How to conduct second line assessments. Barry Beiles-Clinical Director VASM
|
|
|
- Andrew Harvey
- 5 years ago
- Views:
Transcription
1 How to conduct second line assessments Barry Beiles-Clinical Director VASM

2 ASM receives notification of death Surgical case form sent to surgeon for completion by paper or Fellows Interface Completed paper or electronic surgical case form returned to ASM and de-identified Surgical case form sent for first-line assessment by paper or Fellows Interface Yes Is a second-line assessment required? No Case closed Second-line assessment Feedback to surgeon Has an appeal been lodged on the second-line assessment? Yes No Case closed
3
4
5 Principles of a SLA Summarize history and course of treatment Comment on quality of record keeping Provide constructive comments on how the outcome might have been improved, specifically responding to the FLA comments and adverse events/areas of concern- ACONS Suggest changes in future practice Not too brief
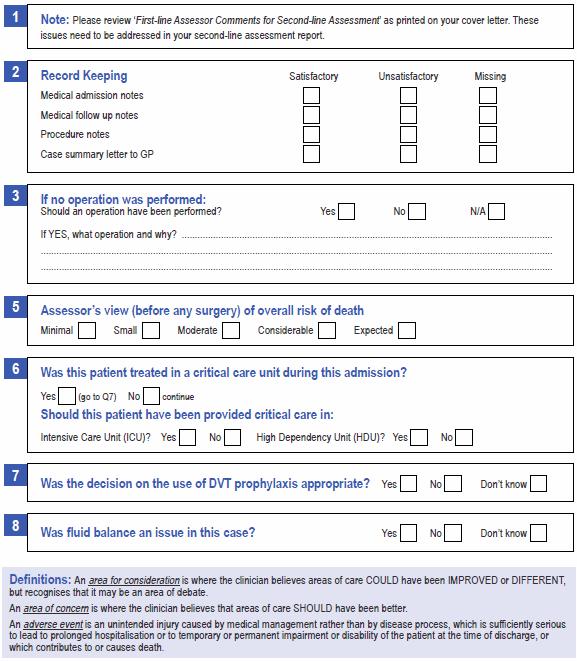
6 Management issues classification An area for CONSIDERATION is where the clinician believes areas of care COULD have been IMPROVED or DIFFERENT, but recognizes that it may be an area of debate. An area of CONCERN is where the clinician believes that areas of care SHOULD have been better. An ADVERSE EVENT is an unintended injury caused by medical management rather than by disease process, which is sufficiently serious to lead to prolonged hospitalization or to temporary or permanent impairment or disability of the patient at the time of discharge, or which contributes to or causes death.
7 Substandard SLA report
8 Suitable SLA report Summary This is the case of an 82 year old, multi morbid patient, admitted on 16 October after a delay at home, with a 7-10 day history of increasing abdominal pain, and lethargy with nausea and anorexia. Her co-morbidities included Congestive heart failure, cardiomyopathy, respiratory disease on CPAP, Chronic Kidney disease, on Warfarin, digoxin and other medications. She had an INR of 10 on 16 Oct and a serum digoxin in the toxic range at 1.3. A diagnosis of acute pancreatitis and sepsis was made on biochemistry and clinical grounds. This was supported by CT. She deteriorated in the emergency department, and sepsis was considered after a MET call. She was moved to the ICU where a central line was considered, but the Right carotid artery inadvertently cannulated. She was then operated upon the morning after admission- 17 October - with removal of the catheter, thrombectomy and vein patch without problem. She rallied and then deteriorated again, with both clinical and biochemical worsening. She was considered for ERCP with stunting and this and US were performed on 18 Oct. She improved biochemically but continued to deteriorate and after discussion with the family active treatment was withdrawn and she was declared dead at 1800 on 20 Oct. The cause of death was felt to be multiorgan failure secondary to ascending cholangitis. A post mortem examination was not performed. Surgical Case Form This was completed by the consultant, who stated concern at the ICU complication, but felt the outcome to be not preventable. First Line Assessment The first line assessor felt there were issues with the pre op investigations and treatment of sepsis, the nature of the carotid artery injury and its treatment, the procedure details and the timing and date of surgery. Also the definitive causes of sepsis and death.
9 Suitable SLA report part 2 Case Notes These were adequate for the report but in general poor with illegibility, missed timings, incompletely completed forms, especially with dates. There was also no apparent decision making notes re the ERCP, indeed the US report indicated a normal calibre bile duct, no obstruction and no calculi in the gallbladder, making the decision for this difficult to understand, though improvement in the LFTs afterwards was dramatic. There is only a brief note that US was used for the attempted CV cannulation and it is not apparent the grade of doctor performing it. The notes of the operations on the carotid and ERCP are adequate. The timing of the US and the time of theatre for ERCP are not apparent, though it appears to me the US report was not seen prior to theatre, certainly there is no comment in the record. There was no record of blood cultures taken in the record. Medication charts are (as seems universal) not completed as per standards. The concern of timings by the First Line Assessor was due to error by reporting surgeon. The concern re diagnosis of ascending cholangitis is that it was apparently made by inference and there is no record of specimens. This is probably of little importance in outcome but is in clinical completeness. It is noted that the clinical coding sheets have multiple alterations. Comments 1. The complication of IJV cannulation of arterial injury is well recognised though with the use of US should be considered unusual, and may represent lack of experience or supervision. 2. The initial surgery was proper, adequate and timely. 3. The decision for ERCP was not well documented. 4. The diagnosis of ascending cholangitis was not verified, in the absence of obstruction. 5. The pancreatitis aetiology not documented or explained, and not mentioned as part of cause of death. 6. The letter to the GP failed to mention the arterial injury and its management. 7. Attention to detail in completion of documents poor. 8. De-identification process makes it difficult to assess grade of the note maker. 9. Given the serious nature of the presentation, and the significant co-morbidities, the pancreatitis/sepsis would most likely have resulted in death. Recommendations 1. The need for full completion of documentation be emphasised to Fellows and Trainees. 2. De-identification to leave status of the person making of notes. 3. That notes of the decision making process be emphasised as part of a complete clinical record.
10 Concordance between the treating surgeon and the first-line assessor (4,905) Clinical management issues Postoperative care Timing of operation Grade/experience of surgeon operating Grade/experience of surgeon deciding Choice of operation Decision to operate at all Intraoperative/technical management Preoperative management/preparation Fluid balance HDU care benefit if not received ICU care benefit if not received Risk of death 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
11 Concordance between the treating surgeon and the second-line assessor (1,200) Clinical management issues Postoperative care Timing of operation Grade/experience of surgeon operating Grade/experience of surgeon deciding Choice of operation Decision to operate at all Intraoperative/technical management Preoperative management/preparation Fluid balance HDU care benefit if not received ICU care benefit if not received Risk of death 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
12 Concordance between the first-line assessor and the second-line assessor (1,200) Clinical management issues Postoperative care Timing of operation Grade/experience of surgeon operating Grade/experience of surgeon deciding Choice of operation Decision to operate at all Intraoperative/technical management Preoperative management/preparation Fluid balance HDU care benefit if not received ICU care benefit if not received Risk of death 0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
13 Validation study 16 (5%) of 329 SLA randomly selected for validation Speciality Second-line cases available for review Cases selected n (%) Cardiothoracic 41 2 (5%) General Surgery (2%) Neurosurgery 32 2 (6%) Obs & Gynae 1 1 (100%) Ophthalmology 1 1 (100%) Orthopaedics 40 2 (5%) Otolaryngology 5 1 (20%) Plastic Surgery 1 1 (100%) Urology 18 1 (6%) Vascular 23 2 (9%) Total (5%)
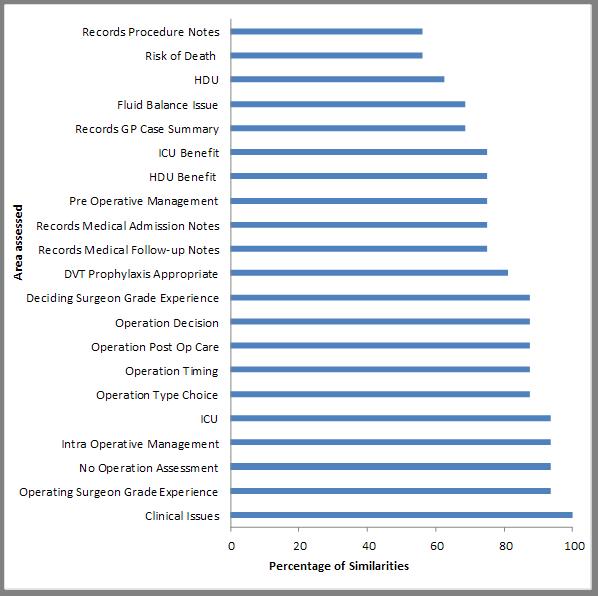
14 Similarities by field
15 Validation Conclusions Good agreement between surgeon and FLA Moderate agreement between surgeon and SLA Poor agreement between FLA and SLA 85% agreement between SLA assessors The process is robust Will repeat this exercise every 2 years
16 Trends in clinical management issues over time 80% 60% Issues (%) 40% 20% 0% None Consideration Concern Adverse event Clinical management issues
17 Frequency of clinical management issues across the audit series ( ) Clinical management issues Current audit period Frequency (%) Operation inappropriate 1,025 (27%) Delay in definitive treatment 970 (26%) Preoperative care issues 500 (13%) Management or protocol issues 478 (13%) Postoperative care issues 370 (10%) General complications after surgery 83 (2%) Communication or poor documentation 177 (5%) Adverse events 91 (2%) Critical care issues 48 (1%) Septicaemia and wound 28 (1%) Transfer problems 19 (<1%)
18 Conclusion Assessors should realize the importance of their contribution to ASM Their assessment is vital to the educational process and should be comprehensive and focused on lessons and not be overly harshly judgmental Total anonymity is assured This is a unique audit-independent and peerreviewed.
Lessons learned from VASM cases. Barry Beiles Clinical Director VASM
 Lessons learned from VASM cases Barry Beiles Clinical Director VASM Operative Mortality by specialty (n=5,184) Specialty Frequency (%) General surgery 2,073 (40.0%) Orthopaedic surgery 1,044 (20.1%) Neurosurgery
Lessons learned from VASM cases Barry Beiles Clinical Director VASM Operative Mortality by specialty (n=5,184) Specialty Frequency (%) General surgery 2,073 (40.0%) Orthopaedic surgery 1,044 (20.1%) Neurosurgery
Australian and New Zealand College of Anaesthetists (ANZCA) Statement on the Handover Responsibilities of the Anaesthetist
 Statement on the Handover Responsibilities of the Anaesthetist") PS53 2013 Australian and New Zealand College of Anaesthetists (ANZCA) Statement on the Handover Responsibilities of the Anaesthetist 1. INTRODUCTION The major responsibility of the anaesthetist during
PS53 2013 Australian and New Zealand College of Anaesthetists (ANZCA) Statement on the Handover Responsibilities of the Anaesthetist 1. INTRODUCTION The major responsibility of the anaesthetist during
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Australian and New Zealand Audit of Surgical Mortality. Royal Australasian College of Surgeons
 Australian and New Zealand Audit of Surgical Mortality Royal Australasian College of Surgeons National Report 2012 CONTACT Royal Australasian College of Surgeons Australia and New Zealand Audit of Surgical
Australian and New Zealand Audit of Surgical Mortality Royal Australasian College of Surgeons National Report 2012 CONTACT Royal Australasian College of Surgeons Australia and New Zealand Audit of Surgical
Guidelines on the Handover of Responsibility of an. Anaesthesiologist
 The Hong Kong College of s Page 1 of 5 Guidelines on the Handover of Responsibility of an Version Effective Date 1 MAY 1994 (reviewed Feb 2002) 2 JUL 2013 Document No. HKCA P12 v2 Prepared by College Guidelines
The Hong Kong College of s Page 1 of 5 Guidelines on the Handover of Responsibility of an Version Effective Date 1 MAY 1994 (reviewed Feb 2002) 2 JUL 2013 Document No. HKCA P12 v2 Prepared by College Guidelines
ANNUAL REPORT Tasmanian Audit of Surgical Mortality
 ROYAL AUSTRALASIAN COLLEGE OF SURGEONS ANNUAL REPORT Tasmanian Audit of Surgical Mortality Contact Lisa Lynch Project Manager TASM 2 Gore Street South Hobart Tasmania 7004 Mr Rob Bohmer Chairman TASM 2
ROYAL AUSTRALASIAN COLLEGE OF SURGEONS ANNUAL REPORT Tasmanian Audit of Surgical Mortality Contact Lisa Lynch Project Manager TASM 2 Gore Street South Hobart Tasmania 7004 Mr Rob Bohmer Chairman TASM 2
St. James s Hospital, Dublin.
 Position Senior House Officer in Anaesthesia Organisational Area Department of Anaesthesia, St. James s Hospital. Closing Date Sunday the 9 th July 2018 SACC Directorate. The Surgery, Anaesthesia and Critical
Position Senior House Officer in Anaesthesia Organisational Area Department of Anaesthesia, St. James s Hospital. Closing Date Sunday the 9 th July 2018 SACC Directorate. The Surgery, Anaesthesia and Critical
Supervision of Residents/Chain of Command
 Supervision of Residents/Chain of Command Creighton University Department of Surgery Residency Training Program Chain of command for Surgery residents at CUMC PGY1: The intern on call covers the two general
Supervision of Residents/Chain of Command Creighton University Department of Surgery Residency Training Program Chain of command for Surgery residents at CUMC PGY1: The intern on call covers the two general
Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath
 Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath Up to 25,000 surgical deaths per year 5-10% of surgical cases are high risk 79% of deaths occur in the high risk group Overall
Carol J. Peden BSC, MB ChB, MD, FRCA, FFICM, MPH Royal United Hospital, Bath Up to 25,000 surgical deaths per year 5-10% of surgical cases are high risk 79% of deaths occur in the high risk group Overall
NCEPOD Recommendations that remain current
 NCEPOD Recommendations that remain current All recommendations from subsequent NCEPOD reports are considered current (Last updated 2014) 1989 The information systems, particularly clinical information
NCEPOD Recommendations that remain current All recommendations from subsequent NCEPOD reports are considered current (Last updated 2014) 1989 The information systems, particularly clinical information
1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure
 ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
ADMISSION & DISCHARGE POLICY FOR ADULT CRITICAL CARE SERVICES CONTENTS Page 1 Introduction 2 2 Definitions of levels of care 3 3 Common principles 4 4 Admission criteria 5 5 Referral procedure 5-7 5.1
7 NON-ELECTIVE SURGERY IN THE NHS
 Recommendations Debate whether, in the light of changes to the pattern of junior doctors working, non-essential surgery can take place during extended hours. 7 NON-ELECTIVE SURGERY IN THE NHS Ensure that
Recommendations Debate whether, in the light of changes to the pattern of junior doctors working, non-essential surgery can take place during extended hours. 7 NON-ELECTIVE SURGERY IN THE NHS Ensure that
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
GENERAL PROGRAM GOALS AND OBJECTIVES
 BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
A Total Colectomy is the surgical removal of the entire colon (last part of the intestine/gut). It does not involve the removal of the rectum.
. It does not involve the removal of the rectum.") Total Colectomy What is a Total Colectomy? A Total Colectomy is the surgical removal of the entire colon (last part of the intestine/gut). It does not involve the removal of the rectum. Before an ileostomy
Total Colectomy What is a Total Colectomy? A Total Colectomy is the surgical removal of the entire colon (last part of the intestine/gut). It does not involve the removal of the rectum. Before an ileostomy
Standard of Care for MTC inpatients
 Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
St. James s Hospital, Dublin.
 Position Fellowship in Anaesthesia for Advanced Airway Management Assignment Department of Anaesthesia, St. James s Hospital. Commencement Date Monday, 09 th July, 2018. Purpose of the Post The St. James
Position Fellowship in Anaesthesia for Advanced Airway Management Assignment Department of Anaesthesia, St. James s Hospital. Commencement Date Monday, 09 th July, 2018. Purpose of the Post The St. James
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY
 SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY Residency Years Included: PGY1_X_ PGY2_X_ PGY3 PGY4 PGY5 Fellow I. The Clinical Mission of the Division of Cardiothoracic Surgery
SURGICAL RESIDENT CURRICULUM FOR THE DIVISION OF CARDIOTHORACIC SURGERY Residency Years Included: PGY1_X_ PGY2_X_ PGY3 PGY4 PGY5 Fellow I. The Clinical Mission of the Division of Cardiothoracic Surgery
Effective Tools to Prevent and Manage Adverse Events
 Effective Tools to Prevent and Manage Adverse Events Based on Office of Inspector General Adverse Events Report Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com Objectives Upon completion
Effective Tools to Prevent and Manage Adverse Events Based on Office of Inspector General Adverse Events Report Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com Objectives Upon completion
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES
 GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES") PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
PGY-7 (2 nd Year) GOALS AND OBJECTIVES VANDERBILT UNIVERSITY MEDICAL CENTER VASCULAR SURGERY PROGRAM ROTATION-BASED GOALS AND OBJECTIVES A. VANDERBILT HOSPITAL VASCULAR SURGERY SERVICE COMPETENCY BASED
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
The deteriorating patient recognition and management Dave Story
 The deteriorating patient recognition and management Dave Story MBBS, MD, BMedSci, FANZCA Professor and Foundation Chair of Anaesthesia Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU)
The deteriorating patient recognition and management Dave Story MBBS, MD, BMedSci, FANZCA Professor and Foundation Chair of Anaesthesia Head of Anaesthesia, Perioperative and Pain Medicine Unit (APPMU)
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Surgical Oncology II: R5 Tuesday, February 02, 2016
 Stanford University General Surgery Residency Program Surgical Oncology II Goals and Objectives for Residents: R-5 Rotation Director: Ralph Greco, MD Description The Surgical Oncology II rotation at Stanford
Stanford University General Surgery Residency Program Surgical Oncology II Goals and Objectives for Residents: R-5 Rotation Director: Ralph Greco, MD Description The Surgical Oncology II rotation at Stanford
West Middlesex Junior Doctors Handbook in Colorectal Surgery
 West Middlesex Junior Doctors Handbook in Colorectal Surgery Page 1 of 10 INTRODUCTION Welcome to surgery and to the colorectal team! This guide is meant to be just that, a guide and has been principally
West Middlesex Junior Doctors Handbook in Colorectal Surgery Page 1 of 10 INTRODUCTION Welcome to surgery and to the colorectal team! This guide is meant to be just that, a guide and has been principally
It s not just Obs and Swabs!
 It s not just Obs and Swabs! Developing a pre-operative assessment service in a complex tertiary referral centre a multidisciplinary approach Emma McCone- Lead Pre op Sister Healthcare at its very best
It s not just Obs and Swabs! Developing a pre-operative assessment service in a complex tertiary referral centre a multidisciplinary approach Emma McCone- Lead Pre op Sister Healthcare at its very best
SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER. Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow
 SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow I. Clinical Mission of the North Carolina Jaycee Burn Center The clinical
SURGICAL RESIDENT CURRICULUM FOR NORTH CAROLINA JAYCEE BURN CENTER Residency years included: PGY1 _X PGY2 PGY3 _X PGY4 PGY5 Fellow I. Clinical Mission of the North Carolina Jaycee Burn Center The clinical
LOMA LINDA UNIVERSITY MEDICAL CENTER SURGERY SERVICE RULES AND REGULATIONS
 I. ORGANIZATION LOMA LINDA UNIVERSITY MEDICAL CENTER SURGERY SERVICE RULES AND REGULATIONS A. Membership: 1. The Surgery Service shall be made up of Physicians and Dentists who perform surgical procedures
I. ORGANIZATION LOMA LINDA UNIVERSITY MEDICAL CENTER SURGERY SERVICE RULES AND REGULATIONS A. Membership: 1. The Surgery Service shall be made up of Physicians and Dentists who perform surgical procedures
Introductions. Welcome to the APAC Global Trigger Tool Session. Dr Carol Haraden IHI Gillian Robb CMDHB. Carol Haraden.
 Welcome to the APAC Global Trigger Tool Session Dr Carol Haraden IHI Gillian Robb CMDHB Carol Haraden Introductions Gillian Robb Outline for this session Introduction to the Global Trigger Tool What is
Welcome to the APAC Global Trigger Tool Session Dr Carol Haraden IHI Gillian Robb CMDHB Carol Haraden Introductions Gillian Robb Outline for this session Introduction to the Global Trigger Tool What is
Advanced Roles and Workforce Planning. Sara Dalby SFA, ANP, SCP Associate Lecturer Winston Churchill Fellow
 Advanced Roles and Workforce Planning Sara Dalby SFA, ANP, SCP Associate Lecturer Winston Churchill Fellow Confusion of Advanced Roles Clinical Support Worker (CSW) Nurse Practitioner (NP) Physicians Associate
Advanced Roles and Workforce Planning Sara Dalby SFA, ANP, SCP Associate Lecturer Winston Churchill Fellow Confusion of Advanced Roles Clinical Support Worker (CSW) Nurse Practitioner (NP) Physicians Associate
Sepsis guidance implementation advice for adults
 Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
NHS HIGHLAND. Significant Event Report
 ` NHS HIGHLAND Significant Event Report Report to - Quality & Patient Safety Raigmore Management Team of Findings from Significant Event Review Meeting QPS040 26/10/2011 1.0 Outline of Significant Event
` NHS HIGHLAND Significant Event Report Report to - Quality & Patient Safety Raigmore Management Team of Findings from Significant Event Review Meeting QPS040 26/10/2011 1.0 Outline of Significant Event
SPC Case Studies Answers
 SPC Case Studies Answers Ref: JC Benneyan, RC Lloyd, PE Plsek, Statistical process control as a tool for research and healthcare improvement, Qual. Saf. Health Care 2003; 12:458 464 doi:10.1136/qhc.12.6.458
SPC Case Studies Answers Ref: JC Benneyan, RC Lloyd, PE Plsek, Statistical process control as a tool for research and healthcare improvement, Qual. Saf. Health Care 2003; 12:458 464 doi:10.1136/qhc.12.6.458
Center for the Future of Surgery
 Center for the Future of Surgery Center for the Future of Surgery 9500 Gilman Drive, La Jolla, CA 92093 858.246.1004 cfs.ucsd.edu Redefining Surgery At UC San Diego Center for the Future of Surgery, our
Center for the Future of Surgery Center for the Future of Surgery 9500 Gilman Drive, La Jolla, CA 92093 858.246.1004 cfs.ucsd.edu Redefining Surgery At UC San Diego Center for the Future of Surgery, our
Provide Safe and Effective Medicines Management in Primary Care
 Primary Drivers Secondary Drivers Aim Safe and reliable prescribing, monitoring and administration of high risk medications that require systematic monitoring Implement systems for reliable prescribing
Primary Drivers Secondary Drivers Aim Safe and reliable prescribing, monitoring and administration of high risk medications that require systematic monitoring Implement systems for reliable prescribing
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart
 Observation Chart") CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
CLINICAL PROTOCOL National Early Warning Score (NEWS) Observation Chart November 2014 1 Document Profile Type i.e. Strategy, Policy, Procedure, Guideline, Protocol Title Category i.e. organisational, clinical,
Inguinal hernia repair integrated care pathway (ICP)
") Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
Name Ward Hosp no DOB Affix patient label Inguinal hernia repair integrated care pathway (ICP) Inclusion criteria Patients undergoing inguinal hernia repair aged under 3 months corrected gestational age
Abdomino-perineal Resection/Excision of the Rectum
 Abdomino-perineal Resection/Excision of the Rectum What is an Abdomino-perineal Resection/Excision of Rectum? An Abdomino-perineal Resection/Excision of Rectum is the surgical removal of part of the large
Abdomino-perineal Resection/Excision of the Rectum What is an Abdomino-perineal Resection/Excision of Rectum? An Abdomino-perineal Resection/Excision of Rectum is the surgical removal of part of the large
TRANSPLANT SURGERY ROTATION (PGY4) A. Medical Knowledge
 A. Medical Knowledge") TRANSPLANT SURGERY ROTATION (PGY4) A. Medical Knowledge The resident will achieve a detailed knowledge of the evaluation and treatment of a variety of disease processes as related to transplantation. Objectives:
TRANSPLANT SURGERY ROTATION (PGY4) A. Medical Knowledge The resident will achieve a detailed knowledge of the evaluation and treatment of a variety of disease processes as related to transplantation. Objectives:
Update on the Maryland Patient Safety Program
 Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Third Annual Maryland Patient
Update on the Maryland Patient Safety Program Department of Heath and Mental Hygiene Wendy Kronmiller, Director Renee Webster, Assistant Director Anne Jones RN, Nurse Surveyor Third Annual Maryland Patient
Critical Care What Makes this so Difficult
 Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Stanford Multiorgan Transplant Surgery: R-1 Tuesday, February 02, 2016
 Stanford University General Surgery Residency Program Abdominal Transplant Surgery Goals and Objectives for Residents: R-1 Rotation Director: Carlos Esquivel, M.D., Ph.D. Description The Abdominal Transplant
Stanford University General Surgery Residency Program Abdominal Transplant Surgery Goals and Objectives for Residents: R-1 Rotation Director: Carlos Esquivel, M.D., Ph.D. Description The Abdominal Transplant
Medical Necessity verses Medical Decision Making. Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC
 Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
The Primary Care Trigger Tool: Practical Guidance
 The Primary Care Trigger Tool: Practical Guidance Reviewing clinical records to detect and reduce patient safety incidents Index Content Page Introduction 2 What is a Trigger Tool Review? 2 What types
The Primary Care Trigger Tool: Practical Guidance Reviewing clinical records to detect and reduce patient safety incidents Index Content Page Introduction 2 What is a Trigger Tool Review? 2 What types
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
IHI Open School Advanced Case Study October 14, 2010 Clemson University
 IHI Open School Advanced Case Study October 14, 2010 Clemson University Catherine Simmons 1, Drew Sargent 1, and Kate Wright 1 Public Health Science Hallie Bagnal 2 and Megan Hohenberger 2 Biological Science
IHI Open School Advanced Case Study October 14, 2010 Clemson University Catherine Simmons 1, Drew Sargent 1, and Kate Wright 1 Public Health Science Hallie Bagnal 2 and Megan Hohenberger 2 Biological Science
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children
 Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Delivering Quality and Value. Focus on: Cholecystectomy A Guide for Commissioners
 Delivering Quality and Value Focus on: Cholecystectomy A Guide for Commissioners Introduction This document will help commissioners and local health communities improve the quality and value of care for
Delivering Quality and Value Focus on: Cholecystectomy A Guide for Commissioners Introduction This document will help commissioners and local health communities improve the quality and value of care for
Coroner's Corner - Inquest into the death of Gwendoline Mead
 Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
Coroner's Corner - Inquest into the death of Gwendoline Mead Date of Findings: 22 June 2017 Coroner: Ainslie Kirkegaard Inquest Place: Brisbane Date of Death: 1 March 2015 Factual Summary: Gwendoline Mead
Introduction, function of ICU. Lorx András
 Introduction, function of ICU Lorx András AOANEANE_1A Intensive Therapy and Anaesthesiology AOVANE104_1A Anaesthesiology and Intensive Therapy Compulsory Elective Credit: 2 Lectures, practices Exam: MCQ
Introduction, function of ICU Lorx András AOANEANE_1A Intensive Therapy and Anaesthesiology AOVANE104_1A Anaesthesiology and Intensive Therapy Compulsory Elective Credit: 2 Lectures, practices Exam: MCQ
(1) Ambulatory surgical center--a facility licensed under Texas Health and Safety Code, Chapter 243.
 Ambulatory surgical center--a facility licensed under Texas Health and Safety Code, Chapter 243.") RULE 200.1 Definitions The following words and terms, when used in this chapter, shall have the following meanings, unless the context clearly indicates otherwise. (1) Ambulatory surgical center--a facility
RULE 200.1 Definitions The following words and terms, when used in this chapter, shall have the following meanings, unless the context clearly indicates otherwise. (1) Ambulatory surgical center--a facility
Developing the role of the Physician Associates in Hospitals
 Developing the role of the Physician Associates in Hospitals Dr Natalie King FRCP Surrey and Sussex Healthcare NHS Trust KSS School of Physician Associates Faculty of Physician Associates at the Royal
Developing the role of the Physician Associates in Hospitals Dr Natalie King FRCP Surrey and Sussex Healthcare NHS Trust KSS School of Physician Associates Faculty of Physician Associates at the Royal
Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence
 Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence Adam P. Johnson MD, MPH, Anisha Kshetrapal MD, Harold Hsu MD, Randi Altmark RN, BSN, Herbert E Cohn MD, FACS, Scott
Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence Adam P. Johnson MD, MPH, Anisha Kshetrapal MD, Harold Hsu MD, Randi Altmark RN, BSN, Herbert E Cohn MD, FACS, Scott
ICU. Rotation Goals & Objectives for Urology Residents
 THE UNIVERSITY OF BRITISH COLUMBIA Department of Urologic Sciences Faculty of Medicine Gordon & Leslie Diamond Health Care Centre Level 6, 2775 Laurel Street Vancouver, BC, Canada V5Z 1M9 Tel: (604) 875-4301
THE UNIVERSITY OF BRITISH COLUMBIA Department of Urologic Sciences Faculty of Medicine Gordon & Leslie Diamond Health Care Centre Level 6, 2775 Laurel Street Vancouver, BC, Canada V5Z 1M9 Tel: (604) 875-4301
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
9/29/2017. Enhanced Recovery After Surgery at the University of Virginia Medical Center. Disclosures. Objectives. None
 Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Enhanced Recovery After Surgery at the University of Virginia Medical Center Bethany Sarosiek, RN, MSN, MPH, CNL University of Virginia Health System Charlottesville, VA ErasRN@virginia.edu Disclosures
Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey
 Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey We want you to nominate the most important topics for future research in anaesthesia and perioperative care. We are therefore asking
Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey We want you to nominate the most important topics for future research in anaesthesia and perioperative care. We are therefore asking
Competency Assessment for Non Medical Prescribing of Blood and Blood Components
 Competency Assessment for Non Medical Prescribing of Blood and Blood Components Name of Candidate (please print). Ward/Department:... Band/Job Title:.. Professional Registration Number Date initial in-house
Competency Assessment for Non Medical Prescribing of Blood and Blood Components Name of Candidate (please print). Ward/Department:... Band/Job Title:.. Professional Registration Number Date initial in-house
SACRAL NERVE STIMULATION (NEUROMODULATION)
") SACRAL NERVE STIMULATION (NEUROMODULATION) Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association
SACRAL NERVE STIMULATION (NEUROMODULATION) Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association
Independent investigation into the death of Mr Jeffrey Rookes a prisoner at HMP Erlestoke on 14 June 2017
 Independent investigation into the death of Mr Jeffrey Rookes a prisoner at HMP Erlestoke on 14 June 2017 Crown copyright 2017 This publication is licensed under the terms of the Open Government Licence
Independent investigation into the death of Mr Jeffrey Rookes a prisoner at HMP Erlestoke on 14 June 2017 Crown copyright 2017 This publication is licensed under the terms of the Open Government Licence
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING
 Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CONSENT FORM UROLOGICAL SURGERY
 CONSENT FORM for UROLOGICAL SURGERY (Designed in compliance with consent form 1) PATIENT AGREEMENT TO INVESTIGATION OR TREATMENT Patient Details or pre-printed label Patient s NHS Number or Hospital number
CONSENT FORM for UROLOGICAL SURGERY (Designed in compliance with consent form 1) PATIENT AGREEMENT TO INVESTIGATION OR TREATMENT Patient Details or pre-printed label Patient s NHS Number or Hospital number
The Scottish Public Services Ombudsman Act 2002
 Scottish Public Services Ombudsman The Scottish Public Services Ombudsman Act 2002 Investigation Report UNDER SECTION 15(1)(a) SPSO 4 Melville Street Edinburgh EH3 7NS Tel 0800 377 7330 SPSO Information
Scottish Public Services Ombudsman The Scottish Public Services Ombudsman Act 2002 Investigation Report UNDER SECTION 15(1)(a) SPSO 4 Melville Street Edinburgh EH3 7NS Tel 0800 377 7330 SPSO Information
Title: Senior Medical Officer Department: Cardiothoracic and Vascular ICU (CVICU) and HDU. Clinical Director, Cardiothoracic and Vascular ICU and HDU
 and HDU. Clinical Director, Cardiothoracic and Vascular ICU and HDU") POSITION DESCRIPTION Position Details: Title: Senior Medical Officer Department: Cardiothoracic and Vascular ICU (CVICU) and HDU Reports to: Location: Clinical Director, Cardiothoracic and Vascular ICU
POSITION DESCRIPTION Position Details: Title: Senior Medical Officer Department: Cardiothoracic and Vascular ICU (CVICU) and HDU Reports to: Location: Clinical Director, Cardiothoracic and Vascular ICU
The ROHNHSFT Experience: Implementing BWCH PEWS
 The ROHNHSFT Experience: Implementing BWCH PEWS Alison Warren Clinical Matron for Children and Young Peoples Services The Royal Orthopaedic Hospital NHS Foundation Trust RGN, RSCN, ENB 415 & 998 PG Cert
The ROHNHSFT Experience: Implementing BWCH PEWS Alison Warren Clinical Matron for Children and Young Peoples Services The Royal Orthopaedic Hospital NHS Foundation Trust RGN, RSCN, ENB 415 & 998 PG Cert
Nurse Led Discharge. Date Approved: 9 th March 2011 Approved by: W&CH Clinical Governance Committee Date for Review: March 2014
 Nurse Led Discharge Specialty: Gynaecology Services Date Approved: 9 th March 2011 Approved by: W&CH Clinical Governance Committee Date for Review: March 2014 ABM UHB Nurse Led Discharge Page 1 of 13 Nurse
Nurse Led Discharge Specialty: Gynaecology Services Date Approved: 9 th March 2011 Approved by: W&CH Clinical Governance Committee Date for Review: March 2014 ABM UHB Nurse Led Discharge Page 1 of 13 Nurse
Reporting Diagnosis Codes in ICD-10
 Reporting Diagnosis Codes in ICD-10 My physician treated a patient for dysphasia secondary to an acute cerebral infarction in the inpatient rehab hospital. Do I need to report two diagnosis codes in ICD-10?
Reporting Diagnosis Codes in ICD-10 My physician treated a patient for dysphasia secondary to an acute cerebral infarction in the inpatient rehab hospital. Do I need to report two diagnosis codes in ICD-10?
Radical cystectomy enhanced recovery plan. Information for patients
 Radical cystectomy enhanced recovery plan Information for patients Your doctor has recommended surgery to remove your bladder (radical cystectomy). This booklet is designed to explain the operation and
Radical cystectomy enhanced recovery plan Information for patients Your doctor has recommended surgery to remove your bladder (radical cystectomy). This booklet is designed to explain the operation and
Ryan O Gowan, MBA, PA-C, FCCM 28 Bourque Road Cumberland, RI 02068
 Ryan O Gowan, MBA, PA-C, FCCM 28 Bourque Road Cumberland, RI 02068 Mission To provide excellent care in a critical care environment and to design and implement tools which maximize the utilization of all
Ryan O Gowan, MBA, PA-C, FCCM 28 Bourque Road Cumberland, RI 02068 Mission To provide excellent care in a critical care environment and to design and implement tools which maximize the utilization of all
Anaesthesia Fellow. Position Description. Department : Department of Anaesthesia & Perioperative Medicine
 Job Title : Anaesthesia Fellow Department : Department of Anaesthesia & Perioperative Medicine Location : Waitemata District Health Board Reporting To : Clinical Director Anaesthesia Direct Reports : Anaesthesia
Job Title : Anaesthesia Fellow Department : Department of Anaesthesia & Perioperative Medicine Location : Waitemata District Health Board Reporting To : Clinical Director Anaesthesia Direct Reports : Anaesthesia
ANTERIOR RESECTION WHAT ARE THE BENEFITS OF HAVING AN ANTERIOR RESECTION?
 WHAT IS AN ANTERIOR RESECTION? ANTERIOR RESECTION This is an operation that is designed to remove part of your lower large bowel and then join the bowel ends back together again. This is called an anastamosis.
WHAT IS AN ANTERIOR RESECTION? ANTERIOR RESECTION This is an operation that is designed to remove part of your lower large bowel and then join the bowel ends back together again. This is called an anastamosis.
Measuring Medication Harm: Advantages of Using a Trigger Tool. Frank Federico Executive Director
 Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
February 2009 [KU 1018] Sub. Code: 4717
![February 2009 [KU 1018] Sub. Code: 4717](/thumbs/79/78949052.jpg "February 2009 [KU 1018] Sub. Code: 4717") February 2009 [KU 1018] Sub. Code: 4717 Second Year Paper II MEDICAL SURGICAL NURSING - I Answer ALL questions. I. Essays: (2x15=30) 1. Mr.Mani 64 yrs old man is admitted with the diagnosis of Benign Prostatic
February 2009 [KU 1018] Sub. Code: 4717 Second Year Paper II MEDICAL SURGICAL NURSING - I Answer ALL questions. I. Essays: (2x15=30) 1. Mr.Mani 64 yrs old man is admitted with the diagnosis of Benign Prostatic
Sec Disconnect Go to End Forward Sec Next Report Go To
 Effective 3/15/04 escription DICTATION SYSTEM FOR INPATIENT HISTORY & PHYSICALS, DISCHARGE SUMMARIES, DELIVERY (NORMAL) NOTES OPERATIVE REPORTS DIAL 3-4000 LISTEN FOR VERBAL PROMPTS. ENTER: First 5 digits
Effective 3/15/04 escription DICTATION SYSTEM FOR INPATIENT HISTORY & PHYSICALS, DISCHARGE SUMMARIES, DELIVERY (NORMAL) NOTES OPERATIVE REPORTS DIAL 3-4000 LISTEN FOR VERBAL PROMPTS. ENTER: First 5 digits
The curriculum is based on achievement of the clinical competencies outlined below:
 ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
ANESTHESIOLOGY CRITICAL CARE MEDICINE FELLOWSHIP Program Goals and Objectives The curriculum is based on achievement of the clinical competencies outlined below: Patient Care Fellows will provide clinical
Simulation to Assess and Improve EHR Safety
 Simulation to Assess and Improve EHR Safety Dr. Jeffrey A. Gold, MD 10/18/17 Disclosures No Commercial Conflicts of Interest Research Funding from AHRQ, AAMC/Donaghue Foundation Patient Safety and EHRs
Simulation to Assess and Improve EHR Safety Dr. Jeffrey A. Gold, MD 10/18/17 Disclosures No Commercial Conflicts of Interest Research Funding from AHRQ, AAMC/Donaghue Foundation Patient Safety and EHRs
E & M Coding. Welcome To The Digital Learning Center. Today s Presentation. Course Faculty. Beyond the Basics. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Community Health Network, Inc. MEDICAL STAFF POLICIES & PROCEDURES
 Community East Community South Community North TITLE: Medical Record Chart Requirements The medical record of care comprises all the data and information about a patient s visit. It functions as both a
Community East Community South Community North TITLE: Medical Record Chart Requirements The medical record of care comprises all the data and information about a patient s visit. It functions as both a
The Royal College of Surgeons of England
 The Royal College of Surgeons of England Guidelines for Clinicians on Medical Records and Notes The Guidelines to Clinical Audit in Surgical Practice issued in June 1995 by The Royal College of Surgeons
The Royal College of Surgeons of England Guidelines for Clinicians on Medical Records and Notes The Guidelines to Clinical Audit in Surgical Practice issued in June 1995 by The Royal College of Surgeons
Domain 5 Cardiothoracic Standards RCoA Accreditation 2017
 1 PRIORITY The Care Pathway 5.4.1.1 The process for preoperative assessment presenting for cardiac and thoracic patients (including thoracic aortic) is defined within the patient pathway. 1 A clinical
1 PRIORITY The Care Pathway 5.4.1.1 The process for preoperative assessment presenting for cardiac and thoracic patients (including thoracic aortic) is defined within the patient pathway. 1 A clinical
Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures
 procedures") Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures I. Medical Knowledge A. Cognitive objectives 1. Know age and size appropriate
Massachusetts Eye and Ear Infirmary CA-3 Rotation in Anesthesiology for Otorhinolaryngologic & Ophthalmolic (ENT) procedures I. Medical Knowledge A. Cognitive objectives 1. Know age and size appropriate
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
ENVIRONMENT Preoperative evaluation clinic. Preoperative evaluation clinic. Preoperative evaluation clinic. clinic. clinic. Preoperative evaluation
 Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
JOHNS HOPKINS HEALTHCARE Physician Guidelines
 Page 1 of 7 ACTION New Procedure Amending Procedure Number: Superseding Procedure Number: Repealing Procedure Number: REFERENCES: AMPT Committee ASA Guidelines CMS Guidelines I. GENERAL ANESTHESIA PROCEDURE:
Page 1 of 7 ACTION New Procedure Amending Procedure Number: Superseding Procedure Number: Repealing Procedure Number: REFERENCES: AMPT Committee ASA Guidelines CMS Guidelines I. GENERAL ANESTHESIA PROCEDURE:
anaesthetic services Chapter 15 Services for neuroanaesthesia and neurocritical care 2014 GUIDELINES FOR THE PROVISION OF ACSA REFERENCES
 Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
Chapter 15 GUIDELINES FOR THE PROVISION OF anaesthetic services ACSA REFERENCES 15.1.1 15.1.2 15.1.3 15.1.4 15.1.5 15.1.8 15.1.9 15.1.11 15.2.1 15.2.9 15.2.13 15.2.17 15.2.18 15.2.19 15.3.2 15.4.2 15.5.1
GUIDELINE FOR STEP-DOWN TRANSFER OF PATIENTS FROM CRITICAL CARE AREAS
 GUIDELINE FOR STEP-DOWN TRANSFER OF PATIENTS FROM CRITICAL CARE AREAS This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the
GUIDELINE FOR STEP-DOWN TRANSFER OF PATIENTS FROM CRITICAL CARE AREAS This guidance does not override the individual responsibility of health professionals to make appropriate decision according to the
INFORMATION FOR PATIENTS
 The British Association of Urological Surgeons 35-43 Lincoln s Inn Fields London WC2A 3PE Phone: Fax: Website: E- mail: +44 (0)20 7869 6950 +44 (0)20 7404 5048 www.baus.org.uk admin@baus.org.uk INFORMATION
The British Association of Urological Surgeons 35-43 Lincoln s Inn Fields London WC2A 3PE Phone: Fax: Website: E- mail: +44 (0)20 7869 6950 +44 (0)20 7404 5048 www.baus.org.uk admin@baus.org.uk INFORMATION
Measuring Harm. Objectives and Overview
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3. Measuring Harm
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
1. Introduction. 1 CMS section
 1. Introduction Anesthesiology is the practice of medicine including, but not limited to, preoperative patient evaluation, anesthetic planning, intraoperative and postoperative care and the management
1. Introduction Anesthesiology is the practice of medicine including, but not limited to, preoperative patient evaluation, anesthetic planning, intraoperative and postoperative care and the management
An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital.
 An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital. Dr L Spooner (CT1 Urology), Mr P Polson (ST4 Urology), Mr I Apakama (Consultant
An audit of the engagement in the Time Out section of the WHO Checklist in Urology Theatres in a district general hospital. Dr L Spooner (CT1 Urology), Mr P Polson (ST4 Urology), Mr I Apakama (Consultant
A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs.
 6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
6. Referral process Key findings A high percentage of patients were referred to critical care by staff in training; 21% of referrals were made by SHOs. Consultant physicians had no knowledge or input into
Abstract. Key words: Documentation, ICU, Classification systems. Masoomeh Najafi (1) Nasrin Rassoulzadeh (2) Maryam Rassouli (3)
 Nasrin Rassoulzadeh (2) Maryam Rassouli (3)") The Evaluation of Compliance of The Records of Nursing Care after Surgery in the Intensive Care Unit of Cardiac Surgery with Clinical Care Classification system Masoomeh Najafi (1) Nasrin Rassoulzadeh
The Evaluation of Compliance of The Records of Nursing Care after Surgery in the Intensive Care Unit of Cardiac Surgery with Clinical Care Classification system Masoomeh Najafi (1) Nasrin Rassoulzadeh
NURSING SCOPE OF PRACTICE POLICY Page 1 of 10 July 2016
 Page 1 of 10 NB: Anaesthetic RN Policy has been incorporated into this policy Policy Applies to: All Mercy Hospital Nursing staff Related Standards: Health Practitioners Competency Assurance Act (HPCA)
Page 1 of 10 NB: Anaesthetic RN Policy has been incorporated into this policy Policy Applies to: All Mercy Hospital Nursing staff Related Standards: Health Practitioners Competency Assurance Act (HPCA)
Health Facility Guidelines
 Health Facility Guidelines Template - Role Delineation Matrix XYZ Hospital, Abu Dhabi Introduction: Role Delineation refers to a level of service that describes the complexity of the clinical activities
Health Facility Guidelines Template - Role Delineation Matrix XYZ Hospital, Abu Dhabi Introduction: Role Delineation refers to a level of service that describes the complexity of the clinical activities
Equivalence Guidance for GMP Domain 1
 Equivalence Guidance for GMP Domain 1 From 1 st August 2011 the new GMC approved curriculum in Intensive Care Medicine (ICM) came into effect. As a result of this new curriculum, all equivalence applications
Equivalence Guidance for GMP Domain 1 From 1 st August 2011 the new GMC approved curriculum in Intensive Care Medicine (ICM) came into effect. As a result of this new curriculum, all equivalence applications
C-GALL PATIENT INFORMATION LEAFLET
 C-GALL PATIENT INFORMATION LEAFLET The purpose of this study is to compare keyhole gall bladder surgery (laparoscopic cholecystectomy) with watchful waiting in people who suffer from pain due to gallstones
C-GALL PATIENT INFORMATION LEAFLET The purpose of this study is to compare keyhole gall bladder surgery (laparoscopic cholecystectomy) with watchful waiting in people who suffer from pain due to gallstones