How Cookeville Regional Medical Center Set Up a Sepsis Program
|
|
|
- Shannon Rodgers
- 6 years ago
- Views:
Transcription

1 How Cookeville Regional Medical Center Set Up a Sepsis Program Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org SepsisSolutionsInternational 2012

2 Cookeville Regional Medical Center 247 Bed Community Hospital (Non- Teaching) Regional referral center in the heart of the Upper Cumberland in middle Tennessee

3 CRMC Sepsis Initiative Go live ICU/CVICU ED and Rapid Response September 2009 Go live Hospital Wide October 2010 Cost Savings per patient Mortality Decrease = Lives Saved!!!

4 Sepsis Disease Specific Certification CRMC March 2015 Shout out to Maury Regional as well who certified this year
5 CRMC Sepsis Initiative JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC 2009 Pre-Sepsis Data Obtained 23 Pts Mortality 70% September 2009 Go live for ICU, CVICU and ED Sep-Dec pts Mortality 49% 2010 Jan-Mar Pts Mortality 31% Apr-Jun Pts Mortality 33% October 2010 Hospital Go Live Jul-Sep Pts Mortality 15% Oct-Dec pts Mortality 14% 2011 Jan-Mar Pts Mortality 16% Apr-Jun Pts Mortality 17% Jul-Sep Pts Mortality 25% Oct-Dec Pts Mortality 27% 2012 Jan-Mar Pts Mortality 17% Apr-Jun Pts Mortality 17% Jul-Sep Pts Mortality 17% Oct Dec Pts Mortality 17%
6 4-Tier Process for Severe Sepsis Program Implementation Credit to Pat Posa and Kathleen Vollman who built this model and have implemented this successfully in over 50 health systems!! Measuring Success Implementation of the Sepsis Bundle Early Screening with Tools and Triggers Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively
7 4-Tier Process for Severe Sepsis Program Implementation Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively
8 Organization Support Executive management at hospital actively supports the Target Severe Sepsis Program Improving care of severe sepsis is aligned with hospital s current year goals Willingness to align resources with program Minimum.5 FTE for project management, data collection & teachable moments
9 Adult Sepsis/Severe Sepsis/Septic Shock Program Charter CRMC Problem Statement: Severe sepsis and septic shock are major healthcare problems, affecting millions of people around the world each year, killing one in four (and often more), and increasing in incidence (1 5). Similar to polytrauma, acute myocardial infarction, or stroke, the speed and appropriateness of therapy administered in the initial hours after severe sepsis develops are likely to influence outcome. ("Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 " appeared in the February 2013 issues of Critical Care Medicine and Intensive Care Medicine) Team Members: Facilitator of Team Angela Craig APN/MS/CCNS Physician Support: Dr. Sully Smith ED, Dr. Pierce Infectious Disease, Dr. Carey Hospitalist, OB/Nursery, 4E, 4N/4W, Education, Nsg Admin, Pharmacy, Respiratory, Lab, ICU, CVICU, 5E, 6E, 5N, 6N, In Pt Rehab, Surgery/PACU, Quality, ED, Hospitalist, Auditor, Infection Prevention Mission: CRMC aspires to be the leading Sepsis Treatment Center of the Upper Cumberland Area. We will expect best outcomes for our septic patients by utilizing national guidelines and evidence to treat them to the best of our ability. Performance Measures: Measure 1: Decrease time to Central Venous Pressure (CVP) goal for septic shock patients in addition to increasing compliance with CVP monitoring. Measure 2: Decrease the time to SCVO2 goal for septic shock patients in addition to increasing compliance with SCVO2 monitoring. Measure 3: Decrease time to administration of antibiotics to within one hour of time zero. Measure 4: Improve the accuracy of initial screening and recognition of severe sepsis/septic shock. Scope: Severe sepsis/septic Shock patients Housewide at CRMC Target Population: Adult Business Case: In comparison to other patients, severe sepsis patients have a higher mortality rate, increased LOS, and an increased need for a ventilator Goals/ Objectives: Become Disease Specific Certified from The Joint Commission Reduce Severe Sepsis Mortality Proper Placement of patients initially (Step-down for severe sepsis and Critical Care for Septic Shock) Milestones: ICU, CVICU, ED, Rapid Response Team Sepsis go live Sept 2009 Housewide sepsis go live October 2010 Working toward disease specific certification 2014 Goal Certification /15
10 Organization Support Understanding that this is a 2 to 3+ year program to make this the standard of practice for this patient population Existing culture that supports change Successfully implemented other major change programs e.g., vent bundle, tight glucose control, CR-BSI Established team in place with ICU physician and nurse champion, ED physician and nurse champion that are recognized leaders in the hospital
11 The Team Is KEY! Can Be Major Barrier If Not Functioning Well Must have nurse and physician champions from ED and ICU (need at least one physician at all meetings) Must be linked in the organization s quality or operational structure Must meet at least 1-2 times per month Team members must be well educated on the evidence and armed with tools and knowledge to change behavior at the bedside MUST have bedside nurses on team provide reality check and best knowledge of barriers
12 Economic Implications of an Evidence-based Sepsis Protocol Objective To determine financial impact of a sepsis protocol designed for use in the ED Design Analysis of results from recent prospective study comparing outcomes in patients with septic shock before and after initiation of sepsis protocol Setting Academic, tertiary care hospital in US Subjects: Adults (n=120) who sequentially presented to ED with septic shock, specifically: ED = Emergency Department Shorr AF et al. Crit Care Med. 2007;35:
13 Summary of Results Post-protocol, savings of ~$6,000/patient observed Translated into total cost difference of $573,000 between the two groups Post-protocol, ICU costs reduced by ~35% (p=0.026) and ward costs fell by 30% (p=0.033) Protocol resulted in a reduction in overall hospital LOS of 5 days (p=0.023) Pre-protocol, 28-day mortality rate was 48.3% vs. 30.0% following protocol initiation (p=0.040) ICU, intensive care unit; LOS, length of stay Shorr AF et al. Crit Care Med. 2007;35:
14 Tier I: Organizational Consensus Milestones and Checklist Define Sepsis Program Goals Team Charter
15 Adult Sepsis/Severe Sepsis/Septic Shock Program Charter CRMC Problem Statement: Severe sepsis and septic shock are major healthcare problems, affecting millions of people around the world each year, killing one in four (and often more), and increasing in incidence (1 5). Similar to polytrauma, acute myocardial infarction, or stroke, the speed and appropriateness of therapy administered in the initial hours after severe sepsis develops are likely to influence outcome. ("Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 " appeared in the February 2013 issues of Critical Care Medicine and Intensive Care Medicine) Team Members: Facilitator of Team Angela Craig APN/MS/CCNS Physician Support: Dr. Sully Smith ED, Dr. Pierce Infectious Disease, Dr. Carey Hospitalist, OB/Nursery, 4E, 4N/4W, Education, Nsg Admin, Pharmacy, Respiratory, Lab, ICU, CVICU, 5E, 6E, 5N, 6N, In Pt Rehab, Surgery/PACU, Quality, ED, Hospitalist, Auditor, Infection Prevention Mission: CRMC aspires to be the leading Sepsis Treatment Center of the Upper Cumberland Area. We will expect best outcomes for our septic patients by utilizing national guidelines and evidence to treat them to the best of our ability. Performance Measures: Measure 1: Decrease time to Central Venous Pressure (CVP) goal for septic shock patients in addition to increasing compliance with CVP monitoring. Measure 2: Decrease the time to SCVO2 goal for septic shock patients in addition to increasing compliance with SCVO2 monitoring. Measure 3: Decrease time to administration of antibiotics to within one hour of time zero. Measure 4: Improve the accuracy of initial screening and recognition of severe sepsis/septic shock. Scope: Severe sepsis/septic Shock patients Housewide at CRMC Target Population: Adult Business Case: In comparison to other patients, severe sepsis patients have a higher mortality rate, increased LOS, and an increased need for a ventilator Goals/ Objectives: Become Disease Specific Certified from The Joint Commission Reduce Severe Sepsis Mortality Proper Placement of patients initially (Step-down for severe sepsis and Critical Care for Septic Shock) Milestones: ICU, CVICU, ED, Rapid Response Team Sepsis go live Sept 2009 Housewide sepsis go live October 2010 Working toward disease specific certification 2014 Goal Certification /15
16 Tier I: Organizational Consensus Milestones and Checklist Define Sepsis Program Goal Team Charter Collect Baseline Data
17 Baseline Data Collection Process Pick time period for medical record query Sample size: minimum of 20 pts per ICU Query strategies: ICD 9 codes: and Patients in ICU on 1-2 antibiotics, ventilator, vasopressor (review charts to see if meet criteria for severe sepsis or septic shock before include in outcome data or process data) Select Data Collection Elements Outcome Process
18 Tier I: Organizational Consensus Milestones and Checklist Sepsis Goals aligned with organizational goals Develop sepsis team (do we have all the right people here?) and schedule monthly (minimum) meeting for at least 6 months Identify nursing and physician champions in ED and ICU and ensure champions attend team meeting Begin to define action plan and timeline for program development and implementation
19 Action Plan Tier Gap Action Steps Tier I: Organizational consensus
20 Action Plan Tier Gap Action Steps Tier I: Organizational consensus Team not meeting regularly anymore Re-formulate a team Meet with unit manager or nursing director to talk about a plan to reformulate the team
21 Second Tier: Implementation of Early Screening Tools and Triggers Early Screening with Tools and Triggers Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively
22 Severe Sepsis: Defining a Disease Continuum Infection SIRS Sepsis Severe Sepsis Adult Criteria A clinical response arising from a nonspecific insult, including 2 of the following: Temperature:> 38 C(100.4) or < 36 C (96.8) Heart Rate: > 90 beats/min Respiration: > 20/min WBC count: > 12,000/mm 3, or < 4,000/mm 3, or > 10% immature neutrophils SIRS = Systemic Inflammatory Response Syndrome Bone et al. Chest.1992;101: SIRS with a presumed or confirmed infectious process Sepsis with 1 sign of organ dysfunction, hypoperfusion or hypotension. Examples: Cardiovascular (refractory hypotension) Renal Respiratory Hepatic Hematologic CNS Unexplained metabolic acidosis Shock
23 Signs & Symptoms of Sepsis Chills Alteration in LOC Tachypnea Unexplained metabolic acidosis Heart rate Altered blood pressure Platelets Bands Skin perfusion Urine output Skin mottling Poor capillary refill Hyperglycemia Purpura/petechia Levy M, et al. Crit Care Med 2003;31:

24 Identifying Acute Organ Dysfunction as a Marker of Severe Sepsis Respiratory Increased Oxygen Requirements Cardiovascular Tachycardia SBP<90mmHg MAP < 70mmHg (despite fluid) Need for Vasopressors Renal Metabolic Unexplained metabolic acidosis Lactate > 1.5 times upper normal UO < 0.5 ml/kg per hr (despite fluid) Hematologic Platelets <80,000/mm 3 Decline in platelet count of 50% over 3 days
25 TIME IS TISSUE!! Why Do You Need to Have a Screening Process? Similar to polytrauma, AMI, or stroke, the speed and appropriateness of therapy administered in the initial hours after severe sepsis develops are likely to influence outcomes. 1 To screen effectively, it must be part of the nurses daily routines i.e., part of admission and shift assessment Must define a process for what to do with the results of the screen If you don t screen you will miss patients that may have benefited from the interventions. 1. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: Crit Care Med. 2008;36:
26 Where do you screen patients for Severe sepsis/ Septic Shock Currently? A: Housewide, all floors do sepsis screening B: Emergency Dept. Only C: Critical Care Areas and Emergency Dept. only D. We have no formal screening process at our hospital
27 Make Screening for Severe Sepsis Process-Dependent Weave into fabric of current practice Assess for on a daily basis Identify strategies for initiation of therapy response once patient is identified
28 Incorporate Screening and Early Identification Throughout the Hospital Emergency Department ICUs Patient Care Units Rapid Response Team
29
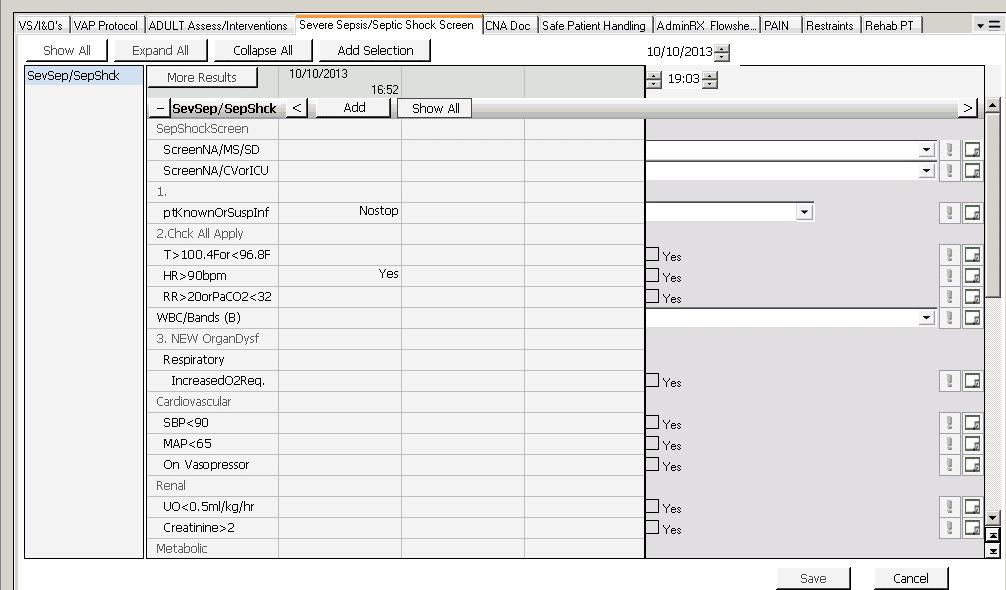
30 ED Screening Tool

31 Rapid Response Team Tool

32
33 What About Automation for Early Recognition? MICU, single center, 442 consecutive patients who met modified SIRS Randomized to automated identification of SIRS with notification to MD or usual care Measure impact on early antibiotics and outcomes in patients with sepsis Results No difference in median time to antibiotic No difference in amount of fluid administered No diff in LOS or mortality Hooper MH, et al. Crit Care Med. 2012;40
34 Screening: Barriers/Strategies Barriers Time for nurses to do it (perception vs. reality) Screening is not sensitive only for severe sepsis Positive screen is not a diagnosis of severe sepsis Strategies Must assign responsibility and enforce accountability Perform audits to measure compliance and identify problems Round on unit and ask nurses how it is going and discuss issues
35 Screening: Barriers/Strategies Lesson learned: Bedside nurse must do daily screening. Education/Simulation/Education Every 6 months Build into orientation Must be part of your documentation structure Practice-Practice-Practice
36 Is Sepsis Training part of your Unit based or hospital based orientation? A: Yes, Unit Based Orientation B: Yes, Hospital Based Orientation C: Yes, Both Hospital and Unit Based Orientation D: No This is an opportunity for my hospital
37 Nursing Care Essentials to Complement SSC Infection Prevention Education: Multimodal/interactive Accountability: Culture of patient safety Surveillance: Continuous Hand Hygiene: Alcohol based gel 1 st, if soiled soap & H 2 0 Prevention of VAP Prevention of CR-BSI Prevention of SSI Prevention of UTI Source control (catheter removal, isolation etc.) Educated to recognize signs of severe sepsis & septic shock Use of early warning system Use of screening tools for early recognition Aitken LM, et al. Crit Care Med;2011;39;39:
38 Nursing Care Essentials to Complement SSC Communications tools be used to improve communication (i.e. SBAR, RSVP (reason, story, vital signs & plan) Initial resuscitation of patients be provided through the use of a rapid response system Education Adequate resources Adequate nurse staffing levels Sepsis six should be promoted in non-critical care areas (care within 1 st hour) (protocol directed care) Starting high oxygen flow Obtaining blood cultures Administering antibiotic therapy Starting IV therapy Obtaining lab work (hgb & lactate levels) Measuring I & O Pre-mixed antibiotics for 1 st dose Tracking systems & daily sepsis rounds Aitken LM, et al. Crit Care Med;2011;39;39:
39 Clinical Scenario I: Early identification and intervention 88 year old, 51.6kg,white, female admit from ED; resided in ECF History: CAD, COPD, dementia, Alzheimer disease, depression, SVT Chief Complaint: rib pain, chest congestion and SOB Awake, alert and oriented, slight combative (history of combative behavior)

40
41 Clinical Scenario I: Early Identification and Intervention Initial VS: Temp: F RR: 31 HR: 109, atrial fib with occasional SVT B/P: 79/51 2L of O2, O2 sat of 96% Does this patient screen positive for severe sepsis?
42 Clinical Scenario II: Early Identification and Intervention 62 yr. old male, 2 days post op s/p colectomy, 73kg, receiving antibiotics Vital signs: HR 120. RR 24, BP 80/40, temp: 102.2; urine output 100ml over last 4 hrs. Does patient screen positive for severe sepsis?
43 Clinical Scenario II: Early identification and intervention 62 yr. old male, 2 days post op s/p colectomy, 73kg,receiving antibiotics Vital signs: HR 120. RR 24, BP 80/40, temp: 102.2; urine output 100ml over last 4 hrs. Screen patient for severe sepsis Positive Screen for Severe Sepsis SIRS: HR>90; RR>20; Temp> Infection: on antibiotics Organ dysfunction: BP 80/40
44 Tier II: Screening for Severe Sepsis Milestones and Checklist Develop screening process for ED, rapid response team and ICU (eventually housewide) Develop audit process to evaluate compliance and effectiveness Ensure screening process has clear next steps defined for nursing staff
45 Screening Compliance Audit Tool Pt. Account # (enter #) Screened Y/N (circle) Y N Patient transferred to appropriate level of care Y/N (circle) (Severe Sepsis Stepdown Septic Shock (ICU/CVICU) Y N Pt. Have known suspected infection Y N Antibiotics hung within 1 hour of time zero? Y N T or < 96.8 HR > 90 RR >20 or PACO 2 <32 WBC >12,000 <4,000 or > 10% Bands SIRS Present Screen done correctly Y/N (circle) Organ Dysfunction Respiratory (increased oxygen requirements) Cardiovascular (SBP less than 90 or MAP less than 65 or on a vasopressor) Renal (Urine output less than 05.ml/kg/hr., creatinine greater than 2) Metabolic (Lactate greater than or equal to 4mmoL/dl) Hematologic (Serum total bilirubin greater than or equal to 4mg/dl) Hepatic (Serum total bilirubin greater than or equal to 4mg/dl) CNS (Altered consciousness unrelated to primary neuro pathology) If screen not done correctly, why? Which labs were sent? ( =obtained) Bld Cult x2 Bld Cult CVAD >48 hr Lactic Acid Was Central Line Inserted? (Critical Care Only) Y N Fluid bolus (30ml/kg) provided for hypotension Y/N (circle) Y N If no how much given 500 ml 1 liter Screened positive for severe sepsis (Y/N) (circle) Y N Comments Pos feedback letter given Neg feedback letter given Other (Explain) Screened positive for Septic Shock Y/N (circle) Y N Positive Screenings If screened positive for Septic Shock in CVICU/ICU was Septic Shock Clinical Pathway (Form PRN) started Y N If screened positive for Severe Septic or Septic Shock (floors other than ICU/ED/ CVICU) was Initial Management of Patient with Severe Sepsis (Form 1135-PRN) completed Y N Unit: Date: Shift: # Audits Completed (Every shift checked considered an audit): # Audit Screened (numerator = number of screenings completed, denominator = audits completed Example: 7 screenings done, 10 audits completed = 70% audits screened) % # of Audits screened correctly? (numerator = number audits screened correctly, denominator = number audits completed ) % % of follow up on incorrect screens (numerator = number of audits followed up on, denominator = number of incorrect audits) %
46 Action Plan Tier Gap Action Steps Tier I: Organizational consensus Tier II: Screening and Early Identification Team not meeting regularly anymore Re-formulate a team Meet with unit manager or nursing director to talk about a plan to re-formulate the team
47 Action Plan Tier Gap Action Steps Tier I: Organizational consensus Tier II: Screening and Early Identification Team not meeting regularly anymore No formal process for screening or follow through Re-formulate a team Meet with unit manager or nursing director to talk about a plan to re-formulate the team Start to develop screens and implement for the ICU and ED
48 Homeostasis Is Unbalanced in Severe Sepsis COAGULATION INFLAMMATION FIBRINOLYSIS Homeostasis Carvalho AC, Freeman NJ. J Crit Illness 1994;9: Kidokoro A, et al. Shock 1996;5: Vervloet MG, et al. Semin Thromb Hemost 1998;24:33-44.



49 Inflammation, Coagulation and Impaired Fibrinolysis In Severe Sepsis Endothelium COAGULATION CASCADE Tissue Factor Monocyte IL-6 IL-1 TNF-α Factor VIIIa Factor Va THROMBIN PAI-1 Suppressed fibrinolysis Neutrophil Fibrin Tissue Factor IL-6 Fibrin clot Inflammatory Response to Infection Thrombotic Response to Infection Fibrinolytic Response to Infection Adapted from Bernard GR, et al. N Engl J Med. 2001;344:
50 MICROCIRCULATION: SUBLINGUAL BLOOD FLOW Healthy Volunteer BP: 120/80 mm Hg SaO 2 : 98% 1. Accessed April Spronk PE, et al. Lancet. 2002;360: Septic Shock Patient Resuscitated with fluids and dopamine HR: 82 BPM BP: 90/35 mmhg SaO 2 : 98% CVP: 25 mmhg
51 Pathophysiologic Characteristics in Severe Sepsis Maldistribution of blood flow Imbalance of oxygen supply & demand Metabolic alterations & activation of the stress response
52 Imbalance of Oxygen Supply & Demand SUPPLY DEMAND Vollman 2001
53

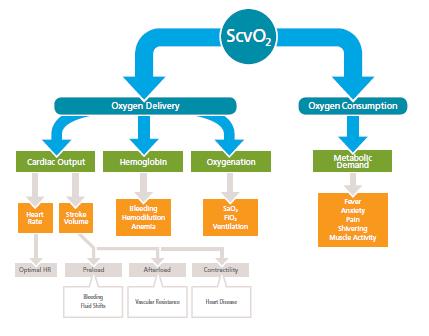
54 OXYGEN SUPPLY/DEMAND DYNAMICS ScvO2 CVP, CO, CI, SV, SVI, SVV

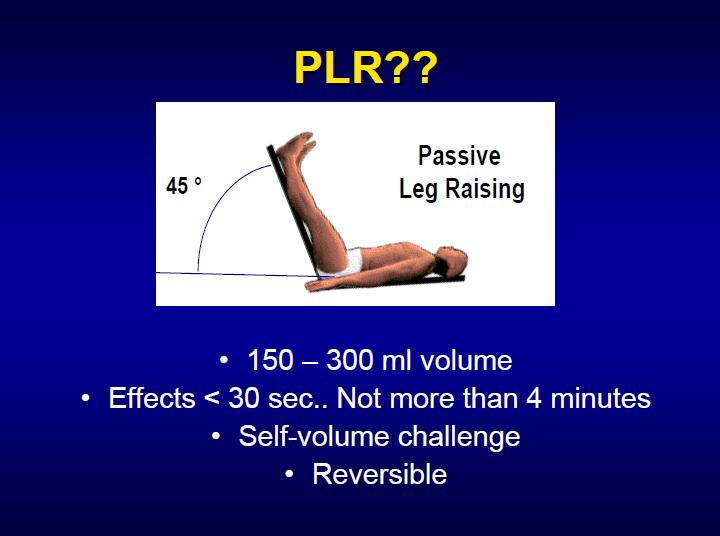
55 Optimize Cardiac Performance Fluid Bolus to define place on curve: Record Stroke Volume (SV) Give NS bolus over 10-15minutes Record SV If see greater than a 10% increase in SV pt. is on steep portion of curve and will still respond to fluid
56
57 O 2 Supply/Demand Compensatory Mechanisms Improve pulmonary gas exchange Increase oxygen delivery Alter the distribution of blood flow
58 Monitoring Oxygen Dynamics Lactates within 3 hours, then if elevated obtain another one prior to 6 hour mark, every 6 hrs. until cleared Correlates with mortality; Expect clearance within 24 hours ScvO2 Subclavian or IJ triple lumen intermittent sampling or continuous monitoring Baseline and then hourly till > 70%;
59 Cornerstones of Multidisciplinary Management of Severe Sepsis/MODS Prevention Screening and Early Identification Early Intervention: Source control, Blood cultures and broad spectrum antibiotics May want to protocolize lactic acid/blood culture collection 3 Hour Bundle 6 Hour Bundle
60 Third Tier: Implementation of Evidence-Based Sepsis Bundles Implementation of the Sepsis Bundle(s) Early Screening with Tools and Triggers Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively
61 Tier III: Implementation of Sepsis Bundles Milestones and Checklist Define who will put in the CVP line for patients when the come from the floor, especially on off shifts and weekends Develop easy to use order sets (ED and ICU should be the same), organized by bundle Order sets approved by appropriate medical and nursing leadership/committees Assess physician/provider skill level with CVP insertion. Create strategy to deal with gap in skill if present We have had classes for physicians for hemodynamics and central line placement
62 Tier III: Implementation of Sepsis Bundles Milestones and Checklist Ability to get lactate results in 30 minutes or less Ability to get antibiotics administered within one hour of diagnosis or first hypotensive episode Identify equipment needs and make capital requests Identify education needs
63 If lactate : target resuscitation to normalize the lactate (2C) Dellinger, etal, Critical Care Medicine, Feb 2013, Vol 41 Number 2
64 SSC Guidelines A: Initial Resuscitation Should be protocolized, quantitative resuscitation of patients with sepsis induced hypoperfusion (defined as hypotension persisting after initial fluid challenge or blood lactate > 4mmol/L) Goals during the first 6 hours of resuscitation: Central venous pressure: 8-12 mmhg Higher with altered ventricular compliance or increased intrathoracic pressure Mean arterial Pressure (MAP) 65mmHg Urine Output 0.5mL/kg/hr Central Venous (superior vena cava) or mixed venous oxygen saturation 70% or 65% respectively (1C)
65
66
67

68 CRMC Septic Shock Clinical Pathway
69
70
71 SBAR Report Form
72 Antibiotic Challenges Appropriate selection determined based upon consensus guidelines and pathogen sensitivity at your institution Timing issues How? Delivery time challenges of antibiotics Possible solutions
73 Clinical Scenario II: Early identification and Intervention 88 year old, 51.6kg,white, female admit from ED; resided in ECF History: CAD, COPD, dementia, Alzheimer disease, depression, SVT Chief Complaint: rib pain, chest congestion and SOB Awake, alert and oriented, slight combative (history of combative behavior) The Rest of the Story
74 Clinical Scenario II : Early Identification and Intervention-ER Labs: WBC: 11.5 Hgb: 15.8 Hct: 47.4 BUN: 28 Creatinine:1.6 Glucose:158 BNP:78 (moderate CHF); troponin:0.03 Lactic acid: 4.6 U/A: positive for bacteria ScvO2: 49.1% Blood cultures X 2 drawn
75 Clinical Scenario II : Early Identification and Intervention-ER CXR: RLL consolidation Additional Interventions: Broad spectrum antibiotics given within 3 hours of presentation Lactic acid >4mmol/L so CVP inserted Fluid resuscitation continued Foley inserted Received total of 3 Liters of NS during 3 hour ED stay ED diagnosis: Severe Shock, Pneumonia, UTI, CHF Transferred to MICU
76 Clinical Scenario II : Early Identification and Intervention--MICU Additional Interventions: Day 1 Continued fluid resuscitation 7 L Low dose vasopressor Low dose steroids Remained on 2 L nasal cannula Labs: ScvO2: 72.8 (after resuscitation) Lactic acid: 4 hours after ICU admission: hours after ICU admission: 3.0
77 Clinical Scenario II : Early Identification and Intervention Day 2: Vasopressor weaned off Lasix to assist with fluid mobilization Lactic acid: 3.0 Day 3: Lactic acid: 1.2 O2 sat 93% on room air Central line discontinued Transferred to intermediate care on Day 3 Discharged from hospital on day 7
78 Tier III: Sepsis Bundle Implementation Milestones and Checklist Identify resistance and barriers to bundle implementation and develop solutions Define educational plan for all staff: Develop implementation plan
79 Action Plan Tier Gap Action Steps Tier I: Organizational consensus Tier II: Screening and Early Identification Tier III: Implementing the Bundles Team not meeting regularly anymore No formal process for screening or follow through Re-formulate a team Meet with unit manager or nursing director to talk about a plan to re-formulate the team Start to develop screens and implement for the ICU and ER
80 Action Plan Tier Gap Action Steps Tier I: Organizational consensus Tier II: Screening and Early Identification Tier III: Implementing the Bundles Team not meeting regularly anymore No formal process for screening or follow through Getting lactate & antibiotics in < 1hr Getting the Central line inserted Re-formulate a team Meet with unit manager or nursing director to talk about a plan to re-formulate the team Start to develop screens and implement for the ICU and ER Lactate: explore point of care & measurement from the ABG machine Antibiotic: Broad spectrum in the Pyxis Central Line: Around the clock Power PICC team
81 Is it difficult to get a central line placed in your institution A: Yes B: No
82 Implementation Hospital resources often focus on planning phase and then back off after implementation. The implementation phase is the most critical. Frequent rounds by project champion recommended on unit to support staff and answer questions. Defined resources for bedside nurse: Project champion has pager to be available 24/7 initially Clinical nurse champions identified on each ICU unit, ED, and all Nsg Care Units to be resources to bedside staff (these staff should be members of the sepsis team/committee from the beginning)
83 Tier III: Develop and Implement the Education Plan Content: (present to physicians, nurses, Pharmacy, and RTs) Significance of problem Sepsis continuum Pathophysiology of severe sepsis Prevention and management (share the evidence) Case studies for staff to practice with bedside tools Methods: Self learning modules Classroom and/or small groups of staff on unit Web-based Ongoing: build into orientation monthly for residents every 6 months for all staff one-on one during rounds
84 TIER III: Develop Implementation Plan Identify who will oversee the implementation and the expectations of that person (sepsis nurse or program coordinator) Define Critical Care/ED/Floor resources for staff that they can call at any time for questions and assistance Example OB Floor
85 TIER III: Develop Implementation Plan Create rounding schedule and process Should begin as daily in the ICU and ED Keep master list of all patients who go on the bundles (and those who should have but didn t if possible) Do real time interventions to ensure patients get the evidence based practices Define follow up process for review and evaluate missed opportunities
86 Fourth Tier: Measuring Process & Outcome Changes Use of evidence-based approach Measuring Success Implementation of the Sepsis Bundle Early Screening with Tools and Triggers Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively
87 Tier IV: Measurement Milestones and Checklist Define outcome and process data elements that will be collected Develop and implement a data collection process Revise and update goals and action plan as needed Execute implementation plan
88 Data Collection Patient Log Define how will find all patients that receive the bundles Real time data collection is optimal then used as checklist to ensure patient receives all appropriate interventions Outcome Mortality (ICU and Hosp) Hosp LOS Cost per case (total and direct) Process SSC database Data elements that measure implementation of resuscitation and management bundle
89 CRMC Data Sample CRMC Septic Shock Data Post Sepsis Protocol Group VIII Oct-Dec 2012 (49 pts) Where Septic Shock Identified ED 14% ICU 82% CVICU 4E 2% 5E 2% 6N 5N 4N 6E Outside Facility Post Sepsis Protocol Group IX Jan-Mar 2013 (65 pts) 43% 55% 2% Serum Lactate Drawn within 6 hr from time zero Blood cultures drawn times 2? Were Bld Cultures drawn w/in 1 hr of time zero? Was 20mL per kg infused? If No was bolus of any amount given? If Yes How much given? Yes 98% No 2% Yes 100% No Yes 71% No 29% Yes 65% No 35% Yes 71% No 29% 100% 94% 6% 72% 28% 65% 35% 57% 43% 500mL 44% 1 liter 56% 2 liter 1.5 liter 38% 62%
90 CRMC Data Sample Was patient hypotensive after fluid bolus? Yes 80% No 20% Not Documented 84% 16% Pt received antibiotic within first hour (added field) Yes 60% No 40% 57% 43% Initial lactate > or equal to 4 Yes 31% No 69% 54% 46% CVP Placed? Yes 49% No 51% Not Documented 61% 39% Was patient on vasopressors > 6 hours? Yes 68% No 32% 71% 29% Patient Expired? *** Yes 33% No 67% 18% 82%
91 Indicator/ Month Jan 26 Feb 25 March 20 1 st Q 71 Apr 11 May 18 Lactate drawn within 3 hrs. of time zero 100% (26/26) 92% (23/25) 95% (19/20) 96% (68/71) 82% (9/11) 100% (18/18) Blood C/S drawn prior to antibiotics 88% (23/26) 92% (23/25) 95% (19/20) 92% (65/71) 100% 89% (16/18) Broad Spectrum antibiotic within 3 hrs. of time zero 92% (24/26) 84% (21/25) 75% (15/20) 85% (60/71) 82% (9/11) 67% (12/18) Administer 30ml/kg crystalloid 65% (17/26) 60% (15/25) 80% (16/20) 68% (48/71) 73% (8/11) 72% (13/18) Administer 30ml/kg crystalloid within 3hrs of time zero 82% (14/17) 100% (15/15) 81% (13/16) 88% (42/48) 100% 8/8 100% (13/13)
92 Central line placed 88% (23/26) 64% (16/25) 75% (15/20) 76% (54/71) 73% (8/11) 78% (14/18) Central line placed within 6 hrs. of time zero 57% (13/23) 94% (15/16) 40% (6/15) 63% (34/54)) 63% (5/8) 43% (6/14) MAP goal met within 6 hrs. of time zero 85% (22/26) 88% (22/25) 60% (12/20) 79% (56/71) 91% (10/11) 56% (10/18) CVP goal met within 6 hrs. of time zero 15% (4/26) 8% (2/25) 10% (2/20) 11% (8/71) 9% (1/11) 0% (0/18) Scv02 goal met within 6 hrs. of time zero 4% (1/26) 0% (0/25) 5% (1/20) 3% (2/71) 0% (0/11) 0% (0/18) Survival Rate 77% (20/26) 64% (16/25) 60% (12/20) 68% (48/71) 82% (9/11) 94% (17/18) Readmission Rate 3.8% (1/26) 4% (1/25) 10% (2/20) 5.6% (4/71) 9% (1/11) N/A (No readmits)
93 Goals 4-Tier Process for Severe Sepsis Program Implementation Tier 1 Complete by May 1 st, 2009 Tier 2 Complete by May 26 th, 2010 Measuring Success Implementation of the Sepsis Bundle Tier 4 Complete by October 2010 Plan in place Tier 3 Complete by August 2010 Educate for 3 weeks Early Screening with Tools and Triggers Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively
94 Three Biggest Challenges
95 Challenge #1: Finding the Patients Redefining what a septic shock patient looks like Before Supine in bed Ventilator Fluids wide open Increasing vasopressors Minimally responsive NOW Sitting up in bed Nasal cannula IV boluses Weaning vasopressors Awake Don t look sick enough to be in ICU or to have a central line Must correct this misperception
96 Additional Strategies: Finding the Patient Unit sepsis champions Sepsis coordinator ED and ICU rounding RRT screen on every call Prospective patient log Discuss sepsis screen as part of Multidisciplinary Rounds Reports Patients who screened positive Lactate
97 Finding the Patients: Prospective Patient Log Unit Pt # Point of Entry Date of Septic Shock Dx Time of Septic Shock Dx Data Obtained Data Complete Comments / Follow-up
98 Sepsis Management: Challenges #2 Physician Buy-in Strategies: Redefining what a septic shock patient looks like Physician Champions-ED and ICU Part of sepsis team Follow up with physician when bundles not followed ED and ICU rounding Unit sepsis champions Sepsis coordinator Data--- Often and detailed Physician specific Administrative support
99 Challenges #3: Not Meeting 3hr and 6hr goals Focused Incremental Goals First hour of care Lactate, blood cultures, antibiotics and 30ml/kg fluid bolus Other goals within 6 hours CVP greater than or equal to 8mmHg MAP greater than or equal to 65mmHg ScvO2 greater than or equal to 70 % Work on 3 hour Bundle First then the 6 hour Bundle
100 Communication Policy Environment **Poor between RN & MD re:diagnosis. (2) **RN not comfortable discussing w/ MD Poor between ER-ICU & OR-ICU (2) Lack of guidance on MN & Weekends (5) No IV line holders at head of bed Nurse does not know where to look for information re:bundles Delay in antibiotic verification in pharmacy. (4) Unclear process (4) No ICU beds to transfer patient to. (4) **Nurse/Patient ratio 1:2 with high acuity (10) Staff overwhelmed with other initiatives. **Signs go unrecognized (8) **Unsure how to follow bundle (8) -RN forgot to screen (2) -Unsure how to measure CVP from PICC (4) **-No sense of urgency (6) goals not achieved in 3hours or 6 hours Materials Order sets not being used. (3) Process **-MD buy in (3) -RN: lack of knowledge -Reoccurrence goes unrecognized -Lack of critical thinking/cant put it all together (3) -RN/MD refuses to follow bundles People
101 Sustaining and Improving: Strategies Independent checks Checklists, pathway Multidisciplinary rounds Real time feedback and on-going education Unit rounds Unit champions Staff meetings Orientation---RN and residents Quarterly with current staff
102 Sustaining and Improving: Strategies Creating sense of urgency Code Sepsis or Sepsis Alert Staffing ratio for initial 6 hours of ICU or ED care Clock on the door Protocol Watch
103 Keys to Success Team in place with key stakeholders overseeing implementation Project coordinator with lead clinical staff on each unit Sepsis resource/coordinator rounds frequently on units Strong physician leadership on team Reminders to staff through use of bedside sepsis tools/checklist
104 Keys to Success Empowerment of nursing staff to prevent errors Administrative support to help manage barriers Review data monthly to identify opportunities for improvement Support from state-wide collaborative/surviving sepsis campaign EDUCATION, DATA, PROCESS, EDUCATION, COMPLIANCE
105 The Nurses Role Early recognition of patients with signs of sepsis Early initiation of evidence based practice therapies appropriate for your area of practice (antibiotics, fluids/blood & pressors) Swift disposition to care areas where the rest of the bundle can be started.
106
107 References: Dellinger et al, Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: Critical Care Medicine. 2013; 41: Vollman, Kathleen and Pat Posa Critical Care Solutions developed the pyramid
The Power of the Pyramid:
 The Power of the Pyramid: A Proven Sepsis Implementation Program for Saving Lives SepsisSolutionsInternational 2011 Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist, Educator, Consultant
The Power of the Pyramid: A Proven Sepsis Implementation Program for Saving Lives SepsisSolutionsInternational 2011 Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist, Educator, Consultant
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers
 Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care. Dial in # 855/ Reference conference ID#
 MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care Dial in # 855/427-9512 Reference conference ID# 61200088 Implementing a Hospital Wide Sepsis Program: Strategies and Challenges
MHA/KHC Mission Possible: Early Identification and Standardization of Sepsis Care Dial in # 855/427-9512 Reference conference ID# 61200088 Implementing a Hospital Wide Sepsis Program: Strategies and Challenges
Stopping Sepsis in Virginia Hospitals and Nursing Homes. Hospital Webinar #6 - Tuesday, December 19, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU)
") Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
STARTER PACK: Webinar #1 SEPSIS
 STARTER PACK: Webinar #1 SEPSIS Welcome to the Sepsis Starter Pack Webinar #1 Why this is important Establishing a Team Best practices Understanding the Measures Completing a gap analysis First Steps Gap
STARTER PACK: Webinar #1 SEPSIS Welcome to the Sepsis Starter Pack Webinar #1 Why this is important Establishing a Team Best practices Understanding the Measures Completing a gap analysis First Steps Gap
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Early Management Bundle, Severe Sepsis/Septic Shock
 Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Sepsis/Septic Shock Pre-Hospital Care
 Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Current Status: Active PolicyStat ID: Guideline: Sepsis Identification And Management in Adults GUIDELINE: COPY
 Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE. Early Recognition and Treatment of Severe Sepsis and Septic Shock
 SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
Northwell Sepsis Collaborative Evidence Based Best Practice
 Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management
 SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
Stop Sepsis: Evidence Based Strategies to Decrease Mortality Across the Continuum
 Stop Sepsis: Evidence Based Strategies to Decrease Mortality Across the Continuum Angela Craig APN, MS, CCNS Clinical Nurse Specialist Critical Care Cookeville Regional Medical Center Cookeville, TN acragi@crmchealth.org
Stop Sepsis: Evidence Based Strategies to Decrease Mortality Across the Continuum Angela Craig APN, MS, CCNS Clinical Nurse Specialist Critical Care Cookeville Regional Medical Center Cookeville, TN acragi@crmchealth.org
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
2014 Maryland Patient Safety Center s Call for Solutions
 Improving Sepsis Outcomes Through Coordinated Early Recognition, Assessment, and Treatment UM-CRMC Sepsis Survival Rate 100% 95% 90% 89.5% CRMC 85% 85.3% 86.1% 86.2% 81.8% 82.3% 85.7% 84.7% 86.1% MD Statewide
Improving Sepsis Outcomes Through Coordinated Early Recognition, Assessment, and Treatment UM-CRMC Sepsis Survival Rate 100% 95% 90% 89.5% CRMC 85% 85.3% 86.1% 86.2% 81.8% 82.3% 85.7% 84.7% 86.1% MD Statewide
APPLICATION FORM. Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes. Director of Quality
 APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
Document Ratification Group Chairman s Action
 Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
Supplementary Appendix
 Supplementary Appendix Table S1: Average Adherence Rate to Combined and Individual Bundle Targets over the total Program Duration of 3.5 years in Severe Sepsis Patients (N=8387) % Not Applied % Not Applicable
Supplementary Appendix Table S1: Average Adherence Rate to Combined and Individual Bundle Targets over the total Program Duration of 3.5 years in Severe Sepsis Patients (N=8387) % Not Applied % Not Applicable
Goals today 6/14/2011. Disclosures, 2004-May Sepsis A Medical Emergency. Jim O Brien, MD, MSc So what is sepsis anyway?
 Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Jim O Brien, MD, MSc James.OBrien@osumc.edu Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Rapid Response Team Building
 Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Presenters. Tiffany Osborn, MD, MPH. Laura Evans, MD MSc. Arjun Venkatesh, MD, MBA, MHS
 Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 6
 Thursday, November 21, 2013 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 6 Sean Townsend MD Terry Clemmer MD Diane Jacobsen MPH,
Thursday, November 21, 2013 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 6 Sean Townsend MD Terry Clemmer MD Diane Jacobsen MPH,
Emergency. Best Critical Care Practices
 Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Jim O Brien, MD, MSc James.OBrien@osumc.edu Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Sepsis A Medical Emergency State of the Science Symposium Best Critical Care Practices 2011 Jim O Brien, MD, MSc James.OBrien@osumc.edu Disclosures, 2004-May 2011 University grant monies: Davis/Bremer
Understand. Learning Objectives Module 1. Surviving Sepsis Campaign Sepsis e learn Module 1. Situation & Background. Sepsis e Learn: Module 1
 Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2 Measure Updates Presentation Transcript Moderator: Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2 Measure Updates Presentation Transcript Moderator: Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives,
Supplementary Online Content
 Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
The Davies Award Is: The HIMSS Nicholas E. Davies Award of Excellence. Awarding IT. Improving Healthcare.
 The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring
 Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Early Recognition of In-Hospital Patient Deterioration Outside of The Intensive Care Unit: The Case For Continuous Monitoring Israeli Society of Internal Medicine Meeting July 5, 2013 Eyal Zimlichman MD,
Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation
 Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation Christine Aceves, MSN, RN, CEN, CNL Sepsis Program Manager, Stanford Health Care Santa Clara County Sepsis Collaborative
Surviving Sepsis: Change in Condition SBAR Situation, Background, Assessment, Recommendation Christine Aceves, MSN, RN, CEN, CNL Sepsis Program Manager, Stanford Health Care Santa Clara County Sepsis Collaborative
For audio, join by telephone at , participant code #
 For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
Greater New York Hospital Association United Hospital Fund. STOP Sepsis Collaborative Toolkit. of Severe Sepsis in the Emergency Department
 Greater New York Hospital Association United Hospital Fund STOP Sepsis Collaborative Toolkit A Protocol-Based Approach to Early Identification and Treatment of Severe Sepsis in the Emergency Department
Greater New York Hospital Association United Hospital Fund STOP Sepsis Collaborative Toolkit A Protocol-Based Approach to Early Identification and Treatment of Severe Sepsis in the Emergency Department
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
ICU - Sepsis, CAUTI and CLABSI Less May Be Better. HRET HIIN ICU Virtual Event April 11, 2017
 ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis
 Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
University of South Dakota Vermillion, South Dakota Department of Nursing
 Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Initiating a Rapid Response Team
 Initiating a Rapid Response Team Trials and Tribulations! Washington County Hospital Facility Location Size Hagerstown, MD 320 bed Programs/Services History Emergency Services, Critical Care, Med/Surg,
Initiating a Rapid Response Team Trials and Tribulations! Washington County Hospital Facility Location Size Hagerstown, MD 320 bed Programs/Services History Emergency Services, Critical Care, Med/Surg,
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING
 SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
Kansas Heart and Stroke Collaborative
 Sepsis in the Long Term Care Facility Aligning with Requirements of Participation Dr. Bob Moser, MD F.A.A.F.P Executive Director, Kansas Heart & Stroke Collaborative University of Kansas Health System
Sepsis in the Long Term Care Facility Aligning with Requirements of Participation Dr. Bob Moser, MD F.A.A.F.P Executive Director, Kansas Heart & Stroke Collaborative University of Kansas Health System
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond. Why the focus on Sepsis?
 The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA. July 26 th, :00 a.m. 12:00 p.m. CDT
 AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA July 26 th, 2016 11:00 a.m. 12:00 p.m. CDT 1 WELCOME AND INTRODUCTIONS Mallory Bender, MA, LCSW, Program Manager, HRET
AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA July 26 th, 2016 11:00 a.m. 12:00 p.m. CDT 1 WELCOME AND INTRODUCTIONS Mallory Bender, MA, LCSW, Program Manager, HRET
Inpatient Quality Reporting Program
 The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Presentation Transcript Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead, Hospital
The Clinician Perspective on Sepsis Care: Early Management Bundle for Severe Sepsis/Septic Shock Presentation Transcript Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead, Hospital
Actionable Patient Safety Solution (APSS) #9: EARLY DETECTION & TREATMENT OF SEPSIS
 #9: EARLY DETECTION & TREATMENT OF SEPSIS") Actionable Patient Safety Solution (APSS) #9: EARLY DETECTION & TREATMENT OF SEPSIS Executive Summary Checklist Commitment from hospital governance and senior administrative leadership to support early
Actionable Patient Safety Solution (APSS) #9: EARLY DETECTION & TREATMENT OF SEPSIS Executive Summary Checklist Commitment from hospital governance and senior administrative leadership to support early
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014
 Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
Preventing Sepsis Mortality
 Murray State's Digital Commons Scholars Week 2017 - Spring Scholars Week Preventing Sepsis Mortality Karli Tabers Follow this and additional works at: http://digitalcommons.murraystate.edu/scholarsweek
Murray State's Digital Commons Scholars Week 2017 - Spring Scholars Week Preventing Sepsis Mortality Karli Tabers Follow this and additional works at: http://digitalcommons.murraystate.edu/scholarsweek
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia
 Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
Failure to Maintain: Missed Care and Hospital-Acquired Pneumonia STTI INDIANAPOLIS, OCTOBER 2017 DIAN BAKER, PHD, RN PROFESSOR, SCHOOL OF NURSING DIBAKER@CSUS.EDU CALIFORNIA STATE UNIVERSITY, SACRAMENTO
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Welcome and Overview. Sepsis Mortality Reduction Boot Camp 3/20/2014
 Welcome and Overview Sepsis Mortality Reduction Boot Camp 3/20/2014 AHA Disclaimer Participation in this virtual event is by express written invitation of the AHA only. Unauthorized participants and/or
Welcome and Overview Sepsis Mortality Reduction Boot Camp 3/20/2014 AHA Disclaimer Participation in this virtual event is by express written invitation of the AHA only. Unauthorized participants and/or
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Number of sepsis admissions to critical care and associated mortality, 1 April March 2013
 Number of sepsis admissions to critical care and associated mortality, 1 April 2010 31 March 2013 Question How many sepsis admissions to an adult, general critical care unit in England, Wales and Northern
Number of sepsis admissions to critical care and associated mortality, 1 April 2010 31 March 2013 Question How many sepsis admissions to an adult, general critical care unit in England, Wales and Northern
5/9/2015. Disclosures. Improving ICU outcomes and cost-effectiveness. Targets for improvement. A brief overview: ICU care in the United States
 Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
Disclosures Improving ICU outcomes and cost-effectiveness CHQI grant, UC Health Travel support, Moore Foundation J. Matthew Aldrich, MD Associate Clinical Professor Interim Director, Critical Care Medicine
HealthONE Sepsis Program
 HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
Hospital Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: V5.4 Measure Updates Questions and Answers Speakers Noel Albritton, RN, BS, Lead Solutions Specialist Hospital Inpatient and Outpatient Process
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: V5.4 Measure Updates Questions and Answers Speakers Noel Albritton, RN, BS, Lead Solutions Specialist Hospital Inpatient and Outpatient Process
Stampede Sepsis: A Statewide Collaborative
 Stampede Sepsis: A Statewide Collaborative Kentucky Sepsis Summit August 24, 2016 T E R I H U L E T T, R N, B S N, C I C, F A P I C P R O G R A M M A N A G E R, I N F E C T I O N P R E V E N T I O N CHA
Stampede Sepsis: A Statewide Collaborative Kentucky Sepsis Summit August 24, 2016 T E R I H U L E T T, R N, B S N, C I C, F A P I C P R O G R A M M A N A G E R, I N F E C T I O N P R E V E N T I O N CHA
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Establishing an Emergency Department Sepsis Screen
 Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky 2 About Us St. Claire Regional Medical Center is
Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky 2 About Us St. Claire Regional Medical Center is
Objectives 10/09/2015. Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935
 Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience. Presented by: Fadwa Jabboury, RN, MSN
 CMC Experience. Presented by: Fadwa Jabboury, RN, MSN") Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
The CAUTI Can-Can. Hennepin County Medical Center August Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion
 Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
Caitlin Eccles-Radtke, MD Infectious Disease and CAUTI Prevention Champion Laura Miller, RN MICU Manager The CAUTI Can-Can Hennepin County Medical Center August 2017 Lynelle Scullard, RN SICU Manager Kathleen
ACEP Emergency Quality (E-QUAL) Network Sepsis Learning Collaborative Funded by the Center for Medicare & Medicaid Innovation (CMMI)
 Network Sepsis Learning Collaborative Funded by the Center for Medicare & Medicaid Innovation (CMMI)") ACEP Emergency Quality (E-QUAL) Network Sepsis Learning Collaborative 2016 Funded by the Center for Medicare & Medicaid Innovation (CMMI) Outline A Case Epidemiology of Sepsis Learn Baseline Protocolize
ACEP Emergency Quality (E-QUAL) Network Sepsis Learning Collaborative 2016 Funded by the Center for Medicare & Medicaid Innovation (CMMI) Outline A Case Epidemiology of Sepsis Learn Baseline Protocolize
SEPSIS Management in Scotland
 SEPSIS Management in Scotland A Report by the Scottish Trauma Audit Group November 2010 STAG NHS National Services Scotland/Crown Copyright 2010 Brief extracts from this publication may be reproduced provided
SEPSIS Management in Scotland A Report by the Scottish Trauma Audit Group November 2010 STAG NHS National Services Scotland/Crown Copyright 2010 Brief extracts from this publication may be reproduced provided
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair
 or Atrial Septal Defect (ASD) Repair") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
Southern California CSU DNP Consortium
 Southern California CSU DNP Consortium California State University, Fullerton California State University, Long Beach California State University, Los Angeles IMPLEMENTATION OF A SEPSIS PROTOCOL: A QUALITY
Southern California CSU DNP Consortium California State University, Fullerton California State University, Long Beach California State University, Los Angeles IMPLEMENTATION OF A SEPSIS PROTOCOL: A QUALITY
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
 Unfolding Clinical Reasoning Case Study: STUDENT Sepsis I. Data Collection History of Present Problem: Jean Kelly is an 82 year old woman who has been feeling more fatigued for the last three days and
Unfolding Clinical Reasoning Case Study: STUDENT Sepsis I. Data Collection History of Present Problem: Jean Kelly is an 82 year old woman who has been feeling more fatigued for the last three days and
Antimicrobial Stewardship in Continuing Care. Nursing Home Acquired Pneumonia Clinical Checklist
 Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease
 Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease Course lead Colette Laws-Chapman Faculty Course / Curriculum Recognising the Deteriorating Adult Target Delegates
Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease Course lead Colette Laws-Chapman Faculty Course / Curriculum Recognising the Deteriorating Adult Target Delegates
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
In a common ICU situation like this, there are two main questions we have to answer daily:
 MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
Buchanan, 1996; Knaus, Felton, Burton, Fobes, & Davis 1997, J. of Nsg Administration
 Can Patients with Moderate to High Risk Acute Coronary Syndromes Be Cared For safely in a Cardiac Acute Care Unit (ACU) Introduction Several studies have evaluated the safety of managing g patient with
Can Patients with Moderate to High Risk Acute Coronary Syndromes Be Cared For safely in a Cardiac Acute Care Unit (ACU) Introduction Several studies have evaluated the safety of managing g patient with
LVHN Sepsis Quality Improvement Project
 LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
Use of TeleMedicine to Improve Clinical and Financial Outcomes
 Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015 Use of TeleMedicine
Use of TeleMedicine to Improve Clinical and Financial Outcomes Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director, Critical Care and eicu Advocate Health Care November 12, 2015 Use of TeleMedicine
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
GAMUT QI Collaborative Consensus Quality Metrics (v. 05/16/2016)
") 1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
1) Ventilator use in patients 1 with advanced airways reported as Percent of patient transport contacts with an advanced airway 2 supported by a mechanical ventilator. 2) Scene and bedside times for STEMI
ASCO s Quality Training Program
 ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
ASCO s Quality Training Program Project Title: Treatment of febrile neutropenia at the University of Virginia Presenter s Name: Tri Le, MD, Tanya Thomas, RN, Michael Keng, MD Institution: University of
Assessment and Reassessment of Patients
 Approved by: Assessment and Reassessment of Patients Senior Director, Operations, Emergency, Medicine, Critical Care & Respiratory - GNCH Senior Director, Operations, Emergency, Medicine, Critical Care
Approved by: Assessment and Reassessment of Patients Senior Director, Operations, Emergency, Medicine, Critical Care & Respiratory - GNCH Senior Director, Operations, Emergency, Medicine, Critical Care
Sepsis Mortality - A Four-Year Improvement Initiative
 Organization: Solution Title: Sinai Hospital of Baltimore Sepsis Mortality - A Four-Year Improvement Initiative Program/Project Description:What was the problem to be solved? How was it identified? What
Organization: Solution Title: Sinai Hospital of Baltimore Sepsis Mortality - A Four-Year Improvement Initiative Program/Project Description:What was the problem to be solved? How was it identified? What
Worth a Thousand Words: Telling a Story with Data
 A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient