Technical Assistance Guide. Enhancing PDMPs: A Comparison of Changes 2010 to 2016
|
|
|
- Norman Banks
- 5 years ago
- Views:
Transcription



1 Technical Assistance Guide Enhancing PDMPs: A Comparison of Changes 2010 to 2016 December 2016 This project was supported by Grant No PM-BX-K001 awarded by the Bureau of Justice Assistance. The Bureau of Justice Assistance is a component of the Office of Justice Programs, which also includes the Bureau of Justice Statistics, the National Institute of Justice, the Office of Juvenile Justice and Delinquency Prevention, and the Office for Victims of Crime. Points of view or opinions in this document are those of the author and do not represent the official position or policies of the U.S. Department of Justice.
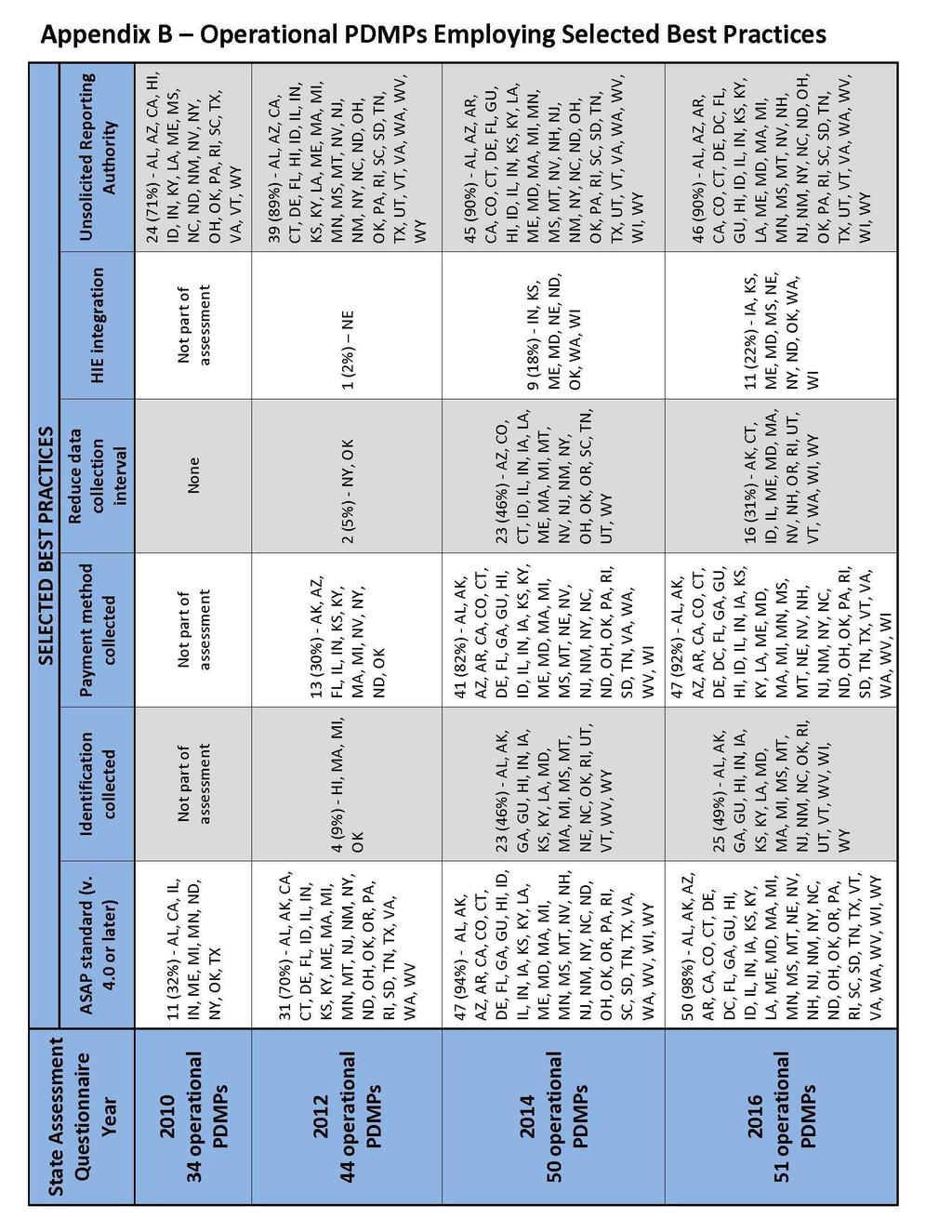
2 Introduction Since 2010, the Prescription Drug Monitoring Program Training and Technical Assistance Center (TTAC) at Brandeis University, with support from the Bureau of Justice Assistance (BJA), has conducted four (4) State Assessments of prescription drug monitoring programs (PDMPs) (2010, 2012, 2014, 2016). The assessments have gathered data on PDMP statutes, regulations, policies and procedures, tracked their changes over time, and identified program trends and candidate practices. As more PDMPs were implemented and new laws and practices were instituted, the TTAC assessments evolved to capture those changes, new practices and trends. When TTAC conducted its first PDMP State Assessment (2010), there were 11 fewer states with a PDMP than when the second one was conducted (2012). Historically, as new PDMPs were implemented they adopted the best practices and proven policies of established PDMPs, took advantage of newer technology, and addressed the needs of a wider group of stakeholders. For example, PDMPs today are seeking to integrate their data into Health Information Exchanges (HIEs), which was not on any PDMP s agenda in Because TTAC adapted its assessments in response to new trends and practices of PDMPs, some questions and topics are covered in all four (4) assessments, while others are unique to a particular one (see Appendix A). Despite their differences, the assessments document PDMPs progress and changes from 2010 to 2016, including which practices were adopted by PDMPs and which were discarded or modified. For example, in 2010 all PDMPs collected information from pharmacies every 30 days, whereas by 2016, over two-thirds of the PDMPs had shortened the data collection interval to 24 hours. (current status map) The response rates on the State Assessments were: 85% (29 of 34 operational PDMPs) in 2010, 73% (32 of 44 operational PDMPs) in 2012, 100% (50 of 50 operational PDMPs) in 2014, and 84% (43 of the 51 operational PDMPs) in Please note that TTAC obtained information from 12 additional PDMPs following the 2012 State Assessment; bringing the response rate to 100%. The additional PDMPs information is included in the results. Efforts are being made to reach 100% for the 2016 State Assessment and this document will be updated accordingly. Please see Appendix B for a table summarizing the findings described below, including the percentage of PDMPs that had adopted each practice as of
3 Methodology In September 2012, the PDMP Center of Excellence (COE) published a white paper entitled Prescription Drug Monitoring Programs: An Assessment of the Evidence for s. Drawing on published research, consensus statements of expert opinion, and accumulated experience among states, this report identified 35 best and promising practices likely to help maximize PDMP effectiveness. These fell into 7 major categories: Data collection and data quality Data linking and analysis User access and report dissemination PDMP recruitment, utilization, and education Inter-organizational best practices for PDMPs Evaluation of PDMPs Funding PDMPs For each practice, the white paper provides the rationale for the best practice, the evidence for its effectiveness, current adoption by states, and barriers to adoption. In many instances, the adoption status, in the white paper, was derived from information collected from the 2012 TTAC State Assessment. of Suggested PDMP s Using data from the four (4) TTAC assessments and information received from the PDMPs separate and subsequent to the assessments, this guide details the changes and evolution PDMPs have undergone between 2010 and 2016 as they apply to the following selected best practices: Adopt uniform and latest ASAP reporting standard Collect positive identification for the person picking up prescriptions Collect data on method of payment, including cash transactions Reduce data collection interval; move toward real-time data collection Integrate PDMP reports with health information exchanges, electronic health records, and pharmacy dispensing systems Send unsolicited reports and alerts to appropriate users o Authority to Provide Unsolicited/Threshold Reports o Engaged in Providing Unsolicited/Threshold Reports Mandate enrollment Mandate utilization Delegate Access Enact and implement interstate data sharing among PDMPs Secure funding independent of economic downturns, conflicts of interest, public policy changes, and changes in PDMP policies 3
4 1. Adopt uniform and latest ASAP reporting standard The American Society for Automation in Pharmacy (ASAP) has developed standards for pharmacy data fields and formats that every PDMP uses. Since 1995, there have been five (5) ASAP versions released; the latest being version 4.2 in A recommended practice is for every PDMP to migrate to the most recent version of ASAP and implement new versions as they become available. The rationale for this practice is that uniform data collection standards facilitate improved data quality, data analysis across PDMP programs and interstate data sharing among PDMPs. According to the assessment results in 2010, there were 11 PDMPs using ASAP version 4.0 or later. In 2012, 31 PDMPs reported using ASAP version 4.0 or later. In 2014, 47 PDMPs reported using ASAP version 4.0 or later. Currently, there are 50 PDMPs using ASAP version 4.0 or later; in fact, 37 PDMPs are using the most recent version of ASAP. (current status map) 2. Collect positive identification for the person picking up prescriptions Verification of the person who is picking up the medication is an effective practice required by some states. In many instances, the person at the pharmacy counter retrieving a prescribed medication is not the patient to whom the medication was prescribed. There have been accounts of a patient s family member or friend obtaining the medication from the pharmacy without the patient s consent or knowledge. Collecting positive identification lessens the risk of abuse, fraud, and diversion or, at a minimum, aids in a diversion investigation following a suspected prescription diversion or fraud incident. Although PDMPs were not surveyed about collecting positive identification in the 2010 and 2012 State Assessments, the topic was covered in 2014 and The PDMPs were asked if they collect the identification on the A) patient, B) person dropping off the prescription (if different from the patient), and C) person picking up the prescription (if different from the patient. Currently, there are 24 PDMPs that collect the patient s identification, 3 PDMPs that collect the identification of the person dropping off the prescription and 11 PDMPs that collect the identification of the person picking up the medication. (current status map) 4
5 3. Collect data on method of payment, including cash transactions The method by which a person pays for their prescription medications can be an indicator of possible questionable activity. Studies (Riggs et al., ) have shown that doctor shoppers and operators of pill mills prefer cash transactions. This limits the information available to insurance companies and other 3 rd party payers to identify potential instances of fraud or patient abuse. According to the 2012 assessment, 13 PDMPs collected method of payment. By 2014, the number of PDMPs collecting the method of payment jumped to 41. The number has increased again in 2016 to 47 PDMPs. This question was not included in the 2010 State Assessment. (current status map) 4. Reduce data collection interval The recommended best practice of reducing the time a pharmacy has to transmit the prescription information to the PDMP (data collection interval), for example from weekly to daily, is based on the rationale that more timely information is of greater use to authorized requestors. Having the most up-to-date prescription history information increases the utility of PDMP data for clinical practice and drug diversion investigations. According to the 2010 State Assessment, none of the operational PDMPs had reduced their data collection interval. In 2012, only 2 PDMPs had reduced their data collection interval. In 2014, 23 PDMPs reduced the interval. Since then, 16 PDMPs have reduced the interval; 36 PDMPs now have daily or real-time data collection. (current status map) 5. Integrate PDMP data with health information exchanges PDMPs continuously seek ways to increase PDMP usage and usability. Simplifying the method of access to the PDMP for prescribers and dispensers makes it more likely that prescription history information will be used in clinical decision-making. One approach, supported by government and industry, is to integrate PDMP data into health information exchanges (HIE). The 2010 and 2012 State Assessments did not cover this topic; however, information other TTAC sources show that, in 2012, there was only 1 PDMP integrated with a HIE (NE). By 2014, the 1 Rigg, et al., Prescription Drug Abuse and Diversion: Role of the Pain Clinic. Journal of Drug Issues
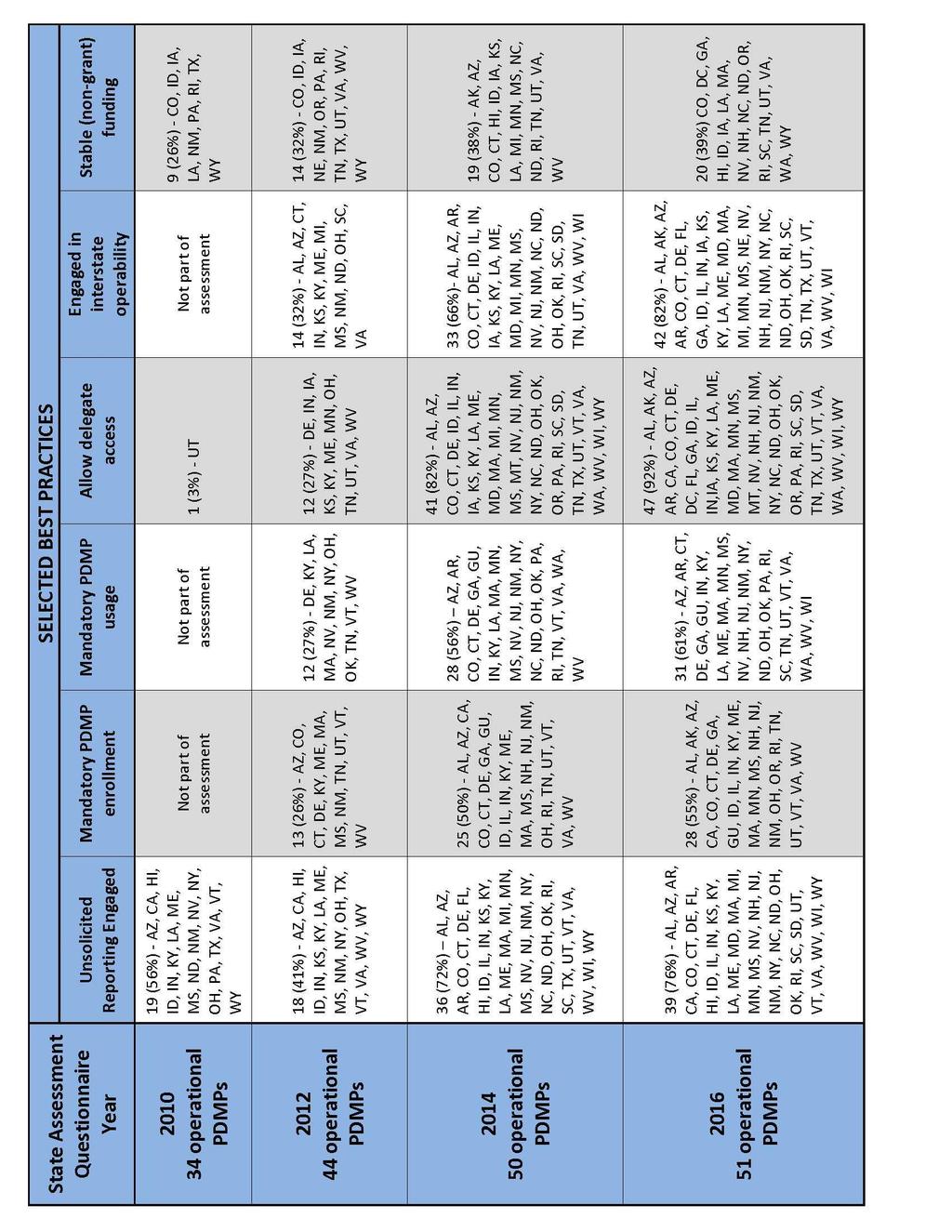
6 number had increased to 9 PDMPs; currently, there are 11 PDMPs integrated with a HIE with several other PDMPs taking steps to integrate. 6. Send unsolicited reports and alerts to appropriate users Unsolicited reports and alerts are methods many PDMPs employ to proactively notify authorized requestors (typically, prescribers and dispensers) that a patient may potentially be engaged in questionable activity (i.e., doctor shopping) or at risk of overdose. The reports may also be sent to licensing/regulatory boards or law enforcement on registrants that may potentially be engaged in inappropriate or illegal prescribing or dispensing. (current status maps: prescriber, dispenser, licensing board, law enforcement) Authority to Provide Unsolicited Reports According to the 2010 State Assessment, there were 24 PDMPs with the statutory authority to provide unsolicited reports; by 2012, this had increased to 39; and by 2014, 46 PDMPs reported having this authority. Engaged in Providing Unsolicited Reports In 2010, there were 19 PDMPs engaged in sending unsolicited reports to authorized users; in 2012, there were 18; in 2014, there were 36 PDMPs sending reports. In 2016, the number has increased to 39 PDMPs. 7. Mandatory PDMP enrollment There are several states whose PDMPs remain under-utilized by a large percentage of prescribers or dispensers. To address this issue, states have passed statutes or enacted regulations that require prescribers and/or dispensers to enroll with the PDMP; the ultimate goal being for practitioners to use PDMP data in clinical care and dispensing. A listing of the various state criteria is available on the TTAC website: Enrollment Conditions. In 2012, 13 PDMPs mandated PDMP enrollment, increasing to 25 in 2014, and to 28 since then. Information on mandated enrollment and utilization (see below) was not collected in (current status map) 6
7 8. Mandate utilization Similar to mandated enrollment, mandated utilization seeks to increase the number of practitioners using the PDMP for clinical care. Unlike enrollment, utilization is typically mandated under certain circumstances, e.g., before prescribing a controlled substance to a new patient, if the prescriber believes a patient is seeking drugs for non-medical reasons, or if the patient has been prescribed opioids for six months or more. A listing of the various state criteria is available on the TTAC website: Utilization Conditions. In 2012, there were 12 PDMPs that mandated PDMP usage; in 2014, there were 28 PDMPs; and the number increased again to 31 PDMPs. This information was not collected in the 2010 State Assessment. (current status map) 9. Delegate Access To allow prescribers more time to treat their patients, many states have allowed them to delegate office staff to access the PDMP data on their behalf ( delegates ). Adding delegates as authorized PDMP users is a recommended best practice since it is believed that this will increase utilization by prescribers. The 2010 State Assessment indicated that only one PDMP (UT) allowed delegate access to the PDMP. In 2012, there were 12 PDMPs that authorized the use of delegate accounts. In 2014, 41 PDMPs authorized delegates. Currently, 47 PDMPs allow PDMP access for delegates. (current status table) 10. Enact and implement interstate data sharing among PDMPs PDMPs are state-based programs initially developed to support the transmission, collection and utilization of prescription data within a state. As more states adopted PDMPs, the next logical step was sharing data across state lines. Interstate sharing of PDMP data is now a top priority to ensure that healthcare professionals have a complete picture of their patients prescription history. In 2012, 14 PDMPs reported that they were engaged in interstate data sharing with at least one other state. According to information received through 2014, 33 PDMPs have implemented interstate data sharing. Currently, there are 42 PDMPs engaged in interstate data sharing; the other 9 PDMPs are considering it or actually in the process of planning, approving agreements with other PDMPs or a hub vendor, or developing the technical capabilities. There are hubs available 7
8 for PDMPs to connect and although cross hub communication is not operational as of this writing. Through the support of BJA, the technology has been developed, tested, and is available to operators of the hubs. A hub is a service that enables sharing of data between two or more states by routing transactions to and from PDMPs. Information on data sharing was not collected in the 2010 State Assessment. (current status map) 11. Obtain secure funding For many PDMPs, obtaining sufficient and secure operating funds continues to be problematic. Were it not for grants or short-term allocated funds, several PDMPs would be without any means of support. For the purposes of this document, secure funding is defined as that coming from state revenue sources or non-grant sources; PDMPs receiving any grant funds (even a small percentage) were excluded. According to the results of the 2010 State Assessment, there were 9 PDMPs operating without any grant funding. Per 2012 information, there were 14 PDMPs operating without grant funding. There were 19 PDMPs operating without grant funding in Currently, there are 20 PDMPs operating solely on state revenue or non-grant sources. (current status map) Note: the above changes and the corresponding numbers from the four (4) TTAC State Assessments and subsequent contact with the PDMPs are listed in tabular form in Appendix B and additional status maps/tables are available on the TTAC website. Conclusion Based on the information provided by PDMPs for the four (4) TTAC assessments, it is evident that PDMPs are continually evolving and becoming more homogeneous; resulting in programs that are more efficient and effective. It is also apparent that enhancements to one PDMP which show positive results, often lead to similar enhancements in other PDMPs. PDMPs are not static; as new prescription abuse and misuse challenges arise, technology improves, and research on PDMP effectiveness reveals, resulting in PDMPs being better able to adapt and improve. To keep abreast of the changes, TTAC will maintain a close working relationship with the PDMPs and plans to routinely conduct state assessments. The assessment results have been compiled and are available to any stakeholder. 8
9 Appendix A List of Questions from State Assessments * 2010 State Assessment (34 operational PDMPs 29 responses received) 1. State/Territory/District 2. Alliance of States with PMP Region 3. Name of Program 4. Acronym, if applicable 5. Website where PMP information is available 6. Name of Agency responsible for management of PMP 7. Agency Type 8. Contact 9. State Population 10. Number of Pharmacies within state (DEA registered or state CS registered) 11. Number of practitioners authorized to prescribe controlled substances (DEA registered or state CS registered 12. Drugs/Schedules Monitored 13. Other drugs, please list 14. Number of prescription records collected in calendar year Frequency of data collection required by law 16. From which dispenser types do you collect data 17. Number of patient history reports produced in calendar year Who is authorized to request patient specific information? 19. Do state law/rules permit deidentified data to be provided to researchers? 20. Year when initial PMP authorizing legislation was signed into law 21. Year when PMP initially became operational 22. Laws/Statute(s) citation(s) 23. Website where located 24. Regulation/Rule(s) citation(s) 25. Website where located 26. Total Annual Budget 27. Source of Funding 28. Total of annual PMP budget spent on PMP staff 29. Total annual dollar amount spent on vendors 30. Total annual dollar amount spent on software/licenses 31. Total number of staff allocated to PMP 32. Does your agency use an in-house or an outside vendor for data collection? 33. Does your agency store the collected data in-house or with an outside vendor? 34. Does your agency use a vendor to host your web portal & provide reports or is it done in-house? 35. From what dispenser types do you collect data? 36. Which version(s) of the American Society for the Automation of Pharmacy (ASAP) standard for PMP data transmission do you allow to be reported? 37. How and when may patient prescription history reports be requested by users and sent-out by your office/ web portal? 38. Do you have a law/ rule/ policy for data retention? 39. What data must be purged? 9
10 * 2010 State Assessment (cont'd) 40. Can data be maintained after this time period if the identification of patients, prescribers and/or dispensers have been encrypted or deidentified? 41. To which groups is your agency authorized to provide unsolicited reports? 42. To which groups is your agency currently providing unsolicited reports? 43. To which groups does your agency currently provide information? 44. Does your PMP provide training courses to users regarding use of PMP data? 45. Please provide the following information regarding the training program developed by PMP or vendor; on web, printed, other; in-person training, other 46. Does your PMP require the following users to be trained in the use of PMP data? Prescribers, pharmacists/pharmacies, law enforcement, regulatory agencies, attorney general staff, patient, researcher * The 2010 State Assessment was sent in 2 parts: questions 1 through 25 were sent at the end of 2009 and questions 26 through 46 were sent at the beginning of State Assessment (44 operational PDMPs 32 responses received) 1. Enter the name of state or territory where the PMP is located. 2. Enter the name of the monitoring program or its acronym, if applicable. 3. Enter the name of the agency responsible for the PMP. 4. Select the type of agency responsible for the PMP. If the agency type is not in the drop-down list, please enter the type in the `other' box. 5. Enter the web address for the PMP, if applicable. 6. Enter the address for the PMP, if applicable. 7. Enter the name for the primary contact person, with their title, for the PMP. 8. Enter the primary contact person's complete mailing address. 9. Enter the primary contact person's telephone number. 10. Enter the primary contact person's address. 11. Enter the state's population from the most recent published census. 12. Select the controlled substance schedules monitored by the PMP. 13. Answer whether or not the PMP has the statutory authority to monitor any other drugs/drug products. If `Yes', please list the other drugs/drug products. 14. Answer whether or not the PMP has the authority to remove any drugs/drug products from being monitored. If `Yes', please list any drugs/drug products that are currently removed from monitoring. 15. Enter the number of days a dispenser is required to submit prescription information to the PMP. If the dispenser is required to submit information on a `real-time' basis, enter Enter the year that legislation, enabling the PMP, was passed by the state. 17. Enter the year that the PMP became operational. If the PMP is not operational at the time of the assessment, please leave blank. 18. Enter the title, chapter and section of or a web link to any laws/statutes pertaining to the PMP. 19. Enter the title, chapter and section of or a web link to any rules/regulations pertaining to the PMP. 20. Enter the title, chapter and section of or a web link to any laws/statutes pertaining to `doctor shopping', if applicable. 21. Enter the title, chapter and section of or a web link to any laws/statutes pertaining to `pill mills', if applicable. 22. Select the version(s) of ASAP that dispensers employ when transmitting prescription information to the PMP. 23. Select the transmission method(s) that dispensers utilize to provide prescription information to the PMP. If another method is used, please indicate in the `other' box. 24. Select the type(s) of entities that transmit prescription information to the PMP. If there are other transmitters, please indicate in the `other' box and briefly describe. 10
11 2012 State Assessment (cont'd) 25. Answer whether or not the PMP is currently engaged in efforts to electronically share data with another state's PMP. (Public Forum) If `Yes', please briefly describe those efforts. (Administrator's Forum) 26. Answer if a prescriber or dispenser is required to register with the PMP. 27. Answer if a patient check of the PMP data is required by the prescriber or dispenser prior to writing a prescription or dispensing a medication. If a check is required, please detail any conditions of the requirement that apply. 28. Select the individuals/entities (in-state and/or out of state) that the PMP is authorized to release solicited and/or unsolicited reports. If there are other individuals/entities, please list notating whether release if authorized for in-state and/or out of state both solicited and/or unsolicited. 29. Please detail any special conditions (i.e. subpoena, court order, warrant, judicial approval, active investigation, etc.) that must be met by law enforcement prior to the release of PMP information. 30. Select the type of prescription history reports that are available to authorized requestors/users. If other types of prescription history reports available, please briefly describe them. 31. Answer whether or not the PMP has the statutory authority to release de-identified prescription information to a researcher. If the answer is yes, please list any conditions that must be met for the release. De-identified data is data where the identities of patients, prescribers, and dispensers has been removed and replaced with a code/number that is unique to individual patients, prescribers, and dispensers. The code/number cannot be reversed to identify the patient, prescriber, or dispenser. (Administrator's Forum) 32. Enter the number of prescribers licensed in your state as of the end of calendar years 2010 and Enter the number of controlled substance prescribers licensed in your state as of the end of calendar years 2010 and 2011 per DEA records. 34. Enter the number of different prescribers issuing a controlled substance prescription as for calendar years 2010 and (Administrator's Forum) 35. Enter the number of pharmacies licensed in your state as of the end of calendar years 2010 and If possible, please provide the number of in-state/resident pharmacies and out of state/non-resident pharmacies for the same time frame. 36. Enter the number of pharmacies licensed in your state as of the end of calendar years 2010 and 2011 per DEA records. 37. Enter the number of pharmacists licensed in your state as of the end of calendar years 2010 and Enter the number of controlled substance prescriptions transmitted to the PMP for calendar years 2010 and If possible, please provide the number by Schedule of controlled substance. Totals (Public Forum); Itemized by Schedule (Administrator's Forum) 39. If possible, please provide the number of controlled substance prescriptions transmitted to the PMP by drug type for calendar years 2010 and Totals (Public Forum); Itemized by Type (Administrator's Forum) 40. Enter the number of dosage units prescribed that were transmitted to the PMP for calendar years 2010 and If possible, please provide the number by Schedule of controlled substance. Totals (Public Forum); Itemized by Schedule (Administrator's Forum) 41. If possible, please provide the number of dosage units prescribed that were transmitted to the PMP by drug type for calendar years 2010 and Totals (Public Forum); Itemized by Type (Administrator's Forum) 42. Enter the number of patient history reports that were released by the PMP for calendar years 2010 and Enter the number of prescriber history reports that were released by the PMP for calendar years 2010 and Enter the number of dispenser history reports that were released by the PMP for calendar years 2010 and Enter the number of statistical history reports that were released by the PMP for calendar years 2010 and Enter the number of unique authorized requestors of prescription history reports for each applicable type for calendar years 2010 and If there are other types of requestors, please list them and their number. (Administrator's Forum) 11
12 2014 State Assessment (50 operational PDMPs 50 responses received) 1. Name of the State or Territory 2. Name of the PDMP (include any acronym) 3. Name of the Agency Responsible for PDMP 4. Type of Agency (i.e., Board of Pharmacy, Consumer Protection, Department of Health, Health Information Exchange, Law Enforcement, Professional Licensing, Substance Abuse, Other) 5. PDMP Website Address 6. PDMP Address 7. Primary Contact Person and Title for PDMP 8. Contact Mailing Address 9. Contact Telephone Number 10. Contact Address 11. Frequency of Data Collection (in days) 12. ASAP Version(s) Employed 13. Data Management - Vendor or In-House 14. Data Access via Web Portal/On-Line 15. Entity Transmitting Data to PDMP 16. Interstate Data Sharing 17. Required to Enroll with PDMP 18. Required to Check PDMP Prior to Issuing/Filling Prescription 19. Method of Payment Captured by PDMP 20. Patient Identification Captured by PDMP 21. Person Dropping Off Prescription Identification Captured by PDMP (if person is not patient) 22. Person Picking Up Medication Identification Captured by PDMP (if person is not patient) 23. PDMP Data Requestors (indicate if PDMP has authority to release data and/or engaged in releasing data; whether solicited/unsolicited; in-state/out of state) 24. Ability to Identify Prescriber's Specialty? 25. Types of PDMP Reports Available 26. Types of PDMP Reports Available to a Prescriber 27. Types of PDMP Reports Available to a Dispenser 28. Types of PDMP Reports Available to Licensing Boards 29. Types of PDMP Reports Available to Law Enforcement 30. Access to Prescription Data via Health Information Exchange (HIE) 31. Access to Prescription Data via Electronic Health Record (EHR) System 32. Access to Prescription Data via Pharmacy Dispensing System 33. Release of De-identified Prescription Information 34. Release of Prescription Information for Epidemiological or Educational Purposes 35. Requirements to Release Data to Law Enforcement 36. Matching Method for Patient Record Queries 37. Link to PDMP On-line Statistical Data 38. PDMP Funding and Staffing 39. Percent of PDMP Funding from Source(s) 40. Upcoming Changes Impacting the PDMP 12
13 2016 State Assessment (51 operational PDMPs 43 responses received) 1. State 2. Agency Responsible (Name of the agency housing the PDMP) 3. Agency Type 4. PDMP Public Website (URL for information about PDMP) 5. PDMP (Published address for PDMP) 6. PDMP Enrollment Website (URL to obtain PDMP account) 7. PDMP Query Website (URL for requestors to query PDMP) 8. PDMP Data Upload Website (URL for data transmitters to upload prescription data) 9. Primary Contact Name - Job Title 10. Address 11. City State Zip 12. Telephone 13. Fax Secondary Contact Name - Job Title 16. Address 17. City State Zip 18. Telephone 19. Fax Controlled Substance Schedules Monitored 22. Authority to Monitor Other Substances 23. If yes, list the other substances 24. Data Collection Frequency (# of days) 25. Enabling Legislation Enacted 26. PDMP Operational Date 27. Beginning Date for Electronic Data Submission (Date of first electronic submission to PDMP) 28. User Access Date (Date requestors were first able to obtain data from PDMP) 29. Law/Statute Citation(s) (Applicable laws/statutes for PDMP) 30. Regulation/Rule Citation(s) (Applicable regulations/rules for PDMP) 31. Doctor Shopper Law/Statute Citation(s) 32. Unauthorized Use of PDMP Data Law/Statute Citation(s) 33. Pill Mill Law/Statute Citation(s) 34. Pain Clinic Law/Statute Citation(s) 35. Weblink for Law/Statute 36. Weblink for Regulation/Rule 37. Automatic Enrollment with License Renewal or Application 38. Describe Enrollment Method(s) (Describe the general process a person follows to obtain a PDMP account (e.g., online enrollment, notarized application)) 39. Minimum criteria for prescribers to obtain PDMP account 40. Minimum criteria for dispensers to obtain PDMP account for querying system 41. Minimum criteria for dispensers to obtain PDMP account for uploading data 42. Minimum criteria for law enforcement to obtain PDMP account 43. Minimum criteria for regulatory/licensing boards to obtain PDMP account 44. Minimum criteria for prescriber delegates to obtain PDMP account 13
14 2016 State Assessment (cont d) 45. Minimum criteria for dispenser delegates to obtain PDMP account 46. Minimum criteria for physician assistants to obtain PDMP account 47. Minimum criteria for nurse practitioners to obtain PDMP account 48. Minimum requirements for other requestors to obtain PDMP account (List the minimum requirements for any other requestor if different from above) 49. Patient Access to List of Users Requesting Their Data 50. If yes, conditions for Patients to Access Query List (List the requirements for patients to get access to PDMP queries) 51. Minimum requirements for Patients to obtain their PDMP history, if allowed (List the requirements for patients to obtain a copy of their own PDMP history) 52. Minimum Requirements for Law Enforcement to Access PDMP (Indicate the lowest threshold for law enforcement to obtain PDMP data) 53. Minimum requirements for other requestors to Access PDMP (List the minimum requirements for any other requestor if different from above) 54. Number of delegates allowed (If there is a maximum number of delegates allowed by statute, list the number) 55. Review/audit of delegate accounts (Are supervising practitioners required by statute to periodically review/audit their delegates PDMP query history?) 56. Minimum data elements to query PDMP by healthcare user (Indicate the fewest fields required to conduct a PDMP query (e.g., last name, first name, dob or partial last name, partial first name, dob)) 57. Query by partial data elements by healthcare user (If allowed, indicate the minimum number of characters to search by) 58. Optional data elements to query PDMP by healthcare user (Indicate other fields available to conduct a PDMP query) 59. Minimum data elements to query PDMP by non-healthcare user (Indicate the fewest fields required to conduct a PDMP query (e.g., last name, first name, dob or partial last name, partial first name, dob)) 60. Query by partial data elements by non-healthcare user (If allowed, indicate the minimum number of characters to search by) 61. Optional data elements to query PDMP by non-healthcare user (Indicate other fields available to conduct a PDMP query) 62. Ability to search for multiple patients in one query 63. If yes, what is the maximum number of patients 64. Prescriber Mandatory Enrollment 65. Dispenser Mandatory Enrollment 66. Mandatory Enrollment Conditions (Stipulated conditions/exceptions for PDMP enrollment) 67. Prescriber Mandatory Use 68. Dispenser Mandatory Use 69. Mandatory Use Conditions (Stipulated conditions/exceptions for PDMP use) 70. Established Advisory Group 71. Payment Method Captured 72. Patient Identification Required to be Presented to Dispenser 73. Patient Identification Captured by PDMP (When patient drops off the prescription) 74. Identification of person captured by PDMP when prescription dropped off (If person is not the same as the patient) 75. Identification of person captured by PDMP when medication is picked up (If person is not the same as the patient) 76. Ability to Identify Prescriber Specialty 77. Authority to Release De-Identified Data 78. Authority to Release raw, bulk, or de-identified PDMP Data for Epidemiological/Educational Purposes 14
15 2016 State Assessment (cont d) 79. Engaged in the Release of raw, bulk, or de-identified PDMP Data for Epidemiological/Educational Purposes 80. Data Retention Policy In Place 81. Data Retention Time Frame 82. Type(s) of PDMP Information Purged (e.g., patient identifiers, medication information, dates issued/filled) 83. Is De-Identified Data Retained 84. PDMP Training Required Prior to Use 85. If yes, list who is required to take the training (e.g., prescribers, dispensers, licensing board investigators, law enforcement investigators) 86. Describe the training format (e.g., web based, in-person, printed materials) 87. If training materials online, provide weblink 88. Is sales data from pharmaceutical manufacturers or distributors available to or accessible by the PDMP 89. If yes, how is sales data accessed (Describe process to obtain sales data) 90. If yes, how frequently is sales data updated 91. If yes, list the sales data elements collected (e.g., manufacturer, date sold, recipient, medication information, quantity) 92. Require zero-reporting by dispensers 93. If yes, indicate the frequency of zero-reporting 94. Required Notification to patients of release of PDMP information 95. Require patient consent prior to release of PDMP information to authorized requestor 96. Does PDMP collect naloxone prescriptions 97. Who reports naloxone prescriptions (e.g., hospitals, law enforcement, ambulance service) 98. Frequency unsolicited alerts/reports generated (Enter 'n/a' if unsolicited reports are not generated) 99. List the unsolicited alerts/reports criteria (Describe the parameters used to generate unsolicited alerts/reports, if applicable) 100. Unsolicited alerts/reports delivery method (Indicate the method by which the unsolicited alerts/reports are provided to the recipient, if applicable) 101. Are unsolicited alerts/reports sent to practitioners who are NOT enrolled with the PDMP 102. Can users set personal threshold for alert notices 103. Ability to do user-led alert notices (Do users have the ability to initiate alert notices to other users) 104. Capture or access to registrant's disciplinary history/status 105. Capture or access to patient lock-in information 106. Capture or access to reports of lost/stolen prescription drugs 107. Capture or access to opioid-related drug overdoses or deaths 108. List any new innovations or activities that are planned or implemented within last year. (Describe any activities or changes in operations/technology that may be of interest for other PDMPs. Note: This information will not be share by TTAC without permission.) 109. Version(s) of ASAP Allowed for Data Transmission 110. Methods Allowed to Provide Data to PDMP (e.g., electronic, fax, mail, other media) 111. Required Prescription Data Transmitters (e.g., in-state pharmacy, mail-order pharmacy, dispensing doctor, veterinarian, Veterans Administration, Department of Defense, Indian Affairs, Indian Health Service) 112. Data Collection Entity (Entity responsible for the collection of data from required transmitters) 113. If Vendor, Provide Name 114. Data Storage Entity (Entity responsible for the storage of received data) 115. If Vendor, Provide Name 116. Report Generation Entity (Entity responsible for production of PDMP reports) 117. If Vendor, Provide Name 15
16 2016 State Assessment (cont d) 118. Data Access Entity (Entity responsible for enabling login and entry to PDMP) 119. If Vendor, Provide Name 120. Is PDMP Data Accessed via HIE (Can users access PDMP data through their health information exchange) 121. If yes, how widespread (i.e., statewide, regional, local) 122. Is PDMP Data Accessed via EHR (Can users access PDMP data through their electronic health record system) 123. If yes, how widespread (i.e., statewide, regional, local) 124. Is PDMP Data Accessed via PDS (Can users access PDMP data through their pharmacy dispensing system) 125. If yes, how widespread (i.e., statewide, regional, local) 126. Engaged in Interstate Data Sharing 127. If yes, which method 128. If yes, list the states with whom you are sharing 129. If no, list the impediments to sharing 130. PDMP certified as a CMS Specialized Registry 131. Method to Match/Cluster Patients (If PDMP matches/clusters same patients, describe the process (exact, probabilistic only, probabilistic and manual)) 132. Does PDMP require information on e-prescriptions 133. Have data-dashboards on public website (Data dashboards are panels summarizing various aggregated PDMP data on PDMP public website) 134. Have user-friendly interfaces (User-friendly interfaces when logged into account, such as decision support tools and patient risk scores) 135. PDMP staff use of automated software and systems to expedite analyses and reports (software or algorithms that analyze PDMP data (e.g., business intelligence software)) 136. Provide online user guides and educational materials on website or with reports 137. Prescriber - Patient Reports (Can prescribers obtain patient reports) 138. Prescriber - Self History (Can prescribers obtain records of their prescribing history) 139. Dispenser - Patient Reports (Can dispensers obtain patient reports) 140. Dispenser - Self History (Can dispensers obtain records of their dispensing history) 141. Licensing Board - Patient Reports (Can Boards obtain patient reports) 142. Licensing Board - Licensee History/Activity (Can Boards obtain reports on their licensees) 143. Law Enforcement - Patient Reports (Can law enforcement obtain patient reports) 144. Law Enforcement - Prescriber History/Activity (Can law enforcement obtain prescriber reports) 145. Law Enforcement - Dispenser History/Activity (Can law enforcement obtain dispenser reports) 146. Provide summary data on or with patient reports (Does PDMP include summary data (e.g., MMEs, MPEs)) 147. Provide reports customized for a type of user (e.g., top prescribers, trend analysis, hot spots) 148. Provide peer comparison reports (e.g., prescribing rates by specialty) 149. Produce a PDMP Annual Report 150. Other type of available report (Describe the report) 151. PDMP Data Requestors (indicate if PDMP has authority to release data and/or engaged in releasing data; whether solicited/unsolicited; in-state/out of state) 152. # of Prescribers Enrolled in PDMP by License Type (e.g., physicians, dentists, veterinarians, podiatrists, osteopaths) 153. # of Dispensers Enrolled in PDMP by License Type (e.g., In-state pharmacy, Mail order pharmacy, dispensing physician) 154. # of Prescribers Enrolled in PDMP by Specialty (e.g., oncology, pediatrics, family medicine, radiology, anesthesiology) 16
17 2016 State Assessment (cont d) 155. # of Unique Prescribers (Number of different prescribers who have issued prescriptions) 156. # of In-State Queries (Number of queries requesting data from home PDMP) 157. # of In-State Queries by Requestor Type (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 158. # of Interstate Queries (Number of queries requesting data from another state's PDMP) 159. # of Interstate Queries by Requestor Type (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 160. # of Positive Matches from Interstate Queries (Number of queries where patient data is found in another state's PDMP) 161. # of Data Errors by Error Type (e.g., missing information, invalid dates, incorrect DEA or NDC) 162. # of Data Errors Corrected 163. # of At-Risk Patients by Risk Factor (e.g., morphine milligram equivalents, multiple provider episodes, overlapping prescriptions) 164. Risk Factor Statistics by Time Frame (e.g., average MMEs, average day's supply for opioids) 165. # of Prescriptions Filled by Controlled Substance Schedule 166. # of Prescriptions Filled by Drug Class (e.g., stimulants, narcotics, sedatives, tranquilizers) 167. # of Dosage Units Dispensed by Controlled Substance Schedule 168. # of Dosage Units Dispensed by Drug Class (e.g., stimulants, narcotics, sedatives, tranquilizers) 169. # of Solicited Prescriber Reports by Requestor Type (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 170. # of Unsolicited Prescriber Reports by Recipient Type (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 171. # of Solicited Dispenser Reports by Requestor Type (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 172. # of Unsolicited Dispenser Reports by Recipient Type (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 173. # of Solicited Patient Reports by Requestor Type (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 174. # of Unsolicited Patient Reports by Recipient Type (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 175. # of Solicited Statistical Reports by Requestor Type (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 176. # of Unsolicited Statistical Reports by Recipient Type (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 177. # of Unique Requestors by Requestor Type (solicited reports) (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 178. # of Unique Recipients by Recipient Type (unsolicited reports) (e.g., prescriber, dispenser, law enforcement, licensing/regulatory board) 179. Are PDMP Statistics Available On-Line 180. If yes, provide website link 181. Statistical Report Generation (How are statistical reports generated (e.g., in-house, vendor)?) 182. # of Employees - Operational Staff (Indicate the number of agency full-time equivalents (FTEs) directly involved with operating the PDMP.) 183. # of Employees - Technical Staff (Indicate the number of agency full-time equivalents (FTEs) directly involved with technical development of the PDMP.) 184. # of Employees - Analytical (Indicate the number of agency full-time equivalents (FTEs) directly involved with the PDMP's analytical or epidemiological activities.) 17
18 2016 State Assessment (cont d) 185. # of Employees - Other (Indicate the number of agency full-time equivalents (FTEs) directly involved with the PDMP and not captured in lines 2-4.) 186. Other' Description (If there are 'other' employees, please briefly describe the position.) 187. State General Fund 188. Licensing Fees 189. Controlled Substance Registration Fees 190. Regulatory Board Fund 191. BJA Harold Rogers Grant 192. SAMHSA Grant 193. CDC Grant 194. Agreed Settlement 195. Other 196. PDMP engaged in supporting or conducting any studies of PDMP effectiveness 197. If yes, provide URL to the study (if available) 198. PDMP engaged in supporting or conducting analyses of PDMP data for surveillance, early warning, evaluation, prevention 199. PDMP engaged in supporting or conducting analyses of health outcome data to measure impact of PDMP or prescription policy changes (Outcome data such as overdoses, deaths, hospitalizations, ER visits, etc.) 200. PDMP engaged in supporting or conducting audits for utilization compliance (Checks to ensure PDMP data is accessed and used appropriately) 201. PDMP engaged in supporting or conducting audits for data reporting compliance (Checks to ensure required data transmitters are reporting appropriately) 202. PDMP engaged in or supporting data correction (Processes in place to identify and remedy data errors) 203. PDMP engaged in supporting or conducting satisfaction and utilization surveys of users 204. PDMP engaged in supporting or conducting outreach to users upon obtaining license or license renewal (PDMP and enrollment information provided to potential users when they apply or renew a license ) 205. PDMP engaged in or supporting promotional methods to increase PDMP utilization and funding (e.g., presentations, newsletters, brochures) 206. List the agencies with whom you are collaborating on any of the above (e.g., health department, Medicaid, substance abuse) 18
19 19
20 20
Alaska. Contact Information. State Registrant Totals and Population. PDMP name: AKPDMP
 Statistics website: Carrillo, Laura - PDMP Manager 550 W. 7th Ave, Ste 1500 Anchorage AK 99501 Office: (907) 269-8404 Fax: (907) 465-2974 Email: laura.carrillo@alaska.gov Alaska PDMP name: AKPDMP PDMP
Statistics website: Carrillo, Laura - PDMP Manager 550 W. 7th Ave, Ste 1500 Anchorage AK 99501 Office: (907) 269-8404 Fax: (907) 465-2974 Email: laura.carrillo@alaska.gov Alaska PDMP name: AKPDMP PDMP
New Mexico. Contact Information. State Registrant Totals and Population. PDMP name: NM PMP
 Statistics website: Ryba, Peter, PharmD - PMP Director 5500 San Antonio Drive NE, Suite C Albuquerque NM 87109 Office: (505) 222-9818 Fax: (505) 222-9845 Email: peter.ryba@state.nm.us New Mexico PDMP name:
Statistics website: Ryba, Peter, PharmD - PMP Director 5500 San Antonio Drive NE, Suite C Albuquerque NM 87109 Office: (505) 222-9818 Fax: (505) 222-9845 Email: peter.ryba@state.nm.us New Mexico PDMP name:
Nevada. Contact Information. State Registrant Totals and Population
 Statistics website: Long, Yenh - Program Administrator 431 W Plumb Ln Reno NV 89509 Office: (775) 687-5694 Fax: (775) 687-5161 Email: ylong@pharmacy.nv.gov Nevada PDMP name: Prescription Controlled Substance
Statistics website: Long, Yenh - Program Administrator 431 W Plumb Ln Reno NV 89509 Office: (775) 687-5694 Fax: (775) 687-5161 Email: ylong@pharmacy.nv.gov Nevada PDMP name: Prescription Controlled Substance
Colorado. Contact Information
 Colorado PDMP name: Prescription Drug Monitoring Program PDMP region: Agency responsible: Colorado State Board of Pharmacy Agency type: Pharmacy Board PDMP email: pdmpinqr@state.co.us PDMP website: https://www.colorado.gov/pacific/dora/pdmp
Colorado PDMP name: Prescription Drug Monitoring Program PDMP region: Agency responsible: Colorado State Board of Pharmacy Agency type: Pharmacy Board PDMP email: pdmpinqr@state.co.us PDMP website: https://www.colorado.gov/pacific/dora/pdmp
North Carolina. Contact Information. State Registrant Totals and Population. PDMP region: PDMP name: Agency responsible:
 PDMP name: Agency responsible: Agency type: PDMP email: PDMP website: Enrollment website: Query website: Data upload website: Statistics website: North Carolina PDMP region: South North Carolina Department
PDMP name: Agency responsible: Agency type: PDMP email: PDMP website: Enrollment website: Query website: Data upload website: Statistics website: North Carolina PDMP region: South North Carolina Department
Tennessee. Contact Information. State Registrant Totals and Population. PDMP name: CSMD
 Statistics website: Bess, D. Todd - Director, CSMD Program 665 Mainstream Drive Nashville TN 37243 Office: (615) 253-1305 Fax: Email: david.bess@tn.gov Tennessee PDMP name: CSMD PDMP region: South Agency
Statistics website: Bess, D. Todd - Director, CSMD Program 665 Mainstream Drive Nashville TN 37243 Office: (615) 253-1305 Fax: Email: david.bess@tn.gov Tennessee PDMP name: CSMD PDMP region: South Agency
Michigan. Contact Information. State Registrant Totals and Population. PDMP name: MAPS
 Michigan PDMP name: MAPS PDMP region: Agency responsible: Bureau of Professional Licensing, Drug Monitoring Section Agency type: Professional Licensing Agency PDMP email: BPL-MAPS@michigan.gov PDMP website:
Michigan PDMP name: MAPS PDMP region: Agency responsible: Bureau of Professional Licensing, Drug Monitoring Section Agency type: Professional Licensing Agency PDMP email: BPL-MAPS@michigan.gov PDMP website:
Kentucky. Kentucky Cabinet for Health and Family Services Office of Inspector General
 PDMP name: Agency responsible: Agency type: PDMP email: PDMP website: Enrollment website: Query website: Data upload website: Statistics website: Kentucky Kentucky Cabinet for Health and Family Services
PDMP name: Agency responsible: Agency type: PDMP email: PDMP website: Enrollment website: Query website: Data upload website: Statistics website: Kentucky Kentucky Cabinet for Health and Family Services
Mississippi. Contact Information. State Registrant Totals and Population
 Statistics website: Mueller, Stephanie - PMP Director 6360 I-55 North, Suite 400 Jackson, MS 39211 Office: (601) 899-0138 Fax: (601) 899-8904 Email: smueller@mbp.ms.gov Mississippi PDMP name: MS PMP Agency
Statistics website: Mueller, Stephanie - PMP Director 6360 I-55 North, Suite 400 Jackson, MS 39211 Office: (601) 899-0138 Fax: (601) 899-8904 Email: smueller@mbp.ms.gov Mississippi PDMP name: MS PMP Agency
Massachusetts. Contact Information. State Registrant Totals and Population. PDMP name: MA Prescription Monitoring Program
 Massachusetts PDMP name: MA Prescription Monitoring Program PDMP region: Agency responsible: Department of Public Health Agency type: Department of Health PDMP email: mapmp.dph@massmail.state.ma.us PDMP
Massachusetts PDMP name: MA Prescription Monitoring Program PDMP region: Agency responsible: Department of Public Health Agency type: Department of Health PDMP email: mapmp.dph@massmail.state.ma.us PDMP
Puerto Rico. Contact Information. State Registrant Totals and Population. PDMP name: PR PDMP
 Statistics website: Rodriguez, Cieni - Program Manager Carr. No. 2 Km 8.2, Bo. Juan Sanchez Bayamon, PR 00960 Office: (787) 763-7575 Fax: (787) 763-3152 Email: cieni.rodriguez@assmca.pr.gov Puerto Rico
Statistics website: Rodriguez, Cieni - Program Manager Carr. No. 2 Km 8.2, Bo. Juan Sanchez Bayamon, PR 00960 Office: (787) 763-7575 Fax: (787) 763-3152 Email: cieni.rodriguez@assmca.pr.gov Puerto Rico
Ohio. Contact Information. State Registrant Totals and Population
 PDMP name: OARRS Agency responsible: State of Ohio Board of Pharmacy Agency type: Pharmacy Board PDMP email: info@pharmacy.ohio.gov PDMP website: www.ohiopmp.gov Enrollment website: https://ohio.pmpaware.net
PDMP name: OARRS Agency responsible: State of Ohio Board of Pharmacy Agency type: Pharmacy Board PDMP email: info@pharmacy.ohio.gov PDMP website: www.ohiopmp.gov Enrollment website: https://ohio.pmpaware.net
Oklahoma. Contact Information. Office: Fax: Statistics
 PDMP name: Agency Responsible: Agency Type: PDMP Website: PDMP Email: Vogt, Don - PMP Program Manager 419 NE 38th Terrace Oklahoma City OK 73105 Office: (405) 530-3140 Fax: (405) 524-7619 Email: dvogt@obn.state.ok.us
PDMP name: Agency Responsible: Agency Type: PDMP Website: PDMP Email: Vogt, Don - PMP Program Manager 419 NE 38th Terrace Oklahoma City OK 73105 Office: (405) 530-3140 Fax: (405) 524-7619 Email: dvogt@obn.state.ok.us
Tennessee. Tennessee Department of Health, Tennessee Board of Pharmacy Pharmacy Board
 PDMP name: Agency Responsible: Agency Type: PDMP Website: PDMP Email: Tennessee Tennessee Department of Health, Tennessee Board of Pharmacy Pharmacy Board http://tn.gov/health/topic/csmd-board csmd.admin@tn.gov
PDMP name: Agency Responsible: Agency Type: PDMP Website: PDMP Email: Tennessee Tennessee Department of Health, Tennessee Board of Pharmacy Pharmacy Board http://tn.gov/health/topic/csmd-board csmd.admin@tn.gov
STATE OF TEXAS TEXAS STATE BOARD OF PHARMACY
 STATE OF TEXAS TEXAS STATE BOARD OF PHARMACY REQUEST FOR INFORMATION NO. 515-15-0002 PRESCRIPTION DRUG MONITORING PROGRAM Reference: CLASS: 920 ITEM: 05 Posting Date: 12/08/2014 RESPONSE DEADLINE: 01/05/2015
STATE OF TEXAS TEXAS STATE BOARD OF PHARMACY REQUEST FOR INFORMATION NO. 515-15-0002 PRESCRIPTION DRUG MONITORING PROGRAM Reference: CLASS: 920 ITEM: 05 Posting Date: 12/08/2014 RESPONSE DEADLINE: 01/05/2015
Prescription Drug Monitoring Program (PDMP)
") Prescription Drug Monitoring Program (PDMP) New York State Information contained in this presentation is accurate as of September 2017 Meet the Speaker Anita Murray, R.Ph., Deputy Director Bureau of Narcotic
Prescription Drug Monitoring Program (PDMP) New York State Information contained in this presentation is accurate as of September 2017 Meet the Speaker Anita Murray, R.Ph., Deputy Director Bureau of Narcotic
Prescription Monitoring Program State Profiles - Michigan
 Prescription Monitoring Program State Profiles - Michigan Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
Prescription Monitoring Program State Profiles - Michigan Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
Prescription Drug Monitoring Program (PDMP)
") Prescription Drug Monitoring Program (PDMP) West Virginia Information contained in this presentation is accurate as of October 2017 What is a Prescription Drug Monitoring Program? A PDMP/PMP is a statewide
Prescription Drug Monitoring Program (PDMP) West Virginia Information contained in this presentation is accurate as of October 2017 What is a Prescription Drug Monitoring Program? A PDMP/PMP is a statewide
Evidence-Based Practices to Optimize Prescriber Use of PDMPs
 Evidence-Based Practices to Optimize Prescriber Use of PDMPs Sheri Lawal, MPH, CHES Senior Associate, Substance Use Prevention and Treatment Initiative, The Pew Charitable Trusts Thomas Clark Research
Evidence-Based Practices to Optimize Prescriber Use of PDMPs Sheri Lawal, MPH, CHES Senior Associate, Substance Use Prevention and Treatment Initiative, The Pew Charitable Trusts Thomas Clark Research
OREGON HEALTH AUTHORITY, DIVISION OF MEDICAL ASSISTANCE PROGRAMS
 OREGON HEALTH AUTHORITY, DIVISION OF MEDICAL ASSISTANCE PROGRAMS DIVISION 121 PHARMACEUTICAL SERVICES Non-Medicaid Rules Prescription Drug Monitoring Program 410-121-4000 Purpose The purpose of the Prescription
OREGON HEALTH AUTHORITY, DIVISION OF MEDICAL ASSISTANCE PROGRAMS DIVISION 121 PHARMACEUTICAL SERVICES Non-Medicaid Rules Prescription Drug Monitoring Program 410-121-4000 Purpose The purpose of the Prescription
Steps Taken to Combat the Opiate Epidemic Through Legal And Technological Channels. Nick Snyder, Esq.
 Steps Taken to Combat the Opiate Epidemic Through Legal And Technological Channels Nick Snyder, Esq. How Can We Impact Inappropriate Over-Prescribing of Opioids in Maine? What have other States or Organizations
Steps Taken to Combat the Opiate Epidemic Through Legal And Technological Channels Nick Snyder, Esq. How Can We Impact Inappropriate Over-Prescribing of Opioids in Maine? What have other States or Organizations
Prescription Monitoring Program State Profiles - Illinois
 Prescription Monitoring Program State Profiles - Illinois Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
Prescription Monitoring Program State Profiles - Illinois Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
District of Columbia Prescription Drug Monitoring Program
 District of Columbia Prescription Drug Monitoring Program What Our Users Need to Know Health Regulation and Licensing Administration Pharmaceutical Control Division February 28, 2017 1 Mission Statement
District of Columbia Prescription Drug Monitoring Program What Our Users Need to Know Health Regulation and Licensing Administration Pharmaceutical Control Division February 28, 2017 1 Mission Statement
Prescription Monitoring Program State Profiles - California
 Prescription Monitoring Program State Profiles - California Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control
Prescription Monitoring Program State Profiles - California Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control
NATIONAL ASSOCIATION FOR STATE CONTROLLED SUBSTANCES AUTHORITIES (NASCSA) MODEL PRESCRIPTION MONITORING PROGRAM (PMP) ACT (2016) COMMENT
 MODEL PRESCRIPTION MONITORING PROGRAM (PMP) ACT (2016) COMMENT") 1 NATIONAL ASSOCIATION FOR STATE CONTROLLED SUBSTANCES AUTHORITIES (NASCSA) MODEL PRESCRIPTION MONITORING PROGRAM (PMP) ACT (2016) SECTION 1. SHORT TITLE. This Act shall be known and may be cited as the
1 NATIONAL ASSOCIATION FOR STATE CONTROLLED SUBSTANCES AUTHORITIES (NASCSA) MODEL PRESCRIPTION MONITORING PROGRAM (PMP) ACT (2016) SECTION 1. SHORT TITLE. This Act shall be known and may be cited as the
Prescription Monitoring Programs - Legislative Trends and Model Law Revision
 Prescription Drug Monitoring Programs Training and Technical Assistance Center Webinar Series National Alliance for Model State Drug Laws: Legislative Round-Up July 22, 2015 Prescription Monitoring Programs
Prescription Drug Monitoring Programs Training and Technical Assistance Center Webinar Series National Alliance for Model State Drug Laws: Legislative Round-Up July 22, 2015 Prescription Monitoring Programs
NCPDP s Recommendations for an Integrated, Interoperable Solution to Ensure Patient Safe Use of Controlled Substances
 National Council for Prescription Drug Programs White Paper NCPDP s Recommendations for an Integrated, Interoperable Solution to Ensure Patient Safe Use of This white paper details a plan to nationally
National Council for Prescription Drug Programs White Paper NCPDP s Recommendations for an Integrated, Interoperable Solution to Ensure Patient Safe Use of This white paper details a plan to nationally
PRESCRIPTION MONITORING PROGRAM STATE PROFILES TENNESSEE
 PRESCRIPTION MONITORING PROGRAM STATE PROFILES TENNESSEE Research current through July 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
PRESCRIPTION MONITORING PROGRAM STATE PROFILES TENNESSEE Research current through July 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
Interim Commissioner Lauren A. Smith and Members of the Public Health Council
 DEVAL L. PATRICK GOVERNOR TIMOTHY P. MURRAY LIEUTENANT GOVERNOR JOHN W. POLANOWICZ SECRETARY LAUREN A. SMITH, MD, MPH INTERIM COMMISSIONER The Commonwealth of Massachusetts Executive Office of Health and
DEVAL L. PATRICK GOVERNOR TIMOTHY P. MURRAY LIEUTENANT GOVERNOR JOHN W. POLANOWICZ SECRETARY LAUREN A. SMITH, MD, MPH INTERIM COMMISSIONER The Commonwealth of Massachusetts Executive Office of Health and
Prescription Drug Monitoring Programs: Promising Practices to Maximize Their Effectiveness
 Prescription Drug Monitoring Programs: Promising Practices to Maximize Their Effectiveness Peter Kreiner, Ph.D. Prescription Monitoring Program Center of Excellence at Brandeis University NGA Meeting September
Prescription Drug Monitoring Programs: Promising Practices to Maximize Their Effectiveness Peter Kreiner, Ph.D. Prescription Monitoring Program Center of Excellence at Brandeis University NGA Meeting September
Prescription Monitoring Program State Profiles - Texas
 Prescription Monitoring Program State Profiles - Texas Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
Prescription Monitoring Program State Profiles - Texas Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
2017 ASAP MIDYEAR CONFERENCE THE FUTURE OF PRESCRIPTION DRUG MONITORING PROGRAMS (PMPS): HIGHLIGHTS OF 2017 STATE BILLS JUNE 22, 2017 SHERRY L.
: HIGHLIGHTS OF 2017 STATE BILLS JUNE 22, 2017 SHERRY L.") 2017 ASAP MIDYEAR CONFERENCE THE FUTURE OF PRESCRIPTION DRUG MONITORING PROGRAMS (PMPS): HIGHLIGHTS OF 2017 STATE BILLS JUNE 22, 2017 SHERRY L. GREEN Disclosures Sherry Green is an employee of Na2onal
2017 ASAP MIDYEAR CONFERENCE THE FUTURE OF PRESCRIPTION DRUG MONITORING PROGRAMS (PMPS): HIGHLIGHTS OF 2017 STATE BILLS JUNE 22, 2017 SHERRY L. GREEN Disclosures Sherry Green is an employee of Na2onal
Prescription Drug Monitoring Program (PDMP)
") Prescription Drug Monitoring Program (PDMP) New Jersey Information contained in this presentation is accurate as of September 2017 Meet the Speaker Sindy Paul, MD, MPH, FACPM Medical Director - NJ Board
Prescription Drug Monitoring Program (PDMP) New Jersey Information contained in this presentation is accurate as of September 2017 Meet the Speaker Sindy Paul, MD, MPH, FACPM Medical Director - NJ Board
BJA COAP Category 5 Grantee Webinar Thursday, June 21, 2018
 BJA COAP Category 5 Grantee Webinar Thursday, June 21, 2018 BJA Update Tara Kunkel Senior Drug Policy Advisor IPA Bureau of Justice Assistance U.S. Department of Justice BJA Grant Project Update: Washington
BJA COAP Category 5 Grantee Webinar Thursday, June 21, 2018 BJA Update Tara Kunkel Senior Drug Policy Advisor IPA Bureau of Justice Assistance U.S. Department of Justice BJA Grant Project Update: Washington
Georgia DPH. Prescription Title Drug Heading Monitoring Program Program. Sheila Pierce April 2018
 Georgia DPH Prescription Title Drug Heading Monitoring Program Program Sheila Pierce April 2018 What is the PDMP? Legislative Mandates Registration Requirements How to use the PDMP Next Steps for Prescribers
Georgia DPH Prescription Title Drug Heading Monitoring Program Program Sheila Pierce April 2018 What is the PDMP? Legislative Mandates Registration Requirements How to use the PDMP Next Steps for Prescribers
Technical Assistance Guide. Prescriber Report Cards
 Technical Assistance Guide Prescriber Report Cards Revised February 17, 2017 This project was supported by Grant No. 2014-PM-BX-K001 awarded by the Bureau of Justice Assistance. The Bureau of Justice Assistance
Technical Assistance Guide Prescriber Report Cards Revised February 17, 2017 This project was supported by Grant No. 2014-PM-BX-K001 awarded by the Bureau of Justice Assistance. The Bureau of Justice Assistance
EPCS FREQUENTLY ASKED QUESTIONS FOR ELECTRONIC PRESCRIBING OF CONTROLLED SUBSTANCES. Revised: March 2016
 FREQUENTLY ASKED QUESTIONS FOR ELECTRONIC PRESCRIBING OF CONTROLLED SUBSTANCES EPCS Revised: March 2016 NEW YORK STATE DEPARTMENT OF HEALTH Bureau of Narcotic Enforcement 1-866-811-7957 www.health.ny.gov/professionals/narcotic
FREQUENTLY ASKED QUESTIONS FOR ELECTRONIC PRESCRIBING OF CONTROLLED SUBSTANCES EPCS Revised: March 2016 NEW YORK STATE DEPARTMENT OF HEALTH Bureau of Narcotic Enforcement 1-866-811-7957 www.health.ny.gov/professionals/narcotic
NEW MEXICO PRACTITIONER S MANUAL
 NEW MEXICO PRACTITIONER S MANUAL An Informational Outline From the New Mexico Board of Pharmacy 5200 Oakland NE Suite A Albuquerque, New Mexico 87113 505-222-9830 800-565-9102 E-Mail: Debra.wilhite@state.nm.us
NEW MEXICO PRACTITIONER S MANUAL An Informational Outline From the New Mexico Board of Pharmacy 5200 Oakland NE Suite A Albuquerque, New Mexico 87113 505-222-9830 800-565-9102 E-Mail: Debra.wilhite@state.nm.us
Bold blue=new language Red strikethrough=deleted language Regular text=existing language Bold Green = new changes following public hearing
 Bold blue=new language Red strikethrough=deleted language Regular text=existing language Bold Green = new changes following public hearing 700.001: Definitions Delegate means an authorized support staff
Bold blue=new language Red strikethrough=deleted language Regular text=existing language Bold Green = new changes following public hearing 700.001: Definitions Delegate means an authorized support staff
Annual Report to the Prescription Drug Monitoring Program Advisory Commission
 2015 Annual Report to the Prescription Drug Monitoring Program Advisory Commission PUBLIC HEALTH DIVISION Oregon Violent Death Reporting System Contents»» Acknowledgments... 1»» Executive summary... 2
2015 Annual Report to the Prescription Drug Monitoring Program Advisory Commission PUBLIC HEALTH DIVISION Oregon Violent Death Reporting System Contents»» Acknowledgments... 1»» Executive summary... 2
Massachusetts Prescription Monitoring Program
 Massachusetts Prescription Monitoring Program PDMP Training and Technical Assistance Center at Brandeis University in partnership with the Bureau of Justice Assistance August 8, 2012 Massachusetts Department
Massachusetts Prescription Monitoring Program PDMP Training and Technical Assistance Center at Brandeis University in partnership with the Bureau of Justice Assistance August 8, 2012 Massachusetts Department
K-TRACS: Review of Program Data and a Qualitative Assessment Study
 K-TRACS: Review of Program Data and a Qualitative Assessment Study Amy Curry, MD Clinical Assistant Professor University of Kansas School of Medicine - Wichita Department of Family and Community Medicine
K-TRACS: Review of Program Data and a Qualitative Assessment Study Amy Curry, MD Clinical Assistant Professor University of Kansas School of Medicine - Wichita Department of Family and Community Medicine
Report of the Task Force on Prescription Monitoring Program Standards
 Report of the Task Force on Prescription Monitoring Program Standards Members Present: Gay Dodson (TX), chairperson; John Dorvee (ME); Danna Droz (OH); Allen F. Dulwick (OR); William Fitzpatrick (MO);
Report of the Task Force on Prescription Monitoring Program Standards Members Present: Gay Dodson (TX), chairperson; John Dorvee (ME); Danna Droz (OH); Allen F. Dulwick (OR); William Fitzpatrick (MO);
GENERAL ASSEMBLY OF NORTH CAROLINA SESSION 2017 S 2 SENATE BILL 750* Health Care Committee Substitute Adopted 6/12/18
 GENERAL ASSEMBLY OF NORTH CAROLINA SESSION 0 S SENATE BILL 0* Health Care Committee Substitute Adopted /1/ Short Title: Health-Local Confinement/Vet. Controlled Sub. (Public) Sponsors: Referred to: May,
GENERAL ASSEMBLY OF NORTH CAROLINA SESSION 0 S SENATE BILL 0* Health Care Committee Substitute Adopted /1/ Short Title: Health-Local Confinement/Vet. Controlled Sub. (Public) Sponsors: Referred to: May,
Prescription Drug Monitoring Program (PDMP) LOUISIANA. Information contained in this presentation is accurate as of September 2017
 LOUISIANA. Information contained in this presentation is accurate as of September 2017") Prescription Drug Monitoring Program (PDMP) LOUISIANA Information contained in this presentation is accurate as of September 2017 Meet the Speaker Julie W. Breithaupt PharmD, MBA President Louisiana Pharmacists
Prescription Drug Monitoring Program (PDMP) LOUISIANA Information contained in this presentation is accurate as of September 2017 Meet the Speaker Julie W. Breithaupt PharmD, MBA President Louisiana Pharmacists
10/4/12. Controlled Substances Dispensing Issues and Solutions. Objectives. Financial Disclosure
 Controlled Substances Dispensing Issues and Solutions Ronald W. Buzzeo, R.Ph. Chief Compliance Officer November 7, 2012 CE Code: Financial Disclosure I have no actual or potentially relevant financial
Controlled Substances Dispensing Issues and Solutions Ronald W. Buzzeo, R.Ph. Chief Compliance Officer November 7, 2012 CE Code: Financial Disclosure I have no actual or potentially relevant financial
during the EHR reporting period.
 CMS Stage 2 MU Proposed Objectives and Measures for EPs Objective Measure Notes and Queries PUT YOUR COMMENTS HERE CORE SET (EP must meet all 17 Core Set objectives) Exclusion: Any EP who writes fewer
CMS Stage 2 MU Proposed Objectives and Measures for EPs Objective Measure Notes and Queries PUT YOUR COMMENTS HERE CORE SET (EP must meet all 17 Core Set objectives) Exclusion: Any EP who writes fewer
Frequently Asked Questions MN Prescription Monitoring Program (PMP)
") Frequently Asked Questions MN Prescription Monitoring Program (PMP) Topics: 1. Purpose of the PMP 2. Reporting/Frequency of Reporting 3. Dispensing for Animals 4. Inappropriate Prescribing 5. Accessing
Frequently Asked Questions MN Prescription Monitoring Program (PMP) Topics: 1. Purpose of the PMP 2. Reporting/Frequency of Reporting 3. Dispensing for Animals 4. Inappropriate Prescribing 5. Accessing
Prescription Monitoring Program State Profiles - Kentucky
 Prescription Monitoring Program State Profiles - Kentucky Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
Prescription Monitoring Program State Profiles - Kentucky Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
E Prescribing E Rx: Background. E Rx: Definition. Rebecca H. Wartman, O.D.
 E Prescribing 2011 E Rx 2011 is presented by Rebecca H. Wartman, O.D. Practice Advancement Committee Member, Clinical and Practice Advancement Group American Optometric Association E Rx: Background Electronic
E Prescribing 2011 E Rx 2011 is presented by Rebecca H. Wartman, O.D. Practice Advancement Committee Member, Clinical and Practice Advancement Group American Optometric Association E Rx: Background Electronic
Prescription Monitoring Program State Profiles - Pennsylvania
 Prescription Monitoring Program State Profiles - Pennsylvania Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control
Prescription Monitoring Program State Profiles - Pennsylvania Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control
SENATE, No STATE OF NEW JERSEY. 216th LEGISLATURE INTRODUCED APRIL 28, 2014
 SENATE, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED APRIL, 0 Sponsored by: Senator LORETTA WEINBERG District (Bergen) Senator JOSEPH F. VITALE District (Middlesex) Senator JAMES W. HOLZAPFEL District
SENATE, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED APRIL, 0 Sponsored by: Senator LORETTA WEINBERG District (Bergen) Senator JOSEPH F. VITALE District (Middlesex) Senator JAMES W. HOLZAPFEL District
MINNESOTA BOARD OF PHARMACY
 MINNESOTA BOARD OF PHARMACY Prescription Drug Waste Reduction Report. (In compliance with Minnesota Session Laws, 2010 First Special Session, Chapter 1, section 21) Cody Wiberg, Pharm.D., M.S., R.Ph. Executive
MINNESOTA BOARD OF PHARMACY Prescription Drug Waste Reduction Report. (In compliance with Minnesota Session Laws, 2010 First Special Session, Chapter 1, section 21) Cody Wiberg, Pharm.D., M.S., R.Ph. Executive
Medication Assisted Treatment for Opioid Use Disorders Reporting Requirements
 This document is scheduled to be published in the Federal Register on 09/27/2016 and available online at https://federalregister.gov/d/2016-23277, and on FDsys.gov DEPARTMENT OF HEALTH AND HUMAN SERVICES
This document is scheduled to be published in the Federal Register on 09/27/2016 and available online at https://federalregister.gov/d/2016-23277, and on FDsys.gov DEPARTMENT OF HEALTH AND HUMAN SERVICES
Notice of Privacy Practices
 River Valley Chiropractic LLC Notice of Privacy Practices Effective 9/2014; Revised 9/2014 If you have any questions about this notice, please contact the River Valley Chiropractic Privacy Officer at 308-534-5840.
River Valley Chiropractic LLC Notice of Privacy Practices Effective 9/2014; Revised 9/2014 If you have any questions about this notice, please contact the River Valley Chiropractic Privacy Officer at 308-534-5840.
Policies Approved by the 2017 ASHP House of Delegates
 House of Delegates Policies Approved by the 2017 ASHP House of Delegates 1701 Ensuring Patient Safety and Data Integrity During Cyber-attacks Source: Council on Pharmacy Management To advocate that healthcare
House of Delegates Policies Approved by the 2017 ASHP House of Delegates 1701 Ensuring Patient Safety and Data Integrity During Cyber-attacks Source: Council on Pharmacy Management To advocate that healthcare
Alabama. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Alabama Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Prescribing and Dispensing Profile Alabama Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
CHI Mercy Health. Definitions
 CHI Mercy Health Definitions If you have any questions about this notice, please contact the CHI Mercy Health s Privacy Office at (701) 845-6540 or 570 Chautauqua Blvd, Valley City ND 58072. Notice of
CHI Mercy Health Definitions If you have any questions about this notice, please contact the CHI Mercy Health s Privacy Office at (701) 845-6540 or 570 Chautauqua Blvd, Valley City ND 58072. Notice of
eprescribing Information to Improve Medication Adherence
 eprescribing Information to Improve Medication Adherence April 2017 (revised) About Point-of-Care Partners Executive Summary Point-of-Care Partners (POCP) is a leading management consulting firm assisting
eprescribing Information to Improve Medication Adherence April 2017 (revised) About Point-of-Care Partners Executive Summary Point-of-Care Partners (POCP) is a leading management consulting firm assisting
2015 Complete Overview of the NCQA Standards Session Code: TU13 Time: 2:30 p.m. 4:00 p.m. Total CE Credits: 1.5 Presenter: Frank Stelling, MEd, MPH
 2015 Complete Overview of the NCQA Standards Session Code: TU13 Time: 2:30 p.m. 4:00 p.m. Total CE Credits: 1.5 Presenter: Frank Stelling, MEd, MPH Introduction to NCQA Credentialing Standards NAMSS Educational
2015 Complete Overview of the NCQA Standards Session Code: TU13 Time: 2:30 p.m. 4:00 p.m. Total CE Credits: 1.5 Presenter: Frank Stelling, MEd, MPH Introduction to NCQA Credentialing Standards NAMSS Educational
The Wisconsin epdmp:
 The Wisconsin epdmp: Frequently Asked Questions Pursuant to 2015 Wisconsin Act 266, effective April 1, 2017, Wisconsin-licensed physicians and other prescribers must review a patient s records from Wisconsin
The Wisconsin epdmp: Frequently Asked Questions Pursuant to 2015 Wisconsin Act 266, effective April 1, 2017, Wisconsin-licensed physicians and other prescribers must review a patient s records from Wisconsin
PRESCRIPTION MONITORING PROGRAM STATE PROFILES MASSACHUSETTS
 PRESCRIPTION MONITORING PROGRAM STATE PROFILES MASSACHUSETTS Research current through July 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
PRESCRIPTION MONITORING PROGRAM STATE PROFILES MASSACHUSETTS Research current through July 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office of National Drug Control Policy.
-Health Update. Encounter Notification System (ENS) Celebrates Five Years! Welcome
 Celebrates Five Years! Welcome") www.crisphealth.org e -Health Update ISSUE 8 Summer 2017 Welcome The e-health Update is a resource that shares current CRISP initiatives as well as pertinent health care related information for our region.
www.crisphealth.org e -Health Update ISSUE 8 Summer 2017 Welcome The e-health Update is a resource that shares current CRISP initiatives as well as pertinent health care related information for our region.
PRIVACY POLICY USES AND DISCLOSURES FOR TREATMENT, PAYMENT, AND HEALTH CARE OPERATIONS
 PRIVACY POLICY As of April 14, 2003, the Federal regulation on patient information privacy, known as the Health Insurance Portability and Accountability Act (HIPAA), requires that we provide (in writing)
PRIVACY POLICY As of April 14, 2003, the Federal regulation on patient information privacy, known as the Health Insurance Portability and Accountability Act (HIPAA), requires that we provide (in writing)
Medicare Advantage and Part D Fraud, Waste and Abuse Compliance Training 2015
 Medicare Advantage and Part D Fraud, Waste and Abuse Compliance Training 2015 Overview This Medicare Advantage and Part D Fraud, Waste and Abuse Compliance Training for first-tier, downstream and related
Medicare Advantage and Part D Fraud, Waste and Abuse Compliance Training 2015 Overview This Medicare Advantage and Part D Fraud, Waste and Abuse Compliance Training for first-tier, downstream and related
Issue Brief. E-Prescribing in California: Why Aren t We There Yet? Introduction. Current Status of E-Prescribing in California
 E-Prescribing in California: Why Aren t We There Yet? Introduction Electronic prescribing (e-prescribing) refers to the computer-based generation of a prescription, electronic transmission of the initial
E-Prescribing in California: Why Aren t We There Yet? Introduction Electronic prescribing (e-prescribing) refers to the computer-based generation of a prescription, electronic transmission of the initial
a remote pharmacy is not necessarily intended to provide permanent??? how do we make it so that it may be only for limited duration.
 Board of Pharmacy Administrative Rules Version 12 January 18, 2013 Part 19 Remote Pharmacies 19.1 General Purpose: (a) This Part is enacted pursuant to 26 V.S.A. 2032 which initially authorized the Board
Board of Pharmacy Administrative Rules Version 12 January 18, 2013 Part 19 Remote Pharmacies 19.1 General Purpose: (a) This Part is enacted pursuant to 26 V.S.A. 2032 which initially authorized the Board
HIE Implications in Meaningful Use Stage 1 Requirements
 s in Meaningful Use Stage 1 Requirements HIMSS Health Information Exchange Steering Committee March 2010 2010 Healthcare Information and Management Systems Society (HIMSS). 1 An HIE Overview Health Information
s in Meaningful Use Stage 1 Requirements HIMSS Health Information Exchange Steering Committee March 2010 2010 Healthcare Information and Management Systems Society (HIMSS). 1 An HIE Overview Health Information
247 CMR: BOARD OF REGISTRATION IN PHARMACY
 247 CMR 9.00: CODE OF PROFESSIONAL CONDUCT; PROFESSIONAL STANDARDS FOR REGISTERED PHARMACISTS, PHARMACIES AND PHARMACY DEPART- MENTS Section 9.01: Code of Professional Conduct for Registered Pharmacists,
247 CMR 9.00: CODE OF PROFESSIONAL CONDUCT; PROFESSIONAL STANDARDS FOR REGISTERED PHARMACISTS, PHARMACIES AND PHARMACY DEPART- MENTS Section 9.01: Code of Professional Conduct for Registered Pharmacists,
Patient Safety. Road Map to Controlled Substance Diversion Prevention
 Patient Safety Road Map to Controlled Substance Diversion Prevention Road Map to Diversion Prevention safe S Safety Teams/ Organizational Structure A Access to information/ Accurate Reporting/ Monitoring/
Patient Safety Road Map to Controlled Substance Diversion Prevention Road Map to Diversion Prevention safe S Safety Teams/ Organizational Structure A Access to information/ Accurate Reporting/ Monitoring/
States that Allow Prescribers and/or Dispensers to Appoint a Delegate to Access the PMP
 States that Allow Prescribers and/or Dispensers to Appoint a Delegate to Access the PMP Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office
States that Allow Prescribers and/or Dispensers to Appoint a Delegate to Access the PMP Research current through December 2014. This project was supported by Grant No. G1399ONDCP03A, awarded by the Office
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017
 Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
Florida s New Law on Controlled Substance Prescribing
 FLORIDA MEDICAL ASSOCIATION Florida s New Law on Controlled Substance Prescribing HB 21, signed into law by Gov. Rick Scott on March 19, 2018, imposes a number of legal requirements on healthcare practitioners
FLORIDA MEDICAL ASSOCIATION Florida s New Law on Controlled Substance Prescribing HB 21, signed into law by Gov. Rick Scott on March 19, 2018, imposes a number of legal requirements on healthcare practitioners
Overview of the Changes to the Meaningful Use Program Called for in the Proposed Inpatient Prospective Payment System Rule April 27, 2018
 Overview of the Changes to the Meaningful Use Program Called for in the Proposed Inpatient Prospective Payment System Rule April 27, 2018 NOTE: These policies have only been proposed. No policies are final
Overview of the Changes to the Meaningful Use Program Called for in the Proposed Inpatient Prospective Payment System Rule April 27, 2018 NOTE: These policies have only been proposed. No policies are final
How to Get the Most Out of Prescription Drug Monitoring Programs
 How to Get the Most Out of Prescription Drug Monitoring Programs Target Audience: Pharmacists and Pharmacy Technicians ACPE#: 0202-0000-18-019-L03-P/T Activity Type: Knowledge-based Disclosures I own 40
How to Get the Most Out of Prescription Drug Monitoring Programs Target Audience: Pharmacists and Pharmacy Technicians ACPE#: 0202-0000-18-019-L03-P/T Activity Type: Knowledge-based Disclosures I own 40
Meaningful Use Hello Health v7 Guide for Eligible Professionals. Stage 2
 Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 2 Table of Contents Introduction 3 Meaningful Use 3 Terminology 4 Computerized Provider Order Entry (CPOE) for Medication, Laboratory
Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 2 Table of Contents Introduction 3 Meaningful Use 3 Terminology 4 Computerized Provider Order Entry (CPOE) for Medication, Laboratory
E-Prescribing: What Is It? Why Should I Do It? What's in the Future?
 American College of Physicians Internal Medicine 2008 Washington, DC May 15-17, 2008 E-Prescribing: What Is It? Why Should I Do It? What's in the Future? Daniel Z. Sands, MD, MPH, FACP Posted Date:May
American College of Physicians Internal Medicine 2008 Washington, DC May 15-17, 2008 E-Prescribing: What Is It? Why Should I Do It? What's in the Future? Daniel Z. Sands, MD, MPH, FACP Posted Date:May
2018 Modified Stage 3 Meaningful Use Criteria for Eligible Professionals (EPs)*
*") 2018 Modified Stage 3 Meaningful Use Criteria for Eligible Professionals (EPs)* n In order for an EP to be considered a meaningful electronic health record (EHR) user, at least 50 percent of the EP s patient
2018 Modified Stage 3 Meaningful Use Criteria for Eligible Professionals (EPs)* n In order for an EP to be considered a meaningful electronic health record (EHR) user, at least 50 percent of the EP s patient
Delegation Oversight 2016 Audit Tool Credentialing and Recredentialing
 Att CRE - 216 Delegation Oversight 216 Audit Tool Review Date: A B C D E F 1 2 C3 R3 4 5 N/A N/A 6 7 8 9 N/A N/A AUDIT RESULTS CREDENTIALING ASSESSMENT ELEMENT COMPLIANCE SCORE CARD Medi-Cal Elements Medi-Cal
Att CRE - 216 Delegation Oversight 216 Audit Tool Review Date: A B C D E F 1 2 C3 R3 4 5 N/A N/A 6 7 8 9 N/A N/A AUDIT RESULTS CREDENTIALING ASSESSMENT ELEMENT COMPLIANCE SCORE CARD Medi-Cal Elements Medi-Cal
State advocacy roadmap: Medicaid access monitoring review plans
 State advocacy roadmap: Medicaid access monitoring review plans Background Federal Medicaid law requires states to ensure Medicaid beneficiaries are able to access the healthcare providers they need through
State advocacy roadmap: Medicaid access monitoring review plans Background Federal Medicaid law requires states to ensure Medicaid beneficiaries are able to access the healthcare providers they need through
Reporting Requirements and Exemptions to Reporting
 Reporting Requirements and Exemptions to Reporting Research current through May 2016. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Reporting Requirements and Exemptions to Reporting Research current through May 2016. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Role of e-prescribing in Preventing Opioid Abuse
 Role of e-prescribing in Preventing Opioid Abuse John Klimek R.Ph. Senior Vice President Standards and Industry IT NCPDP March 16, 2017 Agenda Opioid Epidemic PDMP Benefits and Challenges Comprehensive
Role of e-prescribing in Preventing Opioid Abuse John Klimek R.Ph. Senior Vice President Standards and Industry IT NCPDP March 16, 2017 Agenda Opioid Epidemic PDMP Benefits and Challenges Comprehensive
The History of Meaningful Use
 A Guide to Modified Meaningful Use Stage 2 for Wound Care Practitioners for 2015 The History of Meaningful Use During the first term of the Obama administration in 2009, Congress passed the Health Information
A Guide to Modified Meaningful Use Stage 2 for Wound Care Practitioners for 2015 The History of Meaningful Use During the first term of the Obama administration in 2009, Congress passed the Health Information
Prescriber Use of the PDMP: A Statewide Survey and Multistate Focus Groups
 Prescriber Use of the PDMP: A Statewide Survey and Multistate Focus Groups Richard Deyo, MD, MPH Depts. of Family Medicine & Internal Medicine, Oregon Health & Science University Jessica Irvine, MS Acumentra
Prescriber Use of the PDMP: A Statewide Survey and Multistate Focus Groups Richard Deyo, MD, MPH Depts. of Family Medicine & Internal Medicine, Oregon Health & Science University Jessica Irvine, MS Acumentra
Meaningful Use Modified Stage 2 Roadmap Eligible Hospitals
 Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
TABLE OF CONTENTS. Page OBJECTIVES, SCOPE AND METHODOLOGY... 1 BACKGROUND Organizational Structure and Personnel... 4
 TABLE OF CONTENTS Page OBJECTIVES, SCOPE AND METHODOLOGY... 1 BACKGROUND... 2 Organizational Structure and Personnel... 4 Financial Information... 5 FINDINGS AND RECOMMENDATIONS... 6 1. Financial Management...
TABLE OF CONTENTS Page OBJECTIVES, SCOPE AND METHODOLOGY... 1 BACKGROUND... 2 Organizational Structure and Personnel... 4 Financial Information... 5 FINDINGS AND RECOMMENDATIONS... 6 1. Financial Management...
States that Allow Prescribers and/or Dispensers to Appoint a Delegate to Access the PMP
 States that Allow Prescribers and/or Dispensers to Appoint a Delegate to Access the PMP Research current through May 2016. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of
States that Allow Prescribers and/or Dispensers to Appoint a Delegate to Access the PMP Research current through May 2016. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of
PRESCRIBING IN NEVADA
 PRESCRIBING IN NEVADA An Inside Look at Changes to Nevada Laws Surrounding Prescribing Controlled Substances for the Treatment of Pain These changes to Nevada law do not impact the authority of practitioners
PRESCRIBING IN NEVADA An Inside Look at Changes to Nevada Laws Surrounding Prescribing Controlled Substances for the Treatment of Pain These changes to Nevada law do not impact the authority of practitioners
DOD INSTRUCTION DRUG TAKE BACK PROGRAM
 DOD INSTRUCTION 6025.25 DRUG TAKE BACK PROGRAM Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: April 26, 2016 Releasability: Approved by: Cleared
DOD INSTRUCTION 6025.25 DRUG TAKE BACK PROGRAM Originating Component: Office of the Under Secretary of Defense for Personnel and Readiness Effective: April 26, 2016 Releasability: Approved by: Cleared
LOUISIANA. Downloaded January 2011
 LOUISIANA Downloaded January 2011 SUBCHAPTER A. PHYSICIAN SERVICES 9807. Standing Orders A. Physician's standing orders are permissible but shall be individualized, taking into consideration such things
LOUISIANA Downloaded January 2011 SUBCHAPTER A. PHYSICIAN SERVICES 9807. Standing Orders A. Physician's standing orders are permissible but shall be individualized, taking into consideration such things
Prescribing Standards for Nurse Practitioners (NPs)
") Standards Prescribing Standards for Nurse Practitioners (NPs) Month Year PRESCRIBING FOR NURSE PRACTITIONERS MONTH YEAR i Approved by the College and Association of Registered Nurses of Alberta () Provincial
Standards Prescribing Standards for Nurse Practitioners (NPs) Month Year PRESCRIBING FOR NURSE PRACTITIONERS MONTH YEAR i Approved by the College and Association of Registered Nurses of Alberta () Provincial
Medicare and Medicaid Programs: Electronic Health Record Incentive Program -- Stage 3 and Modifications to Meaningful Use in 2015 through 2017
 Medicare and Medicaid Programs: Electronic Health Record Incentive Program -- Stage 3 and Modifications to Meaningful Use in 2015 through 2017 and 2015 Edition Health Information Technology Certification
Medicare and Medicaid Programs: Electronic Health Record Incentive Program -- Stage 3 and Modifications to Meaningful Use in 2015 through 2017 and 2015 Edition Health Information Technology Certification
How to Participate Today 4/28/2015. HealthFusion.com 2015 HealthFusion, Inc. 1. Meaningful Use Stage 3: What the Future Holds
 Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented by We ll begin momentarily Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented
Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented by We ll begin momentarily Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented
Prescription Monitoring Program:
 Massachusetts Department of Public Health Prescription Monitoring Program: The Massachusetts Prescription Monitoring Tool (MassPAT) November 1, 2016 Goals of the Session Understand the mission and responsibilities
Massachusetts Department of Public Health Prescription Monitoring Program: The Massachusetts Prescription Monitoring Tool (MassPAT) November 1, 2016 Goals of the Session Understand the mission and responsibilities
ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-19 PAIN MANAGEMENT SEVICES TABLE OF CONTENTS
 Medical Examiners Chapter 540-X-19 ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-19 PAIN MANAGEMENT SEVICES TABLE OF CONTENTS 540-X-19-.01 540-X-19-.02 540-X-19-.03 540-X-19-.04
Medical Examiners Chapter 540-X-19 ALABAMA BOARD OF MEDICAL EXAMINERS ADMINISTRATIVE CODE CHAPTER 540-X-19 PAIN MANAGEMENT SEVICES TABLE OF CONTENTS 540-X-19-.01 540-X-19-.02 540-X-19-.03 540-X-19-.04
Meaningful Use Overview for Program Year 2017 Massachusetts Medicaid EHR Incentive Program
 Meaningful Use Overview for Program Year 2017 Massachusetts Medicaid EHR Incentive Program October 23 & 24, 2017 Presenters: Elisabeth Renczkowski, Al Wroblewski, and Thomas Bennett Agenda 2017 Meaningful
Meaningful Use Overview for Program Year 2017 Massachusetts Medicaid EHR Incentive Program October 23 & 24, 2017 Presenters: Elisabeth Renczkowski, Al Wroblewski, and Thomas Bennett Agenda 2017 Meaningful
Auditing Mandatory Electronic. Prescribing in NYS
 Auditing Mandatory Electronic Anita Murray, R.Ph. Deputy Director NYS Department of Health Bureau of Narcotic Enforcement Prescribing in NYS September 12, 2017 Bureau of Justice Assistance Harold Rogers
Auditing Mandatory Electronic Anita Murray, R.Ph. Deputy Director NYS Department of Health Bureau of Narcotic Enforcement Prescribing in NYS September 12, 2017 Bureau of Justice Assistance Harold Rogers
Medicare and Medicaid EHR Incentive Program. Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment
 Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
DC Board of Pharmacy and Pharmaceutical Control Update
 DC Board of Pharmacy and Pharmaceutical Control Update Shauna K. White, Pharm.D, MS Executive Director Board of Pharmacy Program Manager - Pharmaceutical Control Division September 17, 2016 Objectives
DC Board of Pharmacy and Pharmaceutical Control Update Shauna K. White, Pharm.D, MS Executive Director Board of Pharmacy Program Manager - Pharmaceutical Control Division September 17, 2016 Objectives
Request for Information NJ Health Information Network. State of New Jersey. New Jersey HIT Coordinators Office. Request for Information
 State of New Jersey New Jersey HIT Coordinators Office Request for Information New Jersey s Health Information Exchange The New Jersey Health Information Network (NJHIN) July 1, 2011 Page 1 of 11 Table
State of New Jersey New Jersey HIT Coordinators Office Request for Information New Jersey s Health Information Exchange The New Jersey Health Information Network (NJHIN) July 1, 2011 Page 1 of 11 Table