VHA Transformation to a Patient Centered Medical Home Model of Care
|
|
|
- Candace Merritt
- 6 years ago
- Views:
Transcription

1 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov 1
2 VHA Mission Honor America s Veterans by providing exceptional health care that improves their health and well-being. 2
3 VHA Vision VHA will continue to be the benchmark of excellence and value in health care and benefits by providing exemplary services that are both patient-centered and evidence-based. This care will be delivered by engaged, collaborative teams in an integrated environment that supports learning, discovery and continuous improvement. It will emphasize prevention and population health and contribute to the Nation s well-being through education, research and service in national emergencies. 3





4 Better Access, Better Care Before Hospital System After Health System Only Hospitals Hospitals Outpatient Clinics Mobile Clinics Vet Centers Mobile Vet Centers My HealtheVet 4
 to transform VA Health Care from a Hospital System to a Health System. VHA currently has 21 VISNs.")

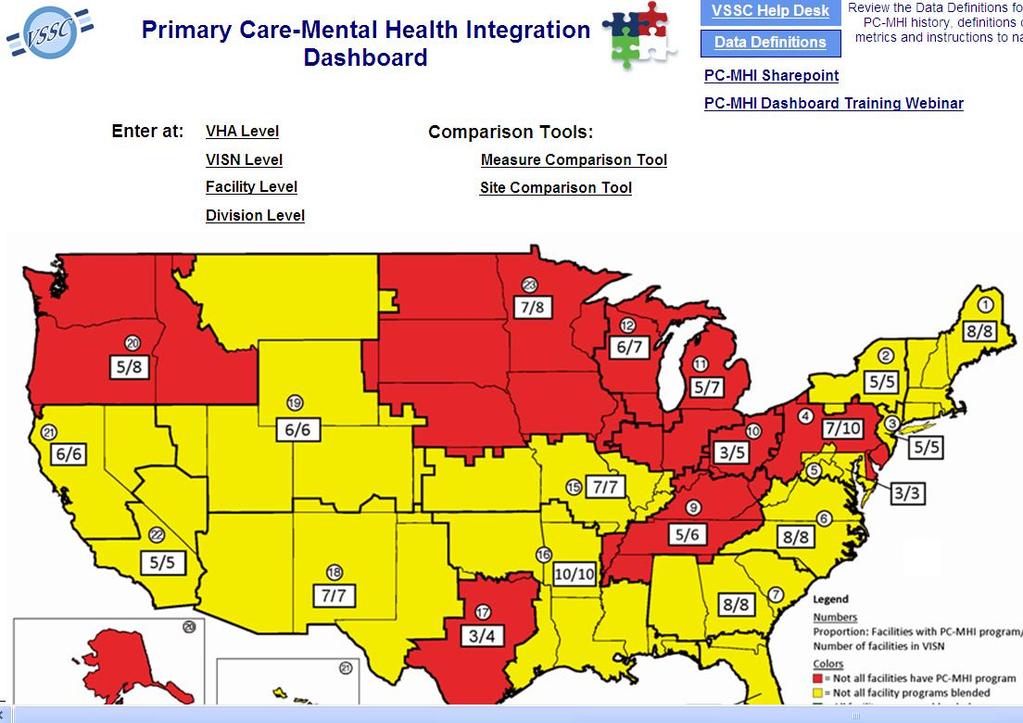
5 Hospital System to Health System In 1996, VA began the creation of Veterans Integrated Service Networks (VISNs) to transform VA Health Care from a Hospital System to a Health System. VHA currently has 21 VISNs. 152 Medical Centers 990 Outpatient Clinics 821 Community-Based 152 Hospital-Based 11 Mobile 6 Independent 300 Vet Centers* 70 Mobile Vet Centers* 102 Domiciliary Residential Rehabilitation Programs 134 Community Living Centers 5



6 VA s Health Care Expertise VA is one of the largest civilian employers in the federal government and one of the largest health care employers in the world. 269,000+ Total VHA Employees 83,000+ Veteran Employees 20,000+ Physicians 69,000+ Nurses* *Includes registered nurses, licensed practical nurses and licensed vocational nurses. 6

7 Million patients Veteran Demographics 44% % Female 21% had encounter in Mental Health 25% 0.0 < up Age 7 Female Male
8 VHA Medical Care Budget $43.9B $47.5B Chart Title $50.9B $53.4B $60.0 $50.0 $40.0 $30.0 $20.0 $10.0 $ Medical Services Medical Support & Compliance Medical Facilities Collections 8
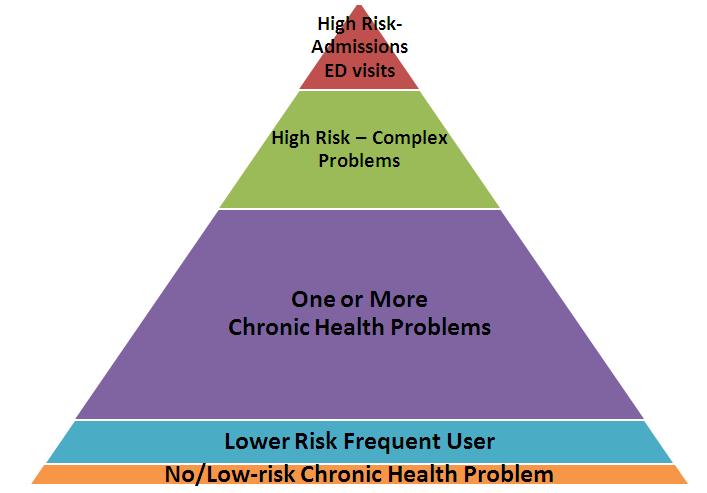
9 VHA costs per capita for top 5% vs. remaining 95% Pharmacy (6%) Top 5% Mean(SD) = $73K($64K) Non VA (10%) NonVA (5%) Remaining 95% Mean(SD) = $4K($5K) Inpatient (9%) Outpatient (26%) Inpatient (58%) Pharmacy (19%) Outpatient (67%) FY2010 data for ~5.2 million VHA patients
10 1993 Under Secretary for Health's Letter, Primary Care as a VHA Priority 1994 Guidance for the Implementation Of Primary Care in VHA 1995 Primary Care in VA Primer 1996 Kizer s Vision for Change and Journey for Change 1998 Guidelines for Implementation of Primary Care 1998 Primary Care Management Module 1999 CPRS (EMR) 2004 Guidance on Primary Care Panel Size 2006 Primary Care Standards 2009 Universal Services Taskforce Report







11 Involving External Subject Matter Experts
12 What the Evidence Indicates: Cost neutral or cost savings (modest) Decreased ED/Urgent Care visits Decreased hospital admissions Increased Primary Care cost and utilization Improved access, patient-centeredness, coordination, safety, and less disparity


13 VA s PACT with Veterans- The journey forward together PACT emphasizes Partnership! 13

14 VHA Patient Aligned Care Teams Comprehensive Services Preventive Health Care Chronic Care Women s Health Urgent Care Mental Health Care Care for High-Risk Patients Population Management Patient Comfort and Pain Management Health Education and Coaching Proactive, Personalized, Patient Driven Health Care Focus 14



15 VHA Patient Aligned Care Teams Implementation Expectations Veterans are less likely to: End up in the hospital End up in the emergency room Miss days from school or work Veterans are more likely to: Have preventive care needs met Have good control of their chronic conditions Say they understand their conditions Receive good help from their practice
16 Using Technology to Implement PACT Computerized Patient Record System Registries PC Almanac Care Management/Coordination Tools Care Assessment Needs Score (CANS) Patient Care Assessment System (PCAS) CPRS templates PACT Compass My HealtheVet & Secure Messaging (Patient Portal) Telehealth telephone store & forward clinical video care E-Consults & project SCAN-ECHO Patient Care Management Module (provider assignment) 16


17 Progress Notes Problem List Orders Consults Vitals Allergy Tracking Pharmacy Lab Radiology Dietetics Clinical Reminders INTEGRATED PATIENT Alerts RECORD SYSTEM Patient Administration VistA Web

18 18

19 Diabetes HTN Ischemic Heart Disease COPD Panel Summary Patient lists by condition with drill down to more information

20 thquality.va.gov/ 20


21 Care Assessment Needs Score (CANS) Tool 21
22
23 Panel Management PRIMARY CARE MANAGEMENT MODULE (PCMM)
 24")

24 Virtual VA e-health University (Web Accessible for All) 24 Exhibit Halls Live Sessions On-Demand Social Media Chats



25 My HealtheVet Overview Veteran s Personal Health Record Self-Service Prescription Refill Access to Labs, Appointments, and Secure Messaging Ability to download Physician Notes and Other content from the Electronic Health Record (EHR) 82 million+ visits 2 million+ registered users 686,000 Veterans have downloaded data 569,000 Veterans use Secure Messaging 36 million prescription refills 25

26 VA Clinical Video Telehealth Programs 148,385 patients treated in 44 clinical specialties in FY 2012 Linked hospital-hospital, and hospitals with clinics using real-time video Clinical enterprise video conferencing network has over 6,600 units Routine outcomes data available at national, regional and local levels Links sites of care using real-time video that interconnects 152 hospitals and 673 Community-Based Outpatient Clinics 93% mean patient satisfaction score Travel cost reduction of $34.45 per consultation Major planned innovations: Tele-audiology Tele-ICU IP Video to the home Services into community living centers 26

27 VA National Home Telehealth Programs Supported care of 119,535 patients in FY 2012 Provides non-institutional care, chronic care management, acute care management and health promotion/disease prevention Routine outcomes data available at national, regional and local levels 42,699 patients supported to live independently in their own homes Reduced bed days of care by 58% Reduced hospital admissions by 38% Mean patient satisfaction score 85% $1,999 per year, per patient cost avoidance Future is to transition services to other information technology platforms 27
28 VA Telemental Health Services VA s telemental health services includes all mental health conditions, with a focus on Post Traumatic Stress Disorder, depression, compensation and pension exams, bipolar disorder, behavioral pain and evidence-based psychotherapy. BY THE NUMBERS 800,000 patients treated since FY fold increase 217,000 telemental health consultations to 76,000 patients in FY ,251 video encounters to 427 patients through the National Telemental Health Center in FY ,100 patients with chronic mental health conditions treated in their homes in FY % reduction in bed days of care as a result of clinical video telehealth 30% planned growth per year, shifting toward in-home IP video-based services 28
29 Reaching Rural Veterans VA estimates approximately 43% of all Veterans live in rural areas. VA continues to expand health access to rural Veterans through: Fee basis care Rural health care partnerships Home-based telehealth Mobile health clinics 29

30 Increasing Rural Access to Specialty Care In many rural and remote areas, Veterans and their primary care providers do not have easy access to specialty care services and expertise. Through VA s SCAN-ECHO* program, Veterans and their primary care team use videoconferencing technology to seek expertise from specialists located miles away. *Scan-Echo: Specialty Care Access Networks-Extension for Community Healthcare Outcomes. 30


31 VA Mobile Applications for Patients and Providers PTSD Coach Patient Viewer Displays EHR data Over 80,000 downloads in 70 countries 31

32 VHA Patient Aligned Care Team Implementation Plan PHASE I: Medical Home Readiness Assessment Baseline Assessment Completed in Oct 2009 Reassess in July 2011 (completed) PHASE II: Build Staffing Infrastructure Staffing Ratio Baseline Completed in Oct 2009 Ongoing PHASE III: Education & Training April 2010 to FY 2014 PHASE IV: Innovation & Evaluation March 2010 to FY 2014 PHASE V: Measurement Ongoing 32

 Provider: 1 FTE RN Care Mgr: 1 FTE Clinical")
 based on staffing, acuity,")
33 Other Team Members Clinical Pharmacy Specialist: ± 3 panels Clinical Pharmacy anticoagulation: ± 5 panels Social Work: ± 2 panels Nutrition: ± 5 panels Case Managers Trainees Integrated Behavioral Health Psychologist ± 3 panels Social Worker ± 5 panels Care Manager ± 5 panels Psychiatrist ± 10 panels Monitored via Primary Care Utilization Data Other Team Members Teamlet: assigned to 1 panel (±1200 patients) Provider: 1 FTE RN Care Mgr: 1 FTE Clinical Associate (LPN, MA, or Health Tech): 1 FTE Clerk: 1 FTE For each parent facility HPDP Program Manager: 1 FTE Health Behavior Coordinator: 1 FTE My HealtheVet Coordinator: 1 FTE Panel size adjusted (modeled) based on staffing, acuity, etc Patient 33


34 PATIENT CENTERED MEDICAL HOME: VHA Patient Aligned Care Team Replaces episodic care based on illness and patient complaints with coordinated care and a long term healing relationship Takes collective responsibility for patient care Is responsible for providing all the patient s health care needs Arranges for appropriate care with other specialties THE PRIMARY CARE TEAM
 Improving Access to Care: Visits with Provider, Team Members, & Non Face to Face Care (telephone, My HealtheVet, Secure Msg) Improving Chronic Illness")
35 Patient Aligned Care Teams Mission Improved Teamwork, Work Design, Maximizing Team Function & Roles Pt Centered Care Improving Care Coordination & Focusing on Critical Transitions of Care (Inpatient to Outpatient, PC to Specialty, VA to Non-VA) Improving Access to Care: Visits with Provider, Team Members, & Non Face to Face Care (telephone, My HealtheVet, Secure Msg) Improving Chronic Illness and Health Promotion/Disease Prevention 35

36 Redesigning Care for Teams: A Typical Primary Care Panel

37 PACT Access and Care Delivery In-person, face to face 1:1 or group visits Non-face to face Telephone, Home Telehealth Virtual faceto-face Clinical Video Telehealth Virtual nonface-to-face Secure messaging


38 PHASE III: Training & Education Collaborative For Trailblazers 5 Regions: 300 Teams 6 Learning Sessions every 3-4 months Comprehensive Start: June 2010 End: FY 2012 Consultation Teams For Special Settings ~25 Site Visits yearly On site evaluation and training By Network/facility request Start: Oct 2010 Ongoing Continuous Improvement Team Based Care Patient Centeredness Learning Centers For Everyone 5 Regions 1250 Teams yearly PACT 101 Start: Fall 2010 Ongoing 38


39 PHASE IV: Innovation & Evaluation Demonstration Laboratories Evaluate the effectiveness and impacts of VHA s PCMH model Apply robust research designs and methods VISN 20 VISN 22 VISN 23 VISN 11 VISN 4 Different practice settings Different geographic locations Develop and test innovative solutions for the core components of the PCMH model Evaluate solutions for effects on Costs Clinical outcomes Patient and provider experience 39

40 PHASE: IV: Innovation & Evaluation Centers of Excellence in Primary Care Education Puget Sound Boise San Francisco Cleveland Connecticut Develop and test innovative approaches to prepare for Primary Care practice in the 21st century Physician residents Students Advanced practice nurse Undergraduate nursing students Associated health trainees Utilize VA primary care settings 40






41 PHASE V Measurement: PACT Process Targets: They will be assigned to an adequately staffed team (3 support staff to 1 provider per panel) They will usually see their own provider 2012 Target 75% When they make an appointment it will be within 7days of when they want or need it 2012 Target 90% Not all their needs require a faceto-face visit but can be handled over the phone, or by Target 20% When they want to see their own provider today, they can frequently do so Target 66% If they are discharged from a VA hospital, someone from their PACT will check on them within 2 days 2012 Target 50% 41
42 PHASE V: Clinical Measurement VHA Primary Care & Private USA Clinical Indicator VA Average Percent Flu Shots for Adults (50-64) na n/a Flu Shots for Adults (65 and older) 3, 4, n/a 69 n/a 2012 (6) (1) HEDIS 2011 (2) Commercial Medicare Medicaid (6) (6) (7) (7) (7) Breast Cancer Screening Cervical Cancer Screening n/a 67 Card Vasc: LDL-C Control (<100 mg/dl) Card Vasc: LDL-C Screening Colorectal Cancer Screening n/a Diabetes Blood Pressure Control (<140/90) Diabetes Eye Exams Diabetes--Annual HbA1c Testing Diabetes LDL-C Controlled (LDL-C<100 mg/dl) Diabetes LDL-C Screening Diabetes Medical Attention for Nephropathy Diabetes- Poor HbA1c Control > Controlling High Blood Pressure - All Pts Advising Smokers To Quit n/a 76 Smoking Cessation - Discussing Medications n/a 44 Smoking Cessation - Discussing Strategies n/a 40 Immunizations: Pneumococcal 3,4, n/a 69 n/a 42

 Face to Face Group")
43 Encounters Millions PACT Workload Trends July 2010 July 2011 July 2012 Total Secure Messages (In+Out) Face to Face Group Telephone

44 PACT Outcome: Admission Rates VHA Acute Admissions per 1000 unique PC patients Represents avoidance of 36,279 admissions July 2010 July 2011 July 2012

45 Visits per 1000 unique PC patients Urgent/Emergent Care VHA Urgent Care VHA ED Represents 21,802 additional visits 0 July 2010 July 2011 July 2012
46 PACT Staff Satisfaction 60% 4 50% 40% 30% 20% 10% Fully staffed Not fully staffed 3.5 0% Burnout Mean Job Satisfaction 3 ***Adequately Staffed Teams Experience Less Burnout and Better Job Satisfaction
47 Effect of Training on PACT Metrics 100% 80% 60% 40% 20% 0% 68% 66% 64% 62% 60% PACT Survey score Untrained Learning Center Collaborative Phone util Same-day Access 2-d post-d/c Continuity 16.5% 16.0% 15.5% 15.0% ED/Urgent Care 14.5% Utilization Rate 14.0% Admission Rate 25% 20% 15% 10% 5% 0% PACT Recognition
48 PACT Training, Burnout and Job Satisfaction 50% 5 45% 40% 35% 30% 25% 20% 15% 10% 5% Training not avail/not involved (14% of respondents) Somewhat or very helpful (66% of respondents) 4 0% Burnout Job Satisfaction 3

49 Patient Satisfaction Based on data Mar-Jul 2012 encounters. N=51,233 responses Coordination Test Follow Up Coordination Med Discuss Coordination Provider Informed Provider Rating 100% 80% 60% 40% 20% 0% Access Communication Comprehensiveness Information Reminder Medication Decisions Information Care After Hours Self Management Office Staff 49






50 PACT Process and Outcome Improvements Overall ACP Medical Home Builder score improved from 69% to 80% Telephone visits increased to over 30% of Primary Care encounters Over 300,000 patients opted in to Secure messaging 90% of patients seen within 7 days of Desired Date Patients see their own provider/team approximately 75% of the time Time to 3rd next available appointment decreased 55% of patients discharged from VHA facilities are contacted by their PACT within 2 days Urgent care visit rates decreased 17% Acute admission rates to VHA facilities decreased by 5%

















51 R E S I D E N T P C P R O V I D E R C L I N I C A L A S S O C I AT E C L E R K RN C A R E M A N A G E R F A M I LY
PACT: The VA s Medical Home
 A5/B5 This presenter has nothing to disclose PACT: The VA s Medical Home What is working to change a big system Mike Davies, MD Director VA Systems Redesign Rich Stark, MD Director VA Primary Care Operations
A5/B5 This presenter has nothing to disclose PACT: The VA s Medical Home What is working to change a big system Mike Davies, MD Director VA Systems Redesign Rich Stark, MD Director VA Primary Care Operations
NATIONAL ACADEMIES COMMITTEE AGENT ORANGE AND HEALTH
 NATIONAL ACADEMIES COMMITTEE AGENT ORANGE AND HEALTH Peter D. Rumm MD, MPH, Director, Pre-9/11 Era Environmental Health Program Post Deployment Health Service, Office of Patient Care Services Veterans
NATIONAL ACADEMIES COMMITTEE AGENT ORANGE AND HEALTH Peter D. Rumm MD, MPH, Director, Pre-9/11 Era Environmental Health Program Post Deployment Health Service, Office of Patient Care Services Veterans
Telehealth in the Veterans Health Administration. Mary C. Foster, DNP, Telehealth Program Manager Mid-Atlantic Health Care Network January 27, 2016
 Telehealth in the Veterans Health Administration Mary C. Foster, DNP, Telehealth Program Manager Mid-Atlantic Health Care Network January 27, 2016 The Vision For Telehealth In VA Patient Focused Makes
Telehealth in the Veterans Health Administration Mary C. Foster, DNP, Telehealth Program Manager Mid-Atlantic Health Care Network January 27, 2016 The Vision For Telehealth In VA Patient Focused Makes
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
My Complete Medications List
 Pharmacy Features 1 My Complete Medications List 2 My HealtheVet: Get Care Get Care: Care Givers Treatment Facilities My Coverage Health insurance Health Calendar To-Do s Wellness Reminders 3 My HealtheVet:
Pharmacy Features 1 My Complete Medications List 2 My HealtheVet: Get Care Get Care: Care Givers Treatment Facilities My Coverage Health insurance Health Calendar To-Do s Wellness Reminders 3 My HealtheVet:
Workflow, Workarounds and Overwork in the Department of Veterans Affairs Problems and Solutions
 Workflow, Workarounds and Overwork in the Department of Veterans Affairs Problems and Solutions Stephan Fihn MD MPH Neil Evans MD Clinton Greenstone MD Austin Frakt PhD November 2017 Veterans Health Administration
Workflow, Workarounds and Overwork in the Department of Veterans Affairs Problems and Solutions Stephan Fihn MD MPH Neil Evans MD Clinton Greenstone MD Austin Frakt PhD November 2017 Veterans Health Administration
The Career Path of a Chief Nursing Officer: The Impact of Nursing Leadership at the Veterans Health Administration Cathy Rick, RN PhD (h), NEA-BC,
, NEA-BC,") The Career Path of a Chief Nursing Officer: The Impact of Nursing Leadership at the Veterans Health Administration Cathy Rick, RN PhD (h), NEA-BC, FACHE, FAAN 1 Conflict of Interest Disclosure Cathy Rick,
The Career Path of a Chief Nursing Officer: The Impact of Nursing Leadership at the Veterans Health Administration Cathy Rick, RN PhD (h), NEA-BC, FACHE, FAAN 1 Conflict of Interest Disclosure Cathy Rick,
September, James Misak, M.D. Linda Stokes, MSPH The MetroHealth System
 Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Better Health Greater Cleveland relies on the presenter to obtain all rights to use and display copyright-protected information. Anyone claiming a right or interest in or to any posted information should
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
HIMSS Davies Enterprise Application --- COVER PAGE ---
 HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
HIMSS Davies Enterprise Application --- COVER PAGE --- Applicant Organization: Hawai i Pacific Health Organization s Address: 55 Merchant Street, 27 th Floor, Honolulu, Hawai i 96813 Submitter s Name:
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
My HealtheVet- Veterans Personal Health Record
 My HealtheVet- Veterans Personal Health Record March 2013 Introduction Brian Vetter R.D. Degree in Dietetics from St. Johns University Clinical dietitian at the St. Cloud VA for 6 years Communication Specialist
My HealtheVet- Veterans Personal Health Record March 2013 Introduction Brian Vetter R.D. Degree in Dietetics from St. Johns University Clinical dietitian at the St. Cloud VA for 6 years Communication Specialist
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
PCMH to ACO: Carilion Clinic s Journey
 PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
PCMH to ACO: Carilion Clinic s Journey Michael P. Jeremiah, MD, FAAFP Chair, Department of Family and Community Medicine Carilion Clinic and the Virginia Tech-Carilion School of Medicine Patient-Centered
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Agenda. NE CAH Region Discussion
 NE CAH Region Discussion Tina Gagner, BSN, RN Clinical Application Analyst Agenda NDHIN Statistics Data Feeds to the HIE Participating Providers Event Notifications Communicate (Direct Secure Messaging)
NE CAH Region Discussion Tina Gagner, BSN, RN Clinical Application Analyst Agenda NDHIN Statistics Data Feeds to the HIE Participating Providers Event Notifications Communicate (Direct Secure Messaging)
Primary Care Redesign Updates to DFM
 Primary Care Redesign Updates to DFM Overview of Care Model Package 2 Care of the Complicated Patient March 5, 2014 Dr. Rich Welnick Susan Marks, Director of Population Health Lori Hauschild, Clinic Operations
Primary Care Redesign Updates to DFM Overview of Care Model Package 2 Care of the Complicated Patient March 5, 2014 Dr. Rich Welnick Susan Marks, Director of Population Health Lori Hauschild, Clinic Operations
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care
 Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
Providing the Highest Quality of Care for the Nation s Veterans
 Providing the Highest Quality of Care for the Nation s Veterans Barbara Fleming, MD, PhD Chief Quality and Performance Officer, Veterans Health Administration Outline Historical Perspective Key Drivers
Providing the Highest Quality of Care for the Nation s Veterans Barbara Fleming, MD, PhD Chief Quality and Performance Officer, Veterans Health Administration Outline Historical Perspective Key Drivers
A How to Guide: Managing Workflows, Developing Protocols, Expanding Roles. November 12, Wisconsin Council on Medical Education & Workforce
 A How to Guide: Managing Workflows, Developing Protocols, Expanding Roles Wisconsin Council on Medical Education & Workforce November 12, 2015 Kathy Kerscher, Team Leader Primary Care Rob MacNeil, Sr.
A How to Guide: Managing Workflows, Developing Protocols, Expanding Roles Wisconsin Council on Medical Education & Workforce November 12, 2015 Kathy Kerscher, Team Leader Primary Care Rob MacNeil, Sr.
St. Johns River Rural Health Network
 St. Johns River Rural Health Network Comprehensive Diabetes Management Presented to: Florida LIP Council January 22, 2009 Nikole Helvey, MS HSA, Network Manager Rural Health Networks In Florida Established
St. Johns River Rural Health Network Comprehensive Diabetes Management Presented to: Florida LIP Council January 22, 2009 Nikole Helvey, MS HSA, Network Manager Rural Health Networks In Florida Established
Disclosures. Platforms for Performance: Clinical Dashboards to Improve Quality and Safety. Learning Objectives
 Platforms for Performance: Clinical Dashboards to Improve Quality and Safety Disclosures The program chair and presenters for this continuing pharmacy education activity report no relevant financial relationships.
Platforms for Performance: Clinical Dashboards to Improve Quality and Safety Disclosures The program chair and presenters for this continuing pharmacy education activity report no relevant financial relationships.
National Survey of Physician Organizations and the Management of Chronic Illness II (Independent Practice Associations)
") If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH STANDARDS. Renewals & Annual Data Requirements
 2014 PCMH STANDARDS Renewals & Annual Data Requirements PCMH Renewal Process Streamlined process for renewal through reduced documentation requirements. Even though some elements do not require documentation,
2014 PCMH STANDARDS Renewals & Annual Data Requirements PCMH Renewal Process Streamlined process for renewal through reduced documentation requirements. Even though some elements do not require documentation,
President Kaiser Permanente Southern California. Great Gains in Quality of Care and Patient Safety: The Kaiser Permanente Experience
 Benjamin K. Chu, MD, MPH President Kaiser Permanente Southern California Great Gains in Quality of Care and Patient Safety: The Kaiser Permanente Experience The triple aim : A blueprint for a more satisfying
Benjamin K. Chu, MD, MPH President Kaiser Permanente Southern California Great Gains in Quality of Care and Patient Safety: The Kaiser Permanente Experience The triple aim : A blueprint for a more satisfying
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
MEANINGFUL USE STAGE FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 MEANINGFUL USE STAGE 2 2014 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives. EPs must meet 3 of the 6 menu measures.
MEANINGFUL USE STAGE 2 2014 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives. EPs must meet 3 of the 6 menu measures.
INTEGRATED CARE SERVICE AND OUTCOMES
 DR. HADAS LEWY INTEGRATED CARE SERVICE AND OUTCOMES 10/8/2014 1 Maccabi Healthcare Services Second largest and fastest growing HMO in Israel ( 25% of Market) Non-profit mutual Recognized health fund -
DR. HADAS LEWY INTEGRATED CARE SERVICE AND OUTCOMES 10/8/2014 1 Maccabi Healthcare Services Second largest and fastest growing HMO in Israel ( 25% of Market) Non-profit mutual Recognized health fund -
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018
 Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned program to be launched
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention
 Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
PCMH Recognition Redesign: Annual Reporting Requirements to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018
 PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
PCMH Recognition Redesign: Annual Reporting to Sustain Recognition Overview & Table Reporting Period: 4/1/2017 3/31/2018 Redesign Goals NCQA is redesigning our PCMH Recognition program. The redesigned
MEANINGFUL USE STAGE 2
 MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Total Worker Health TM
 Total Worker Health TM Promising and Best Practices in the Integration of Occupational Safety and Health Protection with Health Promotion in the Workplace Veterans Health Administration Perspective Kathleen
Total Worker Health TM Promising and Best Practices in the Integration of Occupational Safety and Health Protection with Health Promotion in the Workplace Veterans Health Administration Perspective Kathleen
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
SHORTAGES IN MENTAL HEALTH COVERAGE 10/31/2016. CPE Information and Disclosures. Learning Objectives. CPE Information
 CPE Information and Disclosures Mental Health Clinical Pharmacy Specialists Meeting the Increasing Need for Mental Health Professionals Cynthia A. Gutierrez, PharmD, MS, BCPP Clinical Pharmacy Program
CPE Information and Disclosures Mental Health Clinical Pharmacy Specialists Meeting the Increasing Need for Mental Health Professionals Cynthia A. Gutierrez, PharmD, MS, BCPP Clinical Pharmacy Program
Module 1 Program Description
 Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
FirstHealth Moore Regional Hospital. Implementation Plan
 FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
FirstHealth Moore Regional Hospital Implementation Plan FirstHealth Moore Regional Hospital Implementation Plan For 2016 Community Health Needs Assessment Summary of Community Health Needs Assessment Results
Improving the Health of Our Patients and Our Communities:
 Jason Jones, PhD Executive Director Kaiser Permanente, Southern California Patti Harvey, RN, MPH, CPHQ Senior Vice President Kaiser Permanente, Southern California Improving the Health of Our Patients
Jason Jones, PhD Executive Director Kaiser Permanente, Southern California Patti Harvey, RN, MPH, CPHQ Senior Vice President Kaiser Permanente, Southern California Improving the Health of Our Patients
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018
 Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
Improving Quality Outcomes in a Risk-Based World: A Davies Story Session #100, March 7, 2018 David Cloyed, MS, RN-BC, Applications Manager, Nebraska Medicine Tammy Winterboer, PharmD, BCPS, Director, Clinical
The Virtual Connection: Electronic Visits. Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009
 The Virtual Connection: Electronic Visits Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009 The Holy Grail of Health Care 2009 Cost Reduction Quality Improvement Service Improvement
The Virtual Connection: Electronic Visits Joseph E. Scherger, MD, MPH National Medical Home Summit March 3, 2009 The Holy Grail of Health Care 2009 Cost Reduction Quality Improvement Service Improvement
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
1 Title Improving Wellness and Care Management with an Electronic Health Record System
 HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc.
 Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Care Redesign and Quality Improvement. Beth Averbeck, MD Senior Medical Director, Primary Care HealthPartners Medical Group
 Care Redesign and Quality Improvement Beth Averbeck, MD Senior Medical Director, Primary Care HealthPartners Medical Group Consumer-governed, non-profit HealthPartners Medical Group Primary Care: 500,000
Care Redesign and Quality Improvement Beth Averbeck, MD Senior Medical Director, Primary Care HealthPartners Medical Group Consumer-governed, non-profit HealthPartners Medical Group Primary Care: 500,000
Innovative Coordinated Care Models
 Innovative Coordinated Care Models Rachel Post, LCSW Policy Director Central City Concern Rachel Solotaroff, MD, MCR Medical Director Central City Concern 1 May 2014 Central City Concern: Who we are Providing
Innovative Coordinated Care Models Rachel Post, LCSW Policy Director Central City Concern Rachel Solotaroff, MD, MCR Medical Director Central City Concern 1 May 2014 Central City Concern: Who we are Providing
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Marshfield Clinic Health System MSSP Track I ACO Experience
 Marshfield Clinic Health System MSSP Track I ACO Experience Narayana S Murali MD FACP EVP Care Delivery & Chief Clinical Strategy Officer, MCHS President/CEO MCHS Hospitals Inc. Executive Director, Marshfield
Marshfield Clinic Health System MSSP Track I ACO Experience Narayana S Murali MD FACP EVP Care Delivery & Chief Clinical Strategy Officer, MCHS President/CEO MCHS Hospitals Inc. Executive Director, Marshfield
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff
 Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
Ontario Shores Journey to EMRAM Stage 7. October 21, 2015
 Ontario Shores Journey to EMRAM Stage 7 October 21, 2015 ICE BREAKER Agenda System overview & pervasiveness of use Review Clinical Practice Guideline implementation Discuss Patient Portal implementation
Ontario Shores Journey to EMRAM Stage 7 October 21, 2015 ICE BREAKER Agenda System overview & pervasiveness of use Review Clinical Practice Guideline implementation Discuss Patient Portal implementation
Informatics, PCMHs and ACOs: A Brave New World
 Informatics, PCMHs and ACOs: A Brave New World R. Clark Campbell, MSN, RN-BC, CPHIMS, FHIMSS Kathleen Kimmel, RN, BSN, MHA, CPHIMS, FHIMSS Engagement Executive with Health Catalyst Objectives - Define
Informatics, PCMHs and ACOs: A Brave New World R. Clark Campbell, MSN, RN-BC, CPHIMS, FHIMSS Kathleen Kimmel, RN, BSN, MHA, CPHIMS, FHIMSS Engagement Executive with Health Catalyst Objectives - Define
California Pay for Performance: A Case Study with First Year Results. Tom Williams Integrated Healthcare Association (IHA) March 17, 2005
 March 17, 2005") California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future
 Paul Grundy MD, MPH IBM Director, Healthcare Transformation Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future @Paul_PCPCC 2015 IBM Corporation 1 https://www.youtube.com/watch?v=uy088yyq6ua
Paul Grundy MD, MPH IBM Director, Healthcare Transformation Foundation for New Jersey Healthcare Transformation The Patient Centered Medical Home the Future @Paul_PCPCC 2015 IBM Corporation 1 https://www.youtube.com/watch?v=uy088yyq6ua
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012
 A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
Minnesota Perspective: Fairview Health Services. National Accountable Care Organization Congress October 25, 2010
 Minnesota Perspective: Fairview Health Services National Accountable Care Organization Congress October 25, 2010 Fairview Overview Not-for-profit organization established in 1906 Partner with the University
Minnesota Perspective: Fairview Health Services National Accountable Care Organization Congress October 25, 2010 Fairview Overview Not-for-profit organization established in 1906 Partner with the University
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Making the Medical Home Work/Teamwork in Primary Care. Amy Mullins, MD Trinity Clinic Whitehouse
 Making the Medical Home Work/Teamwork in Primary Care Amy Mullins, MD Trinity Clinic Whitehouse Objectives Objectives Include: 1. Learn how to build your office team. 2. Understand various ways to use
Making the Medical Home Work/Teamwork in Primary Care Amy Mullins, MD Trinity Clinic Whitehouse Objectives Objectives Include: 1. Learn how to build your office team. 2. Understand various ways to use
My HealtheVet. Institute of Medicine Roundtable on Health Literacy Workshop on Health Literacy, ehealth, and Communication: Putting the Consumer First
 My HealtheVet Institute of Medicine Roundtable on Health Literacy Workshop on Health Literacy, ehealth, and Communication: Putting the Consumer First Kim Nazi, FACHE Veterans Health Administration March
My HealtheVet Institute of Medicine Roundtable on Health Literacy Workshop on Health Literacy, ehealth, and Communication: Putting the Consumer First Kim Nazi, FACHE Veterans Health Administration March
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
Joy At Work - BellinHealth and HealthPartners
 Joy At Work - BellinHealth and HealthPartners Restoring Joy in Practice through Team Based Care IHI December 2016 James Jerzak M.D. Kathy Kerscher Bellin Health Green Bay, Wisconsin 1 Agenda Crisis Emerging
Joy At Work - BellinHealth and HealthPartners Restoring Joy in Practice through Team Based Care IHI December 2016 James Jerzak M.D. Kathy Kerscher Bellin Health Green Bay, Wisconsin 1 Agenda Crisis Emerging
Mitzi Cardenas Sr. VP/Strategy, Business Development and Technology Truman Medical Centers
 Mitzi Cardenas Sr. VP/Strategy, Business Development and Technology Truman Medical Centers HIMSS Stage 7: What it Means Heart of America HIMSS and the Missouri Health Information Management Association
Mitzi Cardenas Sr. VP/Strategy, Business Development and Technology Truman Medical Centers HIMSS Stage 7: What it Means Heart of America HIMSS and the Missouri Health Information Management Association
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
VHA Preventive Care Program. Clinician/Educator Programs
 Behavioral Medicine Careers in the VA Health Care System: Clinician/Educator Positions Michael Goldstein, MD, Associate Chief Consultant for Preventive Medicine Margaret (Peg) Dundon, PhD, National Program
Behavioral Medicine Careers in the VA Health Care System: Clinician/Educator Positions Michael Goldstein, MD, Associate Chief Consultant for Preventive Medicine Margaret (Peg) Dundon, PhD, National Program
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost
 Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Meaningful Use and Care Transitions: Managing Change and Improving Quality of Care
 Small Rural Hospital Transition (SRHT) Project HELP Webinar Meaningful Use and Care Transitions: Managing Change and Improving Quality of Care Paul Kleeberg, MD, FAAFP, FHIMSS Aledade Medical Director
Small Rural Hospital Transition (SRHT) Project HELP Webinar Meaningful Use and Care Transitions: Managing Change and Improving Quality of Care Paul Kleeberg, MD, FAAFP, FHIMSS Aledade Medical Director
University of California, Davis Family Practice Center: Update 2014
 University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
University of California, Davis Family Practice Center: Update 2014 by Lisel Blash, Catherine Dower, and Susan Chapman September 2014 Center for the Health Professions at UCSF ABSTRACT In response to long
UPMC Telehealth Program. Leveraging Advances in Technology to Transform Healthcare Delivery through New Models of Care
 UPMC Telehealth Program Leveraging Advances in Technology to Transform Healthcare Delivery through New Models of Care UPMC s Telehealth Expansion Pediatric Specialty Inpatient Dermatology Pre & Post Operative
UPMC Telehealth Program Leveraging Advances in Technology to Transform Healthcare Delivery through New Models of Care UPMC s Telehealth Expansion Pediatric Specialty Inpatient Dermatology Pre & Post Operative
2011 Measures 2013 Objectives Goal is to guide and support care processes and care coordination
 Improve quality, safety, efficiency, and reduce health disparities Provide access to comprehensive patient health data for patient s health care team Use evidencebased order sets and CPOE Apply clinical
Improve quality, safety, efficiency, and reduce health disparities Provide access to comprehensive patient health data for patient s health care team Use evidencebased order sets and CPOE Apply clinical