Preventing Sepsis Mortality
|
|
|
- Sophie Johns
- 5 years ago
- Views:
Transcription



1 Murray State's Digital Commons Scholars Week Spring Scholars Week Preventing Sepsis Mortality Karli Tabers Follow this and additional works at: Part of the Critical Care Nursing Commons Tabers, Karli, "Preventing Sepsis Mortality" (2017). Scholars Week This Poster Presentation is brought to you for free and open access by the The Office of Research and Creative Activity at Murray State's Digital Commons. It has been accepted for inclusion in Scholars Week by an authorized administrator of Murray State's Digital Commons. For more information, please contact msu.digitalcommons@murraystate.edu.
2 RUNNING HEAD: PREVENTING SEPSIS MORTALITY Preventing Sepsis Mortality Karli Tabers Murray State University School of Nursing
3 Table of Contents Process description...4 Theoretical Framework...5 Evidence...6 Proposed Procedures...8 Implementation...10 Conclusion...11 References...12 Appendix A...14 Appendix B
4 Abstract This research paper explores recent evidence based research on preventing sepsis mortality in inpatient units. Sepsis mortality is an increasing problem in the state of Kentucky and demands immediate intervention. At Baptist Health Paducah, 44 deaths were related to sepsis in a 5-month period. Most deaths related to sepsis can be prevented. This research looks at how these deaths can be prevented and how nurses must change their practice to avoid further mortality from sepsis. This paper includes a literature review of recent research proving that sepsis mortality can be prevented by focusing on discharge teaching to all patients, implementing code sepsis in the facility, looking at trends in vital signs over time and strict compliance with sepsis protocols. 3
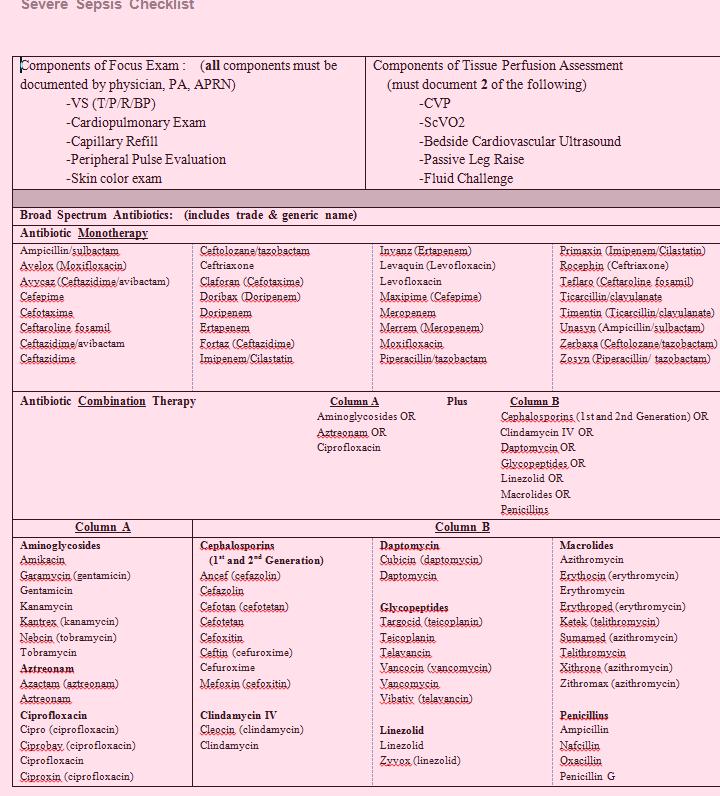
5 Preventing Sepsis Mortality According to the Center for Disease Control (2014), more than one million people are diagnosed with sepsis every year, and 28-50% of those cases result in death. In Kentucky, 16.1% of deaths are related to sepsis. That s 6% higher than the national average of 10.7% (CDC, 2014). Evidence based research shows that early detection and aggressive treatment of sepsis result in more optimistic outcomes. In a recent sepsis meeting at Baptist Health Paducah (BHP), it was identified that 44 people had died from sepsis at this facility in the last year. Factors that can reduce sepsis mortality include compliance with strict protocols, early detection and aggressive treatment of sepsis, looking at trends in vital signs, and educating patients before they are discharged about preventing sepsis to prevent hospital readmissions. Sepsis is defined by the CDC as, a complication caused by the body s overwhelming and life-threatening response to an infection, which can lead to tissue damage, organ failure, and death (2016). Anyone can acquire sepsis from any infection in any part of the body. Sepsis is most commonly caused by infections of the lungs, urinary tract, skin, and gut (CDC, 2016). Since inpatient units typically see patients with these infections, sepsis is prevalent and the prevention of and early treatment of sepsis must be a priority to all staff members. Process Description Currently at BHP, there is a sepsis protocol in place on all units. The sepsis checklist includes specific identifiers that place someone in a category of sepsis. These identifiers are: suspected infection source; SIRS (temp >100.9 or <96.8, HR >90, RR>20, WBH>12,000 or <4000); and organ dysfunction (SBP<90, MAP<65, Acute respiratory failure, Creatinine >2.0, Bilirubin>2.0, platelets <100,000, INR >1.5 or ptt>60 seconds, or lactate >2.0). If the patient 4
6 falls into any of these categories, the nurse begins the sepsis protocol at time zero. Time zero begins when the patient meets the criteria. Within 60 minutes of time zero the initial lactate level should be drawn. If the lactate is greater than 2 at this time, the lactate should be repeated within 4 hours, blood cultures should be drawn, and a broad spectrum antibiotic should be initiated (Baptist, 2017). A copy of this protocol can be located in the Appendix A. When a nurse at this facility suspects sepsis, he/she is to contact the physician and ask for sepsis labs to be drawn (lactate, blood cultures) and for an antibiotic to be ordered which must begin within 60 minutes from time zero. The nurses at BHP have expressed barriers to this process. The most common complaint among nurses is that the physician doesn t order the lactic acid lab in time or doesn t believe that the patient may be septic, which prolongs the process. The nurses at this facility also feel as though they cannot get the sepsis protocol initiated and/or completed in a timely manner due to many reasons. The main reason for failure to initiate the sepsis protocol is that the physician doesn t order the labs, but they also run into issues in prioritizing care and feeling as though they need to take care of a patient that is more sick right now than the patient who may have sepsis. Theoretical Framework Ida Jean Orlando s nursing theory explains the role of the nurse and the importance of meeting the patient s immediate need for help. To be successful at meeting the patient s immediate need for help, the nurse must first assess the patient. Ida Jean Orlando (1990) describes the three elements of the nursing process as, the behavior of the patient, the reaction of the nurse, and the nursing actions which are designed for the patient s benefit (p 36). When a patient has sepsis the nurse must treat each patient on an individual basis and assess them thoroughly. Orlando emphasizes the importance of the nurse physically assessing the patient and 5
7 using his/her best clinical judgment to treat the patient. Furthermore, Orlando emphasizes that the nurse must continually reevaluate the patient s status to decide if the nursing intervention was successful or if the patient requires further treatment. This is crucial in treating the patient with sepsis. The nurse must continue to assess the patient for improvement or deteriorating status and communicate that with the physician promptly. Evidence The nurse must be able to recognize the signs and symptoms of sepsis. According to the sepsis fact sheet found on National Institute of General Medical Sciences, the common signs and symptoms of sepsis are fever, chills, rapid breathing and heart rate, rash, confusion and disorientation (NIGMS, 2017). In the critical care units, sepsis is harder to identify due to the patient s already poor condition. The nurses on these units must be highly aware of these sepsis signs, their patient s individual status and initiate the sepsis protocol immediately. Time is of the essence when treating sepsis. According to Jody Vaughan and Andy Parry in Assessment and management of the septic patient, for every hour delay in treatment, mortality risk increases by 7.6% (p 1198). It is vital that the nurses and physicians communicate at the first sign of sepsis and that labs are ordered. Implementing a code sepsis could be beneficial in improving communication between staff members and result in a quicker response time by physicians and nurses. In a study looking at ten different sepsis bundles, the group labeled code SMART had a higher compliance than the other sepsis bundles. Not only was the compliance higher in the code SMART group but the survival rate at discharge was higher than any of the other groups. When a nurse suspected that a patient had sepsis he/she called code SMART over the overhead the facility. The team that responded to this code included an 6
8 ICU physician, ICU nurse, respiratory care practitioner and pharmacist (LaRosa, Ahmad, Feinberg, Shah, DiBrienza, & Studer, 2012, p 2). Furthermore, the entire staff should be educated on the basic signs and symptoms of sepsis and be prepared to help initiate the sepsis protocol. In a research study by Doerfler, et al. (2015), North Shore-LIJ Health System implemented teaching to not only nurses, but clinical support staff and even clerical staff to help decrease mortality rates from sepsis. For example, when they called a code sepsis the clerical worker was responsible for calling the pharmacy and informing them of the possible need of antibiotics as soon as possible. In addition, the nursing assistants were educated on signs and symptoms of sepsis and were aware of vital signs that may need to be reported to the nurse. The results of this study showed that by including all staff members in the sepsis code, mortality from sepsis at North Shore-LIJ decreased by approximately 50% and increased compliance with sepsis resuscitation bundles (p 208). Often when assessing patients for sepsis the provider is looking only at vital signs for that moment or the most recent vital signs that were recorded. For example, if a patient s heart rate is not greater than the protocol of 90 then the system will not flag that this patient is becoming septic and the provider will not initiate the protocol. In a recent study by Quinten, Meurs, Maaten, & Ligtenberg, the authors discovered that in the septic patient the vital signs begin to form a trend before the system may flag this patient as septic. Therefore, if the nurse is not looking at the trend of vital signs over a period of time he/she would not notice the deteriorating trend in vital signs. Specifically, the authors found that the blood pressure of the patients who had sepsis decreased, the heart rate increased, the MAP decreased, and the temperate increased before the patient s vital signs actually fell into the protocol parameters (Trends in vital signs, 2016). 7
9 Eighty percent of sepsis cases begin outside of the hospital and this is the highest reason for hospital readmissions (NIGMS, 2017). This hospital currently does not have a requirement for discharge patient teaching on sepsis. By teaching patients about the signs and symptoms of sepsis and explaining that sepsis is a medical emergency, sepsis readmission rates could decrease. According to a recent study that looked at 30-day readmission rates, sepsis was the number one reason for readmission and the costliest. The average cost for a patient readmitted because of sepsis was $10,070 (Mayr, F. B., Talisa, V. B., & Balakumar, V., 2017). When a patient at BHP is readmitted due to a sepsis diagnosis, the hospital must pay for that patient s stay. In an investigation looking into 30 day hospital readmissions and ways to prevent those readmissions, Leppin, Gionfriddo, & Kessler (2014) implemented interventions to prevent readmission such as discharge planning that was individualized to each patient, a telephone follow up, patient-directed patient education, home visits, a patient hotline where patients could access healthcare workers for their questions related to their illness, and other interventions specialized to each patient such as meetings with the caregiver and education for them. Organically the authors found that the readmission rate related to sepsis among investigated facilities was 82%. Implementing interventions that are complex, involve more individuals in the care delivery, and support patient capacity for self-care are 1.4, 1.3, and 1.3 times more effective than other interventions (p 1095). Proposed Procedures First and foremost, the nurses must become experts at recognizing the early signs and symptoms of sepsis. This can be implemented throughout the hospital through regular education opportunities and simulation labs. New nurses should participate in extra training for sepsis identification and how to proceed with the sepsis protocol. 8
10 In addition to assessing the patient for sepsis signs and symptoms, the nurse should look at the patient s vital signs over time. The nurse can do this simply in EPIC by pulling up the patient s vital signs over the past 24 hours. If the nurse notices a decline, even if it is not within the sepsis protocol, he/she should communicate this concern to the physician and proceed with the sepsis checklist. To ensure that nurses are following this protocol the patient s trend of vital signs over the last 24 hours should be printed and posted in each patient s room so that the nurses can seamlessly handoff the patient at shift change and continue to monitor the trend in vital signs. The entire staff should be involved in sepsis management; this will address the issue of not having enough time, or the physician not ordering the labs in time. This begins with the nursing assistants/technicians/aids. These clinical support staff members often spend more time at the bedside than nurses and physicians. The support staff should be educated on vital signs that should be reported to the nurse immediately. Once the nurse is notified he/she will call the code sepsis. Code sepsis will notify the physician of the patient s deteriorating condition, the pharmacy will be notified that the floor will need antibiotics soon, and the facility can proceed with their protocol. Code sepsis will improve compliance with the sepsis protocol as it did in the study by LaRosa et al (2012). When a patient is discharged from the hospital because of any infection, they will receive teaching about the signs and symptoms of sepsis and how to proceed with medical help. The nurse should spend time educating the patient, not only giving them a printout to take home, but spending extra time explaining what sepsis is and why it is an issue. An example of the issues that the nurse should go over with the patient are included in the Appendix B. 9
11 Implementation into Practice Currently at this facility there is a sepsis team that meets monthly and works diligently to prevent sepsis. To implement the new protocols, the sepsis team would first be informed of the change. These team members include the directors of every floor at the facility, infection control, quality control, research, and a physician. The directors will then hold a meeting with their charge nurses and educate them about the new policy. The charge nurses will educate staff nurses on when to call a code sepsis and how to respond. The physician will educate the hospitalist team and other physicians that work at the facility about the change and how they will respond when a code sepsis is called. Once every member of the healthcare team has been educated on code sepsis the code can be implemented. Since this is a multitude of changes and new procedures it will take time to implement throughout the entire hospital. The implementation will start in the critical care units. The nursing assistants will be trained on what vital signs to report to the registered nurse. The nurses will be trained on early recognition of sepsis including looking at the trends in vital signs. The printout of vital signs will begin to be posted in each patient s room immediately since this is an easy implementation. The nurses will be educated on what to include on discharge to every patient that is being discharged, a handout can be found in appendix B. Each patient should receive this handout and it should be explained to them at discharge. The patient should understand that sepsis is a medical emergency. The patient should also receive a number that the unit can be reached if they have questions. 10
12 Conclusion Sepsis is a concern not only at the hospital in this study but across all hospitals in Kentucky. The sepsis rate is higher in Kentucky than the national average and the mortality rate from sepsis has increased 31% since 1999 (CDC, 2014). There is evidence based research that proves nurses have a role in improving the outcomes of sepsis by implementing interventions related to early recognition and treatment of sepsis. The barriers to completing the sepsis protocol must be addressed and compliance rates must improve. It is essential that the nurse is diligent in assessing each patient for sepsis and continuing the assessment throughout care. The nurse must also be willing to spend time with each patient at discharge to prevent readmission due to sepsis. Along with the nurse s important role in preventing mortality from sepsis, the healthcare team can work together to improve sepsis recognition and outcomes. 11
13 References Center for Disease Control and Prevention. (2014). Sepsis. Retrieved from Center for Disease Control and Prevention. (2016). Sepsis clinical guidelines. Retrieved from Doerfler, M. E., D Angelo, J., Jacobsen, D., Jarrett, M. P., Kabcenell, A. I., Masick, K. D.,... Stier., L. (2015). Methods for reducing sepsis mortality in emergency departments and inpatient units. The Joint Commission Journal on Quality and Patient Safety, 41 (5), LaRosa, J. A., Ahmad, N., Feinberg, M., Shah, M., DiBrienza, R., & Studer, S., (2012). The use of an early alert system to improve compliance with sepsis bundles and to assess impact on mortality. Critical Care Research and Practice, 1-8. Leppin, A.L., Gionfriddo, M.R., Kessler, M., Brito, J.P., Mair, F. S., Gallacher, K.,... Montori, V.M. (2014). Preventing 30-day hospital readmissions: a systematic review and metanalysis of randomized trials. Journal of American Medical Association, 174 (7), Mayr, F. B., Talisa, V. B., Balakuma, V. (2017). Proportion and cost of unplanned 30-day readmissions after sepsis compared with other medical conditions. Journal of the American Medical Association, 317 (5), National Institutes of Health. (2017, February 01). Sepsis Fact Sheet. Retrieved from: Orlando, J. I. (1990). The dynamic nurse-patient relationship. New York, NY: National League for Nursing. 12
14 Quinten, V. M., Merurs, M., Maaten, J.C., Ligtenberg, J. J., (2016). Trends in vital signs and routine biomarkers in patients with sepsis during resuscitation in the emergency department. BMJ Open, 1-9. Vaughan, J. & Parry A. (2016). Assessment and management of the septic patient: part 2. British Journal of Nursing, 25 (21),

15 Appendix A Baptist Health Paducah Severe Sepsis Checklist 14
16 15

17 Appendix B Patient handout at discharge 16
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU)
") Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
Northwell Sepsis Collaborative Evidence Based Best Practice
 Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
Saving Lives with Best Practices and Improvements in Sepsis Care
 Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Success Story Saving Lives with Best Practices and Improvements in Sepsis Care EXECUTIVE SUMMARY Although Thibodaux Regional Medical Center had achieved sepsis mortality rates below the national average,
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis
 Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Making the Stars Align When Time Matters: Leveraging Actionable Data to Combat Sepsis Licking Memorial Health Systems Patient Impact Where did we begin? EDUCATION EDUCATION EDUCATION EDUCATION EDUCATION
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Stopping Sepsis in Virginia Hospitals and Nursing Homes Hospital Webinar #2 - Tuesday, March 21, 2017 Welcome and Introductions Today s objectives: Introduce Sepsis Practice Collaborative Model Tier 1
Current Status: Active PolicyStat ID: Guideline: Sepsis Identification And Management in Adults GUIDELINE: COPY
 Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Current Status: Active PolicyStat ID: 1537683 Effective: 8/7/2015 Approved: 8/7/2015 Last Revised: 8/7/2015 Expires: 8/6/2018 Author: Chief Nursing Officer Document Area: Nursing Administration References:
Understand. Learning Objectives Module 1. Surviving Sepsis Campaign Sepsis e learn Module 1. Situation & Background. Sepsis e Learn: Module 1
 Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
Surviving Sepsis Campaign Sepsis e learn Module 1 Situation & Background Understand Learning Objectives Module 1 The impact sepsis has on patient mortality and healthcare costs. The importance of improving
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
Sepsis/Septic Shock Pre-Hospital Care
 Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
Sepsis/Septic Shock Pre-Hospital Care MARKUS DORSEY-HIRT, RN CFRN CHIEF FLIGHT NURSE/CNO CARE FLIGHT Chief Flight Nurse/CNO for Care Flight 1 Statistics More than 1.5 million people get sepsis each year
ICU - Sepsis, CAUTI and CLABSI Less May Be Better. HRET HIIN ICU Virtual Event April 11, 2017
 ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
ICU - Sepsis, CAUTI and CLABSI Less May Be Better HRET HIIN ICU Virtual Event April 11, 2017 1 Emily Koebnick, Program Manager, HRET WELCOME AND INTRODUCTIONS 2 Webinar Platform Quick Reference Mute computer
Sepsis The Silent Killer in the NHS
 Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
Sepsis The Silent Killer in the NHS Kate Beaumont, Trustee, UK Sepsis Trust Nurse Director The Learning Clinic Director QGi Ltd Former Head of Patient Safety and lead for deterioration, National Patient
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management
 SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
Sepsis Mortality - A Four-Year Improvement Initiative
 Organization: Solution Title: Sinai Hospital of Baltimore Sepsis Mortality - A Four-Year Improvement Initiative Program/Project Description:What was the problem to be solved? How was it identified? What
Organization: Solution Title: Sinai Hospital of Baltimore Sepsis Mortality - A Four-Year Improvement Initiative Program/Project Description:What was the problem to be solved? How was it identified? What
Personal Protective Equipment Use for Patients with Clostridium difficile
 Murray State's Digital Commons Scholars Week Fall Scholars Week 2016 Nov 14th, 11:30 AM - 1:30 PM Personal Protective Equipment Use for Patients with Clostridium difficile Mallory L. Compton Murray State
Murray State's Digital Commons Scholars Week Fall Scholars Week 2016 Nov 14th, 11:30 AM - 1:30 PM Personal Protective Equipment Use for Patients with Clostridium difficile Mallory L. Compton Murray State
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014
 Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
Using Predictive Analytics to Improve Sepsis Outcomes 4/23/2014 Ryan Arnold, MD Department of Emergency Medicine and Value Institute Christiana Care Health System, Newark, DE Susan Niemeier, RN Chief Nursing
The Davies Award Is: The HIMSS Nicholas E. Davies Award of Excellence. Awarding IT. Improving Healthcare.
 The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
The Davies Award Is: Since 1994, the Nicholas E. Davies Award of Excellence is HIMSS highest global recognition of hospitals, ambulatory practices and clinics, community health organizations, and public
ACTION PLANS. OHA Statewide Sepsis Initiative. January 13, 2016
 ACTION PLANS OHA Statewide Sepsis Initiative January 13, 2016 USING DRIVER DIAGRAMS FOR ACTION PLANS Used to organize theories and ideas in an improvement effort Visual display of why things are the way
ACTION PLANS OHA Statewide Sepsis Initiative January 13, 2016 USING DRIVER DIAGRAMS FOR ACTION PLANS Used to organize theories and ideas in an improvement effort Visual display of why things are the way
Establishing an Emergency Department Sepsis Screen
 Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky 2 About Us St. Claire Regional Medical Center is
Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky 2 About Us St. Claire Regional Medical Center is
Stampede Sepsis: A Statewide Collaborative
 Stampede Sepsis: A Statewide Collaborative Kentucky Sepsis Summit August 24, 2016 T E R I H U L E T T, R N, B S N, C I C, F A P I C P R O G R A M M A N A G E R, I N F E C T I O N P R E V E N T I O N CHA
Stampede Sepsis: A Statewide Collaborative Kentucky Sepsis Summit August 24, 2016 T E R I H U L E T T, R N, B S N, C I C, F A P I C P R O G R A M M A N A G E R, I N F E C T I O N P R E V E N T I O N CHA
APPLICATION FORM. Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes. Director of Quality
 APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
APPLICATION FORM Title of Entry: Sepsis: A Health System s Journey Toward Optimal Patient Care & Outcomes Division: Large Organizations Award: Excellence in Care Entrant s Name and Title: Maurita K. Marhalik,
Keep watch and intervene early
 IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
IntelliVue GuardianSoftware solution Keep watch and intervene early The earlier, the better Intervene early, by recognizing subtle signs Clinical realities on the general floor and in the emergency department
Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of an Early
Ruchika D. Husa, MD, MS
 Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
Early Response Teams Ruchika D. Husa, MD, MS Assistant Professor of Medicine Division i i of Cardiovascular Medicine i The Ohio State University Wexner Medical Center OBJECTIVES Provide an overview of
IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 2
 Thursday, September 26 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 2 John D Angelo, MD, FACEP Andy Odden, MD Diane Jacobsen,
Thursday, September 26 These presenters have nothing to disclose IHI Expedition Treating Sepsis in the Emergency Department and Beyond Session 2 John D Angelo, MD, FACEP Andy Odden, MD Diane Jacobsen,
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
Sepsis Management at Russell Medical
 Sepsis Management at Russell Medical Sarah Beth Gettys V.P. Patient Services Russell Medical Dr. Michele Goldhagen MD, CMO, ED Medical Director Russell Medical Oct 3, 2017 1 Objectives List key success
Sepsis Management at Russell Medical Sarah Beth Gettys V.P. Patient Services Russell Medical Dr. Michele Goldhagen MD, CMO, ED Medical Director Russell Medical Oct 3, 2017 1 Objectives List key success
To Dip or Not To Dip a patient centred approach to improve the management of UTIs in the Care Home environment
 To Dip or Not To Dip a patient centred approach to improve the management of UTIs in the Care Home environment Sharing success AMS Workshop Leeds & London 2016 Elizabeth Beech Pharmacist - NHS Bath and
To Dip or Not To Dip a patient centred approach to improve the management of UTIs in the Care Home environment Sharing success AMS Workshop Leeds & London 2016 Elizabeth Beech Pharmacist - NHS Bath and
Passage to Excellence Our Sepsis Journey
 Passage to Excellence Our Sepsis Journey St. Catherine of Siena Medical Center October/November 2017 St. Catherine of Siena Medical Center 311 bed community hospital Voluntary medical staff leadership
Passage to Excellence Our Sepsis Journey St. Catherine of Siena Medical Center October/November 2017 St. Catherine of Siena Medical Center 311 bed community hospital Voluntary medical staff leadership
Objectives 10/09/2015. Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935
 Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
Screen and Intervene: Improved Outcomes From a Nurse-Initiated Sepsis Protocol C935 2015 ANCC National Magnet Conference October 9, 2015 Kristin Drager MSN RN CNL CEN William S. Middleton Memorial Veterans
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers
 Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
Sepsis: Developing and Implementing a Housewide Sepsis Program Understanding the Four Tiers Pat Posa, RN, BSN, MSA, FAAN Quality Excellence Leader St. Joseph Mercy Hospital Agenda Define Sepsis Establish
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond. Why the focus on Sepsis?
 The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
The Kaiser Sunnyside Sepsis Story Care Improvement from EGDT through ProCESS and Beyond Lauren Bridge, RN, MN NEA-BC Why the focus on Sepsis? Mortality, Intensity of Resources, Risk of Readmission Compared
The POLST Conversation POLST Script
 The POLST Conversation POLST Script The POLST Script provides detailed information in order to develop comfort and competence when facilitating a POLST conversation. The POLST conversation utilizes realistic
The POLST Conversation POLST Script The POLST Script provides detailed information in order to develop comfort and competence when facilitating a POLST conversation. The POLST conversation utilizes realistic
Scholars Week Spring Scholars Week 2016
 Murray State's Digital Commons Scholars Week Spring Scholars Week 2016 Apr 18th, 12:00 PM - 2:00 PM Fall prevention Cody Durbin Murray State University Follow this and additional works at: http://digitalcommons.murraystate.edu/scholarsweek
Murray State's Digital Commons Scholars Week Spring Scholars Week 2016 Apr 18th, 12:00 PM - 2:00 PM Fall prevention Cody Durbin Murray State University Follow this and additional works at: http://digitalcommons.murraystate.edu/scholarsweek
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
Improving the Identification, Delivery of Care, and Outcomes of Hospital-Acquired Sepsis
 University of Kentucky UKnowledge DNP Projects College of Nursing 2016 Improving the Identification, Delivery of Care, and Outcomes of Hospital-Acquired Sepsis Nicholas James Welker University of Kentucky,
University of Kentucky UKnowledge DNP Projects College of Nursing 2016 Improving the Identification, Delivery of Care, and Outcomes of Hospital-Acquired Sepsis Nicholas James Welker University of Kentucky,
Overview of CDC s Sepsis Activities
 Centers for Disease Control and Prevention Overview of CDC s Sepsis Activities WHO Sepsis Technical Expert Meeting Denise M. Cardo M.D. Director, Division of Healthcare Quality Promotion National Center
Centers for Disease Control and Prevention Overview of CDC s Sepsis Activities WHO Sepsis Technical Expert Meeting Denise M. Cardo M.D. Director, Division of Healthcare Quality Promotion National Center
Sepsis, An Interdisciplinary and Collaborative Approach. Bassett Medical Center October/November 2017
 Sepsis, An Interdisciplinary and Collaborative Approach Bassett Medical Center October/November 2017 Bassett Medical Center 180 bed acute care inpatient teaching facility in Cooperstown, New York is the
Sepsis, An Interdisciplinary and Collaborative Approach Bassett Medical Center October/November 2017 Bassett Medical Center 180 bed acute care inpatient teaching facility in Cooperstown, New York is the
Advanced Measurement for Improvement Prework
 Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
Advanced Measurement for Improvement Prework IHI Training Seminar Boston, MA March 20-21, 2017 Faculty: Richard Scoville PhD; Gareth Parry PhD Thank you for enrolling in IHI s upcoming seminar on designing
Inpatient Quality Reporting (IQR) Program
 Program") SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2 Measure Updates Presentation Transcript Moderator: Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock: v5.2 Measure Updates Presentation Transcript Moderator: Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives,
Sepsis guidance implementation advice for adults
 Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Sepsis guidance implementation advice for adults NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Strategy & Innovation
Presenters. Tiffany Osborn, MD, MPH. Laura Evans, MD MSc. Arjun Venkatesh, MD, MBA, MHS
 Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
Sepsis Wave II New recommendations from the Surviving Sepsis Campaign and what do they mean for the ED How to use the E-QUAL Portal and submit Activity 2 Presenters Laura Evans, MD MSc Tiffany Osborn,
South Central HIINergy Partners
 South Central HIINergy Partners Six states partnering for quality and patient safety through the SEPSIS: Nursing and Front-Line Staff Empowerment for Early Identification and Prompt Treatment Welcome and
South Central HIINergy Partners Six states partnering for quality and patient safety through the SEPSIS: Nursing and Front-Line Staff Empowerment for Early Identification and Prompt Treatment Welcome and
QBPs: New Ways To Improve Patient Care
 Module 1: QBPs: New Ways To Improve Patient Care Quality Based Procedures (QBPs) Pathway Improvement Program What are Quality Based Procedures (QBPs)? QBPs are groups of patients with similar diagnoses
Module 1: QBPs: New Ways To Improve Patient Care Quality Based Procedures (QBPs) Pathway Improvement Program What are Quality Based Procedures (QBPs)? QBPs are groups of patients with similar diagnoses
2014 Maryland Patient Safety Center s Call for Solutions
 Improving Sepsis Outcomes Through Coordinated Early Recognition, Assessment, and Treatment UM-CRMC Sepsis Survival Rate 100% 95% 90% 89.5% CRMC 85% 85.3% 86.1% 86.2% 81.8% 82.3% 85.7% 84.7% 86.1% MD Statewide
Improving Sepsis Outcomes Through Coordinated Early Recognition, Assessment, and Treatment UM-CRMC Sepsis Survival Rate 100% 95% 90% 89.5% CRMC 85% 85.3% 86.1% 86.2% 81.8% 82.3% 85.7% 84.7% 86.1% MD Statewide
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Admissions with neutropenic sepsis in adult, general critical care units in England, Wales and Northern Ireland Question What were the: age; gender; APACHE II score; ICNARC physiology score; critical care
Sepsis Management in Scotland. Calum McGregor Consultant Acute Medicine National Clinical Lead for Acute Care Healthcare Improvement Scotland
 Sepsis Management in Scotland Calum McGregor Consultant Acute Medicine National Clinical Lead for Acute Care Healthcare Improvement Scotland Sepsis Management in Scotland Outline: Background on sepsis
Sepsis Management in Scotland Calum McGregor Consultant Acute Medicine National Clinical Lead for Acute Care Healthcare Improvement Scotland Sepsis Management in Scotland Outline: Background on sepsis
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Mobile Communications
 Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Mobile Communications Speakers Brett Moran, MD, BCIM, BCCI Associate Chief Medical Officer and CMIO About me Former Professor of Internal Medicine where he practiced academic medicine at UTSW for 19 years
Monday, August 15, :00 p.m. Eastern
 Monday, August 15, 2016 2:00 p.m. Eastern Dial In: 888.863.0985 Conference ID: 34874161 Slide 1 Speakers Deb Kilday, MSN, RN Senior Performance Partner Performance Services Quality & Safety Premier, Inc.
Monday, August 15, 2016 2:00 p.m. Eastern Dial In: 888.863.0985 Conference ID: 34874161 Slide 1 Speakers Deb Kilday, MSN, RN Senior Performance Partner Performance Services Quality & Safety Premier, Inc.
THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON
 THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations
THE 2017 QUALIS HEALTH AWARDS OF EXCELLENCE IN HEALTHCARE QUALITY IN WASHINGTON Since 2002, Qualis Health has presented the annual Awards of Excellence in Healthcare Quality to outstanding organizations
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE. Early Recognition and Treatment of Severe Sepsis and Septic Shock
 SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
SEVERE SEPSIS & SEPTIC SHOCK CHANGE PACKAGE Early Recognition and Treatment of Severe Sepsis and Septic Shock table of contents severe sepsis & septic shock change package overview...... 1 Background.......................................................
LVHN Sepsis Quality Improvement Project
 LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
LVHN Sepsis Quality Improvement Project Matthew McCambridge, MD, MS Chief Quality Officer 2015 Lehigh Valley Health Network Don Levick, MD, MBA Chief Medical Information Officer LVHN Sepsis Quality Improvement
Running head: LEADERSHIP ANALYSIS: ROUNDING 1
 Running head: LEADERSHIP ANALYSIS: ROUNDING 1 Leadership Analysis: Rounding Jerrene Bramble, Tara Braun, Pamela Dusseau, Angelique Kinyon, William McKinley, Noranne Morin, Nicky Reed, and Ashleigh Wash
Running head: LEADERSHIP ANALYSIS: ROUNDING 1 Leadership Analysis: Rounding Jerrene Bramble, Tara Braun, Pamela Dusseau, Angelique Kinyon, William McKinley, Noranne Morin, Nicky Reed, and Ashleigh Wash
Document Ratification Group Chairman s Action
 Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
Early Identification and Treatment of Sepsis (Non Red Flag, Red Flag and Septic Shock) Type: Clinical Guideline Register No: 13026 Status: Public Developed in response to: Clinical need Contributes to
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Stopping the Chain of Infection: Strategies for Preventing Sepsis in Long Term Care September 20, 2016
 Stopping the Chain of Infection: Strategies for Preventing Sepsis in Long Term Care September 20, 2016 VHQC 1. Private, nonprofit healthcare consulting firm 2. Virginia s QIO since 1984; now the Quality
Stopping the Chain of Infection: Strategies for Preventing Sepsis in Long Term Care September 20, 2016 VHQC 1. Private, nonprofit healthcare consulting firm 2. Virginia s QIO since 1984; now the Quality
HealthONE Sepsis Program
 HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
HealthONE Sepsis Program Gary Winfield, MD Lindy Garvin, MPA, CPHRM June 12, 2017 0 0 This activity is jointly-provided by SynAptiv and the Colorado Hospital Association 1 1 Conflict of Interest Disclosure
For audio, join by telephone at , participant code #
 For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6. If you are having technical
Early Recognition of Sepsis in Long-Term Care
 Early Recognition of Sepsis in Long-Term Care September 19, 2018 HealthInsight Team Donna Thorson Senior Project Manager Nevada Shannon Cupka Project Manager New Mexico Leah Brandis Project Manager Oregon
Early Recognition of Sepsis in Long-Term Care September 19, 2018 HealthInsight Team Donna Thorson Senior Project Manager Nevada Shannon Cupka Project Manager New Mexico Leah Brandis Project Manager Oregon
Sepsis Screening Tool
 S I E M E N S NET A C C E S S Sepsis Screening Tool C L I N I C A L I N F O R M A T I C S M A R C H 2 0 1 2 Screening Objectives Early identification of patients for SEVERE Sepsis Initiate early resuscitation
S I E M E N S NET A C C E S S Sepsis Screening Tool C L I N I C A L I N F O R M A T I C S M A R C H 2 0 1 2 Screening Objectives Early identification of patients for SEVERE Sepsis Initiate early resuscitation
Medication Reconciliation: Preventing Errors and Improving Patient Outcomes
 Murray State's Digital Commons Scholars Week 2016 - Spring Scholars Week Apr 18th, 12:00 PM - 2:00 PM Medication Reconciliation: Preventing Errors and Improving Patient Outcomes Amanda S. Boren Murray
Murray State's Digital Commons Scholars Week 2016 - Spring Scholars Week Apr 18th, 12:00 PM - 2:00 PM Medication Reconciliation: Preventing Errors and Improving Patient Outcomes Amanda S. Boren Murray
A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals
 A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals Joshua Dunn, Pharm.D. Anne Teichman, Pharm.D. School of Pharmacy University of Charleston Charleston WV Corresponding author:
A Survey of Sepsis Treatment Protocols in West Virginia Critical Access Hospitals Joshua Dunn, Pharm.D. Anne Teichman, Pharm.D. School of Pharmacy University of Charleston Charleston WV Corresponding author:
nicheprogram.org 2016 Annual NICHE Conference Care Across the Continuum 1
 Phelps Memorial Hospital Center 5 South Bernadette Hogan, RN, Nurse Manager, Telemetry Mariel Consagra, RN, Anne Moss, RN Blessy Jacob, Pharm D, Clinical Pharmacy Coordinator Demographics 283 acute care
Phelps Memorial Hospital Center 5 South Bernadette Hogan, RN, Nurse Manager, Telemetry Mariel Consagra, RN, Anne Moss, RN Blessy Jacob, Pharm D, Clinical Pharmacy Coordinator Demographics 283 acute care
SPSP: Sepsis in Primary Care Collaborative. Dr Paul Davidson Associate Medical Director Primary Care NHS Highland
 SPSP: Sepsis in Primary Care Collaborative Dr Paul Davidson Associate Medical Director Primary Care NHS Highland Collaborative Ambition Improve early recognition and timely delivery of evidence-based interventions,
SPSP: Sepsis in Primary Care Collaborative Dr Paul Davidson Associate Medical Director Primary Care NHS Highland Collaborative Ambition Improve early recognition and timely delivery of evidence-based interventions,
Evaluating Adherence to the Sepsis Bundle and the Effectiveness of Best Practice Alerts
 University of Kentucky UKnowledge DNP Projects College of Nursing 2017 Evaluating Adherence to the Sepsis Bundle and the Effectiveness of Best Practice Alerts Kate Burnett University of Kentucky, kateburnett06@gmail.com
University of Kentucky UKnowledge DNP Projects College of Nursing 2017 Evaluating Adherence to the Sepsis Bundle and the Effectiveness of Best Practice Alerts Kate Burnett University of Kentucky, kateburnett06@gmail.com
C. difficile INFECTIONS
 A REGIONAL APPROACH TO THE PREVENTION OF C. difficile INFECTIONS Ghinwa Dumyati, M.D. FSHEA Center for Community Health, University of Rochester Medical Center Elizabeth Dodds Ashley, PharmD MHS, FCCP,
A REGIONAL APPROACH TO THE PREVENTION OF C. difficile INFECTIONS Ghinwa Dumyati, M.D. FSHEA Center for Community Health, University of Rochester Medical Center Elizabeth Dodds Ashley, PharmD MHS, FCCP,
Readmissions Moving beyond blame to fill the patient needs. Jackie Conrad RN, MBA, RCC Cynosure Health
 Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Readmissions Moving beyond blame to fill the patient needs Jackie Conrad RN, MBA, RCC Cynosure Health jconrad@cynosurehealth.org 1 51 year old male with 3 acute care admissions and 2 ED visits in the past
Stopping Sepsis in Virginia Hospitals and Nursing Homes. Hospital Webinar #6 - Tuesday, December 19, 2017
 Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Stopping Sepsis in Virginia Hospitals and Nursing Homes 1 Hospital Webinar #6 - Tuesday, December 19, 2017 I Have All This Data: What s Next? Tier 4 Implementation Implementation Your Sepsis Support Team
Preventing Sepsis: National Efforts and New Home Care Initiative in New York State A Presentation to the StateWide Senior Action Council
 Preventing Sepsis: National Efforts and New Home Care Initiative in New York State A Presentation to the StateWide Senior Action Council by Amy Bowerman, RN Al Cardillo, LMSW Tom Heymann, MBA Mohawk Valley
Preventing Sepsis: National Efforts and New Home Care Initiative in New York State A Presentation to the StateWide Senior Action Council by Amy Bowerman, RN Al Cardillo, LMSW Tom Heymann, MBA Mohawk Valley
Supplementary Appendix
 Supplementary Appendix Table S1: Average Adherence Rate to Combined and Individual Bundle Targets over the total Program Duration of 3.5 years in Severe Sepsis Patients (N=8387) % Not Applied % Not Applicable
Supplementary Appendix Table S1: Average Adherence Rate to Combined and Individual Bundle Targets over the total Program Duration of 3.5 years in Severe Sepsis Patients (N=8387) % Not Applied % Not Applicable
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Version 1.0 (posted Aug ) Aaron L. Leppin. Background. Introduction
 Aaron L. Leppin. Background. Introduction") Describing the usefulness and efficacy of discharge interventions: predicting 30 day readmissions through application of the cumulative complexity model (protocol). Version 1.0 (posted Aug 22 2013) Aaron
Describing the usefulness and efficacy of discharge interventions: predicting 30 day readmissions through application of the cumulative complexity model (protocol). Version 1.0 (posted Aug 22 2013) Aaron
SEPSIS Management in Scotland
 SEPSIS Management in Scotland A Report by the Scottish Trauma Audit Group November 2010 STAG NHS National Services Scotland/Crown Copyright 2010 Brief extracts from this publication may be reproduced provided
SEPSIS Management in Scotland A Report by the Scottish Trauma Audit Group November 2010 STAG NHS National Services Scotland/Crown Copyright 2010 Brief extracts from this publication may be reproduced provided
Coding Complexities of Critical Care
 Coding Complexities of Critical Care Jill Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing.
Coding Complexities of Critical Care Jill Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing.
Charting the Future: Implications and Insights for Informatics. Dana Alexander RN MSN MBA FHIMSS FAAN
 Charting the Future: Implications and Insights for Informatics Dana Alexander RN MSN MBA FHIMSS FAAN Conflict of Interest Disclosure Dana Alexander RN Has no real or apparent conflicts of interest to report.
Charting the Future: Implications and Insights for Informatics Dana Alexander RN MSN MBA FHIMSS FAAN Conflict of Interest Disclosure Dana Alexander RN Has no real or apparent conflicts of interest to report.
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING
 SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
SEPSIS RESEARCH WSHFT: THE IMPACT OF PREHOSPITAL SEPSIS SCREENING Dr. Duncan Hargreaves QI Fellow Worthing Hospital Allied Health Sciences Network 2017 SEPSIS IMPROVEMENT AT WSHFT QUESTcollaboration ->
Learning Objectives. John T. Mather Memorial Hospital
 Bringing Molecular Testing into the Clinical Lab: Effectiveness of Rapid Methicillin-Resistant Staphylococcus Aureus (MRSA) Screening in Reducing Hospital Acquired Infections Denise Uettwiller-Geiger,
Bringing Molecular Testing into the Clinical Lab: Effectiveness of Rapid Methicillin-Resistant Staphylococcus Aureus (MRSA) Screening in Reducing Hospital Acquired Infections Denise Uettwiller-Geiger,
If you have an. invasive fungal infection. Why did I get it? What is it? What should I do? What can I expect? INFORMATION FOR YOU AND YOUR FAMILY
 INFORMATION FOR YOU AND YOUR FAMILY my UNDERSTANDING invasive fungal infection If you have an invasive fungal infection What is it? Why did I get it? What can I expect? What should I do? Inside this brochure
INFORMATION FOR YOU AND YOUR FAMILY my UNDERSTANDING invasive fungal infection If you have an invasive fungal infection What is it? Why did I get it? What can I expect? What should I do? Inside this brochure
Number of sepsis admissions to critical care and associated mortality, 1 April March 2013
 Number of sepsis admissions to critical care and associated mortality, 1 April 2010 31 March 2013 Question How many sepsis admissions to an adult, general critical care unit in England, Wales and Northern
Number of sepsis admissions to critical care and associated mortality, 1 April 2010 31 March 2013 Question How many sepsis admissions to an adult, general critical care unit in England, Wales and Northern
Qatar University College of Pharmacy Advanced Clinical Internship WOMEN S HEALTH (OB/GYN)
") Qatar University College of Pharmacy Advanced Clinical Internship WOMEN S HEALTH (OB/GYN) DESCRIPTION The Obstetrics and Gynecology (OB/GYN) Advanced Clinical Internship is a rotation in the Doctor of
Qatar University College of Pharmacy Advanced Clinical Internship WOMEN S HEALTH (OB/GYN) DESCRIPTION The Obstetrics and Gynecology (OB/GYN) Advanced Clinical Internship is a rotation in the Doctor of
Clinical Guidance on the Identification and Evaluation of Possible SARS-CoV Disease among Persons Presenting with Community-Acquired Illness Version 2
 GUIDANCE AND RECOMMENDATIONS Clinical Guidance on the Identification and Evaluation of Possible SARS-CoV Disease among Persons Presenting with Community-Acquired Illness Version 2 This document provides
GUIDANCE AND RECOMMENDATIONS Clinical Guidance on the Identification and Evaluation of Possible SARS-CoV Disease among Persons Presenting with Community-Acquired Illness Version 2 This document provides
AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA. July 26 th, :00 a.m. 12:00 p.m. CDT
 AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA July 26 th, 2016 11:00 a.m. 12:00 p.m. CDT 1 WELCOME AND INTRODUCTIONS Mallory Bender, MA, LCSW, Program Manager, HRET
AHA/HRET HEN 2.0 SEPSIS WEBINAR: TIPS & TRICKS FOR SEPSIS RECOGNITION, BUNDLES & DATA July 26 th, 2016 11:00 a.m. 12:00 p.m. CDT 1 WELCOME AND INTRODUCTIONS Mallory Bender, MA, LCSW, Program Manager, HRET
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS
 WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
WHITE PAPER STRATEGIES AND SOLUTIONS FOR REDUCING INAPPROPRIATE READMISSIONS This paper offers a two-pronged approach to lower readmission rates and avoid Federal penalties. Jasen W. Gundersen, M.D., M.B.A.,
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16
 Schemes for 2015/16") Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Wessex Regional All Cause Deterioration (including Sepsis) Guidance
 Guidance") Wessex Regional All Cause Deterioration (including Sepsis) Guidance For Adult ( 16 non-pregnant) patients WACDG v1 11 th May 2018 Guidance includes models for the following healthcare settings Hospital
Wessex Regional All Cause Deterioration (including Sepsis) Guidance For Adult ( 16 non-pregnant) patients WACDG v1 11 th May 2018 Guidance includes models for the following healthcare settings Hospital
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
Dr Vincent Kirchner, MEDICAL DIRECTOR. Date Version Summary of amendments Oct New Procedure
 OLANZAPINE DEPOT PROCEDURE OCTOBER 2017 Policy title Policy reference Policy category Relevant to Date published Implementatio n date Date last reviewed Next review date Policy lead Contact details Accountable
OLANZAPINE DEPOT PROCEDURE OCTOBER 2017 Policy title Policy reference Policy category Relevant to Date published Implementatio n date Date last reviewed Next review date Policy lead Contact details Accountable
Critical Thinking Steps
 CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
Guidelines for Supervising Residents Updated July 2017
 NORTHWESTERN UNIVERSITY FEINBERG SCHOOL OF MEDICINE DEPARTMENT OF SURGERY POLICIES & PROCEDURES Guidelines for Supervising Residents Updated July 2017 PURPOSE To clearly define the level of patient care
NORTHWESTERN UNIVERSITY FEINBERG SCHOOL OF MEDICINE DEPARTMENT OF SURGERY POLICIES & PROCEDURES Guidelines for Supervising Residents Updated July 2017 PURPOSE To clearly define the level of patient care
Early Management Bundle, Severe Sepsis/Septic Shock
 Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
Early Management Bundle, Severe Sepsis/Septic Shock Audio for this event is available via INTERNET STREAMING. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming
QUALIS HEALTH HONORS WASHINGTON HEALTHCARE PROVIDERS
 LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
Seattle Nursing Research Consortium Abstract Style and Reference Guide
 Seattle Nursing Research Consortium Abstract Style and Reference Guide Page 1 SNRC Revised 7/2015 Table of Contents Content Page How to classify your Project. 3 Research Abstract Guidelines 4 Research
Seattle Nursing Research Consortium Abstract Style and Reference Guide Page 1 SNRC Revised 7/2015 Table of Contents Content Page How to classify your Project. 3 Research Abstract Guidelines 4 Research