Getting Started with Medication Reconciliation in Long Term Care. SHN! MedRec Teleconference September 14, EST
|
|
|
- Dustin Newton
- 5 years ago
- Views:
Transcription

1 Getting Started with Medication Reconciliation in Long Term Care SHN! MedRec Teleconference September 14, EST 1
2 Welcome! By the end of this teleconference, participants will: Understand the key concepts in medication reconciliation in long-term care. Learn how to access the available resources and supports to get started with implementation. Gain insight from long-term care teams who have started medication reconciliation and learn how they are doing it. Have fun! 2
3 Our Guest Speakers Jeanette Cameron R.N Inverary Manor - Director of Resident Care Jo-Anne Thompson R.N - South Eastman region Patient Safety Officer Renee Claire Fox R.N - Quality and Risk Management at the Health and Social Services Centre Jeanne-Mance 3
4 Getting Started with Medication Reconciliation in Long Term Care Margaret Colquhoun, R.Ph., B.Sc.Phm., FCSHP SHN Intervention Lead Medication Reconciliation Project Leader ISMP Canada 4
5 SHN Medication Reconciliation Teams Currently: Acute Care: 340 Long Term Care: 106 Home Care: 30 Total = 476 SHN! Canadian Teams 5
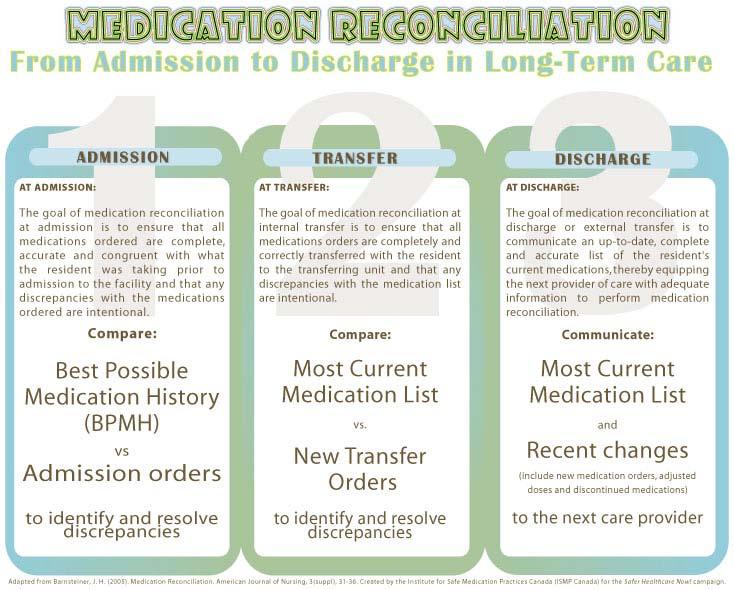
6 Medication Reconciliation in LTC Medication Reconciliation in long-term care is a formal process of: At admission, obtaining a complete list of each resident s current (and pre-admission medications if coming from acute care) including name, dosage, frequency and route (BPMH). Using the BPMH to create admission orders or comparing the list against the resident s admission orders, identifying and bringing any discrepancies to the attention of the prescriber for resolution. Any resulting changes in orders are documented and communicated to the relevant providers of care and resident or family member wherever possible. 6
7 Case for Med Rec in LTC In a 2004 study by Boockvar the incidence of ADEs caused by medication changes at transfer between facilities was 20%. ADEs due to medication changes occurred most often upon transfer from the hospital back to the LTC facility. Incomplete or inaccurate communication between facilities was identified as a potential factor in these occurrences. Boockvar K, Fishman E, Kyriacou CK, et al. Adverse events due to discontinuations in drug use and dose changes in patients transferred between acute and Long-term care facilities. Arch Intern Med. 2004;164:
8 Case for Med Rec in LTC Incomplete or inaccurate medication information is a critical issue reflected in a growing number of LTC studies. A 2007 survey of continuing care nurses and pharmacists in Alberta found: 75% of the time medication information was NOT legible and complete 90% of the time information was NOT available to tell if the prescribed medications were appropriate for the resident s diagnoses. 40% of the time medication information DID NOT arrive the same day as the resident s admission. Earnshaw, K et. al. Perspectives of Alberta Nurses and Pharmacists on Medication Information Received. July 29,
9
 are written by the prescriber 3.")
10 Proactive MedRec Model Occurs when the BPMH is conducted before writing admission medication orders 1. Create the BPMH 2. Using the BPMH, admission medication orders (AMOs) are written by the prescriber 3. Verify that the prescriber has assessed every medication on the BPMH, identifying and resolving any outstanding discrepancies with the prescriber Used with permission from High 5s: Action on Patient Safety Medication Reconciliation Getting Started Kit. 10

11 Getting Started Kit Medication Reconciliation in Long-Term Care Step-by-step guide to the process Model for Improvement Tools and Tips Samples from Canadian teams Website: 11
12

13 13

14 14

15 Enroll Today 15

16 Join SHN Communities of Practice 16

17 Critical Success Factors Get Baseline data Share the data Use teaching moments Create your own stories Requires resident/family participation Use different health disciplines appropriately 17


18 Most Current Medication List and Transfer/Discharge Orders Jeanette Cameron RN, BScN ( Director Resident Care)) Debbie Le Lievre RN, BScN (Unit Manager, 18 ER/OR/DEC/SPD/Oncology)
19 Who We Are Inverary Manor is a 60 bed Long Term Care facility. We are located in a rural area of Cape Breton, N.S., directly behind the hospital. Inverness Consolidated Memorial Hospital is a 39 bed hospital and a busy Emergency/Ambulatory Care Department, with 16,236 (10,052 ER & 6184 Amb Care) visits per year. ( Stats) 19
20 Who we are The two facilities will soon be connected by a link which will include a new 71 bed LTC facility and renovations to the hospital so this is very exciting for everyone. 20
21 Purpose To develop a tool to facilitate more efficient and safer transfer of residents from one facility to another. More specifically, transfers from Inverary Manor to Inverness Consolidated Memorial Hospital. 21
22 Brief History Inverary Manor was introduced to medication reconciliation for admissions in May, This has extremely successful and we now needed help with transfers. ICMH initiated Medication Reconciliation for Admissions, Transfers and Discharge in February of 2008 as a Required Organizational Practice (ROP) for patient safety, but we needed to expand with LTC. 22
23 Brief History Inverary Manor was introduced to medication reconciliation for admissions in May, This has extremely successful and we now needed help with transfers. ICMH initiated Medication Reconciliation for Admissions, Transfers and Discharge in February of 2008 as a Required Organizational Practice (ROP) for patient safety, but we needed to expand with LTC. 23
24 Goals To improve communication and documentation between facilities To decrease the potential for medication misinterpretation and errors To provide the safest delivery of care to residents 24
25 How we got Started A workshop was held in May, 2009, facilitated by Safer Healthcare Now Advisor, Dannie Currie. This was a collaboration between staff from both facilities which included RN s, LPN s, nurse managers and the hospital pharmacist. 25
26 Needs Identified Needs Identified Hospital staff expressed the need for a clear and concise medication list upon receiving resident. Up to this time, Inverary Manor would photocopy MAR sheets to send with resident. Although these were clear to Manor staff, they were confusing to ICMH. 26
27 Needs Identified Inverary Manor staff expressed the need for clear discharge medication orders. Up to this time, there would be discrepancies from the original med list and it wasn t always clear if changes were intended or not intended. For emergencies, no time to write out a med list, so MARS sent. 27
28 There was wonderful discussion, sharing of ideas and understanding of each others point of view which lead to the development of this new tool. Little did we know it was so new and innovative!! 28
29 Out with the old, In with the new The following two slides will show the old format that Manor would photocopy the MAR sheets and send with resident. Some residents would have 5-6 sheets which would be very confusing. The third slide is the form the hospital would send back to Manor with resident. Very difficult to read the orders! 29

30 Old Format 30

31 Medical Conditions H -HOLD cerebrovaswlar R -REFUSED Accident; D - Chronic Allergies Comments Obstructive No P DISPENSEOlU D -DAY Q-HOSPITAL Known L R. -LEAVE A. Allergies PROGRAM Freeman NSUPERVISED LTD. 31

32 32

33 What nurses looked like before! 33
34 Implementing Form Once form was printed, it was circulated to all managers, nursing staff, physicians and pharmacists along with a cover letter on how it came about and how to use it properly. 34
35 How list is compiled List of medications is taken from the medication sheets and include time of last dose. These are the medications that resident takes daily. We are confident this list is current as they are checked monthly when they arrive from pharmacy and any new orders or changes are double checked nightly 35

36 How it Works Completed by Sending Facility Completed by Receiving Facility 36
37 How it Works 37
38 38
39 Challenges What were some barriers? There were no real barriers, everyone worked in collaboration and education was provided. The form was well received and all comments have been positive, from all Health Care providers. 39

40 After the form, a happy nurse! 40
41 Things we learned One oversight was the prescription of narcotics cannot be filled without duplicate copy so still need seperate Rx for those. (Doesn t occur often) This tool has simplified transfers for nurses and physicians but the greatest feeling is working together to provide the best, safest care possible for our residents. 41

42 We leave you with a photo of Inverness Beach. 42
43 Contact Information Names :Jeanette Cameron RN, BScN Director Resident Care, Inverary Manor Debbie LeLievre RN,BScN Unit Manager, ER/OR/DEC/SPD/Oncology- ICMH (902) ext 1133 or (902) (cell) 43

44 MEDICATION RECONCILIATION Jo-Anne Thompson RN Patient Safety Officer South Eastman Health

45 WHO ARE WE? There are 11 regional health authorities in Manitoba. Churchill Burntwood Nor-Man North Eastman Parkland Interlake Brandon Assiniboine Central South Eastman Winnipeg
46 SOUTH EASTMAN RHA population 66,984 (6% of MB) Source: Manitoba Health (June 2009)
47 PERSONAL CARE HOME BEDS N = 334 St. Adolphe 42 Ste. Anne 66 Steinbach 60 St. Pierre-Jolys 22 Steinbach 60 Grunthal 40 Vita 44 47
48 SOUTH EASTMAN S MED. REC. STEERING COMMITTEE Jo-Anne Thompson (Chair) - Patient Safety Officer Jan Gunness (Executive Sponsor) - Manager of Quality & Corporate Planning Cecile Dumesnil- Regional Director of Pharmacy Lothar Dueck Pharmacist Dr. S. Migally Physician Brenda Barkman Clinical Resource Nurse (CRN) Rehab Unit Donna Bella Home Care Case Coordinator Charleen Barkman Staff Development Coordinator-LTC Shirley Bezditny Staff Development Coordinator- Acute Care Tannis Nickel-Director of Nursing (DON) Rest Haven Nursing Home Public Health, Mental Health (Reps needed)
49 WHAT ARE WE TRYING TO ACCOMPLISH? Develop and implement a regional Medication Reconciliation process throughout the continuum of care, which will help prevent medication errors from occurring and reduce the potential for harm to patients. It has started in Acute Care (Phase I) and will continue to spread to all other areas of service i.e.) Long Term Care, Home Care, Community etc Phase II commenced Spring Pilot site: Rest Haven Nursing Home.
50 HOW WILL WE DO THIS? PDSA ( Plan-Do-Study-Act) Improvement Model PLAN: DO: STUDY: ACT: Creating forms that work within South Eastman Health Testing the forms on the pilot sites - Rest Haven Nursing Home (LTC) Evaluating and modifying the forms. Implementing changes on the forms and planning for the next cycle.
51 HOW WILL WE KNOW WE ARE MAKING A DIFFERENCE? The team is currently performing baseline chart audits in order to measure our successes. Discrepancies between the home medications and the admission orders are measured. The goal of the Med.Rec. project is to reduce these discrepancies over time. Ongoing testing will occur at various points of the project to assess the impact of the Med.Rec. process.
52 WHAT ARE WE MEASURING? No discrepancies Intentional discrepancies Physician has made an intentional choice to add, change or discontinue a medication and is clearly documented. Undocumented Intentional Discrepancy Physician has made an intentional choice to add, change or discontinue a medication but this choice is not clearly documented. i.e) Nitro-patch put on hold or discontinued but no reason given. * This captures the accuracy in documentation* Unintentional Discrepancy Physician unintentionally changed, added or omitted a medication the patient was taking prior to admission. * This reflects the errors that inadvertently occur when writing orders. The primary goal is to eliminate the undocumented intentional and unintentional discrepancies through the medication reconciliation process.
53 GOAL The area of focus will be to decrease the mean # of undocumented intentional discrepancies on patients admitted to the hospital & LTC facilities by 75%, as well as the unintentional discrepancies by 75%.
54 SO HOW DO WE KNOW THAT WE ARE SUCCEEDING? To know that we are succeeding in LTC the undocumented & unintentional discrepancies will need to meet the set goal line over 6 consecutive months to master this process. LTC is tracking the percentage of residents reconciled at admission which coincides with Accreditation Canada standards which is 100%.
55 MedRec LTC 1 Mean Number of Undocumented Intentional Discrepancies in LTC Rest Haven Mean Nov 2007 Feb 2008 May 2008 Aug 2008 Nov 2008 Feb 2009 May 2009 Aug 2009 Nov 2009 Feb 2010 May 2010 Aug 2010 Nov 2010 Feb 2011 May 2011 Aug 2011 Nov 2011 Month Actual Goal
56 MedR ec LTC 2 Mean Number of Unintentional Discrepancies in LTC Rest Haven Mean Nov 2007 Feb 2008 May 2008 Aug 2008 Nov 2008 Feb 2009 May 2009 Aug 2009 Nov 2009 Feb 2010 May 2010 Aug 2010 Nov 2010 Feb 2011 May 2011 Aug 2011 Nov 2011 Month Actual Goal
57 MedRec LTC 3 Percentage of Long Term Care Residents Rec onc iled at Admission 100.0% 90.0% 80.0% 70.0% 60.0% Mean 50.0% 40.0% 30.0% 20.0% 10.0% 0.0% Nov 2007 Feb 2008 May 2008 Aug 2008 Nov 2008 Feb 2009 May 2009 Aug 2009 Nov 2009 Feb 2010 May 2010 Aug 2010 Nov 2010 Feb 2011 May 2011 Aug 2011 Nov 2011 Month Actual Goal
58 Medication Reconciliation Baseline Audit February 2008 Vita & St.Pierre Bethesda & Ste.Annes MedRec Process Implemented MedRec Process NOT Implemented Chart # No Discrepancy Intentional Discrepancy Undocumented Intentional What Does the Audit results reveal for our 4 sites. Discrepancy Unintentional discrepancy No Discrepancy Intentional Discrepancy Undocumented Intentional Discrepancy Unintentional discrepancy Med process not used, no nursing Hx and M.D. orders? Med process used but no reconciliation done. No discharge process completed. Med Hx not properly completed Med Rec not completed, patient transferred out. 7 1 Patient not on meds No admission Hx (ER triage list) M.D. orders done on ward, missing 5/14 meds Patient not on meds. No meds documented at all Reported on Hx, no meds. 20 Med Rec not done. 5
59 POSITIVE GAINS WITH THE PROCESS Earlier identification of issues with patient home medications Developed a Medication Risk Assessment Tool used on admission that engages Pharmacists by referral Increased documentation of allergies Decreased duplication in recording medication histories (Both for Physician & Nurse) Improved communication of medication histories to all disciplines Improved communication to next healthcare provider for changing or not ordering home medications
60 CHALLENGES As we progress in spread challenges may present it self. The steering committee team will work on resolving issues on a ongoing basis. Continuous Education for all new employee s hired
61 SOUTH EASTMAN HEALTH Team work involves the Patient/Client/Families, Nurses, Physicians and Pharmacists Working as a team in South Eastman Health we can make a difference by improving patient safety and reducing potential adverse outcomes of care related to medications
62 REFERENCES Canadian Patient Safety Institute Manitoba Institute for Patient Safety Safer Healthcare NOW!


63

64 Health and Social Services Centre Jeanne-Mance MEDICATION RECONCILIATION LONG-TERM CARE Renée Claire Fox, B.A., M.Sc. Inf. 64 Sept













65 Health and Social Services Centre Jeanne-Mance 7 LONG-TERM CARE FACILITIES 1200 beds 3 CLSC population Affiliated with the U of Mtl teaching and research 65
66 Objective Sharing our journey of medication reconciliation implementation in long-term care 66
67 Leadership commitment Central clinical planning committee: Associate Director General long-term care Associate Director General community services, public health, teaching and research Director of Nursing Director Professional services, Quality and Risk Management Medical Director 67

68 Fundamental question Planning and implementation in more than 1 sector Planning and implementation in 1 sector only 68
69 Med Rec Steering Committee Nurse clinician Representatives long-term care: Nurse Manager Physician Pharmacist Representatives home care services: Nurse Manager Physician Pharmacist from community Quality and risk management coordinator Representatives of specialty areas link with partners, communication, archives, IT 69
70 management multiple contexts Medication Reconciliation client/family processes medication confidentiality Systemic Approach Communication Infrastructure Transversal Approach information technology interdisciplinary team different cultures Intra / inter site Partners and community outcomes measure & evaluation transition points 70
71 Challenges It s not just about a new form, it s about changing the way we do things around here. Engagement of an Interdisciplinary team Participation of community pharmacists Information Transfers from acute care Information technology Organisational context 71
72 Considerations for Planning Volume of admissions/ transfers Nurse/resident ratio Time needed to complete BPMH Roles : nurse, physician and pharmacist Admission /transfer processes in use before Med Rec Present functioning of pharmacies (3) Getting doctors on board Tools : no duplication, less transcribing Types of discrepancies Medication profiles from private pharmacies in community and from acute care facilities Communication plan Link to risk management 72
73 Team members?????? Pharm. technician nurse pharmacist client physician 73
74 Med Rec Model All admissions Proactive process Long-term care Transfers/discharge to home care to other long-term care facility 74
75 Med Rec Processes Long-term care Role: nurse Role: phys Role: pharm Long-term care admission transfers Data collection 75


76 Indicators CLINIBASE % Med Rec long-term care at admission and transfer/discharge Data for Board members and management 76
77 And the discrepancies? ACCESS Analyse data Make recommendations 77
78 Measure and evaluation Audit tools for : BPMH Reconciliation 78
79 Management and spread Plan for management to oversee/support Med Rec in each long-term care facility Global management plan to spread Med Rec to all long-term cares facilities within Centre Jeanne-Mance 79
80 Tools Tool for Admission Med Rec Tool for clinical information 80
81 81
82 82
83 Questions? 83
Who s s on What? Latest Experience with the Framework Challenges and Successes. November 29, Margaret Colquhoun Project Leader ISMP Canada
 Who s s on What? Latest Experience with the Framework Challenges and Successes November 29, 2005 Margaret Colquhoun Project Leader ISMP Canada 1 Outline ISMP Canada Partnership with SHN The Canadian Getting
Who s s on What? Latest Experience with the Framework Challenges and Successes November 29, 2005 Margaret Colquhoun Project Leader ISMP Canada 1 Outline ISMP Canada Partnership with SHN The Canadian Getting
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU. Change Package.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
St. Michael s Hospital Medication Reconciliation Learning Package
 St. Michael s Hospital Medication Reconciliation Learning Package What is Medication Reconciliation? A formal process which begins with obtaining a complete and accurate list of each patient s home medications
St. Michael s Hospital Medication Reconciliation Learning Package What is Medication Reconciliation? A formal process which begins with obtaining a complete and accurate list of each patient s home medications
Getting Started Kit MEDICATION RECONCILIATION IN LONG-TERM CARE. Reducing Harm Improving Healthcare Protecting Canadians
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN LONG-TERM CARE Getting Started Kit March 2012 www.saferhealthcarenow.ca Safer Healthcare Now! We invite you to join
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN LONG-TERM CARE Getting Started Kit March 2012 www.saferhealthcarenow.ca Safer Healthcare Now! We invite you to join
Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting
 Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting Natalie McMurtry, BSc Pharm, Sr. Medication Consultant; Vanessa Moorgen,
Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting Natalie McMurtry, BSc Pharm, Sr. Medication Consultant; Vanessa Moorgen,
Mental Health Pharmacist Education. Medication Reconciliation Patient Safety Initiative
 Mental Health Pharmacist Education Medication Reconciliation Patient Safety Initiative August 2015 Introductions Agenda MedRec Project Overview Project Structure Implementation/Dates MedRec Basics What
Mental Health Pharmacist Education Medication Reconciliation Patient Safety Initiative August 2015 Introductions Agenda MedRec Project Overview Project Structure Implementation/Dates MedRec Basics What
Making a case for medication reconciliation in primary care
 Safer Healthcare Now! MedRec National Teleconference Making a case for medication reconciliation in primary care Speakers: Karen Hall Barber, BSc (Hons), MD, CCFP Sherri Elms, BSc (Pharm), RPh ACPR Danyal
Safer Healthcare Now! MedRec National Teleconference Making a case for medication reconciliation in primary care Speakers: Karen Hall Barber, BSc (Hons), MD, CCFP Sherri Elms, BSc (Pharm), RPh ACPR Danyal
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
Medication Reconciliation Review
 The Medication Reconciliation Review tool provides step-by-step instructions for conducting a review of closed patient records to identify errors related to unreconciled medications. Organizations that
The Medication Reconciliation Review tool provides step-by-step instructions for conducting a review of closed patient records to identify errors related to unreconciled medications. Organizations that
Medication Reconciliation
 Medication Reconciliation ISMP Canada Annual Report to CPSI Safer Healthcare Now! Medication Reconciliation Intervention April 2010 to March 2011 Safer Healthcare Now! Medication Reconciliation Intervention
Medication Reconciliation ISMP Canada Annual Report to CPSI Safer Healthcare Now! Medication Reconciliation Intervention April 2010 to March 2011 Safer Healthcare Now! Medication Reconciliation Intervention
How to Fill Out the Admission Best Possible Medication History (BPMH) Tool
 Tool") How to Fill Out the Admission Best Possible Medication History (BPMH) Tool Medication Reconciliation On Admission Updated: August 21, 2014 Medication Reconciliation on Admission How to Fill Out an admission
How to Fill Out the Admission Best Possible Medication History (BPMH) Tool Medication Reconciliation On Admission Updated: August 21, 2014 Medication Reconciliation on Admission How to Fill Out an admission
Quality Improvement Medication Reconciliation Tools, Techniques and Tales
 Quality Improvement Medication Reconciliation Tools, Techniques and Tales Presented by: Marsha Nicholson, Steve Scott, City of Toronto Long-Term Care Homes and Services Division January 10, 2012 Outline
Quality Improvement Medication Reconciliation Tools, Techniques and Tales Presented by: Marsha Nicholson, Steve Scott, City of Toronto Long-Term Care Homes and Services Division January 10, 2012 Outline
Getting Started Kit MEDICATION RECONCILIATION IN LONG-TERM CARE. Version 3. Reducing Harm Improving Healthcare Protecting Canadians.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN LONG-TERM CARE Getting Started Kit Version 3 Marc h 2017 w w w.patientsafetyinstitute.c a This Getting Started Kit has
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN LONG-TERM CARE Getting Started Kit Version 3 Marc h 2017 w w w.patientsafetyinstitute.c a This Getting Started Kit has
Medication Reconciliation in Transitions of Care
 Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Safer Healthcare Now! Medication Reconciliation in Homecare Pilot Project
 1 Safer Healthcare Now! Medication Reconciliation in Homecare Pilot Project FINAL REPORT Prepared by: Deborah Conrad R.N. - Pilot Project Coordinator Catherine Butler, RN, BA, BScN, MHA VON Project Lead
1 Safer Healthcare Now! Medication Reconciliation in Homecare Pilot Project FINAL REPORT Prepared by: Deborah Conrad R.N. - Pilot Project Coordinator Catherine Butler, RN, BA, BScN, MHA VON Project Lead
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02
 Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Medicines Reconciliation Policy
 Medicines Reconciliation Policy Lead executive Medical Director Authors details Senior Clinical Pharmacy Technician - 01244 39 7494 Document level: Trustwide (TW) Code: MP19 Issue number: 3 Type of document
Medicines Reconciliation Policy Lead executive Medical Director Authors details Senior Clinical Pharmacy Technician - 01244 39 7494 Document level: Trustwide (TW) Code: MP19 Issue number: 3 Type of document
Medication Reconciliation
 Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Learner Manual. Document Best Possible Medication History (BPMH)
") Learner Manual Document Best Possible Medication History (BPMH) Table of Contents Medication safety... 1 Medication errors impact everyone... 1 Who should obtain the BPMH?... 1 When is the BPMH obtained?...
Learner Manual Document Best Possible Medication History (BPMH) Table of Contents Medication safety... 1 Medication errors impact everyone... 1 Who should obtain the BPMH?... 1 When is the BPMH obtained?...
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME
 Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Medication Reconciliation - Inpatient
 Page 1 of 8 Home Previous Page Print Medication Reconciliation - Inpatient Administrative Policies & Procedures Document Number: MHC-ADMIN-02-1280 v6 Document Owner: Donna Ciufo, DNP, RN Date Last Updated:
Page 1 of 8 Home Previous Page Print Medication Reconciliation - Inpatient Administrative Policies & Procedures Document Number: MHC-ADMIN-02-1280 v6 Document Owner: Donna Ciufo, DNP, RN Date Last Updated:
YOUR DISCHARGE IS SOMEONE S ADMISSION
 YOUR DISCHARGE IS SOMEONE S ADMISSION Today s Facilitator Kim Streitenberger Project Lead, ISMP Canada 2 Welcome Mike Cass Patient Safety Improvement Lead, CPSI 3 Welcome to our francophone attendees Bienvenue
YOUR DISCHARGE IS SOMEONE S ADMISSION Today s Facilitator Kim Streitenberger Project Lead, ISMP Canada 2 Welcome Mike Cass Patient Safety Improvement Lead, CPSI 3 Welcome to our francophone attendees Bienvenue
MedRec in the Home Care Setting: Sharing Ontario s Central Community Care and Access Centre s Success Story
 SHN MedRec National Teleconference MedRec in the Home Care Setting: Sharing Ontario s Central Community Care and Access Centre s Success Story Medication Management Support Services (MMSS) Speakers: Mary
SHN MedRec National Teleconference MedRec in the Home Care Setting: Sharing Ontario s Central Community Care and Access Centre s Success Story Medication Management Support Services (MMSS) Speakers: Mary
Pharmaceutical Services Report to Joint Conference Committee September 2010
 Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Medication Reconciliation Bundle of Care. Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013
 Medication Reconciliation Bundle of Care Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013 Overview Problem of medication errors at transitions of care Who is at risk Recognition as a patient
Medication Reconciliation Bundle of Care Margaret Duguid, Pharmaceutical Advisor Singapore, 21 August 2013 Overview Problem of medication errors at transitions of care Who is at risk Recognition as a patient
Getting Started Kit MEDICATION RECONCILIATION IN ACUTE CARE. Version 4. Reducing Harm Improving Healthcare Protecting Canadians.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN ACUTE CARE Getting Started Kit Version 4 Marc h 2017 w w w.patientsafetyinstitute.c a This Getting Started Kit has been
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN ACUTE CARE Getting Started Kit Version 4 Marc h 2017 w w w.patientsafetyinstitute.c a This Getting Started Kit has been
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016
 UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
Required Organizational Practices. September 2011
 s September 2011 CONTENTS OVERVIEW...1 ABOUT THE ROP HANDBOOK...2 SAFETY CULTURE Adverse events disclosure...3 Adverse events reporting...4 Client safety as a strategic priority...5 Client safety quarterly
s September 2011 CONTENTS OVERVIEW...1 ABOUT THE ROP HANDBOOK...2 SAFETY CULTURE Adverse events disclosure...3 Adverse events reporting...4 Client safety as a strategic priority...5 Client safety quarterly
Medication Reconciliation: Preventing Errors and Improving Patient Outcomes
 Murray State's Digital Commons Scholars Week 2016 - Spring Scholars Week Apr 18th, 12:00 PM - 2:00 PM Medication Reconciliation: Preventing Errors and Improving Patient Outcomes Amanda S. Boren Murray
Murray State's Digital Commons Scholars Week 2016 - Spring Scholars Week Apr 18th, 12:00 PM - 2:00 PM Medication Reconciliation: Preventing Errors and Improving Patient Outcomes Amanda S. Boren Murray
VNAA Blueprint for Excellence PATHWAY TO BEST PRACTICES
 VNAA Blueprint for Excellence PATHWAY TO BEST PRACTICES Patient Safety: Medication Reconciliation and Management VNAA Best Practice for Hospice and Palliative Care Medication Reconciliation and Adherence
VNAA Blueprint for Excellence PATHWAY TO BEST PRACTICES Patient Safety: Medication Reconciliation and Management VNAA Best Practice for Hospice and Palliative Care Medication Reconciliation and Adherence
Making a PDiF-ference Results of the PDiF Quality Improvement Initiative
 Making a PDiF-ference Results of the PDiF Quality Improvement Initiative March 2014 www.saferhealthcarenow.ca Bienvenue! Welcome also to our francophone attendees Bienvenue à nos participants francophones
Making a PDiF-ference Results of the PDiF Quality Improvement Initiative March 2014 www.saferhealthcarenow.ca Bienvenue! Welcome also to our francophone attendees Bienvenue à nos participants francophones
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
University of Mississippi Medical Center University of Mississippi Health Care. Pharmacy and Therapeutics Committee Medication Use Evaluation
 University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
Fundamentals of Self-Limiting Conditions Prescribing for Manitoba Pharmacists. Ronald F. Guse Registrar College of Pharmacists of Manitoba (CPhM)
") Fundamentals of Self-Limiting Conditions Prescribing for Manitoba Pharmacists Ronald F. Guse Registrar College of Pharmacists of Manitoba (CPhM) 1 Learning Objectives Upon successful completion of this
Fundamentals of Self-Limiting Conditions Prescribing for Manitoba Pharmacists Ronald F. Guse Registrar College of Pharmacists of Manitoba (CPhM) 1 Learning Objectives Upon successful completion of this
Medication Error Reporting Program (MERP) Update. April 2010 *********************************************
 Update. April 2010 *********************************************") Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
Medication Error Reporting Program (MERP) Update April 2010 ********************************************* Overview and presentation of our readiness Opening PowerPoint completed and under review by Quality
MEDICINES RECONCILIATION GUIDELINE Document Reference
 MEDICINES RECONCILIATION GUIDELINE Document Reference G358 Version Number 1.01 Author/Lead Job Title Jackie Stark Principle Pharmacist Clinical Services Date last reviewed, (this version) 29 November 2012
MEDICINES RECONCILIATION GUIDELINE Document Reference G358 Version Number 1.01 Author/Lead Job Title Jackie Stark Principle Pharmacist Clinical Services Date last reviewed, (this version) 29 November 2012
Licensed Pharmacy Technicians Scope of Practice
 Licensed s Scope of Practice Adapted from: Request for Regulation of s Approved by Council April 24, 2015 DEFINITIONS In this policy: Act means The Pharmacy and Pharmacy Disciplines Act means an unregulated
Licensed s Scope of Practice Adapted from: Request for Regulation of s Approved by Council April 24, 2015 DEFINITIONS In this policy: Act means The Pharmacy and Pharmacy Disciplines Act means an unregulated
Avoiding Errors During Transitions of Care: Medication Reconciliation
 in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Objectives THE BASICS AND USING TECHNICIANS 3/22/2017
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Pharmacy Technicians and Interns: Charting New Territory
 Pharmacy Technicians and Interns: Charting New Territory Peter Dippel Pharm.D, BCPS Clinical Pharmacist II Baptist Health Medical Center NLR Objectives Understand what Pharmacist Extenders are and why
Pharmacy Technicians and Interns: Charting New Territory Peter Dippel Pharm.D, BCPS Clinical Pharmacist II Baptist Health Medical Center NLR Objectives Understand what Pharmacist Extenders are and why
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1)
 Medication Chart implementation and training guide (version 1.1)") Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Improving the Pre-Empted Medication Error Reporting System at St. Charles Hospital, Port Jefferson, NY
 Improving the Pre-Empted Medication Error Reporting System at St. Charles Hospital, Port Jefferson, NY Contributed by Kathleen LeDoux, MS, RN, BC, CPHQ Performance Improvement Nurse, St. Charles Hospital,
Improving the Pre-Empted Medication Error Reporting System at St. Charles Hospital, Port Jefferson, NY Contributed by Kathleen LeDoux, MS, RN, BC, CPHQ Performance Improvement Nurse, St. Charles Hospital,
NHS Grampian Medicines Reconciliation Protocol. Organisational: Area:
 Title: Unique Identifier: NHS Grampian Medicines Reconciliation Protocol NHSG/Guid/Med_RecMGPG711 Replaces: N/A New document Across NHS Boards Organisation Wide Yes Directorate Clinical Service Sub Department
Title: Unique Identifier: NHS Grampian Medicines Reconciliation Protocol NHSG/Guid/Med_RecMGPG711 Replaces: N/A New document Across NHS Boards Organisation Wide Yes Directorate Clinical Service Sub Department
Patient Safety Initiatives
 Patient Safety Initiatives Nursing Responsibilities Policies and Procedures Objectives To provide overview of Safer Healthcare Now! Ensure staff have an understanding of new policies Provide an opportunity
Patient Safety Initiatives Nursing Responsibilities Policies and Procedures Objectives To provide overview of Safer Healthcare Now! Ensure staff have an understanding of new policies Provide an opportunity
JHQ 177 Medication Reconciliation: A Necessity in Promoting a Safe Hospital Discharge
 JHQ 177 Medication Reconciliation: A Necessity in Promoting a Safe Hospital Discharge Donna L. Poole, Juliane N. Chainakul, Mary Pearson, LeAnn Graham Keywords: Discharge, Information technology, Medication
JHQ 177 Medication Reconciliation: A Necessity in Promoting a Safe Hospital Discharge Donna L. Poole, Juliane N. Chainakul, Mary Pearson, LeAnn Graham Keywords: Discharge, Information technology, Medication
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
High 5s Project: Action on Patient Safety. SOP Flow Charts. 20 th International Forum on Quality and Safety in Healthcare April 2015 London, UK
 High 5s Project: Action on Patient Safety SOP Flow Charts 20 th International Forum on Quality and Safety in Healthcare 21-24 April 2015 London, UK Performance of Correct Procedure at Correct Body Site
High 5s Project: Action on Patient Safety SOP Flow Charts 20 th International Forum on Quality and Safety in Healthcare 21-24 April 2015 London, UK Performance of Correct Procedure at Correct Body Site
4/28/2017. Medication Management for Improved Compliance & Home Care Satisfaction PREPARED FOR NEHCC Presenter. Overview
 Medication Management for Improved Compliance & Home Care Satisfaction PREPARED FOR NEHCC 2017 Presenter Debra Demar, MS is the Community Liaison for White Cross Pharmacy, serving RI, MA and CT. She has
Medication Management for Improved Compliance & Home Care Satisfaction PREPARED FOR NEHCC 2017 Presenter Debra Demar, MS is the Community Liaison for White Cross Pharmacy, serving RI, MA and CT. She has
Chapter 13. Documenting Clinical Activities
 Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY. April 2009 September 2012
 MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY April 2009 September 2012 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire des médicaments du
MEDICATION SAFETY SELF-ASSESSMENT FOR LONG-TERM CARE ONTARIO SUMMARY April 2009 September 2012 Institute for Safe Medication Practices Canada Institut pour l utilisation sécuritaire des médicaments du
SPSP Medicines December 2016 WebEx NHS Lothian Reducing medicines harm across transitions
 SPSP Medicines December 2016 WebEx NHS Lothian Reducing medicines harm across transitions Welcome AIM: Support the learning and sharing between boards regarding medication reconciliation as a whole system
SPSP Medicines December 2016 WebEx NHS Lothian Reducing medicines harm across transitions Welcome AIM: Support the learning and sharing between boards regarding medication reconciliation as a whole system
Medication Reconciliation with Pharmacy Technicians
 Technician Education Day March 29, 2014 Jacksonville, FL Outline with Pharmacy Technicians Roma Merrick RPhT., CPhT. Pharmacy Technician Coordinator St. Vincent s Medical Center Southside Jacksonville,
Technician Education Day March 29, 2014 Jacksonville, FL Outline with Pharmacy Technicians Roma Merrick RPhT., CPhT. Pharmacy Technician Coordinator St. Vincent s Medical Center Southside Jacksonville,
The Search for Best Practice in Medication Reconciliation
 The Search for Best Practice in Medication Reconciliation National Medicines Forum November 2013 Marie Kehoe O Sullivan Director, Safety and Quality Improvement HIQA HIQA Collaboration with IHI Open School
The Search for Best Practice in Medication Reconciliation National Medicines Forum November 2013 Marie Kehoe O Sullivan Director, Safety and Quality Improvement HIQA HIQA Collaboration with IHI Open School
Optimizing Medication Safety in Maryland Assisted Living Facilities. Panel Discussion Moderated by: Nicole Brandt, PharmD
 Optimizing Medication Safety in Maryland Assisted Living Facilities Panel Discussion Moderated by: Nicole Brandt, PharmD 11 Objectives At the end of this knowledge based activity, the participants should
Optimizing Medication Safety in Maryland Assisted Living Facilities Panel Discussion Moderated by: Nicole Brandt, PharmD 11 Objectives At the end of this knowledge based activity, the participants should
MAR/MEDICATION AUDIT NAME NAME NAME
 MAR/MEDICATION AUDIT NAME NAME NAME DATE Copies of all current prescriptions in file (correlate with MAR, Meds on hand and Healthcare Communication Forms) MAR reflects current correct medications, correct
MAR/MEDICATION AUDIT NAME NAME NAME DATE Copies of all current prescriptions in file (correlate with MAR, Meds on hand and Healthcare Communication Forms) MAR reflects current correct medications, correct
Medicine Management Policy
 INDEX Prescribing Page 2 Dispensing Page 3 Safe Administration Page 4 Problems & Errors Page 5 Self Administration Page 7 Safe Storage Page 8 Controlled Drugs Best Practice Procedure Page 9 Controlled
INDEX Prescribing Page 2 Dispensing Page 3 Safe Administration Page 4 Problems & Errors Page 5 Self Administration Page 7 Safe Storage Page 8 Controlled Drugs Best Practice Procedure Page 9 Controlled
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives"
 2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
IHA Regional Pharmacy Best Possible Medication History Practice Standard
 IHA Regional Pharmacy Best Possible Medication History Practice Standard Section: None Origin Date: June 24, 2009 Number: None Reviewed Date: June 24, 2009 Revised Date: September 24, 2009 PRINTED copies
IHA Regional Pharmacy Best Possible Medication History Practice Standard Section: None Origin Date: June 24, 2009 Number: None Reviewed Date: June 24, 2009 Revised Date: September 24, 2009 PRINTED copies
What is Transition of Care?
 Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Transitions of Care and Reducing Readmissions Jackie Vance, RN, CDONA, FACDONA Director of Clinical Affairs and Industry Relations, AMDA NTOCC is chaired and coordinated by CMSA in partnership with sanofi
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Pharmacy Medication Reconciliation Workflow Emergency Department
 Objectives of the Pharmacy Forum Page To become familiar with EPIC functionalities used in prior to admission (PTA) medication reconciliation (Section 1) 2 7 To understand the pharmacy technicians role
Objectives of the Pharmacy Forum Page To become familiar with EPIC functionalities used in prior to admission (PTA) medication reconciliation (Section 1) 2 7 To understand the pharmacy technicians role
Safe Medication Practices
 Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
Safe Medication Practices Patient Safety: Preventing Adverse Events OHA Conference Renaissance Toronto Hotel at SkyDome Toronto June 14, 2004 David U President & CEO, ISMP Canada Agenda ISMP Canada Patient
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
Required Organizational Practices Resources for 2016
 Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Introduction of EPMA in paediatric practice in UK:
 Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Disclosure. SwedishAmerican Hospital A Division of UW Health. Learning Objectives. Medication History. Medication History 2/2/2017
 Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses
 Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses March 2018 College of Licensed Practical Nurses of Nova Scotia http://clpnns.ca Starlite Gallery, 302-7071 Bayers Road,
Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses March 2018 College of Licensed Practical Nurses of Nova Scotia http://clpnns.ca Starlite Gallery, 302-7071 Bayers Road,
Medicines Reconciliation: Standard Operating Procedure
 Clinical Medicines Reconciliation: Standard Operating Procedure Document Control Summary Status: Version: Author/Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
Clinical Medicines Reconciliation: Standard Operating Procedure Document Control Summary Status: Version: Author/Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS
 MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
Report on the. Results of the Medication Safety Self- Assessment for Long Term Care. Ontario s Long-Term Care Homes
 Report on the Results of the Medication Safety Self- Assessment for Long Term Care by Ontario s Long-Term Care Homes Report Submitted to: Ministry of Health And Long-Term Care Prepared by: ISMP Canada
Report on the Results of the Medication Safety Self- Assessment for Long Term Care by Ontario s Long-Term Care Homes Report Submitted to: Ministry of Health And Long-Term Care Prepared by: ISMP Canada
Using MEDMARX for Reporting and Benchmarking. Anne Skinner, RHIA Katherine Jones, PhD, PT
 Using MEDMARX for Reporting and Benchmarking Anne Skinner, RHIA Katherine Jones, PhD, PT Purpose of the Grant: Assist small rural hospitals to Voluntarily report and analyze medication errors Identify
Using MEDMARX for Reporting and Benchmarking Anne Skinner, RHIA Katherine Jones, PhD, PT Purpose of the Grant: Assist small rural hospitals to Voluntarily report and analyze medication errors Identify
Medication Reconciliation
 Medication Reconciliation Wendy Jordan, Pharm.D. Inpatient Pharmacy Manager St. Bernards Medical Center Jonesboro, AR Disclosure The speaker does not have anything to disclose Objectives Describe pharmacy
Medication Reconciliation Wendy Jordan, Pharm.D. Inpatient Pharmacy Manager St. Bernards Medical Center Jonesboro, AR Disclosure The speaker does not have anything to disclose Objectives Describe pharmacy
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project
 Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
Medication Management of Chronic Diseases in a Medical Home Model: CMS Medicaid Transformation Project Marie Smith, PharmD University of Connecticut School of Pharmacy Marghie Giuliano, RPh, CAE CT Pharmacists
All Wales Multidisciplinary Medicines Reconciliation Policy
 All Wales Multidisciplinary Medicines Reconciliation Policy June 2017 This document has been prepared by the Quality and Patient Safety Delivery Group of the All Wales Chief Pharmacists Group, with support
All Wales Multidisciplinary Medicines Reconciliation Policy June 2017 This document has been prepared by the Quality and Patient Safety Delivery Group of the All Wales Chief Pharmacists Group, with support
2017/18 Quality Improvement Plan
 2017/18 Improvement Plan Aim Change Enough information at discharge. Readmissio ns CHF Readmissio ns COPD Did you receive enough information from hospital staff about what to do if you were worried about
2017/18 Improvement Plan Aim Change Enough information at discharge. Readmissio ns CHF Readmissio ns COPD Did you receive enough information from hospital staff about what to do if you were worried about
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety
: Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety") Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Measure #130 (NQF 0419): Documentation of Current Medications in the Medical Record National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process
Electronic Medication Reconciliation and Depart Process Overview Nursing Deck
 Electronic Medication Reconciliation and Depart Process Overview Nursing Deck Revised: 8/16/2011 1 Introduction To achieve the highest standard of care that our system aspires to, as well as to meet the
Electronic Medication Reconciliation and Depart Process Overview Nursing Deck Revised: 8/16/2011 1 Introduction To achieve the highest standard of care that our system aspires to, as well as to meet the
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Medication Reconciliation
 Medication Reconciliation Define the term medication. Define medication reconciliation. Describe the potential barriers to obtaining an accurate medication list and resolution strategies to overcome these
Medication Reconciliation Define the term medication. Define medication reconciliation. Describe the potential barriers to obtaining an accurate medication list and resolution strategies to overcome these
A Pharmacist Network for Integrated Medication Management in the Medical Home
 A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
A Pharmacist Network for Integrated Medication Management in the Medical Home Marie Smith, PharmD UConn School of Pharmacy Professor/Dept. Head Pharmacy Practice Asst. Dean, Practice and Public Policy
CRAIG HOSPITAL POLICY/PROCEDURE
 CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
IMPROVING MEDICATION RECONCILIATION WITH STANDARDS
 Presented by NCPDP and HIMSS for the Pharmacy Informatics Community IMPROVING MEDICATION RECONCILIATION WITH STANDARDS December 13, 2012 Keith Shuster, Manager, Acute Pharmacy Services, Norwalk Hospital
Presented by NCPDP and HIMSS for the Pharmacy Informatics Community IMPROVING MEDICATION RECONCILIATION WITH STANDARDS December 13, 2012 Keith Shuster, Manager, Acute Pharmacy Services, Norwalk Hospital
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING
 Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Medication Reconciliation Harmonization
 Medication Reconciliation Harmonization June 5, 2018 Context Fall 2017 Behavioral Health SC discussion about medication reconciliation Desire for greater alignment in measure specifications April 2018
Medication Reconciliation Harmonization June 5, 2018 Context Fall 2017 Behavioral Health SC discussion about medication reconciliation Desire for greater alignment in measure specifications April 2018
Constant Pursuit of Medication Safety. Geraldine Koh Chief Pharmacist
 Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
CHAPTER 7 Safe Medication Administration
 64 SECTION 3 READING MEDICATION LABELS AND SYRINGE CALIBRATIONS CHAPTER 7 Safe Medication Administration Objectives The learner will: 1. read a MAR to identify medications to be administered. 2. record
64 SECTION 3 READING MEDICATION LABELS AND SYRINGE CALIBRATIONS CHAPTER 7 Safe Medication Administration Objectives The learner will: 1. read a MAR to identify medications to be administered. 2. record
Medication Reconciliation
 Medication Reconciliation The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health Netsmart Technologies Today
Medication Reconciliation The Care Transitions Network National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental Health Netsmart Technologies Today
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Pharmacy Technician led model to reduce the rate of omitted medicines
 Pharmacy Technician led model to reduce the rate of omitted medicines By Fleur Baylis Lead Pharmacist Patient Safety Brighton and Sussex University Hospitals NHS Trust Outline NPSA alert Missed doses Trust
Pharmacy Technician led model to reduce the rate of omitted medicines By Fleur Baylis Lead Pharmacist Patient Safety Brighton and Sussex University Hospitals NHS Trust Outline NPSA alert Missed doses Trust
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Safer Healthcare Now! Instructions for Data Entry and Submission Using Measurement Worksheets
 Instructions for Data Entry and Submission Using Measurement Worksheets SHN Central Measurement Team January 30, 2009 Table of Contents Section 1. General and Background Information... 2 CAMPAIGN BACKGROUND...
Instructions for Data Entry and Submission Using Measurement Worksheets SHN Central Measurement Team January 30, 2009 Table of Contents Section 1. General and Background Information... 2 CAMPAIGN BACKGROUND...
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Medication Accuracy at Transitions in Care Let s start!
 Medication Accuracy at Transitions in Care Let s start! @PatVei Erica Van der Schrieck-De Loos MSc, Project leader WHO H5s NL CBO Dutch Institute for Healthcare Improvement EU Union Network PaSQ Med Rec
Medication Accuracy at Transitions in Care Let s start! @PatVei Erica Van der Schrieck-De Loos MSc, Project leader WHO H5s NL CBO Dutch Institute for Healthcare Improvement EU Union Network PaSQ Med Rec