MATH, SCIENCE & HEALTH PROFESSIONS NURSING PROGRAM
|
|
|
- Juliana Lane
- 5 years ago
- Views:
Transcription
1 MATH, SCIENCE & HEALTH PROFESSIONS NURSING PROGRAM ALTERATIONS IN HEALTH V NRS 230 Lab Manual Spring 2014
2 Welcome to NRS 230! This will be an exciting course for you, because you will be building on the concepts that you already learned in the previous courses. NRS 230 is a continuation of the concepts of elimination, oxygenation and perfusion, emphasizing the concepts of elimination, oxygenation and perfusion across the lifespan. You also will continue to develop critical thinking and clinical judgment skills when caring for the adult and pediatric patient who experiences alterations in elimination, oxygenation and perfusion. Please use this lab manual to prepare for class. The first section is a clinical skills check list. Please review these skills. If you are weak in any area, the simulation lab is an excellent resource for you to review these skills. Please be sure to let your lab instructor know. Also, you will see two simulation scenarios. Your lab instructor will decide who will be having simulation that week. Please be prepared for these simulations by researching the topics and the medications used for each simulation scenario that is provided. You will be graded on your reflection of this simulation in a journal format. Please see the grading rubric. Following the simulations found in the lab manual, you will see a week by week guide. Again, please be prepared to do drug calculations and case studies. Have a great semester!
3 NRS clinical skills Assessment checklist Student Name Course Identified skill Confident Need Assistance Never done Comments (# of times) Blood Pressure (Manual) Apical Rate Pulse Respirations Temperature Pulse Oximetry Weight Pain as the 5 th vital sign Urinary catheterization Continuous Bladder Irrigation Wound Care Sterile Dressing Changes Pressure Ulcer Care Skin Care Mouth Care Bathing Complete Bedmaking Unoccupied Bedmaking Occupied Range of Motion ABG Analysis Oxygen Therapy Continued
4 identified skill Confident Need Assistance Never done Comments (# of times) Tracheostomy Care Suctioning Hanging IV s Changing IV Dressings Infusiport Management PICC Line Management Central Line Management IV Pumps PCA and Epidural Pumps TPN Administration Administer Oral Meds IM Injections SQ Injections Glucometer Inserting NG Tube Tube Feedings PEG Tube Feedings NG Tube Drains (JP, Hemovac) Ostomy care Chest Tube Care Postmortem Care Isolation Procedures Dysrhythmias SBAR Reporting Dialysis Catheter Delegation Skills 1/12
5 Simulation for Urinary elimination and polynephritis (Weeks 1-4) Name: Nanna Krause Gender: female Age: 21 Weight: /kg 125 lb Height: _5.5_ft/in Religion: none Major Support: friends Allergies: none Immunizations: not sure Attending Physician/Team Doctor: Dr. Smith Attending ER physician PMH: 3 urinary Tract infections 2 Cranberry Capsules BID Vitamin C 1 Tablet BID Phenazophyridine unsure of dose and how many times a day she takes History of Present Illness: Nanna states she experienced burning sensation with urination, mild abdominal pain, and had frequent urination. Nanna awoke this morning with a high fever, vomiting, and severe abdominal pain. Nanna further adds that she had moderate bilateral flank pain. Social History: Nanna smokes a few cigarettes on the weekends when she goes out. She drinks 5 to 6 beers on Friday and Saturday nights. She has frequent sexual activity with no use of protection or birth control. Brief Overview of Scenario: Nanna came to the Emergency Department about She states she experienced burning sensation with urination, mild abdominal pain, and had frequent urination. She states I seriously had to go every 10 minutes. She has been having these signs and symptoms for 5 days now. Nanna was advised by her good friend to take cranberry pills, vitamin C and phenazopyridine. She began taking the medication after she researched them on the Internet because they seemed to be what I needed. Nanna awoke this morning with a high fever, vomiting, and severe abdominal pain. Nanna further adds that she had moderate bilateral flank pain. Nanna reports that she began having frequent urinary tract infections about the time she began college. She states I know what they feel like. IV Fluids: normal saline Oral meds: Vicodin 5/500mg PO q 4-6 hours PRN pain, Tylenol 1000mg Po x1 for fever IVPB: Ciprofloxacin 400mg BID IV Push: Zofran 4mg IVP q 4-6 PRN nausea and vomiting, Morphine 4mg IVP one dose for pain
6 Make sure during simulation you verbalize why the medication is being used, its action, intended effect, and any lethal side effects. Psychomotor Skills required prior to simulation: IV set up and insertion Medication administration Foley catheter insertion Vital Signs
7 Simulation for Cardiogenic Shock (Weeks 1-4) Name: Charles Case Gender: male Age: 65 Weight: _95.5_/kg 210 lb Height: _6_ft/in Religion: none Major Support: 2 children Allergies: none Immunizations: unsure Attending Physician/Team Doctor Pressman Attending Cardiologist PMH: Stable exertional angina for 7 years Type 2 DM HTN History of Present Illness: Chest pain unrelieved with rest and nitroglycerin x 3 doses SL Social History: Smoked for 45 years packs a day No use of recreational drugs Brief Overview of Scenario: Charles Case is a 65 year old man who was admitted to the Coronary Care Unit with a diagnosis of acute anterior wall MI. Mr. Case is complaining of severe sub sternal chest pain lasting over 6 hours that was accompanied by a choking feeling severe SOB, and diaphoreses. He described the pain as a deep pressure that was unrelieved by rest, antacids, and 3 sublingual nitroglycerin tablets. Mr. Case drove himself to the emergency room. In the emergency room department, Mr. Case s assessment revealed he is overweight and in obvious distress. Vital signs are: B/P 164/100 HR 122 RR 34 Temp. 99.5
8 Be prepared and look up these medications prior to lab. Be able to calculate ml/hour for dose ordered. Additionally, understand what lab studies would be ordered and what these lab studies mean. IV Fluids: normal saline Oral meds: Metoprolol 25mg PO BID (hold SBP <90, HR 40) once off of IV metoprolol. Colace 100mg PO BID IV Push: Morphine 2-5mg IVP q 2 hours PRN chest pain Metoprolol 5mg IV push now then q6 hours IV Drips Nitroglycerin IV start at Heparin gtt IV weight based 25,000units/250ml NS Neosynephrin gtt 50mg/250ml NS Dobutamine 500mg/250ml NS Morphine 50mg/50 ml NS Versed 50mg/50 ml NS IM or SC: Apidra insulin subcutaneous given ac & hs per sliding scale Make sure during simulation you verbalize why the medication is being used, its action, intended effect, and any lethal side effects.
9 Guidelines for Written Assignments: Mercer County Community College NRS 230 Simulation Journaling Activity Grading Rubric and Guidelines The purpose of journaling is to give the student the opportunity to reflect back on the simulation event and consider what was learned, what was successful or done well and what areas of content/skills are weak and could use more practice or study. Each student is required to submit this journal, by in a word document, within 24 hours of the completion of the lab. Students will receive feedback from the instructor each week. This journaling activity represents 5% of your course grade and is evidence of having met the day s/week s lab simulation objectives. It is important that you take it seriously spending the appropriate amount of time in this activity and truly reflect on the learning that has occurred. Level of Performance Deficient Score of 0 Emerging Score of 1 Competent Score of 2 Content Clinical outcomes not assessed by student or no reflection of experience provided. Journal entry assesses most of the clinical outcomes, but not all. Superficial reflection present, but student needs more depth in thought process. Log/journal entry assesses each clinical outcome of assignment. Reflection of clinical experience demonstrates insight and personal assessment. Reflection of Clinical Experience Reflection lacks evidence of understanding of nurse s role in the particular clinical setting. Lacks evidence of relationship between theory and clinical practice. Reflection demonstrates lack of or poor enhancement of student s theoretical base and clinical practice. Demonstrates little effort toward seeking opportunities for reflection. Examples do not demonstrate student learning or professional Reflection demonstrates limited understanding of the nurse s role in the particular clinical setting. Some connections established between theory and clinical practice. Slight professional growth demonstrated in theory base and clinical practice. Poor Student reflection demonstrates understanding of the nurse s role in the particular clinical setting. Identification of relationship between theory and clinical practice established. Reflection of clinical experience shows evidence of enhancement of student theoretical base and
10 Level of Performance Deficient Score of 0 Emerging Score of 1 Competent Score of 2 Critical Thinking Format growth. Evidence of critical thinking principles and nursing process lacking and not defended in log/journal. Student does not incorporate principles into planned client care. Student fails to evaluate the effectiveness of planned client care utilizing critical thinking/nursing processes. Client plan of care is not revised as needed. Student fails to identify the necessity of constructive feedback from others. Student reacts inappropriately to feedback. Communicated peer feedback is not accepted or incorporated into nursing practice. Entry is not submitted by within the expected time frame. Journal entry is unorganized in ideas and unreadable in format. examples of student learning and professional growth. Some evidence of use of critical thinking principles and nursing process communicated and but poorly defended in journal. Student incorporates some principles into planned client care. Student partially evaluates the effectiveness of planned client care utilizing critical thinking/nursing processes. Following evaluation, client plan of care is not revised as needed and alternative solutions are determined but not implemented. Student can identify the necessity of constructive feedback from others. Communicated feedback from peers is accepted but not incorporated into nursing practice. Entry is not submitted by within the expected time frame. Journal entry is unreadable or lacks clinical practice. Specific examples of learning and professional growth provided by student. Evidence of critical thinking principles and nursing process communicated and clearly defended in journal. Student incorporates principles into planned client care. Student evaluates the effectiveness of planned client care utilizing critical thinking/nursing processes. Following evaluation, client plan of care is revised as needed and alternative solutions are determined/implemented. Student can identify the necessity of constructive feedback from others. Communicated peer feedback is incorporated into nursing practice. Entry is submitted by within the expected time frame. Journal is readable and provides organization of
11 Level of Performance Deficient Score of 0 Emerging Score of 1 Competent Score of 2 organization of ideas. R. Lewis Copyright 2006, University of Charleston ideas. Below are some suggestions on topics to be considered (but not limited to) in the journal writing. Was there anything during the lab experience that was confusing to you? What was it? How did you handle that situation? Was there anything you could have done to better prepare yourself? Was there any time during the lab when you didn t know what to do? How did you feel? What would you do differently having had this experience? Was there anything about the lab experience that troubled or disturbed you? What was it? What will help make it easier for you to deal with this experience in the future? Was there anything about the lab experience that made the light bulb come on - something that made the content clearer to you? What was it and explain what happened to illuminate your understanding? Do you still have questions about the topic/content? What are they? How will you resolve these questions? How did today s experience assist you in meeting the course/topic/program objectives? 16 points = 100% 15 points = 93.75% 14 points = 87.50% Etc. The journal assignment will equate to 5% of the course grade.
12 Week 1 NRS 230 will also focus on titrating of critical medications. Please calculate the following medications. 1) The physician ordered Norepinephrine (Levophed) for a patient who is septic with a low blood pressure. The levophed is mixed 4mg in 250mL D5W. Levophed is to be started at 10mcg/min. Please calculate the rate of flow. ml/hr. 2) Ordered is amiodorone. It is mixed 900mg in 500mL D5W. The physician wants the medication started at 0.5mg/min. Calculate the rate of flow. ml/hr. 3) Ordered is Dopamine. The physician wants the medication started at a renal dose which is 5mcg/kg/min. The medication is prepared 400mg/250 ml D5W. The patient weighs 150lbs. Calculate the rate of flow. ml/hr. 4) The same patient was admitted to the ICU with dopamine infusing. You notice that it is running at 46mL/hr. How many mcg/kg/min is that? mcg/kg/min. 5) Heparin is to be infused at 960 units/hr. The medication is prepared 25,000/250 ml D5W. Calculate the rate of flow ml/hr.
13 CASE STUDY URINARY TRACT INFECTION Shelly Homes is a 4 y/o preschooler who lives with her parents and younger brother. She and her brother attend a local daycare center during the week while their parents are at work. In the evenings, she and her brother take a bath. After the bath, their parents read to them before bedtime at 8:00pm. Shelly s daycare class includes many children her age and she enjoys playing outside with them. Although snack times are planned, Shelly would rather play and does not always finish her beverages. Shelly s mother calls the pediatric clinic in town and tells the nurse that Shelly has been running a fever of 101 F for the past 2 days. Although her temperature decreased to 99 F with Tylenol, it returns to 101 F within 4 hours of each dose. Furthermore, her mother also has noticed that Shelly complains that it hurts when I go pee-pee. Shelly s mother also has noticed that her daughter seems to be in the bathroom every hour. She makes an appointment to see the pediatrician this afternoon. 1. What is the significance of Shelly s clinical manifestations? 2. What other assessment data would be helpful for the nurse to have to prepare Shelly s care plan? 3. What are Shelly s anatomic risk factors for developing a UTI? 4. What are the relationship between Shelly s hygiene habits and her risk for developing a UTI? 5. How does Shelly s level of growth and development places her at risk for the developing a UTI? 6. Shelly s urine culture is positive for Escherichia coli. What is the significance of this finding? 7. What are the priorities for Shelly s care? 8. Shelly is prescribed trimethoprim-sulfamethoxazole 60mg every 12 hours for 10 days. What is this drug and is her prescribed dose safe? Shelly weighs 33 lbs. 9. What are the teaching priorities for Shelly and her mother prior to her leaving the clinic? 10. Shelly is scheduled for a return visit to the clinic in 2 weeks. What is the purpose of this appointment?
14 CASE STUDY Acute Pyelonephritis Case Mrs. Reese is a 27 year old female who had a sudden onset of abdominal pain at 2:00am. The pain became so severe that she went to the ER. Upon her arrival to the ER, she described her pain as a constant ache in her lower right quadrant of her abdomen that radiates across the flank of her lower back. She rates her pain a 9 out of 10 on a 0-10 pain scale. She is also complaining of nausea and has vomited 3 times prior to arrival. She is febrile and complaining of chills. Assessment: Mrs. Reese s vital signs are BP 118/60, HR 108, RR 24, and temp. 40 C (104.1F) Her oxygen saturation is 100% on room air. The nurse asks Mrs. Reese if she has noticed any recent changes in her voiding, such as burning, frequency, or feeling as if she is unable to empty her bladder completely. The nurse also asks Mrs. Reese if she has had a fever in the days prior to coming to the hospital. Mrs. Reese states, Now that I think about it, I have been going to the bathroom more often than usual, and it smelled a little funny. The other day I noticed a dull pain in my lower back. I figured it was from picking up my daughter. Yesterday I remember thinking I felt warm, but my daughter was getting into something and I got distracted and never took my temperature. Upon physical examination, Mrs. Reese s skin is warm, and her face is flushed. Her abdomen is slightly distended and tender on palpation. Her bowel sounds are hypoactive in all four quadrants. She is admitted with a suspected diagnosis of acute pyelonephritis. Mrs. Reese will be hospitalized for a few days. She expressed concern to the nurse stating, I need to hurry up and get better. My husband works two jobs, and my parents can only stay at my house for a day or two to care for my daughter. I need to get home as soon as possible. My daughter needs me. Intravenous (IV) fluids are prescribed as ½ normal saline (1/2 NS) at 100 ml per hour. Diagnostic tests include a complete blood count with differential (CBC with diff), comprehensive metabolic panel (CMP), urinalysis with culture and sensitivity (U/A C& S), X-ray of the kidneys, ureters, and bladder (KUB) with intravenous pyelography (IVP), and blood cultures X 2 sites. Medications prescribed include ketorolac tromethamine, ondansetron hydrochloride, and levofloxin. Results of the CBC include a white blood cell (WBC) count of 14,200 cells/mm3. Her CMP results are all within normal limits. The urinalysis reveals the presence of a large amount of occult blood, protein 30mg/dL, 6-10 WBCs, red blood cells, moderate mucous and moderate amount of bacteria. The urine culture and sensitivity is positive for Escherichia coli
15 (E. coli) bacteria. The KUB with IVP shows normal urinary structures without the presence of stones or obstructions. 1. While in the ER, the nurse asks Mrs. Reese if she has noticed any recent changes in her voiding or a fever in the days prior to hospitalization. Explain how the assessment data relates to Mrs. Reese s admitting diagnosis? 2. Women are more likely to experience a UTI up until age 50 years, when the risk is similar in both genders. Explain why women are at increased risk and why older men experience more UTI s then younger men do? 3. Discuss the pathophysiology of acute pyelonephritis and identify the most common organism causing this infection? 4. Identify the risk factors that placed Mrs. Reese at greater risk for the development of acute pyelonephritis. 5. What are the characteristic clinical manifestations of pyelonephritis? 6. Mrs. Reese has a KUB with IVP. Explain this diagnostic test. How do the results help the health care provider to confirm the admitting diagnosis? 7. Mrs. Reese has no known allergies. She has been prescribed the following medications, ketorolac tromethamine, ondansetron hydrochloride, and levofloxin. Provide a rationale for why each medication has been included as part of her medical management and any potential contraindication(s) of her taking these medications. 8. The nurse is designing Mrs. Reese s plan of care. Identify three priority nursing diagnoses for inclusion in the plan. 9. The nurse places highest priority on the nursing diagnosis acute pain r/t inflammation and irritation of urinary tract. State an outcome goal appropriate for Mrs. Reese and at least two nursing interventions to help achieve the goal. 10. Two days later, Mrs. Reese is afebrile and her nausea and vomiting have resolved. She is being discharged on an oral antibiotic. Provide the patient with education about her prescribed antibiotic and symptoms that warrant notification of her health care provider. 11. While the nurse is discontinuing the IV access, Mrs. Reese asks, My doctor said that there is a chance I could get sick with this infection again. Is there anything I can do to help prevent that? Offer Mrs. Reese at least five health promotion behaviors to help prevent a UTI and recurrent acute pyelonephritis.
16 12. Mrs. Reese asks the nurse, I heard if you drink cranberry juice it can cure a urinary tract infection. Is this true? How will the nurse respond and what are three other complimentary therapies that the nurse might suggest? CASE STUDY Chronic Renal Failure Mr. Rossi is a 58 year old male diagnosed with diabetic nephropathy 10 years ago. He is now in end stage renal failure and has recently started continuous ambulatory peritoneal dialysis (CAPD) in his home. On a snowy day in February, the visiting nurse has come to see Mr. Rossi and his wife to reinforce instructions regarding the proper technique for peritoneal dialysis and to assess how the Rossi s are coping. When the nurse arrives, Mr. Rossi is resting comfortably in a reclining chair with a bottle of diet cola on the tray next to his chair. The nurse has concerns about Mr. Rossi s diet, and during the home visit, the nurse observes several behaviors that indicate a need for further teaching. 1. Briefly discuss how Mr. Rossi s past medical history increased his risk of developing renal failure. 2. Describe the physiologic changes in the kidneys that lead to chronic renal failure (CRF). 3. What is glomerular filtration rate (GFR)? How is GFR measured and what is the normal range in a healthy adult? 4. According to the national Kidney Foundation s five- stage classification system of chronic kidney disease, which stage of CKD is Mr. Rossi in, and what would you anticipate his GFR to be? 5. Briefly describe the changes in urine output characteristic of ESRD. 6. Briefly explain how peritoneal dialysis clears the body of excess water and waste products of metabolism. Describe three main types of peritoneal dialysis. 7. What are some advantages of peritoneal dialysis as compared to hemodialysis? Discuss why peritoneal dialysis is more favorable for Mr. Rossi than the hemodialysis treatment option. 8. Mrs. Rossi shows the nurse where they have cleared a clean space in their garage to store the supplies for Mr. Rossi s dialysis. What should the nurse remind the Rossis to do before attaching the dialysate to Mr. Rossi s peritoneal catheter? 9. The nurse asks Mrs. Rossi about the last few meals she prepared for her husband. Mrs. Rossi indicates the following meals: a. Whole grain cereal with milk, orange juice, and a banana
17 b. A roast beef sandwich with cheese and mayonnaise c. White bread toast, apple juice, and tea d. A peanut butter and jelly sandwich with diet cola Clarify to Mrs. Smith which of these meals was the most appropriate for Mr. Rossi regarding his renal diet and your concerns about the other meals she prepared. 10. The Nurse notices that by the reclining chair where Mr. Rossi sits is a 2 liter bottle of diet cola. Why is the nurse concerned? 11. Who should the visiting nurse arrange to meet with the Rossis to provide additional teaching regarding appropriate food and beverage choices for a patient with renal failure? 12. Mrs. Rossi asks the nurse, Someone at church said I should watch that my husband does not fall. They said he could break his hip very easily because people with bad kidney disease have very brittle bones. Is that true? Help the nurse explain why patients with renal failure develop changes in their bones and offer some examples of renal osteodystrophy that may develop. 13. Identify 5 priority nursing diagnoses for Mr. Rossi. 14. The nurse reminds Mr. Rossi that he is a risk of becoming anemic. Briefly explain to him why he is at risk and what are the signs and symptoms he should report to his heath care provider. 15. The nurse notices a napkin on the kitchen table with two calcium carbonate (Tums) tablets on it. When the nurse asks Mr. Rossi if he is taking his Tums with every meal, he replies, Sometimes I remember. Sometimes I forget. I figure it is not a problem if I forget once in a while. I don t have any symptoms of heart burn anyway. In lay terminology, how might the nurse explain to Mr. Rossi the importance of taking his Tums with every meal? 16. Mrs. Rossi calls the visiting nurse to report that When my husband s solution was drained out of his belly today, I noticed is was cloudy looking and he has a fever of 102 F (38.9 C). Briefly discuss the common complication of peritoneal dialysis that Mr. Rossi appears to have developed. What should the nurse tell the Rossi s to do? 17. Discuss the lifestyle changes imposed upon the patient who is on peritoneal dialysis and how these changes may affect the patient s quality of life.
18 Week 2 Practice Problems: 1. Dopamine 400 mg in 250 ml D 5 W to infuse at 5 mcg/kg/min. The patient s weight is 200 pounds. How many ml/hour would this be on an infusion pump? 2. A Dopamine drip (400mg in 250 cc of IV fluid) is infusing on your 80 kg patient at 20 ml/hour. How many mcg/kg/min are infusing for this patient? 3. A Nitroglycerin drip is ordered for your patient to control his chest pain. The concentration is 100 mg in 250 ml D 5 W. The order is to begin the infusion at 20 mcg/min. What is the rate you would begin the infusion on the infusion pump? 4. A Nitroglycerin drip (100mg in 250 cc D 5 W) is infusing on your patient at 28 ml/hour on the infusion pump. How many mcg/min is your patient receiving? 5. A procainamide drip is ordered (2gms in 250 ml D 5 W) to infuse at 4 mg/min. The patient weighs 165 pounds. Calculate the drip rate in ml/hour for which the infusion pump will be set at. 6. A Lidocaine drip is infusion on your 90 kg patient at 22 ml/hour. The Lidocaine concentration is 2 grams in 250 cc of D 5 W. How many mg/min is your patient receiving?
19 Case Study The Client with Heart Failure A 74-year-old woman is admitted to the hospital with heart failure. She had been growing progressively weaker and had ankle edema, dyspnea on exertion, and three-pillow orthopnea. On admission, she is severely dyspneic and can answer questions only with one-word phrases. She is diaphoretic, with a heart rate of 132 beats/min, and blood pressure 98/70. She is extremely anxious. The nurse performs a physical assessment of the client with heart failure and defers questions until the client has gained some relief as a result of emergency interventions. The priority assessments are as follows: 1. Considering the process of congestive heart failure, explain the symptoms she is having. Your client s presenting symptoms are as follows: 2. Based on assessment, identify nursing diagnoses for this client. 3. The physician orders the following items for this client. (Start an IV, then give dobutamine 3 mg/kg/hr IV; Furosemide (Lasix) 40 mg IV stat; Digoxin 0.5 mg PO stat, then every 6 hours for three doses, with ECG before doses 3 and 4; Morphine 2 mg IV stat and then 2 mg IV every 1 to 2 hours prn; Oxygen 4 L/min per nasal cannula; Schedule for an echocardiogram; No added salt diet; Weigh daily and monitor input and output) Explain the rationale for these medications and treatments.
20 Case Study The Patient with a Dysrhythmia A 78-year-old woman is admitted to a telemetry unit directly from her physician s office for evaluation and management of congestive heart failure. She has a history of systemic hypertension and chronic moderate mitral regurgitation. Her medication orders include furosemide (Lasix) 80 mg PO four times a day, digoxin mg PO daily, and diltiazem (Cardizem) 60 mg PO three times a day. Your initial assessment of the client reveals a pulse rate that is rapid and very irregular. The client is restless, her skin is pale and cool, she states she is dizzy when she stands up, and she is slightly short of breath. Her blood pressure is 106/88. She is short of breath and anxious. Her ECG monitor pattern shows uncontrolled atrial fibrillation, with a rate ranging from 150 to 170 beats per minute. Her oxygen saturation level is 90%. 1. Given the assessment findings, what should you do first? 2. What additional physical assessment techniques would you perform? 3. Because the length of time the client has been in atrial fibrillation is unknown, what potential complication may occur if cardioversion is attempted? 4. Based on your answer for number 3, what should be done before elective cardioversion is attempted? 5. What other medical therapy might this client receive before elective cardioversion is done? 6. Later that evening, the client calls the nurse because she feels "like something terrible is going to happen." She complains of chest pain, has increased shortness of breath, and has coughed up blood-tinged sputum. What do you suspect? What is the first thing the nurse should do, and what further assessments should be performed at this time?


21 Please identify the rhythms and how to treat them.
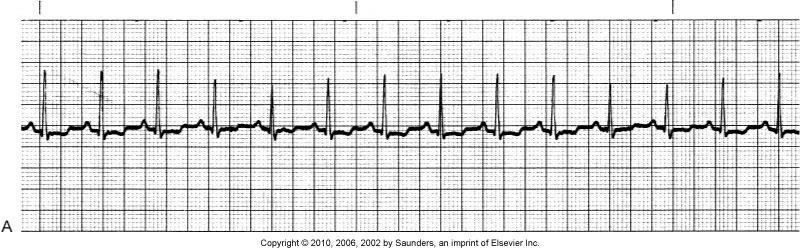
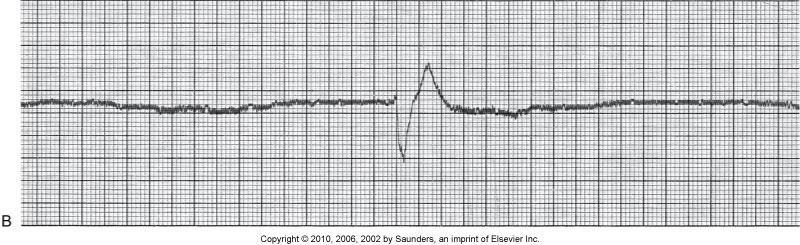
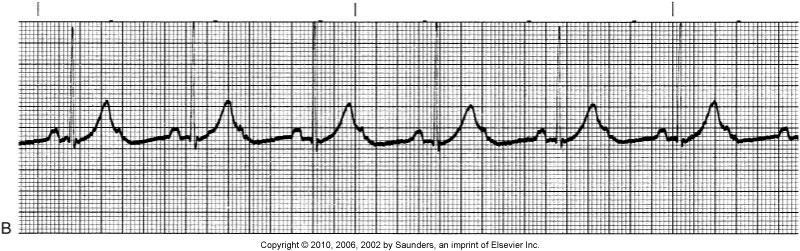
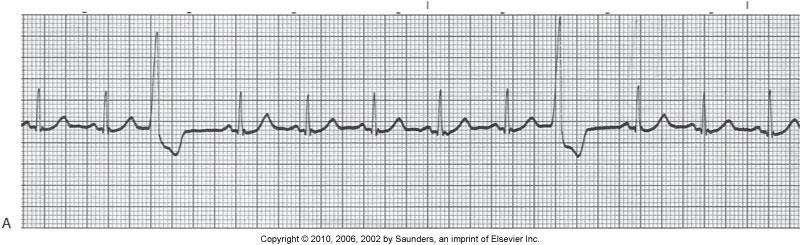
22
23 Week 3 Practice problems 1. Order-Dexamethasone 1 mg Drug available-dexamethasone 0.5 mg per tablet 2. Order-Tagamet 0.6g Drug available-tagamet 300 mg per tablet 3. Order-Phenobarbital 60 mg Drug available-phenobarbital 15 mg per tablet 4. Order-Ampicillin 0.5g Drug available-ampicillin 250 mg per 5 ml 5. Order-Dicloxacillin 125 mg Drug Available-Dicloxacillin 62.5 mg per 5 ml 6. Order-Medrol 75 mg IM Drug Available-Medrol 125 mg per 2 ml Practice Problems: Calculate how many drops per minute. 7. Order-1000 ml over 6 hrs IV set 15 gtts/ml 8. Order- 50mL over 20 min. IV set 15 gtts/ml 9. Order-100 ml over 20 min. IV set is 60 gtts/ml
24 CASE STUDY Chest Trauma and Acute Respiratory Distress Syndrome A 36-year-old woman is brought to the hospital following a head-on car accident. She was unrestrained and sustained a blunt injury to the chest from hitting the steering wheel. Initially, she is asymptomatic. Initial orders include a stat chest x-ray, arterial blood gases, and oxygen at 4 L/minute via Venturi mask. 1. What other assessments should be made when she arrives in the ED? 2. Gradually over the next 24 hours, she develops difficulty breathing, hypoxemia, and secretions increase. The nurse notifies the physician who orders an arterial blood gas and a chest x-ray. The chest x-ray obtained in the ED showed no abnormalities; however, the repeat x-ray now shows a hazy opacity in the lobes and the physician makes a diagnosis of pulmonary contusion. What physical assessments will accompany this diagnosis? 3. Arterial blood gas results show: Pao2 68 mm Hg, Paco2 32 mm Hg, and ph What do these values suggest? 4. What interventions should be implemented based on the laboratory results? 5. The patient temporarily responds to the high-flow oxygen therapy, but later the nurse notes that the patient demonstrates hyperpnea, grunting respiration, cyanosis, pallor, and intercostal and substernal retractions, with a change in mental status. The nurse suspects ARDS and calls the physician to obtain an order for which primary laboratory study used to establish this diagnosis? 6. Discuss the pathophysiology of ARDS. 7. The patient is intubated for respiratory failure. Describe how the nurse would secure the ET in place. 8. The patient is placed on a respirator with PEEP. Why is PEEP necessary? 9. Explain the rationale for the use of corticosteroids, antibiotics, and colloids in the management of the patient with ARDS.
25 Interventions for Critically Ill Patients with Respiratory Problems CRITICAL THINKING CHALLENGE The client is a 36-year-old woman who had a laminectomy yesterday for a ruptured lumbar disk. She has had pain for several months and has been unable to participate in her usual exercise program. She smokes one pack of cigarettes per day and drinks about two glasses of wine per week. Her other medications include oral contraceptives, ibuprofen PRN for joint and muscle pain, and sumatriptan(imitrex) several times a month for migraine headaches. When you go to assess her this morning, she tells you that she is nauseated and having some chest pain. 1. What risk factors does she have for a pulmonary embolism? 2. For what other clinical manifestations should you assess? 3. Is oxygen by mask appropriate for this client? Why or why not? 4. What other actions should you initiate? CRITICAL THINKING CHALLENGE 2 A patient with a PE is going home. She will continue warfarin therapy for at least 1 month. 1. What will you tell this client about warfarin therapy? 2. Is this client still at risk for a PE? Why or why not? 3. How can this client reduce her risk for PE?
26 NCLEX AND DECISION-MAKING CHALLENGES You are assigned to care for a 60-year-old woman who is in the medical intensive care unit (MICU) for community-acquired pneumonia requiring mechanical ventilation. She is a 1 pack per day (ppd) smoker and does not use alcohol or recreational drugs. Before admission, she had several days with shortness of breath (SOB), a productive cough, and generalized fatigue. While in the MICU, she was on strict bedrest because of mechanical ventilatory support. Her drugs include erythromycin for community-acquired pneumonia, hydromorphone (Dilaudid) as needed for pain, and acetaminophen (Tylenol) as needed for fever. Two hours ago, she was extubated, and the mechanical ventilation discontinued. As you begin your morning physical assessment, you notice that she is agitated, confused, and tachycardic, and has tachypneic breathing at 35 times per minute; her oxygen saturation by pulse oximetry is 86%. 1. What should be your first action? 2. What risk factors does she have for a pulmonary embolism? 3. For what other manifestations should you assess? 4. Is oxygen by mask appropriate for this patient? Why or why not? 5. What other actions should you take?
27 Week 4 Math Practice (Find the ml/hr) 1) Cardizem 250mg in 250ml of 0.9% NaCl to infuse at 10mg/hr 2) Heparin 25,000 units in 500ml 0.9% NaCl to infuse at 1150units/hr 3) Insulin 200 units in 100ml of 0.9% NaCl to infuse at 4units/hr 4) Lasix 200mg in 100ml of 0.9% NaCl to infuse at 2mg/hr 5) Dopamine 800mg in 250ml of D5%W to infuse at 10mcg/kg/min. The patient weighs 83kg. 6) Dobutamine 250mg in 250ml of D5%W to infuse at 10mcg/kg/min. The patient weighs 62kg. 7) Lidocaine 1G in 250ml of D5%W to infuse at 2mg/min 8) Nitroglycerine 50mg in 250ml D5%W to infuse at 10mcg/min
28 Case Study Hypovolemic Shock Case Study Andrew Jones is a 34 year old convenience store clerk who sustained a gunshot wound to the right chest during a robbery. When the paramedics arrive, his BP was barely palpable at 50 mmhg. His heart rate was 130, and his RR was 35. His skin was pale, cold, and clammy with delayed capillary refill, his radial pulse was weak and thready, and he was unresponsive. His respirations were deep and rapid and supplemental O2 was give via a 100% NRB. Two 14 gauge peripheral IV lines were started and LR was started wide open. Upon arrival in the ED, Mr. Jones SBP was 90 mmhg systolic, HR 120, and RR 26. He was restless and responded only to pain. His skin was pale and cool, and his capillary refill had a defined delay. His chest expansion was unequal and his breath sounds were grossly diminished on the right side. Chest Xray confirmed a right pneumothorax. Labs and a type and cross were drawn and sent. A 36F chest tube was inserted in the right 8 th intercostal space in the mid axillary line. Fifteen hundred ml of blood immediately evacuated, with continued bloody drainage up to 2500ml in 30 minutes. Mr. Jones admission ABG (on 100% NRB mask) and CBC were as follows: ph 7.21 Hgb 8.2 PaCO2 45 Hct 24.1 PaO2 91 Platlets 263 SaO2 95% RBC 2.17 HCO3 15 WBC 5.8 A foley catheter was inserted and 100ml clear yellow urine was drained. LR continued wide open and patient had received 6 liters IVF and 4 units of O- blood was rapidly infused over 30 minutes prior to going to the OR. In the OR a right thoracotomy with right pneumonectomy was performed, with repair to the right axillary artery. Mr. Jones received 14L of crystalloid, 20 units of PRBC, 6 units of FFP, and 10 units of Platelets. He was transferred to the CTCU. Upon arrival to the unit Mr. Jones is still sedated and intubated. He is hemodynamically stable with a BP 110/70, HR 96, and CVP of 10. His vent settings are AC 12, TV 700, FiO2 80%, Peep 5. He is not assisting ventilation at this time. His skin is warm and dry, pulses are palpable, and
29 capillary refill is normal. The nurse notes that his thoracotomy dressing is blood-soaked and diffuse oozing is apparent from all insertion sites. Significant clinical data are as follows: PT 18.7 Hgb 10.1 Platelets 108 PTT 71.9 Hct 32 RBC 4.6 Fibrinogen 78 WBC 6 1. Define hypovolemic shock. 2. Was Mr. Jones in hypovolemic shock when the paramedics arrived? What clinical manifestations of hypovolemic shock did he exhibit? 3. Why was LR the fluid of choice for Mr. Jones initial fluid resuscitation? 4. What other fluids might be considered in initial resuscitation of hypovolemic shock? 5. What is the preferred route of vascular access for fluid resuscitation in hypovolemic shock? 6. A CVP line is inserted in the patient s right subclavian vein during surgery. What are the potential complications of a CVP insertion? Four hours after admission to the CTCU, Mr. Jones BP dropped to 72/50, his HR rose to 120, and his CVP was 3mmHg. He received 2 L of LR over the next hour, at which time his BP was 86/60, HR 112, and CVP 5mmHg. His urine output for the last hour was 15 ml. A Pulmonary Artery Catheter was inserted. 7. Placement of a pulmonary artery catheter allows for accurate and detailed cardiopulmonary assessment. What hemodynamic alterations would be expected in hypovolemic shock? Mr. Jones initial hemodynamic profile revealed the following: CVP 2 CI 1.8 PAP 20/10 SVR 1420 PAWP 2 BP 88/66 CO 4
30 8. What therapy would be appropriate at this point? 9. During the initial resuscitative period, Mr. Jones received 4 units of PRBC. WHY? 10. What is autotransfusion? Would it be useful in this case? 11. What factors in Mr. Jones case indicate a coagulopathy? 12. What are other complications of massive blood transfusions? 13. When Mr. Jones arrived in the ED, his ph was 7.21, PaCO2 45, PaO2 91, and HCO3 15. What was his acid-base status? What was the etiology of the acid-base balance? 14. List the major compensatory mechanisms in hypovolemic shock and briefly explain each: a. Sympathetic Response b. Renin-Angiotensin-Aldosterone System c. Synthesis of Antidiuretic Hormone d. Body Fluid Shifts from Interstitial Spaces into the Intravascular Space e. Reverse Stress-Relaxation of Circulatory System 15. Mr. Jones hypovolemia resulted from hemorrhage. What are the common causes of hyovolemic shock? 16. What are the possible renal complications of hypovolemic shock? 17. What are the nursing diagnoses apply in this case?
31 CASE STUDY Cardiogenic Shock Case Study Mrs. Settles, a 50 year old woman, came to the emergency department at 0630 with complaining of being nauseous, achy, and just over all not feeling well for about 2 days. She decided to come to the ED because for the past 2 hours she has been is mildly diaphoretic, slightly short of breath, and she sates she is still nauseous. Upon, a quick assessment reveals bibasilar crackles, S 3 w/o a murmur, Sinus Tachycardia on the monitor and chest xray shows no abnormalities. VS are BP 156/98, HR 124, RR 34, O 2 sat 91 on RA, Temp is 37 C(98.6 F). Mrs. Settles has a history of HTN, stable angina, dyslipidemia, TAH, 20 year history of smoking cigarettes, she quit 10 years ago and Cervical CA 10 years ago. However, she revealed that for the past 3 weeks, she had experienced substernal pain radiating to her back with any type of activity. The pain would last for an hour but was relieved by sublingual NTG and rest. There is a family history of a brother dying form an MI and a sister with a history of 3 MI s. Patient takes the following medications daily: Aspirin 81mg daily Propranolol hydrochloride (Inderal LA) 80mg daily Isosorbide mononoitrate (Imdur SR) 30 mg daily Lisinopril (Zestril) 10mg daily Upon arrive to the ED an 18g IV was started in her right AC and labs were drawn and sent stat, NTG IV 50mg in 250 ml of D5W was started and titrated to the patient s pain level and blood pressure and to start a heparin gtt IV 25,000 Units in 250ml D5W using the cardiac weight based protocol. She was given Morphine Sulfate 2 mg IV push stat, and oxygen at 6L NC was started. You titrated the NTG gtt to 20mcg/min and bolus her with 5000 units IV push heparin and start the gtt at 1000 units/hour Labs results are: WBC 13.9 BUN 6 Cl 103 Glucose 117 Myoglobin 120 CK-MB 30 Hgb 15 K 4 CO 2 24 Hct 41.8 Troponin 0 Creatinine 0.9 Na minute later Mrs. Settles denies any pain and states she is feeling better. It is a very busy day in the ED and a patient just arrived having a stroke. An hour in a half later you go and check on
32 Mrs. Settles. The EKG technician came and did her 12 lead EKG and placed it in the file bin. You note that the 12 lead EKG reveals early Q waves and massive ST segment elevation in leads V 1 thur V 4. You note that the patient is having frequent multifocal PVC s on the monitor. You reassess the patient and note that she still has S 3, is SOB at rest, VS BP 160/102, HR 140, RR 30, O 2 sats 89% on 6LNC. You update the ED physician. Stat cardiac enzymes and arterial blood gases are drawn and the interventional cardiologist is consulted. Labs are: Myoglobin 150 CK-MB 36 Troponin 37 ph PO 2 60 PCO HCO You and the ED physician call a code MI. You change her oxygen to 100% NRB mask VS are BP140/100, HR 148, RR 34, O 2 93%. Dr. Heart and the cath lab team assess the patient. She is intubated with a #7 ETT 23 cm at the right lip by the anesthesiologist using propofol and etomidate. You start 2 more 18g IV. Mrs Settles is taken to the cardiac cath lab emergently. In the cath lab Mrs. Settles did have sustained run of v-tach which required defibrillation twice. She received 3 drug eluting stents to her LAD which was 100% occluded. A right heart catherazation was performed and revealed the following. Mrs. Settles EF was 12%, CO 2.5, CI 1.5, SVR 1800, PCWP 22, BP 90/48, HR 90. A Pulmonary Artery Catheter is placed along with an intra aortic balloon pump 1:1 timing. Mrs. Settles remained intubated. Upon arrival to the CCU these were the following orders. Start an amioderone gtt 900mg/500ml D5W 1mg/min for 6 hours then 0.5mg/min for the next 18 hours Phenylephrine 10mg/250ml D5W titrate to maintain MAP greater then 60 Versed gtt 50mg/50ml D5W titrate for a Ramsey score of 3 Maintain Heparin gtt using cardiac weight based protocol Lopressor 5mg IV push every 6 hours hold for SBP <90 or HR <60 Asprin 325mg NGT daily Plavix 75mg NGT daily Protonix 40mg IV daily Strict I&O Stat 12 lead EKG post procedure
33 1. What is the clinical presentation of a patient having an acute myocardial infarction? Identify Mrs. Settles clinical presentation to the ED. How may Mrs. Settles signs and symptoms differ from a man with the same diagnosis. 2. How is a diagnosis of AMI determined? Identify the results for Mrs. Settles that confirm the diagnoses of AMI. 3. What are the treatment goals for a patient with an AMI? 4. Discuss the role of thrombolytic therapy vs. interventional therapy for a patient having AMI. 5. Explain the use of Nitrates, Beta blockers, ACE inhibitors and anticoagulation in a patient with an AMI. 6. What complications are commonly seen after an MI? What are the most common complications seen with an anterior wall MI? 7. What significant 12 lead EKG changes are sometimes seen following an anterior wall MI? What 12 lead EKG changes occurred with Mrs. Settles? How often are EKG changes seen with a patient having an AMI? 8. Define cardiogenic shock and why it occurs after an anterior wall MI. What is the prognosis for a patient with cardiogenic shock? 9. What are the hemodynamic parameters seen in the patient with cardiogenic shock in comparison with normal hemodynamic parameters? 10. Discuss the goals of pharmacologic management in cardiogenic shock. Which medications were used for Mrs. Settles? 11. What type of mechanical support devices can be used for patients in cardigenic shock and why? Which type was used for Mrs. Settles? Identify any specific nursing responsibilities for the devices chosen for Mrs. Settles. 12. What are the nursing diagnoses for the patient in cardiogenic shock after and anterior wall MI? 13. Identify what process may have been a contributor to Mrs. Settles going into cardiogenic shock. How would you deal with that as a nurse?
34 CASE STUDY Septic Shock Case Study Emergency Department John Budd, a 72 year old arrived in the ED unconscious, with stab wounds to the upper right abdomen and lower right chest that were sustained in his home while fighting off a burglar. The paramedics secured 2 large bore IV sights in his right and left anticubital spaces and started LR wide open in both sites. An endotracheal tube was inserted, and ventilation with a resuscitation bag at 100% was begun. Medical anti shock trousers were in place. Pressure dressings to both wounds were secured. A 5 cm stab wound to his right lower chest and a 7.5 cm stab wound to his upper right abdomen was inspected. Chest tubes were inserted into the upper right and lower right mid axillary regions. Immediately, 500ml of red drainage returned via the lower chest tube. His heart rate was 125, ST without ectopy, BP 70/50, and he was placed on the mechanical ventilator and O2 saturations are 95% on 100% O2. A Foley catheter resulted in draining of 400 ml clear dark yellow urine. After infusion of more than 2000ml of LR solution, Mr. Budd was sent to surgery within 50 minutes of sustaining his injuries, still in a hypotensive state. Preoperative body eight was 74kg. Surgical Intervention During surgery, a right thoracotomy and right abdominal laparotomy were performed. The right chest wound was explored, and a lacerated intercostal artery was ligated. Exploration of his upper-right abdominal wound revealed more extensive damage. The liver and the duodenum were lacerated. Extensive hemorrhage and leaking of intestinal contents were apparent after opening the peritoneum. Mr. Budd s injuries were repaired, the peritoneal cavity was irrigated with antibiotic solution, and incisional sump drains were placed in the duodenum. During the 4 hour surgery, Mr. Budd received 6 units of PRBC and an additional 3 liters of LR. A pulmonary artery catheter and right radial a-line was inserted. ICU after Surgery Mr. Budd arrived to the ICU, he was on a mechanical ventilator settings were as follows. Assist Control with a rate of 12 FiO2 60% Tidal Volume 800ml
35 Vital Signs and hemodynamic parameters immediately after surgery were the following. BP 92/52 HR 114 Temp 97.2 PAP 20/8 PCWP 6mmHg CVP 4mmHg CO 5 CI 2.9 SVR 1040 Arterial Blood Gases are normal. WBC is 13 and hemoglobin 10, Mr. Budd s other lab values are within normal limits. Post op day 1 Mr. Budd remained drowsy and received vent support for 24 hours, then was extubated to 50% venti mask. His pain was controlled by morphine IV. The NGT continues to drain large amounts of green fluid, and an incisional duodenal sump tube drained large amounts of greenish brown fluid. His chest and abdominal dressings remained dry. Breath sounds were diminished on the right side but clear on the left. His chest tubes continued to drain small amounts of bloody fluid. Urine output was 40-60ml per hour. His abdomen was slightly firm and distended, and he had no bowel sounds. Post op Day 2 Mr. Budd s condition remained stable until today. At this time he became difficult to arouse but did respond to commands. His RR was 28 shallow and labored. His urine output is 20 ml per hour. His skin became war, dry, and flushed. Other clinical data included the following: BP 80/50 HR 132 Temp 97.2
36 PAP 14/7 PCWP 4mmHg CVP 2mmHg CO 8 L/min CI 4.7L/min/m 2 SVR 560 WBC 22 Glucose 270 Culture and sensitivity reports from wound drainage to indicated gram-negative bacilli. Intravenous antibiotics are administered, as well as IV hydrocortisone and naloxone (Narcan). A consult was placed for a nutritionist to formulate and calculate nutritional needs, and TPN was started. To prepare for the suspected hyperdynamic phase of septic shock, infusion of LR was increased to 150ml per hour, and dopamine at 7 mcg/kg/min was started with a concentration of 400mg/250 ml of D5W. Post op day 6 By day 6, Mr. Budd s condition had deteriorated dramatically. His skin was cool, mottled, and moist. His sclera were yellow tinged. He no longer responds to stimuli. A norepinephrine (levophed) drip was infused at 6mcg per min. with a concentration of 4 mg/250ml of D5W, along with a dopamine drip at 2mcg/kg/min continued. His monitor showed sinus tachycardia with short runs of Vtach. ST segment elevation, T wave inversion, and the development of Q waves over most of the anterior V leads on his 12 lead EKG. A 75mg bolus of lidocaine was given followed by a drip of 2mg/min with a concentration of 2g/500ml of D5W. His breath sounds revealed crackles throughout his chest. Urine output was 5ml/hour and was grossly bloody. His abdomen was enlarged and firm. His abdominal suture lines had dehisced, and the peritoneum could be seen. The duodenal sump and NGT drainage started to turn red. All arterial and venous puncture sites began oozing blood. Further clinical data included. BP 70/52 HR 140 RR14
37 Temp 96.4 PAP 44/26 PCWP 24mmHg CVP 8mmHg CO 2L/min CI 1.1L/min/m 2 SVR 2000 ph 7.14 Pco2 49 Po2 46 SaO2 85 Latic acid 14 Na 152 K 5.9 Creatinine 3.4 Amylase 290 Lipase 3.9 ALT 100 AST 82 FDP 39 Platelets 75 PT 22 PTT 98 Fibrinogen 130
38 CK 640 Troponin 50 Final Developments Despite attempts to reduce the afterload with sodium nitroprusside (Nipride) and increase contractility with Dobutamine, Mr. Budd s hemodynamic status failed even further. When his cardiac rhythm deteriorated into Vfib, resuscitation efforts were unsuccessful. An autopsy revealed several small abscessed areas in the lung, acute hepatic failure, multiple hemorrhagic areas, and an acute MI. 1. Discuss the magnitude of bacteremia and sepsis in hospitalized patients and the relationship between these two diagnoses. 2. What are the risk factors for infection and development of septic shock? Identify those that applied to Mr. Budd. 3. Discuss the rationale for use of a PAC in monitoring Septic Shock. 4. What organism most commonly cause septic shock? In which sites is an infection most often seen? 5. What pathophysiologic process occurs with septic shock? What are the effects of these processes on the patient s vascular tank, volume, and pump? 6. Discuss clinical, lab, and therapy changes that occurred on Mr. Budd second postoperative day. 7. What is the rational for each of the following therapeutic modalities ordered for Mr. Budd on the second postoperative day and calculate what the RN would set the IV pump at? Increased IV rate Dopamine Steroids Narcan TPN 8. Discuss the clinical changes that occurred during Mr. Budd s 6 th postoperative day.
Unit 8 Med Surg Nursing Quiz
 Unit 8 Med Surg Nursing Quiz 1. How will the nurse assess the flank area of a patient with pyelonephritis for tenderness? a. Push gently into the two lowest intercostal spaces. b. Palpate along both sides
Unit 8 Med Surg Nursing Quiz 1. How will the nurse assess the flank area of a patient with pyelonephritis for tenderness? a. Push gently into the two lowest intercostal spaces. b. Palpate along both sides
Subacute Care. 1. Define important words in the chapter. 2. Discuss the types of residents who are in a subacute setting
 175 26 Subacute Care 1. Define important words in this chapter 2. Discuss the types of residents who are in a subacute setting 3. List care guidelines for pulse oximetry 4. Describe telemetry and list
175 26 Subacute Care 1. Define important words in this chapter 2. Discuss the types of residents who are in a subacute setting 3. List care guidelines for pulse oximetry 4. Describe telemetry and list
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
University of South Dakota Vermillion, South Dakota Department of Nursing
 Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Surgical Treatment. Preparing for Your Child s Surgery
 Surgical Treatment Preparing for Your Child s Surgery If your child needs an operation, it will be performed at a hospital that has special expertise in heart surgery for children. This may be a hospital
Surgical Treatment Preparing for Your Child s Surgery If your child needs an operation, it will be performed at a hospital that has special expertise in heart surgery for children. This may be a hospital
 Unfolding Clinical Reasoning Case Study: STUDENT Sepsis I. Data Collection History of Present Problem: Jean Kelly is an 82 year old woman who has been feeling more fatigued for the last three days and
Unfolding Clinical Reasoning Case Study: STUDENT Sepsis I. Data Collection History of Present Problem: Jean Kelly is an 82 year old woman who has been feeling more fatigued for the last three days and
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Student name: Section: Date: Patient initials: Time began: Time ended: Points: Faculty: Points deducted due to:
 MEDICATION ACTIVITY This is a timed medication administration check off. It is worth 6 points. It is divided into 3 points for clinical reasoning, being able to correctly identify which meds should be
MEDICATION ACTIVITY This is a timed medication administration check off. It is worth 6 points. It is divided into 3 points for clinical reasoning, being able to correctly identify which meds should be
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Neighborhood Hospital
 Physician Progress Notes Time Mon S/P HoLEP Procedure without complications; estimated blood loss < 100 ml; stable condition to recovery room. 1530 To be admitted to Urology following PACU. Dan Stein,
Physician Progress Notes Time Mon S/P HoLEP Procedure without complications; estimated blood loss < 100 ml; stable condition to recovery room. 1530 To be admitted to Urology following PACU. Dan Stein,
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Returned Missionary Study Guide
 Returned Missionary Study Guide Skills to Refresh if Returning to Capstone: 1st Semester skills Head to Toe Assessment (Need to be able to document each of these.) o Vital Signs BP Pulse Respirations Temperature
Returned Missionary Study Guide Skills to Refresh if Returning to Capstone: 1st Semester skills Head to Toe Assessment (Need to be able to document each of these.) o Vital Signs BP Pulse Respirations Temperature
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition
 Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
HEALTH PROFESSIONS NURSING PROGRAM
 HEALTH PROFESSIONS NURSING PROGRAM ALTERATIONS IN HEALTH IV NRS 235 Lab Manual Fall 2018 1 Welcome to NRS 235! This will be an exciting course for you because you will be building on the concepts that
HEALTH PROFESSIONS NURSING PROGRAM ALTERATIONS IN HEALTH IV NRS 235 Lab Manual Fall 2018 1 Welcome to NRS 235! This will be an exciting course for you because you will be building on the concepts that
HEALTH PROFESSIONS NURSING PROGRAM
 HEALTH PROFESSIONS NURSING PROGRAM ALTERATIONS IN HEALTH IV NRS 235 Lab Manual Spring 2018 1 Welcome to NRS 235! This will be an exciting course for you because you will be building on the concepts that
HEALTH PROFESSIONS NURSING PROGRAM ALTERATIONS IN HEALTH IV NRS 235 Lab Manual Spring 2018 1 Welcome to NRS 235! This will be an exciting course for you because you will be building on the concepts that
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
PATIENT MOVEMENT RECORD DATA PROTECTED BY PRIVACY ACT OF 1974
 SECTION I PATIENT MOVEMENT RECORD DATA PROTECTED BY PRIVACY ACT OF 1974 PERMANENT MEDICAL RECORD (S) - Information needed to submit patient movement record PATIENT IDENTIFICATION (s) NAME (Last, First,
SECTION I PATIENT MOVEMENT RECORD DATA PROTECTED BY PRIVACY ACT OF 1974 PERMANENT MEDICAL RECORD (S) - Information needed to submit patient movement record PATIENT IDENTIFICATION (s) NAME (Last, First,
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
CVICU. Attending feedback in the course of patient care. Assessment of clinical decisions Observation on Rounds. Annual In-service evaluation
 ACGME Competency-based Goals and Objectives ROTATION Cardiovascular Critical Care Unit, PGY 4, 5, 6 CVICU Goal 1. Develop a comprehensive and physiology-based understanding of evolving illness in children
ACGME Competency-based Goals and Objectives ROTATION Cardiovascular Critical Care Unit, PGY 4, 5, 6 CVICU Goal 1. Develop a comprehensive and physiology-based understanding of evolving illness in children
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
CRITICAL THINKING IN THE ICU: IMPLEMENTING BEST PRACTICES. Your Presenter: Carol Lynn Esposito, Ed.D., JD, MS, RN
 CRITICAL THINKING IN THE ICU: IMPLEMENTING BEST PRACTICES Your Presenter: Carol Lynn Esposito, Ed.D., JD, MS, RN NYSNA is accredited as a provider of continuing nursing education by the American Nurses
CRITICAL THINKING IN THE ICU: IMPLEMENTING BEST PRACTICES Your Presenter: Carol Lynn Esposito, Ed.D., JD, MS, RN NYSNA is accredited as a provider of continuing nursing education by the American Nurses
About the Critical Care Center
 Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Using Study Strategies Specific to Alternate Format Questions. What you need to know to answer a question correctly:
 Using Study Strategies Specific to Alternate Format Questions Marnie Kramer-Kile RN, PhD What you need to know to answer a question correctly: Basic content knowledge Ability to combine concepts Ability
Using Study Strategies Specific to Alternate Format Questions Marnie Kramer-Kile RN, PhD What you need to know to answer a question correctly: Basic content knowledge Ability to combine concepts Ability
Outpatient/Community Health Nursing
 2043_Ch08_125-144.qxd 9/25/08 3:37 PM Page 125 8 Outpatient/Community Health Nursing Intuition will tell the thinking mind where to look next. Jonas Salk ABBREVIATION LIST ACE AHA BP D5W ECG GERD HCP H&H
2043_Ch08_125-144.qxd 9/25/08 3:37 PM Page 125 8 Outpatient/Community Health Nursing Intuition will tell the thinking mind where to look next. Jonas Salk ABBREVIATION LIST ACE AHA BP D5W ECG GERD HCP H&H
2016 SUMMER STUDENT NURSE EXTERNSHIP PROGRAM SKILLS CHECK LIST
 2016 SUMMER STUDENT NURSE EXTERNSHIP PROGRAM SKILLS CHECK LIST STUDENT NURSE EXTERNNAME SCHOOL OF NURSING STUDENT AGREEMENT: I request the Clinical Skills Check list be released to (hospital/agency). I
2016 SUMMER STUDENT NURSE EXTERNSHIP PROGRAM SKILLS CHECK LIST STUDENT NURSE EXTERNNAME SCHOOL OF NURSING STUDENT AGREEMENT: I request the Clinical Skills Check list be released to (hospital/agency). I
RECOMMENDATION FOR CONSIDERATION
 Board Meeting Date: June 15, 2016 RECOMMENDATION FOR CONSIDERATION Subject: Critical Care Transfer of Care Data Elements and Form VTR#: 0616-04 Committee/Task Force: Critical Care Transport Task Force
Board Meeting Date: June 15, 2016 RECOMMENDATION FOR CONSIDERATION Subject: Critical Care Transfer of Care Data Elements and Form VTR#: 0616-04 Committee/Task Force: Critical Care Transport Task Force
NUR 181 PHYSICAL ASSESSMENT PREPARATION FOR UNIT 1 MODULE
 NUR 181 PHYSICAL ASSESSMENT PREPARATION FOR UNIT 1 MODULE This Module is intended to give you a head start as you begin the Physical Assessment course in the Bergen Community College Nursing Program. The
NUR 181 PHYSICAL ASSESSMENT PREPARATION FOR UNIT 1 MODULE This Module is intended to give you a head start as you begin the Physical Assessment course in the Bergen Community College Nursing Program. The
NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination.
 NURSING CARE PLAN NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination. Goal: Provision of fluid balance. Demonstrate adequate hydration as evidenced by stable vital signs, palpable
NURSING CARE PLAN NURSING DIAGNOSIS: Risk for fluid volume deficit related to frequent urination. Goal: Provision of fluid balance. Demonstrate adequate hydration as evidenced by stable vital signs, palpable
Medication Calculation Practice Problems LEVEL II, III and IV 1. The order reads for digoxin mg IM daily. Available to the nurse is digoxin
 Medication Calculation Practice Problems LEVEL II, III and IV 1. The order reads for digoxin 0.125 mg IM daily. Available to the nurse is digoxin 0.25 mg/ml. The nurse would administer how many ml s? 2.
Medication Calculation Practice Problems LEVEL II, III and IV 1. The order reads for digoxin 0.125 mg IM daily. Available to the nurse is digoxin 0.25 mg/ml. The nurse would administer how many ml s? 2.
Clinic al Pathway: Ventricular Septal Defect (VSD) Repair
 Repair") Clinic al Pathway: Ventricular Septal Defect (VSD) Repair Notes: (1) This pathway is a general guideline and variations can occur based on professional judgment to meet individual patient needs. (2) This
Clinic al Pathway: Ventricular Septal Defect (VSD) Repair Notes: (1) This pathway is a general guideline and variations can occur based on professional judgment to meet individual patient needs. (2) This
NUR 203 BURNS CASE STUDY CHAPTER 25 SPRING 2016
 NUR 203 BURNS CASE STUDY CHAPTER 25 SPRING 2016 You are working in the emergency department (ED) of a community hospital when the ambulance arrives with A.N., a 28-year-old woman who was involved in a
NUR 203 BURNS CASE STUDY CHAPTER 25 SPRING 2016 You are working in the emergency department (ED) of a community hospital when the ambulance arrives with A.N., a 28-year-old woman who was involved in a
Cyclophosphamide INFUSION Infusion 4 Plus
 Cyclophosphamide Infusion Day DEPARTMENT OF RHEUMATOLOGY DAY CASE ADMISSION RECORD PATIENT DAY CASE BOOKING REQUEST To be completed by Consultant, Registrar requesting day case Admission Hospital No. Forename
Cyclophosphamide Infusion Day DEPARTMENT OF RHEUMATOLOGY DAY CASE ADMISSION RECORD PATIENT DAY CASE BOOKING REQUEST To be completed by Consultant, Registrar requesting day case Admission Hospital No. Forename
Enhanced Recovery Programme
 Enhanced Recovery Programme Page 14 Contact details South Tyneside NHS Foundation Trust Harton Lane South Shields Tyne and Wear NE34 0PL For advice please contact ward 1 on 4041001 Or ward 3 on 0191 4041003.
Enhanced Recovery Programme Page 14 Contact details South Tyneside NHS Foundation Trust Harton Lane South Shields Tyne and Wear NE34 0PL For advice please contact ward 1 on 4041001 Or ward 3 on 0191 4041003.
A PATIENT S GUIDE TO UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES. By Maureen Kroning EdD, RN
 A PATIENT S GUIDE TO UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES By Maureen Kroning EdD, RN Dedication This handbook is dedicated to patients, families, communities and the nurses that touch their lives
A PATIENT S GUIDE TO UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES By Maureen Kroning EdD, RN Dedication This handbook is dedicated to patients, families, communities and the nurses that touch their lives
Faculty of Social and Health Sciences Department of Nursing Bachelor of Nursing HEAL6011 NURSING PRACTICE OLDER ADULT SEMESTER GROUP 3
 Faculty of Social and Health Sciences Department of Nursing Bachelor of Nursing HEAL6011 NURSING PRACTICE OLDER ADULT SEMESTER 1 2016 GROUP 3 End of Course Summative Exam QUESTION BOOKLET Weighting: 60%
Faculty of Social and Health Sciences Department of Nursing Bachelor of Nursing HEAL6011 NURSING PRACTICE OLDER ADULT SEMESTER 1 2016 GROUP 3 End of Course Summative Exam QUESTION BOOKLET Weighting: 60%
University of South Dakota Vermillion, South Dakota Department of Nursing. Simulation Scenario Complex Patient: Acute MI. Overview
 Simulation Scenario Complex Patient: Acute MI Overview Title: Acute MI with Dysrhythmias Concept: Complex Patient To cite this reference: Target Group: Second Year Nursing Students Kisner, T. & Warren,
Simulation Scenario Complex Patient: Acute MI Overview Title: Acute MI with Dysrhythmias Concept: Complex Patient To cite this reference: Target Group: Second Year Nursing Students Kisner, T. & Warren,
Goals & Objectives 4/17/2014 UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN. Why would someone need to do this?
 By Maureen Kroning, EdD, RN. Why would someone need to do this?") UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN Goals & Objectives Participants will increase their knowledge about AHCD Review AHCD documents used at the hospital Role
UNDERSTANDING ADVANCE HEALTH CARE DIRECTIVES (AHCD) By Maureen Kroning, EdD, RN Goals & Objectives Participants will increase their knowledge about AHCD Review AHCD documents used at the hospital Role
2. Unlicensed assistive personnel: any personnel to whom nursing tasks are delegated and who work in settings with structured nursing organizations.
 XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
DRAFT. WORKING DRAFT Nursing associate skills annexe. Part of the draft standards of proficiency for nursing associates. Page 1
 WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
UW MEDICINE PATIENT EDUCATION. Angiography: Kidney Exam. How to prepare and what to expect. What is angiography? DRAFT. Why do I need this exam?
 UW MEDICINE PATIENT EDUCATION Angiography: Kidney Exam How to prepare and what to expect This handout explains how to prepare and what to expect when having a kidney exam using angiography. What is angiography?
UW MEDICINE PATIENT EDUCATION Angiography: Kidney Exam How to prepare and what to expect This handout explains how to prepare and what to expect when having a kidney exam using angiography. What is angiography?
N: Emergency Nursing. Alberta Licensed Practical Nurses Competency Profile 135
 N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
Simulation Design Template. Location for Reflection:
 Simulation Design Template Date: Discipline: Expected Simulation Run Time: Location: Admission Date: Today s Date: Brief Description of Client Name: Gender: Age: Race: File Name: Student Level: Guided
Simulation Design Template Date: Discipline: Expected Simulation Run Time: Location: Admission Date: Today s Date: Brief Description of Client Name: Gender: Age: Race: File Name: Student Level: Guided
TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry
 TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry DEPARTMENT: PERSONNEL: Telemetry Telemetry Personnel EFFECTIVE DATE: 6/86 REVISED: 02/00, 4/10, 12/14 Admission Procedure: 1. The admitting
TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry DEPARTMENT: PERSONNEL: Telemetry Telemetry Personnel EFFECTIVE DATE: 6/86 REVISED: 02/00, 4/10, 12/14 Admission Procedure: 1. The admitting
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
Skills/Experience Checklist Home Health Registered Nurse
 This form is a self-assessment of your current skills and abilities. This form is also used to document skill demonstration. EMPLOYEE PROFILE Last Name First Name Middle Initial Employee Number Direct
This form is a self-assessment of your current skills and abilities. This form is also used to document skill demonstration. EMPLOYEE PROFILE Last Name First Name Middle Initial Employee Number Direct
Sepsis/Septic Shock Pre-Hospital Care
 Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Initial Pool Process: Resident Interview
 Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
During the hospital medicine rotation, residents will focus on the following procedures as permitted by case mix:
 Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Al al-bayt University. Nursing Faculty. Adult Health Nursing-1 ( ) Course Syllabus
 Course Syllabus") Al al-bayt University Nursing Faculty Adult Health Nursing-1 (1001221) Course Syllabus 2009/2010 1 Course Title: Adult Health Nursing-1 (1001221) Credit Hours: 3 Hours. Pre-requisite: (1001171) Date: first
Al al-bayt University Nursing Faculty Adult Health Nursing-1 (1001221) Course Syllabus 2009/2010 1 Course Title: Adult Health Nursing-1 (1001221) Credit Hours: 3 Hours. Pre-requisite: (1001171) Date: first
Contents. Welcome to the Cath Lab P4/5
 Contents Welcome to the Cath Lab Preparation Instructions : information to ensure you are ready for your procedure in the Cath Lab, set out for you as questions (Q) and answers (A) How the day will go
Contents Welcome to the Cath Lab Preparation Instructions : information to ensure you are ready for your procedure in the Cath Lab, set out for you as questions (Q) and answers (A) How the day will go
Course Outline and Assignments
 Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
Facilitation Interns Acquisition of
 Facilitation Interns Acquisition of Medical Knowledge and Core Skills through Experiential Learning Raquel Belforti, DO, Kevin Hinchey, MD Reham Shaaban, DO Mihaela Stefan, MD Baystate Medical Center Tufts
Facilitation Interns Acquisition of Medical Knowledge and Core Skills through Experiential Learning Raquel Belforti, DO, Kevin Hinchey, MD Reham Shaaban, DO Mihaela Stefan, MD Baystate Medical Center Tufts
Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair
 or Atrial Septal Defect (ASD) Repair") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
Texas Concept-Based Curriculum NTCC ADN Program RNSG 1216 Professional Nursing Competencies Fall 2015
 SEMESTER HOURS 2 CONTACT HOURS LAB: 8 PREREQUISITES: ADMISSION TO ADN PROGRAM COREQUISITES: RNSG 1125, 1128, 1430, 1161 Course Description Development of professional nursing competencies in the care of
SEMESTER HOURS 2 CONTACT HOURS LAB: 8 PREREQUISITES: ADMISSION TO ADN PROGRAM COREQUISITES: RNSG 1125, 1128, 1430, 1161 Course Description Development of professional nursing competencies in the care of
Laparoscopic partial nephrectomy
 Laparoscopic partial nephrectomy This leaflet is written to give you information and answer questions you may have about your surgery. If you have any further questions, please speak to your doctor or
Laparoscopic partial nephrectomy This leaflet is written to give you information and answer questions you may have about your surgery. If you have any further questions, please speak to your doctor or
CLINICAL SKILLS & OBSERVATION CHECKLIST
 CLINICAL SKILLS & OBSERVATION CHECKLIST Employee: Please check Yes or No at time of hire and annually for Adult and/or Pediatric experience RN Supervisor: Please date and initial after observation & demonstration
CLINICAL SKILLS & OBSERVATION CHECKLIST Employee: Please check Yes or No at time of hire and annually for Adult and/or Pediatric experience RN Supervisor: Please date and initial after observation & demonstration
NM DDSD Intensive Medical Living Services Eligibility Parameter Tool A. MEDICATION ADMINISTRATION SEVERE 4 SIGNIFICANT 3 MODERATE 2 LOW 1 NONE - 0
 FACT Scheduled Medications: Note: Any injections provided by Home Health, Hospice or other clinical providers may not be included in these totals for the agency nursing time. Do not include delivery of
FACT Scheduled Medications: Note: Any injections provided by Home Health, Hospice or other clinical providers may not be included in these totals for the agency nursing time. Do not include delivery of
2. Unlicensed assistive personnel: any personnel to whom nursing tasks are delegated and who work in settings with structured nursing organizations.
 XVII. MANAGEMENT AND DELEGATION A. General Information: The judgments that you make in management and delegation situations have to be based on knowledge. You MUST know your content, and then you can move
XVII. MANAGEMENT AND DELEGATION A. General Information: The judgments that you make in management and delegation situations have to be based on knowledge. You MUST know your content, and then you can move
UW MEDICINE PATIENT EDUCATION. Angiography: Percutaneous Gastrostomy. What to expect when you have a G-tube. What is a percutaneous gastrostomy?
 UW MEDICINE PATIENT EDUCATION Angiography: Percutaneous Gastrostomy What to expect when you have a G-tube This handout explains a percutaneous gastrostomy tube and what to expect when you have one. What
UW MEDICINE PATIENT EDUCATION Angiography: Percutaneous Gastrostomy What to expect when you have a G-tube This handout explains a percutaneous gastrostomy tube and what to expect when you have one. What
UW MEDICINE PATIENT EDUCATION. Angiography: Percutaneous or Transjugular Liver Biopsy. How to prepare and what to expect. What is a liver biopsy?
 UW MEDICINE PATIENT EDUCATION Angiography: Percutaneous or Transjugular Liver Biopsy How to prepare and what to expect This handout explains how to prepare and what to expect when having a percutaneous
UW MEDICINE PATIENT EDUCATION Angiography: Percutaneous or Transjugular Liver Biopsy How to prepare and what to expect This handout explains how to prepare and what to expect when having a percutaneous
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Medication Math Homework Part 1. Part A. Convert the following patient weights from pounds to kilograms lbs lbs. 6.
 Medication Math Homework Part 1 Part A. Convert the following patient weights from pounds to kilograms 1. 22 lbs 4. 150 lbs 7. 250 lbs 2. 80 lbs 5. 180 lbs 8. 300 lbs 3. 100 6. 200 lbs 9. 35 lbs Part B.
Medication Math Homework Part 1 Part A. Convert the following patient weights from pounds to kilograms 1. 22 lbs 4. 150 lbs 7. 250 lbs 2. 80 lbs 5. 180 lbs 8. 300 lbs 3. 100 6. 200 lbs 9. 35 lbs Part B.
Blood and Blood Products Administration
 NCAL Patient Care Services 2016 Blood and Blood Products Administration Objectives: On completing this module, you will be able to: Identify blood group systems Describe compatibility requirements List
NCAL Patient Care Services 2016 Blood and Blood Products Administration Objectives: On completing this module, you will be able to: Identify blood group systems Describe compatibility requirements List
Protocol: Name of supervising ED provider: Name of RDTC Faculty: Disposition: Date: / / Time: : (military)
") RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Proactive Care Team Contingency Plan Original completed: Patient Details. Frameworki Number: First Name: Margaret Lives Alone: Yes No
 Proactive Care Team Contingency Plan Original completed: Patient Details Surname: Jones NHS Number: Frameworki Number: First Name: Margaret Lives Alone: Yes No Known As: Maggie Key safe: Yes No Number
Proactive Care Team Contingency Plan Original completed: Patient Details Surname: Jones NHS Number: Frameworki Number: First Name: Margaret Lives Alone: Yes No Known As: Maggie Key safe: Yes No Number
CARDIAC DISORDERS COMPREHENSIVE EXAMINATION
 2504_Ch03_073-112.qxd 102 11/4/10 9:45 PM Page 102 MED-SURG SUCCESS CARDIAC DISORDERS COMPREHENSIVE EXAMINATION 1. Which population is at a higher risk for dying from a myocardial infarction? 1. Caucasian
2504_Ch03_073-112.qxd 102 11/4/10 9:45 PM Page 102 MED-SURG SUCCESS CARDIAC DISORDERS COMPREHENSIVE EXAMINATION 1. Which population is at a higher risk for dying from a myocardial infarction? 1. Caucasian
You will be having surgery to remove a the distal or tail part of your pancreas.
 Distal pancreatectomy You will be having surgery to remove a the distal or tail part of your pancreas. This handout will help you learn about the surgery, how to prepare for surgery and your care after
Distal pancreatectomy You will be having surgery to remove a the distal or tail part of your pancreas. This handout will help you learn about the surgery, how to prepare for surgery and your care after
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
Your Hospital Stay After Your TAVR
 UW MEDICINE PATIENT EDUCATION Your Hospital Stay After Your TAVR What to expect This handout explains what to expect during your hospital stay after your transcatheter aortic valve replacement (TAVR).
UW MEDICINE PATIENT EDUCATION Your Hospital Stay After Your TAVR What to expect This handout explains what to expect during your hospital stay after your transcatheter aortic valve replacement (TAVR).
ACCOUNT NO. MED. REC. NO. NAME BIRTHDATE. Patient Identification ALL ORDERS MUST BE MARKED IN INK WITH A CHECKMARK ( ) TO BE ACTIVE.
 TO BE ACTIVE.") PO7071 *PO7071* Page 1 of 4 ALL MUST BE MARKED IN INK WITH A CHECKMARK ( ) TO BE ACTIVE. Weight: kg Height: cm Allergies: Treatment Start Date: Date(s) of Transfusion(s): Current Labs: WBC: Hgb/Hct: Platelets:
PO7071 *PO7071* Page 1 of 4 ALL MUST BE MARKED IN INK WITH A CHECKMARK ( ) TO BE ACTIVE. Weight: kg Height: cm Allergies: Treatment Start Date: Date(s) of Transfusion(s): Current Labs: WBC: Hgb/Hct: Platelets:
CHALLENGE OF NURS 205 (DRUG DOSAGE CALCULATION) AND/OR NURS 212 (PHARMACOLOGY FOR NURSES) BY EXAM
 AND/OR NURS 212 (PHARMACOLOGY FOR NURSES) BY EXAM") CONTRA COSTA COLLEGE LAVA DIVISION ASSOCIATE DEGREE NURSING PROGRAM CHALLENGE OF NURS 205 (DRUG DOSAGE CALCULATION) AND/OR NURS 212 (PHARMACOLOGY FOR NURSES) BY EXAM POLICY: A nursing applicant who has
CONTRA COSTA COLLEGE LAVA DIVISION ASSOCIATE DEGREE NURSING PROGRAM CHALLENGE OF NURS 205 (DRUG DOSAGE CALCULATION) AND/OR NURS 212 (PHARMACOLOGY FOR NURSES) BY EXAM POLICY: A nursing applicant who has
Royal Alexandra Hospital Emergency Department Nurse Initiated Protocol
 Royal Alexandra Hospital Emergency Department Nurse Initiated Protocol ACETAMINOPHEN FOR PAIN, DISCOMFORT AND/OR FEVER PROTOCOL APPROVING AUTHORITY EMERGENCY MEDICINE SITE CHIEF: DR COLIN PETERSON EXECUTIVE
Royal Alexandra Hospital Emergency Department Nurse Initiated Protocol ACETAMINOPHEN FOR PAIN, DISCOMFORT AND/OR FEVER PROTOCOL APPROVING AUTHORITY EMERGENCY MEDICINE SITE CHIEF: DR COLIN PETERSON EXECUTIVE
Preparing for Thoracic Surgery and Recovery
 Division of Thoracic Surgery Preparing for Thoracic Surgery and Recovery A Guide for Patients and Families Brigham And Women s/faulkner Hospitals Important Phone Numbers Important Phone Numbers BWH NUMBERS
Division of Thoracic Surgery Preparing for Thoracic Surgery and Recovery A Guide for Patients and Families Brigham And Women s/faulkner Hospitals Important Phone Numbers Important Phone Numbers BWH NUMBERS
Brief Summary. Educational Rationale. Learning Objectives: Nurse. Learning Objectives: Doctor
 Simulation Scenario Title Bacterial meningitis Version 10 Target Audience FY doctors & student nurses Run time 10-15 mins Authors Niamh Feely, Andrew Smith, Udesh Naidoo, Paul Wilder, Mark Loughrey Last
Simulation Scenario Title Bacterial meningitis Version 10 Target Audience FY doctors & student nurses Run time 10-15 mins Authors Niamh Feely, Andrew Smith, Udesh Naidoo, Paul Wilder, Mark Loughrey Last
Accountability and Collaboration Working With A Physician Assistant
 Accountability and Collaboration Working With A Physician Assistant Anthony Derro, RN Practice Consultant Linda Levesque, RN Outreach Consultant, Acute Care Karen Riddell, Director, Professional Practice
Accountability and Collaboration Working With A Physician Assistant Anthony Derro, RN Practice Consultant Linda Levesque, RN Outreach Consultant, Acute Care Karen Riddell, Director, Professional Practice
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
The STEMI ALERT Packet
 The STEMI ALERT Packet (At a PCI-capable institution) Use of a STEMI ALERT Packet is a key step in optimizing treatment of the STEMI patient. Opening a STEMI ALERT Packet upon first recognition of STEMI
The STEMI ALERT Packet (At a PCI-capable institution) Use of a STEMI ALERT Packet is a key step in optimizing treatment of the STEMI patient. Opening a STEMI ALERT Packet upon first recognition of STEMI
University of South Dakota Vermillion, South Dakota Department of Nursing. Simulation Scenario Leadership: Triage/Prioritization (Part 1) Overview
 Overview") Title: To cite this reference: Triage/Prioritization (Part 1 of 2) University of South Dakota Simulation Scenario Leadership: Triage/Prioritization (Part 1) Overview Target Group: Second Year Concept:
Title: To cite this reference: Triage/Prioritization (Part 1 of 2) University of South Dakota Simulation Scenario Leadership: Triage/Prioritization (Part 1) Overview Target Group: Second Year Concept:
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool
 Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Improving Patient Surveillance: Instituting a Respiratory Risk Screening Tool Sandra Maddux, RN, MSN, CNS-BC, Michelle Giffin, RN, BSN, & Patti Leglar, RN-C, BSN Purpose To share an evidence-based protocol
Circumstances of Injury: Cause of burn %Burn Smoke Inhalation: Yes No How accident happened:
 Shriners Hospitals for Children Date: Galveston Burn Hospital Time: 815 Market Street Resource: Galveston, Texas 77550 Contact: Referral Calls: 409-770-6773 Fax #: 409-770-6539 Patient Name: Sex: Home
Shriners Hospitals for Children Date: Galveston Burn Hospital Time: 815 Market Street Resource: Galveston, Texas 77550 Contact: Referral Calls: 409-770-6773 Fax #: 409-770-6539 Patient Name: Sex: Home
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
Simulation Design Template
 Simulation Design Template Date: May 7/8, 2008 File Name: Discipline: RN, Charge nurse, medical radiology, pharmacy tech, social work, medicine (whatever is available at the institution) Student Level:
Simulation Design Template Date: May 7/8, 2008 File Name: Discipline: RN, Charge nurse, medical radiology, pharmacy tech, social work, medicine (whatever is available at the institution) Student Level:
CPNE. Clinical Performance in Nursing Examination Study Guide 21 st Edition SUMMARY
 CPNE Clinical Performance in Nursing Examination Study Guide 21 st Edition SUMMARY Effective NOVEMBER 2014 2 CONTENTS Clinical Performance in Nursing Examination 3 Summary Description 3 Peripheral Neurovascular
CPNE Clinical Performance in Nursing Examination Study Guide 21 st Edition SUMMARY Effective NOVEMBER 2014 2 CONTENTS Clinical Performance in Nursing Examination 3 Summary Description 3 Peripheral Neurovascular
Patient s Care Path Note: Welcome to Providence Orthopaedic & NeuroSpine TOTAL HIP ARTHROPLASTY. Questions/Concerns. Midlands. Orthopaedics, P.A.
 TOTAL HIP ARTHROPLASTY Welcome to Providence Orthopaedic & NeuroSpine Institute. You are scheduled for surgery on your hip. The Care Path is a guide designed to help you and your family know what to expect
TOTAL HIP ARTHROPLASTY Welcome to Providence Orthopaedic & NeuroSpine Institute. You are scheduled for surgery on your hip. The Care Path is a guide designed to help you and your family know what to expect
Staff Relief Nursing Assistant/Orderly Test
 Staff Relief Nursing Assistant/Orderly Test Directions: Select the one best answer. Indicate your choice by entering the letter on the answer sheet provided. Administered To: Nurse Assistant/Orderly providing
Staff Relief Nursing Assistant/Orderly Test Directions: Select the one best answer. Indicate your choice by entering the letter on the answer sheet provided. Administered To: Nurse Assistant/Orderly providing
Skilled Nursing Facility Admission Orders
 Diagnosis Allergies SNF Admission- Required SNF Regulatory Admit to Skilled Nursing Facility Date: All orders good for 45 days unless otherwise indicated Follow Up Appointment Follow up appointment(s):
Diagnosis Allergies SNF Admission- Required SNF Regulatory Admit to Skilled Nursing Facility Date: All orders good for 45 days unless otherwise indicated Follow Up Appointment Follow up appointment(s):
UW MEDICINE PATIENT EDUCATION. How to prepare and what to expect DRAFT. What is an IVC filter?
 UW MEDICINE PATIENT EDUCATION Angiography: Inferior Vena Cava (IVC) Filter How to prepare and what to expect This handout explains what an inferior vena cava filter is and what to expect when you have
UW MEDICINE PATIENT EDUCATION Angiography: Inferior Vena Cava (IVC) Filter How to prepare and what to expect This handout explains what an inferior vena cava filter is and what to expect when you have
Minimally Invasive Surgery (MIS) and Open Nephrectomy
 and Open Nephrectomy") P ATIENT INFORMATION Minimally Invasive Surgery (MIS) and Open Nephrectomy (Partial, Radical and Donor) Please bring this book to the hospital on the day of your surgery THE OTTAWA HOSPITAL CP 95 B (03/2013)
P ATIENT INFORMATION Minimally Invasive Surgery (MIS) and Open Nephrectomy (Partial, Radical and Donor) Please bring this book to the hospital on the day of your surgery THE OTTAWA HOSPITAL CP 95 B (03/2013)
2 Midnight Case Examples and Documentation Tips. Ralph Wuebker, MD Executive Health Resources, Inc. All rights reserved.
 2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
About Your Colectomy
 UW MEDICINE PATIENT EDUCATION About Your Colectomy How to prepare and what to expect This handout explains a colectomy operation, including how to prepare for surgery, what to expect afterward, recovering
UW MEDICINE PATIENT EDUCATION About Your Colectomy How to prepare and what to expect This handout explains a colectomy operation, including how to prepare for surgery, what to expect afterward, recovering
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance?
 Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Clinical Pathway: Tetralogy of Fallot (TOF) Repair
 Repair") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Tetralogy of Fallot (TOF) Repair Notes: (1) This pathway is a general guideline and variations can occur based on professional
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Tetralogy of Fallot (TOF) Repair Notes: (1) This pathway is a general guideline and variations can occur based on professional
During pre-briefing, you will be assigned one of these roles according to the description below to participate in the simulation as a nurse.
 Student Instructions for Standardized Simulation NR 452 Eric Chilton PURPOSE The following information is to be used in guiding your preparation and participation in the scenario for this course. This
Student Instructions for Standardized Simulation NR 452 Eric Chilton PURPOSE The following information is to be used in guiding your preparation and participation in the scenario for this course. This
University of South Dakota Vermillion, South Dakota Department of Nursing. Simulation Scenario Infection: Post Anesthesia Care Unit (Part 1) Overview
 Overview") Title: To cite this reference: University of South Dakota Simulation Scenario Infection: Post Anesthesia Care Unit (Part 1) Overview Post Anesthesia Care Target Group: First Year Concept: Infection Unit
Title: To cite this reference: University of South Dakota Simulation Scenario Infection: Post Anesthesia Care Unit (Part 1) Overview Post Anesthesia Care Target Group: First Year Concept: Infection Unit
RN - Skilled Nursing Visit
 Clinician: Mileage: Gender: Agency Name/Branch: M F Time In: Time Out: DOB: HCPCS Select the home health service type that reflects the primary reason for this visit: (G0154) Direct skilled services of
Clinician: Mileage: Gender: Agency Name/Branch: M F Time In: Time Out: DOB: HCPCS Select the home health service type that reflects the primary reason for this visit: (G0154) Direct skilled services of