Time. 9.45am. 9.45am. 9.45am. 9.45am. Video am am am. To followw am am
|
|
|
- Clyde Simmons
- 6 years ago
- Views:
Transcription



1 Meeting of the Board of Directors 20 December am Boardroom, Trust Headquarters Royal Albert Edward Infirmary, Wigann Lane, Wigan WN1 2NN Agenda PART 1: Held in public Item Time Encl. Purpose Presenter 1. Chairman and quorum 9.45am Verbal Compliance R Armstrong 2. Apologies for absence 9.45am Verbal Information P Howard 3. Declarations of interest 9.45am Verbal Information As required 4. Cancer Strategy Presentation 9.45am Discussion Drr Sundar 5. Minutes of the previous meeting and review of action log 10.05am Approval R Armstrong 6. Patient story 10.05am Video Discussion P Law 7. Chairman and Chief Executive s opening remarks 10.15am Verbal Information R Armstrong and A Foster 8. ASSURANCE AND GOVERNANCE 8.1 Reports of Committees 10.25am Discussion Committee Chairs 8.2 Performance report 10.35am Discussion M Fleming and P Law 8.3 Financial position as at 30 November am To followw Discussion R Forster 8.4 Board Assurance Framework 11.15am Approval R Armstrong
2 Item Time Encl. Purpose Presenter 8.5 Safe staffing report 11.20am Report P Law 9. ITEMS FOR APPROVAL 9.1 Emergency Preparedness, Resilience and Response (EPRR) Compliance Statement am Approval M Fleming 9.2 Health and Safety Annual Report 11.28am Approval P Law 9.3 Freedom to Speak Up update 11.31am Approval A Balson 10. ITEMS FOR INFORMATION No items 11. CLOSING MATTERS 11.1 Identification of key successes and risks 11.35am Verbal Discussion R Armstrong 11.2 Review of meeting effectiveness 11.40am Verbal Discussion R Armstrong 11.3 Questions from the public 11.43am Verbal Information R Armstrong 12. RESOLUTION TO EXCLUDE PRESS AND PUBLIC 12.1 Resolution to exclude press and public 11.45am Verbal Approval R Armstrong 13. DATE, TIME AND VENUE OF NEXT MEETING January 2018, TBC in the Boardroom, Trust Headquarters 11.45am Verbal Information R Armstrong


3 Cancer Services: Dr Ram Sundar WWL Cancer Services ranked No 1 out of 135 NHS Trusts 1

4 Services Provided Lung Patient Telephone Consultation Service 2ww Straight to Test Colorectal Pathway Chemotherapy Treatments for Lung, Colorectal, Breast and Haematological Cancers - Christie at Wigan Complimentary Therapy Services within the Cancer Care Centre Macmillan Information Centres at RAEI and TLC along with an information point at Leigh Infirmary Breast unit specialising in breast cancer and reconstructive surgery. New patient referral is less than one week for cancer patients and 100% of patients are seen within two weeks. Weekly Tumour specific local and Network MDT meetings New Lung Cancer pathway Telephone consultation Comparison of Q1 last year and Q1 this year. Average wait from 2ww referral to tertiary treatment Average wait to CARP out Cancer Waiting Times 62 day performance Number of breach s Patient s 1st seen within 7 days Since the new lung pathway has been implemented patients have a STT CT scan which is then reviewed by the consultant. If lung Ca is suspected then the patient receives a telephone consultation and further investigations are requested. This saves a large amount of time in the pathway as the patient does not need to wait for a clinic appointment to request the investigations. This has resulted in improved performance and less breaches. Q1 2016/17 (before telephone consultation) Q1 2017/18 (post telephone consultation) % % % % Currently this year we have A performance of 91.67% A total of 2 breaches against 11 last year An average wait of 50.4 days from referral to treatment An average wait of 28.7 days from referral to CARP out. This shows further improvement from Q1 this year. 2
5 Tumour Sites Overview Majority of tumour pathways are investigated locally. Weekly MDTs with live capturing of the data. EBUS/EUS PET Sector MDTs SAFETY NET The Christie at Wigan From April 2016 to April 2017 we have provided approximately 5,000 chemotherapy and supportive treatments, an increase of 1500 on the previous year. The strong working relationship between WWL and Christie hospitals has enabled the centre to provide: Increased chemotherapy treatment activity Continued improved compliance with SACT (Systemic Anti-Cancer Therapy) dataset Lung chemotherapy regimen now in use at Wigan Continued expansion of chemotherapy regimens used locally offering more treatment options for metastatic disease Blood service on bank holidays to ensure smooth running of service Sharing of good practice Bolton chemotherapy service has spent time on unit to gain ideas of how they can improve and expand their service as well as representatives from Crewe, who have visited to see how the business model can be introduced within their trust. 3


6 Workload of Cancer Care Centre From April 2016 to April 2017 approximately 5,000 chemotherapy and supportive treatments were administered at WWL. An increase of 43% from the previous year Haematology Chemotherapy Activity This activity has risen continuously over the last three years and has shown a steady increase month on month due to the expansion of chemotherapy regimes and increasing patient figures. Total Annual Treatments 2015 = = =
7 National Cancer Patient Experience Survey 2016 RESULTS There were some areas of the patient experience highlighted in which improvements could be made and an action plan has been developed to address these recommendations. These areas included: Hospital Staff gave information on getting Financial help Patient given clear written information on discharge Staff told patient who to contact if worried post discharge Patient given understandable information about whether chemotherapy was working Given practical advice and support when dealing with side effects of treatment Taking part in cancer research discussed with patient Overall, the survey has shown very positive results and congratulations must go to the staff delivering the service to the patients. Cancer Performance 2017/18 All 14, 31 and 62 day Cancer Waiting Times targets have been achieved We have achieved over 90% every month in 2017/18 for the 62 day standard which has been our most consistent performance sine the targets began One of the 8 key priorities set by NHS England was for all tumour pathways to achieve the 85% required for the 62 day standard. In 2016/17 5 of our 9 tumour pathways exceeded 85% in 2017/18 this has improved to 7 of the 9. COSD is our monthly data submission to the Cancer Registry consisting of over 400 data items. Our compliance for cancer staging, patient performance status and specialist nurse contact are monitored. We are only 1 of 6 trusts who achieve above the required 70% on all 3 measures. Our current staging performance is 93% 5
8 14 Day target 98.0% 97.0% 96.0% 95.0% 94.0% 93.0% WWL National Target 92.0% 91.0% 90.0% April May June July August September October 31 day target 101.0% 100.0% 99.0% 98.0% 97.0% WWL National Target 96.0% 95.0% 94.0% April May June July August September October 6
9 62 day target 100.0% 95.0% 90.0% 85.0% 80.0% WWL National Target 75.0% 70.0% 65.0% April May June July August September October Median wait from referral to treatment Median target Breast Gynae Lower GI Haem H+N Skin Urology Upper GI Lung 7
10 Performance Challenges To keep up with the demand for 2ww referrals. Some tumour sites have seen a 90% increase since As diagnostics and treatment progress and become more tailored to the individual patient additional tests can be required but we still need to accommodate within the existing timeframes To eliminate any avoidable 104+ day breaches. Review has shown that some of the main reasons have been repeat investigations, patients being investigated by multiple MDTs and delays in diagnostics when clinicians haven t requested as a target Radiology Diagnostics are clearly key to Cancer Performance WWL consistently achieves National Diagnostic Access Standard Locally aim for 5 day total turnaround for Ca patients Challenges Solutions Scanner Capacity Reporting Capacity MDT attendance GM PACS Project GM Radiology Programme PET Scanner / Wrightington Research Centre 8

11 Living With and Beyond Cancer Background In 2010, 2 million patients living with cancer in the UK. By 2030 there will be approx. 4 million patients. Wigan and Leigh Locality - Over 2000 patients diagnosed with cancer every year What is the Recovery Package? WWL Progress Increase in number of CNS using HNA with patients (paper and electronic) Two Health and Wellbeing Events held at Wigan and Leigh. One Breast specific programme. Treatment Summaries developed awaiting support from HIS Team The Recovery Package is the standard of care for all cancer patients including: Written care plans based on holistic needs assessments (HNA) An invitation to a health and wellbeing event. Treatment summaries A cancer care review undertaken in primary care Acts as a flag for a Cancer Care Review by the GP practice Implementing key elements of the Recovery Package will lead to Stratified/Self Management Pathways and reduce outpatient follow up Challenges Ahead for Cancer Services Maintaining the Cancer Clinical Nurse Specialist Workforce Career Day planned for January 2018 to raise the profile of the CNS Nurse and to offer students and the newly qualified an insight into the role of the CNS. Janet Irvine, Macmillan Lead Nurse for Cancer and Palliative Care In 2018 we will have an additional measure to report on. Day 28, which is essentially all 2ww referrals should have a cancer or noncancer diagnosis by day 28 of the pathway We will begin by shadow monitoring this to see where the gaps currently are and what changes/improvements we need to make to capture this data. Julie Fletcher, Cancer Services Manager 9

12 Challenges Ahead for Cancer Services The biggest challenge during 2018 will be to fully implement the Recovery Package with all tumour sites and specifically implement new self -management /stratified pathways for Breast, Colorectal and Prostate as an alternative to traditional models of long term clinic follow up. Plan to hold pathways events with the 3 clinical teams and divisional managers to implement the new pathways of aftercare. Kathryn Place, Macmillan Transformation Manager Newer technology and immunotherapy. Dr Ram Sundar, Clinical Director for Medicine 10
13 WRIGHTINGTON, WIGAN AND LEIGH NHS FOUNDATION TRUST MINUTES OF A MEETING OF THE BOARD OFF DIRECTORS HELD ON 29 NOVEMBER 2017 AT 9.45AM AT KILHEY COURT, CHORLEY ROAD, STANDISH, WIGAN WN1 2XN Members attendance record 25/01/ /02/ /03/ /04/ /05/ /06/ /07/ /09/ /10/ /11/ /12/2017 Mr R Armstrong Chair A Dr S Arya Medical Director A Mrs A Balson Director of Workforce A A Mr N Campbell Non-Executive Director A Mrs M Fleming Mr R Forster Director of Operations and Performance Director of Financee & Informatics/Deputy Chief Executive A A Mr A Foster Chief Executive A Mr M Guymer Non-Executive Director Mrs C Hudson Non-Executive Director Mrs P Law Director of Nursing Mr J Lloyd Non-Executive Director A A A Mr R Mundon Director of Strategyy A Mrs C Parker Stubbs Non-Executive Director A A Mr N Turner Non-Executive Director Prof T Warne Non-Executive Director A A Key: : attended In attendance A: apologies sent s : did not attend --- not a member of the board at thee date of the meeting Mrs E Bradbury, Associate Non-Executive Director Mrs L Hancock, Corporate Services Administrator (minutes) Mr P Howard, Trust Board Secretary Mr A Twist, Divisional Medical Director for Surgery
14 1262 Chair s opening remarks The Chair opened the meeting of the Board of Directors and confirmed that the meeting was quorate Apologies No apologies for absence were received Declarations of interest There were no opening declarations of interest Minutes of the previous meeting The minutes of the Board of Directors meeting held on 25 October 2017 were agreed to be a true and accurate record. Completed action updates were received and noted Patient story The Director of Nursing introduced a video clip to the Board of Directors which outlined the positive experience of a patient who had undergone a hip operation at Wrightington. It was noted that the patient had been impressed by the care and consideration that had been shown to her whilst at the hospital. The experience had highlighted the vital importance of good communication between staff and patients and she was keen that her story was shared with members of staff as an example of good care. The Board received and noted the contents of the video. The story re-enforced the message that it was the smaller acts of kindness and compassion which made the difference to patient experience. The Board expressed their appreciation to staff involved in the care of the patient for their efforts despite organisational pressures. It was noted that the video would be used for training purposes in the future Chair and Chief Executive s report and matters for the Board to note The Chair reported that a number of the Non-Executive Directors had attended a recent Council of Governors meeting to discuss their individual roles within the Board. This had been appreciated by Governors. The Chair went on to provide an update in relation to a new regional initiative that was being implemented which aimed to improve the care and safety of the elderly. An inaugural meeting would soon be taking place which would be attended by WWL representatives. The Chief Executives report had been circulated separately and the following points were highlighted: Accident and Emergency (A&E) continued to be under significant pressure. A huge amount of work was being undertaken to drive improvements in performance and maintain patient safety Minutes of a meeting of the Board of Directors held on 29 November
15 Uptake of flu vaccinations was on track to achieve the required 70% by the end of December Overseas recruitment of doctors continued with a recent exercise in India resulting in the identification of 268 potential candidates to come to the North West to learn, earn and return The CQC and NHS Improvement Well Led Inspections were currently underway at the Trust The Board received and noted the contents of the report Reports of committees (a) Report from the Audit Committee The Chair of the Audit Committee provided a verbal update to the Board. It was noted that the next meeting would be taking place on 6 December 2017 and an update from this would be provided at the next Board of Directors meeting. (b) Report from the Workforce Committee The Chair of the Workforce Committee noted that the next meeting of the Committee would be taking place in March The Board Assurance Framework (BAF) objectives monitored by the Committee were unchanged since the last review by the Board. The WWL Way 4Wards Strategy continued to be rolled out across the organisation with an interactive experience available to all staff on the Leigh site. (c) Report from the Quality and Safety committee The Chair of the Quality and Safety Committee provided a verbal update to the Board to accompany the minutes of the meeting held on 8 November The following key points were noted: There had been an increased number of risks on the Corporate Risk Register which highlighted the pressures on the organisation overall. A number of these were in relation to workforce, particularly nursing. Appropriate actions were in place to ensure quality and safety of care for patients was maintained A report had been received from the Child Safeguarding team which had highlighted increasing levels of activity and the high prevalence of domestic violence within the Borough. Concerns had also been raised in relation to capacity; a business case was being prepared to enhance the team Assurance had been taken that the Trust was responding well to Prevention of Future Deaths (PFD) notices A good level of assurance had been taken by the Committee with regard to an independent review of End of Life Care cases at the Trust. The findings had Minutes of a meeting of the Board of Directors held on 29 November
16 outlined that care and engagement with families had been appropriate and as expected The Board noted that specific concerns had been raised at the Quality and Safety Committee meeting in October in relation to sepsis performance. Clarity around this had been provided at the November meeting and assurances given that the apparent dip in performance had been due to the audit process rather than a change in practice. Improvements to data capture had been implemented and the Trust was currently performing well. The Board reflected on the high levels of domestic violence in the Borough. It would be important for the Trust, as the main employer in Wigan, to undertake all possible action to assist with local focus on this. The Board received and noted the verbal report. (d) Report from the Finance and Investment Committee The Chair of the Finance and Investment Committee provided a verbal update to the Board to accompany the minutes of the meeting held on 21 November The following key points were noted: Discussion had taken place with regard to A&E performance and the impact of the Hospital Information System (HIS) implementation The Committee had noted the continuing pressures on divisional operating costs and the uncertainties around commissioning intentions and contract discussions A year to date deficit of 3.7m had been reported but it had been noted that, with the inclusion of the Leigh Walk In Centre data, quarter two Sustainability and Transformation (S&T) Funding had been achieved An excellent presentation had been delivered by the Medicine division which had provided a good level of assurance to the Committee in relation to financial and operational performance The Board received and noted the verbal report Performance report The Director of Nursing and the Director of Operations and Performance presented the performance report for October and highlighted the following points: There had been initial issues with data reporting following the implementation of HIS in A&E on the 17 October It had been felt prudent to suspend reporting until the system stabilised and this had recommenced from 6 November Validation of data between 17 October and 5 November had been undertaken and it had been proposed to NHS Improvement that patients during this period would be cohorted. NHS Improvement had confirmed this to be acceptable. As a result, A&E performance year to date had improved to 87%. If Leigh Walk In Centre data was included this increased further to just over 90% performance Minutes of a meeting of the Board of Directors held on 29 November
17 An electronic job planning system would be implemented in early January. It was anticipated that this would address current concerns around the effectiveness and consistency of Consultant job planning There had been a 52 week breach in relation to a child awaiting routine surgery. The incident had been due to human error and did not link with any previous cases of 52 week breaches. Actions were being taken to ensure this was not repeated and a report would be taken to Quality & Safety Committee following completion of the Root Cause Analysis (RCA) It was noted that the number of Never Events was incorrectly reported as zero within the performance report. There had actually been one Never Event in relation to a wrong site surgery in Dermatology. The lessons learned from this would be shared at the next Quality and Safety Committee meeting The Board received the contents of the performance report for October and noted that operational pressures were a significant priority for the Trust with focus on safety issues and recovery Financial position as at 31 October 2017 The Director of Finance and Informatics presented the finance report for October and highlighted the following points: The Trust had reported a 400k loss in month against a planned surplus of 1m The year to date positon was a 3.7m deficit against a planned deficit of 2.2m Cost Improvement Programmes (CIP) had delivered 6.1m which was behind plan by 700k Capital expenditure and cash continued to be closely monitored A Use of Resources rating of 3 had been achieved in line with plan Quarter one and two control totals had been achieved but the challenge would increase for quarters three and four The NHS Improvement Use of Resources assessment had taken place and had been positive. Additional information had been requested and was being provided Quarter two S&T Funding for A&E had been achieved with the inclusion of the Leigh Walk In Centre data. Discussion continued with regard to the ongoing inclusion of this Funding of 962k had been received for the locality from the Digital Collaboration Board for Greater Manchester (GM) - 632k of this would sit with WWL Minutes of a meeting of the Board of Directors held on 29 November
18 Further winter funds had been released nationally. WWL would be applying for a portion of this to assist with operational pressures Discussion continued in relation to Commissioning Intentions and the block contract. Further updates would be provided when available The Board received the contents of the finance report and noted that national discussions continued in relation to the Orthopaedic tariff. In recognition of the current organisational pressures, a number of initiatives had been implemented for staff including Amazon delivery lockers, financial assistance schemes and the provision of refreshments. Additionally, staff would receive their birthday as annual leave next year as a token of appreciation for their efforts Board Assurance Framework The Board approved the Board Assurance Framework (BAF). The scores proposed by the sub-committees and the Executive team were agreed to be appropriate Safe Staffing report The Director of Nursing presented the Safe Staffing report to the Board of Directors and highlighted the following key points: The fill rate for registered nurses had increased during October as a result of additional incentives put in place Specialist Nurses had been encouraged to undertake a shift per week on the wards for additional support the response to this had been positive Six wards appeared on the risk register at a score of 20 for staffing levels however only two of these had an issue with fill rates Operational demands in Maternity were impacting on staffing a review of the staffing model would be undertaken Rainbow Ward had achieved 100% compliance for the presence of an Advanced Paediatric Life Support (APLS) trained member of staff on each shift. The Board received and noted the contents of the report Items requiring approval The following items were presented to the Board of Directors for approval: Safeguarding Children annual report The Board received the report and confirmed approval Items for information There were no items received for information. Minutes of a meeting of the Board of Directors held on 29 November
19 1275 Key successes/risks The Board discussed and agreed the key successes and risks as follows: Risks Ongoing pressures within A&E Risks around workforce, particularly nursing The financial position and challenges Issues in relation to the implementation of HIS Successes Progress being made within the Safeguarding teams, particularly in increasing training compliance The confirmation of funding via the Digital Collaboration Board funding Achievement of performance targets for 18 Weeks Referral to Treatment (RTT) and cancer 1276 Board effectiveness feedback The board recognised the excellent quality of papers which had facilitated efficient discussions Questions from the public There were no questions received from the public Exclusion of the public The Board resolved that representatives of the press and other members of the public be excluded from the remainder of the meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest Date of the next meeting The next meeting of the Board of Directors will be held on 20 December 2017, 9.45am at Royal Albert Edward Infirmary, Wigan Lane, Wigan, WN1 2NN. Minutes of a meeting of the Board of Directors held on 29 November


20 Trust Board Action Log P1 Date of meeting Agenda ref No. Item Actions carried forward from previous meetings Na. Actions from this meeting Na. Action required Assigned to Target date Date completed
21 REPORT AGENDAA ITEM: 8.1 To: Board of Directors Date: 20 December 2017 Subject: Reports of Committees Presented by: Committee Chairs Purpose: For report Executivee summary The Reports of Committees are presented to the Board of Directors to provide an overview of discussions which have taken place at Sub Committee meetings over o the course of October. Risks associated with this report Risks as identified by the Sub Committees are highlighted within the reports. Link(s) to The WWL Way 4wards Patients Performance People Partnerships
22
23 MINUTES OF A MEETING OF THE AUDIT COMMITTEEE HELD ON 6 DECEMBER 2017 AT 9.30AM AT ROYAL ALBERT EDWARD INFIRMARY, WIGAN LANE, WIGAN WN1 2NNN Members attendancee record Mr N Campbell Mr M Guymer Mrs C Hudson Mr N Turnerr Non-Executive Director Non-Executive Director Non-Executive Director (Chair) Non-Executive Director A A Key: : attended A: apologies sent : did not attend --- not a member at the date of the meeting In attendance Ms C Alexander Associate Director of Governance and Assurance Mrs A Balson Director of Workforce Mrs E Bradbury Associate Non-Executive Director Ms A Gent - Audit Manager, Deloitte Mrs L Hancock Corporate Services Administrator (minutes) Mr P Howard Trust Secretary Mr D Hughes Associate Director of Finance (representing the Director of Finance & Informatics) Mr R Mundon Director of Strategy Mrs D Pullen Compliance Lead Mrs C Ryan Local Anti-Fraud Specialist Mrs L Warner Senior Internal Audit Manager, Mersey Internal Audit Agencyy (MIAA)
24 1. Committee chair s opening remarks The chair opened the meeting of the Audit Committee. 2. Apologies for absence Apologies for absence were received as indicated in the attendance record. 3. Declarations of interest There were no opening declarations of interest. 4. Minutes of the last meeting The minutes of the Audit Committee held on the 4 October 2017 were agreed to be a true and accurate record. 5. Matters arising a. Action updates from the last meeting Completed action updates were received and noted. 6. Internal Audit a. Progress report The committee received and noted the progress report submitted by MIAA. Reports were provided on each of the completed reviews: Consultant Job Planning The review had provided no assurance. A number of inconsistencies had been identified during the course of the review including job plans which were out of date, had incomplete information within them or had not been appropriately signed off. There were also instances of inconsistency between information on job plans and that held on Electronic Staff Records (ESR). No evidence had been seen in relation to quality assurance reviews. The Director of Workforce noted that the Trust had specifically requested this review to be undertaken as part of the audit cycle due to lack of assurances around job planning and the report provided valuable insight into the issues to be addressed. It was noted that work was underway to implement an electronic job planning system which would transform the way the process was undertaken. It was anticipated that this would go live in January with all existing job plans to be in place by the end of March. The new system would give full traceability and it was pleasing to note that clinical engagement had been very positive to date. There was a good level of confidence that the Trust would be in a better position by the end of March. The Committee accepted the conclusion of Internal Audit and noted concern at the lack of assurance in relation to job planning. It would be important to address these issues swiftly and the Committee were heartened to receive the update in relation to the electronic system. Minutes of a meeting of the Audit Committee held on 6 December
25 It was agreed that the matter would be referred to the Workforce Committee for monitoring with an update back to the next Audit Committee. The Director of Workforce and Medical Directors were identified to be the Executive leads. Action: Director of Workforce and Medical Director The report would be shared with the Non-Executive Directors for information. Medical Devices The review had provided limited assurance. Action: Corporate Services Administrator It had been noted that there was no definitive system in place to demonstrate that staff were trained to use devices competently. A sample of ward training documentation had been reviewed and inconsistencies identified. It had further been identified that there was no electronic tracking system in place increasing the risk of equipment going missing or remaining in use without the necessary services. The Committee accepted the findings of Internal Audit. It was noted that the Estates and Facilities team were currently in the process of procuring a system to record training compliance and device maintenance. In the interim, the risk around this featured on the Corporate Risk Register and manual record keeping and additional vigilance had been implemented in mitigation. It was recommended that this was referred to Quality & Safety Committee for further monitoring. Attendance Management The review had provided limited assurance. Action: Associate Director of Governance and Assurance It had been noted that while there was a good policy in place at the Trust, managers were not always complying with it. There had been instances identified where Return to Work forms could not be located or had not been completed on the day of return. The Committee accepted the conclusions of Internal Audit and noted that management action was being taken to address the issues highlighted. It was recommended that this was referred to the Workforce Committee for further monitoring. Action: Director of Workforce National Institute for Health and Care Excellence (NICE) Quality Standards The review had provided limited assurance. It was noted that the review had been undertaken at the request of the Trust as there had been recognition that the current system for assessing NICE Quality Standards needed to be refreshed. The Trust had already commenced work with this regard. The review had identified a number of areas for consideration including recording the rationale for assessing NICE Quality Standards as not applicable, the potential requirement for additional triage Minutes of a meeting of the Audit Committee held on 6 December
26 resource to ensure quality standards were disseminated within the agreed 4 days, ensuring alignment of quality standards with a key owner and breaches to the Trusts 12 week deadline. The Associate Director of Governance and Assurance advised that the review had been a helpful process which had identified the requirement to re-consider the treatment of NICE Quality Standards as these were currently being treated in the same way as NICE Clinical Guidelines. Discussions with regard to this had commenced and would continue later in December. The Committee accepted the findings of Internal Audit. It was recommended that this was referred to the Quality and Safety Committee for further monitoring. Do Not Attempt to Resuscitate (DNA CPR) The review had provided limited assurance. Action: Associate Director of Governance and Assurance It was noted that the review had been undertaken across 5 areas and 30 DNA CPR forms. Issues had been identified in terms of completeness of documentation and consistency. The Trust management team had agreed actions to respond to the review and would be keeping the Quality and Safety team updated as to progress. The Committee accepted the findings as presented by Internal Audit. It would be important to ensure clinical engagement around the completion of documentation. It was recommended that this would be referred to the Quality and Safety Committee for monitoring. Action: Associate Director of Governance and Assurance Information Technology (IT) Critical Application review Allscripts system The review had provided limited assurance. A number of areas of good practice had been identified as part of the review but also areas for further improvement. The Committee accepted the findings of Internal Audit and reflected on the importance of ensuring that matters around IT governance were picked up at the appropriate level in the absence of the Information Management and Technology (IM&T) Strategy Committee. It was noted that the Executive team were giving consideration to this currently. The report would be shared with Non-Executive Directors for information. Action: Corporate Services Administrator Internal Audit advised the Committee that the review of Taylor Unit had been removed from the audit plan as the Neuro Rehabilitation Service would be moving from the Trust in the new financial year. It was proposed that the audit days would instead be used to review the Mutually Agreed Resignation Scheme and the Hospital Information System (HIS) discharge process. The Committee approved these amendments. Minutes of a meeting of the Audit Committee held on 6 December
27 b. Tracking report The Committee received and noted the tracking report submitted by MIAA. Good progress was being made against recommendations with no outstanding issues or concerns to report. The Committee received and noted the contents of the report. c. MIAA insight update The MIAA insight update paper providing details of upcoming events was received and noted by the committee. It was noted that MIAA would be undertaking a review for the Trust in relation to readiness for European Union General Data Protection Regulations (EU GDPR). The findings would be reported to the Audit Committee. The Committee noted that a risk had been flagged at an earlier meeting in relation to resourcing for implementation. Assurances around this would be provided to the meeting in February via the Associate Director of IM&T although it was noted that work was underway to produce a business case for additional resource. 7. External Audit Action: Associate Director of IM&T Ms A Gent provided a verbal update in relation to recent External Audit activity. The Committee received and noted the contents of the verbal update. 8. Counter fraud a. Progress report The Local Anti-Fraud Specialist presented a report outlining recent counter fraud activity. It was noted that the NHS Counter Fraud Authority now replaced NHS Protect. An exercise around the Association of the British Pharmaceutical Industry (ABPI) database had been undertaken with a very positive response from staff. The Fraud Annual Survey had been distributed to staff in November. Uptake so far had been disappointing and consideration would be given in the future as to how the campaign could be improved to increase engagement. The Committee received and noted the contents of the report 9. Risk and Environmental Management Committee (REMC) minutes and risk tracker The Director of Strategy and Planning presented the risk tracker and the minutes from the meeting of REMC held on 16 November There were no specific risks for escalation to Audit Committee on this occasion. It was noted that the Corporate Risk Register (CRR) had an increased level of risks which demonstrated the increasing pressures on the organisation. REMC continued to monitor Minutes of a meeting of the Audit Committee held on 6 December
28 progress against the management of Service Level Agreements (SLAs) which had been discussed at earlier Audit Committee meetings. Work was being undertaken to develop a new policy in relation to this. Similarly, concerns raised at the previous Audit Committee with regard to the implementation of the new Datix system were being considered. The Committee received and noted the contents of the report. 10. Corporate governance a. Losses and compensations report The Associate Director of Finance presented a report outlining losses and special payments for the period 1 April 2017 to 31 October The Committee received the report and noted that there had been no stock losses raised in relation to Pharmacy. It was requested that Pharmacy provide some assurances with regard to frequency and outcomes of stock audits. The Associate Director of Finance would liaise with Pharmacy to provide this. b. Clinical Audit Quarter 2 report Action: Associate Director of Finance The Compliance Lead presented the Clinical Audit Quarter 2 report to the Committee. The Committee received the contents of the report and were pleased to note the positive progress that had been made in the quarter. c. Gifts and Hospitality Register The Gifts and Hospitality Register was received and noted by the Committee for information. It was noted that the annual Christmas reminder of obligations around the declaration of Gifts and Hospitality would soon be circulated to all staff. The Committee received and noted the contents of the report. It was suggested that the register included a specific section to record approval for acceptance and that greater emphasis was made around staff disclosing an estimated value as part of the declaration. d. ABPI declarations Action: Trust Secretary The Local Anti-Fraud Specialist presented the ABPI declaration report to the Committee. It was noted that work was underway to produce an overarching Declaration Policy which would encompass ABPI and Gifts and Hospitality. This would be brought to the Committee in February for discussion. The Committee received and noted the contents of the report. Minutes of a meeting of the Audit Committee held on 6 December
29 e. Asset lives The Associate Director of Finance presented a report to the Committee which outlined the proposed approach to extending asset lives within the organisation. It was noted that this was in discussion with Deloitte (External Audit) and the Trust were in the process of providing any necessary information. The Committee received the contents of the report and noted their support of the approach outlined. It was agreed that the recommendation from Deloitte would be taken to the Finance & Investment Committee for final sign off. 11. Single tender waiver requests Action: Associate Director of Finance A report detailing single tender waivers submitted between 1 September 2017 and 31 October 2017 was received and noted by the committee for information. The Committee received and noted the contents of the report. 12. Chairs reports of other sub committees for consideration The chairs reports from sub committees were received and noted by the Committee for information. 13. Any other business There were no further items of business raised for discussion. 14. Key successes / risks Key successes were agreed to be: Anti-Fraud progress The quality of the Internal Audit reports The excellent and effective connectivity between REMC, Sub Committees and Board Key risks were agreed to be: Job planning Compliance with medical device training and services Attendance management NICE compliance DNA CPR 15. Date and time of next meeting A meeting of the Audit Committee will be held on 7 th February 2018 at 9.30am at Royal Albert Edward Infirmary, Wigan Lane, Wigan WN1 2NN. Minutes of a meeting of the Audit Committee held on 6 December
30

31 Chairpersons Report Chairpersons Name Tony Warne Committee Name Q&S Committee Date of Meeting Name of Receiving Committee Board of Directors meeting Date of Receiving Committee meeting December 2017 Strategic Items for referral to Trust Board WHO Surgical Checklist compliance Items for escalation? Yes No If yes, to which Committee Please detail up to 3 key successes or achievements discussed at the meeting 1. The Quality Improvement Strategy 2. The excellent quality of the SEC Q2 report 3. Improvements around mortality and the momentum behind the work 4. The CQC Fundamental Standards reports and progress made Details of the top three risks identified during the course of the meeting and initials of primary member of staff actioning 1. The longstanding actions remaining on the PFD action plan 2. The challenges around achievement of some of the Quality Accounts Priorities Attendance at the meeting (please highlight): Excellent (well attended) X Acceptable (some apologies) Unacceptable (quorate) Unacceptable (not quorate) Was the agenda fit for purpose and reflective of the Committees terms of reference? Absolutely a good mix of emergent issues, and reports providing assurance and noting progress Chairman: Robert Armstrong Chief Executive: Andrew Foster CBE Reviewed December 2016, next review December 2017 Narrative report of the key issues of the meeting A range of informative and high quality reports facilitated a great deal of helpful discussion and action planning decision making. Recognition was also given to the human factor issues and impact on people involved in many of the issues. For example, a comprehensive report had been prepared on the unfortunate dermatology wrong site never event. This provided a full explanation and an action plan to ensure this wouldn t happen again. The discussion included acknowledging the staff involved in this and the best way of supporting them in working through the never event, but also highlighted an urgent need to scope the number of LocSSIPs currently in use. This would better enable targeting of the human factors in ensuring their use in practice. It was good to see the PFD reports now presented using an action plan/report that was rag rated in terms of progress. The committee noted that the 22 page report was necessary for this initial presentation, but future updates would be exception reports. An excellent SEC report was presented. The comprehensive nature of the information and analysis was high quality, provided examples of how data, information and actions could be triangulated. It was a high quality report that the committee felt would be important to share with the full Trust Board. For the first time, a mid-year decision was taken to remove (or rather replace) one of the BAF risks. This was around Infection Control the original risk reduction target had been achieved and the proposal was
32 to replace the existing risk with one that moved the focus to any lapses in care. This was a good example of ensuring the BAF review moves from being a rhetorical device to something that is live and responsive. This was the last meeting that Lynda Hancock would be recording the discussions and actions something she has done for the entire tenue of role as Chair, and has done to an exemplary standard with high quality, accurate and clear minutes always being presented. I extend my thanks and on behalf of the committee wish her all the very best for her new role. Key outcomes from the reports taken at the meeting The actions are listed below but key outcomes include: Recognition that work needs to continue around responding to the human factor issues associated with compliance (oxygen prescribing; LocSSIPs). The impact of the on-going workforce concerns were acknowledged (Majors waiting room bottleneck; dermatology skilled workforce; H&S reporting) and assurance gained that mitigating responses were being taken forward. The high quality and comprehensive nature of many of the reports (H&S, SEC; PFD; Mortality; Quality strategy) provided clear both opportunities to celebrate progress and included achievable action plans for issues still to be addressed Agreed actions from the meeting A further update on oxygen prescribing to be scheduled for the March meeting The Health and Safety Manager to meeting with the Director of Nursing to agree a target for the timely reporting of RIDDOR The Head of Quality Improvement to consider links with Go Engage, the potential to utilise leadership and apprenticeship programmes for staff to undertake quality improvement projects and the possibility of widening the Quality Champions project to other areas of the Trust as well as external organisations in the locality (Quality Improvement Strategy) Information to be provided to the Committee in relation to the use of majors for patient following triage: number of patients affected and details of processes in place to ensure identification of the deteriorating patient The issues around WHO Surgical Checklist compliance to be escalated to the Board An update on LocSSIPs to be provided to a future meeting which outlined the smaller areas carrying out invasive procedures and progress towards implementation A report to be provided at the next meeting which provided a full update on outstanding PFD actions The SEC Q2 report to be shared with the Board for information A presentation with regard to MEWS to be arranged for March and DNA CPR for January Name of primary lead for the actions Trust Secretary Health & Safety Manager Head of Quality Improvement Governance Lead for Medicine Committee Chair Associate Director of Governance and Assurance Associate Director of Governance and Assurance Corporate Services Administrator Associate Director of Governance and Assurance 2
33 MINUTES OF A MEETING OF THE QUALITY AND SAFETY COMMITTEE HELD ON 13 DECEMBER 2017 AT 9.30AM AT ROYAL ALBERT EDWARD INFIRMARY, WIGAN LANE, WIGAN, WN1 2NN Members attendance record Mr R Armstrong Dr S Arya Mrs A Balson Mrs M Fleming Mr R Forster Chair Medical Director Director of Workforce Director of Operations and Performancee Director of Finance and Informatics / Deputy CEO A A A A A A A A A A A A A A A A A Mr A Foster Mrs C Hudson Mrs P Law Mr J Lloyd Mr R Mundon Mrs C Parker Stubbs Prof T Warne Chief Executive Non-Executive Director Director of Nursing Non-Executive Director Director of Strategy Non-Executive Director Non-Executive Director (Committee Chair) A A A A -- A A A A A A A A A A A Key: : attended A: apologies sent : did not attend --- not a member of thee Committee at the date of the meeting In attendance Ms C Alexander Associate Director of Mrs L Hancock Corporate Services Governancee and Assurance Administrator Mrs L Atherton Health & Safety Manager Mr P Howard Trust Secretary Dr I Aziz Consultant Chest Physician Mrs J Prescott Head of Nursing for Surgery Mrs L Barkess Jones Associate Director of Mrs D Pullen Compliance Lead Infection Prevention and Control Mr J Rowland Obstetricss and Gynaecology Mrs L Boyd Governance Lead for Medicine Consultant Mrs A Cheesman Associate Director of Nursing Mrs G Smith Governance Lead for Specialist for Professional Practice Services Mr S Clancy Fire Safety Manager Mrs C Stanford Governance Lead for Maternity Ms G Edwards Associate Director of Finance and Children ss Services Dr M Farrier Associate Medical Director Mrs L Sykes Public Governor Mrs C Greenhalgh Head of Quality Improvement
34 1. Oxygen presentation Dr I Aziz, Consultant Chest Physician, was in attendance to deliver a presentation to the Committee which outlined the current position in relation to the prescribing of oxygen for hospital patients. It was noted that the Trust had been in receipt of a Prevention of Future Deaths (PFD) notice some time ago which raised concerns that oxygen was not prescribed. In response the Trust had implemented a Task and Finish Group to make improvements in this area. Progress had been made but there was further work to be done. Oxygen prescribing had been included on the Hospital Information System (HIS) which was positive but there was requirement to focus on training and education of junior doctors and nursing staff. The Committee received the contents of the presentation and noted the positive steps being taken. A further progress update was requested to the March meeting given the importance of the work. Dr I Aziz left the meeting. 2. Committee Chair s opening remarks The Chair welcomed all to the meeting and opening introductions were made. 3. Apologies for absence Apologies for absence were noted as indicated in the attendance record above. 4. Declarations of interest There were no opening declarations of interest. 5. Minutes of the last meeting Action: Trust Secretary The minutes of the Quality and Safety Committee meeting held on 8 November 2017 were agreed to be a true and accurate record. 6. Matters arising a. Actions from the last meeting Completed actions from the Quality and Safety Committee meeting held on 8 November 2017 were received and noted. 7. Health & Safety Annual Report The Health and Safety Manager was in attendance to present the Health and Safety Annual Report to the Committee. It was noted that the incidence of violence and aggression had increased during the past year which was felt to be partly attributable to the high number of mental health patients in the hospital. A working group had been established to look into this and to consider staff training. Incidents relating to sharps injuries remained stubbornly high despite a number of Minutes of a meeting of the Quality and Safety Committee held on 13 December
35 awareness campaigns. A training model had been produced in draft format and work remained ongoing. A concern had been identified in terms of the Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 1995 (RIDDOR) in that statutory timescales for report were not being achieved. It would be important to establish a target for the division in order to drive improvement. The Health and Safety Manager would meet with the Director of Nursing to discuss this further. Action: Health & Safety Manager The Committee received the contents of the report. It was concerning to note the increased levels of violence and aggression however the Committee took assurance that appropriate action was being undertaken and that this was on the Corporate Risk Register (CRR). It would be important to continue to promote the message of zero tolerance and to encourage staff to report incidents. The Committee thanked the Health & Safety Manager for a comprehensive report. Mrs L Atherton left the meeting. 8. Quality Improvement Strategy The Head of Quality Improvement was in attendance to present the Quality Improvement Strategy to the Committee. It was noted that the document had been co-designed with a variety of stakeholders and was reflective of the regional and national Quality Improvement Strategy. The Committee were requested to provide their support in driving this forward. The Committee received the contents of the report and agreed that the strategy was excellent and would be fully supported. The Head of Quality Improvement was asked to consider infrastructure links with Go Engage, the potential to utilise leadership and apprenticeship programmes for staff to undertake quality improvement projects and the possibility of widening the Quality Champions project to other areas of the Trust as well as external organisations in the locality. Mrs C Greenhalgh left the meeting. 9. Risk management a. Risk tracker Action: Head of Quality Improvement The risk tracker from the Risk and Environmental Management Committee (REMC) was received and noted by the Committee. The Director of Strategy and Planning noted the high number of risks on the tracker which reflected the pressures on the organisation. A number of risks were in relation to nurse staffing vacancies. It was noted that risks around workforce were regularly discussed by the Board of Directors, as were financial risks. A risk escalation around the use of the major s (Accident & Emergency) waiting room would be discussed later in the meeting. Minutes of a meeting of the Quality and Safety Committee held on 13 December
36 The Committee received and noted the contents of the report. b. Use of majors waiting room The Governance Lead for Medicine was in attendance to present a risk escalation to the Committee in relation to the use of the majors waiting room during time of pressure for patients following triage. It was noted that the risk had been escalated to the Committee previously and continued to be scored at 20. A number of mitigations had been put in place including the use of winter funding to provide additional nurse cover in the area, prioritisation of patients and hourly rounding. While the risk was being managed, it was noted that the situation was not ideal and was stressful for staff. The Committee received the risk escalation and noted the assurances provided around actions taken. It was agreed that it would be beneficial for the Committee to have some understanding at a future meeting around the number of patients using the waiting room while awaiting a cubicle and what processes were in place to ensure deteriorating patients were identified swiftly. Action: Governance Lead for Medicine c. Verbal update on serious incidents in month by exception / Strategic Executive Information System (StEIS) report The Compliance Lead presented the StEIS report to the Committee. There had been four StEIS incidents submitted in November, including one Never Event. In addition to this there had been two further Never Events submitted to StEIS in the month of December. This took the Trust to four Never Events in the financial year to date. Investigations of all incidents were in progress and actions from previous Never Events would be revisited to ensure learning had been taken. The Committee received the contents of the report and noted concerns at the number of Never Events reported by the Trust, particularly as a proportion of these were in relation to wrong site surgery. Discussion took place around the robustness of the WHO Surgical Checklist and the importance of ensuring 100% compliance. It was agreed that it would be appropriate to escalate this to the Board for further consideration. d. Dermatology Never Event Action: Committee Chair The Divisional Head of Governance and Directorate Matron for Specialist Services presented a report to the Committee which outlined the findings of the investigation into a wrong site surgery incident in Dermatology. It was noted that a robust action plan was in place and was scrutinised by the Divisional Quality Executive Committee. Particular consideration would be given to patient flow and scheduling of lists as these had been contributory factors to the incident. The Committee received the contents of the report and reflected on the impact of Never Events on the staff concerned, as well as patients. It would be important to offer the Minutes of a meeting of the Quality and Safety Committee held on 13 December
37 necessary support to staff in such circumstances. A further update on Local Safety Standards for Invasive Procedures (LocSSIPs) was requested for a future meeting which identified smaller areas carrying out invasive procedures and progress towards implementing LocSSIPs. 10. Prevention of Future Deaths (PFD) action plan update Action: Associate Director of Governance and Assurance The Associate Director of Governance and Assurance presented the PFD action plan to the Committee for information. It was noted that the Trust had received four PFD notices year to date. There were two longstanding actions which remained outstanding in relation to North West Boroughs access to HIS and the implementation of a joint pro-forma with Greater Manchester Police (GMP) for patients under police escort. Discussions around these remained ongoing. The Committee received and noted the contents of the report. A report would be brought to the next meeting which provided a fuller update on outstanding actions. 11. Safe, Effective and Caring (SEC) report Action: Associate Director of Governance and Assurance The Compliance Lead presented the SEC report to the Committee for quarter two. It was noted that the report had been amended to reflect feedback from an earlier meeting. The report contained five recommendations for consideration by the divisions and the Committee were asked to endorse these. The Committee received the contents of the report and confirmed endorsement for the divisional recommendations outlined. The Compliance Lead was commended for the production of an excellent report and it was agreed that the report would be shared with the Board of Directors for information. 12. Mortality report Action: Corporate Services Administrator The Associate Director of Governance and Assurance presented the mortality report to the Committee for quarter two. It was noted that there had been one unexpected death in the quarter as a result of a fall; a full investigation had been undertaken and concluded that the Trust had taken all possible preventative action. The Trust had responded to an alert from the Imperial College London in relation to Alcoholic Liver Disease and this had now been closed by the Care Quality Commission (CQC). It was noted that the Trust was currently not meeting one of the requirements of the National Guidance on Learning from Deaths in relation to the publication of quarterly deaths information via the Board of Directors meeting. This would commence from January Minutes of a meeting of the Quality and Safety Committee held on 13 December
38 The Committee received and noted the contents of the report. 13. Quality Account Priorities The Associate Director of Governance and Assurance presented a report which provided an update on the Quality Account Priorities for It was noted that there continued to be challenges in achieving 95% compliance for the completion of venous thromboembolism (VTE) risk assessments. The Trust was currently achieving around 85% and it was felt that redesign of the assessment within HIS would be required to progress further, however, the HIS team were currently stretched in a number of priority areas. A review and audit of anti-coagulation management had been scheduled for January A presentation with regard to Modified Early Warning Scores (MEWS) had been received at the Committee meeting in November which had outlined actions being undertaken in relation to early identification of the deteriorating patient. It was recommended that a further update came back to the Committee in March. It was noted that Mersey Internal Audit Agency (MIAA) had conducted a review of Do Not Attempt Resuscitation (DNA CPR) processes at the Trust. This had provided limited assurance. It was recommended that the Committee received a presentation in relation to this at the January meeting. The Committee received the contents of the report and agreed that further discussion around MEWS and DNA CPR would be conducted as recommended. 14. Care Quality Commission (CQC) a. New engagement approach Action: Associate Director of Governance and Assurance The Compliance Lead provided an update to the Committee with regard to the new approach that the CQC would be taking around engagement. The Committee received and noted the contents of the verbal report. b. CQC Fundamental Standards report: Cleanliness, Safety and Suitability of Premises and Equipment The Committee received and noted the CQC Fundamental Standards report in relation to Cleanliness, Safety and Suitability of Premises and Equipment. It was noted that there was partial compliance in four areas; appropriate action was being taken to move these to full compliance. c. CQC Fundamental Standards report: Safe Care and Treatment The Committee received and noted the CQC Fundamental Standards report in relation to Safe Care and Treatment. It was noted that action was being taken to address areas of partial compliance. Minutes of a meeting of the Quality and Safety Committee held on 13 December
39 d. CQC Fundamental Standards report: Dignity and Respect The Committee received and noted the CQC Fundamental Standards report in relation to Dignity and Respect. It was noted that all areas were fully compliant. 15. BAF scoring The Committee discussed the scoring for the risks associated with the achievement of the corporate objective: to deliver safe, high quality, effective, evidence-based patient care. a. Failure to achieve an improved benchmarked position for mortality The Committee reflected on the improvements that had been seen around HSMR but agreed that it would be appropriate to retain the current score of 5 x 4 = 20 due to winter pressures. b. Failure to achieve infection control trajectories The Committee agreed with the recommendation to close this risk as the trajectory for Clostridium Difficile infections had already been exceeded. A new risk would be formulated which would consider lapses in care. The risk was closed. c. Failure to reduce clinical variation and drug costs by 10% The Committee noted that the position remained unchanged since the last meeting. It was agreed to retain the current score of 4x4= Items received by the Committee for information The Committee received and noted Chairs reports from reporting meetings for information. 17. Key successes and risks The Committee discussed and agreed the following key successes and risks: Successes The Quality Improvement Strategy The excellent quality of the SEC Q2 report Improvements around mortality and the momentum behind the work The CQC Fundamental Standards reports and progress made Risks The longstanding actions remaining on the PFD action plan The challenges around achievement of some of the Quality Accounts Priorities Date and time of next meeting The next meeting of the Quality and Safety Committee will be held on 10 January 2018 from 9.30am at the Royal Albert Edward Infirmary. Minutes of a meeting of the Quality and Safety Committee held on 13 December
40
41 REPORT AGENDAA ITEM: 8.2 To: Board of Directors Date: 20 December 2017 Subject: Performance report for November 2017 Presented by: Director of Operations and Performance / Director off Nursing Purpose: For report Executivee summary The performance report is presented to performance during November the Board of Directors to provide an overview of Risks associated with this report One of the organisation s corporate objectives is to achieve all report outlines the risk to achievement of this objective. national access targets. This Link(s) to The WWL Way 4wards Patients Performance People Partnerships
42
43 Performance Report November 2017
44 About the Trust Wrightington, Wigan and Leigh NHS Foundation Trust (WWL) is a major acute Trust serving the people of the Borough of Wigan a population of over 300,000. The Trust employs approximately 5,000 members of staff, all of whom play their part in delivering high quality, safe and effective patient care from the following facilities: Royal Albert Edward Infirmary our main district general hospital site, located in central Wigan, that hosts our Accident and Emergency Department Wrightington Hospital a specialist centre of orthopaedic excellence Leigh Infirmary an outpatient, diagnostic and treatment centre Thomas Linacre Centre a dedicated outpatient centre in central Wigan WWL Eye Unit a specialist ophthalmology unit based at Boston House in central Wigan About the Report This report is designed to provide a clear insight into the Quality & Performance of the Trusts services. We hope you find the report intuitive however please feel free to send any queries to BI.Performance.Report@wwl.nhs.uk who will be more than happy to help. Key Contacts Change Log ID Version No Change of Wording to 'Booked by 12+6 Weeks' on Page 5.1: Midwifery - Part 1 Inclusion of GP Streaming Attendances in 4 Hour A&E Breach Performance on NHSI M Inclusion of GP Streaming Attendances in 4 Hour A&E Breach Performance on Page 3. Removal of Targets and RAG Ratings for MSSA and E-coli on Page 1.2: Harm Free Removal of 'Diagnostics: Physiological Measurement - Urodynamics - Pressures Removal of 'Diagnostics: Physiological Measurement - Neurophysiology - Periphe Removal of 'Diagnostics: Physiological Measurement - Cardiology' from Access P Removal of 'Diagnostics: Physiological Measurement - Audiology' from Access Pa Removal of 'Diagnostics: Imaging - Non- Obstetric Ultrasound' from Access Part 2 Removal of 'Diagnostics: Imaging - Magnetic Resonance Imaging' from Access Part 2 Removal of 'Diagnostics: Imaging - DEXA Scan' from Access Part 2 Removal of 'Diagnostics: Imaging - Computed Tomography' from Access Part 2 Removal of 'Diagnostics: Imaging - Barium Enema' from Access Part 2 Removal of 'Diagnostics: Endoscopy - Gastroscopy' from Access Part 1 Removal of 'Diagnostics: Endoscopy - Flexi Sigmoidoscopy' from Access Part 1 Report Considerations Change Change Date Requested By 14/11/2017 Mary Fleming BI 14/11/2017 Mary Fleming BI 14/11/2017 Mary Fleming BI Authorised By 14/11/2017 Pauline Law BI 10/08/2017 Mary Fleming BI 10/08/2017 Mary Fleming BI 10/08/2017 Mary Fleming BI 10/08/2017 Mary Fleming BI 10/08/2017 Mary Fleming BI 10/08/2017 Mary Fleming BI 10/08/2017 Mary Fleming BI 10/08/2017 Mary Fleming BI 10/08/2017 Mary Fleming BI 10/08/2017 Mary Fleming BI 10/08/2017 Mary Fleming BI Chief Executive Deputy Chief Executive & Director of Finance Director of Operations & Performance Director of Nursing Director of Strategy & Planning Director of Workforce Medical Director Andrew Foster Rob Forster Mary Fleming Pauline Law Richard Mundon Alison Balson Sanjay Arya Provisional Positions Other (based on information still being validated) - 18 weeks, Diagnostics, Total Pay vs Budget, Clinical & Non Clinical Vacancy Rate and Cancer Date Printed/Run: 13/12/2017 Page 2 of 18
45 Objective Page(s) No Target Green Metrics Amber Metrics Red Metrics Total Metrics Highlights 1.1 : Harm Free 1.2 : Harm Free - Infections 2 : Mortality Performance against 18 weeks, diagnostics and cancer targets remains strong and the Trust remains in the top 10% in the country for 18 weeks and cancer. Still no grade 3/4 pressure ulcers year to date. Patient Experience Survey - discharge question improved by 29% from last month. 3.1 : Access : Access - Cancer : Access - Tumour Pathways : Access - A&E : Productivity - Part Lowlights 4.2 : Productivity - Part : Midwifery - Part : Midwifery - Part : Patient Experience - Part Continued pressures in unscheduled care continues to impact A&E, cancelled operations, stroke performance, theatre effectiveness and length of stay. 1 Never Event in November. Further 2 Clostridum Difficile cases, which took the Trust over the 19 trajectory, with 2 cases judged to be lapses in care. 6.2 : Patient Experience - Part : Workforce NHSI Total * Summary based on latest available data ~ RAG based on whether actual is achieving target 18 Weeks: Incomplete Cancer 62 Day: GP Referral Month Diagnostics: 6 Weeks A&E: 4 Hour Target C. Difficile Infections Year To Date Serious Falls Never Events MRSA 94.52% 96.30% 99.62% 73.11% Target: >=92.0% Target: >=85.0% Target: >=99.0% Target: >=95.0% YTD Target: 11 FY Target: 0 FY Target: 0 FY Target: 0 Date Printed/Run: 13/12/2017 Page 3 of 18
46 1.1 : Harm Free Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Min. Value Max. Value Period Harms: Total Serious Harms: Total Serious Harms: Number of Never Events Serious Harms: Number of Serious Falls Serious Harms: Grade 3-4 Pressure Ulcers Number of Serious Incidents Mod/Low Harms: Hospital Acquired Pressure Ulcer Grade 2 Mod/Low Harms: Number of Moderate Falls Mod/Low Harms: Safety Thermometer Mod/Low Harms: Settled Clinical Litigation Cases Mod/Low Harms: VTE Assessments (% of Admissions) ** 78 Nov Oct ** 7 Nov-17 5 Oct <=0 1 Nov-17 0 Oct <=0 0 Nov-17 0 Oct ** 0 Nov-17 0 Oct <=0 4 Nov-17 3 Oct ** 5 Nov-17 3 Oct <=0 1 Nov-17 3 Oct >=95.0% 98.00% Nov % Oct % 96.56% 99.73% ** 4 Nov-17 1 Oct >=90.0% 86.04% Nov % Oct % 76.34% 89.04% Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Commentary (Page Owner : Director of Nursing) *Threshold not confirmed **Threshold not confirmed ~ based on assumption During November there were four incidents which were reported to the Strategic Executive Information System (StEIS); one of which was a Never Event. Additionally, during November, there was a further Never Event but this was reported to STEIS in December and will feature in December s Serious Incident figures. During December there was a Never Event identified from October; this again will feature in December s figures. As at the 11th December, there have been 4 Never Events, year to date. Investigation teams are being established to look into these incidents and action plans will be developed thereafter. There were no breaches to the deadline date for submission to the Commissioners. The Safety Thermometer was undertaken on the 15th November patients were surveyed, of whom 2% had suffered harm whilst in hospital. 4 patients had a VTE, 1 patient had suffered a grade 2 pressure ulcer, 2 patients had suffered a fall with harm and 1 patient had contracted a CA-UTI. Date Printed/Run: 13/12/2017 Page 4 of 18
47 1.2 : Harm Free - Infections Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Min. Value Max. Value Period Infections/Bacteraemias: Total Serious Harms: Infections: Clostridium Difficile Serious Harms: Infections: Clostridium Difficile Lapses in Care Serious Harms: Infections: Central Line Serious Harms: Infections: Ventilator Acquired Pneumonia Infections: Catheter Associated Urinary Tract Serious Harms: Bacteraemias: MRSA Serious Harms: Bacteraemias: MRSA - Avoidable Cases Serious Harms: Bacteraemias: MSSA Serious Harms: Bacteraemias: E-coli Bacteraemias: Klebsiella Bacteraemias: Pseudomonas ** 8 Nov-17 7 Oct <=2 2 Nov-17 1 Oct <=0 0 Nov-17 0 Oct <=0 0 Nov-17 0 Oct <=0 0 Nov-17 0 Oct <=0 1 Nov-17 0 Oct <=0 0 Nov-17 0 Oct ** 0 Nov-17 0 Oct ** 2 Nov-17 1 Oct ** 2 Nov-17 3 Oct ** 1 Nov-17 1 Oct ** 0 Nov-17 1 Oct Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 May-17 Nov-16 Nov-16 Apr-17 Apr-17 Commentary (Page Owner : Director of Nursing) *Threshold not confirmed **Threshold not confirmed ~ based on assumption In November 17: 0 MRSA bacteraemia, 2 MSSA bacteraemia, 2 E. coli bacteraemia, 1 Klebsiella bacteraemia, 2 cases C.difficile diarrhoea. Year to date total for C.difficile = 21 cases, which has exceeded the annual reduction target of 19. Two cases judged as "lapses in care" to date. Numbers of other bacteraemia episodes remain low despite significant pressures in the system Date Printed/Run: 13/12/2017 Page 5 of 18
48 2 : Mortality Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Min. Value Max. Value Period Hospital Crude Death Rate Number of Hospital Deaths PFD Coroner Notifications Deaths after Readmission SHMI over rolling 12 months HSMR (Latest Month) HSMR (Latest YTD) HSMR Weekday HSMR Weekend ** 1.41% Nov % Oct % 1.30% 2.42% ** 103 Nov Oct ** 0 Nov-17 1 Oct ** 28 Nov Oct <= Mar Dec-16 N/A <= Aug Jul-17 N/A * Aug Jul-17 N/A <= Aug Jul-17 N/A <= Aug Jul-17 N/A Nov-16 Nov-16 Nov-16 Nov-16 Dec-15 to Mar-17 Nov-16 to Aug-17 Mar-17 to Aug-17 Nov-16 to Aug-17 Nov-16 to Aug-17 Commentary (Page Owner : Medical Director) *Threshold not confirmed **Threshold not confirmed ~ based on assumption This month s Mortality Data is very similar to last months. We remain around the average HSMR for the country an improvement from previously. SHMI remains high, but reflects a different, earlier time period. We are able to make predictions about the mortality rates for the months through to November. They will also be average or below average. Crude death rates have been relatively low through these months and the admission rates have been high. Date Printed/Run: 13/12/2017 Page 6 of 18
49 3.1 : Access Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Access: 18 Weeks Referral To Treatment Incomplete Pathway Access: Referral to Treatment over 52 weeks wait >=92.0% 94.52% Nov % Oct % 94.52% 96.05% Min. Value <=0 1 Nov-17 1 Oct Max. Value Period Nov-16 Nov-16 Outpatients: Backlog of Follow Ups Stroke - High Risk TIA Patients Treated within 24 Hrs Stroke - Stroke Patients spending 90% of their Hospital Stay on a Stoke unit Diagnostics: Patients waiting over 6 weeks ** 10,615 Nov-17 10,622 Oct-17 N/A 8,992 10,779 >=60.0% 72.00% Nov % Oct % 50.00% 88.89% >=80.0% 77.14% Oct % Sep % 75.00% 85.37% >=99.0% 99.62% Nov % Oct % 97.61% 99.62% Nov-16 Nov-16 Nov-16 to Oct-17 Nov-16 Commentary (Page Owner : Director of Operations & Performance) *Threshold not confirmed **Threshold not confirmed ~ based on assumption All three clinical divisions continue to achieve the 18-week incomplete target in November, despite continued pressures in unscheduled care. In order to help alleviate bed pressures all overnight routine elective cases were cancelled for a two-week period which has impacted specific specialties. The patient who is reported over 52 weeks which was also reported in the previous month will continue to be reported until the patient has their treatment on their chosen date in January. Unfortunately, we did not achieve the 80% stroke target due to two patients not moving to a stroke ward due to continued bed pressures. Yet another strong month for Radiology, with a month end radiology diagnostics position of only 8 patients waiting beyond 6 weeks, an excellent performance considering the volume of activity undertaken by this service. Date Printed/Run: 13/12/2017 Page 7 of 18
50 3.2 : Access - Cancer Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Two week wait from referral to date first seen: all urgent cancer referrals (cancer suspected) Two week wait from referral to date first seen: symptomatic breast patients (cancer not initally suspected) All Cancers: 31 day wait for diagnosis to first treatment All Cancers: 31 day wait for second or subsequent treatment: anti cancer drug treatments All Cancers: 31 day wait for second or subsequent treatment: surgery All Cancers: 62 Day Cancer Standard Treated - Pre Allocation All Cancers: 62 day wait for first treatment from urgent GP referral to treatment All Cancers: 62 day wait for first treatment from consultant screening service referral >=93.0% 97.44% Nov % Oct % 95.65% 99.19% >=93.0% 97.60% Nov % Oct % 93.52% 97.60% Nov-16 Nov-16 >=96.0% % Nov % Oct % 98.92% % Nov-16 >=98.0% % Nov % Oct % % % Nov-16 >=94.0% % Nov % Oct % % % Nov-16 ** 95.41% Nov % Oct % 92.31% % Nov-16 >=85.0% 96.30% Nov % Oct % 85.23% 98.15% Nov-16 >=90.0% 96.55% Nov % Oct % 95.35% % Nov-16 Min. Value Max. Value Period Commentary (Page Owner : Director of Operations & Performance) *Threshold not confirmed **Threshold not confirmed ~ based on assumption All 14, 31 and 62-day Cancer Waiting times targets have been achieved for October Our 62-day performance remains consistent with over 90% of suspected cancer GP referrals, consultant upgrades and screening patients treated within 62 days. We have had 1.5 accountable breaches of the 62-day standard in October. These have been reviewed to identify the cause and where applicable make improvements. One of the breaches was mainly due to diagnostic delays and repeat tests that were required to gain a definitive diagnosis. The other was a shared breach with the treating trust which was patient choice to be treated beyond day 62. Date Printed/Run: 13/12/2017 Page 8 of 18
51 3.3 : Access - Tumour Pathways Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Min. Value Max. Value Period Cancer - Breast 62 Day Wait Cancer - Colorectal 62 Day Wait Cancer - Gynaecology 62 Day Wait Cancer - Haematology 62 Day Wait Cancer - Head & Neck 62 Day Wait Cancer - Lung 62 Day Wait Cancer - Skin 62 Day Wait Cancer - Upper GI 62 Day Wait Cancer - Urology 62 Day Wait >=85.0% % Oct % Sep % % % Nov-16 to Oct-17 >=85.0% % Oct % Sep % 60.00% % Nov-16 to Oct-17 >=85.0% % Oct % Sep % 55.56% % Nov-16 to Oct-17 >=85.0% % Oct % Sep % 0.00% % Nov-16 to Oct-17 >=85.0% 33.33% Oct % Sep % 33.33% % Nov-16 to Oct-17 >=85.0% % Oct % Sep % 60.00% % Nov-16 to Oct-17 >=85.0% % Oct % Sep % % % Nov-16 to Oct-17 >=85.0% % Oct % Sep % 40.00% % Nov-16 to Oct-17 >=85.0% 92.31% Oct % Sep % 83.33% % Nov-16 to Oct-17 Commentary (Page Owner : Director of Operations & Performance) *Threshold not confirmed **Threshold not confirmed ~ based on assumption All 14, 31 and 62-day Cancer Waiting times targets have been achieved for October Our 62-day performance remains consistent with over 90% of suspected cancer GP referrals, consultant upgrades and screening patients treated within 62 days. We have had 1.5 accountable breaches of the 62-day standard in October. These have been reviewed to identify the cause and where applicable make improvements. One of the breaches was mainly due to diagnostic delays and repeat tests that were required to gain a definitive diagnosis. The other was a shared breach with the treating trust which was patient choice to be treated beyond day 62. Date Printed/Run: 13/12/2017 Page 9 of 18
52 3.4 : Access - A&E Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart 4 Hour A&E Breach Performance % (inc GP Streaming Activity) Number of A&E Attendances >=95.0% 73.11% Nov % Oct % 73.11% 92.66% Min. Value ** 6,959 Nov-17 7,460 Oct-17 59,435 6,604 7,796 Max. Value Period Nov-16 Nov-16 Average Daily A&E Attendances A&E Attendances: Out of Area NWAS: Conveyances from Care Homes A&E Attendances that result in an admission A&E Attendances: % Result in Admissions - Aged 75+ ** Nov Oct ** 865 Nov Oct-17 7, ** 312 Oct Sep-17 2, * 2,201 Nov-17 2,291 Oct-17 17,609 1,761 2,291 * 31.08% Nov % Oct % 28.72% 34.34% Nov-16 Nov-16 Nov-16 to Oct-17 Nov-16 Nov-16 Commentary (Page Owner : Director of Operations & Performance) *Threshold not confirmed **Threshold not confirmed ~ based on assumption Despite a reduction in the number of attendances to A&E, the position in November worsened when compared with the previous month. Performance for the Trust at 73.11% remains significantly lower than expected, and is 81.37% when including the Leigh Walk-in Centre activity. An intensive program of work is ongoing in order to refine the Health Information system in and work is also ongoing to ensure flow from A&E to inpatient areas is efficient as possible and bed capacity meets demand. Although the out of area attendances have seen a reduction they have not returned to levels seen prior to pressures in neighbouring Trusts. Date Printed/Run: 13/12/2017 Page 10 of 18
53 4.1 : Productivity - Part 1 Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Min. Value Max. Value Period Hospital Cancelled OP Appointments % Hospital Cancelled OP Appointments < 6 weeks Cancelled Operations % Cancelled Operations: 2nd Urgent Hospital Average Spell Length of Stay (Elective Inpatient) Average Spell Length of Stay (Non Elective) Delayed Transfers of Care Delayed Transfer of Care Days <=5.0% 6.94% Nov % Oct % 5.97% 7.87% <=0.0% 5.40% Nov % Oct % 4.67% 6.13% <=0.8% 1.71% Nov % Oct % 1.17% 2.65% <=0 0 Nov-17 0 Oct * 3.8 Days Nov Days Oct Days 3.0 Days 3.8 Days * 3.7 Days Nov Days Oct Days 3.4 Days 5.0 Days ** 42 Nov Oct ** 138 Nov Oct-17 1, Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Feb-17 Feb-17 Commentary (Page Owner : Director of Operations & Performance) *Threshold not confirmed **Threshold not confirmed ~ based on assumption There has been a slight improvement in patients having their outpatient appointments cancelled. There are a variety of reasons why appointments are cancelled and this will include appointments brought forward or booked into a more appropriate clinic. We have however seen an increase in the number of operations cancelled which is representative of the pressures in unscheduled care and D&V outbreak on the Wrightington site. The average length of stay for elective patients in Surgery reduced to 1.3 days in November, as a result of cancelling inpatient cases to help ease the bed pressures. Average Length of Stay for Primary joint replacement is static at 4 days. Projects are underway to improve the provision of Enhanced Recovery to further reduce Length of Stay. Date Printed/Run: 13/12/2017 Page 11 of 18

54 4.2 : Productivity - Part 2 Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Min. Value Max. Value Period Theatre Effectiveness % - Total Theatre Effectiveness % - RAEI Theatre Effectiveness % - Wrightington Theatre Effectiveness % - Leigh >=70.0% 62.05% Nov % Oct-17 N/A 60.83% 67.00% >=70.0% 57.19% Nov % Oct-17 N/A 52.00% 61.86% >=70.0% 64.81% Nov % Oct-17 N/A 63.52% 74.00% >=70.0% 57.39% Nov % Oct-17 N/A 47.80% 57.39% Nov-16 Nov-16 Nov-16 Nov-16 Commentary (Page Owner : Director of Operations & Performance) *Threshold not confirmed **Threshold not confirmed ~ based on assumption Theatre effectiveness across the RAEI and Wrightington sites is lower than the previous month, primarily due to a high number of on the day cancellations due to continued pressures in unscheduled care and a D&V outbreak on the Wrightington site. The Leigh site remained unaffected and saw a slight increase in theatre effectiveness, this is expected to increase in January when an additional theatre closes. Date Printed/Run: 13/12/2017 Page 12 of 18
55 5.1 : Midwifery - Part 1 Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Min. Value Max. Value Period Maternity: Midwife / Birth Ratio Maternity: Skills drills/2 day Mandatory Training Attendance Maternity: Total monthly bookings Maternity: Booked by 12+6 Weeks Maternity: Induction of Labour Maternity: Normal Deliveries Maternity: Water Births Maternity: Instrumental Deliveries Maternity: Elective Caesarean Sections Maternity: Emergency / Non Elective Caesarean Sections Maternity: Total Caesarean Sections <= Nov Oct-17 N/A >=88.0% 82.51% Nov % Oct-17 N/A 0.00% 96.00% >= Oct Sep-17 1, >=90.0% 89.43% Oct % Sep-17 N/A 87.61% 97.15% <=30.0% 32.21% Nov % Oct-17 N/A 29.46% 40.50% >=60.0% 58.92% Nov % Oct-17 N/A 56.67% 69.26% >=8 10 Nov Oct <=10.0% 11.61% Nov % Oct-17 N/A 6.56% 16.22% <=15.0% 7.46% Nov % Oct-17 N/A 7.46% 16.74% <=17.0% 21.16% Nov % Oct-17 N/A 12.74% 21.16% <=27.0% 28.62% Nov % Oct-17 N/A 24.18% 30.74% Nov-16 Nov-16 Nov-16 Nov-16 to Oct-17 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Commentary (Page Owner : Director of Nursing) *Threshold not confirmed **Threshold not confirmed ~ based on assumption There has been an increase in bookings, however, the number of births has remained within the target parameters. The midwife to birth ratio based on Birth rate + is at 1:29 and below the 1:28 recommendations. The Induction Of Labour rate remains consistently high due to the thresholds of the reduced fetal movements /fetal growth pathways. A Regional review of the reduced fetal movement pathway is currently in progress. Date Printed/Run: 13/12/2017 Page 13 of 18
56 5.2 : Midwifery - Part 2 Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Min. Value Max. Value Period Maternity: Total Births Maternity: Episiotomy with normal birth Maternity: 3rd/4th degree tears Maternity: Initiation of breastfeeding Maternity: Average post-natal length of stay Maternity: Still Births (>24 weeks) Maternal Readmissions within 30 Days Maternal admissions to ICU Maternity Complaints Maternity: New Claims >= Nov Oct-17 1, <=6.0% 4.22% Nov % Oct-17 N/A 2.63% 9.16% <=3.0% 0.83% Nov % Oct-17 N/A 0.47% 2.64% >=55.0% 50.04% Nov % Oct-17 N/A 48.79% 54.87% <= Nov Oct-17 N/A <=1 0 Nov-17 0 Oct <=5 2 Nov-17 1 Oct <=2 3 Nov-17 1 Oct <=2 1 Nov-17 3 Oct * 0 Nov-17 0 Oct Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 Dec-16 Commentary (Page Owner : Director of Nursing) *Threshold not confirmed **Threshold not confirmed ~ based on assumption Booking by 12+6 weeks gestation remains below 90% for the third consecutive month. A full review is in progress to explore reasons and for us to address accordingly. There are no known issues with clinic booking capacity. The total caesarean section rate has increased in November. However, there has been significant reduction of 5.28% in elective caesarean sections. Three quarters of the total caesarean sections have been emergency deliveries. There has been a decrease of 4.61% in instrumental births. A further increase of 1.4% in the initiation of breast feeding is noted, however, it is still below the Trust target of 55%. Continued work to promote breast feeding initiation and maintenance is ongoing supported by the infant feeding team. Mandatory training has exceeded the planned trajectory for 2 consecutive months with continued plans to increase training compliance that will address the deficits from previous months. Date Printed/Run: 13/12/2017 Page 14 of 18
57 6.1 : Patient Experience - Part 1 Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Min. Value Max. Value Period Number of Complaints Upheld by Ombudsman ** 0 Nov-17 0 Oct Nov-16 Percentage of Complaints Responded to on Time RTPS: Did you find someone to talk to about your worries and fears? RTPS: Do you know which Doctor/Consultant is treating or looking after you? RTPS: Do you think the hospital staff did everything they could to help control your pain? RTPS: During your stay have you been treated with compassion by the hospital staff? RTPS: Has there been healthy food on the hospital menu? RTPS: Have staff treating and examining you introduced themselves? RTPS: Have you always had access to a call bell when you needed it? RTPS: Have you been given enough privacy when being examined treated or discussing your care? ** 66.67% Nov % Oct % 48.48% 92.00% >=90.0% 88.00% Nov % Oct % 88.00% 97.22% >=90.0% 76.00% Nov % Oct % 76.00% 90.71% >=90.0% 90.00% Nov % Oct % 90.00% 98.40% Nov-16 Nov-16 Nov-16 Nov-16 >=90.0% 96.00% Nov % Oct % 96.00% % Nov-16 >=90.0% 94.00% Nov % Oct % 87.10% 97.73% >=90.0% 98.00% Nov % Oct % 88.64% 99.26% >=90.0% 94.00% Nov % Oct % 93.50% 99.40% Nov-16 Nov-16 Nov-16 >=90.0% 92.00% Nov % Oct % 92.00% % Nov-16 Commentary (Page Owner : Director of Nursing) *Threshold not confirmed **Threshold not confirmed ~ based on assumption During November, 20 out of the 30 complaint responses were sent within the timescales agreed with the complainant at the start of the complaints process (67%), representing a decrease in performance when compared with last month. No reports were issued by the Parliamentary Health Service Ombudsman (PHSO). Comprehensive, open and transparent responses to complainants are incredibly important and improve patient experience and satisfaction. For Real Time Patient Survey commentary, please see overleaf. Date Printed/Run: 13/12/2017 Page 15 of 18
58 6.2 : Patient Experience - Part 2 Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart RTPS: Have you been given the care you felt you required when you needed it most? RTPS: Have you been involved as much as you wanted to be about your discharge home? RTPS: Have you been involved as much as you wanted to be in decisions about your care and treatment? RTPS: Have you been offered a choice of food during your stay? RTPS: If your family or someone else close to you wanted to talk to a doctor did they have enough opportunity to do >=90.0% 88.00% Nov % Oct % 88.00% % Nov-16 >=90.0% 88.00% Nov % Oct % 55.88% 88.00% >=90.0% 84.00% Nov % Oct % 82.17% 95.17% >=90.0% 96.00% Nov % Oct % 95.00% 99.24% >=90.0% 96.00% Nov % Oct % 88.82% 96.00% Min. Value Max. Value Period Nov-16 Nov-16 Nov-16 Nov-16 Commentary (Page Owner : Director of Nursing) *Threshold not confirmed **Threshold not confirmed ~ based on assumption In relation to the Real Time Patient Survey, the discharge question improved significantly (29.09%), the highest score recorded for this metric. On the whole, the results for November on average have decreased slightly with 8 out of 13 questions decreasing, including privacy and dignity which had previously been at 100%. Three of the larger decreases in scores were pain control, being given the care and treatment required when the patient felt they needed it most (both have previously scored well) and knowledge of which consultant is currently treating you. Date Printed/Run: 13/12/2017 Page 16 of 18
59 7 : Workforce Latest Previous YTD Sparkline - Latest 13 Months Metric Title Target Actual Period RAG Trend Actual Period Actual RAG Chart Min. Value Max. Value Period Agency vs NHSI Ceiling Friends & Family Test - Recommendation as place for treatment Friends & Family Test - Recommendation as place to work Total Pay vs Budget Clinical & Non Clinical Overall Vacancy Rate Sickness absence - Total Quarterly Engagement Score Appraisals over rolling 12 months Job Plan Compliance over rolling 12 months Mandatory Training over rolling 12 months <= 457 k 474 k Nov k Oct-17 3,100 k 298 k 615 k >=80.0% 83.11% Nov % Oct-17 N/A 80.55% 83.33% >=75.0% 73.78% Nov % Oct-17 N/A 70.83% 75.99% <= 0 k 1,676 k Nov-17 1,270 k Oct-17 7,773 k -25 k 1,676 k <=4.5% 6.23% Nov % Oct % 2.62% 7.31% <=4.0% 4.44% Oct % Sep % 3.77% 4.69% >= Nov Oct-17 N/A >=90.0% 92.19% Nov % Oct-17 N/A 87.10% 92.19% >=100.0 % 11.19% Nov % Oct-17 N/A 11.19% 20.59% >=95.0% 96.63% Nov % Oct-17 N/A 95.10% 96.70% Nov-16 Jan-17 Jan-17 Nov-16 Dec-16 Nov-16 to Oct-17 Nov-16 Nov-16 Nov-16 Nov-16 Commentary (Page Owner : Director of Workforce) *Threshold not confirmed **Threshold not confirmed ~ based on assumption Rolling 12-month sickness from Nov 16 - Oct 17 has increased marginally to 4.23% (compared to 4.21% last reported). The in-month sickness for Oct 17 has also increased to 4.44% (from 3.98% last reported). Temporary spend in Nov 17 has increased to 1,453k from 1,211k in Oct 17 (an increase of 242k). The results of the October 2017 Staff Engagement Quarterly Pulse Check highlights an increased level of engagement within the Trust since the previous quarter. Date Printed/Run: 13/12/2017 Page 17 of 18
60 NHSI Metrics Latest Previous YTD Sparkline - Latest 13 Months MetricTitle Target Actual Period RAG Trend Actual Period Actual RAG Chart 4 Hour A&E Breach Performance % (inc GP Streaming Activity) Access: 18 Weeks Referral To Treatment Incomplete Pathway Diagnostics: Patients waiting over 6 weeks Two week wait from referral to date first seen: all urgent cancer referrals (cancer suspected) Two week wait from referral to date first seen: symptomatic breast patients (cancer not initally suspected) All Cancers: 62 Day Cancer Standard Treated - Pre Allocation All Cancers: 62 day wait for first treatment from urgent GP referral to treatment All Cancers: 62 day wait for first treatment from consultant screening service referral Serious Harms: Infections: Clostridium Difficile Serious Harms: Infections: Clostridium Difficile Lapses in Care >=95.0% 73.11% Nov % Oct % 73.11% 92.66% >=92.0% 94.52% Nov % Oct % 94.52% 96.05% >=99.0% 99.62% Nov % Oct % 97.61% 99.62% >=93.0% 97.44% Nov % Oct % 95.65% 99.19% >=93.0% 97.60% Nov % Oct % 93.52% 97.60% Nov-16 Nov-16 Nov-16 Nov-16 Nov-16 ** 95.41% Nov % Oct % 92.31% % Nov-16 >=85.0% 96.30% Nov % Oct % 85.23% 98.15% Nov-16 >=90.0% 96.55% Nov % Oct % 95.35% % Nov-16 Min. Value <=2 2 Nov-17 1 Oct <=0 0 Nov-17 0 Oct Max. Value Period Nov-16 Nov-16 The updated Single Oversight Framework has been published, this will be reviewed and metrics developed accordingly. *Threshold not confirmed **Threshold not confirmed ~ based on assumption Date Printed/Run: 13/12/2017 Page 18 of 18
61 Unscheduled Care update
62 A&E Performance and Patient Flow Pressures: November 17 Update Introduction This report has been produced to outline the August 2017 performance and highlight any actions intended to either maintain or improve patient flow. November 2017 Summary Performance The graph indicates the 4 hour A&E performance for the month of November 2017 which was 73.11% and 81.37% with the Walk in Centre included WWL is currently ranked 4 th in Greater Manchester Year to Date with 86.69% including type 3 activity. Overview of November Performance A&E performance in November was below the trajectory agreed by NHSI for quarter 3 (92%) and shows deterioration against October performance. Week Ending AE Breach Total Breach (inc WIC) 05/11/ % 83.22% 12/11/ % 82.09% 19/11/ % 86.39% 26/11/ % 80.12% The service continues to experience considerable pressures due to a number of factors including the Implementation of the HIS system, increased patient acuity, an increase in the number of stranded patients and nursing staff shortages on the wards which impacts on flow. The implementation of the HIS system has continued to put additional pressure on the A&E department and there has been a marked increase in the length of time that patients are waiting to see a doctor which is having a direct impact on the number of patients who are waiting in the department for longer than 4 hours. The graph below shows that the average length of time to be seen by a doctor has increased by approximately 75 minutes which is primarily due to the increased time taken to see a patient and input the clinical records electronically.
63 Spike due to PAS downtime backloading HIS launched in week 42 The number of Ambulances presenting in A&E has increased slightly on the previous month (2455 vs 2715) however we have seen a reduction in the percentage of patients admitted to hospital following an arrival to A&E by Ambulance ( 51.6% vs 55.2%) We also saw a 6% increase in the number of patients presenting in A&E aged 70 and Over. We have seen an increase in the number of patients who have a length of stay over seven days which has impacted on bed availability and flow from A&E. This could be in part attributed to the increase in the number of Elderly patients presenting in A&E. We have also continued to experience nurse staffing gaps on wards and assessment areas which has continued to impact on flow and the ability to consistently facilitate timely handovers Actions The current pressures within A&E are multi factorial and require a whole system approach to improve the current position. The Division of Medicine has formulated a recovery plan with the support of the Executive Team and system wide partners in order to address the issues highlighted in this report. This recovery plan is monitored on a weekly basis within the Division and with Executive presence at the Weekly Divisional Comm-cell and it is also part of a system wide action plan which is being monitored by the CCG through the System Resilience Operation Group (SROG). The recovery plan is attached to this report for reference and to provide assurance of actions being taken to improve the current position. Microsoft Excel Worksheet Recommendations The committee is asked to note this report..
64
65 Unscheduled Care: The Headlines Business Intelligence December 2017

66 A&E Performance WWL v National and GM From October 2016 WWL performance dipped to match the national average having outperformed it every month since December As A&E performance has fallen, HSMR figures have worsened. WWL performance has dropped below both the national and GM performance for the first time in October by 6.56%, November performance is also low
67 A&E attendances A&E Attendances are fairly static, however the number of breaches has continued to rise paediatric breaches Mid Nov higher than whole of October and increasing

68 Patient Arrival to Patient Seen (Apr-Nov 2017). October tale of two halves % with 3 consecutive days over 95%... Second half 69.8%... Excluded all patients breaching by 75 minutes.. 87% and 90.2% WIC as opposed to 84.94% and 89% WIC
69 Admissions through A&E There has been an increase in admissions, the primary diagnosis are within mental health related, abdominal pain and chest pain.

70 Ambulance arrivals For the period April to November 2017 there were an additional 813 ambulance arrivals compared to the same period in
71 A&E attendances ambulance arrival and handover times Ambulance handover times between minutes and over 60 minutes have almost tripled during November 17, however November figures are indicative until NWAS publish their final figures, so may change.
72 Out of Area Patients The number of out of area patients attending A&E increased in March A&E attendance levels, although having a slight reduction in recent months, remain significantly high compared with previous years. The number of A&E attendances resulting in admission for out of area patients increased correspondingly. Recent months admissions remain high.
73 Ageing Population Year on year there continues to be an increase in attendances for patients aged 75 and above. There has been a corresponding increase in admissions compared to 2015/16.
74 Longer Stays for Medical Patients An additional 14 Medicine beds were in use each day for non-elective admissions during compared with (based on average length of stay and number of admissions). This is largely the result of the increase in length of stay from Medicine patients (including the increase in older patients) N.B. Data is for RAEI only and includes Paediatric and Maternity Spells
75 Average Non-Elective Length of Stay (Dr Foster Data)
76 Beds per 1000 Population GM Trusts, Available General & Acute beds as at compared with population served 1, ,000 1, , , , , , , , ,000 - CENTRAL MCR UNI HOSPITALS NHS FT SALFORD ROYAL NHS FT TAMESIDE HOSPITAL NHS FT BOLTON NHS FT UNI HOSPITAL OF SOUTH MCR NHS FT WRIGHTINGTON, PENNINE ACUTE WIGAN AND LEIGH HOSPITALS NHS FT NHS FT STOCKPORT NHS FT - G&A Beds as at ** Population from CCG Jan 17
77 Summary A&E performance dropped below both national and GM levels for the first time in October 17 and has continued along this trend A&E attendance levels remain static overall Breaches have increased, as have ambulance arrivals and handover times - times between minutes and over 60 minutes have almost tripled, reflective of a congested ECC. Admissions via A&E have increased across all age groups, mainly 75+ patients Dr Foster non elective data shows general medicine (highest volume of spells) LOS below expected in general, for shorter stay patients. 3 rd Lowest bed base per 1000 population in GM
78
79 REPORT AGENDAA ITEM: 8.3 To: Board of Directors Date: 20 December 2017 Subject: Finance report for November Presented by: Deputy Chief Executive Purpose: For report Executivee summary The finance report is presented to the Board of Directors to provide an overview of the financial performance during November Risks associated with this report One of the organisation s corporate objectives is to achieve two-year budget stability. This report outlines the risk to achievement of this objective. Link(s) to The WWL Way 4wards Patients Performance People Partnerships
80
81 Finance report
82 Finance Report Month 8 Contents Executive Summary... 3 Capital Expenditure & Statement of Financial Position... 3 Cash, Liquidity and UOR... 3 Appendix 1 I&E Summary... 4 Appendix 2 Statement of Financial Position... 5 Appendix 3 Cash Flow Statement... 6 Page 2 of 6
83 Finance Report Month Executive Summary The Trust is reporting a year to date trading deficit (pre impairments) of 3.3m which is 1.9m worse than plan. In Month Year to Date Key Metrics Actual Plan Var Actual Plan Var UOR 2 1 (1) 3 2 (1) Operating Surplus / (Deficit) (459) (3,309) (1,415) (1,894) Capital Expenditure (3) 3,247 4,458 1,211 Cash 11,085 5,984 5,101 11,085 5,984 5, After impairments the Trust is reporting a technical deficit of 4.4m which is 3.0m behind plan. Cumulative income of 197.1m is 5.6m better than plan. Cumulative expenditure is 200.4m which is 7.5m worse than plan. The UOR rating for the Trust in month is a 2 which is behind the plan of 1. The Income & Expenditure summary can be seen at Appendix Capital Expenditure & Statement of Financial Position The Trust has spent 3.2m on capital expenditure versus planned expenditure of 4.4m. The statement of financial position can be found in Appendix Cash, Liquidity and UOR The cash balance is 11.1m, which is 5.1m higher than the planned balance. The UOR rating is a 2 against a plan of 1. YTD the UOR rating is a 3 against a plan of 2. The cash flow statement can be found in Appendix 3. Page 3 of 6
84 Finance Report Month 8 Appendix 1 I&E Summary In Month Year to Date Actual Plan Var Actual Plan Var Income A & E Attendances ,620 7,700 (79) Daycase 2,863 2,987 (124) 22,076 22,937 (861) Elective 2,399 2,764 (365) 20,391 21,247 (856) Non Electives 5,021 4, ,712 37,129 2,583 Outpatients 3,721 3,927 (206) 28,400 30,174 (1,773) Other** 11,275 9,380 1,895 78,896 72,334 6,562 Total Income 26,257 24,657 1, , ,521 5,575 Operating Expenses Pay (16,945) (15,425) (1,520) (131,040) (124,902) (6,138) Non Pay (8,659) (8,040) (619) (66,995) (64,659) (2,335) Reserves 0 (75) 75 0 (981) 981 Total Operating Expenses (25,604) (23,540) (2,065) (198,035) (190,542) (7,493) EBITDA 653 1,117 (464) (940) 978 (1,918) EBITDA % 2.5% 4.5% (2.0)% (0.5)% 0.5% (1.0)% Non Operating Expenses (294) (299) 5 (2,369) (2,393) 24 Surplus / (Deficit) (459) (3,309) (1,415) (1,894) Surplus / (Deficit )% 1.4% 3.3% (2.0)% (1.7)% (0.7)% (0.9)% Impairment (19) 0 (19) (1,061) 0 (1,061) Tech Surplus/ Def (478) (4,370) (1,415) (2,955) Page 4 of 6
85 Finance Report Month 8 Appendix 2 Statement of Financial Position Opening '000 In Month - '000 Movement to previous month - '000 Full Year '000 Actual Actual Plan Variance Last month Movement Plan Non-current assets 148,658 Property, plant and equipment 146, ,813 (26,014) 146,893 (94) 173,408 2,413 Intangibles 1,788 1,849 (61) 2,003 (215) 1, Trade and other non-current receivables (63) 735 (373) , , ,087 (26,138) 149,631 (682) 175,429 Current assets 4,121 Inventories 4,364 4,810 (446) 4, ,810 25,230 Trade and other receivables 20,112 17,228 2,884 17,960 2,152 11,886 11,669 Cash and cash equivalents 11,085 5,984 5,101 10, ,209 41,020 35,561 28,022 7,539 32,925 2,636 24, ,260 Total assets 184, ,109 (18,599) 182,556 1, ,334 Current liabilities (28,711) Trade and other payables (26,911) (27,537) 626 (25,351) (1,560) (25,977) (4,420) Borrowings (4,421) (2,538) (1,883) (4,421) 0 (2,538) (329) Provisions (338) (1,361) 1,023 (367) 29 (1,517) (1,535) Other liabilities (1,942) (2,031) 89 (1,860) (82) (2,031) (34,995) (33,612) (33,467) (145) (31,999) (1,613) (32,063) 6,025 Net current assets/(liabilities) 1,949 (5,445) 7, ,023 (7,158) 157,265 Total assets less current liabilities 150, ,642 (18,744) 150, ,271 Non-current liabilities (25,819) Borrowings (23,545) (25,377) 1,832 (23,545) 0 (23,279) (3,154) Provisions (2,927) (2,820) (107) (2,927) 0 (2,820) (300) Other liabilities (150) (150) 0 (150) 0 (150) (29,273) (26,622) (28,347) 1,725 (26,622) 0 (26,249) 127,992 Total assets employed 124, ,295 (17,019) 123, ,022 Financed by Taxpayers' equity 95,806 Public dividend capital 96,456 95, , ,806 22,823 Revaluation reserve 22,823 32,410 (9,587) 22, ,410 9,363 Retained earnings 4,997 13,079 (8,082) 4, , ,992 Total taxpayers' equity 124, ,295 (17,019) 123, ,022 Page 5 of 6
86 Finance Report Month 8 Appendix 3 Cash Flow Statement Full Year - '000 Actual Plan Variance Actual Plan Variance Plan Opening cash 10,795 3,359 7,436 11,669 9,422 2,247 9,422 Operating activities Technical surplus / (deficit) (476) (4,370) (1,416) (2,954) (687) Net interest accrued (5) (5) 384 PDC dividend expense (83) 2,103 2,768 (665) 4,153 Unwinding of discount (3) 48 Operating surplus / (deficit) per annual accounts 634 1,198 (564) (1,983) 1,644 (3,627) 3,898 Depreciation and amortisation (42) 4,691 5,179 (488) 7,767 Impairments / (impairment reversals) , ,061 0 (Gain) / loss on disposal (19) 0 (19) 0 Non cash donations/grants credited to income 0 (10) 10 (26) (80) 54 (120) Changes in working capital (Inc)/Dec in Inventories (194) 0 (194) (243) 0 (243) 0 (Inc)/Dec in trade & other receivables (1,775) 961 (2,736) 4,566 (3,314) 7,880 2,033 Inc/(Dec) in trade & other payables 1, ,160 (1,880) 1,919 (3,799) 1,100 Inc/(Dec) in other liabilities Inc/(Dec) in provisions (33) 35 (68) (249) 281 (530) 422 Other movements in operating cash flows Investing activities Interest received Purchase of non-current assets (315) (312) (3) (3,247) (4,458) 1,211 (7,330) Proceeds from sale of equipment Financing activities In Month - '000 Year to Date - '000 Public dividend capital received Loans received from ITFF Other loans received Loan principal repaid (2,397) (2,324) (73) (4,422) Interest paid (219) (229) 10 (438) PDC dividend paid (1,715) (2,076) 361 (4,153) Total net cash inflow / (outflow) 290 2,625 (2,335) (584) (3,438) 2,854 (1,213) Closing cash 11,085 5,984 5,101 11,085 5,984 5,101 8,209 Page 6 of 6
87 REPORT AGENDAA ITEM: 8.4 To: Board of Directors Date: 20 December 2017 Subject: Board Assurance Framework Presented by: Trust Secretary Purpose: Approval Executivee summary The Board Assurance Framework is presented to the Board of Directors D forr approval. Risks to the delivery of corporate objectives have been scored by the relevant Sub-Committees. Executive Directors have reviewed those risks that could not be scored by the overseeing Committee. Risks associated with this report As described within the Board Assurance Framework. Link(s) to The WWL Way 4wards Patients Performance People Partnerships
88
89 Quality Corporate Objective: Board Assurance Framework To deliver safe, high quality, effective, evidence-based patient Lead Director: care P Law, Director of Nursing / S Arya, Medical Directorr Responsible Monitoring Committee: Quality & Safety Measurement Mortality; compliance with 10 DNACPR Always Events; reduction in moderate and serious falls; reduction in hospital acquired infections; development of a metric to measuree Right Patient Right Ward; Development of ward accreditation system; reduce avoidable harms measures through a reduction in SI s theatre effectiveness; accurate and validated SLR figures; prioritise in terms of short, medium and long term, implement choose wisely UK campaign with 100% adherence; reduce unnecessary investigations by 10%, interventions by 10% and prescription drugs by 10% What does the objective mean? To deliver safe, high quality, effective, evidence-basedd patient care Impact of not achieving Unsafe, poor quality care, regulatory enforcement; increase in STEIS reportable incidents (serious incidents), complaints and clinical claims, poor patient experience. the objective Key Risk Key Controls What are the key What Where we can gain risks to achieving this controls/systems are evidence or assurance corporate objective? currently in place to that our mitigate the risk? control/systems are effective? Failure to achieve an improved Weekly death audits HSMR/SHMI data and annual summary Trust Board benchmarked position for mortality identifying themes; Focussed Performance Report; Dr Foster Mortality improvements in Alerts; relation to Sepsis and AKI; Quarterly mortality reports to Quality and Mortality Framework Safety Committee. linking with the management of serious incidents; Joint project with the CCG reviewing deaths within 30 days of discharge; Assurance on controls Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Trust-wide mortality group Trust-wide understanding/ plan for areas requiring focus/improvement Month April May June Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Q&S Mortality data for the Trust was still high ; Na unscheduled care pressures had contributed to this position as well as the increased morbidity of patients and delays in transfers to care homes; a significant amount of internal work was being done including the establishment of a mortality group. The Committee agreed to retain the proposed opening score of 25 Q&S The Mortality Group would be meeting for Na the first time on The mortality data hadn t changed since the last meeting. It was agreed to retain the score at 25 Q&S The Committee had received and noted the Na update from the Mortality Working Group
90 Key Risk What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Failure to achieve an improved benchmarked position for mortality cont. Key Controls System to review deaths of patients with a learning disability. Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S and had taken assurance that appropriate action and discussions were taking place. However, there remained concerns around the mortality data and it was agreed to retain the score at 25 July August Q&S The Medical Director reported that theree Na had been a reduction in hospital mortality during May and June. It was anticipated that this trajectory would continue into July. The Committee noted that discussions with external organisations and the work of the Mortality Working Group continued. The Committee agreed to retain the score at 5 x 5 = 25 pending confirmation that the improving trajectory continued ECC ECC reviewed the risk and agreed that this Na could be reduced to 5 x 4 = Sept Oct Q&S Mortality group meetings, attended by Na external stakeholders, continued to be held with focus on outlying areas. The number of deaths in hospital had reduced but there was further improvement to be made. Concerns around the use of disparate sets of data had been raised at Clinical Commissioning Group (CCG) and Medical Director level across the region. The Committee agreed to retain the score at 5 x 4 = 20 Q&S The Committee reflected on the update provided by the Associate Medical Director which had advised that the HSMR and SHMI positions remained unchanged. However, it had been noted that the number 5of deaths in hospital had increased. The
91 Key Risk What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Failure to achieve an improved benchmarked position for mortality cont. Key Controls Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Committee agreed to retain the score at 5 x 4 = 20 Nov Dec Jan Feb March Q&S Th Q&S Th he Committee reflected on the earlier discussion with the Medical Director around Mortality and the improvements noted in relation to HSMR. It was agreed to retain the score at 5 x 4 = 20 until a sustained position was seen. he Committee reflected on the improvements that had been seen around HSMR but agreed that it would be appropriate to retain the current score due to winter pressures
92 Key Risk What are the key risks to achieving this corporate objective? Failure to achieve infection control trajectories Key Controls Infection control audits and follow up Deep clean schedule; PLACE Assessments Cleanest hospital for three years running. Assurance on controls What Where we can gain Potential areas of controls/systems are evidence or assurance weakness that may currently in place to mitigate the risk? that our control/systems are require additional controls/further effective? consideration? Infection control Numbers of CDT s; Benchmarking data team; MRSA; MSSA; e-coli with other infections Trust organisations Strategy and work- Board Performance plan; Report; Process for new reporting standards Infection Control Learning from infection Committee; investigations/ /scrutiny; Compliance issue with ANTT; System for infection Achievement of CDT investigations/ trajectory for Availability of side scrutiny; (19); rooms. No lapses in care. Gaps in Initial Target Control and or risk risk Assurance C L S C L S Month April May June Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Q&S As a consequence of the pressures on the hospital system, it was noted that infection rates had started to increase. The acuity and dependency of patients meant increased susceptibility to infection. There had been one CDT in April and a possible other case that was being investigated. There would need to be focus on maintaining the Trusts internal standards. The Committee agreed to retain the proposed opening score of 20 Q&S The Committee had received a paper from Na the Infection Control team. It was noted that the deep clean schedule had been postponed due to bed pressures. It was agreed to retain the score at 20 until the deep cleans could be commenced Q&S L Barkess Jones advised that this would be Na a very challenging year in terms of Infection Control. The Committee agreed to retain the score at 20 Na July Q&S The Director of Nursing reported that the Na deep clean scheduless were progressing as planned although these could be affected by bed pressures. The Committee agreed to retain the score at 5 x 4 = August ECC ECC reviewed the risk and agreed to retain Na the current score of
93 Key Risk What are the key risks to achieving this corporate objective? Failure to achieve infection control trajectories cont. Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Sept Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Q&S In consideration of the challenges outlined in discussions with regard to C diff infections, the Committee agreed to retain the score at 5 x 4 =20 Na Oct Nov Q&S It was noted that the Trust would be likely to breach the trajectory for C Diff infections in the year but lapses in care remained very low. The Committee agreed to retain the score at 5 x 4 =20. Q&S It was noted that the Trust would be certain to breach the trajectory for Clostridium Difficile infections in the year but lapses in care remained very low. The Committeee agreed to change the score to 5 x 3 =15 and reflected on the appropriateness of amending the risk to reflect lapses in care. This would be furtherr discussed at the Board of Directors meeting Dec Q&S The Committee agreed with the recommendation to close this risk as the trajectory for Clostridium Difficile infections had already been exceeded. A new risk would be formulated which would consider lapses in care. Risk closed 5
94 Key Risk What are the key risks to achieving this corporate objective? Failure to reduce clinical variation and drug costs by 10% Key Controls What Where we can gain Potential areas of controls/systems are evidence or assurance weakness that may currently in place to mitigate the risk? that our control/systems are require additional controls/further effective? consideration? Agreement on focus Weekly Delivery Board; Availability of of scheme: clinical Management Board necessary and variation and accurate data to demand inform decision management are two making areas of scope within this work. One area has been identified for each Division: Colorectal, Gastroenterology and hips and knees; Project group established; Plan to undertake a retrospective review; 10 things we should stop doing presented to Management Board in January 2017 Assurance on controls Gaps in Initial Target Control and or risk risk Assurance C L S C L S Month April May June July August Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Q&S Risk could not be scored this time Q&S The Committee noted that work had commenced around clinical variation with key specialties identified for focus. It was agreed to retain the opening score of 20 Q&S A Abbasi advised that work continued within Na the Divisions and was led clinically. Fortnightly meetings were taking place and good progress was being made. The Committee agreed to retain the score at 20 Q&S The Medical Director reported that positive Na progress was being made to reduce drug costs. In terms of clinical variation, it was noted that data collection continued. The Committee agreed to retain the score at 4 x 5 = 20 ECC ECC reviewed the risk and agreed to retain Na the score of 20 Na Na Sept Q&S It was noted that good progress was being made, particularly with regard to the reduction of drug costs. The Committee agreed to reduce the score to 4 x 4 = 16 Na Oct Q&S The Committee had not received evidence in relation to this risk during the course of discussions and therefore agreed to maintain the score at 4 x 4 = Nov Q&S The Medical Director advised that positive progress was being made in terms of medication cost reduction however theree
95 Key Risk What are the key risks to achieving this corporate objective? Failure to reduce clinical variation and drug costs by 10% Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S was more to be done in terms of reducing clinical variation. It was agreed to retain the score at 4 x 4 = 16. Dec Jan Q&S The Committee noted that the position remained unchanged since the last meeting. It was agreed to retain the current score of 4x4= Feb Mar 7
96 Workforce Corporate Objective: Have a safe and flexible workforce that meets the needs of the service now and for the future Lead Director: A Balson, Director of Workforce Responsible Workforce Monitoring Committee: Measurement What does the objective mean? Pay bill reduce agency expenditure below agency ceiling and to under 2.11% of pay bill, reduce cap breaches by 15%, pay bill reduction by Carter definition of 7%; Rostering vacancy rate under 3.5% %, nursing shift fill rates over 89%, 100% job plan completion aligned to standardised SPA framework, block contract and locality plan; Health & Wellbeing sickness rate below 4%, statistically significant improvement in pulse survey score for energy, reduction in health age from 4 years 7 months as defined by Britain s Health Workplace survey, be in top 50% of Britain s Healthiest workplaces, below average sickness rate for S4W programme participants; Learning and Development draw down more than 85% of the apprenticeship levy fund, mitigate the pay billl impact of apprenticeship levy to under 4%, statistically significant improvements in pulse survey scoress - personal development, statistically significant reduction in reason for leaving lack of personal development d As above Impact of Unsafe patient care, poor staff morale and unsafe staffing levels. not achieving the objective Key Risk Key Controls Assurance on controls What are the key What Where we can gain risks to achieving this controls/systems are evidence or assurance corporate objective? currently in place to that our mitigate the risk? control/systems are effective? Failure to stay Workforce under agency Committee ceiling, impact of IR35 and associated impact F&I Committee on safe staffing levels Trust Grade Medical posts to be advertised to mitigate expected vacancies GM Strategic Workforce Board Procurement framework to GM HRD network support reduction in rate cards Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month GM / NW April agreement and implementation May June Committee Workforce Workforce Workforce Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Could not be scored for April template not complete Not scored for May The Committee agreed to score the risk at 5 Na x 3 = 15. This was on the basis that the risk could impact on the provision of safe staffing levels. However it was noted that the Trust had successfully reduced its agency spend and pro-active work was being undertaken to enhance recruitment, retention and improve wellbeing of staff 8
97 Key Risk Key Controls Redesign of staffing models to reduce demand for temp staffing E-locum shift management system Assurance on controls What are the key What Where we can gain risks to achieving this controls/systems are evidence or assurance corporate objective? currently in place to that our mitigate the risk? control/systems are effective? Failure to stay Development of under agency regional capped ceiling, impact of IR35 and rates associated impact on safe staffing levels cont. Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? July Month August Sept Oct Committee ECC Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S ECC ECC reviewed the risk and agreed to retain Na the current score of 15 Workforce ECC ECC noted that good progress was being Na made in terms of the agency ceiling. It was agreed to retain the score at 5 x 3 = 15 Progress against the agency ceiling was on Na trajectory. It was agreed to retain the score at 5 x 3 = 15 The risk was reviewed by the Executive Directors and it was agreed to retain the current score of 5 x 3 = 15 Na Nov Dec Jan ECC ECC The risk was reviewed by the Executive Na Directors. It was noted that agency spend remained under the ceiling. It was agreed to retain the current score of 5 x 3 = 15 The risk was reviewed by the Executive Na Directors. It was noted that the position remained unchanged since the risk was last scored Feb Mar 9
98 Key Risk Key Controls reports Manual job planning processes for Medical Staff Nursing & Midwifery strategy MCH & MMED earn, learn & return programmes GM Workforce Strategy Assurance on controls What are the key What Where we can gain Potential areas of risks to achieving controls/systems are evidence or assurance weakness that may this corporate objective? currently in place to mitigate the risk? that our control/systems are require additional controls/further effective? consideration? National shortage E-rostering Workforce Lack of e-job occupations and system and Committee planning inefficient use of available resources associated system GM Strategic Workforce Board Gaps in Initial Target Control and or risk risk Assurance C L S C L S National shortagess Month April May June July Committee Workforce Workforce Workforce ECC Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Could not be scored for April template not complete Not scored for May The Committee agreed to score this risk at Na x 4 = 20. While significant work had gone into rostering and nurse shift patterns, these would not be implemented until July. Good progress had been made with the Mch programmes but there were still uncertainties in certain specialties and around apprenticeship standards ECC noted that theree had been good Na progress with the Mch programme but there were potential issuess around certificates of sponsorship. It was agreed to retain the score at 5 x 4 =20 Aug ECC ECC reviewed the risk and agreed to retain Na the current score of Sept Workforce The Committee had discussed and noted the continued challenges in nurse recruitment. However, actions were being taken to try to address this. It was agreed to retain the score at 20 Na Oct ECC The risk was reviewed by the Executive Directors and it was agreed to retain the Na
99 Key Risk What are the key risks to achieving this corporate objective? National shortage occupations and inefficient use of available resources Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Nov Dec Jan Committee ECC ECC Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S current score of 5 x 4 = 20 The risk was reviewed by the Executive Na Directors. It was noted that there had been successful overseas recruitment in relation to medical staff but nursing gaps were significant. It was agreed to retain the score at 5 x 4 = 20 The risk was reviewed by the Executive Na Directors. It was noted that the position remained unchanged since the risk was last scored. Feb Mar 11
100 Key Risk What are the key risks to achieving this corporate objective? Sickness absence impacts on safe staffin levels and ability to g reduce pay bill (including failure to achieve flu vaccinationn target for health care workers) Key Controls Attendance Management Policy Steps 4 Wellness Programme Well Being Partners Occupational Health Service Go Engage The WWL Way Assurance on controls What Where we can gain controls/systems are evidence or assurance currently in place to that our mitigate the risk? control/systems are effective? s Workforce Committee Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month Counselling April capacity May June July Aug Committee Workforce Workforce Workforce ECC Discussion/Rationale for score ncluding further actions agreed and timescale for delivery Could not be scored for April template not - complete Not scored for May It was agreed to score this risk at 4 x 3 = 12. Na Lots of positive work was being undertaken to improve sickness levels but there remained pockets of high absence ECC noted that sickness absence levels remained at a steady rate of 4%. It was agreed to keep the score at 4 x 3 = 12 ECC ECC reviewed the risk and agreed to retain the current score of 12 Relevant Corporate Risks Identified In- year - Na Na Current Score C L S Flu vaccination campaign Sept Workforce The Committee noted that there were initiative in place to assist staff with health and wellbeing, uptake needed to be increased. Sickness levels were at just over 4% %. It was agreed to retain the current score of 12. Na Oct ECC The risk was reviewed by the Executive Directors and it was agreed to retain the current score of 4 x 3 = 12 Na Nov ECC The risk was reviewed by the Executive Directors. It was noted that current sickness absence rates were at around 4%. Further initiatives would be implemented as part of the Winter Wellbeing Campaign. It was Na
101 Key Risk What are the key risks to achieving this corporate objective? Sickness absence impacts on safe staffing levels and ability to reduce pay bill (including failure to achieve flu vaccinationn target for health care workers) Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Dec Jan Feb Mar Committee ECC Discussion/Rationale for score ncluding further actions agreed and timescale for delivery agreed to retain the current score of 4 x 3 = 12 The risk was reviewed by the Executive Directors. It was noted that the position remained unchanged since the risk was last scored. Relevant Corporate Risks Identified In- year Na Current Score C L S
102 Key Risk What are the key risks to achieving this corporate objective? Key Controls Failure to WWL Route Workforce utilise available Planner Committee resources to improve personal development Participation in trailblazer apprenticeship GM HRD network GM Strategic opportunities, programmes e.g. Workforce Board which impacts nursing on retention associate and does not mitigate the cost of the Membership of apprenticeship apprenticeship working group to levy (including inform new reduction in standards regional CPD funding) Development of apprenticeship targets to Divisions Workforce planning GM workforce strategy Divisional prioritisation of education needs Additional CPD Assurance on controls What Where we can gain controls/systems are evidence or assurance currently in place to that our mitigate the risk? control/systems are effective? Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month Lack of suitable April apprenticeship standardss May Out of June workplace learning impact on staffing levels July Aug Sept Oct Nov Dec Committee Workforce Workforce Workforce ECC Discussion/Rationale for score ncluding further actions agreed and timescale for delivery Could not be scored for April template not - complete Not scored for May The Committee agreed to score this risk at 4 Na x 4 =16. The significant risks around the lack of CPD funding internally and nationally were noted and the potential impact on recruitment and retention. Theree was also concern at the delay in developing apprenticeship standards ECC noted the concerns around the lack of funding for CPD. It was agreed to retain the score at 4 x 4 = 16 ECC ECC reviewed the risk and agreed to retain the current score of 16 Workforce ECC ECC ECC The Committee noted the positive progress that was being made in terms of apprenticeships however iit was agreed to increase the score to 4 x 5=20. The risk was reviewed by the Executive Directors and it was agreed to retain the current score of 4 x 5 = 20 Relevant Corporate Risks Identified In- year - Na Na Na Na The risk was reviewed by the Executive Na Directors. It was noted that the reduction in Continuous Professional Development funding was impacting on staff retention. It was agreed to retain the score at 4 x 5 = 20 The risk was reviewed by the Executive Directors. Na It was noted that the position remained unchanged since the risk was last scored. 14 Current Score C L S
103 Key Risk What are the key risks to achieving this corporate objective? Key Controls Assurance on controls What Where we can gain controls/systems are evidence or assurance currently in place to that our mitigate the risk? control/systems are effective? funding identified through Go Engage sales Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Jan Feb Committee Discussion/Rationale for score ncluding further actions agreed and timescale for delivery Relevant Corporate Risks Identified In- year Current Score C L S Mar 15
104 Key Risk What are the key risks to achieving this corporate objective? Key Controls Options appraisal for e- learning resources Centralisation of all education roles and functions into one team Assurance on controls What Where we can gain controls/systems are evidence or assurance currently in place to that our mitigate the risk? control/systems are effective? Lack of centralised training Scoping exercise led by Educational Educational Governancee Committee records creates Governancee reporting inaccuracies and potential Committee Business case Workforce Committee organisational risk in compliance development for Audit Committee medical device training records Gaps in Initial Control and or risk Assurance Potential areas of C L S weakness that may require additional controls/further consideration? Target risk C L No current single system to manage and hold all training records S Month Oct Nov Dec Jan Feb Committee Director of Workforce ECC ECC Discussion/Rationale for score ncluding further actions agreed and timescale for delivery In year risk added 24 th October 2017 The Director of Workforce has assessed the opening score for the risk to be 3 x 5 = 15. The risk was reviewed by Executive Directors. Yes It was noted that work was currently in progress in relation to the lack of centralised recording of training. This was being undertaken with Bolton. It was agreed to retain the score at 3 x 5 = 15 The risk was reviewed by the Executive Yes Directors. It was noted that the position remained unchanged since the risk was last scored. Relevant Corporate Risks Identified In- year Yes Current Score C L S Mar 16
105 Staff Engagement Corporate Objective: To improve levels of staff engagement, developing a culture of confidence and optimism where staff can directly influence change Lead Director: A Balson, Director of Workforce Responsible Workforce Monitoring Committee: Measurement What does the objective mean? Overall engagement score 4 (national staff survey); FFT recommendations above 80%; statistically significant improvements in pulse survey scores - influence, mindset, clarity and recognition; implement new leadership framework and behaviours assessed through new 360 As above. Impact of Poor staff morale, poor staff retention, increased sickness absence not levels and deterioration of staff survey results. achieving the objective Key Risk Key Controls Strategic narrative work programme WWL Route Planner Locality Assurance on controls What are the key What Where we can gain Potential areas of risks to achieving this controls/systems are evidence or assurance weakness that may corporate objective? currently in place to that our require additional mitigate the risk? control/systems are controls/further effective? consideration? Engagement does Go Engage Workforce Improved not improve The WWL Way Committee internal direct correlation between staff communication engagement and Pulse surveys National Staff methods (new patient satisfaction / outcomes Survey intranet) Steps 4 Wellness Programmes Locality Workforce Uncertainty Plan caused by external Pulse surveys environment Gaps in Initial Target Control and or risk risk Assurance C L S C L S Month April May June July Committee Workforce Workforce Workforce ECC Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Could not be scored for April template not complete Not scored for May The Committee agreed to score the risk at 4 Na x 3 = 12. There was a significant amount of positive work being undertaken around the strategic narrative. There had been positive results from the Friends and Family test recommending WWL as a good place of work. It was noted that there had been a dip in engagement levels in the Corporate Division ECC noted that theree had been a positive Na Pulse survey in June but it was agreed to retain the score at 4 x 3 = 12 pending the launch of the strategic narrative 17
106 Key Risk Key Controls What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? workforce programmes Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month August Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S ECC ECC reviewed the risk and agreed to retain Na the current score of Partnership working with trade unions Sept Workforce The Committee noted the work being undertaken in relation to staff engagement but noted that the pulse scores had remained at a plateau. It was agreed to retain the score of 12 Na Oct ECC The risk was reviewed by the Executive Directors and it was agreed to retain the current score of 4 x 3 = 12 Na Nov Dec ECC ECC The risk was reviewed by the Executive Na Directors. It was noted that consideration would be given to the removal of this risk. In the meantime, the score would be kept at 4 x 3 = 12 The risk was reviewed by the Executive Directors. Na It was noted that the position remained unchanged since the risk was last scored Jan Feb Mar 18
107 Performance Corporate Objective: To meet all national access targets Lead Director: M Fleming, Director of Operations Responsible Monitoring Committee: Finance and Investment and Performance Measurement A& E 4 hour target (90% Q1, 91.5% Q2, 92% Q3, 92.8% Q4); 18 weeks/rtt Incompletee Pathway (92%); Cancer targets 2 weeks to be seen, 31 days to first treatment and 62 day wait urgent GP referral to first treatment; Diagnostic-seen within 6 weeks. What does the objective mean? The Trust is required to meet a number of national access targets in relation to A&E, cancer treatment and diagnostics. Impact of not achieving Impact on quality of care and financial position. Possibility of regulatory action. the objective Key Risk Key Controls Assurance on controls What are the key What Where we can gain Potential areas of risks to achieving controls/systems are evidence or assurance weakness that may this corporate objective? currently in place to mitigate the risk? that our control/systems are require additional controls/further effective? consideration? Failure to meet the Emergency Demand Daily and Weekly Not achieving 95% A&E 4 hour target & patient flow meetings: standard (90% Q1, 91.5% Q2, management 92% Q3, 92.8% Q4) arrangements Patient Flow meeting Daily Board rounds Commissioner Contracting If the Trust is Emergency Achievement against (Chorley A& &E) unable to manage Department Standard standard reported to the level of Operating F&I Committeee & Trust Increased Acuity of emergency demand Procedures. it may lead to: board via Performance patients Report. An inability to Monthly Performance Weakness in local/ deliver operational management Daily/weekly regional standards. Affect quality of care for large number of patients. meeting NHSI A&E Improvement Plan Winter Resilience performance data monitoring/ NHS England/Urgent Care Dashboards Escalation Process Co-location of Primary Care Unmanageablee staff workloads. Negative financial position. Regulatory action. Plan Patient Flow Projects Gettinge HIS Friends and Family Feedback Output from A&E Quality Improvement Managing Demand Access to Community Beds Group Gaps in Initial Target Control and or risk risk Assurance C L S C L S Month April May June Committee F&I F&I Discussion/Rationale for score ncluding further actions agreed and timescale for delivery The Committee noted that the only risk to the Na achievement of national access targets was the achievement of A&E. Currently, A&E was performing well at over 90% achievement. There were no concerns around the achievement in April. The Committee agreed a score of 5 x 3 = 15 The Committee noted that A&E had achieved Na the revised trajectory of 90% in April. There were currently no concerns around performance. The Committee agreed to retain the score of F&I The Committee noted that A&E was currently Na meeting the revised trajectory of 90% and there were no concerns around the delivery of Q1. However it was noted that, whilst the A& &E team had implemented a number of improvement initiatives, there were increased Relevant Corporate Risks Identified In- year 19 Current Score C L S
108 Key Risk What are the key risks to achieving this corporate objective? Failure to meet the A&E 4 hour target cont. Key Controls Assurance on controls What Where we can gain controls/systems are evidence or assurance currently in place to that our mitigate the risk? control/systems are effective? A&E Delivery Outputs Systems Resilience Operational group CQC inspection Board Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month Committee Discussion/Rationale for score ncluding further actions agreed and timescale for delivery attendances to A&E by young mental health patients and out of area patients which provided additional pressure and could potentially put year end achievement of 95% at risk. The Committee noted and discussed the potential to lose S&T funding should the target not be achieved. It was agreed that the Committee needed to have visibility of GP out of hours, deflection projects and community bed plans to gain assurance around the external factors impacting on delivery. The Committee agreed to score as 4 x 4 = 16 Relevant Corporate Risks Identified In- year Current Score 4 C L S 4 16 July F&I The Committee noted that A&E performance continued to be under pressure and thatt Q1 had been achieved with the inclusion of walk in centre activity. The concerns of the Board had been escalated to the A&E Delivery Board. The Committee agreed to increase the score to 4 x 5 = 20 Na Aug ECC The risk was reviewed and discussed at ECC Na and it was agreed to amend the risk score to 5 x 4 = 20 to better reflect the position
109 Key Risk What are the key risks to achieving this corporate objective? Failure to meet the A&E 4 hour target cont. Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Sept Committee F&I Discussion/Rationale for score ncluding further actions agreed and timescale for delivery The Committee received assurance thatt the Na Trust was delivering all national targets with the exception of A&E which continued to be an area of challenge. Assurance was given that there were tactical and strategic plans in place to help improve A&E performance. On the basis of continuing A&E challenge, it was agreed to retain the score at 5 x 4 = 20 Relevant Corporate Risks Identified In- year Current Score C L S Oct F&I The Committee noted that, while A&E was still failing the target, there had been strong performance at the latter end of September but there were concerns around sustainability. WWL continued to track slightly above the national average for England. There were two areas for consideration : impact on S&T funding and quality and safety. Flu was a concern for the winter and it would be important to have a plan across the borough. It was agreed to retain the score at 5 x 4 = 20 Na Nov F&I The Committee noted earlier discussions around the ongoing challenges in relation to A&E performance. It was noted that an NHSI colleague would be visiting the Trust to help the Trust to identify any areas for further improvement. It was agreed to retain the score at 5 x 4 =20 Na Dec ECC The risk was reviewed by the Executive Directors. It was noted that the position remained unchanged since the risk was last scored. Na Jan 21
110 Key Risk What are the key risks to achieving this corporate objective? Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Feb Committee Discussion/Rationale for score ncluding further actions agreed and timescale for delivery Relevant Corporate Risks Identified In- year Current Score C L S March 22
111 Finance Corporate Objective: To achievee two year budget stability Lead Director: R Forster, Director of Finance and Informatics Responsible Monitoring Committee: Finance and Investment Measurement Financial Budget and Control Total; FRR; Big 12 schemes; Capital Investment versus plan What does the objective mean? As above Impact of not achieving the objective Budget overspend will lead to non-achievement of the Sustainable Transformation fund Key Risk What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Failure to Deliver the 12 big sch Key Controls Executive L eads emes for all big schemes; Weekly delivery meetings; Monthly Management Board Assurance on controls Where we can gain Potential areas of evidence or assurance weakness that may that our require additional control/systems are controls/further effective? consideration? Gaps in Initial Target Control and or risk risk Assurance C L S C L S Month Strategy Committee; Savings from 12 big April Finance and schemes to be Investment; defined; Big 12 May Trust Board: Monthly Finance Summary reports Report (with trend and variance analysis); External audit/internal audit June sign off reviews. Committee F&I F&I F&I Discussion/Rationale for score ncluding further actions agreed and timescale for delivery The Committee was not able to score this time as the template not complete The Committee noted that work around the Big 12 continued to progress. It was not anticipated that the schemes would deliver the full savings required but plans were in place to cover the shortfall by Divisional CIP Relevant Corporate Risks Identified In- year Na Na The Committee noted that there continued to Na be thorough investigation into and scrutiny of the Big 12 schemes. It was agreed to score the risk at 5 x 3 = 15 Current Score C L S July F&I The Committee noted that, while progress Na continued to be made on the Big 12, it was likely that some of the schemes may not deliver as anticipated. Replacement schemes
112 Key Risk Key Controls What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Failure to Deliver the 12 big schemes cont. Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month Aug Committee Discussion/Rationale for score ncluding further actions agreed and timescale for delivery would be considered. The Committee agreed to increase the score of the risk to 5 x 4 = 20 ECC The risk was discussed and reviewed at ECC Na and it was agreed to retain the current score of 20 Relevant Corporate Risks Identified In- year Current Score C L S Sept F&I The Committee noted the need to refocus this Na risk as there was now a more holistic approach being taken to delivering savings and the Big 12 and CIP had been incorporated into this. It was agreed to retain the score of 5 x 4 = 20 this time with a view to a new risk being put forward at the next meeting for consideration Oct F&I The risks around this objective were in the process Na of review. It was agreed to retain the current score Nov Dec F&I ECC Na The Committee noted that progress was being made in relation to the Big 12 schemes although there were some areas of concern. Given the potential impact of non-delivery agreed to retain the score at 5 x 4 = 20 on the budget, it was The risk was reviewed by the Executive Directors. Na It was noted that the position remained unchanged since the risk was last scored Jan Feb Mar 24
113 Key Risk What are the key risks to achieving this corporate objective? Key Controls What controls/systems are currently in place to mitigate the risk? Failure to CIP Oversight Deliver reviews; Divisional CIPs Divisional Performance Reviews Assurance on controls Where we can gain Potential areas of evidence or assurance weakness that may that our require additional control/systems are controls/further effective? consideration? Strategy Divisional CIP Committee; process/plan; Finance and Quality Impact Investment; Assessments External audit/internal audit sign off reviews. Gaps in Initial Target Control and or risk risk Assurance C L S C L S Month April May June Committee F&I F&I F&I Discussion/Rationale for score ncluding further actions agreed and timescale for delivery The Committee was not able to score this time as the template not complete The Committee had not had the opportunity to Na scrutinise CIP plans as yet so it was agreed to score the risk at 5 x 4 = 20 The Committee had not yet seen the Na Divisional CIP plans but assurance was given by the ED team that Divisions continued to work on plans. It was also noted that the Divisional CIP requirement had reduced to 4m. It was agreed to score the risk at 5 x 3 = 15 Relevant Corporate Risks Identified In- year Na Current Score C L S July F&I The Committee noted that a process led by the Director of Operations and Performance had been put in place to monitor divisional CIPs. It was agreed to score the risk at 5 x 3 = 15 Na Aug ECC The risk was discussed and reviewed at ECC Na and it was agreed to retain the current score of Sept F&I The Committee noted the need to refocus this Na risk as there was now a more holistic approach being taken to delivering savings and the Big 12 and CIP had been incorporated into this. It was agreed to retain the score of 5 x 3 = 15 this time with a view to a new risk being put forward at the next meeting for consideration
114 Key Risk What are the key risks to achieving this corporate objective? Failure to Deliver Divisional CIPs cont. Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Oct Nov Dec Jan Committee F&I F&I ECC Discussion/Rationale for score ncluding further actions agreed and timescale for delivery The risks around this objective were in the process of review. It was agreed to retain the current score The Committee noted that good progress continued to be made by the divisions in relation to CIP. It was agreed to retain the score at 5 x 3 = 15 The risk was reviewed by the Executive Directors. It was noted that the position remained unchanged since the risk was last scored. Relevant Corporate Risks Identified In- year Na Na Current Score C L S Feb Mar 26
115 Key Risk What are the key risks to achieving this corporate objective? Budget overspend; Cashflow reductions and liquidity Key Controls What Where we can gain Potential areas of controls/systems are evidence or assurance weakness that may currently in place to mitigate the risk? that our control/systems are require additional controls/further effective? consideration? Divisional Performance Reviews; DFM weekly cash monitoring; Monthly Capital Committee. Assurance on controls Finance and Investment; Trust Board: Monthly Finance Report (with trend and variance analysis); REMC escalation of in- year risks; External audit/internal audit sign off reviews. Gaps in Initial Target Control and or risk risk Assurance C L S C L S Month None identified April May June Committee F&I F&I F&I Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S The Committee was not able to score this Na time as the template not complete The Committee noted that M1 had achieved Na to plan and that the cash position was strong. It was agreed to score the risk at 5 x 2 = 10 The Committee noted that, whilst the budget Na was overspent, theree were robust plans in place to address this. The cash position continued to be good. It was agreed to score the risk at 5 x 2 = 10 July F&I The Committee noted that the cash position Na continued to be closely monitored however there continued to be overspend against budget in M3. It was agreed to score the risk at 5 x 3 = Aug ECC The risk was discussed and reviewed at ECC and it was agreed to retain the current score of 15 Na Sept F&I The Committee noted that the cash position Na continued to be closely monitored and was currently ahead of plan. It was agreed to retain the score at 5 x3 = Oct F&I The risks around this objective were in the process of review. It was agreed to retain the current score Na
116 Key Risk What are the key risks to achieving this corporate objective? Budget overspend; Cashflow reductions and liquidity cont. Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Nov Dec Jan Committee F&I ECC Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S The Committee noted that the cash position Na continued to be closely monitored. It was agreed to retain the score at 5 x 3 = 15 The risk was reviewed by the Executive Na Directors. It was noted that the position remained unchanged since the risk was last scored. Feb Mar 28
117 IT Corporate Objective: Make the most of our IT Investment to improve quality and efficiency Lead Director: R Forster, Director of Finance and Informatics Responsible Strategy Monitoring Committee: Measurement HIS phase 2 implementation; HIS usage; paper reduction usage; success on GM Digital funding application; digital maturity score What does the objective mean? As above Impact of not achieving the objective Key Risk Key Controls What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Failure to achieve HIS Phase 2 project timescales Senior IT Team; Digital Delivery Board; HIS Phase 2 project plan. Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? See gaps in Assurance External and Internal Audit Reports; IG toolkit Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? IT Trust Board Report; No defined reporting arrangements for IM&T following the ceasing of the IM&T Strategy Board Month April May June July August Committee Strategy Strategy Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Could not be scored for April template not - complete Not scored for May ECC It was agreed to score this risk at 3 x 3 =9 Na ECC The launch of the A& &E system was on track. Na It was agreed to score at 3 x 3 =9 ECC ECC reviewed the risk and agreed to retain Na the current score of Sept Review by Exec Review undertaken by Executive Director for Informatics with a recommendation to increase the score to 3 x 4 = 12 Na
118 Key Risk Key Controls What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Failure to achieve HIS Phase 2 project timescales cont. Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Oct Month Committee Strategy 3/10/17 Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S It was noted that there was limited Na assurance on the delivery of HIS phase 2 as there had been some issues which had delayed implementation. It was agreed to increase the score to 4 x 4 =16 with a report to the Board of Directors providing revised timescales, key risks and mitigation. Nov Dec Jan ECC ECC The risk was reviewed by Executive Na Directors. It was noted that HIS phase 2 had now gone live. It was agreed to retain the score at 4 x 4 = 16 The risk was reviewed by Executive Na Directors. It was agreed to increase the risk score to 5 x4 = 20 given the ongoing issues around HIS in A&E Feb Mar 30
119 Key Risk What are the key risks to achieving this corporate objective? Failure of the organisation to successfully adopt technology Key Controls Assurance on controls What Where we can gain Potential areas of controls/systems are evidence or assurance weakness that may currently in place to mitigate the risk? that our control/systems are require additional controls/further effective? consideration? Senior IT Team; Audit Committee Digital Delivery IT Trust Board Report; No Board; HIS Other Committees defined Phase 2 project plan; (F&I, Q&S) reporting arrangements HIS Champions SIRO meetings and Floorwalkers for IM&T following the Data Quality ceasing of the meetings IM&T Strategy Board Gaps in Initial Target Control and or risk risk Assurance C L S C L S Month April May June July Committee Strategy Strategy Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S The Committee was not able to score this time as the template not complete Not scored for May ECC It was agreed to score this at 3 x 3 = 9 ECC Na The adoption of HIS at WWL had been Na strong and was cited as an exemplar. However, the removal of costs following the reduction in paper had not yet been demonstrated. It was agreed to leave the score at 3 x 3 = 9 - Na Aug ECC ECC reviewed the risk and agreed to increase the score to 5 x 4=20 Na Sept Review by Exec Review undertaken by Executive Director for Informatics with a recommendation to retain the score to 5 x 4 = 20 Na Oct Strategy The Committee reviewed the score and agreed to retain the current score of 5 x 4 = 20. Na Nov Dec ECC ECC The risk was reviewed by Executive Na Directors. It was noted that, despite initial challenges, the A&E system had been well received by staff. It was agreed to retain the score at 5 x 4 = 20 The risk was reviewed by the Executive Na Directors. It was noted that the position remained unchanged since the risk was last scored
120 Key Risk What are the key risks to achieving this corporate objective? Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Jan Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Feb Mar 32
121 Key Risk What are the key risks to achieving this corporate objective? Failure to mitigate against Cyber- attacks Key Controls What Where we can gain Potential areas of controls/systems are evidence or assurance weakness that may currently in place to mitigate the risk? that our control/systems are require additional controls/further effective? consideration? Senior IT Team; External and IT Helpdesk and Internal Audit alerts process reports disseminating information GM Digital Board across the organisation; Business Continuity Plans; SIRO Meetings; Incident Debriefs Malware Software Assurance on controls Gaps in Initial Target Control and or risk risk Assurance C L S C L S Intelligence from latest incident (Debrief scheduled) Month April May June July Aug Committee Strategy Strategy Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S The Committee was not able to score this time as the template not complete Not scored for May ECC It was noted that work was being undertaken to strengthen cyber security. It was agreed to score at 4 x 4 = 16 and to reduce further once implementation was complete ECC Work continued with regard to strengthening Na cyber security. It was agreed to keep this score at 4 x 4 = 16 ECC ECC reviewed the risk and agreed to reduce the score to 4 x 3 =12 Na - Na Na Sept Review by Exec Review undertaken by Executive Director for Informatics with a recommendation to increase the score to 4 x 3 = 12 Na Oct Strategy The Committee reviewed the score and agreed to retain the current score of 4 x 3 = 12 Na Nov Dec ECC ECC The risk was reviewed by Executive Na Directors. It was noted that additional resilience was being built in to protect systems against cyber-attacks. It was agreed to retain the score at 4 x 3 = 12 The risk was reviewed by the Executive Na Directors. It was noted that the position remained unchanged since the risk was last scored
122 Key Risk What are the key risks to achieving this corporate objective? Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Jan Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Feb Mar 34
123 Key Risk What are the key risks to achieving this corporate objective? Key Controls What controls/systems are currently in place to mitigate the risk? Lack of funding Senior IT Team; for upgrades and Capital developments prioritisation SIRO Meetings Assurance on controls Where we can gain Potential areas of evidence or assurance weakness that may that our require additional control/systems are controls/further effective? consideration? See gaps in Assurance External and Internal Audit Reports; SIRO breach reports Gaps in Initial Target Control and or risk risk Assurance C L S C L S Security patches Windows 2003/XP Quarantine for infected devices External systems (patches not controlled by WWL) Month April May June July Aug Sept Committee Strategy Strategy Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S The Committee was not able to score this time as the template not complete Not scored for May ECC It was noted that some funding had been available to the IT team for necessary upgrades and developments. The score was agreed at 4 x 3 = 12 ECC It was noted that funding had been made available for necessary upgrades. It was agreed to reduce the score to 4 x 2 = 8 ECC ECC reviewed the risk and agreed to retain Na the current score of 8 Review by Exec Review undertaken by Executive Director for Informatics with a recommendation to increase the score to 4 x 2 =8 Na - Na Na Na Oct Strategy The Committee reviewed the score and agreed to retain the current score of 4 x 2 = 8. Na Nov ECC The risk was reviewed by Executive Na Directors. It was noted that the implementation of the new EU GDPR regulations would be significant for the Trust and would require additional resource. The risks around this weree receiving scrutiny via REMC and Audit Committee. It was agreed to increase the score to 4 x 3 =
124 Key Risk What are the key risks to achieving this corporate objective? Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Dec Jan Committee ECC Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S The risk was reviewed by Executive Na Directors. It was agreed to reduce the risk to 4 x 2 =8 given the confirmation of funding via the Digital Collaboration Board Feb Mar 36
125 Partnerships Corporate Objective: Improve hospital services through Partnership with Wigan locality commissioners and local provider partners in order to best meet the needs of Wigan residents Lead Director: R Mundon, Director of Strategy and Planning Responsible Strategy Monitoring Committee: Measurement What does the objective mean? Phase 2 of Transformation Fund successfully achieved; WWL to be integral part of Healthier Wigan Partnership through alliance agreement by March 2018; ICS metrics agreed by September 2017; Primary Care (including GP OOH) to be located adjacent to A&E by October 2017; WWL component of Locality Plan successfully delivered Impact of Patient flow and quality of healthcaree is diminished; loss on income not achieving the objective Key Risk What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Failure to agree Governance Structures Key Controls Cross Borough stakeholder meetings including Health and Wellbeing Board and Wigan Leaders; Secondary Care Transformation Board Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Trust Board Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month Integrated April Community Services Model: May relationship between cause June and effect metrics; July Committee Strategy Strategy Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Could not be scored for April template not - complete Not scored for May ECC It was agreed to increase the score to 4 x 4 Na = 16 given the ongoing work around the move to single commissioning and provision frameworks and the associated risks ECC Work continued in relation to the move to single commissioning and provision frameworks. It was agreed to retain the score at 4 x 4 = 16 - Na August ECC ECC reviewed the risk and agreed to retain Na the current score of
126 Key Risk Key Controls What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Failure to agree Governance Structures cont. Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month Sept Committee Review by Exec Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Recommend that this remains at 16. Na The Council and CCG have agreed the broad components of the Strategic Commissioning Function and this should be communicated by the end of September alongside the commissioning intentions. The alliance contract for the ACO should be in place by the end of the year. Healthier Wigan Partnerships Working Group is driving this forward Oct Strategy The Committee noted that progress had been made but there were still some risks. It was agreed to keep the risk at 4 x 4 = 16. Na Nov Dec Jan ECC ECC The risk was reviewed by the Executive Na Directors. It was noted that plans were in place to move towards a single commissioning function between the Council and CCG. It was agreed to retain the current score of 4 x 4 = 16 The risk was reviewed by the Executive Na Directors. It was noted that the position remained unchanged since the risk was last scored Feb Mar 38
127 Key Risk What are the key risks to achieving this corporate objective? Key Controls What controls/systems are currently in place to mitigate the risk? Changes to WWL commissioning relationshipss arrangements with in Greater commissioners Manchester and information may slow sharing processes Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? GM Health and Social Care Partnership; Strategy Committee; Healthier Wigan Partnership Board Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month Consideration April of further strengthening of relationships May with appropriate stakeholders June Committee Strategy Strategy Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S The Committee was not able to score this time as the template not complete Not scored for May ECC It was agreed to retain the score at 3 x 3 = 9 Na as there was little detail around this Na July ECC There had been no change in relation to this Na risk so it would remain at 3 x 3 = Aug ECC ECC reviewed the risk and agreed to retain Na the current score of Sept Review by Exec Recommend that this remains at 9. Na The GM Review of Commissioning Group is now meeting regularly and overseeing these arrangements. Feedback from the PM (Tim Deeprose) suggests that there is significant similarity between Boroughs and PwC are expected to have supported each through their design work. The biggest outstanding issue is about GM v Locality based commissioning, but this is unlikely to slow down Wigan specific solutions significantly Oct Strategy The Committee noted the lack of insight Na into the form that this would take so agreed to escalate the risk score to 4 x 3 =
128 Key Risk What are the key risks to achieving this corporate objective? Changes to commissioning arrangements in Greater Manchester may slow processes cont. Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Nov Dec Jan Committee ECC ECC Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S The risk was reviewed by the Executive Na Directors. It was noted that this was a regional rather than a local risk and unlikely to be a significant concern in the current year. It was agreed to reduce the score to 4 x 2 = 8 The risk was reviewed by the Executive Na Directors. It was noted that the position remained unchanged since the risk was last scored. Feb Mar 40
129 Standardised Hospital Care Corporate Objective: Fully support Standardised Hospital Care across GM and play a lead provider role in standardising Orthopaedics Lead Director: R Mundon, Director of Strategy and Planning Responsible Strategy Monitoring Committee: Measurement What does the objective mean? HT implementation underway by June 2017; Shared Services Board to have met 4 times; NW Sector priority services scoped and implementation plan in place; MoU in place with GM/CMFT by June 2017; GM Theme 3 implications scoped by Sep 2017 Impact of Wigan residents receive poorer services than other residents in not Greater Manchester achieving the objective Key Risk What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Healthier Together: Failure to achieve standardised hospital services could result in stranded services and costs WWL are unable to meet Key Controls Transformation Fund; Healthier Together Delivery Board; North West Sector Partnership Board Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Strategy Committee; Trust Board Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month None identified April May June Committee Strategy Strategy Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Could not be scored for April template not - complete Not scored for May ECC It was noted that the Healthier Together Na team had been made aware of concerns in relation to stranded costs and were considering these. The score would remain at 4 x4=16 pending resolution July ECC` There had been no change since the last Na discussion. This would remain at 4 x 4 = August ECC ECC reviewed the risk and agreed to retain Na the current score of
130 Key Risk Key Controls What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Healthier Together: Failure to achieve standardised hospital services could result in stranded services and costs WWL are unable to meet cont. Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Month Sept Committee Review by Exec Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S Recommend that this remains at 16. GM now pushing ahead with implementation. Committees in Common expected to approve business case on 1 September, which will trigger release of capital funds. Outstanding issues around double ambulance journeys, surgical trainees and counterbalancing flows all raised with HT team and being addressed 19 th Na Oct Strategy The Committee noted that while the business case had been approved, there remained unresolved issues with regard to surgical trainees, management of emergency surgical patients at non-hub sites, and reciprocal work flows. It was agreed to retain the current score of 4 x 4 = 16. Na Nov Dec Jan ECC ECC The risk was reviewed by Executive Na Directors. It was noted that progresss was being made in allaying some of the concerns in relation to Healthier Together. It was agreed to reduce the score to 4 x 3 =12 The risk was reviewed by the Executive Na Directors. It was noted that the position remained unchanged since the risk was last scored Feb 42
131 Key Risk Key Controls What are the key What risks to achieving this controls/systems are corporate objective? currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Mar Committee Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S 43
132 Key Risk What are the key risks to achieving this corporate objective? NW Sector: Failure to agree what the portfolio of services looks like and to understand the codependences of services in the portfolio Key Controls What controls/systems are currently in place to mitigate the risk? NW Sector Priorities Group; NW Sector Partnership Board; Shared Services Board Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Strategy Committee; Trust Board Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Clinical Engagement Month April May June Committee Strategy Strategy Discussion/Rationale for score ncluding further actions agreed and timescale for delivery The Committee was not able to score this time as the template not complete Not scored for May ECC Priority services had been agreed within the NW Sector and detailed discussions were taking place. It was agreed to retain the score at 3 x 4 =12 Relevant Corporate Risks Identified In- year Na - Na Current Score C L S July Aug ECC Discussions continued with regard to a portfolio of services. It was agreed to retain the score at 3 x 4 = 12 Na ECC ECC reviewed the risk and agreed to increasena the current score to 4 x4 = Sept Review by Exec Recommend that this remains at 16. Na Joint Strategy team working with Bolton should help with this. Clarity on four in-scope services and jigsaw model developed to show consequences of scenarios Oct Strategy The Committee agreed to retain the current score of 4 x 4 = 16. Na Nov Dec ECC ECC The risk was reviewed by Executive Directors. It was noted that there was a good understanding of what the portfolio of services looked like. It was agreed to retain the score at 4 x 4 = 16 The risk was reviewed by the Executive Directors. It was noted that the position Na Na
133 Key Risk What are the key risks to achieving this corporate objective? Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Jan Committee Discussion/Rationale for score ncluding further actions agreed and timescale for delivery remained unchanged since the risk was last scored. Relevant Corporate Risks Identified In- year Current Score C L S Feb Mar 45
134 Key Risk What are the key risks to achieving this corporate objective? GM Theme 3: Failure to generate orthopaedic business or to generate too much business to meet demand Key Controls Assurance on controls What Where we can gain controls/systems are evidence or assurance currently in place to that our mitigate the risk? control/systems are effective? Theme 3 Strategy Delivery Board; Committee; Trust GM Health and Board Care Partnership Board Gaps in Initial Target Control and or risk risk Assurance Potential areas of C L S C L S weakness that may require additional controls/further consideration? Completion of detailed plan (in design stage) Month April May June July Aug Committee Strategy Strategy Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S The Committee was not able to score this time as the template not complete Not scored for May ECC A GM wide consensus had been agreed on Na the consolidation of Orthopaedic activity but there was analysis to be undertaken around the potential impact of tariff. It was agreed for this reason to increase the score to 4x4=16 ECC Discussions continued with regard to Na Orthopaedic activity. It was agreed to retain the score at 4 x 4 = 16 ECC ECC reviewed the risk and agreed to retain Na the current score of 16 Na Sept Review by Exec Recommend that this remains at 16. Na Orthopaedic case for change going to GM Clinical Reference Group on 22 September. The clinical model, which describes proposed reconfiguration, will follow by the end of December Oct Strategy The Committee agreed to retain the current Na score of 4 x 4 = Nov ECC The risk was reviewed by Executive Na Directors. It was noted that a workshop was taking place in early January to discuss the Themee 3 model of care
135 Key Risk What are the key risks to achieving this corporate objective? Key Controls What controls/systems are currently in place to mitigate the risk? Assurance on controls Where we can gain evidence or assurance that our control/systems are effective? Gaps in Initial Control and or risk Assurance Potential areas of C L weakness that may require additional controls/further consideration? Target risk S C L S Month Dec Jan Committee ECC Discussion/Rationale for score Relevant Current ncluding further actions agreed and Corporate Risks Score timescale for delivery Identified Inyear C L S The score would be reviewed following that discussion. It was agreed to retain the score at 4 x 4 = 16 The risk was reviewed by the Executive Na Directors. It was noted that the position remained unchanged since the risk was last scored. Feb Mar 47
136
137 REPORT AGENDAA ITEM: 8.5 To: Board of Directors Date: 20 December 2017 Subject: Safe staffing report r Presented by: Director of Nursing Purpose: For report Executivee summary This report provides a monthly summary of Safe Staffing on all in-patienrelated incidents and red flags which are wards across the t Trust. It includes exception reports related to staffing levels, then triangulated with a range of quality indicators. Risks associated with this report Nurse staffing levels and vacancies impact on the organisation s corporate c objectives: To deliver safe, high quality, effective, evidence-based patient care Have a safe and flexible workforce that meets the needs of the service now and for the future Link(s) to The WWL Way 4wards Patients Performance People Partnerships
138
139 Safe Staffing report
140 Safe Staffing Report November INTRODUCTION This report provides a monthly summary of Safe Staffing on all in-patient wards across the Trust. It includes exception reports related to staffing levels, related incidents and red flags which are then triangulated with a range of quality indicators. 2.0 SAFER STAFFING EXCEPTION REPORT The safe staffing exception report (Appendix1), provides the established versus actual fill rates on a ward by ward basis. Fill rates are RAG rated with supporting narrative by exception, and a number of related factors are displayed alongside the fill rates to provide an overall picture of safe staffing. Sickness rate and Vacancy rate are the two main factors that affect fill rates. The monthly point prevalence sample audit of Care Indicators was suspended in September The Trust is currently developing a ward accreditation system which will support the collection of quality indicators alongside real time patient safety flags. It is envisaged that this work will be completed within the forthcoming financial year and be fully operational by the end of March This metric has been removed from the report and will be reinstated once the new indicators are launched. Datix incident submissions related to staffing and Red Flags are monitored on a daily basis to act as an early warning system and inform future planning. Nurse Sensitive Indicators demonstrate the outcome for patients by measuring harm. o Cases of Clostridium Difficile (CDT); o Pressure Ulcers Grade 1&2 / Grade 3&4; o *Falls resulting in physical harm / not resulting in physical harm; o *Medication administration errors resulting in harm / not resulting in harm. (*All incidents displayed by: those that resulted in moderate and severe harm / resulted in minor or no harm) The impact of Nurse staffing on Patients Experience is demonstrated by two specific questions from the monthly Real Time Patient Experience Survey. The NICE guidance on safe staffing in hospitals suggests using a number of questions in the form of a patient experience survey. For some of the NICE questions the trust has an equivalent question, or proxy question within the monthly Real Time Patient Experience survey or Always Events Survey, with the two questions matching most closely featuring in this report. There are a number of wards that have not been able to maintain fill rates throughout the month of November, and this is clearly associated with higher rates of sickness/absence, vacancies or a combination of both. Active recruitment to the vacancies remain ongoing. The average fill rate across all areas has improved for registered nurses from 82.43% in September to 86.1% in October. Following on from the successful recruitment campaign in the summer fill rates for unqualified staff are currently 110.3%. Safe Staffing for each ward is assessed on a daily basis by the relevant Divisional Matrons and, during the evenings and at weekends the Duty Matron has responsibility for ensuring safe staffing of all ward areas across the Trust.
141 There are currently 14 risks noted on the Corporate Risk Register associated with nurse staffing levels and skill mix; 10 in Medicine, 1 in surgery and 3 in Specialist Services. Risk scores associated with the risk assessments are either rated as 15 or 20 dependant on the number of vacancies within the area and the associated clinical risk to patients as a consequence. Following the introduction of the pay initiatives in October there continues to be an improvement in fill rates across the Trust throughout November, although pressures still remain which are related to sickness, vacancies and maternity leave, and the outbreak of Norovirus on the Wrightington site. Table 1 demonstrates the number of red metrics for fill rates from September to November. The Surgical Division has the largest number of areas with red metrics. Long term sickness is being proactively managed within the division and there is ongoing recruitment across the division to address the shortfalls in staffing levels. No areas of September 2017 October 2017 November 2017 Red Red Metrics Red Red Metrics Red Metrics Metrics Registered Metrics Registered Registered Registered staff Registered Staff Days Staff Nights staff Days staff Nights Nights Red Metrics Registered staff Days Table 1. The Board should note that the fill rates reported in the appendix do not reflect movement of substantive staff to cover Highfield ward and therefore it is likely that the fill rates reported are slightly inflated. In November the Board will note registered nurse fill rates for ICU/HDU day shifts was remains less than 50% for day shifts. Staff have continued to work flexibly to ensure staff to patient ratios have been maintained in accordance with national guidance based on occupancy and demand. Current vacancies within Nursing are provided in Table 2 below. The figures represent all registered and unregistered nurse vacancies across the 3 clinical divisions and therefore include wards, departments and theatres. Vacancies are expressed as WTE. Data provided from the divisions indicates an overall reduction in registered nurse vacancies by 2.8 WTE and an increase in unqualified vacancies of 3.21 WTE. Specialty Qualified Unqualified Medicine Surgery Specialist Services Total Table 2. Current Registered staff labour turnover remains around 13.62%. On consideration of the HR data provided at Appendix 1 Standish and Lowton wards are both outliers with respect to sickness. Standish is also an outlier with respect to high levels of vacancies and this is reflected in the fill rates. OD support is being requested to understand whether there is any correlation between the two factors and to work with the ward team to identify interventions that will benefit staff health and wellbeing. Vacancies are particularly high in the following areas, Astley, Standish, CDW, Mau, Orrell Maternity and Ward A on the Wrightington site.
142 There have been 66 incidents reported in October under the nursing red flags criteria. The largest number recorded was by Aspull (N24) and these are attributed to vacancies, maternity leave and short and long term sickness. The breakdown of red flag incidents reported by category is demonstrated in table 3. Red Flag Category No. of Incidents Shortfall of more than 8 hours or 25% of registered nurses in a shift 56 Delay of 30 minutes or more for the administration of pain relief 0 Delay or omission of intentional rounding 1 Less than 2 registered nurses on shift 6 Vital signs not assessed or recorded as planned 3 Unplanned omission of medication 0 Total 66 Table 3 Triangulation of red flags raised and red fill rate indicators demonstrates that there is an issue with reporting the impact or consequence of staffing shortfalls. The following areas have raised no red flags despite having below 85% fill rates; Standish, ICU, Orrell and Swinley. This report is to be shared with Heads of Nursing and Matrons, and the Patient Safety Team are to identify low reporting rates via the daily teleconference to address this. There have been 9 Midwifery Red Flag incidents for the reporting period. The reason for the red flags is detailed in Table 4 below. Red Flag Category No. of Incidents Delayed or cancelled time critical activity 1 Unit on Divert 3 Co-Ordinator Unable to Remain Super-numery 2 Missed or delayed care (for example, delay of 60 minutes or more 2 in washing and suturing) Missed medication during an admission to hospital or midwifery-led 0 unit (for example, diabetes medication) Delay of 2 hours or more between admission for induction and 0 beginning of process Any occasion when 1 midwife is not able to provide continuous 1 one-to-one care and support to a woman during established labour Total 9 Table 4. This is only the second month where Midwifery Red Flags have been reported. The Board should note that the fill rate is high within Maternity services during the month and that the red flag triggers are associated with peaks in activity, acuity and transfer of women in utero rather than deviation from planned staffing levels.


















143 The Model Hospital was undated in November with August data. The e information in the chart above indicates that the Trust continues to perform well with w respectt to the provision of care hours per patient day in comparisonn to the peer and national position, and the average costs of nursing and midwifery staff is lower than peer and national average. The Trust continues to review the workforce model to deliver safe, effective care that is responsive to the needs of patients ass part of the Nursing,, Midwifery y and Allied Health Professionals Strategy. No falls or medication administration errors resulting in harm h have been reported in November. 2 CDTs have been reported in month on Astley and Standish respectively. RCA s are currently being progressed and it is not known at the time of the t report whether there have been any lapses in care in these cases. Rainbow Ward achieved 100% compliance with the presence of an APLSS qualified nurse on every shift throughout November There continues to bee a programme of education to support the clinical area to place 2 APLSS trained nurses on duty on each shift. 5.0 SUMMARY During the month of November 2017 the wards have continued to experience staffing pressures that equired assessment of risk and agreed safe s working solutionss to be implemented on a daily basis. However the Board should note that the initiatives implemented throughout October and November have continued to impact positively on fill rates. 6.0 RECOMMENDATIONS The Board is asked to receivee the paper for information and discussion. Allison Edis Deputy Director of Nursing
144 Appendix 1 SAFE STAFFING EXCEPTION REPORT November 2017 Division of Medicine Scheduled Care
145 Division of Medicine Unscheduled Care RN / RM Average Fill Rates (%) & CHPPD CSW Staff Availability Staff Experience Nurse Sensitive Indicators Patient Experience % (Number surveyed) Ward Day shift (%) Night shift (%) CHPPD Day shift (%) Night shift (%) CHPPD Sickness (%) Vacancies (%) Datix Incidents - related to staffing/red Flags CDT Falls (Harm / No Harm) PU (Grade 1&2 / Grade 3 & 4) Drug Admin Errors (Harm / No Harm) Do you think the hospital staff did everything they could do to control your pain? Have you been given the care you felt you required when you needed it most? A&E Emg Care 97.0% 99.3% 95.4% 190.2% 5.64% 0.00% / 1 A&E Paeds 83.0% 121.2% 2.08% 2.27% / 0 CDW 96.8% 96.8% 75.0% 108.1% 0.75% 18.51% / 0 0 / 1 100% 100% Lowton 92.3% 84.0% 125.0% 115.4% 13.99% 0.45% / 7 2 / 0 0 / 5 100% 100% MAU 89.5% 83.0% 111.0% 102.3% 1.13% 12.26% / 4 0 / 0 100% 100%
146 Division of Surgery Average Fill Rates (%) & CHPPD RN / RM CSW Staff Availability Nurse Sensitive Indicators Patient Experience % (Number surveyed) Ward Day shift (%) Night shift (%) CHPPD Day shift (%) Night shift (%) CHPPD Sickness (%) Vacancies (%) Staff Experience Datix Incidents - related to CDT staffing/red Drug Admin Falls (Harm / No PU (Grade 1&2 / Errors (Harm / Harm) Grade 3 & 4) No Harm) Do you think the Have you been hospital staff did given the care you everything they felt you required could do to control when you needed it your pain? most? ICU/HDU 42.10% 81.60% % 0.00% % 4.49% / 0 0 / 0 n/a n/a Orrell 78.10% 66.70% % 98.10% % 14.40% / 1 2 / 0 0 / 0 40% 60% Langtree 59.70% 79.70% % % % 1.69% / 3 0 / 0 100% 100% Swinley 84.70% 98.30% % % % 0.00% / 1 0 / 0 67% 67% Maternity Unit % 95.50% % 94.60% % 16.94% / 0 0 / 0 100% 100% Neonatal Unit 95.50% % % 0.00% % 0.00% / 0 1 / 0 0 / 3 No eligible patients No eligible patients Rainbow % 97.70% % 67.80% % 3.00% / 0 0 / 1 No eligible patients No eligible patients Rainbow ward: During the month of November 2017 safe staffing has been maintained within the framework set out in the Standard Operational Procedures for the safe running of Rainbow ward and Escalation procedure.
147 Division of Specialist Services RN / RM Average Fill Rates (%) & CHPPD CSW Staff Availability Staff Experience Nurse Sensitive Indicators Patient Experience % (Number surveyed) Ward Day shift (%) Night shift (%) CHPPD Day shift (%) Night shift (%) CHPPD Sickness (%) Vacancies (%) Datix Incidents - related to staffing/red Flags CDT Falls (Harm / No Harm) PU (Grade 1&2 / Grade 3 & 4) Drug Admin Errors (Harm / No Harm) Do you think the Have you been hospital staff did given the care you everything they felt you required could do to control when you needed it your pain? most? Aspull 87.90% 75.60% % % % 4.14% / 3 0 / 2 100% 100% Ward A 94.10% 83.30% % 97.80% % 14.91% / 0 0 / 0 100% 100% Ward B % 86.30% % 95.30% % 0.00% / 0 0 / 0 100% 100% JCW % % % 99.90% % 6.33% / 0 0 / 0 n/a n/a
148
149 REPORT AGENDAA ITEM: 9.1 To: Board of Directors Date: 20 December 2017 Subject: Emergency Preparedness, Resilience and Response (EPRR) Compliance Statement 2017 Presented by: Director of Operations and Performance Purpose: Approval Executivee summary The attached document sets out the organisation s self-assessed declaration in relation to compliance against the NHS England Core Standards Risks associated with this report Actions to be taken to improve compliance further are outlined within the document. Link(s) to The WWL Way 4wards Patients Performance People Partnerships
150
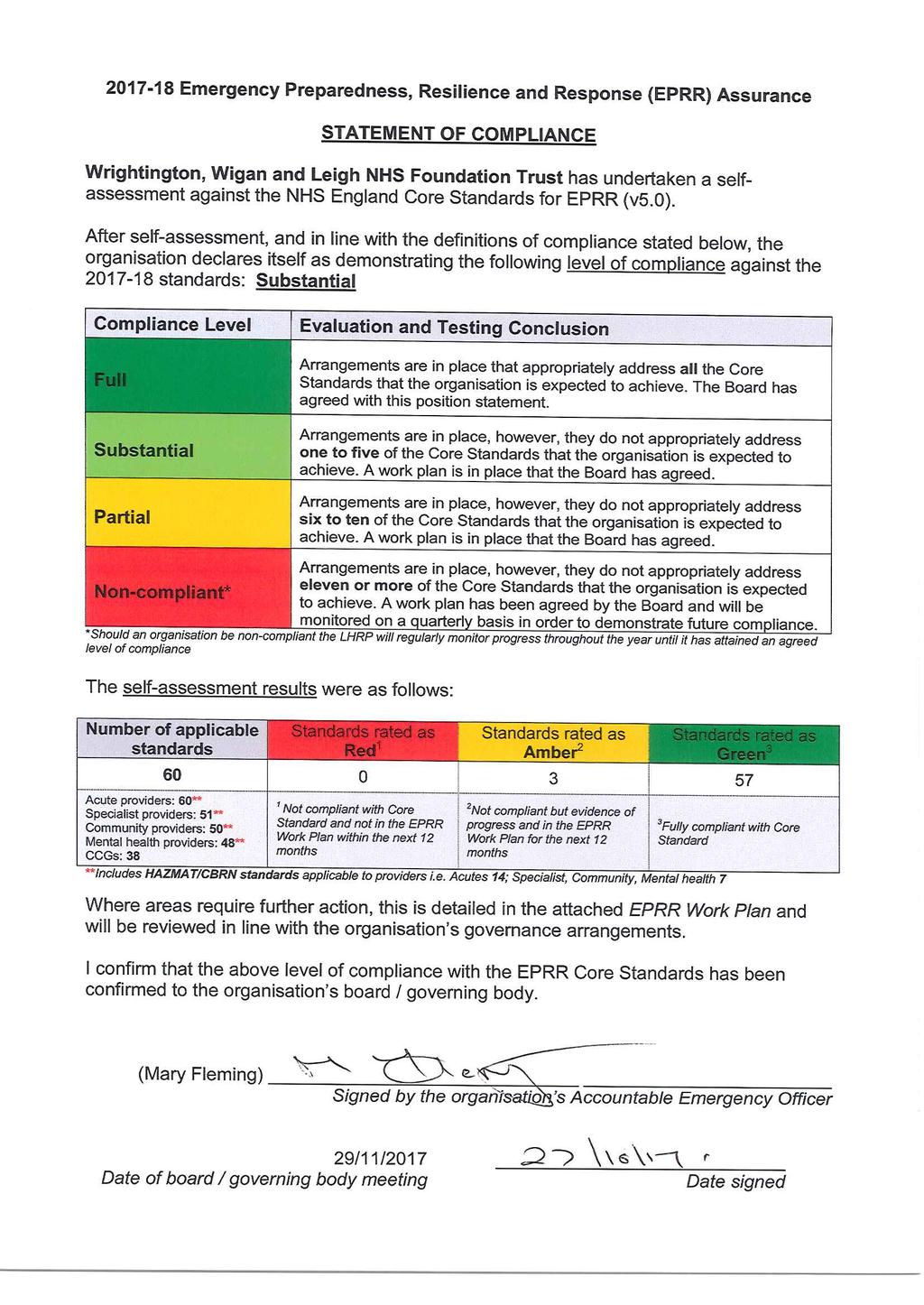
151
152
153 REPORT AGENDAA ITEM: 9.2 To: Board of Directors Date: 20 December 2017 Subject: Health and Safety Annual Report Presented by: Director of Nursing Purpose: Approval Executivee summary This report provides analysis of the currentt standard for the financial year of health and safety throughout the t Trust Risks associated with this report Risks associated with the report are the consequencess to the Trust of non-compliance with The Health and Safety at Work Act Examples of prosecutions s against Healthcare Providers are included within the report. Link(s) to The WWL Way 4wards Patients Performance People Partnerships
154
155 Health & Safety Annual Report
156 CONTENTS PAGE 1. Introduction 3 2. Service Strategy 4 3. Occupational Health and Safety Management System (OH&SMS) Risk Assessment Safety Inspections 6 4. Health and Safety Legislation and HSE Update New Legislation Health and Safety Consultations HSE Intervention/Investigations specific to NHS Organisations 7 5. Communication and Consultation Occupational Safety and Health Committee Health and Safety Intranet Page 9 6. Health and Safety Training and Awareness Classroom Based Training ecompulsory Training Campaigns Non-clinical Incident Reporting Type and Cause of Incidents RIDDOR Status of Incident Investigations, Corrective and Preventative Actions Incident Investigation Analysis Measuring Performance Health and Safety Support Visits Health and Safety Performance Report Audit, Monitoring and Review Health and Safety Objectives Conclusion Actions Required 16 Appendix 1: HSE Consultations 17 Key: Achieved Ongoing objective Not achieved Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 2 of 17
157 1. INTRODUCTION This report provides analysis of the current standard of health and safety throughout the Trust for the financial year The Health and Safety at Work etc. Act 1974 provides a legislative framework to promote, stimulate and encourage high standards of health and safety at work. In particular it requires organisations to provide and maintain: a) A Health and Safety Policy and written statement of intent; b) A system to manage and control risks in connection with the use, handling, storage and transport of articles and substances; c) A safe and secure working environment, including provision and maintenance of access to and egress from premises; d) Safe and suitable plant, work equipment and systems of work that are without risks; e) Information, instruction, training and supervision as is necessary; f) Adequate welfare facilities. The legislation is enforced by the Health and Safety Executive (HSE) who have far reaching powers, which include: a) Access to work premises at any reasonable hour; b) Freedom to interview staff and visitors, contractors or patients; c) Confiscation of equipment and applicable documents; d) Taking statements, photographs, measurements and samples; e) Issuing notices (Improvement and Prohibition) requiring respectively improvements within a certain timeframe or stopping work until improvements are made also within a timeframe; f) Initiating criminal court proceedings for alleged. The Health and Safety Team consists of: Band 7-1 x WTE Health Safety Manager Band 6-1 x WTE Health and Safety Advisor Band 4-1 x 0.8 WTE Health and Safety Co-ordinator The team is responsible for: a) Advising senior and middle managers, safety representatives and staff on matters of health and safety at work; b) Developing, implementing and maintaining an Occupational Safety Management System on behalf of the Trust; c) Developing and delivering bespoke health and safety training courses as appropriate; d) Developing and implementing health and safety policies and procedures to improve the management of health and safety across the Trust; e) Providing information and corporate data analysis in respect of Trust-wide health and safety compliance. The Health and Safety Team are part of the Governance and Assurance Department. The Team report to the Occupational Safety and Health Committee which in turn reports to the Trust Quality & Safety Committee, a sub-committee of the Trust Board. Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 3 of 17
158 2. SERVICE STRATEGY The Health and Safety at Work etc. Act 1974, and associated regulations, address the way in which health and safety should be tackled by all organisations. The purpose is to ensure the health, safety and welfare of employees and anyone who may be affected by the Trust s work activities. The Trust fulfils its legal responsibility for health and safety by: Maintaining a small team of professionals to provide advice and support in relation to health and safety matters; Offering and facilitating a range of classroom based health and safety training courses in addition to the emandatory modules; Measuring compliance with health and safety policies through Health and Safety Support Visits; Trust-wide and Divisional Health and Safety Performance Reports; Consulting, in various ways, with the workforce in relation to health, safety and welfare. This financial year, the team have built on and further embedded proactive systems designed to raise awareness, and as far as is reasonably practicable, prevent or reduce the risk of harm occurring. These included: Reviewing the following Policies and SOPs: Health and Safety Policy; Risk Management Procedure; Laser Safety File and Log Book (undertaken by the Division of Surgery); Non Clinical Slips, Trips Falls; DSE Policy (Display Screen Equipment) DSE Questionnaire and SOP DSE for Managers SOP DSE Eye and Eyesight Test SOP Personal Protective Equipment Policy Respiratory Protective Equipment SOP Driving for Work (Online Driving Licence Check) SOP Continuing to develop the Health and Safety Intranet Page; Ongoing work to develop the safety management systems in place for: the persistently highest reported non-clinical incidents i.e. sharps injuries and violence and aggression; COSHH (Control of Substances Hazardous to Health) DSE (Display Screen Equipment) Objective for The Health and Safety Team will continue to focus on developing Policies and Procedures where gaps have been identified and will review the Trust s Health and Safety Policies and SOPs to ensure they are up to date and aligned with current legislation. Status 3. OCCUPATIONAL HEALTH AND SAFETY MANAGEMENT SYSTEM (OH&SMS) One objective for the previous financial year was to identify weaknesses in the current system and identify areas for improvement and highlight priority topics to be addressed. The Legal Register below uses a red/amber/green colour code to indicate the perceived level of compliance: Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 4 of 17
159 Legend Currently enforced by HSE (taken from their legislation website) Enforced by the Police Considered to be: Non-compliant Partially compliant Compliant R A G Ref Date Legal or other requirement Subject Matter or Theme Acts Act or Statutory Instrument Guidance Division RAG Health and Safety at Work etc. Act General Management A N/A All A Employment Medical Advisory Service Act Enforcement A N/A HR G Health and Safety (Offences) Act Enforcement A N/A All N/A Corporate Manslaughter and Corporate Homicide Act Enforcement A N/A All N/A Health and Safety 'Six Pack' Management of Health and Safety at Work Regulations and Management of Health and Safety at Work Regulations Amendment Regulations 2006 General Management SI HSG65, INDG Health and Safety (Display Screen Equipment) Regulations as amended by the General Management - SI INDG36 All Health and Safety Miscellaneous Regulations 2002 Offices G Manual Handling Operations Regulations (as amended) General Management SI Leaflets All / M&H QSM G Personal Protective Equipment Regulations 2002 and (24a) Personal Protective General Management SI L25 All Equipment at Work (amended) Regulations G Provision and Use of Work Equipment Regulations Work Equipment SI L117, L112, All L114, L22 A Workplace (Health Safety and Welfare) Regulations General Management SI L60, L24 All G Other H&S Regulations (in alphabetical order) Classification, Labelling and Packaging (CLP) Regulations CLP SI G Confined Space Regulations Confined Spaces SI L101 E&F G Construction (Design and Management) Regulations Construction SI L153 E&F G Control of Artificial Optical Radiation at Work Regulations Radiation SI AOR Surgery A Control of Asbestos Regulations 2012 Asbestos SI Guidance L143 E&F G Control of Lead at Work Regulations Lead SI L132 E&F TBC Control of Noise at Work Regulations 2005 Noise SI L108 All A Control of Substances Hazardous to Health amendment Regulations 2003 and amendments (48a) 2002, (48b) 2004 All COSHH SI L5 All Control of Vibration at Work Regulations Vibration SI L141 All TBC Dangerous Substances (Notification and Marking of Sites) Regulations Dangerous Substances / SI N/A E&F Fire and Explosion TBC Dangerous Substances and Explosive Atmospheres Regulations Dangerous Substances / SI L138, L134, Fire Team Fire and Explosion L137, L133, TBC Electrical Equipment (Safety) Regulations Electrical Safety L135 All TBC Electricity at Work Regulations Electrical Safety SI L128 E&F G Employers' Liability (Compulsory Insurance) Act General Management G Gas Appliances (Safety) Regulations Gas SI E&F TBC The Gas Cooking Appliances (Safety) Regulations Gas SI E&F TBC Gas Safety (Installation and Use) Regulations Gas SI L56 E&F TBC Gas Safety (Management) Regulations Gas SI External N/A Gas Safety (Rights of Entry) Regulations Gas SI External N/A Good Laboratory Practice Regulations (as amended 2004) Biosafety SI? TBC Health and Safety (Consultation with Employees) Regulations General Management SI L95, CD207 All A The Health and Safety and Nuclear (Fees) Regulations Enforcement SI HSE47 N/A Health and Safety (First Aid at Work) Regulations (as amended 1995) General Management SI L43, L74 All G Health and Safety (Leasing Arrangements) Regulations General Management SI Procurement TBC Health and Safety (Safety Signs and Signals) Regulations General Management - SI L64 All TBC Signs Health and Safety (Sharp Instruments in Healthcare) Regulations Biosafety SI All A Health and Safety (Training for Employment) Regulations General Management SI N/A All TBC Health and Safety Information for Employees Regulations (as amended 2009) General Management SI N/A A Ionising Radiation (Medical Exposure) Regulations (IRMER) Radiation SI SSD TBC Ionising Radiation Regulations Radiation SI L121 SSD TBC Legionnaires' Disease: The Control of Legionella Bacteria in Water Systems Biosafety L8 E&F G Lifting Operations and Lifting Equipment Regulations Work Equipment SI L113 E&F A Lift Regulations 2016 Work Equipment E&F TBC 55 Plugs and Sockets etc. Safety Regulations 1994 Electrical Safety All TBC Pressure Equipment Regulations (as amended 2015) Work Equipment E&F TBC Pressure System Safety Regulations Pressurised Systems SI L122 and E&F TBC Leaflets Radiation (Emergency Preparedness and Public Information) Regulations Radiation TBC Registration, Evaluation, Authorisation and restriction of CHemicals (REACH) REACH N/A Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 1995 and General Management SI L73 All G RIDDOR (Amendment) 2012) Safety Representatives and Safety Committees Regulations General Management SI L87, L146 All G Supply of Machinery Regulations (as amended 2011) Work Equipment All TBC The Medicines (Administration of Radioactive Substances) Regulations (MARS) (as Radiation SSD amended 1995 and 2006) TBC Work at Height Regulations and (54a) Work at Height Regulations amendment Regulations Work at Height SI Falls All 2007 Guidance TBC G A Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 5 of 17
160 3.1 Risk Assessment The completion of risk assessments is a statutory requirement under the Management of Health and Safety at Work Regulations To support the Trust in its compliance, the Health and Safety Team continued to offer training in the Principles of Risk Assessment and provide advice and guidance in the development of risk assessments. The Trust has a Risk Management Process (SOP) (TW10/002) to support this Divisional Risk Register COSHH (Control of Substances Hazardous to Health): Progress against the COSHH risk has positive in this financial year. The COSHH risk score remains at 12 but it is anticipated that this will reduce in the new financial year , when any identified residual risk, specific to any challenges associated with local implementation, will transfer to respective Divisions. This year has seen: The Trust-wide launch of the Sevron COSHH365 online assessment system; The roll-out of a classroom based training programme on how to use the above system, which was mandatory for all nominated COSHH Co-ordinators and Ward/Department Managers. The appointment of a Pre-Employment Placement who assisted with the population of the on-line substance inventory. Health and Safety (Sharps in Healthcare) Regulations: In 2015 a dedicated working group was set up, which continues to meet regularly. The risk score, however, remains at 12 because, despite the positive work undertaken, the number of incidents reported remains stubbornly static. The Quality and Safety Committee agreed to post-incident training for those involved in such incidents. The Health and Safety Manager and Medical Equipment Nurse Specialist are in the process of developing this training course, which, it is hoped, will be in place by the autumn of First Aid at Work A review of the Trust s compliance against its business case was undertaken and whilst a small number of gaps were identified, the risk is now considered to be low, and the risk score reduced to a 3. Divisions have been advised of any gaps that exist and a Register of First Aiders has been circulated. Further training courses will be available in the new financial year Corporate Risk Register A risk assessment regarding the unacceptably high number of violent and aggressive incidents occurring within the Trust was placed on the register in this financial year. A risk score of 15 was awarded. The dedicated working group that was set up in 2015 continues to meet regularly and is making good progress against its action plan Safety Inspections Objective for Status Achieve 75% Divisional compliance with health and safety inspections; Achieve 75% completion of actions arising from health and safety inspections; Implement monitoring of health and safety inspections compliance. Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 6 of 17
161 In response to the objective set above, Divisions have confirmed the following compliance: Division % Health & Safety Inspections Completed % Actions Arising Completed Estates and Facilities Division 96% 85% Medicine Division 96% 83% Specialist Services Division 77% 85% Surgery Division 88% 55% 4. HEALTH AND SAFETY LEGISLATION AND HEALTH AND SAFETY EXECUTIVE (HSE) UPDATE 4.1. New Legislation The Control of Electromagnetic Fields at Work Regulations 2016 came into force in July Advice from the Trust s Radiation Protection Supervisor is being sought regarding any potential impact The Health and Safety and Nuclear (Fees) Regulations 2016 came into force in April The Regulations revoke Health and Safety (Fees) Regulations These Regulations relate to the HSE s Fees for Intervention (FFI). There is no additional impact on the Trust The guidance on the Health and Safety (Safety Signs and Signals) Regulations 1996 was updated. There is no additional impact for the Trust Health and Safety Consultations In this financial year there was only 1 consultation relevant to healthcare, which has now closed. For full details refer to Appendix HSE Intervention/Investigations specific to NHS Organisations Wrightington, Wigan and Leigh NHS Foundation Trust The Trust received an enquiry from the HSE regarding the Bioquell Q-10 Hydrogen Peroxide Vapour (HPV) machine. The HSE had received a concern from an employee who alleged that the gas detection sensor used in conjunction with the HPV machine, to detect whether or not a room was safe to be used, had been faulty resulting in employee(s) being exposed to unacceptably high levels of H2O2 (hydrogen peroxide) for several years. The HSE requested the Trust investigate this concern and provide a response to the allegation. The Trust was tasked with providing any supporting documentation that showed the adequacy and working condition of the H2O2 detection hardware i.e. Dräeger gas sensor, including inspection and maintenance records, and records of gas level recordings that had been taken. The HSE also requested the Trust clarify what steps had been taken, or would be taken, to address any identified weaknesses in the associated safety management system, which led to the concerns being raised. The above information was provided and the HSE confirmed a satisfactory response to the concerns raised had been provided, and based on the information made available the HSE did not intend to take any further action. Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 7 of 17
162 The Health and Safety Executive s Sector Plan for health and safety in public services was launched in draft. Their top 3 priorities are: Reducing the high levels of ill health from work-related stress and musculoskeletal disorders; Tackling specific safety issues in high-hazard activities, such as realistic training in the military; Maintaining established standards as service provision becomes fragmented and new forms of delivery emerge Other Healthcare Providers There were 6 prosecutions of a Healthcare Provider during this financial year: Royal Berkshire NHS Foundation Trust was prosecuted when a patient fell from a trolley and sustained a fractured neck while in x-ray and died later. The Trust was fined 200, with total costs awarded to the HSE of 76, University Hospitals of Morecambe Bay NHS Trust were prosecuted for the unsafe use of bedrails. The Trust was fined 100, with total costs awarded to HSE of 18, Pennine Care NHS Foundation Trust was prosecuted following the death of a patient who was taking part in an outdoor activity when he removed his buoyancy aid and jumped into the water in an attempt to end his own life. The Trust were fined a total of 30, with total costs awarded to the HSE of 51, St Christopher's Hospice was prosecuted following a diagnosis of legionella found in an inpatient. No fines were noted in this case but costs were awarded to the HSE in the sum of 25,000. Norfolk and Suffolk NHS Foundation Trust was prosecuted following the death of a patient by drowning on a specialist dementia ward. The Trust was fined 366,000 and ordered to pay costs of 12, Royal United Hospital (Bath) NHS Foundation Trust was prosecuted following the death of a vulnerable patient who fell to their death from a window. The Trust was fined 200, COMMUNICATION AND CONSULTATION 5.1. Occupational Safety and Health Committee The work to improve the functionality of the Committee, which began in , was completed in this financial year. The Committee has a nominated chairperson who has provided consistency and strong leadership. Objective for Review of: o Terms of Reference o Agenda o Workplan Status Divisional Health and Safety Groups Divisional Health and Safety Groups, with the exception of Estates and Facilities, have again struggled to hold meetings in this financial year often due to competing Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 8 of 17
163 work demand, and when meeting have been held, they have struggled to achieve quorum. Objective for Status Review of: o Terms of Reference o Agenda o Workplan 5.2. Health and Safety Intranet Page Significant progress has been made in this financial year in developing the Health and Safety Intranet Pages to ensure it s informative and user friendly. Objective for Work to continue on developing the Health and Safety Intranet Page. Status 6. HEALTH AND SAFETY TRAINING AND AWARENESS Training enables people to acquire the skills and knowledge necessary to make them competent members of staff and also influences their attitude and safety culture at work. The degree of training required depends on the complexity of the respective tasks and any existing level of competence. The Health and Safety Team offer a blended learning approach: 6.1. Classroom Based Classroom based health and safety training and awareness continues to remain popular with all course participants and feedback remains consistently positive. Since the introduction of classroom based health and safety training, 663 members of staff have been trained. The following courses have continued to run: CIEH Level 2 Health and Safety in the Workplace CIEH Level 3 Health and Safety in the Workplace Principles of Risk Assessment The Sevron COSHH365 Training Course, a system which holds the Trust-wide inventory for all hazardous substances and incorporates an online tool to assist with the development of COSHH risk assessments, was introduced in March 2017 and was mandatory for all nominated COSHH Co-ordinators and Ward/Department Managers. Below is a breakdown of courses by Division and by course type: Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 9 of 17

164 Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 10 of 17
165 The Health and Safety Manager has developed a Health and Safety Training Strategy. The Strategy has been used to develop a Health and Safety Training Plan and Training Needs Analysis (TNA). This ensures that health and safety training needs are incorporated into core skills required by staff and allows for the delivery of the required training through the training plan and TNA. It is hoped that the Health and Safety Training Strategy and Plan will be circulated for organisational consultation early in the new financial year emandatory Training The end of the financial year saw the Trustwide compliance with the emandatory 95% target had been achieved in the following 2 modules: Health and Safety = 96.5% Slips, Trips and Falls (Non-clinical) = 98.3% 6.3. Campaigns Violence and Aggression Working Group The following numbers of reported violence and aggression incidents have been reported: 2014/ / / The way in which violent or aggressive incidents were reported changed in , to recognise whether an violent or aggressive episode was as a result of a patient s medical condition or not. This change was welcomed by the workforce. A checklist to assist Wards and Departments to develop local risk assessments was created and is due to be rolled out in the new financial year, following a trial. A full review of training specific to violence and aggression has been undertaken. MAYBO training has been withdrawn and other training courses are being sourced. The Trust has opted for the Team Teach model for the Paediatric Services and consideration will be given in the new financial year as to the suitability of this training for vulnerable adults. Work is ongoing Sharps Injury Action Group The Sharps Injury Action Group continue to meet regularly; however, despite the good work of the group, sharps injuries remain one of the highest reported non-clinical incidents within the Trust. This year has highlighted the lack of local incident investigation post incident therefore, in the new financial year, the group will start to review incident investigation outcomes to establish if additional learning can take place and an investigation tool will be developed. The first Sharps and Needlestick Trauma Awareness (SANTA) campaign was held. The number of entries was disappointingly lower than anticipated but this did not distract from the quality of the displays produced. The importance of sharps awareness was very clear and the displays provided some new initiatives that could easily be further explored and implemented to make improvements. Work is ongoing. Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 11 of 17


166 7. NON-CLINICAL INCIDENT REPORTING The following data relates to the number of incidents reported that are specific to staff and organisational non-clinical incidents, and only includes the data that is relevant to health and safety and is not featured in the annual reports of other Specialist Advisors. This financial year saw an overall reported total of 824 incidents. The graph below plots the trends of reported incidents for the key categories broken down by quarter, commencing 1 st April st March 2017: Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 12 of 17
167 Below is a summary of incidents reported by sub category for the financial year As can be seen, incidents relating to needlesticks and sharps are the highest reported incident, followed very closely by adverse events that effect staffing levels Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 1995 (RIDDOR) The number of incidents reported to the HSE in compliance with RIDDOR was 29. Broken down as follows: Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 13 of 17


168 Incidents reported in this financial year are slightly lower than those reported in the last financial year (1). There was 1 incident reported in relation to patient falls. As can be seen from the graph opposite, the majority of reportable incidents were attributable to Over 7 Day Injury. Over-7-day injury - where a staff member is away from work for over three days as a result of the injury; Specified Injury - usually bone fracture; Dangerous occurrence no injury but significant injury could have resulted; Fatality Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 14 of 17
169 There was a decline in compliance with the reporting timescales laid out by RIDDOR during (16) in comparison to the number of RIDDOR reportable incidents in reported outside of timescales (9). 8. STATUS OF INCIDENT INVESTIGATIONS, CORRECTIVE AND PREVENTATIVE ACTIONS 8.1. Incident Investigation Analysis Like last year s annual report, over the year a number of non-clinical incidents were selected at random across all Divisions / Directorates to establish the extent and quality of incident investigation. The quality of investigations appears to have improved. 9. MEASURING PERFORMANCE 9.1. Health and Safety Support Visits The Health and Safety Team have completed 22 visits across the Trust. Health and Safety Support Visits continue to be positively received Health and Safety Performance Reports The Health and Safety Team continue to produce quarterly Health and Safety Performance Reports. These reports look at general health and safety performance from a Trust-wide and Divisional perspective. The reports are generally well received and form the basis of the majority of Divisional Health and Safety Groups and the Occupational Safety and Health Committee Audit, Monitoring and Review WARD / DEPARTMENT HEALTH AND SAFETY AUDITS An in-house health and safety audit was undertaken as part of the Health and Safety Support Visit programme in the Outpatient s Department, Leigh Infirmary. The only identified area for improvement was to complete new task based COSHH assessments once the new Sevron COSHH365 system is available EXTERNAL AUDITS Sidhill Ltd carried out an audit of bedrails at the request of the Trust, in November 2016 following a never event. The findings of the audit were shared with the Divisions for local action to be taken against the recommendations made. Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 15 of 17
170 10. HEALTH AND SAFETY OBJECTIVES The Health and Safety Team have identified the following objectives for the period Objectives 1. Work Equipment 2. COSHH 3. Achieve 75% Divisional compliance with the 12-monthly safety inspections Achieve 75% completion of actions arising from health and safety inspections Implement monitoring of health and safety inspections compliance 4. The Health and Safety Team will continue to focus on developing Policies and Procedures where gaps have been identified and will review the Trust s Health and Safety Policies and SOPs to ensure they are up to date and aligned with current legislation. 11. CONCLUSION The report highlights the work that has been undertaken during in contributing to the ongoing improvements in the management of health and safety in the Trust. The Health and Safety Team continue to improve visibility and awareness and provide advice and guidance to managers and staff to ensure they are able to meet the needs of the Trust in its compliance with health and safety legislation. The Team continue to engage with other specialist services within the Trust to assist in the development of future strategies. 12. ACTIONS REQUIRED The Trust Board and Senior Managers are asked to note and accept the content of this annual report and authorise its publication on the Intranet for access by employees, stakeholders and other interested parties. Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 16 of 17
171 HSE Consultations APPENDIX 1 Consultation Paper Implications Action Plan / Comments CLOSED CONSULATIONS 2016 / 2017 (note: there are no open consultations) CD282 - laying down basic safety standards for protection against the dangers arising from exposure arising to ionising radiation. Briefly the main changes are: Dose Limit for exposure to the lens of the eye and implementation of the Directive the Directive introduces a reduction of equivalent dose from 150mSv to 20mSv in a year. Currently exposure to ionising radiation is calculated and assessed on a calendar year basis, this would require individual dose limits to be re-calculated for the remainder of the year. HSE propose to introduce on 1st January 2018, to avoid confusion and any additional cost burden to businesses. Graded Approach - introduction of a new three tiered risk-based system of regulatory control. The Directive refers to these levels as notification, registration, and licensing - the higher the radiation protection risk associated with the work, the greater the requirements. It requires HSE to have in place a positive system of authorisation whereby permission is granted to duty holders for higher risk activities through registration and licensing. Began on and ended on Changes to the Ionising Radiation Regulations 1999 (IRR1999), with effect from 1 st January Advice from the Trust s Radiation Protection Supervisor has been sought any potential impact is being addressed. The Trust s Radiation Protection Advisor from The Christie has some concerns about one Consultant in respect of the proposed changes. Matter is being addressed within the Radiology Division. Document: Health and Safety Annual Report: 2016/2017 Date of Issue: May 2017 Author: Health and Safety Manager Page: 17 of 17
172
173 REPORT AGENDAA ITEM: 9.3 To: Board of Directors Date: 20 December 2017 Subject: Freedom to Speak Up Guardian 6 month report Presented by: Director of Workforce Purpose: Report Executivee summary The report gives an update from the Trust s Freedom to Speak Up Guardian in relation to developments and gives a summary from a recent review of raising concerns at another local Trust, considers how WWL can improve its own processes andd maintain an open culture of reporting. The report also reflects on the recent CQC inspection into Well Led, from the perspectivee of raising concerns. This report provides a summary on the cases referred to the Freedom to Speak Up Guardian, Local Anti-Fraud Specialist, Stafff side or HRR in relation to matters that are under the auspices of Raising Concerns (Whistleblowing) withinn the first 6 monthss of 2017/18 and to provide assurance these are being managed appropriately and in accordance with the Trust ss Raising Concerns Policy. Risks associated with this report Delivery of the trust objective to: Improve levels of Staff Engagement, developing a culture of confidencee and optimism where staff can directly influence change. Link(s) to The WWL Way 4wards Patients Performance People Partnerships
174
175 Freedom to Speak Up Guardian 6 month report
176 Freedom to Speak Up Guardian 6 Month Report December 2017 Aim The report provides an update from the Trusts Freedom to Speak Up (FTSU) Guardian on national or local developments in Raising Concerns or Whistleblowing during April to October This report advises on the outcome and conclusions from a review undertaken by the National Guardian s Office into a local Trust and reflects on this in terms of the Trust s practices and policies in relation to Raising Concerns. As the Trust has just complied with an inspection into the CQC s Key Line of Enquiry (KLOE) relating to Well-Led, this report also provides some reflection on the discussion undertaken when the FTSU Guardian was interviewed by the CQC inspection team. This report provides a summary on the cases referred to the Freedom to Speak Up Guardian, Local Anti-Fraud Specialist, Staff side or HR in relation to matters that are under the auspices of Raising Concerns (Whistleblowing) within April to October 2017/2018 and to provide assurance these are being managed appropriately and in accordance with the Trust s Raising Concerns Policy. 6 monthly 2017/18 Freedom to Speak Up (FTSU) Guardian Update - In the previous report to Trust Board, the FTSU Guardian reported that raising concerns activity and involvement from the FTSU Guardian had been limited during 2016/17. Over the last six months the FTSU Guardian has been involved in more concerns raised directly with them. Those concerns are outlined on page 6. The National Office for Freedom to Speak Up published their first case review in November Trusts or individuals can refer cases for review if it is considered that the concerns raised were not managed appropriately. A summary of the case review and the Trusts response is outlined below. The National Office is due to publish a revised job description for FTSU Guardians. The Trust s FTSU Guardian does not have dedicated or protected time to undertake the role and therefore could not be as active as Guardians whose day job is to undertake the role. The Trust maintains that concerns raised by staff should not all go to the Guardian. The Trust encourages staff to approach their line managers in the first instance and other routes, such as HR which are also outlined in the Raising Concerns Policy. The role will be reviewed following receipt of the new job description from the National Office. The focus for the next six months is to engage with more vulnerable groups in relation to FTSU. The FTSU Guardian will attend the BME Forum and Junior Doctors Forum to raise awareness of the Guardian role. The FTSU Guardian continues to attend the twice yearly National FTSU conferences and North West Network events. The National Guardian s Office review of Southport and Ormskirk Hospital NHS Trust This was conducted in response to workers speaking up. In particular, the National Guardian s Office received information that a bullying and discriminatory culture existed across the Trust. The purpose of the review was to find evidence of where speaking up processes, policies and culture did not meet with good practice and to make recommendations to remedy this. The Trust fully supported the review and provided all necessary information for its completion. The conclusion of the report was that there was evidence to suggest workers were not always supported to speak up and additionally that the Trust did not appropriately support black and ethnic minority workers. 3
177 The review however did conclude that there was evidence that, under the new leadership team, it was taking steps to improve the speaking up processes, policies and culture. The Trust has been asked to produce an action plan in response to the 22 recommendations made. The full report is available here:- FTSU review southportormskirk 20 The review and report, which is easy to follow and very informative, gives our Trust the opportunity to pause and consider the recommendations within the report and understand any potential risks in relation to current policies, procedures and culture, and contemplate any appropriate actions in response. The review identifies 22 recommendations. Each of these recommendations has been reflected on by the FTSU Guardian and Head of HR, who have determined that in general this Trust is complying with the themes within the report. There are however distinct areas where there are reminders, learning and potential actions for us to take forward in order to ensure we continue on our journey to encourage, and embrace, an open culture where concerns are raised as part of normal and natural practice across the organisation. Recognising the importance and maintenance of the visibility of senior leaders at all sites across the Trust in listening and resolving concerns; promoting the significance and need for staff to raise concerns; and how to speak up. The importance of the most senior leaders to set the tone and culture across the organisation. Opportunities to develop our managers further by facilitating bullying and harassment awareness sessions and additionally raising concerns awareness sessions. (This has been raised with the Trust s OD team to explore potential options as part of its leadership portfolio). Assurance that staff are confident that concerns will be investigated and responded to in a timely and appropriate manner. Consideration for minority groups and their specific concerns inclusive of BME Workers and also temporary workers such as trainees, volunteers and students. The FTSU Guardian and Head of HR recommend that this report is cascaded as appropriate to the senior management group within the Trust and encouraged to read and reflect in respect to the services they lead and their approach to listening and responding to concerns. Care Quality Commission (CQC) Well Led Inspection The CQC undertook their Well Led review over 3 days, commencing on 29 November During this time the CQC interviewed the FTSU Guardian to understand and question the approach both the Trust and the FTSU Guardian takes in respect of assuring the Trust Board that there are appropriate routes for employees to raise concerns and that these concerns are managed and dealt with in a suitable manner. During the discussion the FTSU Guardian was requested to consider if their substantive nonclinical role had any detrimental effect on undertaking the role of the FTSU Guardian such as resolving clinical concerns. The FTSU Guardian was also asked whether their role was independent enough to challenge all levels of staff inclusive of the Executive team. The FTSU Guardian was able to respond positively about the Trust s approach to raising concerns and how this role has been met with positivity and engagement from the staff as an additional and welcome route aside from line management, HR and staff side. 4
178 The CQC queried about the ability for staff to report in the absence of the FTSU Guardian during periods of annual leave. The FTSU Guardian gave assurance about the availability of alternative routes for reporting of concerns and reinforced the culture in the Trust for staff to raise concerns as part of everyday discussions with their teams and line management. The FTSU Guardian outlined the cohesive reporting mechanisms used by the HR, Local Anti- Fraud Specialist and FTSU Guardian in order for all formal issues to be captured in one location and providing full oversight by these stakeholders. 2017/ month update Reported concerns The recorded cases within 2017/18 totals 18. These matters are considered as formally raised issues. Within the stages of the Raising Concerns procedure there is the opportunity for individuals to raise matters informally initially. This informal process has been promoted with the Trust s open culture however in terms of capturing data we currently are unable to report the number of concerns that are raised and resolved informally, at source, via line management or another route such as Staff side, HR or the FTSU Guardian. It is important to note that concerns relating to bullying or harassing behaviour within employment may be raised via the Trust s Grievance process and/or via the Raising Concerns process therefore may be recorded via separate methods and reported as such, however all data is held within the HR department. The Trust actively promotes the raising of all employee concerns and therefore is happy to record matters according to the process under which they are reported. Formal Concerns - 18 matters have been recorded formally under the auspices of raising concerns during April to October 2017/18. Of these cases 12 were referred by the Local Anti-Fraud Specialist. Out of these 12 concerns the Local Anti-Fraud Specialist reports:- 5 individuals allegedly acted fraudulently 2 individuals allegedly making false representations 2 allegation of theft 2 allegations of combination of theft and fraudulent behaviour 1 allegation of bullying and harassment against colleagues Of these:- 7 matters were raised anonymously 5 matters were raised by individuals who disclosed their identity From these allegations:- 5 concerns were determined as having no evidence to support action. 3 matters have closed for Local Anti-Fraud Specialist but remain open for HR action. 1 matters closed with NHS Professionals follow up required. 1 matter closed with Local Anti-Fraud Specialist with referral made to trading standards and HR. 1 matter closed but referred to manager for consideration. 1 matter resolved as the employee resigned ahead of any evidence identified or action required The Local Anti-Fraud Specialist has recovered in redress monies for 2016/17, the total figure for 2017/18 will be reported in the 2017/18 annual report. The Local Anti-Fraud Specialist provides an annual report on matters to the Audit Committee; a bi-monthly update report to Audit 5
179 Committee and updates to the Director of Finance. Included within the updates and reports are outcomes from investigations; ongoing investigations; breaches of the Trust s Standing Financial Instructions; and financial redress from matters. There are 6 remaining concerns, all of which were initially received by, or referred in the first instance to the Trust s Freedom to Speak Up Guardian. Of these 6 matters, 4 were in relation to Quality and Safety and the remaining 2 related to Attitudes and Behaviours. Quality and Safety concern raised in relation to actions and behaviours displayed on a ward, with potential effect on patient care/experience. Union and HR both involved. Ongoing at October Attitude and Behaviour concern raised to FTSU Guardian in relation to behaviour of colleagues within team. HR and Executive awareness and supporting as appropriate. Ongoing at October Attitude and Behaviour concern was raised to the FTSU Guardian about line manager attitude. Informal discussions and actions agreed. Employee supported to discuss issue directly with manager. Matter closed. Quality and Safety concern referred to FTSU Guardian following to CEO. Concern raised in relation to IT systems. CEO responded directly. Matter closed. Quality and Safety FTSU Guardian contacted directly but anonymously. Concerns raised about staff behaviour on a ward within potential patient safety impact. Referred to Head of Nursing and action taken following the individual being identified as a worker provided by an external stakeholder. Corporate mortality review undertaken. Review showed no concerns or impact on patient safety. Matter closed. Quality and Safety FTSU Guardian contact directly but anonymously. Concern related to patient care possibly being at risk on a ward. Matter raised with Head of Nursing for Division. Head of Nursing to address context of concern within Senior Nurse meeting. Matter closed. From all concerns, inclusive of those where no evidence is identified, scrutiny is given to the tightening or modifying of policies or procedures so that greater assurance is possible in order to reduce further concerns where relevant. Where possible to give feedback to those individuals who have given contact details or a means of response, this has been undertaken in each case. 6
180 The following data shows a rolling 12 month summary of cases reported: 18 WHISTLEBLOWING NOV 16 OCT Quality & Safety Fraud Attitudes and Behaviours Policies, Processes and Procedures Raised via HR Raised via FTSU Guardian Raised via Counterfraud Matters raised in accordance with PIDA Whilst the Trust s Raising Concerns policy embraces but is not limited to those concerns or disclosures raised in accordance with the PIDA it should be noted which matters would qualify under this Act for the purposes of reporting. Qualifying disclosures are disclosures of information where the worker reasonably believes (and it is in the public interest) that one or more of the following matters is either happening, has taken place, or is likely to happen in the future. A criminal offence The breach of a legal obligation A miscarriage of justice A danger to the health and safety of any individual Damage to the environment Deliberate attempt to conceal any of the above. In this regard the Trust would report that within 2017/18 16 concerns have been reported which could qualify under the Act. Out of all concerns reported to date in 2017/18 there have been no conclusions that any reports or concerns raised have been made maliciously. Evaluation & Development The key stakeholders in raising concerns continue to reflect on improving processes and also the promotion of raising concerns within the organisation. The Local Ant-Fraud Specialist developed and promoted an online survey for staff within November in relation to fraud awareness and raising 7
181 concerns. There has also been promotion during November to refresh awareness to staff in regard to the importance of raising concerns. There is also a divisional risk held in relation to the impact on the Trust s CQC rating if employees approach an external body to report a concern if they are not assured that the Trust embraces the culture of promoting staff to report their concerns. The communication plan, talk safe initiative and new strategy all assist in increasing awareness. The risk currently stands at 6 and is held by the Workforce Division. Issues from within the 2017/18 cases have been reported to various forums within the year inclusive of Audit Committee and Workforce Committee where relevant to do so. The majority of matters reported are anonymous with regards to the Local Anti-Fraud Specialist however where the reporter is known and would like an understanding of progression of the case, appropriate feedback via a relevant representative, such as the FTSU Guardian, HR or Staff side is appointed. Supportive mechanisms are also offered to staff where appropriate. Additional information available linked to raising concerns:- NB This information was previously reported within the annual report presented in July 2017 and will be updated within the next annual report in June Staff Survey Report 2016 Reporting errors, incidents or near misses 90% of respondents felt the organisation encouraged them to report errors, incidents or near misses (91% in 2015) 74% of respondents felt the organisation takes action following to ensure that they do not happen again (78% in 2015) 54% of respondents felt they were given feedback about the changes made in response following a report of an error, incident or near miss (62% in 2015) Raising concern of unsafe clinical practice 93% respondents knew how to report a concern of unsafe clinical practice (93% also in 2015) 71% felt secure to raise a concern about unsafe clinical practice (72% in 2015) 65% in 2016 felt confident the organisation would address their concern about unsafe clinical practice (66% in 2015) Although the above results are not specifically identifiable against matters reported under the auspices of Raising Concerns, it is important to reflect on the outcome scores. Of the results above focus will be taken forward by the HR team and FTSU Guardian with the support of other stakeholders to ensure those staff who raise concerns are appropriately fedback to in order to recognise they have been heard by the Trust. Conclusion The Trust continues to maintain focus on raising concerns and key stakeholders work together to identify opportunities for improvement to the process and how to promote within the organisation. Recommendations The Trust Board is asked to consider if it continues to support the current approach taken by the Trust to maintain a culture of raising concerns and recommend any further actions to enhance or improve the current status. The Trust Board is asked to consider sharing the National Guardian s Office review of Southport and Ormskirk Hospital NHS Trust with the wider senior management team. 8

182 Southport and Ormskirk Hospital NHS Trust A case review of speaking up processes, policies and culture
Na. Acceptable (some apologies) x. Yes. Narrative report of the key issues of the meeting
 x. Yes. Narrative report of the key issues of the meeting") Chairpersons Report Chairpersons Name Carole Hudson Committee Name Audit Committee Date of Meeting 03.08.16 Name of Receiving Committee Trust Board Date of Receiving Committee meeting September 2016 Strategic
Chairpersons Report Chairpersons Name Carole Hudson Committee Name Audit Committee Date of Meeting 03.08.16 Name of Receiving Committee Trust Board Date of Receiving Committee meeting September 2016 Strategic
Chairpersons Report Chairpersons Name
 Chairpersons Report Chairpersons Name Tony Warne Committee Name Q&S Committee Date of Meeting 14.06.17 Name of Receiving Committee Trust Board Date of Receiving Committee meeting June 2017 Strategic Items
Chairpersons Report Chairpersons Name Tony Warne Committee Name Q&S Committee Date of Meeting 14.06.17 Name of Receiving Committee Trust Board Date of Receiving Committee meeting June 2017 Strategic Items
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
CENTRAL MANCHESTER UNIVERSITY HOSPITALS NHS FOUNDATION TRUST
 CENTRAL MANCHESTER UNIVERSITY HOSPITALS NHS FOUNDATION TRUST Report of: Paper prepared by: Gill Heaton -Director of Patient Services/Chief Nurse - Assistant Director of Nursing Date of paper: February
CENTRAL MANCHESTER UNIVERSITY HOSPITALS NHS FOUNDATION TRUST Report of: Paper prepared by: Gill Heaton -Director of Patient Services/Chief Nurse - Assistant Director of Nursing Date of paper: February
Summarise the Impact of the Health Board Report Equality and diversity
 AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
Cancer services improvement plan to achieve cancer standard August 2015
 Cancer services improvement plan to achieve cancer standard August 2015 Action Timeline to recovery Lead Officer Current Position Current RAG rating against timeline Key next steps General January 2016
Cancer services improvement plan to achieve cancer standard August 2015 Action Timeline to recovery Lead Officer Current Position Current RAG rating against timeline Key next steps General January 2016
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM)
") PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation Team YHSCN HULL AND EAST YORKSHIRE HOSPITALS Hull And East Yorkshire Hospitals Haematology MDT (13-2H-1) - 2015 Peer Review Visit
PEER REVIEW VISIT REPORT (MULTI-DISCIPLINARY TEAM) Network Organisation Team YHSCN HULL AND EAST YORKSHIRE HOSPITALS Hull And East Yorkshire Hospitals Haematology MDT (13-2H-1) - 2015 Peer Review Visit
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone Fax
 Agenda Item Meeting of Lanarkshire NHS Board 25 February 2009 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.co.uk WAITING TIMES 1.
Agenda Item Meeting of Lanarkshire NHS Board 25 February 2009 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.co.uk WAITING TIMES 1.
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10. Date of Meeting: 31 st August 2018 TITLE OF REPORT:
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting: 31 st August 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting: 31 st August 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Annual Members Meeting 27 September Gillian Norton, Chairman
 Annual Members Meeting 27 September 2018 Gillian Norton, Chairman Council of Governors update Kathryn Harrison, Lead Governor Celebrating the NHS at 70 A short film Patient story Libby Keating I ve had
Annual Members Meeting 27 September 2018 Gillian Norton, Chairman Council of Governors update Kathryn Harrison, Lead Governor Celebrating the NHS at 70 A short film Patient story Libby Keating I ve had
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
WAITING TIMES AND ACCESS TARGETS
 NHS Board Meeting Tuesday 17 December 2013 Lead Director (Acute Services Division) Board Paper No 13/60 Recommendation: WAITING TIMES AND ACCESS TARGETS The NHS Board is asked to note progress against
NHS Board Meeting Tuesday 17 December 2013 Lead Director (Acute Services Division) Board Paper No 13/60 Recommendation: WAITING TIMES AND ACCESS TARGETS The NHS Board is asked to note progress against
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Northern Ireland Peer Review of Cancer MDTs. EVIDENCE GUIDE FOR LUNG MDTs
 Northern Ireland Peer Review of Cancer MDTs EVIDENCE GUIDE FOR LUNG MDTs CONTENTS PAGE A. Introduction... 3 B. Key questions for an MDT... 6 C. The Review of Clinical Aspects of the Service... 8 D. The
Northern Ireland Peer Review of Cancer MDTs EVIDENCE GUIDE FOR LUNG MDTs CONTENTS PAGE A. Introduction... 3 B. Key questions for an MDT... 6 C. The Review of Clinical Aspects of the Service... 8 D. The
CT Scanner Replacement Nevill Hall Hospital Abergavenny. Business Justification
 CT Scanner Replacement Nevill Hall Hospital Abergavenny Business Justification Version No: 3 Issue Date: 9 July 2012 VERSION HISTORY Version Date Brief Summary of Change Owner s Name Issued Draft 21/06/12
CT Scanner Replacement Nevill Hall Hospital Abergavenny Business Justification Version No: 3 Issue Date: 9 July 2012 VERSION HISTORY Version Date Brief Summary of Change Owner s Name Issued Draft 21/06/12
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Governing Body meeting on 13th September 2018
 Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
: Geraint Davies, Director of Commercial Services
 Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Quality Assurance Accreditation Scheme Assignment Report 2016/17. University Hospitals of Morecambe Bay NHS Foundation Trust
 Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May 2016
 Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Liverpool Heart & Chest Hospital NHS Foundation Trust Thomas
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Liverpool Heart & Chest Hospital NHS Foundation Trust Thomas
Urology Clinical Forum. 11 th March 2015
 Urology Clinical Forum 11 th March 2015 Welcome and Introductions Justin Vale, Chair of the LCA Urology Pathway Group Progress of the Urology Pathway Group Justin Vale, Chair of the LCA Urology Pathway
Urology Clinical Forum 11 th March 2015 Welcome and Introductions Justin Vale, Chair of the LCA Urology Pathway Group Progress of the Urology Pathway Group Justin Vale, Chair of the LCA Urology Pathway
Revised Terms of Reference Trust Management Committee
 Revised Terms of Reference Trust Management Committee Safe & Effective Kind & Caring Exceeding Expectation Agenda Item No: 11.5 Meeting Date: 26 March 2018 Title: Revised Terms of Reference for Trust Management
Revised Terms of Reference Trust Management Committee Safe & Effective Kind & Caring Exceeding Expectation Agenda Item No: 11.5 Meeting Date: 26 March 2018 Title: Revised Terms of Reference for Trust Management
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Quality Committee (known as the Committee in these terms of reference) for the purpose of:
QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Quality Committee (known as the Committee in these terms of reference) for the purpose of:
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
Quality and Safety Committee Terms of Reference
 Approved May 2016 Quality and Safety Committee Terms of Reference 1. Constitution The Quality and Safety Committee is established as a sub-committee of The Hillingdon Hospitals NHS Foundation Trust (THH)
Approved May 2016 Quality and Safety Committee Terms of Reference 1. Constitution The Quality and Safety Committee is established as a sub-committee of The Hillingdon Hospitals NHS Foundation Trust (THH)
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
INTERNAL VALIDATION REPORT (MULTI-DISCIPLINARY TEAM)
") INTERNAL VALIDATION REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT GMCCN SALFORD ROYAL Salford Specialist Gynae MDT (11-2E-2) - 2011/12 Date Self Assessment Completed 30th June 2011 Date of IV Review
INTERNAL VALIDATION REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT GMCCN SALFORD ROYAL Salford Specialist Gynae MDT (11-2E-2) - 2011/12 Date Self Assessment Completed 30th June 2011 Date of IV Review
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Barnet Health Overview and Scrutiny Committee 6 October 2016
 Barnet Health Overview and Scrutiny Committee 6 October 2016 Title Health Tourism Report of Wards Status Urgent Key Enclosures Officer Contact Details Barnet Clinical Commissioning Group All Public No
Barnet Health Overview and Scrutiny Committee 6 October 2016 Title Health Tourism Report of Wards Status Urgent Key Enclosures Officer Contact Details Barnet Clinical Commissioning Group All Public No
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Central Alerting System (CAS) Policy
 Policy") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
CA1 Enhanced Supportive Care for Advanced Cancer Patients
 CA1 Enhanced Supportive Care for Advanced Cancer Patients Scheme Name QIPP Reference Eligible Providers CA1 Enhanced Supportive Care (ESC) Access for Advanced Cancer Patients QIPP 16-17 S23- Cancer Cancer
CA1 Enhanced Supportive Care for Advanced Cancer Patients Scheme Name QIPP Reference Eligible Providers CA1 Enhanced Supportive Care (ESC) Access for Advanced Cancer Patients QIPP 16-17 S23- Cancer Cancer
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Workforce and Organisational Development Committee. Minutes of the meeting held on in the Board Room, Ysbyty Gwynedd and via videoconference
 Workforce and Organisational Development Committee Minutes of the meeting held on 13.3.14 in the Board Room, Ysbyty Gwynedd and via videoconference Present: Dr P Higson Ms J Dean Dr C Tillson Mr K McDonogh
Workforce and Organisational Development Committee Minutes of the meeting held on 13.3.14 in the Board Room, Ysbyty Gwynedd and via videoconference Present: Dr P Higson Ms J Dean Dr C Tillson Mr K McDonogh
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Overall rating for this trust Good. Inspection report. Ratings. Are services safe? Requires improvement. Are services effective?
 Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Welcome. Annual Members Meeting 7 September Excellence in specialist and community healthcare
 Welcome Annual Members Meeting 7 September 2017 Excellence in specialist and community healthcare Gillian Norton, Chairman Introduction Excellence in specialist and community healthcare Louise Peters,
Welcome Annual Members Meeting 7 September 2017 Excellence in specialist and community healthcare Gillian Norton, Chairman Introduction Excellence in specialist and community healthcare Louise Peters,
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Annual Health and Safety Report 01 April March 2012
 Annual Health and Safety Report 01 April 2011 31 March 2012 Version 1.0 August 2012 Introduction The purpose of this report to provide Trust Board with information relating to performance, key developments
Annual Health and Safety Report 01 April 2011 31 March 2012 Version 1.0 August 2012 Introduction The purpose of this report to provide Trust Board with information relating to performance, key developments
Introducing a 7-day service: the benefits of increased consultant presence
 Introducing a 7-day service: the benefits of increased consultant presence This Future Hospital Programme case study comes from Wrightington, Wigan & Leigh NHS Foundation Trust (WWL). Here, Dr Stephen
Introducing a 7-day service: the benefits of increased consultant presence This Future Hospital Programme case study comes from Wrightington, Wigan & Leigh NHS Foundation Trust (WWL). Here, Dr Stephen
CLINICAL GOVERNANCE AND QUALITY COMMITTEE. Final - Terms of Reference - Final
 CLINICAL GOVERNANCE AND QUALITY COMMITTEE Final - Terms of Reference - Final CONSTITUTION 1. The Board of Directors approved the establishment of the Clinical Governance and Quality Committee (known as
CLINICAL GOVERNANCE AND QUALITY COMMITTEE Final - Terms of Reference - Final CONSTITUTION 1. The Board of Directors approved the establishment of the Clinical Governance and Quality Committee (known as
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016
 Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
Minutes of Part 1 of the Merton Clinical Commissioning Group Governing Body Tuesday, 26 th January 2016 Chair: Dr Andrew Murray Present: CC Cynthia Cardozo Chief Finance Officer CChi Dr Carrie Chill GP
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Report of the Care Quality Commission. May 2017
 Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Freedom to Speak Up Guardian Annual Report. Alison Balson, Director of Workforce. Approve Adopt Receive for information
 Trust Board Agenda Item 11a. Date: 26.07.17 Title of Report Purpose of the report and the key issues for consideration/decision Prepared by: me & Title Presented by: Freedom to Speak Up Guardian Annual
Trust Board Agenda Item 11a. Date: 26.07.17 Title of Report Purpose of the report and the key issues for consideration/decision Prepared by: me & Title Presented by: Freedom to Speak Up Guardian Annual
Quality, Safety & Experience (QSE) Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph
 Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph") 1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
AGENDA ITEM 17b Annex (i)
") QUALITY AND PATIENT SAFETY COMMITTEE Minutes of the meeting held on 10 th April 2014 Welsh Health Specialised Services Committee Offices Unit 3a, Van Road Caerphilly Business Park Caerphilly CF83 3ED Present
QUALITY AND PATIENT SAFETY COMMITTEE Minutes of the meeting held on 10 th April 2014 Welsh Health Specialised Services Committee Offices Unit 3a, Van Road Caerphilly Business Park Caerphilly CF83 3ED Present
Visit to Hull & East Yorkshire Hospitals NHS Trust
 Yorkshire and the Humber regional review 2014 15 Visit to Hull & East Yorkshire Hospitals NHS Trust This visit is part of a regional review and uses a risk-based approach. For more information on this
Yorkshire and the Humber regional review 2014 15 Visit to Hull & East Yorkshire Hospitals NHS Trust This visit is part of a regional review and uses a risk-based approach. For more information on this
Job Description. CNS Clinical Lead
 Job Description CNS Clinical Lead POST: BASE: ACCOUNTABLE TO: REPORTS TO: RESPONSIBLE FOR: CNS Clinical Lead St John s Hospice Head of Nursing and Quality Head of Nursing and Quality Community Clinical
Job Description CNS Clinical Lead POST: BASE: ACCOUNTABLE TO: REPORTS TO: RESPONSIBLE FOR: CNS Clinical Lead St John s Hospice Head of Nursing and Quality Head of Nursing and Quality Community Clinical
FULL TEAM AHEAD: UNDERSTANDING THE UK NON-SURGICAL CANCER TREATMENTS WORKFORCE
 FULL TEAM AHEAD: UNDERSTANDING THE UK NON-SURGICAL CANCER TREATMENTS WORKFORCE DECEMBER 2017 Publication date 04/12/17 Registered Charity in England and Wales (1089464), Scotland (SC041666) and the Isle
FULL TEAM AHEAD: UNDERSTANDING THE UK NON-SURGICAL CANCER TREATMENTS WORKFORCE DECEMBER 2017 Publication date 04/12/17 Registered Charity in England and Wales (1089464), Scotland (SC041666) and the Isle
Board of Directors Meeting
 Board of Directors Meeting Date: 30 July 2008 Agenda item: 10.2, Part 1 Title: Prepared by: Presented by: Action required: Elaine Hobson, Director of Operations Elaine Hobson, Director of Operations The
Board of Directors Meeting Date: 30 July 2008 Agenda item: 10.2, Part 1 Title: Prepared by: Presented by: Action required: Elaine Hobson, Director of Operations Elaine Hobson, Director of Operations The
MDT Peer Review Report Proforma
 Network Trust NICaN Western Health and Social Care Trust Lung MDT Visit Date 13 September 2017 Structure and function of the service The Western Health and Social Care Trust (WHSCT) was established on
Network Trust NICaN Western Health and Social Care Trust Lung MDT Visit Date 13 September 2017 Structure and function of the service The Western Health and Social Care Trust (WHSCT) was established on
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board. Audit year: Issued: October 2015 Document reference: 491A2015
 Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12. Date of Meeting: 23 rd March 2018 TITLE OF REPORT:
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12 Date of Meeting: 23 rd March 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12 Date of Meeting: 23 rd March 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
YORKSHIRE AMBULANCE SERVICE NHS TRUST Quality Improvement Action Plan 23/05/1017 FINAL. Deputy/ Associate Director. Executive Director TRUST WIDE
 YORKSHIRE AMBULANCE SERVICE NHS TRUST Quality Improvement Action Plan 23/05/1017 FINAL CQC findings TRUST WIDE 1.1 1.2 Ensure that at all times there are qualified experienced staff (including Staff communication
YORKSHIRE AMBULANCE SERVICE NHS TRUST Quality Improvement Action Plan 23/05/1017 FINAL CQC findings TRUST WIDE 1.1 1.2 Ensure that at all times there are qualified experienced staff (including Staff communication
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST COUNCIL OF GOVERNORS NATIONAL CANCER PATIENT EXPERIENCE SURVEY 2014
 Agenda item 7(v) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST COUNCIL OF GOVERNORS NATIONAL CANCER PATIENT EXPERIENCE SURVEY 2014 1. INTRODUCTION AND OVERVIEW The Cancer Patient Experience Survey
Agenda item 7(v) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST COUNCIL OF GOVERNORS NATIONAL CANCER PATIENT EXPERIENCE SURVEY 2014 1. INTRODUCTION AND OVERVIEW The Cancer Patient Experience Survey
REFERRAL TO TREATMENT ACCESS POLICY
 Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Overview. Dr Stephen Gulliford & AKI Specialist Nurse Suzanne Wilson Page 1
 Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Summary Annual Report 2017/18
 Summary Annual Report 2017/18 Reporting back Guy s and St Thomas has, once again, performed well both operationally and financially, despite a challenging year which has seen unprecedented demand on our
Summary Annual Report 2017/18 Reporting back Guy s and St Thomas has, once again, performed well both operationally and financially, despite a challenging year which has seen unprecedented demand on our
INTERNAL VALIDATION REPORT (MULTI-DISCIPLINARY TEAM)
") INTERNAL VALIDATION REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT GMCCN SALFORD ROYAL Salford Pituitary MDT Neuroscience MDT (11-2K-4) - 2011/12 Date Self Assessment Completed 15th December 2011 Date
INTERNAL VALIDATION REPORT (MULTI-DISCIPLINARY TEAM) Network Trust MDT GMCCN SALFORD ROYAL Salford Pituitary MDT Neuroscience MDT (11-2K-4) - 2011/12 Date Self Assessment Completed 15th December 2011 Date
Please indicate: For Decision For Information For Discussion X Executive Summary Summary
 Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
2. This year the LDP has three elements, which are underpinned by finance and workforce planning.
 Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
Policies, Procedures, Guidelines and Protocols
 Policies, Procedures, Guidelines and Protocols Document Details Title Complaints and Compliments Policy Trust Ref No 1353-29025 Local Ref (optional) N/A Main points the document This policy and procedure
Policies, Procedures, Guidelines and Protocols Document Details Title Complaints and Compliments Policy Trust Ref No 1353-29025 Local Ref (optional) N/A Main points the document This policy and procedure
South Powys Cluster Plan
 South Powys Cluster Plan 2016-17 The Cluster Network Development Domain with the Quality & Outcomes Framework supports medical practices to work collaboratively to: Understand local health needs and priorities
South Powys Cluster Plan 2016-17 The Cluster Network Development Domain with the Quality & Outcomes Framework supports medical practices to work collaboratively to: Understand local health needs and priorities
WAITING TIMES AND ACCESS TARGETS
 NHS Board Meeting Tuesday 17 February 2015 Chief Officer (Acute Services) Board Paper No.15/08 WAITING TIMES AND ACCESS TARGETS Recommendation: The NHS Board is asked to note progress against the national
NHS Board Meeting Tuesday 17 February 2015 Chief Officer (Acute Services) Board Paper No.15/08 WAITING TIMES AND ACCESS TARGETS Recommendation: The NHS Board is asked to note progress against the national
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11 PAGE 2 WE PLAN. WE ACHIEVE We achieve 2009/10 was another great year
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11 PAGE 2 WE PLAN. WE ACHIEVE We achieve 2009/10 was another great year
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 26 th January 2106 Agenda No: 5 Attachment: 04 Title of Document: Clinical Chair and Chief Officer Report Report Author: Adam
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 26 th January 2106 Agenda No: 5 Attachment: 04 Title of Document: Clinical Chair and Chief Officer Report Report Author: Adam
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Minutes of a meeting of the Governance and Risk Committee held on 25 th June 2008 held in the Boardroom at Trust Headquarters.
 2 Minutes of a meeting of the Governance and Risk Committee held on 25 th June 2008 held in the Boardroom at Trust Headquarters. TOP THREE RISKS DISCUSSED 1. Decontamination Wrightington Theatres 2. BAF
2 Minutes of a meeting of the Governance and Risk Committee held on 25 th June 2008 held in the Boardroom at Trust Headquarters. TOP THREE RISKS DISCUSSED 1. Decontamination Wrightington Theatres 2. BAF
Meeting people s needs A Wales Cancer Alliance Policy Paper Summer 2017
 Meeting people s needs A Wales Cancer Alliance Policy Paper Summer 2017 Meeting people s needs: overview More work needs to be done to meet the needs of patients, both as they undergo treatment for cancer
Meeting people s needs A Wales Cancer Alliance Policy Paper Summer 2017 Meeting people s needs: overview More work needs to be done to meet the needs of patients, both as they undergo treatment for cancer
Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018
 Produced in February 2018") 6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
INFORMATION REQUEST UNDER THE FREEDOM OF INFORMATION ACT 2000
 Trust HQ The Elms RAEI Wigan Lane Wigan WN1 2NN Mr Andrew Foster, Chief Executive Email: Andrew.foster@wwl.nhs.uk Ref: FOI2012/1316 Date Received: 19/07/2012 Response Due: 16/08/2012 20 th August 2012
Trust HQ The Elms RAEI Wigan Lane Wigan WN1 2NN Mr Andrew Foster, Chief Executive Email: Andrew.foster@wwl.nhs.uk Ref: FOI2012/1316 Date Received: 19/07/2012 Response Due: 16/08/2012 20 th August 2012
NHS England (Wessex) Clinical Senate and Strategic Networks. Accountability and Governance Arrangements
 Clinical Senate and Strategic Networks. Accountability and Governance Arrangements") NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
COMMISSIONING SUPPORT PROGRAMME. Standard operating procedure
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE COMMISSIONING SUPPORT PROGRAMME Standard operating procedure April 2018 1. Introduction The Commissioning Support Programme (CSP) at NICE supports the
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE COMMISSIONING SUPPORT PROGRAMME Standard operating procedure April 2018 1. Introduction The Commissioning Support Programme (CSP) at NICE supports the
(Committee Chair) Chair) Asst. Lead Director for Children & Strategic Lead for Mental Health. Head of Estates and Property (MHSA/16/01-08 only)
 Chair) Asst. Lead Director for Children & Strategic Lead for Mental Health. Head of Estates and Property (MHSA/16/01-08 only)") POWYS TEACHING HEALTH BOARD MENTAL HEALTH SERVICES ASSURANCE COMMITTEE CONFIRMED MINUTES OF THE MEETING HELD ON THURSDAY 07 JANUARY 2016, AT 09.30AM, HAFREN TRAINING ROOM, HAFREN WARD, BRONLLYS HOSPITAL
POWYS TEACHING HEALTH BOARD MENTAL HEALTH SERVICES ASSURANCE COMMITTEE CONFIRMED MINUTES OF THE MEETING HELD ON THURSDAY 07 JANUARY 2016, AT 09.30AM, HAFREN TRAINING ROOM, HAFREN WARD, BRONLLYS HOSPITAL
Presentation to the Care Quality Commission. Dr. Lucy Moore, CEO 15 September 2015
 Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious