REDUCING READMISSIONS
|
|
|
- Virginia Parsons
- 5 years ago
- Views:
Transcription
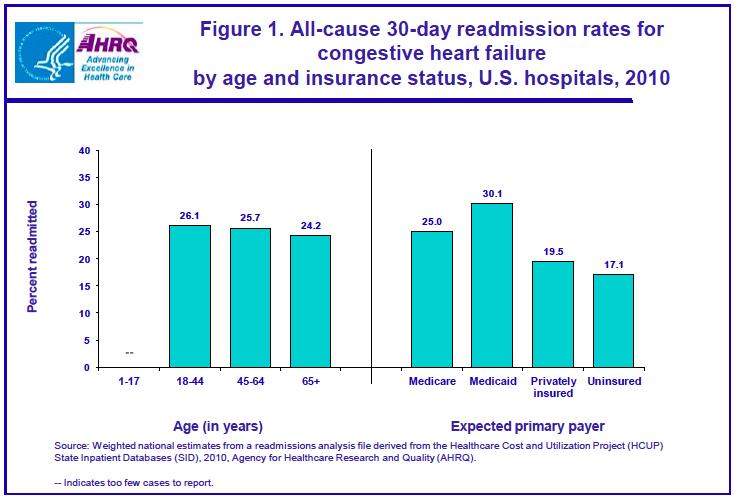
1 REDUCING READMISSIONS Focus on Medicaid, the Emergency Department and Behavioral Health Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies February
2 Objectives What are hospitals with hospital-wide results doing? How does that differ from what we are doing? What are 3 practical ways to expand our strategies?
3 Key Messages Medicaid adults have high readmission rates Medicaid patients need to be specifically identified as high-risk of readmission Readmission reduction efforts must include the ED High risk targeting should include presence of BH comorbidities and High Utilizers with any diagnoses
4 THANK YOU CMS 6 game-changing messages from CMS policies..
5 6 Very Important Messages from CMS Readmission reduction pays inaction hurts Hospitals must update & standardize transitional care processes Reducing readmissions is a cross-continuum effort Attend to non-clinical needs for post-hospital supports & services We will flood the market with all best ideas on our dime Reducing readmissions requires better data
6 HOWEVER. Powerful messages from powerful agencies can create blinders
7 CMS Medicare Focus Has Created Blinders 1. HF, AMI, PNA COPD, hip/knee replacement NOT the 5 most frequent diagnoses leading to readmissions CMS discharge diagnosis-specific penalty obscured other meaningful categorizations s/a frequent utilizer, social complexity, BH, functional status 2. Driven a Medicare focus to the exclusion of other high risk patient groups Medicaid adults have higher readmission rates than Medicare FFS 3. Driven a case-finding approach Interventions often limited to Medicare FFS with certain diagnosis Created a 2- tiered discharge process - at odds with principles of quality 4. Preferred first move among hospitals: hire a Transitional Care FTE Lost the focus on reliable redesign on transitional care for all patients Hire dedicated staff to focus only on penalty condition patients
8 Medicare Readmission Penalties October September Up to 3% reduction in all Medicare payments for hospitals 6 Dx: AMI, HF, PNA, COPD and hip and knee replacement Average penalty DOUBLED this year 2,160 hospitals penalized; $480 MILLION
9 CRUNCHING THE NUMBERS Will your current strategy get you to your goal?
10 Let s Run the Numbers: One Strategy Won t Get Us There Number Rate Medicare admits/year 5,000 admissions Medicare RA rate 18% # Medicare RA /year 900 readmissions Pilot project 200 high risk patients Pilot group RA rate 25% Expected # RA pilot 50 Expected effect of pilot 20% # RA reduced by pilot 10 # Medicare RA/year = = 890 1%
11 Hospitals with hospital-wide results Know their data Analyze, trend, track, display, share, post Broad concept of readmission risk Way beyond case finding for diagnoses Multifaceted strategy Improve standard care, collaborate across settings, enhanced care Use technology to make this better, quicker, automated Automated notifications, implementation tracking, dashboards
12 EXPAND EFFORTS FOR IMPACT Broad concept of risk, broad understanding of patient needs
13 Next Frontier: Medicaid Readmissions What is different? What is similar? Population analyses of Medicaid readmission rates are low Because they include high-volume deliveries (OB) and pediatric discharges Readmission rates appear low and providers think there is no problem in Medicaid Emerging experience suggests that social, financial, behavioral health factors greatly influence risk of readmission Adult Medicaid patients would be expected to have a high prevalence of social, financial and behavioral health issues Little has been described about readmission rates and the factors that contribute to readmissions among the younger adult population

14 1. Know Your Data 2. Inventory Readmission Efforts 3. Develop a Portfolio of Strategies 4. Improve Hospital-based Transitional Care 5. Collaborate with Cross Setting Partners 6. Provide Enhanced Services 13 new Tools

15 Tools 1. Readmission Data Analysis 2. Readmission Interview 3. Data Analysis Synthesis 4. Hospital Inventory 5. Cross-Continuum Team Inventory 6. Conditions of Participation Checklist 7. Portfolio Design 8. Readmission Reduction Impact 9. Readmission Risk 10. Whole-Person Assessment 11. Discharge Information Checklist 12. Forming a Cross-Continuum Team 13. Community Resource Guide
16 KNOW YOUR (OWN) DATA Analyze, track, trend, raw unadjusted data to identify opportunities
17 Readmission Analysis Use the most recent 12 months of data available. Using all hospital discharge data, exclude patients <18, all OB (DRG ), discharges dead, or transfers to another acute care hospital. Define a readmission as any return to inpatient status within 30-days of discharge from inpatient status. Measure Total Medicare Medicaid Private A. Total Discharges B. Total Readmissions C. Readmission Rate (B/A) D. Total Discharges to Home E. Total Discharges to SNF F. Total Discharges to Home Health Care G. Total Discharges with any coded Behavioral Health Diagnosis ( ) H. Total Readmissions with any coded Behavioral Health Diagnosis I. Number / % of readmissions occurring within 7 days of d/c J. Number of patients with 4 hospitalizations in past year K. Total number of discharges among [J] L. Total Number of 30-day readmissions among [J] M. Top 10 Discharge Diagnoses Resulting in Readmission, by Payer All Payer Medicare Medicaid N. Proportion of all readmissions represented by top 10 discharge diagnoses X% Y% Z% Collaborative Healthcare Strategies 2015
18 Readmission Analysis Use the most recent 12 months of data available. Using all hospital discharge data, exclude patients <18, all OB (DRG ), discharges dead, or transfers to another acute care hospital. Define a readmission as any return to inpatient status within 30-days of discharge from inpatient status. Measure Total Medicare Medicaid Uninsured A. Total Discharges (7%) B. Total Readmissions (64%) 77 C. Readmission Rate (B/A) 13.1% 14.1% 17.9% 9.2% D. Total Discharges to Home (Routine Discharge) (50%) 4460 (77%) 731 E. Total Discharges to SNF (25%) F. Total Discharges to Home Health Care (25%) G. Total Discharges with any coded Behavioral Health Diagnosis) 7456 (60%) H. Total Readmissions with any coded Behavioral Health Diagnosis 1320 (82%) I. Number of readmissions occurring within 7 days of d/c 578 (36%) J. Number of patients with 4 hospitalizations in past year K. Total number of discharges among [J] 1734 (14%) (21%) 55 L. Total Number of 30-day readmissions among [J] 563 (35%) M. Proportion of All Readmissions Accounted for by top 10 Diagnoses 28% Collaborative Healthcare Strategies 2015
19 All-Payer by Payer Readmission Analysis Medicare Medicaid Comm. Unins. Total ARF (1384) Sickle Cell (478) Chemo (290) Pancreatitis (187) Sepsis (1859) Sepsis (1366) Sepsis (175) CVA (276) Chemo (157) ARF (1800) PNA (1336) Chemo (175) Arthritis (260) DKA (136) PNA (1750) COPD (1211) COPD (173) Sepsis (222) CVA (125) CVA (1622) CVA (1140) DKA (156) PNA (188) COPD (109) COPD (1608) UTI (1038) PNA (145) ARF (182) ARF (97) UTI (1608) Afib (851) ARF (137) CAD (181) Sepsis (96) HF (1115) HF (822) HF (129) Pancreatitis (153) PNA (81) CAD (1092) CAD (746) Pancreatitis (127) Afib (152) ETOH w/d (76) Afib (1092) Method: DRG, age>18, exclude OB

20 Methods: - Used CCS groupers - Included OB Top 10 Medicaid Dx: 1. Mood disorder 2. Schizophrenia 3. Diabetes complications 4. Comp. of pregnancy 5. Alcohol-related 6. Early labor 7. CHF 8. Sepsis 9. COPD 10. Substance-use related Top 10 Medicare Dx: 1. CHF 2. Sepsis 3. Pneumonia 4. COPD 5. Arrythmia 6. UTI 7. Acute renal failure 8. AMI 9. Complication of device 10. Stroke
21
22 County Hospital Readmission Stats Measure # % Total Discharges 11,850 Total Medicare Discharges 967 8% total Total (adult non-ob) Medicaid Discharges 4,288 36% total Total 30-day Readmissions 1,631 14% RA rate Total Medicare Readmissions 154, 9% total 16% RA rate Total (adult-non-ob) Medicaid Readmissions 823, 50% total 19% RA rate Medicaid RA are 35% higher than all-payer RA Medicaid RA account for 50% of ALL Readmissions

23 Medicare v. Medicaid Discharge Disposition Measure Medicare Medicaid Discharge to Home 55% 84% Discharge to SNF/IRF/LTAC 24% 5% Discharge to Home with Home Health 14% 8% Other 7% 3%
24 Medicaid High Utilizers - AHRQ >3 hospitalizations/year 85% are over age 21 Average ~6 hospitalizations/year v. 1.3 for non-high utilizers Average LOS 6.1 days v. 4.5 for non-high utilizers Average cost per hospitalization $11,600 v. $9,000 for non high-utilizers Readmission rate 52% v. 8% for non high-utilizers 74% of high utilizers are discharged to home Top Dx: mood disorders, schizophrenia, DM, chemo, sickle cell, ETOH, sepsis, CHF, COPD Jiang et al. HCUP Statistical Brief #184 Nov 2014
25 ASK YOUR PATIENTS WHY Interview patients, caregivers for the story behind the chief complaint
26 Understand the story behind the chief complaint 61M with 8 hospitalizations this year for shortness of breath returns to the hospital 10 days after discharge with shortness of breath. 45F with HIV hospitalized for pneumonia discharged to home returns to the hospital 8 days later with pneumonia. 32M with uncontrolled DM, cognitive limitations, bipolar disorder, active substance use, homeless presents with flank pain to one hospital, readmitted with chest pain to another hospital Chart reviews and administrative analyses will NOT reveal what you need to know: you must talk to your patients, their families and caregivers, providers
27 Root Cause of Chest Pain Admission: Shelter I need housing, not a shelter. I need someone to help make sure I take my medicines. In a shelter they don't do that and they kick you out every morning. I need a stable residence and no one is able to help with that." Acute Care Utilization over 180 days of freedom 15#Sep'Prison' Prison' Prison' Prison' Prison' Released' 22#Sep' ED' DC' 29#Sep' 6#Oct' ED' ED' IN' IN' 13#Oct'IN' IN' DC' 20#Oct' ED' DC' 27#Oct' IN' ED' DC' ED' 3#Nov'IN' IN' IN' IN' IN' DC/ED' IN' 10#Nov'IN' IN' ED' IN' IN' IN' IN' 17#Nov'IN' IN' DC' ED' IN' IN' ED/DC' 24#Nov'IN' ED' ED' ED' IN' 1#Dec'ED' IN' DC' ED' 8#Dec'IN' IN' IN' IN' IN' IN' IN' 15#Dec'IN' IN' DC' 22#Dec' 29#Dec' 5#Jan' ED' ED' IN' DC' ED' 12#Jan' ED' 19#Jan'ED' IN' IN' IN' IN' DC' ED' 26#Jan'DC' ED' ED' IN' 2#Feb'IN' IN' IN' IN' IN' IN' IN' 9#Feb'IN' IN' IN' IN' IN' IN' IN' 16#Feb'IN' IN' IN' DC' IN' IN' IN' ED'(DC' 23#Feb'IN' IN' Brockton)' IN'?' ED' '' 2#Mar' IN' IN' DC/ED' IN' 9#Mar'DC' ED' DC' ED' IN' IN' IN' 16#Mar'IN' IN' ''
28 There is Never One Reason for Readmission.. KP team reviewed 523 readmissions across ~14 hospitals: 250 (47%) deemed potentially preventable Found an average of 9 factors contributed to each readmission Assessed factors related to 5 domains: 73% - care transitions planning & care coordination 80% - clinical care 49% - logistics of follow up care 41% - advanced care planning & end of life 28% - medications 250 readmissions identified 1,867 factors! Feingenbaum et al Medical Care 50(7): July 2012
29 Interviewed 60 patients who returned to ED after d/c from ED <9days Average age 43 (19-75) Majority had a PCP, but cited ED gave more tests, quicker answers, single site and ED more likely to treat the symptoms Most reported no problem filling medications 19//60 thought they didn t get prescribed the medications they needed (pain) 24/60 expressed concerns about clinical evaluation and diagnosis Primary reason for returning: fear and uncertainty about their condition Patients need more reassurance during and after episodes of care Patients need access to advice between visits Annals of Emergency Medicine
30 DESIGN A PORTFOLIO OF STRATEGIES Readmission reduction = System transformation

31 Develop A Multifaceted Portfolio of Efforts Improve hospital-based care processes for all patients, including ED Collaborate with cross-setting partners, including payers, BH, Social Services, EMS, public health, SUD Provide enhanced services Use data, analytics, flags, workflow prompts, automation, dashboards to support continuous improvement, ensure reliability, drive to results
32 EXPANDING EFFORTS TO DRIVE IMPACT Adding ED, BH, social stabilization to your portfolio

33 2 Hospitals Multifaceted Portfolios Valley Baptist (TX) Frederick Memorial (MD) Improve Standard Hospital-based Processes ED-based SW/CM identify patients at point of entry CM screen for all patients move from 8P to behavioral interview Collaborate with Providers 25-member cross continuum team, meets monthly Track and trend H-SNF readmissions, review each, INTERACT Track and trend H-HH patients, weekly comanagement virtual rounds (move up the continuum from HH to direct SNF if needed) Warm handoffs, points of contact with community BH provider Use off-site urgent care center for post-d/c appointments if needed Provide Enhanced Services to High Risk CM refer via order entry to Care Transitions Team Multi-disciplinary team works the case x 30+ days Cardiology NP Heart Bridge Clinic Courtesy of Angela Blackford and Heather Kirby
34 Hospital-wide Results Valley Baptist (TX) All Cause Readmission Rate: FY 2011: 28% FY 2013: 21% FY 2014: 14% Frederick Memorial (MD) FY % FY 13 9% FY % CMS Penalty: Year 1: 0.8% (of possible 1%) Year 2: 0.2% (of possible 2%) Year % (of possible 3%) Courtesy of Angela Blackford and Heather Kirby
35 Interventions Led by the ED Hallmark Health System 2 hospital system, 20 ED docs, 17 PAs Why are almost all SNF patients admitted? Patients only seen once a month ; can t do IVs, etc If they send them here they can t take care of them Actions: Asked ED clinicians 5 whys Education: posted INTERACT SNF capacity sheets in ED Simplicity : establish contacts, standard transfer information Results: increase in number of patients transferred from ED to SNF Source: Dr Steven Sbardella, CMO and Chief of ED Hallmark Health System Melrose, MA
36 Interventions Led by the ED ED- Community BH Services ED County DPH Health Alliance Hospital High ED boarding Data showed 75% d/c to home Identified linkage to care as need ED didn t know BH center Called meeting; weekly x 10 weeks Reassigned ED RN to be BH ED navigator Redesigned triage / flow Effectively link to BH care BH deployed existing case workers Reduced high-user ED BH visits Carroll County, Maryland County- peer recovery navigators Were underutilized Reached out to ED Co-located peer navigators in ED Connected and followed after ED 30% reduction high-user ED BH
37 Transitional Care: Actively Address Social Complexity Social Work Transitional Care Assess person in context Employ motivational interviewing Connect, assess, reassess Needs change over time Navigate clinical follow up Ensure linkage to services Don t over medicalize complexity Multi-Disciplinary Care Teams NP, RN, SW, Pharm, Navigator Address full complement of medical, social, logistical needs Navigator position particularly valuable for outreach, relationships Highland Hospital: team actively inquires about SUD, links to care, harm reduction approach Courtesy of Maia White, Highland Hospital
38 No Shortage of Great Practices to Emulate! 1. INTERACT SNF-ED-SNF 2. County DPH peer recovery workers in ED to connect and navigate 3. ED Community Mental Health and CHC effective linkage to post-ed follow up 4. ED-based High Utilizer Care Team, using ED to identify, connect, follow 5. Automated flag in ED Record to indicate 30-day return 6. MGH High Cost Beneficiary Demo page care team from ED to avert admission 7. Payer (MCO) deployed transitional care staff colocated in hospital 8. Payer (MCO) supported CHW navigator programs 9. Payer (MCO) supported sickle cell urgent care clinic 10. County workforce development program CHW training 11. County-EMS home visit program 12. Reverse co-location medical providers (NP) co-located in community BH centers 13. Housing with services multi-disciplinary team co-located at housing sites 14. Warm handoffs hospital-snf with call-back 15. Virtual rounding hospital-snf to co-manage over numerous transitions
39 Let s Run the Numbers: Three-part strategy Medicare admits/year Number 5,000 admissions Rate Medicare RA rate 20% # Medicare RA /year 1,000 readmissions 1. Improve standard care 5,000 admissions (20% RA rate) Expected effect 10% Expected # RA reduction 100 RA avoided 2. Collaborate with receivers 1650 admissions (1/3 total) (30% RA rate) Expected effect 20% Expected # RA reduction 3. Enhanced Service for Pilot 99 RA avoided 200 admissions (25% RA rate) Expected effect 20% Expected # RA reduction 10 RA avoided Total (*illustrative) 209 RA avoided* 209/1000 = 20% overall* Amy Boutwell 2013
40 46-study Meta-Analysis: What Works? Preventing 30-Day Hospital Readmissions A Systematic Review and Meta-analysis of Randomized Trials Leppin et al; JAMA Internal Medicine (online first) May Review of 42 published studies of discharge interventions Found that multi-faceted interventions were 1.4 times more effective Many components More people Support patient self-care Interventions published more recently had fewer components are were found to be less effective
41 Recommendations Know your data and your patients Adopt a broad concept of readmission risk Capture all reasons, whole-person approach Develop a multifaceted strategy Start in ED Expand partners, include agencies, payers Provide enhanced services Use technologies to make work better, quicker, automated
42 THANK YOU Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Lexington, Massachusetts
REDUCING READMISSIONS
 REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
REDUCING READMISSIONS - 2015 Expanding efforts to drive to hospital-wide results Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies January 2015 Objectives What are hospitals with hospital-wide
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
ASPIRE to Reduce Readmissions
 ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
ASPIRE to Reduce Readmissions Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Objectives Explain the value of a data-informed, whole-person approach to reducing readmissions Identify
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
STRATEGIES TO REDUCE READMISSIONS
 STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
STRATEGIES TO REDUCE READMISSIONS Delivering whole-person transitional care Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies Co-Principal Investigator, Designing and Delivering Whole-Person
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
Reducing Medicaid Readmissions Webinar 3: High Impact Medicaid-Specific Strategies Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project March 25, 2015 Overview:
ASPIRE to Knockout Pneumonia Readmissions Webinar #1. Amy Boutwell, MD, MPP March 1, 2018
 ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
ASPIRE to Knockout Pneumonia Readmissions Webinar #1 Amy Boutwell, MD, MPP March 1, 2018 NCHA Pneumonia Knockout Team Karen Southard VP, Quality & Clinical Performance Improvement pne@ncha.org Trish Vandersea
NoCVA Preventing Avoidable Readmissions. Moving Beyond the Basics March 27, 2014
 NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
NoCVA Preventing Avoidable Readmissions Moving Beyond the Basics March 27, 2014 Dr. Amy Boutwell REDUCING READMISSIONS IN 2014 Using data to drive an expanded, multifaceted strategy Amy E. Boutwell, MD,
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia. Webinar #3 Post-Acute Care Readmissions September 8, 2016
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #3 Post-Acute Care Readmissions September 8, 2016 HOUSEKEEPING Slides were sent this morning Webinar is being
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement.
 Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
Emergency Department Visits After Inpatient Discharge in Massachusetts: Applying Insights from Data to Inform Improvement November 15, 2017 Today Introductory Remarks Patricia M. Noga, PhD, RN, FAAN, Vice
5/26/2015. January 26, 2015 INCENTIVES AND PENALTIES. Medicare Readmission Penalties. CMS Bundled Payment Providers & ACOs in NE
 Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
Agenda ESTABLISHING SHARED EXPECTATIONS New tool of ACOs, Bundled Payments & Readmission Reduction Update on current market pressures driving a focus on care across settings & over time at lowest cost
REDUCING READMISSIONS FOR SNF PATIENTS
 REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
HOUSEKEEPING. Slides were sent this morning Webinar is being recorded Please use the telephone option
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Webinar #6 Deep Dive Series: ED-based Strategies January 25, 2017 HOUSEKEEPING Slides were sent this morning Webinar
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge. July 24, 2018
 FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
FHA HIIN Readmissions Peer Sharing Webinar: Improving Care Transitions through a Discharge Lounge July 24, 2018 Welcome & Overview How are we doing on Reducing Readmissions? Peer Sharing Presentation:
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Readmissions Moving beyond blame to fill the patient needs. Jackie Conrad RN, MBA, RCC Cynosure Health
 Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings
 Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings PT, MS, DPT C &V SENIOR CARE SPECIALISTS, INC. STAR RATINGS QUALITY OF PATIENT CARE STAR RATING METHODOLOGY Process
Integrating Behavioral Health with Chronic Care to Improve Outcomes and Star Ratings PT, MS, DPT C &V SENIOR CARE SPECIALISTS, INC. STAR RATINGS QUALITY OF PATIENT CARE STAR RATING METHODOLOGY Process
2016 Embedded and Rapid Response Care Management
 2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
2016 Embedded and Rapid Response Care Management Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Embedded and Rapid Response Care Management Program Evaluation
Hospital Readmission Reduction: Not Just Nursing s Job
 Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
Hospital Readmission Reduction: Not Just Nursing s Job David Farrell, LNHA, MSW Affordable Care Act - Three Aims Better patient experience Better outcomes Lower costs 1 Linking Payments to Quality Outcomes
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings Executive Summary The Alliance for Home Health Quality and
30-day Hospital Readmissions in Washington State
 30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
30-day Hospital Readmissions in Washington State May 28, 2015 Seattle Readmissions Summit 2015 The Alliance: Who We Are Multi-stakeholder. More than 185 member organizations representing purchasers, plans,
Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014
 Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014 Data analysis at a population level Implications for our care model Facilitated discussion Population management
Monica Bharel and Jessie M. Gaeta Boston Health Care for the Homeless Program NHCHC May 2014 Data analysis at a population level Implications for our care model Facilitated discussion Population management
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives
 SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
SNF * Readmissions Bootcamp The SNF Readmission Penalty, Post-Acute Networks, and Community Collaboratives Lindsay Holland, MHA Associate Director, Care Transitions Health Services Advisory Group (HSAG)
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Transitional Care Management. Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA
 Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Transitional Care Management Marianne Durling, MHA, RHIA, CCS,CDIP, CPC,CPCO,CIC & Heather Greene, MBA, RHIA, CPC, CPMA 2 Agenda Definitions Why Transitional Care TCM Overview TCM Model Case Study 3 Definitions
Chapter VII. Health Data Warehouse
 Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
L19: Improving Transitions from the Hospital to Post Acute Care Settings
 This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
This presenter has nothing to disclose L19: Improving Transitions from the Hospital to Post Acute Care Settings Gail A. Nielsen December 8, 2013 25th Annual National Forum on Quality Improvement in Health
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014
 USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
USING ACUTE CARE PLANS TO IMPROVE COORDINATION AMONG ED HIGH UTILIZER PATIENTS MASSACHUSETTS GENERAL HOSPITAL Publication Year: 2014 SUMMARY: High utilizer patients often get a full work-up every time
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES
 EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling
 Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Improving Service Delivery for Medicaid Clients Through Data Integration and Predictive Modeling Getty Images David Mancuso, PhD July 28, 2015 1 The Medicaid Environment Program costs are often driven
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Behavioral Health Division JPS Health Network
 Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Behavioral Health Division JPS Health Network Macro Trends 1 in 5 Adults in America experience a mental illness Diversion of Behavioral Health patients from jail Federal Prisons Mental Illness State Prison
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Balancing State, Federal and Internal Bundle Payment Initiatives
 Balancing State, Federal and Internal Bundle Payment Initiatives Vanderbilt University Medical Center Brittany Cunningham, MSN, RN, CSSBB Director, Episodes of Care Key Take Aways What are the different
Balancing State, Federal and Internal Bundle Payment Initiatives Vanderbilt University Medical Center Brittany Cunningham, MSN, RN, CSSBB Director, Episodes of Care Key Take Aways What are the different
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Overview of New Nursing Roles in Whole Person Care. Session 1
 Overview of New Nursing Roles in Whole Person Care Session 1 1 Introductions Anne Shields, MHA, RN Associate Director, UW AIMS Center 2 Learning Objectives RN Primary Care Managers Focus Patient Population:
Overview of New Nursing Roles in Whole Person Care Session 1 1 Introductions Anne Shields, MHA, RN Associate Director, UW AIMS Center 2 Learning Objectives RN Primary Care Managers Focus Patient Population:
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Community Performance Report
 : Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
: Wenatchee Current Year: Q1 217 through Q4 217 Qualis Health Communities for Safer Transitions of Care Performance Report : Wenatchee Includes Data Through: Q4 217 Report Created: May 3, 218 Purpose of
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Maryland s Integrated Care Network. Heading into Year Three
 Maryland s Integrated Care Network Heading into Year Three Facilitator David Finney Chief of Staff, CRISP Partner, Leap Orbit Learning Objectives At the end of this session, you will be able to Explain
Maryland s Integrated Care Network Heading into Year Three Facilitator David Finney Chief of Staff, CRISP Partner, Leap Orbit Learning Objectives At the end of this session, you will be able to Explain
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Executive Summary MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA
 HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q STATE OF CALIFORNIA") MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
MEDICARE FEE-FOR-SERVICE (FFS) HOSPITAL READMISSIONS: QUARTER 4 (Q4) 2012 Q3 2013 Executive Summary STATE OF CALIFORNIA The Centers for Medicare & Medicaid Services (CMS) has tasked Health Services Advisory
The STAAR Initiative
 The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
The STAAR Initiative A quality effort at the heart of system redesign Amy E. Boutwell, MD, MPP The Center for Innovative Healthcare Strategies amy@innovativehealthcarestrategies.org Please note: Dr Boutwell
Community Discharge and Rehospitalization Outcome Measures (Fiscal Year 2011)
") Andrew Kramer, MD Ron Fish, MBA Sung-joon Min, PhD Providigm, LLC Community Discharge and Rehospitalization Outcome Measures (Fiscal Year 2011) A report by staff from Providigm, LLC, for the Medicare Payment
Andrew Kramer, MD Ron Fish, MBA Sung-joon Min, PhD Providigm, LLC Community Discharge and Rehospitalization Outcome Measures (Fiscal Year 2011) A report by staff from Providigm, LLC, for the Medicare Payment
Improving Heart Failure Outcomes through Interactive Patient Care: The Sentara Virginia Beach General Hospital Experience
 WHITE PAPER Improving Heart Failure Outcomes through Interactive Patient Care: The Sentara Virginia Beach General Hospital Experience 06.05.09 executive summary In the United States, Heart Failure has
WHITE PAPER Improving Heart Failure Outcomes through Interactive Patient Care: The Sentara Virginia Beach General Hospital Experience 06.05.09 executive summary In the United States, Heart Failure has
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Molina Healthcare Michigan Health Care Services Department Phone: (855) Fax: (800)
 Fax: (800)") Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions
 Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
Collaborative Approach to Improving Care and Reducing Readmissions Edna Clifton, MBA, BSN, RN Associate Director, Care Coordination Health Services Advisory Group (HSAG) March 14, 2017 Presentation Objectives
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. Bluebonnet Trails Community Services
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings
 Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
Medicare Spending and Rehospitalization for Chronically Ill Medicare Beneficiaries: Home Health Use Compared to Other Post-Acute Care Settings May 11, 2009 Avalere Health LLC Avalere Health LLC The intersection
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth
: Improving Quality While Slowing Spending Growth") The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
The Alternative Quality Contract (AQC): Improving Quality While Slowing Spending Growth Dana Gelb Safran, ScD Senior Vice President, Performance Measurement and Improvement Presented at: MAHQ 16 April
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
How to Win Under Bundled Payments
 How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
Improving Care Transitions
 Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
Care Transitions Collaborative Improving Care Transitions Laura Cole, RN South Carolina Partnership for Health SPECIFIC QUESTIONS WE WILL EXPLORE TODAY: Why the focus on care transitions? What strategies
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Regional Partnership for Health System Transformation Regional Transformation Plan Final Report Due: December 7, 2015
 Regional Partnership for Health System Transformation Regional Transformation Plan Final Report Due: December 7, 2015 Regional Partner: Trivergent Health Alliance Maryland s Vision for Transformation:
Regional Partnership for Health System Transformation Regional Transformation Plan Final Report Due: December 7, 2015 Regional Partner: Trivergent Health Alliance Maryland s Vision for Transformation:
Connected Care Connected Car Program Connected Care
 Connected Care Program Connected Care Initiative to improve the connection and coordination of care for those with Serious Mental Illness among health plans, PCPs, and behavioral health providers in outpatient,
Connected Care Program Connected Care Initiative to improve the connection and coordination of care for those with Serious Mental Illness among health plans, PCPs, and behavioral health providers in outpatient,
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Readmission Program. Objectives. Todays Inspiration 9/17/2018. Kristi Sidel MHA, BSN, RN Director of Quality Initiatives
 The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The In s and Out s of the CMS Readmission Program Kristi Sidel MHA, BSN, RN Director of Quality Initiatives Objectives General overview of the Hospital Readmission Reductions Program Description of measures
The Role of Analytics in the Development of a Successful Readmissions Program
 The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
The Role of Analytics in the Development of a Successful Readmissions Program Pierre Yong, MD, MPH Director, Quality Measurement & Value-Based Incentives Group Centers for Medicare & Medicaid Services
Integrated Care Management in the Age of Population Health: What does that mean?!?
 Integrated Care Management in the Age of Population Health: What does that mean?!? Integrated Care Management Conference September 21 and 22, 2016 Dot Verbrugge, MD Medical Director of Integrated Care
Integrated Care Management in the Age of Population Health: What does that mean?!? Integrated Care Management Conference September 21 and 22, 2016 Dot Verbrugge, MD Medical Director of Integrated Care
Public Policy and Health Care Quality. Readmissions: Taking Progress into the Future
 Public Policy and Health Care Quality Readmissions: Taking Progress into the Future Today s Agenda The Current State -- The Hospital Readmissions Reduction Program What Have We Learned? Polish Up the Crystal
Public Policy and Health Care Quality Readmissions: Taking Progress into the Future Today s Agenda The Current State -- The Hospital Readmissions Reduction Program What Have We Learned? Polish Up the Crystal
READMISSION ROOT CAUSE ANALYSIS REPORT
 USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
USE RESTRICTED TO ABC Hospital READMISSION ROOT CAUSE ANALYSIS REPORT State: Community Name: YZ Cohort: Hospital: A ABC Hospital Reviewer: Jane Doe Abstraction Period: 1/1/2014 6/30/2014 Charts Abstracted:
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health
 Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
Christi McCarren, SVP, Retail Health & Community Based Care Lynnell Hornbeck, Manager, Home Health Webinar: Northwest Regional Telehealth Resource Center October 27, 2016 1 MultiCare Health System MultiCare
PSYCHIATRY SERVICES UPDATE
 PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
Central Valley/West Valley Care Coordination Coalitions. Quarterly Community Meeting
 Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
Central Valley/West Valley Care Coordination Coalitions Ettie Lande, MS, RN Associate Director, Care Coordination (HSAG) Today s Agenda Welcome and Introduction Spotlight on Social Determinant of Health
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH
 INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model. ACO Congress November 5, 2013 Charles Kennedy
 Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Technology Driven Strategies for Enhancing Patient Engagement Within an ACO Model ACO Congress November 5, 2013 Charles Kennedy Aetna s values drive ACS strategy apple 2 Changing the emphasis from volume
Transitions of Care Innovations in the Medical Practice Setting
 Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
Transitions of Care Innovations in the Medical Practice Setting Linda Wendt, System Director of Quality- UnityPoint Clinic Sheila Tumilty, Senior Project Manager- UnityPoint Clinic Session Objectives After
PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER
 PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER PROJECT PURPOSE To reduce hospital readmissions for CHF, pneumonia patients To improve patient satisfaction with the discharge
PARAMEDIC-NURSE READMISSION PROJECT VALLEY AMBULANCE- REGIONAL WEST MEDICAL CENTER PROJECT PURPOSE To reduce hospital readmissions for CHF, pneumonia patients To improve patient satisfaction with the discharge
UCSF Transitional Care Program. Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016
 UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
UCSF Transitional Care Program Maureen Carroll RN CHFN Transitional Care Manager Heart Failure Program Coordinator November 1, 2016 Session Objectives Describe elements necessary for building a cross continuum
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
ILLINOIS 1115 WAIVER BRIEF
 ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Readmission Reduction: Patient Interviews. KHA Quality Conference March, 2018
 Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy
 Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Transitions Through the Care Continuum: Discussions on Barriers to Patient Care, Communications, and Advocacy Scott Matthew Bolhack, MD, MBA, CMD, CWS, FACP, FAAP April 29, 2017 Disclosure Slide I have
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute