Appleton, WI Lori Arnoldussen Kim Wildes
|
|
|
- Steven Dickerson
- 5 years ago
- Views:
Transcription

1 Appleton, WI Lori Arnoldussen Kim Wildes
2 The speaker has no actual or potential conflict of interest in relation to this presentation.
3







4 ThedaCare Physicians 200 Providers 27 Clinic locations 480, 260 office visits-2012 Cadence EpicCare My Chart Prelude OpTime Radiant Resolute Softmed Voice Stork Independent Specialty 150 Physicians 17 Specialty Practices Integrated Patient EMR Hospitals Beds Appleton 160 Theda Clark 260 New London 40 Waupaca 26 Shawano 25 ADT Cadence ASAP E-ICU EpicCare Beaker OpTime EpicRX Radiant Resolute Softmed Transcription Voice Stork Home Care 160 admits/month Epic Home Care
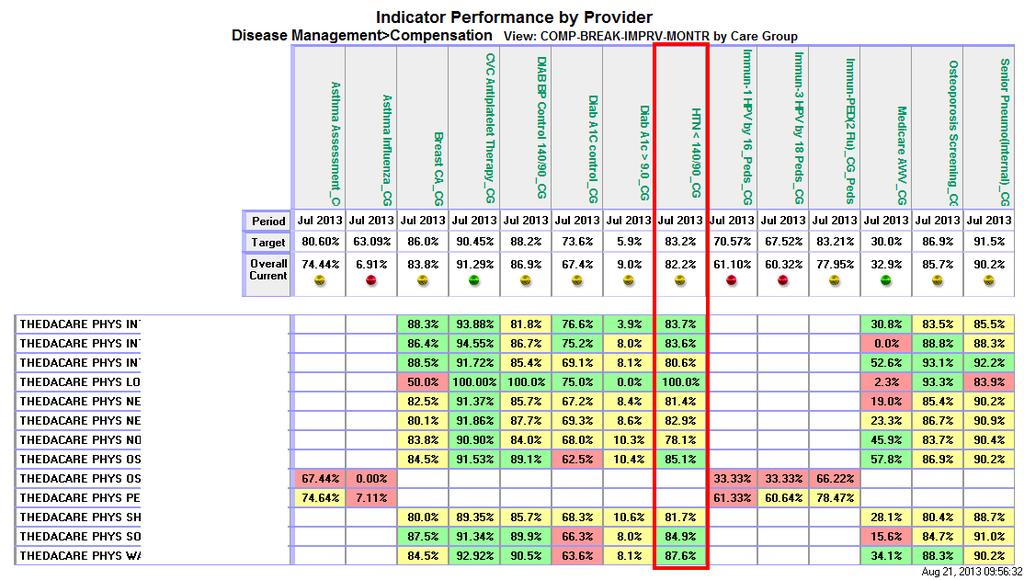
5 Approximately 50 million individuals in the United States have Hypertension. The higher the BP, the greater the risk of heart attack, heart failure, stroke, and kidney disease. Hypertension is the #1 diagnosis at ThedaCare (16,000+ patients). AMGA HTN Learning Collaborative AMGF Measure Up/Pressure Down campaign Million Hearts Hypertension Control Challenge Reference: (JNC-7) The seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure.
 20% improvement year to year Division Quality Goal Ambulatory Physicians Pay for")
6 Control to < 140/90 mm Hg System Quality Goals 90 th percentile in Wisconsin Collaborative for Healthcare Quality (WCHQ) 20% improvement year to year Division Quality Goal Ambulatory Physicians Pay for Performance
7 Primary goal of project was to see BP improvement in those patients with HTN who are currently not at goal (>140/90 mm Hg) Baseline rate = 72% Goal = 80% AUGUST 2013 Rate = 83% Target providers processes to increase HTN control Patient self-management 7
 Community involvement (i.e. pharmacy) LEAN tools 8")
8 Senior leadership support of QI initiatives Physician compensation plan EMR, data warehouse, HTN registry Worksheets Physician Scorecards Transparent results Wisconsin Collaborative for Healthcare Quality (WCHQ) Community involvement (i.e. pharmacy) LEAN tools 8
9 Clinical Variation Operational Competing priorities Data Volume
10 Clinical Pharmacist HTN Guideline (providers) Training and yearly competency on blood pressure measurement Patient-Self Management: Under Pressure program Operational Pre-visit scrub of chart Add BP goal to problem list Standard Work for Nurse & MA BP visits After-Visit Summary Monthly site-level, multi-disciplinary Disease Management meetings Data Larger lists than they were used to Develop trust in data

11
12

13

14
15
16 JNC 8 CME Remember the 17% that are not controlled Continuous discussion, focus, improvement, reminders


17
18 HTN Best Practice: Billings Clinic s Journey through the lenses of Complexity and Adaptive Leadership Elizabeth L. Ciemins, PhD, MPH, MA September 26, 2013 Health Care, Education and Research
19 I learned it because my friends were all doing it and it looked fun. My friend taught me, not my teacher. ~Cameron Leo, age 11, on why she learned The Cup Song, July 2013 Health Care, Education and Research
20 We yearn for frictionless, technological solutions. But people talking to people is still the way that norms and standards change. ~Atul Gawande from Slow Ideas, New Yorker, July 29, 2013 Health Care, Education and Research
21 Complexity Science-Informed Approach & Adaptive Leadership Model Health Care, Education and Research
22 Complexity Science Science that attempts to: Understand and explain the behavior and dynamics of systems composed of many interacting elements Uncover the principles and processes that explain how order, change and innovation emerge in these systems Consider health care organizations as Complex Adaptive Systems Health Care, Education and Research
23 What is a Complex Adaptive System? System implies: Multiple Agents Agents are Interdependent and Connected Complex implies: Diversity Many Elements Large Number of Connections Adaptive implies: Capacity to Alter or Change Health Care, Education and Research

24

25

26 Health Care, Education and Research 26
27 Interdependent Attributes Self-Organization & Emergence Adaptable Elements Order & Disorder Embedded Systems Diversity Non-Linearity Distributed Control 27 Health Care, Education and Research

28 Because Complex Adaptive Systems are nonlinear, a small change may produce a large effect, or a large change may produce a small or no effect. Inability to Predict: Outcomes are unpredictable. Think Many Small Actions The Butterfly Effect Health Care, Education and Research
29 We yearn for frictionless, technological solutions. But people talking to people is still the way that norms and standards change. Health Care, Education and Research
30 Adaptive Leadership: A Management Theory (Heifetz) Problem contexts vary Technical Challenges Expertise enables you to do outstanding work using your know-how and procedures and design of your organization
31 Adaptive Leadership: Problem contexts vary Adaptive Challenges demand a response outside your current toolkit or repertoire; Gap between goals and operational capacity that cannot be closed by existing expertise and procedures
32 Adaptive Leadership: Closing the Gap Understanding that problems often have both technical and adaptive challenges Avoiding treating adaptive challenge as technical Mobilizing people s hearts and minds to operate differently Helping staff and managers develop new capacity Being able, both individually and collectively, to take on the gradual but meaningful process of adaptation.
33 33



34 Consider Type of Problem, Match Solution to Problem Technical Change Adaptive Work Health Care, Education and Research

35

36

37 Conventional Change Model Complexity-informed Change Model Health Care, Education and Research
38 Complexity Science Tells Us.. 1. Relationships matter 2. Look for bright spots or positive deviants 3. Foster self-organization 4. Embrace uncertainty Health Care, Education and Research
39 Adaptive Leadership Model Tells Us.. 1. Solution needs to match the problem a. Technical problems need technical solutions b. Adaptive problems need adaptive solutions 2. Many (most?) problems are both technical AND adaptive a. Need both technical and adaptive solution 3. If solution fails, consider what s missing Health Care, Education and Research
40 Regional Strategies Face-to-face visits to rural/regional/frontier clinics Menus not Mandates Telemedicine lunch and learns Ownership, not buy-in
41 Ownership vs. Buy-in * Ownership Invited to participate at start of project Participation a choice Helped design change Debated alternatives, contributed to decisionmaking Buy-in Invited to participate well into project Participation mandated Asked to accept change designed by others Unaware of alternatives discussed, not part of any decision-making *Henri Lipmanowicz, co-founder Plexus Institute, co-developer, Liberating Structures
42 Strategies (cont.): Billings (aka the Mothership): Attended daily/weekly huddles Attended existing meetings Foster ownership, not buy in Train-the-trainer approach Bottom up: team creates protocols Look for bright spots or positive deviants and spread the word Health Care, Education and Research
43 Strategies (cont.) Join a national campaign Explain why Solicit input from EVERYONE Engage patients Health Care, Education and Research
44 Why train everyone? Team-based care: every discipline plays a role in HTN management Patient part of team Project ownership (vs. buy-in)

45 RESULTS
46 Percent with most recent bp < 130/80 Complicated HTN Patients with DM or CKD Billings Clinic Comparator Q Q4 Q Q2 Q3 Q4 Q Q2 Q3 Q4 Q Q2 Time Period
47 Percent with Most Recent BP < 140/90 Billings Clinic: All Patients < 85 years Billings Clinic Comparator Q Q4 Q Q2 Q3 Q4 Q Q2 Q3 Q4 Q Q2 Time Period
48 Percent of Patients with most recent BP < 140/90 Stillwater Billings Clinic: All Patients 85 (p=0.004) Billings Clinic y = x Comparator Q Q4 Q Q2 Q3 Q4 Q Q2 Q3 Q4 Q Q2 Quarter
49 Percent of Patients with ALL BPs < 140/90 Billings Clinic: All HTN Patients 85 (p<0.001) Year
50 Percent of Patients with most recent BP < 140/90 Stillwater Billings Clinic: All Patients 85 (p<.001) Year
51 Summary 1. Examining problem/issue through lens of complexity science, including recognizing health system as a Complex Adaptive System, facilitated focus on attributes and design of appropriate interventions. 2. Applying the Adaptive Leadership Model helped us match appropriate problems (technical/adaptive) with appropriate solutions (technical/adaptive). 3. Sensemaking: opportunities for teams to talk, discuss, debate ANY TOPIC will result in stronger, more cohesive teams. 4. Spread through self-organization more effective than through centralized approach. 5. Importance of fostering ownership versus persuading buy-in.


52 Questions? Elizabeth Ciemins:
53 How Well Are We Monitoring Blood Pressure? 94% have a documented BP measurement within the past 12 months 1348 patients do not Rates for annual monitoring vary between practice teams o 7 Practice Groups scored 95% o 8 Practice Groups scored between 91-94% o The remaining Pratice Groups were charaterized by lower volumes of HTN Patients and their scores were more variable - ranging from 30%-89%
54 How Does BP Monitoring Vary Across Care Teams? Group HTN Patients Percent w/o BP Patients w/o BP Marinette Family Practice 59 0% 0 Howard Internal Medicine % 40 Sheboygan Family Practice 301 3% 10 Luxemburg Family Practice % 59 St Marys Internal Medicine % 128 East De Pere Family Practice % 137 East DePere Internal Medicine % 68 East Mason Internal Medicine % 143 Howard Family Practice % 104 East Mason Family Practice 891 6% 53 Pulaski Family Practice 757 6% 47 Allouez Internal Medicine % 143 Oconto Family Practice 466 8% 39 Ashwaubenon Family Practice % 143 West De Pere Family Practice % 119 Oconto Internal Medicine % 44 St Marys Geriatrics % 61 Plymouth Family Practice 54 28% 15 East DePere Geriatrics 10 70% 7 Compliance Rates 95% or better 91-94% 30-89%
55 How Well Are We MANAGING BLOOD PRESSURE? Prevea s rate of achieving target blood pressures is already better than the national average of 53.5% The goal of the AMGA s Measure Up Pressure Down initiative is to reach a goal of 80% patients managed to their therapeutic target Patients with diabetes or chronic kidney disease, BP < 130/80 All other patients, BP < 140/90 Of those HTN patients with BP measurement within the year, 30% (6,025) had a measurement indicating they are ABOVE therapeutic target.
56 How We Got HERE Automated messaging to identify and notify patients due for recommended care Replaced episodic care with coordinated, long-term care through adoption of the Patient Centered Medical Home Model and NCQA Accreditation for all Primary Care locations o 18 onsite Care Managers 56
57 Never Settle For Better than National Average Hypertensive patients who received automated communication messages were significantly more likely to have both a chronic carerelated visit and a systolic blood pressure reading recorded in the 1 EMR (odds ratio=3.18, 95% confidence interval ) 76% of Hypertensive patients cared for under the medical home model improved or were at therapeutic target after 12 months vs 52% who were cared for under the traditional delivery system Despite this, blood pressure control and compliance outcome measures have remained static for over 18 months 1 Ashok Rai, Paul Prichard, Richard Hodach, and Ted Courtemanche. Population Health Management. August 2011, 14(4): doi: /pop
58 The 60 Day Challenge 4 Pilot sites o 8000 Hypertensive patients Re-examine delivery system and revise current protocols o o o o Extreme variation persisted care managers could not articulate workflow in response to an elevated blood pressure reading Some departments rechecked blood pressure at the visit, others did not No standard for follow up care - Some had a follow up at 2 weeks, some at 4, others none at all No standard for documenting the second reading, if it was done at all. Update educational material on healthy lifestyle behaviors, smoking cessation, increased physical activity, reduced dietary salt, and stress management Address barriers to access and patient s non-adherence to treatment Find solutions to insufficient access to healthful foods and physical activity 58
59 The 60 Day Challenge Redesigned standards that are easy to follow and quick to implement o During rooming, if patient s blood pressure is > 140/90 or >130/80 for patient with chronic conditions, Care Manager will add to Chief Complaint o Physician will repeat blood pressure o Follow up Care Manager visit scheduled for 2 weeks if no changes to medications o Follow up Care Manager visit scheduled for 4 weeks if changes to medications made o Care Manager will take blood pressure and pulse at follow up visit and route encounter to physician o Physician will provide directives based on reading, follow up instruction and route back to Care Manager 59

60 Transparency Monitor the degree of process compliance and rate at which therapeutic BP goals are achieved Results analyzed for individual providers, provider groups, and program average and are compared to performance targets Incorporating results into group communications increases familiarity with guidelines and professional accountability for performance Visibility to peak performers (best practice indicator) and low performers allows us to learn from others 60

61 Registries Registries include gaps in care created based on appointment date, provider, care manager assignment to target specific subpopulations for more intensive follow-up, such as assignment to a care manager, specialist referral/coordination of care, and selfmanagement education 61

62 Management on the Individual Patient Level BP measurements for a patient over time are summarized on each patient s record in graphic and list format is helpful to review in conjunction with counseling a patient towards a therapeutic goal Patients not at treatment goal or with new/modified prescribed medication are seen within 30 days In the event that a patient is a no show, a care manager can identify that event and contact patient to re-engage them 62
63 Routine Blood Pressure Measurement 100.0% 99.4% 98.0% 96.0% 95.9% 95.6% 96.4% 94.0% Baseline T % 90.0% 88.0% Pilot Clinic 1 Pilot Clinic 2 Pilot Clinic 3 Pilot Clinic 4 63

64 Blood Pressure Control <140/90 90% 80.8% 80% 70% 68.1% 75.3% 65.9% 60% 50% 40% Baseline T60 30% 20% 10% 0% Pilot Clinic 1 Pilot Clinic 2 Pilot Clinic 3 Pilot Clinic 4 64
65 Next Steps Onboarding non-treating departments Address physician resistance to allow Care Managers to own major parts of process Develop similar model for sites without Care Manager Test and retest. Refine process as needed Analyze results frequently. What did we expect vs what we observed 65
66 Questions? Thank You. Ashok Rai, MD President and Chief Executive Officer Prevea Health
Prevea Health Automates Population Health Management and Improves Health Outcomes
 CASE STUDY Prevea Health Prevea Health Automates Population Health Management and Improves Health Outcomes After adopting the patient-centered medical home care delivery model to improve the health and
CASE STUDY Prevea Health Prevea Health Automates Population Health Management and Improves Health Outcomes After adopting the patient-centered medical home care delivery model to improve the health and
CREATING A NATIONAL CAMPAIGN TO IMPROVE HYPERTENSION CONTROL. Improving chronic care: It takes a team
 F I N D I N G S T R E N G T H Improving chronic care: It takes a team CREATING A NATIONAL CAMPAIGN TO IMPROVE HYPERTENSION CONTROL Jerry Penso, MD, MBA, chief medical and quality officer American Medical
F I N D I N G S T R E N G T H Improving chronic care: It takes a team CREATING A NATIONAL CAMPAIGN TO IMPROVE HYPERTENSION CONTROL Jerry Penso, MD, MBA, chief medical and quality officer American Medical
Improving Diabetes Care in 75 Minutes. Moderator: Jerry Penso, M.D., M.B.A., President & CEO, AMGA
 Improving Diabetes Care in 75 Minutes Moderator: Jerry Penso, M.D., M.B.A., President & CEO, AMGA SESSION OBJECTIVES 1. Identify specific tactics that health care delivery systems can implement to improve
Improving Diabetes Care in 75 Minutes Moderator: Jerry Penso, M.D., M.B.A., President & CEO, AMGA SESSION OBJECTIVES 1. Identify specific tactics that health care delivery systems can implement to improve
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc.
 Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
A M.A.P. for improving blood pressure: Application within the QIN-QIO community
 A M.A.P. for improving blood pressure: Application within the QIN-QIO community Donna Daniel, PhD Director, Improving Health Outcomes Strategies American Medical Association Michael Rakotz, MD Director,
A M.A.P. for improving blood pressure: Application within the QIN-QIO community Donna Daniel, PhD Director, Improving Health Outcomes Strategies American Medical Association Michael Rakotz, MD Director,
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Primary Care Redesign Updates to DFM
 Primary Care Redesign Updates to DFM Overview of Care Model Package 2 Care of the Complicated Patient March 5, 2014 Dr. Rich Welnick Susan Marks, Director of Population Health Lori Hauschild, Clinic Operations
Primary Care Redesign Updates to DFM Overview of Care Model Package 2 Care of the Complicated Patient March 5, 2014 Dr. Rich Welnick Susan Marks, Director of Population Health Lori Hauschild, Clinic Operations
Team Care Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc.
 2008 Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc. November 12-14, 2008, Scottsdale, AZ Great Falls Clinic, LLP Great Falls, Montana Team Care
2008 Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc. November 12-14, 2008, Scottsdale, AZ Great Falls Clinic, LLP Great Falls, Montana Team Care
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Hypertension Management Improvement Automated Cuffs Implementation and Training
 Hypertension Management Improvement Automated Cuffs Implementation and Training Rae Ann Williams, MD, FACP Regional Assistant Medical Director Jo McLaughlin, MA, BSN, RN Director Nursing and Nutrition
Hypertension Management Improvement Automated Cuffs Implementation and Training Rae Ann Williams, MD, FACP Regional Assistant Medical Director Jo McLaughlin, MA, BSN, RN Director Nursing and Nutrition
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
HealthPartners and the Triple Aim. IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners
 HealthPartners and the Triple Aim IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners HealthPartners Not for profit, consumer governed Integrated care and financing
HealthPartners and the Triple Aim IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners HealthPartners Not for profit, consumer governed Integrated care and financing
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
EHR Innovations for Improving Hypertension Challenge Winners and Phase 2
 EHR Innovations for Improving Hypertension Challenge Winners and Phase 2 January 23, 2015 Agenda Million Hearts Blood Pressure Protocols Hilary Wall, MPH Green Spring Internal Medicine Holly Dahlman, MD,
EHR Innovations for Improving Hypertension Challenge Winners and Phase 2 January 23, 2015 Agenda Million Hearts Blood Pressure Protocols Hilary Wall, MPH Green Spring Internal Medicine Holly Dahlman, MD,
Evaluation of the West Virginia Cardiovascular Health Program (CVHP)
") Evaluation of the West Virginia Cardiovascular Health Program (CVHP) 2013 Background/Introduction: The West Virginia Cardiovascular Health Program (CVHP) and the West Virginia University Office of Health
Evaluation of the West Virginia Cardiovascular Health Program (CVHP) 2013 Background/Introduction: The West Virginia Cardiovascular Health Program (CVHP) and the West Virginia University Office of Health
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Hypertension Efforts Mercy Medical Group, Inc. November 5, 2016 Alan R. Ertle, MD, MPH, MBA Chief Medical Officer
 Hypertension Efforts Mercy Medical Group, Inc November 5, 2016 Alan R. Ertle, MD, MPH, MBA Chief Medical Officer Mercy Medical Group, Inc. 420+ provider multi-specialty group in the Sacramento metro area
Hypertension Efforts Mercy Medical Group, Inc November 5, 2016 Alan R. Ertle, MD, MPH, MBA Chief Medical Officer Mercy Medical Group, Inc. 420+ provider multi-specialty group in the Sacramento metro area
Journey in managing practice variation in Diabetes and Hypertension (Part 2/2)
") Journey in managing practice variation in Diabetes and Hypertension (Part 2/2) For Part 1 of this presentation, go to http://rightcare.berkeley.edu/sacramento-university-of-best-practices Parag Agnihotri,
Journey in managing practice variation in Diabetes and Hypertension (Part 2/2) For Part 1 of this presentation, go to http://rightcare.berkeley.edu/sacramento-university-of-best-practices Parag Agnihotri,
Managing Patients with Multiple Chronic Conditions
 Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
Change is Good: You Go First
 Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009 Foundation s goals Support organizations that: Strengthen
Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009 Foundation s goals Support organizations that: Strengthen
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Presentation Outline
 Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Target BP: First Year in Review
 Target BP: First Year in Review Teaching Clinic Point of View R. Bruce Hanlin, M.D. Care Coordination Institute and American Medical Association The MAP Hypertension Control QI Project R. Bruce Hanlin,
Target BP: First Year in Review Teaching Clinic Point of View R. Bruce Hanlin, M.D. Care Coordination Institute and American Medical Association The MAP Hypertension Control QI Project R. Bruce Hanlin,
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework
 The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
The Four Pillars of Ambulatory Care Management - Transforming the Ambulatory Operational Framework Institution: The Emory Clinic, Inc. Author/Co-author(s): Donald I. Brunn, Chief Operating Officer, The
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Improving Effectiveness in the PCMH. Shawn Stinson, MD FACP
 Improving Effectiveness in the PCMH Shawn Stinson, MD FACP 1 Overview Introduction to BCBSSC PCMH program Must haves for successful outcomes in a primary care practice Agreement on evidence based practices
Improving Effectiveness in the PCMH Shawn Stinson, MD FACP 1 Overview Introduction to BCBSSC PCMH program Must haves for successful outcomes in a primary care practice Agreement on evidence based practices
HIMSS Davies Enterprise Application --- COVER PAGE ---
 HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
Hypertension Control: Self-Measured Blood Pressure Monitoring
 Source: Flickr Hypertension Control: Self-Measured Blood Pressure Monitoring High blood pressure, or hypertension (HTN), is a major risk factor for heart disease, stroke and kidney disease. It affects
Source: Flickr Hypertension Control: Self-Measured Blood Pressure Monitoring High blood pressure, or hypertension (HTN), is a major risk factor for heart disease, stroke and kidney disease. It affects
Midmark IQvitals Zone Technology: Connecting Vitals Acquisition within the Point of Care Ecosystem
 Midmark White Paper Midmark IQvitals Zone Technology: Connecting Vitals Acquisition within the Point of Care Ecosystem Introduction This is Part Two of Midmark s Point of Care Ecosystem Series that examines
Midmark White Paper Midmark IQvitals Zone Technology: Connecting Vitals Acquisition within the Point of Care Ecosystem Introduction This is Part Two of Midmark s Point of Care Ecosystem Series that examines
NCQA PCSP 2016 Quality Measurement and Improvement Worksheet
 PURPOSE: This worksheet is to help practices organize the measures and QI activities that are required by PCSP 6, Element C. Refer to PCSP 6, Elements A C for additional information. NOTE: Practices are
PURPOSE: This worksheet is to help practices organize the measures and QI activities that are required by PCSP 6, Element C. Refer to PCSP 6, Elements A C for additional information. NOTE: Practices are
Complex Patient Care Redesign: ThedaCare Innovation. Gregory Long, MD Chief Medical Officer
 Complex Patient Care Redesign: ThedaCare Innovation Gregory Long, MD Chief Medical Officer ThedaCare Northeastern Wisconsin An Integrated Community Health System; >7000 employees Primary service area of
Complex Patient Care Redesign: ThedaCare Innovation Gregory Long, MD Chief Medical Officer ThedaCare Northeastern Wisconsin An Integrated Community Health System; >7000 employees Primary service area of
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Blood Pressure Control: Path to the Million Hearts Award. Jessicca Moore, MSN, FNP Associate Clinical Director Nurit Licht, MD, Chief Medical Officer
 Blood Pressure Control: Path to the Million Hearts Award Jessicca Moore, MSN, FNP Associate Clinical Director Nurit Licht, MD, Chief Medical Officer The Million Hearts Program Started in 2011, a national
Blood Pressure Control: Path to the Million Hearts Award Jessicca Moore, MSN, FNP Associate Clinical Director Nurit Licht, MD, Chief Medical Officer The Million Hearts Program Started in 2011, a national
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Alabama Department of Public Health Bureau of Health Promotion and Chronic Disease Hypertension Control Initiatives Request for Proposals FY 2018
 I. Overview and Purpose Alabama Department of Public Health Bureau of Health Promotion and Chronic Disease Hypertension Control Initiatives Request for Proposals FY 2018 One in three American adults, about
I. Overview and Purpose Alabama Department of Public Health Bureau of Health Promotion and Chronic Disease Hypertension Control Initiatives Request for Proposals FY 2018 One in three American adults, about
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Alexander Valley Healthcare Hypertension Blood Pressure Control Redwood Community Health Coalition Promising Practice
 AVH Promising Practice Hypertension Control 08/23/18 PG. 1 Alexander Valley Healthcare Hypertension Blood Pressure Control Redwood Community Health Coalition Promising Practice PROMISING PRACTICE OVERVIEW
AVH Promising Practice Hypertension Control 08/23/18 PG. 1 Alexander Valley Healthcare Hypertension Blood Pressure Control Redwood Community Health Coalition Promising Practice PROMISING PRACTICE OVERVIEW
EVOLENT HEALTH, LLC. Asthma Program Description 2018
 EVOLENT HEALTH, LLC Asthma Program Description 2018 1 Evolent Health Asthma Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Asthma Program Description 2018 1 Evolent Health Asthma Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
PHASE Preventing Heart Attacks & Strokes Everyday
 PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Webinar Housekeeping 1. Lines are muted. 2. Chat in questions or unmute your line by pressing *7 to ask a question
PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Webinar Housekeeping 1. Lines are muted. 2. Chat in questions or unmute your line by pressing *7 to ask a question
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations
 ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
IMPACT OF RN HYPERTENSION PROTOCOL
 1 IMPACT OF RN HYPERTENSION PROTOCOL Joyce Cheung, RN, Marie Kuzmack, RN Orange County Hypertension Team Kaiser Permanente, Orange County Joyce.m.cheung@kp.org and marie-aline.z.kuzmack@kp.org Cell phone:
1 IMPACT OF RN HYPERTENSION PROTOCOL Joyce Cheung, RN, Marie Kuzmack, RN Orange County Hypertension Team Kaiser Permanente, Orange County Joyce.m.cheung@kp.org and marie-aline.z.kuzmack@kp.org Cell phone:
An Integrative Health Home Pilot
 An Integrative Health Home Pilot Kellye Hudson, DNP, PMHNP-BC Director of Nursing Helen Ross McNabb Center December 2016 TN Healthcare Innovation Initiative Primary Care Transformation Launched in 2013
An Integrative Health Home Pilot Kellye Hudson, DNP, PMHNP-BC Director of Nursing Helen Ross McNabb Center December 2016 TN Healthcare Innovation Initiative Primary Care Transformation Launched in 2013
WPS Integrated Care Management Improving health, one member at a time
 WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
Working with GPs to help deliver the NHS Health Checks Programme
 Working with GPs to help deliver the NHS Health Checks Programme Dr Matt Kearney GP Castlefields, Runcorn National Clinical Advisor Public Health England and NHS England Why do we need GP engagement? 1.
Working with GPs to help deliver the NHS Health Checks Programme Dr Matt Kearney GP Castlefields, Runcorn National Clinical Advisor Public Health England and NHS England Why do we need GP engagement? 1.
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
Joy At Work - BellinHealth and HealthPartners
 Joy At Work - BellinHealth and HealthPartners Restoring Joy in Practice through Team Based Care IHI December 2016 James Jerzak M.D. Kathy Kerscher Bellin Health Green Bay, Wisconsin 1 Agenda Crisis Emerging
Joy At Work - BellinHealth and HealthPartners Restoring Joy in Practice through Team Based Care IHI December 2016 James Jerzak M.D. Kathy Kerscher Bellin Health Green Bay, Wisconsin 1 Agenda Crisis Emerging
Kaiser Permanente Northern California Large Scale Hypertension Control Program
 Kaiser Permanente Northern California Large Scale Hypertension Control Program Marc Jaffe, MD Clinical Leader, Kaiser Northern California Cardiovascular Risk Reduction Program Clinical Leader, Kaiser National
Kaiser Permanente Northern California Large Scale Hypertension Control Program Marc Jaffe, MD Clinical Leader, Kaiser Northern California Cardiovascular Risk Reduction Program Clinical Leader, Kaiser National
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Healthy Patients/Engaged Patients
 Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Healthy Patients/Engaged Patients PRESENTED BY: SUE LING LEE RN, MPA KENNETH FELDMAN, PHD, FACHE CHCANYS 2015 STATEWIDE CONFERENCE AND CLINICAL FORUM FACULTY DISCLOSURE It is the policy of the AAFP that
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
IT Enabled Quality Measurement IOM Dec 2012
 IT Enabled Quality Measurement IOM Dec 2012 Kevin Larsen MD, FACP Medical Director of Meaningful Use, ONC December 6, 2012 Our National Quality Strategy Aims Better Health for the Population Better Care
IT Enabled Quality Measurement IOM Dec 2012 Kevin Larsen MD, FACP Medical Director of Meaningful Use, ONC December 6, 2012 Our National Quality Strategy Aims Better Health for the Population Better Care
Objectives. Prototyping tools and resources. The M.A.P. framework. Hypertension statistics. Barriers to success
 The M.A.P. Framework and Hypertension Control Linda Murakami, RN, BSN, MSHA Senior Program Manager, Quality Improvement Objectives Understand the M.A.P. Framework Learn the importance of accurate blood
The M.A.P. Framework and Hypertension Control Linda Murakami, RN, BSN, MSHA Senior Program Manager, Quality Improvement Objectives Understand the M.A.P. Framework Learn the importance of accurate blood
Patient Centered Medical Home 2011 Standards
 PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
Disease State Management Clinics: A Pharmacist Perspective
 Disease State Management Clinics: A Pharmacist Perspective Eva Berrios Colon, Pharm.D, MPH, BCPS Associate Professor, Touro College of Pharmacy Email: evb9001@nyp.org 5/12/11 The Brooklyn Hospital Center
Disease State Management Clinics: A Pharmacist Perspective Eva Berrios Colon, Pharm.D, MPH, BCPS Associate Professor, Touro College of Pharmacy Email: evb9001@nyp.org 5/12/11 The Brooklyn Hospital Center
Research Opportunities to Improve Hypertension Control
 Research Opportunities to Improve Hypertension Control Barry L. Carter, Pharm.D., FCCP, FAHA, FASH The Patrick E. Keefe Professor in Pharmacy Department of Pharmacy Practice and Science College of Pharmacy
Research Opportunities to Improve Hypertension Control Barry L. Carter, Pharm.D., FCCP, FAHA, FASH The Patrick E. Keefe Professor in Pharmacy Department of Pharmacy Practice and Science College of Pharmacy
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
Member Satisfaction: Moving the Needle
 Member Satisfaction: Moving the Needle Webinar for IPAs and Providers January 4, 2017 Accreditation of Medi-Cal and L.A. Care Covered. L.A. Care QI Webinar 1 Agenda Topic Introduction CG-CAHPS Recommended
Member Satisfaction: Moving the Needle Webinar for IPAs and Providers January 4, 2017 Accreditation of Medi-Cal and L.A. Care Covered. L.A. Care QI Webinar 1 Agenda Topic Introduction CG-CAHPS Recommended
Primer on Quality Improvement and Integrating MOC into my Practice. Erik Stratman, MD
 Primer on Quality Improvement and Integrating MOC into my Practice Erik Stratman, MD PRIMER ON QUALITY IMPROVEMENT AND INTEGRATING MOC INTO MY PRACTICE DISCLOSURE I, Erik Stratman, MD FAAD have no relevant
Primer on Quality Improvement and Integrating MOC into my Practice Erik Stratman, MD PRIMER ON QUALITY IMPROVEMENT AND INTEGRATING MOC INTO MY PRACTICE DISCLOSURE I, Erik Stratman, MD FAAD have no relevant
CROSSWALK FOR AADE S DIABETES EDUCATION ACCREDITATION PROGRAM
 Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
COMPASS Workflow & Core Elements
 COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
COMPASS Workflow & Core Elements Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services,
Passport Advantage (HMO SNP) Model of Care Training (Providers)
 Model of Care Training (Providers)") Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Passport Advantage (HMO SNP) Model of Care Training (Providers) 2018 Passport Advantage (HMO SNP) is an HMO Special Needs plan with a Medicare contract and an agreement with the Kentucky Department for
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Edmonds Family Medicine Clinic
 Add your company logo here 2008-20 Best Practices in Managing Hypertension Sponsored by AMGA and Daiichi Sankyo. Wrap-Up Meeting November 18-20, 20 San Diego, CA Edmonds Family Medicine Clinic Controlling
Add your company logo here 2008-20 Best Practices in Managing Hypertension Sponsored by AMGA and Daiichi Sankyo. Wrap-Up Meeting November 18-20, 20 San Diego, CA Edmonds Family Medicine Clinic Controlling
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
New Models of Care: Diabetes and the Triple Aim
 Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
University of Utah PGY-1 Pharmacy Practice Primary Care: Ambulatory I & II Rotation Salt Lake City, Utah
 University of Utah PGY-1 Pharmacy Practice Primary Care: Ambulatory I & II Rotation Salt Lake City, Utah Primary Preceptors: Redwood Health Center Macheala Jacquez, PharmD, BCACP; Megan Lowe, PharmD, BCACP;
University of Utah PGY-1 Pharmacy Practice Primary Care: Ambulatory I & II Rotation Salt Lake City, Utah Primary Preceptors: Redwood Health Center Macheala Jacquez, PharmD, BCACP; Megan Lowe, PharmD, BCACP;
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Innovation. Successful Outpatient Management of Kidney Stone Disease. Provider HealthEast Care System
 Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
Rapid-Learning Healthcare Systems
 Rapid-Learning Healthcare Systems in silico Research and Best Practice Adoption in Promoting Rapid Learning Sharon Levine MD July 11, 2012 NIH Training Institute for Dissemination and Implementation Rapid-Learning
Rapid-Learning Healthcare Systems in silico Research and Best Practice Adoption in Promoting Rapid Learning Sharon Levine MD July 11, 2012 NIH Training Institute for Dissemination and Implementation Rapid-Learning
Obesity and corporate America: one Wisconsin employer s innovative approach
 Focus On... Obesity Obesity and corporate America: one Wisconsin employer s innovative approach Amy Helwig, MD, MS; Dennis Schultz, MD, MSPH; Len Quadracci, MD Introduction The United States has an obesity
Focus On... Obesity Obesity and corporate America: one Wisconsin employer s innovative approach Amy Helwig, MD, MS; Dennis Schultz, MD, MSPH; Len Quadracci, MD Introduction The United States has an obesity
Progress Notes Extra
 Medical Staff Office Cathy Crabtree : (937) 734-1212 Deb Charles: (937) 734-1229 Josie Hall: (937-734-1216 Tanya Webber: (937) 734-1213 September 2013 Progress Notes Extra Fall General Medical Staff Meeting
Medical Staff Office Cathy Crabtree : (937) 734-1212 Deb Charles: (937) 734-1229 Josie Hall: (937-734-1216 Tanya Webber: (937) 734-1213 September 2013 Progress Notes Extra Fall General Medical Staff Meeting
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE
 ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
ACHIEVING POPULATION HEALTH: THE POWER OF TEAM BASED CARE JAMES JERZAK M.D. KATHY KERSCHER, MBA BELLIN HEALTH GREEN BAY WI IHI NATIONAL FORUM 12 13 2017 2 GREEN BAY, WISCONSIN Agenda Why Team-Based Care
Iowa Healthcare Collaborative Care Coordination Workshop April 20, 2017
 Iowa Healthcare Collaborative Care Coordination Workshop April 20, 2017 Intended Audience Physicians, nurse managers, critical care nurses, staff nurses, pharmacists, health coaches, care coordinators,
Iowa Healthcare Collaborative Care Coordination Workshop April 20, 2017 Intended Audience Physicians, nurse managers, critical care nurses, staff nurses, pharmacists, health coaches, care coordinators,
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
2017 QUALITY PLAN WORK PLAN. Kaiser Permanente of Washington 2017 Quality Work Plan
 Kaiser Permanente of Washington 2017 Quality Work Plan 1 Achieve 2017 Quality Goals: Improve population health, the quality, safety and satisfaction of the customer experience while improving affordability
Kaiser Permanente of Washington 2017 Quality Work Plan 1 Achieve 2017 Quality Goals: Improve population health, the quality, safety and satisfaction of the customer experience while improving affordability
Managing Your Patient Population: How do you measure up?
 Managing Your Patient Population: How do you measure up? Paul M. Palevsky, M.D. Chief, Renal Section VA Pittsburgh Healthcare System Professor of Medicine University of Pittsburgh School of Medicine Ben
Managing Your Patient Population: How do you measure up? Paul M. Palevsky, M.D. Chief, Renal Section VA Pittsburgh Healthcare System Professor of Medicine University of Pittsburgh School of Medicine Ben
Driving Advanced Care Planning
 Driving Advanced Care Planning Palliation model in Post-acute, Long Term Care Laura Seleen RN System Long Term Care Clinical Specialist Essentia Health St. Mary s 1027 Washington Avenue Detroit Lakes,
Driving Advanced Care Planning Palliation model in Post-acute, Long Term Care Laura Seleen RN System Long Term Care Clinical Specialist Essentia Health St. Mary s 1027 Washington Avenue Detroit Lakes,
Blending Behavioral Health and Primary Care. Applying the Model. Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist
 Blending Behavioral Health and Primary Care Applying the Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Overview Introducing the Model to Patients Key Components
Blending Behavioral Health and Primary Care Applying the Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Overview Introducing the Model to Patients Key Components
Menu Item: Population Management
 Cover Page Menu Item: Population Management Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Cover Page Menu Item: Population Management Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration
 The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration January 26, 2012 1 Session Overview Partners in Innovation and Service
The UNC Health Care System & BlueCross BlueShield of North Carolina Model Medical Practice: A Blueprint for Successful Collaboration January 26, 2012 1 Session Overview Partners in Innovation and Service
NURSING (MN) Nursing (MN) 1
 Nursing (MN) 1") Nursing (MN) 1 NURSING (MN) MN501: Advanced Nursing Roles This course explores skills and strategies essential to successful advanced nursing role implementation. Analysis of existing and emerging roles
Nursing (MN) 1 NURSING (MN) MN501: Advanced Nursing Roles This course explores skills and strategies essential to successful advanced nursing role implementation. Analysis of existing and emerging roles
The Role of Medication Management in a Patient-Centered Medical Home
 The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
The Role of Medication Management in a Patient-Centered Medical Home David W. Moen, MD Medical Director Care Model Innovation Fairview Health Services Disclosures The faculty reported the following financial
EVOLENT HEALTH, LLC. Asthma Program Description 2017
 EVOLENT HEALTH, LLC Asthma Program Description 2017 1 Evolent Health Asthma Program Description 2017 Table of Contents Section Page Number I. Introduction.. 3 II. Program Scope 3 III. Program Goals 4 IV.
EVOLENT HEALTH, LLC Asthma Program Description 2017 1 Evolent Health Asthma Program Description 2017 Table of Contents Section Page Number I. Introduction.. 3 II. Program Scope 3 III. Program Goals 4 IV.
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating