Patient Safety Initiatives of the VA National Center for Patient Safety
|
|
|
- Rebecca Jenkins
- 6 years ago
- Views:
Transcription
1 Patient Safety Initiatives of the VA National Center for Patient Safety At the Quality Colloquium at Harvard University John Gosbee, MD, MS August 27, 2003 National Center for Patient Safety Department of Veterans Affairs Ann Arbor, MI
2 Presentation Overview What is VA? What is National Center for Patient Safety? Example initiatives Tool development Correct surgery directive Curriculum development Lowlights Highlights My Predictions 2
3 Veterans Health Administration 21 Veterans Integrated Service Networks I N J ANUARY 2002 VISN S 13 AND 14 WERE INTEGRATED AND RENAMED VISN 23 3
4 Veterans Health Administration Facilities 163 Hospitals 800 Hospital and Community-Based Clinics 135 Nursing Homes (Long-Term Care) Size 21,000 Beds 185,000 Staff 4 Million Patients 4
5 Origin of the VA Patient Safety Improvement Program VA identified patient safety as a high priority issue in 1997 and began a Patient Safety Improvement Initiative. The VA s National Center for Patient Safety was designed in 1998/1999 to: Develop the tools and training to make it happen Use local multidisciplinary teams to analyze reports. Analyze common safety issues and solutions Recognize the importance of close call analysis in strategies to prevent adverse events. 5
6 It s a Full-Time Job NCPS Personnel Legal, medical, nursing, pharmacy, engineering, etc Senior managers, analysts, information specialists Hands-on ( is our enemy!) Patient Safety Managers Hired or assigned for each of 163 VA hospitals and each of the 21 networks Report to facility management, not NCPS. Doing RCAs and other safety activities takes Additional 200 FTEs/yr spread throughout VA 6
7 Not Blame Free, But Just and Appropriate Accountability Adverse Events and RCAs are protected by VAspecific statute: 38 USC-5705 Not discoverable Confidential (cannot be used for personnel action) Intentionally unsafe acts not part of the safety system defined as a criminal act; a purposefully unsafe act; an act related to alcohol or substance abuse by an impaired provider and/or staff; or events involving alleged or suspected patient abuse of any kind. Adverse events and close calls are screened for 1) Actual AND potential severity of the event 2) Probability of occurrence according to specific definitions. 7
8 Products of the VA Patient Safety Program Guidance is provided via Courses (Patient Safety 101 and Patient Safety 202) Regional workshops (RCA and HFMEA) Newsletter (Topics in Patient Safety -- TIPS) Monthly conference calls Patient Safety Alerts and Advisories Based on information from RCAs and other sources Vulnerabilities are especially serious and specific Measures have been identified to prevent or reduce occurrence 8
9 NCPS-developed Patient Safety Tools Cognitive aid: Triage Questions for RCAs Series of questions that help the identification of root causes in six major areas Five Rules of Causation (Adapted from David Marx) Other cognitive aids on laminated cards & posters Healthcare Failure Mode and Effect Analysis (HFMEA) Advanced Root Cause Analysis Tools Escape and Elopement Management Fall Prevention and Management 9
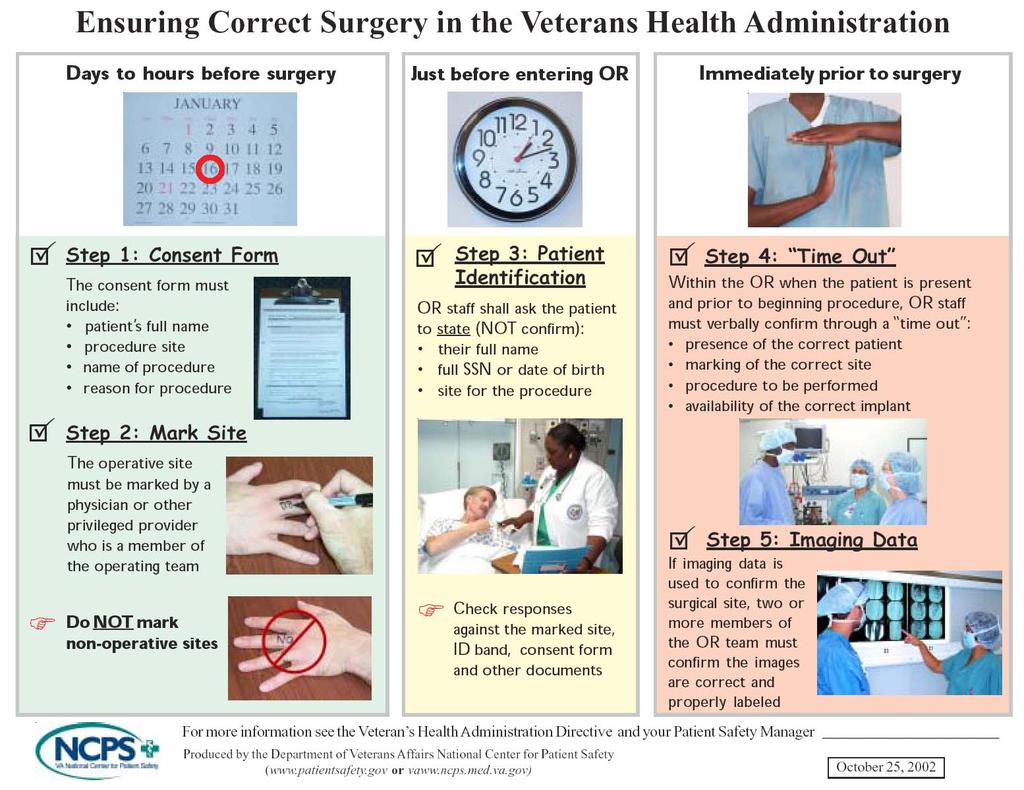
10 Ensuring Correct Surgery: VHA Directive (Policy) # Ensure: Correct patient Correct site Correct procedure Correct implant (if applicable) 10
11 Summary of VA Root Cause Analyses: 44% were left-right mix-ups on the correct patient 36% were wrong patient 14% were wrong implant or procedure on correct patient 7% were wrong site (not left-right) on correct patient 11
12 Location of the Event Eye Groin or Genitals Chest Leg Hand, Wrist, or Finger Abdomen Back Head, Neck, Mouth, Anus, Colon, Buttock 12
13 13
14 Current Status NCPS Implementation materials Poster Patient Brochure Videotape Power Point Presentation and CD-ROM Results to date No reports of in-or adverse events Related Challenges Preventing adverse events associated with out-of-or invasive procedures 14
15 Patient Safety Curriculum for Medical Residents It is the right thing to do Necessary part of treating the whole patient Healthcare facilities need resident participation in RCAs and HFMEAs ACGME, AAMC, IOM, JCAHO Example: ACGME core competencies 15
16 Quote It helps you attack the problem [of patient safety], instead of avoid it ; I think I was very impacted by your course...stuff that was thought to be common sense does need study (Excerpt from follow-up phone interview to resident patient safety rotation in 1999 at Michigan State University) 16
17 Goals of the VA Curriculum Agent of change towards systems and quality approach, and away from blame and train model Incorporate understanding of human performance & high reliability organizations into Patient care Patient safety activities Become a better consumer and implementer of computer and medical device technology 17
18 Six Teaching Modules 1. Patient safety overview (interactive presentation - IP) 2. Human factors engineering - patient safety (IP) 3. Effective patient safety interventions (IP) 4. Root Cause Analysis RCA (exercise) 5. Usability testing group project (exercise) 6. Journal club (interactive group discussion) 18
19 Pilot Tested at Several VA s and University Affiliates (2002-3) Mostly volunteers from over 12 sites Mixture of allies Leaders in resident education Educators fresh out of residency VA Patient Safety Managers Modules tested many times many ways Outcome and Findings? Modules 2-5 significantly better than 1 Meeting report from retreat in progress Make it real, hands-on, you know, the usual 19
20 RCA Categorization & Analysis Field Reports of Adverse Events & Close Calls Prioritize SAC Score Safety Reports Root Cause Categories Based on Triage Card questions used NCPS Data Classification and Analysis Goal Is To Prevent Harm To The Patient Change Happens Locally Validate and Investigate For Widespread Use Pseudo Trends Can Point To Need For RCA 20
21 Major influences 1998 VA Patient Safety Advisory Committee Narrative, narrative, narrative Avoid boxing people in James Farrier (aviation safety database expert) Narrative is key Premature categorization cheapens, hurts reports Even experts can not agree on agreed upon terms Chris Johnson (Univ. of Glasgow Accident Analysis Group) Most databases serve researchers and policy people Not designers, builders, operations people 21
22 Other Considerations Many categories sound logical, easy, fast, In real-life application, they are not NCPS can t use taxonomies that contradict major policies and philosophies Violation of policy is not a root cause Title of person involved with the event is not generally useful and potentially harmful If category does not inform us on a solution, it it is not useful 22
23 Five Categories Done at NCPS 1. Location (49) Some nested Major and minor 2. Event Outcome (8) (e.g., fall, suicide, other) 3. Activity or Process (24) 4. Actions (32) 5. Outcome Measures (11) 23
24 Special Analysis and Classifications Completed and online (see MRI hazards Oxygen Cylinders (see web site) Used to Develop Policy Patient Misidentification Wrong Site Surgery In Progress Suicide Elopement/wandering Wrong Tube, Wrong Hole, Wrong Connector Retained Sponges 24
25 Natural Language Processing Early stages of scoping this work Synonyms for our keywords are many, and some hard to see in a sea of text As conceptual understanding changes, manual recategorization unlikely It may lead to learning system that finds trends we could not across thousands of RCAs 25
26 Recognition of the VA Patient Safety Program Interest and adoption by health care systems of Japan United Kingdom Denmark (translating RCA cognitive aids) Australia (implementing some of VA system nationwide) An honor to receive Innovations in American Government Award (Kennedy School of Government at Harvard University) John Eisenberg Award (AHA?) 26
27 Challenges (Lowlights) Implementation of safety interventions Hard to do right Often boring Everyone gets worse, some stay Learning curve dips down before slow rise Similar findings in aviation, manufacturing Enthusiastic, but mostly under qualified personnel Teaching is hard, thankless, non-reimbursable 27
28 Implementation of safety interventions Hard to do right A theme repeated often in this Colloquium Made worse by rare use of human factors engineering iterative design methods Often boring Mere details are the project 28
29 At first, everyone gets worse (Similar findings in aviation, manufacturing) Active Involvement Quality Passive Involvement Time 29
30 Enthusiastic, but mostly under qualified personnel Teaching complexity of safety and healthcare system is hard Innovation has gone nearly thankless Clinical patient safety work is nonreimbursable 30
31 Successes (Highlights) Huge increase in REPORTED close calls Full analyses (RCAs) on close calls Honest change of heart by many Establishing primary care patient safety as acceptable career route Changing existing or future device design 31
32 My predictions The following are not necessarily the recommendations or conclusions of VA, VA NCPS, or others. 32
33 More Information Available NCPS information and resources are available at: One-page handouts (backgrounders) in your course packet 33
A Systems Approach to Patient Safety at the VA
 BRIGHT IDEAS A Systems Approach to Patient Safety at the VA Erika Hatva The Department of Veterans Affairs (VA) operates the largest integrated healthcare system in the United States, serving 8.76 million
BRIGHT IDEAS A Systems Approach to Patient Safety at the VA Erika Hatva The Department of Veterans Affairs (VA) operates the largest integrated healthcare system in the United States, serving 8.76 million
Department of Defense INSTRUCTION. SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP)
 Patient Safety Program (PSP) (MHSPSP)") Department of Defense INSTRUCTION NUMBER 6025.17 August 16, 2001 SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP) ASD(HA) References: (a) Sections 742 and 754 of the Floyd D.
Department of Defense INSTRUCTION NUMBER 6025.17 August 16, 2001 SUBJECT: Military Health System (MHS) Patient Safety Program (PSP) (MHSPSP) ASD(HA) References: (a) Sections 742 and 754 of the Floyd D.
National Health Regulatory Authority Kingdom of Bahrain
 National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
National Health Regulatory Authority Kingdom of Bahrain THE NHRA GUIDANCE ON SERIOUS ADVERSE EVENT MANAGEMENT AND REPORTING THE PURPOSE OF THIS DOCUMENT IS TO OUTLINE SERIOUS ADVERSE EVENTS THAT SHOULD
ADMINISTRATIVE POLICY & PROCEDURE PATIENT SAFETY PLAN
 PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
PAGE #: 1 of 6 CROSS REFERENCES: Administrative Policy PI-01: Administrative Policy PI-03: Administrative Policy RI-20: Administrative Policy EC-25: Sentinel Event Risk Management Plan Guidelines for Disclosure
NERC Improving Human Performance
 NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
NERC Improving Human Performance Sentinel Event Reporting, Analysis and Prevention in Healthcare March 28, 2012 Charles A. Mowll, FACHE, CSSBB Executive Vice President The Joint Commission Healthcare Worker
February New Zealand Health and Disability Services National Reportable Events Policy 2012
 February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
February 2012 New Zealand Health and Disability Services National Reportable Events Policy 2012 Table of Contents 1. Purpose 2. Treaty of Waitangi 3. Background 4. Scope 5. Policy 6. Review and Evaluation
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Never Events LISA Matt Provost
 Never Events LISA 2017 Matt Provost mattpro@yelp.com/@hypersupermeta Yelp s Mission Connecting people with great local businesses. History of the NHS World s first universal health care system - June 1948
Never Events LISA 2017 Matt Provost mattpro@yelp.com/@hypersupermeta Yelp s Mission Connecting people with great local businesses. History of the NHS World s first universal health care system - June 1948
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
Root Cause Analysis: The NSW Health Incident Management System
 Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
Root Cause Analysis: The NSW Health Incident Management System SARAH MICHAEL, RN, GradDipQHCM PAUL DOUGLAS, MB, BS, DRACOG, MHA, FRACMA With a background in intensive care, Sarah is a Principal Analyst
VA Radiotherapy Incident Reporting and Analysis System (RIRAS)
") VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
Incident Reporting Systems and Future Strategies for Patient Safety Improvement
 WHITE PAPER: Incident Reporting Systems and Future Strategies for Patient Safety Improvement Author: Datix Date: 2016/17 Driving down harm How can healthcare providers most successfully pursue the goal
WHITE PAPER: Incident Reporting Systems and Future Strategies for Patient Safety Improvement Author: Datix Date: 2016/17 Driving down harm How can healthcare providers most successfully pursue the goal
(10+ years since IOM)
") Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Preventing Serious Reportable Events in Health Care
 Preventing Serious Reportable Events in Health Care The National Quality Forum (NQF), a coalition of public and private healthcare sector leaders who are focused on improving healthcare quality and patient
Preventing Serious Reportable Events in Health Care The National Quality Forum (NQF), a coalition of public and private healthcare sector leaders who are focused on improving healthcare quality and patient
Measurability of Patient Safety
 Measurability of Patient Safety Marsha Fleischer IMPO Conference, November 17, 2016 External requirements in Germany lead to a higher need for safety and risk management, among others arising from the:
Measurability of Patient Safety Marsha Fleischer IMPO Conference, November 17, 2016 External requirements in Germany lead to a higher need for safety and risk management, among others arising from the:
BAY-ARENAC BEHAVIORAL HEALTH AUTHORITY POLICIES AND PROCEDURES MANUAL
 Page: 1 of 14 Policy It is the policy of Bay-Arenac Behavioral Health Authority (BABHA) that all adverse events, such as unusual events (including risk), critical incidents (including all deaths) and sentinel
Page: 1 of 14 Policy It is the policy of Bay-Arenac Behavioral Health Authority (BABHA) that all adverse events, such as unusual events (including risk), critical incidents (including all deaths) and sentinel
The goal of this checklist is to provide tips and approaches to lead and build a culture of safety in your team.
 Checklist for Building a Safety Culture The goal of this checklist is to provide tips and approaches to lead and build a culture of safety in your team. Create knowledge and understanding of patient safety
Checklist for Building a Safety Culture The goal of this checklist is to provide tips and approaches to lead and build a culture of safety in your team. Create knowledge and understanding of patient safety
United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI)
") United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI) March 11, 2015 Laura Lally, Caring Communities Victor Lane Rose, ECRI
United Methodist Association National Conference Integrating Risk Management and Quality Assurance and Performance Improvement (QAPI) March 11, 2015 Laura Lally, Caring Communities Victor Lane Rose, ECRI
FAMILY PHARMACEUTICAL SERVICES NOTICE OF PRIVACY PRACTICES effective 9/23/2013
 FAMILY PHARMACEUTICAL SERVICES NOTICE OF PRIVACY PRACTICES effective 9/23/2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
FAMILY PHARMACEUTICAL SERVICES NOTICE OF PRIVACY PRACTICES effective 9/23/2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
#104 - Prevention of Medical Errors [1]
![#104 - Prevention of Medical Errors [1]](/thumbs/74/70423609.jpg "#104 - Prevention of Medical Errors [1]") Published on Excellence In Learning (https://excellenceinlearning.net) Home > #104 - Prevention of Medical Errors #104 - Prevention of Medical Errors [1] Please login [2] or register [3] to take this course.
Published on Excellence In Learning (https://excellenceinlearning.net) Home > #104 - Prevention of Medical Errors #104 - Prevention of Medical Errors [1] Please login [2] or register [3] to take this course.
NOTICE OF PRIVACY PRACTICES
 Amended September 2013 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Amended September 2013 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY.
Optimizing Medical Device Safety: A Closed Loop Process
 Optimizing Medical Device Safety: A Closed Loop Process Session #149, February 22, 2017, 8:30AM Shelly Crisler & Katrina Jacobs US Department of Veterans Affairs 1 Speaker Introduction Shelly Crisler,
Optimizing Medical Device Safety: A Closed Loop Process Session #149, February 22, 2017, 8:30AM Shelly Crisler & Katrina Jacobs US Department of Veterans Affairs 1 Speaker Introduction Shelly Crisler,
GAO INDUSTRIAL SECURITY. DOD Cannot Provide Adequate Assurances That Its Oversight Ensures the Protection of Classified Information
 GAO United States General Accounting Office Report to the Committee on Armed Services, U.S. Senate March 2004 INDUSTRIAL SECURITY DOD Cannot Provide Adequate Assurances That Its Oversight Ensures the Protection
GAO United States General Accounting Office Report to the Committee on Armed Services, U.S. Senate March 2004 INDUSTRIAL SECURITY DOD Cannot Provide Adequate Assurances That Its Oversight Ensures the Protection
Alpert Medical School of Brown University Clinical Psychology Internship Training Program Rotation Description
 Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
Rotation Title: Neuropsychology Track Neuropsychological Assessment Rotation Location: VA Medical Center Rotation Supervisor(s): Stephen Correia, Ph.D. (Primary Supervisor) Megan Spencer, Ph.D. Donald
Financial Disclosure. Learning Objectives: Preventing and Responding to Sentinel Events in Surgery 10/13/2015
 Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Preventing and Responding to Sentinel Events in Surgery Beverly Kirchner, BSN, RN, CNOR, CASC April 2014 Financial Disclosure I DO NOT have an actual, potential or perceived conflict of interest to disclose
Design Considerations for a Patient Safety Improvement Reporting System
 Design Considerations for a Patient Safety Improvement Reporting System By Brian Raymond and Robert M. Crane Institute for Health Policy Kaiser Permanente One Kaiser Plaza Oakland, CA 94612 April 2001
Design Considerations for a Patient Safety Improvement Reporting System By Brian Raymond and Robert M. Crane Institute for Health Policy Kaiser Permanente One Kaiser Plaza Oakland, CA 94612 April 2001
Serious Reportable Events in Healthcare 2011 Update
 Serious Reportable Events in Healthcare 2011 Update July 19, 2011 1 Overview Purpose 2002, 2006, 2011 Facilitate uniform, comparable public reporting Enable systematic learning Ensure currency & appropriateness
Serious Reportable Events in Healthcare 2011 Update July 19, 2011 1 Overview Purpose 2002, 2006, 2011 Facilitate uniform, comparable public reporting Enable systematic learning Ensure currency & appropriateness
The Patient Safety Act Reporting and RCA Requirements
 The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
ECRI Patient Safety Organization HFACS and Healthcare
 October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
October 15, 2015 ECRI Patient Safety Organization HFACS and Healthcare Thomas W. Diller, MD, MMM VP System Chief Medical Officer CHRISTUS Health Learning Objectives Understand the human factors errors
ETHICAL CONSIDERATIONS THAT ARISE IN LONG TERM CARE PART 2 REPORTING OBLIGATIONS
 ETHICAL CONSIDERATIONS THAT PART 2 REPORTING OBLIGATIONS Brian D. Pagano, Esq Burns White LLC bdpagano@burnswhite.com Event: Different Types of Events A discrete, auditable, and clearly defined occurrence.
ETHICAL CONSIDERATIONS THAT PART 2 REPORTING OBLIGATIONS Brian D. Pagano, Esq Burns White LLC bdpagano@burnswhite.com Event: Different Types of Events A discrete, auditable, and clearly defined occurrence.
Incident Reporting and Investigation Guideline
 Incident Reporting and Investigation Guideline Guideline Owner: Director Human Resources Services Centre Keywords: 1) Accident 2) Investigation 3) Reporting 4) Incident 5) Guideline Intent Organisational
Incident Reporting and Investigation Guideline Guideline Owner: Director Human Resources Services Centre Keywords: 1) Accident 2) Investigation 3) Reporting 4) Incident 5) Guideline Intent Organisational
Reducing Risk: Mental health team discussion framework May Contents
 Reducing Risk: Mental health team discussion framework May 2015 Contents Introduction... 3 How to use the framework... 4 Improvement area 1: Unscheduled absence and managing time off the ward... 5 Improvement
Reducing Risk: Mental health team discussion framework May 2015 Contents Introduction... 3 How to use the framework... 4 Improvement area 1: Unscheduled absence and managing time off the ward... 5 Improvement
Fostering a Culture of Safety
 Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
Fostering a Culture of Safety June 11, 2017 Alabama Society of Health System Pharmacists Presenter: Trey Gwin, RPh, MBA, Medication Safety Coordinator, Infirmary Health Financial Disclosure The speaker
STATE OF FLORIDA DEPARTMENT OF. NO TALLAHASSEE, April 1, Safety INCIDENT REPORTING AND ANALYSIS SYSTEM (IRAS)
") CFOP 215-6 STATE OF FLORIDA DEPARTMENT OF CF OPERATING PROCEDURE CHILDREN AND FAMILIES NO. 215-6 TALLAHASSEE, April 1, 2013 Safety INCIDENT REPORTING AND ANALYSIS SYSTEM (IRAS) 1. Purpose. This operating
CFOP 215-6 STATE OF FLORIDA DEPARTMENT OF CF OPERATING PROCEDURE CHILDREN AND FAMILIES NO. 215-6 TALLAHASSEE, April 1, 2013 Safety INCIDENT REPORTING AND ANALYSIS SYSTEM (IRAS) 1. Purpose. This operating
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Consumers Union/Safe Patient Project Page 1 of 7
 Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Implementing Surgeon Use of a Patient Safety Checklist in Ophthalmic Surgery
 Report on a QI Project Eligible for Part IV MOC Implementing Surgeon Use of a Patient Safety Checklist in Ophthalmic Surgery Instructions Determine eligibility. Before starting to complete this report,
Report on a QI Project Eligible for Part IV MOC Implementing Surgeon Use of a Patient Safety Checklist in Ophthalmic Surgery Instructions Determine eligibility. Before starting to complete this report,
Patient safety reporting systems: A literature review of international practice
 Patient safety reporting systems: A literature review of international practice June 2016 Contents 1. Introduction... 3 2. Approach... 3 3. History of PSRS... 4 4. Challenges facing PSRS... 5 5. Characteristics
Patient safety reporting systems: A literature review of international practice June 2016 Contents 1. Introduction... 3 2. Approach... 3 3. History of PSRS... 4 4. Challenges facing PSRS... 5 5. Characteristics
1. Student clearances (criminal background checks) a. Discussions with Dr. Kay Lopez in Nursing i. She is getting clearances through Board of Nursing
 a. Discussions with Dr. Kay Lopez in Nursing i. She is getting clearances through Board of Nursing") 1. Student clearances (criminal background checks) a. Discussions with Dr. Kay Lopez in Nursing i. She is getting clearances through Board of Nursing (they get it through the State Police) for undergraduates
1. Student clearances (criminal background checks) a. Discussions with Dr. Kay Lopez in Nursing i. She is getting clearances through Board of Nursing (they get it through the State Police) for undergraduates
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
NOTICE OF PRIVACY PRACTICES
 535 East 70th Street New York, NY 10021 (212) 606-1000 Specialists in Mobility NOTICE OF PRIVACY PRACTICES Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE
535 East 70th Street New York, NY 10021 (212) 606-1000 Specialists in Mobility NOTICE OF PRIVACY PRACTICES Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Root Cause Analysis. Why things happen
 Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
Root Cause Analysis Why things happen Secret There is really no such thing as a root cause There are contributing factors and there is no end to them Purpose of a Root Cause Analysis The purpose is to
ORIGINAL ARTICLE. Incorrect Surgical Procedures Within and Outside of the Operating Room
 ONLINE FIRST ORIGINAL ARTICLE Incorrect Surgical Procedures Within and Outside of the Operating Room A Follow-up Report Julia Neily, RN, MS, MPH; Peter D. Mills, PhD, MS; Noel Eldridge, MS; Brian T. Carney,
ONLINE FIRST ORIGINAL ARTICLE Incorrect Surgical Procedures Within and Outside of the Operating Room A Follow-up Report Julia Neily, RN, MS, MPH; Peter D. Mills, PhD, MS; Noel Eldridge, MS; Brian T. Carney,
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations.
 ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations. 1 Thornton Kirby, President & CEO South Carolina Hospital Association Lorri Gibbons, RN, MSHL Vice President
ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations. 1 Thornton Kirby, President & CEO South Carolina Hospital Association Lorri Gibbons, RN, MSHL Vice President
Mandatory Reporting A process
 Mandatory Reporting A process guide for employers, facility operators and nurses Table of Contents Introduction.... 3 What is the purpose of mandatory reporting?... 3 What does the College do when it receives
Mandatory Reporting A process guide for employers, facility operators and nurses Table of Contents Introduction.... 3 What is the purpose of mandatory reporting?... 3 What does the College do when it receives
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Midwest Alliance for Patient Safety Patient Safety Organization Getting Started with a PSO. An Illinois Hospital Association Company
 Midwest Alliance for Patient Safety Patient Safety Organization Getting Started with a PSO An Illinois Hospital Association Company Today s Roadmap Objectives: 1. Explain the PSQIA and PSO Basics 2. Learn
Midwest Alliance for Patient Safety Patient Safety Organization Getting Started with a PSO An Illinois Hospital Association Company Today s Roadmap Objectives: 1. Explain the PSQIA and PSO Basics 2. Learn
Post Market Surveillance Requirements. SAMED Regulatory Conference 2 December 2015
 Post Market Surveillance Requirements SAMED Regulatory Conference 2 December 2015 Topics Surveillance & Vigilance Adverse Events Reportable Adverse Events Reporting Adverse Events Time frames Exemptions
Post Market Surveillance Requirements SAMED Regulatory Conference 2 December 2015 Topics Surveillance & Vigilance Adverse Events Reportable Adverse Events Reporting Adverse Events Time frames Exemptions
National Patient Safety Goals
 III. PATIENT SAFETY National Patient Safety Goals The National Patient Safety Goals for Hospital, Laboratory and Home Health Programs have been developed to improve patient safety. Ask your Volunteer Office
III. PATIENT SAFETY National Patient Safety Goals The National Patient Safety Goals for Hospital, Laboratory and Home Health Programs have been developed to improve patient safety. Ask your Volunteer Office
Joint Commission Accreditation
 HIGH RELIABILITY Joint Commission Accreditation Peggy Lavin, LCSW, Senior Associate Director Coleen Smith, Director, High Reliability Initiatives Anne Kelly, MA, BSN, Vice President, Clinical Service,
HIGH RELIABILITY Joint Commission Accreditation Peggy Lavin, LCSW, Senior Associate Director Coleen Smith, Director, High Reliability Initiatives Anne Kelly, MA, BSN, Vice President, Clinical Service,
SKAC240 Manage health, safety, security and welfare in sport and active leisure
 Manage health, safety, security and welfare in sport and active leisure Overview Health, safety, security and welfare are of vital importance in sport and active leisure. Incidents may occur that will
Manage health, safety, security and welfare in sport and active leisure Overview Health, safety, security and welfare are of vital importance in sport and active leisure. Incidents may occur that will
ADVERSE HEALTH EVENTS IN MINNESOTA
 S E C O N D ANNUAL F EBRUARY 2006 TABLE OF CONTENTS Introduction.................................................. 3 Background................................................... 4 How to use this report.........................................
S E C O N D ANNUAL F EBRUARY 2006 TABLE OF CONTENTS Introduction.................................................. 3 Background................................................... 4 How to use this report.........................................
Self-Assessment Questionnaire: Establishing a Health Information Technology Safety Program
 Self-Assessment Questionnaire: Establishing a Health Information Technology Safety Program Initial assessment by: Date: In consultation with: Date of previous assessment: The success of a health information
Self-Assessment Questionnaire: Establishing a Health Information Technology Safety Program Initial assessment by: Date: In consultation with: Date of previous assessment: The success of a health information
Catholic Charities Disabilities Services. In-Home Behavioral Support Services (2017)
") Catholic Charities Disabilities Services In-Home Behavioral Support Services (2017) A Program funded through a Family Support Services Grant from OPWDD Submit Application and supporting documentation to:
Catholic Charities Disabilities Services In-Home Behavioral Support Services (2017) A Program funded through a Family Support Services Grant from OPWDD Submit Application and supporting documentation to:
Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE
 Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE Acknowledgement and disclaimer Funding acknowledgement: This project is funded by the National Institute for Health Research Health
Intravenous Infusion Practices and Patient Safety: Insights from ECLIPSE Acknowledgement and disclaimer Funding acknowledgement: This project is funded by the National Institute for Health Research Health
RCA in Healthcare 3/23/2017. Why Root Cause Analysis is Performed. Root Cause Analysis in Healthcare Part - 1. Contd. Contd.
 Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Why Root Cause Analysis is Performed Root Cause Analysis in Healthcare Part - 1 Prof (Col) Dr R N Basu Executive Director Academy of Hospital Administration Kolkata Chapter The goal of the root cause analysis
Designing for Safety
 2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
2014 FGI Guidelines Update Series FGI Guidelines Update #1 July 11, 2013 Designing for Safety Ellen Taylor, AIA, MBA, EDAC In 2010 one of the topics introduced to the Guidelines for Design and Construction
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. WHY ARE YOU GETTING
NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. WHY ARE YOU GETTING
Chapter 17 EMS Quality Assurance Program February 2009
 Division 05 Emergency Medical February 2009 POLICY This General Order establishes policy and procedures for the continuous evaluation and improvement of emergency medical services (EMS) provided by the
Division 05 Emergency Medical February 2009 POLICY This General Order establishes policy and procedures for the continuous evaluation and improvement of emergency medical services (EMS) provided by the
Provider Initiatives in Quality Enhancement and Medical Error Reduction Timothy T. Flaherty M.D., Chair, NPSF Board of Directors
 The Quality Colloquium Provider Initiatives in Quality Enhancement and Medical Error Reduction Timothy T. Flaherty M.D., Chair, NPSF Board of Directors National Patient Safety Foundation www.npsf.org Mission
The Quality Colloquium Provider Initiatives in Quality Enhancement and Medical Error Reduction Timothy T. Flaherty M.D., Chair, NPSF Board of Directors National Patient Safety Foundation www.npsf.org Mission
HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots
 HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots Sharon Burnett, R.N., BSN, MBA Vice President of Clinical and Regulatory Affairs Missouri Hospital Association Objectives Discuss how the results of the
HCAHPS, HSOPS, HACs and HIQRP Connecting the Dots Sharon Burnett, R.N., BSN, MBA Vice President of Clinical and Regulatory Affairs Missouri Hospital Association Objectives Discuss how the results of the
EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS
 I International Symposium Engineering Management And Competitiveness 2011 (EMC2011) June 24-25, 2011, Zrenjanin, Serbia EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS Branislav Tomić * Senior
I International Symposium Engineering Management And Competitiveness 2011 (EMC2011) June 24-25, 2011, Zrenjanin, Serbia EFFECTIVE ROOT CAUSE ANALYSIS AND CORRECTIVE ACTION PROCESS Branislav Tomić * Senior
Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project
 Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project Linda Cronenwett, PhD, RN, FAAN Principal Investigator, QSEN Gwen Sherwood, PhD, RN, FAAN Co-Investigator, QSEN
Innovations for Integrating Quality and Safety in Education and Practice: The QSEN Project Linda Cronenwett, PhD, RN, FAAN Principal Investigator, QSEN Gwen Sherwood, PhD, RN, FAAN Co-Investigator, QSEN
Incident Reporting and Investigations. Mary Bolbrock, RN MSN Ann Marie McDonald, RN EdD
 Incident Reporting and Investigations Mary Bolbrock, RN MSN Ann Marie McDonald, RN EdD Objectives To serve as a training tool for identification of incidents and conduction of incident investigations To
Incident Reporting and Investigations Mary Bolbrock, RN MSN Ann Marie McDonald, RN EdD Objectives To serve as a training tool for identification of incidents and conduction of incident investigations To
NOTICE OF PRIVACY PRACTICE UNIVERSITY OF CALIFORNIA SAN FRANCISCO DENTAL CENTER
 Effective Date: February 1, 2018 NOTICE OF PRIVACY PRACTICE UNIVERSITY OF CALIFORNIA SAN FRANCISCO DENTAL CENTER THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW
Effective Date: February 1, 2018 NOTICE OF PRIVACY PRACTICE UNIVERSITY OF CALIFORNIA SAN FRANCISCO DENTAL CENTER THIS NOTICE DESCRIBES HOW HEALTH INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW
NOTICE OF PRIVACY PRACTICES UNIVERSITY OF CALIFORNIA RIVERSIDE CAMPUS HEALTH CENTER
 NOTICE OF PRIVACY PRACTICES UNIVERSITY OF CALIFORNIA RIVERSIDE CAMPUS HEALTH CENTER Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
NOTICE OF PRIVACY PRACTICES UNIVERSITY OF CALIFORNIA RIVERSIDE CAMPUS HEALTH CENTER Effective Date: April 14, 2003 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND
Child Care Program (Licensed Daycare)
") Chapter 1 Section 1.02 Ministry of Education Child Care Program (Licensed Daycare) Follow-Up on VFM Section 3.02, 2014 Annual Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended Actions
Chapter 1 Section 1.02 Ministry of Education Child Care Program (Licensed Daycare) Follow-Up on VFM Section 3.02, 2014 Annual Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended Actions
VERMONT2008 Patient Safety, Surveillance, and Improvement System
 VERMONT2008 Patient Safety, Surveillance, and Improvement System Report to the Legislature on Act 215 (2006), 18 V.S.A. 1913(e) 108 Cherry Street, PO Box 70 Burlington, VT 05402 1.802.863.7341 healthvermont.gov
VERMONT2008 Patient Safety, Surveillance, and Improvement System Report to the Legislature on Act 215 (2006), 18 V.S.A. 1913(e) 108 Cherry Street, PO Box 70 Burlington, VT 05402 1.802.863.7341 healthvermont.gov
NOTICE OF PRIVACY PRACTICES
 EFFECTIVE DATE: APRIL 14, 2003 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
EFFECTIVE DATE: APRIL 14, 2003 NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
Understanding the High Reliability Organization and Why It's Important to Your Lab
 Understanding the High Reliability Organization and Why It's Important to Your Lab Jennifer Rhamy MBA, MA, MT(ASCP)SBB, HP Executive Director, Laboratory Accreditation High Reliability Organization (HRO)
Understanding the High Reliability Organization and Why It's Important to Your Lab Jennifer Rhamy MBA, MA, MT(ASCP)SBB, HP Executive Director, Laboratory Accreditation High Reliability Organization (HRO)
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference November 3, 2017 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Safe medication practice what can we learn from root cause analysis and related methods?
 Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
Safe medication practice what can we learn from root cause analysis and related methods? Dr David Gerrett, Senior Pharmacist Patient Safety NHS Improvement Information Day on Medication Errors 20 October
NOTICE OF PRIVACY PRACTICES
 THIS NOTICE OF PRIVACY PRACTICES ( NOTICE ) DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED, AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. Respect for
THIS NOTICE OF PRIVACY PRACTICES ( NOTICE ) DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED, AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. Respect for
Self Assessment Guide for an Effective Safety and Health Program
 Self Assessment Guide for an Effective Safety and Health Program The revised Rural Electric Safety Achievement Program provides the frame work for cooperatives to develop safety and health programs that
Self Assessment Guide for an Effective Safety and Health Program The revised Rural Electric Safety Achievement Program provides the frame work for cooperatives to develop safety and health programs that
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
PGY1 Medication Safety Core Rotation
 PGY1 Medication Safety Core Rotation Preceptor: Mike Wyant, RPh Hours: 0800 to 1730 M-F Contact: (541)789-4657, michael.wyant@asante.org General Description This rotation is a four week rotation in duration.
PGY1 Medication Safety Core Rotation Preceptor: Mike Wyant, RPh Hours: 0800 to 1730 M-F Contact: (541)789-4657, michael.wyant@asante.org General Description This rotation is a four week rotation in duration.
Seven steps to patient safety A guide for NHS staff
 Seven steps to patient safety A guide for NHS staff Seven steps to patient safety Step 1 Build a safety culture Step 2 Lead and support your staff Step 3 Integrate your risk management activity Step 4
Seven steps to patient safety A guide for NHS staff Seven steps to patient safety Step 1 Build a safety culture Step 2 Lead and support your staff Step 3 Integrate your risk management activity Step 4
Unit 2 Clinical Governance & Risk Management Awareness
 Unit 2 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
Unit 2 Clinical Governance & Risk Management Awareness Incl. investigation of accidents, complaints and claims Unit 2 Clinical Governance & Risk Management Awareness Including investigation of accidents,
MHA Patient Safety Organization
 MHA Patient Safety Organization Membership Benefits 2014 Copyright ECRI Institute PSO MHA PSO does more than analyze reported events and near misses. They provide members with tools and resources to help
MHA Patient Safety Organization Membership Benefits 2014 Copyright ECRI Institute PSO MHA PSO does more than analyze reported events and near misses. They provide members with tools and resources to help
Policies, Procedures, Guidelines and Protocols
 Policies, Procedures, Guidelines and Protocols Document Details Title Complaints and Compliments Policy Trust Ref No 1353-29025 Local Ref (optional) N/A Main points the document This policy and procedure
Policies, Procedures, Guidelines and Protocols Document Details Title Complaints and Compliments Policy Trust Ref No 1353-29025 Local Ref (optional) N/A Main points the document This policy and procedure
Serious Reportable Events Madeleine Biondolillo, MD Associate Commissioner Public Health Council August 2014
 Serious Reportable Events 2011-2013 Madeleine Biondolillo, MD Associate Commissioner Public Health Council August 2014 1 Overview Background Serious Reportable Events Quality Improvement Initiative Outcomes
Serious Reportable Events 2011-2013 Madeleine Biondolillo, MD Associate Commissioner Public Health Council August 2014 1 Overview Background Serious Reportable Events Quality Improvement Initiative Outcomes
Department of Community Justice Policy and Procedures
 DIVISION: Department of Community Justice Department of Community Justice Policy and Procedures SUBJECT: Sexual Victimization Prevention and Response (Prison Rape Elimination Act - PREA) APPROVAL: Deena
DIVISION: Department of Community Justice Department of Community Justice Policy and Procedures SUBJECT: Sexual Victimization Prevention and Response (Prison Rape Elimination Act - PREA) APPROVAL: Deena
Health Information Management. Copyright 2011, 2007, 2003, 1999 by Saunders, an imprint of Elsevier Inc. All rights reserved.
 Health Information Management 1 Introduction Health information management is a relatively new field that continues to grow in popularity among students of the health professions. The advent of computer-based
Health Information Management 1 Introduction Health information management is a relatively new field that continues to grow in popularity among students of the health professions. The advent of computer-based
Incident reporting systems: Future strategies for patient safety improvement
 White paper Incident reporting systems: Future strategies for patient safety improvement There has been much global focus on improving patient safety in recent years but despite this, progress has been
White paper Incident reporting systems: Future strategies for patient safety improvement There has been much global focus on improving patient safety in recent years but despite this, progress has been
Root Cause Analysis A Necessary Evil? Dr Joseph Lui HA Convention 8 th May 2012
 Root Cause Analysis A Necessary Evil? Dr Joseph Lui HA Convention 8 th May 2012 Root Cause Analysis (RCA) The use of RCA as an organization learning tool first deployed by Veteran Affairs Hospitals in
Root Cause Analysis A Necessary Evil? Dr Joseph Lui HA Convention 8 th May 2012 Root Cause Analysis (RCA) The use of RCA as an organization learning tool first deployed by Veteran Affairs Hospitals in
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES Effective Date: May 31, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
NOTICE OF PRIVACY PRACTICES Effective Date: May 31, 2013 THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
What Every Patient Safety Officer Must Know:
 What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
The Domains of Psychiatric Nursing
 The Domains of Psychiatric Nursing 1 Nursing is and exciting, challenging, dynamic profession embedded in a stressed, underdeveloped, and rather chaotic health care system whatever nurses may say about
The Domains of Psychiatric Nursing 1 Nursing is and exciting, challenging, dynamic profession embedded in a stressed, underdeveloped, and rather chaotic health care system whatever nurses may say about
NOTICE OF PRIVACY PRACTICES
 NOTICE OF PRIVACY PRACTICES Effective Date: July 12, 2017 THIS NOTICE OF PRIVACY PRACTICES ( NOTICE ) DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED, AND HOW YOU CAN GET ACCESS TO
NOTICE OF PRIVACY PRACTICES Effective Date: July 12, 2017 THIS NOTICE OF PRIVACY PRACTICES ( NOTICE ) DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED, AND HOW YOU CAN GET ACCESS TO
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
New Mexico DDSD General Events Report (GER) Guide
 Guide") New Mexico DDSD General Events Report (GER) Guide GER APPLICABILITY: All events that occur during delivery of Supported Living, Family Living, Intensive Medical Living, Customized In-Home Supports, Customized
New Mexico DDSD General Events Report (GER) Guide GER APPLICABILITY: All events that occur during delivery of Supported Living, Family Living, Intensive Medical Living, Customized In-Home Supports, Customized
Hendricks Regional Health Patient Safety Strategic Plan
 Hendricks Regional Health Patient Safety Strategic Plan Strategic Planning Achieve Excellence in Healthcare Industry Role: Administration, Medical staff leaders and patient safety staff will participate
Hendricks Regional Health Patient Safety Strategic Plan Strategic Planning Achieve Excellence in Healthcare Industry Role: Administration, Medical staff leaders and patient safety staff will participate
INCIDENT MANAGEMENT PROGRAM
 INCIDENT MANAGEMENT PROGRAM Last updated: December 2017 1.0 PURPOSE An effective incident management program ensures that occupational incidents, including near misses, are reported and investigated in
INCIDENT MANAGEMENT PROGRAM Last updated: December 2017 1.0 PURPOSE An effective incident management program ensures that occupational incidents, including near misses, are reported and investigated in
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators