between a patient s and surgeon s decision to proceed with surgery, and the time the procedure is conducted. The 90 th percentile is the point at which 90% of the patients received their treatment while the other 10% waited longer. The 90 th percentile wait time is an actual wait time of a patient and is not estimated. Steps: 1. Wait Days = Procedure Date Decision to Treat Date Patient Unavailable Days. 2. Sort the records in ascending order (i.e. patients with short wait days on top and patients with long wait days at the bottom). 3. Count the total number of cases and multiply by 0.90 to get the 90 th percentile patient. If this value has a decimal digit greater than zero, then round up (ex. 6.6 ~ 7, 6.0 ~ 6, ~ 18). 4. The number of wait days for the 90 th percentile patient is the indicator value. Excludes: 1. Procedures no longer required; 2. Procedures assigned as priority level 1; 3. Wait list entries identified by hospitals as data entry errors; and 4. If unavailable days fall outside the decision to treat date up to procedure date, unavailable days are not deducted from patients wait days. These are considered data entry errors. (ii) LHIN Target H-SAA Amending Agreement Page 12 of 31
86 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Target: maintain or improve current performance 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Target: The LHIN s Accountability Agreement target or better (iii) Performance Corridor 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Corridor: less than or equal to the LHIN s Accountability Agreement target 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Corridor: 10% (f) 90 th Percentile Wait Times for Joint Replacement (Hip) (i) Definition. This indicator measures the time between a patient s and surgeon s decision to proceed with surgery, and the time the procedure is conducted. The 90 th percentile is the point at which 90% of the patients received their treatment while the other 10% waited longer. The 90 th percentile wait time is an actual wait time of a patient and is not estimated. Steps: 1. Wait Days = Procedure Date Decision to Treat Date Patient Unavailable Days. 2. Sort the records in ascending order (i.e. patients with short wait days on top and patients with long wait days at the bottom.) 3. Count the total number of cases and multiply by 0.90 to get the 90 th percentile patient. If this value has a decimal digit greater than zero, then round up (ex. 6.6 ~ 7, 6.0 ~ 6, ~ 18). 4. The number of wait days for the 90 th percentile patient is the indicator value. Excludes: 1. Procedures no longer required; H-SAA Amending Agreement Page 13 of 31
87 2. Procedures assigned as priority level 1; 3. Wait list entries identified by hospitals as data entry errors; and 4. If unavailable days fall outside the decision to treat date up to procedure date, unavailable days are not deducted from patients wait days. These are considered data entry errors. (ii) LHIN Target. 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Target: maintain or improve current performance 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Target: the LHIN s Accountability Agreement target or better (iii) Performance Corridor 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Corridor: less than or equal to Accountability Agreement target 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Corridor: 10% (g) 90 th Percentile Wait Times for Joint Replacement (Knee) (i) Definition. This indicator measures the time between a patient s and surgeon s decision to proceed with surgery, and the time the procedure is conducted. The 90 th percentile is the point at which 90% of the patients received their treatment while the other 10% waited longer. The 90 th percentile wait t time is an actual wait time of a patient and is not estimated. Steps: 1. Wait Days = Procedure Date Decision to Treat Date Patient Unavailable Days. 2. Sort the records in ascending order (i.e. patients with short wait days on top and patients with long wait days at the bottom). 3. Count the total number of cases and multiply by 0.90 to get the 90 th percentile patient. If this value H-SAA Amending Agreement Page 14 of 31
88 has a decimal digit greater than zero, then round up (ex. 6.6 ~ 7, 6.0 ~ 6, ~ 18). 4. The number of wait days for the 90 th percentile patient is the indicator value Excludes: 1. Procedures no longer required; 2. Procedures assigned as priority level 1; 3. Wait list entries identified by hospitals as data entry errors; and 4. If unavailable days fall outside the decision to treat date up to procedure date, unavailable days are not deducted from patients wait days. These are considered data entry errors. (ii) LHIN Target 1. For hospitals performing at the LHIN s Accountability Agreement target or better: PerformanceTarget: maintain or improve current performance 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Target: the LHIN s Accountability Agreement target or better (iii) Performance Corridor 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Corridor: less than or equal to the LHIN s Accountability Agreement target 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding Performance Corridor: 10% (h) 90 th Percentile Wait Times for Diagnostic Magnetic Resonance Imaging (MRI) Scan (i) Definition. This indicator measures the wait time from when a diagnostic scan is ordered, until the time the actual exam is conducted. This interval is typically referred to as intent to treat. The 90 th percentile is the point at which 90% of the patients received their treatment while the other 10% waited longer. H-SAA Amending Agreement Page 15 of 31
89 Steps: 1. Wait Days = Procedure Date Decision to Treat Date Patient Unavailable Days. 2. Sort the records in ascending order (i.e. patients with short wait days on top and patients with long wait days at the bottom). 3. Count the total number of cases and multiply by 0.90 to get the 90 th percentile patient. If this value has a decimal digit greater than zero, then round up (ex. 6.6 ~ 7, 6.0 ~ 6, ~ 18). 4. The number of wait days for the 90 th percentile patient is the indicator value Excludes: 1. Procedures no longer required; 2. Procedures assigned as priority level 1; 3. Wait list entries identified by hospitals as data entry errors; 4. If unavailable days fall outside the decision to treat date up to procedure date, unavailable days are not deducted from patients wait days. These are considered data entry errors; and 5. As of January 1, 2008, diagnostic imaging cases classified as specified date procedures (timed procedures). (ii) LHIN Target 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Target: maintain or improve current performance 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Target: the LHIN s Accountability Agreement target or better (iii) Performance Corridor 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Corridor: less than or equal to the LHIN s Accountability Agreement target H-SAA Amending Agreement Page 16 of 31
90 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Corridor: 10% (i) 90 th Percentile Wait Times for Diagnostic Computed Tomography (CT) Scan (i)) Definition. This indicator measures the wait time from when a diagnostic scan is ordered, until the time the actual exam is conducted. This interval is typically referred to as intent to treat. The 90 th percentile is the point at which 90% of the patients received their treatment while the other 10% waited longer. Steps: 1. Wait Days = Procedure Date Decision to Treat Date Patient Unavailable Days. 2. Sort the records in ascending order (i.e. patients with short wait days on top and patients with long wait days at the bottom). 3. Count the total number of cases and multiply by 0.90 to get the 90 th percentile patient. If this value has a decimal digit greater than zero, then round up (ex. 6.6 ~ 7, 6.0 ~ 6, ~ 18). 4. The number of wait days for the 90 th percentile patient is the indicator value Excludes: 1. Procedures no longer required; 2. Procedures assigned as priority level 1; 3. Wait list entries identified by hospitals as data entry errors; 4. If unavailable days fall outside the decision to treat date up to procedure date, unavailable days are not deducted from patients wait days. These are considered data entry errors; and 5. As of January 1, 2008, diagnostic imaging cases classified as specified date procedures (timed procedures). ii) LHIN Target 1. For hospitals performing at the LHIN s Accountability Agreement target or better: H-SAA Amending Agreement Page 17 of 31
91 Performance Target: maintain or improve current performance 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Target: the LHIN s Accountability Agreement target or better (iii) Performance Corridor 1. For hospitals performing at the LHIN s Accountability Agreement target or better: Performance Corridor: less than or equal to the LHIN s Accountability Agreement target 2. For hospitals performing above the LHIN s Accountability Agreement target with incremental wait time funding: Performance Corridor: 10% and (b) All references to Schedules A, G, or H being read as referring to Schedules A1, G2 or H2 respectively. 8.0 REPORTING OBLIGATIONS 8.1 The reporting obligations set out in Article 8 of Schedule B, as amended by B1, apply to Fiscal Year 11/ The following reporting obligations are added to Article 8 of Schedule B: (a) French Language Services. If the Hospital is required to provide services to the public in French under the provisions of the French Language Services Act, the Hospital will be required to submit a French language implementation report to the LHIN. If the Hospital is not required to provide services to the public in French under the provisions of the French Language Service Act, it will be required to provide a report to the LHIN that outlines how the Hospital addresses the needs of its local Francophone community. 9.0 LHIN SPECIFIC PERFORMANCE OBLIGATIONS 9.1 Except where specifically limited to a given year, the obligations set out in Article 9 of Schedule B, as amended by B1, apply to Fiscal Year 11/12. Without limiting the foregoing, waivers or conditional waivers for 08/09, 09/10 and 10/11 do not apply to 11/ The following provisions are added to Article 9 of Schedule B (a) The Hospital has advised the LHIN that it anticipates incurring a deficit of H-SAA Amending Agreement Page 18 of 31
92 no more than $2,000,000 by March 31, The Hospital agrees that it will not exceed $2,000,000 and will fund this deficit out of its working capital. (b) Subject to (a) the LHIN will waive the requirements of (a) from April 1, 2011 to March 31, 2012 provided that: (i) (ii) (iii) (iv) (v) the Hospital revises its Hospital Improvement Plan (the HIP ) that will enable the Hospital to achieve a balanced operating position no later than March 31, 2013; the hospital board approved revised HIP is delivered to the LHIN within 6 weeks of the formal notice of the Hospital s 2011/12 funding allocation; the revised HIP is acceptable to the LHIN; the Hospital implements the revised HIP as directed by the LHIN; and the Hospital will report at any time if it is determined that their projected deficit for 2011/12 becomes greater than $2,000,000. The report will contain explanations for the variance and recovery plan. 9.3 (a) i. The hospitals will be required to report on the obligations and expectations listed in Table 1 and the indicators listed in Table 2. Non-acute hospitals will report only on relevant indicators Table 1 LHIN Specific Performance Obligation Risk Management Plans Client Experience Definition HSP Boards must ensure that an established and documented Risk Management Process is in place such that risks are identified and reported to the LHIN when there is a moderate or serious risk of impact on the achievement of the Accountability Agreements. HSP s will provide the LHIN with a summary of the satisfaction survey results required under section 5 of the Excellent Care for all Act. The summary will include overall client satisfaction and overall satisfaction of employees and others working for the HSP. H-SAA Amending Agreement Page 19 of 31
93 LHIN Specific Performance Obligation Falls Prevention and Reduction Program Wound Care Reporting of Clinical Data Submissions to CIHI and MOHLTC LHIN Specific Performance Expectation Care Connections Participation Definition HSPs will ensure that a falls prevention and reduction program is established for atrisk clients. The program will be aligned with the LHIN-wide Integrated Regional Falls Program. Minimum requirements of this program will include: The identification of individuals at risk for falls The collection of information about the number of clients experiencing falls, falls resulting in harm, falls resulting in ER visits, and falls resulting in inpatient admissions A strategy to reduce the number of falls resulting in harm HSPs will ensure that risk identification and prevention activities to address Wound Care in alignment with the NSM LHIN Guidelines for Wound Care and that data is collected and reported to the LHIN. HSPs will ensure that all clinical data submission timelines for CIHI submission are adhered to. Definition HSPs are expected to collaborate with system partners and Local Leadership Councils to implement the 12 Areas of Focus for Care Connections. HSPs will ensure Senior Management or delegate representation at all meetings for Care Connections oversight structures as agreed to between the HSP and the LHIN, and other meetings that may be scheduled from time to time as appropriate. Table 2 LHIN Specific Indicator Total ALC Days (as reported by NSM LHIN Hospitals) Definition Total number of inpatient days designated as ALC in a given time period Includes: 1. Data from acute care hospitals, including those with psychiatric beds (AP hospitals) and without psychiatric beds (AT hospitals) 2. Individuals designated as ALC Excludes: 1. Newborns and stillborns 2. Records with missing or invalid Discharge Date H-SAA Amending Agreement Page 20 of 31
94 LHIN Specific Indicator Average (mean) length of stay for ALC patients Proportion of Diabetics getting HbA1c testing Proportion of Diabetics getting LDL testing Proportion of Diabetics getting Retinal Exams Proportion of Diabetics with Diabetes in Control (HbA1c <=7) Total number of Falls among clients (patients) Definition Total number of inpatient days designated as ALC in a given time period divided by the total number of discharges designated ALC Includes: 1. Data from acute care hospitals, including those with psychiatric beds (AP hospitals) and without psychiatric beds (AT hospitals) 2. Individuals designated as ALC Excludes: 1. Newborns and stillborns 2. Records with missing or invalid Discharge Date The percentage of ambulatory care diabetic patients age 18 and older who have received hemoglobin A1C (HbA1C) tests within the appropriate guideline period. Includes: Number of unique patients age >18 registered with Hospital Diabetic Education Centers Excludes: women with gestational diabetes The percentage of ambulatory care diabetic patients age 18 and older who have received a lipoprotein-cholesterol LDL-C test within the appropriate guideline period. Includes: Number of unique patients age >18 registered with Hospital Diabetic Education Centers Excludes: women with gestational diabetes The percentage of ambulatory care diabetic patients age 18 and older who have received retinal eye exams within the appropriate guideline period Includes: Number of unique patients age >18 registered with Hospital Diabetic Education Centers Excludes: women with gestational diabetes The percentage of ambulatory diabetic patients age 18 and older who have received hemoglobin A1C (HbA1C) test with a measurement value of less than or equal to 7.0%. Includes: Number of unique patients age >18 registered with Hospital Diabetic Education Centers Excludes: women with gestational diabetes A count of the total number of occurrences of falls among those clients presenting at the Emergency Room. H-SAA Amending Agreement Page 21 of 31
HOSPITAL SERVICE ACCOUNTABILITY AGREEMENT: Indicator Technical Specifications
 2015-16 HOSPITAL SERVICE ACCOUNTABILITY AGREEMENT: Indicator Technical Specifications November 2014 2015/16 HSAA Technical Specifications Page 1 TABLE OF CONTENTS PATIENT EXPERIENCE ACCESS, EFFECTIVE,
2015-16 HOSPITAL SERVICE ACCOUNTABILITY AGREEMENT: Indicator Technical Specifications November 2014 2015/16 HSAA Technical Specifications Page 1 TABLE OF CONTENTS PATIENT EXPERIENCE ACCESS, EFFECTIVE,
H-SAA AMENDING AGREEMENT
 H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: NORTH EAST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND (the Hospital ) WHEREAS
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: NORTH EAST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND (the Hospital ) WHEREAS
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of October, 2016
 is made as of the 1 st day of October, 2016") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of October, 216 B E T W E E N: SOUTH WEST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND St. Joseph's Health
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of October, 216 B E T W E E N: SOUTH WEST LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND St. Joseph's Health
H-SAA AMENDING AGREEMENT B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND
 AND") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND WOMEN'S COLLEGE
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: TORONTO CENTRAL LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND WOMEN'S COLLEGE
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of July, 2017
 is made as of the 1 st day of July, 2017") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of July, 2017 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND University of Ottawa
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of July, 2017 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND University of Ottawa
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016
 is made as of the 1 st day of April, 2016") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Pembroke Regional Hospital
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Pembroke Regional Hospital
Hospital Service Accountability Agreements
 2017-2018 Schedule A Funding Allocation 2017-2018 [1] Estimated Funding Allocation Section 1: FUNDING SUMMARY LHIN FUNDING LHIN Global Allocation (Includes Sec. 3) Health System Funding Reform: HBAM Funding
2017-2018 Schedule A Funding Allocation 2017-2018 [1] Estimated Funding Allocation Section 1: FUNDING SUMMARY LHIN FUNDING LHIN Global Allocation (Includes Sec. 3) Health System Funding Reform: HBAM Funding
MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard /10 Q3
 MLAA Performance Assessment Dashboard /10 Q3") MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard - 29/1 Q3 README The 29/1 MLAA Dashboard has been designed to reflect various reporting fiscal periods as well as the
MINISTRY/LHIN ACCOUNTABILITY AGREEMENT (MLAA) MLAA Performance Assessment Dashboard - 29/1 Q3 README The 29/1 MLAA Dashboard has been designed to reflect various reporting fiscal periods as well as the
Hospital Service Accountability Agreement. Indicator Technical Specifications
 2016-17 Hospital Service Accountability Agreement Indicator Technical Specifications October 2015 TABLE OF CONTENTS PATIENT EXPERIENCE ACCESS, EFFECTIVE, SAFE, PERSON-CENTERED... 5 PERFORMANCE... 5 90th
2016-17 Hospital Service Accountability Agreement Indicator Technical Specifications October 2015 TABLE OF CONTENTS PATIENT EXPERIENCE ACCESS, EFFECTIVE, SAFE, PERSON-CENTERED... 5 PERFORMANCE... 5 90th
Balanced Scorecard Highlights
 Balanced Scorecard Highlights Highlights from 2011-12 fourth quarter (January to March) Sick Time The average sick hours per employee remains above target this quarter at 58. Human Resources has formed
Balanced Scorecard Highlights Highlights from 2011-12 fourth quarter (January to March) Sick Time The average sick hours per employee remains above target this quarter at 58. Human Resources has formed
Hospital Service Accountability Agreement. Indicator Technical Specifications
 2018-19 Hospital Service Accountability Agreement Indicator Technical Specifications October 2017 TABLE OF CONTENTS PATIENT EXPERIENCE ACCESS, EFFECTIVE, SAFE, PERSON-CENTERED... 5 PERFORMANCE... 5 90th
2018-19 Hospital Service Accountability Agreement Indicator Technical Specifications October 2017 TABLE OF CONTENTS PATIENT EXPERIENCE ACCESS, EFFECTIVE, SAFE, PERSON-CENTERED... 5 PERFORMANCE... 5 90th
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2017
 is made as of the 1 st day of April, 2017") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2017 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Deep River and District
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2017 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Deep River and District
Wait Time Information in Priority Areas: Definitions
 Wait Time Information in Priority Areas: Definitions 1 Background In 2004, Canada's first ministers agreed to work towards reducing wait times for five priority areas: cancer treatment, cardiac care, diagnostic
Wait Time Information in Priority Areas: Definitions 1 Background In 2004, Canada's first ministers agreed to work towards reducing wait times for five priority areas: cancer treatment, cardiac care, diagnostic
HAPS GUIDELINES HOSPITAL ACCOUNTABILITY PLANNING SUBMISSION (HAPS) GUIDELINES
 GUIDELINES") HOSPITAL ACCOUNTABILITY PLANNING SUBMISSION (HAPS) GUIDELINES 2018-19 October 2017 1 Contents 1. Introduction... 3 1.1 Process for the Development of the HAPS... 4 1.2 Roles and Responsibilities within
HOSPITAL ACCOUNTABILITY PLANNING SUBMISSION (HAPS) GUIDELINES 2018-19 October 2017 1 Contents 1. Introduction... 3 1.1 Process for the Development of the HAPS... 4 1.2 Roles and Responsibilities within
H-SAA Monitoring & Assessment Process & Overview 2012/13 Q4
 H-SAA Monitoring & Assessment Process & Overview H-SAA MONITORING & ASSESSMENT PROCESS & OVERVIEW The Hospital Service Accountability Agreement (H-SAA) has been developed to monitor and analyze the current
H-SAA Monitoring & Assessment Process & Overview H-SAA MONITORING & ASSESSMENT PROCESS & OVERVIEW The Hospital Service Accountability Agreement (H-SAA) has been developed to monitor and analyze the current
Report on Provincial Wait Time Strategy
 Hôpital régional de Sudbury Regional Hospital Report on Provincial Wait Time Strategy May 2007 Provincial Wait-time Strategy Announced by Minister of Health in November 2004 Focus is to increase access
Hôpital régional de Sudbury Regional Hospital Report on Provincial Wait Time Strategy May 2007 Provincial Wait-time Strategy Announced by Minister of Health in November 2004 Focus is to increase access
Health Quality Ontario
 Health Quality Ontario The provincial advisor on the quality of health care in Ontario November 15, 2016 Under Pressure: Emergency department performance in Ontario Technical Appendix Table of Contents
Health Quality Ontario The provincial advisor on the quality of health care in Ontario November 15, 2016 Under Pressure: Emergency department performance in Ontario Technical Appendix Table of Contents
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016
 is made as of the 1 st day of April, 2016") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Queensway Carleton
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Queensway Carleton
H-SAA AMENDING AGREEMENT. THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 2016
 is made as of the 1 st day of April, 2016") H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Cornwall Community Hospital
H-SAA AMENDING AGREEMENT THIS AMENDING AGREEMENT (the Agreement ) is made as of the 1 st day of April, 216 B E T W E E N: CHAMPLAIN LOCAL HEALTH INTEGRATION NETWORK (the LHIN ) AND Cornwall Community Hospital
Service Accountability Agreements Update
 Service Accountability Agreements Update Central East Local Health Integration Network Board Meeting Date: December 21, 2016 Presented By: System Finance and Performance Management Overview Context Service
Service Accountability Agreements Update Central East Local Health Integration Network Board Meeting Date: December 21, 2016 Presented By: System Finance and Performance Management Overview Context Service
March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan
 BRIEFING NOTE March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan PURPOSE To provide the WWLHIN Board of Directors with a recommendation to endorse the proposed
BRIEFING NOTE March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan PURPOSE To provide the WWLHIN Board of Directors with a recommendation to endorse the proposed
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
Protocol for Assigning Hospitals to Groups under The Public Hospitals Act Stakeholders Copy
 Protocol for Assigning Hospitals to Groups under The Public Hospitals Act Stakeholders Copy LHIN Liaison Branch Relations and Coordination Branch Ministry of Health and Long-Term Care Table of Contents
Protocol for Assigning Hospitals to Groups under The Public Hospitals Act Stakeholders Copy LHIN Liaison Branch Relations and Coordination Branch Ministry of Health and Long-Term Care Table of Contents
TC LHIN Quality Indicators: Big Dot (System) and Small Dot (Sector Specific) Indicators. November 29, 2013
 and Small Dot (Sector Specific) Indicators. November 29, 2013") TC LHIN Quality Indicators: Big Dot (System) and Small Dot (Sector Specific) Indicators November 29, 2013 1 Contents 1. TC LHIN Quality Framework, Themes and Focus Areas 2. Big Dot System Indicators 3.
TC LHIN Quality Indicators: Big Dot (System) and Small Dot (Sector Specific) Indicators November 29, 2013 1 Contents 1. TC LHIN Quality Framework, Themes and Focus Areas 2. Big Dot System Indicators 3.
CENTRAL EAST LHIN MLPA PERFORMANCE INDICATOR DASHBOARD Performance effective as of August 2011
 LHIN Starting LHIN Indicator Provincial Point or Actual LHIN Current LHIN Reporting PI No. Performance Indicator (PI) FY211/12 Trend Data Source Type Target Baseline Performance Status Ranking Period Target
LHIN Starting LHIN Indicator Provincial Point or Actual LHIN Current LHIN Reporting PI No. Performance Indicator (PI) FY211/12 Trend Data Source Type Target Baseline Performance Status Ranking Period Target
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives"
 2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
Accountability Agreements in Ontario s Health System: How Can They Accelerate Quality Improvement and Enhance Public Reporting?
 Accountability Agreements in Ontario s Health System: How Can They Accelerate Quality Accountability Agreements in Ontario s Health System: How Can They Accelerate Quality Improvement and Enhance Public
Accountability Agreements in Ontario s Health System: How Can They Accelerate Quality Accountability Agreements in Ontario s Health System: How Can They Accelerate Quality Improvement and Enhance Public
Ministry-LHIN Performance Agreement (MLPA) Patient Flow Report
 Patient Flow Report") Ministry-LHIN Performance Agreement (MLPA) Patient Flow Report Quality and Safety Committee Hamilton Niagara Haldimand Brant (HNHB) Local Health Integration Network (LHIN) November 21, 2012 Agenda 2012-13
Ministry-LHIN Performance Agreement (MLPA) Patient Flow Report Quality and Safety Committee Hamilton Niagara Haldimand Brant (HNHB) Local Health Integration Network (LHIN) November 21, 2012 Agenda 2012-13
2018 Press Ganey Award Criteria
 2018 Press Ganey Award Criteria Guardian of Excellence Award SM This award honors clients who have reached the 95th percentile for patient experience, engagement or clinical quality performance. Guardian
2018 Press Ganey Award Criteria Guardian of Excellence Award SM This award honors clients who have reached the 95th percentile for patient experience, engagement or clinical quality performance. Guardian
Developmental /Category III Explanatory/Category II Not Defined Explanatory/Category II Defined Proposed Priority
 The Rehabilitative Care System supports high quality patient experiences through the utilization of best practices to enhance outcomes for individuals with functional goals. This evaluationframework has
The Rehabilitative Care System supports high quality patient experiences through the utilization of best practices to enhance outcomes for individuals with functional goals. This evaluationframework has
Hospital Improvement Plan Niagara Health System
 Hospital Improvement Plan Niagara Health System Presentation to Hamilton Niagara Haldimand Brant Local Health Integration Network (HNHB LHIN) Board of Directors November 25, 2008 HNHB LHIN Staff Health
Hospital Improvement Plan Niagara Health System Presentation to Hamilton Niagara Haldimand Brant Local Health Integration Network (HNHB LHIN) Board of Directors November 25, 2008 HNHB LHIN Staff Health
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/28/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/28/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Hospital Improvement Plan Niagara Health System Staff Report December 16, Hamilton Niagara Haldimand Brant Local Health Integration Network
 Hospital Improvement Plan Niagara Health System Staff Report December 16, 2008 Hamilton Niagara Haldimand Brant Local Health Integration Network Question: Emergency Medical Services (EMS) The EMS stated
Hospital Improvement Plan Niagara Health System Staff Report December 16, 2008 Hamilton Niagara Haldimand Brant Local Health Integration Network Question: Emergency Medical Services (EMS) The EMS stated
Guidelines for the Submission and Review of Magnetic Resonance Imaging (MRI) Stakeholders Copy
 Stakeholders Copy") Guidelines for the Submission and Review of Magnetic Resonance Imaging (MRI) Stakeholders Copy Implementation Branch LHIN Liaison Branch Ministry of Health and Long-Term Care July 2009 Table of Contents
Guidelines for the Submission and Review of Magnetic Resonance Imaging (MRI) Stakeholders Copy Implementation Branch LHIN Liaison Branch Ministry of Health and Long-Term Care July 2009 Table of Contents
2014/15 Quality Improvement Plan (QIP) Narrative
 Narrative") 2014/15 Quality Improvement Plan (QIP) Narrative 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop a quality improvement plan.
2014/15 Quality Improvement Plan (QIP) Narrative 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop a quality improvement plan.
Services That Require Prior Authorization
 Services That Require Prior Authorization Some of the services listed in the Medical Benefits Chart are covered only if your doctor or other network provider gets approval in advance (sometimes called
Services That Require Prior Authorization Some of the services listed in the Medical Benefits Chart are covered only if your doctor or other network provider gets approval in advance (sometimes called
GIC Employees/Retirees without Medicare
 GIC Active Employees & Retirees without Medicare 7/1/18 GIC Employees/Retirees without Medicare HMO Summary of Benefits Chart This chart provides a summary of key services offered by your Health New England
GIC Active Employees & Retirees without Medicare 7/1/18 GIC Employees/Retirees without Medicare HMO Summary of Benefits Chart This chart provides a summary of key services offered by your Health New England
Hospital Authority Key Performance Indicator Annual Review
 - 1 - For decision on 25.1.2018 AOM-P1352 Hospital Authority 2017 Key Performance Indicator Annual Review Purpose This paper informs Members of the progress of the 2017 Key Performance Indicator (KPI)
- 1 - For decision on 25.1.2018 AOM-P1352 Hospital Authority 2017 Key Performance Indicator Annual Review Purpose This paper informs Members of the progress of the 2017 Key Performance Indicator (KPI)
CE LHIN Hospital Proposals - New Funding for MRI Machines. July 20 th, 2010
 CE LHIN Hospital Proposals - New Funding for MRI Machines July 20 th, 2010 Operational Funding for MRI Machines Background Wait Times Strategy (WTS) has issued an invitation for hospitals to submit proposals
CE LHIN Hospital Proposals - New Funding for MRI Machines July 20 th, 2010 Operational Funding for MRI Machines Background Wait Times Strategy (WTS) has issued an invitation for hospitals to submit proposals
The Regional Cardiac Care Program at Southlake
 The Regional Cardiac Care Program at Southlake The Future Vision of Regional Cardiac Services Serving the Populations of York, Simcoe, Muskoka, and Dufferin Regions Copyright 2009. Southlake Regional Health
The Regional Cardiac Care Program at Southlake The Future Vision of Regional Cardiac Services Serving the Populations of York, Simcoe, Muskoka, and Dufferin Regions Copyright 2009. Southlake Regional Health
Indicator Definition
 Patients Discharged from Emergency Department within 4 hours Full data definition sign-off complete. Name of Measure Name of Measure (short) Domain Type of Measure Emergency Department Length of Stay:
Patients Discharged from Emergency Department within 4 hours Full data definition sign-off complete. Name of Measure Name of Measure (short) Domain Type of Measure Emergency Department Length of Stay:
4.10. Organ and Tissue Donation and Transplantation. Chapter 4 Section. Background. Follow-up to VFM Section 3.10, 2010 Annual Report
 Chapter 4 Section 4.10 Ministry of Health and Long-Term Care Organ and Tissue Donation and Transplantation Follow-up to VFM Section 3.10, 2010 Annual Report Chapter 4 Follow-up Section 4.10 Background
Chapter 4 Section 4.10 Ministry of Health and Long-Term Care Organ and Tissue Donation and Transplantation Follow-up to VFM Section 3.10, 2010 Annual Report Chapter 4 Follow-up Section 4.10 Background
The goal of Ontario s Wait Time Strategy launched in
 Special Report Evaluating Outcomes in Ontario s Wait Time Strategy: Part 4 Joann Trypuc, Alan Hudson and Hugh MacLeod The goal of Ontario s Wait Time Strategy launched in November 2004 was to improve access
Special Report Evaluating Outcomes in Ontario s Wait Time Strategy: Part 4 Joann Trypuc, Alan Hudson and Hugh MacLeod The goal of Ontario s Wait Time Strategy launched in November 2004 was to improve access
2017/18 and 2018/19 National Tariff Payment System Annex E: Guidance on currencies without national prices. NHS England and NHS Improvement
 2017/18 and 2018/19 National Tariff Payment System Annex E: Guidance on currencies without national prices NHS England and NHS Improvement December 2016 Contents 1. Introduction... 3 2. Critical care adult
2017/18 and 2018/19 National Tariff Payment System Annex E: Guidance on currencies without national prices NHS England and NHS Improvement December 2016 Contents 1. Introduction... 3 2. Critical care adult
Meeting Date: July 26, 2017 Action: Decision Topic: Item 13.0 Grand River Hospital MRI and Nuclear Medicine Replacement Pre-Capital Submission
 BRIEFING NOTE Mission: To make it easy for you to be healthy and to get the care and support you need. Vision: Healthy People. Thriving Communities. Bright Futures. Core Value: Acting in the best interest
BRIEFING NOTE Mission: To make it easy for you to be healthy and to get the care and support you need. Vision: Healthy People. Thriving Communities. Bright Futures. Core Value: Acting in the best interest
FOCUS on Emergency Departments DATA DICTIONARY
 FOCUS on Emergency Departments DATA DICTIONARY Table of Contents Contents Patient time to see an emergency doctor... 1 Patient emergency department total length of stay (LOS)... 3 Length of time emergency
FOCUS on Emergency Departments DATA DICTIONARY Table of Contents Contents Patient time to see an emergency doctor... 1 Patient emergency department total length of stay (LOS)... 3 Length of time emergency
This profile provides an overview of the services provided at the Royal Inland Hospital in the areas of:
 Facility Profile This profile provides an overview of the services provided at the in the areas of: Inpatient Cases & Days Inpatient Surgery & Surgical Day Care Emergency Department The information provided
Facility Profile This profile provides an overview of the services provided at the in the areas of: Inpatient Cases & Days Inpatient Surgery & Surgical Day Care Emergency Department The information provided
March 24, Ms. Angela Robertson Executive Director Central Toronto Community Health Centres 168 Bathurst Street Toronto, ON M5V 2R4
 425 Bloor Street East, Suite 201 Toronto, ON M4W 3R4 Tel: 416 921-7453 Fax: 416 921-0117 Toll Free: 1 866 383-5446 www.torontocentrallhin.on.ca March 24, 2016 Ms. Angela Robertson Executive Director Central
425 Bloor Street East, Suite 201 Toronto, ON M4W 3R4 Tel: 416 921-7453 Fax: 416 921-0117 Toll Free: 1 866 383-5446 www.torontocentrallhin.on.ca March 24, 2016 Ms. Angela Robertson Executive Director Central
NEIGHBORHOOD HEALTH PARTNERSHIP POS SUMMARY OF BENEFITS
 XV-2 $30/$60/$200/$1,000/80% R NEIGHBORHOOD HEALTH PARTNERSHIP POS SUMMARY OF BENEFITS A quick glance at this Summary of Benefits will introduce you to the Point of Service (POS) Plan you have with Neighborhood
XV-2 $30/$60/$200/$1,000/80% R NEIGHBORHOOD HEALTH PARTNERSHIP POS SUMMARY OF BENEFITS A quick glance at this Summary of Benefits will introduce you to the Point of Service (POS) Plan you have with Neighborhood
News SEPTEMBER. Hospital Outpatient Quality Reporting Program. Support Contractor
 Volume 1, Issue 4 Hospital Outpatient Quality Reporting Program Support Contractor News SEPTEMBER 2011 In This Issue... Emergency Department Arrival and Departure Times Page 2 Hospital OQR Benchmarks Page
Volume 1, Issue 4 Hospital Outpatient Quality Reporting Program Support Contractor News SEPTEMBER 2011 In This Issue... Emergency Department Arrival and Departure Times Page 2 Hospital OQR Benchmarks Page
The Federal Joint Committee (G-BA) and Quality Assurance in Health Care
 and Quality Assurance in Health Care") The Federal Joint Committee (G-BA) and Quality Assurance in Health Care HOPE Study Tour Berlin Quality assurance in German Hospital Care 30./31. October 2014 Markus Wörz Department of Quality Assurance
The Federal Joint Committee (G-BA) and Quality Assurance in Health Care HOPE Study Tour Berlin Quality assurance in German Hospital Care 30./31. October 2014 Markus Wörz Department of Quality Assurance
FACILITY BASED SERVICES
 FACILITY BASED SERVICES Inpatient Hospital Care Elective Inpatient Admission or Elective Inpatient Surgery Inpatient Rehabilitation Care Skilled Nursing Facility Admission Non-Custodial Nursing Home Care
FACILITY BASED SERVICES Inpatient Hospital Care Elective Inpatient Admission or Elective Inpatient Surgery Inpatient Rehabilitation Care Skilled Nursing Facility Admission Non-Custodial Nursing Home Care
CUSTODIAL NURSING HOME CARE
 CUSTODIAL NURSING HOME CARE Chiropratic Services Custodial Nursing Home Care DME Equipment and Supplies Incontinence Supplies: Diapers, briefs, wipes, gloves, pads Infusion (IV, Enteral) Services Outpatient
CUSTODIAL NURSING HOME CARE Chiropratic Services Custodial Nursing Home Care DME Equipment and Supplies Incontinence Supplies: Diapers, briefs, wipes, gloves, pads Infusion (IV, Enteral) Services Outpatient
UTILIZATION MANAGEMENT AND CARE COORDINATION Section 8
 Overview The focus of WellCare s Utilization Management (UM) Program is to provide members access to quality care and to monitor the appropriate utilization of services. WellCare s UM Program has five
Overview The focus of WellCare s Utilization Management (UM) Program is to provide members access to quality care and to monitor the appropriate utilization of services. WellCare s UM Program has five
Supporting Best Practice for COPD Care Across the System
 Supporting Best Practice for COPD Care Across the System May 3, 2017 Health Quality Ontario The provincial advisor on the quality of health care in Ontario Overview Health Quality Ontario background QBP
Supporting Best Practice for COPD Care Across the System May 3, 2017 Health Quality Ontario The provincial advisor on the quality of health care in Ontario Overview Health Quality Ontario background QBP
CKHA Quality Improvement Plan (QIP) Scorecard
 Scorecard") CKHA Quality Improvement Plan () Scorecard 217-18 Quality dimension Performance Indicator 217-18 Performance Goals results where available Current Value Page Safety Medication Reconciliation completed
CKHA Quality Improvement Plan () Scorecard 217-18 Quality dimension Performance Indicator 217-18 Performance Goals results where available Current Value Page Safety Medication Reconciliation completed
FACILITY BASED SERVICES
 CUSTODIAL NURSING HOME CARE Chiropratic Services Custodial Nursing Home Care DME Equipment and Supplies Incontinence Supplies: Diapers, briefs, wipes, gloves, pads Infusion (IV, Enteral) Services Outpatient
CUSTODIAL NURSING HOME CARE Chiropratic Services Custodial Nursing Home Care DME Equipment and Supplies Incontinence Supplies: Diapers, briefs, wipes, gloves, pads Infusion (IV, Enteral) Services Outpatient
OVERVIEW SCOPE & DEMONSTRATION OF IMPACT
 210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: 705 326-7750 Toll Free: 1 866 903-5446 Fax: 705 326-1392 www.nsmlhin.on.ca 210, avenue Mémorial, Bureaux 128 Orillia, ON L3V 7V1 Téléphone : 705
210 Memorial Avenue, Suite 128 Orillia, ON L3V 7V1 Tel: 705 326-7750 Toll Free: 1 866 903-5446 Fax: 705 326-1392 www.nsmlhin.on.ca 210, avenue Mémorial, Bureaux 128 Orillia, ON L3V 7V1 Téléphone : 705
About the Data: Adult Health and Disease - Chronic Illness 2016/17, 2014/15 (archived) Last Updated: August 29, 2018
 Last Updated: August 29, 2018") About the Data: Adult Health and Disease - Chronic Illness 2016/17, 2014/15 (archived) Last Updated: August 29, 2018 Adult Health and Disease: 2016/17 Denominator: Ontario Ministry of Health and Long-Term
About the Data: Adult Health and Disease - Chronic Illness 2016/17, 2014/15 (archived) Last Updated: August 29, 2018 Adult Health and Disease: 2016/17 Denominator: Ontario Ministry of Health and Long-Term
Children s Hospital of Eastern Ontario
 Children s Hospital of Eastern Ontario April 1, 2011 Children s Hospital of Eastern Ontario 1 Part A: Overview of Our Hospital s Quality Improvement Plan 1. Overview of our quality improvement plan for
Children s Hospital of Eastern Ontario April 1, 2011 Children s Hospital of Eastern Ontario 1 Part A: Overview of Our Hospital s Quality Improvement Plan 1. Overview of our quality improvement plan for
Health System Performance and Accountability Division MOHLTC. Transitional Care Program Framework
 Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Mississauga Hospital 100 Queensway West Mississauga, ON L5B 1B8
 Credit Valley Hospital 2200 Eglinton Avenue West Mississauga, ON L5M 2N1 Mississauga Hospital 100 Queensway West Mississauga, ON L5B 1B8 Queensway Health Centre 150 Sherway Drive Toronto, ON M9C 1A5 This
Credit Valley Hospital 2200 Eglinton Avenue West Mississauga, ON L5M 2N1 Mississauga Hospital 100 Queensway West Mississauga, ON L5B 1B8 Queensway Health Centre 150 Sherway Drive Toronto, ON M9C 1A5 This
Martin s Point US Family Health Plan Pre-Authorization Requirements
 Martin s Point US Family Health Plan Requirements Requirements described below are for covered benefits only and this information is provided for summary purposes only. Please call 1-888-732-7364 for complete
Martin s Point US Family Health Plan Requirements Requirements described below are for covered benefits only and this information is provided for summary purposes only. Please call 1-888-732-7364 for complete
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Benchmarking variation in coding across hospitals in Canada: A data surveillance approach
 Benchmarking variation in coding across hospitals in Canada: A data surveillance approach Lori Kirby Canadian Institute for Health Information October 11, 2017 lkirby@cihi.ca cihi.ca @cihi_icis Outline
Benchmarking variation in coding across hospitals in Canada: A data surveillance approach Lori Kirby Canadian Institute for Health Information October 11, 2017 lkirby@cihi.ca cihi.ca @cihi_icis Outline
Champlain Health System Performance and Accomplishments
 hamplain Health System Performance and Accomplishments Technical Report November 2015 Table of ontents Page Number(s) Section A Overview Status of All Indicators A1-A2 Section B Ministry LHIN Accountability
hamplain Health System Performance and Accomplishments Technical Report November 2015 Table of ontents Page Number(s) Section A Overview Status of All Indicators A1-A2 Section B Ministry LHIN Accountability
Access to Health Care Services in Canada, 2003
 Access to Health Care Services in Canada, 2003 by Claudia Sanmartin, François Gendron, Jean-Marie Berthelot and Kellie Murphy Health Analysis and Measurement Group Statistics Canada Statistics Canada Health
Access to Health Care Services in Canada, 2003 by Claudia Sanmartin, François Gendron, Jean-Marie Berthelot and Kellie Murphy Health Analysis and Measurement Group Statistics Canada Statistics Canada Health
PROPOSED RULEMAKING DEPARTMENT OF HEALTH
 PROPOSED RULEMAKING DEPARTMENT OF HEALTH [28 PA. CODE CHS. 51, 136, 138, 139 AND 158]] Health Facility Licensure The Department of Health (Department) proposes to amend Part IV (relating to health facilities)
PROPOSED RULEMAKING DEPARTMENT OF HEALTH [28 PA. CODE CHS. 51, 136, 138, 139 AND 158]] Health Facility Licensure The Department of Health (Department) proposes to amend Part IV (relating to health facilities)
NEVADA HEALTH CO-OP SOUTHERN STAR/ESTRELLA GOLD 100% 34996NV
 NEVADA HEALTH CO-OP SOUTHERN STAR/ESTRELLA GOLD 100% 34996NV003 0002 Attachment A Benefit Schedule Lifetime Maximum: Unlimited. Benefits apply when you obtain or arrange for Covered through a Nevada Health
NEVADA HEALTH CO-OP SOUTHERN STAR/ESTRELLA GOLD 100% 34996NV003 0002 Attachment A Benefit Schedule Lifetime Maximum: Unlimited. Benefits apply when you obtain or arrange for Covered through a Nevada Health
Top Choice. Level of cover with Australian Unity. Excess options. Cover availability. Hospital and Extras Cover Effective from 1 April 2018 $500
 Hospital and Extras Cover Effective from 1 April 2018 Level of cover with Australian Unity Cover availability Excess options $500 HOSPITAL TOP EXTRAS MID SINGLE COUPLE FAMILY EXCESS Excess is waived for
Hospital and Extras Cover Effective from 1 April 2018 Level of cover with Australian Unity Cover availability Excess options $500 HOSPITAL TOP EXTRAS MID SINGLE COUPLE FAMILY EXCESS Excess is waived for
2017 Summary of Benefits
 H5209 004_DSB9 23 16 File & Use 10/14/2016 DHS Approved 10 7 2016 This is a summary of drug and health services covered by Care Wisconsin Medicare Dual Advantage Plan (HMO SNP) January 1, 2017 to December
H5209 004_DSB9 23 16 File & Use 10/14/2016 DHS Approved 10 7 2016 This is a summary of drug and health services covered by Care Wisconsin Medicare Dual Advantage Plan (HMO SNP) January 1, 2017 to December
SITE PROFILE CORNER BROOK
 SITE PROFILE CORNER BROOK Western Memorial Regional Hospital 1 Brookfield Avenue P.O. Box 2005 Corner Brook, NL A2H 6J7 709-637-5000 Site Information: Western Memorial Regional Hospital (WMRH), located
SITE PROFILE CORNER BROOK Western Memorial Regional Hospital 1 Brookfield Avenue P.O. Box 2005 Corner Brook, NL A2H 6J7 709-637-5000 Site Information: Western Memorial Regional Hospital (WMRH), located
HOSPITAL UTILIZATION DATABASE
 Medical Facilities Utilization Reporting System HOSPITAL UTILIZATION DATABASE Broward Regional Health Planning Council, Inc. 915 Middle River Drive, Suite 120 Fort Lauderdale, FL 33304 Phone: (954) 561-9681
Medical Facilities Utilization Reporting System HOSPITAL UTILIZATION DATABASE Broward Regional Health Planning Council, Inc. 915 Middle River Drive, Suite 120 Fort Lauderdale, FL 33304 Phone: (954) 561-9681
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs
 2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
2017 Quality Reporting: Claims and Administrative Data-Based Quality Measures For Medicare Shared Savings Program and Next Generation ACO Model ACOs June 15, 2017 Rabia Khan, MPH, CMS Chris Beadles, MD,
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING
 MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
Choice PPO Retired Employees Health Program Non-Medicare Eligible Retired Members
 Choice PPO Retired Employees Health Program Non-Medicare Eligible Retired Members DEDUCTIBLE (per calendar year) Annual in-network deductible must be paid first for the following services: Imaging, hospital
Choice PPO Retired Employees Health Program Non-Medicare Eligible Retired Members DEDUCTIBLE (per calendar year) Annual in-network deductible must be paid first for the following services: Imaging, hospital
Shield Spectrum PPO SM
 Shield Spectrum PPO SM Combined Evidence of Coverage and Disclosure Form City of Los Angeles Effective Date: January 1, 2014 An independent member of the Blue Shield Association NOTICE This Evidence of
Shield Spectrum PPO SM Combined Evidence of Coverage and Disclosure Form City of Los Angeles Effective Date: January 1, 2014 An independent member of the Blue Shield Association NOTICE This Evidence of
Health System Funding Reform: Driving Change using Technology Presentation to Canadian Health Informatics Association
 Health System Funding Reform: Driving Change using Technology Presentation to Canadian Health Informatics Association April 2014 Ministry of Health and Long-Term Care V2.4 (2014-04-28) Session Objectives
Health System Funding Reform: Driving Change using Technology Presentation to Canadian Health Informatics Association April 2014 Ministry of Health and Long-Term Care V2.4 (2014-04-28) Session Objectives
INPATIENT/COMPREHENSIVE REHAB AUDIT DICTIONARY
 Revised 11/04/2016 Audit # Location Audit Message Audit Description Audit Severity 784 DATE Audits are current as of 11/04/2016 The date of the last audit update Information 1 COUNTS Total Records Submitted
Revised 11/04/2016 Audit # Location Audit Message Audit Description Audit Severity 784 DATE Audits are current as of 11/04/2016 The date of the last audit update Information 1 COUNTS Total Records Submitted
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Release Notes for the 2010B Manual
 Release Notes for the 2010B Manual Section Rationale Description Screening for Violence Risk, Substance Use, Psychological Trauma History and Patient Strengths completed Date to NICU Cesarean Section Clinical
Release Notes for the 2010B Manual Section Rationale Description Screening for Violence Risk, Substance Use, Psychological Trauma History and Patient Strengths completed Date to NICU Cesarean Section Clinical
SUBSTANCE ABUSE & HEALTH CARE SERVICES HEALTH SERVICES. Fiscal Year rd Quarter
 HEALTH SERVICES To administer and manage contracted services to eligible persons in need of health care or related support services, and to promote health maintenance through education and intervention.
HEALTH SERVICES To administer and manage contracted services to eligible persons in need of health care or related support services, and to promote health maintenance through education and intervention.
(1) Ambulatory surgical center--a facility licensed under Texas Health and Safety Code, Chapter 243.
 Ambulatory surgical center--a facility licensed under Texas Health and Safety Code, Chapter 243.") RULE 200.1 Definitions The following words and terms, when used in this chapter, shall have the following meanings, unless the context clearly indicates otherwise. (1) Ambulatory surgical center--a facility
RULE 200.1 Definitions The following words and terms, when used in this chapter, shall have the following meanings, unless the context clearly indicates otherwise. (1) Ambulatory surgical center--a facility
The Federal Joint Committee (G-BA) and Quality Assurance in Health Care
 and Quality Assurance in Health Care") The Federal Joint Committee (G-BA) and Quality Assurance in Health Care The Hague, 18. November 2010 Dr. Dorothea Bronner Chief Executive Director Federal Joint Committee (G-BA) The Federal Joint Committee
The Federal Joint Committee (G-BA) and Quality Assurance in Health Care The Hague, 18. November 2010 Dr. Dorothea Bronner Chief Executive Director Federal Joint Committee (G-BA) The Federal Joint Committee
CALIFORNIA Small Group HMO Aetna Health of California, Inc. Plan Effective Date: 04/01/2007. Aetna Value Network* HMO $30/$40
 PLAN FEATURES Deductible (per calendar year) Member Coinsurance Lifetime Maximum Primary Care Physician Selection Referral Requirement PHYSICIAN SERVICES CALIFORNIA Small Group HMO Primary Care Physician
PLAN FEATURES Deductible (per calendar year) Member Coinsurance Lifetime Maximum Primary Care Physician Selection Referral Requirement PHYSICIAN SERVICES CALIFORNIA Small Group HMO Primary Care Physician
Health System Funding Reform
 Health System Funding Reform July 6 th, 2015 Brian Pollard A/Director, Health System Funding Policy Branch Health System Funding and Quality Ministry of Health and Long-Term Care Patients First: Action
Health System Funding Reform July 6 th, 2015 Brian Pollard A/Director, Health System Funding Policy Branch Health System Funding and Quality Ministry of Health and Long-Term Care Patients First: Action
2015 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators
 215 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators TAB Intro Population IP ED MH OBS LHIN map, the list of acronyms, and key definitions 1. Paediatric Population Overview Ontario
215 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators TAB Intro Population IP ED MH OBS LHIN map, the list of acronyms, and key definitions 1. Paediatric Population Overview Ontario
Pediatric Cardiology Clinical Privileges
 Name: Effective from / / to / / Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants should meet the following requirements as approved by the governing body,
Name: Effective from / / to / / Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants should meet the following requirements as approved by the governing body,
2016 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators
 216 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators TAB Intro Population IP ED MH OBS LHIN map, the list of acronyms, and key definitions 1. Paediatric Population Overview Ontario
216 Ontario Hospitals Maternal-Child Services Report LHIN-level Indicators TAB Intro Population IP ED MH OBS LHIN map, the list of acronyms, and key definitions 1. Paediatric Population Overview Ontario
Hospitalizations for Ambulatory Care Sensitive Conditions (ACSC)
") Hospitalizations for Ambulatory Care Sensitive Conditions (ACSC) Resource for Indicator Standards (RIS) Health Analytics Branch, Ministry of Health and Long-Term Care Indicator description RIS indicator
Hospitalizations for Ambulatory Care Sensitive Conditions (ACSC) Resource for Indicator Standards (RIS) Health Analytics Branch, Ministry of Health and Long-Term Care Indicator description RIS indicator
Schedule of Benefits Harvard Pilgrim Health Care, Inc.
 Schedule of Benefits Harvard Pilgrim Health Care, Inc. THE HARVARD PILGRIM-LAHEY SELECT HMO OOA MASSACHUSETTS 6-SPF, 01/13 MD0000002737 Please Note: In this plan, Member s have access to network benefits
Schedule of Benefits Harvard Pilgrim Health Care, Inc. THE HARVARD PILGRIM-LAHEY SELECT HMO OOA MASSACHUSETTS 6-SPF, 01/13 MD0000002737 Please Note: In this plan, Member s have access to network benefits
Anthem Blue Cross Effective: January 1, 2017 Your Plan: University of California High Option Supplement to Medicare
 Anthem Blue Cross Effective: January 1, 2017 Your Plan: University of California High Option Supplement to Medicare Please Note: this medical plan is a complement to your existing Medicare plan. Medicare
Anthem Blue Cross Effective: January 1, 2017 Your Plan: University of California High Option Supplement to Medicare Please Note: this medical plan is a complement to your existing Medicare plan. Medicare
How to Calculate CIHI s Cost of a Standard Hospital Stay Indicator
 Job Aid December 2016 How to Calculate CIHI s Cost of a Standard Hospital Stay Indicator This handout is intended as a quick reference. For more detailed information on the Cost of a Standard Hospital
Job Aid December 2016 How to Calculate CIHI s Cost of a Standard Hospital Stay Indicator This handout is intended as a quick reference. For more detailed information on the Cost of a Standard Hospital
COMMITTEE REPORTS TO THE BOARD
 Item # 9 F i COMMITTEE REPORTS TO THE BOARD To From South East LHIN Board Members Quality Committee Reviewed by Quality Committee Committee Members of the Committee were given the opportunity to review
Item # 9 F i COMMITTEE REPORTS TO THE BOARD To From South East LHIN Board Members Quality Committee Reviewed by Quality Committee Committee Members of the Committee were given the opportunity to review
INFORMATION ABOUT YOUR OXFORD COVERAGE REIMBURSEMENT PART I OXFORD HEALTH PLANS OXFORD HEALTH PLANS (NJ), INC.
, INC.") OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
Smart Choice. Level of cover with Australian Unity. Excess options. Cover availability. Hospital and Extras Cover Effective from 15 February 2018 $500
 Hospital and Extras Cover Effective from 15 February 2018 Level of cover with Australian Unity Cover availability Excess options $500 HOSPITAL MID EXTRAS MID SINGLE COUPLE FAMILY EXCESS Excess is waived
Hospital and Extras Cover Effective from 15 February 2018 Level of cover with Australian Unity Cover availability Excess options $500 HOSPITAL MID EXTRAS MID SINGLE COUPLE FAMILY EXCESS Excess is waived
Outpatient Quality Reporting Program
 Outpatient Quality Reporting Program Hospital Outpatient Quality Reporting (OQR) Program 2018 Specifications Manual Update Questions & Answers Moderator: Pam Harris, BSN, RN Speaker: Melissa Thompson,
Outpatient Quality Reporting Program Hospital Outpatient Quality Reporting (OQR) Program 2018 Specifications Manual Update Questions & Answers Moderator: Pam Harris, BSN, RN Speaker: Melissa Thompson,
Hospital Care for Future Generations
 Hospital Care for Future Generations May 26 Huntsville; May 27 Bracebridge; May 28 - Gravenhurst Outstanding Care ~ People Focused Purpose & Desired Outcomes Provide an overview of the required planning
Hospital Care for Future Generations May 26 Huntsville; May 27 Bracebridge; May 28 - Gravenhurst Outstanding Care ~ People Focused Purpose & Desired Outcomes Provide an overview of the required planning
NOTE: New Hampshire rules, to
 NOTE: New Hampshire rules, 309.01 to 309.08 Email Request: Selected Items in Table of Contents: (8) Time Of Request: Sunday, August 07, 2011 18:11:07 EST Send To: MEGADEAL, ACADEMIC UNIVERSE UNIVERSITY
NOTE: New Hampshire rules, 309.01 to 309.08 Email Request: Selected Items in Table of Contents: (8) Time Of Request: Sunday, August 07, 2011 18:11:07 EST Send To: MEGADEAL, ACADEMIC UNIVERSE UNIVERSITY
Integrated Health Services Plan
 Integrated Health Services Plan 3 2013-2016 02 IHSP 3 Central West LHIN Contents i ii iii Contents Executive Summary Strategic Directions 1 Section A: Today s Health Care Environment 1 Why LHINs? 2 Planning
Integrated Health Services Plan 3 2013-2016 02 IHSP 3 Central West LHIN Contents i ii iii Contents Executive Summary Strategic Directions 1 Section A: Today s Health Care Environment 1 Why LHINs? 2 Planning