The Way UP: How Four Cross-Cutting Strategies Can Reduce Harm Across the Board. DFW Tuesday January 9 th, 2018 Barbara DeBaun, RN, MSN, CIC
|
|
|
- Sandra Park
- 5 years ago
- Views:
Transcription


1 The Way UP: How Four Cross-Cutting Strategies Can Reduce Harm Across the Board DFW Tuesday January 9 th, 2018 Barbara DeBaun, RN, MSN, CIC 1

2 A Fresh Approach to Harm Reduction Script Up Soap Up Get Up Wake Up The Way UP 2
3 Polling Question The UP Campaign is: Brand new information for me Something we just started working on Something we have fully executed Something we don t have time for at the moment
4 Questions to Run On How can we better engage front-line caregivers without creating additional burdens? What could introducing a simple, cross-cutting set of practices accomplish with your hospitals? How can you deploy a program like the UP Campaign with your hospitals and strengthen front-line engagement? 4

5 Are Checklists Enough?
6 Why Incorporate UP? Patient safety with UP & checklists together! Checklists have been integrated into many processes (necessary). Have staff become too task- focused? UP enhances critical thinking. UP & checklists create synergy for patient safety.


7 We may be inadvertently reducing the joy in work by adding successive, well evidenced tools that become a growing burden in the work flow of our front-line caregivers. 7

8 8
9 Why the UP Campaign? Increases impact on harm reduction Generates momentum in your organization Focuses support from leadership Engages front line staff connects the dots creates a vision Applies throughout organization Simplifies patient safety implementation Help patients recover faster and with fewer complications Goal: engage front-line staff and leaders and to increase critical thinking skills. 9
10 Can we streamline and simplify, making it easier for front-line staff and still improve safety? 10

11 Objectives Outline the UP Campaign crosscutting interventions Identify essential next steps for WAKE- UP, GET-UP, SOAP-UP and SCRIPT-UP Develop an implementation plan for the UP Campaign 11






12 # 1 Opioid & Sedation Management ADE Failure to Rescue Delirium Falls Airway Safety VTE VAE W A K E - UP 12

13 # 2 Early Progressive Mobility Falls PrU Delirium CAUTI VAE VTE Readmissions Worker Safety G E T - U P 13
14 # 3 Hand Hygiene CDI CAUTI SSI VAE CLABSI Sepsis MDRO S O A P - U P 14






15 #4 Optimize Medications ADE Readmissions Falls CDI CAUTI SSI VAE CLABSI Sepsis MDRO S C R I P T - UP 15
16 FOUNDATIONAL QUESTIONS: 1. Is my patient awake enough to get up? 2. Have I protected my patient from infections? 3. Does my patient need any medication changes? 16
17 # 1 Opioid & Sedation Management ADE FTR Delirium Falls AS VTE VAE W A K E - UP 17
18 Polling Question Have you ever taken care of a patient who appeared to be resting/sleeping comfortably? Yes No

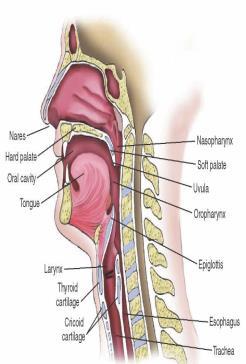
19 Sleep vs Sedation 19
20 Not Just Sedatives and Opioids Antihistamines/anticholinergics Antipsychotics Some antidepressants Anti-emetics Muscle relaxants 20
21 ICU Pitfalls of Sedatives and Analgesics Sedatives and analgesics may contribute to: Increased duration of mechanical ventilation Length of intensive care requirement Impede neurological examination May predispose to delirium Kollef M, et al. Chest. 114: Pandharipande et al. Anesthesiology. 2006;124:
22 Med/Surg Pitfalls of Sedatives and Analgesics Over sedation Transfer to ICU Hypoxic encephalopathy Death 22
23 MUST DO's 23
24 WAKE-UP MUST DO's 1. Establish Expectations 2. Pair POSS & Pain 3. Manage with Multiple Modalities 24
25 MUST DO #1 Establish Expectations Goals of Pain Management: Relieve suffering Achieve early mobilization Reduce hospital length of stay THE GOAL IS NOT ZERO PAIN! 25


26 MUST DO #2 Pair POSS & Pain Just Right! Over Medicated: Hibernating Under Medicated: Not Happy 26
27 No discharge from PACU No additional opioids S = Sleep, easy to arouse Acceptable; no action necessary; may increase opioid dose if needed 1 = Awake and alert Acceptable; no action necessary; may increase opioid dose if needed 2 = Slightly drowsy, easily aroused Acceptable; no action necessary; may increase opioid dose if needed 3 = Frequently drowsy, arousable, drifts off to sleep during conversation Unacceptable; monitor respiratory status and sedation level closely until sedation level is stable at less than 3 and respiratory status is satisfactory; decrease opioid dose 25% to 50% 1 or notify primary 2 or anesthesia provider for orders; consider administering a non-sedating, opioid-sparing nonopioid, such as acetaminophen or a NSAID, if not contraindicated; ask patient to take deep breaths every minutes. 4 = Somnolent, minimal or no response to verbal and physical stimulation Unacceptable; stop opioid; consider administering naloxone 3,4 ; stay with patient, stimulate, and support respiration as indicated by patient status; call Rapid Response Team (Code Blue) if indicated; notify primary 2 or anesthesia provider; monitor respiratory status and sedation level closely until sedation level is stable at less than 3 and respiratory status is satisfactory. *Appropriate action is given in italics at each level of sedation. 1 If opioid analgesic orders or hospital protocol do not include the expectation that the opioid dose will be decreased if a patient is excessively sedated, such orders should be promptly obtained. 2 For example, the physician, nurse practitioner, advanced practice nurse, or physician assistant responsible for the pain management prescription. 3 For adults experiencing respiratory depression give intravenous naloxone very slowly while observing patient response ( titrate to effect ). If sedation and respiratory depression occurs during administration of transdermal fentanyl, remove the patch; if naloxone is necessary, treatment will be needed for a prolonged period, and the typical approach involves a naloxone infusion. Patient must be monitored closely for at least 24 hours after discontinuation of the transdermal fentanyl. 4 Hospital protocols should include the expectation that a nurse will administer naloxone to any patient suspected of having life-threatening opioid-induced sedation and respiratory depression. 1994, Pasero C. Used with permission. As cited in Pasero C, McCaffery M. Pain Assessment and Pharmacologic Management, p St. Louis, Mosby/Elsevier,
28 Two Scales are Better than One for Narcotic and Sedation Administration PAIN ALONE Risk factors may be absent Objective? Dosage based on number or range Patients and families understand the numeric dosing PAIN & POSS Two scales allow for safer dosing High pain scale with high POSS scale no narcotics High pain scale low POSS - med dose 28

29 MUST DO #3 Multi-Modal Pain Management Pharmacological and Non-pharmacological 29
30 MULTIMODAL PAIN MANAGEMENT Combination of opioid and one or more other drugs acetaminophen (Tylenol, others) ibuprofen (Advil, Motrin IB, others) celecoxib (Celebrex) ketamine (Ketalar) gabapentin (Gralise, Neurontin) Non-pharmacological interventions 30
31 CAN WE MANAGE PAIN WITH NON- PHARMACOLOGIC METHODS? What do we do at home? Comfort measures: Pet therapy Warm compresses, blankets Ice packs Extra pillows Aromatherapy Massage Herbal tea Stress ball Music 31
32 DO COMFORT ITEMS HELP? These modalities can: Reduce anxiety Reduce pain Reducing anxiety can reduce pain Non-pharmacologic pain reduction methods reduce the need for pain medications 32
33 POSITIVE RESULTS Pain scores Nausea scores Anxiety scores. All decreased by more than 50% NEXT: Looking to see if opioid usage and opioid ADEs are both decreased. 33
34 WAKE UP Success, Barriers & Help Must Do s 1. Establish Expectations 2. Pair POSS & Pain 3. Manage with Multiple Modalities Next Steps Are you setting pain management expectations ("0" is not the goal) prior to admission? Are you asking about comfort level in addition to pain score? Are you using the Pasero Opioidinduced Sedation Scale (POSS) prior to and after opioid administration? Do you offer multimodal pain management; both pharmacologic and nonpharmacologic modalities?
35 # 2 Early Progressive Mobility Falls PrU Delirium CAUTI VAE VTE Readmissions Worker Safety G E T - U P 35
36 Polling Question In our facility, we do the following for our alert critically ill patients who happen to require ventilation support: Keep them on strict bedrest Try to get them up in a chair Actively assist them to ambulate

37 Pathophysiological changes within 24H of bed rest Image retrieved at: Mobilization of Vulerable Elders in Ontario (MOVE ON) 37

38 What happened to mobility? There is an inherent tension between preventing falls and promoting mobility Growdon, Shorr, Inouye
 27% still dependent in walking 3 months post discharge (Mahoney 1998) 39")
39 Cumulative impact on quality of life New Walking Dependence occurs in 16-59% in older hospitalized patients (Hirsh 1990, Lazarus 1991, Mahoney 1998) 65% of patients had a significant functional mobility decline by day 2 (Hirsh 1990) 27% still dependent in walking 3 months post discharge (Mahoney 1998) 39

40 It s Simple If they came in walking, keep them walking 40

41 Use mobility to accelerate progress When am I going to walk? I walked yesterday. It s better than just being in the chair. I feel better when I am walking. 41
42 What is progressive mobility? Progressive mobility is defined as a series of planned movements in a sequential matter beginning at a patient's current mobility status with goal of returning to his/her baseline (Vollman 2010) Ambulation Dangling Elevate HOB Manual turning PROM AROM CLRT and Prone positioning Upright / leg down position Chair position Vollman, KM. Introduction to Progressive Mobility. Crit Care Nurs. 2010;30(2):
43 TEAMING UP TO MOBILIZE OT PT RN Admin CNA MD RT Family 43
44 MUST DO's 44
45 GET-UP MUST DO S! 1. Walk in, walk during, walk out! 2. Grab and go mobility devices. 3. Three laps a day keeps the nursing home away! 45


46 MUST DO #1 Walk In, Walk During, Walk Out! 46


47 MUST DO #1 Walk In, Walk During, Walk Out! Determine pre admission ambulation status Don t assume a frail appearance means weakness Use Get Up and Go test to assess ambulation skills 47

48 Mobility begins on admission Wood W, et al.(2014) A Mobility Program for an Inpatient Acute Care Medical Unit &Journal_ID=54030&Issue_ID=

49 MUST DO #2 Grab and Go Mobility Devices! Gait Belts in every room* Patients and staff have access to mobility devices Safe mobilization and patient handling training for staff Gait belts are used to help control the patient s center of balance. *with the exception of rooms for behavioral health patients 49

50 MUST DO #3 3 Laps a Day, Keeps the Nursing Home Away! 50
51 Facing the Facts about Mobility Mobility interventions are regularly missed Nursing perceptions Lack of time Ease of omission Belief it is PTs responsibility Survey results Concern for patients level of weakness, pain and fatigue Presence of devices IVs and Urinary Catheters Lack of staff to assist Doherty-King, B Bowers, B. How nurses decide to ambulate hospitalized older adults: development of a conceptual model. Gerontologist Dec:51(6):
52 Tips for Promoting Mobility Order Modifications Delete orders for Bedrest Ad lib Replace with specific orders Times, activities, distance Promote Team Mobility Management Delegation of patient mobility Replace sitters with a mobility aide Rehab and Nursing face-to-face bedside handoffs Document plans and progress on white boards 52
53 GET UP Success, Barriers & Help Must Do s Next Steps 1. Walk in, walk during, walk out! 2. Grab and go mobility devices. 3. Three laps a day keeps the nursing home away! Do you have a mobility team? Do you have a mobility protocol? Have you clearly identified staff that have the capacity to ambulate patients daily? Do your nurses or rehabilitation/physical therapists evaluate each patient s mobility status upon admission? Is mobility equipment readily available for nurses and patients to access? (canes, walkers, lifting and safe patient handling devices, gait belts) Do you have a way to document and 53 monitor daily mobility?

54 # 3 Hand Hygiene CDI CAUTI SSI VAE CLABSI Sepsis MDRO S O A P - U P 54
55 Hand-washing an OLD intervention Since 1847 we have understood that hand hygiene (HH) makes a difference in the spread of infections Dr. Ignaz Semmelweis in Vienna Childbed fever Dr. Lister Operating Room 1980 s concepts of hand hygiene in health care emerged 2002 alcohol based hand rub adopted WHO Global clean hands initiative Yet the average HH compliance is 48% 55

56 We need to get it right! Protect our patients from HAI by performing HH. Promote patient and family engagementgive them permission to speak up for clean hands. Promote patient HH for patients. 56
57 Polling Question In our facility, if a nurse observes another nurse who forgets to perform hand hygiene, s/he will: Likely ignore it Say something to the nurse later on in the shift Speak up immediately to remind the nurse to perform hand hygiene
58 MUST DO's 58
59 SOAP-UP Must Do s - beyond your current plan 1. Prompt Peer Performance 2. Track Quietly and Trend Loudly 3. Drive Drift Down 59

60 MUST DO # 1 Prompt Peer Performance 60


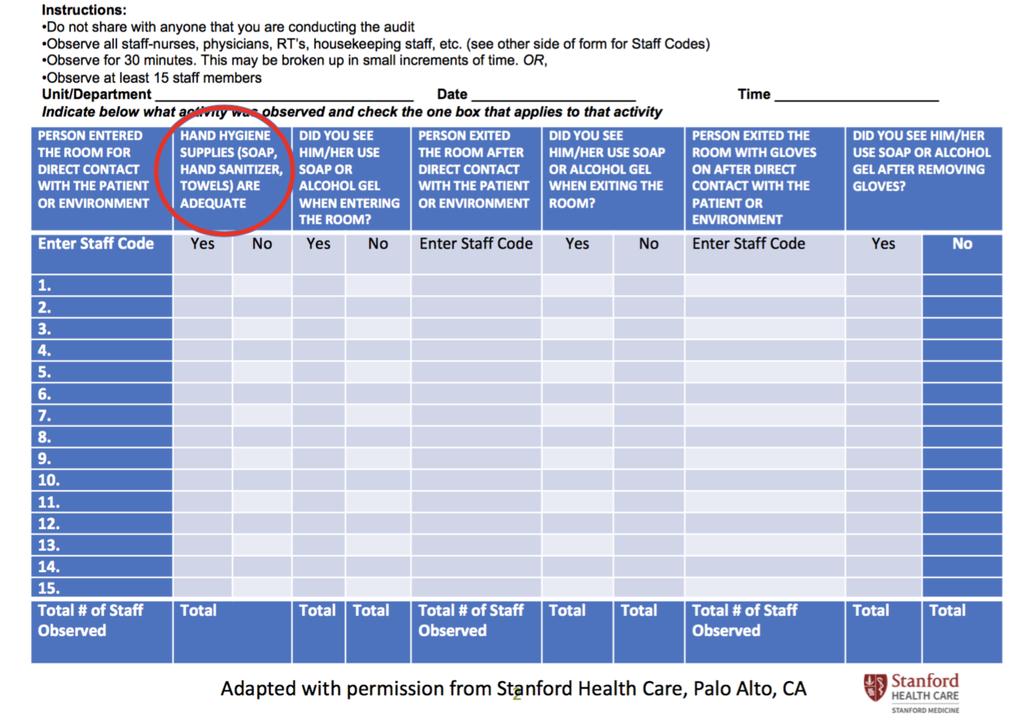
61 MUST DO #2 Track Quietly and Trend Loudly Hand Hygiene vs. Healthcare-Associated Infections 61
62 Track Quietly and Trend Loudly SOAP UP Started New observers trained Scripting education January February March April May June HH Compliance HAI 62

63 MUST DO #3 Drive Drift Down 63
64 The Right Balance Person model System model Important to get the balance right. Both extremes have their pitfalls. 64
65 Shared Accountability 65


66 What Works? Observation and surveillance of hand hygiene is the best way to ensure appropriate compliance. Schedule an unscheduled observation by trained observers. Intervene immediately if a breach in HH is observed. Provide scripts for reminding peers to perform HH. Promote culture of safety. 66
67 SOAP UP Success, Barriers & Help Must Do s 1. Prompt Peer Performance 2. Track Quietly and Trend Loudly 3. Drive Drift Down Next Steps Do you display hand hygiene (HH) compliance results in highly visible places at the department/unit level? Have you implemented scripting to remind other team members to perform HH when it is not observed? Do you have a system in place that holds all team members accountable to the HH expectations?
68 #4 Optimize Medications ADE Readmissions Falls CDI CAUTI SSI VAE CLABSI Sepsis MDRO S C R I P T - UP 68
69 Polling Question In my facility, Antibiotic Stewardship is: Firing on all cylinders Just getting started Gaining traction Not a priority due to resource limitations
70 Why It Matters Adverse drug events are the most common cause of harm (AHRQ) Overuse and inappropriate use of antibiotics is the key cause of antibiotic resistance (CDC) Beers Criteria Medications are linked to poor health outcomes, including confusion, falls, and mortality (Am. Geriatric Society) Risk of ADEs almost doubles with > 5 meds (Bourgeois, Shannon et al, 2010)

71 MUST DO's 71
72 SCRIPT UP- MUST DO s 1. Match the drug to the bug 2. Follow Beers if they're up in years 3. Use appropriate meds -- Less may be more Ask if patient needs any medication changes

73 Must Do #1 Match the Bug to the Drug Implement antibiotic time outs at 48 or 72 hours to de-escalate and modify therapy Verify the presence of a bacterial or fungal infection

74 One Idea Pharmacists focus review on patients with a fluoroquinolone order 48 hours if cultures are back Review 7-10 patients daily ~50% require intervention Antibiotic monitoring form is completed by pharmacists Recommendations made during interdisciplinary rounds or by phone call NCD Pacing Event 2/9/2017


75 Getting Started Decide what antibiotic to target by considering: Potential risk Volume used High cost Set up a review process Monitor your results Spread to other antibiotics when you can
76 Must Do #2: Follow Beers, if they re up in years Anticholinergics Flag, stop and replace medications on the Beers list If needed, switch to a safer agent If not needed, discontinue medication Antispasmodic agents Sleep aids Benzodiazepines NSAIDS Cardiac drugs
77 Medications to avoid in those over 65yrs Anticholinergics Antispasmodic agents Sleep aids Benzodiazepines NSAIDS Cardiac drugs Benadryl, Phenergan, Vistaril Donnatal, Bentyl, Librax, Probanthine Ambien, Luminal, Dalmane, Nembutal Ativan, Valium, Xanax, Librium, Klonopin Advil, Motrin, Aleve Digoxin > 0.125mg/day, Procardia, Catapres
78 Provide Alternatives Drug Class Preferred Alternative Special dosing considerations for the elderly Benzodiazepines - For insomnia: - emphasize sleep hygiene - treat for underlying disrupters - evaluate timing of other medications and alcohol - For chronic anxiety: - consider buspirone or SSRIs or SNIRs - consider psych referral Pain Medications - Risk of fall doubled if used more than 14 days Avoid meperidine


79 Provide Alternatives Drug Class Preferred Alternative Special dosing considerations for the elderly Cardiovascular agents Skeletal muscle relaxants - For HTN alone - ACE inhibitors, betablockers, or calcium channel blockers preferred Most significant risk is orthostatic hypotension Monitor closely and educate patient Slowly increase to full dose Monitor length of use and discontinue as soon as no longer indicated; recommended for short use only Help your physicians by providing guidelines about alternatives and any special dosing or monitoring considerations.

80 Must Do #3 Use appropriate meds -- less may be more Consider shortening med lists, especially PRN medications When adding a med, ask What can I discontinue?

81 Why Less May Be Better There is no set number of medications defining polypharmacy The CDC uses 6 Concerns Increased ADE Increased drug interactions Increased costs Prescribing cascade Associated with Decreased quality of life, mobility and cognition
82 Script UP Success, Barriers & Help Must Do s 1. Match the drug to the bug 2. Follow Beers if they're up in years 3. Use appropriate meds -- Less may be more Ask if patient needs any medication changes Next Steps Have you implemented a time out after hours of antibiotic therapy to re-assess and optimize therapy? Do the staff, providers, and pharmacists have ready access to reminders and alerts to avoid medications on the Beers list for patients over 65 years old? Is there a specific number of medications on a patient s medication list (e.g., 10) that will trigger a review by a pharmacist?

83 Summary & Discussion
84 Reminders Complete the post-webinar Survey Monkey that will be sent to you via Must have participated on the webinar for a minimum of 50 minutes Required to complete survey to earn 1 CE credit CE certificates will be issued to you via within one week
85 Barbara DeBaun, RN, MSN, CIC Improvement Advisor Cynosure Health
HRET-HIIN Roadshow The Way UP. Barb DeBaun, MSN, RN,CIC & Pat Teske, MHA, RN Kentucky State Hospital Association HIIN Roadshow March 15, 2017
 HRET-HIIN Roadshow The Way UP Barb DeBaun, MSN, RN,CIC & Pat Teske, MHA, RN Kentucky State Hospital Association HIIN Roadshow March 15, 2017 1 The Way UP 2 Objectives Outline the three UP Campaign crosscutting
HRET-HIIN Roadshow The Way UP Barb DeBaun, MSN, RN,CIC & Pat Teske, MHA, RN Kentucky State Hospital Association HIIN Roadshow March 15, 2017 1 The Way UP 2 Objectives Outline the three UP Campaign crosscutting
HRET HIIN UP Campaign. Thursday, February 16, :00 a.m. 11:50 a.m. CT
 HRET HIIN UP Campaign Thursday, February 16, 2017 11:00 a.m. 11:50 a.m. CT 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Agenda for Today 11:00-11:10 a.m. Welcome and Introductions
HRET HIIN UP Campaign Thursday, February 16, 2017 11:00 a.m. 11:50 a.m. CT 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Agenda for Today 11:00-11:10 a.m. Welcome and Introductions
Get UP to Drive Harm Down. ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health
 Get UP to Drive Harm Down ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health What is your role in your organization? Quality Leader RN MD Rehab specialist RT Other- please chat in your
Get UP to Drive Harm Down ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health What is your role in your organization? Quality Leader RN MD Rehab specialist RT Other- please chat in your
Raise your game: The UP Campaign. Bruce Spurlock, M.D. Cynosure Health
 Raise your game: The UP Campaign Bruce Spurlock, M.D. Cynosure Health 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Can we streamline & simplify making it easier for front-line staff and still improve safety? 16
Raise your game: The UP Campaign Bruce Spurlock, M.D. Cynosure Health 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Can we streamline & simplify making it easier for front-line staff and still improve safety? 16
HOSPITAL IMPROVEMENT INNOVATION NETWORK (HIIN) Jessica Stultz, Director of Clinical Quality May 23, 2017
 Jessica Stultz, Director of Clinical Quality May 23, 2017") HOSPITAL IMPROVEMENT INNOVATION NETWORK (HIIN) Jessica Stultz, Director of Clinical Quality May 23, 2017 Great things are happening! Hospital milestone 4 achievement Total 91.8% or 67 HIIN hospitals Earn
HOSPITAL IMPROVEMENT INNOVATION NETWORK (HIIN) Jessica Stultz, Director of Clinical Quality May 23, 2017 Great things are happening! Hospital milestone 4 achievement Total 91.8% or 67 HIIN hospitals Earn
South Central HIINergy Partners
 Six states partnering for quality and patient safety through the Hospital Improvement Innovation Network UP Your Game with HIIN! Purpose is a group of six geographically proximal state hospital associations
Six states partnering for quality and patient safety through the Hospital Improvement Innovation Network UP Your Game with HIIN! Purpose is a group of six geographically proximal state hospital associations
Foundation for Healthy Communities NH Partnership for Patients Hospital Improvement & Innovation Network (HIIN) 2.0
 2.0") Foundation for Healthy Communities NH Partnership for Patients Hospital Improvement & Innovation Network (HIIN) 2.0 Hospital NHSN Workshop February 22, 2017 Greg Vasse Anne Diefendorf Our charge is clear:
Foundation for Healthy Communities NH Partnership for Patients Hospital Improvement & Innovation Network (HIIN) 2.0 Hospital NHSN Workshop February 22, 2017 Greg Vasse Anne Diefendorf Our charge is clear:
Let s Join the Movement Towards Movement Using the UP Campaign Strategies to Decrease Falls and other HACs. June 13, 2018
 Let s Join the Movement Towards Movement Using the UP Campaign Strategies to Decrease Falls and other HACs June 13, 2018 1 Agenda Morning Welcome Get UP as a cross cutting strategy to reduce harm 12:00-12:30
Let s Join the Movement Towards Movement Using the UP Campaign Strategies to Decrease Falls and other HACs June 13, 2018 1 Agenda Morning Welcome Get UP as a cross cutting strategy to reduce harm 12:00-12:30
Opioid Sedation Comparison Study
 Opioid Sedation Comparison Study Barbara U. Ochampaugh, RN, BSN, CPAN Level IV; Sandra Lowery, RN, CPAN Level III; Deborah J. Marra, RN, BS, CPAN Level III; and Nancy Salerno RN, MSN Respiratory depression
Opioid Sedation Comparison Study Barbara U. Ochampaugh, RN, BSN, CPAN Level IV; Sandra Lowery, RN, CPAN Level III; Deborah J. Marra, RN, BS, CPAN Level III; and Nancy Salerno RN, MSN Respiratory depression
VAE PROJECT MASTER ACTION PLAN. Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies
 VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
AHA/HRET HEN 2.0 GET UP WEBINAR MOVE IT OR LOSE IT : CROSSCUTTING INTERVENTIONS TO ACCELERATE IMPROVEMENT. May 26, :00 a.m. 12:00 p.m.
 AHA/HRET HEN 2.0 GET UP WEBINAR MOVE IT OR LOSE IT : CROSSCUTTING INTERVENTIONS TO ACCELERATE IMPROVEMENT May 26, 2016 11:00 a.m. 12:00 p.m. CT 1 WELCOME AND INTRODUCTIONS Emily Koebnick, Program Manager,
AHA/HRET HEN 2.0 GET UP WEBINAR MOVE IT OR LOSE IT : CROSSCUTTING INTERVENTIONS TO ACCELERATE IMPROVEMENT May 26, 2016 11:00 a.m. 12:00 p.m. CT 1 WELCOME AND INTRODUCTIONS Emily Koebnick, Program Manager,
HEN 2.0 Monthly Update
 HEN 2.0 Monthly Update Jessica Rowden, MHA, BSN, R.N., CPHQ Director of Clinical Quality http://web.mhanet.com/quality-and-health-improvement.aspx HEN 2.0 Monthly Webinar Agenda Data Stipend Update Reports
HEN 2.0 Monthly Update Jessica Rowden, MHA, BSN, R.N., CPHQ Director of Clinical Quality http://web.mhanet.com/quality-and-health-improvement.aspx HEN 2.0 Monthly Webinar Agenda Data Stipend Update Reports
EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION
 EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION FOR HEALTHY COMMUNITIES Objectives Review 2015 NH Adverse
EXPERIENCE OF NH HOSPITALS: FALLS DATA NH FALLS RISK REDUCTION TASK FORCE ANNUAL DATA MEETING MARCH 7, 2017 PRESENTED BY: ANNE DIEFENDORF FOUNDATION FOR HEALTHY COMMUNITIES Objectives Review 2015 NH Adverse
4/28/17. New Jersey Antimicrobial Stewardship Learning Action Collaborative. Antimicrobial Stewardship Efforts in New Jersey. Update May 10, 2017
 New Jersey Antimicrobial Stewardship Learning Action Collaborative Update May 10, 2017 Antimicrobial Stewardship Efforts in New Jersey Acute Care Hospitals Outpatient Settings (ED, physician practices)
New Jersey Antimicrobial Stewardship Learning Action Collaborative Update May 10, 2017 Antimicrobial Stewardship Efforts in New Jersey Acute Care Hospitals Outpatient Settings (ED, physician practices)
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
HRET HIIN ADVERSE DRUG EVENTS (ADE)
") HRET HIIN ADVERSE DRUG EVENTS (ADE) Adjuncts and Alternatives to Opioids for Pain: It s All About Love February 14, 2017 1 Shereen Shojaat, MS, Program Manager HRET WELCOME AND INTRODUCTIONS 2 Agenda 12:00-12:05
HRET HIIN ADVERSE DRUG EVENTS (ADE) Adjuncts and Alternatives to Opioids for Pain: It s All About Love February 14, 2017 1 Shereen Shojaat, MS, Program Manager HRET WELCOME AND INTRODUCTIONS 2 Agenda 12:00-12:05
Chasing Zero Infections Coaching Call CLABSI: Reducing PICC and Central Line Utilization to Eliminate Bloodstream Infection April 10, 2018
 Chasing Zero Infections Coaching Call CLABSI: Reducing PICC and Central Line Utilization to Eliminate Bloodstream Infection April 10, 2018 Agenda Welcome & FHA Mission to Care HIIN Trends and Progress:
Chasing Zero Infections Coaching Call CLABSI: Reducing PICC and Central Line Utilization to Eliminate Bloodstream Infection April 10, 2018 Agenda Welcome & FHA Mission to Care HIIN Trends and Progress:
Focus Group results RN Perspective
 Focus Group results RN Perspective Category Themes Communication Patient Condition Communicate Expectations and plan of care Early 1. Communicate to patient at beginning of shift and throughout shift (pain
Focus Group results RN Perspective Category Themes Communication Patient Condition Communicate Expectations and plan of care Early 1. Communicate to patient at beginning of shift and throughout shift (pain
FHA MTC HIIN Lead Quarterly Virtual Meeting April 30, 2018
 FHA MTC HIIN Lead Quarterly Virtual Meeting April 30, 2018 Today s Agenda Welcome and Overview for today s HIIN Lead Virtual Meeting HIINgagment and HIINaction Florida s Success, Opportunities and Line
FHA MTC HIIN Lead Quarterly Virtual Meeting April 30, 2018 Today s Agenda Welcome and Overview for today s HIIN Lead Virtual Meeting HIINgagment and HIINaction Florida s Success, Opportunities and Line
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
FHA MTC HIIN Quarterly Virtual Meeting January 22, 2018
 FHA MTC HIIN Quarterly Virtual Meeting January 22, 2018 Today s Agenda Purpose of the Call UP Campaign Review of the data Needs Assessment Feedback What do you Need? CMS HIIN GOALS GOALS: 20% Overall Reduction
FHA MTC HIIN Quarterly Virtual Meeting January 22, 2018 Today s Agenda Purpose of the Call UP Campaign Review of the data Needs Assessment Feedback What do you Need? CMS HIIN GOALS GOALS: 20% Overall Reduction
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress
 Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD
 Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD TD Nursing Professor in Critical Care Research, Sunnybrook Health Sciences Centre Associate Professor, LSBFON, University of Toronto CIHR New Investigator
Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD TD Nursing Professor in Critical Care Research, Sunnybrook Health Sciences Centre Associate Professor, LSBFON, University of Toronto CIHR New Investigator
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Antibiotic Stewardship Program (ASP)
") Introduction: Antibiotics are among the most frequently prescribed medications in nursing centers, with up to 70% of nursing home patients receiving one or more courses of systemic antibiotics in a year.
Introduction: Antibiotics are among the most frequently prescribed medications in nursing centers, with up to 70% of nursing home patients receiving one or more courses of systemic antibiotics in a year.
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
HRET HIIN MDRO Taking MDRO Prevention to the Next Level!
 HRET HIIN MDRO Taking MDRO Prevention to the Next Level! October 17, 2017 12:30 p.m. 1:30 p.m. CT 1 Kristin Preihs Senior Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference
HRET HIIN MDRO Taking MDRO Prevention to the Next Level! October 17, 2017 12:30 p.m. 1:30 p.m. CT 1 Kristin Preihs Senior Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference
The impact of nighttime intensivists on medical intensive care unit infection-related indicators
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 The impact of nighttime intensivists on medical intensive care unit infection-related indicators Abhaya Trivedi
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 The impact of nighttime intensivists on medical intensive care unit infection-related indicators Abhaya Trivedi
SOAP UP w. July 18, 2017
 SOAP UP Hand w Hygiene July 18, 2017 Agenda Welcome and Introductions IHA Hand Hygiene Survey Results Hospital Features SOAP UP Campaign Resources and Support Hand Hygiene Webinar Series 2 Indiana s Bold
SOAP UP Hand w Hygiene July 18, 2017 Agenda Welcome and Introductions IHA Hand Hygiene Survey Results Hospital Features SOAP UP Campaign Resources and Support Hand Hygiene Webinar Series 2 Indiana s Bold
Exemplary Professional Practice: Patient Care Delivery Model(s)
") Exemplary Professional Practice: Patient Care Delivery Model(s) EP7EO Nurses systematically evaluate professional organizations standards of practice, incorporating them into the organization s professional
Exemplary Professional Practice: Patient Care Delivery Model(s) EP7EO Nurses systematically evaluate professional organizations standards of practice, incorporating them into the organization s professional
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Policies and Procedures. Title:
 Policies and Procedures Title: PATIENT CONTROLLED ANALGESIA (PCA) LPN Additional Competency: Patient Controlled Analgesia with an Established Plan of Care RN Entry-Level Competency Authorization: [X] Former
Policies and Procedures Title: PATIENT CONTROLLED ANALGESIA (PCA) LPN Additional Competency: Patient Controlled Analgesia with an Established Plan of Care RN Entry-Level Competency Authorization: [X] Former
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
Pharmacy Services. Division of Nursing Homes
 Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Medication Related Changes Phase 1&2
 Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Medication Related Changes Phase 1&2 Medicare and Medicaid Programs Reform of Requirements for Long-Term Care Facilities Published January 23, 2017 Medication- Related Changes* Changes will be implemented
Acknowledgement. Speaker Disclosure Statement. ASPMN 21 st National Conference Tucson, AZ September 9,
 Monitoring Over Sedation in Adult and Pediatric Patients Receiving Opioids for Michele Farrington, BSN, RN, CPHON michele farrington@uiowa.edu Staff Nurse Anne Smith, MSN, RN BC anne m smith@uiowa.edu
Monitoring Over Sedation in Adult and Pediatric Patients Receiving Opioids for Michele Farrington, BSN, RN, CPHON michele farrington@uiowa.edu Staff Nurse Anne Smith, MSN, RN BC anne m smith@uiowa.edu
Sedation/Analgesia by Non-Anesthesiologists. THE UNIVERSITY OF TOLEDO Approving Officer:
 Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Clinical Intervention Overview: Objectives
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
TOTAL HIP REPLACEMENT FLOW SHEET
 TOTAL HIP REPLACEMENT FLOW SHEET Before Surgery: Nothing to eat or drink after midnight the night before surgery. Make sure you have a bowel movement the day before surgery. Be sure to attend your pre-op
TOTAL HIP REPLACEMENT FLOW SHEET Before Surgery: Nothing to eat or drink after midnight the night before surgery. Make sure you have a bowel movement the day before surgery. Be sure to attend your pre-op
Chasing Zero Infections Coaching Call Strategies to Reduce Surgical Site Infections March 14, 2018
 Chasing Zero Infections Coaching Call Strategies to Reduce Surgical Site Infections March 14, 2018 Agenda Welcome & FHA Mission to Care HIIN Trends and Progress: Surgical Site Infections Cheryl Love, RN,
Chasing Zero Infections Coaching Call Strategies to Reduce Surgical Site Infections March 14, 2018 Agenda Welcome & FHA Mission to Care HIIN Trends and Progress: Surgical Site Infections Cheryl Love, RN,
Barriers to Early Rehabilitation in Critically Ill Patients. Shannon Goddard, MD Sunnybrook Health Sciences Centre
 Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
Barriers to Early Rehabilitation in Critically Ill Patients Shannon Goddard, MD Sunnybrook Health Sciences Centre Disclosures/Funding No financial disclosures or conflicts of interest Work is funding by
The CMS State Operations Manual Overview and Changes
 The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
The CMS State Operations Manual Overview and Changes Omnicare, Inc. Page 1 Overview of the CMS State Operations Manual Executive Summary Historical Perspective The Requirements Pharmacy Services Labeling
Chasing Zero Infections Webinar: SOAP UP / Hand Hygiene
 Chasing Zero Infections Webinar: SOAP UP / Hand Hygiene October 24, 2017 Agenda Welcome & HIIN Update Sally Forsberg, RNC-OB, BSN, MBA, NEA-BC, CPHQ, Clinical Performance Improvement Advisor, FHA Hospitals
Chasing Zero Infections Webinar: SOAP UP / Hand Hygiene October 24, 2017 Agenda Welcome & HIIN Update Sally Forsberg, RNC-OB, BSN, MBA, NEA-BC, CPHQ, Clinical Performance Improvement Advisor, FHA Hospitals
Contents. Introduction 3. Required knowledge and skills 4. Section One: Knowledge and skills for all nurses and care staff 6
 Decision-making frameworks in advanced dementia: Links to improved care project. Page 2 of 17 Contents Introduction 3 Required knowledge and skills 4 Section One: Knowledge and skills for all nurses and
Decision-making frameworks in advanced dementia: Links to improved care project. Page 2 of 17 Contents Introduction 3 Required knowledge and skills 4 Section One: Knowledge and skills for all nurses and
MDS Essentials. MDS Essentials: Content. Faculty Disclosures 5/22/2017. Educational Activity Completion
 MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
Patient Centered Care Planning and Behaviors. Presented by: Pam Paulsen, RN/BC,RAC-CT Angela Johnson, PharmD, BCGP
 Patient Centered Care Planning and Behaviors Presented by: Pam Paulsen, RN/BC,RAC-CT Angela Johnson, PharmD, BCGP Objectives 1 2 3 Identify 3 ways to promote patient centered care throughout communication
Patient Centered Care Planning and Behaviors Presented by: Pam Paulsen, RN/BC,RAC-CT Angela Johnson, PharmD, BCGP Objectives 1 2 3 Identify 3 ways to promote patient centered care throughout communication
Subject: Skilled Nursing Facilities (Page 1 of 6)
") Subject: Skilled Nursing Facilities (Page 1 of 6) Objective: I. To ensure that Tuality Health Alliance (THA) and delegated Providence Health Plan Medicare members are appropriately placed in skilled nursing
Subject: Skilled Nursing Facilities (Page 1 of 6) Objective: I. To ensure that Tuality Health Alliance (THA) and delegated Providence Health Plan Medicare members are appropriately placed in skilled nursing
SCIP. Surgical Care Improvement Project. Making Surgeries Safer. By: Roshini Mathew, RN
 SCIP Surgical Care Improvement Project Making Surgeries Safer By: Roshini Mathew, RN Importance Hospitals could prevent 13,000 patient deaths and 271,000 surgical complications each year 4 measures are
SCIP Surgical Care Improvement Project Making Surgeries Safer By: Roshini Mathew, RN Importance Hospitals could prevent 13,000 patient deaths and 271,000 surgical complications each year 4 measures are
MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER
 KINGSTON GENERAL HOSPITAL MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER LEARNING GUIDE FOR REGISTERED NURSES AND REGISTERED PRACTICAL NURSES Prepared by: Nursing Education Date: 2001 November Revised:
KINGSTON GENERAL HOSPITAL MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER LEARNING GUIDE FOR REGISTERED NURSES AND REGISTERED PRACTICAL NURSES Prepared by: Nursing Education Date: 2001 November Revised:
Abdominal Surgery. Beyond Medicine. What to Expect While You Are in the Hospital. ilearning about your health
 ilearning about your health Abdominal Surgery What to Expect While You Are in the Hospital www.cpmc.org/learning Beyond Medicine. Table of Contents On the Day of Your Surgery...3 Your Nursing Care...3
ilearning about your health Abdominal Surgery What to Expect While You Are in the Hospital www.cpmc.org/learning Beyond Medicine. Table of Contents On the Day of Your Surgery...3 Your Nursing Care...3
Using Electronic Health Records for Antibiotic Stewardship
 Using Electronic Health Records for Antibiotic Stewardship STRENGTHEN YOUR LONG-TERM CARE STEWARDSHIP PROGRAM BY TRACKING AND REPORTING ELECTRONIC DATA Introduction Why Use Electronic Systems for Stewardship?
Using Electronic Health Records for Antibiotic Stewardship STRENGTHEN YOUR LONG-TERM CARE STEWARDSHIP PROGRAM BY TRACKING AND REPORTING ELECTRONIC DATA Introduction Why Use Electronic Systems for Stewardship?
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool
 Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Measuring Medication Harm: Advantages of Using a Trigger Tool. Frank Federico Executive Director
 Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
Measuring Medication Harm: Advantages of Using a Trigger Tool Frank Federico Executive Director ffederico@ihi.org Objectives Review the use of the trigger tool Discuss how to use the trigger tool for high-alert
PROCEDURAL SEDATION AND ANALGESIA: HOSPITAL-WIDE POLICY
 CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
Organization: Solution Title: Program/Project Description, including Goals: What is this project? Why is this project important?
 Organization: Hebrew Home of Greater Washington (The Charles E. Smith Life Communities) The Hebrew Home provides post-acute services and long-term care to a daily average census of 500 residents. The Home
Organization: Hebrew Home of Greater Washington (The Charles E. Smith Life Communities) The Hebrew Home provides post-acute services and long-term care to a daily average census of 500 residents. The Home
PATIENT SAFETY PART OF THE JOINT COMMISSION SPEAK UP PROGRAM
 PATIENT SAFETY PART OF THE JOINT COMMISSION SPEAK UP PROGRAM UM/Sylvester Comprehensive Cancer Center 1475 N.W. 12th Avenue Miami, Florida 33136 305-243-1000 1-800-545-2292 UM/Sylvester at Deerfield Beach
PATIENT SAFETY PART OF THE JOINT COMMISSION SPEAK UP PROGRAM UM/Sylvester Comprehensive Cancer Center 1475 N.W. 12th Avenue Miami, Florida 33136 305-243-1000 1-800-545-2292 UM/Sylvester at Deerfield Beach
Antibiotics - Are they OVERUSED? 4/6/2018. Antibiotic Stewardship Key Clinical Strategies for Successful Outcomes. Pathway Health 1.
 Antibiotic Stewardship Key Clinical Strategies for Successful Outcomes Louann Lawson, BA, RN, RAC-CT, CIMT Nurse Consultant Clinical Reimbursement Team Leader/Clinical Education Manager Pathway Health
Antibiotic Stewardship Key Clinical Strategies for Successful Outcomes Louann Lawson, BA, RN, RAC-CT, CIMT Nurse Consultant Clinical Reimbursement Team Leader/Clinical Education Manager Pathway Health
Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare. Friday October 14, 2016
 Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare Friday October 14, 2016 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National
Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare Friday October 14, 2016 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Case: Comparing Two Scenarios
 The Case: Case: Comparing Two Scenarios Dale Urdick and Lauren Weizhart are both Quality Improvement Managers at two large pediatric hospitals in different provinces. Although hundreds of kilomiles separate
The Case: Case: Comparing Two Scenarios Dale Urdick and Lauren Weizhart are both Quality Improvement Managers at two large pediatric hospitals in different provinces. Although hundreds of kilomiles separate
Effective Tools to Prevent and Manage Adverse Events: Lesson 2
 Effective Tools to Prevent and Manage Adverse Events: Lesson 2 Based on the Office of Inspector General Adverse Events Report February 2014 Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com
Effective Tools to Prevent and Manage Adverse Events: Lesson 2 Based on the Office of Inspector General Adverse Events Report February 2014 Diane C. Vaughn, RN, C-DONA/LTC; LNHA vaughndiane@hotmail.com
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
HealthInsight HIIN Onboarding Event: DATA, DATA, DATA. April 12, a.m. to noon PT Noon to 1 p.m. MT
 HealthInsight HIIN Onboarding Event: DATA, DATA, DATA April 12, 2017 11 a.m. to noon PT Noon to 1 p.m. MT Welcome So glad you are able to join us! This session is being recorded and a copy of the slides
HealthInsight HIIN Onboarding Event: DATA, DATA, DATA April 12, 2017 11 a.m. to noon PT Noon to 1 p.m. MT Welcome So glad you are able to join us! This session is being recorded and a copy of the slides
Early Progressive Mobility- Letting Go of Bedrest
 Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Early Progressive Mobility- Letting Go of Bedrest Jacqueline Clapp BSN, RN Lehigh Valley Health Network Holly Leighton
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Early Progressive Mobility- Letting Go of Bedrest Jacqueline Clapp BSN, RN Lehigh Valley Health Network Holly Leighton
HRET HIIN Adverse Drug Events Virtual Event. Opioid Safety Fishbowl Event #4: Moving the Fish Forward August 24, 2017
 HRET HIIN Adverse Drug Events Virtual Event Opioid Safety Fishbowl Event #4: Moving the Fish Forward August 24, 2017 1 Erin Craig Senior Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform
HRET HIIN Adverse Drug Events Virtual Event Opioid Safety Fishbowl Event #4: Moving the Fish Forward August 24, 2017 1 Erin Craig Senior Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform
THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON
 THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations
THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations
Restraint Reduction. Moving Towards Restraint Free Care
 Restraint Reduction Moving Towards Restraint Free Care Revised: BW/January 2016 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
Restraint Reduction Moving Towards Restraint Free Care Revised: BW/January 2016 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
Today s webinar will begin in a few minutes.
 Today s webinar will begin in a few minutes. Please press *6 to mute your line or use the mute button on your phone. If you have questions for the presenter or need to contact TCPS staff, type your comments
Today s webinar will begin in a few minutes. Please press *6 to mute your line or use the mute button on your phone. If you have questions for the presenter or need to contact TCPS staff, type your comments
A Changing Landscape Regulatory Impact on Medication Management
 2015 Remedi SeniorCare Annual Conference August 30, 2018 A Changing Landscape Regulatory Impact on Medication Management William M. Vaughan RN Vice President, Education / Clinical Affairs Remedi SeniorCare
2015 Remedi SeniorCare Annual Conference August 30, 2018 A Changing Landscape Regulatory Impact on Medication Management William M. Vaughan RN Vice President, Education / Clinical Affairs Remedi SeniorCare
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Patient s Care Path Note: Welcome to Providence Orthopaedic & NeuroSpine TOTAL HIP ARTHROPLASTY. Questions/Concerns. Midlands. Orthopaedics, P.A.
 TOTAL HIP ARTHROPLASTY Welcome to Providence Orthopaedic & NeuroSpine Institute. You are scheduled for surgery on your hip. The Care Path is a guide designed to help you and your family know what to expect
TOTAL HIP ARTHROPLASTY Welcome to Providence Orthopaedic & NeuroSpine Institute. You are scheduled for surgery on your hip. The Care Path is a guide designed to help you and your family know what to expect
Clinical Training: Medication Reconciliation. VNAA Best Practice for Home Health
 Clinical Training: Medication Reconciliation VNAA Best Practice for Home Health Learning Objectives To understand why medication reconciliation is important to providing quality care To understand the
Clinical Training: Medication Reconciliation VNAA Best Practice for Home Health Learning Objectives To understand why medication reconciliation is important to providing quality care To understand the
SOLUTION TITLE: Can Critical Care Become A Restraint Free Environment?
 ORGANIZATION: ST AGNES MEDICAL CENTER SOLUTION TITLE: Can Critical Care Become A Restraint Free Environment? PROGRAM/PROJECT DESCRIPTION INCLUDING GOALS: The critical care environment is perhaps the last
ORGANIZATION: ST AGNES MEDICAL CENTER SOLUTION TITLE: Can Critical Care Become A Restraint Free Environment? PROGRAM/PROJECT DESCRIPTION INCLUDING GOALS: The critical care environment is perhaps the last
Nursing Home Pearls or
 Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation
 Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation Potential and Mobility Plan Amy Dean, MS, RN, CCRN Kristin
Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation Potential and Mobility Plan Amy Dean, MS, RN, CCRN Kristin
Proposed Standards Revisions Related to Pain Assessment and Management
 Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Project of: Seniors Health Strategic Clinical Network (SCN) in collaboration with Addiction & Mental Health SCN
 in collaboration with Addiction & Mental Health SCN") Project of: Seniors Health Strategic Clinical Network (SCN) in collaboration with Addiction & Mental Health SCN This PowerPoint describes the steps and strategies developed by the Appropriate use of Antipsychotics
Project of: Seniors Health Strategic Clinical Network (SCN) in collaboration with Addiction & Mental Health SCN This PowerPoint describes the steps and strategies developed by the Appropriate use of Antipsychotics
How to Safely Transport a Client
 How to Safely Transport a Client INTRODUCTION Medical problems and/or physical limitations can and often do restrict a client s ability to ambulate and move, and transporting clients is a primary responsibility
How to Safely Transport a Client INTRODUCTION Medical problems and/or physical limitations can and often do restrict a client s ability to ambulate and move, and transporting clients is a primary responsibility
Peer Review Example: Clinician 4 (Meets Expectations)
") Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Appendix A: Encyclopedia of Measures (EOM)
") Appendix A: Encyclopedia of Measures (EOM) Great Lakes Partners for Patients HIIN Hospital Improvement Innovation Network (HIIN) Program Evaluation Measures Adapted from Version 1.0 AHA/HRET HEN 2.0 HIIN
Appendix A: Encyclopedia of Measures (EOM) Great Lakes Partners for Patients HIIN Hospital Improvement Innovation Network (HIIN) Program Evaluation Measures Adapted from Version 1.0 AHA/HRET HEN 2.0 HIIN
Checklists for Preventing and Controlling
 Checklists for Preventing and Controlling Clostridium difficile Infection (CDI) This document has been developed to specifically assist senior management and all ward staff to take appropriate actions,
Checklists for Preventing and Controlling Clostridium difficile Infection (CDI) This document has been developed to specifically assist senior management and all ward staff to take appropriate actions,
Staff Responsible Procedure Rationale/Reason
 Subject: Patient Controlled Analgesia Date: October 2011 UPMC St. Margaret UPMC St. Margaret Harmar Outpatient Center Clinical Practice Council Policy #2005 Overview: To promote appropriate PCA use and
Subject: Patient Controlled Analgesia Date: October 2011 UPMC St. Margaret UPMC St. Margaret Harmar Outpatient Center Clinical Practice Council Policy #2005 Overview: To promote appropriate PCA use and
Your Anesthesiologist, Anesthesia and Pain Control
 You can reduce your pain level after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in
You can reduce your pain level after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in
Implementing Antimicrobial Stewardship Programs- Suggestions for Rural and Critical Access Hospitals-a Hospital Story
 Pharmacy Roundtable Implementing Antimicrobial Stewardship Programs- Suggestions for Rural and Critical Access Hospitals-a Hospital Story Presenter: Jon C. Francisco, Pharm.D, BCPS Clinical Specialist
Pharmacy Roundtable Implementing Antimicrobial Stewardship Programs- Suggestions for Rural and Critical Access Hospitals-a Hospital Story Presenter: Jon C. Francisco, Pharm.D, BCPS Clinical Specialist
Pre-surgical / Pre-procedure INFORMATION FOR ADULT PATIENTS
 Pre-surgical / Pre-procedure INFORMATION FOR ADULT PATIENTS LANDMARK HOSPITAL OF SOUTHWEST FLORIDA Form OP.SS.851 (Original 05/2017) PRE-SURGICAL INSTRUCTIONS Thank you for choosing Landmark Hospital for
Pre-surgical / Pre-procedure INFORMATION FOR ADULT PATIENTS LANDMARK HOSPITAL OF SOUTHWEST FLORIDA Form OP.SS.851 (Original 05/2017) PRE-SURGICAL INSTRUCTIONS Thank you for choosing Landmark Hospital for
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV TREPROSTINIL (REMODULIN ) Job Title of Reviewer: Director, Pharmacy POLICY
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV TREPROSTINIL (REMODULIN ) Job Title of Reviewer: Director, Pharmacy POLICY
Interim Final Interpretive Guidelines Version 1.1
 Interim Final Interpretive Guidelines Version 1.1 Big Changes from November 2008 to January 2009 418.54 Condition of participation: Initial and Comprehensive assessment of the patient L522 418.54(a) Standard:
Interim Final Interpretive Guidelines Version 1.1 Big Changes from November 2008 to January 2009 418.54 Condition of participation: Initial and Comprehensive assessment of the patient L522 418.54(a) Standard:
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Improving Resident Care: A look at CMS quality of care initiatives
 Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Improving Resident Care: A look at CMS quality of care initiatives W H I T E P A P E R by Diane L. Brown dbrown@hcpro.com What do reduction in rehospitalization, caring for dementia patients and preventing
Quality From the View Point of the Patient
 Rethinking Critical Care: Building a Foundation with Reliability Terry P. Clemmer, MD LDS Hospital Salt Lake City, Utah terry.clemmer@imail.org Quality From the View Point of the Patient Don t Kill Me
Rethinking Critical Care: Building a Foundation with Reliability Terry P. Clemmer, MD LDS Hospital Salt Lake City, Utah terry.clemmer@imail.org Quality From the View Point of the Patient Don t Kill Me
Reducing Ventilator Associated Pneumonia (V.A.P) System and Patient Tracer
 System and Patient Tracer") Reducing V.A.P.: SYSTEM Tracer Begin with Large Group General Questions: 1. Describe your surgical and then medical process related to the prevention of V.A.P. 2. The Team Leader will create questions
Reducing V.A.P.: SYSTEM Tracer Begin with Large Group General Questions: 1. Describe your surgical and then medical process related to the prevention of V.A.P. 2. The Team Leader will create questions
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE PROCEDURAL SEDATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Health Professions Strategy & Practice PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
TITLE PROCEDURAL SEDATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Health Professions Strategy & Practice PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
Review of the 3 Step Medication Reconciliation Process
 Review of the 3 Step Medication Reconciliation Process CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation Medication Reconciliation*
Review of the 3 Step Medication Reconciliation Process CHAMP Activities are possible with generous support from The Atlantic Philanthropies and The John A. Hartford Foundation Medication Reconciliation*
Preventing Falls in the Home
 ~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers
 Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Be comfortable with comfort Meds
 DIAMOND PHARMACY SERVICES Be comfortable with comfort Meds Understanding Hospice medications Presented By: Daniel Barnes, RN Infusion RN Annual Educational Conference Thursday, April 16, 2015 1 Diamond
DIAMOND PHARMACY SERVICES Be comfortable with comfort Meds Understanding Hospice medications Presented By: Daniel Barnes, RN Infusion RN Annual Educational Conference Thursday, April 16, 2015 1 Diamond