Agenda and Papers. NHS West Kent Clinical Commissioning Group Governing Body. Tuesday 25 th June 2013 At 1.30pm
|
|
|
- Angelina Dean
- 5 years ago
- Views:
Transcription



1 Agenda and Papers for the NHS West Kent Clinical Commissioning Group Governing Body To be held on Tuesday 25 th June 2013 At 1.30pm In The River Centre, Medway Wharf Road, Tonbridge, TN9 1RE NHS West Kent Clinical Commissioning Group
2 Page 2 of 112 Notice is hereby given of the meeting of the NHS West Kent CCG Governing Body meeting to be held on Tuesday, 25 June 2013, at pm, in The River Centre, Medway Wharf Road, Tonbridge, TN9 1RE This meeting will be held in public. Questions from the public The Chairman will take questions from the public relating to items on the agenda or other aspects of the CCG business. Chairman is Dr. Bob Bowes *Papers for approval A G E N D A Part 1 Time Agenda no. Agenda Item Lead Required Action 1.30pm 108/13 Questions from the public Chair TO DISCUSS 1.50pm 109/13 Welcomes and Introductions Chair TO NOTE 110/13 Apologies for Absence Chair TO NOTE 111/13 Quorum Chair TO NOTE 112/13 Declaration of Member s Interests *113/13 Minutes from the previous meetings held on /13 Actions arising from the previous meetings held on /13 Matters Arising from the meeting held on not covered elsewhere on the agenda. Chair Chair Chair Chair TO NOTE FOR APPROVAL Pages 5-19 TO DISCUSS AND NOTE Page 20 TO DISCUSS AND NOTE
3 Page 3 of 112 Chief Member Reports and Strategy Papers 2.05pm 116/13 Chief Officer s Report Ian Ayres ORAL REPORT 117/13 Chairman s Report Chair ORAL REPORT Performance and Assurance Reports 3.15pm Break 3.30pm 118/13 Board Assurance Framework Update Richard Segall Jones TO NOTE Pages /13 Chief GP Commissioner and Clinical Strategy Group Report Dr. Sanjay Singh FOR INFORMATION Pages /13 Performance report Reg Middleton 121/13 Quality Report Steve Beaumont TO NOTE Pages TO NOTE Pages Corporate Reports 122/13 Medicines Optimisation Group Report 123/13 Practice Engagement Committee Report Dr. Tim Palmer Dr. Garry Singh TO NOTE Pages TO NOTE Pages pm 124/13 Programme Governance Evelyn White FOR APPROVAL Page pm 125/13 NHS West Kent CCG Older People Strategy Martine McChanon/ Dr Bruno Capone FOR APPROVAL Pages
4 Page 4 of 112 Resolution: That representatives of the press and other members of the public be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest. Date of the next meeting: Tuesday 23 July 2013, pm, The Village Hotel, Castle View, Forstal Road, Sandling, Maidstone, ME14 3AQ. Sylvia.robson2@nhs.net Dates of Future Meetings Tuesday 27 August 2013, pm, The Riverside Centre, Medway Wharf Road, Tonbridge, TN9 1RE Tuesday 24 September 2013, pm, The Village Hotel, Maidstone Tuesday 22 October 2013, pm, The River Centre, Tonbridge Tuesday 26th November 2013, pm, The Village Hotel, Maidstone Tuesday 17 December 2013, pm, The River Centre, Tonbridge Tuesday 28th January 2014, pm, The Village Hotel, Maidstone Tuesday 25 February 2014, pm, The River Centre, Tonbridge Tuesday 25 March 2014, pm, The Village Hotel, Maidstone
5 Page 5 of 112 DRAFT MINUTES of the Governing Body meeting Held in Public Meeting held on 28 th May 2013, in The Village Hotel, Maidstone, Kent Castle View, Forstal Road, Sandling, Maidstone Kent ME14 3AQE. Date of Approval: Present; Dr. Bob Bowes Ian Ayres Steve Beaumont Reg Middleton Dr. Sanjay Singh Dr. Nic Goodger Dr. Bruno Capone Dr. Tim Palmer Malti Varshney Jim Hedges Sue Southon Dr. Nick Cheales Dr. Mark Whistler Dr. Andrew Roxburgh Dr David Chesover Dr. Gary Singh Chair of the Governing Body Chief Officer/Accountable Officer Chief Nurse Chief Finance Officer Chief GP Commissioner and GP Governing Body Member Secondary Care Clinician GP Governing Body Member Chair of MOG & GP Governing Body Member Public Health Consultant Lay Member for Governance Lay Member for Patient and Public Engagement GP Governing Body Member Chair of the UCB & GP Governing Body Member GP Governing Body Member GP Governing Body Member GP Governing Body Member In Attendance Richard Segall Jones Kofo Abayomi Company Secretary Interim Governance Support Manager Apologies Gail Arnold Evelyn White Chief Operating Officer Acting Chief Operating Officer
6 Page 6 of 112 Dr Mark Ironmonger Dr Meriel Wynter Dr Tony Jones GP Governing Body Member GP Governing Body Member GP Governing Body Member
7 Page 7 of /13 Questions from the Public Question from Mr Geoff Parsons. I am gathering information about Sevenoaks District as a Dementia Friendly Community. The DGSCCG has given information about priorities for Dementia at meetings this covers some of the Northern Parishes. I was wondering whether WKCCG could give us something on your policies and priorities for our Southern Parishes. This background will inform our developing understanding of the ways in which residents, businesses and visitors can develop all of our towns and villages as dementia friendly communities. Also, it would be of interest as to whether your PPGs are interested in growing clinical health and care problems for Sevenoaks District. The Chair stated that Mr Parson could not be at the meeting; however Mr Segall Jones had prepared a response to be read at the meeting and subsequently communicated to Mr Parson. Mr Segall Jones responded by highlighting WKCCG policies and priorities on dementia as follows: Increasing diagnosis rate range of initiatives from awareness raising, GP checklist that SILK have developed for the first trip to the GP with memory concerns, changing pathway, which you all know about, introduction of technology cantabmobile to support early identification, implementation of the national Cquin in our hospitals MTW and DVH meeting the target to identify people who need referral for memory concerns. Supporting people to live well with dementia, wherever they live dementia friendly communities so people can feel safe and well supported in their community, support to care homes included Excellence in Kent project with Bradford University (Care homes in Sevenoaks yet to sign up), skilling up community OPMH staff to support care home in behavioural management, skilling up intermediate care staff in KCHT to improve access and experience of ICT services maximising independence and enabling people to return home. Improving dignity in care in our hospitals both MTW and DVH have developed plans to improve the quality of care to pwd and hopefully improve outcomes, reduce lengths of stay and increase proportion of people returning home investment in hospital environments, investment in staff training, introduction of buddy schemes, DVH introducing Forget Me Not scheme to help all staff to identify people with dementia and to be aware of their needs. Support Carers investment in carers support, introducing rapid access in primary care to carers support, crisis service to be reviewed to ensure we have good response in a crisis. End of Life helping people to die in the place of their choice with dignity. Investment in EOL training for primary care staff, to support care homes. The Chair commented that a response is yet to be obtained from Sevenoaks regarding the Patient Participation Group. This will be communicated once obtained. (Please see annexure). Mr Ayres commented on questions raised at the last meeting not covered in the Minutes. A question was raised by a member of the public, who is a voluntary car driver. He enquired
8 Page 8 of 112 whether WKCCG would be participating in the Voluntary Drivers Scheme by issuing West Kent ID badges to voluntary car drivers. Mr Ayres stated that historically drivers were automatically issued with badges, but this is no longer the practice due to requirements to safeguard vulnerable adults and children and the need to carry out due diligence on all drivers. Action: Mr Ayres agreed to explore this matter with provider of transport services, whether this is a role they can undertake. Following a question on WKCCG procurement policy at the last Governing Body Meeting, Mr Ayres commented that Monitor had issued a guideline on Procurement Patient Choice and Cooperation for consultation. The guideline is to be incorporated in WKCCG procurement policy. Action: Mr Ayres would provide detailed information at the Governing Body Meeting in July. Mr Richard Davison, reiterated his question from the previous meeting, he enquired whether there was non-gp participation in the West Kent Health & Wellbeing Board. The Chair responded that Malti Varshney sits on the Local Health & Wellbeing Board as a non-gp member as well as Cllr Roger Gough, KCC Cabinet member for Health. 91/13 Welcomes and Introductions The Chair welcomed members to the meeting. He introduced Ms Abayomi to members and informed them she had recently taken over administration of the Governing Body meetings. Governing Body expressed its thanks to Natalie Jacobs for her support previously. 92/13 Apologies for Absence Apologies for absence were received from Dr Tony Jones, Dr Meriel Wynter, Ms Gail Arnold and Ms Evelyn White. 93/13 Quorum The Governing Body agreed the meeting was quorate. 94/13 Declaration of Member s Interests There were no changes to declaration of Members Interests declared. 95/13 Minutes from the previous meetings held on /13 Matters arising from Item 57/13: Incentive Scheme The words Practices where population is high to be deleted and replaced with population weighting. 80/13 Standing Financial Instructions incorporating Scheme of Budgetary Delegation 4 th paragraph, line 7 the words best value for money to be deleted and replaced with cheapest.
9 Page 9 of /13 Chief GP Commissioner and Clinical Strategy Group Report 4th paragraph, line 4 th line, the word patient to be deleted and replace with staff. 84/13 Finance Report 1 st paragraph should be redrafted to read CCG position reflected an overspend of a 799k. In context, the PCT is achieving target of surplus for the year. It is felt we are in a sound financial situation going forward. 96/13 Actions arising from the previous meetings held on o 83/13 Performance Report Mr Middleton stated that he was yet to receive the required information. o Dr Chesover to chase outstanding action from last meeting. 97/13 Matters Arising from the meeting held on not covered elsewhere on the agenda. There were no matters arising from the meeting held on that were not covered elsewhere on the agenda. 98/13 Chief Officer s Report Mr Ayres advised the Governing Body that Monitor had issued the following guidelines: How can the NHS payment system do more for patients. Mr Ayres stated that WKCCG would respond to the issues outlined in the guideline. Guideline for Commissioners on ensuring the continuity of health care service. This describes how CCG s will advise Monitor on which services that must remain local should a Foundation Trust enter into administration. Mr Ayres informed the Governing Body that a consultation draft on NHS assurance is now available. WKCCG would map this with existing framework and reproduce a document representing both requirements. 98.1/13 Amendment to the CCG s Constitution Mr Segall Jones explained the need to amend the CCG s constitution. He stated that NHS England is seeking assurance that the CCG Constitution does not contain any provision that may be perceived as an attempt to cut across the right of any individual, under the Public Interest Disclosure Act, to raise concerns in the public interest.
10 Page 10 of 112 Mr Segall Jones stated that the amendment is straightforward and requires redrafting section 9.9 of NHS West Kent CCG constitution. If amendment is approved by the Governing Body, it would also need to be ratified by members of the CCG as a variation to the existing constitution. Mr Segall Jones also commented on the recently approved CCG whistle blowing policy. He stated that the policy would be reviewed by Internal Audit and Counter Fraud to ensure it is fit for purpose. Mr Segall Jones requested that the Governing Body approve the rewording of section 9.9 of the constitution in order to obtain CCG member and NHS England approval. Decision: The Governing Body approved the amendment to WKCCG constitution. 98.2/13 Troubled Families, West Kent Overview Ms Varshney explained that the report gives an overview of the Troubled Families Programme in Kent and focuses on development within West Kent. It highlighted the national criteria being used for Troubled Families- non- school attendance, anti-social behaviour and youth crime and worklessness. The report further explained the multi-agency approach being adopted by Kent and the mechanisms for local engagement i.e. through Local Operational Groups and provided details of the nomination process for year 2. Ms Varshney stated that the overall aim was to update the Governing Body and for them to add value to it. The Governing Body enquired where the statistics presented in the report were derived from. Ms Varshney responded that the statistics were derived using national criteria. The Governing Body requested detailed data if the programme is successfully implemented. Ms Varshney was not currently in a position to provide this detail, however she assured the Governing Body that she was confident this programme would be successful in achieving the desired outcome. 99/13 Chairman s Report The Governing Body noted the report. The Chair provided updates on the following: Ethical Commissioning The Chair requested that Governing Body note the paper on Ethical Commissioning principles while making commissioning decisions. Mapping the Future
11 Page 11 of 112 Four workshops had taken place and two more would be organised. The Chair stated that the programme is run by external consultants who would be looking at the CCG s approach to commissioning in the next few years. The current thinking is that for the CCG to continue to commission services in the current way, will not be sustainable. The Chair encouraged members of the public not to feel isolated from developing the blueprint; as a draft would be circulated to the public for input. Deputy Clinical Chair The Chair highlighted a need for a Deputy Clinical Chair i.e. a GP Governing Body Member to fill the role of Chair in his absence. The principle was accepted and Dr Bowes agreed to discuss the matter in more detail outside the meeting. He added that this role should not be confused with that of Mr Hedges who would need to deputise in the chair at Governing Body meetings when any conflict of interest would exclude the GP Lead members from discussion. 99.1/13 GP & Practice Engagement Vision Dr Garry Singh presented the GP & Practice Engagement Vision to the Governing Body. The report proposed how WKCCG intends to engage with its GPs and their practices. The report describes the engagement drivers, vision, strategy & themes, implementation and the engagement steering committee. The Governing Body was asked to agree the following: To the change in Committee name to Practice Engagement Committee Approve and sign up to the engagement vision Ratify the terms of reference of the Committee Endorse the additional responsibility of Engagement Lead for Governing Body Members The Governing Body raised the issue of membership. Dr Garry Singh explained the difficulties in recruiting nurses for the Committee and recommended that one practice nurse would be sufficient. Another view was for each locality to be represented by a practice nurse or manager. Dr Gary Singh advised the need to limit membership of this Committee. Quorum of the Committee was discussed and the general consensus was that quorum should be increased due to nature and size of the committee. The Governing Body also considered the need for representatives from PPG Group in order to obtain input from patients. Decision: The Governing Body agreed the following: The name of the Committee was changed to Practice Engagement Committee Approved and signed up to the engagement vision
12 Page 12 of 112 Approved Terms of Reference with the following changes. It was agreed that the Committee would have one practice nurse and one PPG representative. The quorum would be seven members of which three would need to be GPs. The Governing Body endorsed the additional responsibilities of Engagement Leads by agreeing that GP members of the Practice Engagement Committee would be Governing Body members. 100/13 Chief GP Commissioner and Clinical Strategy Report Dr Sanjay Singh provided a summary of the Clinical Strategy Report and highlighted matters and actions from the Clinical Strategy Group meeting held on the 14 th of May as follows: Antibiotics/C.difficile Dr Beaumont is leading actions arising from this matter. He is to share root cause analysis with Practices where antibiotic started in the community and is thought to be a cause of C.difficile. Mr Beaumont is also to be notified of any concerns by the Microbiology department around nursing homes having excessive antibiotic prescribing. Long List of Proposals and Prioritisation Dr Sanjay Singh stated that this is being refined and it would go back to the CSG June meeting. The aim is to group the list and proprieties into categories and identify commissioning intentions for A paper titled Sustainable NHS Provider Landscape for WKCCG in 2016 was summarised as Dr Sanjay Singh s vision towards Mapping the Future. This model is at developmental stage and would be submitted to the NHS England Area Team. DESMOND This was an expansion of an existing plan and was approved by the CSG. Open Access Endoscopy Following recommendations by CSG members, Dr Sanjay Singh had made necessary alterations to the pathway and sent to MTW. The aim is to reduce waiting time. Governance Structure A final paper would be presented at the CSG June meeting. Unbundling Diagnostics
13 Page 13 of 112 Dr Sanjay Singh explained that risks and opportunities were identified. Further to discussions at the meeting, it was agreed that a pathway would be developed. Gynaecology paper CSG approved gynaecology communications by Dr Meriel Wynter on behalf of WKCCG. WKCCG Older People Strategy Dr Sanjay Singh stated that this was a framework for commissioning intentions. Amendments suggested at the meeting had been incorporated and will be brought to the next Governing Body meeting for approval and thus to the public domain. Shared Care Record Dr Sanjay Singh advised that an IT working Group had been set up. Dr Mark Whistler is working with the group from a strategic clinical perspective. Dr Sanjay Singh invited comments from the Governing Body. Sue Southon enquired how Mapping the Future fits with the Older People Strategy. Dr Sanjay Singh responded that the Older People Strategy fits in the plan till 2017 while mapping the future considers all areas and how to achieve plans beyond /13 Performance Report Mr Middleton provided a joint Performance and Finance report. It was noted that the report included activity, finance and performance information to month 1 (except where stated). The following key points were highlighted: Performance Key points: A& E performance against target in month 1 was somewhat below the planned level. But more recent performance indicates significant improvement which, if sustained, would help the Trust achieve the quarterly target. Due to NHS organisations having had to close their 2012/13 accounts, the CCG would not be reporting a month 1 financial position. Limited data was available but Mr Middleton was confident that financial performance was on track.. The key performance issues were highlighted. Governing Body members were referred to page 46 of the Board Pack. Mr Middleton explained section 4 (Are health outcomes improving for local people) he stated that areas with a lighter shade blue indicated better performance. Item which is of most concern to the CCG relates to incidence of C.difficile in West Kent. Trust Trajectory for is 42 cases, approximating to some 3.5 per month. Performance in April has proven higher than this trajectory (6), and is the subject of detailed scrutiny alongside MTW.
14 Page 14 of 112 NHS Constitution performance result for April and May, indicator of Ambulance response time. This performance shows improvement. Governing Body is asked to note that data provided in the report is Kent wide. Awaiting data on referral treatment waiting times for non-urgent consultant led treatment. A diagnostic waiting time to date is 94% showed commendable effort by MTW in maintaining performance. Ms Southon pointed out that patient experience of GP out of hours services in WKCCG was placed at 69% positive experience and enquired if there is a need for concern. Mr Middleton confirmed that this placed WKCCG on the same level as other CCGs, therefore no need for concern at this stage. Action: Governing Body requested that Mr Middleton prepare a thorough briefing on section 4 of his report, indicating how the outcomes were arrived at i.e. what was measured /13 Decision Making Governance for Continuing Health Care and Medicines Management Mr Middleton presented the paper to the Governing Body for approval. He explained the decision making eligibility, placement process, CHC invoice approval and entry of patient orientated invoices on high cost drug database flow chart. He stated that the Finance and Performance Committee had reviewed the arrangement and this would remain on the Committee agenda. The Governing Body considered this matter and it was agreed that an open plan check would be required. Action: The Governing Body requested that Dr Tim Palmer prepare a guide on definition of high cost drugs. This would serve as a guide to the practices. Mr Middleton advised that Gaye Lewington (KMCS Medicines Management) is preparing a master schedule on definitive measures of high cost drugs. This would be circulated to the Governing Body. Decision: the Governing Body approved the Decision making Governance for Continuing HealthCare and Medicines Management with the additional measures of work to be provided by KMCS. 102/13 Finance Report Financial performance had been discussed along with the Performance update. 103/13 Quality Report Mr Beaumont provided the following updates from the recent Quality Committee meeting. Infection control Action plan for C.Dificile at MTW is being reviewed. There were six cases confirmed for April A whole system approach which includes GPs, Medicines
15 Page 15 of 112 Management and the Community Services is being established to address this issue. Mr Beaumont confirmed that an Interim Infection Control Nurse working with Public Health is now in post. NHS 111 issues are being resolved on an on-going basis. Chief Nurse meeting the four Chief Nurses of the CCGs in Kent meet on a monthly basis to share best practice with the focus being on quality and safety. All Chief Nurses will be working alongside clinicians in practice. This has been approved by providers and updates would be provided to the Governing Body. KPMT a recent meeting was held with KPMT with regards to the enhanced surveillance that had been implemented. Mr Beaumont stated that KMPT demonstrated that they had outstanding issues with the rule 43 (Coroners report on attempted suicide), staffing issues and IAPT waiting list. It was recommended that KMPT are put back on routine surveillance with regards to rule 43 and IAPT waiting list. Enhanced surveillance would be lifted for the workforce issues once the action plans regarding the staffing issues have been clarified. Dr Beaumont requested that GP Practices prepare a root cause analysis of patients who had been diagnosed with C.difficile in the last 72 hours. GPs were advised to exercise caution in carrying out this task. It was identified that West Kent Practices had a high level of prescribing antibiotics compared with National Statistics, it was agreed that this would be monitored. In the absence of Dr Meriel Wynter, the Chair communicated her suggestion that GPs are welcome to attend Locality meetings. Action; Chair to write to GP members to invite them to Quality committee meetings Mr Beaumont informed the Governing Body that a Quality inbox is now available for comments regarding quality issues. The Chair raised matters concerning the Francis report. He stated that impacts of the report should be on Governing Body meeting agenda going forward. 104/13 Medicines Optimisation Group Report Dr Palmer provided the following updates from the recent Medicines Optimisation Group meeting: Prescribing budget update: At February 2013, WKCCG prescribing budget is predicted an underspend of 2.87%, 1,877,370. Two more doctors to be elected by the Medicines Optimisation Group, i.e. dispensing & non-dispensing and a community doctor. Positive feedback from Medicines Optimisation team on sensible prescribing. Joint Prescribing Formulary to update current formulary in association with Acute Trust. 105/13 Feedback from Locality It was agreed for this item to be removed from the Governing Body meeting agenda now that the Practice Engagement Committee had been established and would be reporting to Governing Body.
16 Page 16 of /13 Board Assisted Reproductive Techniques (ART) Briefing Document for Kent and Medway Mr Beaumont advised the Governing Body that the recent publication of new national guidance and legislation had implications for local ART policies. CCGs in Kent and Medway have commissioned KMCS to work with clinicians and patients to review local policy in light of the new NICE Clinical Guidelines and other recently issued legislation. This is a complex task and will take some time to work through. 107/13 Collaborative Commissioning Agreement Dr Beaumont presented the Collaborative Commissioning Agreement to the Governing Body for approval. The Governing Body was also asked to approve adoption of Kent and Medway decision making. A Policy Recommendation and Guidance Group which had previously been set up, continues in its present format. Dr Beaumont reported that he had been appointed Chair of the Group.. Dr Beaumont advised the Governing Body that a GP member representative is required in the Group. Dr Andrew Roxburgh agreed to sit in the Group as the GP member. The Chair enquired whether the Governing Body found the agreement acceptable. Decision: the Governing Body approved the proposal for the Collaborative Commissioning Agreement.
17 Page 17 of 112 Date of the next meeting: Tuesday 25 th June pm, The River Centre, Tonbridge. Dates of Future Meetings Tuesday 23 July 2013, pm, The Village Hotel, Castle View, Forstal Road, Sandling, Maidstone, ME14 3AQ Tuesday 27 August 2013, pm, The River Centre, Medway Wharf Road, Tonbridge, TN9 1RE Tuesday 24 September 2013, pm, The Village Hotel, Maidstone Tuesday 22 October 2013, pm, The River Centre, Tonbridge Tuesday 26th November 2013, pm, The Village Hotel, Maidstone Tuesday 17 December 2013, pm, The River Centre, Tonbridge Tuesday 28th January 2014, pm, The Village Hotel, Maidstone Tuesday 25 February 2014, pm, The River Centre, Tonbridge Tuesday 25 March 2014, pm, The Village Hotel, Maidstone
18 Page 18 of 112 Annexure Response to Public Question Dear Geoff Thanks again for your question. This was read out at the Governing Body meeting on 28 th May and I summarise below the CCG s response with regard to local healthcare policies and priorities on dementia services. 1. Increasing diagnosis rates there is a range of initiatives awareness raising a GP checklist that SILK (Social Innovation Laboratory for Kent part of KCC) have developed for the first trip to the GP with memory concerns reviewing pathways introduction of Cantabmobile technology (new touchscreen test for memory impairment) to support early identification implementation of the national CQIN (see in Maidstone and Tunbridge Wells and Darent Valley Hospitals to meet the target to identify people who need referral for memory concerns. 2. Supporting people to live well with dementia, wherever they live contributing to work on dementia friendly communities so people can feel safe and well supported in their community support to care homes including the Excellence in Kent project with Bradford University (although no care homes in Sevenoaks have signed up yet) skilling up community OPMH (Older People s Mental Health) staff to support care homes in behavioural management skilling up intermediate care staff in Kent Community Healthcare Trust to improve access and experience of Intermediate Care Team services maximising independence and enabling people to return home. 3. Improving dignity in care in our hospitals both MTW and DVH have developed plans to improve the quality of care to people with dementia and hopefully improve outcomes, reduce lengths of stay and increase the proportion of people returning home investment in hospital environments investment in staff training introduction of buddy schemes DVH is introducing the Forget Me Not scheme ( to help all staff to identify people with dementia and to be aware of their needs. 4. Supporting Carers
19 Page 19 of 112 investment in carers support introducing rapid access in primary care to carers support crisis service to be reviewed to ensure we have good response in a crisis. 5. End of Life helping people to die in the place of their choice with dignity investment in EOL training for primary care staff support to care homes With regard to PPGs, we are very committed to working with PPGs from all the Practices within West Kent, to ensure that we involve local people in our plans about local services and that we get feedback from patients and carers about their experiences, to inform those plans. We recognise that many PPGs are in early stages of development and are therefore primarily looking at issues within their Practice, rather than wider issues, but we are keen to support and work with them in understanding and getting involved in decisions about the services provided locally. To this end we have an established PPG Chairs Group which supports two-way informationsharing between the CCG and the PPGs. The meetings provide an opportunity for the PPG Chairs to hear about the business of the CCG, how it makes commissioning decisions and the priority areas for service development - one of which is care of people with dementia so that they can relay this information to their respective PPGs. We welcome and encourage feedback on any issues discussed through, for example, feedback via the Chairs, attending and sharing information at PPG meetings, via our address: westkent.ccg@nhs.net and our website, which includes information on commissioning plans and the minutes from the PPG Chairs meetings. To our knowledge, none of the Sevenoaks PPGs is currently giving priority attention to the development of dementia friendly communities. I appreciate this is rather a health-centric response. The CCG is keen to work with stakeholders to understand better what dementia friendly communities will look like and to work with other relevant agencies to help develop these. We would be pleased to pursue a dialogue with interested parties to see what contribution the CCG can make in this holistic approach to helping people with dementia. Please feel free to come back to me with any further questions. Best wishes, Richard Richard Segall Jones, Company Secretary & Head of Corporate Services NHS West Kent CCG
20 Page 20 of 112 Action Points of West Kent CCG Governing Body (WK CCG GB) Meeting was held on 28 th May, 2013, commence time was 1.30pm, in The Village Hotel, Castleview, Forstal Road, Sandling, Maidstone, ME14 3AQ. Action No (in accordance with agenda no) 90/13 Question from the Public Action Points Officer Status A member of the public enquired whether WKCCG would be participating in the Voluntary Drivers Scheme by issuing West Kent ID Badges to voluntary car drivers. Action: Mr Ayres agreed to explore this matter with provider of transport services, whether this is a role they can undertake. IA 101.1/13 Decision making Governance 103/13 Quality Report Following a question on WKCCG procurement policy at the last Governing Body meeting, Mr Ayres commented that Monitor had issued a guideline on Procurement Patient Choice and Cooperation for consultation. The guideline is to be incorporated in WKCCG procurement policy. Action: Mr Ayres would provide detailed information at the Governing Body meeting in July. Action: The Governing Body requested that Dr Tim Palmer prepare a guide on definition of high cost drugs to serve as a guide to practices. In the absence of Dr Meriel Wynter, the Chair communicated her suggestion that GPs are welcome to attend locality meetings. Action: The Chair is to write to GP members to invite them to Quality Committee meetings IA TP BB

21 Page 21 of 112 Governing Body Meeting, 25 th June 2013 Board Assurance Framework Presented by: Richard Segall Jones Introduction This paper summarises the current position relating to the key risks to the achievement of the organisation s objectives. The risks are aligned to WKCCG strategic goals. The following is a summary of changes since the Governing Body meeting held in February Summary There are 40 risks recorded on the Assurance Framework. All entries have been reviewed by the relevant senior officer. Actions and assurances have been updated where appropriate. Changes in Risk Assessment Further to review, the following risks had changes in risk assessment Goal A: A thriving local NHS provider landscape for the West Kent Population that delivers safe and high quality urgent and non-urgent care, in particular: to work with MTW to support them to be a Foundation Trust in the top quartile in terms of productivity and safety. MTW fail to deliver in the top quartile in terms of safety. This risk now has a reduced risk score of 12 (Previously 15). Goal G: Sustainable financial future Providers may seek to grow income above contracted SLA levels in order to meet their financial pressures. This risk now has a reduced risk score of 9 (previously 12) Local provider long term financial viability may require financial support above contracted levels of income. This risk now has a reduced risk score of 9 (previously 12). New risks identified
22 Page 22 of 112 Goal G: Sustainable financial future Changes in the requirements for accessing Patient identifiable data is impairing the ability of the CCG and KMCS to properly validate claims from suppliers. This could lead to delays in payment to providers, and/or inappropriate payment being made with potential loss to the CCG. Controls, gaps in controls and actions required with stipulated timescale have been advised by the Chief Finance Officer. (Details highlighted in the Board Assurance Framework). This risk has a risk score of 12. Goal H: Reputation There is a risk that the CCG will inappropriately share personal confidential data (PCD), either through a one-off request for information or a new service commencing and breach on their data protection requirements. This could result in an ICO monetary penalty. Controls, gaps in controls and actions required with stipulated timescale have been advised by the Chief Finance Officer. (Details highlighted in the Board Assurance Framework). This risk has a risk score of 9 Red Risks Following review of the BAF, three entries have a current risk rating of 15 or above (red) and have controls in place and ongoing mitigating actions in place. The risks are highlighted below: Goal B: Improved value for money and outcomes for Mental Health conditions including dementia in particular. developing improved community based services that support individuals manage their mental health problems without the need to be admitted to an inpatient bed. This risk has an increased risk score of 15, previously 12 (Amber). Goal D: Improved and Integrated health and social care packages for the elderly population, in particular: To align community health and social care team around clusters of practices to improve the integration of care and keep people out of hospital. Increasing population of elderly people is resulting in demand exceeding capacity across Health and Social Care. This risk has a risk score of 16. Goal G: Sustainable financial future CCG QIPP schemes may not deliver reductions in our costs with providers and so provider contracts may become unaffordable. This risk has a risk score of 16.

23 Page 23 of 112 Clinical Strategy Group report: June 2013 Dr Sanjay Singh Chief GP commissioner Patient focused Providing quality, improving outcomes
24 Page 24 of 112 The CSG met on 11/6/13 and discussed the following items: Transforming OPD Services and GP referrals CSG members discussed a proposal to commission a prime vendor triage & management model for certain specialities, where the benefits of transformation could be maximised. It was highlighted that unbundling of diagnostics impacted this area, therefore if used in the right way it could be a good opportunity. The CSG considered this matter and it was agreed that the proposal would proceed to the planning stage. This should evidence the cost effectiveness of the proposed model over the current model and enhance patient experience via adopting new pathways. Commissioning Intentions for : Next steps and key issue It was agreed that a short list would be made available in September 2013 and the business case would commence thereafter. Patient groups will start to get the Long list in batches from July to prioritise whilst GPs will get the whole list in August. Risk Stratification & MDT DES: It was agreed that risk stratification would be handled by WKCCG on behalf of the Area Team. The CSG is to agree the content for local DES to be followed by the GPs. Further to discussion by members the following were agreed: Risk Stratification would be used as a guide Proforma and free text to be used as long as vital areas are covered MDT meetings would be held bi-monthly as a minimum Practices will be notified of the same soon. Falls Pilot Evaluation CSG considered the positive analysis regarding the implementation of the community falls service and feedback from patch meetings across West Kent in consideration of this service. It was noted with satisfaction the reduction in falls related admissions and fractures in West Kent since the Pilot began.
25 Page 25 of 112 Options regarding the West Kent Community falls service were presented to the CSG and the Group was asked to make a decision on which option would be suited for WKCCG. The options discussed are as follows: Commission the service after June 2014 for a further two years following evidence that the outcomes are being achieved in relation to the reduction in acute care activity. Decommission the West Kent Community falls service after June 2014 and develop business case proposal to reinvest this money for example additional physios and OTs. Further to discussions by the CSG it was agreed that: The Community falls services be extended for a further two years with a further tweaking of KPIs and service spec. It was also agreed that Mr Middleton would review this matter to determine how it is to be progressed i.e. from a procurement perspective. The low engagement of Ambulance services and Acute Trust was noted with a view to address the same. West Kent Hernia Pilot Proposal A proposal was made to the CSG to run a pilot project and if successful to subsequently introducing a "Prime Vendor "or "Integrated Pathway Hub" commissioning model. This will initially treat a group of surgical reference conditions, namely primary inguinal, femoral and umbilical hernia. The explicit aim will be to improve clinical and patient experience outcomes and to reduce cost. The service will be paid for by in-year savings and therefore will be free of commissioner financial risk. The proposition is to improve systematic value and deliver a "win-winwin" that benefits the patient, the commissioner and providers. The CSG agreed that the paper highlighted some major performance issues regarding the delivery of current hernia services which were mainly around costs and patient pathways rather than safety or clinical outcomes. The CSG felt that such issues should be first tried to be dealt via contract management and Service specification route with MTW, failing which other options could be considered. Programme Governance This matter was brought back to the CSG to note the revised document which incorporates CSG feedback from the last meeting. CSG adopted the Programme Governance and it was agreed that the next stage would be to approach individuals to chair the groups.
26 Page 26 of 112 Denosumab Use in Primary Care A proposal was presented to the CSG by Medicines Management team, for approval of Denosumab (Prolia )to be prescribed as an option for the treatment of osteoporosis in postmenopausal women at increased risk of fractures, for both primary and secondary prevention. This matter was considered by the CSG and it was approved with a proviso that dental check-up should be done prior to prescribing the drug to patients. Safety issues were also flagged and it was agreed that there would be strict guidelines on how the drug is to be administered.
27 Page 27 of 112 Performance Report May 13 Patient focused Providing quality, improving outcomes
28 Page 28 of 112 Performance Report May 13 Executive Summary The performance Report reflects a departure from the format received by the CCG Governing Board during its preparatory year. Key objectives of the report are: Reflects the introduction of the national CCG Assurance Framework Provides for the incorporation of Local priorities for the CCG, which will change with time Will evolve over time, but will strive to utilise comparative data where this is available, graphical presentation where appropriate, and identify the most recently available data to enable the Governing Body and CCG to respond swiftly where performance is not on track. Begins to integrate finance and activity with performance data Current Performance The attention of the Governing Body is drawn to the following key areas: Performance of the South East Coast Ambulance service relating to response times The number of people waiting in excess of 52 weeks The number of Cdifficile cases at the end of May The value of changes to the CCG Resource Limit, reflecting a shift in responsibility to NHS England for a range of activities The significant level of financial risk associated with the achievement of QIPP cost reductions The impact of the new arrangements governing access to Patient identifiable Data and the consequences for validation of charges to the CCG. Whilst the cost of services provided by MTW for the CCG is still subject to validation, there are indications that both volume and value of services is exceeding planned levels. A provision of 0.5m YTD has been factored into the financial position.
29 CCG Assurance Framework Local Page 29 of 112 Scorecard Indicator RAG Previous Current Movement Overall RAG Trend Quality Clinical Constitution Finance Green Amber Red Yes No Green Amber Red Green Amber Red A/G A/G G AR Local Green Amber Red G
30 Page 30 of 112 Are health outcomes improving for local people? The following sets out the Indicators that the CCG will be measured against with regards to the Quality Indicators across the 5 Domains. In the proposed CCG Assurance Framework, the CCG has made its best endeavours to interpret the information received from NHS England and this will be verified with NHSE in the coming weeks. Indicative dates for review have been provided by NHSE and these still need to be verified with NHSE with a few still under development or to be confirmed. Appendix A has been included to provide further glossary for the 5 Domains. With regard to Cdifficile, whilst the target within the CCG Assurance Framework is expressed as the number of cases per 100,000 population (being confirmed), we are tracking the absolute number of hospital acquired Cdifficile cases. As at the 9 th June 2013, the number of hospital acquired cases of Cdifficile infection at Maidstone & Tunbridge Wells NHS Trust stood at 10. The trajectory by the end of June is 12 cases (annual total 42), and therefore there is a small margin before trajectories are breached. The Trust is providing a high level of focus on this area as evidenced by the nature of staff communication on this issue and a focus upon the level of antibiotic usage within the Trust. This latter issue is also the subject of review and scrutiny amongst practitioners with the CCG. Are health outcomes improving for local people? Overall RAG rating: G National and local Quality measures Baseline Period Value Actual Target Nat Average Indicative Publication Date/s Potential years of life lost from causes considered amenable to healthcare: Male ,756 1,700 2,048 Jun-14 Potential years of life lost from causes considered amenable to healthcare: Female ,549 1,499 1,716 Jun-14 Preventing people from dying prematurely Under 75 mortality from cardiovascular disease Jun-14 Under 75 mortality from respiratory disease Jun-14 Under 75 mortality from liver disease 0 0 Jun-14 Under 75 mortality from cancer Jun-14 Health-related quality of life for people with long-term conditions Sep-14 People feeling supported to manage their condition 52% 52% 52% Sep-14 Enhancing the quality of life for people with long-term conditions Unplanned hospitalisation for chronic ambulatory care sensitive conditions 2011/ Dec-13 Unplanned hospitalisations for asthma, diabetes and epilepsy in under 19s 2011/ Dec-13 Estimated diagnosis rate for people with dementia Under Development TBC
31 Page 31 of 112 Helping people to recover from episodes of ill health or following injury Emergency admissions for acute conditions that should not usually require hospital admission 2011/ Emergency readmissions within 30 days of discharge from hospital 2010/ Emergency admissions for children with lower respiratory tract infections 2011/ Dec 13, Mar 14, Jun 14, Sept 14 Dec 13, Mar 14, Jun 14, Sept 14 Dec 13, Mar 14, Jun 14, Sept 14 PROMs for elective procedures: hip replacement 2011/ Sep-15 PROMs for elective procedures: knee replacement 2011/ Sep-15 PROMs for elective procedures: groin hernia 2011/ Sep-15 Patient experience of GP services 2011/12 90% 89% Ensuring that people have a positive experience of care Patient experience of GP out of hours services 2011/12 69% 70% Sep-14 Patient experience of hospital care Sep-13 Friends and family test for acute inpatient care and A&E. NHS OF indicator in development 81% 82% TBC Treating and caring for people in a safe environment and protecting them from harm Incidence of healthcare associated infection: MRSA Incidence of healthcare associated infection: C difficile 29 TBC 28 Sep 13, Dec 13, Mar 14, Jun 14 Sep 13, Dec 13, Mar 14, Jun 14
32 Page 32 of 112 Are local people getting good quality care? The CCG Assurance Framework sets out a number of indicators relating to the provision of good quality care. As a CCG we are working closely with MTW to reduce the number of C Diff cases. This work involves a whole system approach which involves GP and other healthcare providers working in the community. Concerns over the Friends and Family Test relate to an extremely low response rate within A&E (2.3%). MTW have introduced an action plan to address this and we will continue to monitor their progress. In subsequent reports, the content of this report will be extended to other key providers in the local health system.
33 Page 33 of 112 Are local people getting good quality care? Overall RAG rating: A/G Indicator Providers CCG Has local provider been subject to enforcement action by the CQC? Has local provider been flagged as as a 'quality compliance risk' by Monitor and/or are requirements in place around breaches of provider licence conditions? Has local provider been been subject to enforcement action by the NHS TDA based on 'quality' risk? Does feedback from the Friends and Family test (or any other patient feedback) indicate any causes for concern? Has the provider been identified as a 'negative outlier' on SHMI or HSMR? Do provider level indicators from the National Quality Dashboard show that: MRSA cases are above zero the provider has reported more C difficile cases than trajectory MSA breaches are above zero Does the provider currently have any unclosed Serious Untoward Incidents (SUIs)? Has the provider experienced any 'Never Events' during the last quarter? Clinical Governance Does the CCG have any outstanding conditions of authorisation in place on clinical governance? Has the CCG self-assessed and identified any risks associated with the following: Concerns around quality issues being discussed regulary by the CCG governing body Concerns around the arrangements in place to proactively identify early warnings of a failing service Concerns around the arrangements in place to deal with and learn from serious untoward incidents and never events Concerns around being an active participant in its Quality Surveillance Group EPRR If there was an emergency event in the last quarter, has the CCG self-assessed and identified any areas of concern on the arrangements in place for dealing with such an event? Winterbourne Review Has the CCG self-assessed and identifed any risk to progess against its Winterbourne View action plan? MTW Provider 2 Provider 2 Period No Yes No No Yes No Yes No Yes No Yes No No Yes
34 Page 34 of 112 Are patient rights under the NHS Constitution being promoted? The CCG has met or exceeded a number of indicators year to date, with slight concerns around Ambulance calls namely Cat A within 8 mins (Red 1 & Red 2), but these are both still within the lower thresholds. The main concern is within patients waiting over 52 weeks currently 9 against a lower threshold of 10, there have been no breaches recorded at MTW and the 9 are made up as follows EKHUFT: 1; Guy s: 2; Kings: 4 and 2 at the Horder Centre. The CCG will be assessed at the end of the quarter with regards to achievement of this individual indicator. The CCG will also be instigating the contractual clause with regards to 18 weeks which result in a 5000 penalty per breach with the Trusts highlighted in this report. Are patient rights under the NHS Constition being promoted? Overall RAG rating: G Indicator Period Actual Operational Target Lower Threshold Actual Admitted patients to start treatment within a maximum of 18 weeks from referral Apr % 90% 85% Referral To Treatment waiting times for nonurgent consultant-led treatment Non-admitted patients to start treatment within a maximum of 18 weeks from referral Apr % 95% 90% Patients on incomplete non-emergency pathways (yet to start treatment) should have been waiting no more than 18 weeks from referral Apr % 92% 87% Number of patients waiting more than 52 weeks Apr Diagnostic test waiting times Patients waiting for a diagnostic test should have been waiting less than 6 weeks from referral Apr % 99% 94% A&E waits Patients should be admitted, transferred or discharged within 4 hours of their arrival at an A&E department W/E 09/06/ % 95% 90% Cancer waits 2 week wait Maximum two-week wait for first outpatient appointment for patients referred urgently with suspected cancer by a GP Apr % 93% 88% Maximum two-week wait for first outpatient appointment for patients referred urgently with breast symptoms (where cancer was not initially suspected) Qtrly 93% 88%
35 Page 35 of 112 Maximum one month (31-day) wait from diagnosis to first definitive treatment for all cancers Apr % 96% 91% Cancer waits 31 days Maximum 31-day wait for subsequent treatment where that treatment is surgery Qtrly 94% 89% Maximum 31-day wait for subsequent treatment where that treatment is an anti-cancer drug regimen Qtrly 98% 93% Maximum 31-day wait for subsequent treatment where the treatment is a course of radiotherapy Qtrly 94% 89% Maximum two month (62-day) wait from urgent GP referral to first definitive treatment for cancer Apr % 85% 80% Cancer waits 62 days Maximum 62-day wait from referral from an NHS screening service to first definitive treatment for all cancers Qtrly 90% 85% Maximum 62-day wait for first definitive treatment following a consultant s decision to upgrade the priority of the patient (all cancers) Qtrly No operational standard set Category A calls resulting in an emergency response arriving within 8 minutes (Red 1) 10-Jun % 75% 70% Category A ambulance calls Category A calls resulting in an emergency response arriving within 8 minutes (Red 2) 10-Jun % 75% 70% Category A calls resulting in an ambulance arriving at the scene within 19 minutes 10-Jun % 95% 90% Mixed Sex Accommodation Breaches Minimise breaches Monthly Cancelled Operations Mental Health All patients who have operations cancelled, on or after the day of admission (including the day of surgery), for non-clinical reasons to be offered another binding date within 28 days, or the patient s treatment to be funded at the time and hospital of the patient s choice. Care Programme Approach (CPA): The proportion of people under adult mental illness specialties on CPA who were followed up within 7 days of discharge from psychiatric in-patient care during the period Not Rated Qtrly 95% 90%
36 Page 36 of 112 Financial Outcomes Indicators Finance Indicators Overall RAG rating: AR Indicator Period YTD Plan YTD Actual YTD Variance FOT Plan FOT Actual FOT Variance YTD FOT Underlying Recurrent Surplus ( '000) Apr-13 2,459 2, ,753 14,753 0 Surplus - Year to Date ( '000) Apr Surplus - Full Year Forecast ( '000) Apr-13 4,660 4, % Non Recurrent Funds ( '000) Apr ,320 9,320 0 QIPP - Year to Date ( '000) Apr-13 2,189 2, QiPP - Full Year Forecast ( '000) Apr-13 16,125 16, Activity Trends - Year To Date Apr TBC Activity Trends - Full Year Forecast Apr TBC Running Costs ( '000) Apr-13 1,858 1, ,146 11,146 0 Financial Risk Apr-13 Risk Mitigated Residual 14,625 14,625 0 This covers Internal and external audit opinions, and an assessment of the timeliness and quality of returns. Apr-13 Balance sheet indicators including cash management and BPCC Apr-13
37 Page 37 of 112 Local Outcomes Indicators The CCG has chosen the following three Local Outcomes Indicators as areas the CCG will be concentrating on for this year up and above the Outcomes, Clinical, Constitution and Financial Indicators set by NHS England. Ultimately, performance in these areas will affect the achievement of the Quality Premium which may result in a financial incentive being accessed by the CCG in The CCG has set itself an ambitious target for improvement against these three indicators. These also form part of the assessment of the CCG by NHSE. In addition to the three Local indicators the CCG has added an additional one under the heading Others. Over time, the scope of local data reported to the Governing Body may be extended, according to local priorities and in response to performance issues. Local Outcome Indicators Overall RAG rating: G National and local Quality measures Period Baseline Acutal Target Reducing gap between recorded prevalence versus expected prevalence 67.6% 74% Local Outcome indicators Direct admissions to Stroke Unit from arrival at hospital 43.5% 75% People diagnosed less than one year referred to structured education 0% 15% Others IAPT Coverage - perfromance against plan
38 Page 38 of 112 Financial Individual Outcomes Indicators Summary Financial Position The table below reflects achievement of a small surplus of 344k at the end of month 2, which is below the planned level. Across the year as a whole the CCG continues to reflect the planned surplus of 1% ( 4.66m). In addition, the table adjusts financial performance for NR applications of funds. The principal item is the 2% Headroom reserve ( 9.3m), together with a small amount of Non-recurrent expenditure items ( 0.8m). Adjusting the planned in-year performance for these items produces an underlying recurrent surplus of 14.8m. A summary of the CCGs financial performance is shown in the Table below: '000 Year to Date Full Year Plan Actual Variance Plan Forecast Variance Total Resource Limit 80,405 75,455 (4,949) 482, ,768 (5,659) Total Programme costs (77,678) (73,228) (4,450) (466,067) (460,408) (5,659) Total Administration (1,950) (1,883) 67 (11,700) (11,700) 0 Total Expenditure (79,628) (75,111) (4,383) (477,767) (472,108) (5,659) Net Surplus /(Deficit) ,660 4,660 0 Non Recurrent Items 1,682 1, ,093 10,093 0 Underlying Surplus /(Deficit) 2,459 2, ,753 14,753 0 Graphs and Trend analysis to be inserted once available
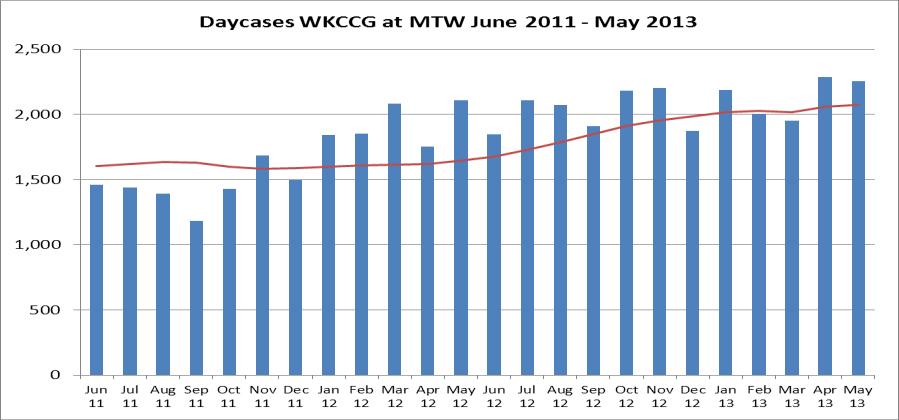
39 Page 39 of 112 Overall Financial Position The CCG position reported for Month 2 is a surplus albeit below the planned level. The mian driver for this position relates to performance at MTW where costs appear to be exceeding plan- particularly in the area of daycases, outpatients and direct access pathology/radiology. High levels of expenditure in Critical care in Month 1 have returned closer to plan in Month 2. For the remainder of the programme costs, the CCG has accrued to plan due to minimal data received from providers as at month 2. The CCG has identified a number of risks relating to the financial year and these are articulated with the Financial Risk element of this report. Data relating to over performance at MTW yet to be validated. Further updates should be available by the Governing Body meeting and a verbal update will be provided. At this early stage, insufficient data is available to support any deviation from agreed plans. Year To Date Year End Forecast Plan Actual Variance Plan Forecast Variance Overall Financial Position 75,455 75, Overall Financial Position 476, ,108 4,660 Year To Date Plan Actual Variance Year End Forecast Plan Forecast Variance '000 '000 '000 '000 '000 '000 Mental Health 6,417 6,417 0 Mental Health 38,502 38,502 0 Acute 42,980 43, Acute 257, ,883 0 Primary Care 12,337 12,337 0 Primary Care 74,023 74,023 0 Continuing Care 4,783 4,783 0 Continuing Care 28,698 28,698 0 Community Health Services 5,957 5,957 0 Community Health Services 35,743 35,743 0 Other 1, Other 30,219 25,559 4,660 Total Programme costs 73,505 73, Total Programme costs 465, ,408 4,660 Corporate (Running Costs Allowance) 1,950 1, Corporate (Running Costs Allowance) 11,700 11,700 0 Total Administration 1,950 1, Total Administration 11,700 11,700 0 Total 75,455 75, Total 476, ,108 4,660
40 Page 40 of 112 Graphs and Trend analysis to be inserted once available Resource Limit The Resource Limit below has been agreed with NHS England and the initial anticipated adjustments for Specialist Commissioning and Dental have now been adjusted for, however we are still anticipating further adjustments for Specialist Commissioning once these have been finalised by NHSE. Further detail will be provided on a monthly basis to reflect any additional adjustments that may take place for the remainder of the year. These reductions in Resource Limit are accompanied by an equivalent level of cost reduction, which reflects the intended outcome of neutrality agreed with NHS England. Year To Date Year End Forecast Plan Actual Variance Plan Forecast Variance k k k k k k Resource Limit 80,404 75,455 (4,949) Resource Limit 482, ,768 (5,658) Plan Actual Variance Plan Actual Variance k k k k k k Opening Resource Limit 75,924 75,924 0 Opening Resource Limit 455, ,546 0 Grow th 1,746 1,746 0 Adjustment 1 10,478 10,478 0 Running Cost Allow ance 1,950 1,950 0 Adjustment 2 11,700 11, Closing Resource Limit 79,621 79,621 0 Closing Resource Limit 477, ,724 0 Anticipated Anticipated Carry forw ard 784 1, Carry forw ard 4,702 4,702 0 Specialist Commissioning deduction - South (3,355) (3,355) Specialist Commissioning deduction - South (3,355) (3,355) Transfer of service to K&S Area Team - Dental (2,303) (2,303) Transfer of service to K&S Area Team - Dental (2,303) (2,303) Anticipated Resource Limit 784 (4,165) (4,949) Anticipated Resource Limit 4,702 (956) (5,658) Total Resource Limit 80,404 75,455 (4,949) Total Resource Limit 482, ,768 (5,658)
41 Page 41 of 112 Graphs and Trend analysis to be inserted once available Cash Management The CCG is carrying a high level of cash at present and this primarily due to information governance issues with regards to KMCS. There are 6.5m uncoded invoices within the system at present. The CCG has prioritised this issue with a view to managing the associated risks arising. Year To Date Year End Forecast Plan Actual Variance Plan Forecast Variance k k k k k k Cash Balance 3,790 9,217 5,427 Cash Balance 12,688 15,159 2,471 Year to Date Year End Forecast Plan Actual Variance Plan Forecast Variance k k k k k k Balance B/F - 0 Balance B/F 0 Receipts 0 Receipts 0 Draw dow n 77,831 77,831 0 Draw dow n 411, ,794 (796) BACS 0 BACS 0 Chaps 0 Chaps 0 RFT 0 RFT 0 Other 0 Other 0 77,831 77, , ,794 (796) Payments Payments RFT (NHS) 65,949 64,378 (1,571) RFT 331, ,145 62,966 BACS 8,092 3,826 (4,266) BACS 58, (57,397) Other Other 9, (8,836) 74,041 68,614 (5,427) 398, ,635 (3,267) Balance C/F 3,790 9,217 5,427 Balance C/F 12,688 15,159 2,471 Graphs and Trend analysis to be inserted once available
42 Page 42 of 112 Running Costs The CCG is showing breakeven year to date and forecasted breakeven for the year. Further analysis is being carried to effectively report in further detail against the headings below and this will be included in the next report. Year To Date Year End Forecast Plan Actual Variance Plan Forecast Variance k k k k k k Running Costs Running Costs Year To Date Full Year Plan Actual Variance Plan Forecast Variance k k k k k k Cost Type Cost Type CCG Pay Costs - CCG Pay Costs - CSU Recharge - CSU Recharge - NHS Property Services re-charge NHS Property Services re-charge Other Non-pay - Other Non-pay - Total Running Costs Total Running Costs Graphs and Trend analysis to be inserted once available
43 Page 43 of 112 Statement of Financial Position The work to transfer balances from the former West Kent PCT into legacy organisations continues. The CCG can expect to receive transfers with respect to Fixed Assets (primarily IT related), and any legacy debtors/creditor balances where transactions have not been concluded by the end of June. It is now expected that this legacy programme work may continue through until the end of August/September. At this moment, some delays are being experienced in processing payments and is being compounded by the impact of Information Governance rules relating to validation of patient data supporting invoices. This has been highlighted as a key risk to the CCG. Finally, the level of cash balance at the end of May is higher than would be expected as part of managing the on-going position. CCGs have yet to be provided with a formal cash limit for the year. Once this is received, the level of cash drawings will need to be re-profiled and geared towards minimising the level of cash balances at the end of each month.
44 Page 44 of 112 Full Year Actual Notes Plan Forecast Variance Notes k k k k Property, Plant and Equipment - Property, Plant and Equipment (533) Intangible Assets - Intangible Assets - Other Assets - Other Assets - Non Current Assets Non Current Assets - Inventories Inventories - Trade and Other Receivables 26,739 Trade and Other Receivables - Cash and Cash Equivalents 9,217 Cash and Cash Equivalents Non Current Assets Held for Sale - Non Current Assets Held for Sale - Current Assets Current Assets Trade and Other Payables - Trade and Other Payables 1,500 1,500 Borrow ings - Borrow ings - Other Financial Liabilities - Other Financial Liabilities - Provisions - Provisions - Other Liabilities - Other Liabilities - Current Liabilities Current Liabilities - - Borrow ings - Borrow ings - Provisions - Provisions (6,767) (6,767) - Trade and Other Payables (32,804) Trade and Other Payables (23,683) (12,340) 11,343 Non Current Liabilities Non Current Liabilities - Provisions - Provisions (626) (626) - TOTAL ASSETS EMPLOYED 3,152 TOTAL ASSETS EMPLOYED (30,203) (17,793) 12,410 Financed by: Financed by: Public Dividend Capital 3,152 Public Dividend Capital (34,862) (22,452) 12,410 Retained Earnings - Retained Earnings - Surplus/(Deficit) for Year - (Surplus)/Deficit for Year 4,659 4,659 - Revaluation Reserve - Revaluation Reserve - TOTAL TAXPAYERS EQUITY 3,152 TOTAL TAXPAYERS EQUITY (30,203) (17,793) 12,410
45 Page 45 of 112 Capital The CCG has a modest Capital expenditure plan in place for NHS England has yet to confirm the level of allocation that will be available to CCGs, and we should therefore proceed with caution at this stage. There has been no expenditure recorded to date. Year To Date Year End Forecast Plan Actual Variance Plan Forecast Variance k k k k k k Capital Capital Capital k Capital k Budget Actual Variance Budget Actual Variance Source of Funds k k k Source of Funds k k k Capital Funds Allocation 0 Capital Funds Allocation Additional Capital - Additional Capital - Transfer from Revenue - Transfer from Revenue Application of Funds Application of Funds CCG IT Equipment CCG IT Equipment Activity Performance Management System Activity Performance Management System Data transfer to support Performance management Data transfer to support Performance management Total Total Graphs and Trend analysis to be inserted once available
46 Page 46 of 112 QIPP The CCG has set an ambitious target for QIPP (Commissioning Intentions) in 2013/14. There are 31 plans to deliver a QIPP total of 16.1m to enable the CCG to meet its plan or 13.6m as submitted to NHS England. To date the CCG is showing breakeven against plan, but it contains a certain number of risks specifically around plans that are still being worked up for schemes starting in year. Year To Date Plan Actual Variance Year End Forecast Plan Forecast Variance Month k k k k k k QIPP Plans 2,189 2,189 - QIPP Plans 16,125 16,125 - Monthly Run Rate 2 1,095 1,095 - Monthly Run Rate 1,344 1,344 - Year To Date Year End Forecast Risk Adjusted Delivery for Year End Adjusted Plan Actual Variance Plan Forecast Variance Original YTD Red Amber Green Year End Workstream Workstream Plan Delivered (50%) (75%) (100%) Forecast Variance k k k k k k k k k k k k k Diabetes high quality care - integrated model Diabetes high quality care - integrated model End of life Care (104) (104) End of life Care 165 (104) Community Redesign ,036 1,036 0 Community Redesign 1, ,036 0 Dementia Dementia Care of the Elderly / Discharge to Assess ward Romney Ward model ,229 1,229 0 Care of the Elderly / Discharge to Assess ward Romney Ward model 1, ,028 1,229 0 Reduction in A&E high tariff charges for minor injuries and illnesses Reduction in A&E high tariff charges for minor injuries and illnesses Referral Gateway Referral Gateway Paula Carr Surveillance Clinics Paula Carr Surveillance Clinics Glaucoma Monitoring Glaucoma Monitoring Decision Tools Decision Tools GPwSI ENT Clinic Snodland GPwSI ENT Clinic Snodland Respiratory Winter Project Respiratory Winter Project Better discharge schemes Better discharge schemes Primary care quality respiratory schemes Primary care quality respiratory schemes Free nursing care Free nursing care New / FU ratios ,325 1,325 0 New / FU ratios 1, ,104 1,325 0 MRIs / CTs MRIs / CTs Paed Assessment Paed Assessment Manage KMPT Manage KMPT Manage KCHT Manage KCHT DMO (34) (34) 0 (206) (206) 0 DMO (206) (34) 0 0 (172) (206) 0 Con to Con Con to Con Ambulatory Care Activity Ambulatory Care Activity Microsuction Microsuction Hysteroscopy Hysteroscopy Paediatric NEL and o/p Paediatric NEL and o/p Medicines Management ,619 3,619 0 Medicines Management 3, ,016 3,619 0 Mental Health Mental Health Mental Health ,200 1,200 0 Mental Health 1, ,000 1,200 0 QIPP Plan Total 2,189 2, ,125 16,125 0 Total 16,125 2, ,936 16,125 0
47 Page 47 of 112


48 Page 48 of 112 Activity The CCG is in process of articulating the activity in the table below and this will be included in future reports. The table below represents the template that NHS England will be monitoring the CCG with regards to achieving its activity plans for the year. The CCG has included additional graphs that give a breakdown with regards to trends within the areas included in the table below. The data source is a real-time data which includes all activity for WKCCG residents including specialist activity which is the responsibility of NHSE. Year To Date Year End Forecast Plan Actual Variance Plan Forecast Variance Total Activity Total Activity 0 Year To Date Plan Actual Variance Year End Forecast Plan Forecast Variance Elective 0 Elective 0 Non-Elective 0 Non-Elective 0 Outpatient - First Att 0 Outpatient - First Att 0 A&E Att (Avg) 0 A&E Att (Avg) 0 Total Activity Total Activity 0 0 0

49 Page 49 of 112
50 Page 50 of 112 Financial Risk The CCG has identified a number of risks for and these are provided in more detail in the table below. The level of risk remains at a significant level, and in the absence of evidence to the contrary, then the CCG needs to develop mitigation plans to accommodate significant deviation from financial plans. Of particular concern is the delivery of QIPP plans particularly relating to capacity to oversee delivery. Some progress has been made in confirming specialist commissioning adjustments with NHS England South, but there remains a risk relating to NHS England London. The underlying principle of neutrality remains in force, and therefore there should be an expectation of avoiding significant exposure to financial risk as a result of these structural changes. Forecast '000 Residual Financial Risk 14,625 Mitigated 14,625 Residual Risk 0 Probability Prinicipal financial risks YTD RAG Forecast Total of risk being Residual Position Explanation of Risk RAG '000 realised value (75 / 50 /25)% Minimal data available to support position with regard Acute SLAs 10,000 50% 5,000 Relates to activity and case mix /coding impact to principal SLAs. Community SLAs Mental Health SLAs % 250 Relatively low probability, as a result of further Continuing Care 2,000 25% 500 significant investment in continuing care placements Minimal data available to support achievement of QIPP Past experience of QIPP achievement has been in the QIPP Under-Delivery 13,000 25% 3,250 on a Year to date basis. Concerns over capacity within range 60% to 70%. commissioning team. Performance Issues Action if Risk materialises Others Interim position agreed and adopted with South of England Commissioners. To be kept under review. Movement to new commissioning architecture 7,500 75% 5,625 Residual risk relates to Other NHS England Commissioners Specifically relating to the possibility that the allocation deduction advised to to the CCG exceeds the level of cost reduction that will be achieved during See below. TOTAL RISKS 33,000 14,625 MITIGATION YTD RAG Forecast RAG Total '000 IMPACT MITIGATION NEXT STEPS Uncommitted Funds (Excluding 2% NR Headroom): Contingency Held 2, % 2,330 Contract Reserves 100% - Investments Uncommitted 100% - Actions to implement: - Further QIPP extensions 4,000 50% 2,000 Non-recurrent measures 3,000 69% 2,070 Will slow down pace of investment of 2% reserves and Delay / reduce Investment plans 2, % 2,000 other key investments. Others - Renegotiate allocation transfer with NCB 5, % 5,625 Renegotiate allocation transfer with LA 2,000 30% 600 TOTAL MITIGATIONS 18,955 14,625 Identify additional measures to eliminate waste and avoid cost Specific schemes to be worked up See key risk above. Assumes the ability to open up a dialogue with NHS England in the event of signficiant and material gaps between allocation reductions and expenditure change The CCG has identified a possible anomaly within allocation adjustments made in respect of Public Health (Local Authority ) adjustments, which it intends to pursue To be discussed at Clinical Strategy Group, to agree list of schemes to extend current QIPP programme Specific schemes to be worked up Range of options to be devised and brought to Clinical Strategy Group.
51 Appendix A Page 51 of 112
52 Domain 2 Domain 1 Page 52 of 112 NHS OF Objective Outcomes Indicator Threshold Current Performance Target Clinical Rationale Monitoring Frequency Potential years of life lost from causes considered amenable to healthcare: Male Potential years of life lost from causes considered amenable to healthcare: Female Causes considered amenable to health care are those from which premature deaths should not occur in the presence of timely and effective health care. The concept of amenable mortality generally relates to deaths under age 75, due to the difficulty in determining cause of death in older people who often have multiple morbidities. The Office for National Statistics (ONS) produces mortality data by cause, which excludes deaths under 28 days (for which cause of death is not classified by ICD-10 codes). These indicators therefore relate to deaths between 28 days and 74 years of age inclusive. Preventing people from dying prematurely Under 75 mortality from cardiovascular disease The potential years of life lost (adjusted for sex and age) from amenable mortality for a CCG population will need to reduce by at least 3.2% between 2013 and Under 75 mortality from respiratory disease (rate per 100,000 pop) One of four improvement areas which account for the large portions of the disease burden amenable to health care. Progress in these outcomes therefore provides a useful initial analysis of what accounts for progress in the overarching indicators. This indicator measures premature mortality from cardiovascular disease, and seeks to encourage measures such as the prompt diagnosis and effective management of cardiovascular conditions and treatments to reduce the re-occurrence of cardiovascular disease events and to prevent or to slow the process of chronic cardiovascular conditions. The detection of risk factors for, and the diagnosis and effective treatment of, cardiovascular disease will influence mortality associated with cardiovascular disease. One of four improvement areas which account for the large portions of the disease burden amenable to health care. Progress in these outcomes therefore provides a useful initial analysis of what accounts for progress in the overarching indicators. This indicator measures premature mortality from respiratory disease, and seeks to encourage measures such as early and accurate diagnosis, optimal pharmacotherapy, physical interventions, prompt access to specialist respiratory care, structured hospital admission and appropriate provision of home oxygen. The detection of risk factors for, and the diagnosis and effective treatment of, respiratory disease will influence mortality associated with respiratory disease. Annual Under 75 mortality from liver disease NB Information available at CCG level will involve small numbers Under 75 mortality from cancer One of four improvement areas which account for the large portions of the disease burden amenable to health care. Progress in these outcomes therefore provides a useful initial analysis of what accounts for progress in the overarching indicators. This indicator measures premature mortality from cancer, and seeks to encourage measures such as early and accurate diagnosis, optimal pharmacotherapy, physical interventions, prompt access to specialist cancer care, structured hospital admission and appropriate provision of home oxygen. Health-related quality of life for people with long-term conditions The overarching indicator (together with complementary improvement indicators) provide a picture of the NHS contribution to improving the quality of life for those affected by long-term conditions. People feeling supported to manage their condition Enhancing the quality Unplanned hospitalisation for chronic of life for people with ambulatory care sensitive conditions long-term conditions Unplanned hospitalisations for asthma, diabetes and epilepsy in under 19s Reduction or a zero per cent change in emergency admissions for these conditions for a CCG population between 2012/13 and 2013/14. (rate per 100,000 pop) 52% 52% Together with the overarching indicator, this improvement indicator should provide a picture of the NHS contribution to improving the quality of life for those with long-term conditions. The intent of this indicator is to measure effective management and reduced serious deterioration in people with ambulatory care sensitive (ACS) conditions. Active management of ACS conditions such as COPD, diabetes, congestive heart failure and hypertension can prevent acute exacerbations and reduce the need for emergency hospital admission. Estimated diagnosis rate for people with dementia To be developed
53 Domian 5 Domain 4 Domian 3 Page 53 of 112 Emergency admissions for acute conditions that should not usually require hospital admission Preventing conditions such as ear, nose or throat infections; kidney or urinary tract infections or heart failure) from becoming more serious. Some emergency admissions may be avoided for acute conditions that are usually managed in primary care. Rates of emergency admissions are therefore used as a proxy for outcomes of care. Emergency readmissions within 30 days of discharge from hospital Effective recovery from illnesses and injuries requiring hospitalisation. Some emergency re-admissions within a defined period after discharge from hospital result from potentially avoidable adverse events, such as incomplete recovery or complications. Emergency re-admissions are therefore used as a proxy for outcomes of care. Helping people to recover from episodes of ill health or following injury Emergency admissions for children with lower respiratory tract infections Reduction or a zero per cent change in emergency admissions for these conditions for a CCG population between 2012/13 and 2013/14. (rate per 100,000 pop) Preventing lower respiratory tract infections (LRTIs) in children from becoming more serious, for example, by preventing complications in vulnerable children and improving the management of conditions in the community, whilst taking into account that some children's conditions and cases might require an emergency hospital admission as part of current good clinical practice. For example, a clinical guideline for bronchiolitis published in November recommends that children showing low oxygen saturation as measured by pulse oxymetry should be admitted to in-patient care. 1 SIGN - Scottish Intercollegiate Guidelines Network (November 2006). Guideline 91. Bronchiolitis in Children - a national clinical guideline. Accessed: Quarterly and Annual PROMs for elective procedures: hip replacement PROMs for elective procedures: knee replacement Measuring health gained as assessed by patients for planned treatments. PROMs for elective procedures: groin hernia Patient experience of GP services 90% CCGs not responsible for commissioning services. Data will be available for transparency purposes. Patient experience of GP out of hours services 69% Improvement in patients experiences of GP out of hours services. Patient experience of hospital care Improvement in patients experiences of NHS inpatient care. Ensuring that people have a positive experience of care Friends and family test for acute inpatient care and A&E. NHS OF indicator in development There will need to be: 1) assurance that all relevant local providers of services commissioned by a CCG have delivered the nationally agreed roll-out plan to the national timetable, 2) an improvement in average FFT scores for acute inpatient care and A&E services between Q1 2013/14 and Q1 2014/15 for acute hospitals. 81% Improving the number of positive recommendations to friends and family by people receiving NHS treatment for the place where they received this care. Quarterly and Annual Treating and caring for people in a safe environment and protecting them from harm Incidence of healthcare associated infection: MRSA Incidence of healthcare associated infection: C difficile No cases of MRSA bacteraemia for the CCG s population (rate per 100,000 pop) C. difficile cases are at or below defined thresholds for CCGs. (rate per 100,000 pop) Reducing the incidence of healthcare associated infections (HCAI) Reducing the incidence of healthcare associated infections (HCAI). Quarterly and Annual
54 Page 54 of 112 Front Sheet for Papers Title of Report: Quality Committee Report This paper is for: Information Recommendation: For further information or for any enquiries relating to this report please contact: Dr Steve Beaumont Reporting Officer: Dr Steve Beaumont Chief Nurse Lead Director: Dr Meriel Wynter Chair of Quality Committee Report Summary: Date: 25 Jun 13 Agenda Item: Version: An update of Quality Issues. FOI status: State either: This paper is disclosable under the FOI Act Strategic objectives links: Board Assurance Framework links: Identified risks & risk management actions: Quality Committee discussions and recommendations support the delivery of all strategic objectives, in particular Strategic Objective A: A thriving local NHS provider landscape for the West Kent Population that delivers safe and high quality urgent and non-urgent care, in particular: To work with MTW to support them to be a Foundation Trust in the top quartile in terms of productivity and safety. Links to Risk Assurance relating to all clinical matters, especially strategic objective A (above) N/A
55 Page 55 of 112 Resource implications: Legal implications including equality and diversity assessment N/A N/A Report history: Appendices None None Next steps: For further information or for any enquiries relating to this report please contact Dr Steve Beaumont, Chief Nurse.
56 Page 56 of 112 GOVERNING BODY QUALITY UPDATE 25 JUN 2013 Infection Control The issues with C Diff at Maidstone and Tunbridge Wells Hospitals NHS Trust continues to be monitored. In May 2013 there were 4 cases of C Diff. West Kent CCG is still working closely with the Trust with this issue. Mental Health The CCG has been made aware of issues with patients with mental health issues being held in police custody. In response to this, the CCG is now involved with a multiagency approach to explore these issues to ensure that the needs of mental health patients are met. These issues have also been taken on as a project by the Strategic Clinical Network as issues. Friends and Family Test The results of the Friends and Family Test will be included in future Governing Body Meetings. The CCG is aware of a low response in the A & E Department at MTW (2.3% for April 2013). The Hospital Trust has developed and action plan to address this and the CCG will continue to monitor the response rate. Hospital Visits The Chief Nurse has made visits in May 2013 to: The Benenden Hospital. BMI Somerfield Hospital. The visit reports are awaiting ratification. Dr S P Beaumont Chief Nurse West Kent CCG
57 Page 57 of 112 Title of meeting: WK CCG Board Meeting Date: June 2013 Title of report: MOG Report to Board June 2013 Agenda item: Reporting Officer: Lead Director: FOI status: Priscilla Kankam, Interim Lead Prescribing Advisor Dr Tim Palmer, GP Prescribing Lead, WK CCG This paper is disclosable under the FOI Act Report Summary: This report informs the governing body of the Forecast Outturn for WKCCG Prescribing Budget for 2012/13 and the approved minutes for MOG meeting held in March Purpose: This paper is for (please tick) Assurance Approval Decision Information Recommendation: Board is asked to note the attached documents as agreed by the MOG. Strategic objectives Links Board Assurance Framework links Identified risks & risk management actions Resource implications Legal implications including equality and diversity assessment Report history: Next steps Appendices Supports financial control through cost-effective prescribing. NHS Outcomes Framework 2013/14; National Prescribing Guidance; National QIPP and Locally defined Prescribing targets; epact Data. No risks identified None identified No known and/or potential legal implications of the recommendations identified. No equality and diversity implications. This report makes reference to previous Board reports as stated and is derived from MOG reports. Implementation of Board decisions. Supporting information embedded in document. For further information or for any enquiries relating to this report please contact: Priscilla Kankam T: E: Dr Tim Palmer E:
58 Page 58 of 112 For Information 1. Prescribing Budget: Update At March 2013, NHS WK CCG Prescribing Budget The year ended with an underspend of 2.74% ( 1,788,010) to the baseline budget, this figure excludes contingencies and expenditure by Upper Grosvenor Road and Burrswood but includes adjustments to date due to incorrect allocation by PPD. The full year-end balance is yet to be finalised. Cumulative data at CCG Level is tabulated below WK CCG Prescribing Budget (excluding contingencies): 65,347,641 (from January & February 2013 data excludes spend by Upper Grosvenor Road & Burrswood but includes PPD adjustments to date) Month YE Outturn Diff from Budget % Diff Risk February ,490,071-1,857, Green March ,559,661-1,788, Green Graphs showing Practice level spend data as at March 2013 are embedded below WKCCG prescribing Forecast outturn Mar See embedded document as separate paper. 2. MOG Minutes May 2013 Minutes of the May meeting of the Medicines Optimisation Group (MOG) are embedded below. These minutes were approved at the MOG meeting on 6 th June 2013.
59 Page 59 of 112 Title of Report: Practice Engagement Committee Report This paper is for: Recommendation: Information Governing Body is asked to note this report. For further information or for any enquiries relating to this report please contact: Richard Segall Jones, Company Secretary Reporting Officer: Richard Segall Jones, Company Secretary Lead Director: Dr Garry Singh, Chair, Practice Engagement Committee Agenda Item: 123/13 Version: Report Summary: This report summarises discussion, decisions and recommendations from the initial meeting of the Practice Engagement Committee meeting held on 5 th June FOI status: This paper is disclosable under the FOI Act Strategic objectives links: Board Assurance Framework links: Identified risks & risk management actions: Resource implications: Legal implications including equality and diversity assessment Report history: Appendices All strategic objectives are served by the work of the Practice Engagement Committee. The work of the Practice Engagement Committee links to all BAF components. Not applicable. Not applicable Not applicable Not applicable None Next steps: Not applicable
60 Page 60 of 112 Practice Engagement Committee report: June 2013 Dr Garry Singh Chair, Practice Engagement Committee
61 Page 61 of 112 The Practice Engagement Committee met for the first time on 5 th June The following matters were covered. Engagement Vision and Committee Terms of Reference; GP and Practice Engagement Strategy; and Locality Engagement framework The policy documents were noted and the Committee s terms of reference, agreed at the May Governing Body meeting, were adopted. There was discussion about appointments to the Practice Nurse and Practice manager representative positions on the Committee. The Committee agreed that clarity was needed on how GP Leads and CCG staff would communicate with the Localities the type of meeting, location and frequency. It was agreed that Localities should be allowed flexibility in this although equity in the reimbursement of practices for their staff s time would also be important. Evelyn White updated the Committee on recruitment to the Commissioning Team and explained that Locality teams were being established. The Commissioning Manager leads for each locality were as follows: - M&M: Kirsteen Murray - T&TW: Mark Atkinson - Sevenoaks: Dave Holman (starting in August); Meuthia Endrojono-Ellis covering - Invicta: To be appointed; Martine McCahon covering An updated structure chart would be issued. Quality and Performance Indicators a) 2012/13 The Committee noted, with appreciation, the successful completion of the 2012/13 QP round. b) 2013/14 The Committee made a number of suggestions aimed at making the 2013/14 QP indicators more focused and effective. It was noted that the NHS England Area Team had asked to be kept informed of the QP process and would require to be a part of the final review and award arrangements. GP Practice Incentive Scheme 2013/14 The Committee noted that its role would be to make a proposal to the Chief Officer and Chief Financial Officer for them to present to Governing Body. Only the non-gp members of Governing Body would consider that proposal as the GP Leads would have a conflict of interest. The Committee then made a number of suggestions aimed at making the 2013/14 Incentive Scheme more focused and effective. The areas for work this year would be: GP Outpatient Referrals; Pathology Tests; and Practice Access, Patient Surveys, Long Term Condition prevalence and Pulse Checks.
62 Page 62 of 112 Other matters The Committee noted that the LMC was planning a joint LMC and Kent CCGs conference in November 2013 and it was hoped that NHS West Kent CCG would be well represented. A regular newsletter was requested to aid communication and engagement with the practices. It was noted that GP Registrars would now be allowed a half day per week to get involved in CCG work if they wished. The Committee welcomed this. Future meetings The Committee agreed that future meetings should take place on the first Thursday of each month, from 1.00 to 3.00pm, with the venue rotating between Wharf House, 11 Station Road, Dr Jones s practice and Dr Roxburgh s practice. The next meeting would take place on 4 th July at 1.00pm at 11 Station Road.
63 Page 63 of 112 Front Sheet for Papers Title of Report: QOF QP Work Programme 2013/14 This paper is for: Decision Recommendation: The board is asked to approve the QOF QP Work Programme 2013/14 to be undertaken by GP practices within NHS West Kent CCG. For further information or for any enquiries relating to this report please contact: Dr. K. Singh Date: 25/06/2012 Reporting Officer: Mark Atkinson Agenda Item: 124/13 Lead Director: Evelyn White Version: v1 Report Summary: This report outlines the proposed QOF QP Work Programme for GP practices to be undertaken within NHS West Kent CCG during 2013/14 as presented at the last Practice Engagement Committee (PEC) held on Wednesday 5 th June The QP Work Programme has been designed this year to act as a catalyst for the generation of clinically led commissioning intentions by requesting practices to critically reflect and make recommendations on current patient care pathways. As per the QP Work Programme for 2013/14 there are 3 main focus areas: outpatient referrals, emergency admissions and A&E attendances. Practices are required to undertake internal reviews and meet with peers externally to discuss the outcomes, common themes and future commissioning intentions. In addition practices are also required to audit their utilisation of the six care pathways developed within QP 2012/13 of: Lower Back Pain with or without Sciatica, Palpitations, Atrial Fibrillation, Falls, COPD Exacerbation and EOL care. Practice achievement will be monitored by CCG approval panel members who will include the three Heads of Locality, two support administrators/commissioners, one Finance and a Local Area Team representative. Practice appeals and sample checking of the panel teams sign off
64 Page 64 of 112 achievement scores will be undertaken by the Head of Finance and Chief Operating Officer. FOI status: This paper is disclosable under the FOI Act Strategic objectives links: Planned care (Effective and efficient pathways) Integrated commissioning (incl: LTC, Older people, Dementia, EofL) Urgent care (Emergency, Urgent and Unscheduled care) Board Assurance Framework links: Identified risks & risk management actions: Resource implications: Legal implications including equality and diversity assessment Goal A (All indicators), Goal C (QP 6 EOL), Goal E (QP9) None or a delay in approval and subsequence launch of the QP Work Programme to practices may limit the scope of activiites able to be undertaken within 2013/14. NHS Kent and Medway Local Area Team holds the budget for QP Work Programme but has delegated implementation responsibility to NHS West Kent CCG. None Report history: Appendices None None Next steps: The QOF QP Work Programme 2013/14 if approved will be formally launched to GP practices. GP practice achievement will be signed off by Heads of Locality at various milestones throughout the year in conjunction with a local area team representative.

65 Page 65 of 112 QOF Quality & Productivity Work Programme 2013/14 Practice Engagement Committee Clinical Lead: Dr. K. Singh Patient focused Providing quality, improving outcomes
66 Page 66 of 112 QP Indicator 1 Outpatient referrals QP1 Indicator Practice Actions Monitoring/ evidence Points The practice meets internally to review The QP1 evidence template is 5 data on secondary care outpatient completed and returned to the CCG by referrals. 30 th September Practices to review outpatient referrals for top 3 specialties using either: - Outpatient data supplied by the CCG - Review of referrals as they are generated in the practice - Retrospective peer review of referrals using records held within the practice clinical system Referral Review Period: 1 st April 30 th June 2013 using CCG data. Practices using their own referrals or clinical data may continue until the evidence submission deadline). The Head of Locality to sign off the practice evidence return by 31 st October 2013.
67 Page 67 of 112 QP1. Summary Evidence Template Date(s) of the internal review meeting(s)/session(s): Names of GP(s) present in the review meeting(s)/session(s): The total number of outpatient GP referrals reviewed over the 3 month audit period: (minimum amount 10 per 1,000 on list size ) Names of the 3 main speciality referral areas reviewed Summary of Review Findings: The practice should comment on areas such as: - Reasons for any anomalies in activity levels between the practice and others - Any areas for improvement either internally within the practice or externally to services, care pathways or processes - Specify any educational or training needs which the CCG could support the practice with e.g.
68 Page 68 of 112 Development of inter or intra practice referrals - Clinical practice changes/lessons learnt/sharing of best practice As a result of the review what related commissioning intention recommendations would the practice want to be implemented during 2014/15? e.g. - New commissioned service - Clinical pathway changes - Contract variation/change to existing service - Decommission service
69 Page 69 of 112 QP Indicator 2 Outpatient referrals QP2 Indicator Practice Actions Monitoring/ evidence Points The practice participates in an external Practices to present QP1 findings at One single QP 2 template produced for 5 peer review with a group of practices to patch meeting for peer review and all participating practices submitted to compare its secondary care outpatient discussion of learning points. the CCG by 31 st October referral data and proposes areas for commissioning or service design improvements. The locality meeting will focus on identifying collective actions to improve internal practice performance and commissioning intentions to be taken forward by the CCG. Head of Locality to sign off returns made by 30 th November 2013
70 Page 70 of 112 QP2. Summary Evidence Template Date(s) of the external review meeting(s) Names of GP practice(s) and GPs present in the review meeting(s): Summary of Review Findings across all practices: The patch group should comment on areas such as: - Reasons for any anomalies in activity levels between practices - Any areas for improvement either internally within practices or externally to services, care pathways or processes - Specify any educational or training needs which the CCG could support practices with e.g. Development of inter or intra practice referrals - Clinical practice changes/lessons learnt/sharing of best practice
71 Page 71 of 112 As a result of the review what commissioning intention recommendations would the practices collectively want to be implemented during 2014/15? e.g. - New commissioned service - Clinical pathway changes - Contract variation/change to existing service - Decommission service (One single report to be generated for the whole patch group)
72 Page 72 of 112 QP Indicator 3 Outpatient referrals QP3 Indicator Practice Actions Monitoring/ evidence Points The practice engages with the The practice will evidence their The QP3 evidence template provided 11 development of and follows three adherence to the 3 developed care below is completed and returned to the agreed care pathways for improving the pathways (1 st July st Dec CCG by 31 st January ) by entering a read code when management of patients in the primary patients are managed / referred onto care setting to avoid inappropriate them. outpatient referrals. 1. Lower back pain with or without sciatica (Read Code 8CMW0) 2. Palpitations (Read Code 8CMWB) 3. Atrial Fibrillation (Read Code 8CMW2) In addition the practice will review their clinical practice changes, patient outcome improvements and any further recommended changes to the 3 clinical pathways. The Head of Locality to sign off the practice evidence return by 28 th February (Note - Read Code utilisation may be subject to random audit by the CCG during 2013/14)
73 Page 73 of 112 QP3. Summary Evidence Template Number of patients per 1000 the practice has referred and number of patients per 1000 managed in the primary care via the NHS West Kent CCG Lower Back Pain Pathway with or without sciatica (From 1 st July st Dec 2014 who have been Read Coded on the practice s clinical system) Number of patients per 1000 the practice has referred and number of patients per 1000 managed via the NHS West Kent CCG Palpitation Pathway (From 1 st July st Dec 2014 who have been Read Coded on the practice s clinical system) Number of patients per 1000 the practice has referred and number of patients per 1000 managed via the NHS West Kent CCG Atrial Fibrillation Pathway (From 1 st July st Dec 2014 who have been Read Coded on the practice s clinical system)
74 Page 74 of 112 AF Prevalence Rate (over 65s) 1 st April 2013: 1 st Jan 2014: (CCG average to be collated and shared with the practice) The practice should provide a summary of their utilisation of the 3 care pathways in terms of: - Reflect upon the data - Changes in clinical practice - Patient clinical outcome improvements - Any suggested amendments including new components to the existing care pathways - Lessons Learnt
75 Page 75 of 112 QP Indicator 4 Emergency Admissions QP4 Indicator Actions Monitoring/ evidence Points The practice meets internally to review The QP9 evidence template is returned 5 data on emergency admissions. to the CCG by 31 st October Practices to complete a review of all emergency admissions (In and Out of Hours) from data supplied by the CCG or generated by the GP practice via their clinical system records. Referral Review Period: 1 st April 30 th June The Head of Locality to sign off the practice evidence return by 30 th November 2013.
76 Page 76 of 112 QP4. Summary Evidence Template Date(s) of the internal review meeting(s)/session(s): Names of GP(s) present in the review meeting(s)/session(s): Number of emergency GP admissions reviewed (split by in hours and those via GP OOH service) (All admissions during the audit period are to be reviewed) Summary of Review Findings: The practice should comment on areas such as: - Reasons for any anomalies in activity levels between the practice and others - Any areas for improvement either internally within the practice or externally to services, care pathways or processes - Specify any educational or training needs which the CCG could support the practice with? - Clinical practice
77 Page 77 of 112 changes/lessons learnt/sharing of best practice, steps taken to intervene/ prevent emergency admissions As a result of the review what commissioning intention recommendations would the practice want to be implemented during 2014/15? e.g. - New commissioned service - Clinical pathway changes - Contract variation/change to existing service - Decommission service
78 Page 78 of 112 QP Indicator 5 Emergency Admissions QP5 Indicator Actions Monitoring/ evidence Points The practice participates in an external Practices to present QP4 findings at One single QP 5 template produced for 15 peer review with a group of practices to locality meeting for peer review all participating practices and submitted compare its data on emergency discussion and learning points. to the CCG by 30 th November admissions and propose areas for commissioning or service design improvements. Head of Locality to sign off returns made by 31 st December 2013
79 Page 79 of 112 QP5. Summary Evidence Template Date(s) of the external review meeting(s) Names of GP practice(s) and GPs present in the review meeting(s): Summary of Review Findings across all practices: The patch group should comment on areas such as: - Reasons for any anomalies in activity levels between practices in or during OOH periods - Any areas for improvement either internally within practices or externally to services, care pathways or processes - Specify any educational or training needs which the CCG could support practices with - Clinical practice changes/lessons learnt/sharing of best practice, Focus on how the practice can amend or improve their
80 Page 80 of 112 treatment including primary prevention/risk assessment and management of patient sin primary care to help avoid emergency admissions. As a result of the review what commissioning intention recommendations would the practices collectively want to be implemented during 2014/15? e.g. - New commissioned service - Clinical pathway changes - Contract variation/change to existing service - Decommission service (One single report to be generated for the whole patch group)
81 Page 81 of 112 QP Indicator 6 Emergency Admissions QP6 Indicator Actions Monitoring/ evidence Points The practice engages with the The practice will evidence their The QP6 evidence template provided 28 development of and follows three adherence to the 3 developed care below is completed and returned to the agreed care pathways for improving the pathways (1 st July st Dec CCG by 31 st January ) by entering a read code when management and treatment of patients patients are managed / referred onto in the primary care setting to avoid them. emergency admissions. 1. Falls (Read Code 8CMW4) 2. COPD Exacerbation Pathway (Read Code 8CMW5) 3. EOL (8CMW3) In addition the practice will review their clinical practice changes, patient outcome improvements and any further recommended changes to the 3 clinical pathways. The Head of Locality to sign off the practice evidence return by 28th February (Read Code utilisation rates may be subject to random audit by the CCG during 2013/14)
82 Page 82 of 112 QP6. Summary Evidence Template Number of patients per 1000 the practice has referred and number of patients per 1000 the practice has managed in primary care via the NHS West Kent CCG Falls Pathway (From 1 st July st Dec 2014 who have been Read Coded on the practice s clinical system) Number of patients per 1000 the practice has referred and number of patients per 1000 the practice has managed via the NHS West Kent CCG COPD Exacerbation Pathway (From 1st July st Dec 2014 who have been Read Coded on the practice s clinical system) Number of patients per 1000 the practice has referred and number of patients per 1000 the practice has managed via the NHS West Kent CCG End of Life Pathway. (From 1st July st Dec 2014 who have been Read Coded on the practice s clinical system)
83 Page 83 of 112 Number/Percentage of patients on the practices EOL register who died in their preferred place of death COPD Prevalence Rate 1 st April 2013: 1 st Feb 2014: (CCG average to be collated and shared with the practice) The practice should provide a summary of their utilisation of the 3 care pathways in terms of: - Reflect upon the data - Changes in clinical practice - Patient clinical outcome improvements - Any suggested amendments including new components to the existing care pathways - Lessons learnt
84 Page 84 of 112 QP Indicator 7 Accident & Emergency attendances QP7 Indicator Actions Monitoring/ evidence Points The practice meets internally to review Practices to complete a review of A&E The QP7 evidence template provided 7 data on A&E attendances. The review attendances from data supplied by the below is completed and returned to the will include consideration of whether CCG. CCG by 28 th February 2014 for sign off access to clinicians in the practice is by the Head of locality. appropriate in light of the patterns on Data will initially be supplied for the A&E attendance. final quarter of 2012/13 (1 st January 31 st March and then monthly thereafter until 31 st December 2013).
85 Page 85 of 112 QP7. Summary Evidence Template Date of Internal Review Meeting: GPs Present in meeting: Total number of A&E attendances reviewed (A&E referrals provided to be reviewed split by in hours and OOH periods) Summary of Review Findings: - Number of avoidable A&E attendances during in hours periods with an explanation and proposed solutions - Number of avoidable A&E attendances during OOH periods with an explanation and proposed solutions - Explore the reasons for registered patients attendance(s) at A&E, identifying any emerging
86 Page 86 of 112 patterns and discussing this with reference to available care pathways and the capability and access with primary care services to see and treat patients. - Focus should be a) older patients with comorbidities at high risk of admission, b) Children with minor illness / injury. C) Frequent attendees that can be dealt with in primary care - A summary of the review of the practice s same day access arrangements. E.g. Are all patients who request a same day appointment offered an appointment, is clinical triage by nurse or doctor by telephone undertaken, is an open access clinic available or are patients told to telephone before a set time?
87 Page 87 of 112 As a result of the review what commissioning intention recommendations would the practice want to be implemented during 2014/15? e.g. - New commissioned service - Clinical pathway changes - Contract variation/change to existing service - Decommissioning of services
88 Page 88 of 112 QP Indicator 8 Accident & Emergency attendances QP8 Indicator Actions Monitoring/ evidence Points The practice participates in an external Practices to bring completed QP 7 One single QP 8 template produced for 9 peer review with a group of practices to templates to patch/locality meeting. all participating practices and submitted compare its data on A&E attendances to the CCG by 28 th February 2014 for and agrees an improvement plan. The sign off by the Head of Locality. review should include, if appropriate, proposals for improvement to access arrangements in the practice in order to reduce avoidable A&E attendances and may also include proposals for commissioning or service design improvements.
89 Page 89 of 112 QP8. Summary Evidence Template Date(s) of the external review meeting(s) Names of GP practice(s) and GPs present in the review meeting(s): Summary of Review Findings across all practices, discuss variances, reflect upon the reasons. The patch group / Locality should comment on areas such as: - An overview of practices current same day access models and the benefits or constraints of different models E.g. Are all patients who request a same day appointment offered an appointment, is clinical triage by nurse or doctor by telephone undertaken, is an open access clinic available or are patients told to telephone before s set time etc. - What overall themes did the practices observe regarding inappropriate
90 Page 90 of 112 or avoidable in hours attendances? And where improvements can be made - What overall themes did the practices observe regarding inappropriate or avoidable out of hours attendances? And where improvements can be made As a result of the review what commissioning intention recommendations would the practices collectively want to be implemented during 2014/15? e.g. - New commissioned service - Clinical pathway changes - Contract variation/change to existing service - Decommissioned services
91 Page 91 of 112 QP Indicator 9 Accident & Emergency attendances QP9 Indicator Actions Monitoring/ evidence Points The practice implements the The practice produces an improvement The practice should submit the 15 improvement plan that aims to reduce plan outlining their actions and findings attached A&E improvement plan avoidable A&E attendances and from QP7 and QP 8. template by February 28 th 2014 for sign produces a report of the action taken. off by the Head of Locality.
92 Page 92 of 112 QP9. Improvement Plan to reduce avoidable accident and emergency attendances Description of what actions were/will be taken by the practice to reduce avoidable A&E attendances? (Please describe the actions in terms of: patient target group ( Elderly with co-morbidities, children with minor illness / injuries, frequent attendees), methodology, resource requirements, cost (if any), timescale and any other relevant information) What action(s) worked well/did not work well, what supporting evidence is there and could the initiative(s) be rolled out to other practices/areas? If the improvement action is still to be implemented please describe how you will monitor the effectiveness of the initiative or any actions to mitigate risk? Has the practice identified any other areas where the practice could be supported by the CCG? E.g. could include any of the following: Same Day Access/Clinical Triage Training, Acute consultant advice ( /direct bypass number) Roaming GP for acute/home visits, Collaborative/Buddying up of GP Practice working, GP in A&E/Acute Service Integration, OOH Surgeries, GPOOH model review
93 Page 93 of 112 Front Sheet for Papers Title of Report: Programme Governance Structure This paper is for: Approval Recommendation: The Governing Body are asked to approve the development of the programme governance framework set out in the report that will support West Kent Clinical Commissioning Group s (CCG) duty to commission health care. For further information or for any enquiries relating to this report please contact: Evelyn White Acting Chief Operating Officer evelyn.white@nhs.net Reporting Officer: Evelyn White Lead Director: Evelyn White Report Summary: Date: Agenda Item: Version: The paper outlines a proposed programme governance framework to support West Kent Clinical Commissioning Group s (CCG) duty to commission health care. It builds on a review of the CCG s constitution and standing orders and a discussion with members of the Clinical Strategy Committee (CSG) as well as key officers within the CCG. The paper focuses predominantly on those committees and groups which have a direct influence on the commissioning of health care. The paper was approved by CSG on 11 th June FOI status: This paper is disclosable under the FOI Act Strategic objectives links: Board Assurance Framework links: Identified risks & risk management actions: Resource implications: Legal implications The development of this structure will contribute to the mitigation the risks identified in the Assurance Framework relating to programme delivery and assurance. Commissioning Plan delivery The development of this structure will contribute to the mitigation the risks identified in the Assurance Framework relating to programme delivery and assurance. No additional resources will be required n/a
94 Page 94 of 112 including equality and diversity assessment Report history: This paper was approved by CSG on 11 th June Appendices Annex 1 and 2 to report Next steps: Establish programme oversight groups that ensure delivery of plans for 13/14 and support the development of planning for 14/15 onwards as set out in the report
95 Page 95 of 112 WEST KENT CLINICAL COMMISSIONING GROUP Report to Governing Body Programme Governance Arrangements Developing and delivering the Commissioning Strategy 1 INTRODUCTION 1.1 This document outlines a proposed programme governance framework to support West Kent Clinical Commissioning Group s (CCG) duty to commission health care. It builds on a review of the CCG s constitution and standing orders and a discussion with members of the Clinical Strategy Committee (CSG) as well as key officers within the CCG. 1.2 The paper focuses predominantly on those committees and groups which have a direct influence on the commissioning of health care. 2 STATUTORY FUNCTIONS AND ACCOUNTABILITY 2.1 Whilst recognising that the Governing Body (GB) has operational accountability for ensuring the Group s duties to commission health care are met, it has delegated functions to four standing committees. These provide a more informal and targeted arena within which to develop strategies appropriate to their remit, provide assurance to the GB that these strategies are being delivered and develop any supporting policies to ensure effective governance. These committees cover: Finance and Performance Quality and Safety Clinical Strategy Group (CSG) Practice Engagement 2.2 Given that the CCG is in the early stages of operating within its agreed constitution, the modus operandi for its committees are kept under review in order to reduce the risk of unnecessary duplication of effort or confusion in decision making. 2.3 If the committees are to remain strategic and provide an overarching view of CCG performance then they will need to be supported by an effective underpinning planning and delivery structure. This structure will be need to be able to manage the flow of information to these committees and support the extensive stakeholder engagement that will be needed deliver local commissioning priorities. 3 PROPOSED PROGRAMME GOVERNANCE STRUCTURE 3.1 The proposed programme governance structure outlined in the Tables 1 and 2 build on the CCG s values and a set of principles that seek high quality innovative service change through active stakeholder engagement. This includes not only active membership involvement and public and patient engagement but also access to the support and expertise from other health and social care providers, the public, private and voluntary sector as appropriate. 3.2 Table 1 shows the scope and reporting arrangement of the proposed programme agenda and Table 2 the associated roles and responsibilities of the proposed governance structure within the CCG. 3.3 The four proposed programme areas of Planned Care, Integrated Commissioning, Urgent Care and Mental Health have been identified as the key areas of focus for the four locality teams (see Table 3) and underpinning clinical priorities aligned accordingly.
96 Page 96 of 112 These underpinning priorities include both condition specific and cross cutting strategies such as medicine management and risk stratification to secure a coherent approach to health improvement. 3.4 To drive each clinical programme four oversight groups are proposed. The form of these groups needs to reflect their function and their relationship to the four Governing Body standing committees, mentioned earlier (A draft TOR can be found in Annex 1). 3.5 To support this programme approach, member representatives from the four localities appointed to the Governing Body and the CSG will have a lead responsibility within each programme and supported by locality commissioning teams will be accountable for the delivery of a wide range of commissioning priorities. 3.6 The CSG will oversee the individual work programmes making sure that the locality / programme teams work closely with each other particularly around cross cutting priorities e.g. the need to support new integrated models of care for people with LTC whether in designing new pathways, addressing inequalities in access and in managing times of crisis; and also that dementia services works closely with mental health provision to maximise access to high quality care. 3.7 Each programme s oversight group will work within a programme management framework which: Helps the CSG to identify commissioning priorities tested and agreed with the key stakeholders and evidencing that these: o o o Add value to the patient experience building on an evidence base and are in line with the JSNA Are deliverable and do not conflict with any other clinical commissioning priority Deliver an economic model of care which addresses the demographic and financial challenges facing the health economy Uses the agreed planning tools and expertise within the Programme Management Office to deliver the agreed plans. 3.8 The CCG Programme Management Office (PMO) will work with locality commissioning teams and programme oversight groups to ensure appropriate operational, administrative, programme and project management support is given to each priority. An indicative programme management process has been outlined in Table 4 to start to describe the roles and links between the different decision making levels within the organisation (this will need further refinement). 3.9 As the CCG is still developing both its GP and Practice engagement and its PPE strategy (annex 2) the programme governance framework cannot be specific about how stakeholder engagement will operate. Nevertheless it is important this is targeted and timely and examples of where stakeholder engagement (particularly member engagement) would be of benefit have been highlighted in the programme management process in Table The underpinning structure for each programme needs to reflect the priorities it seeks to address and as such should remain adaptable to changing need. For example access to clinical networks provides the CCG with access to specialist input when identifying best practice and or reviewing clinical pathways (through simulation techniques). However they could operate as a virtual forum of informed stakeholders brought together for a specific task or project which may in some instances be facilitated by providers e.g. HASCIP, or social care. 4 CONCLUSION 4.1 The Clinical Strategy Committee is asked to recommend this proposal to the CCG Governing Body. In doing so to seek its support for the: Appointment of strategic clinical leads for each programme area
97 Page 97 of 112 CSG in monitoring the effectiveness of programme governance as a mechanism for delivering the CCG commissioning strategy.
98 Membership engagement from 62 practices, 12 patches and 4 Localities Page 98 of 112 Table 1: Commissioning Governance overview Vision and Values A safe sustainable and affordable patient focused healthcare service that provides quality patient experience and improves outcomes for local people Focused on the values of: Clinical leadership; quality and safety; focus on benefits; working in partnership; openness and transparency; evidence based decisions; Individuals; courage; trust; the team Programme Governance and Partnerships Governing Body Health and Wellbeing Board Quality & Safety Committee Finance & Performance Committee Practice Engagement Committee Clinical Strategy Committee 4 Clinical programmes (whole system approach) Public Health (KCC) Locality commissioning teams and PMO Kent and Medway Commissioning Support (KMCS) Senior Management team Strategic Aims A thriving local NHS provider landscape for the West Kent population which delivers safe and high quality urgent and non- urgent care. Improved patient and carer experience of End of Life Care. Improved and integrated health and social care arrangements for vulnerable adults. Support and enhance healthcare provided by General Practice. Engaged and empowered patients who are Clinical Programmes (indicative areas of focus) Based on following guiding principles: Quality contribution to the NHS Outcomes Framework; Clinical leadership; Patient and public voice; Equality and health inequalities; Innovation and service improvement. Planned care Community & Primary Care (an integrated approach) LTC pathways (including Diabetes Network, Cancer, CHD and Heart failure) Elective pathways including Out of hospital care Primary care improvement (Medicine Optimisation, Tackling Inequalities) Older People (including: Dementia, EOL care, integrated health and social care teams supporting LTC, falls management, carers, self care management) Children and Maternity (Vulnerable children, disabilities, acute care - KMCS led) Learning Disability (KMCS led) Continuing Health Care (KMCS Led) Enablers to support the drive for improvement System leadership whole system strategy. Locality commissioning team supporting Primary care improvement, strategic planning, contract management and performance review Public heath links via MOU and underpinned by JSNA and H&WB strategy Quality and safety strategy (including Workforce development);
99 Page 99 of 112 able to manage their own health and make informed decisions. Improved value for money and outcomes for people with Mental Health needs including dementia. Urgent care Mental Health Emergency care (Trauma Networks, Critical care response) Urgent care(a&e, Minor Injury and illness, NHS 111 and OOH) Unscheduled care (Rapid response, Intermediate care, complex multiple LTC management) Live it well (Psychological therapies; Stable long term conditions) Acute care (Payment by Results; Pathways delivering more in the community) Child and Adolescent Mental Health Services Dementia (linked to community and primary care) Recovery Finance and 3-5 year investment plans; Contracting and performance management framework including PMO and BI from KMCS; Communication strategy and engagement framework (Patients and Public, voluntary sector and wider stakeholders); IM&T strategy
100 Page 100 of 112 Table 2: Governance Roles and Responsibilities / Terms of reference Governing Body Committees (also includes Audit & Remuneration committee) focused on Strategy, Assurance and Policy Clinical Programme Oversight Groups Strategy, Prioritisation through engagement and Redesign with Project management Locality teams Programme Management office Management team Tasked by Members to Lead the Group s work commissioning health services. Ensure the Group is well governed. Determining and paying salaries and allowances. Reserves to itself Plan and set strategy Set culture Ensure control and good governance Build organisational effectiveness Provide accountability to Members Delegated to committees Clinical Strategy Practice Engagement Quality and safety Finance and Performance Recommend to the governing body a clinical strategy and annual commissioning plan and oversee the delivery of the commissioning plan. Under the leadership of the Clinical Strategy committee strategic change programmes will be driven by members and cocreated with providers across the whole range of service priorities. Steer the development and implementation of a GP & Practice engagement strategy. Support members in terms of capacity and capability to deliver on target and commissioning intentions. Act as a conduit with the locality team. Assure the performance management of and improve quality and safety of commissioned services; leading the groups work on safeguarding and supporting NHS England to secure continuous improvement in primary medical services. Assure the governing body that its expenditure delivers value for money and key national targets Planned Care (includes LTC Networks) Community and Primary care (an integrated approach - including Primary care, Older people Children & Maternity and L Disability) Urgent Care (Emergency, Urgent and Unscheduled care) Mental Health (Joint Commissioning - all age) Programme Leadership focused on: Strategic commissioning: Agreeing intentions set in the context of JSNA and health equity audits and action planning delivered through a robust project management framework. Service Redesign: Linking to priorities within: H&WBS, other strategic programmes, NHSCB specialist commissioning, localities and primary care. Stakeholder engagement: In line with both the GP and Practice engagement and the Patient and Public engagement strategies to secure an effective local network for providers, service users and carers to support monitoring and pathway redesign. Shaping Supply: Developing strategies to address gaps or weakness in the supply chain. Performance Management: Reviewing performance in relation to national and local targets and strategic priorities; reviewing trends in current service user and carer experience. Working in a matrix framework each locality team will be responsible for: Delivering improvements in local clinical services as well as driving forward one of four core programme areas: Planned Care Community and Primary Care Urgent Care Mental Health For each programme area they will have responsibility for driving the oversight group and providing project / programme management expertise to deliver agreed commissioning intentions. This will also include a lead role on key provider contracts. Each locality will also focus on supporting improvements across primary care working closely with Practice Engagement committee and picking up the actions associated with the programme boards including services identified in the HWBS. To deliver five key functions: Governance and performance reporting (including budget expenditure) Value Adding Performance Management (benchmarking) Benefits Delivery Assurance (assessing priorities scope and impact) Portfolio / Programme Management (providing tools and quality assure key documents) Programme / Project Management Excellence (training) To sense check all project proposals emerging from the agreed strategies before presenting for approval to the Clinical Strategy Group to ensure that commissioning intentions meet the test of improving outcomes and address the financial challenges within the local health economy
101 Page 101 of 112 Health and Wellbeing Board NHS England To lead and advise on work to improve the health and wellbeing of the people of Kent through joined up commissioning across the NHS, social care, public health and other services in order to secure better health and wellbeing outcomes in Kent and better quality of care for all patients and care users. The HWB has a primary responsibility to make sure that health care services paid for by public monies are provided in a cost-effective manner and in doing so will: Assess the needs of the local population and lead the statutory joint strategic needs assessment. Promote integration and partnership across areas, including through promoting joined up commissioning plans across NHS, social care and public health. Support joint commissioning and pooled arrangements, where all parties agree this makes sense. Primary care, Specialised commissioning, Accountability
102 Table 3: Locality commissioning / programme management team Page 102 of 112
103 Page 103 of 112 Chief Finance Officer Reg Middleton Chief Operating Officer Gail Arnold* Business Support Rachael Barnes Deputy Chief operating officer Invicta locality & integrated commissioning VACANT Head of M&M locality commissioning & Planned Care 8c Kirsteen Murray (interim) Head of T&TW locality commissioning & Urgent Care programme area Mark Atkinson Head of Sevenoaks locality commissioning & Mental Health Dave Holman Head of PMO Mark Lisher (Interim) Head of medicines Optimisation Heather Carter** Senior Admin Support Sarah Barlow Children & maternity commissioning Project support officer Ife Adesola Integrated commissioning support Business Intelligence Finance Head of programme area Martine McCahon Commissioning Manager Neil Francis Project Managers Sandra Wilson Pharmacy Technicians Jo Skinner / vacant Commissioning Support Officer Sam Padfield Admin Support officer Kimberly Watt Project support officer Lorna Willis PCB Team Project support officer Mutsa Machiri Business Intelligence Finance Commissioning Manager 8a Mona Hara (Interim) Commissioning Manager Nazima Chauhan Project Managers Claire Ripley Jo Beech Angela Broomby Project officer Band 6 VACANT Pharmacy Technician Kirsite Moody Admin Support Officer Stella Caswell Finance Business Intelligence Commissioning Manager 8a Martyn Kent (Interim) Project Manager Michelle Armstrong Project Officer Band 6 VACANT Pharmacy Technicians Sarah Trimmer/ vacant Admin Support officer Yasmin Blunden Project support officer Joyce Domaley Finance PMO support officer Fay Lacey Business Intelligence Commissioning manager 8a James De Pury (Interim) Project Manager band 7 VACANT Pharmacy Technician Louise Downs Admin Support officer Adam Hall Prescribing advisor T&TW Weald Sevenoaks Jagdeep Minhas Prescribing advisor Invicta & M&M Janice Moorekite Administrator Nathalie Mulroy Project support officer 4 Programme coordinator 6 *Acting Chief Operating officer Evelyn White **Acting Head of Medicines Optimisation Priscilla Kankam
104 Page 104 of 112 Table 4 Indicative Programme Governance and Commissioning Road Map
105 Start contact negotiations Page 105 of 112 Indicative roadmap - Delivering West Kent CCG s Clinical Strategy Governing Body meetings Membership and stakeholder engagement points Programme flow Governing Body Committees Practice Engagement Clinical Strategy Agree vision and strategic objectives Agree and or review GP engagement strategy and policy Review Needs assessment Agree strategic programme priorities and financial strategy Identify commissioning priorities Review primary care performance and strengthen capacity and capability to respond to commissioning intentions Review all programmes and test coherence within CCG commissioning framework Agree draft commissioning intentions Finalise annual commissioning plans Agree final commissioning intentions Finance and Performance Quality and Safety Agree and or review finance strategy performance and contracting framework Agree and or review quality and safety strategy and policy Programme oversight groups Planned care Community and Primary care Establish stakeholder engagement and planning processes to address strategic priorities Test coherence of implementation plans across the programme and advise on commissioning intentions Finalise work programme and ongoing engagement framework Bi monthly monitoring to CSG Identify impact on contracts and investment plans Urgent care Mental health Locality Commissioner Project management / PMO Secure Project management capacity and capability Develop implementation plan and 3-5 year goals, outcomes and KPIs for each priority area Draft PID / business plan for key commissioning intentions Project management delivery and engagement process Senior Management team Sense check PIDs
106 Page 106 of 112 Annex 1 Terms of reference for Programme Oversight Groups Overview For each programme area an oversight group will have responsibility for supporting the delivery of the CCG s strategic aims providing project / programme management expertise to deliver agreed commissioning intentions. The oversight groups will promote joint working in both design and implementation of new clinical pathways with members, patient and public and partner organisations and report to the Clinical Strategy Committee on progress. Membership The membership of the group shall consist of: The Clinical Lead for the programme (who will chair the PM Oversight group); The Lead locality commissioner for the programme; The Lead finance officer for the programme Commissioning leads (clinical and or managerial) for the main agreed sub programmes Programme / project management support (from the locality team) Objectives Help the CSG identify the priorities for the programme set in the context of the JSNA and health equity audits. Coordinate the work plan and ensure alignment across the programme with other programmes, with other localities and the overarching CCG priorities. Promote good practice and effective ways of working including the adoption of an appropriate project management approach for each project and within this ensure an effective mechanism is established for the realisation of benefits. Identify and manage any subsequent consultation and communication strategy associated with commissioning intentions. Approve and monitor the financial management of the Programme securing financial control and oversight of associated QiPP plans. In line with both the GP and Practice and the Patient and Public engagement strategies secure an effective local network for providers, service users and carers to support monitoring and pathway redesign. Implement and manage a risk management framework across the programme. Identify and where agreed, develop plans to address gaps or weaknesses in the supply chain Review performance in relation to national and local targets and strategic priorities; reviewing trends in current service user and carer experience. Frequency of meetings The group should meet at least monthly and more frequently when the agenda requires it. Reporting The group should report to the Clinical Strategy Committee on a bi-monthly basis against agreed priorities. Review The terms of references should be reviewed by the Clinical strategy committee at least annually
107 Page 107 of /15 Indicative Scope of the Strategic Oversight Groups Programme Planned Care Sub programme area Elective care pathways including Care Closer to Home Current Clinical focus and underpinning strategies Includes reforming outpatient flows and referral management Long term condition pathways Includes but not exclusive to: Diabetes (Network in place) COPD Heart Failure Risk Stratification Opthamology, and Audiology Ensure pathways are effective Integrated Commissioning Primary Care Medicine management (steering group exists) Health Inequalities Urgent care Older People / Long term conditions Children Learning Disability Critical care pathways Integrated working o Health and social care integration o Practice focused MDTs Improving outcomes and patient experience o Dementia o End of Life care Reablement (linked to Urgent Care) Vulnerable children Children with disabilities Implement recommendations following Winterbourne View report Improve SAF performance Trauma Networks Stroke Urgent care models Ambulatory services (NHS111/OOH/Minor illness and injury) Unscheduled care Intermediate care and support for complex co morbidity in LTC o Integrated rapid response Mental Health Acute care Payment by results New pathways Recovery Living well IAPT Community mental Health workers
108 Page 108 of 112 Other Drugs and alcohol disorders Personality disorders Dementia (linked to Integrated Commissioning)

109 Page 109 of 112 Annex 2 - Public and Patient Engagement GP Practice Patient Participation Groups 39 GP Practices in West Kent have established Patient Participation Groups (PPGs) and another 12 are in the process of setting them up. These are the core groups through which West Kent CCG will initiate patient and public dialogue. The Chairs or nominated representatives meet 4 to 6 weekly with the CCG Chair and Lay Board Member to gain greater understanding of the work of the CCG and how the PPGs can contribute. The CCG will review individual and collective feedback from Practice surveys and act on key themes that can be addressed at CCG level. CCG Patient Reference Group (PRG) West Kent CCG has created a forum in which PPG Chairs or nominated representatives can meet with the CCG Chair and Lay Board member with responsibility for patient and public engagement to promote feedback from individual practices up to the CCG and vice versa. A website has been set up where the groups can access and add West Kent PPG and CCG information: CCG Patient representation on the Board The Board lay member plays, and will continue to play, a key role in developing West Kent CCG s approach to public and patient engagement. Alongside the Board lay member it is planned to have a representative from the CCG PRG who will be selected to sit as observer on the Board, with the Board lay member providing mentorship. The PRG representative will ensure key messages are fed up to the Board from the PRG and vice versa. CCG HealthNetwork Since April people and organisations in West Kent have been invited to become a member of a virtual Patient and Public Network. This will be used to share CCG information, via a HealthNetwork newsletter and through the members contacts database. Members will be invited to take part in surveys, focus groups, special interest groups etc. as required. Invitations to join have been sent out to community venues and GP practices and have been promoted at internal and external events. The membership is currently nearly 200. Collating, comparing and using patient experience/insights Patient experience is currently captured by a range of commissioning and provider organisations across the. Work is being conducted with all key insights/experience/complaints leads across the West Kent CCG locality to: map what is currently collected / known; identify what intelligence could be pooled as a shared database; identify potential complementary activity that could inform commissioning and/or designing/improving services. This centralised system of shared knowledge and intelligence will be used to report back to the Quality Committee, to ensure that information from patient feedback, complaints and incidents is used to continuously improve patient experience of commissioned services (from the CCG s Constitution).
DRAFT MINUTES of the NHS West Kent CCG Governing Body Meeting Held in Public
 DRAFT MINUTES of the NHS West Kent CCG Governing Body Meeting Held in Public Meeting held on Tuesday 23 rd May 2017 at 13.30 hrs At the Hadlow Manor Hotel, Maidstone Road, Tonbridge, Kent, TN11 OJH Date
DRAFT MINUTES of the NHS West Kent CCG Governing Body Meeting Held in Public Meeting held on Tuesday 23 rd May 2017 at 13.30 hrs At the Hadlow Manor Hotel, Maidstone Road, Tonbridge, Kent, TN11 OJH Date
Agenda and Papers. NHS West Kent Clinical Commissioning Group Governing Body. Tuesday 24 th February 2015 At 1.30 pm
 Agenda and Papers for the NHS West Kent Clinical Commissioning Group Governing Body To be held on Tuesday 24 th February 2015 At 1.30 pm at The Village Hotel, Castle View, Forstal Road, Sandling, Maidstone
Agenda and Papers for the NHS West Kent Clinical Commissioning Group Governing Body To be held on Tuesday 24 th February 2015 At 1.30 pm at The Village Hotel, Castle View, Forstal Road, Sandling, Maidstone
Clinical Strategy Group
 Clinical Strategy Group April 2016 This paper is for: Governing Body Recommendation: To note the report from the Clinical Strategy Group For further information or for any enquiries relating to this report
Clinical Strategy Group April 2016 This paper is for: Governing Body Recommendation: To note the report from the Clinical Strategy Group For further information or for any enquiries relating to this report
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Figure 1: Domains of the Three Adult Outcomes Frameworks
 Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Integrated Performance Report
 Integrated Performance Report January 2015 1 Patient focused, Providing quality, improving outcomes Contents: Page: Executive Summary 3 Assurance Framework Scorecard 4 NHS Outcomes Domains are health outcomes
Integrated Performance Report January 2015 1 Patient focused, Providing quality, improving outcomes Contents: Page: Executive Summary 3 Assurance Framework Scorecard 4 NHS Outcomes Domains are health outcomes
Whittington Health Quality Strategy
 Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Outcomes benchmarking support packs: CCG level
 Outcomes benchmarking support packs: CCG level NHS South Devon and Torbay CCG Produced with input from: Public Health England Forward and Introduction Local decision making is at the heart of the NHS,
Outcomes benchmarking support packs: CCG level NHS South Devon and Torbay CCG Produced with input from: Public Health England Forward and Introduction Local decision making is at the heart of the NHS,
NHS Ashford Clinical Commissioning Group. Integrated Performance Report. November 2013
 NHS Ashford Clinical Commissioning Group Integrated Performance Report November 2013 Page 1 Contents Executive Summary... 6 Assurance Framework Overview... 10 Are local people getting good quality care?...
NHS Ashford Clinical Commissioning Group Integrated Performance Report November 2013 Page 1 Contents Executive Summary... 6 Assurance Framework Overview... 10 Are local people getting good quality care?...
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016
 Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Sheet. Discussion. For: Decision. Noting. title: Author: Lead Director. Quality t Office. Director: and - 1 -
 Governing Body Paper Summary Sheet Date of Meeting: 23 April 2013 For: Decision Discussion Noting Agenda item and title: Author: GOV/13/04b/08 Operational Targets 2013/14 John Dudgeon Head of Information
Governing Body Paper Summary Sheet Date of Meeting: 23 April 2013 For: Decision Discussion Noting Agenda item and title: Author: GOV/13/04b/08 Operational Targets 2013/14 John Dudgeon Head of Information
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Newham Borough Summary report
 Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
Westminster Partnership Board for Health and Care. 21 February pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
West Mid Beds Locality Development Plan
 West Mid Beds Locality Development Plan 2013-14 Contents Introduction..3 1. Key Progress 2012/13.. 4 2. Locality Objectives 2013/14.5 2.1 Commissioning.5 2.2 Performance & Finance.. 9 2.3 Engagement 11
West Mid Beds Locality Development Plan 2013-14 Contents Introduction..3 1. Key Progress 2012/13.. 4 2. Locality Objectives 2013/14.5 2.1 Commissioning.5 2.2 Performance & Finance.. 9 2.3 Engagement 11
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Agenda and Papers. NHS West Kent Clinical Commissioning Group Governing Body Meeting. Tuesday 27 th June 2017 At 1.30pm
 Agenda and Papers for the NHS West Kent Clinical Commissioning Group Governing Body Meeting To be held on Tuesday 27 th June 2017 At 1.30pm at The Village Hotel, Forstal Road, Maidstone, Kent ME14 3AQ
Agenda and Papers for the NHS West Kent Clinical Commissioning Group Governing Body Meeting To be held on Tuesday 27 th June 2017 At 1.30pm at The Village Hotel, Forstal Road, Maidstone, Kent ME14 3AQ
Report to the Merton Clinical Commissioning Group Governing Body
 MCCG GB 19.09.1 Pt1 Att 09 Report to the Merton Clinical oning Group Governing Body Date of Meeting: 16 th September 01 Agenda No: 8.1 Attachment: 09 Title of Document: Performance Framework and Balanced
MCCG GB 19.09.1 Pt1 Att 09 Report to the Merton Clinical oning Group Governing Body Date of Meeting: 16 th September 01 Agenda No: 8.1 Attachment: 09 Title of Document: Performance Framework and Balanced
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Quality Framework Supplemental
 Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE
 Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
National Clinical Audit programme
 National Clinical Audit programme Danny Keenan Medical Director www.hqip.org.uk Who are HQIP? HQIP is a not-for profit, professional/patient partnership, aiming to change and improve health and social
National Clinical Audit programme Danny Keenan Medical Director www.hqip.org.uk Who are HQIP? HQIP is a not-for profit, professional/patient partnership, aiming to change and improve health and social
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Delegated Commissioning Updated following latest NHS England Guidance
 Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
Draft Minutes. Agenda Item: 16
 Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
NHS Rushcliffe CCG Governing Body Meeting. CCG Improvement and Assurance Framework. 15 March 2018
 RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16
 Schemes for 2015/16") Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Quality, Safety and Patient Experience Strategy
 Quality, Safety and Patient Experience Strategy November 2015 www.castlepointandrochfordccg.nhs.uk Document Name Quality, Safety & Patient Experience Strategy Version V7 Author/s Name Job Title/s Jenny
Quality, Safety and Patient Experience Strategy November 2015 www.castlepointandrochfordccg.nhs.uk Document Name Quality, Safety & Patient Experience Strategy Version V7 Author/s Name Job Title/s Jenny
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
QUALITY IMPROVEMENT COMMITTEE
 : 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
: 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
Improvement and Assessment Framework Q1 performance and six clinical priority areas
 Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
NHS THANET CLINICAL COMMISSIONING GROUP GOVERNING BODY. TUESDAY 21 NOVEMBER 2017 AGENDA PART ONE (Public) - 13:00-13:10. Chair Dr Tony Martin
 - 13:00-13:10. Chair Dr Tony Martin") NHS THANET CLINICAL COMMISSIONING GROUP GOVERNING BODY HELD IN THE HARBOUR SANDS MEETING ROOM, 3 RD FLOOR, THANET DISTRICT COUNCIL TUESDAY 21 NOVEMBER 2017 AGENDA PART ONE (Public) - 13:00-13:10 Chair
NHS THANET CLINICAL COMMISSIONING GROUP GOVERNING BODY HELD IN THE HARBOUR SANDS MEETING ROOM, 3 RD FLOOR, THANET DISTRICT COUNCIL TUESDAY 21 NOVEMBER 2017 AGENDA PART ONE (Public) - 13:00-13:10 Chair
NHS Leeds West CCG Clinical Commissioning Strategy. 2013/14 to 2015/16
 NHS Leeds West CCG Clinical Commissioning Strategy 2013/14 to 2015/16 Working together locally to achieve the best health and care in all our communities 1 Contents Section 1: Summary Page 3 Section 2:
NHS Leeds West CCG Clinical Commissioning Strategy 2013/14 to 2015/16 Working together locally to achieve the best health and care in all our communities 1 Contents Section 1: Summary Page 3 Section 2:
NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION
 NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: [78] NHS England Effective Date: 1 December 2015 April 2017 CONTENTS Part Description Page Foreword 1 1 Introduction and Commencement
NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: [78] NHS England Effective Date: 1 December 2015 April 2017 CONTENTS Part Description Page Foreword 1 1 Introduction and Commencement
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Appendix 1: Croydon Clinical Commissioning Group Risk Register and Board Assurance Framework - 9th April 2013
 Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
A new mindset: the Five Year Forward View for mental health
 A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Strategy for Delivery of Clinical Quality and Patient Safety. North Norfolk Clinical Commissioning Group
 Strategy for Delivery of Clinical Quality and Patient Safety North Norfolk Clinical Commissioning Group V5 Document Control Sheet Name of document: Quality Strategy 2016-18 Version: 5 Owner: Head of Clinical
Strategy for Delivery of Clinical Quality and Patient Safety North Norfolk Clinical Commissioning Group V5 Document Control Sheet Name of document: Quality Strategy 2016-18 Version: 5 Owner: Head of Clinical
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session. Date of Meeting: 24 March 2015
 Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session Date of Meeting: 24 March 205 For: Decision Discussion Noting Agenda Item and title: Author: GOV/5/03/20
Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session Date of Meeting: 24 March 205 For: Decision Discussion Noting Agenda Item and title: Author: GOV/5/03/20
NHS East and North Hertfordshire Clinical Commissioning Group. Quality Committee. Terms of Reference Version 4.0
 NHS East and North Hertfordshire Clinical Commissioning Group Quality Committee Terms of Reference Version 4.0 1. Introduction 1.1 The Quality Committee (the committee) is established in accordance with
NHS East and North Hertfordshire Clinical Commissioning Group Quality Committee Terms of Reference Version 4.0 1. Introduction 1.1 The Quality Committee (the committee) is established in accordance with
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Wolverhampton CCG Commissioning Intentions
 Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Marginal Rate Emergency Threshold. Executive Summary
 Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR:
 MINDING THE GAP COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR: GOVERNANCE ASSURANCE AND PERFORMANCE. 1. INTRODUCTION AND CONTEXT Providing, delivering and developing the highest standards
MINDING THE GAP COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR: GOVERNANCE ASSURANCE AND PERFORMANCE. 1. INTRODUCTION AND CONTEXT Providing, delivering and developing the highest standards
WOLVERHAMPTON CCG. Governing Body Meeting 9 th September 2014
 WOLVERHAMPTON CCG Governing Body Meeting 9 th September 2014 ` Agenda item:12 TITLE OF REPORT: REPORT PRESENTED BY: Title of Report: Purpose of Report: Commissioning Committee Summary Kamran Ahmed Update
WOLVERHAMPTON CCG Governing Body Meeting 9 th September 2014 ` Agenda item:12 TITLE OF REPORT: REPORT PRESENTED BY: Title of Report: Purpose of Report: Commissioning Committee Summary Kamran Ahmed Update
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan
 Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health and Social Care Directorate Quality standards Process guide
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health and Social Care Directorate Quality standards Process guide December 2014 Quality standards process guide Page 1 of 44 About this guide This guide
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health and Social Care Directorate Quality standards Process guide December 2014 Quality standards process guide Page 1 of 44 About this guide This guide
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014
 Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
MEMORANDUM OF UNDERSTANDING
 MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
Review of Terms of Reference of Quality Assurance Committee
 Review of Terms of Reference of Quality Assurance Committee Governing Body meeting 3 May 2018 H Author(s) Sponsor Director Purpose of Paper Sue Laing, Corporate Services Risk and Governance Manager Mandy
Review of Terms of Reference of Quality Assurance Committee Governing Body meeting 3 May 2018 H Author(s) Sponsor Director Purpose of Paper Sue Laing, Corporate Services Risk and Governance Manager Mandy
ENCLOSURE: J. Date of Trust Board 29 February Pressure Ulcer Clinical Improvement Programme. Purpose of Report
 ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
CODE OF CONDUCT WHERE GP PRACTICES OR CONSORTIA ARE POTENTIAL PROVIDERS OF CCG COMMISISONED SERVICES
 CODE OF CONDUCT WHERE GP PRACTICES OR CONSORTIA ARE POTENTIAL 1. Introduction PROVIDERS OF CCG COMMISISONED SERVICES 1.1. Managing potential conflicts of interest appropriately is needed to protect the
CODE OF CONDUCT WHERE GP PRACTICES OR CONSORTIA ARE POTENTIAL 1. Introduction PROVIDERS OF CCG COMMISISONED SERVICES 1.1. Managing potential conflicts of interest appropriately is needed to protect the
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 23 rd March 2017 Agenda No: 9.3 Attachment: 15 Title of Document: CCG Governing Body Assurance Report & Scorecards: Month 9 Quality &
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 23 rd March 2017 Agenda No: 9.3 Attachment: 15 Title of Document: CCG Governing Body Assurance Report & Scorecards: Month 9 Quality &
Healthwatch Kent - September 2017 Discharge from Hospital in West Kent
 Healthwatch Kent - September 2017 Discharge from Hospital in West Kent Foreword We hear from people about their experience of being discharged from hospital all over Kent. We ve recently done a large project
Healthwatch Kent - September 2017 Discharge from Hospital in West Kent Foreword We hear from people about their experience of being discharged from hospital all over Kent. We ve recently done a large project
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Review of Local Enhanced Services
 Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
Telford and Wrekin Clinical Commissioning Group. Prospectus 2013/2014
 Telford and Wrekin Clinical Commissioning Group Prospectus 2013/2014 Who we are Telford and Wrekin Clinical Commissioning Group (CCG) is responsible for healthcare in the Telford and Wrekin area. We Plan
Telford and Wrekin Clinical Commissioning Group Prospectus 2013/2014 Who we are Telford and Wrekin Clinical Commissioning Group (CCG) is responsible for healthcare in the Telford and Wrekin area. We Plan
INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS
 MAY 2007 INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS Practice Based Commissioning North and South Essex Local Medical Committees CLARIFYING THE RELATIONSHIP BETWEEN PBC GROUPS AND PCTS AIMS The aim of
MAY 2007 INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS Practice Based Commissioning North and South Essex Local Medical Committees CLARIFYING THE RELATIONSHIP BETWEEN PBC GROUPS AND PCTS AIMS The aim of
Title of meeting: Primary Care Joint Commissioning Committee (JCC) Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7
 Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7") Title of meeting: Primary Care Joint Commissioning Committee (JCC) Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7 Title Sponsoring Director (name and job title) Sponsoring
Title of meeting: Primary Care Joint Commissioning Committee (JCC) Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7 Title Sponsoring Director (name and job title) Sponsoring
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 15 December 2016 Agenda No: 3.3 Attachment: 04 Title of Document: Surgery Readiness Option Report Author: Andrew Moore (Programme Director
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 15 December 2016 Agenda No: 3.3 Attachment: 04 Title of Document: Surgery Readiness Option Report Author: Andrew Moore (Programme Director
JOB DESCRIPTION. Joint Commissioning Manager for Older People s Residential Care and Nursing Homes
 JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
Hospital Discharge and Transfer Guidance. Choice, Responsiveness, Integration & Shared Care
 Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
Hospital Discharge and Transfer Guidance Choice, Responsiveness, Integration & Shared Care Worcestershire Mental Health Partnership NHS Trust Information Reader Box Document Type: Document Purpose: Unique
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service
 Service") DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service Executive summary: The Cornwall Sustainability and Transformation Plan known as Shaping our Future will describe a new model of
DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service Executive summary: The Cornwall Sustainability and Transformation Plan known as Shaping our Future will describe a new model of
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean